
Drugs Used for Diuresis
Study Questions
Practice Questions 2
A nurse is providing information to a client who has a new prescription for hydrochlorothiazide (Hydrodiuril). Which of the following information should the nurse include?
Explanation
Hydrochlorothiazide is a thiazide diuretic that inhibits the sodium-chloride symporter in the distal convoluted tubule. It promotes the excretion of sodium, chloride, and water to treat hypertension and congestive heart failure. Common side effects include hypokalemia, hyperuricemia, and gastric irritation.
Rationale for correct answer
A. Thiazide diuretics can cause significant gastrointestinal distress and mucosal irritation. Administering the medication with food or milk minimizes gastric upset and improves patient adherence. This practice ensures gastric protection while the drug is absorbed in the digestive tract.
Rationale for incorrect answers
B. Administering diuretics at bedtime is contraindicated because it causes nocturia and disrupts sleep patterns. Patients should take the dose in the morning to ensure peak diuresis occurs during waking hours. This timing prevents sleep deprivation and reduces the risk of nighttime falls.
C. Hydrochlorothiazide is indicated to reduce extracellular fluid volume and treat peripheral edema. A client should expect a decrease in ankle swelling, not an increase, as the drug promotes fluid excretion. Increased edema would indicate a treatment failure or worsening of the underlying condition.
D. Restricting fluid intake in the morning is unnecessary and can lead to severe dehydration. Clients should maintain adequate hydration to support renal function while the medication works. Limiting fluids does not enhance the pharmacological effect of the thiazide diuretic.
Test-taking strategy
- Identify the drug category: Hydrochlorothiazide is a diuretic. The primary purpose of a diuretic is to remove fluid, which helps eliminate options that suggest fluid retention.
- Consider timing of administration: Any drug that increases urination should be scheduled to avoid interfering with the client's rest. This allows you to rule out bedtime administration.
- Apply general pharmacology principles: Many oral medications that cause GI irritation are best tolerated when taken with food. This makes option 1 the most plausible safety and comfort intervention.
- Evaluate therapeutic goals: The goal of treatment for edema is the reduction of swelling. Therefore, expecting "increased swelling" is a negative outcome and can be ruled out as correct "information to include" for a standard prescription.
Take home points
- Thiazide diuretics should be taken in the morning to prevent nocturia and ensure the safety of the client during diuresis.
- Gastric upset is a common side effect of hydrochlorothiazide, which can be mitigated by taking the dose with meals.
- Patients on thiazide therapy must monitor for signs of electrolyte imbalance, particularly hypokalemia and hyponatremia.
- Effective therapy should result in decreased weight and reduced peripheral edema, reflecting successful fluid volume reduction.
The client admitted for heart failure (HF) has been receiving hydrochlorothiazide (Microzide). Which of the following laboratory levels should the nurse carefully monitor? Select all that apply
Explanation
Hydrochlorothiazide is a thiazide diuretic that inhibits the Na+/Cl- symporter in the distal convoluted tubule. This interference promotes the excretion of electrolytes, potentially leading to hypokalemia, hyponatremia, and metabolic alkalosis. It can also cause hyperuricemia and hyperglycemia by affecting renal tubular secretion and insulin sensitivity.
Rationale for correct answers
C. Thiazides increase the delivery of sodium to the collecting duct, which enhances potassium secretion into the tubular lumen. This pharmacological action often results in significant hypokalemia, defined as levels < 3.5 mEq/L. Low potassium increases the risk of life-threatening cardiac dysrhythmias and dig-toxicity in heart failure patients.
D. By blocking the reabsorption of sodium in the distal tubule, the drug causes direct sodium loss. This can lead to clinical hyponatremia, especially in elderly patients or those with high water intake. Monitoring ensures the serum sodium stays within the physiological range of 135 to 145 mEq/L.
E. Hydrochlorothiazide competes with uric acid for the organic acid secretory pathway in the proximal tubule. This competition leads to decreased excretion and elevated serum levels, potentially precipitating a gouty attack. Monitoring is essential for patients with a history of hyperuricemia or joint pain.
Rationale for incorrect answers
A. Routine thiazide therapy does not typically alter the production or destruction of the platelet count. Thrombocytopenia is an extremely rare idiosyncratic reaction rather than a standard metabolic effect of the drug. Therefore, frequent monitoring of thrombocytes is not a primary requirement for this medication.
B. The WBC count is generally not affected by the administration of thiazide diuretics like hydrochlorothiazide. These medications lack significant bone marrow suppressive properties under normal therapeutic conditions. Nurses prioritize metabolic panels over hematological counts when assessing the direct impact of this diuretic.
Test-taking strategy
- Identify the drug class: Hydrochlorothiazide is a thiazide diuretic. Focus on the "hypo" and "hyper" metabolic effects associated with this class.
- Recall electrolyte impact: Thiazides waste most electrolytes (potassium, sodium, magnesium) but retain calcium. This allows you to select options 3 and 4 immediately as they represent primary wasting risks.
- Identify metabolic side effects: Use the mnemonic "Hyper-GLUC" (Glycemia, Lipidemia, Uricemia, Calcemia). This helps you remember that uric acid (option 5) will increase and must be monitored.
- Eliminate hematological distractors: Platelets and WBCs (options 1 and 2) are related to immune function and clotting. Since diuretics act on renal tubules and fluid balance, these choices are less relevant than laboratory values reflecting electrolyte and metabolic shifts.
Take home points
- Thiazide diuretics require regular monitoring of serum potassium and sodium to prevent severe electrolyte imbalances.
- Hyperuricemia is a common metabolic side effect that can trigger gout in susceptible individuals.
- Patients with heart failure are particularly vulnerable to hypokalemia-induced arrhythmias when taking hydrochlorothiazide.
- Unlike loop diuretics, thiazide diuretics tend to cause hypercalcemia by increasing calcium reabsorption in the distal tubule.
A nurse is caring for a client taking metolazone (Zaroxolyn). Which of the following clinical manifestations may indicate that the client is experiencing hypokalemia?
Explanation
Metolazone is a thiazide-like diuretic that targets the distal convoluted tubule by inhibiting sodium-chloride symporters. This interference triggers obligatory water loss alongside the depletion of essential ions. It is specifically indicated for refractory edema and hypertension. The resulting electrolyte imbalance frequently presents as muscle weakness, fatigue, and life-threatening cardiac conductivity changes.
Rationale for correct answer
C. Potassium is essential for maintaining the resting membrane potential of cardiac myocytes. Depletion of this cation by metolazone results in delayed repolarization and increased myocardial irritability. These physiological changes manifest as lethal cardiac dysrhythmias, such as premature ventricular contractions or torsades de pointes. The nurse must prioritize monitoring the electrocardiogram for U waves.
Rationale for incorrect answers
A. Diuretics are typically administered to treat high blood pressure by reducing the total intravascular volume. Hypokalemia does not typically cause an increase in systemic vascular resistance or blood pressure. Instead, excessive diuresis is more likely to result in orthostatic hypotension or a decrease in baseline pressure readings.
B. Polydipsia, or excessive thirst, is a classic clinical hallmark of hyperglycemia or diabetes insipidus rather than low potassium. While fluid loss from diuretics can cause dry mouth, it is not a pathognomonic sign of hypokalemia. The nurse should assess for serum glucose levels if this symptom persists in the absence of dehydration.
D. A skin rash is usually indicative of a hypersensitivity reaction or a dermatological side effect of a medication. It is not an objective finding associated with the depletion of intracellular or extracellular potassium levels. Integumentary changes are generally unrelated to the electrical or muscular dysfunction caused by an electrolyte deficiency.
Test-taking strategy
- Identify the physiological priority: When a question asks for a manifestation of an electrolyte imbalance like hypokalemia, always look for the system that is most affected by electrical conduction, which is the heart.
- Recall the function of potassium: Potassium is the primary intracellular cation responsible for muscle contraction and nerve impulse transmission. This should lead you directly to choices involving muscular or cardiac dysfunction.
- Eliminate based on medication intent: Metolazone is used to lower blood pressure, so selecting hypertension (choice 1) as a side effect is counterintuitive to the drug's therapeutic goal.
- Differentiate between metabolic and allergic responses: A rash (choice 4) is an immune-mediated or allergic response. Polydipsia (choice 2) is metabolic/endocrine. Neither describes the neuromuscular irritability or cardiac instability inherent to potassium depletion.
Take home points
- Metolazone is often used synergistically with loop diuretics to achieve profound diuresis in patients with diuretic resistance or advanced heart failure.
- Cardiac dysrhythmias and the presence of U waves on an EKG are critical clinical indicators of severe hypokalemia that require immediate intervention.
- Serum potassium levels should be maintained between 3.5 and 5.0 mEq/L to ensure safe pharmacological therapy with thiazide-like diuretics.
- Hypokalemia may also present as paralytic ileus, muscle cramping, and decreased deep tendon reflexes due to impaired smooth and skeletal muscle function.
The nurse is providing teaching to a client who has been prescribed furosemide (Lasix). Which of the following should the nurse teach the client?
Explanation
Furosemide is a sulfonamide-derived loop diuretic that inhibits the Na+/K+/2Cl- cotransporter in the thick ascending limb. It induces potent natriuresis and fluid volume reduction to treat acute pulmonary edema or hypertension. Rapid fluid shifts cause orthostatic hypotension and significant electrolyte wasting.
Rationale for correct answer
B. Loop diuretics significantly decrease intravascular volume and lower systemic venous pressure. This reduction in preload can lead to a sudden drop in blood pressure during postural changes. Rising slowly allows baroreceptors to compensate, preventing syncope and potential falls.
Rationale for incorrect answers
A. Kale, cauliflower, and cabbage are high in vitamin K, which interferes with warfarin therapy, not diuretics. Furosemide typically requires increasing intake of potassium-rich foods like bananas or spinach. Restricting these vegetables is medically unnecessary for a patient on digitalis-free diuretic therapy.
C. Counting the apical pulse for 60 seconds is a standard nursing requirement for digoxin, not furosemide. While diuretics affect hemodynamics, they do not have a primary chronotropic effect necessitating a full-minute count. Blood pressure assessment is a more pertinent vital sign priority.
D. Restricting fluids to 1 L per 24 hours is a strict intervention for advanced renal failure or severe hyponatremia. Unless specifically ordered for a comorbid state, such fluid restriction could lead to severe dehydration and prerenal azotemia. Clients should maintain adequate hydration unless directed otherwise.
Test-taking strategy
- Identify the physiological consequence of the drug: Furosemide is a powerful diuretic. Its primary effect is a rapid reduction in circulating blood volume.
- Prioritize safety interventions: Whenever a drug causes volume depletion, the most immediate safety risk is orthostatic hypotension. Teaching the client to move slowly is a direct risk reduction strategy for preventing syncope and injury.
- Rule out irrelevant nutritional restrictions: Differentiate between potassium-wasting diuretics (furosemide) and vitamin K interactions (warfarin). Since furosemide is not an anticoagulant, restricting leafy greens (option 1) is a distractor.
- Distinguish between drug classes: Recognize that heart rate monitoring (option 3) is a specific requirement for cardiac glycosides or beta-blockers. For diuretics, the circulatory priority is volume and pressure, not heart rate.
Take home points
- Orthostatic hypotension is a common and dangerous side effect of loop diuretics due to rapid decreases in intravascular hydrostatic pressure.
- Furosemide is a potassium-wasting medication that often necessitates the increased consumption of dietary potassium to avoid hypokalemia.
- Clients should be taught to take the medication in the morning to avoid nocturia and ensure optimal sleep hygiene.
- Any sudden weight gain of more than 2 pounds in 24 hours should be reported as it may indicate worsening heart failure or decreased drug efficacy.
Practice Questions 3
A nurse is monitoring a client who is receiving spironolactone (Aldactone). Which of the following findings should the nurse report to the provider?
Explanation
Spironolactone is a potassium-sparing diuretic that acts as a competitive aldosterone antagonist in the distal tubule. It inhibits sodium reabsorption while causing potassium retention to treat heart failure and primary hyperaldosteronism. Side effects include gynecomastia and life-threatening cardiac arrhythmias.
Rationale for correct answer
D. This medication functions by retaining potassium ions while promoting the excretion of water and sodium. A serum level of 5.2 mEq/L exceeds the normal range of 3.5 to 5.0 mEq/L. This hyperkalemia requires immediate reporting to prevent potential cardiac arrest.
Rationale for incorrect answers
A. Serum sodium of 148 mEq/L represents hypernatremia as the normal range is 135 to 145 mEq/L. While abnormal, spironolactone typically causes hyponatremia by promoting sodium excretion. This finding is likely unrelated to the direct pharmacological effect of the medication.
B. A urine output of 120 mL over 4 hours averages to 30 mL/hr. This meets the minimum threshold for adequate renal perfusion. It indicates a therapeutic response to the diuretic without suggesting acute failure.
D. A blood pressure of 140/90 mm Hg indicates hypertension, which is a common indication for this drug. Spironolactone is used to achieve normotension. This reading suggests the medication has not yet reached full therapeutic efficacy.
Test-taking strategy
- Identify the medication mechanism: Recognize spironolactone as a potassium-sparing diuretic. This immediately alerts the nurse to monitor for "high" potassium rather than the "low" potassium seen with loop or thiazide diuretics.
- Evaluate electrolyte ranges: Recall that the therapeutic range for potassium is narrow (3.5 to 5.0 mEq/L). Any value outside this range, especially on the high side for this specific drug, is a critical safety priority.
- Assess physiological minimums: Use the 30 mL/hr rule for urine output. Since 120 divided by 4 equals exactly 30, the output is sufficient and does not require urgent reporting.
- Prioritize safety risks: Hyperkalemia (choice 3) poses an immediate risk to cardiac electrical conduction. Hypertension (choice 4) or mild sodium deviations (choice 1) are less acutely life-threatening than potential ventricular fibrillation from high potassium.
Take home points
- Spironolactone carries a black box warning for hyperkalemia, necessitating regular monitoring of serum electrolytes and renal function.
- Patients should be instructed to avoid salt substitutes containing potassium chloride to prevent cumulative toxicity.
- The drug is often used in combination with loop diuretics to balance potassium loss and optimize fluid removal.
- Clinical signs of hyperkalemia include muscle weakness, peaked T-waves on an EKG, and eventual bradycardia.
A client with a history of heart failure will be started on spironolactone (Aldactone). Which of the following drug groups should not be used, or used with extreme caution in clients taking potassium-sparing diuretics?
Explanation
Spironolactone is a steroid-based aldosterone antagonist that inhibits mineralocorticoid receptors in the collecting duct. It blocks sodium reabsorption and reduces potassium excretion, treating hyperaldosteronism and heart failure. Side effects include hyperkalemia and gynecomastia. Contraindications include acute renal failure or serum potassium levels > 5.0 mEq/L.
Rationale for correct answer
D. Both ACE inhibitors and angiotensin receptor blockers (ARBs) suppress the renin-angiotensin-aldosterone system, which naturally reduces potassium elimination. When combined with spironolactone, these agents create a synergistic effect that significantly increases the risk of severe hyperkalemia. This drug-drug interaction requires vigilant monitoring of serum electrolytes to prevent fatal cardiac arrhythmias.
Rationale for incorrect answers
A. Nonsteroidal anti-inflammatory drugs (NSAIDs) can reduce the diuretic efficacy of spironolactone by inhibiting prostaglandin synthesis and causing sodium retention. While they may impact renal blood flow, they do not directly precipitate potassium retention as significantly as blockers of the aldosterone system. Their primary risk involves decreased therapeutic response to the diuretic rather than immediate electrolyte toxicity.
B. Corticosteroids generally possess mineralocorticoid activity that promotes the renal excretion of potassium and the retention of sodium. This effect is physiologically opposite to the action of potassium-sparing diuretics, which might actually help balance electrolyte levels. They do not typically cause dangerous elevations in serum potassium when used concurrently with aldosterone antagonists.
C. Loop diuretics, such as furosemide, inhibit the sodium-potassium-chloride cotransporter, which leads to substantial potassium wasting. They are frequently prescribed alongside spironolactone specifically to counteract the risk of potassium imbalance while maximizing fluid removal. This combination is a standard clinical practice rather than a contraindication in patients with refractory edema.
Test-taking strategy
- Analyze the drug mechanism: Identify spironolactone as a potassium-sparing diuretic. Focus on the primary risk of "saving" too much potassium.
- Identify drug interactions that compound the risk: Look for other medication classes that also increase potassium levels.
- ACE inhibitors (ending in -pril) and ARBs (ending in -sartan) both decrease aldosterone levels, leading to potassium retention.
- Combining two "potassium-retaining" mechanisms creates a high risk for toxicity.
- Eliminate based on electrolyte effects:
- Rule out loop diuretics (option 3) because they waste potassium, making them a safe and common companion to spironolactone.
- Rule out corticosteroids (option 2) as they typically cause potassium loss, not retention.
- Consider clinical priorities: While NSAIDs (option 1) can impair renal function, the question asks for groups that must be used with "extreme caution" specifically because of the nature of the potassium-sparing diuretic, making the RAAS-blocking agents the superior choice.
Take home points
- Concurrent use of spironolactone with ACE inhibitors or ARBs carries a significant risk of life-threatening hyperkalemia.
- Serum potassium levels must be monitored closely and should generally remain within the range of 3.5 to 5.0 mEq/L.
- Patients should be instructed to avoid salt substitutes containing potassium chloride while taking potassium-sparing diuretics.
- Clinical signs of hyperkalemia, such as peaked T-waves on an EKG or muscle weakness, require immediate medical notification.
The nurse is checking the laboratory data for a client taking spironolactone (Aldactone). Which result would be a potential concern?
Explanation
Spironolactone is a steroid-based aldosterone antagonist that competitively inhibits mineralocorticoid receptors in the cortical collecting duct. This potassium-sparing diuretic prevents the reabsorption of sodium and secretion of potassium ions. It is specifically indicated for congestive heart failure, hepatic cirrhosis with ascites, and primary hyperaldosteronism. Excessive retention leads to life-threatening cardiac dysrhythmias or heart block.
Rationale for correct answer
D. Spironolactone inhibits the exchange of sodium for potassium, which significantly increases the risk for hyperkalemia. A serum level of 5.8 mEq/L exceeds the normal physiological threshold of 3.5 to 5.0 mEq/L. This finding represents a critical safety concern requiring immediate medical intervention. The nurse must assess for electrocardiogram changes such as peaked T waves.
Rationale for incorrect answers
A. A serum sodium level of 140 mEq/L falls well within the standard reference range of 135 to 145 mEq/L. While this diuretic promotes natriuresis, this specific value indicates a stable and normal concentration of extracellular sodium. It does not represent a clinical complication or a cause for immediate concern. Reporting this value would be unnecessary for the health care provider.
B. The serum calcium level of 10.2 mg/dL is within the normal expected limits of 9.0 to 10.5 mg/dL. Spironolactone does not exert a significant direct effect on calcium homeostasis compared to thiazide or loop diuretics. This finding indicates that the patient is maintaining appropriate mineral balance during treatment. There is no evidence of medication-induced hypercalcemia or hypocalcemia in this laboratory result.
D. A magnesium level of 2.0 mg/dL is consistent with the normal therapeutic range of 1.3 to 2.1 mEq/L. Potassium-sparing diuretics often help retain magnesium along with potassium, preventing the hypomagnesemia commonly seen with other diuretic classes. This result shows the patient is not currently experiencing magnesium depletion. The nurse should continue to monitor but does not need to report this stable laboratory finding.
Test-taking strategy
- Identify the drug class and its metabolic footprint: Recognize spironolactone as a potassium-sparing diuretic. The most dangerous side effect of this class is the retention of potassium, leading to hyperkalemia.
- Compare laboratory values to standard reference ranges:
- Sodium 140 mEq/L (Normal: 135 to 145 mEq/L).
- Calcium 10.2 mg/dL (Normal: 9.0 to 10.5 mg/dL).
- Magnesium 2.0 mg/dL (Normal: 1.3 to 2.1 mEq/L).
- Potassium 5.8 mEq/L (Normal: 3.5 to 5.0 mEq/L).
- Prioritize the abnormal result: Since options 1, 2, and 4 are within normal limits, they are ruled out as "potential concerns." Choice 3 is the only abnormal value provided.
- Focus on life-threatening complications: Potassium imbalances are highly prioritized in nursing exams because they directly impact the cardiac conduction system and can lead to sudden death. Any potassium level > 5.0 mEq/L in a patient taking a potassium-sparing agent is a red flag.
Take home points
- Hyperkalemia is the most common and dangerous adverse effect of spironolactone therapy, necessitating regular serum electrolyte monitoring.
- Patients should be educated to avoid high-potassium foods and salt substitutes containing potassium chloride while taking aldosterone antagonists.
- Spironolactone is contraindicated in patients with significant renal impairment (creatinine clearance < 30 mL/min) due to the extreme risk of potassium accumulation.
- Clinical signs of hyperkalemia include muscle twitching, paresthesia, bradycardia, and characteristic peaked T waves on an electrocardiogram.
A nurse is providing education for a client with heart failure who is taking daily doses of spironolactone (Aldactone). Which of the following statements must be included in the teaching?
Explanation
Spironolactone is a steroid-based aldosterone antagonist that competitively inhibits mineralocorticoid receptors in the collecting duct. This potassium-sparing diuretic prevents the reabsorption of sodium and secretion of potassium ions. It is specifically indicated for congestive heart failure, hepatic cirrhosis with ascites, and primary hyperaldosteronism. Excessive retention leads to life-threatening cardiac dysrhythmias or heart block.
Rationale for correct answer
B. Spironolactone functions by inhibiting the exchange of sodium for potassium, which significantly increases the risk for hyperkalemia. Educating the client to avoid potassium-rich foods prevents the serum level from exceeding the normal limit of 5.0 mEq/L. This nutritional modification is essential to prevent lethal cardiac conduction abnormalities. Vigilant dietary adherence ensures that the medication remains within its safe therapeutic window.
Rationale for incorrect answers
A. Consuming large quantities of high-potassium foods while taking an aldosterone antagonist would lead to dangerous electrolyte accumulation. Unlike loop or thiazide diuretics, this drug does not cause wasting of this specific cation. Encouraging high intake would likely precipitate symptomatic hyperkalemia and potential cardiac arrest. This advice is contraindicated for patients taking any potassium-sparing pharmacological agent.
C. Grapefruit juice is a potent inhibitor of the cytochrome P450 3A4 enzyme system in the small intestine. While it affects many cardiovascular drugs, spironolactone does not have a major clinically significant interaction with this specific juice. Avoiding grapefruit is not a standard or mandatory instruction for this diuretic therapy. Patients should focus more on electrolyte and volume status instead.
D. Fiber intake is generally managed to regulate bowel movements and improve overall metabolic health in cardiac patients. A low-fiber diet has no scientific correlation with the pharmacodynamics or the side effect profile of spironolactone. In fact, high-fiber diets are typically encouraged for heart failure patients to prevent straining during defecation. This instruction is medically irrelevant to the therapeutic management of diuretic therapy.
Test-taking strategy
- Identify the pharmacological classification: Spironolactone is a potassium-sparing diuretic. This classification should immediately trigger the thought of "retaining potassium" rather than "losing potassium."
- Determine the safety priority: Since the drug keeps potassium in the body, the primary safety risk is hyperkalemia. To mitigate this risk, the nurse must teach the patient to limit the intake of external potassium sources.
- Rule out distractors:
- Identify that loop/thiazide diuretics require high-potassium diets, which is the opposite of spironolactone.
- Recognize that "grapefruit juice" is a common distractor for many drug questions (like statins or calcium channel blockers) but is not the primary concern for aldosterone antagonists.
- Evaluate the goal of teaching: The "most important" teaching for this drug class always centers on preventing potassium toxicity. Therefore, option 2 is the most scientifically sound and safe choice for a client being discharged on this specific medication.
Take home points
- Hyperkalemia is the most common and dangerous adverse effect of spironolactone therapy, requiring regular serum electrolyte monitoring.
- Patients should be educated to avoid high-potassium foods and salt substitutes containing potassium chloride while taking aldosterone antagonists.
- Clinical signs of hyperkalemia include muscle twitching, paresthesia, bradycardia, and characteristic peaked T waves on an electrocardiogram.
- Spironolactone is frequently used in heart failure to prevent myocardial remodeling and decrease mortality rates by blocking the effects of aldosterone.
A nurse is monitoring laboratory test results for clients receiving loop and thiazide diuretics. The nurse knows to look for which of these results?
Explanation
Loop and thiazide diuretics are potassium-wasting agents that inhibit sodium reabsorption in the thick ascending limb and distal tubule respectively. This increased distal delivery of sodium promotes obligatory potassium excretion, leading to clinical hypokalemia. These medications also impact metabolic homeostasis, potentially causing hyperuricemia or hyperglycemia.
Rationale for correct answer
A. Both loop and thiazide diuretics effectively block the reabsorption of sodium, which significantly increases sodium delivery to the late distal tubule and collecting duct. This physiological process stimulates the exchange of sodium for potassium, resulting in potassium depletion. Serum levels dropping below 3.5 mEq/L are a common adverse effect of these pharmacological therapies.
Rationale for incorrect answers
B. While thiazide diuretics tend to increase serum calcium by enhancing distal tubular reabsorption, loop diuretics actually promote calcium excretion. Loop diuretics are sometimes used therapeutically to treat life-threatening hypercalcemia by inducing calciuresis. Because these two classes have opposing effects on calcium, an increase is not a consistent finding for both.
C. Thiazide and loop diuretics are known to cause hyperglycemia rather than decreased serum glucose levels. The mechanism involves the inhibition of insulin secretion from the pancreas and decreased peripheral insulin sensitivity. Diabetic or pre-diabetic patients must monitor for elevated glucose while on these specific diuretic regimens.
D. The fundamental therapeutic purpose of all diuretics is to promote the renal excretion of sodium and water to reduce extracellular fluid volume. This action typically results in hyponatremia or decreased serum sodium levels rather than an increase. An increased sodium level would indicate a failure of the medication to achieve its primary osmotic goal.
Test-taking strategy
- Identify the shared characteristic: The question asks for a lab result common to "both" loop and thiazide diuretics.
- Recall electrolyte-wasting patterns: Both classes are classified as potassium-wasting diuretics because they act proximal to the potassium-sparing sites in the collecting duct. This makes hypokalemia (decreased potassium) the most predictable shared lab finding.
- Differentiate calcium effects: Use the mnemonic "Loop Loses" to remember that loop diuretics decrease calcium, whereas thiazides "save" calcium. Since their effects on calcium differ, option 2 is incorrect.
- Evaluate metabolic side effects: Remember that these diuretics tend to cause "highs" in non-electrolyte labs: high glucose (hyperglycemia), high uric acid (hyperuricemia), and high lipids. This allows you to rule out option 3, which suggests decreased glucose.
- Apply the basic definition of diuresis: Diuretics work by pulling sodium into the urine. Therefore, serum sodium is expected to decrease or stay normal, making option 4 incorrect.
Take home points
- Hypokalemia is the most significant and frequent electrolyte disturbance shared by loop and thiazide diuretic therapies.
- Thiazide diuretics are unique for causing hypercalcemia, whereas loop diuretics are utilized clinically to treat elevated calcium levels.
- Both diuretic classes can impair glucose tolerance, necessitating frequent blood sugar monitoring in patients with diabetes mellitus.
- Severe depletion of potassium (levels < 3.0 mEq/L) can precipitate lethal cardiac arrhythmias and potentiate digoxin toxicity.
For the client taking a diuretic, a combination such as triamterene and hydrochlorothiazide may be prescribed. The nurse realizes that this combination is ordered for which purpose?
Explanation
Triamterene is a pteridine derivative that functions as a potassium-sparing diuretic by blocking epithelial sodium channels in the distal nephron. Combined with hydrochlorothiazide, it mitigates the obligatory potassium loss typically induced by thiazide-mediated inhibition of the sodium-chloride symporter. This formulation treats hypertension while preventing severe electrolyte disturbances. Side effects include hyperkalemia or hyperuricemia. Contraindications involve serum potassium levels > 5.5 mEq/L or significant renal impairment characterized by a creatinine clearance < 30 mL/min.
Rationale for correct answer
B. Hydrochlorothiazide is a non-potassium-sparing diuretic that facilitates the renal excretion of potassium, potentially leading to symptomatic hypokalemia. Triamterene inhibits sodium-potassium exchange, effectively acting to increase serum potassium by retaining the cation. The primary clinical objective of this combination is to maintain homeostatic levels between 3.5 and 5.0 mEq/L. This synergistic approach prevents the development of lethal cardiac arrhythmias associated with potassium depletion.
Rationale for incorrect answers
A. Thiazide diuretics used in isolation frequently lead to a decrease in potassium, which can cause muscle weakness and metabolic alkalosis. Adding triamterene specifically opposes this effect to prevent the serum level from dropping below 3.5 mEq/L. Therefore, the combination is not designed to lower potassium, as this would exacerbate the risk of hypokalemia. Therapeutic goal is stabilization of electrolytes, not further reduction of this critical cation.
C. Thiazide diuretics are well-documented to interfere with pancreatic insulin release and peripheral glucose uptake, often leading to a diabetogenic effect. Neither triamterene nor hydrochlorothiazide possesses a pharmacological mechanism that would decrease glucose levels in the bloodstream. Consequently, this combination cannot be used to treat hyperglycemia or lower blood sugar. Patients must monitor for elevated glucose rather than a reduction during therapy.
D. While hydrochlorothiazide is known to potentially increase glucose levels, this metabolic side effect is a complication rather than the intended purpose of the combination. Triamterene is added strictly for its electrolyte-sparing properties and does not influence the glucose-raising profile of the thiazide component. The rationale for the dual-drug formulation is focused on potassium balance rather than intentionally altering glycemic parameters. This choice describes a secondary adverse effect instead of the primary therapeutic indication.
Test-taking strategy
- Analyze the drug combination: Recognize that one drug is potassium-wasting (hydrochlorothiazide) and the other is potassium-sparing (triamterene).
- Identify the physiological purpose of combination therapy: In diuretic therapy, pairing these two classes is a classic strategy to achieve "net zero" change in potassium.
- Evaluate the specific goal relative to the wasting agent: Since the thiazide component naturally causes potassium loss, the "purpose" of adding the second drug is to counteract that loss.
- To counteract loss, the second drug must increase serum potassium (or keep it from falling).
- Rule out distractors based on metabolic knowledge:
- Eliminate glucose-related options (3 and 4) because diuretics are not prescribed for their effects on blood sugar; these are merely side effects.
- Focus on the electrolyte mentioned (potassium) as it is the hallmark of the "sparing" vs. "wasting" distinction in pharmacology.
Take home points
- The combination of triamterene and hydrochlorothiazide is designed to utilize the diuretic effect of both while maintaining a stable serum potassium level.
- Nurses must monitor for signs of hyperkalemia, such as tall peaked T waves on an EKG, especially in patients with decreased renal function.
- This medication should not be used concurrently with potassium supplements or ACE inhibitors unless closely supervised, due to the extreme risk of potassium accumulation.
- Serum potassium levels should be assessed periodically to ensure they remain within the safe physiological range of 3.5 to 5.0 mEq/L.
Comprehensive Questions
A client who has increased intracranial pressure is receiving mannitol (Osmitrol). Which of the following findings should the nurse report to the provider?
Explanation
Mannitol is an osmotic diuretic that elevates plasma osmolality to pull water from the interstitial space into the intravascular compartment. It is utilized to reduce intracranial pressure and intraocular pressure. Side effects include pulmonary edema and electrolyte imbalances like hyponatremia.
Rationale for correct answer
C. Mannitol rapidly expands the circulating blood volume by drawing intracellular fluid into the vascular space. This sudden shift can overwhelm the left ventricle, leading to pulmonary congestion and subsequent dyspnea. This clinical manifestation indicates a life-threatening complication of heart failure.
Rationale for incorrect answers
A. A blood glucose level of 150 mg/dL is mildly elevated but is not a direct complication of osmotic therapy. Mannitol is a sugar alcohol and does not significantly alter glycemic control in most patients. This finding is not the most urgent priority to report.
B. A urine output of 40 mL/hr is above the minimum physiological threshold of 30 mL/hr. This indicates that the kidneys are responding to the diuretic effect of the medication. The nurse should continue to monitor but does not need to report this.
D. While a headache is a known side effect of mannitol due to cerebral dehydration, it is often the original symptom of increased intracranial pressure. If the headache is not worsening significantly, it is expected during treatment. It is less critical than respiratory distress symptoms.
Test-taking strategy
- Prioritize using ABCs: In this question, dyspnea represents a compromise of the Airway and Breathing status. Whenever a choice involves respiratory distress, it typically takes precedence over stable vital signs or expected side effects.
- Identify the mechanism of action: Recognize that mannitol is a volume expander before it is a diuretic. Understanding that it pulls fluid into the blood vessels helps predict that the heart might struggle with the increased load.
- Evaluate quantitative data: Use the standard nursing benchmark of 30 mL/hr for urine output. Since 40 mL/hr is a normal finding, you can safely eliminate option 2 as an urgent concern.
- Differentiate expected vs. adverse: Distinguish between a common side effect like a mild headache and a systemic complication like pulmonary edema. This differentiation allows for the selection of the answer that represents the highest risk to patient safety.
Take home points
- Mannitol administration requires frequent auscultation of lung sounds to detect early signs of pulmonary edema or crackles.
- The medication must be administered through a filter because it has a tendency to crystallize at room temperature.
- Serum osmolality should be monitored and generally maintained below 320 mOsm/kg to prevent acute kidney injury.
- Mannitol effectively reduces cerebral edema by creating an osmotic gradient that moves fluid across the blood-brain barrier.
A nurse is reviewing a client’s medication history and notes that the client is taking digoxin (Lanoxin), an antihypertensive medication, and NSAIDs. The client has a new prescription for torsemide (Demadex).
The nurse should plan to monitor for which of the following medication interactions? Select all that apply
Explanation
Torsemide is a high-ceiling loop diuretic that inhibits the Na+/K+/2Cl- symporter in the thick ascending limb. This facilitates potent natriuresis to manage congestive heart failure and systemic hypertension. Resulting electrolyte depletion, specifically hypokalemia (potassium < 3.5 mEq/L), significantly increases the risk of myocardial digitalis toxicity. Contraindications include anuria and severe hepatic coma.
Rationale for correct answers
B. Torsemide facilitates the rapid renal excretion of potassium ions along with water and sodium. This pharmacological action frequently leads to hypokalemia, which is a primary concern for the nurse. Low serum potassium levels sensitize the myocardium to cardiac glycosides. This increases the danger of electrolyte disturbances during therapy.
C. The concurrent use of torsemide and other antihypertensive agents creates a synergistic reduction in intravascular volume. This potent combined effect can lead to significant hypotension, especially during the initiation of therapy. The nurse must assess for symptoms of orthostatic changes to ensure safety. Monitoring arterial pressure is vital to prevent syncopal episodes.
D. Nonsteroidal anti-inflammatory drugs inhibit renal prostaglandins, which are necessary for maintaining adequate glomerular filtration. This biochemical interference effectively blunts the diuretic response, resulting in a low urine output despite medication administration. The NSAIDs cause sodium and water retention, directly opposing the therapeutic goals. This interaction complicates volume management in heart failure.
E. Hypokalemia induced by loop diuretics significantly increases the affinity of digoxin for the myocardial Na+/K+-ATPase pump. This biochemical shift predisposes the client to lethal ventricular dysrhythmias and other conduction abnormalities. Monitoring the cardiac rhythm is essential when these medications are administered together. The risk of sudden cardiac arrest is heightened by this interaction.
Rationale for incorrect answers
A. Loop diuretics do not typically cause a significant decrease in serum digoxin levels through pharmacokinetic interference. Instead, they increase the pharmacodynamic sensitivity of the heart to the existing digoxin concentration. The total glycoside level remains relatively stable, but its toxic potential rises due to potassium loss. Therefore, monitoring for a drop in the level is scientifically incorrect.
Test-taking strategy
- Analyze the medication list: The client is taking a loop diuretic (torsemide), a cardiac glycoside (digoxin), an antihypertensive, and NSAIDs.
- Identify key interactions:
- Loop Diuretic + Digoxin: Look for hypokalemia (Option 2) and the resulting risk of dysrhythmias (Option 5). Potassium loss is the "bridge" between these two drugs.
- Loop Diuretic + Antihypertensives: Expect a combined drop in blood pressure, leading to hypotension (Option 3).
- Loop Diuretic + NSAIDs: Recall that NSAIDs block prostaglandins, which are needed for diuresis. This results in low urine output (Option 4) or fluid retention.
- Rule out outliers: Option 1 is incorrect because diuretics make digoxin more dangerous, not less present in the blood.
- Focus on safety: Prioritize answers that address life-threatening complications like cardiac instability and renal interference.
Take home points
- Loop diuretics like torsemide are the primary cause of hypokalemia, which significantly potentiates the risk of digoxin toxicity.
- NSAIDs antagonize the effects of diuretics by inhibiting renal prostaglandins, leading to fluid retention and decreased urine output.
- Synergistic effects between diuretics and antihypertensive medications increase the risk of profound hypotension and falls.
- Continuous monitoring of serum electrolytes and cardiac rhythm is mandatory for clients on multi-drug regimens involving digoxin and diuretics.
A nurse is planning for a clients’ discharge from the hospital. Which of the following teaching points would be included for the client going home with a prescription for chlorothiazide (Diuril)?
Explanation
Chlorothiazide is a benzothiadiazide derivative that inhibits the sodium-chloride symporter within the distal convoluted tubule. This thiazide diuretic increases the delivery of sodium to the collecting duct, facilitating obligatory water loss. It is indicated for hypertension and congestive heart failure management. Common complications include hypokalemia, hyperuricemia, and sulfonamide-related hypersensitivity reactions.
Rationale for correct answer
C. Thiazides promote the renal excretion of potassium, potentially leading to serum levels below 3.5 mEq/L. Muscle cramping and profound physical weakness are hallmark clinical manifestations of hypokalemia. The patient must report these symptoms to avoid lethal cardiac dysrhythmias. This assessment is vital for maintaining neuromuscular function.
Rationale for incorrect answers
A. Increasing salt intake directly antagonizes the therapeutic goal of reducing extracellular fluid volume and blood pressure. Thiazides are intended to induce a negative sodium balance to treat edema. Encouraging high salt consumption could exacerbate fluid retention and lead to treatment failure. This advice contradicts standard cardiovascular nursing protocols.
B. While grapefruit and oranges contain vitamins, the primary dietary need for a patient on chlorothiazide is potassium. Vitamin C does not mitigate the electrolyte depletion risks inherent to this drug class. Patients should focus on potassium-rich options to prevent the metabolic disturbances associated with non-potassium-sparing agents. This instruction lacks pharmacological relevance.
D. Administering diuretics during the evening hours causes nocturia, which significantly disrupts the normal sleep-wake cycle. Chlorothiazide does not typically possess sedative properties or cause central nervous system depression leading to drowsiness. Doses should be scheduled for the morning hours to ensure patient safety and rest. This prevents nighttime fall risks.
Test-taking strategy
- Identify the drug classification: Chlorothiazide is a thiazide diuretic, which is known for its potassium-wasting effects and blood pressure reduction.
- Assess the physiological impact of the drug:
- Diuretics remove sodium and water; therefore, recommending more salt (option 1) is illogical and counter-therapeutic.
- Diuretics increase urination; therefore, taking them at night (option 4) is a safety and comfort error.
- Connect symptoms to electrolyte shifts: Muscle weakness and cramping (option 3) are specific, classic indicators of potassium deficiency.
- Prioritize clinical safety: In discharge teaching, the most important points relate to recognizing adverse effects that require provider intervention. While nutrition is important, identifying signs of life-threatening electrolyte imbalance like hypokalemia is a higher priority than generalized vitamin C intake (option 2).
Take home points
- Hypokalemia is a primary concern with thiazide diuretics and presents as muscle weakness, cramping, or cardiac palpitations.
- Diuretic doses should be taken in the morning to prevent nocturia and decrease the risk of falls during the night.
- Patients should monitor their daily weight and report any gain of 2 to 3 pounds within a 24-hour period.
- Thiazide diuretics are structurally related to sulfonamides and may cause cross-sensitivity in patients with sulfa allergies.
A client with diabetes has a new prescription for a thiazide diuretic. Which statement will the nurse include in teaching the client about the thiazide drug?
Explanation
Thiazide diuretics are benzothiadiazide derivatives that inhibit the Na+/Cl- symporter in the distal convoluted tubule. This interference induces natriuresis and potential hypokalemia, while simultaneously decreasing insulin secretion and peripheral glucose tolerance. This class is indicated for hypertension and edema but is contraindicated in patients with severe sulfonamide hypersensitivity or anuria. Common side effects include hyperuricemia, hypercalcemia, and metabolic alkalosis.
Rationale for correct answer
D. Thiazide diuretics decrease insulin sensitivity and inhibit the release of insulin from pancreatic beta cells. This pharmacological effect leads to secondary hyperglycemia, which is especially significant in patients with pre-existing diabetes mellitus. Monitoring blood glucose levels is essential to ensure that glycemic control is maintained during diuretic therapy. Dose adjustments of antidiabetic medications may be required to offset this drug-induced glucose elevation.
Rationale for incorrect answers
A. Informing a client there is nothing to concern them is medically inaccurate and negates the nurse's duty for informed consent. Thiazide diuretics possess a significant side effect profile including electrolyte imbalances and metabolic shifts. Professional nursing practice requires thorough education on potential risks to ensure patient safety and adherence.
B. Thiazides are non-potassium-sparing agents that promote the renal excretion of potassium ions into the urine. Clients should be encouraged to consume potassium-rich foods to prevent the development of symptomatic hypokalemia. Advising a patient to avoid potassium while on a wasting diuretic could precipitate life-threatening cardiac dysrhythmias.
C. Scheduling a diuretic at night is contraindicated because it induces nocturia and disrupts the patient's sleep-rest pattern. There is no pharmacological evidence that nocturnal administration prevents biochemical interactions with oral hypoglycemic agents or insulin. Doses should be taken in the morning to align peak diuresis with waking hours.
Test-taking strategy
- Identify the specific patient population: The question highlights that the client has diabetes, which is the most critical contextual clue.
- Recall metabolic side effects of thiazides: Use the mnemonic Hyper-GLUC (Glycemia, Lipidemia, Uricemia, Calcemia) to remember what levels increase with this drug class.
- Since glycemia (blood sugar) increases, the nurse must prioritize teaching related to glucose monitoring.
- Evaluate the safety of each instruction:
- Rule out option 2 because thiazides waste potassium; avoiding potassium would be dangerous.
- Rule out option 3 because diuretics should never be taken at bedtime due to nocturia and fall risks.
- Rule out option 1 because it provides false reassurance and ignores the scientific reality of drug side effects.
- Select the answer that addresses the comorbidity: Option 4 is the only choice that directly connects the new medication (thiazide) to the patient's existing condition (diabetes).
Take home points
- Thiazide diuretics can impair glucose metabolism, necessitating more frequent blood glucose monitoring in diabetic patients.
- Hypokalemia is a common complication of thiazide therapy, often requiring dietary potassium supplementation or the addition of a potassium-sparing agent.
- Nocturia and subsequent sleep deprivation are prevented by administering diuretic doses in the morning rather than at night.
- Thiazides are structurally related to sulfonamides, so nurses must assess for sulfa allergies before the first dose is administered.
The provider’s order reads: Give mannitol 0.5 g/kg IV now, over 2 hours. The client weighs 165 lb and you have a 100-mL vial of 20% mannitol. How many grams will the client receive? How many milliliters of mannitol will you prepare for this infusion?
Explanation
Mannitol is an osmotic diuretic that remains in the extracellular compartment to create an osmotic gradient across the blood-brain barrier. It facilitates the passive movement of water from the parenchyma into the intravascular space to reduce intracranial pressure. Clinical indications include cerebral edema and intraocular pressure reduction. Contraindications include established anuria from severe renal disease, pulmonary edema, or active intracranial bleeding.
Rationale for correct answer
The nurse must first convert the weight from pounds to kilograms.
This is by dividing 165 by 2.2.
Resulting in 75 kg.
Next step is multiplying the weight by the ordered dose (0.5 g/kg)
This determines that the client requires 37.5 g of mannitol.
Since a 20% solution contains 20 g per 100 mL, the nurse divides the desired 37.5 g by 0.20 to calculate the infusion volume.
Correct answer: 187.5 mL
This mathematical process ensures the precise administration of the prescribed osmotic load.
Test-taking strategy
- Convert weight first: Always convert pounds to kilograms (lb / 2.2) before performing dosage calculations in medical math.
- 165 lb / 2.2 = 75 kg.
- Determine total grams needed: Multiply the kg by the ordered g/kg dose.
- 75 kg x 0.5 g/kg = 37.5 g.
- Understand percentage concentrations: Recall that percent (%) in medications means grams per 100 mL.
- 20% mannitol = 20 g in 100 mL (or 0.2 g per 1 mL).
- Calculate final volume: Divide the required grams by the concentration per mL.
- 37.5 g / 0.2 g/mL = 187.5 mL.
- Verify the logic: Since the dose (37.5 g) is nearly double the amount in one 100 mL vial (20 g), the answer must be nearly double the volume of one vial.
- Avoid unit confusion: Ensure the final answer is in mL as requested by the second part of the question.
Take home points
- Mannitol requires the use of an in-line filter during administration because the solution is prone to crystallization at room temperature.
- Osmotic diuretics act by increasing the osmolality of the glomerular filtrate, which prevents the tubular reabsorption of water.
- Neurological status, hourly urine output, and serum osmolality must be monitored strictly to evaluate the effectiveness of the therapy.
- Rapid administration of high-dose mannitol can cause a transient increase in blood volume, which may exacerbate heart failure or pulmonary congestion.
A client is taking an aminoglycoside antibiotic for pneumonia and will also be taking the loop diuretic furosemide (Lasix) due to fluid overload. The nurse will monitor carefully for which potential effect from the interaction of these two drugs?
Explanation
Loop diuretics are potent inhibitors of the Na+/K+/2Cl- symporter in the thick ascending limb of the loop of Henle. These agents manage fluid overload but can disrupt the endolymph potential in the inner ear. Concomitant use with aminoglycosides increases the risk of irreversible sensorineural hearing loss and vestibular dysfunction. These drugs are contraindicated in states of anuria or severe sulfonamide hypersensitivity.
Rationale for correct answer
B. Both loop diuretics and aminoglycosides possess inherent ototoxic properties that affect the cochlear and vestibular systems. When administered concurrently, they exert a synergistic toxic effect on the hair cells within the inner ear. This interaction can lead to permanent deafness or significant tinnitus. The nurse must perform baseline and periodic auditory assessments to detect early damage.
Rationale for incorrect answers
A. While aminoglycosides are well-documented to cause renal tubular necrosis, furosemide is not primarily classified as a potent nephrotoxic agent. Although excessive diuresis can lead to prerenal azotemia, the specific synergy for renal damage is less characteristic than the synergy for auditory damage. The combined risk of ototoxicity is the most specific and profound interaction between these drug classes.
C. Pulmonary fibrosis is a chronic progressive lung disease often associated with medications like amiodarone or bleomycin. Neither aminoglycoside antibiotics nor loop diuretics are scientifically linked to the development of alveolar scarring or fibrotic changes. Monitoring for respiratory distress in this patient is related to their pneumonia and fluid overload, not a drug-induced fibrotic reaction.
D. Hepatotoxicity involves drug-induced injury to the hepatic parenchyma, commonly seen with medications like acetaminophen or isoniazid. Aminoglycosides and loop diuretics are primarily cleared and processed via renal mechanisms rather than hepatic pathways. There is no significant pharmacological evidence suggesting that this specific combination leads to liver failure. Serum transaminase monitoring is not the priority for this specific drug-drug interaction.
Test-taking strategy
- Identify shared adverse effects: When two different drug classes are administered together, look for a common "toxic" thread in their side effect profiles.
- Recall specific toxicities:
- Aminoglycosides (e.g., gentamicin) are known for ototoxicity and nephrotoxicity.
- Loop diuretics (e.g., furosemide) are known for ototoxicity, especially when given in high doses or rapidly.
- Apply the principle of synergy: Since both drugs can damage the same physiological system (the auditory nerve/inner ear), the combined risk is significantly amplified.
- Eliminate based on primary organ systems:
- Rule out option 4 (liver) and option 3 (lungs) as these drugs do not target those tissues.
- While nephrotoxicity (option 1) is a risk for aminoglycosides, the "interaction" or synergy with loop diuretics is most classically and dangerously associated with hearing loss.
Take home points
- The combination of loop diuretics and aminoglycosides significantly elevates the risk of permanent sensorineural ototoxicity.
- Nurses should monitor patients for symptoms such as tinnitus, vertigo, or perceived hearing loss during therapy.
- Rapid intravenous infusion of furosemide (exceeding 4 mg/min) should be avoided to minimize the risk of transient or permanent deafness.
- Baseline and serial audiograms may be indicated for patients receiving prolonged courses of these interacting medications.
The nurse knows that which of the following statements is correct regarding nursing care of a client receiving hydrochlorothiazide (HCTZ)? Select all that apply
Explanation
Hydrochlorothiazide is a benzothiadiazide derivative inhibiting the Na+/Cl- symporter in the distal convoluted tubule. This thiazide diuretic increases distal sodium delivery, facilitating obligatory potassium excretion and volume reduction. It manages hypertension and edema but is contraindicated in anuria or sulfonamide hypersensitivity. Adverse effects include hypokalemia, hyperuricemia, and hyperglycemia, requiring frequent monitoring of metabolic parameters and renal function to prevent systemic toxicity.
Rationale for correct answers
B. Thiazide diuretics promote the renal excretion of potassium into the tubular lumen. To maintain a serum level between 3.5 and 5.0 mEq/L, potassium supplements are frequently prescribed. This pharmacological intervention prevents hypokalemia, which could otherwise trigger lethal cardiac arrhythmias. Consistent replacement is vital for patients with high-dose therapy.
C. Hydrochlorothiazide consistently causes significant depletion of serum potassium levels during active diuresis. Simultaneously, it competes with uric acid for secretion in the proximal tubule, leading to hyperuricemia. Monitoring these specific laboratory values is essential to identify metabolic disturbances or potential gouty flares. Nurses must track these biochemical shifts regularly.
D. The primary therapeutic objective of hydrochlorothiazide is the reduction of systemic blood pressure through volume depletion. Baseline and serial assessments of pressure are mandatory to evaluate drug efficacy. This prevents the administration of the drug in cases of hypotension, which would compromise vital organ perfusion. It ensures the patient remains hemodynamically stable.
E. Oliguria, defined as urine output < 400 mL per 24 hours, indicates significant renal impairment or severe dehydration. Thiazide diuretics lose their efficacy when the glomerular filtration rate falls below 30 mL/min. Notifying the health care provider is critical because anuria is a strict contraindication for diuretic use. Immediate intervention prevents further acute kidney injury.
Rationale for incorrect answers
A. Thiazide diuretics are well-documented to interfere with pancreatic insulin release and peripheral glucose uptake. This physiological mechanism leads to hyperglycemia rather than decreased blood sugar. Assessing for hypoglycemia is clinically inappropriate as it does not align with the known metabolic side effects of this class. Diabetic patients must monitor for elevated glucose.
F. Clinical studies indicate that thiazide diuretics can cause a transient increase in low-density lipoproteins. They are associated with hyperlipidemia, not a reduction in serum lipids. Expecting to see decreased cholesterol levels is scientifically incorrect based on the drug's metabolic profile. These medications often negatively impact the lipid panel during long-term use.
Test-taking strategy
- Identify the drug class: Recognize hydrochlorothiazide as a thiazide diuretic and recall its primary effects on electrolytes and fluid balance.
- Determine wasting vs. retaining: Thiazides waste potassium (options 2 and 3) but retain calcium and uric acid (option 3).
- Assess clinical priorities:
- Safety first: Always check the vital sign the drug is intended to treat (blood pressure, option 4).
- Contraindications: Recall that diuretics require functioning kidneys; thus, low urine output (option 5) is a major red flag.
- Evaluate metabolic "highs": Use the mnemonic "Hyper-GLUC" (Glycemia, Lipidemia, Uricemia, Calcemia) to remember what goes up.
- This allows you to rule out option 1 (hypoglycemia) and option 6 (decreased lipids) because both glucose and lipids are expected to increase, not decrease.
- Select all that apply: Treat each option as a true/false statement based on the established side effect profile of benzothiadiazides.
Take home points
- Serum potassium and uric acid must be monitored to prevent hypokalemia-induced arrhythmias and hyperuricemia-induced gout.
- Blood pressure should always be assessed prior to administration to prevent severe hypotension and ensure therapeutic efficacy.
- Oliguria or anuria are clinical indicators that thiazide therapy should be withheld and the provider notified immediately.
- Patients with diabetes must monitor for hyperglycemia because thiazides can impair insulin sensitivity and glucose tolerance.
A client has heart failure, and a high dose of furosemide (Lasix) is ordered. What suggests a favorable response to Lasix?
Explanation
Furosemide is a sulfonamide-derived loop diuretic that inhibits the Na+/K+/2Cl- symporter in the thick ascending limb. It induces potent natriuresis to alleviate acute pulmonary edema and systemic fluid volume overload. Successful therapy reduces pulmonary hydrostatic pressure, thereby resolving dyspnea, orthopnea, and crackles. Toxicity risks include ototoxicity and severe electrolyte depletion, specifically potassium levels < 3.5 mEq/L.
Rationale for correct answer
B. Effective diuresis reduces pulmonary vascular congestion by decreasing intravascular volume and preload. This physiological shift improves alveolar gas exchange and reduces the work of breathing. A reduction in the respiratory rate toward the normal range of 12 to 20 breaths/min indicates clinical stabilization. Increased tidal volume depth confirms improved pulmonary compliance following fluid mobilization.
Rationale for incorrect answers
A. A decreased level of consciousness often signals worsening cerebral hypoxia or metabolic disturbances such as hyponatremia. It is not a therapeutic goal and may indicate poor perfusion to the central nervous system. Sleeping more could be a sign of extreme fatigue or impending hypercapnic respiratory failure. The nurse must monitor for acute mental status changes as a negative outcome.
C. Increased congestion and subjective complaints of dyspnea indicate that the medication has failed to achieve fluid mobilization. These findings represent a worsening of heart failure and potential progression toward respiratory arrest. Shortness of breath suggests that hydrostatic pressure in the pulmonary capillaries remains pathologically high. The nurse should anticipate escalating the dose or adding adjunctive therapy immediately.
D. An output of 50 mL over 4 hours averages only 12.5 mL/hour, which is significantly below the minimum renal threshold of 30 mL/hour. This oliguric state, especially with a 200 mL intake, suggests treatment failure or acute kidney injury. A favorable response requires a significant net loss where output exceeds intake. The nurse must assess for catheter patency or worsening renal perfusion.
Test-taking strategy
- Identify the therapeutic goal: The question asks for a "favorable response" to a loop diuretic in a heart failure patient. Diuretics are given to remove excess fluid from the lungs and body.
- Prioritize the ABCs:
- Airway and Breathing are the top priorities in heart failure.
- A favorable response must show improved respiratory status.
- Option 2 shows a decreased respiratory rate (moving toward normal) and better depth, which are direct indicators of improved oxygenation.
- Evaluate fluid balance:
- A diuretic should cause output to be greater than intake.
- In option 4, the intake (200 mL) is four times the output (50 mL), indicating fluid retention rather than diuresis.
- Eliminate neurological decline:
- Option 1 describes a decline in consciousness, which is never a favorable sign for any cardiovascular or respiratory medication.
- Recognize clinical worsening:
- Option 3 describes worsening physical assessment findings (increased congestion), which is the opposite of the drug's intended effect.
Take home points
- A primary indicator of furosemide efficacy in heart failure is the resolution of respiratory distress and the clearing of lung sounds.
- Successful diuresis is characterized by a urine output that exceeds fluid intake, typically maintaining a minimum of 30 mL per hour.
- Nurses must monitor for signs of dehydration and hypotension, such as tachycardia or skin tenting, after high-dose administration.
- Improved exercise tolerance and a decrease in daily body weight are long-term indicators of effective diuretic management.
A nurse is caring for a client on mannitol. What does the nurse know to be correct concerning the use of mannitol (Osmitrol) ?
Explanation
Mannitol is an osmotic diuretic that increases the osmolality of the glomerular filtrate, thereby inhibiting the tubular reabsorption of water. It is primarily utilized to reduce intracranial pressure or manage acute glaucoma crises. Administration must occur via a filtered needle to prevent the infusion of microscopic crystals. Serum osmolality should be monitored, targeting levels < 320 mOsm/kg.
Rationale for correct answer
A. Mannitol creates an osmotic gradient between the blood and the brain parenchyma, pulling intracellular fluid into the intravascular compartment. This rapid fluid shift effectively decreases cerebral edema and lowers pathologically elevated intracranial pressure. It is a standard pharmacological intervention for traumatic brain injury or neurosurgical prophylaxis. The nurse should observe for improved neurological status during therapy.
Rationale for incorrect answers
B. Mannitol is actually indicated to decrease, not increase, the intraocular pressure in patients suffering from acute angle-closure glaucoma. By elevating the plasma osmotic pressure, it draws aqueous humor from the eyeball into the bloodstream. This reduces the mechanical strain on the optic nerve. An increase in pressure would signify treatment failure or disease progression.
C. Mannitol facilitates the excretion of water and several electrolytes, which typically leads to electrolyte depletion rather than retention. While initial volume expansion might occur, the ultimate renal effect is the loss of sodium and potassium. Retention of these ions is characteristic of potassium-sparing agents, not osmotic diuretics. Nurses must monitor for signs of hyponatremia and hypokalemia.
D. Mannitol acts rapidly, with the onset of diuresis occurring within 30 to 60 minutes, not over several days. Its effects on intracranial pressure are even faster, often seen within 15 to 30 minutes of intravenous administration. Delayed diuresis would be a sign of acute tubular necrosis or significant renal obstruction. This medication is prioritized for its acute and immediate efficacy.
Test-taking strategy
- Identify the drug class: Mannitol is an osmotic diuretic, which works fundamentally differently than loop or thiazide diuretics.
- Determine the clinical indication: Osmotic diuretics are rarely used for peripheral edema; they are reserved for "hard" compartments like the skull and the eye.
- Evaluate the direction of pressure change: Diuretics are designed to reduce volume and pressure. Therefore, any choice suggesting an increase in pressure (option 2) is logically incorrect.
- Analyze the timeline of action: In critical care settings where mannitol is used, such as for brain herniation, a drug that takes days to work (option 4) would be useless.
- Recall electrolyte effects: Standard diuretics "wash out" solutes. Since mannitol keeps water in the tubule by osmotic force, it carries electrolytes with it, making "retention" (option 3) a false statement.
- Focus on the primary nursing priority: Reducing intracranial pressure is the most common and critical reason for mannitol administration in clinical practice.
Take home points
- Mannitol is a critical care medication used to reduce intracranial pressure by drawing fluid out of brain tissue through osmosis.
- The nurse must use an in-line filter or a filtered needle for administration because mannitol solution frequently crystallizes at room temperature.
- Vital assessments include monitoring for pulmonary edema and heart failure, as the initial shift of fluid into the blood can cause volume overload.
- Adequate renal function is required for use; the nurse must monitor hourly urine output to ensure the kidneys can handle the osmotic load.
The client has been receiving spironolactone (Aldactone) 50 mg/day for heart failure. The nurse should closely monitor the client for which condition?
Explanation
Spironolactone is a steroid-based aldosterone antagonist that competitively inhibits mineralocorticoid receptors in the distal renal tubules. This potassium-sparing diuretic prevents the reabsorption of sodium while inhibiting the active secretion of potassium and hydrogen ions. It effectively manages heart failure by mitigating the deleterious effects of hyperaldosteronism and cardiac remodeling. Side effects include gynecomastia, menstrual irregularities, and life-threatening electrolyte disturbances.
Rationale for correct answer
B. By antagonizing the mineralocorticoid receptor, spironolactone prevents the renal collecting duct from excreting potassium in exchange for sodium. This pharmacological mechanism leads directly to the retention of potassium, resulting in hyperkalemia (serum potassium > 5.0 mEq/L). This condition is the most dangerous metabolic complication of therapy. The nurse must monitor for cardiac dysrhythmias or peaked T-waves.
Rationale for incorrect answers
A. Loop and thiazide diuretics cause the loss of potassium, but spironolactone belongs to the potassium-sparing class which prevents such depletion. Consequently, hypokalemia is not a characteristic adverse effect of this specific medication. Patients are actually instructed to avoid high-potassium diets. This prevents the risk of myocardial instability associated with low potassium.
C. Spironolactone does not interfere with pancreatic insulin secretion or hepatic gluconeogenesis pathways to cause a drop in blood sugar. While some diuretics impact glucose, hypoglycemia is not a documented or expected side effect of aldosterone antagonists. The drug primarily influences electrolyte homeostasis rather than carbohydrate metabolism. Diabetic monitoring focuses more on potassium-induced insulin shifts.
D. Although diuretics can occasionally influence secondary mineral levels, spironolactone is not a primary cause of significant hypermagnesemia. Excessive magnesium levels ( > 2.2 mEq/L) are typically associated with renal failure or antacid overuse. The clinical priority for this drug remains the potassium balance. Magnesium shifts are rarely the primary clinical concern during standard dosing.
Test-taking strategy
- Identify the drug class: Categorize spironolactone as a potassium-sparing diuretic.
- Recall the physiological trade-off:
- Normal aldosterone causes the body to keep sodium and lose potassium.
- An aldosterone antagonist does the opposite: it loses sodium and keeps potassium.
- Evaluate the suffix/prefix: Recognize the "one" suffix often denotes a steroid-related structure, which in this case competes with the steroid hormone aldosterone.
- Match the mechanism to the risk: If the body is "sparing" or keeping potassium, the primary risk must be an excess of that ion.
- Differentiate from other diuretics: Contrast this with "potassium-wasting" diuretics like furosemide (loop) or hydrochlorothiazide (thiazide).
- Select the high-acuity answer: Hyperkalemia (Option 2) is the most common and life-threatening risk associated with this specific drug's mechanism of action.
Take home points
- Spironolactone is used in heart failure to block the effects of aldosterone, which helps prevent myocardial fibrosis and sodium retention.
- The most critical nursing priority is monitoring for hyperkalemia, especially in patients with impaired renal function or those taking ACE inhibitors.
- Patients should be educated to avoid salt substitutes containing potassium chloride, as these can cause lethal increases in serum potassium.
- Endocrine side effects such as gynecomastia or breast tenderness may occur because spironolactone can also bind to androgen and progesterone receptors.
A client who is diagnosed with heart failure has been taking a diuretic as part of the treatment and recently developed symptoms of drowsiness, confusion, and muscle weakness.
The nurse is assessing the client in the scenario who has been taking diuretics for several months for signs of dehydration. What should the nurse assess for? Select all that apply
Explanation
Diuretics induce therapeutic negative fluid balance by increasing renal solute and water excretion. Excessive diuresis precipitates hypovolemia, characterized by reduced intravascular volume and potential cellular dehydration. Signs include decreased ocular tension and poor skin mobility. Hemato-concentration occurs as plasma volume contracts. Serum sodium may fluctuate, while increased blood urea nitrogen typically accompanies this state. Hypotension and tachycardia often follow significant fluid deficit.
Rationale for correct answers
C. Inadequate intravascular and interstitial fluid volume reduces the production of saliva by the salivary glands. This physiological shift results in oral mucous membranes that appear dry, dull, and significantly sticky to the touch. It is a reliable clinical indicator of systemic water deficit.
D. As the total volume of plasma decreases due to diuresis, the cellular components of the blood become relatively more concentrated. This process, known as hematoconcentration, results in laboratory values for hematocrit and hemoglobin that are artificially elevated above the patient's baseline. It reflects a contraction of the vascular compartment.
E. Intraocular pressure is partially maintained by the volume of aqueous and vitreous humors. Systemic dehydration leads to a reduction in these fluids, causing the eyeballs to appear soft or sunken within the orbits. This physical finding is a hallmark of moderate to severe volume depletion.
F. A reduction in circulating blood volume leads to decreased stroke volume and lower peripheral perfusion pressure. Consequently, the nurse will palpate pedal pulses that feel diminished, thready, or weak upon physical examination. This reflects the body's inability to maintain robust peripheral arterial tension.
H. The hypothalamus contains osmoreceptors that detect increased plasma osmolality associated with fluid loss. This triggers a potent neurological drive for water intake, manifesting as excessive thirst or polydipsia. It is the body's primary compensatory mechanism to restore homeostatic fluid levels during active diuresis.
Rationale for incorrect answers
A. Healthy, well-hydrated skin possesses elastic turgor, meaning it immediately returns to its original position after being pinched. Dehydration causes the skin to lose this elasticity, resulting in a phenomenon called tenting, where the skin remains peaked. Elastic turgor indicates a euvolemic state rather than a fluid deficit.
B. Lowering of the hematocrit and hemoglobin levels from baseline typically suggests either active hemorrhage or fluid volume overload. In states of hemodilution, the excess plasma volume makes the red cell count appear decreased relative to the total volume. This is the opposite of what occurs during diuretic-induced dehydration.
G. Crackles are adventitious breath sounds produced by the snapping open of small airways filled with fluid. They are a classic clinical sign of pulmonary edema or volume overload often seen in heart failure. Dehydration would result in clear lung fields as the pulmonary interstitial fluid is mobilized.
Test-taking strategy
- Identify the core clinical problem: The question asks for signs of dehydration (fluid volume deficit).
- Apply the "Dry" principle: Focus on symptoms that represent a lack of moisture or volume.
- This directly points to dry mucous membranes (option 3), sunken eyeballs (option 5), and thirst (option 8).
- Recall physiological concentration:
- When water is lost from the blood, the remaining solids (like red blood cells) become more concentrated. This explains why elevated lab values (option 4) are correct and lower values (option 2) are incorrect.
- Assess perfusion and tension:
- Less volume means less pressure. This leads to weak pulses (option 6).
- Less volume in the skin means it loses its "bounce." Therefore, elastic turgor (option 1) must be incorrect because "elastic" implies normal hydration.
- Rule out volume overload: Crackles (option 7) indicate too much fluid in the lungs, which is what the diuretic is meant to treat, not a side effect of over-diuresis.
Take home points
- Dehydration in patients on diuretics is often evidenced by hematoconcentration, resulting in elevated hemoglobin and hematocrit levels.
- Physical assessment findings such as sunken eyes, sticky mucous membranes, and skin tenting are critical indicators of a fluid volume deficit.
- Weak peripheral pulses and orthostatic hypotension signify that the intravascular volume has dropped below the level required for optimal perfusion.
- The nurse must distinguish between signs of heart failure (crackles, edema) and signs of over-treatment with diuretics (thirst, weakness, dehydration).
The nurse discusses the importance of careful monitoring of laboratory values to the client in the scenario who has been switched from thiazide to furosemide (Lasix). Which statement by the client indicates a need for further education?
Explanation
Loop diuretics like furosemide inhibit the Na+/K+/2Cl- symporter in the thick ascending limb of the loop of Henle. This class induces profound natriuresis and rapid fluid mobilization to alleviate systemic edema or pulmonary congestion. High-potency diuresis frequently precipitates severe electrolyte imbalances, specifically hypokalemia (potassium < 3.5 mEq/L), and may cause ototoxicity or acute kidney injury.
Rationale for correct answer
B. Transitioning from a thiazide to a more potent loop diuretic significantly increases the risk of metabolic disturbances. The client's belief that lab monitoring can be discontinued suggests a dangerous knowledge deficit regarding the medication's high potency. Frequent monitoring of serum electrolytes and renal function is mandatory during the initial phase of furosemide therapy. This statement requires immediate nursing intervention and further education to ensure patient safety.
Rationale for incorrect answers
A. Maintaining a consistent schedule for laboratory assessments is a standard requirement for patients on long-term diuretic therapy. The client's statement confirms that they understand the need for periodic monitoring to track electrolyte stability. Since thiazides and loop diuretics both cause potassium wasting, continuing this habit is an appropriate self-care behavior. This reflects an accurate understanding of the chronic management of their condition.
C. Loop diuretics carry a high risk of inducing excessive fluid loss, which leads to intravascular volume depletion. The client correctly identifies that laboratory values, such as elevated blood urea nitrogen and hematocrit, serve as indicators of dehydration. Acknowledging the importance of these markers shows that the educational objectives have been successfully met. This awareness helps prevent complications like orthostatic hypotension or syncopal episodes.
D. Initiating a new pharmacological regimen requires increased vigilance to determine the drug's impact on organ perfusion. Furosemide can lead to prerenal azotemia or direct tubular damage if diuresis is too aggressive. The client's willingness to undergo frequent testing is a correct response to a new prescription for a potent diuretic. It ensures that any renal impairment is detected and addressed by the healthcare provider early.
Test-taking strategy
- Analyze the question stem: Focus on the phrase "needs further education," which indicates you are looking for an incorrect or unsafe statement by the client.
- Compare drug potency: Recognize that furosemide (a loop diuretic) is much stronger than thiazide diuretics and carries a higher risk for electrolyte depletion and dehydration.
- Identify safety risks:
- Monthly lab checks (option 1) are a safe and standard practice.
- Recognizing dehydration signs (option 3) is a positive safety behavior.
- Increasing lab frequency for a new med (option 4) is the gold standard for nursing care.
- Evaluate the "disruption" of monitoring: Option 2 suggests stopping monitoring because the drug is working. In pharmacology, the more effective a drug is at moving fluid, the more monitoring is required, not less.
- Select the outlier: Option 2 is the only statement that describes a reduction in clinical surveillance, which is never appropriate when escalating to a more potent diuretic.
Take home points
- Furosemide is more potent than thiazide diuretics and requires more frequent monitoring of electrolytes and renal function.
- Clients must understand that therapeutic stabilization of edema does not eliminate the risk of drug-induced metabolic alkalosis or hypokalemia.
- Laboratory monitoring of the blood urea nitrogen and creatinine ratio is essential to distinguish between heart failure progression and diuretic-induced dehydration.
- Any statement by a client suggesting a decrease in medical follow-up while on high-potency diuretics must be corrected immediately to prevent life-threatening complications.
A nurse is reviewing the common and serious adverse effects of furosemide (Lasix) therapy with the client in the scenario. Indicate with an X which are the common adverse effects and which are the serious adverse effects.
Explanation
Furosemide is a sulfonamide-derived loop diuretic that inhibits the Na+/K+/2Cl- symporter in the thick ascending limb of Henle. It facilitates profound diuresis and natriuresis to manage congestive heart failure and pulmonary edema by reducing intravascular volume. This drug frequently induces electrolyte depletion and metabolic disturbances, necessitating serum monitoring of potassium and magnesium levels. Adverse effects range from typical fluid shifts to life-threatening nephrotoxicity or ototoxicity if administered intravenously at rates exceeding 4 mg/min.
Rationale for correct answer
Common:
Hypokalemia. Renal excretion of potassium is an expected physiological consequence of increased sodium delivery to the distal tubule. This common effect requires dietary supplementation or pharmacological replacement to maintain serum levels between 3.5 and 5.0 mEq/L. It is a standard metabolic shift.
Hyperglycemia. Loop diuretics can interfere with pancreatic insulin release and diminish peripheral glucose utilization. This represents a common effect in patients with or without pre-existing diabetes mellitus. Nurses must monitor blood glucose levels periodically during long-term maintenance therapy.
Muscle cramps. Rapid loss of electrolytes, specifically potassium, magnesium, and calcium, leads to neuromuscular irritability. These common effects often occur during the initial phases of aggressive diuresis. They serve as a physical indicator of shifting fluid and ion balance.
Orthostatic hypotension. Significant reduction in circulating plasma volume diminishes the body's ability to maintain arterial pressure during postural changes. This common effect increases the risk of falls and syncope. Clients must be taught to move from supine positions slowly.
Hyperuricemia. Furosemide competes with uric acid for secretion in the proximal tubule, leading to increased serum concentrations. This is a common effect that may trigger acute gouty arthritis in susceptible individuals. It is a frequent biochemical byproduct of chronic loop diuretic use.
Dry mouth. Increased renal water clearance leads to systemic dehydration and decreased salivary secretion. This is a common effect and a subjective indicator of the drug's intended diuretic action. It reflects the overall volume depletion occurring within the extracellular compartment.
Severe:
Confusion. Alterations in mental status signal severe fluid-electrolyte imbalances or metabolic alkalosis affecting the central nervous system. This is a serious effect that requires immediate clinical intervention to prevent coma. It indicates profound cerebral dehydration or hyponatremia.
Tremors. Involuntary muscle contractions often result from severe hypomagnesemia or electrolyte derangements. This is a serious effect that can progress to tetany or cardiac arrhythmias if not addressed. It indicates a critical deficiency of essential divalent cations.
Test-taking strategy
- Categorize by severity: Distinguish between "nuisance" side effects that are predictable and "critical" changes that indicate organ dysfunction or life-threatening instability.
- Recall the "Hyper/Hypo" rules: Loop diuretics cause "hypo" states for most ions (potassium, sodium, magnesium) but "hyper" states for glucose and uric acid.
- Identify neurological triggers: Confusion and tremors are never "common" or expected; they indicate a neurological emergency secondary to severe electrolyte depletion.
- Link mechanism to symptoms:
- Dehydration naturally causes dry mouth and orthostatic hypotension.
- Electrolyte loss naturally causes muscle cramps.
- Evaluate metabolic impact: Hyperglycemia and hyperuricemia are standard metabolic disturbances associated with the loop of Henle's interaction with the proximal and distal tubules.
- Prioritize patient safety: Any symptom affecting consciousness or motor control (confusion/tremors) must be classified as serious.
Take home points
- Common adverse effects of furosemide involve predictable metabolic shifts like hypokalemia, hyperglycemia, and hyperuricemia.
- Hemodynamic changes, such as orthostatic hypotension and dry mouth, are expected results of the intended reduction in intravascular volume.
- Serious adverse effects like confusion and tremors indicate dangerous levels of dehydration or electrolyte depletion and require immediate medical assessment.
- Effective nursing care involves educating the client on both the expected minor discomforts and the critical symptoms that warrant an emergency call.
The nurse is discussing the possible adverse effects of thiazide diuretic therapy with a client. The nurse recognizes that further education is needed when the client makes which statement?
Explanation
Thiazide diuretics inhibit the sodium-chloride symporter within the distal convoluted tubule to induce moderate natriuresis and manage systemic hypertension. These agents are contraindicated in cases of anuria or severe sulfonamide hypersensitivity. Metabolic complications typically involve hyperuricemia (serum urate > 7 mg/dL), hyperglycemia, and secondary hypokalemia.
Rationale for correct answer
A. Thiazide diuretics are utilized to treat hypertension and edema by facilitating renal fluid excretion, but they do not typically cause renal failure. The client's belief that their kidneys will shut down represents a significant misconception regarding the drug's safety profile and therapeutic intent. While high doses can cause prerenal azotemia, permanent organ failure is not an expected adverse effect. This statement requires immediate clarification and corrective education.
Rationale for incorrect answers
B. Hydrochlorothiazide is a first-line pharmacological intervention for the management of primary hypertension. The client's statement accurately reflects the intended therapeutic goal of achieving better blood pressure control through volume reduction. This understanding demonstrates that the patient has a correct grasp of why the medication was prescribed. It shows an appropriate expectation of clinical improvement once the drug reaches steady-state concentrations.
C. Thiazides compete with uric acid for secretion in the proximal tubule, which frequently results in elevated serum urate levels. This metabolic shift can precipitate an acute gout flare, characterized by podagra or significant joint inflammation. The client correctly identifies the need to report these symptoms to the healthcare provider for evaluation. This awareness is a vital component of safe medication self-management and risk reduction.
D. Most thiazide diuretics facilitate the loss of potassium ions into the urine, which can lead to life-threatening hypokalemia. The client's acknowledgment of the need for periodic blood work is essential for monitoring electrolyte homeostasis. Maintaining serum potassium within the 3.5 to 5.0 mEq/L range prevents cardiac arrhythmias. This statement indicates that the patient understands the necessity of ongoing laboratory surveillance during therapy.
Test-taking strategy
- Analyze the question goal: Identify that the question asks for a statement indicating a need for further education, meaning you must select the incorrect or false statement.
- Evaluate the severity of claims:
- Option 1 claims "kidneys to shut down," which is an extreme and usually incorrect expectation for a drug meant to assist renal function in fluid removal.
- Moderate diuretics like thiazides are generally safe and do not cause acute tubular necrosis in standard doses.
- Match drug knowledge to options:
- Thiazides treat hypertension (validates option 2).
- Thiazides cause hyperuricemia and can trigger gout (validates option 3).
- Thiazides are potassium-wasting (validates option 4).
- Select the outlier: Option 1 is the only statement describing a catastrophic, non-standard side effect, confirming it as the knowledge deficit.
- Bold key medical concepts: Focus on the distinction between expected metabolic shifts (potassium, uric acid) and unrealistic organ failure.
Take home points
- Thiazide diuretics are commonly used for hypertension and generally do not cause renal failure unless the patient is severely hypovolemic or in shock.
- Hyperuricemia is a common side effect of thiazides, and patients with a history of gout must be monitored for acute joint pain and swelling.
- Periodic laboratory monitoring is mandatory to detect hypokalemia, as low potassium levels can predispose patients to cardiac conductivity issues.
- Effective patient education must emphasize that while diuretics affect kidney output, they are intended to preserve heart and kidney health by reducing workload.
The nurse taking the client’s blood pressure notes a decrease in the value from recent readings. What explanation will the nurse give the client in the scenario currently taking furosemide (Lasix) regarding this change?
Explanation
Furosemide is a potent loop diuretic that acts on the thick ascending limb of the loop of Henle to inhibit the Na+/K+/2Cl- symporter. By preventing the reabsorption of sodium and chloride, it forces the renal excretion of water, which significantly reduces intravascular volume and cardiac preload. This pharmacological action is the primary mechanism for treating hypertension and pulmonary edema. Adverse effects include profound hypokalemia (potassium < 3.5 mEq/L), orthostatic hypotension, and potential ototoxicity if infused too rapidly.
Rationale for correct answer
C. The intended therapeutic effect of furosemide is the reduction of total body fluid through increased urine output. As the volume of circulating blood decreases, the pressure exerted against the arterial walls naturally drops. This explanation provided by the nurse accurately reflects the hemodynamic shift expected during active diuresis. It educates the client on how the medication is successfully achieving its goal of lowering systemic blood pressure and reducing fluid overload.
Rationale for incorrect answers
A. Assuming a decreased reading is a measurement error without assessment data ignores the expected pharmacological outcome of a loop diuretic. While the nurse should ensure accuracy, labeling a therapeutic response as an error may cause unnecessary confusion or alarm for the client. The drop in pressure is a predictable result of volume depletion. Relying on rechecks alone fails to acknowledge the drug's physiological impact on the cardiovascular system.
B. Attributing a decrease in blood pressure to anxiety or worry is scientifically inconsistent with physiological responses to stress. Psychological stress typically activates the sympathetic nervous system, leading to tachycardia and an increase in blood pressure via vasoconstriction. This explanation provides incorrect information to the client and misses an opportunity for essential medication education. It ignores the direct relationship between the diuretic and the patient's hemodynamic status.
D. A decrease in blood pressure is an indicator of a positive response to diuretic therapy, not a failure. Stating the client is not responding correctly is a significant clinical misinterpretation of the data presented. Furosemide is prescribed specifically to reduce pressure and volume; therefore, a lower reading suggests therapeutic efficacy. Reevaluating the medication based on a successful drop in pressure would be counterproductive to the treatment plan for heart failure or hypertension.
Test-taking strategy
- Identify the drug's primary action: Furosemide is a diuretic. Diuretics remove fluid. Less fluid in the pipes (vessels) means lower pressure.
- Distinguish between therapeutic effects and errors: A lower blood pressure reading after starting an antihypertensive diuretic is an expected outcome, not an error (ruling out option 1).
- Apply physiological principles:
- Stress usually raises BP, it doesn't lower it (ruling out option 2).
- If the drug is meant to lower BP, and the BP is lower, the drug is working (ruling out option 4).
- Focus on patient education: The most "nursing-centric" and scientifically accurate answer is the one that explains the mechanism of action (volume reduction) in understandable terms (option 3).
- Analyze the relationship between volume and pressure: Always remember that in a closed system, a decrease in intravascular volume leads to a decrease in hydrostatic pressure.
Take home points
- Diuretics lower blood pressure primarily by reducing the total volume of blood the heart must pump through the vascular system.
- A decrease in blood pressure measurements is a standard therapeutic goal and a sign of effective furosemide therapy.
- Nurses must monitor for orthostatic hypotension, as a rapid drop in volume can lead to dizziness when the patient stands.
- Accurate patient education involves explaining that the "water pill" works by shifting fluid out of the blood and into the urine.
The nurse was caring for a client who asked for a pain pill (ibuprofen) for a recent arm fracture and was currently taking the diuretic furosemide (Lasix). What would be an appropriate response by the nurse?
Explanation
Nonsteroidal anti-inflammatory drugs inhibit cyclooxygenase enzymes, reducing prostaglandin synthesis within the renal parenchyma. This biochemical interference blunts renal vasodilation, directly opposing the therapeutic efficacy of loop diuretics. Prostaglandins are essential for maintaining glomerular filtration and facilitating sodium excretion in the thick ascending limb. When these local hormones are suppressed, the kidney retains sodium and water, potentially exacerbating fluid overload or causing acute nephrotoxicity.
Rationale for correct answer
D. Ibuprofen reduces the production of renal prostaglandins which normally facilitate the vasodilatory response required for optimal diuretic action. By inhibiting these local vasodilators, the diuretic effect of furosemide is significantly antagonized or blunted. Consequently, the client may require an increased dosage of the loop diuretic to achieve the desired net fluid loss. This pharmacological interaction necessitates close monitoring of the client's weight and edema status.
Rationale for incorrect answers
A. Stating that the two medications do not interact is a significant clinical error that ignores the documented antagonistic relationship between loop diuretics and NSAIDs. Ibuprofen causes renal sodium retention, which directly contradicts the intended natriuretic goal of furosemide therapy. Providing this information to the client would be medically inaccurate and potentially dangerous. The nurse must recognize the metabolic impact on renal hemodynamics.
B. Telling a client that no pain medication can be given is an inappropriate and dismissive response to acute pain. While ibuprofen has a known interaction, other analgesics like acetaminophen can be safely utilized without affecting renal prostaglandins. The nurse should collaborate with the provider to find a compatible alternative rather than denying all pain relief. Effective pain management is a fundamental component of orthopedic nursing care.
C. This statement incorrectly suggests that the pain medication will enhance or increase the potassium-wasting or fluid-removing properties of furosemide. In reality, NSAIDs decrease the efficiency of the diuretic, leading to a diminished effect rather than an increased one. This misconception could lead the client to expect excessive urination when the opposite is true. The interaction results in fluid retention, not increased diuresis.
Test-taking strategy
- Identify the drug interaction: Recognize that furosemide (a loop diuretic) and ibuprofen (an NSAID) have a classic antagonistic relationship.
- Recall the mechanism:
- Furosemide relies on renal blood flow and prostaglandin-mediated vasodilation to work effectively.
- NSAIDs block prostaglandins.
- Therefore, NSAIDs make diuretics less effective.
- Evaluate the clinical outcome: If a drug is less effective, you either need a higher dose of that drug or you need to stop the interfering substance. Option 4 correctly identifies the need for an increased dosage.
- Eliminate false negatives: Option 1 is false because an interaction definitely exists.
- Eliminate clinical extremes: Option 2 is an extreme "no" that ignores other pain management options.
- Assess direction of effect: Option 3 incorrectly predicts an "increased effect," which contradicts the antagonistic nature of the interaction.
Take home points
- Nonsteroidal anti-inflammatory drugs like ibuprofen can cause significant sodium and water retention by inhibiting renal prostaglandins.
- When taken concurrently with furosemide, NSAIDs can reduce the antihypertensive and diuretic effectiveness of the medication.
- Clients taking this combination should be monitored for signs of worsening heart failure, such as peripheral edema and sudden weight gain.
- Acetaminophen is generally preferred for mild to moderate pain in patients on diuretic therapy because it does not interfere with renal function.
The nurse knows that individuals with impaired renal function, cirrhosis of the liver, or diabetes mellitus need to be given diuretics cautiously because they are known to cause what effect? Select all that apply
Explanation
Diuretics modulate hydro-electrolytic homeostasis by altering tubular reabsorption of solutes in the nephron. These agents treat heart failure and portal hypertension, but their metabolic profile often induces hyperglycemia and significant fluid shifts. In patients with hepatic or renal impairment, altered pharmacokinetics can lead to rapid circulatory collapse or encephalopathy.
Rationale for correct answers
A. Thiazide and loop diuretics interfere with pancreatic insulin release and peripheral glucose utilization. This pharmacological interference leads to hyperglycemia, requiring frequent monitoring in diabetic populations. Elevated blood glucose levels can destabilize metabolic control. Dosage adjustments of hypoglycemic agents may be necessary.
B. Cirrhotic patients often exhibit baseline peripheral vasodilation and decreased effective volume. Diuretic-induced fluid removal can precipitously lower intravascular pressure, resulting in severe orthostatic hypotension. Rapid shifts in fluid compartments increase the risk of syncope. This can further compromise already fragile hepatic perfusion.
C. Impaired kidneys cannot effectively regulate the excretion and retention of ions during forced diuresis. This leads to profound electrolyte imbalances, specifically hypokalemia, hyponatremia, and hypermagnesemia. Careful monitoring of serum chemistries is required to prevent life-threatening cardiac dysrhythmias. Renal clearance directly dictates the severity of these disturbances.
Rationale for incorrect answers
D. Diuretics are associated with metabolic "highs," including elevated glucose, rather than hypoglycemia. The decrease in insulin sensitivity and potassium-related inhibition of insulin secretion prevents low sugar states. Using the term hypoglycemia is scientifically inaccurate for this medication class. Patients are at higher risk for ketoacidosis than insulin shock.
E. Diuretics are specifically indicated to reduce, not cause, edema by promoting natriuresis. If edema develops during therapy, it is likely due to the underlying renal disease rather than a side effect of the drug. Claiming diuretics cause secondary edema contradicts their primary physiological function. Successful therapy results in a net loss of interstitial fluid.
Test-taking strategy
- Identify the drug-condition interaction: The question focuses on how diuretics affect specific vulnerable populations like those with renal, hepatic, or diabetic issues.
- Recall metabolic effects: Use the "Hyper" rule for diuretics (Hyperglycemia, Hyperlipidemia, Hyperuricemia).
- This allows for the selection of option 1 (hyperglycemia) and the elimination of option 4 (hypoglycemia).
- Assess hemodynamic risks:
- Cirrhotic patients have low oncotic pressure. Removing fluid from their blood volume quickly leads to hypovolemia.
- This makes orthostatic hypotension (option 2) a correct and logical safety concern.
- Consider organ function:
- Renal disease means the kidneys cannot balance ions well.
- Diuretics force ion movement.
- Therefore, electrolyte imbalances (option 3) are inevitable and must be monitored.
- Evaluate therapeutic goals:
- Diuretics are the treatment for edema.
- Therefore, saying they "cause edema" (option 5) is a direct contradiction of their medical purpose.
Take home points
- Diuretics are known to increase blood glucose levels, necessitating close surveillance of diabetic patients for hyperglycemia.
- In cirrhosis, diuretics must be titrated slowly to prevent rapid volume depletion and subsequent orthostatic hypotension or hepatic coma.
- Renal impairment increases the risk of severe electrolyte disturbances because the kidneys cannot compensate for drug-induced ion losses.
- Thiazides and loop diuretics should be avoided or used with extreme caution if the glomerular filtration rate is significantly diminished.
The nurse monitoring the client in the scenario using diuretics to reduce peripheral edema will watch for which therapeutic response?
Explanation
Diuretics modulate renal hemodynamics to facilitate the excretion of sodium and water, effectively reducing interstitial fluid accumulation in peripheral tissues. They are the primary pharmacological intervention for volume overload, targeting the nephron to induce significant natriuresis and weight loss. Contraindications include anuria and severe electrolyte depletion, while monitoring focuses on orthostatic hypotension and potassium levels.
Rationale for correct answer
B. The specific clinical objective for treating peripheral edema is the mobilization of fluid from the extracellular compartment back into the intravascular space. Successful diuresis is objectively confirmed when the volume of urine output significantly exceeds the fluid intake. As this excess fluid is excreted by the kidneys, the visible swelling in the extremities resolves. This represents a direct and favorable response to the medication.
Rationale for incorrect answers
A. While certain specialized agents like osmotic diuretics can reduce cerebral edema, standard diuretics used for peripheral swelling do not primarily target the brain. Headaches are more likely to be a side effect of dehydration rather than a sign of therapeutic success. A reduction in intracranial pressure is not the intended outcome for typical volume overload management. Standard loop or thiazide diuretics have limited efficacy in crossing the blood-brain barrier.
C. Ascites refers to the pathological accumulation of fluid within the peritoneal cavity, which is distinct from the subcutaneous tissue of the limbs. Although diuretics are used for liver congestion, the question specifically asks for the response related to peripheral edema. Monitoring for a reduction in abdominal girth would be the priority for hepatic cirrhosis patients. Peripheral responses and central cavity responses involve different assessment protocols and physiological goals.
D. Diuretics do not inherently cause an improvement in the underlying filtration capacity of the kidneys. In many cases, aggressive diuresis can actually lead to a temporary increase in creatinine due to decreased perfusion. The drug manages the symptoms of fluid retention rather than repairing renal disease or structural damage. Using these agents primarily targets systemic fluid balance rather than intrinsic renal rehabilitation.
Test-taking strategy
- Define the clinical problem: The question focuses on "peripheral edema," which is swelling of the limbs.
- Match the symptom to the outcome:
- If the problem is edema (excess fluid), the therapeutic response must be a reduction in edema.
- Diuretics work by increasing urination, so increased urine output must be present.
- Rule out anatomical distractors:
- Option 1 (cerebral) and Option 3 (ascites/liver) refer to fluid in different body compartments.
- Peripheral edema is assessed in the extremities, not the brain or abdomen.
- Distinguish between symptom management and cure:
- Option 4 is incorrect because diuretics treat the symptoms (edema) of heart or kidney failure, not the cause (renal function itself).
- Identify the most direct response: Option 2 combines the physical assessment (less edema) with the physiological mechanism (more urine), making it the most complete answer.
Take home points
- The primary indicator of successful diuretic therapy for peripheral edema is a measurable increase in urine output and a decrease in extremity circumference.
- Nurses should monitor daily weights at the same time each morning as the most accurate non-invasive measure of fluid loss.
- Resolution of pitting edema and improved skin integrity are key physical findings that signal a therapeutic response to diuresis.
- A lack of increased urine output following administration may indicate renal resistance or the need for a different class of diuretic medication.
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Describe the definition and primary therapeutic purposes of diuretics in clinical practice.
- Identify the major classes of diuretics and their specific nephron sites of action.
- Explain the mechanism of action and pharmacologic effects of carbonic anhydrase inhibitors.
- Discuss the mechanism, clinical significance, and adverse effects of loop diuretics.
- Summarize the mechanism, indications, and monitoring requirements for thiazide diuretics.
- Explain how potassium-sparing diuretics conserve potassium while promoting mild diuresis.
- Describe the rationale, mechanisms, and clinical benefits of combination diuretic products.
- Identify common and serious adverse effects associated with each class of diuretics.
- Outline nursing interventions, monitoring strategies, and patient education for diuretic therapy.
- Evaluate therapeutic effectiveness and safety of diuretics using fluid balance, electrolytes, and clinical outcomes.
Introduction
Definition
Diuretics are medications that increase urine output by acting on specific segments of the nephron to promote the excretion of sodium and water.
By reducing intravascular volume, diuretics decrease blood pressure, preload, and edema, making them essential in cardiovascular, renal, and endocrine disorders.
Primary Purposes of Diuretic Therapy
Diuretics are prescribed to:
- Reduce fluid overload in conditions such as heart failure, renal disease, and liver cirrhosis
- Manage hypertension by lowering circulating blood volume
- Decrease edema (peripheral, pulmonary, cerebral)
- Correct or prevent electrolyte imbalances in specific clinical situations
- Reduce intraocular pressure and intracranial pressure (select agents)
Sites of Action in the Nephron
Each class of diuretics works at a different location within the nephron, which determines its potency and electrolyte effects:
- Proximal Convoluted Tubule (PCT): Carbonic anhydrase inhibitors
- Loop of Henle (Ascending Limb): Loop diuretics
- Distal Convoluted Tubule (DCT): Thiazide diuretics
- Collecting Duct: Potassium-sparing diuretics
Understanding the site of action helps predict:
- Degree of diuresis
- Electrolyte losses
- Acid–base effects
- Drug combinations used in therapy
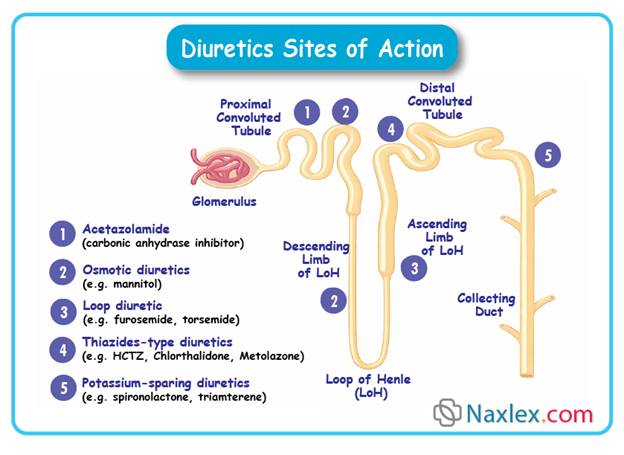
Major Classes of Diuretics
Diuretics are broadly classified into:
- Carbonic Anhydrase Inhibitors
- Example: Acetazolamide
- Loop Diuretics
- Sulfonamide-type: Furosemide, Bumetanide, Torsemide
- Non-sulfonamide: Ethacrynic acid
- Thiazide and Thiazide-Like Diuretics
- Examples: Hydrochlorothiazide, Chlorthalidone, Metolazone
- Potassium-Sparing Diuretics
- Aldosterone antagonists: Spironolactone
- Sodium channel blockers: Amiloride, Triamterene
- Combination Diuretic Products
- Fixed-dose combinations to enhance efficacy and minimize potassium imbalance
Most diuretics work by blocking sodium reabsorption at specific nephron sites.
Because water follows sodium, inhibition of sodium reabsorption leads to increased water excretion.
Key principles:
- Greater sodium blockade = greater diuretic effect
- Electrolyte losses depend on nephron location
- Potent diuresis increases the risk of hypovolemia and electrolyte imbalance
Therapeutic Uses of Diuretics
Common clinical indications include:
- Heart failure (acute and chronic)
- Hypertension
- Pulmonary edema
- Chronic kidney disease
- Nephrotic syndrome
- Ascites due to liver disease
- Glaucoma
- Increased intracranial pressure
Carbonic Anhydrase Inhibitors
Examples:
• acetazolamide (Diamox)
• methazolamide (Neptazane)
Mechanism of Action & Drug Effects:
Carbonic anhydrase inhibitors act by inhibiting carbonic anhydrase in the proximal renal tubule.
This enzyme normally catalyzes the conversion of carbon dioxide and water to bicarbonate and hydrogen ions.
Inhibition leads to:
• Decreased reabsorption of bicarbonate → increased urinary bicarbonate excretion.
• Increased excretion of sodium, potassium, and water → mild diuresis.
• Alkalinization of urine and mild metabolic acidosis due to bicarbonate loss.
• Reduced intraocular pressure (secondary effect; relevant in glaucoma).
Key pharmacologic effects in diuresis:
• Mild diuretic effect – less potent than loop or thiazide diuretics.
• Reduction of extracellular fluid volume.
• Limited natriuresis compared with other diuretics; primarily used in specific indications.
• Alters urinary pH – may affect drug excretion and electrolyte balance.
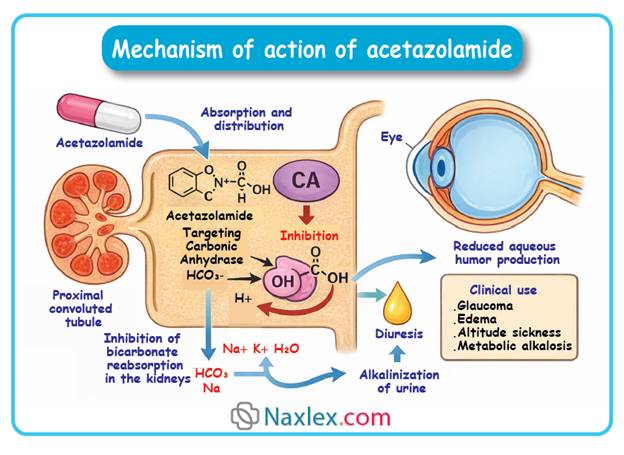
Clinical Significance:
Carbonic anhydrase inhibitors are primarily used when mild diuresis is needed or in combination therapy.
They are rarely used as first-line diuretics for chronic fluid overload because of limited efficacy.
Useful in conditions requiring urinary alkalinization, reduction of intraocular pressure, or metabolic alkalosis correction.
Indications (for diuretic use):
• Edema associated with mild fluid retention.
• Adjunct therapy in heart failure when other diuretics are insufficient.
• Prevention or treatment of metabolic alkalosis.
• Treatment of glaucoma-related fluid overload (secondary benefit).
Nursing relevance:
• Monitor fluid balance – intake/output, weight, and signs of dehydration.
• Assess electrolytes, particularly potassium and sodium, due to increased excretion.
• Observe for signs of metabolic acidosis.
Adverse Effects:
Common effects:
• Polyuria
• Fatigue or drowsiness
• Mild hypokalemia and sodium loss
Serious or rare effects:
• Metabolic acidosis – may exacerbate underlying conditions
• Severe electrolyte imbalance – especially with prolonged use or combination therapy
• Nephrolithiasis – due to alkaline urine promoting stone formation
Nursing Tip:
Encourage patients to maintain adequate fluid intake to reduce the risk of dehydration and kidney stones.
Contraindications / Precautions:
• Severe renal or hepatic impairment
• Pre-existing electrolyte imbalance
• Adrenocortical insufficiency
• Sulfonamide hypersensitivity
Drug Interactions:
• Digoxin – risk of toxicity increases with hypokalemia
• Other diuretics – additive electrolyte disturbances
• Amphetamines – urinary alkalinization may reduce excretion of some drugs
• Lithium – increased risk of lithium toxicity
Nursing Insight:
• Administer with food to reduce gastrointestinal upset.
• Monitor electrolytes closely during therapy.
• Educate patients on recognizing early signs of hypokalemia (muscle weakness, cramps, arrhythmias).
• Encourage adherence even if mild diuresis is not immediately noticeable.
• Adjust dosing based on renal function and patient response.
Rationale:
By inhibiting carbonic anhydrase, these drugs increase urinary excretion of bicarbonate, sodium, potassium, and water, providing mild diuresis. Electrolyte monitoring and patient education are critical to prevent complications.
Monitoring & Evaluation:
• Fluid balance – daily weights, intake/output
• Serum electrolytes – sodium, potassium, bicarbonate
• Renal function – serum creatinine, BUN
• Acid-base status – monitor for metabolic acidosis
• Clinical response – reduction in edema and improvement in fluid overload symptoms
Loop Diuretics
Examples:
Sulfonamide-type:
• furosemide (Lasix)
• bumetanide (Bumex)
• torsemide (Demadex)
Non-sulfonamide:
• ethacrynic acid (Edecrin)
Mechanism of Action & Drug Effects:
Loop diuretics act primarily on the thick ascending limb of the loop of Henle.
They inhibit the Na⁺-K⁺-2Cl⁻ symporter, preventing reabsorption of sodium, potassium, and chloride.
This results in:
• Profound diuresis – rapid and potent fluid removal.
• Increased urinary excretion of sodium, potassium, chloride, calcium, and magnesium.
• Reduction of extracellular fluid volume – effective in edema and volume overload.
• Decreased blood pressure secondary to volume depletion.
• Mild vasodilation – contributes to decreased preload and afterload in heart failure.
Key pharmacologic effects in diuresis:
• Rapid onset of action – especially when given IV.
• Highly efficacious even in renal impairment.
• Potent natriuresis – superior to thiazides for severe fluid overload.
Clinical Significance:
Loop diuretics are first-line agents for acute edema and severe fluid overload.
They are essential in conditions requiring rapid diuresis and in patients with impaired renal function, as they remain effective when GFR is low.
Indications (for diuretic use):
• Pulmonary edema – especially secondary to heart failure.
• Peripheral edema – due to chronic heart failure, nephrotic syndrome, or cirrhosis.
• Hypertension – primarily when fluid overload contributes.
• Hypercalcemia – enhances calcium excretion.
Nursing relevance:
• Monitor fluid balance – intake/output, daily weight, edema.
• Assess electrolytes – particularly potassium, sodium, magnesium, and calcium.
• Observe for hypotension due to rapid volume depletion.
Adverse Effects:
Common effects:
• Hypokalemia – may cause muscle weakness or arrhythmias
• Hyponatremia
• Hypomagnesemia
• Orthostatic hypotension
Serious or rare effects:
• Ototoxicity – usually with high IV doses or rapid administration
• Severe dehydration – especially in elderly or renal-impaired patients
• Electrolyte imbalance leading to arrhythmias or seizures
Nursing Tip:
Monitor electrolytes closely and encourage potassium-rich foods or supplementation when appropriate.
Contraindications / Precautions:
• Anuria – ineffective if urine output absent
• Severe electrolyte depletion – can exacerbate hypokalemia or hyponatremia
• Sulfa allergy – caution with sulfonamide-type loop diuretics
• Hepatic coma – risk of worsening encephalopathy due to electrolyte imbalance
Drug Interactions:
• Digoxin – increased risk of toxicity with hypokalemia
• Aminoglycosides – additive ototoxicity risk
• Lithium – altered renal clearance can increase toxicity
• Other diuretics – additive electrolyte disturbances
• NSAIDs – may reduce diuretic efficacy
Nursing Insight:
• Administer IV doses slowly to reduce ototoxicity risk.
• Educate patients on signs of electrolyte imbalance – muscle cramps, weakness, palpitations.
• Monitor daily weights and fluid status closely.
• Adjust doses based on renal function and response.
• Encourage adherence and explain the need for follow-up labs.
Rationale:
Loop diuretics inhibit the Na⁺-K⁺-2Cl⁻ symporter, producing potent diuresis and electrolyte excretion. Rapid fluid removal improves edema and pulmonary congestion, but monitoring is essential to prevent complications.
Monitoring & Evaluation:
• Fluid balance – daily weight, intake/output
• Serum electrolytes – sodium, potassium, magnesium, calcium
• Renal function – BUN, creatinine
• Blood pressure – monitor for hypotension
• Clinical assessment – edema reduction, pulmonary status, signs of dehydration or arrhythmia
Thiazide Diuretics
Examples:
• hydrochlorothiazide (Microzide)
• chlorthalidone (Hygroton)
• indapamide (Lozol)
• metolazone (Zaroxolyn)
Mechanism of Action & Drug Effects:
Thiazide diuretics act on the distal convoluted tubule of the nephron.
They inhibit the Na⁺-Cl⁻ symporter, reducing sodium and chloride reabsorption.
This leads to:
• Moderate diuresis – less potent than loop diuretics.
• Increased urinary excretion of sodium and water.
• Mild potassium and magnesium loss – can contribute to electrolyte imbalance.
• Reduction in peripheral vascular resistance – contributes to antihypertensive effects.
• Enhanced calcium reabsorption – useful in preventing kidney stones.
Key pharmacologic effects in diuresis:
• Effective for mild to moderate edema.
• Slower onset compared to loop diuretics – oral administration preferred.
• Often used in chronic management rather than acute fluid overload.
Clinical Significance:
Thiazides are first-line agents for mild edema, hypertension, and fluid retention associated with heart failure.
They are particularly beneficial in elderly patients and those with normal or mildly impaired renal function.
Indications (for diuretic use):
• Mild to moderate edema – due to heart failure, hepatic cirrhosis, or nephrotic syndrome.
• Hypertension – especially when volume expansion contributes.
• Prevention of calcium-containing kidney stones – enhances calcium reabsorption.
• Mild hypercalciuria – reduces urinary calcium excretion.
Nursing relevance:
• Monitor fluid balance – daily weights, intake/output.
• Assess electrolytes – potassium, sodium, magnesium, calcium.
• Evaluate blood pressure – risk of hypotension or dizziness.
Adverse Effects:
Common effects:
• Hypokalemia – may cause muscle weakness or arrhythmias
• Hyponatremia
• Hypomagnesemia
• Hypercalcemia – generally mild, may be beneficial in osteoporosis
• Dizziness, hypotension
Serious or rare effects:
• Hyperuricemia – may precipitate gout attacks
• Hyperglycemia – may affect diabetic patients
• Severe electrolyte imbalance – may lead to arrhythmias or neuromuscular symptoms
Nursing Tip:
Encourage potassium-rich diet or supplementation if hypokalemia occurs. Monitor for dehydration and hypotension.
Contraindications / Precautions:
• Anuria – ineffective if no urine output
• Severe renal impairment – reduced effectiveness
• Hypersensitivity to thiazides or sulfonamide allergy
• Electrolyte imbalances – may worsen hyponatremia or hypokalemia
• Pregnancy and lactation – use only if clearly indicated
Drug Interactions:
• Digoxin – hypokalemia increases risk of toxicity
• Lithium – altered renal clearance may increase toxicity
• NSAIDs – may reduce antihypertensive and diuretic effect
• Other antihypertensives – additive hypotensive effects
• Corticosteroids – may exacerbate potassium loss
Nursing Insight:
• Administer in the morning to reduce nocturia.
• Educate patients on electrolyte monitoring and dietary considerations.
• Encourage adherence and routine lab follow-up.
• Monitor weight and edema for therapeutic response.
• Observe for orthostatic hypotension in elderly patients.
Rationale:
Thiazide diuretics inhibit sodium-chloride reabsorption, producing moderate diuresis. They are effective for chronic edema and hypertension management, but require monitoring for electrolyte imbalances.
Monitoring & Evaluation:
• Fluid balance – intake/output, daily weight
• Electrolytes – sodium, potassium, magnesium, calcium
• Blood pressure – monitor response and hypotension
• Renal function – BUN, creatinine
• Clinical assessment – reduction in edema, signs of dehydration or electrolyte imbalance
Potassium-Sparing Diuretics
Examples:
• amiloride (Midamor)
• spironolactone (Aldactone)
• triamterene (Dyrenium)
Mechanism of Action & Drug Effects:
Potassium-sparing diuretics act in the distal convoluted tubule and collecting ducts of the nephron.
Two main mechanisms exist:
- Aldosterone antagonists – spironolactone blocks aldosterone receptors, reducing sodium reabsorption and potassium excretion.
- Sodium channel inhibitors – amiloride and triamterene directly inhibit epithelial sodium channels, preventing sodium uptake while conserving potassium.
Key pharmacologic effects include:
• Mild diuresis – weaker than thiazide or loop diuretics.
• Sodium excretion is increased, while potassium is retained.
• Reduction of edema – often adjunct therapy.
• Prevention of hypokalemia – useful in combination with potassium-losing diuretics.
Clinical Significance:
Potassium-sparing diuretics are important in preventing hypokalemia during chronic diuretic therapy.
They are less effective alone for significant fluid overload but valuable as adjunct therapy in heart failure, cirrhosis, or nephrotic syndrome.
Indications (for diuretic use):
• Edema associated with heart failure, hepatic cirrhosis, nephrotic syndrome.
• Adjunct therapy with loop or thiazide diuretics to prevent potassium loss.
• Hyperaldosteronism – spironolactone is used for primary or secondary forms.
• Hypertension – particularly when potassium conservation is desired.
Nursing relevance:
• Monitor electrolytes – especially potassium and sodium.
• Assess fluid balance – daily weights, intake/output.
• Observe for signs of hyperkalemia – muscle weakness, arrhythmias.
• Evaluate blood pressure response and edema reduction.
Adverse Effects:
Common effects:
• Hyperkalemia – risk increased when combined with ACE inhibitors or potassium supplements
• Dizziness or hypotension
• Nausea, vomiting, diarrhea
• Endocrine effects – gynecomastia, menstrual irregularities (spironolactone)
Serious or rare effects:
• Arrhythmias – due to severe hyperkalemia
• Nephrotoxicity – rare, particularly in renal impairment
• Stevens-Johnson syndrome – extremely rare
Nursing Tip:
Monitor potassium levels closely and educate patients to avoid high-potassium diets if hyperkalemia risk exists.
Contraindications / Precautions:
• Hyperkalemia – can worsen dangerous electrolyte imbalance
• Severe renal impairment – reduced excretion increases toxicity risk
• Hypersensitivity to specific drug
• Pregnancy and lactation – use only if benefits outweigh risks
• Concomitant use with ACE inhibitors, ARBs, or potassium supplements – caution required
Drug Interactions:
• ACE inhibitors / ARBs – increase hyperkalemia risk
• Potassium supplements – additive risk for hyperkalemia
• NSAIDs – may reduce diuretic efficacy
• Lithium – altered renal clearance may increase toxicity risk
• Other diuretics – combination often used for additive diuretic effect
Nursing Insight:
• Administer in the morning to avoid nocturia.
• Educate patients about dietary potassium and hyperkalemia signs.
• Monitor weight, blood pressure, and edema for therapeutic effect.
• Observe ECG for arrhythmias in at-risk patients.
• Encourage adherence and routine lab follow-up.
Rationale:
Potassium-sparing diuretics produce mild diuresis while conserving potassium. They are particularly useful to prevent hypokalemia during chronic diuretic therapy, but require careful monitoring of potassium to prevent hyperkalemia.
Monitoring & Evaluation:
• Electrolytes – potassium, sodium, magnesium
• Fluid balance – daily weight, intake/output
• Blood pressure – monitor for hypotension
• Renal function – BUN, creatinine
• Clinical assessment – edema reduction, hyperkalemia signs, adherence
Combination Diuretic Products
Examples:
• hydrochlorothiazide / triamterene (Dyazide, Maxzide)
• hydrochlorothiazide / amiloride (Moduretic)
• furosemide / spironolactone (various formulations)
Mechanism of Action & Drug Effects:
Combination diuretic products merge two different diuretic mechanisms to maximize fluid removal while minimizing electrolyte imbalance.
• Thiazide + potassium-sparing – thiazide promotes sodium and water excretion; potassium-sparing component prevents hypokalemia.
• Loop + potassium-sparing – loop diuretic produces strong diuresis; potassium-sparing agent mitigates potassium loss.
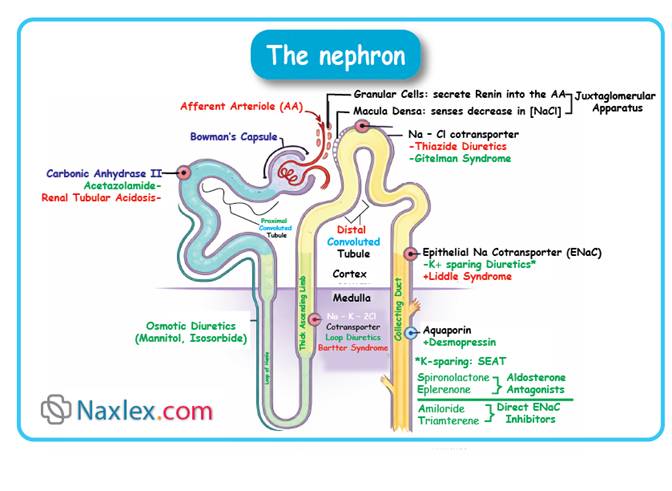
Key pharmacologic effects include:
• Enhanced diuresis compared to single-agent therapy.
• Sodium excretion is significantly increased.
• Potassium retention reduces risk of hypokalemia.
• Blood pressure reduction via volume depletion.
• Edema reduction in heart failure or renal disease.
Clinical Significance:
These products are useful when monotherapy diuretics are insufficient or when electrolyte balance must be maintained.
They are often prescribed in hypertension, heart failure, or chronic edema management.
Indications (for diuretic use):
• Hypertension – particularly in patients prone to hypokalemia.
• Edema associated with heart failure, liver cirrhosis, or nephrotic syndrome.
• Adjunct therapy – combination allows smaller doses of each diuretic to reduce side effects.
• Management of chronic fluid overload when single-agent therapy is inadequate.
Nursing relevance:
• Monitor electrolytes, especially potassium and sodium.
• Observe for fluid balance – intake/output, daily weights.
• Assess for hypotension or dizziness.
• Watch for signs of hyperkalemia or hyponatremia.
• Evaluate therapeutic effectiveness via edema reduction and blood pressure control.
Adverse Effects:
Common effects:
• Electrolyte imbalance – hyperkalemia or hyponatremia
• Dizziness or hypotension
• Nausea, vomiting, diarrhea
• Headache
Serious or rare effects:
• Cardiac arrhythmias – particularly with hyperkalemia or hypokalemia
• Severe dehydration – excessive fluid loss
• Renal impairment – especially in pre-existing kidney disease
Nursing Tip:
Combination therapy requires careful monitoring of electrolytes and fluid status to prevent complications.
Contraindications / Precautions:
• Hyperkalemia or existing severe electrolyte imbalance
• Severe renal impairment – may increase toxicity risk
• Hypersensitivity to any component
• Pregnancy and lactation – evaluate risk versus benefit
• Caution in elderly or patients on multiple antihypertensives
Drug Interactions:
• ACE inhibitors / ARBs – may increase potassium levels
• NSAIDs – can reduce diuretic effectiveness
• Other diuretics – additive effect increases dehydration risk
• Lithium – altered renal clearance may increase toxicity risk
• Digoxin – potassium imbalance may precipitate arrhythmias
Nursing Insight:
• Administer in the morning to prevent nocturia.
• Educate patients about signs of electrolyte imbalance – fatigue, muscle cramps, irregular heartbeat.
• Encourage adherence and routine laboratory follow-up.
• Monitor weight, blood pressure, and edema for therapeutic effect.
• Adjust doses carefully in patients with renal or hepatic impairment.
Rationale:
Combination diuretics provide synergistic diuresis while reducing potassium loss risk. Careful monitoring prevents electrolyte disturbances and optimizes fluid management, especially in chronic or severe edema.
Monitoring & Evaluation:
• Electrolytes – potassium, sodium, chloride, magnesium
• Fluid balance – daily weight, intake/output
• Blood pressure – evaluate for hypotension
• Renal function – BUN, creatinine
• Clinical assessment – edema reduction, signs of dehydration or electrolyte imbalance
• Patient adherence – understanding of combination therapy and monitoring importance
Summary
- Diuretics increase urine output by acting on specific nephron segments to promote sodium and water excretion.
- Reduce intravascular volume, lowering blood pressure, preload, and edema.
- Essential in cardiovascular, renal, and endocrine disorders.
Primary Purposes of Diuretic Therapy
- Reduce fluid overload: heart failure, renal disease, liver cirrhosis.
- Manage hypertension via decreased circulating blood volume.
- Reduce edema: peripheral, pulmonary, cerebral.
- Correct or prevent electrolyte imbalances.
- Reduce intraocular or intracranial pressure (select agents).
Sites of Action in the Nephron
- Proximal Convoluted Tubule (PCT): Carbonic anhydrase inhibitors
- Loop of Henle (Ascending Limb): Loop diuretics
- Distal Convoluted Tubule (DCT): Thiazide diuretics
- Collecting Duct: Potassium-sparing diuretics
- Site determines diuretic potency, electrolyte loss, and acid-base effects.
Major Classes of Diuretics
- Carbonic Anhydrase Inhibitors – Acetazolamide, Methazolamide
- Loop Diuretics – Furosemide, Bumetanide, Torsemide, Ethacrynic acid
- Thiazide and Thiazide-like Diuretics – Hydrochlorothiazide, Chlorthalidone, Metolazone
- Potassium-Sparing Diuretics – Spironolactone, Amiloride, Triamterene
- Combination Diuretic Products – fixed-dose combinations to improve efficacy and electrolyte balance
Therapeutic Uses
- Heart failure (acute/chronic), hypertension, pulmonary edema
- Chronic kidney disease, nephrotic syndrome, ascites
- Glaucoma, increased intracranial pressure
Carbonic Anhydrase Inhibitors
- Mechanism: inhibit carbonic anhydrase → ↓ bicarbonate reabsorption → mild diuresis.
- Effects: urine alkalinization, mild Na⁺/K⁺/water excretion, ↓ intraocular pressure.
- Clinical use: mild edema, adjunct therapy in heart failure, metabolic alkalosis, glaucoma.
- Nursing: monitor electrolytes, fluid balance, signs of acidosis.
- Adverse: polyuria, hypokalemia, metabolic acidosis, nephrolithiasis.
Loop Diuretics
- Mechanism: inhibit Na⁺-K⁺-2Cl⁻ symporter in loop of Henle → potent diuresis.
- Effects: ↑ excretion of Na⁺, K⁺, Cl⁻, Ca²⁺, Mg²⁺; ↓ blood pressure.
- Indications: acute edema, pulmonary edema, peripheral edema, hypercalcemia.
- Nursing: monitor fluid/electrolytes, weight, blood pressure; educate on hypokalemia signs.
- Adverse: hypokalemia, hyponatremia, hypotension, ototoxicity, dehydration.
Thiazide Diuretics
- Mechanism: inhibit Na⁺-Cl⁻ symporter in distal tubule → moderate diuresis.
- Effects: ↑ Na⁺/water excretion, mild K⁺/Mg²⁺ loss, enhanced Ca²⁺ reabsorption.
- Clinical: mild/moderate edema, hypertension, kidney stone prevention.
- Nursing: monitor BP, electrolytes, daily weight; administer in morning.
- Adverse: hypokalemia, hyponatremia, hypercalcemia, hyperuricemia, hyperglycemia.
Potassium-Sparing Diuretics
- Mechanisms:
- Aldosterone antagonists (spironolactone) block Na⁺ reabsorption, retain K⁺.
- Sodium channel blockers (amiloride, triamterene) conserve K⁺.
- Effects: mild diuresis, prevent hypokalemia.
- Indications: edema, hyperaldosteronism, adjunct with loop/thiazide diuretics.
- Nursing: monitor K⁺ closely, observe for hyperkalemia, educate patients.
- Adverse: hyperkalemia, hypotension, endocrine effects, arrhythmias.
Combination Diuretic Products
- Combine two mechanisms: thiazide + potassium-sparing or loop + potassium-sparing.
- Effects: enhanced diuresis, reduced risk of hypokalemia, BP reduction.
- Indications: hypertension prone to hypokalemia, heart failure, chronic fluid overload.
- Nursing: monitor electrolytes, fluid balance, BP, edema; educate on signs of imbalance.
- Adverse: electrolyte imbalance, hypotension, dehydration, arrhythmias.
Key Nursing & Monitoring Principles
- Daily weight, intake/output, edema assessment
- Electrolytes: Na⁺, K⁺, Mg²⁺, Ca²⁺
- Renal function: BUN, creatinine
- Blood pressure monitoring
- Patient education: diet, adherence, signs of hypokalemia/hyperkalemia, fluid status
