
Safety
Lessons
- Objectives
- Introduction
- Factors Affecting Patient Safety
- Common Potential Hazards Throughout The Life Span
- Types Of Accidents
- Nursing Diagnosis
- Nursing Assessment
- Practice Exercise 1
- Preventing Specific Hazards I
- Practice Exercise 2
- Preventing Specific Hazards II
- Restraints
- Practice Exercise 3
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Describe the factors affecting environmental safety.
- Describe methods to assess a client’s risk for injury.
- Identify common potential hazards throughout the life span.
- Describe the categories of safety risks in a health care agency.
- Describe nursing interventions specific to a patients’ age for reducing risk of falls, fires, poisonings, radiation and electrical hazards.
- Discuss implementation of seizure precautions.
- Discuss the use and legal implications of restraints
- Describe alternatives to restraints.
Introduction
Safety, often defined as freedom from psychological and physical injury, is a basic human need.
Registered nurses (RNs) are responsible for providing the client with a safe environment through the delivery of professional, quality nursing care that incorporates safety precautions, infection control practices, and hygiene assistance.
A safe environment:
- Reduces the risk for illness and injury
- Helps to contain the cost of health care by preventing extended lengths of treatment
- Improves or maintaining a patient’s functional status
- Increases the patient’s sense of well-being.
A safe environment protects the staff as well, allowing them to function optimally.
Vulnerable groups who often require help in achieving a safe environment include infants, children, older adults, the ill, the physically and mentally disabled, the illiterate, and the poor.
Factors Affecting Patient Safety
The ability of people to protect themselves from injury is affected by several factors. Nurses need to assess each of these factors when they plan care or teach clients to protect themselves.
- Age and development: For the very young, learning about the environment is essential to avoid what is potentially harmful. Older adults can have difficulty with movement and diminished sensory-neurologic acuity, which can contribute to the likelihood of injury.
- Lifestyle: Includes unsafe work environments; residence in neighborhoods with high crime rates; access to firearms; insufficient income to purchase safety equipment or make necessary repairs; and access to illicit drugs.
- Mobility and health status: paralysis, muscle weakness, diminished balance, and lack of coordination place clients at risk for injury.
- Ability to communicate: Individuals with diminished ability to receive and convey information are at risk for injury. They include clients with aphasia, language barriers, or the ability to read.
- Emotional state: Stressful situations can reduce a person’s level of concentration, cause errors of judgment, and decrease awareness of external stimuli. Extreme emotional states can alter the ability to perceive environmental hazards.
- Sensory-perceptual alterations: People with impaired touch perception, hearing, taste, smell, and vision are highly susceptible to injury.
- Cognitive awareness: include people lacking sleep; people who are unconscious or semiconscious; disoriented people; people who perceive stimuli that do not exist; and people whose judgment is altered by disease or medications, such as narcotics, tranquilizers, hypnotics, and sedatives.
- Safety awareness: Lack of knowledge about unfamiliar equipment, such as oxygen tanks, intravenous tubing, and hot packs, is a potential hazard.
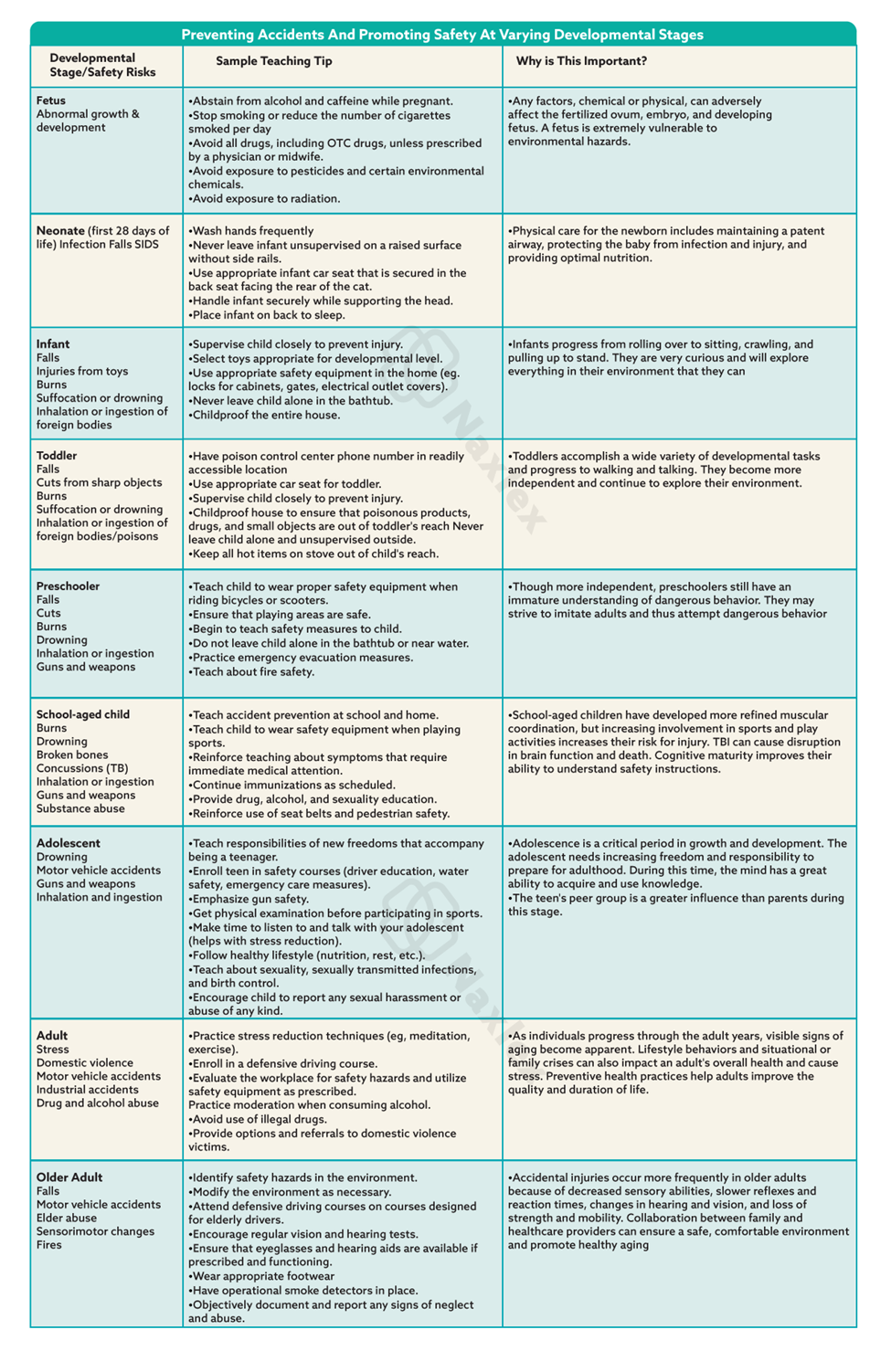
Common Potential Hazards Throughout The Life Span
Developing fetus:
Exposure to:
- Maternal smoking, alcohol consumption, addictive drugs.
- X-rays (first trimester)
- Pesticides
Newborns and infants:
- Falling
- Choking
- Suffocation in crib
- Burns from hot water or other spilled hot liquids
- Placement in the prone position
- Automobile crashes, crib or playpen injuries
- Suffocation when entangled in cords
- Electric shock, poisoning
Toddlers:
- Physical trauma from falling
- Running into objects
- Aspiration of small toys
- Getting cut by sharp objects
- Automobile crashes
- Burns; poisoning; drowning; and electric shock
Preschoolers:
- Injury from traffic, playground equipment, and other objects
- Choking, suffocation, and obstruction of airway or ear canal by foreign objects
- Poisoning
- Drowning; fire and burns
- Harm from other people or animals
Adolescents:
- Vehicular (automobile, bicycle) crashes
- Recreational injuries
- Firearms, substance abuse
- Sexually transmitted diseases.
Older adults:
- Falls
- Burns
- Pedestrian and automobile crashes
Types Of Accidents
In the health care setting, accidents are categorized by their causative agent: client behaviors, therapeutic procedures, or equipment:
1. Client behavior accidents occur when the client’s behavior or actions precipitate the incident, for example, poisonings, burns, and self-inflicted cuts and bruises.
2. Therapeutic procedure accidents occur during the delivery of medical or nursing interventions, for example, medication errors, client falls during transfers, contamination of sterile instruments or wounds, and improper performance of nursing activities.
3. Equipment accidents result from the malfunction or improper use of medical equipment, for example, electrocution and fire.
Nursing Diagnosis
The primary nursing diagnosis risk for injury exists when the client is at risk for injury as a result of environmental conditions interacting with the individual’s adaptive and defensive resources.
NANDA (North American Nursing Diagnosis Association) has six defined subcategories of specific risk factors for this diagnostic labeling:
- Risk for suffocation: An accentuated risk of accidental suffocation.
- Risk for poisoning: An accentuated risk of accidental exposure to, or ingestion of, drugs or dangerous products in doses sufficient to cause poisoning
- Risk for trauma: An accentuated risk of accidental tissue injury (e.g., wound, burn, fracture)
- Risk for aspiration: Risk for entry of gastrointestinal secretions, oropharyngeal secretions, solids, or fluids into the tracheobronchial passages
- Risk for disuse syndrome: Risk for deterioration of body or body systems as the result of prescribed or unavoidable musculoskeletal inactivity
- Risk for latex allergy response: Risk for allergic response to natural latex rubber products
Nursing Assessment
During the assessment process thoroughly assess each patient and critically analyze findings to ensure that you make patient-centered clinical decisions required for safe nursing care.
Patients usually do not purposefully put themselves in jeopardy. When they are uninformed or inexperienced, threats to their safety occur.
To conduct a thorough patient assessment, consider possible threats to a patient’s safety, including the immediate environment and any individual risk factors.
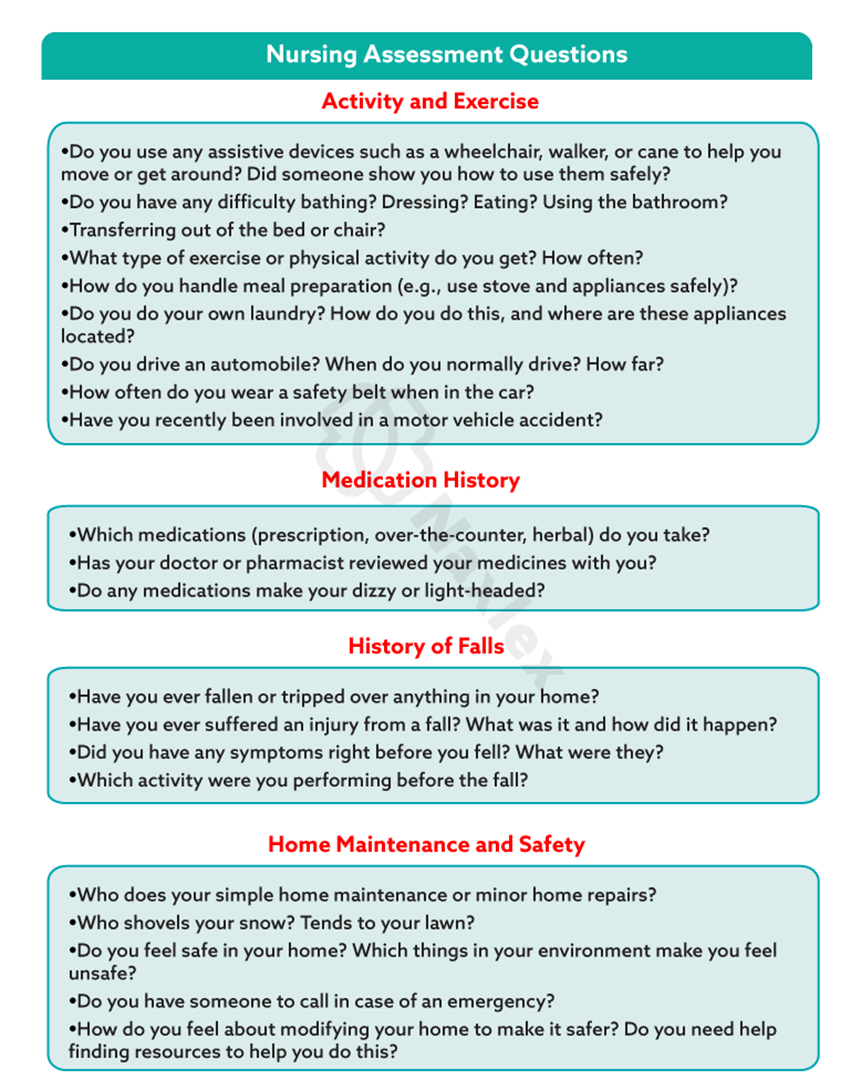
Health care environment:
When the patient is cared for within a health care facility, you need to determine if any hazards exist in the immediate care environment.
- placement of equipment (e.g., drainage bags, IV pumps) or furniture
- positioning of the patient’s bed
- assistance with ambulation
- multiple tubes or IV lines
- call bell within reach
Risk for Medical Errors:
Be alert to factors within your own work environment that create conditions in which medical errors are more likely to occur.
- overwork and fatigue
- patient’s identification by using two identifiers
Nursing insights:
- Nurses need awareness of what constitutes a safe environment for specific individuals and for groups of people in the home, community, and workplace.
- Hazards to safety occur at all ages and vary according to the age and development of the individual.
Preventing Specific Hazards I
Falls
People of any age can fall, but infants and older adults are particularly prone to falling and causing serious injury. Falls are the leading cause of injuries among older adults.
It is important to assess clients for fall risk on admission, whenever a change in physical or mental status occurs, on transfer, and before discharge.
Fall risk appraisal:
|
Risk Factor |
Points |
|
Age 60-69 years (1 point) 70-79 years (2 points) ≥80 years (3 points |
|
|
Fall History One fall within 6 months before admission (5 points) |
|
|
Elimination (Bowel and Urine) Incontinence (2 points) Urgency or frequency (2 points) Urgency/frequency and incontinence (4 points) |
|
|
Medications: Includes PCA/Opiates, Anticonvulsants, Antihypertensives, Diuretics, Hypnotics, Laxatives, Sedatives, and Psychotropics On one high fall–risk drug (3 points) On two or more high fall–risk drugs (5 points) Sedated procedure within past 24 hours (7 points) |
|
|
Patient Care Equipment: Any Equipment That Tethers Patient (e.g., IV Infusion, Chest Tube, Indwelling Catheters, SCDs) One present (1 point) Two present (2 points) 3 or more present (3 points) |
|
|
Mobility (Multi-select, Choose All That Apply and Add Points Together) Requires assistance or supervision for mobility, transfer, or ambulation (2 points) Unsteady gait (2 points) Visual or auditory impairment affecting mobility (2 points) |
|
|
Cognition (Multi-select, Choose All That Apply and Add Points Together) Altered awareness of immediate physical environment (1 point) Impulsive (2 points) Lack of understanding of one’s physical and cognitive limitations (4 points) |
|
|
TOTAL: Moderate risk = 6-13 total points High risk = >13 total points |
|
NB: The data obtained from the client’s fall risk appraisal will identify which clients require special nursing measures to prevent falls.
Fall Prevention strategies
1. Assessment
- Perform client injury risk appraisal and identify fall risks. Update status of fall risks daily and as needed on a nursing care plan.
- Assess effects of medications administered that increase risk of falling.
2. Client teaching
- On admission, orient clients to their surroundings and explain the call system.
- Instruct client and significant others on correct use of hospital equipment.
- Instruct client with risk for falls to call for assistance when ambulating or performing activities of daily living (ADL).
3. Environmental interventions:
- Keep the environment tidy; keep light cords from underfoot and furniture out of the way.
- Carefully assess the client’s ability to ambulate and transfer.
- Provide walking aids and assistance as required.
- Encourage the client to use the call light to request assistance. Ensure that the light is within easy reach.
- Place bedside tables and overbed tables near the bed or chair so that clients do not overreach and consequently lose their balance.
- Always keep hospital beds in the low position and wheels locked when not providing care so that clients can move in or out of bed easily.
- Encourage clients to use grab bars mounted in toilet and bathing areas and railings along corridors.
- Make sure nonskid bath mats are available in tubs and showers.
- Encourage the client to wear nonskid footwear.
- Closely supervise the clients at risk for falls, especially at night.
- Use individualized interventions (e.g., alarm sensitive to client position) rather than side rails for confused clients.
- Use mechanical or electronic ceiling lifts to transfer dependent clients.
4. Direct nursing care:
- Respond promptly to call lights and verbal requests for assistance.
- Provide assistance with ADL.
- Maintain close supervision by performing hourly safety assessments.
- Encourage significant others to stay with high-risk clients.
- Provide proper equipment for ambulation and elimination needs.
- Document in the client’s medical record.
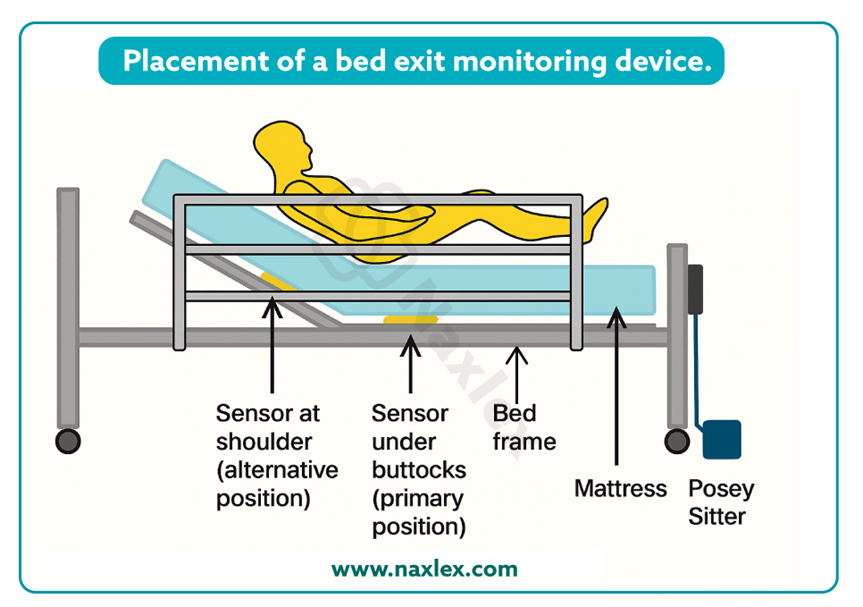
The alarm device is position sensitive; that is, when it approaches a near-vertical position (such as in walking, crawling, or kneeling as the client attempts to get out of bed), the audio alarm will be triggered.
Fire safety
Fire is a potential danger to all people in an institutional or a home environment. It occurs with the interaction of three elements: sufficient heat to ignite the fire, combustible material, and oxygen to support the fire.
Common causes of fire are:
- smoking in bed
- discarding cigarette butts in trash cans
- faulty electrical equipment
Immobilized or incapacitated clients are at increased risk during a fire.
Interventions aimed at reducing the risk of fire:
- Clearly marking fire exits
- Knowing locations of fire extinguishers and their operation
- Practicing fire evacuation procedures
- Posting emergency phone numbers by all telephones
- Keeping open spaces and hallways clear of clutter
- Checking electrical cords and outlets for exposed or damaged wires
- Reporting identified electrical hazards
- Educating clients about fire hazards
In the event of a fire:
Nursing interventions during a fire are directed at protecting the client from injury and containing the fire.
When smoke or fire is detected, two mnemonics can help the nurse remember the steps to follow. First is the RACE protocol:
- Rescue: If the area is safe to enter, protect and evacuate clients who are in immediate danger.
- Alarm: Pull the fire alarm and report the fire details and location to the hospital’s fire emergency extension.
- Confine: Contain the fire by closing the doors to all rooms and the fire doors at each entrance to the unit.
- Extinguish: Extinguish the fire. Use the appropriate type of fire extinguisher (see the PASS mnemonic) OR Evacuate the area if the fire is too large for a fire extinguisher.
The nurse follows the mnemonic PASS when using a fire extinguisher:
- Pull out the extinguisher’s safety pin.
- Aim the hose at the base of the fire.
- Squeeze or press the handle to discharge the material onto the fire.
- Sweep the hose from side to side across the base of the fire until the fire appears to be out.
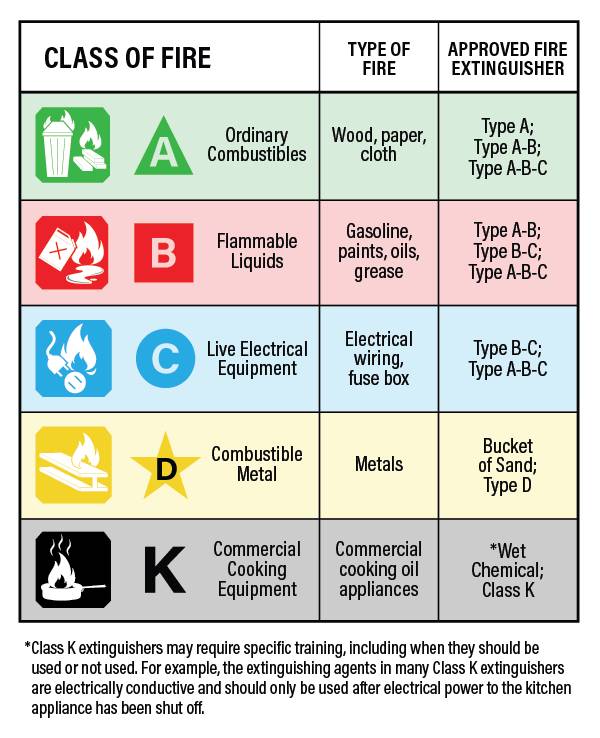
Extinguishing the fire requires knowledge of three categories of fire, classified according to the type of material that is burning:
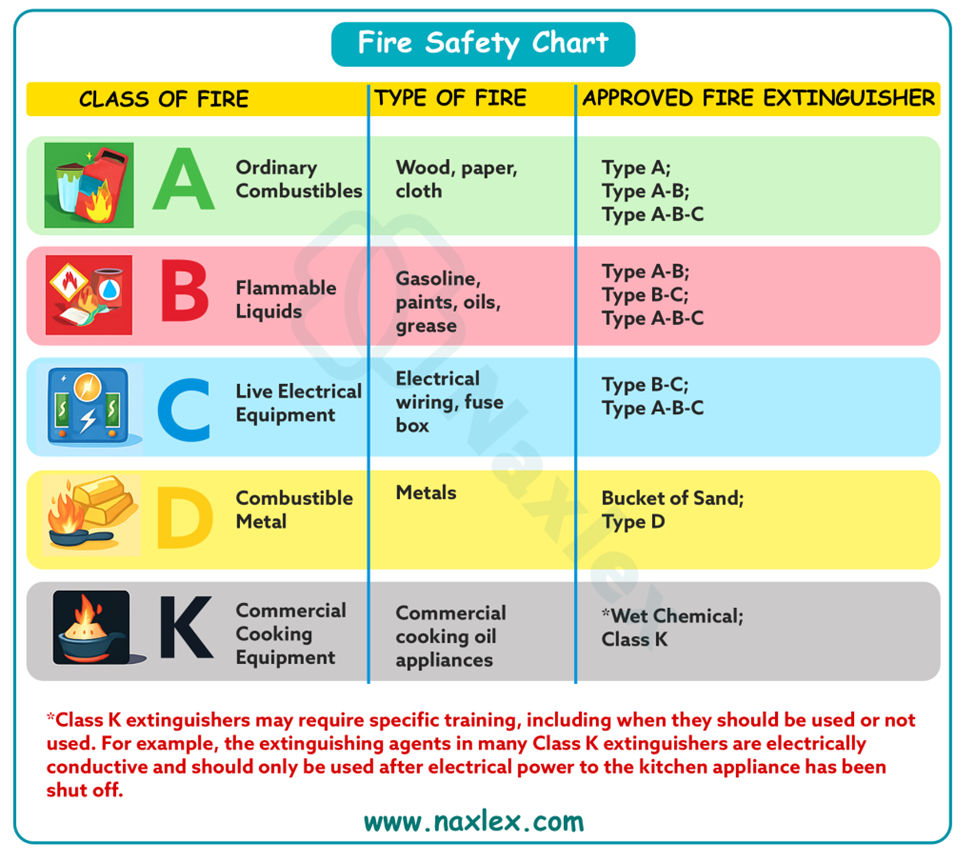
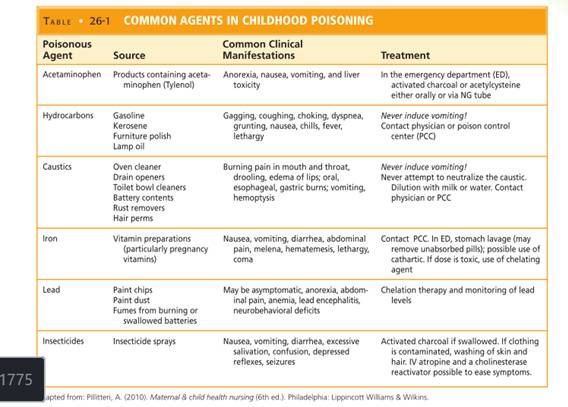
Poisoning
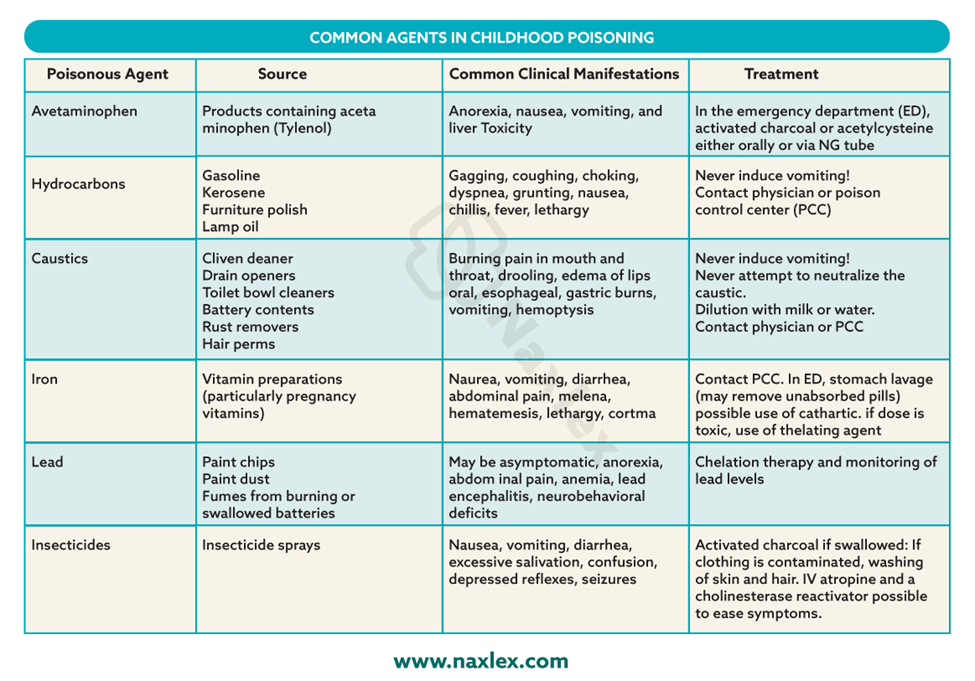
A poison is any substance that causes an alteration in the client’s health, such as injury or death, when inhaled, injected, ingested, or absorbed by the body.
Antidotes and treatments are available for some but not all types of poisonings.
Causes of poisonings are:
• Inadequate supervision of children
• Ingestion of household plants
• Improper storage of toxic substances
• Insect or snake bites
• Accidental ingestion of a toxic substance or medication overdose- due to failing eyesight/ impaired memory.
• Carbon monoxide poisoning
Carbon monoxide poisoning: Carbon monoxide (CO) is an odorless, colorless, tasteless gas that is very toxic. Exposure to CO can cause symptoms that include headaches, dizziness, weakness, nausea, vomiting, or loss of muscle control. Prolonged exposure to CO can lead to unconsciousness, brain damage, or death.
Preventing poisoning:
- Lock potentially toxic agents, in a cupboard, or attach special plastic hooks to the insides of cabinet doors to keep them securely closed.
- Do not let children watch you open the latches.
- Store medications in child-resistant containers.
- Do not take medications in front of children.
- Avoid storing toxic liquids or solids in food containers.
- Do not remove container labels or reuse empty containers to store different substances.
- Do not rely on cooking to destroy toxic chemicals in plants.
- Teach children never to eat any part of an unknown plant.
- Do not keep poisonous plants in the home, and avoid planting poisonous plants in the yar
- Place poison warning stickers designed for children on containers with toxic substances.
- Read and follow label directions on all products before using them.
- Keep syrup of ipecac on hand at all times.
- Display the phone number of the poison control center near or on all telephones in the home so that it is available to babysitters, family, and friends.
Interventions in accidental poisoning:
1. Assess for signs or symptoms of ingestion of harmful substance:
- nausea, vomiting
- foaming at the mouth, drooling
- difficulty breathing
- sweating, and lethargy.
2. Terminate exposure to the poison by having the person empty his or her mouth of pills, plant parts, or other material.
3. If poisoning is caused by skin or eye contact, irrigate the skin or eye with copious amounts of cool tap water for 15 to 20 minutes.
4. In the case of an inhalation exposure, safely remove the victim from the potentially dangerous environment.
5. Identify the type and amount of substance ingested to help determine the correct type and amount of antidote needed.
6. Call the local poison control center or the national toll-free poison control center number (1-800-222-1222) before attempting any intervention.
7. If the victim has collapsed or stopped breathing, call 911 for emergency transportation to the hospital. Initiate CPR if indicated until emergency personnel arrive.
8. Position the victim with head turned to the side to reduce risk for aspiration.
9. Never induce vomiting if the victim has ingested the following poisonous substances: lye, household cleaners, hair care products, grease or petroleum products, furniture polish, paint thinner, or kerosene.
10. Never induce vomiting in an unconscious or convulsing victim because vomiting increases risk for aspiration.
Electrical hazards
All electric equipment must be properly grounded. Grounding prongs offer a path of least resistance to stray electric currents.
The electric plug of grounded equipment has three prongs. The two short prongs transmit the power to the equipment. The third, longer prong is the grounding device, which carries short circuits or stray electric current.
Faulty equipment such as equipment with a frayed cord presents a danger of electric shock or may start a fire.
Actions to reduce electrical hazards:
- Check cords for fraying or other signs of damage before using an appliance. Do not use it if damage is apparent.
- Avoid overloading outlets and fuse boxes with too many appliances.
- Use only grounded outlets and plugs.
- Always pull a plug from the wall outlet by firmly grasping the plug and pulling it straight out. Pulling a plug by its cord can damage the cord and plug unit.
- Never use electric appliances near sinks, bathtubs, showers, or other wet areas, because water readily conducts electricity.
- Keep electric cords and appliances out of the reach of young children.
- Place protective covers over wall outlets to protect young children.
- Have all non-insulated wiring in the home altered to meet safety standards.
- Carefully read instructions before operating electric equipment. Clients who do not understand how to operate the equipment should seek advice.
- Always disconnect appliances before cleaning or repairing them.
- Unplug any appliance that has given a tingling sensation or shock and have an electrician evaluate it for stray current.
- Keep electric cords coiled or taped to the ground away from areas of traffic to prevent others from damaging the cords or tripping over them.
If a client receives an electrical shock:
- Turn off or remove the electric source before touching the client.
- The client’s pulse should be checked.
- If the client has no pulse, CPR should be initiated.
- If the client has a pulse, the nurse should assess vital signs, mental status, and skin integrity for burns.
- A prescribing practitioner should be notified of the event.
- The nurse should note points of entry and exit of electrical current to assess for potential complications.
Preventing Specific Hazards II
Radiation
Clients are exposed to radiation during diagnostic testing and therapeutic interventions.
Injury can occur from radiation if there is overexposure or exposure to untargeted tissues.
Radiation therapy destroys cancer cells, with minimal exposure of normal cells to the damaging effects of radiation; the damaged cells die or become unable to divide.
Radiation therapy is effective on tissues directly within the path of the radiation beam.
Side effects include local skin changes and irritation, alopecia (hair loss), fatigue (most common side effect of radiation), and altered taste sensation; the effects vary according to the site of treatment.
Types of radiation therapy:
External beam radiation (also called teletherapy) and internal radiation (also called brachytherapy) are the types of radiation therapy most commonly used to treat cancer.
a) External beam radiation (teletherapy):
The actual radiation source is external to the client.
1. Instruct the client regarding self-care of the skin.
2. The client does not emit radiation and does not pose a hazard to anyone else.
b) Brachytherapy
1. The radiation source comes into direct, continuous contact with tumor tissues for a specific time.
2. The radiation source is within the client; for a period of time, the client emits radiation and can pose a hazard to others.
3. Brachytherapy includes an unsealed source or a sealed source of radiation.
Unsealed radiation source
a. Administration is via the oral or IV route or by instillation into body cavities.
b. The source is not confined completely to one body area, and it enters body fluids and eventually is eliminated via various excreta, which are radioactive and harmful to others. Most of the source is eliminated from the body within 48 hours; then neither the client nor the excreta is radioactive or harmful.
Sealed radiation source
a. A sealed, temporary or permanent radiation source (solid implant) is implanted within the tumor target tissues.
b. The client emits radiation while the implant is in place, but the excreta are not radioactive.
Radiation safety:
1. Know the protocols and guidelines of the health care agency.
2. Label potentially radioactive material.
3. To reduce exposure to radiation, do the following.
- Limit the time spent near the source.
- Make the distance from the source as great as possible.
- Use a shielding device such as a lead apron.
4. Monitor radiation exposure with a film (dosimeter) badge.
5. Place the client who has a radiation implant in a private room.
6. Never touch dislodged radiation implants/ body fluids from client.
7. Keep all linens in the client’s room until the implant is removed.
8. Label all potentially radioactive material.
9. Dispose of radioactive substances in special containers.
Seizures
A seizure is a single temporary event that consists of uncontrolled electrical neuronal discharge of the brain that interrupts normal brain function.
Causes of seizures:
The etiology or cause of the seizure can be different based on the age of the client.
- Trauma during birth is the leading cause of seizures in newborns.
- Infants and children develop seizures as a result of fever, trauma, and infections of the central nervous system.
- Adults- most commonly related to structural abnormalities of the brain such as tumors, strokes, and trauma.
Types of seizures:
Partial seizures (also called focal) involve electrical discharges from one area of the brain.
Generalized seizures affect the whole brain.
NB: Clients are at risk for injury if they experience seizures that involve the entire body such as grand mal (tonic-clonic) seizures or any seizure that includes loss of consciousness.
Seizure precautions:
Seizure precautions are safety measures taken by the nurse to protect clients from injury should they have a seizure.
Include:
1. Assessment
Assess the patient's seizure history and knowledge of precipitating factors.
Assess medication history and patient’s adherence.
Assess for medical and surgical conditions, including electrolyte disturbances
2. Environmental considerations
Pad the bed of any client who might have a seizure.
Secure blankets or other linens around the head, foot, and side rails of the bed.
Put oral suction equipment and oxygen equipment in place and test to ensure that it is functional.
3. In the event of a seizure:
Note time, stay with patient, and call for help.
Track duration of seizure.
Notify health care provider immediately. Have staff member bring an emergency cart to the bedside.
Position the patient safely. If standing or sitting, guide the patient to the floor and protect the head by cradling in the nurse's lap or placing a pad under head. Turn the patient onto one side, head tilted slightly forward.
Clear surrounding area of furniture. If the patient is in bed, remove pillows and raise side rails.
Do not restrain the patient; hold limbs loosely if they are flailing.
Loose clothing such as a collar or belt.
Maintain the patient's airway and suction as needed.
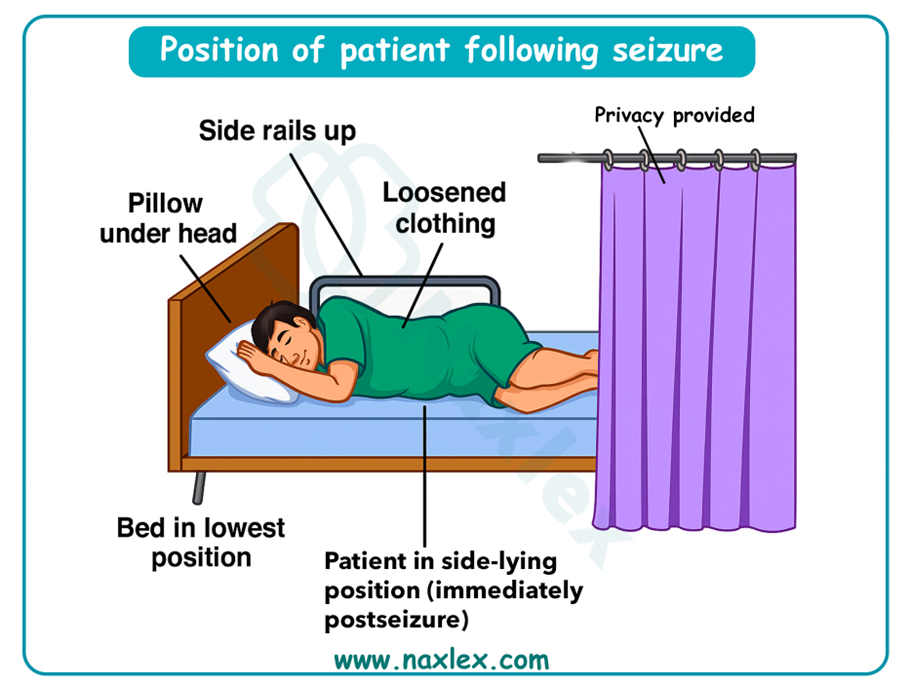
1. Post seizure:
Assist patient to position of comfort in bed with side rails up (one rail down for easy exit).
Place the bed in the lowest position.
Place the call light or intercom system within reach.
Provide a quiet, non-stimulating environment.
Record thoroughly in nurses’ notes your observations before, during, and after seizure.
Firearms
The following basic firearm safety rules must be implemented for any gun:
- Store all guns in sturdy locked cabinets without glass and make sure the keys are inaccessible to children.
- Store the bullets in a different location from the guns.
- Tell children never to touch a gun or stay in a friend’s house where a gun is accessible.
- Teach children never to point the barrel of a gun at anyone.
- Ensure the firearm is unloaded and the action is open when handing it to someone else.
Restraints
Restraints are devices used to limit the physical activity of a client or a part of the body.
All patients have the right to be free from restraint or seclusion, of any form, imposed as a means of coercion, discipline, convenience, or retaliation by staff.
Restraint or seclusion may only be imposed to ensure the immediate physical safety of the patient, a staff member, or others and must be discontinued at the earliest possible time.
Restraints can be classified as:
- physical restraints
- chemical restraints
- use of seclusion
Physical restraints: Any manual method, physical or mechanical device, material, or equipment that immobilizes or reduces the ability of a patient to move his or her arms, legs, body, or head freely.
Examples: Leather or cloth wrist and ankle restraints, soft belts or vests, hand mitts, pelvic ties, gerichairs, and overchair tables.
Chemical restraints: Using a medication to control behavior or to restrict the client’s freedom of movement.
Seclusion: This is the involuntary confinement of a client alone in a room or area from which the client is physically prevented from leaving.
Seclusion may only be used for the management of violent or self-destructive behavior that is an immediate threat to the client’ s physical safety.
Risks of improper use of restraints:
Improper use of restraints and lack of monitoring can lead to injury and death and to psychological harm. Restraints can cause injury to clients through:
- Hazards of immobility (e.g., muscle atrophy, bone loss, contractures, pressure ulcers, constipation, and decreased appetite)
- Confusion, boredom and loneliness, depression, and loss of dignity.
- Death can result due to strangulation, suffocation, broken necks, burns, pneumonia, and sepsis.
Standards for Use of Restraints:
- Restraints should be used only after every other possible means of ensuring safety have been unsuccessful and documented.
- There must be a face-to-face evaluation of the client within 1 hour by the physician or LIP, or an RN or physician assistant (PA) who has been trained.
- A written restraint order for an adult with violent or self-destructive behavior, following evaluation, is valid for only 4 hours for up to a total of 24 hours.
- Primary care provider’s order for restraints include: delineation of the reason for, specific time frame (only for violent or self-destructive behavior), and type of restraint necessary.
- Restrained clients must be monitored regularly.
- Restraint or seclusion must be discontinued at the earliest possible time.
- “As-needed” (prn) orders for restraints are prohibited.
Selecting a restraint:
5 criteria:
- It restricts the client’s movement as little as possible.
- It is safe for the particular client.
- It does not interfere with the client’s treatment or health problems.
- It is readily changeable.
- It is as discreet as possible
Applying restraints:
- Obtain consent from the client or guardian.
- Assure the client and the client’s support people that the restraint is temporary and protective.
- Pad bony prominences (e.g., wrists and ankles) before applying a restraint over them.
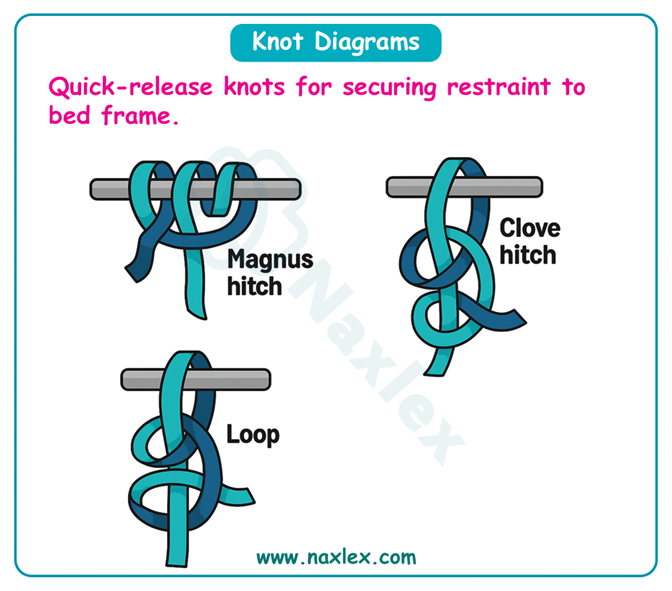
- Always tie a limb restraint with a knot (e.g., a clove hitch) that will not tighten when pulled.
- Tie the ends of a body restraint to the part of the bed that moves to elevate the head.
- Never tie the ends to a side rail or to the fixed frame of the bed if the bed position is to be changed.
- Apply a restraint so that it can be released quickly in case of an emergency and with the body part in a normal anatomic position.
- Check restraint for constriction by inserting two fingers under restraint.
- Assess skin integrity per agency protocol (e.g., every 2 hours), and provide range-of-motion (ROM) exercises and skin care when restraints are removed.
- Assess and assist with basic needs: nutrition, hydration, hygiene, elimination.
- Reassess the continued need for the restraint.
- Immediately report to the nurse in charge and record on the client’ s chart any persistent reddened or broken skin areas under the restraint.
- At the first indication of cyanosis or pallor, coldness of a skin area, or a client’s complaint of a tingling sensation, pain, or numbness, loosen the restraint and exercise the limb.
Alternatives to restraints:
- Ask family members or significant others to stay with the client.
- Reduce stimulation (e.g., noise, lights); play soothing music.
- Assign nurses in pairs to act as “buddies” so that one nurse can observe the client when the other leaves the unit.
- Place unstable clients in an area that is constantly or closely supervised.
- Prepare clients before a move to limit relocation shock and resultant confusion.
- Use rocking chairs to help confused clients expend some of their energy so that they will be less inclined to wander.
- To quiet agitated clients, try a warm beverage, soft lights, a back rub, or a walk.
- Use “environmental restraints,” such as pieces of furniture or large plants as barriers, to keep clients from wandering beyond appropriate areas.
- Place a picture or other personal item on the door to clients’ rooms to help them identify their room.
- Try to determine the causes of the client’s sundowner-syndrome.
Nursing insights:
Measures to ensure the safety of people of all ages focus on:
(a) observation or prediction of situations that are potentially harmful
(b) client education that empowers clients to safeguard themselves and their families from injury.
Summary
- Nurses need awareness of what constitutes a safe environment for specific individuals and for groups of people in the home, community, and workplace.
- Hazards to safety occur at all ages and vary according to the age and development of the individual.
- Nurses assess clients at risk for injury through methods such as nursing history and physical examination, risk assessment tools, and home hazard appraisal.
Comprehensive Questions
Falls
People of any age can fall, but infants and older adults are particularly prone to falling and causing serious injury. Falls are the leading cause of injuries among older adults.
It is important to assess clients for fall risk on admission, whenever a change in physical or mental status occurs, on transfer, and before discharge.
Fall risk appraisal:
|
Risk Factor |
Points |
|
Age 60-69 years (1 point) 70-79 years (2 points) ≥80 years (3 points |
|
|
Fall History One fall within 6 months before admission (5 points) |
|
|
Elimination (Bowel and Urine) Incontinence (2 points) Urgency or frequency (2 points) Urgency/frequency and incontinence (4 points) |
|
|
Medications: Includes PCA/Opiates, Anticonvulsants, Antihypertensives, Diuretics, Hypnotics, Laxatives, Sedatives, and Psychotropics On one high fall–risk drug (3 points) On two or more high fall–risk drugs (5 points) Sedated procedure within past 24 hours (7 points) |
|
|
Patient Care Equipment: Any Equipment That Tethers Patient (e.g., IV Infusion, Chest Tube, Indwelling Catheters, SCDs) One present (1 point) Two present (2 points) 3 or more present (3 points) |
|
|
Mobility (Multi-select, Choose All That Apply and Add Points Together) Requires assistance or supervision for mobility, transfer, or ambulation (2 points) Unsteady gait (2 points) Visual or auditory impairment affecting mobility (2 points) |
|
|
Cognition (Multi-select, Choose All That Apply and Add Points Together) Altered awareness of immediate physical environment (1 point) Impulsive (2 points) Lack of understanding of one’s physical and cognitive limitations (4 points) |
|
|
TOTAL: Moderate risk = 6-13 total points High risk = >13 total points |
|
NB: The data obtained from the client’s fall risk appraisal will identify which clients require special nursing measures to prevent falls.
Fall Prevention strategies
1. Assessment
- Perform client injury risk appraisal and identify fall risks. Update status of fall risks daily and as needed on a nursing care plan.
- Assess effects of medications administered that increase risk of falling.
2. Client teaching
- On admission, orient clients to their surroundings and explain the call system.
- Instruct client and significant others on correct use of hospital equipment.
- Instruct client with risk for falls to call for assistance when ambulating or performing activities of daily living (ADL).
3. Environmental interventions:
- Keep the environment tidy; keep light cords from underfoot and furniture out of the way.
- Carefully assess the client’s ability to ambulate and transfer.
- Provide walking aids and assistance as required.
- Encourage the client to use the call light to request assistance. Ensure that the light is within easy reach.
- Place bedside tables and overbed tables near the bed or chair so that clients do not overreach and consequently lose their balance.
- Always keep hospital beds in the low position and wheels locked when not providing care so that clients can move in or out of bed easily.
- Encourage clients to use grab bars mounted in toilet and bathing areas and railings along corridors.
- Make sure nonskid bath mats are available in tubs and showers.
- Encourage the client to wear nonskid footwear.
- Closely supervise the clients at risk for falls, especially at night.
- Use individualized interventions (e.g., alarm sensitive to client position) rather than side rails for confused clients.
- Use mechanical or electronic ceiling lifts to transfer dependent clients.
4. Direct nursing care:
- Respond promptly to call lights and verbal requests for assistance.
- Provide assistance with ADL.
- Maintain close supervision by performing hourly safety assessments.
- Encourage significant others to stay with high-risk clients.
- Provide proper equipment for ambulation and elimination needs.
- Document in the client’s medical record.
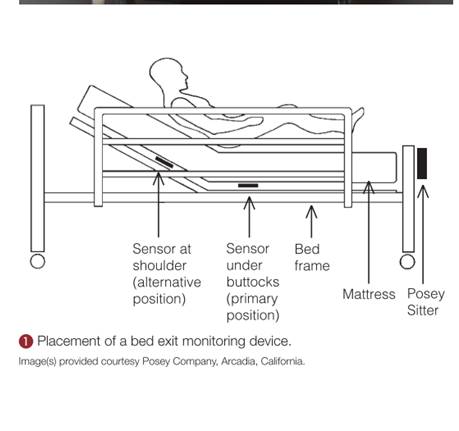
The alarm device is position sensitive; that is, when it approaches a near-vertical position (such as in walking, crawling, or kneeling as the client attempts to get out of bed), the audio alarm will be triggered.
Fire safety
Fire is a potential danger to all people in an institutional or a home environment. It occurs with the interaction of three elements: sufficient heat to ignite the fire, combustible material, and oxygen to support the fire.
Common causes of fire are:
- smoking in bed
- discarding cigarette butts in trash cans
- faulty electrical equipment
Immobilized or incapacitated clients are at increased risk during a fire.
Interventions aimed at reducing the risk of fire:
- Clearly marking fire exits
- Knowing locations of fire extinguishers and their operation
- Practicing fire evacuation procedures
- Posting emergency phone numbers by all telephones
- Keeping open spaces and hallways clear of clutter
- Checking electrical cords and outlets for exposed or damaged wires
- Reporting identified electrical hazards
- Educating clients about fire hazards
In the event of a fire:
Nursing interventions during a fire are directed at protecting the client from injury and containing the fire.
When smoke or fire is detected, two mnemonics can help the nurse remember the steps to follow. First is the RACE protocol:
- Rescue: If the area is safe to enter, protect and evacuate clients who are in immediate danger.
- Alarm: Pull the fire alarm and report the fire details and location to the hospital’s fire emergency extension.
- Confine: Contain the fire by closing the doors to all rooms and the fire doors at each entrance to the unit.
- Extinguish: Extinguish the fire. Use the appropriate type of fire extinguisher (see the PASS mnemonic) OR Evacuate the area if the fire is too large for a fire extinguisher.
The nurse follows the mnemonic PASS when using a fire extinguisher:
- Pull out the extinguisher’s safety pin.
- Aim the hose at the base of the fire.
- Squeeze or press the handle to discharge the material onto the fire.
- Sweep the hose from side to side across the base of the fire until the fire appears to be out.
Extinguishing the fire requires knowledge of three categories of fire, classified according to the type of material that is burning:
Poisoning
A poison is any substance that causes an alteration in the client’s health, such as injury or death, when inhaled, injected, ingested, or absorbed by the body.
Antidotes and treatments are available for some but not all types of poisonings.
Causes of poisonings are:
• Inadequate supervision of children
• Ingestion of household plants
• Improper storage of toxic substances
• Insect or snake bites
• Accidental ingestion of a toxic substance or medication overdose- due to failing eyesight/ impaired memory.
• Carbon monoxide poisoning
Carbon monoxide poisoning: Carbon monoxide (CO) is an odorless, colorless, tasteless gas that is very toxic. Exposure to CO can cause symptoms that include headaches, dizziness, weakness, nausea, vomiting, or loss of muscle control. Prolonged exposure to CO can lead to unconsciousness, brain damage, or death.
Preventing poisoning:
- Lock potentially toxic agents, in a cupboard, or attach special plastic hooks to the insides of cabinet doors to keep them securely closed.
- Do not let children watch you open the latches.
- Store medications in child-resistant containers.
- Do not take medications in front of children.
- Avoid storing toxic liquids or solids in food containers.
- Do not remove container labels or reuse empty containers to store different substances.
- Do not rely on cooking to destroy toxic chemicals in plants.
- Teach children never to eat any part of an unknown plant.
- Do not keep poisonous plants in the home, and avoid planting poisonous plants in the yar
- Place poison warning stickers designed for children on containers with toxic substances.
- Read and follow label directions on all products before using them.
- Keep syrup of ipecac on hand at all times.
- Display the phone number of the poison control center near or on all telephones in the home so that it is available to babysitters, family, and friends.
Interventions in accidental poisoning:
1. Assess for signs or symptoms of ingestion of harmful substance:
- nausea, vomiting
- foaming at the mouth, drooling
- difficulty breathing
- sweating, and lethargy.
2. Terminate exposure to the poison by having the person empty his or her mouth of pills, plant parts, or other material.
3. If poisoning is caused by skin or eye contact, irrigate the skin or eye with copious amounts of cool tap water for 15 to 20 minutes.
4. In the case of an inhalation exposure, safely remove the victim from the potentially dangerous environment.
5. Identify the type and amount of substance ingested to help determine the correct type and amount of antidote needed.
6. Call the local poison control center or the national toll-free poison control center number (1-800-222-1222) before attempting any intervention.
7. If the victim has collapsed or stopped breathing, call 911 for emergency transportation to the hospital. Initiate CPR if indicated until emergency personnel arrive.
8. Position the victim with head turned to the side to reduce risk for aspiration.
9. Never induce vomiting if the victim has ingested the following poisonous substances: lye, household cleaners, hair care products, grease or petroleum products, furniture polish, paint thinner, or kerosene.
10. Never induce vomiting in an unconscious or convulsing victim because vomiting increases risk for aspiration.
Electrical hazards
All electric equipment must be properly grounded. Grounding prongs offer a path of least resistance to stray electric currents.
The electric plug of grounded equipment has three prongs. The two short prongs transmit the power to the equipment. The third, longer prong is the grounding device, which carries short circuits or stray electric current.
Faulty equipment such as equipment with a frayed cord presents a danger of electric shock or may start a fire.
Actions to reduce electrical hazards:
- Check cords for fraying or other signs of damage before using an appliance. Do not use it if damage is apparent.
- Avoid overloading outlets and fuse boxes with too many appliances.
- Use only grounded outlets and plugs.
- Always pull a plug from the wall outlet by firmly grasping the plug and pulling it straight out. Pulling a plug by its cord can damage the cord and plug unit.
- Never use electric appliances near sinks, bathtubs, showers, or other wet areas, because water readily conducts electricity.
- Keep electric cords and appliances out of the reach of young children.
- Place protective covers over wall outlets to protect young children.
- Have all non-insulated wiring in the home altered to meet safety standards.
- Carefully read instructions before operating electric equipment. Clients who do not understand how to operate the equipment should seek advice.
- Always disconnect appliances before cleaning or repairing them.
- Unplug any appliance that has given a tingling sensation or shock and have an electrician evaluate it for stray current.
- Keep electric cords coiled or taped to the ground away from areas of traffic to prevent others from damaging the cords or tripping over them.
If a client receives an electrical shock:
- Turn off or remove the electric source before touching the client.
- The client’s pulse should be checked.
- If the client has no pulse, CPR should be initiated.
- If the client has a pulse, the nurse should assess vital signs, mental status, and skin integrity for burns.
- A prescribing practitioner should be notified of the event.
- The nurse should note points of entry and exit of electrical current to assess for potential complications.
