
Fetal Development
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
Upon completion of this comprehensive review, the nursing student will be able to:
• Articulate the intricate processes of human fertilization, implantation, and early embryonic development.
• Delineate the sequential developmental milestones of the fetus across all three trimesters of gestation.
• Identify critical physiological changes occurring within the developing fetus, encompassing organogenesis, growth, and maturation.
• Recognize the impact of various teratogens on fetal development during sensitive periods of gestation.
• Formulate evidence-based nursing interventions and patient education strategies pertinent to each trimester of pregnancy.
• Comprehend the significance of diagnostic assessments utilized throughout gestation to monitor fetal well-being and identify potential complications.
• Integrate knowledge of fetal development into holistic maternal-newborn nursing care, optimizing outcomes for both mother and neonate.
Introduction
The trajectory of human fetal development is a complex and exquisitely orchestrated biological process, commencing with the fusion of gametes and culminating in the birth of a neonate capable of extrauterine existence. This profound journey, spanning approximately 40 weeks of gestation, involves intricate cellular differentiation, tissue morphogenesis, and organ system maturation. A comprehensive understanding of these developmental phenomena is paramount for professional nursing practice within the maternal-newborn specialty. This document aims to provide an extensive, scientifically rigorous overview of fetal development, emphasizing key physiological milestones, potential vulnerabilities, and essential nursing considerations, thereby equipping nursing students with the requisite knowledge for exemplary patient care and academic success.
First Trimester: Weeks 1-13
The first trimester represents a period of rapid and profound developmental changes, laying the foundational structures for all subsequent growth and maturation.
1. Fertilization and Implantation
• Gamete Genesis and Transport:
➤ Spermatogenesis involves the continuous production of spermatozoa within the seminiferous tubules of the testes, a process typically lasting approximately 70 days. Mature spermatozoa possess a distinct morphology, including a head containing the haploid nucleus, a midpiece replete with mitochondria for ATP generation, and a flagellum for propulsive motility.
➤ Oogenesis, the developmental process of ova, initiates prenatally with primordial germ cells differentiating into oogonia. Meiosis I is arrested in prophase I until the onset of puberty. During each ovarian cycle, under hormonal influence, one primary oocyte completes meiosis I to yield a large secondary oocyte and a diminutive first polar body. Meiosis II is subsequently arrested in metaphase II, only completing upon successful fertilization.
➤ Ovulation typically occurs around day 14 of a standardized 28-day menstrual cycle, wherein the mature secondary oocyte is expelled from the ruptured graafian follicle and expeditiously captured by the fimbriae of the fallopian tube.
➤ Spermatozoa, deposited in the posterior vaginal fornix during coitus, undertake a formidable journey through the cervical canal, across the endometrial cavity, and into the fallopian tubes. Spermatozoal viability within the female reproductive tract can persist for up to 72 hours, although their fertilizing capacity significantly diminishes beyond 24 hours. Conversely, the ovum maintains its fertilizable capacity for a more limited window of approximately 12-24 hours post-ovulation.
• Fertilization:
➤ Fertilization, defined as the intricate fusion of a single spermatozoon with a secondary oocyte, most commonly transpires within the ampulla of the fallopian tube.
➤ Capacitation: This is a crucial physiological conditioning process that spermatozoa undergo within the female reproductive tract, culminating in enhanced motility and preparing them for the subsequent acrosomal reaction. It entails the enzymatic removal of a glycoprotein coat and seminal plasma proteins from the acrosomal region of the sperm head.
➤ Acrosomal Reaction: Upon encountering the corona radiata and the underlying zona pellucida, the glycoprotein layer surrounding the ovum, the capacitated sperm's acrosome releases an array of hydrolytic enzymes, notably hyaluronidase and acrosin. These enzymes facilitate the localized degradation of the extracellular matrix, enabling sperm penetration through these protective layers.
➤ Sperm Penetration: A singular spermatozoon successfully traverses the zona pellucida and subsequently fuses with the oocyte's plasma membrane.
➤ Cortical Reaction: The binding and entry of the first spermatozoon into the oocyte cytoplasm instantaneously trigger the cortical reaction. This exocytotic event involves the release of specialized cortical granules from the oocyte's periphery into the perivitelline space. The contents of these granules induce biochemical alterations in the zona pellucida, rendering it impermeable to subsequent spermatozoa and thereby critically preventing polyspermy (fertilization by multiple sperm, which would result in a non-viable triploid zygote).
➤ Completion of Meiosis II: The influx of calcium ions following sperm penetration stimulates the secondary oocyte to promptly complete its second meiotic division. This results in the formation of a mature ovum (ootid), containing the female pronucleus, and the extrusion of a second polar body.
➤ Pronuclei Formation and Fusion: The haploid nucleus of the fertilizing spermatozoon decondenses to form the male pronucleus, while the newly formed ovum's nucleus becomes the female pronucleus. These two pronuclei replicate their DNA and subsequently fuse, establishing a single diploid nucleus. The resultant unicellular entity, now possessing a full complement of 46 chromosomes (23 from each gamete), is designated a zygote.
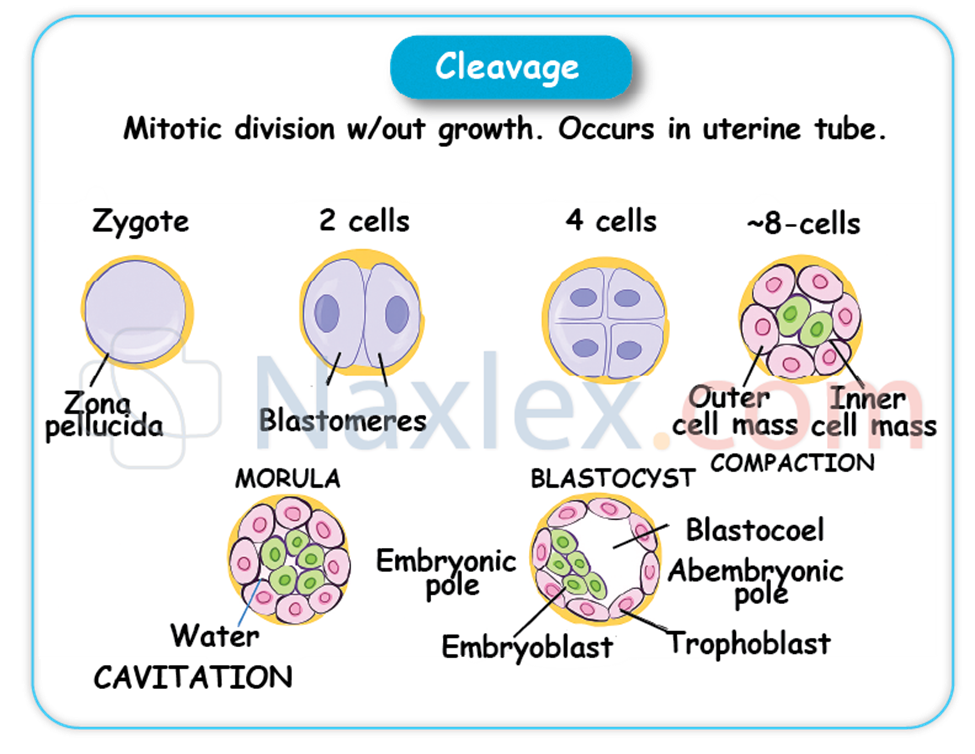
• Cleavage and Morula Formation:
➤ Following fertilization, the zygote commences a series of rapid mitotic divisions, collectively termed cleavage, as it embarks on its journey down the fallopian tube towards the uterine cavity.
➤ These divisions are characterized by an increase in cell number (blastomeres) without a concomitant increase in the overall size of the conceptus.
➤ By approximately 3-4 days post-fertilization, the cleaving zygote typically comprises 12-32 blastomeres, forming a compact, solid ball resembling a mulberry, which is termed the morula.
• Blastocyst Formation:
➤ As the morula enters the uterine cavity, fluid from the uterine glands begins to permeate its intercellular spaces, coalescing to form a progressively expanding fluid-filled cavity known as the blastocoel (or blastocyst cavity).
➤ This cavitation process transforms the morula into a blastocyst, a developmental stage typically achieved by day 4-5 post-fertilization.
➤ The blastocyst differentiates into two primary, functionally distinct cell populations:
◆ Trophoblast: This is the outer epithelial layer of cells that will predominantly contribute to the formation of the embryonic portion of the placenta. Trophoblast cells are pivotal in mediating the intricate processes of implantation and subsequent nutrient and gas exchange between the maternal and fetal circulations.
◆ Inner Cell Mass (Embryoblast): This is an eccentrically positioned cluster of pluripotent cells located within the blastocoel. The embryoblast is destined to develop into the embryo proper and several extraembryonic membranes.
• Implantation:
➤ Implantation, the critical process by which the blastocyst firmly embeds itself into the prepared endometrial lining (now termed the decidua due to its gestational modifications), typically occurs approximately 6-10 days after fertilization. The most common site for implantation is the posterior superior wall of the uterine fundus.
➤ The trophoblast cells, particularly the syncytiotrophoblast, secrete proteolytic enzymes that enzymatically erode the compact layer of the decidua, facilitating the invasive embedding of the blastocyst.
➤ Human Chorionic Gonadotropin (hCG): Crucially, the syncytiotrophoblast cells commence the secretion of human chorionic gonadotropin (hCG) shortly after implantation. This glycoprotein hormone is indispensable for rescuing and maintaining the corpus luteum in the ovary. The corpus luteum, under the sustained stimulation of hCG, continues to produce vital progesterone, which is essential for sustaining the integrity of the endometrial lining and inhibiting the onset of menstruation. This hormonal support is critical for the early maintenance of pregnancy. The detection of elevated hCG levels in maternal serum or urine forms the biochemical basis for current pregnancy tests.
Nursing Insights:
• Practical Application: Patient Education on Conception: A comprehensive understanding of the precise timing of ovulation and the lifespan of spermatozoa and ova is fundamental for nurses when providing patient education regarding optimizing conception efforts or implementing natural family planning methods. For instance, advising couples to engage in coitus around the estimated time of ovulation, considering sperm viability, can significantly increase the likelihood of fertilization.
• Practical Application: Preventing Polyspermy: The cortical reaction is a highly specialized biological mechanism. Nurses should appreciate that while not directly intervened upon in clinical practice, its failure could lead to non-viable pregnancies, reinforcing the precision of early human development.
• Practical Application: Confirming Pregnancy and Early Management: The detection of hCG through qualitative or quantitative assays serves as the earliest biochemical confirmation of pregnancy. Nurses utilize this principle daily, interpreting positive home pregnancy tests and ordering serum quantitative hCG levels to monitor early pregnancy progression or evaluate potential complications such as ectopic pregnancy or miscarriage. Serial hCG levels are often monitored to assess the viability and progression of the early gestation.
2. Embryonic Period (Weeks 3-8)
This period is characterized by unparalleled cellular proliferation, intricate differentiation, and complex morphogenesis, culminating in the establishment of all major organ systems. Consequently, it represents the most sensitive and critical window of vulnerability to teratogenic insults.
• Development of the Bilaminar Disc (Week 2):
➤ During the second week of development, the embryoblast undergoes further differentiation, forming two distinct, apposed germ layers, giving rise to the bilaminar embryonic disc:
◆ Epiblast: This dorsal, columnar cell layer is directly adjacent to the developing amniotic cavity and will serve as the progenitor for the three primary germ layers during gastrulation.
◆ Hypoblast: This ventral, cuboidal cell layer is adjacent to the primary yolk sac.
➤ Concurrently, the amniotic cavity expands within the epiblast, providing a protective fluid-filled environment for the developing embryo.
• Gastrulation and Formation of the Trilaminar Embryonic Disc (Week 3):
➤ Gastrulation is a profoundly significant developmental event occurring during the third week, involving extensive cell migration, rearrangement, and differentiation. During this process, the epiblast cells migrate through the primitive streak to form three distinct primary germ layers, establishing the trilaminar embryonic disc:
◆ Ectoderm: This outermost germ layer differentiates to form the central nervous system (including the brain, spinal cord, and cranial nerves), the epidermis and its appendages (skin, hair, nails, sweat glands), mammary glands, the anterior pituitary gland, the enamel of teeth, and the sensory epithelia of the eyes, ears, and nose.
◆ Mesoderm: This middle germ layer is highly diverse, giving rise to the entire musculoskeletal system (muscles, bones, cartilage, connective tissues), the cardiovascular system (heart, blood vessels, blood cells, lymphatic vessels), the urogenital system (kidneys, gonads, reproductive ducts), the spleen, the adrenal cortex, and the dermis of the skin.
◆ Endoderm: This innermost germ layer forms the epithelial lining of the entire gastrointestinal tract (from pharynx to anus), the epithelial lining of the respiratory system (trachea, bronchi, lungs), the parenchyma of associated glands such as the liver and pancreas, the thyroid and parathyroid glands, and the thymus.
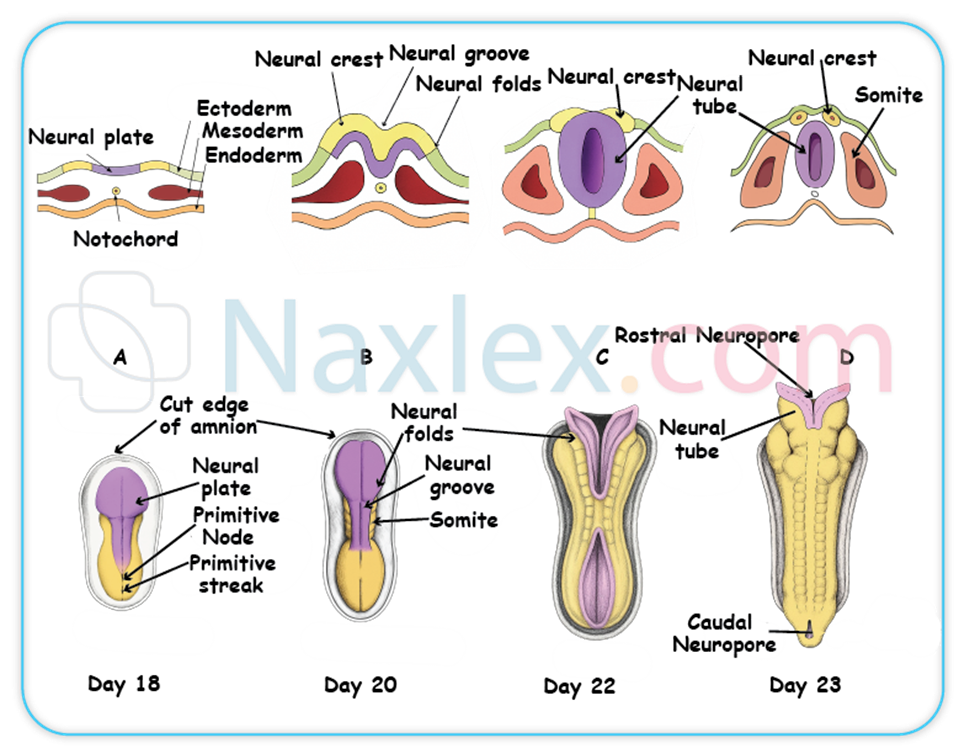
• Neurulation (Weeks 3-4):
➤ Neurulation is the process by which the neural plate forms, folds, and fuses to create the neural tube. This critical process commences during the third week and completes by the end of the fourth week.
➤ The ectoderm overlying the notochord (a transient, mesoderm-derived rod-like structure that serves as a primary inducer) thickens to form the neural plate.
➤ The neural plate then invaginates centrally, forming the neural groove, flanked by neural folds.
➤ The neural folds subsequently elevate and fuse dorsally, effectively closing off to form the neural tube.
➤ The neural tube is the primordium of the entire brain and spinal cord.
➤ Neural tube defects (NTDs), such as spina bifida (incomplete closure of the caudal neural tube) and anencephaly (incomplete closure of the cranial neural tube, resulting in absence of major parts of the brain and skull), arise from incomplete fusion of the neural tube. Folic acid supplementation (specifically 400 mcg daily for all women of childbearing age, and 4 mg daily for those with a prior history of NTD-affected pregnancy) is unequivocally critical for the primary prevention of NTDs.
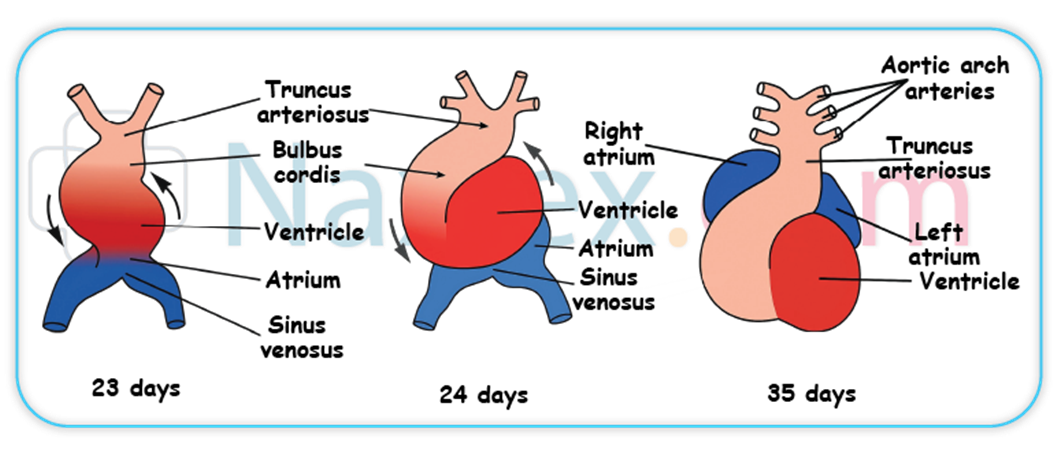
• Cardiovascular Development (Weeks 3-8):
➤ The primitive heart tube begins to form from cardiogenic mesoderm during the third week and initiates rudimentary circulation by the end of week 3 or early week 4, making the cardiovascular system the first major organ system to become functionally active.
➤ By week 5, the tubular heart has folded and begins to beat rhythmically, propelling blood through the embryonic circulation.
➤ By week 6, fetal cardiac activity is typically definitively detectable via transvaginal ultrasound, providing objective evidence of embryonic viability.
➤ During this period, the heart undergoes septation to form the four distinct chambers, and major blood vessels (e.g., aorta, pulmonary artery) develop.
• Other Organogenesis:
➤ Limb Buds: Upper limb buds emerge at the end of week 4, followed closely by the appearance of lower limb buds during week 5. These buds elongate and flatten to form paddle-like structures.
➤ Eye and Ear Placodes: Early developmental precursors of the sensory organs, specifically the optic placodes (future eyes) and otic placodes (future ears), become discernible.
➤ Gastrointestinal Tract: The primitive gut tube differentiates into foregut, midgut, and hindgut. Liver and pancreatic buds, crucial for digestive and metabolic functions, emerge from the endoderm.
➤ Respiratory System: The laryngotracheal groove forms, and lung buds emerge from the foregut, initiating the development of the bronchial tree.
➤ Kidney Development: A sequence of kidney precursors appears: the pronephros (transient), followed by the mesonephros, before the definitive kidney, the metanephros, begins its formation.

Nursing Insights:
• Practical Application: Teratogen Counseling: The embryonic period (weeks 3-8) is the most vulnerable to teratogens due to the simultaneous rapid organogenesis of all major body systems. Nurses must provide rigorous and comprehensive patient education regarding the avoidance of known teratogens, including alcohol, illicit drugs, certain prescription and over-the-counter medications (e.g., isotretinoin, thalidomide), excessive radiation exposure, and specific infectious agents (e.g., rubella, cytomegalovirus). For example, a pregnant patient presenting for their first prenatal visit at 7 weeks gestation needs explicit counseling on discontinuing alcohol consumption immediately due to the risk of Fetal Alcohol Spectrum Disorders.
• Practical Application: Folic Acid Adherence: Nurses must vehemently emphasize the critical role of folic acid supplementation in the periconceptional period to prevent neural tube defects. This involves counseling all women of childbearing potential, not just those planning pregnancy, on daily supplementation, as neural tube closure occurs very early in gestation, often before pregnancy is even recognized. Documenting patient adherence to folic acid supplementation is a vital nursing responsibility.
• Practical Application: Early Pregnancy Viability Assessment: The visualization of fetal cardiac activity via transvaginal ultrasound as early as 6 weeks gestation is a pivotal finding for confirming pregnancy viability and providing significant reassurance to expectant parents. Nurses preparing patients for such scans should explain what to expect and be prepared to address the emotional responses to this early visualization of life.
3. Fetal Period (Weeks 9-13)
By the commencement of the fetal period at week 9, all major organ systems have been established in rudimentary form. This subsequent period is predominantly characterized by exponential growth, accelerated maturation, and functional refinement of these existing structures.
• Differentiation and Growth:
➤ From week 9 onward, the developing organism is unequivocally referred to as a fetus.
➤ This period witnesses a rapid linear increase in crown-rump length and a substantial gain in overall body mass. By the completion of week 12, the fetus typically measures approximately 6-7 cm in crown-rump length and possesses a body mass of around 14 grams.
➤ During these early fetal weeks, the head remains disproportionately large in relation to the developing trunk and limbs, reflecting the accelerated growth and differentiation of the brain.
• Organ System Maturation:
➤ Cardiovascular System: The four-chambered heart is fully formed, and cardiac septation is complete. The unique fetal circulatory patterns, incorporating critical shunts such as the ductus arteriosus (connecting the pulmonary artery to the aorta), foramen ovale (an opening between the right and left atria), and ductus venosus (bypassing the liver), are well-established to optimize oxygen delivery in the intrauterine environment.
➤ Renal System: The metanephros, the definitive kidney, becomes functional and commences urine production. This fetal urine is subsequently excreted into the amniotic fluid, playing a vital role in contributing to and maintaining its volume. By week 12, the kidneys are demonstrable as functionally active.
➤ Gastrointestinal System: The intestines, which undergo a transient physiological herniation into the umbilical cord during the embryonic period, complete their retraction into the abdominal cavity by approximately week 10. The liver, a significant hematopoietic organ at this stage, begins to produce bile.
➤ External Genitalia: Gross differentiation of the external genitalia progresses sufficiently to allow for the reliable determination of fetal sex via ultrasound examination by week 12-14.
➤ Musculoskeletal System: The limbs are well-formed with identifiable digits (fingers and toes). While fetal movements are present and discernible on ultrasound, they are generally not yet strong enough to be perceived by the expectant mother.
➤ Endocrine System: The thyroid gland initiates the production of thyroid hormones, crucial for fetal growth and neurological development. The pancreas begins to synthesize insulin.
➤ Hematopoietic System: The primary site of erythropoiesis (red blood cell production) transitions from the yolk sac to the developing liver, signifying the increasing sophistication of fetal organ function.
Nursing Insights:
• Practical Application: Transition from Embryo to Fetus: Nurses should effectively communicate to parents that the transition from "embryo" to "fetus" at week 9 signifies the completion of major organ formation. This typically corresponds to a decreased, though not absent, susceptibility to gross congenital anomalies, shifting the developmental focus towards growth and functional maturation.
• Practical Application: Fetal Kidney Function and Amniotic Fluid: The understanding that fetal urine production is the primary contributor to amniotic fluid volume after the first trimester is critical. Nurses should recognize that oligohydramnios (abnormally low amniotic fluid) can be an indicator of underlying fetal renal dysfunction or urinary tract obstruction. Conversely, polyhydramnios (excessive amniotic fluid) may suggest impaired fetal swallowing or other anomalies.
• Practical Application: Sex Determination and Communication: While sex determination by ultrasound at 12-14 weeks can be an exciting milestone for expectant parents, nurses must approach this topic with sensitivity. Some parents may prefer not to know, or the visualization may be challenging, requiring careful communication to manage expectations and provide accurate information.
Second Trimester: Weeks 14-27
The second trimester is frequently referred to as the "golden trimester" in maternal health, attributable to a notable reduction in the common discomforts of early pregnancy for the expectant mother and a period characterized by substantial fetal growth and intricate refinement of developing organ systems.
1. Continued Growth and Maturation
• Growth and Proportions:
➤ This trimester is marked by a prodigious increase in fetal length and overall body mass. By the cessation of week 27, the fetus typically attains a crown-heel length of approximately 37 cm and weighs around 1000 grams (1 kg), reflecting exponential growth.
➤ Fetal body proportions gradually normalize; while cephalic growth continues, the accelerated development of the trunk and limbs leads to a more proportionate and recognizable human form.
➤ Fundal Height Measurement: The uterine fundal height, meticulously measured in centimeters from the symphysis pubis to the superior aspect of the uterine fundus, generally correlates precisely with the gestational age in weeks after the 20th week of gestation (e.g., 20 cm at 20 weeks). At 16 weeks gestation, the anticipated fundal height measurement is approximately 14-18 cm. This clinical assessment provides a rapid, non-invasive estimation of fetal growth and gestational age.
• Integumentary System:
➤ Lanugo: A fine, soft, downy hair, known as lanugo, begins to uniformly cover the fetal body. This serves as a primary insulating layer, aiding in thermoregulation within the aqueous amniotic environment.

➤ Vernix Caseosa: A unctuous, white, and protective substance, comprised of desquamated epithelial cells and sebaceous gland secretions, commences its formation and uniformly coats the fetal skin around week 19-20. The vernix caseosa acts as a crucial barrier, safeguarding the delicate fetal skin from chronic maceration and desiccation by the amniotic fluid, and also contributes to postnatal thermoregulation.

➤ Subcutaneous fat deposition initiates during this period, contributing to a more rounded and less translucent appearance of the fetal integument.
• Musculoskeletal System:
➤ The process of ossification and subsequent hardening of the fetal skeleton continues progressively.
➤ Fetal musculature gains strength and tone, leading to increasingly coordinated and purposeful movements.
➤ Quickening: The maternal perception of initial fetal movements, termed quickening, typically occurs around weeks 16-20 for primigravida mothers (those experiencing their first pregnancy). Multigravida mothers, having prior experience, often perceive quickening earlier due to heightened awareness of sensations. This is a profound and emotionally significant milestone for expectant parents.
• Sensory Development:
➤ The eyes are structurally well-developed, and the eyelids typically remain fused shut until approximately 26 weeks of gestation, after which they separate and can open.
➤ The auditory system continues its intricate maturation, enabling the fetus to respond to external sound stimuli.
➤ Taste buds are actively differentiating and maturing on the fetal tongue.
• Respiratory System:
➤ The pulmonary system undergoes continued branching of bronchioles and proliferation of alveolar ducts.
➤ Surfactant Production: Type II pneumocytes, specialized alveolar cells within the fetal lungs, initiate the production of surfactant (a complex lipoprotein that functions to reduce surface tension at the air-liquid interface within the alveoli, preventing alveolar collapse during expiration) around week 24. Although present, surfactant levels at this stage are not yet sufficient to support independent, sustained extrauterine respiration. Adequate surfactant is paramount for successful lung expansion and gas exchange post-birth.
• Hematopoietic System:
➤ The primary site of red blood cell production undergoes a significant physiological shift from the liver to the developing bone marrow.
Nursing Insights:
• Practical Application: Fetal Movement Education: Nurses must comprehensively educate expectant mothers on the significance of quickening and, subsequently, the importance of daily fetal movement counts (kick counts) as a simple yet effective non-invasive method for assessing fetal well-being. A reduction in perceived movements warrants immediate evaluation. For example, instruct a patient to lie on their side and count movements for an hour; if fewer than 10 distinct movements are felt, advise them to consume a sugary beverage and re-count, contacting their provider if still fewer than 10 movements occur within two hours.
• Practical Application: Explaining Fetal Skin Coverings: When parents inquire about the appearance of their newborn, nurses should explain the physiological roles of lanugo and vernix caseosa. This can alleviate potential concerns regarding their presence at birth, emphasizing their protective functions in utero rather than indicating an abnormality.
• Practical Application: Pulmonary Maturity and Preterm Birth: The knowledge of surfactant production onset around 24 weeks is crucial for understanding fetal viability at earlier gestational ages. Nurses caring for patients at risk of preterm labor will anticipate and administer antenatal corticosteroids (e.g., betamethasone) to accelerate fetal lung maturity, demonstrating a direct correlation between scientific understanding and clinical intervention.
2. Fetal Milestones
• Week 14: The fetus demonstrates active, coordinated movements, including suck and swallow movements, indicative of advancing neurological maturation.
• Week 16: Fetal sex is typically reliably determinable via high-resolution ultrasound. The external genitalia are visually distinct. The uterine fundus is palpable approximately midway between the symphysis pubis and the umbilicus.
• Week 18: Fetal heart tones are typically audible with a traditional fetoscope, providing an audibly reassuring sign of fetal viability.
• Week 20: Quickening is almost universally perceived by primigravida mothers. Both lanugo and vernix caseosa become evident. The fetus measures approximately 25 cm in crown-heel length.
• Week 24: The pulmonary system achieves a critical milestone with the initiation of significant surfactant production. At this gestational age, the fetus is considered to reach the threshold of viability, meaning it possesses a reasonable chance of survival outside the uterus with advanced intensive medical support.
• Week 26: The fetal eyelids separate, allowing the eyes to open and close. Distinct fetal sleep-wake cycles emerge, reflecting neurological maturation. The fetus demonstrates responsiveness to auditory stimuli.
• Diagnostic Tests:
➤ Ultrasound (Mid-Pregnancy Anomaly Scan, typically 18-22 weeks): This is a comprehensive, detailed anatomical assessment to meticulously evaluate fetal structures for congenital anomalies, ascertain precise fetal growth parameters, confirm placental location, and measure amniotic fluid volume. This ultrasound is paramount for early detection of potential structural abnormalities.
➤ Amniocentesis: This invasive diagnostic procedure may be performed between weeks 15-20 to obtain amniotic fluid for genetic analysis. It is indicated for the diagnosis of chromosomal abnormalities (e.g., Down syndrome), specific genetic disorders, or neural tube defects, particularly in high-risk pregnancies (e.g., advanced maternal age, abnormal genetic screening results, family history of genetic conditions).
➤ Maternal Serum Alpha-Fetoprotein (MSAFP) Screening (15-20 weeks): This maternal blood test is a screening tool used to assess the risk for neural tube defects (elevated MSAFP) and certain chromosomal abnormalities, notably Down syndrome (decreased MSAFP in conjunction with other markers in a quad screen). It is a screening, not diagnostic, test.
Nursing Insights:
• Practical Application: Explaining Diagnostic Test Results: Nurses are often the primary point of contact for patients receiving results from diagnostic tests like the mid-pregnancy ultrasound, amniocentesis, and MSAFP screening. It is imperative to provide accurate, empathetic explanations of the findings, implications, and subsequent management plans. For example, if an MSAFP is elevated, explain it is a screening test and does not mean the fetus definitely has an NTD, but warrants further diagnostic testing such as a targeted ultrasound.
• Practical Application: Counseling on Viability: While acknowledging fetal viability around 24 weeks is important, nurses must also provide realistic counseling regarding the prognosis for survival and the potential for long-term morbidity in extremely preterm infants. Emphasize that while medical advancements improve outcomes, the highest likelihood of healthy survival is achieved with advancing gestational age.
• Practical Application: Promoting Prenatal Care Adherence: Regularly scheduled second-trimester prenatal visits are crucial for monitoring maternal and fetal well-being. Nurses reinforce the importance of these visits, which include fundal height measurements, fetal heart tone auscultation, and preparation for the mid-pregnancy ultrasound, ensuring comprehensive care.
Third Trimester: Weeks 28-40+
The third trimester represents the culminating phase of intrauterine development, characterized by intensive fetal growth, substantial weight accrual, and the final functional maturation of all organ systems, meticulously preparing the fetus for the physiological demands of extrauterine existence.
1 Advanced Fetal Maturation
• Weight Gain and Fat Accumulation:
➤ The fetus experiences a pronounced growth spurt during the third trimester, gaining approximately half of its total birth weight during the last 8-10 weeks of gestation.
➤ There is a significant and progressive deposition of subcutaneous adipose tissue (fat), which serves as a crucial insulating layer for thermoregulation post-birth and provides vital energy reserves for neonatal adaptation.
➤ By week 26, the approximate fetal weight ranges from 600-800 grams. By the completion of gestation at term (week 40), the average fetal weight is typically within the range of 2.5-4 kg.
• Respiratory System Maturation:
➤ The pulmonary system continues its intricate maturation, involving the development of more complex alveolar sacs and a sustained increase in the production of surfactant.
➤ Surfactant production reaches levels considered sufficient to support independent and effective extrauterine lung function in the majority of fetuses around week 34-36. This critical protein-lipid complex lowers surface tension within the alveoli, preventing their collapse upon exhalation and ensuring adequate gas exchange.
➤ Fetal breathing movements (FBMs) become more regular and vigorous, playing a crucial role in the development and conditioning of the pulmonary musculature and fluid clearance from the airways.
• Nervous System Development:
➤ This trimester is marked by exponential brain growth and development, including continued gyration and sulcation, which increase the cortical surface area.
➤ The process of myelination of nerve fibers progresses rapidly, particularly in the central nervous system, enhancing the speed and efficiency of neural impulse transmission, thereby improving coordination and reflex integration.
➤ The central nervous system assumes greater control over vital physiological functions, including thermoregulation and respiratory drive.
➤ Coordinated reflexes, such as the sucking reflex, become more refined around weeks 32-34, essential for successful oral feeding after birth.
• Immunological Development:
➤ Passive Immunity: A critical protective mechanism is established through the active transfer of maternal immunoglobulin G (IgG) antibodies across the placenta to the fetus. This transfer predominantly occurs during the third trimester, commencing significantly around week 33. These maternal antibodies confer passive immunity to the neonate, providing temporary protection against common bacterial and viral infections to which the mother has developed immunity, safeguarding the infant during the initial vulnerable months of extrauterine life.
• Gastrointestinal System:
➤ Fetal digestive enzymes are present and functional.
➤ Meconium, the first intestinal discharge of the neonate, accumulates within the fetal intestines. This sterile, greenish-black, viscous substance is composed of shed epithelial cells, lanugo, intestinal secretions, and bile pigments.
• Renal System:
➤ The fetal kidneys are fully functional and play a substantial role in maintaining the appropriate volume of amniotic fluid through continuous urine production and excretion.
• Sensory Organs:
➤ The pupillary light reflex is established.
➤ The auditory system is fully developed, enabling the fetus to consistently react to external auditory stimuli, including maternal voice and environmental sounds.
Nursing Insights:
• Practical Application: Fetal Movement Monitoring (Kick Counts): Nurses must diligently educate expectant mothers on the consistent monitoring of fetal movements (often referred to as "kick counts") as a simple, non-invasive, and effective daily assessment of fetal well-being, particularly in the third trimester. A significant decrease or cessation of fetal movements necessitates immediate medical evaluation. Instructing the patient to choose a consistent time each day, lie on her side, and count distinct movements (e.g., report if fewer than 10 movements occur within 2 hours) is a standard protocol.
• Practical Application: Antenatal Corticosteroid Administration: When managing a patient at risk for preterm labor, nurses understand the critical importance of administering betamethasone (or dexamethasone). This corticosteroid medication, given intramuscularly to the mother, accelerates fetal lung maturity by stimulating surfactant production, significantly reducing the incidence and severity of respiratory distress syndrome in preterm neonates. Nurses monitor for potential side effects and ensure timely administration within the therapeutic window.
• Practical Application: Explaining Neonatal Immunity: Nurses should counsel parents about the concept of passive immunity acquired from the mother, explaining that it provides temporary protection. This knowledge helps parents understand why routine childhood immunizations are crucial even if the baby received maternal antibodies, as these antibodies gradually wane.
2 Preparation for Birth
• Fetal Position and Presentation:
➤ As the fetus rapidly grows and occupies an increasing proportion of the intrauterine space, it typically assumes a characteristic position within the uterus.
➤ The most common and physiologically advantageous fetal position for vaginal birth is vertex (cephalic) presentation, where the fetal head is positioned inferiorly, towards the maternal pelvis.
➤ Lightening: This maternal sensation, often described as the fetus "dropping," occurs when the fetal head descends and engages into the maternal pelvis. This typically transpires a few weeks prior to term in primigravida individuals and often closer to the actual onset of labor in multigravida individuals. Physiologically, lightening can alleviate maternal dyspnea by reducing pressure on the diaphragm, but it concurrently increases pressure on the bladder, leading to more frequent urination.
• Amniotic Fluid Volume:
➤ The volume of amniotic fluid generally peaks around week 32-36 of gestation, subsequently undergoing a gradual physiological decrease as term approaches.
➤ Deviations from normal amniotic fluid volume, specifically oligohydramnios (abnormally low amniotic fluid, often associated with uteroplacental insufficiency or fetal renal anomalies) or polyhydramnios (excessive amniotic fluid, potentially indicative of fetal gastrointestinal anomalies or gestational diabetes), can serve as significant indicators of underlying fetal or maternal complications, necessitating further diagnostic evaluation and management.
• Placental Maturation and Aging:
➤ While the placenta continues to grow throughout gestation, it exhibits physiological signs of aging as term approaches and especially beyond term. These changes include calcifications and decreased vascularity, which can lead to diminished efficiency in nutrient and gas exchange. This phenomenon is termed placental insufficiency, and it can compromise fetal well-being in post-term pregnancies.
• Maternal Assessment for Fetal Well-being:
➤ Leopold's Maneuvers: This systematic series of four abdominal palpation techniques is a fundamental nursing skill performed typically after 28 weeks of gestation. Leopold's maneuvers enable the clinician to accurately determine fetal presentation (e.g., vertex, breech), fetal position (e.g., left occiput anterior), the fetal lie (longitudinal, transverse, oblique), and provide an estimation of fetal weight. This assessment is critical for planning labor management.
➤ Non-Stress Test (NST): The NST is a non-invasive antepartum fetal surveillance test performed to assess fetal well-being. It involves monitoring the fetal heart rate (FHR) response to spontaneous fetal movements. A reactive NST, characterized by two or more FHR accelerations (defined as an increase of at least 15 beats per minute above baseline, lasting at least 15 seconds) within a 20-minute period, indicates adequate fetal oxygenation and an intact autonomic nervous system.
➤ Biophysical Profile (BPP): The BPP is a comprehensive, non-invasive assessment tool that combines the Non-Stress Test with real-time ultrasonography. It evaluates five parameters: fetal breathing movements, gross body movements, fetal tone, amniotic fluid volume, and the reactive NST. Each parameter is scored 0 or 2, with a maximum score of 10. A score of 8-10 is generally considered reassuring for fetal well-being.
• Signs of Labor:
➤ Nurses are instrumental in educating patients on the crucial differentiation between true labor (characterized by regular, progressively stronger, and longer uterine contractions leading to cervical effacement and dilation) and false labor (Braxton Hicks contractions, which are irregular, do not increase in intensity, and resolve with rest or position change).
➤ Other important pre-labor and early labor signs include progressive cervical ripening, passage of the "bloody show" (mucus plug mixed with blood), and rupture of membranes (spontaneous amniotomy).
Nursing Insights:
• Practical Application: Mastering Leopold's Maneuvers: Nurses must develop proficiency in performing Leopold's maneuvers, as this skill directly impacts labor and delivery care. For instance, identifying a breech presentation necessitates preparing for potential external cephalic version or planned cesarean delivery, whereas a vertex presentation guides the expectation of a vaginal birth. Practicing this palpation technique on multiple patients enhances accuracy.
• Practical Application: Preterm Labor Recognition and Response: Nurses provide explicit instructions to patients on recognizing the subtle and overt signs and symptoms of preterm labor (e.g., regular uterine contractions, pelvic pressure, low backache, increased vaginal discharge, vaginal spotting) and emphasizing the critical importance of prompt medical evaluation should these symptoms arise. Early recognition and intervention can significantly impact neonatal outcomes.
• Practical Application: Explaining Antenatal Surveillance: When fetal surveillance tests such as NSTs and BPPs are ordered, nurses are responsible for thoroughly explaining the purpose, procedure, and interpretation of these tests to expectant parents. For example, explain that a non-reactive NST does not necessarily mean distress but requires further evaluation, often with a BPP or contraction stress test, to gain more comprehensive insight into fetal status. This transparency alleviates anxiety and promotes informed decision-making.
Summary
The remarkable journey of fetal development, commencing from a singular zygote and culminating in a highly complex human neonate prepared for independent extrauterine existence, is a testament to extraordinarily intricate biological programming. The first trimester, encompassing the pivotal events of fertilization, implantation, and the critical embryonic period (weeks 3-8), is characterized by profoundly rapid cellular division and the foundational establishment of all major organ systems. This embryonic phase is unequivocally the most susceptible window for teratogenic insults, necessitating rigorous patient education on avoidance. The second trimester (weeks 14-27) transitions into a period of substantial fetal growth, intricate refinement of organ systems, and the emotionally significant maternal perception of fetal movements. Finally, the third trimester (weeks 28-40+) is defined by exponential fetal weight gain, the critical final maturation of the pulmonary and neurological systems, and a comprehensive physiological preparation for the demands of birth and subsequent extrauterine life. Throughout these gestational trimesters, a series of critical physiological milestones—including the development of a beating heart, functional kidneys, and adequate surfactant production—are essential for the eventual success of independent survival. Nursing care across the entire gestational continuum necessitates a comprehensive understanding of these developmental stages, emphasizing proactive health promotion, meticulous risk reduction strategies, precise patient education, and the skillful application and interpretation of various diagnostic assessments. This holistic approach ensures optimal maternal and fetal outcomes, embodying competent and compassionate maternal-newborn nursing practice.
