
Oxygenation
Study Questions
Practice Exercise 1
A client with chronic pulmonary disease has a bluish tinge around the lips. The nurse charts which term to most accurately describe the client’s condition?
Explanation
Central cyanosis manifests as a bluish discoloration of the mucous membranes and perioral skin due to an absolute increase in deoxygenated hemoglobin levels exceeding 5 g/dL. This clinical sign indicates significant hypoxemia or pulmonary shunting, often necessitating immediate arterial blood gas analysis to assess oxygenation status and ventilation. In chronic pulmonary disease, chronic hypoxia leads to compensatory polycythemia, which can paradoxically make cyanosis more clinically apparent despite marginal oxygen saturation levels.
Rationale for correct answer
4. Cyanosis describes the physical finding of a bluish tinge around the lips caused by excessive desaturated hemoglobin in the capillaries. It is a specific clinical observation rather than a systemic physiological state or subjective symptom. Diagnosis requires visual confirmation of the integumentary and mucosal surfaces.
Rationale for incorrect answers
1. Hypoxia refers to a deficiency in tissue oxygenation at the cellular level which may not be visible. While it often accompanies a bluish tinge, it describes a functional deficit rather than the physical color change. It is an internal physiological state.
2. Hypoxemia refers specifically to a low partial pressure of oxygen or oxygen saturation within the arterial blood supply. Although it is the primary cause of central discoloration, it represents a laboratory value rather than a visible physical assessment finding. It requires blood gas verification.
3. Dyspnea describes the subjective sensation of shortness of breath or labored breathing reported by the patient. While frequently observed in chronic pulmonary disease, it is a symptom of respiratory distress rather than a visible blue discoloration. It reflects the patient's perceived breathing effort.
Test-taking strategy
- Identify the nature of the data: Distinguish between subjective symptoms, objective physiological states, and physical assessment findings. The question asks for a term to describe a visible “bluish tinge,” which is a physical sign.
- Analyze terminology:
- Eliminate 3 (Dyspnea) because it is a subjective feeling of breathing difficulty, not a color change.
- Differentiate between 1 (Hypoxia) and 2 (Hypoxemia); both are internal physiological conditions (cellular vs. arterial) and cannot be directly seen without diagnostic tools.
- Select 4 (Cyanosis) as it is the specific medical descriptor for the visual manifestation of blue-tinted skin or membranes.
- Apply clinical definitions: Remember that cyanosis is the only term in the list that refers to the visual inspection of skin color. Using the process of elimination based on assessment types (inspection vs. palpation vs. reporting) leads directly to the correct descriptor for charting.
Take home points
- Cyanosis is clinically detectable when the concentration of reduced hemoglobin in the subpapillary venous plexus exceeds 5 g/dL.
- Central cyanosis affecting the lips and tongue indicates a systemic decrease in arterial oxygenation rather than local vasoconstriction.
The nurse makes the assessment that which client has the greatest risk for a problem with the transport of oxygen from the lungs to the tissues? A client who has
Explanation
Oxygen transport relies on the physiological capacity of hemoglobin to bind and carry molecular oxygen through the systemic circulation. This process, termed convection, is dependent on adequate erythrocyte concentration and functional heme groups to satisfy metabolic demands. In states of reduced red blood cell mass, the carrying capacity of the blood is severely diminished, leading to cellular hypoxia despite normal pulmonary ventilation and atmospheric oxygen tension.
Rationale for correct answer
1. This condition involves a quantitative or qualitative deficiency in hemoglobin, which is the primary vehicle for moving oxygen to distal cells. Without sufficient binding sites, the blood cannot effectively transport oxygen, regardless of how well the lungs are functioning. It represents a direct failure of the blood's delivery system.
Rationale for incorrect answers
2. While a systemic inflammatory response increases metabolic oxygen demand, it does not inherently impair the primary mechanical or chemical transport of oxygen molecules. The body usually compensates through increased cardiac output and respiratory rate to meet the needs of the tissues. It is a demand issue, not a transport failure.
3. This injury primarily affects the mechanical phase of ventilation by causing pain and guarding, which limits chest wall expansion and tidal volume. While it can lead to secondary hypoxemia due to alveolar hypoventilation, it does not interfere with the blood's ability to carry oxygen once it enters the stream. It is a restrictive ventilatory defect.
4. The brainstem houses the primary respiratory centers that regulate the involuntary drive to breathe and maintain rhythmic ventilation. Damage here results in a failure of respiratory drive, leading to apnea or irregular breathing patterns, which is a ventilatory failure. It does not affect the circulatory transport of oxygen once gas exchange has occurred.
Test-taking strategy
- Analyze the question stem: Focus on the specific phrase “transport of oxygen from the lungs to the tissues.” This is a physiological hint pointing toward the circulatory system and blood components.
- Differentiate respiratory phases:
- Rule out 3 and 4 because they are ventilation problems (getting air into the lungs).
- Rule out 2 because it is a metabolic demand problem (using oxygen at the tissue site).
- Identify the vehicle: Recognize that hemoglobin is the “bus” for oxygen. If you have Anemia, you have fewer “buses” available to transport the oxygen to its destination.
- Match pathology to step: Always match the patient's condition to the specific step of respiration (ventilation, diffusion, transport, or cellular utilization) mentioned in the question.
Take home points
- Oxygen transport is primarily determined by the hemoglobin concentration and the cardiac output.
- Ventilation involves the movement of air into and out of the lungs, whereas transport involves the delivery of oxygen via the blood.
A nurse observes a client experiencing shortness of breath when lying down who must assume an upright or sitting position to breathe more comfortably and effectively. What should the nurse document?
Explanation
Positional respiratory distress is often a manifestation of increased venous return and pulmonary congestion when the body is in a recumbent position. This physiological phenomenon occurs as fluid shifts from the lower extremities to the thoracic compartment, increasing pulmonary capillary wedge pressure. Patients often utilize accessory muscles and gravity to decrease the work of breathing and improve diaphragmatic excursion by maintaining an upright posture.
Rationale for correct answer
3. Orthopnea describes respiratory distress that occurs when the patient is in a supine position and is relieved by sitting or standing. It is a classic clinical marker for congestive heart failure or advanced chronic obstructive pulmonary disease. Precise documentation of this finding is vital for tracking fluid volume status.
Rationale for incorrect answers
1. Dyspnea is a general term for any subjective sensation of labored breathing or air hunger regardless of the patient's physical position. While the patient in the scenario is experiencing this, it is not the most specific term for the positional nature of the distress. It lacks the descriptive precision required for this assessment.
2. Hyperpnea refers to an increased depth and rate of ventilation, often seen during exercise or as a compensatory response to metabolic acidosis. It describes the character of the breathing pattern rather than the relationship between breathing ease and the patient's posture. It is a description of respiratory effort and volume.
4. Acapnea signifies a condition of diminished carbon dioxide levels in the arterial blood, typically resulting from hyperventilation. It describes a biochemical state rather than a physical symptom or a positional requirement for comfortable breathing. It is the opposite of hypercapnia and is not related to the scenario.
Test-taking strategy
- Keywords in stem: Look for “lying down” and “upright or sitting position.” These are the defining characteristics of a positional breathing disorder.
- Eliminate general terms: While Option 1 (Dyspnea) is technically true, the NCLEX and medical boards require the most specific answer. Orthopnea specifically addresses the positional component.
- Define Suffixes and Prefixes:
- “Ortho-” relates to straight or upright.
- “A-” means without (Acapnea).
- “Hyper-” means excessive (Hyperpnea).
- Select the Clinical Descriptor: Choice 3 is the standard clinical term used in nursing documentation to describe a patient who needs multiple pillows or a chair to breathe effectively at night.
Take home points
- Orthopnea is frequently quantified by the number of pillows a patient requires to sleep comfortably.
- The physiological cause is often the redistribution of fluid into the lungs when the effect of gravity on the lower extremities is removed.
A client has a fractured rib and is breathing less often and with less depth because of the pain. The nurse would document this finding using which term?
Explanation
Alveolar ventilation is the process by which gas exchange occurs between the atmosphere and the pulmonary capillaries to maintain homeostatic blood gas levels. When a patient experiences thoracic trauma, pain-induced splinting leads to a reduction in tidal volume and respiratory frequency. This physiological state, known as hypoventilation, results in the retention of carbon dioxide and a subsequent decrease in arterial oxygen saturation, potentially leading to respiratory acidosis.
Rationale for correct answer
4. Hypoventilation accurately describes a respiratory state characterized by inadequate alveolar gas exchange due to decreased rate and depth of breathing. In the context of a rib fracture, the patient limits chest expansion to minimize pain, which directly results in this clinical finding. It is the specific descriptor for the ventilation deficit described.
Rationale for incorrect answers
1. Fremitus refers to the palpable vibration transmitted through the chest wall when a patient speaks, usually assessed during physical examination. It is a tool for detecting lung consolidation rather than a term for a breathing pattern or rate.
2. Hyperventilation signifies a state of ventilation that exceeds metabolic demands, characterized by rapid or deep breathing that lowers arterial pCO2. The client in the scenario is doing the opposite by breathing less often and with less depth. It would lead to respiratory alkalosis, not the state described.
3. Pleural friction rub is an adventitious breath sound produced by the inflammation of the visceral and parietal layers of the lung lining. While it can occur with chest trauma, it is an auscultatory finding (a sound) rather than a term describing the rate or depth of the respiratory cycle. It is identified via stethoscope.
Test-taking strategy
- Define the prefix: Use linguistic roots to identify the correct term. “Hypo-” means below or deficient, while “Hyper-” means above or excessive.
- Match symptoms to definitions:
- “Less often” - decreased rate.
- “Less depth” - decreased volume.
- Decreased rate + Decreased depth = Hypoventilation.
- Eliminate unrelated assessments:
- Rule out 1 (Fremitus) as it is a tactile assessment of vibration.
- Rule out 3 (Rub) because it is a sound, not a pattern of breathing.
- Focus on the “why”: The patient is splinting because of pain. Splinting always leads to hypoventilation because the patient is afraid to take a deep breath.
Take home points
- Hypoventilation leads to an increase in partial pressure of arterial carbon dioxide (PaCO2).
- Pain management is a primary nursing intervention to improve ventilation in patients with thoracic injuries.
A nurse is aware that abdominal breathing at 30 to 60 breaths/minute with an irregular pattern of rate and depth would closely describe the breathing patterns of what age group?
Explanation
Neonatal and infantile respiratory physiology is characterized by a reliance on the diaphragm as the primary muscle of inspiration, resulting in distinct abdominal wall excursions. This age group exhibits a high metabolic oxygen demand and a compliant chest wall, leading to a rapid baseline respiratory rate that typically ranges from 30 to 60 breaths per minute. Furthermore, the immature neurological control of breathing often produces periodic breathing, which is a normal finding of irregular rate and depth in healthy neonates.
Rationale for correct answer
2. The respiratory rate of 30 to 60 breaths per minute is the standard normative range for a newborn or young infant. The inclusion of an irregular pattern and abdominal movement confirms this developmental stage, as infants are obligate nose breathers with immature respiratory centers. This is a hallmark physiological observation for this demographic.
Rationale for incorrect answers
1. The respiratory rate for an aged adult should remain within the normal range of 12 to 20 breaths per minute unless pathology is present. While some elderly patients may have altered breathing patterns due to chronic disease, a rate of 60 is a sign of critical respiratory failure. It is not a descriptive norm for this group.
3. By early childhood, the respiratory rate typically slows to a range of 20 to 30 breaths per minute as lung capacity increases. While these children still use abdominal muscles more than adults, the rate and irregularity described are significantly higher than expected for a toddler or preschooler. It would indicate respiratory distress.
4. In late childhood and adolescence, the respiratory rate further declines toward the adult standard of 14 to 20 breaths per minute. The breathing pattern becomes more thoracic and regular as the skeletal system matures and the diaphragm becomes less dominant. A rate of 30 to 60 would be highly abnormal and life-threatening.
Test-taking strategy
- Identify the numerical range: Focus on 30 to 60 breaths/minute. In nursing, this high rate is only normal for the neonatal/infant period.
- Match technique to development:
- Adults/Children: Mostly thoracic breathing.
- Infants: Abdominal breathing (diaphragmatic).
- Evaluate the pattern: Irregular is a major clue; periodic breathing of the newborn is a well-known physiological phenomenon.
- Eliminate outliers: Rule out 1, 3, and 4 because a rate of 60 in any of those groups constitutes a medical emergency (tachypnea) rather than a descriptive norm.
Take home points
- Newborns often exhibit brief pauses in breathing (less than 10 to 15 seconds) known as periodic breathing.
- The infant's respiratory rate should be counted for a full minute due to the inherent irregularity of the rhythm.
Practice Exercise 2
The nurse assists the client with coughing and deep-breathing exercises to prevent postoperative complications. This is best accomplished by implementing which of the following?
Explanation
Effective pulmonary hygiene in the postoperative phase focuses on maintaining alveolar patency and promoting the clearance of secretions. Surgical anesthesia and analgesia often suppress the cough reflex and reduce tidal volume, leading to atelectasis and potential pneumonia. Utilizing a controlled expiration technique minimizes airway collapse and reduces the physical strain on surgical incisions while ensuring optimal gas exchange.
Rationale for correct answer
3. This technique uses low-pressure exhalation to move secretions into larger airways without the high intrathoracic pressure of forceful coughing. Performing it every 2 hours ensures pulmonary clearance while preventing significant fatigue or incisional dehiscence in the recovering patient. It is the most effective routine for secretion management.
Rationale for incorrect answers
1. Separating these exercises based on meal times is clinically inefficient and lacks physiological justification for preventing complications like atelectasis. Respiratory interventions must be frequent and consistent rather than scheduled around gastric emptying or nutritional intake. This timing would allow for prolonged periods of lung stasis.
2. Vigorous, uncontrolled coughing can cause excessive pain, increase thoracic pressure, and lead to the collapse of small airways. It places unnecessary stress on surgical sites and may cause the patient to avoid further respiratory exercises due to discomfort. Controlled techniques are always preferred over forceful efforts.
4. While these techniques improve ventilation and oxygenation, the frequency of four times a day is insufficient for preventing postoperative pneumonia. Postoperative protocols require more frequent intervention, typically every 1 to 2 hours, to maintain lung expansion and prevent the accumulation of stagnant secretions. The dosage is inadequate for high-risk patients.
Test-taking strategy
- Prioritize Frequency and Safety: In postoperative care, the “gold standard” for respiratory interventions is frequency. Most protocols require interventions every 1 to 2 hours while the patient is awake to prevent stasis.
- Evaluate Technique: Compare the mechanical impact of each cough type.
- Rule out 2 because “forceful” and “as many times as tolerated” can lead to exhaustion and injury.
- Rule out 1 because meal-based scheduling is arbitrary and does not address the constant risk of alveolar collapse.
- Rule out 4 because, while the technique is good, the frequency (4 times a day) is too low for acute postoperative prevention.
- Select the Evidence-Based Option: Huff coughing (forced expiratory technique) is the recognized standard for moving secretions without causing airway collapse, and the 2-hour interval aligns with standard nursing protocols for pulmonary hygiene.
Take home points
- Huff coughing utilizes an open glottis to create pressure gradients that move mucus toward the trachea safely.
- Frequent repositioning and respiratory exercises every 1 to 2 hours are critical to prevent the development of hypostatic pneumonia.
A client with emphysema is prescribed corticosteroid therapy on a short-term basis for acute bronchitis. The client asks the nurse how the steroids will help him. The nurse responds by saying that the corticosteroids will do which of the following?
Explanation
Glucocorticoids function by inhibiting the synthesis of pro-inflammatory mediators and reducing the migration of leukocytes to the bronchial mucosa. This pharmacological action stabilizes the lysosomal membranes and decreases capillary permeability, effectively reducing mucosal edema and mucus hypersecretion. In obstructive pulmonary diseases, these agents attenuate the hyperresponsiveness of the airways to triggers, thereby improving the diameter of the bronchial lumen and facilitating air movement.
Rationale for correct answer
4. The primary therapeutic effect of steroids in the respiratory tract is the reduction of airway edema and inflammation. By dampening the immune response, the drug minimizes the swelling that narrows the passages during an acute exacerbation of bronchitis. This directly targets the underlying pathophysiology of the obstruction.
Rationale for incorrect answers
1. Unlike beta-2 agonists, corticosteroids do not exert a direct effect on the smooth muscle to cause immediate relaxation or expansion. While they facilitate better airflow over time by reducing swelling, they are not classified as bronchodilators in a pharmacological sense. They do not provide rapid rescue relief.
2. Steroids do not act as expectorants or mucolytics to directly assist the mechanical act of coughing. While a decrease in inflammation may eventually lead to less mucus production, the drug's mechanism is not designed to stimulate the cough reflex or clear secretions. It is an anti-inflammatory, not a mechanical aid.
3. Corticosteroids are actually immunosuppressive and can potentially mask or increase the risk of developing a secondary infection. They do not have antimicrobial properties and are administered alongside antibiotics if an infection is present. Their goal is to manage the inflammatory response, not kill pathogens.
Test-taking strategy
- Identify drug class: Recognize that corticosteroid is synonymous with anti-inflammatory.
- Distinguish mechanism of action:
- Rule out 1 because bronchodilation is the role of adrenergics/anticholinergics.
- Rule out 3 because steroids actually suppress the immune system rather than preventing infection.
- Match pathology to treatment: In emphysema and bronchitis, the narrowing of the airway is caused by both muscle constriction and tissue swelling. Steroids specifically address the swelling (inflammation).
- Focus on the “Why”: When a patient asks how a drug helps, the nurse should explain the primary physiological impact. Decreasing inflammation is the most accurate and scientific explanation for steroid use in respiratory distress.
Take home points
- Corticosteroids reduce the production of cytokines and chemokines that drive airway inflammation.
- In chronic lung disease, systemic steroids are typically reserved for acute exacerbations to avoid long-term side effects.
When auscultating a client’s breath sounds, the nurse detects a continuous, musical sound heard on expiration. The nurse identifies this sound as which of the following?
Explanation
Adventitious lung sounds are abnormal acoustic signals superimposed over the normal breath sounds, indicating underlying pathophysiology of the airways or parenchyma. High-pitched, musical vibrations are generated when air is forced through constricted or partially obstructed lumens. This phenomenon typically occurs during expiration when the intrathoracic pressure naturally narrows the bronchioles, further compressing the already restricted air passages.
Rationale for correct answer
2. Wheezes are continuous, high-pitched musical sounds produced by air flowing through narrowed small airways. They are hallmark signs of bronchospasm, mucosal edema, or excessive secretions commonly found in asthma or chronic obstructive pulmonary disease. The description in the stem perfectly matches this clinical finding.
Rationale for incorrect answers
1. Crackles are discontinuous, popping sounds heard primarily during inspiration when collapsed alveoli or small airways snap open. They are often associated with fluid in the air spaces or interstitial edema, rather than a musical or continuous vibration. They are often described as sounding like Velcro or hair rubbing together.
3. Bronchial sounds are normal, loud, high-pitched sounds heard specifically over the trachea and mainstem bronchi. While they are loud, they are not musical or adventitious and represent the normal turbulence of air in large conduits. Finding them in peripheral lung fields would be abnormal, but the description does not fit.
4. Pleural friction rub is a dry, creaking, or grating sound caused by the rubbing together of inflamed pleural surfaces during the respiratory cycle. It is not musical in nature and is often compared to the sound of two pieces of leather rubbing together. It usually ceases when the patient holds their breath.
Test-taking strategy
- Identify key descriptors: Focus on continuous and musical. These two words are classic medical jargon specifically reserved for describing wheezes.
- Differentiate timing:
- Wheezes are most common on expiration.
- Crackles are most common on inspiration.
- Analyze the sound character:
- Musical - Wheeze.
- Popping/Bubbling - Crackle.
- Grating - Friction Rub.
- Eliminate normal findings: Rule out 3 (Bronchial sounds) because the question implies an abnormal finding detected during assessment, and bronchial sounds are normal only in specific locations.
Take home points
- Wheezing is a physical sign of increased airway resistance and reduced airflow.
- Monophonic wheezes suggest a single obstructed airway, while polyphonic wheezes suggest widespread bronchoconstriction.
A nurse is aware that air that develops in the pleural space is referred to as:
Explanation
The pleural space is a potential cavity between the visceral and parietal pleurae maintained at a negative pressure to ensure lung inflation. Pathological accumulation of atmospheric air within this space disrupts the surface tension and vacuum, leading to partial or complete pulmonary collapse. This condition, known as a pneumothorax, can result from blunt trauma, spontaneous alveolar rupture, or iatrogenic injury during thoracentesis or central line placement.
Rationale for correct answer
1. Pneumothorax specifically identifies the presence of air within the pleural cavity that causes lung collapse. It is the correct medical nomenclature derived from the Greek word for air or breath. Management often requires the insertion of a chest tube to evacuate the air and restore negative pressure.
Rationale for incorrect answers
2. Pleural effusion refers to the abnormal accumulation of fluid, such as transudate or exudate, within the pleural space rather than air. While it also compresses the lung tissue and impairs ventilation, the physical state of the matter is liquid. It is often secondary to heart failure or malignancy.
3. Hemothorax describes the presence of blood in the pleural space, typically following thoracic trauma or vascular rupture. It is a distinct clinical entity that requires drainage to prevent clot formation and fibrothorax. The density of blood is significantly different from the air described in the stem.
4. Atelectasis is a condition of alveolar collapse within the lung parenchyma itself, not the accumulation of a substance in the pleural space. It occurs when the small air sacs become deflated or filled with alveolar fluid. It is an internal lung tissue problem rather than a pleural space issue.
Test-taking strategy
- Differentiate pleural content:
- Air - Pneumothorax.
- Blood - Hemothorax.
- Fluid - Pleural effusion.
- Distinguish location: Recognize that 1, 2, and 3 are pleural problems (outside the lung), while 4 (Atelectasis) is a parenchymal problem (inside the lung).
- Focus on the question: The stem is a direct definition question. Matching the substance “air” to the prefix “pneumo-” provides the most efficient path to the correct choice.
Take home points
- A tension pneumothorax is a life-threatening emergency where air enters the pleural space but cannot escape, shifting the mediastinum.
- Clinical signs of pneumothorax include sudden chest pain, dyspnea, and diminished breath sounds on the affected side.
A nurse is teaching a client about pulse oximetry. Which statement would the nurse most likely include in the discussion?
Explanation
Pulse oximetry is a non-invasive technology that utilizes spectrophotometry to determine the percentage of hemoglobin saturated with oxygen. The device emits red and infrared light through a peripheral vascular bed, measuring the absorption differences between oxygenated and deoxygenated hemoglobin. This assessment provides a continuous real-time estimation of arterial oxygenation, allowing for the rapid detection of hypoxemia before clinical signs such as cyanosis become visible.
Rationale for correct answer
1. A saturation level (SpO2) between 95% and 100% represents the standard physiological objective for most healthy individuals. This range indicates that the majority of hemoglobin binding sites are occupied by oxygen molecules, ensuring adequate tissue perfusion. It is the fundamental baseline used in clinical assessment.
Rationale for incorrect answers
2. Pulse oximetry specifically measures arterial oxygen saturation by detecting the pulsatile flow of blood in the capillaries. It does not measure venous blood, which has significantly lower oxygen levels after oxygen has been unloaded at the tissue level. The “pulse” in the name refers to the arterial beat.
3. This is a non-invasive, external procedure that does not require any pre-test restrictions or dietary modifications. It is a bedside tool used for immediate assessment and does not involve the laboratory processing or blood draws associated with fasting requirements. It can be performed at any time.
4. While useful for monitoring, oximetry cannot measure pH, partial pressure of carbon dioxide (pCO2), or bicarbonate levels. Therefore, it is a supplement to, but not a replacement for, arterial blood gas analysis when a complete acid-base assessment is required. It provides a limited picture of respiratory status.
Test-taking strategy
- Analyze the technology: Remember that pulse oximeters look for pulsatile flow, which is only found in arteries. This eliminates Option 2.
- Determine clinical utility: Recognize that while SpO2 is helpful, it is incomplete compared to an ABG. Option 4 is incorrect because a replacement would imply it provides identical data, which it does not.
- Evaluate practicality: Oximetry is used in every hospital room every few hours; if fasting were required (Option 3), it would be impossible to use as a routine vital sign.
- Select the standard: Option 1 is the classic medical definition of normative oxygen saturation, making it the most likely teaching point for a client.
Take home points
- Factors such as fingernail polish, cold extremities, and carbon monoxide poisoning can cause inaccurate pulse oximetry readings.
- Pulse oximetry (SpO2) is an estimate of arterial oxygen saturation (SaO2) and usually correlates within 2%.
Practice Exercise 3
The nurse is preparing to perform tracheostomy care. Prior to beginning of the procedure the nurse performs which action?
Explanation
Tracheostomy management involves maintaining a patent airway while preventing stoma infection and accidental decannulation. The procedure involves manipulating a bypass of the upper airway, which can be physically and psychologically distressing for the patient who is temporarily unable to speak. Establishing a communication method is a critical safety intervention to address potential hypoxia or respiratory distress during the care process.
Rationale for correct answer
1. Establishing a non-verbal signal allows the client to communicate respiratory distress or pain during a procedure where they cannot vocalize. This promotes patient safety and reduces anxiety by providing the client a sense of control over the intervention. It must occur before beginning the sterile portion of care.
Rationale for incorrect answers
2. Replacing the securing mechanism is one of the final steps of tracheostomy care and should not be performed prematurely. Doing this prior to cleaning increases the risk of accidental decannulation if the tube is not properly stabilized during the entire process. Security is a priority throughout the procedure.
3. Cleaning the peristomal area is a core component of the procedure itself, not a preparatory action. Performing this before the setup and communication plan violates the sterile sequence and logical flow of nursing interventions. It follows the assessment and preparation of the patient.
4. Assessing the tension of the ties is part of the ongoing assessment and final stabilization, but it does not take precedence over establishing emergency communication. While ensuring the knot is secure is important, the nurse must first ensure the patient can signal for help. Assessment of ties occurs after the new ties are applied.
Test-taking strategy
- Identify the phase of care: The question asks for an action “prior to beginning” the procedure. This indicates a preparatory or assessment step.
- Prioritize communication: In any procedure where the patient's airway is involved or their ability to speak is compromised, establishing a signal is the highest priority for safety and psychological support.
- Eliminate procedure steps:
- Rule out 2 and 3 as these are parts of the actual procedure, not pre-procedural preparation.
- Rule out 4 because checking the ties is a secondary assessment; the primary pre-procedure action for a conscious patient is ensuring they can communicate a life-threatening feeling of distress.
- Apply safety principles: The nurse must use the nursing process to prepare the environment and the patient. Setting up a signal for pain or distress is a fundamental safety protocol for any airway-related task.
Take home points
- Non-verbal communication techniques are essential for patients with artificial airways to prevent panic and ensure safety during care.
- Tracheostomy ties should always be secured with enough space to allow one or two fingers to fit between the tie and the neck.
A nurse is preparing to perform suctioning for a client. Which action by the nurse represents proper nasopharyngeal/ nasotracheal suction technique?
Explanation
Nasopharyngeal and nasotracheal suctioning involves the mechanical aspiration of secretions from the lower airway to maintain patency and optimize alveolar gas exchange. The procedure carries significant risks of trauma, cardiac arrhythmias, and severe hypoxemia if the technique is improper. Utilizing a rotational motion during the withdrawal phase ensures that the catheter tip clears all surfaces of the airway wall, maximizing secretion removal while minimizing localized tissue injury.
Rationale for correct answer
3. Rotating the catheter during withdrawal prevents the suction tip from adhering to the respiratory mucosa, which can cause localized invagination and trauma. This maneuver ensures a comprehensive aspiration of secretions from all aspects of the internal airway lumen. It is a standard safety requirement for effective suctioning.
Rationale for incorrect answers
1. Using oil-based lubricants like petroleum jelly is contraindicated because it poses a significant risk for lipid pneumonia if aspirated into the lungs. Only water-soluble lubricants should be utilized to facilitate the passage of the catheter through the nasal turbinates. Petroleum products can also damage the catheter material.
2. Suction must never be applied during the insertion phase as it causes mucosal damage and depletes the patient's oxygen reserves prematurely. The catheter should be advanced carefully without suction until the carina or a cough reflex is reached. Suction is only activated during the withdrawal phase.
4. While pre-oxygenation is essential, doing so for 30 minutes is clinically excessive and can lead to oxygen toxicity or absorption atelectasis. Standard protocols recommend hyperoxygenation with 100% oxygen for only 30 to 60 seconds immediately prior to and after the procedure. Prolonged exposure is unnecessary and potentially harmful.
Test-taking strategy
- Identify contraindicated materials: Recognize that petroleum-based products (Option 1) are never used in the airway due to the risk of aspiration pneumonia; always look for water-soluble.
- Distinguish insertion vs. withdrawal: In suctioning questions, the rule is always “no suction on insertion” to prevent tissue damage and hypoxia. This immediately eliminates Option 2.
- Evaluate timeframes: Analyze the 30-minute timeframe in Option 4. In acute care, 30 minutes is an eternity; hyperoxygenation is a brief, targeted intervention to create an oxygen reserve.
- Focus on Technique: Rotation is the specific mechanical action required to ensure the catheter does not grab the delicate tracheal lining while pulling out secretions.
Take home points
- Suction should be applied intermittently or continuously for no longer than 10 to 15 seconds to prevent severe hypoxemia.
- Nasotracheal suctioning is a sterile procedure requiring a surgical aseptic technique to prevent the introduction of pathogens into the lower tract.
A nurse is educating a client about incentive spirometry. Which client statement informs the nurse that his teaching about the proper use of an incentive spirometer was effective?
Explanation
Incentive spirometry is a mechanical intervention designed to facilitate sustained voluntary hyperinflation of the lungs to prevent or treat respiratory complications. The primary goal is to increase transpulmonary pressure and inspiratory volumes, thereby re-expanding collapsed alveoli and improving surfactant production. Proper technique emphasizes slow, deep inspiration rather than forceful expiration to ensure the even distribution of air throughout the lung parenchyma.
Rationale for correct answer
2. Effective use requires a slow, controlled inhalation to create the negative pressure necessary to lift the indicator. This technique ensures maximal alveolar expansion and allows the nurse to visualize the patient's inspiratory capacity during the exercise. It promotes the physiological goals of lung re-expansion.
Rationale for incorrect answers
1. This statement describes the technique for peak flow meters, not incentive spirometry. Exhaling forcefully into the device is a misapplication of the tool and does not contribute to the goal of lung expansion. It may lead to dizziness or unnecessary physical exertion without clinical benefit.
3. Using the device only three times a day is clinically insufficient for a postoperative or immobilized patient. Standard protocols typically mandate using the spirometer 5 to 10 times every hour while awake. Infrequent use allows for the progression of atelectasis and stasis.
4. Proper hygiene for the device focuses on the mouthpiece, which should be cleaned after each use. While the device should be kept clean, the weekly washing of the entire device is not the priority of patient education regarding its therapeutic function. Clinical effectiveness is the primary teaching focus.
Test-taking strategy
- Identify the physiological goal: Distinguish between devices that measure expiration (peak flow) and those that encourage inspiration (incentive spirometry). The goal here is inhalation.
- Evaluate frequency: In nursing questions regarding pulmonary hygiene, three times a day is rarely the correct frequency; interventions like turning, coughing, and deep breathing are almost always hourly.
- Analyze the cation:
- Eliminate 1 because it describes an expiratory effort.
- Eliminate 3 due to the inadequate frequency.
- Eliminate 4 as it focuses on maintenance rather than the correct technique for the educational objective.
- Select the best evidence of learning: Option 2 correctly identifies the slow and steady inhalation required to reach a target volume and maintain alveolar patency.
Take home points
- Incentive spirometry encourages patients to take long, slow, deep breaths to maximize lung inflation.
- Patients should be instructed to hold their breath for at least 3 seconds at the end of inhalation to allow for collateral ventilation.
A client with chest tubes is ambulating. The connection between the tube and the water seal dislodges. Which action by the nurse is most appropriate?
Explanation
A chest tube drainage system maintains the negative intrapleural pressure necessary for lung expansion by creating a one-way valve. If the connection to the water seal is lost, the negative pressure is compromised, placing the patient at immediate risk for an atypical or tension pneumothorax. Immediate restoration of the closed-circuit system is the priority to prevent atmospheric air from entering the pleural space and causing lung collapse.
Rationale for correct answer
2. The nurse's immediate priority is to restore the integrity of the closed system to prevent air from being sucked into the pleural space. Rapidly reconnecting the tube minimizes the volume of atmospheric air that can enter the chest during inspiration. This action addresses the acute safety risk of lung collapse.
Rationale for incorrect answers
1. While returning the client to bed is eventually necessary, it is a secondary action that does not address the immediate threat to the airway. Allowing the client to walk with an open pleural space increases the risk of rapid respiratory decompensation. Reconnection must happen at the site of the incident.
3. Auscultation of lung sounds is an important assessment, but it should be performed after the system has been secured. Delaying the repair of the drainage system to perform an assessment allows more air to enter the pleural space, potentially worsening the client's condition. Intervention takes priority over assessment in this emergency.
4. Forcing the client to cough while the tube is disconnected can exacerbate the loss of negative pressure and increase the risk of air entering the chest. While coughing helps expel air in a functional system, it is dangerous when the system is open to the atmosphere. It is an inappropriate and harmful instruction in this context.
Test-taking strategy
- Prioritize the Emergency: This is a critical safety question where the integrity of a life-support system has been breached. The priority is to stop the leak.
- Apply the nursing process (Modified): While assessment usually comes first, in situations where an intervention is needed to prevent immediate harm (like a disconnected chest tube), you must act.
- Evaluate options:
- Rule out 1 because it delays the solution.
- Rule out 3 because assessment while the hole is still open is counterproductive.
- Rule out 4 because coughing with an open tube can be physiologically detrimental.
- Focus on restoration: The most appropriate action is the one that immediately restores negative pressure and stabilizes the patient's respiratory status by reattaching the water seal.
Take home points
- If the drainage system breaks or is disconnected, the nurse should place the end of the tube in sterile water to create a temporary water seal.
- If the chest tube is accidentally pulled out of the patient, the site must be covered immediately with an occlusive dressing taped on three sides.
The nurse is planning to perform percussion and postural drainage. Which is an important aspect of planning the client’s care?
Explanation
Postural drainage and percussion involve the utilization of gravity and mechanical kinetic energy to mobilize secretions from the peripheral lung segments toward the central airways. The procedure requires specific positioning of the patient to allow segmental bronchi to drain into the trachea for expectoration. Timing is a critical planning factor to prevent regurgitation and optimize the patient's respiratory effort throughout the day.
Rationale for correct answer
1. Performing these maneuvers before meals prevents emesis and aspiration that may occur if the stomach is full during head-down positioning. Additionally, clearing the airways before eating reduces fatigue, allowing the patient to tolerate the physical exertion of a meal. It maximizes both safety and nutritional intake.
Rationale for incorrect answers
2. The logical sequence of pulmonary hygiene must begin with positioning to allow gravity to start the drainage process before applying percussion. Suctioning or coughing should be the final step to remove the secretions that have been mobilized to the upper airways. The suggested order is mechanically inefficient.
3. Performing these exercises immediately after breakfast significantly increases the risk of aspiration due to the Trendelenburg or side-lying positions required. The mechanical jarring of percussion on a full stomach can induce nausea and vomiting. Timing should always favor an empty stomach for comfort and safety.
4. Hyperoxygenation is typically reserved for invasive procedures like tracheal suctioning and is not a standard requirement for chest physiotherapy. While monitoring oxygen saturation is important, a 3-minute delivery of 100% oxygen is an excessive and non-standard intervention for this procedure. It is not supported by routine clinical protocols.
Test-taking strategy
- Prioritize safety (Aspiration risk): Any procedure involving positioning or percussion carries a risk of vomiting if done after a meal. This makes before meals the safest choice.
- Analyze the sequence: Think of the procedure as “moving the fluid.” You must position the patient first to use gravity, then use percussion to vibrate the secretions loose, and finally have them cough or suction them out.
- Identify excessive interventions: 100% oxygen (Option 4) is a high-level intervention. Always question if such an extreme measure is necessary for a non-invasive procedure like drainage.
Take home points
- Postural drainage should be avoided for at least 2 hours after meals to minimize the risk of gastroesophageal reflux.
- Percussion is performed by cupping the hands to create an air cushion, avoiding the spine and internal organs.
- Each position in postural drainage should be maintained for approximately 10 to 15 minutes to allow for effective gravity flow.
Comprehensive Questions
A nurse is planning care for a client with chronic lung disease who is receiving oxygen through a nasal cannula. What does the nurse expect?
Explanation
Patients with advanced chronic obstructive pulmonary disease often develop a compensatory reliance on hypoxemic drive for respiratory regulation. In these individuals, the central chemoreceptors become desensitized to chronic hypercapnia, leaving low arterial oxygen levels as the primary stimulus for ventilation. Administering high concentrations of supplemental oxygen can inadvertently suppress this respiratory drive, leading to carbon dioxide narcosis and acute respiratory failure.
Rationale for correct answer
2. Maintaining a low flow rate, typically 2 L/min or less, prevents the suppression of the patient's natural stimulus to breathe. It provides enough supplemental oxygen to treat hypoxemia without causing a dangerous rise in arterial pCO2. This reflects the standard safety protocol for managing chronic CO2 retainers.
Rationale for incorrect answers
1. While humidification is beneficial for comfort, it is generally not required for low-flow nasal cannulas at rates of 4 L/min or less. It is a comfort measure rather than an expected safety requirement for chronic lung disease management. The priority in this scenario is the flow rate itself.
3. Drawing arterial blood gases every 4 hours is an invasive and unnecessary frequency for a stable client on a nasal cannula. Monitoring is typically performed using non-invasive pulse oximetry once a baseline has been established. Frequent punctures increase the risk of vascular trauma and infection without providing continuous data.
4. Delivering oxygen at 6 L/min or more is contraindicated for most patients with chronic hypercapnia because it may abolish their drive to breathe. High-flow rates through a cannula can also be drying and irritating to the nasal mucosa. It exceeds the safe therapeutic window for this specific patient population.
Test-taking strategy
- Identify the patient population: Chronic lung disease (like COPD) is a major red flag in oxygen therapy questions. These patients are almost always CO2 retainers.
- Apply the hypoxic drive rule: In CO2 retainers, high oxygen is dangerous. Look for the lowest effective dose.
- Evaluate practicality:
- Rule out 3 because q4h blood gases are only for the most critically ill ICU patients.
- Rule out 4 because 6 L/min is the maximum for a cannula and is too high for this population.
- Focus on standard practice: 2 L/min is the classic starting rate for chronic lung disease to ensure safety and maintain the respiratory drive.
Take home points
- The goal of oxygen therapy in chronic lung disease is often an oxygen saturation (SaO2) between 88% and 92%.
- Nasal cannulas are low-flow systems that deliver an inspired oxygen fraction (FiO2) of approximately 24% to 44%.
A nurse is caring for a client who is breathing spontaneously. Which oxygen delivery device would the nurse expect to use to provide the highest concentration of oxygen to this client?
Explanation
High-concentration oxygen delivery systems utilize a reservoir bag and one-way valves to achieve a high fractional inspired oxygen (FiO2) concentration. This configuration prevents the entrainment of ambient air and the rebreathing of exhaled carbon dioxide, ensuring the patient inspires almost pure oxygen. In a spontaneously breathing patient with severe hypoxemia, this device is the final step in non-invasive respiratory support before progressing to positive pressure ventilation or endotracheal intubation.
Rationale for correct answer
2. Nonrebreather mask is equipped with a reservoir and two one-way valves that allow for the delivery of an FiO2 between 60% and 90%. It is the only non-invasive system capable of providing the highest concentration of oxygen to a patient who is still breathing on their own. It is used in acute emergencies to rapidly stabilize saturation levels.
Rationale for incorrect answers
1. A partial rebreather allows the first third of exhaled air to enter the reservoir, resulting in a maximum oxygen concentration of approximately 60%. It lacks the one-way valve system required to prevent the dilution of inspired oxygen with exhaled gases and room air. It provides significantly less oxygen than a nonrebreather.
3. The simple face mask delivers oxygen concentrations ranging from 35% to 50% at flow rates of 6 to 12 L/min. It depends heavily on the fit of the mask and the patient's inspiratory flow rate, making it a low-to-moderate delivery device. It cannot achieve the high concentrations needed in critical respiratory distress.
4. Venturi mask is designed for precision rather than high concentration, using different-sized orifices to provide a fixed FiO2. While it is excellent for patients requiring controlled oxygen levels, its maximum output is typically capped at 50%. It is used for accuracy in chronic lung disease, not for maximum oxygenation.
Test-taking strategy
- Identify the objective: The question asks for the highest concentration. This is a superlative that points toward a device with a reservoir and one-way valves.
- Compare percentages:
- Simple mask: ~40%
- Venturi mask: ~50%
- Partial rebreather: ~60%
- Nonrebreather: ~90%
- Apply logic of design: The “non” in nonrebreather means the patient is not rebreathing anything but the oxygen from the bag, which logically leads to the highest concentration.
- Eliminate low-flow: Rule out 3 and 4 immediately as they are designed for routine or precise delivery rather than emergency hyperoxygenation.
Take home points
- The reservoir bag on a nonrebreather mask must be kept at least one-third to one-half full during inhalation to ensure adequate delivery.
- One-way valves on the mask's side ports prevent room air from entering during inspiration.
A nurse is performing oropharyngeal suctioning on a client. Which action would the nurse include?
Explanation
Oropharyngeal suctioning is the mechanical removal of secretions from the posterior pharynx to maintain airway patency and prevent aspiration. The procedure is indicated when a patient is unable to clear oral debris through coughing or swallowing, which can lead to stertorous respirations or respiratory distress. Maintaining catheter patency is essential during the procedure to ensure the vacuum pressure remains effective for the removal of thick or tenacious mucus.
Rationale for correct answer
3. The nurse must rinse the catheter with sterile water or normal saline between passes to clear the lumen of accumulated secretions. This ensures that subsequent suctioning attempts are not hindered by clogged tubing and maintains a clean interface for the procedure. It is a fundamental step in catheter maintenance.
Rationale for incorrect answers
1. While oropharyngeal suctioning is not strictly a sterile procedure like endotracheal suctioning, modern hospital protocols generally require sterile technique to prevent the introduction of pathogens. Using only clean technique (non-sterile gloves) is often considered inadequate in an acute care setting where the risk of cross-contamination is high. Standard practice prioritizes aseptic precautions.
2. Suction should never be applied during the insertion of the catheter, as this can cause unnecessary trauma to the oral mucosa and deplete the patient's oxygen. The nurse must only engage the suction port while withdrawing the catheter. This follows universal safety principles for all suctioning procedures.
4. Suctioning for 25 to 30 seconds is excessively long and can lead to severe hypoxemia and vagal stimulation. The maximum duration for a single suction pass should be limited to 10 to 15 seconds to allow for adequate recovery and oxygenation. Prolonged intervals increase the risk of cardiac arrhythmias.
Test-taking strategy
- Prioritize safety timing: Remember the 10 to 15 second rule for all suctioning. Option 4 (25-30 seconds) is a dangerous distractor that could cause harm.
- Evaluate procedure flow:
- Rule out 2 because suction on insertion is always incorrect.
- Rule out 1 because sterile is a higher standard of care than clean in the airway, and NCLEX-style questions usually favor the highest safety standard.
- Identify maintenance needs: Think about the physical reality of the task; if you suck up thick mucus, the tube will get blocked. Option 3 is the logical solution to maintain the tool's function.
- Match technique to anatomy: Oropharyngeal involves the mouth and throat; flushing between passes keeps the path clear for effective pulmonary hygiene.
Take home points
- Oropharyngeal suctioning should be performed only when clinically indicated by the presence of visible or audible secretions.
- The nurse should encourage the patient to cough and deep breathe between suctioning passes to facilitate oxygenation.
A nurse is educating a client about inhalers. Effective use of a metered-dose inhaler requires that the client accomplish which action?
Explanation
Metered-dose inhalers (MDIs) are pressurized canisters that deliver a precise dose of aerosolized medication directly to the lower respiratory tract. The efficacy of the therapy depends on the deposition of the drug into the bronchioles rather than the oropharyngeal cavity. Proper coordination of actuation and inhalation ensures that the medication bypasses the upper airway and reaches the targeted receptors for maximum therapeutic effect.
Rationale for correct answer
3. Holding the breath for 5 to 10 seconds allows the medication particles to settle onto the respiratory mucosa through sedimentation. This pause prevents the immediate exhalation of the drug and ensures the active ingredients reach the smaller airways. It is a critical step for maximizing drug absorption.
Rationale for incorrect answers
1. The client must breathe in through the mouth to ensure a direct and unobstructed path for the aerosol to enter the trachea. Breathing through the nose acts as a filter and traps the majority of the medication in the nasal passages. Mouth breathing is essential for lower airway delivery.
2. Patients should only inhale one spray per breath to ensure the medication is properly distributed and the dosage is accurate. Inhaling two sprays simultaneously increases the likelihood of the drug hitting the back of the throat and being swallowed. Most prescriptions specify a waiting period of 1 minute between puffs.
4. Exhaling quickly prevents the medication from reaching the distal alveoli and staying there long enough to work. The correct technique involves a slow, controlled exhalation through pursed lips after the breath-hold. Quick exhalation significantly reduces the amount of medication that remains in the lungs.
Test-taking strategy
- Visualize the goal: The goal of an inhaler is to get medicine down deep and make it stay there.
- Evaluate the options for “deep” and “stay”:
- Rule out 1 (Nose) because it filters out the medicine.
- Rule out 4 (Quick exhale) because it blows the medicine back out.
- Rule out 2 (Two sprays) because it causes “clumping” in the throat.
- Select the most logical retention method: Holding the breath (Option 3) is the only action listed that helps the medicine stay in the lungs to be absorbed.
- Focus on timing: The 5 to 10 second hold is a classic educational benchmark for MDI training.
Take home points
- Using a spacer or holding chamber can significantly improve the delivery of medication to the lungs for patients with poor coordination.
- Patients should wait 1 to 2 minutes between puffs of the same medication to allow the first dose to begin bronchodilation.
A client has chronic obstructive pulmonary disease (COPD). The nurse has taught the client that pursed-lip breathing helps them by:
Explanation
Pursed-lip breathing is a therapeutic maneuver used to manage the mechanical consequences of expiratory airflow limitation. In chronic obstructive pulmonary disease, the loss of elastic recoil leads to the premature collapse of small airways during exhalation. By creating positive back-pressure at the lips, this technique splints the bronchioles open, allowing for a more complete emptying of the alveoli and improving the efficiency of the respiratory cycle.
Rationale for correct answer
4. This technique generates a resistive pressure that prevents the bronchiolar collapse typically seen in obstructive disease. By keeping the airways patent longer, it facilitates the removal of trapped air, thereby reducing residual volume and work of breathing. It is a primary strategy for managing dyspnea in stable and acute phases.
Rationale for incorrect answers
1. The objective of respiratory therapy in this population is to facilitate the clearance of carbon dioxide, not to increase it. Elevated carbon dioxide levels lead to respiratory acidosis and can suppress the neurological drive to breathe in chronic retainers. Inducing hypercapnia would be physiologically detrimental to the patient.
2. The goal of this maneuver is to prolong expiration and shorten the inspiratory phase relative to the total cycle. Extending the expiratory time allows more air to leave the lungs, addressing the hyperinflation characteristic of the disease. Shortening expiration would worsen air trapping and increase respiratory distress.
3. Pursed-lip breathing is a mechanical ventilation strategy and has no chemical or physical effect on the viscosity of mucus. Methods to liquefy secretions include systemic hydration, humidification, and the administration of mucolytic pharmacological agents. It does not assist with the mobilization of thick sputum.
Test-taking strategy
- Identify the primary defect: In COPD/Emphysema, the problem is air trapping. The correct answer must address exhalation.
- Evaluate pressure mechanics: Pursed lips act like a valve. Think about how back-pressure would help a floppy tube (bronchiole) stay open.
- Eliminate harmful options:
- Rule out 1 because increasing CO2 is never the goal for a COPD patient.
- Rule out 2 because you want a longer exhale to get the trapped air out.
- Match technique to outcome: Decreasing air trapping (Option 4) is the direct result of keeping those airways open with positive pressure.
Take home points
- Pursed-lip breathing should be performed by inhaling through the nose and exhaling through the mouth as if whistling.
- The exhalation phase should be at least twice as long as the inhalation phase to maximize air clearance.
A client develops sudden cardiac arrest. It is imperative to begin CPR as soon as possible. What is the critical time that the nurse must keep in mind before irreversible brain damage occurs?
Explanation
Sudden cardiac arrest results in the immediate cessation of systemic perfusion, depriving the cerebral cortex of essential oxygen and glucose. The brain possesses negligible metabolic reserves and relies on continuous arterial flow to maintain cellular integrity. Once circulation stops, a cascade of biochemical failure begins, leading to neuronal death and permanent functional deficits if oxygenation is not restored within a very narrow ischemic window.
Rationale for correct answer
3. Clinical evidence indicates that the brain can typically survive without oxygenation for a maximum of 4 to 6 minutes before cells begin to die. Beyond this threshold, the likelihood of biological death and irreversible neurological damage increases exponentially. This timeframe underscores the urgency of immediate cardiopulmonary resuscitation and defibrillation.
Rationale for incorrect answers
1. While starting CPR within this timeframe is ideal and results in the highest survival rates, irreversible damage usually has not occurred yet. The first 3 minutes represent the “golden period” where resuscitation is most likely to result in full neurological recovery. It is a safe zone, not the limit.
2. This range is also within the window where cerebral function can often be fully restored if perfusion is resumed. While every second counts, the threshold for permanent cellular destruction is generally considered to be slightly longer than 4 minutes. It represents a period of high urgency.
4. By the time 8 to 10 minutes have elapsed without circulation, the vast majority of patients will have suffered profound and permanent brain damage. Survival at this point is rare, and those who are resuscitated often remain in a persistent vegetative state. This timeframe is far beyond the window of safety.
Test-taking strategy
- Identify the physiological threshold: The 4-to-6-minute window is a classic medical fact used in Basic Life Support (BLS) training.
- Analyze the consequences:
- Under 4 minutes: High chance of recovery.
- 4 to 6 minutes: Damage begins to become permanent.
- Over 10 minutes: Brain death is highly likely.
- Eliminate extremes:
- Rule out 1 and 2 as being too early for irreversible damage.
- Rule out 4 as being too late (damage has already happened).
- Focus on the limit: The question asks for the critical time before damage occurs, which is the tipping point identified in Choice 3.
Take home points
- Early high-quality chest compressions maintain a small but vital amount of blood flow to the brain and heart.
- For every minute that passes without CPR and defibrillation, the chance of survival decreases by approximately 7% to 10%.
A client is in the hospital with a medical diagnosis of viral pneumonia. They are receiving oxygen through a simple face mask. The nurse ensures that the mask fits snugly over the client’s face for which reason?
Explanation
Simple face masks act as a reservoir for supplemental oxygen, increasing the fractional inspired oxygen (FiO2) concentration above atmospheric levels. In viral pneumonia, inflammation and exudate within the interstitial spaces impair the diffusion of gases across the alveolar-capillary membrane. A secure fit is necessary to prevent the entrainment of ambient room air, which would dilute the oxygen concentration and diminish the therapeutic efficacy of the delivery system.
Rationale for correct answer
4. Ensuring a snug fit prevents the leakage of oxygen and the unintentional inhalation of room air around the edges of the mask. This maintenance of the seal ensures that the client receives the prescribed concentration of oxygen required to manage the hypoxemia caused by pneumonia. It is essential for consistent clinical outcomes.
Rationale for incorrect answers
1. While preventing movement can reduce friction, a “snug” fit that is too tight can actually increase the risk of pressure injuries over the bridge of the nose and cheeks. The primary reason for a secure fit relates to the gas concentration rather than the integrity of the integumentary system. Skin care is a separate nursing priority.
2. Many patients find a tight-fitting mask to be a source of anxiety or claustrophobia rather than security. The psychological comfort of the patient is not the scientific justification for the physical fit of an oxygen delivery device. Clinical effectiveness takes precedence over the subjective feeling of mask tightness.
3. The design of a simple mask includes exhalation ports to allow for the clearance of carbon dioxide. The goal of oxygen therapy is to improve oxygenation, not to promote the retention of CO2, which could lead to respiratory acidosis. Retention of waste gases is a complication to be avoided, not a goal.
Test-taking strategy
- Identify the Primary Goal: The goal of any oxygen mask is to deliver the correct concentration of oxygen to the lungs.
- Analyze the Impact of Air: Room air is only 21% oxygen. If the mask is loose, the patient breathes in room air, which dilutes the 40% to 60% oxygen coming from the mask.
- Eliminate Physiological Errors: Rule out 3 immediately; the nurse never wants to “maintain” CO2 retention in a pneumonia patient.
- Focus on Efficacy: Choice 4 is the most “scientific” and “results-oriented” answer, focusing on the accuracy of the medical intervention.
Take home points
- A simple face mask requires a minimum flow rate of 5 to 6 L/min to prevent the rebreathing of carbon dioxide.
- Viral pneumonia can cause ventilation-perfusion mismatching, necessitating supplemental oxygen to maintain saturation above 92%.
- The nurse must assess the skin under the mask and over the ears every 2 to 4 hours for signs of pressure.
- Simple masks can deliver an FiO2 of 35% to 50% depending on the flow rate and the patient's inspiratory demand.
A nurse suctioning a client through a tracheostomy tube was careful not to occlude the Y port when inserting the suction catheter because this would do which of the following?
Explanation
Tracheal suctioning involves the mechanical removal of secretions from the lower respiratory tract using a sub-atmospheric vacuum pressure. The tracheal lining is composed of delicate, ciliated columnar epithelium that is highly susceptible to mechanical injury and desiccation. Engaging the suction during the insertion phase causes the catheter tip to adhere to and invaginate the mucosal tissue, leading to localized hemorrhage and edema.
Rationale for correct answer
2. Applying suction during insertion causes the catheter tip to grab the mucosal lining, leading to significant tissue trauma and potential bleeding. This injury can compromise the protective barrier of the airway and increase the risk of infection or scarring. Suction must remain off until the catheter is being withdrawn.
Rationale for incorrect answers
1. Occluding the Y port actually activates the suctioning process rather than preventing it. If the port is covered, the vacuum is directed through the distal tip of the catheter. The nurse avoids this during insertion specifically because they do not want suction to occur at that time.
3. Breaking sterile technique is a result of the catheter touching non-sterile surfaces, not the timing of suction application. While maintaining asepsis is critical, the specific act of occluding the Y port is a mechanical control of pressure, not a violation of the sterile field. Contamination is a separate procedural error.
4. While suctioning does remove some oxygen and gases, it is impossible to suction out “all” the carbon dioxide from the pulmonary system. The primary danger of early suctioning is not gas removal, but the mechanical damage to the anatomical structures of the trachea. The focus remains on preventing tissue injury.
Test-taking strategy
- Rule of Suctioning: Always remember the universal rule: No suction on insertion.
- Identify the Outcome of the Error: If you violate the rule and apply suction while pushing the tube down, the tube will stick to the walls of the throat.
- Select the Most Specific Damage: Stickiness + Movement = Trauma. Choice 2 is the standard medical explanation for why we keep the port open during insertion.
- Analyze the Y-Port Mechanism: Understand that covering the hole (occluding the port) starts the vacuum. Therefore, “not occluding” means keeping the vacuum off.
Take home points
- The suction catheter should be inserted only as far as the pre-measured length or until the cough reflex is elicited.
- Applying suction only during withdrawal (in a rotating motion) protects the integrity of the tracheal mucosa.
- Suction pressure should be set between 80 and 120 mmHg for adults to provide effective clearance without excessive force.
- Pre-oxygenating the patient before suctioning helps mitigate the transient hypoxia that occurs when air is removed from the lungs.
A nurse is preparing to administer oxygen to a client. Which action does the nurse use to follow safe technique when using a portable oxygen cylinder?
Explanation
Oxygen cylinders are high-pressure vessels containing compressed medicinal gas that require strict regulatory compliance and safety protocols to prevent catastrophic failure or fire. The maintenance of adequate volume is a clinical priority to ensure that oxygen delivery is not interrupted during patient transport or in emergency settings. Proper management involves assessing the pressure gauge to verify that the remaining gas is sufficient for the intended duration of use based on the flow rate.
Rationale for correct answer
1. Verifying the available pressure on the regulator is a fundamental safety action to ensure the cylinder will not run out during use. A full cylinder typically registers 2,000 psi, and the nurse must calculate if the remaining amount is adequate for the patient's needs. This prevents the life-threatening cessation of oxygen therapy during transport.
Rationale for incorrect answers
2. A cylinder containing only 500 psi is generally considered near empty and should not be used for patient transfers. Standard safety protocols require replacing the tank when it reaches 500 psi to provide a safety margin against total depletion. Using such a low-pressure tank increases the risk of the patient losing their oxygen supply mid-transport.
3. Placing an unsecure cylinder directly on a stretcher next to a patient is a significant safety hazard because the tank could fall or the valve could shear. If a pressurized valve is damaged, the cylinder can become a dangerous projectile. Tanks must be secured in a designated rack or the specific holder on the transport vehicle.
4. Turning the key counterclockwise actually opens the valve further rather than closing it. To discontinue flow and secure the cylinder, the key must be turned clockwise until the valve is completely seated. Operating the valve in the wrong direction can lead to rapid gas loss and depletion of the resource.
Test-taking strategy
- Identify the priority: In oxygen tank questions, safety and resource availability are the main goals.
- Analyze the pressure: Remember the 500 psi rule. In many facilities, 500 psi is the minimum threshold where a tank is replaced. Therefore, starting a transfer with only 500 psi is risky.
- Determine mechanical direction: For almost all medical and industrial valves, turning the handle clockwise closes the system. Choice 4 is a technical error.
- Select the most reliable step: Choice 1 is the only option that represents a universal, standardized pre-procedure safety check for oxygen administration.
Take home points
- Oxygen is an oxidizer and must be kept away from oils, greases, and open flames to prevent combustion.
- The duration of flow for a cylinder can be calculated by multiplying the psi by the tank factor and dividing by the flow rate.
A nurse is performing tracheal suctioning for a client. Which of the following assessments should the nurse consider when performing tracheal suctioning? Select all that apply
Explanation
Tracheal suctioning is an invasive procedure that involves the mechanical aspiration of secretions from the lower respiratory tract via a tracheostomy or endotracheal tube. This intervention is associated with significant physiological risks, including cardiac arrhythmias, bronchospasm, and sudden arterial oxygen desaturation. Comprehensive monitoring of the patient's hemodynamic and respiratory status is mandatory to detect and mitigate the adverse effects of vagal stimulation and oxygen removal.
Rationale for correct answers
1. Constant clinical surveillance is required throughout the procedure to identify signs of respiratory distress, cyanosis, or changes in consciousness. Baseline data must be compared to findings during and after the intervention to ensure the patient tolerates the suctioning and recovers effectively. It is a core nursing responsibility.
2. Delivery of 100% oxygen for 30 to 60 seconds provides an oxygen reservoir that helps prevent the hypoxia normally caused by removing air from the lungs. This pre-oxygenation and post-suctioning recovery period are essential for maintaining arterial saturation levels and cardiac stability during the procedure.
4. Suctioning can stimulate the vagus nerve, leading to profound bradycardia or other dysrhythmias. Frequent assessment of the heart rate allows the nurse to stop the procedure immediately if the patient becomes hemodynamically unstable. Pulse monitoring is a primary safety indicator during airway manipulation.
5. Utilizing a vacuum range of 80 to 120 mm Hg provides sufficient force to remove secretions without causing excessive trauma to the delicate tracheal walls. Pressures exceeding this range increase the risk of mucosal invagination and atelectasis. Correct pressure settings are a fundamental component of safe technique.
Rationale for incorrect answers
3. Applying suction for 20 to 30 seconds is dangerously long and can lead to severe hypoxemia. Clinical standards dictate that each suction pass must be limited to a maximum of 10 to 15 seconds to protect the patient's oxygen supply. Prolonged suctioning is a major cause of procedural complications.
6. Advancing the catheter as far as it will go can cause significant trauma to the carina, leading to bleeding and severe coughing. The catheter should be inserted only to the pre-measured length or until resistance is met, then withdrawn 1 to 2 cm before applying suction. Forcing the catheter to the limit is an incorrect and harmful practice.
Test-taking strategy
- Identify safe time limits: Rule out any option that allows suctioning for more than 15 seconds. This eliminates Choice 3.
- Identify correct anatomical depth: In the airway, “as far as it will go” is a red flag for trauma. This eliminates Choice 6.
- Verify standards:
- 80–120 mm Hg is the standard adult pressure range.
- Hyperoxygenation is a standard safety protocol.
- Monitoring (Pulse/ABCs) is the nursing priority.
- Select comprehensive monitoring: In a SATA question, prioritize options that focus on patient safety, monitoring, and adherence to evidence-based physiological limits.
Take home points
- Suctioning should never be performed as a routine schedule but rather based on clinical assessment of airway sounds.
- The diameter of the suction catheter should not exceed half the internal diameter of the tracheostomy or endotracheal tube.
The nurse is preparing to perform nasotracheal suctioning on a client. Arrange the steps in order.
Explanation
1. Perform hand hygiene (Step 7)
Hand hygiene reduces the risk of introducing pathogens into the airway and prevents cross-contamination. It is always the first step before any invasive procedure.
2. Assist client to semi-Fowler’s or high Fowler’s position, if able (Step 2)
Upright positioning promotes lung expansion, improves oxygenation, and makes insertion of the catheter easier by aligning the airway.
3. Apply sterile gloves (Step 6)
Sterile gloves maintain asepsis during suctioning, which is a sterile procedure. This protects both the patient and nurse from infection.
4. Have client take deep breaths (Step 4)
Deep breathing increases oxygen reserves and reduces the risk of hypoxia during suctioning, since suctioning temporarily interrupts airflow.
5. Lubricate catheter with water-soluble lubricant (Step 5)
Lubrication minimizes trauma to the nasal mucosa and facilitates smooth passage of the catheter through the nares.
6. Advance catheter through nares and into trachea (Step 3)
The catheter is gently inserted until resistance or coughing indicates entry into the trachea. This ensures secretions are accessed at the source.
7. Apply suction (Step 1)
Suction is applied while withdrawing the catheter, not during insertion, to avoid mucosal damage and hypoxia. Suction removes secretions effectively.
8. Withdraw catheter (Step 8)
The catheter is withdrawn while rotating to maximize secretion removal. This completes the suctioning cycle safely.
Test-taking strategy
- Standardize the start: Nearly every nursing procedure begins with hand hygiene (7).
- Prioritize preparation: You must position the patient (2) and prepare the sterile field/gloves (6) before touching the patient or equipment.
- Avoid trauma: Always lubricate (5) before you insert (3).
- Apply the safety rule: You must hyperoxygenate (4) before you suction, and you must never apply suction (1) while pushing the tube in; it only happens during withdrawal (8).
Take home points
- Water-soluble lubricant is mandatory to prevent lipid pneumonia and facilitate smooth passage through the nares.
- Semi-Fowler's or high Fowler's position helps the patient hyperventilate and facilitates the anatomical passage of the catheter.
A nurse is caring for a client with a chest tube in situ. Which number corresponds to the spot where the nurse would assess for an air leak?
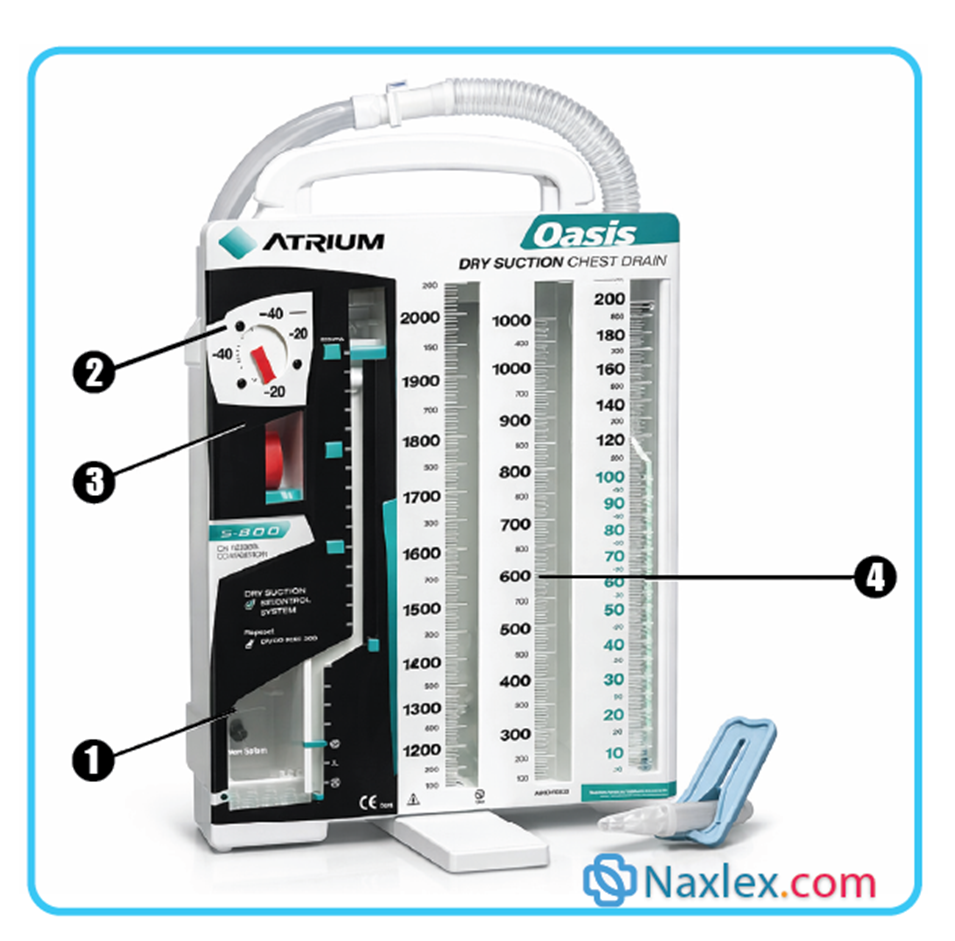
A portable chest tube drainage system shows four labels marked 1 to 4 as:
Explanation
The water-seal chamber is a diagnostic component of a chest drainage system designed to maintain a one-way valve between the patient and the environment. This chamber is partially filled with sterile water to prevent atmospheric air from entering the pleural space while allowing the escape of air and fluid. Visual inspection of this compartment for bubbling is the primary clinical method for identifying a pneumothorax or a breach in the integrity of the closed-circuit system.
Rationale for correct answer
1. This compartment contains the water column that serves as a pressure-sensitive indicator for the pleural cavity. The presence of bubbling within this specific chamber signifies that air is passing through the water, which indicates an air leak from either the patient's lung or the tubing connections. Nurses monitor this area for tidaling and bubbling to assess the progression of respiratory healing.
Rationale for incorrect answers
2. This area contains the suction control regulator, which determines the amount of negative pressure applied to the pleural space. While it is essential for managing the rate of drainage and lung re-expansion, it does not provide visual data regarding the presence of an air leak. It is a mechanical setting rather than a diagnostic assessment window.
3. This section houses the bellows or suction indicator, which confirms that the vacuum source is active and functioning at the prescribed level. It serves as a visual confirmation that the dry suction mechanism is operational and properly connected to the wall regulator. It does not communicate information regarding the patient's internal air leaks or pleural status.
4. These graduated columns are designated for the collection and measurement of fluid, blood, or serosanguinous exudate from the chest. While monitoring the volume and character of the output is a critical nursing assessment, this chamber is not used to detect the passage of air. It tracks the quantitative resolution of a hemothorax or pleural effusion.
Test-taking strategy
- Identify the diagnostic window: In chest tube systems, the water-seal chamber (usually at the bottom left) is the gold standard for leak detection.
- Differentiate chamber functions:
- Chamber 1 (Water Seal) - Air Leak Detection.
- Chamber 4 (Collection) - Fluid Measurement.
- Area 2/3 (Suction Control) - Vacuum Management.
- Apply clinical logic: To “see” air, it must pass through a liquid medium. Therefore, the nurse must look at the water in chamber 1 to identify bubbles escaping from the patient.
- Select for evidence: Choice 1 is the only section of the device that facilitates the visualization of air movement from the pleural space into the drainage unit.
Take home points
- Intermittent bubbling in the water-seal chamber during exhalation is expected if a pneumothorax is present.
- Continuous bubbling suggests a persistent air leak in the patient or a disconnection in the drainage tubing.
The nurse is caring for a client with a chest tube for treatment of a right pneumothorax. Which assessment finding necessitates immediate notification of the health care provider?
Explanation
A chest tube drainage system functions by maintaining a negative pressure environment in the pleural space to allow for lung re-expansion. The water-seal chamber acts as a one-way valve, allowing air to exit the pleural space while preventing atmospheric air from entering. While intermittent bubbling is expected as a pneumothorax resolves, the sudden onset of continuous, vigorous bubbling indicates a significant disruption in the integrity of the closed system or a worsening of the underlying pleural leak.
Rationale for correct answer
1. Sudden, vigorous bubbling in the water-seal chamber is a classic sign of a large air leak within the drainage system or the patient's pleural space. This finding suggests that the negative pressure necessary for lung expansion is lost, placing the patient at risk for a tension pneumothorax. The provider must be notified immediately to identify the source of the leak and prevent further respiratory collapse.
Rationale for incorrect answers
2. A scant amount of sanguineous drainage on the dressing is a common and expected finding following the insertion of a chest tube. As long as the drainage is not excessive or rapidly increasing, it represents localized tissue trauma from the procedure rather than a systemic complication. It should be monitored and marked for future comparison but does not require immediate notification.
3. Diminished breath sounds on the side of a pneumothorax are a typical clinical finding, as the lung is not yet fully re-expanded. As long as the breath sounds are clear and the patient is stable, this represents the baseline state of the condition being treated. Improvement is usually gradual and confirmed via daily chest radiographs.
4. A pain score of 2 on a 10-point scale indicates that the prescribed analgesic is effective and the patient's pain is well-controlled. Since the patient is reporting only mild discomfort following an invasive procedure, no immediate escalation of care or notification is required. Effective pain management actually facilitates better deep breathing and lung expansion.
Test-taking strategy
- Identify the emergency: Look for signs of system failure. In a chest tube system, vigorous bubbling where there was none before is a primary indicator of a mechanical or physiological crisis.
- Distinguish expected vs. unexpected:
- Rule out 2 because a scant amount of blood after surgery is expected.
- Rule out 3 because diminished sounds are the reason the patient has the tube in the first place.
- Evaluate pain levels: A score of 2 is a normal goal for postoperative care; it is not a reason for immediate notification.
- Prioritize the air leak: In the context of a pneumothorax, the water-seal chamber is the most important component to monitor for troubleshooting.
Take home points
- Intermittent bubbling in the water-seal chamber during expiration or coughing is normal until the pneumothorax resolves.
- Continuous bubbling suggests a leak in the system, which can be localized by briefly clamping the tube near the insertion site.
The nurse is caring for a client with pneumonia. On entering the room, the nurse finds the client lying in bed, coughing, and unable to clear secretions. What should the nurse do first?
Explanation
Pneumonia causes an inflammatory exudate to accumulate within the alveoli, impairing gas exchange and increasing the viscosity of respiratory secretions. When a patient is in a supine position, the weight of the abdominal contents and the effects of gravity reduce diaphragmatic excursion and promote the pooling of secretions in the dependent lung segments. Positioning the patient is the most rapid non-invasive intervention to optimize lung expansion and facilitate the mechanical clearance of the airway.
Rationale for correct answer
2. Elevating the head of the bed to 45 degrees (Fowler's position) uses gravity to shift the diaphragm downward, allowing for maximal thoracic expansion. This position decreases the work of breathing and helps the patient utilize their cough more effectively to mobilize secretions. It is the immediate action in the nursing process to improve respiratory status.
Rationale for incorrect answers
1. While oxygen therapy may be necessary, it does not address the mechanical problem of secretions blocking the airway. Oxygen should be administered after the patient's position has been optimized and the airway has been assessed for patency. Proper positioning may even reduce the immediate need for supplemental oxygen by improving ventilation.
3. An incentive spirometer is a tool for preventing atelectasis but is not the priority for a patient currently struggling to clear active secretions. The patient must first be repositioned and stabilized before they can effectively perform the slow, deep inspirations required for spirometry. It is a secondary, preventive intervention.
4. Notifying the healthcare provider is appropriate if the patient's condition does not improve, but the nurse must first perform nursing interventions to stabilize the patient. Calling the doctor before attempting to reposition the patient is a failure of independent nursing judgment in an acute situation. Initial stabilization is always the nurse's priority.
Test-taking strategy
- Identify the least invasive first: In respiratory distress, positioning is almost always the first and fastest action the nurse can take independently.
- Apply the nursing process: Before calling for help or starting medications, the nurse should optimize the patient's anatomical ability to breathe.
- Evaluate the priority:
- Rule out 4 because you must act before you call.
- Rule out 3 because it's for prevention, not acute distress.
- Rule out 1 because airway and positioning come before oxygenation (ABC).
- Focus on gravity: Elevating the head of the bed is the gold standard first step for any patient who is coughing or short of breath.
Take home points
- High Fowler's position (60 to 90 degrees) provides the greatest decrease in abdominal pressure on the diaphragm.
- Frequent position changes help prevent the pooling of secretions and the development of hypostatic pneumonia.
The nurse is caring for a client with an artificial airway. Which of the following are reasons to suction the client? Select all that apply
Explanation
Suctioning is a high-risk intervention used to maintain patency in patients with artificial airways who cannot clear secretions independently. Because the procedure can cause hypoxia and mucosal trauma, it should never be performed as a routine or scheduled task. Clinical decisions to suction must be based on a thorough assessment of the patient's respiratory status, including physical signs of obstruction and changes in physiological monitoring.
Rationale for correct answers
1. The presence of visible secretions within the endotracheal or tracheostomy tube is a direct indication that the airway is obstructed. These secretions increase airway resistance and must be removed to ensure adequate tidal volumes and oxygenation. It is one of the most objective signs that suctioning is required.
2. A sawtooth pattern on the capnography (EtCO2) waveform is a specific monitor finding that indicates turbulent airflow caused by secretions in the circuit or airway. This visual indicator allows the nurse to identify the need for suctioning even before audible adventitious sounds are heard. It is a highly sensitive clinical marker.
5. Excessive, unproductive coughing often indicates that secretions are irritating the carina or obstructing the airway lumen, but the patient is unable to move them. Suctioning provides the mechanical assistance needed to clear these irritants and restore comfortable ventilation. It helps prevent patient exhaustion.
Rationale for incorrect answers
3. Clear breath sounds indicate that the lower airways are patent and free of obstructive secretions. Suctioning a patient with clear sounds is unnecessary and exposes the patient to the risks of mucosal trauma and hypoxia without clinical benefit. Assessment findings must justify the intervention.
4. Suctioning should be performed on a PRN (as needed) basis rather than a fixed schedule like “every 3 hours.” Scheduled suctioning increases the frequency of iatrogenic injury to the trachea and increases the risk of introducing pathogens. The nurse should assess frequently but only suction when indications are present.
Test-taking strategy
- Identify PRN vs. scheduled: Always rule out scheduled suctioning (Option 4). The correct approach is always based on assessment.
- Evaluate clinical signs:
- Clear breath sounds (Option 3) means do nothing.
- Visible secretions (Option 1) and coughing (Option 5) are red flags for obstruction.
- Identify advanced monitoring: Recognize that modern monitors provide clues; a sawtooth on EtCO2 (Option 2) is the textbook waveform for secretions.
- Select for necessity: In SATAs only choose the options that represent a deficit or an abnormal finding that requires intervention.
Take home points
- Indications for suctioning include increased peak inspiratory pressure, decreased oxygen saturation, and audible crackles over the trachea.
- Routine saline instillation before suctioning is no longer recommended as it may push bacteria deeper into the lungs.
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Outline the structure and function of the respiratory system.
- Describe the processes of breathing (ventilation) and gas exchange (respiration).
- Explain the role and function of the respiratory system in transporting oxygen and carbon dioxide to and from body tissues.
- Describe the mechanisms for respiratory regulation.
- Identify factors influencing respiratory function.
- Identify four major types of conditions that can alter respiratory function.
- Describe nursing assessments for oxygenation status.
- Describe nursing measures to promote respiratory function and oxygenation.
- Explain the use of therapeutic measures such as medications, inhalation therapy, oxygen therapy, artificial airways airway suctioning, and chest tubes to promote respiratory function.
- State outcome criteria for evaluating client responses to measures that promote adequate oxygenation.
- Verbalize the steps used in: a. Administering oxygen by cannula, face mask, or face tent. b. Oropharyngeal, nasopharyngeal, and nasotracheal suctioning. c. Providing tracheostomy care.
Introduction
Oxygen, a clear, odorless gas that constitutes approximately 21% of the air we breathe, is necessary for proper functioning of all living cells. The absence of oxygen can lead to cellular, tissue, and organism death.
Cellular metabolism produces carbon dioxide, which must be eliminated from the body to maintain normal acid–base balance.
Delivery of oxygen and removal of carbon dioxide require the integration of several systems including the hematologic, cardiovascular, and respiratory systems.
Respiration is the process of gas exchange between the individual and the environment and involves four components:
- Ventilation or breathing, the movement of air in and out of the lungs as we inhale and exhale
- Alveolar-capillary gas exchange, which involves the diffusion of oxygen and carbon dioxide between the alveoli and the pulmonary capillaries
- Transport of oxygen and carbon dioxide between the tissues and the lungs
- Movement of oxygen and carbon dioxide between the systemic capillaries and the tissues.
Structure And Processes Of The Respiratory System
The structure of the respiratory system facilitates gas exchange and protects the body from foreign matter such as particulates and pathogens. The four processes of the respiratory system include pulmonary ventilation, alveolar gas exchange, transport of oxygen and carbon dioxide, and systemic diffusion.
I. Structural of the respiratory system
The respiratory system is categorized into two main tracts designed to filter, warm, and transport air.
Upper respiratory system
- Mouth & Nose: Entry points. The nose warms, humidifies, and filters air via hairs and nasal turbinates.
- Pharynx (Throat): Shared pathway for food and air; contains lymphoid tissue to destroy pathogens.
- Larynx (Voice Box): Identifiable as the “Adam’s apple.”
- Function: Maintains airway patency and protects the lower airway.
- Epiglottis: A flap that closes during swallowing to route food to the esophagus.
Lower respiratory system
- Trachea: Leads to the right and left main bronchi.
- Bronchial Tree: Successive branching of bronchi into smaller bronchioles, ending in terminal bronchioles.
- Lungs: Contain the respiratory zone (respiratory bronchioles, alveolar ducts, and alveoli).
- Alveoli: Tiny air sacs where all gas exchange occurs. They are covered in a pulmonary capillary mesh.
- Pleura: Double-layered membrane (parietal and visceral) with pleural fluid that reduces friction and creates surface tension to keep lungs expanded.
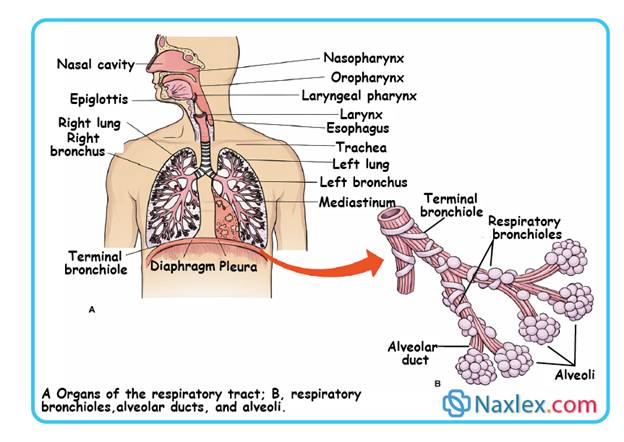
II. The Four Processes of Respiration
1. Pulmonary ventilation (Breathing)
The movement of air into (inspiration) and out of (expiration) the lungs.
- Mechanism: Driven by pressure changes.
- Inspiration: Diaphragm and intercostals contract 🡪 thoracic cavity volume increases 🡪 intrapulmonary pressure drops 🡪 air rushes in.
- Expiration: Muscles relax 🡪 lungs recoil 🡪 intrapulmonary pressure rises 🡪 air is expelled.
- Key Factors:
- Compliance: The stretchability of lung tissue.
- Recoil: The tendency of lungs to collapse away from the chest wall.
- Surfactant: A lipoprotein that reduces surface tension in alveoli, preventing lung collapse.
- Tidal Volume: The amount of air inspired/expired in a normal breath (~500 mL).
2. Alveolar gas exchange
The diffusion of gases between the alveoli and the pulmonary capillaries across the respiratory membrane. The partial pressure (the pressure exerted by each individual gas in a mixture according to its concentration in the mixture) of oxygen (PO2) in the alveoli is about 100 mmHg (sometimes referred to as torr, which is the same as millimeters of mercury), whereas the PO2 in the venous blood of the pulmonary arteries is about 60 mmHg or torr.
- Oxygen: Diffuses from alveoli (PO2 ≈ 100mmHg) to blood (PO2 ≈ 60 mmHg).
- Carbon Dioxide: Diffuses from blood (PCO2 ≈ 45mmHg) to alveoli (PCO2 ≈ 40mmHg).
3. Transport of oxygen and carbon dioxide
The movement of gases via the blood to and from the tissues.
- Oxygen Transport: 97% is carried as oxyhemoglobin in red blood cells (RBCs); 3% is dissolved in plasma.
- Influenced by: Cardiac output, RBC count (hematocrit), and exercise.
- Carbon Dioxide Transport: 65% as Bicarbonate (HCO3-).
- 30% as Carbaminohemoglobin (bound to hemoglobin).
- 5% dissolved in plasma or as carbonic acid.
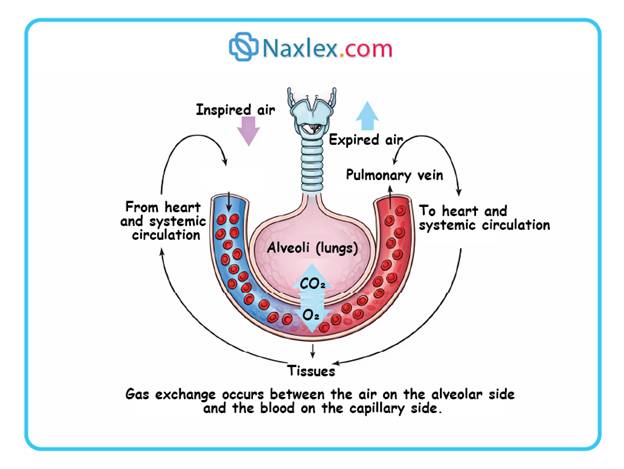
Several factors affect the rate of oxygen transport from the lungs to the tissues:
- Cardiac output
- Number of erythrocytes and blood hematocrit
- Exercise.
Any pathologic condition that decreases cardiac output (e.g.,damage to the heart muscle, blood loss, or pooling of blood in the peripheral blood vessels) diminishes the amount of oxygen delivered to the tissues.
4. Systemic Diffusion
The exchange of gases between the systemic capillaries and the actual body cells.
- Oxygen diffuses into cells as they consume it (moving down the concentration gradient).
- Carbon dioxide, a byproduct of metabolism, diffuses from cells into the blood.
III. Respiratory Regulation
The body adjusts breathing rates to maintain constant PO2 and PCO2 levels. Respiratory regulation includes both neural and chemical controls to maintain the correct concentrations of oxygen, carbon dioxide, and hydrogen ions in body fluids.
|
Control Type |
Mechanism |
Location |
|
Neural |
Respiratory centers control rhythm and depth. |
Medulla and Pons (Brainstem) |
|
Chemical (Central) |
Sensitive to increased CO2 and H+ levels. |
Chemosensitive center in Medulla |
|
Chemical (Peripheral) |
Sensitive to decreased O2 levels. |
Carotid and Aortic bodies |
Nursing insights
Hypoxic Drive: In some chronic conditions (like emphysema), the brain becomes desensitized to high CO2. In these cases, low oxygen levels become the primary stimulus for breathing. Providing too much supplemental oxygen can dangerously depress their respiratory rate.
3.1 FACTORS AFFECTING RESPIRATORY FUNCTION
Factors that influence oxygenation affect the cardiovascular system as well as the respiratory system. These factors include age, environment, lifestyle, health status, medications, and stress.
I. Age and Developmental Factors
Respiratory function evolves significantly from birth through the later stages of life.
Neonatal Transition
- First Breath: Triggered by rising PCO2 levels and the draining of fetal lung fluid.
- Expansion: Full lung inflation is typically achieved by 2 weeks of age.
Older Adults (The aging process)
Aging reduces the respiratory reserve, making the system vulnerable during stress or infection.
- Structural changes: The chest wall and airways become more rigid and less elastic; muscle strength/endurance decreases.
- Defense mechanisms: Decreased cough reflex, less effective ciliary action, and a drier/more fragile mucosal lining.
- Immune function: Overall decrease in immune efficiency increases infection risk.
- Secondary risks:
- Osteoporosis: Can lead to kyphosis, compromising lung expansion.
- GERD: Increased incidence of gastroesophageal reflux increases the risk of aspiration, which can trigger inflammatory bronchospasms.
II. Environmental influences
External conditions dictate the availability of oxygen and the presence of irritants.
- Altitude: Higher altitudes have lower PO2. The body compensates by increasing respiratory rate, depth, and cardiac rate.
- Pollution: Exposure to smog or secondhand smoke can cause acute symptoms (stinging eyes, coughing). In patients with pre-existing lung disease, pollution can severely limit self-care abilities.
- Temperature: Both extreme heat and cold can place additional stress on oxygenation.
III. Lifestyle and occupation
Daily habits and work environments play a cumulative role in lung health.
Physical activity
- Active individuals: Regular exercise promotes alveolar expansion and deep-breathing patterns.
- Sedentary individuals: Lack deep-breathing habits, making them less resilient to respiratory stressors.
Occupational hazards
Specific jobs expose workers to particles that cause chronic lung diseases:
- Silicosis: Sandstone blasters and potters.
- Asbestosis: Asbestos workers.
- Anthracosis: Coal miners.
- Organic dust disease: Farmers working with moldy hay.
IV. Health status and medications
Current medical conditions and the substances used to treat them directly impact respiratory drive.
- Health status: While a healthy system meets all metabolic demands, respiratory diseases (like COPD or pneumonia) directly impair blood oxygenation.
- Medications: Certain drugs can cause respiratory depression (decreased rate and depth).
- Benzodiazepines: e.g., Valium, Ativan, Versed.
- Barbiturates: e.g., Phenobarbital.
- Opioids: e.g., Morphine.
- Nursing Note: Older adults are at higher risk and usually require lower dosages.
V. Stress response
Stress triggers both psychological and physiological shifts in oxygenation.
- Psychological (hyperventilation): Stress-induced rapid breathing causes PO2 to rise and PCO2 to fall.
- Symptoms: Light-headedness, numbness, and tingling (paresthesia) around the mouth and extremities.
- Physiological (sympathetic nervous system): Stress releases epinephrine, which causes bronchodilation. While adaptive for fight or flight by increasing oxygen to muscles, chronic stress can lead to cardiovascular disease.
3.2 ALTERATIONS IN RESPIRATORY FUNCTION
1. Core mechanisms of respiratory dysfunction
Respiratory impairment stems from failures in one or more of the following physiological processes:
- Patency: Maintenance of an unobstructed airway.
- Ventilation: The mechanical movement of air into and out of the lungs.
- Diffusion: The exchange of O2 and CO2 at the alveolar-capillary membrane.
- Perfusion and transport: The movement of oxygenated blood to tissues and deoxygenated blood to the lungs via the cardiovascular system.
2. Airway obstruction (patency issues)
Upper Airway Obstruction: Occurs in the nose, pharynx, or larynx.
- Etiology: Foreign bodies, tongue displacement (common in unconscious states), or accumulation of secretions.
- Clinical signs: Low-pitched snoring sounds during inspiration (partial); gurgling/bubbling sounds (secretions).
Complete obstruction: Extreme inspiratory effort without chest movement; inability to speak or cough; marked sternal and intercostal retractions.
Lower airway obstruction: Occlusion of the bronchi or smaller passages.
- Etiology: Increased mucus production or inflammatory exudate.
- Clinical signs: Stridor (harsh, high-pitched inspiratory sound), adventitious breath sounds, restlessness, and dyspnea.
3. Alterations in ventilation and breathing patterns
- Eupnea: Normal, quiet, rhythmic respirations.
- Tachypnea: Rate > 20 breaths per minute. Seen in pyrexia, metabolic acidosis, pain, and hypoxemia.
- Bradypnea: Abnormally slow rate. Associated with opioids/sedatives, metabolic alkalosis, or increased intracranial pressure (ICP).
- Apnea: Total cessation of breathing.
- Hypoventilation: Inadequate alveolar ventilation (slow or shallow). Leads to hypercarbia (hypercapnia) and hypoxemia.
- Hyperventilation: Increased rate and depth resulting in CO2 elimination exceeding CO2 production.
- Kussmaul's Breathing: Compensatory hyperventilation in metabolic acidosis to blow off acid in the form of CO2.
- Dyspnea: Subjective feeling of shortness of breath. Objective signs include nasal flaring, tachycardia, cyanosis, and diaphoresis.
- Orthopnea: Inability to breathe effectively unless in an upright (sitting or standing) position.
Irregular Rhythms:
- Cheyne-Stokes: Rhythmic waxing and waning from deep to shallow breathing with periods of apnea; common in chronic disease, increased ICP, or drug overdose.
- Biot's (Cluster) Respirations: Shallow breaths interrupted by apnea; associated with Central Nervous System (CNS) disorders.
4. Diffusion impairment and hypoxemia
Pathophysiology: Impaired gas exchange at the alveolar level. O2 is typically affected more than CO2 due to lower solubility.
- Hypoxemia: Reduced O2 in the blood. Causes include pulmonary edema, atelectasis (alveolar collapse), or low hemoglobin levels.
- Hypoxia: Insufficient oxygenation at the cellular/tissue level.
Clinical Manifestations of Hypoxia:
- Acute: Anxiety, drawn, fatigued facial expression, sitting forward to expand the thoracic cavity.
- Chronic: Fatigue, lethargy, and finger or toe clubbing.
- Clubbing: Nail base angle increases to > 180 degrees with bulbous enlargement of digits.
- Cyanosis: Bluish tint of skin and mucous membranes. Requires > 5 g of unoxygenated hemoglobin per 100 mL of blood and dilated surface capillaries. Note: May be absent in severe anemia despite hypoxia.
- Cerebral Impact: The cerebral cortex can only tolerate hypoxia for 3 to 5 minutes before permanent neurological damage occurs.
5. Transport and perfusion failures
- Cardiovascular interdependence: Effective respiration requires adequate cardiac output.
Impairment Factors:
- Hypovolemia: Decreased blood volume reduces O2 carrying capacity.
- Congestive Heart Failure (CHF): Decreases cardiac output and the body's ability to compensate for hypoxemia.
- Compensatory mechanisms: The heart increases rate and stroke volume to maintain tissue oxygenation during respiratory distress.
Nursing Management Of Oxygenation
5.1 NURSING ASSESSMENT:
1. NURSING HISTORY
A focused history identifies current dysfunction, chronic conditions, and environmental triggers.
Current Respiratory Status:
- Dyspnea: Identify precipitating activities and severity.
- Orthopnea: Document the number of pillows used for sleep.
- Cough: Frequency, timing, and nature (productive vs. nonproductive).
- Sputum: Evaluate volume, color (e.g., purulent, clear), consistency, odor, and presence of hemoptysis (blood-tinging).
- Chest Pain: Location, duration, onset during inspiration vs. expiration, and associated symptoms (nausea, palpitations).
Past medical history:
- Childhood and chronic illnesses: Asthma, Tuberculosis (TB), Bronchitis, Emphysema, or Pneumonia.
- Allergies and previous treatment modalities.
Lifestyle and risk factors:
- Tobacco Use: Pack-years, current status, and exposure to environmental tobacco smoke (ETS).
- Occupational Exposure: Fumes, coal dust, asbestos, or silica.
- Comorbidities: Obesity (BMI > 30), sedentary lifestyle, and high saturated fat intake (increased cardiovascular risk).
- Medications: Use of bronchodilators, inhalants, or narcotics (which may depress respiratory drive).
2. PHYSICAL EXAMINATION
Inspection:
- Respiratory rate, depth, and rhythm: Observe for tachypnea or shallow breathing.
- Thoracic configuration: Check for Barrel Chest (increased anteroposterior diameter), common in emphysema.
- Client positioning: Note Tripod Position or use of accessory muscles.
Palpation:
- Assessing for tenderness, masses, or vocal (tactile) fremitus (vibrations felt on the chest wall).
Percussion:
- Diaphragmatic excursion: Measuring the movement of the diaphragm (less common in acute settings).
Auscultation:
- Evaluation of normal versus adventitious (abnormal) breath sounds.
3. DIAGNOSTIC AND LABORATORY STUDIES
- Sputum and throat cultures: To identify infectious pathogens.
- Pulmonary Function Tests (PFTs): Noninvasive measurement of lung volumes and capacities.
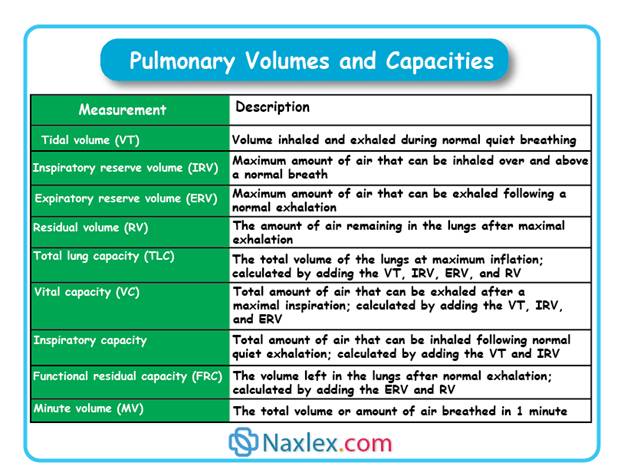
Nursing responsibility: Explain the procedure, ensure client cooperation (tiring), and provide rest periods post-test.
- Arterial Blood Gases (ABGs): Direct measurement of O2, CO2, and pH from radial, brachial, or femoral arteries.
Safety slert: Apply pressure to the puncture site for ≥ 5 minutes post-extraction to prevent hemorrhage due to high arterial pressure.
- Pulse Oximetry: Noninvasive measurement of arterial oxygen saturation (SpO2).
5.2 NURSING DIAGNOSES (NANDA-I)
- Ineffective Airway Clearance: Inability to maintain a clear passage due to secretions or obstruction.
- Ineffective Breathing Pattern: Inadequate ventilation (rate/depth issues).
- Impaired Gas Exchange: Imbalance in O2/CO2 at the alveolar-capillary membrane level.
- Activity Intolerance: Insufficient energy to complete daily tasks due to respiratory compromise.
- Secondary Diagnoses: Anxiety (feeling of suffocation), Fatigue, Social Isolation, and Insomnia (due to orthopnea).
5.3 PLANNING AND OUTCOMES
Primary goals for the oxygenated-compromised client:
- Maintain a patent airway.
- Optimize pulmonary ventilation and oxygenation.
- Improve physical activity tolerance.
- Prevent complications: Skin breakdown (from O2 tubing/immobility), acid-base imbalances, and syncope.
5.4 NURSING IMPLEMENTATION (INTERVENTIONS)
Examples of nursing interventions to facilitate pulmonary ventilation may include:
- Positioning: Semi-Fowler’s or High-Fowler’s to allow maximum chest expansion.
- Deep Breathing and Coughing: Exercises to clear secretions and inflate alveoli.
- Hydration: Maintaining fluid intake to liquefy thick secretions.
- Suctioning: Removal of secretions when the client is unable to cough effectively.
- Facilitating Diffusion: Encouraging activity as tolerated and postural drainage.
- Collaborative/Dependent Interventions:
- Oxygen Therapy: Delivery of supplemental O2.
- Chest Tube Management and Tracheostomy Care.
- Analgesia: Administering pain medication prior to coughing exercises to improve compliance.
HOME CARE AND DISCHARGE PLANNING
- Assessment: Evaluate financial resources, family support, and home environment (pollutants/stairs).
- Referrals: Home health services or respiratory therapy.
- Teaching: Instructing the client on portable oxygen safety and energy conservation techniques.
5.5 EVALUATING
Using the goals and desired outcomes identified in the planning stage of the nursing process, the nurse collects data to evaluate the effectiveness of interventions. If outcomes are not achieved, the nurse, client, and support person if appropriate need to explore the reasons before modifying the care plan. For example, if the outcome “Respirations unlabored and rate is within expected range” is not met, examples of questions that need to be considered include the following:
- What is the client’s perception of the problem?
- Is the client complaining of shortness of breath or difficulty breathing?
- Is the client taking medications or performing treatments such as percussion, vibration, and postural drainage as prescribed?
- Has the client been exposed to an upper respiratory infection that is affecting breathing?
- Do other factors need to be considered, such as the client’s psychological stress level?
Examples of questions to consider if the outcome “Able to complete ADLs without fatigue” is not met include the following:
- What other factors may be affecting the client’s ability to complete ADLs?
- Is the client getting adequate sleep? If not, what is interfering with the client’s rest?
- Are there assistive devices (e.g., a shower chair, clothing that is easy to put on) that could help the client achieve this goal?
- Does the client need help with housework and other ADLs?
- Is the client’s diet adequate to meet nutritional needs?
Nursing Interventions
7.1 GENERAL INTERVENTIONS
1. PROMOTING VENTILATION AND CHEST EXPANSION
Immobility and pain lead to shallow respirations, which inhibit diaphragmatic excursion and lung distensibility. This results in pooling of secretions and potential atelectasis.
Optimal Positioning:
- Semi-Fowler’s or High-Fowler’s: Facilitates maximum chest expansion by allowing gravity to pull the diaphragm downward.
- Orthopneic position: Client sits upright leaning over an overbed table. This stabilizes the chest and reduces the work of breathing.
- Tripod position: Client leans forward on arms/elbows to assist accessory muscle use.
- Lateral positioning: In unilateral lung disease (e.g., pneumonia), position the “good lung down” to optimize ventilation-perfusion matching and O2 diffusion.
- Ambulation: Early and frequent mobilization prevents stasis of secretions and maintains pulmonary function.
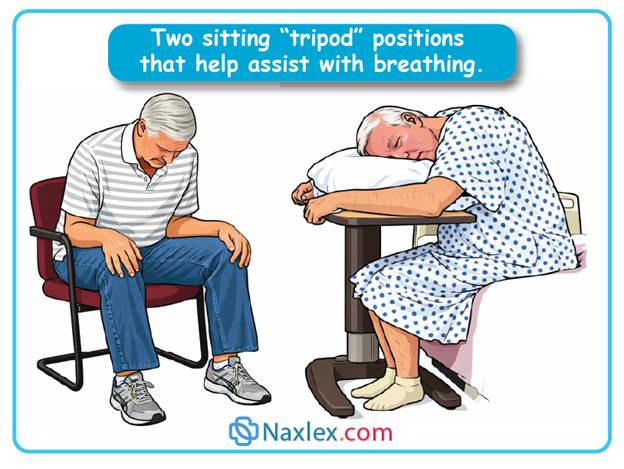
2. BREATHING AND COUGHING TECHNIQUES
- Deep breathing and coughing: Essential for mobilizing secretions and re-inflating collapsed alveoli.
- Pursed-lip breathing:
- Technique: Inhale through the nose; exhale slowly through pursed lips (as if whistling).
- Purpose: Alleviates dyspnea by creating back-pressure that keeps airways open during exhalation and assists abdominal muscle contraction.
- Coughing Techniques:
- Forceful cough: Inhale deeply, then perform 2 sharp coughs during one exhalation.
- Huff coughing (forced expiratory technique): Exhale through pursed lips and make a “huff” sound mid-exhalation. This prevents high expiratory pressures that collapse diseased airways (common in COPD).
3. HYDRATION AND HUMIDIFICATION
- Systemic hydration: High fluid intake (as tolerated) maintains thin, watery respiratory secretions for easier ciliary clearance. Dehydration leads to thick, tenacious mucus.
- Humidifiers: Add water vapor to inspired air to prevent mucous membrane irritation.
- Nebulizers: Deliver moisture and/or medications directly to the respiratory tract to loosen secretions.
4. PHARMACOLOGICAL INTERVENTIONS
- Bronchodilators (Sympathomimetics and Xanthines): Reduce bronchospasm. Preferred route is inhalation to minimize systemic effects.
- Monitoring: Monitor for tachycardia, hypertension, anxiety, and restlessness (sympathetic activation).
- Anti-inflammatory drugs (Glucocorticoids): Reduce airway edema.
- Administration Rule: If both are ordered, administer the bronchodilator first to open the airways, followed by the corticosteroid to ensure deeper tissue penetration.
- Leukotriene modifiers: Suppress bronchoconstriction and mucous production.
- Expectorants (e.g., Guaifenesin): Reduce mucus viscosity to facilitate expectoration.
- Cough suppressants (e.g., Codeine): Used only when frequent coughing prevents rest/sleep.
- Cardiac medications: Digitalis or beta-agonists (Dobutamine) improve cardiac output/O2 transport.
- Caution: Beta-blockers (Propranolol) can cause bronchoconstriction in asthma/COPD clients.
5. INCENTIVE SPIROMETRY (SUSTAINED MAXIMAL INSPIRATION - SMI)
Purpose: Mimics natural sighing to expand collapsed alveoli, improve ventilation, and loosen secretions.
Types:
- Flow-Oriented: Client elevates balls/disks by maintaining inspiratory flow.
- Volume-Oriented: Measures the specific volume of air inhaled via a rising piston.
Nursing Care: Ensure the client is upright; emphasize slow, deep inhalations rather than rapid breaths.
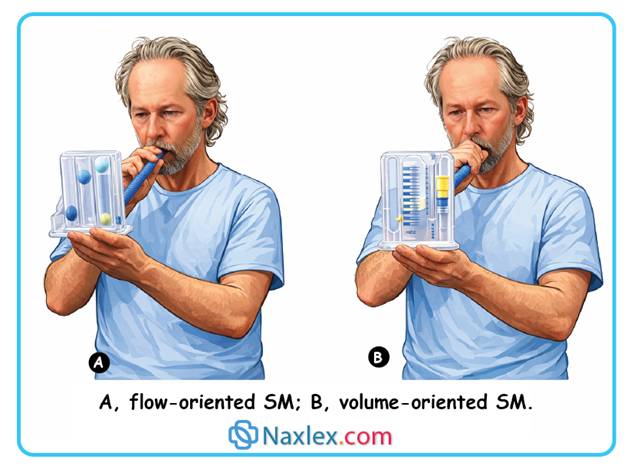
Nursing insights:
CLIENT TEACHING: Using an Incentive spirometer
- Hold or place the spirometer in an upright position. A tilted flow-oriented device requires less effort to raise the balls or disks; a volume-oriented device will not function correctly unless upright.
- Exhale normally.
- Seal the lips tightly around the mouthpiece.
- Take in a slow, deep breath to elevate the balls or cylinder, and then hold the breath for 2 seconds initially, increasing to 6 seconds (optimum), to keep the balls or cylinder elevated if possible.
- For a flow-oriented device, avoid brisk, low-volume breaths that snap the balls to the top of the chamber. Greater lung expansion is achieved with a very slow inspiration than with a brisk, shallow breath, even though it may not elevate the balls or keep them elevated while you hold your breath. Sustained elevation of the balls or cylinder ensures adequate ventilation of the alveoli (lung air sacs).
- If you have difficulty breathing only through the mouth, a nose clip can be used.
- Remove the mouthpiece and exhale normally.
- Cough after the incentive effort. Deep ventilation may loosen secretions, and coughing can facilitate their removal.
- Relax and take several normal breaths before using the spirometer again.
- Repeat the procedure several times and then four or five times hourly. Practice increases inspiratory volume, maintains alveolar ventilation, and prevents atelectasis (collapse of the air sacs).
- Clean the mouthpiece with water and shake it dry.
6. CHEST PHYSIOTHERAPY: PERCUSSION, VIBRATION, AND POSTURAL DRAINAGE (PVD)
Percussion (Clapping): Forceful striking with cupped hands over congested lung segments to dislodge secretions. Avoid the sternum, spine, kidneys, and breasts.
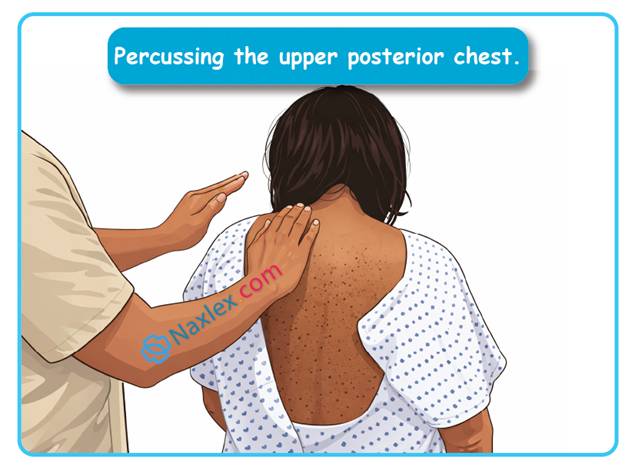
Vibration: Vigorous quivering of the chest wall during 5 exhalations. Used after percussion to increase air turbulence.
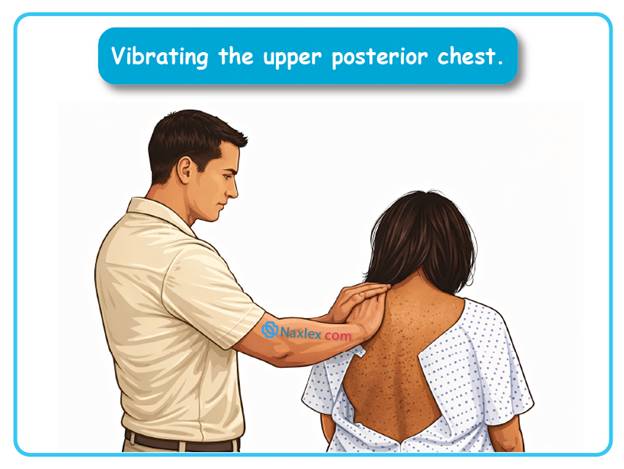
Postural drainage: Uses gravity to drain secretions from lung segments.
- Timing: 2 to 3 times daily (before meals and at bedtime) to prevent vomiting/aspiration.
- Duration: 10 to 15 minutes per position.
- Monitoring: Stop if the client exhibits pallor, diaphoresis, dyspnea, or nausea.
7. MUCUS CLEARANCE DEVICES (MCD)
Flutter device: A handheld device containing a steel ball.
- Mechanism: Fast exhalation causes the ball to vibrate, transmitting vibrations to the airways to loosen mucus.
- Indication: Used for cystic fibrosis, COPD, and bronchiectasis.
8. CLIENT TEACHING FOR RESPIRATORY HEALTH
- Maintain erect posture for full lung expansion.
- Exercise regularly and breathe through the nose.
- Avoid environmental pollutants: Secondhand smoke, pesticides, and unventilated stoves.
- Eliminate household triggers: Use building materials with low vapor emission and ensure proper furnace ventilation.
7.2 OXYGEN THERAPY
Principles of oxygen administration
Oxygen is a therapeutic gas considered a medication. Administration requires a provider order specifying concentration, delivery method, and flow rate in L/min. Nurses may initiate oxygen in emergencies but must obtain a subsequent order.
Indications for therapy
- Hypoxemia: Decreased arterial oxygen tension.
- Impaired Diffusion: Reduced gas exchange across the alveolar-capillary membrane.
- Reduced lung surface area: Resulting from lobectomy, pneumonectomy, or neoplasms.
- Hematologic Deficiencies: Severe anemia or hemorrhage (reduced hemoglobin/erythrocyte count).
- Hyperventilation: Compensatory respiratory patterns.
Oxygen sources and equipment
- Supply systems: Wall-mounted outlets (acute care) or portable cylinders/tanks.
- Home therapy: Liquid oxygen, small cylinders, or oxygen concentrators.
- Humidification: Essential for flow rates > 4 L/min to prevent dehydration of respiratory mucous membranes. Humidifiers add 20% to 40% humidity. Very low flows (1 to 2 L/min) typically do not require humidification.
- Pressure regulation: A regulator must be attached to cylinders to reduce pressure to safe levels. The content gauge indicates remaining pressure; the flow meter indicates L/min.
Safety precautions and toxicity
- Combustion: Oxygen facilitates rapid combustion. Materials like bed sheets burn explosively in oxygen-enriched environments.
- Hypoxia: Inadequate oxygenation leading to cellular senescence and death.
- Oxygen toxicity: Risk increases when breathing > 50% oxygen for > 12 hours. Can cause pulmonary parenchymal damage and prolonged mechanical ventilation.
- Clinical goal: Use the lowest FiO2 (Fraction of Inspired Oxygen) to maintain SpO2 ≥ 90%.
LOW-FLOW DELIVERY SYSTEMS
These devices provide supplemental oxygen that is diluted with atmospheric air; FiO2 varies with the patient's inspiratory flow, tidal volume, and respiratory rate.
1. Nasal Cannula
- Flow: 2 to 6 L/min.
- Concentration: 24% to 45%.
- Considerations: Most common and least invasive; allows eating and speaking. Rates > 6 L/min cause aerophagia without increasing FiO2.
2. Reservoir Nasal Cannula (Oxymizer)
- Function: Stores 100% oxygen bolus during exhalation.
- FiO2: ≥ 0.5 (50%).
- Benefit: Higher concentration at lower flow rates; requires no external humidification.
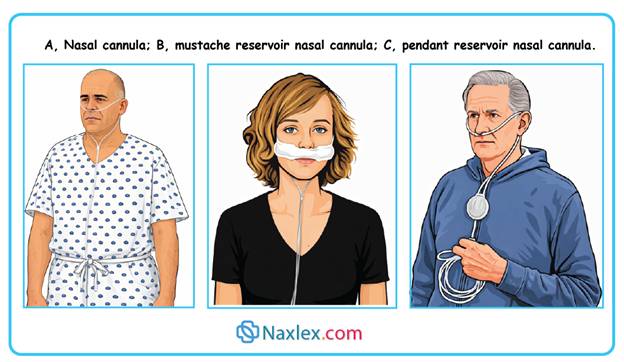
3. Simple Face Mask
- Flow: 5 to 8 L/min.
- Concentration: 40% to 60%.
4. Partial Rebreather Mask
- Flow: 6 to 10 L/min.
- Concentration: 40% to 60%.
- Mechanism: Reservoir bag allows rebreathing of the first third of expired air. Bag must remain 1/3 to 1/2 full during inspiration.
5. Nonrebreather Mask
- Flow: 10 to 15 L/min.
- Concentration: 95% to 100%.
- Mechanism: One-way valves prevent room air and exhaled air from entering the reservoir bag. Bag must not totally deflate on inspiration.
6. Face Tent
- Flow: 4 to 8 L/min.
- Concentration: 30% to 50%.
- Use: For patients who cannot tolerate tight-fitting masks.
HIGH-FLOW DELIVERY SYSTEMS
These systems provide a precise, constant FiO2 regardless of the patient's ventilatory pattern.
1. Venturi Mask
- Flow: 4 to 10 L/min.
- Concentration: 24% to 50%.
- Mechanism: Uses large-bore tubing and color-coded jet adapters (e.g., Blue = 24% at 4 L/min; Green = 35% at 8 L/min).
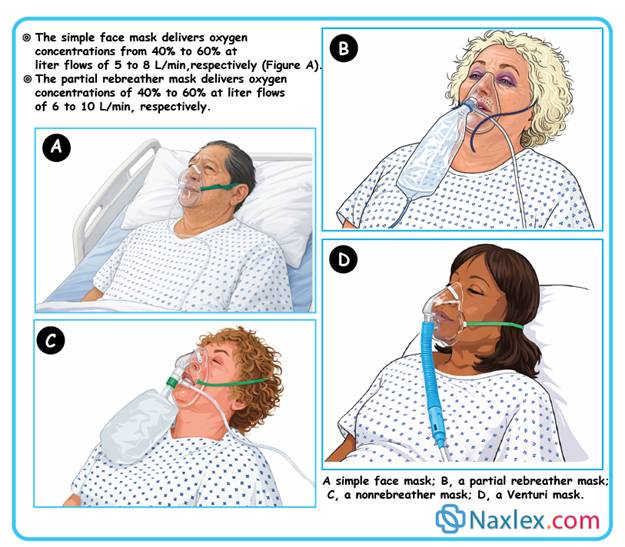
SPECIALIZED DELIVERY METHODS
Transtracheal Catheter
- Surgically created tract in the lower neck.
- Flow: 1 to 20 L/min (requires humidification at rates > 1 L/min).
Noninvasive Positive Pressure Ventilation (NPPV) Used for respiratory failure, pulmonary edema, COPD, and Obstructive Sleep Apnea (OSA).
- CPAP (Continuous Positive Airway Pressure): Provides constant pressure during both inhalation and exhalation to maintain airway patency.
- BiPAP (Bilevel Positive Airway Pressure): Provides higher pressure during inhalation and lower pressure during exhalation.
Nursing interventions
- Monitor vital signs and SpO2 (pulse oximetry).
- Ensure proper fit of delivery devices.
- Assess skin integrity, particularly for face masks and face tents (check for moisture and chafing).
- Titrate oxygen as ordered to maintain target saturation.
- Educate patients on combustion risks (oxygen is odorless/colorless).
|
SKILL: ADMINISTRATION OF OXYGEN (CANNULA, MASK, AND TENT) Pre-administration parameters Prior to initiation, the clinician must verify: Medical Order: Specific delivery device and flow rate (L/min) or FiO2 percentage. Laboratory Data: Baseline Arterial Blood Gases (ABGs). Normal PaO2 = 80 to 100 mmHg; Normal PaCO2 = 35 to 45 mmHg. Pulse Oximetry: Noninvasive SpO2 if ABGs are unavailable. COPD Status: Patients with Chronic Obstructive Pulmonary Disease may rely on a hypoxic drive to breathe; excessive oxygen can suppress ventilation. Planning and delegation Professional Scope: Initiation of oxygen therapy is a nursing responsibility and cannot be delegated to Unlicensed Assistive Personnel (UAP). UAP Role: May reapply the delivery device and report observations to the nurse. Interprofessional Collaboration: Respiratory therapists often establish initial equipment and contribute to the clinical plan. Implementation protocol Preparation: Verify the provider order and perform a respiratory baseline. Position the client in semi-Fowler's to facilitate maximal diaphragmatic excursion and chest expansion. Explain safety protocols (combustion risks). Equipment Set-up: Attach the flow meter in the "off" position. Fill the humidifier with distilled water (required for flows > 4 L/min). Connect tubing and verify oxygen flow (bubbles in humidifier, audible/palpable flow at the prongs/mask). Application Techniques: Nasal Cannula: Insert prongs into nares; loop tubing over ears. Pad the tubing at the ears and cheekbones to prevent pressure injuries. Face Mask: Apply from the nose downward. Ensure a snug fit to prevent oxygen leakage into the eyes. Face Tent: Fits over the chin and nose; ideal for patients with claustrophobia or facial trauma. Monitoring and evaluation Initial Assessment: Re-evaluate the patient 15 to 30 minutes after initiation. Skin Integrity: Cannula: Inspect nares for encrustation/irritation. Use water-soluble lubricants only (avoid petroleum-based products). Mask/Tent: Inspect facial skin for dampness or chafing; dry the skin frequently. Equipment Maintenance: Check water levels in the humidifier and ensure no condensation exists in the dependent loops of the tubing. Documentation: Record the flow rate, delivery device, SpO2 levels, and the patient's respiratory response. |
7.3 ARTIFICIAL AIRWAYS AND AIRWAY MANAGEMENT
Artificial airways are technical interventions used to maintain a patent air passage for patients with actual or potential airway obstruction. Clinical patency is mandatory for gas exchange between the external environment and the pulmonary parenchyma.
TYPES OF ARTIFICIAL AIRWAYS
1. Oropharyngeal and nasopharyngeal airways
Used to maintain upper airway patency by preventing the tongue or secretions from obstructing the pharynx. Indicated for patients who are sedated, semicomatose, or have an altered level of consciousness (ALC).
Oropharyngeal airways
- Indication: Patients with ALC (general anesthesia, overdose, head injury).
- Contraindication: Conscious patients; these devices stimulate the gag reflex.
- Insertion Procedure:
- Position patient supine or semi-Fowler's.
- Lubricate with water or saline.
- Insert with distal end curved upward along the top of the tongue.
- Rotate 180 degrees downward when distal end reaches the soft palate.
- Clinical Nursing Care:
- Do not tape in place.
- Remove when cough or gag reflex returns.
- Provide oral hygiene every 2 to 4 hours.
- Remove and reassess oral mucosa every 8 hours.
Nasopharyngeal airways
- Indication: Better tolerated by alert patients.
- Insertion: Inserted through the nares and terminates in the oropharynx.
- Clinical Nursing Care:
- Lubricate with water-soluble gel before insertion.
- Provide frequent care to nares and oral cavity.
- Reinsert in the contralateral naris every 8 hours to prevent mucosal necrosis.
2. Endotracheal tubes (ETT)
- Indications: General anesthesia or emergency mechanical ventilation.
- Insertion: Performed by advanced providers (Anesthesiologist, CRNA, Primary Care Provider, Respiratory Therapist).
- Anatomy: Inserted via mouth or nose into the trachea using a laryngoscope. Terminates superior to the tracheal bifurcation (carina).
- Physiological Impact: Passes through the epiglottis and glottis, rendering the patient unable to speak.
- Features: May include an air-filled cuff to prevent air leaks and facilitate positive pressure ventilation.
3. Tracheostomy
A surgical or percutaneous opening into the trachea through the neck.
- Techniques:
- Traditional open surgical: Performed in the operating room.
- Percutaneous: Can be performed at the bedside in critical care units.
- Components:
- Outer Cannula: Maintains the airway stoma.
- Inner Cannula: Removable for cleaning to prevent mucous obstruction.
- Obturator: Used only during insertion; must be kept at bedside (along with two spare tubes, one of the same size and one smaller) for emergency reinsertion.
- Flange: Secures the tube to the neck using ties or Velcro.
- Tube Types:
- Fenestrated: Has openings allowing air to pass over vocal cords for communication.
- Cuffed: Essential for mechanical ventilation; creates an airtight seal to prevent aspiration.
- Low-pressure cuff: Minimizes risk of tracheal tissue necrosis.
- Foam cuff: Conforms to trachea via ambient air; must be deflated for insertion/removal.
- Clinical Nursing Care:
- Sterile technique for new tracheostomies.
- Suction and clean every 1 to 2 hours initially.
- Provide humidification (mist collar or Swedish nose) since upper airway filtration/warming is bypassed.
Clinical purposes
- Airway Patency: Removal of obstructing secretions.
- Infection Control: Maintaining cleanliness of the stoma and site.
- Skin Integrity: Preventing excoriation from moisture or drainage.
- Wound Healing: Facilitating the healing process of the tracheostomy incision.
Assessment parameters
- Respiratory Status: Ease of breathing, rate, rhythm, depth, lung sounds, and SpO2.
- Cardiovascular Status: Pulse rate.
- Stoma/Incision: Redness, swelling, odor, or purulent discharge.
- Secretions: Character, color, and volume of drainage on the dressing or ties.
Delegation and practice
- Clinical Scope: Tracheostomy care requires sterile technique and scientific problem-solving. It must be performed by a Registered Nurse or Respiratory Therapist.
- Communication: Establish a non-verbal signal (e.g., eye blinking, finger raising) before starting to allow the patient to indicate distress.
Implementation protocol
- PREPARATION
- Position: semi-Fowler’s or Fowler’s position.
- Initial Suctioning: Suction the tracheostomy tube prior to care if secretions are present. Allow the patient to rest and re-oxygenate afterward.
- Field Setup: Establish a sterile field. Pour sterile normal saline (and soaking solution if prescribed) into separate containers.
- INNER CANNULA CARE
- Removal: Apply clean gloves. Unlock and remove the inner cannula following its natural curvature.
- Soaking: Place the non-disposable inner cannula in the soaking solution to loosen dried secretions.
- Cleaning: Apply sterile gloves. Use a sterile brush or pipe cleaner moistened with saline to clean the lumen.
- Inspection: Hold the cannula at eye level and look through it to ensure no obstructions remain.
- Drying: Tap against the saline container and dry the interior with a folded pipe cleaner. Leave the exterior moist to act as a lubricant for reinsertion.
- Reinsertion: Lock the cleaned (or new disposable) inner cannula back into the outer cannula.
- STOMA AND FLANGE CARE
- Cleaning: Use sterile applicators or gauze moistened with saline.
- Technique: Use each applicator only once. Clean from the stoma outward to avoid contamination.
- Hydrogen Peroxide: Only use if required for crusty secretions and according to agency policy. Must be rinsed thoroughly with saline to prevent skin irritation.
- Drying: Thoroughly pat the skin and tube flanges dry to prevent fungal growth and excoriation.
- DRESSING APPLICATION
- Materials: Use a commercially prepared split-gauze (non-raveling).
- Contraindication: Never cut standard 4x4 gauze squares; loose fibers can be aspirated and cause tracheal abscesses.
- Placement: Slide the dressing under the flange while supporting the tube to prevent movement/irritation.
- SECURING THE TUBE (TIES AND COLLARS)
- Safety: A two-person technique is recommended to prevent accidental decannulation (tube dislodgement). One person holds the tube while the second replaces the ties.
- Methods:
- Two-Strip Twill Tape: Use unequal lengths (25 cm and 50 cm) so the knot sits at the side of the neck.
- One-Strip Twill Tape: Thread through both flanges and tie at the side.
- Velcro Collar: Faster and less abrasive to the skin.
- Tension Rule: Always place one finger between the tie/collar and the patient’s neck while the neck is flexed. Prevents the tie from being too tight, which can obstruct jugular venous return or interfere with coughing.
LONG-TERM AND HOME CARE CONSIDERATIONS
- Technique Evolution: For tracheostomies older than 1 month, clean technique (rather than sterile) is typically used in the home setting.
- Caregiver Training: Ensure the caregiver can perform a return demonstration and identify signs of infection.
- Emergency Prep: Provide emergency contact numbers and support group information for permanent tracheostomies.
DOCUMENTATION
Record the following:
- Suctioning details.
- Tracheostomy care and dressing change.
- Assessment of the stoma site and respiratory status.
- Patient tolerance of the procedure.
7.4 SUCTIONING PROTOCOLS
The aspiration of secretions to maintain patency. Based on clinical assessment, not a fixed schedule.
Assessment for suctioning indications
- Dyspnea.
- Adventitious breath sounds (bubbling/rattling).
- Pallor, duskiness, or cyanosis.
- Restlessness or tachycardia.
- Decreased O2 saturation (SpO2).
Complications of suctioning
- Hypoxemia.
- Airway trauma.
- Nosocomial infection.
- Cardiac dysrhythmias.
- Increased intracranial pressure.
- Bronchospasm.
Mitigation strategies
- Hyperoxygenation: Delivery of 100% oxygen before and between suction passes. Best method to prevent hypoxemia.
- Hyperinflation: Delivering breaths greater than tidal volume.
- Hyperventilation: Increasing the respiratory rate via ventilator or manual resuscitation bag.
- Technique: Use sterile technique. Limit suctioning to “as needed” status.
- Saline Instillation: Prohibited. Research indicates it causes hypoxemia and increases pneumonia risk.
Equipment types
- Yankauer: For oral cavity suctioning.
- Whistle-tipped catheter: Less irritating to tissues.
- Open-tipped catheter: Effective for thick mucous plugs.
- Closed/In-line suctioning: Catheter remains in a plastic sheath attached to ventilator circuit; reduces caregiver exposure and maintains PEEP.
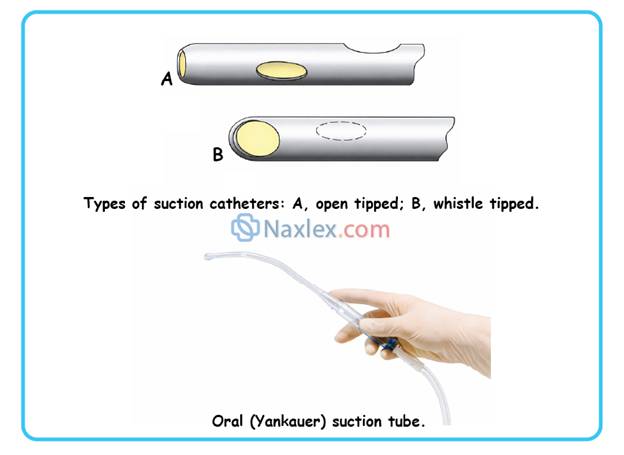
|
SKILL: OROPHARYNGEAL, NASOPHARYNGEAL, AND NASOTRACHEAL SUCTIONING Clinical preparation and orientation Verification: Confirm patient identity via institutional protocol. Education: Inform the patient that suctioning relieves respiratory distress but may trigger the cough, gag, or sneeze reflex. Infection Control: Perform hand hygiene and adhere to Standard Precautions. Privacy: Provide appropriate draping and environment. Patient positioning Conscious Patient (Functional Gag Reflex): Oral Suctioning: Semi-Fowler’s with head turned to one side. Nasal Suctioning: Semi-Fowler’s with neck hyperextended. Rationale: Facilitates catheter advancement and prevents aspiration. Unconscious Patient: Lateral position facing the clinician. Rationale: Prevents the tongue from obstructing the catheter and facilitates pharyngeal drainage. Equipment settings and general rules Suction Pressure: Use the lowest negative pressure required to clear secretions. Rationale: Excessively high pressure can cause the catheter to adhere to the tracheal wall, resulting in mucosal trauma or irritation. Insertion Rule: Never apply suction during insertion. Total Duration: Limit total suctioning time to 5 minutes. Specific implementation by route Oral and oropharyngeal suctioning Gloves: Clean gloves are sufficient. Lubrication: Moisten the Yankauer or catheter tip with sterile water or saline. Technique: Advance the catheter 10 to 15 cm (4 to 6 in.) along the side of the mouth to the oropharynx. Rationale: Sideward placement minimizes stimulation of the gag reflex. Nasopharyngeal and nasotracheal suctioning Gloves: Sterile technique is required. Use a sterile glove for the dominant hand (to handle the catheter) and a clean glove for the nondominant hand (to handle the suction port). Lubrication: Use water-soluble lubricant to reduce friction and mucosal trauma. Insertion: Advance the catheter along the floor of the nasal cavity to avoid the nasal turbinates. Do not force against obstructions.
|
|
SKILL: OROPHARYNGEAL, NASOPHARYNGEAL, AND NASOTRACHEAL SUCTIONING continued
Suctioning execution (performance) Rotation: Apply suction and gently rotate the catheter during withdrawal. Rationale: Ensures contact with all mucosal surfaces and prevents localized trauma. Timing: Apply suction for only 5 to 10 seconds per pass. Total attempt (insertion to removal) should not exceed 10 to 15 seconds. Oxygenation: Provide supplemental oxygen and allow time for ventilation between passes. Encourage deep breathing and coughing. Rinsing: Flush the catheter with sterile saline between passes to maintain patency. Sputum specimen collection (sputum trap) Interpose a sterile sputum trap between the suction catheter and the suction tubing. Perform suctioning; mucus will collect in the trap. To seal: Disconnect the catheter and connect the trap's own tubing to its air vent to prevent contamination or leakage. Post-procedure care and documentation Patient Comfort: Provide oral and nasal hygiene. Position for optimal lung expansion. Equipment Disposal: Wrap the catheter in the glove during removal. Ensure new kits are available at the bedside for emergency use. Assessment: Auscultate breath sounds, monitor SpO2, skin color, and respiratory rate. Clinical documentation requirements Sputum Characteristics: Amount, consistency, color, and odor (e.g., thick, green-tinged, or blood-flecked). Respiratory Status: Pre-procedure and post-procedure lung sounds and oxygen saturation. Frequency: Note the number of times suctioning was required during the shift.
|
7.6 CHEST TUBES AND DRAINAGE SYSTEMS
Physiology and indications
The pleural space maintains negative pressure to keep the lungs expanded. Loss of this pressure causes lung collapse.
- Pneumothorax: Accumulation of air in the pleural space.
- Hemothorax: Accumulation of blood in the pleural space.
- Pleural Effusion: Excessive fluid in the pleural space.
- Purpose of Chest Tubes: To restore negative pressure and evacuate air or fluid.
Anatomical placement
- Air (Pneumothorax): Upper anterior thorax (air rises).
- Fluid/Blood (Hemothorax/Effusion): Lower lateral chest wall (fluid settles).
Drainage system components
- Suction control chamber: Regulates the amount of suction applied; may require water to maintain levels.
- Water-seal chamber: One-way valve that allows air to exit the pleural space during exhalation but prevents atmospheric air from entering during inhalation.
- Collection chamber: A closed reservoir to receive and measure drainage.
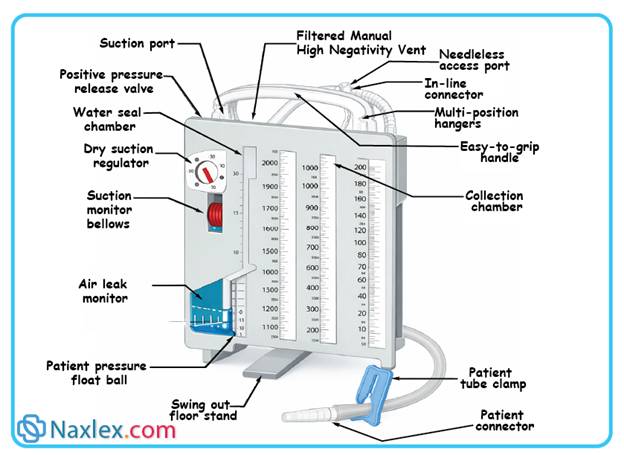
Specialized valves
- Heimlich Valve: A one-way flutter valve for ambulatory patients. Arrows must point away from the patient. Not for fluid collection.
- Pneumostat: One-way valve with a small built-in collection chamber for pneumothorax patients with minimal drainage.
Nursing responsibilities and monitoring
- Assessment: Monitor vital signs, SpO2, and cardiovascular status. Perform bilateral auscultation to ensure symmetry of breath sounds.
- Site Care: Inspect the dressing every 4 hours for bleeding or foul odor.
- Subcutaneous Emphysema: Palpate for a crackling sensation under the skin, indicating air is leaking into the subcutaneous tissues.
- Positioning: Keep the collection device below the level of the chest at all times. Reposition the patient every 2 hours; use rolled towels to prevent the patient from occluding the tubing.
Maintaining system integrity
- Taping: Ensure all connections are securely taped.
- Tidaling: The water-seal level should fluctuate (rise and fall) with the patient's respiratory effort.
- Evaporation: Monitor water levels in the water-seal and suction chambers; add sterile water as needed.
- Milking/Stripping: Avoid aggressive manipulation. It creates excessive negative pressure that can damage pleural tissue.
- Clamping: Strictly prohibited during transport. Only clamp momentarily to change the drainage unit or check for leaks. Prolonged clamping risks a tension pneumothorax.
Emergency interventions
- System Disconnection: Immediately submerge the distal end of the chest tube in 2.5 cm (1 in.) of sterile saline or water to create a temporary water seal.
- Accidental tube removal: Cover the site immediately with a dry sterile dressing. If an air leak is audible, ensure the dressing is not occlusive to prevent air buildup.
- Tension pneumothorax: A life-threatening complication where air accumulates under pressure, shifting mediastinal structures and compromising cardiac output.
Patient mobility and comfort
- Exercises: Perform Range of Motion (ROM) of the affected shoulder 3 times per day.
- Pulmonary hygiene: Encourage coughing and deep breathing every 2 hours (unless contraindicated, as in pneumonectomy). Use a pillow to splint the insertion site during these exercises.
- Pain management: Medicate as indicated, especially prior to chest tube removal.
Tube removal
- Procedure: Performed by a primary care provider or specially trained nurse.
- Technique: Requires sterile technique.
- Dressing: An occlusive dressing is applied post-removal to prevent air from entering the pleural space.
Summary
- Respiration is the process of gas exchange between the individual and the environment.
- The respiratory system contributes to effective respiration through pulmonary ventilation (the movement of air between the atmosphere and the lungs), the diffusion of oxygen and carbon dioxide across the pulmonary membrane, transport of oxygen from the tissues to the lungs and carbon dioxide from the tissues to the lungs, and transport of oxygen and carbon dioxide between the systemic capillaries and the tissues.
- Normal respirations are quiet and unlabored; altered respiratory patterns include tachypnea, bradypnea, hyperventilation, hypoventilation, and dyspnea. Shortness of breath is a subjective sensation of not getting enough air.
- Diagnostic tests that may be performed to assess oxygenation include sputum and throat culture specimens; blood tests such as arterial blood gases; pulmonary function tests; and visualization procedures such as x-rays, lung scans, laryngoscopy, and bronchoscopy.
- Nursing interventions to promote oxygenation include promoting healthy breathing, deep breathing and coughing, and hydration; administering medications; implementing measures to clear secretions (e.g., incentive spirometry, percussion, vibration, postural drainage, and mucus clearing devices); initiating and monitoring oxygen therapy; initiating or assisting with procedures to maintain the airway (e.g., artificial airways and suctioning); providing tracheostomy care; and monitoring chest drainage systems.
