
Fluids and Electrolytes & Acid-Base Balance
Lessons
- Objectives
- Introduction
- Fluid Compartments
- Fluid Balance
- Electrolytes
- Movement Of Body Fluids And Electrolytes
- Practice Exercise 1
- Fluid Imbalances
- Electrolyte Imbalances
- Practice Exercise 2
- Acid Base Imbalances
- Respiratory Acid-base Imbalances
- Metabolic Acid-base Imbalances
- The Nursing Process For Fluid, Electrolyte, And Acid–base Balance
- Practice Exercise 3
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Determine what processes regulate fluid distribution, extracellular fluid volume (ECV), and body fluid osmolality.
- Explain processes that regulate electrolyte balance.
- Explain processes that regulate acid-base balance.
- Recall common fluid, electrolyte, and acid-base imbalances.
- Identify risk factors for fluid, electrolyte, and acid-base imbalances
- Explain rationale and procedures for initiating and discontinuing an intravenous (IV) line.
Introduction
In good health, a delicate balance of fluids, electrolytes, acids, and bases maintains the body.
This balance, or homeostasis, depends on multiple physiological processes that regulate fluid intake and output, as well as the movement of water and the substances dissolved in it between body compartments.
Fluid Compartments
3.1 FLUID COMPARTMENTS
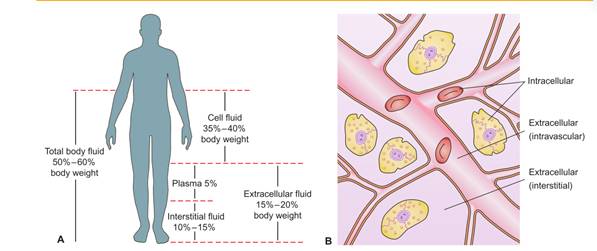
The body’s fluid is contained within three compartments: cells, blood vessels, and the tissue space (space between the cells and blood vessels).
There are two types of body fluid:
- intracellular fluid (ICF)- found within the cells of the body. It constitutes approximately two thirds of the total body fluid in adults.
- extracellular fluid (ECF)- found outside the cells and accounts for about one third of total body fluid.
ECF is further subdivided into compartments. The two main compartments of ECF are:
- Intravascular-or plasma, accounts for approximately 20% of ECF and is found within the vascular system
- Interstitial- accounting for approximately 75% of ECF, surrounds the cells.
The other compartments of ECF include the lymph and transcellular fluids (cerebrospinal, pericardial, pancreatic, pleural, intraocular, biliary, peritoneal, and synovial fluids).
Water in the body functions primarily to:
- Provide a medium for transporting nutrients to cells and wastes from cells
- Provide a medium for transporting substances such as hormones, enzymes, blood platelets, and red and white blood cells throughout the body
- Facilitate cellular metabolism and proper cellular chemical functioning
- Act as a solvent for electrolytes and nonelectrolytes
- Help maintain normal body temperature
- Facilitate digestion and promote elimination
- Act as a tissue lubricant
Variations in Fluid content:
Variations in the fluid content from the normal 50% to 60% of the body’s weight can occur, depending on such factors as the person’s age, body fat, and gender.
Fat cells contain little water, whereas lean tissue is rich in water. Thus, the more obese a person is, the smaller the person’s percentage of total body water is when compared with body weight.
- Because women tend to have proportionally more body fat than men do, they also have less body fluid than men.
- Older adults lose muscle mass as a part of aging. The combined increase of fat and loss of muscle results in reduced total body water; after the age of 60, total body water is about 45% of a person’s body weight.
- Infants have considerably more total body fluid and ECF than adults. Because ECF is more easily lost from the body than ICF, infants are more prone to fluid volume deficits.
Fluid Balance
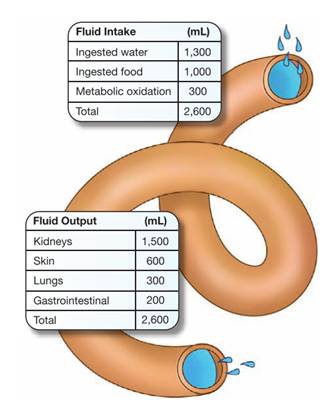
The desirable amount of fluid intake and loss in adults ranges from 1,500 to 3,500 mL each 24 hours.
A person’s intake should normally be approximately balanced by output or fluid loss.
In healthy adults, the output of urine normally approximates the ingestion of liquids, and the water from food and oxidation is balanced by the water loss through the feces, the skin, and the respiratory process.
Fluid sources:
The human body obtains water from several sources, including ingested liquids, food, and as a by-product of metabolism.
Fluid losses:
Fluid is lost from the body through sensible and insensible losses.
- Sensible losses can be measured and include fluid lost during urination, defecation, and wounds.
- Insensible losses can’t be measured or seen and include fluid lost from evaporation through the skin and as water vapor from the lungs during respiration.
Homeostatic mechanisms:
Almost every organ and system in the body helps in some way to maintain fluid homeostasis.
- Kidneys:
- Regulate extracellular fluid (ECF) volume and osmolality by selective retention and excretion of body fluids
- Regulate electrolyte levels in the ECF by selective retention of needed substances and excretion of unneeded substances
- Regulate pH of ECF by excretion or retention of hydrogen ions
- Excrete metabolic wastes (primarily acids) and toxic substances
- Heart and blood vessels:
- Circulate blood through the kidneys under sufficient pressure for urine to form (pumping action of the heart)
- React to hypovolemia by stimulating fluid retention (stretch receptors in the atria and blood vessels).
- Lungs:
- Eliminate about 13,000 mEq of hydrogen ions (H+) daily.
- Act promptly to correct metabolic acid–base disturbances; regulate H+ concentration (pH) by controlling the level of carbon dioxide (CO2) in the extracellular fluid as follows:
- Metabolic alkalosis causes compensatory hypoventilation, resulting in CO2 retention.
- Metabolic acidosis causes compensatory hyperventilation, resulting in CO2 excretion.
- Remove approximately 300 mL of water daily through exhalation (insensible water loss) in the normal adult.
- Adrenal glands:
- Regulate blood volume and sodium and potassium balance by secreting aldosterone:
- The primary regulator of aldosterone appears to be angiotensin II, which is produced by the renin–angiotensin system. A decrease in blood volume triggers this system and increases aldosterone secretion, which causes sodium retention (and thus water retention) and potassium loss.
- Decreased secretion of aldosterone causes sodium and water loss and potassium retention.
- Cortisol, another adrenocortical hormone, has only a fraction of the potency of aldosterone.
- However, secretion of cortisol in large quantities can produce sodium and water retention and potassium deficit.
- Pituitary gland:
- Stores and releases the antidiuretic hormone (ADH):
- Maintains osmotic pressure of the cells by controlling renal water retention or excretion
- When osmotic pressure of the ECF is greater than that of the cells (as in hypernatremia— excess sodium—or hyperglycemia), ADH secretion is increased, causing renal retention of water.
- When osmotic pressure of the ECF is less than that of the cells (as in hyponatremia), ADH secretion is decreased, causing renal excretion of water.
- Controls blood volume (less influential than aldosterone)
- When blood volume is decreased, an increased secretion of ADH results in water conservation.
- When blood volume is increased, a decreased secretion of ADH results in water loss.
- Nervous system
- Inhibits and stimulates mechanisms influencing fluid balance; acts chiefly to regulate sodium and water intake and excretion.
- Regulates oral intake by sensing intracellular dehydration, which triggers thirst (thirst center located in hypothalamus).
- Parathyroid gland
- Regulate calcium (Ca2+) and phosphate (HPO4 2-) balance by means of parathyroid hormone (PTH);
- PTH influences bone reabsorption, calcium absorption from the intestines, and calcium reabsorption from the renal tubules.
- Increased secretion of PTH causes: a. Elevated serum calcium concentration b. Lowered serum phosphate concentration
- Conversely, decreased secretion of PTH causes: a. Lowered serum calcium concentration b. Elevated serum phosphate concentration.
Electrolytes
Electrolytes are substances that are capable of breaking into particles called ions.
An ion is an atom or molecule carrying an electrical charge.
- Some ions develop a positive charge and are called cations. The major cations in body fluid are sodium, potassium, calcium, hydrogen, and magnesium ions.
- Other ions develop a negative charge and are called anions. The major anions in body fluid are chloride, bicarbonate, and phosphate.
Fluids in various compartments of the body differ in their constituents.
- Major electrolytes in the ECF include sodium, chloride, calcium, and bicarbonate.
- Major electrolytes in the ICF include potassium, phosphorus, and magnesium.
Major electrolytes:
|
Electrolyte |
Functions |
Sources & Losses |
Regulation |
|
Sodium (Na+): 135–145 mEq/L |
Transmission of nerve impulses
|
Derived easily from dietary sources, such as salt added to processed foods, sodium preservatives added to processed foods
Lost from gastrointestinal tract, kidneys, and skin |
Transported out of the cell by the sodium potassium pump Sodium concentrations affected by salt, as well as water, intake Regulated by renin-angiotensin-aldosterone system Elimination and reabsorption regulated by the kidneys |
|
Potassium (K+): 3.5–5.0 mEq/L |
|
Adequate quantities usually in a well-balanced diet Leading food sources: fruits and vegetables, dried peas and beans, whole grains, milk, meats Lost via kidneys, stool, sweat Gastrointestinal (GI) secretions contain potassium in large quantities, so can be lost through vomitus |
Regulated by aldosterone Eliminated by the kidneys (no effective method of conserving potassium) Additional regulation via transcellular shift between the ICF and ECF compartments |
|
Calcium (Ca2+): Total serum calcium level: 8.6–10.2 mg/dL Ionized serum calcium level: 4.5–5.1 mg/dL
|
|
Absorbed from foods in the presence of normal gastric acidity and vitamin D
Sources include milk, milk products, cheese, and dried beans; fortified orange juice; green leafy vegetables, small fish with bones, and dried peas and beans
Lost via feces and urine
|
Primarily excreted by gastrointestinal tract; lesser extent by kidneys
Regulated by parathyroid hormone and calcitonin
High serum phosphate results in decreased serum calcium level; low serum phosphate leads to increased serum calcium |
|
Magnesium (Mg2+): 1.3–2.3 mEq/L |
|
Enters the body via gastrointestinal tract Magnesium found in green leafy vegetables, nuts, seafood, whole grains, dried peas and beans; cocoa
Lost via urine with use of loop diuretics |
Eliminated by kidneys Regulated by parathyroid hormone |
|
Chloride (Cl-): 97–107 mEq/L |
|
Enters body via gastrointestinal tract Almost all chloride in diet comes from salt Found in foods high in sodium, processed foods |
Normally paired with sodium; excreted and conserved with sodium by the kidneys Regulated by aldosterone alongside sodium Low potassium level leads to low chloride level |
|
Bicarbonate (HCO₃⁻ ) |
|
Losses possible via diarrhea, diuretics, and early renal insufficiency; excess possible via over ingestion of acid neutralizers, such as sodium bicarbonate |
Bicarbonate levels regulated primarily by the kidneys Bicarbonate readily available as a result of carbon dioxide formation during metabolism |
|
Phosphate (PO4 -): |
|
Enters body via gastrointestinal tract Sources include all animal products (meat, poultry, eggs, milk, bread, ready-to-eat cereal) Absorption is diminished by concurrent ingestion of calcium, magnesium, and aluminum |
Eliminated by kidneys Regulation by parathyroid hormone and by activated vitamin D Phosphate and calcium are inversely proportional; an increase in one results in a decrease in the other |
Movement Of Body Fluids And Electrolytes
Key terms used in explaining the movement of molecules in body fluids are:
• Solute: Substance dissolved in a solution
• Solvent: Liquid that contains a substance in solution
• Permeability: Capability of a substance, molecule, or ion to diffuse through a membrane (covering of tissue over a surface, organ, or separating spaces)
• Semipermeable: Selectively permeable (All membranes in the body allow some solutes to pass through the membrane without restriction but will prevent the passage of other solutes.)
Permeability allows the cell to acquire the nutrients it needs from ECF to carry on metabolism and to eliminate metabolic waste products.
The concentration of solutes in body fluids is usually expressed as the osmolality.
Solutions may be termed isotonic, hypertonic, or hypotonic.
- An isotonic solution has the same osmolality as ECF Eg. Normal saline, 0.9% sodium chloride.
- Hypertonic solutions, such as 3% sodium chloride, have a higher osmolality than ECF.
- Hypotonic solutions, such as 0.45% sodium chloride, have a lower osmolality than ECF.
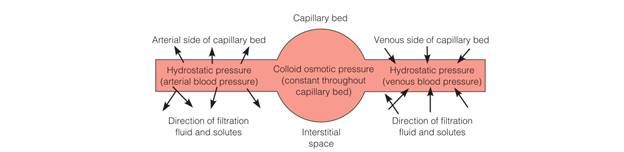
Osmotic pressure is the power of a solution to pull water across a semipermeable membrane
Plasma proteins also exert osmotic pressure called colloid osmotic pressure or oncotic pressure, holding water in plasma, and when necessary pulling water from the interstitial space into the vascular compartment.
Hydrostatic pressure is the pressure exerted by a fluid within a closed system on the walls of the container in which it is contained.
- Diffusion occurs when two solutes of different concentrations are separated by a semipermeable membrane.
- Osmosis: specific kind of diffusion in which water moves across cell membranes, from the less concentrated solution.
- Filtration is a process whereby fluid and solutes move together across a membrane from an area of higher pressure to an area of lower pressure.
- Active transport is the movement of solutes across cell membranes from a less concentrated solution to a more concentrated one.
Fluid Imbalances
Fluid imbalances are of two basic types: isotonic and osmolar.
Isotonic imbalances occur when water and electrolytes are lost or gained in equal proportions, so that the osmolality of body fluids remains constant.
Osmolar imbalances involve the loss or gain of only water, so that the osmolality of the serum is altered.
Thus, four categories of fluid imbalances may occur:
-
- an isotonic loss of water and electrolytes- fluid volume deficit
- an isotonic gain of water and electrolytes- fluid volume excess
- a hyperosmolar loss of only water- hyperosmolar imbalance/ dehydration
- a hypo-osmolar gain of only water- overhydration (hypo-osmolar imbalance)
1. FLUID VOLUME DEFICIT:
Isotonic fluid volume deficit (FVD) occurs when the body loses both water and electrolytes from the ECF in similar proportions. Thus, the decreased volume of fluid remains isotonic.
In FVD, fluid is initially lost from the intravascular compartment, so it often is called hypovolemia. FVD generally occurs as a result of
- abnormal losses through the skin, gastrointestinal tract, or kidney
- decreased intake of fluid due to anorexia, nausea, inability to access fluids, impaired swallowing, confusion, depression
- bleeding
- movement of fluid into a third space
Clinical manifestations:
- Complaints of weakness and thirst
- Weight loss: • 2% loss = mild FVD • 5% loss = moderate • 8% loss = severe
- Decreased tissue turgor
- Dry mucous membranes, sunken eyeballs, decreased tearing
- Subnormal temperature
- Weak pulse; tachycardia Decreased blood pressure
- Postural (orthostatic) hypotension (significant drop in BP when moving from lying to sitting or standing position)
- Decreased capillary refill
- Decreased central venous pressure
- Decreased urine volume (<30 mL/hr)
- Increased specific gravity of urine (>1.030)
- Increased hematocrit
- Increased blood urea nitrogen (BUN)
Nursing interventions:
- Assess for clinical manifestations of FVD.
- Monitor weight and vital signs, including temperature.
- Assess tissue turgor.
- Monitor fluid intake and output.
- Monitor laboratory findings.
- Administer oral and IV fluids as indicated.
- Provide frequent mouth care.
- Implement measures to prevent skin breakdown.
- Provide for safety (e.g., provide assistance for a client rising from bed or chair).
Third space syndrome:
In third space syndrome, fluid shifts from the vascular space into an area where it is not readily accessible as extracellular fluid.
Third spacing has two distinct phases: loss and reabsorption.
The client with third space syndrome during the loss phase has an isotonic fluid deficit. During the reabsorption phase, tissues begin to heal and fluid moves back into the intravascular space
Because fluid shifts from the vascular compartment (loss phase) and then back into the vascular compartment after time (reabsorption phase), assessment for manifestations of fluid volume deficit and excess is vital.
2. FLUID VOLUME EXCESS
Fluid volume excess (FVE) occurs when the body retains both water and sodium in similar proportions to normal ECF.
This is commonly referred to as hypervolemia (increased blood volume).
Specific causes of FVE include:
- excessive intake of sodium chloride
- administering sodium-containing infusions too rapidly, particularly to clients with impaired regulatory mechanisms
- disease processes that alter regulatory mechanisms, such as heart failure, renal failure, cirrhosis of the liver, and Cushing’s syndrome.
Clinical manifestations:
- Weight gain: • 2% gain = mild FVE • 5% gain = moderate • 8% gain = severe
- Fluid intake greater than output
- Full, bounding pulse; tachycardia Increased blood pressure and central venous pressure
- Distended neck veins
- Moist crackles (rales) in lungs; dyspnea, shortness of breath
- Edema
- Mental confusion
Nursing interventions:
- Assess for clinical manifestations of FVE.
- Monitor weight and vital signs.
- Assess for edema.
- Assess breath sounds.
- Monitor fluid intake and output.
- Monitor laboratory findings.
- Place in Fowler’s position.
- Administer diuretics as ordered.
- Restrict fluid intake as indicated.
- Restrict dietary sodium as ordered.
- Implement measures to prevent skin breakdown.
3. DEHYDRATION
Dehydration, or a hyperosmolar fluid imbalance, occurs when water is lost from the body, leaving the client with excess sodium.
Water is drawn into the vascular compartment from the interstitial space and cells, resulting in cellular dehydration.
4. OVERHYDRATION
Overhydration, or a hypo-osmolar fluid imbalance, occurs when water is gained in excess of electrolytes, resulting in low serum osmolality and low serum sodium levels.
Electrolyte Imbalances
a. Hyponatremia:
Is a sodium deficit, or serum sodium level of less than 135 mEq/L.
Risk factors:
Loss of Sodium
- Gastrointestinal fluid loss
- Sweating
- Use of diuretics
Gain of Water
- Hypotonic tube feedings
- Excessive drinking of water
- Excess IV D5W (dextrose in water) administration
Syndrome of Inappropriate ADH (SIADH)
- Head injury
- AIDS
- Malignant tumors
Clinical manifestations
- Lethargy, confusion, apprehension
- Muscle twitching
- Abdominal cramps
- Anorexia, nausea, vomiting
- Headache
- Seizures, coma
- Laboratory findings: Serum sodium < 135 mEq/L Serum osmolality < 280 mOsm/kg
Nursing interventions
- Assess clinical manifestations.
- Monitor fluid intake and output.
- Monitor laboratory data (e.g., serum sodium).
- Assess client closely if administering hypertonic saline solutions.
- Encourage food and fluid high in sodium if permitted (e.g., table salt, bacon, ham, processed cheese).
- Limit water intake as indicated.
b. Hypernatremia
Risk factors
Loss of Water
- Insensible water loss (hyperventilation or fever)
- Diarrhea
- Water deprivation
Gain of Sodium
- Parenteral administration of saline solutions
- Hypertonic tube feedings without adequate water
- Excessive use of table salt (1 tsp contains 2,300 mg of sodium)
- Conditions such as: • Diabetes insipidus • Heat stroke
Clinical manifestations
- Thirst
- Dry, sticky mucous membranes
- Tongue red, dry, swollen Weakness
- Severe hypernatremia:
- Fatigue, restlessness • Decreasing level of consciousness • Disorientation • Convulsions
- Laboratory findings: Serum sodium > 145 mEq/L Serum osmolality > 300 mOsm/kg
Nursing interventions:
- Monitor fluid intake and output.
- Monitor behavior changes (e.g., restlessness, disorientation).
- Monitor laboratory findings (e.g., serum sodium).
- Encourage fluids as ordered.
- Monitor diet as ordered (e.g., restrict intake of salt and foods high in sodium).
c. Hypokalemia
Risk factors:
- Vomiting and gastric suction
- Diarrhea
- Heavy perspiration
- Use of potassium-wasting drugs (e.g., diuretics)
- Poor intake of potassium (as with debilitated clients, alcoholics, anorexia nervosa)
- Hyperaldosteronism
Clinical manifestations:
- Muscle weakness, leg cramps
- Fatigue, lethargy
- Anorexia, nausea, vomiting
- Decreased bowel sounds, decreased bowel motility
- Cardiac dysrhythmias
- Depressed deep-tendon reflexes
- Weak, irregular pulses
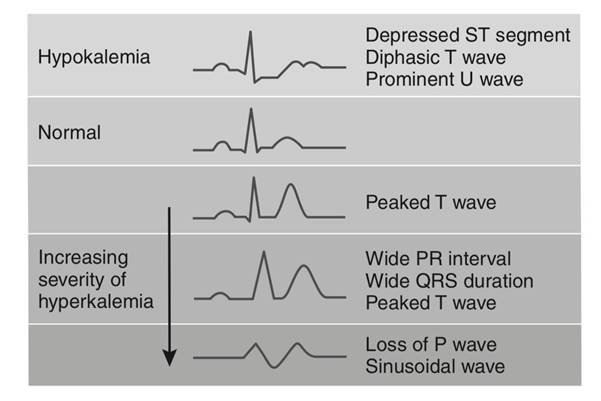
- Laboratory findings: Serum potassium < 3.5 mEq/L Arterial blood gases (ABGs) may show alkalosis T-wave flattening and ST-segment depression on ECG.
Nursing interventions:
- Monitor heart rate and rhythm.
- Monitor clients receiving digitalis (e.g., digoxin) closely, because hypokalemia increases risk of digitalis toxicity.
- Administer oral potassium as ordered with food or fluid to prevent gastric irritation.
- Administer IV potassium solutions at a rate no faster than 10–20 mEq/h; never administer undiluted potassium intravenously.
- For clients receiving IV potassium, monitor for pain and inflammation at the injection site.
- Teach client about potassium-rich foods.
- Teach clients how to prevent excessive loss of potassium (e.g., through abuse of diuretics and laxatives).
d. Hyperkalemia
Risk factors:
Decreased Potassium Excretion
- Renal failure
- Hypoaldosteronism
- Potassium-conserving diuretics
High Potassium Intake
- Excessive use of K+ containing salt substitutes
- Excessive or rapid IV infusion of potassium
- Potassium shift out of the tissue cells into the plasma (e.g., infections, burns, acidosis)
Clinical manifestations:
- Gastrointestinal hyperactivity, diarrhea
- Irritability, apathy, confusion
- Cardiac dysrhythmias or arrest
- Muscle weakness, areflexia (absence of reflexes)
- Decreased heart rate Irregular pulse
- Paresthesias and numbness in extremities
- Laboratory findings: Serum potassium > 5.0 mEq/L Peaked T wave, widened QRS on ECG
Nursing interventions:
- Closely monitor cardiac status and ECG.
- Administer diuretics and other medications such as glucose and insulin as ordered.
- Hold potassium supplements and K+ conserving diuretics.
- Monitor serum K+ levels carefully; a rapid drop may occur as potassium shifts into the cells.
- Teach clients to avoid foods high in potassium and salt substitutes.
e. Hypocalcemia:
Risk factors:
Surgical Removal of the Parathyroid Glands
Conditions such as:
- Hypoparathyroidism
- Acute pancreatitis
- Hyperphosphatemia
- Thyroid carcinoma
Inadequate Vitamin D Intake
- Malabsorption
- Hypomagnesemia
- Alkalosis
- Sepsis
- Alcohol abuse
Clinical manifestations:
- Numbness, tingling of the extremities and around the mouth
- Muscle tremors, cramps; if severe can progress to tetany and convulsions
- Cardiac dysrhythmias; decreased cardiac output
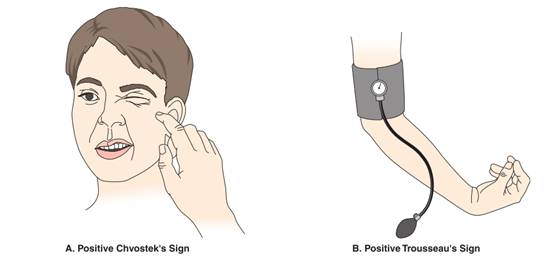
- Positive Trousseau’s and Chvostek’s signs
- Confusion, anxiety, possible psychoses
- Hyperactive deep-tendon reflexes
- Laboratory findings: Serum calcium < 8.5 mg/dL (total) or 4.5 mEq/L (ionized) Lengthened QT intervals Prolonged ST segments
Nursing interventions:
Closely monitor respiratory and cardiovascular status. Take precautions to protect a confused client. Administer oral or parenteral calcium supplements as ordered.
When administering intravenously, closely monitor cardiac status and ECG during infusion. Teach clients at high risk for osteoporosis about:
- Dietary sources rich in calcium.
- Recommendation for 1,000–1,500 mg of calcium per day.
- Calcium supplements.
- Regular exercise.
- Estrogen replacement therapy for postmenopausal women.
f. Hypercalcemia:
Risk factors:
Prolonged immobilization
Conditions such as:
- Hyperparathyroidism
- Malignancy of the bone
- Paget’s disease
Clinical manifestations:
- Lethargy, weakness
- Depressed deep-tendon reflexes
- Bone pain
- Anorexia, nausea, vomiting
- Constipation Polyuria, hypercalciuria
- Flank pain secondary to urinary calculi
- Dysrhythmias, possible heart block
- Laboratory findings: Serum calcium > 10.5 mg/dL (total) or 5.5 mEq/L (ionized)
- ECG: Shortened QT intervals, Shortened ST segments
Nursing interventions:
- Increase client movement and exercise.
- Encourage oral fluids as permitted to maintain a dilute urine.
- Teach clients to limit intake of food and fluid high in calcium.
- Encourage ingestion of fiber to prevent constipation.
- Protect a confused client; monitor for pathologic fractures in clients with long-term hypercalcemia.
- Encourage intake of acid–ash fluids (e.g., prune or cranberry juice) to counteract deposits of calcium salts in the urine.
g. Hypomagnesemia:
Risk factors:
- Excessive loss from the gastrointestinal tract (e.g., from nasogastric suction, diarrhea, fistula drainage)
- Long-term use of certain drugs (e.g., diuretics, aminoglycoside antibiotics)
- Conditions such as:
- Chronic alcoholism
- Pancreatitis
- Burns
Clinical manifestations:
- Neuromuscular irritability with tremors
- Increased reflexes, tremors, convulsions
- Positive Chvostek’s and Trousseau’s signs
- Tachycardia, elevated blood pressure, dysrhythmias
- Disorientation and confusion
- Vertigo
- Anorexia, dysphagia
- Respiratory difficulties
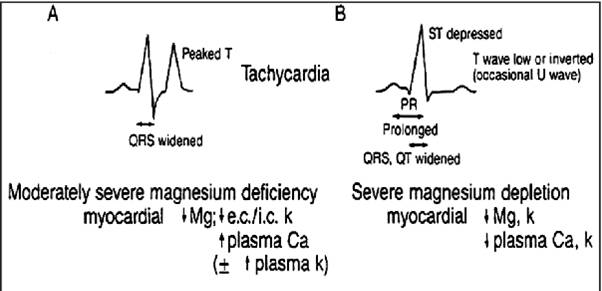
Laboratory findings: Serum magnesium < 1.5 mEq/L
ECG: Prolonged PR intervals, widened QRS complexes, prolonged QT intervals, broad flattened T waves, prominent U waves
Nursing interventions
Assess clients receiving digitalis for digitalis toxicity.
Hypomagnesemia increases the risk of toxicity.
Take protective measures when there is a possibility of seizures:
- Assess the client’s ability to swallow water prior to initiating oral feeding.
- Initiate safety measures to prevent injury during seizure activity.
- Carefully administer magnesium salts as ordered
Encourage clients to eat magnesium-rich foods if permitted (e.g., whole grains, meat, seafood, and green leafy vegetables).
Refer clients to alcohol treatment programs as indicated.
h. Hypermagnesemia:
Risk factors:
Abnormal retention of magnesium, as in:
- Renal failure
- Adrenal insufficiency
- Treatment with magnesium salts
Clinical manifestations:
- Peripheral vasodilation, flushing
- Nausea, vomiting
- Muscle weakness, paralysis
- Hypotension, bradycardia
- Depressed deep-tendon reflexes
- Lethargy, drowsiness
- Respiratory depression, coma
- Respiratory and cardiac arrest if hypermagnesemia is severe
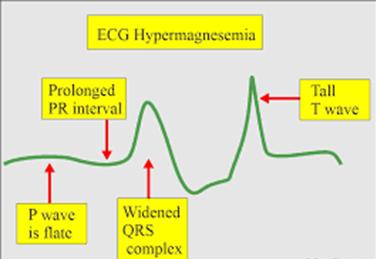
- Laboratory findings: Serum magnesium > 2.5 mEq/L Electrocardiogram showing prolonged QT interval, prolonged PR interval, widened QRS complexes, tall T waves
Nursing interventions:
- Monitor vital signs and level of consciousness when clients are at risk. If patellar reflexes are absent, notify the primary care provider.
- Advise clients who have renal disease to contact their primary care provider before taking over-the-counter drugs.
Acid Base Imbalances
Hydrogen ions: Vital to life because hydrogen ions determine the pH of the body, which must be maintained in a narrow range between 7.35 and 7.45.
Acids: Produced as end products of metabolism and contain hydrogen ions.
Bases: Are considered hydrogen ion acceptors; they accept hydrogen+ ions from acids to neutralize or decrease the strength of a base or to form a weaker acid. Normal serum levels of bicarbonate (HCO₃⁻ ) are 21 to 28 mEq/L (21 to 28 mmol/L).
Regulatory Systems for Hydrogen ion concentration in the blood
Include:
- Buffers
- Lungs
- Kidneys
- BUFFERS:
Are reactors that function only to keep the pH within the narrow limits of stability.
Buffers absorb or release hydrogen ions as needed.
|
Hemoglobin |
Plasma protein system |
Carbonic acid–bicarbonate system |
Phosphate buffer system |
|
Maintains acid-base balance by a process called chloride shift. |
Functions along with the liver to vary the amount of hydrogen ions in the chemical structure of plasma proteins |
Carbonic acid concentration is controlled by the excretion of CO2 by the lungs; the rate and depth of respiration change in response to changes in the CO2 e. The kidneys control the bicarbonate concentration and selectively retain or excrete bicarbonate in response to bodily needs |
Acts like bicarbonate and neutralizes excess hydrogen ions. |
- LUNGS
They interact with the buffer system to maintain acid-base balance.
- During acidosis, the pH decreases and the respiratory rate and depth increase in an attempt to exhale acids. The carbonic acid created by the neutralizing action of bicarbonate can be carried to the lungs, where it is reduced to CO2 and water and is exhaled; thus, hydrogen ions are inactivated and exhaled.
- During alkalosis, the pH increases and the respiratory rate and depth decrease; CO2 is retained and carbonic acid increases to neutralize and decrease the strength of excess bicarbonate.
- KIDNEYS
- During acidosis, the pH decreases and excess hydrogen ions are secreted into the tubules and combine with buffers for excretion in the urine.
- During alkalosis, the pH increases and excess bicarbonate ions move into the tubules, combine with sodium, and are excreted in the urine.
Note: When the client experiences an acid-base imbalance, monitor the potassium level closely, because the potassium moves in or out of the cells in an attempt to maintain acid-base balance. The resulting hypokalemia or hyperkalemia predisposes the client to associated complications.
Acid base imbalances:
Respiratory Acid-base Imbalances
The respiratory function indicator is PaCO₂.
pH will be elevated with a decreased PaCO₂ (alkalosis) or the pH will be decreased with an elevated PaCO₂ (acidosis).
|
|
Respiratory acidosis: |
Respiratory alkalosis: |
|
Definition |
Caused by primary defects in the function of the lungs or changes in normal respiratory patterns |
A deficit of carbonic acid and a decrease in hydrogen ion concentration that results from the accumulation of base or from a loss of acid without a comparable loss of base in the body fluids |
|
Causes |
Asthma Bronchiectasis Bronchiectasis CNS Depressants-sedatives, opioids Pneumonia Emphysema COPD |
Conditions that cause overstimulation of the respiratory system: Hyperventilation Fever Overventilation by mechanical ventilators Severe anxiety |
|
Clinical manifestations |
Chronic:
|
Complaints of shortness of breath, chest tightness Light-headedness with circumoral paresthesias and numbness and tingling of the extremities Difficulty concentrating Tremulousness, blurred vision |
|
Laboratory findings |
Arterial blood pH < 7.35 PaCO₂ > 45 mmHg HCO₃⁻ normal or slightly elevated in acute; > 26 mEq/L in chronic |
Arterial blood pH > 7.45 PaCO₂ < 35 mmHg HCO₃⁻ normal |
|
Nursing interventions |
Frequently assess respiratory status and lung sounds. Monitor airway and ventilation; insert artificial airway and prepare for mechanical ventilation as necessary. Administer pulmonary therapy measures such as inhalation therapy, percussion and postural drainage, bronchodilators, and antibiotics as ordered. Monitor fluid intake and output, vital signs, and arterial blood gases. Administer narcotic antagonists as indicated. Maintain adequate hydration (2–3 L of fluid per day).
|
Monitor vital signs and ABGs. Assist client to breathe more slowly. Help client breathe in a paper bag or apply a rebreather mask (to inhale CO2). |
Metabolic Acid-base Imbalances
Metabolic function indicator is the bicarbonate ion (HCO₃⁻ ).
The pH will be elevated and HCO₃⁻ will be elevated (alkalosis), or the pH will be decreased and HCO₃⁻ will be decreased (acidosis).
|
|
Metabolic acidosis: |
Metabolic alkalosis: |
|
Definition: |
A total concentration of buffer base that is lower than normal, with a relative increase in the hydrogen ion concentration, resulting from loss of too much base and/or retention of too much acid. |
A deficit of carbonic acid and a decrease in hydrogen ion concentration that results from the accumulation of base or from a loss of acid without a comparable loss of base in the body fluids. |
|
Causes: |
Diabetes ketoacidosis Malnutrition Acetylsalicylic acid overdose Acute kidney injury Severe diarrhoea |
Diuretics Excessive vomiting Gastrointestinal suctioning Hyperaldosteronism Massive transfusion of whole blood |
|
Clinical manifestations: |
Kussmaul’s respirations (deep, rapid respirations) Lethargy, confusion Headache Weakness Nausea and vomiting |
Decreased respiratory rate and depth Dizziness Circumoral paresthesias, numbness and tingling of the extremities Hypertonic muscles, tetany |
|
Laboratory findings: |
Arterial blood pH < 7.35 Serum bicarbonate less than 22 mEq/L PaCO₂ < 38 mmHg with respiratory compensation |
Arterial blood pH > 7.45 Serum bicarbonate > 26 mEq/L PaCO₂ > 45 mmHg with respiratory compensation |
|
Nursing interventions |
Monitor ABG values, intake and output, and LOC. Administer IV sodium bicarbonate carefully if ordered. Treat underlying problem as ordered. |
Monitor intake and output closely. Monitor vital signs, especially respirations, and LOC. Administer ordered IV fluids carefully. Treat underlying problem. |
Compensation:
Compensation refers to the body processes that occur to counterbalance the acid-base disturbance. When full compensation has occurred, the pH is within normal limits.
The Nursing Process For Fluid, Electrolyte, And Acid–base Balance
ASSESSING:
The nursing assessment is directed toward the following:
- Identifying patients at high risk for fluid, electrolyte, and acid–base imbalances
- Determining that a specific imbalance is present and identifying the nature of the imbalance along with its severity, etiology, and defining characteristics or assessment findings
- Determining the plan of care, including the appropriate nursing diagnoses or collaborative problems, followed by the identification of specific outcomes, associated interventions, and the evaluation of the effectiveness of the plan of care
A comprehensive nursing history includes questions related to the patient’s fluid, electrolyte, and acid–base balance.
Physical assessment related to fluid, electrolyte, and acid–base balance includes assessment of the skin and mucous membranes, vital signs, and a neurological assessment, as well as identification of relative symptoms or conditions.
Fluid Intake and Output- measure all fluids entering and leaving the body.
The record of a patient’s daily weight may more accurately depict fluid balance status, due to possible numerous sources of inaccuracies in fluid intake and output measurement.
Laboratory studies:
- Complete blood count:
- Determines the total number of red blood cells and values for hemoglobin and hematocrit.
- Increased hematocrit values: found in severe fluid volume deficit and shock.
- Decreased hematocrit values: found with acute, massive blood loss.
- Urine pH and specific gravity:
- Lower than normal urinary pH can occur with metabolic acidosis, diabetic ketosis, and diarrhea.
- Higher than normal urinary pH can occur with respiratory alkalosis, potassium depletion, and chronic renal failure.
- Increased urine specific gravity can occur with dehydration, vomiting, diarrhea, and heart failure.
- Decreased urine specific gravity can occur with renal damage.
- Arterial blood gases (ABGs): are laboratory tests commonly used to determine the adequacy of oxygenation and ventilation, as well as in the assessment and treatment of acid–base imbalance.
Nursing insights: Measuring fluid intake and output
Instruct the patient and family regarding the need for a record of all fluids entering the body and all fluid output.
A sign posted in the patient’s room and a bedside form for recording intake and output are helpful reminders for both the patient and nurses.
Record intake and output totals for each 8-hour shift and total each 24 hours.
The patient’s Fluid intake includes the following:
- All fluids and foods that are liquid at room temperature (ice cream, gelatin dessert [Jell-O], etc.)
- Use the agency’s designation of specific volumes for common food containers (e.g., juice glass 90 mL; milk carton=240 mL).
- All parenteral fluids
- Other fluids taken into the body: subcutaneous fluids, gastrointestinal tube feedings and flushes; IV flushes
The patient’s Fluid output includes the following:
- Urine; vomitus; diarrhea; drainage from fistulas, wounds, and ulcers; and drainage from suctioning devices or other tubes.
- Urine or liquid feces in diapers or bed clothes, vomitus on clothing or bed linens, wound drainage saturating dressings, and so forth, need to be estimated.
- Heavy perspiration, noted on the output record, especially when the patient’s clothing or bed linens are soaked
- Hyperventilation (water vapor loss) also noted on the output record. Record the rate and depth of respirations
DIAGNOSING:
NANDA International includes the following diagnostic labels that relate to fluid and acid–base imbalances:
- Deficient Fluid Volume: Decreased intravascular, interstitial, and/ or intracellular fluid. This refers to dehydration, water loss alone without change in sodium.
- Excess Fluid Volume: Increased isotonic fluid retention.
- Risk for Imbalanced Fluid Volume: Vulnerable to a decrease, increase, or rapid shift from one to the other of intravascular, interstitial, and/or intracellular fluid, which may compromise health. This refers to body fluid loss, gain, or both.
- Risk for Deficient Fluid Volume: Vulnerable to experiencing decreased intravascular, interstitial, and/or intracellular fluid volumes, which may compromise health.
- Impaired Gas Exchange: Excess or deficit in oxygenation and/or carbon dioxide elimination at the alveolar-capillary membrane.
Fluid, electrolyte, and acid–base imbalances affect many other body areas and as a consequence may be the etiology of other nursing diagnoses, such as these:
- Impaired Oral Mucous Membrane related to fluid volume deficit
- Impaired Skin Integrity related to dehydration and/or edema
- Decreased Cardiac Output related to hypovolemia and/or cardiac dysrhythmias secondary to electrolyte imbalance (K+ or Mg2+)
- Ineffective Tissue Perfusion related to decreased cardiac output secondary to fluid volume deficit or edema
- Activity Intolerance related to hypervolemia
- Risk for Injury related to calcium shift out of bones into extracellular fluids
- Acute Confusion related to electrolyte imbalance.
PLANNING:
When planning care, a nurse identifies nursing interventions that will assist the client to achieve these broad goals:
- Maintain or restore normal fluid balance.
- Maintain or restore normal balance of electrolytes in the intracellular and extracellular compartments.
- Maintain or restore gas exchange and oxygenation.
- Prevent associated risks (tissue breakdown, decreased cardiac output, confusion, other neurologic signs).
IMPLEMENTING
Nurses can promote clients’ health by providing wellness teaching that will help them maintain fluid and electrolyte balance.
Enteral Fluid and Electrolyte Replacement
Fluids and electrolytes can be provided orally in the home or hospital if a client’s health permits, meaning that the client is not vomiting, has not experienced an excessive fluid loss, and has an intact gastrointestinal tract and gag and swallow reflexes.
Parenteral Fluid and Electrolyte Replacement
IV fluid therapy is essential when clients are unable to take sufficient food and fluids orally. It is an efficient and effective method of supplying fluids directly into the intravascular fluid compartment and replacing electrolyte losses.
Factors Influencing Flow Rates
- The position of the forearm. Sometimes a change in the position of the client’ s arm decreases flow. Slight pronation, supination, extension, or elevation of the forearm on a pillow can increase flow.
- The position and patency of the tubing. Tubing can be obstructed by the client’ s weight, a kink, or a clamp closed too tightly. The flow rate also diminishes when part of the tubing dangles below the puncture site.
- The height of the infusion bottle. Elevating the height of the infusion bottle a few inches can speed the flow by creating more pressure.
- Possible infiltration or fluid leakage. Swelling, a feeling of coldness, and tender ness at the venipuncture site may indicate infiltration.
- Relationship of the size of the angiocath to the vein. A catheter that is too large may impede the infusion flow.
Nursing insights: Signs and Symptoms of Common Local Complications of Infusion Therapy
INFILTRATION
- Coolness of skin around site • Skin blanching, tautness (i.e., client states it feels “tight”)
- Edema at, above, or below the insertion site • Leakage at insertion site
- Absence of or “pinkish” blood return Difference in size of opposite hand or arm
EXTRAVASATION
Same as infiltration and can also include:
- Burning, stinging pain
- Redness followed by blistering, tissue necrosis, and ulceration
PHLEBITIS
- Redness at the site
- Skin warm
- Swelling
- Palpable cord along the vein Increase in temperature
Summary
- A balance of fluids, electrolytes, acids, and bases in the body is necessary for good health.
- Body fluid is divided into two major compartments: intracellular fluid (ICF) inside the cells and extracellular fluid (ECF) outside the cells.
- ECF is subdivided into two compartments: intravascular (plasma) and interstitial. It constitutes about one third of total body fluid.
- The acid–base balance (pH range) of body fluids is maintained within a precise range of 7.35 to 7.45.
- Acid–base balance is regulated by buffers, which neutralize excess acids or bases; the lungs, which eliminate or retain carbon dioxide, a potential acid; and the kidneys, which excrete or conserve bicarbonate and hydrogen ions.
- Fluid imbalances include fluid volume deficit (FVD), also referred to as hypovolemia; fluid volume excess (FVE), also referred to as hypervolemia; dehydration, a deficit in water and an increase in serum sodium level; and overhydration, an excess of water and decrease in serum sodium level.
