
Pain
Lessons
- Objectives
- Introduction to Pain Management
- Practice Exericise 1
- Pain Transmission (Nociception)
- Central Sensitization and Neuroplasticity
- Referred Pain
- Classification of pain
- Practice Exercise 2
- Pain assessment
- Management of pain
- Nursing and collaborative management
- Challenges to Effective Pain Management
- Ethical issues in pain management
- Managing pain in special populations
- Practice Exercise 3
- Summary
- Comprehensive questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Differentiate between the four neural mechanisms of pain: transduction, transmission, perception, and modulation.
- Compare and contrast the characteristics, causes, and treatment approaches for nociceptive (superficial somatic, deep somatic, and visceral) and neuropathic (central, peripheral, deafferentation, and sympathetically maintained) pain.
- Analyze subjective and objective data from a pain assessment to formulate a comprehensive understanding of a patient's pain experience.
- Formulate an interdisciplinary pain management plan that incorporates both pharmacological (nonopioid, opioid, adjuvant) and nonpharmacological (cutaneous stimulation, distraction, relaxation, imagery, acupuncture, environmental modifications, extremity elevation) interventions.
- Develop a teaching plan for patients and caregivers addressing effective self-management techniques, realistic pain control goals, potential side effects of therapies, and the importance of reporting unrelieved pain.
- Explain the differences between tolerance, physical dependence, pseudoaddiction, and addiction in the context of opioid therapy, and describe appropriate nursing responses to each.
- Discuss the ethical principles, including the rule of double effect, relevant to pain management, particularly concerning the fear of hastening death and the use of placebos.
- Adapt pain assessment and management strategies for special populations, specifically nonverbal patients and those with substance abuse problems.
Introduction to Pain Management
Effective pain management is a cornerstone of patient care, aiming to alleviate suffering and improve quality of life. This comprehensive overview explores the multifaceted nature of pain, from its underlying physiological mechanisms to its assessment, various management strategies, and the ethical considerations involved. It highlights the critical role of nurses within an interdisciplinary team, emphasizing patient-centered care and effective communication to overcome common challenges and misconceptions associated with pain.
McCaffery's and IASP Definitions
In 1968, Margo McCaffery, a nurse and pioneer in pain management, defined pain as:
“Whatever the person experiencing the pain says it is, existing whenever the person says it does.”
The International Association for the Study of Pain (IASP) defines pain as:
“An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”
These definitions highlight pain’s subjective nature, emphasizing that the client’s self-report is the most valid measure of pain. This becomes complex when caring for nonverbal patients (e.g., comatose individuals, infants, or those with dementia), where behavioral and physiological cues must guide assessment.
Pain is multidimensional, affecting the individual on multiple levels:
|
Dimension |
Description |
|
Physiologic |
Genetic, anatomical, and physical factors influence how noxious stimuli are recognized and processed. |
|
Affective |
Emotional responses such as fear, anger, anxiety, and depression can heighten pain perception and reduce quality of life. |
|
Cognitive |
Beliefs, memories, and attitudes shape a person’s understanding and reaction to pain. Catastrophizing (e.g., “My pain will never end”) worsens outcomes. |
|
Behavioral |
Observable expressions (e.g., grimacing, restlessness) may indicate pain; used especially in nonverbal clients. |
|
Sociocultural |
Culture, gender, and social support influence how pain is perceived, reported, and managed. Expectations, stigma, and family roles play a role. |
|
Men |
Women |
|
Less likely to report pain |
More frequent reports of chronic pain |
|
Report more control over pain |
More likely to experience migraine, IBS, fibromyalgia, arthritis |
|
Less likely to use alternative pain therapies |
Often under-medicated for chest/abdominal pain |
|
Greater pain tolerance |
Experience greater pain sensitivity even with same conditions |
Consequences of Unrelieved Acute Pain
|
System |
Potential Effects |
|
Endocrine/Metabolic |
↑ Cortisol, ACTH, catecholamines → hyperglycemia, catabolism, insulin resistance |
|
Cardiovascular |
↑ HR, ↑ BP, ↑ coagulability → angina, MI, DVT |
|
Respiratory |
↓ Tidal volume, ↓ cough → atelectasis, pneumonia |
|
Renal |
↓ Output, fluid retention → electrolyte imbalance |
|
GI |
↓ Motility → constipation, ileus, anorexia |
|
Musculoskeletal |
Muscle spasm, fatigue, immobility |
|
Neurologic |
Confusion, poor cognition |
|
Immune |
↓ Immunity → infection risk |
Pain Transmission (Nociception)
Nociception is the neurophysiological process by which tissue damage is detected and interpreted as pain by the nervous system. It involves four distinct phases: transduction, transmission, perception, and modulation
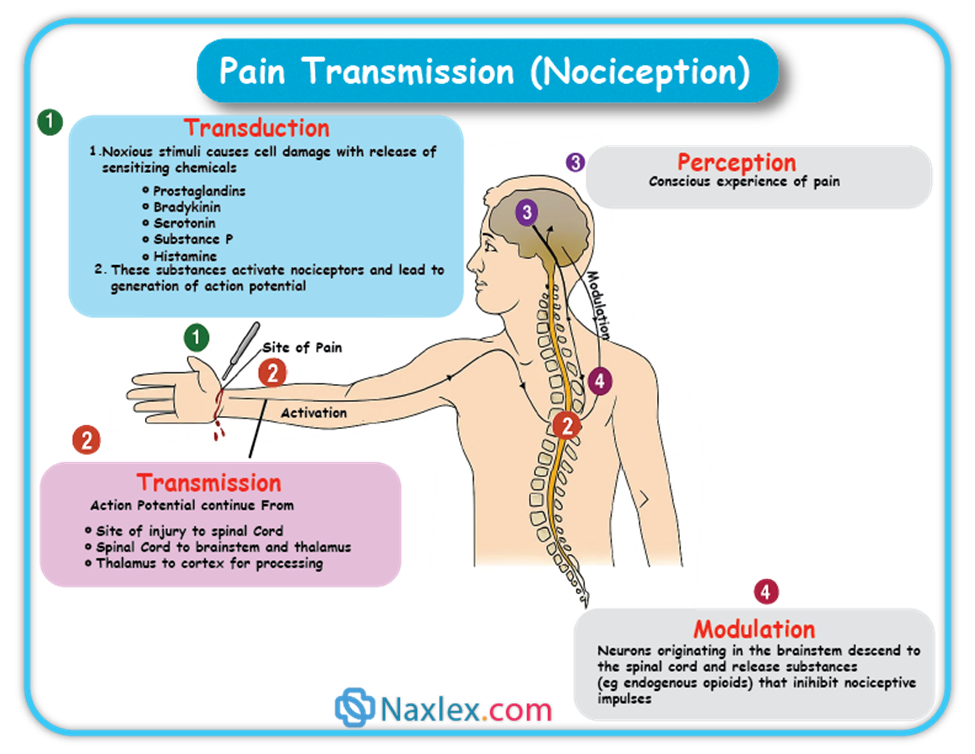
Transduction is the initial step where a noxious (tissue-damaging) stimulus is converted into an electrical signal, known as an action potential.
- What happens: When tissues are damaged by mechanical (e.g., surgical incision), thermal (e.g., sunburn), or chemical (e.g., toxic substances) stimuli, various chemicals are released into the injured area. These include:
- Hydrogen ions
- Substance P
- Adenosine triphosphate (ATP)
- Serotonin
- Histamine
- Bradykinin
- Prostaglandins
- Interleukins
- Tumor Necrosis Factor (TNF)
- Role of Nociceptors: These chemicals activate nociceptors, which are specialized receptors or free nerve endings. Once activated, nociceptors generate an action potential that travels to the spinal cord.
Transmission is the process of relaying these pain signals from the periphery (injury site) to the spinal cord and then to the brain.
- Peripheral Nerve Fibers: Pain impulses are carried by primary afferent fibers, specifically:
- A-delta fibers: Small, myelinated fibers that conduct pain rapidly, responsible for initial, sharp pain.
- C fibers: Small, unmyelinated fibers that transmit pain more slowly, producing a dull, aching, or throbbing sensation.
- These fibers extend directly from the injury site to the dorsal horn of the spinal cord without synapsing.
- Dorsal Horn Processing: Upon reaching the dorsal horn of the spinal cord, the nociceptive signal is processed.
- Neurotransmitters: Released from afferent fibers, these bind to receptors on nearby cells. Some (e.g., glutamate, aspartate, substance P) activate cells, while others (e.g., GABA, serotonin, norepinephrine) inhibit activation.
- Opioid Involvement: Both exogenous (e.g., morphine) and endogenous (e.g., enkephalin, β-endorphin) opioids bind to opioid receptors in this area, blocking neurotransmitter release (especially substance P) and producing analgesic effects.
- Transmission to Thalamus and Cortex: From the dorsal horn, the signal is communicated to third-order neurons, primarily in the thalamus, and then to various regions of the cerebral cortex where pain is perceived. Pathways involved include the spinothalamic and spinoreticular tracts.
- Therapeutic Interventions: Medications like opioid analgesics and baclofen work by affecting transmission in these pathways.
- Dermatomes: The way nerve fibers enter the spinal cord relates to dermatomes, which are specific areas of skin innervated by a single spinal cord segment. This explains patterns of pain or rashes (e.g., shingles).
Perception is when the individual becomes consciously aware of pain, recognizing it, defining it, and assigning it meaning.
- Brain Structures: There isn't one specific pain center; instead, several brain structures are involved:
- Reticular Activating System (RAS): Warns the individual to attend to the pain.
- Somatosensory System: Responsible for localizing and characterizing the pain.
- Limbic System: Involved in emotional and behavioral responses to pain.
- Cortical Structures: Crucial for constructing the meaning of the pain.
- Impact of Perception: Understanding this allows for effective pain management strategies like distraction and relaxation, which can reduce the sensory and emotional components of pain. Opioids, antiseizure drugs, and antidepressants also modify pain perception.
Modulation involves the activation of descending pathways from the brain that can either inhibit or facilitate the transmission of pain signals.
- Mechanism: These descending fibers release chemicals such as serotonin, norepinephrine, GABA, and endogenous opioids, which can inhibit pain transmission at various levels (periphery, spinal cord, brainstem, cerebral cortex).
- Therapeutic Interventions: Antidepressants like tricyclic antidepressants and SNRIs interfere with the reuptake of serotonin and norepinephrine, increasing their availability to inhibit noxious stimuli, making them useful in chronic pain management.
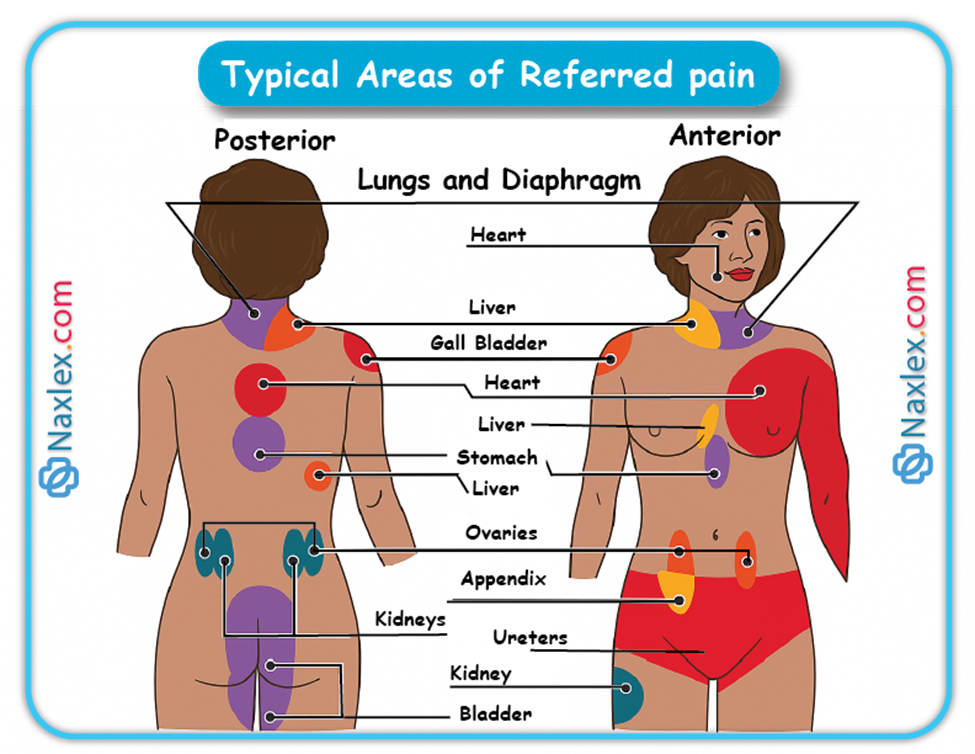
Referred Pain
Referred pain is pain perceived at a location distant from the actual site of the painful stimulus. This is important to consider when evaluating pain, especially concerning visceral organs, as misinterpreting its location can lead to incorrect diagnoses and treatments. For example, liver pain might be felt in the neck or flank, not just the abdomen.
Typical Areas of Referred pain
Classification of pain
Pain can be categorized in several ways. Most commonly, pain is categorized as nociceptive or neuropathic based on underlying pathology. Another useful scheme is to classify pain as acute or chronic.
Classification by Underlying Pathology
This classification focuses on how the pain signals are generated and processed in the nervous system.
Definition: This type of pain results from the normal processing of stimuli that damage normal tissue, or have the potential to do so if prolonged. It's essentially the body's warning system for actual or potential tissue injury.
Treatment: Generally responds well to both non-opioid and opioid medications.
Types of Nociceptive Pain:
- Superficial Somatic Pain:
- Origin: Skin, mucous membranes, and subcutaneous tissue.
- Characteristics: Tends to be well-localized, often described as sharp, burning, or prickly.
- Examples: Sunburn, skin contusions.
- Deep Somatic Pain:
- Origin: Muscles, fasciae, bones, and tendons.
- Characteristics: Can be localized or diffuse and radiating, often described as deep, aching, or throbbing.
- Examples: Arthritis, tendonitis, myofascial pain.
- Visceral Pain:
- Origin: Internal organs (e.g., GI tract, bladder) and the lining of body cavities.
- Characteristics: Can be well or poorly localized, often referred to cutaneous (skin) sites. It responds to inflammation, stretching (like from a tumor or obstruction causing distention), and ischemia, producing intense cramping pain.
- Examples: Appendicitis, pancreatitis, cancer affecting internal organs, irritable bowel syndrome, surgical incision pain.
Definition: This pain arises from abnormal processing of sensory input by either the peripheral or central nervous system due to damage to nerves or CNS structures.
Treatment: Often not well-controlled by opioid analgesics alone. Treatment typically involves a multimodal approach including adjuvant analgesics like tricyclic antidepressants, SNRIs, antiseizure drugs (e.g., gabapentin, pregabalin), transdermal lidocaine, α2-adrenergic agonists, and sometimes NMDA receptor antagonists like ketamine.
Characteristics: It's frequently described as numbing, hot, burning, shooting, stabbing, sharp, or electric shock-like. It can be sudden, intense, short-lived, or lingering, often with paroxysmal (sudden, intense) firing of injured nerves. Patients might also experience numbness, allodynia (pain from non-painful stimuli), or changes in reflexes and motor strength. No single symptom is diagnostic.
Common Causes: Trauma, inflammation (e.g., from a herniated disc), metabolic diseases (e.g., diabetes mellitus), alcoholism, nervous system infections (e.g., herpes zoster, HIV), tumors, toxins, and neurological diseases (e.g., multiple sclerosis).
Types of Neuropathic Pain:
- Central Pain:
- Cause: Primary lesion or dysfunction in the central nervous system (CNS).
- Examples: Post-stroke pain, pain associated with multiple sclerosis.
- Peripheral Neuropathies:
- Cause: Damage to one or many peripheral nerves.
- Examples: Diabetic neuropathy, alcohol-nutritional neuropathy, trigeminal neuralgia, postherpetic neuralgia.
- Deafferentation Pain:
- Cause: Results from a loss of afferent (incoming) input due to peripheral nerve injury (e.g., amputation) or CNS damage (e.g., spinal cord injury).
- Examples: Phantom limb pain, post-mastectomy pain, spinal cord injury pain.
- Sympathetically Maintained Pain:
- Cause: Pain that persists due to dysregulation of the sympathetic nervous system activity.
- Examples: Phantom limb pain, complex regional pain syndrome (CRPS).
- Complex Regional Pain Syndrome (CRPS): A particularly debilitating type of neuropathic pain with dramatic changes in skin color and temperature, intense burning pain, skin sensitivity, sweating, and swelling.
- CRPS Type I: Often triggered by tissue injury, surgery, or a vascular event.
- CRPS Type II: Includes all features of Type I plus a peripheral nerve lesion.
- Complex Regional Pain Syndrome (CRPS): A particularly debilitating type of neuropathic pain with dramatic changes in skin color and temperature, intense burning pain, skin sensitivity, sweating, and swelling.
This classification helps differentiate between pain that is temporary and pain that has become a persistent condition.
Onset: Sudden.
Duration: Typically less than 3 months, or for as long as it takes for normal healing to occur.
Severity: Can range from mild to severe.
Cause: Usually a clearly identifiable precipitating event (e.g., illness, surgery, trauma, infection, acute ischemia).
Course: Generally decreases over time and resolves as recovery occurs.
Typical Manifestations: Often reflects sympathetic nervous system activation, such as increased heart rate, respiratory rate, and blood pressure; diaphoresis (sweating), pallor, anxiety, agitation, confusion, and urine retention.
Goals of Treatment: Pain control with eventual elimination, and treatment of the underlying cause (e.g., splinting a fracture, antibiotics for an infection).
Note: Acute pain that persists can lead to disabling chronic pain states through processes like central sensitization and neuroplasticity. Aggressive and effective treatment of acute pain is crucial to prevent the development of chronic pain.
Chronic Pain (Persistent Pain)
Onset: Can be gradual or sudden.
Duration: Lasts for longer periods, often defined as more than 3 months, or beyond the expected healing time for an acute injury.
Severity: Can range from mild to severe.
Cause: May not be known. The original cause of the pain might differ from the mechanisms that maintain the pain over time.
Course: Typically, the pain does not go away. It is characterized by periods of increasing and decreasing intensity.
Typical Manifestations: Predominantly behavioral manifestations, such as a flat affect, decreased physical activity, fatigue, and withdrawal from social interaction. Unlike acute pain, chronic pain does not appear to have an adaptive warning role.
Goals of Treatment: Pain control to the extent possible, with a primary focus on enhancing function and improving quality of life.
Pain assessment
Pain assessment is a crucial and often underestimated component of effective pain management. It involves a systematic approach to understanding a patient's pain experience to guide appropriate interventions.
Core Principles of Pain Assessment
Effective pain assessment is guided by fundamental principles:
- Patient's Right to Assessment and Management: All patients should be regularly screened for pain, and when present, a thorough assessment should be conducted.
- Pain is Subjective: The patient's self-report is the most reliable indicator of pain. Healthcare providers should accept and respect this report unless there are clear reasons for doubt.
- Physiological and Behavioral Signs are Not Reliable Alone: Objective signs like tachycardia or grimacing are not specific or reliable indicators of pain on their own. Do not rely primarily on these unless the patient cannot self-report.
- Pain is a Sensory and Emotional Experience: Assessment must address both the physical and psychological aspects of pain.
- Assessment Approaches Must Be Appropriate: Tools and methods should be tailored to the patient population, especially for those with communication difficulties. Involving family members is often appropriate.
- Pain Can Exist Without a Physical Cause: Do not attribute pain solely to psychological causes if a physical origin cannot be found.
- Individual Pain Response Varies: A uniform pain threshold does not exist; different patients experience different levels of pain from comparable stimuli.
- Chronic Pain Can Increase Sensitivity: Patients with chronic pain may be more sensitive to pain and other stimuli. Pain tolerance varies significantly among individuals due to factors like heredity, energy levels, coping skills, and prior experiences.
- Unrelieved Pain Has Adverse Consequences: Untreated acute pain can lead to physiological changes that increase the likelihood of developing persistent (chronic) pain. Patients should be encouraged to report pain, especially if they are reluctant or deny it.
Goals of a Nursing Pain Assessment
- Describe the Patient's Pain Experience: To identify and implement appropriate pain management techniques.
- Identify Patient's Goals and Resources: To establish goals for therapy and determine resources for self-management.
Elements of a Pain Assessment
A comprehensive pain assessment involves direct interview, observation, and complementary diagnostic and physical examination findings. The assessment should always be multidimensional, adapting to the clinical setting and patient.
Important Note: Patients may use words other than "pain" (e.g., "soreness," "aching"). Document their specific terms and consistently use those when asking about their pain.
Subjective Data
1. Pain Pattern:
- Onset:
- Acute Pain: Patients usually know precisely when it started (e.g., from injury, acute illness, surgery).
- Chronic Pain: Patients may have difficulty pinpointing the exact start time.
- Duration: How long the pain has lasted helps determine if it's acute or chronic and can guide diagnostic workups (e.g., new severe back pain in a cancer patient with chronic back pain could indicate new metastatic disease).
- Course:
- Constant (Around-the-clock) Pain: Pain is present all the time.
- Intermittent Pain: Periods of pain interspersed with pain-free periods.
- Breakthrough Pain (BTP): Transient, moderate to severe pain that occurs in patients whose baseline persistent pain is otherwise well-controlled. It can be predictable or unpredictable, typically peaking in 3-5 minutes and lasting up to 30 minutes or longer. Specific transmucosal fentanyl products are used for BTP.
- End-of-Dose Failure: Pain that occurs before the expected duration of a specific analgesic (e.g., increased pain after 48 hours on a 72-hour fentanyl patch). This indicates a need for dose or schedule adjustments, not BTP.
- Episodic, Procedural, or Incident Pain: A transient increase in pain triggered by a specific activity or event (e.g., dressing changes, movement, catheterization).
2. Location:
- Identifying the exact or general location(s) of pain is crucial for identifying causes and guiding treatment.
- Patients may describe specific sites, point to areas on their body, or mark areas on a pain map.
- Referred Pain: Pain perceived distant from its origin (e.g., myocardial infarction causing left shoulder pain). (Refer to FIG. 9-2).
- Radiating Pain: Pain that spreads from its origin to another site (e.g., angina pectoris radiating from the chest to the jaw or left arm; sciatica radiating down the leg).
- Document all pain locations, as many patients have multiple sites of pain.
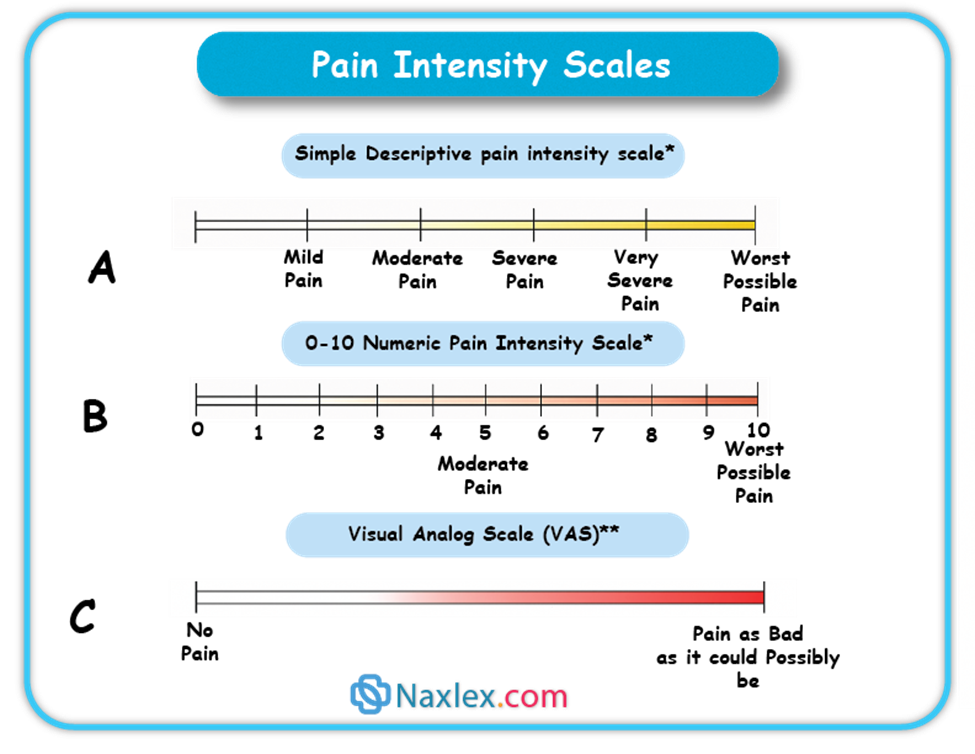
3. Intensity (Severity):
- A reliable measure for determining treatment type and effectiveness.
- Pain Scales: Help patients communicate intensity. Choice of scale should be based on developmental needs and cognitive status.
- Numeric Scales: 0 = no pain, 10 = worst pain.
- Verbal Descriptor Scales: None, a little, moderate, severe.
- Visual Scales: Pain Thermometer Scale (FIG. 9-3), Wong-Baker FACES Pain Rating Scale, FACES Pain Scale–Revised (useful for patients with cognitive or language barriers).
- Important Caution: Do not dose opioids solely based on reported pain scores. Balance pain relief with sedation level and respiratory status to ensure safe practice and minimize adverse events.
4. Quality:
- Refers to the nature or characteristics of the pain.
- Neuropathic Pain Descriptors: Burning, numbing, shooting, stabbing, electric shock-like, itchy.
- Nociceptive Pain Descriptors: Sharp, aching, throbbing, dull, cramping.
- These descriptors help classify the pain (e.g., neuropathic, nociceptive, visceral) and guide appropriate treatment options based on the underlying pain mechanism.
5. Associated Symptoms:
- Ask about symptoms that may exacerbate or be exacerbated by pain, such as anxiety, fatigue, and depression.
- Inquire about activities and situations that increase or alleviate pain (e.g., movement affecting musculoskeletal pain, resting decreasing pain). This helps characterize the pain and inform treatment choices.
6. Management Strategies:
- Ask patients what methods they are currently using to control pain, what they've used previously, and their outcomes.
- Include prescription and nonprescription drugs, and non-drug therapies (e.g., hot/cold applications, complementary therapies like acupuncture, relaxation techniques).
- Document both effective and ineffective strategies.
7. Impact of Pain:
- Assess how pain influences the patient's quality of life and functioning:
- Ability to sleep, enjoy life, interact with others.
- Performance of work and household duties.
- Engagement in physical and social activities.
- Impact on mood and emotional well-being.
8. Patient's Beliefs, Expectations, and Goals:
- Assess attitudes and beliefs that might hinder effective treatment (e.g., fear of opioid addiction).
- Ask about the patient's expectations and goals for pain management.
- In acute care settings, a more abbreviated assessment should still include effects on sleep, daily activities, relationships, physical activity, emotional well-being, pain descriptors, and coping strategies.
Objective Data
- Physical Examination: Includes evaluation of functional limitations.
- Psychosocial Evaluation: Includes assessment of mood.
- Diagnostic Studies: Complete the initial assessment.
Documentation
- Thorough documentation of the pain assessment is critical for effective communication among healthcare team members.
- Many facilities use specific tools for initial pain assessment, treatment, and reassessment.
- Examples of multidimensional pain assessment tools include the Brief Pain Inventory, McGill Pain Questionnaire, Memorial Pain Assessment Card, and Neuropathic Pain Scale.
Reassessment
- Critical Step: Pain must be reassessed at appropriate intervals to evaluate the effectiveness of interventions.
- Frequency and Scope: Guided by factors such as:
- Pain severity.
- Physical and psychosocial condition.
- Type of intervention and risk of adverse effects.
- Institutional policy.
- Examples: Postoperative patients should be reassessed within 30 minutes of an IV analgesic dose. Residents in long-term care with chronic pain are reassessed at least quarterly or with a change in condition or functional status.
NURSING INSIGHT:
The Subjectivity and Multidimensionality of Pain as a Core Principle in Management: A recurring insight across pain assessment, management, and ethical considerations is that pain is fundamentally subjective. The patient's self-report is highlighted as the "gold standard," and nurses are explicitly told to "accept and respect this self-report unless there are clear reasons for doubt." This subjectivity necessitates a multidimensional assessment (pattern, location, intensity, quality, associated symptoms, impact, management strategies) and forms the basis for collaborative treatment planning where the plan "should ensure that pain will be treated based on the patient’s perception and report of pain." This core understanding then informs communication strategies (patients need to feel believed), ethical justifications (intent in the rule of double effect focuses on pain relief), and adaptations for special populations (behavioral cues become proxy for self-report in nonverbal patients).
Management of pain
Pain management involves a combination of nonpharmacological and pharmacological approaches, tailored to the individual patient's needs and the nature of their pain (acute vs. chronic, mild vs. severe).
I. Nonpharmacological Pain Management
These strategies aim to reduce pain without medication, often by influencing pain pathways, distracting from pain, or promoting relaxation.
- Cutaneous (Skin) Stimulation:
- Transcutaneous Electrical Nerve Stimulation (TENS): Delivers mild electrical impulses through electrodes on the skin to interrupt pain pathways.
- Heat Application: Increases blood flow to the area, which can reduce stiffness and promote healing.
- Cold Application: Reduces inflammation and swelling, often used for acute injuries.
- Therapeutic Touch: Involves gentle contact or near-body passes, believed to facilitate relaxation and pain relief.
- Massage: Reduces muscle tension, improves circulation, and promotes relaxation.
- Distraction:
- Diverts the patient's attention away from the pain sensation.
- Includes activities like: ambulation, deep breathing exercises, engaging with visitors, watching television, listening to music.
- Relaxation Techniques:
- Aims to reduce muscle tension and promote a sense of calm, thereby decreasing pain perception.
- Includes: meditation, yoga, progressive muscle relaxation.
- Imagery:
- Involves focusing on a pleasant thought or mental image to divert attention from pain.
- Requires the patient's ability to concentrate.
- Acupuncture:
- Involves inserting tiny needles into specific points on the skin and subcutaneous tissues.
- These needles may be vibrated or stimulated electrically. The mechanism is believed to involve the release of endorphins and modulation of pain signals.
- Reduction of Pain Stimuli in the Environment:
- Minimizing environmental factors that can exacerbate pain, such as loud noises, bright lights, or uncomfortable temperatures.
- Elevation of Edematous Extremities:
- Raising swollen limbs to promote venous return, which helps decrease swelling and can reduce pain associated with pressure.
II. Pharmacological Interventions
Analgesics are the primary medications used for pain relief and are classified into three main categories: nonopioids, opioids, and adjuvants.
WHO Analgesic Ladder
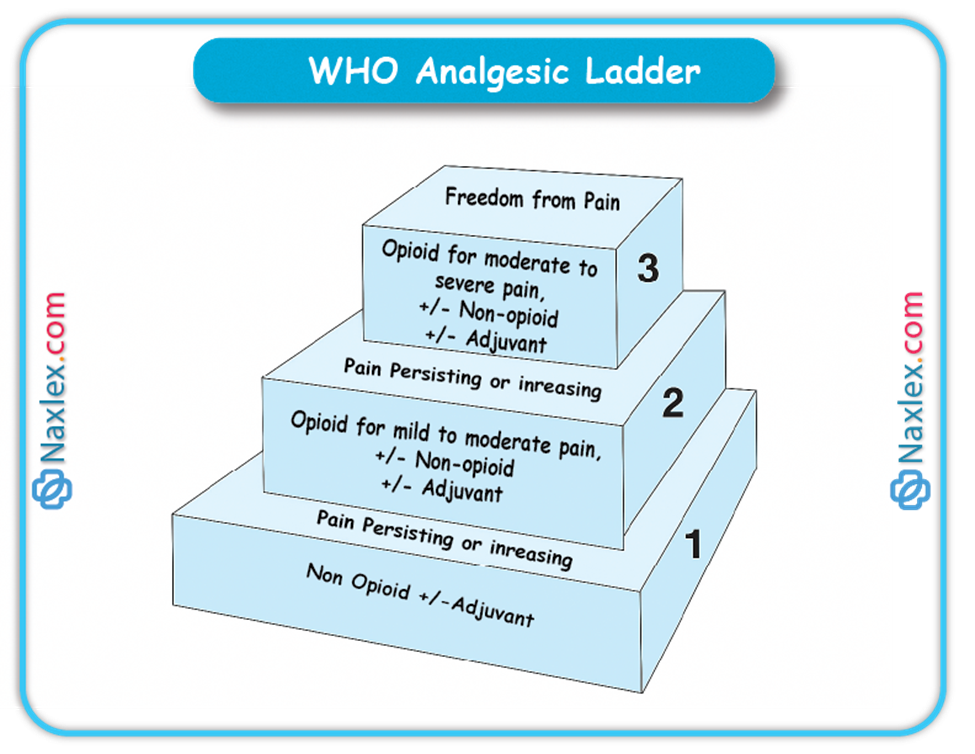
A. Nonopioid Analgesics
- Examples: Acetaminophen, Nonsteroidal Anti-inflammatory Drugs (NSAIDs) including salicylates (e.g., aspirin).
- Appropriate for: Mild to moderate pain.
- Key Considerations:
- Acetaminophen:
- Hepatotoxicity: Be aware of potential liver damage.
- Dosage Limit: Healthy adults should not exceed 4 g/day.
- Combination Products: Be mindful of opioids that also contain acetaminophen (e.g., hydrocodone/acetaminophen combinations like Vicodin) to avoid exceeding the daily limit.
- NSAIDs/Salicylates:
- Salicylism (with salicylates): Monitor for symptoms like tinnitus (ringing in ears), vertigo, and decreased hearing acuity.
- Gastric Upset: Administer with food or antacids to prevent stomach irritation.
- Bleeding Risk: Monitor for signs of bleeding with long-term NSAID use.
- Acetaminophen:
B. Opioid Analgesics
- Examples: Morphine sulfate, fentanyl (Sublimaze), codeine, hydromorphone (Dilaudid).
- Appropriate for: Moderate to severe pain (e.g., postoperative pain, myocardial infarction pain, cancer pain).
- Key Administration Principles:
- Acute Severe Pain: For immediate, short-term relief, around-the-clock parenteral (IV/IM) administration is often preferable to PRN dosing for consistent control in the initial 24-48 hours.
- Chronic Pain: The oral route is generally preferred for chronic, non-fluctuating pain due to convenience and sustained effect.
- Consistent Dosing: Regular, consistent timing and dosing ensure steady pain control.
- Essential Monitoring and Intervention for Adverse Effects:
- Constipation: This is a very common side effect. Employ a preventative approach:
- Monitor bowel movements.
- Encourage increased fluid and fiber intake.
- Administer stool softeners and/or stimulant laxatives.
- Consider enemas if necessary.
- Orthostatic Hypotension:
- Advise patients to sit or lie down if feeling light-headed or dizzy.
- Instruct slow position changes (lying to sitting to standing).
- Provide assistance with ambulation to prevent falls.
- Urinary Retention:
- Monitor intake and output (I&O).
- Assess for bladder distention.
- Administer bethanechol (Urecholine) if prescribed.
- Catheterization may be necessary in severe cases.
- Nausea/Vomiting:
- Administer antiemetics (anti-nausea medications).
- Advise patients to lie still and move slowly.
- Eliminate strong odors.
- Sedation:
- Monitor level of consciousness.
- Implement safety precautions (e.g., bed alarms, assist with ambulation).
- Warning Sign: Sedation often precedes respiratory depression.
- Respiratory Depression:
- Monitor Respiratory Rate: Check respiratory rate before and after opioid administration, especially in opioid-naïve patients.
- Initial Treatment: Generally, a reduction in opioid dose.
- Reversal: If necessary, slowly administer diluted naloxone (Narcan) to reverse opioid effects.
- Constipation: This is a very common side effect. Employ a preventative approach:
C. Adjuvant Analgesics
- Purpose: These medications enhance the effects of nonopioids, alleviate symptoms that worsen pain (e.g., depression, seizures, inflammation), and are particularly useful for treating neuropathic pain.
- Examples of Adjuvant Medications:
- Anticonvulsants: Carbamazepine (Tegretol) - often used for neuropathic pain.
- Antianxiety Agents: Diazepam (Valium).
- Tricyclic Antidepressants: Amitriptyline (Elavil) - also used for neuropathic pain.
- Antihistamine: Hydroxyzine (Vistaril) - can have sedative and anxiolytic effects.
- Glucocorticoids: Dexamethasone (Decadron) - potent anti-inflammatory.
- Antiemetics: Ondansetron (Zofran) - used to manage opioid-induced nausea/vomiting.
D. Patient-Controlled Analgesia (PCA)
- Mechanism: A medication delivery system allowing patients to self-administer safe, pre-programmed doses of opioids.
- Benefits:
- Consistent Plasma Levels: Small, frequent dosing maintains steady drug levels.
- Increased Control: Patients have less lag time between feeling pain and receiving medication, enhancing their sense of control.
- Potentially Less Medication: Increased control may reduce the overall amount of medication needed.
- Typical Opioids: Morphine and hydromorphone (Dilaudid).
- Patient Education:
- Patients should inform the nurse if the pump is not adequately controlling their pain.
- Safety Rule: Only the patient should push the PCA button to prevent accidental overdose.
III. General Strategies for Effective Pain Management
- Proactive Approach: Administer analgesics before pain becomes severe. It takes less medication to prevent pain than to treat established severe pain.
- Timely Reporting: Instruct patients to report developing or recurrent pain promptly, rather than waiting for it to become severe, especially for PRN pain medication.
- Address Misconceptions: Educate patients about common misconceptions regarding pain and pain medication.
- Reduce Fear and Anxiety: Help patients alleviate fear and anxiety, which can worsen pain perception.
- Holistic Treatment Plan: Create a comprehensive plan that integrates both nonpharmacological and pharmacological pain-relief measures.
Strategies Specific for Relieving Chronic Pain
In addition to the general strategies, chronic pain management often involves:
- Long-Acting Opioids: Administering long-acting or controlled-release opioid analgesics, including transdermal patches (e.g., fentanyl patches).
- Around-the-Clock Dosing: Administering analgesics on a regular, around-the-clock schedule instead of a PRN (as needed) basis to maintain consistent pain control.
Nursing and collaborative management
Nurses are vital members of the interdisciplinary pain management team, playing a multifaceted role in ensuring patients receive effective care. This involves not only direct care but also strong communication, education, and advocacy.
Nursing and Collaborative Pain Management
As a nurse, your contribution to pain management is comprehensive. You'll actively participate in the assessment and reassessment of pain, ensuring its characteristics, intensity, and impact are thoroughly understood. You're also key in planning and implementing treatments, which includes educating patients and families, advocating for their needs, and providing crucial support. Since pain can affect anyone in any healthcare setting, it's essential to stay informed about current therapies and be open to trying new approaches.
Collaborating with the patient, you should help develop a written pain management plan. This plan should be based on the patient's perception and report of pain. It should also clearly outline any gradual tapering of analgesic doses, especially for opioids, with a focus on transitioning from parenteral (injectable) to long-acting oral preparations, and ultimately, if appropriate, the cessation of opioids.
While nursing roles like assessing pain, administering treatment, and monitoring for side effects are fundamental, their success hinges on your ability to build a trusting relationship with the patient and their caregiver. Addressing their concerns about pain and its treatment is paramount.
Effective Communication in Pain Management
Because pain is a deeply subjective experience, patients need to feel confident that their pain reports will be believed and not dismissed as "complaining." It's crucial for both the patient and their caregiver to know that you acknowledge their pain's significance and understand how profoundly it can disrupt a person's life.
Communicate genuine concern and commit to helping the patient achieve pain relief and cope with any unrelieved pain. This might involve a period of trial and error to find the most effective therapeutic plan, and your support during this time is invaluable. It's also important to clarify everyone's roles in pain relief, helping the patient understand what to expect from the healthcare team and their own responsibilities. Beyond specific assessment and treatment, always evaluate the overall impact of pain on the lives of both the patient and their caregiver.
Challenges to Effective Pain Management
Several common misunderstandings about pain medications can create barriers to effective pain management. It's important for you to understand and clearly explain these concepts to patients and caregivers.
- Tolerance
- What it is: A normal physiological response to chronic drug exposure, where a person needs an increased opioid dose to maintain the same degree of analgesia. While side effects (except constipation) often develop tolerance more predictably, the need for increased doses might also indicate disease progression.
- Nursing Action: Always assess for other causes of increased pain, like disease progression or infection. If significant tolerance develops, or side effects become intolerable, opioid rotation (switching to a different opioid) can be considered, as a new opioid might be more effective at lower, equianalgesic doses. Be aware that very high opioid doses can sometimes cause opioid-induced hyperalgesia, paradoxically increasing pain.
- Physical Dependence
- What it is: A normal physiological response to ongoing drug exposure, resulting in a withdrawal syndrome if the drug is suddenly stopped or significantly reduced.
- Symptoms of Opioid Withdrawal:
- Early (6-12 hours): Anxiety, tearing (lacrimation), runny nose (rhinorrhea), sweating (diaphoresis), yawning, goosebumps (piloerection), shaking, chills.
- Late (48-72 hours): Excitation, diarrhea, dilated pupils, anorexia, tremor, restlessness, fever, nausea and vomiting, abdominal cramping pain, hypertension, tachycardia, insomnia.
- Nursing Action: When opioids are no longer needed, use a tapering schedule with careful monitoring to avoid withdrawal symptoms. For example, a common tapering approach involves reducing the daily dose incrementally every two days until discontinuation.
- Pseudoaddiction
- What it is: Occurs when pain is inadequately treated. Patients may exhibit behaviors commonly associated with addiction (like frequent requests for refills or higher doses), but these behaviors resolve once their pain is adequately managed.
- Risk: These patients are often mislabeled as "drug-seeking," leading to mistrust.
- Prevention: Effective communication and optimal pain management can prevent this.
- Addiction
- What it is: A complex neurobiologic condition characterized by compulsive drug use, loss of control over use, and continued use despite harm. It is not indicated by tolerance or physical dependence, which are normal physiological responses.
- Prevalence: Addiction rarely occurs in patients receiving opioids for pain control.
- Nursing Action: If addiction is suspected, it requires careful investigation and diagnosis; do not imply it without evidence, as this can severely hinder pain management.
- Hallmarks:
- Compulsive use.
- Loss of control of use.
- Continued use despite risk of harm.
- Important Note: While factors like younger age or a history of substance abuse can increase risk, the potential for addiction should not prevent healthcare providers from effectively treating moderate to severe acute and chronic pain with opioids when appropriate.
Overcoming Barriers Through Patient & Caregiver Teaching
Many other barriers can hinder effective pain management. Your role in educating patients and caregivers is crucial to address these concerns:
- Fear of addiction: Explain that addiction is uncommon when opioids are used for pain.
- Fear of tolerance: Teach that tolerance is a normal response, dosages can be increased if needed, and tolerance to side effects (except constipation) develops slowly.
- Concern about side effects: Provide methods for prevention and treatment, and reassure that many side effects decrease over time or can be managed with different medications.
- Fear of injections: Emphasize that oral medications are preferred, and other non-injection routes (transdermal, indwelling parenteral) are available if oral isn't feasible.
- Desire to be a "good" patient or stoic: Explain that open communication about pain is essential for effective care, and that not reporting pain leads to undertreatment.
- Forgetting to take analgesic: Offer practical solutions like pill organizers and record-keeping, and encourage caregiver involvement.
- Concern that pain indicates disease progression: Explain that increased pain can be due to tolerance or new, non-life-threatening issues, and provide psychological support and accurate information about their condition.
- Sense of fatalism: Reassure patients that pain can be managed for most, therapies often require trial and error, and side effects are manageable.
- Ineffective medication: Explain that there are multiple options within each drug category, and finding the best regimen often requires trying different approaches, including non-drug therapies.
Ethical issues in pain management
When managing pain, healthcare professionals often encounter complex ethical considerations that require careful thought and adherence to professional guidelines.
I. Ethical Issues in Pain Management
A. Fear of Hastening Death by Administering Analgesics
A significant concern for healthcare professionals and caregivers is the apprehension that providing sufficient pain medication, especially opioids, to a terminally ill person might unintentionally hasten their death.
- Scientific Evidence: Currently, there is no scientific evidence to suggest that opioids, when appropriately administered to relieve pain, can hasten death, even in patients at the very end of life.
- Moral Obligation: As a nurse, you have a moral and ethical obligation to provide comfort and pain relief at the end of life. This is a fundamental aspect of compassionate care.
- Rule of Double Effect: Even when there's a concern about the possibility of hastening death, the rule of double effect provides ethical justification. This rule states that if an unwanted, foreseeable consequence (e.g., hastened death) occurs as a result of an action taken to achieve a moral good (e.g., pain relief), the action is ethically justified if the nurse's primary intent is to relieve pain and not to hasten death. The focus is on the primary intention behind the action.
B. Requests for Assisted Suicide
Unrelieved and intractable pain is one of the reasons that patients may make requests for assisted suicide.
- Pain Management's Role: Aggressive and adequate pain management may actually decrease the number of such requests, as patients find their suffering is being effectively addressed.
- Legal Status: Assisted suicide is a complex issue with significant legal and ethical dimensions that extend beyond pain management alone. Its legality varies by jurisdiction. For instance, in the United States, as of the provided text, it was legal in Oregon, Washington, and Montana.
- Nurses' Role: Organizations like the Oregon Nurses Association have developed position papers to guide nurses through the legal and ethical complexities of such unique situations, emphasizing the importance of providing comprehensive palliative care and pain relief.
C. Use of Placebos in Pain Assessment and Treatment
The use of placebos (substances with no pharmacological effect, like saline, given as if they are active drugs) to assess or treat pain involves deception.
- Ethical Condemnation: The use of placebos for pain assessment or treatment is condemned by several professional organizations.
- Reason for Condemnation: This practice involves deceiving patients by making them believe they are receiving an analgesic when they are, in fact, receiving an inert substance. This undermines trust in the healthcare provider and the therapeutic relationship, which is fundamental to effective pain management. It can also lead to misdiagnosis of pain severity and inappropriate treatment plans.
Managing pain in special populations
Managing pain in special populations presents unique challenges, particularly when patients cannot self-report their pain or have a history of substance abuse. Tailored approaches are crucial to ensure these individuals receive effective and compassionate pain relief.
I. Patients Unable to Self-Report Pain
While a patient's self-report is considered the gold standard for pain assessment, many conditions can impair this ability. These include:
- Advanced dementia
- Progressive neurological diseases (e.g., Parkinson's disease, multiple sclerosis)
- Cerebrovascular disease
- Psychosis
- Delirium
For these individuals, nurses must be highly attuned to behavioral and physiological changes, which may be the only indicators of pain. Recognizing these behavioral symptoms is a critical skill.
- Assessment Techniques:
- Obtain Self-Report When Possible: Never assume a person is unable to give a verbal report. Always attempt to elicit a self-report first.
- Investigate Potential Causes: Look for conditions or procedures that are likely to cause pain (e.g., recent surgery, injury, infection, immobility).
- Observe Behaviors: Look for specific behaviors that indicate pain, such as:
- Grimacing, frowning, or other facial expressions
- Rubbing a painful area
- Groaning, moaning, or crying
- Restlessness, agitation, or guarding
- Changes in usual behavior (e.g., increased confusion, withdrawal, aggression)
- Obtain Surrogate Reports: Gather information from professional and family caregivers who know the patient best, as they can often identify subtle changes indicative of pain.
- Trial Analgesics: Administering an analgesic and then reassessing the patient for a decrease in pain-related behaviors can help confirm the presence of pain and the effectiveness of the intervention.
- Specialized Scales: Several scales have been developed to assess pain-related behaviors specifically for nonverbal patients, particularly those with advanced dementia. Resources for these tools are available from organizations like the City of Hope Pain and Palliative Care Resource Center.
II. Patients With Substance Abuse Problems
Healthcare providers often express reluctance to administer opioids to patients with substance abuse problems due to concerns about promoting or enhancing addiction. However, current evidence does not support the idea that providing appropriate opioid analgesia in any way worsens their addictive disease. In fact, the stress of unrelieved pain can actually contribute to relapse in recovering patients or increase drug use in those actively abusing drugs.
- Ethical Right to Care: Guidelines, such as those from the American Society for Pain Management Nursing, emphasize that patients with addictive disease and pain have the right to be treated with dignity, respect, and the same quality of pain assessment and management as all other patients.
- Team Approach: Managing pain in patients with addiction is challenging and requires an interdisciplinary team approach, ideally including pain management and addiction specialists. Team members must be aware of their own attitudes and biases towards individuals with substance abuse problems, as these can lead to undertreatment of pain.
- Assessment and Management Strategies:
- Determine Drug Use: If the patient acknowledges opioid use, it's important to determine the specific types and amounts of drugs used.
- Avoid Drug of Abuse: It is generally best to avoid exposing the patient to their specific drug of abuse.
- Equianalgesic Dosing: If daily drug doses are known, effective equianalgesic doses of other opioids can be determined.
- Suspect Abuse if Doses are Ineffective: If a history of drug abuse is unknown or the patient does not acknowledge substance abuse, suspicion of abuse should arise if normal doses of analgesics do not provide expected relief. Toxicology screens may be helpful in determining recently used drugs. Discussing these findings with the patient in a non-judgmental way may help gain their cooperation in pain control.
- Higher Opioid Doses: Severe pain in these patients should be treated with opioids, often at much higher doses than those used with drug-naïve patients, due to built-in tolerance.
- Single Opioid Preferred: The use of a single opioid is generally preferred.
- Avoid Mixed Agonist-Antagonists: Avoid using mixed opioid agonist-antagonists (e.g., butorphanol) or partial agonists (e.g., buprenorphine) as these drugs may precipitate withdrawal symptoms in opioid-tolerant individuals.
- Multimodal Approach: Nonopioid and adjuvant analgesics, as well as non-drug pain relief measures, should be used as appropriate.
- Around-the-Clock Dosing: To maintain consistent opioid blood levels and prevent withdrawal symptoms, provide analgesics around the clock rather than PRN.
- Breakthrough Pain Management: Use supplemental doses to treat breakthrough pain.
- Acute Pain Management: For acute pain, IV or Patient-Controlled Analgesia (PCA) infusions may be considered.
NURSING INSIGHT
Addressing Misconceptions and Building Trust as Central to Overcoming Pain Management Barriers: A significant portion of the text is dedicated to challenges in effective pain management, primarily stemming from "misunderstandings about tolerance, physical dependence, and addiction." The content consistently emphasizes the nurse's role in educating patients and caregivers to debunk these myths. For instance, explaining that addiction is uncommon, tolerance is normal, and physical dependence requires careful tapering, not abandonment. This educational effort is directly linked to establishing a "trusting relationship" and fostering "effective communication," which are deemed essential for the success of any pain management action. The text explicitly states that pseudoaddiction arises from inadequate treatment and can be avoided by effective communication, underscoring how crucial trust and accurate information are in preventing negative patient behaviors and improving outcomes.
Summary
- Understanding Pain: Pain is categorized by its pathology (nociceptive vs. neuropathic) and duration (acute vs. chronic).
- Nociceptive pain arises from tissue damage and can be superficial somatic, deep somatic, or visceral.
- Neuropathic pain results from nerve damage and includes central, peripheral, deafferentation, and sympathetically maintained types.
- The Pain Process (Nociception): Pain involves four distinct physiological steps:
- Transduction: Noxious stimuli convert into electrical signals.
- Transmission: Signals travel along nerve fibers to the spinal cord and brain.
- Perception: The brain interprets and gives meaning to the pain.
- Modulation: Descending pathways can inhibit or facilitate pain signals.
- Pain Assessment: A crucial, subjective process where the patient's self-report is gold standard. Assessment is multidimensional, covering pattern, location, intensity, quality, associated symptoms, and impact. Special considerations apply to nonverbal patients.
- Management Strategies: A balanced approach combining:
- Nonpharmacological methods: Cutaneous stimulation (TENS, heat, cold, massage), distraction, relaxation, imagery, acupuncture, and environmental adjustments.
- Pharmacological interventions:
- Nonopioids: Acetaminophen and NSAIDs for mild-to-moderate pain, with careful monitoring for side effects (e.g., hepatotoxicity, gastric upset, bleeding).
- Opioids: For moderate-to-severe pain, administered around-the-clock for acute pain, and orally for chronic pain. Close monitoring for adverse effects like constipation, orthostatic hypotension, urinary retention, nausea/vomiting, sedation, and respiratory depression (which can be reversed with naloxone) is vital.
- Adjuvants: Enhance nonopioids, alleviate aggravating symptoms, and are key for neuropathic pain (e.g., anticonvulsants, antidepressants).
- Patient-Controlled Analgesia (PCA): Allows patient self-administration, providing consistent pain control and an increased sense of control.
- Nursing and Collaborative Role: Nurses are integral to the interdisciplinary team, providing assessment input, developing patient-centered plans, educating, advocating, and supporting. Building trust is paramount.
- Addressing Challenges: Understanding and clarifying common misconceptions is crucial:
- Tolerance: A normal physiological response requiring increased doses, not addiction.
- Physical Dependence: A normal physiological response with withdrawal upon abrupt cessation, requiring careful tapering.
- Pseudoaddiction: Drug-seeking behaviors due to undertreated pain, resolving with adequate management.
- Addiction: A complex neurobiologic condition distinct from tolerance and physical dependence, rarely occurring with therapeutic opioid use.
- Ethical Considerations:
- Fear of Hastening Death: Opioids don't hasten death when used for pain; the rule of double effect justifies pain relief even if death is a foreseeable, unintended consequence.
- Assisted Suicide Requests: Aggressive pain management may reduce such requests.
- Placebo Use: Condemned by professional organizations due to deception and undermining trust.
