
Please set your exam date
Growth And Development In School-age Children
Study Questions
Practice Exercise 1
A hallmark of cognitive development in the school-age child is in what Piaget describes as concrete operations. In this stage the child:
Explanation
Piaget’s Concrete Operational Stage occurs between the ages of 7 and 11 years. During this stage, children develop the ability to think logically about concrete, tangible objects and events. They gain skills like conservation, classification, decentering, reversibility, and cause-and-effect reasoning.
Rationale for correct answer:
1. Using thought processes to experience events and actions accurately describes the concrete operational stage, where school-age children develop logical reasoning skills. They are no longer bound by intuition or perception alone. They begin to apply thought processes systematically and logically to concrete experiences, which enhances their learning, problem-solving, and understanding of rules and relationships.
Rationale for incorrect answers:
2. The child being unable to see things from another’s point of view describes egocentrism, typical of the preoperational stage (ages 2–7), not the concrete operational stage. By age 7, children generally begin to consider others’ perspectives.
3. Children in the concrete operational stage begin to understand that different people may see the same situation in different ways, showing the development of decentration and perspective-taking. Therefore, this is not characteristic of this stage.
4. Making judgments based on what he or she sees is a feature of preoperational thinking, where children focus on appearance rather than logic. School-age children start to use logical operations to assess situations rather than relying solely on visual impressions.
Take home points
- The Concrete Operational Stage (7–11 years) is defined by logical thinking about real-life situations.
- Children move from egocentric thought to understanding others' perspectives and objective reasoning.
- Conservation, reversibility, and cause-and-effect are key milestones.
- Nurses and educators should tailor communication strategies to support this stage’s growing cognitive complexity.
A school nurse in middle school (grades 6, 7, and 8) is preparing an outline for a sex education class. Which of these statements represent important concepts to be covered in discussing this topic with this age-group? Select all that apply
Explanation
Sex education for middle school-aged children (typically ages 11–14) should be developmentally appropriate, evidence-based, and sensitive to emotional and cultural factors. This is a critical period when adolescents experience puberty, increased curiosity, and peer influence. Effective education should foster accurate knowledge, promote healthy decision-making, and dispel misinformation.
Rationale for correct answers:
1. Consider separating the boys and girls into same-sex groups with a leader of the same sex: This can foster comfort and openness, particularly when discussing sensitive topics like puberty and reproduction. It may also reduce embarrassment and encourage more engagement in discussion.
2. Answer questions matter-of-factly and honestly and appropriate to the children’s level of understanding: Providing truthful, age-appropriate information builds trust and ensures students receive accurate knowledge. It helps reduce myths and prevents misinformation from peers or media.
5. Discuss common myths and misconceptions associated with sex and the reproductive process: Adolescents often hold inaccurate beliefs about sex, reproduction, and menstruation. Addressing these myths helps students make informed, healthy choices and reduces stigma or fear.
Rationale for incorrect answers:
3. Use vernacular or slang terms to describe human physiologic functions: Using slang can cause confusion and may appear unprofessional. Proper anatomical terms promote clear understanding and normalize the discussion of the human body.
4. Avoid discussing sexually transmitted diseases (STDs) in this age-group: STDs should definitely be discussed, as this age group is beginning to explore sexuality. Early education promotes awareness, prevention, and responsibility.
6. Avoid controversial topics such as birth control: Avoidance of such topics leaves children uninformed and unprepared. Discussing contraception within a factual, respectful, and developmentally appropriate context is critical for informed decision-making and public health.
Take home points
- Sex education for middle schoolers should be honest, age-appropriate, and respectful.
- Using same-gender groups can help ease discomfort during sensitive discussions.
- It is vital to address myths, STDs, and contraception early to build a foundation for informed decisions.
- Nurses play a key role in creating a safe, respectful learning environment that fosters healthy attitudes about sexuality.
According to Erikson, what psychosocial crisis are school-age children primarily working to resolve?
Explanation
Erik Erikson's theory of psychosocial development outlines stages that individuals pass through from infancy to adulthood, each marked by a central conflict that shapes personality and behavior. For school-age children, the focus shifts to productivity, competence, and social comparison as they navigate school, peers, and structured activities.
Rationale for correct answer:
4. Industry vs. Inferiority: During this stage, children strive to develop a sense of competence through academic achievement, skill-building, and positive reinforcement from adults and peers. Success leads to a feeling of industry (confidence in their abilities), while repeated failure or criticism may result in feelings of inferiority and low self-worth.
Rationale for incorrect answers:
1. Trust vs. Mistrust: This stage occurs during infancy (birth to ~18 months) and centers on developing a sense of trust in caregivers to meet basic needs.
2. Autonomy vs. Shame and Doubt: This is the toddler stage (~1–3 years), where children seek independence in tasks like feeding and toileting.
3. Initiative vs. Guilt: This applies to the preschool age (~3–5 years), where children begin asserting power through play and decision-making, with the risk of developing guilt if discouraged.
Take home points
- Industry vs. Inferiority is the key psychosocial task of school-age children, focused on building confidence and a sense of capability.
- Success in this stage promotes resilience, responsibility, and motivation.
- Supportive environments, at home, school, and in peer groups, are crucial to foster industry.
- Nurses and caregivers can help by praising effort, encouraging learning, and helping children cope with setbacks constructively.
What is the average annual weight gain for a school-age child?
Explanation
During the school-age years, children experience steady, gradual growth in both height and weight. Monitoring growth patterns helps identify nutritional status and developmental concerns. The expected annual weight gain is a reliable indicator of normal physical development during this stage.
Rationale for correct answer:
2. 2–3 kg (4.4–6.6 lbs): This is the typical average annual weight gain for a school-age child. It reflects the steady physical development characteristic of this age group, with a consistent rate that supports bone growth, muscle development, and organ maturation.
Rationale for incorrect answers:
1. 0.5–1 kg (1.1–2.2 lbs): This is below the expected range and could indicate undernutrition or other health issues if sustained.
3. 5–7 kg (11–15.4 lbs): This is more typical of growth spurts seen during adolescence, not the gradual growth of middle childhood.
4. 8–10 kg (17.6–22 lbs): This is excessive for a typical year in middle childhood and may raise concerns about obesity or other growth abnormalities if not associated with puberty.
Take home points
- The average school-age child gains 2–3 kg (4.4–6.6 lbs) per year.
- Growth during this period is steady and predictable, making it ideal for tracking long-term health.
- Significant deviations from this pattern may warrant evaluation for dietary, hormonal, or psychosocial issues.
- Nurses should provide anticipatory guidance on nutrition, physical activity, and regular growth monitoring.
Practice Exercise 2
Which of the following are reasons that stealing occurs in school-age children? Select all that apply
Explanation
Stealing in school-age children is often a behavioral signal tied to emotional, social, or developmental issues. At this stage, children are still developing their understanding of ownership, consequences, and right versus wrong.
Rationale for correct answers:
3. Low expectations of family/peers: Children who feel that their family or peers expect little from them may act out through dishonest behaviors such as stealing, feeling there’s little to lose or no accountability.
4. Lack of sense of propriety: Younger school-age children may not fully understand the concept of personal property, especially if such boundaries haven't been consistently taught.
5. Strong desire to own something: A child may steal out of envy or a powerful longing to possess something that peers have, especially when they believe it's the only way to obtain it.
Rationale for incorrect answers:
1. To escape punishment: This may occur in isolated situations but is not a primary developmental reason for stealing in this age group. It's more reactive than characteristic of school-age motives. However, children often lie and not to escape punishment.
2. High self-esteem: Children with high self-esteem are generally more secure and less likely to engage in dishonest behavior for validation or attention. Stealing is more common in children with low self-worth or unmet emotional needs.
Take home points
- Stealing in school-age children can stem from unclear moral understanding, emotional insecurity, or social comparison.
- Positive expectations and consistent guidance from adults help reduce these behaviors.
- Teaching children about ownership, respect for others' property, and empathy builds long-term ethical behavior.
- Interventions should focus on support, understanding, and teaching, not just punishment.
What does the concept of "goodness of fit" in relation to temperament refer to?
Explanation
During middle childhood, children experience significant emotional, social, and behavioral growth. A key aspect of this development is temperament, the child’s natural style of interacting with the world.
Rationale for correct answer:
2. Goodness of fit is a concept in developmental psychology that refers to how well a child’s temperament matches or is supported by their environment, especially parenting style and other external expectations. When there is a good fit, the child's development is supported, and behaviors are more easily managed. A poor fit can lead to increased conflict, stress, or behavioral problems, not because of the temperament itself, but because of a mismatch between what the child needs and how the environment responds.
Rationale for incorrect answers:
1. The physical fitness level of the child is not related to temperament. “Goodness of fit” is a psychosocial and behavioral concept, not physical fitness.
3. The child's ability to adapt to new situations easily may be a trait of a child with an easy temperament, but it’s not the definition of “goodness of fit.” That term refers to the match between the child and the environment.
4. The compatibility of the child's diet with their activity level relates to nutrition and health, not temperament or psychological development.
Take home points
- Goodness of fit supports healthy emotional and behavioral development.
- Caregivers and teachers can foster this by adjusting expectations and interactions to align with the child’s individual temperament.
- Recognizing a child’s unique needs helps reduce conflict and promote resilience.
Which of the following are common fears experienced by school-age children? Select all that apply
Explanation
School-age children experience a shift in their fears from the imaginary and fantastical, common in early childhood, to more realistic and socially based concerns. These fears often relate to performance, acceptance, and safety, reflecting their growing awareness of the world and their place within it.
Rationale for correct answers:
2. Fear of academic failure becomes prominent in this stage as children begin to internalize expectations from teachers, parents, and themselves. Anxiety over performance in tests is a common and developmentally appropriate fear.
3. Although more typical of early childhood, fear of being alone can persist in school-age children, particularly if it’s connected to safety concerns or emotional insecurity.
4. As peer relationships grow in importance, fear of being excluded or ridiculed becomes a significant emotional stressor. Social acceptance is a key developmental task in this age group.
Rationale for incorrect answers:
1. Monsters under the bed is more typical of preschool-aged children who have difficulty distinguishing fantasy from reality. School-age children tend to grow out of these types of imaginary fears.
5. Attachment to transitional objects like stuffed animals is common in younger children. While a school-age child may still value such objects, the emotional fear associated with losing them is less intense and less developmentally typical at this stage.
Take home points
- Common fears in school-age children shift toward real-life concerns such as academic performance, peer relationships, and personal safety.
- Understanding these fears allows caregivers and educators to provide reassurance, build coping skills, and support emotional development.
- Dismissing or minimizing these fears can increase anxiety; instead, validate the child's feelings and help them problem-solve.
- Encouraging open communication and fostering a safe, supportive environment helps children build resilience.
A school-age child consistently tells elaborate stories that are not true, often to avoid getting in trouble. What is the most appropriate initial nursing approach to this dishonest behavior?
Explanation
Dishonest behavior in school-age children often arises as they experiment with social boundaries, fear punishment, or seek attention. Developmentally, they are beginning to understand moral concepts but still require guidance in applying them consistently.
Rationale for correct answer:
3. Calmly discuss the behavior, explore the underlying reasons, and emphasize the importance of honesty: This approach acknowledges the behavior without shaming the child. It opens the door to understanding emotional drivers like fear of failure, low self-esteem, or seeking approval. The nurse or caregiver models calm and honest communication, promoting trust and reinforcing honesty as a value.
Rationale for incorrect answers:
1. Isolation is punitive and may cause further emotional harm or increase deceptive behavior as a coping strategy. It does not address the root cause or promote learning.
2. Harsh punishment can increase fear and dishonesty. It may suppress the behavior temporarily but fails to help the child internalize the value of truthfulness.
4. While some dishonesty is developmentally typical, ignoring consistent lying misses a critical opportunity for guidance and character development.
Take home points
- Consistent lying in school-age children often signals emotional needs, fear, or gaps in moral understanding.
- Supportive, non-punitive conversations help children reflect on their behavior and choose honesty.
- Teaching honesty should involve empathy, role modeling, and helping children handle mistakes constructively.
- Ignoring or punishing dishonesty without discussion can reinforce the behavior or harm the child’s self-concept.
Regarding latchkey children, which of the following are important safety considerations for parents to implement? Select all that apply
Explanation
Latchkey children, those who return home from school to an empty house due to their parents’ work schedule, require extra safety planning and emotional support. Parents must take proactive steps to ensure their child’s safety, emotional well-being, and decision-making capabilities while unsupervised.
Rationale for correct answers:
2. Establishing clear rules for visitors to the home: It's essential that children understand and follow safety rules about allowing others into the home when alone, which reduces the risk of harm from strangers or unsafe situations.
3. Ensuring the child has an emergency plan and knows who to contact: Children need to know what to do in case of fire, injury, or feeling unsafe. This includes knowing emergency phone numbers and having basic problem-solving skills.
5. Providing a list of "safe" adults the child can contact for help: Trusted adults such as neighbors, relatives, or family friends can provide a lifeline in emergencies or if the child feels frightened or confused.
Rationale for incorrect answers:
1. Allowing unlimited unsupervised online access: This increases the risk of exposure to inappropriate content, cyberbullying, and online predators. Parental controls and screen time limits should be established.
5. Discouraging participation in after-school programs: On the contrary, structured after-school programs provide supervision, socialization, and enrichment, which help reduce the risks associated with being home alone.
Take home points
- Latchkey children need clear safety guidelines, reliable communication plans, and emotional reassurance.
- Parents should educate their children on safe behaviors and provide resources for emergencies.
- Encouraging safe after-school activities and setting digital boundaries enhance safety and well-being.
- Empowering children with rules, plans, and trusted contacts fosters independence with security.
Practice Exercise 3
School-age children are prone to accidental injury primarily because of:
Explanation
School-age children (ages 6–12) are at increased risk for accidental injuries due to their growing independence, curiosity, and desire for peer approval. As children become more socially active, they may experiment with physical challenges, engage in unsupervised play, and participate in risky activities to fit in or gain status among peers.
Rationale for correct answer:
1. As school-age children grow, they often seek peer acceptance, which can lead them to take unsafe risks, such as climbing too high, biking without helmets, or engaging in dares. These behaviors are not always well thought out due to developing judgment and impulse control. Peer influence is a major contributor to accidental injuries in this age group.
Rationale for incorrect answers:
2. Physical awkwardness and clumsiness is more characteristic of toddlers and early preschoolers, not school-age children who typically have improved coordination. While minor accidents still occur, physical development is generally steady and refined by this stage.
3. While supervision remains important, school-age children often play independently or with peers, especially in school and community settings. Injury risk is more closely tied to behavioral factors and social influence than parental neglect.
4. Attempts to impress members of the opposite sex is more typical during adolescence, when romantic interests begin to develop. In younger school-age children, motivation to impress is usually directed toward same-sex peers or involves general attention-seeking, not romantic appeal.
Take home points
- Peer pressure and a desire to fit in are major contributors to injury in school-age children.
- Children may underestimate danger or overestimate their abilities during play or sports.
- Injury prevention efforts should focus on teaching safety rules, encouraging protective gear use, and fostering environments that support safe risk-taking.
- Nurses and caregivers should provide age-appropriate education about safety while still promoting autonomy and exploration.
A nurse is providing health promotion education to a 10-year-old child during a well-child clinic visit.
Which of the following is an appropriate patientcare goal for the teaching session? The child will:
Explanation
Health promotion for school-age children includes education on nutrition, physical activity, dental hygiene, injury prevention, and immunizations. At this stage, children begin to take more personal responsibility for their health behaviors, and nurses play a crucial role in reinforcing developmentally appropriate preventive practices during routine visits.
Rationale for correct answer:
1. Dental hygiene is a key area of health promotion for 10-year-olds. Brushing twice daily with fluoride toothpaste helps prevent cavities and gum disease, which are common issues in this age group. This goal is age-appropriate, promotes daily self-care, and aligns with recommended guidelines from dental associations.
Rationale for incorrect answers:
2. The first dose of meningococcal conjugate vaccine (MenACWY) is recommended at age 11–12, not at age 10. Therefore, this is premature for a 10-year-old child during a routine visit.
3. While swimming lessons are encouraged earlier in childhood, this statement is not a measurable or time-specific goal for a 10-year-old. It’s too vague and lacks the clarity needed for an actionable teaching objective during a clinic visit.
4. Bicyclists should ride on the right-hand side of the road, going with the flow of traffic, not against it. Teaching otherwise increases the risk of injury.
Take home points
- Daily dental hygiene using fluoride toothpaste is essential and age-appropriate for school-age children.
- Meningococcal vaccination begins at age 11–12, not 10.
- Safety education should include correct bicycle riding practices, including riding with traffic.
- Health goals for children should be specific, measurable, realistic, and developmentally appropriate.
How many hours of sleep are generally recommended for school-age children per night?
Explanation
Sleep is essential for the healthy growth, development, and functioning of school-age children. It supports cognitive performance, emotional regulation, immune function, and overall well-being. Sleep deprivation in this age group can lead to behavioral problems, academic difficulties, and health issues.
Rationale for correct answer:
3. According to the American Academy of Sleep Medicine and the CDC, school-age children should get 9 to 12 hours of sleep per 24 hours to function optimally. This range accounts for individual variability while ensuring enough rest to support development and daily functioning.
Rationale for incorrect answers:
1. 6–8 hours is insufficient for school-age children and more appropriate for adults. Chronic sleep deprivation at this age can negatively affect physical and mental health.
2. 8–9 hours still falls short of the lower end of the recommended range. Some children may cope, but it is generally not enough for optimal growth and learning.
4. 12–14 hours is typically excessive for school-age children and more consistent with the needs of toddlers and preschoolers.
Take home points
- School-age children need 9–12 hours of sleep nightly to support healthy development and daily functioning.
- Consistent bedtime routines and limiting screen time before bed help promote adequate sleep.
- Parents and caregivers should monitor for signs of sleep deprivation such as irritability, difficulty focusing, or falling asleep during the day.
- Sleep education is a key part of promoting academic success and emotional stability in this age group.
What is the nurse's role in injury prevention for school-age children? Select all that apply
Explanation
Injury prevention is a key component of pediatric nursing care, particularly for school-age children who are increasingly independent and physically active. Nurses play a vital role in equipping both children and caregivers with the knowledge and tools needed to stay safe across various environments, home, school, and the community.
Rationale for correct answers:
2. Providing anticipatory guidance on age-appropriate safety measures: Nurses educate families about potential risks based on developmental stage, such as bicycle safety, pedestrian rules, water safety, and appropriate supervision.
3. Educating on proper use of safety equipment such as helmets: Reinforcing the consistent use of safety gear helps prevent serious injuries. Nurses can demonstrate correct usage and explain its importance.
4. Advocating for community safety initiatives: Nurses can influence policies and support programs such as safe playgrounds, crossing guards, and injury-prevention campaigns to improve child safety at a broader level.
Rationale for incorrect answers:
1. Allowing children to learn from their own mistakes, even if it results in injury: While natural consequences can be instructive, nurses must prioritize prevention. Injury is not an acceptable teaching tool when it can be avoided through proactive education and supervision.
5. Minimizing discussions about risky behaviors to avoid scaring children: Age-appropriate education about risky behaviors is essential. Avoiding the topic deprives children of the opportunity to make informed, safe decisions.
Take home points
- Nurses are essential in promoting safety for school-age children through education, anticipatory guidance, and advocacy.
- Injury prevention should be proactive and developmentally appropriate, not reactive.
- Teaching children about risks and safety empowers them to make better choices.
- Community involvement and proper safety gear use significantly reduce injury rates.
A nurse is providing education to parents about screen time for their school-age child. What is the most appropriate recommendation regarding recreational screen time?
Explanation
As children grow into the school-age years, screen use becomes a routine part of daily life for education, entertainment, and social connection. However, excessive recreational screen time can negatively impact sleep, physical activity, mental health, and academic performance. Nurses guide families on establishing healthy digital habits.
Rationale for correct answer:
2. Limit recreational screen time to 1–2 hours per day: This recommendation aligns with guidelines from the American Academy of Pediatrics (AAP), which advises parents to limit non-educational/recreational screen time to no more than 1–2 hours per day for school-age children. This promotes balance between screen use and essential activities like physical play, homework, family interaction, and sleep.
Rationale for incorrect answers:
1. Encourage unlimited screen time for educational purposes: Even educational content should be monitored and balanced with other developmental needs like physical activity, sleep, and in-person social interactions.
3. Allow 3–4 hours of screen time on weekdays and more on weekends: This exceeds recommended limits and increases risks for obesity, behavioral issues, and sleep disturbances.
4. Screen time should be completely eliminated for this age group: This is unrealistic and unnecessary. Screens are a part of modern life, and the goal is moderation and responsible use, not elimination.
Take home points
- School-age children should have no more than 1–2 hours of recreational screen time daily, with an emphasis on quality content and supervision.
- Families should create screen-free zones (e.g., bedrooms, dining areas) and model healthy screen habits.
- Balance is key, screen time should not replace physical activity, sleep, or meaningful family and peer interaction.
- Nurses play a crucial role in helping families set consistent screen time limits and media-use plans.
Comprehensive Questions
Which of the following cognitive abilities typically emerge during Piaget's concrete operational stage? Select all that apply
Explanation
According to Jean Piaget, the concrete operational stage occurs approximately between ages 7 and 11. During this stage, school-age children develop logical thinking skills but are still limited to reasoning about concrete, tangible concepts. Their thinking becomes more organized and flexible, laying the groundwork for more complex cognitive development.
Rationale for correct answers:
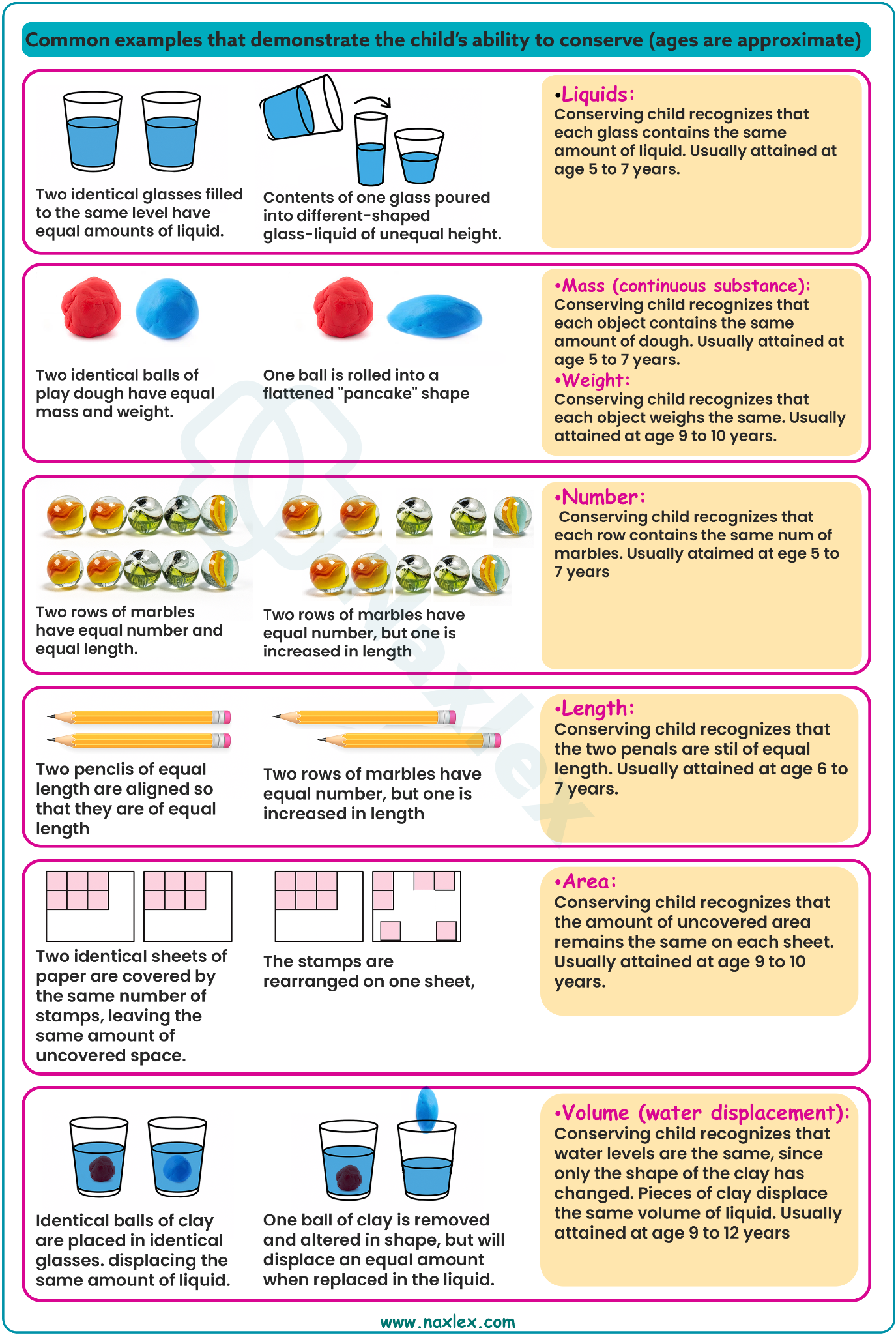
2. Conservation: This is the understanding that quantity remains the same even when its shape or appearance changes (e.g., liquid in different containers). It's a hallmark achievement of the concrete operational stage.
4. Classification: Children begin to understand how to group objects based on shared characteristics and recognize relationships among categories (e.g., sorting animals by type or tools by function).
5. Reversibility: The ability to mentally reverse actions or understand that something can return to its original state (e.g., realizing that 3 + 2 = 5 means 5 – 2 = 3) develops during this stage.
Rationale for incorrect answers:
1. Abstract thinking: This develops in the next stage, the formal operational stage (typically beginning around age 12). Abstract thinking involves reasoning about hypothetical situations, symbolism, and concepts without physical references.
4. Egocentrism: Egocentric thinking, where the child has difficulty seeing things from others’ perspectives, is characteristic of the preoperational stage. In the concrete operational stage, children begin to decenter and consider other viewpoints.
Take home points
- The concrete operational stage marks a shift toward logical, organized thinking tied to concrete situations.
- Key abilities gained include conservation, classification, and reversibility.
- Children become less egocentric and more capable of perspective-taking.
- Nurses and educators should support learning with hands-on activities and real-life examples during this stage.
Characteristics of bullying include:
Explanation
Bullying refers to intentional, repeated aggressive behavior that involves a power imbalance between the bully and the victim. It can be physical, verbal, emotional, or social, and typically occurs in school-aged children. Bullying negatively affects both the victim’s and the perpetrator’s emotional development, academic success, and mental health. Early recognition and intervention are key.
Rationale for correct answer:
2. This definition aligns with the widely accepted criteria for bullying: intentional, repetitive, and involving an imbalance of power. Whether through name-calling, exclusion, hitting, or cyber aggression, the behavior aims to intimidate or hurt another child over time.
Rationale for incorrect answers:
1. Unintentional harm may occur during normal play or social learning, but it does not qualify as bullying, which must be deliberate and repeated.
3. While peer dynamics can influence bullying, it is not primarily a strategy for social inclusion. In fact, bullying is often an attempt to dominate or control, not to be accepted.
4. Bullying can be a sign of emotional or behavioral issues, but it is not diagnostic of a personality disorder. Not all children who bully develop psychiatric disorders later in life.
Take home points
- Bullying is intentional, repeated, and harmful behavior involving a power imbalance.
- It can be physical, verbal, social, or emotional in nature.
- Bullying is not a normal part of social development and should always be addressed early.
- Nurses, teachers, and caregivers must identify signs of bullying, support victims, and guide bullies toward healthier social behavior.
In terms of social development, the school-age child does which of the following? Select all that apply
Explanation
Social development in the school-age child (ages 6–12) is marked by a shift from family-focused relationships to increasing interest in peer groups and the outside world. Children at this stage seek approval from peers, form friendships often with those of the same gender, and begin to value group norms, fairness, and belonging. Peer groups play a critical role in developing identity, self-esteem, and social skills.
Rationale for correct answers:
1. School-age children begin to develop relationships with teachers, classmates, and community members. They become more independent, socially curious, and eager to explore beyond the immediate family unit.
3. At this age, children tend to form same-gender peer groups, such as sports teams or clubs. This is a developmentally normal way to explore identity and friendship within a comfortable social framework.
5. Friendships during this period are often close and emotionally significant, commonly formed between children of the same gender. These relationships support emotional development, communication skills, and empathy.
Rationale for incorrect answers:
2. Interest in the opposite sex typically becomes more apparent during adolescence, not in early or middle childhood. School-age children often show a preference for same-gender interactions and may even view the opposite gender with disinterest or aversion.
4. School-age children usually strive to fit in with peers, not to stand out. They often conform to group norms to gain acceptance and avoid rejection. Standing out may cause discomfort or anxiety during this stage.
Take home points
- Peer relationships are central to the social development of school-age children.
- Children often prefer same-sex friends and clubs, helping to form a sense of belonging and identity.
- School-age children value group approval and tend to conform to group norms.
- Nurses and educators should encourage positive peer interaction and support the development of healthy friendships during this critical stage.
The nurse is assessing a 12-year-old boy during a well-child clinic visit. Which of the following findings would the nurse expect to see?
Explanation
Physical development in 12-year-old children varies, especially as they enter puberty. Growth spurts are common, with noticeable increases in height and weight, and physiological changes like secondary sexual characteristics begin. Monitoring growth patterns, vital signs, and dental development helps identify whether a child is progressing along a healthy developmental trajectory.
Rationale for correct answer:
2. Height increase of 2 in. (5.5 cm) since the last visit 1 year previously is within the normal range for preadolescent boys. On average, children at this age grow about 2–2.5 inches (5–6.5 cm) per year until they hit their adolescent growth spurt. A 2-inch gain in one year is typical and expected in a 12-year-old boy not yet in full puberty.
Rationale for incorrect answers:
1. Weight gain of 2¼ lb (1 kg) since the last visit 1 year previously is insufficient for this age. Normal weight gain in a 12-year-old is typically about 4–7 lb (1.8–3.2 kg) per year, with more if the child has entered puberty. A 1 kg gain may suggest poor nutrition, chronic illness, or growth concerns.
3. By age 12, children typically have most or all of their 28 permanent teeth (excluding third molars/wisdom teeth). Having only 20 permanent teeth is more consistent with younger school-aged children who still retain primary teeth.
4. Heart rate 124 is elevated for a 12-year-old at rest. The normal resting heart rate for this age group ranges from 70 to 110 beats per minute. A rate of 124 could indicate anxiety, fever, dehydration, or cardiac abnormality and warrants further evaluation if persistent.
Take home points
- Expected annual height gain for a 12-year-old is around 2 inches (5–6 cm).
- Normal weight gain is typically 4–7 lb (1.8–3.2 kg) annually unless a pubertal growth spurt is underway.
- By age 12, most children should have nearly all of their 28 permanent teeth.
- Resting heart rate in a healthy 12-year-old should be between 70 and 110 bpm; sustained elevation should be evaluated.
A nurse is providing health promotion education to the parent of a 6-year-old child during a well-child clinic visit. Which of the following statements by the parent would indicate that further teaching is needed?
Explanation
Health promotion for 6-year-old children includes reinforcing healthy habits related to sleep, physical activity, oral hygiene, discipline, and screen time. At this age, children thrive on consistency, boundaries, and positive reinforcement that supports healthy development. Nurses educate parents on promoting wellness while avoiding habits that can interfere with routines and behavior regulation.
Rationale for correct answer:
3. “I let my child watch television for a half hour in bed after bedtime when my child has been really good.” Television use close to or after bedtime can disrupt sleep patterns, affect melatonin production, and lead to poor sleep hygiene. Using screen time as a reward can also inadvertently reinforce poor bedtime behavior.
Rationale for incorrect answers:
1. “Eating raisins and jelly beans is worse for my child’s teeth than is drinking sugary soft drinks.” Sticky foods like raisins and jelly beans adhere to teeth longer than liquids, increasing the risk for dental caries. The parent demonstrates an understanding of how food texture impacts oral health.
2. “My child loves to kick balls around the yard, so I think I will enroll my child in a soccer camp.” Organized sports help children develop motor skills, teamwork, and discipline, making this a positive parenting decision.
4. “My child took a pack of gum from the local store the other day, so I made my child give it back to the manager.” This demonstrates effective discipline and teaching about honesty and consequences. Returning the gum reinforces moral development, which is appropriate for this developmental stage.
Take home points
- Screen time should be limited and not used as a bedtime reward, as it can disrupt healthy sleep habits.
- Sticky sugary foods pose a higher risk to dental health than sugary drinks.
- Structured physical activities like soccer are beneficial for motor and social development.
- Parents should use developmentally appropriate discipline to teach values like honesty and responsibility.
The parent of a 7-year-old child telephones the nurse at the child’s school and states, “My child has had a stomachache and headache every morning this week. Is there a virus going around the school?”
Which of the following responses would be appropriate for the nurse to make at this time? Select all that apply
Explanation
School-age children may report physical symptoms such as headache, stomachache that occur regularly in the absence of clinical findings. These can be a manifestation of emotional distress, such as school phobia, bullying, separation anxiety, or academic pressure.
Rationale for correct answers:
1. “Has your child ever expressed any concerns about school?” This helps assess for school-related anxiety, fear of failure, teacher conflict, or social challenges, which may manifest as somatic complaints.
2. “Does your child seem to feel better once your child has missed school?” This question screens for school avoidance behavior, where symptoms improve when the stressor is removed such as staying home.
3. “Has your child had any problems with any of the other children in school?” Bullying or peer conflicts are common triggers of psychosomatic symptoms in school-age children.
4. “I would recommend taking your child to the child’s primary health-care provider for a complete assessment.” Always rule out organic causes first before attributing symptoms to emotional or psychological issues.
Rationale for incorrect answer:
5. “Unless your child is exhibiting additional symptoms like a fever or a rash, I would recommend that the child return to school.” Although a fever or rash could indicate illness, the pattern of recurring complaints without proper evaluation warrants further investigation. Dismissing the symptoms could delay addressing underlying causes such as anxiety or bullying.
Take home points
- Somatic complaints in children may reflect underlying emotional distress, especially when no physical illness is found.
- Ask open-ended questions to explore potential school-related issues such as bullying or anxiety.
- Always recommend a medical evaluation first to rule out physical illness before considering psychosocial causes.
- Avoid dismissing symptoms as trivial without a thorough assessment.
The nurse has confirmed that a 9-year-old child understands the concept of conservation when the child makes which of the following statements?
Explanation
Conservation is a key cognitive milestone in Piaget’s Concrete Operational Stage (ages 7 to 11 years). It refers to the understanding that quantity remains the same despite changes in shape or appearance. Children who grasp this can tell that mass, volume, or number doesn’t change just because the container or form has changed.
Rationale for correct answer:
1. “There is the same amount of clay in a snake made out of a ball of clay than there was when it
was a ball.” This child demonstrates an understanding that changing the shape of an object does not change its amount, which is the essence of conservation. Recognizing that a ball and a snake-shaped piece of clay contain the same amount of clay indicates cognitive development consistent with Piaget’s stage of concrete operations.
Rationale for incorrect answers:
2. “I don’t get as tired when I ride up in an elevator than I do when I walk up a whole flight of
stairs.” This reflects an understanding of physical exertion or energy use, not conservation. It’s about perceived effort, not quantity or matter.
3. “I’d rather read books and play video games than to play baseball or soccer.” This shows personal preference for activities, which is unrelated to the concept of conservation or cognitive reasoning about mass or volume.
4. “I try to get my homework done as soon as I get home from school.” This is a behavioral statement about responsibility or routine and does not demonstrate the cognitive skill of conservation.
Take home points
- Conservation is the understanding that quantity remains the same despite changes in shape, position, or appearance.
- It typically emerges during the Concrete Operational Stage (ages 7–11), per Piaget's theory of cognitive development.
- Assessing a child’s understanding of conservation involves using familiar materials (like clay, liquid, or objects) in tasks that change appearance but not quantity.
A nurse is interviewing a group of 4th grade children. It would be appropriate for the nurse to diagnose the child who made which of the following statements as at “Risk for Altered Coping related to poor psychosocial development”?
Explanation
During the school-age years (6–12 years), children experience critical developmental milestones related to self-esteem, competence, and peer relationships. According to Erikson’s stage of Industry vs. Inferiority, children strive to master tasks, gain approval, and develop confidence through accomplishments in school and social activities.
Rationale for correct answer:
3. “I strike out every time I bat when we play soft ball in gym class.” This statement reflects repeated failure, negative self-perception, and potential feelings of inferiority, indicating a risk for altered coping. It suggests the child may not be developing the confidence and resilience expected at this stage.
Rationale for incorrect answers:
1. “My teacher put the picture I drew up on the board.” This reflects positive recognition and encouragement, which foster confidence and healthy development.
2. “I made a goal during our soccer game yesterday.” Indicates success, peer interaction, and a sense of achievement, all markers of healthy psychosocial growth.
4. “My teacher let me read out loud last week and again this week.” Shows that the child is entrusted with tasks and may feel valued and competent, which supports effective coping.
Take home points
- School-age children (like 4th graders) are in Erikson’s Industry vs. Inferiority stage.
- Feelings of competence promote healthy psychosocial development, while persistent failure can result in poor coping skills.
- Nurses should identify signs of low self-esteem, negative self-talk, or repeated perceived failure as potential red flags.
- Early support and interventions help children build resilience, self-worth, and effective coping strategies.
A child’s 3rd grade teacher informs the parents, “Your child’s handwriting is quite poor. It is important that your child practice skills that might improve the handwriting.” Which of the following activities could the parents encourage the child to perform? Select all that apply
Explanation
Fine motor skills are essential for tasks such as handwriting, drawing, and self-care. In school-age children (typically 6–12 years old), these skills continue to mature through purposeful activities that involve hand-eye coordination, manual dexterity, and precision movement.
Rationale for correct answers:
2. Playing a musical instrument such as a piano or a violin enhances fine finger movements, timing, and coordination, which are foundational for improved handwriting.
3. Building a model such as a house, airplane, or LEGO structure requires detailed finger work and spatial awareness, promoting fine motor development and problem-solving.
5. Drawing and painting require controlled wrist, finger, and hand movements, which directly support pencil grip, pressure control, and shape formation used in writing.
Rationale for incorrect answers:
1. While throwing a ball back and forth improves gross motor coordination, it primarily engages large muscle groups of the arms and shoulders, not the fine motor control needed for writing improvement.
4. Dancing enhances gross motor skills, rhythm, and balance, but it does not significantly target hand or finger dexterity relevant to handwriting.
Take home points
- Handwriting difficulties in school-age children often reflect underdeveloped fine motor skills.
- Activities that involve precise hand and finger movements, such as drawing or building, can enhance handwriting.
- Gross motor activities, while beneficial for overall development, are less effective in improving handwriting.
- Encouraging regular, enjoyable fine motor practice supports classroom performance and self-confidence.
The nurse working in a local school district is developing the curriculum for a new sex education program for the 2nd grade students. Which of the following content would be appropriate to include in the class?
Explanation
Sex education for early school-age children, such as 2nd graders (typically 7–8 years old), should be developmentally appropriate, focusing on basic anatomy, body awareness, personal boundaries, and safety. Education at this stage lays the foundation for healthy attitudes about the body and respectful relationships.
Rationale for correct answer:
1. Teaching the names of external genitalia helps children understand their bodies in a scientific, respectful way. This supports healthy development and is part of most evidence-based, age-appropriate sex education curricula for early elementary students. It also empowers children to communicate clearly in cases of abuse or discomfort.
Rationale for incorrect answers:
2. Listing names of the registered sex offenders living in the school district is inappropriate and potentially frightening for young children. Discussions about safety should be general and empowering, focusing on stranger danger, body autonomy, and safe vs. unsafe touch, rather than introducing criminal records.
3. At this age, the focus should be on friendship, kindness, and body awareness, not sexual orientation or relationships. These topics may be introduced at older ages when children can better understand complex social and emotional content.
4. This involves complex medical information about disease transmission that exceeds the cognitive and emotional capacity of a 2nd-grade audience. Health and hygiene topics may be introduced, but disease etiology is better suited for older students.
Take home points
- Sex education for 2nd graders should focus on basic anatomy, personal safety, and respecting personal space.
- Using correct anatomical terms for body parts helps reduce confusion, shame, and vulnerability to abuse.
- Avoid complex, frightening, or developmentally advanced content such as disease etiology or sexual relationships.
- Nurses and educators should ensure sex education aligns with age-appropriate, culturally sensitive, and evidence-based standards.
The nurse is providing prehospital admission education to a 9-year-old child and family.
Which of the following methods would be most appropriate for the nurse to utilize during the teaching session?
Explanation
According to Piaget’s cognitive development theory, children in this stage are in the concrete operational phase, meaning they understand logical sequences and real-life scenarios but may still struggle with abstract reasoning. Effective preparation helps reduce fear and anxiety, encourages cooperation, and fosters a sense of control during hospitalization.
Rationale for correct answer:
4. Taking a tour of the pediatric unit helps a school-age child form realistic expectations about the hospital experience. It allows for hands-on learning, which is appropriate for this developmental stage, and fosters a sense of security and trust by introducing the care team.
Rationale for incorrect answers:
1. Speaking with another child who was hospitalized may not be helpful or reliable. The discharged child's experience may not apply and could unintentionally increase anxiety by sharing negative or confusing stories.
2. Verbal explanation alone is too abstract for many children at this age. Without visual or tangible support, it may not effectively prepare the child or address specific fears.
3. Playing a board game about hospitals may help with general understanding, but it lacks the personalized, concrete exposure that a hospital tour provides. It may also oversimplify or misrepresent what the child will actually experience.
Take home points
- School-age children benefit from concrete, hands-on teaching methods that allow for real-life experience and logical understanding.
- Hospital tours reduce anxiety by making the unknown environment familiar.
- Relying solely on verbal instruction or peer stories may be less effective or even counterproductive.
- Nurses should aim to engage children actively and address fears using age-appropriate, experiential approaches.
During a well-child visit, the nurse asks the parents and their 11-year-old child about safety issues. In which of the following situations should the nurse provide disease prevention education?
Explanation
Injury prevention and disease prevention are both important components of well-child care. Nurses must assess behaviors that could lead to cumulative health risks, such as sun exposure, and provide anticipatory guidance to promote long-term wellness. Proper protective behaviors reduce risk for both accidental injuries and preventable diseases such as skin cancer.
Rationale for correct answer:
1. Applying sunscreen every 4 hours is inadequate protection during prolonged sun exposure. The child and parents should be educated on applying broad-spectrum SPF 30+ sunscreen at least every 2 hours and after water exposure. Early education supports lifelong skin health and reduces the risk of melanoma and sun damage.
Rationale for incorrect answers:
2. Sitting in the backseat in a car restraint system is an appropriate safety measure for an 11-year-old and does not indicate the need for additional education at this time.
3. Wearing proper body and head protection while rollerblading is a positive safety behavior, indicating that no immediate safety intervention is necessary.
4. Using 2 oven mitts and being assisted by a parent during oven use demonstrates adequate supervision and precaution, which is developmentally appropriate and safe.
Take home points
- Disease prevention education should be provided when current practices are insufficient or incomplete, even if partially protective.
- Sun safety is a key area of education during well-child visits due to the cumulative effects of UV exposure.
- Reinforce protective behaviors (helmets, seat belts, adult supervision) and correct any gaps in disease prevention practices.
- Nurses should use well-child visits to guide families toward evidence-based safety and prevention behaviors.
The successful resolution of developmental tasks for the school-age child, according to Erikson, would be identified by:
Explanation
Erik Erikson's psychosocial theory outlines a series of developmental stages that individuals progress through across the lifespan. For school-age children, the relevant stage is Industry vs. Inferiority. The main developmental task during this stage is to develop a sense of competence and self-worth through success in school, sports, hobbies, and peer interactions.
Rationale for correct answer:
2. Developing a sense of worth and competence directly reflects the successful resolution of the Industry vs. Inferiority stage, in which children gain confidence in their ability to be productive and valued contributors in school and social settings.
Rationale for incorrect answers:
2. When school-age children experience support and success, they develop industry, which means they feel capable, confident, and valued. This sense of competence promotes positive self-esteem and motivation, key indicators of healthy psychosocial development at this age.
Rationale for incorrect answers:
1. While repetition can support skill-building, this alone does not reflect Erikson’s psychosocial resolution. Without a sense of mastery or competence, repetition does not necessarily foster development.
3. Using fantasy and magical thinking to cope with problems is more characteristic of preschool-age children in Erikson’s Initiative vs. Guilt stage and reflects immature coping strategies, not appropriate for school-age development.
4. Developing a sense of trust belongs to the Trust vs. Mistrust stage, which occurs in infancy (birth to 1 year). It is not the relevant developmental task for a school-age child.
Take home points
- School-age children (6–12 years) are in Erikson’s Industry vs. Inferiority stage.
- Success and encouragement lead to a sense of worth and competence, the desired outcome of this stage.
- Failure without support can lead to feelings of inferiority, negatively impacting self-esteem.
- Nurses and caregivers can promote healthy development by providing praise, responsibility, and opportunities to succeed.
Which activities will promote weight loss in an obese school-age child? Select all that apply
Explanation
Healthy weight management in school-age children involves the entire family, structured routines, regular physical activity, and age-appropriate involvement in lifestyle changes. Encouraging healthy behaviors, not restrictive diets, is the goal.
Rationale for correct answers:
2. Role modeling by family: Children learn by example. When family members eat nutritious meals, exercise, and avoid sedentary behaviors, children are more likely to adopt those habits too.
3. Becoming active in sports: Regular physical activity helps increase energy expenditure, improve mood, and support weight management in a fun and social environment.
5. Involving child in meal planning and grocery shopping: Engaging children in decisions about food empowers them, builds nutrition knowledge, and encourages healthier choices.
Rationale for incorrect answers:
1. Unlimited computer and TV time: Sedentary behavior contributes to weight gain and should be limited. Screen time should be no more than 1–2 hours per day for school-age children.
4. Eating unstructured meals: Lack of meal structure can lead to overeating, snacking on unhealthy foods, and poor portion control. Regular, planned meals support better nutrition.
6. Drinking three glasses of water per day: While hydration is important, three glasses may be insufficient for a child, and water alone will not significantly impact weight loss without lifestyle changes.
Take home points
- Family involvement and healthy role modeling are essential to successful weight management in children.
- Physical activity should be fun and age-appropriate, team sports, biking, or active play are great options.
- Involving the child in meal planning and food selection builds lifelong healthy habits.
- Limit screen time, encourage structured meals, and ensure adequate hydration and nutrition rather than focusing on restriction.
As the school nurse conducting screening for vision in a 6-year-old child, you would refer the child to a specialist if the visual acuity in both eyes is:
Explanation
Vision screening in children helps detect amblyopia and other visual disorders early to prevent long-term visual impairment. For a 6-year-old child, referral to a specialist is typically recommended when visual acuity is worse than 20/40 in either eye.
Rationale for correct answer:
4. 20/50: At age 6, children should achieve at least 20/40 vision in each eye. A visual acuity of 20/50 in both eyes indicates subnormal vision that may interfere with reading, learning, and development. Early referral ensures prompt diagnosis and treatment, potentially preventing permanent vision loss or academic difficulties.
Rationale for incorrect answers:
1. 20/20: This is normal vision and no referral is needed. It represents clear, age-appropriate acuity.
2. 20/25: Slightly less than perfect but still within the normal range for a 6-year-old. No referral is required.
3. 20/30: Also within the acceptable range for this age. Continued observation may be done, but referral is not indicated unless the child has symptoms or concerns.
Take home points
- Refer 6-year-old children if visual acuity is worse than 20/40 in either eye.
- 20/50 or worse requires prompt referral to identify and manage potential vision disorders.
- Slight variations like 20/25 or 20/30 are still within normal limits and do not typically require intervention.
- Early vision problems can impact academic performance and social development, early detection is crucial.
The mother of two sons, ages 6 and 9, states they want to play on the same baseball team. As the school nurse, what advice would you give their mother?
Explanation
School-age children are in a period of rapid developmental change, particularly in motor skills, attention span, and social maturity. While they may share interests, their physical and cognitive capabilities differ significantly by age.
Rationale for correct answer:
2. A 6-year-old and a 9-year-old are at different developmental stages. The older child typically has better coordination, attention span, and understanding of rules, which gives them a distinct advantage. Placing them on different teams ensures each child is matched with peers at a similar developmental level, supporting both safety and positive skill development.
Rationale for incorrect answers:
1. While having both boys on the same team may be more convenient for the parent, convenience should not outweigh developmental appropriateness and safety.
3. Although both are school-age, there's a wide developmental range within this group. Treating it as a single category oversimplifies their abilities.
4. Sibling rivalry is not the primary concern here; the issue is developmental readiness and appropriate team placement.
Take home points
- Grouping children in sports should be based on developmental stage, not just age category.
- A 3-year age difference in school-age children often reflects significant physical and cognitive differences.
- Placement with similar-age peers supports skill development, safety, and enjoyment.
- Parental convenience is secondary to the child’s developmental needs and safety in team sports.
Exams on Growth And Development In School-age Children
Custom Exams
Login to Create a Quiz
Click here to loginLessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Analyze the physiologic changes in school-aged children, specifically the steady gain in height/weight and the replacement of deciduous teeth.
- Evaluate the psychosocial stage of Industry vs. Inferiority, identifying how children achieve a sense of competence through tasks.
- Identify cognitive milestones in Piaget’s Concrete Operations stage, including conservation, classification, and reversibility.
- Discuss the development of self-concept and body image, noting the influence of peer comparison and social feedback.
- Interpret Kohlberg’s moral development, focusing on the "good boy/nice girl" orientation and the importance of rules.
- Assess the impact of the school environment, including peer group dynamics, "latchkey" status, and school-related stress.
- Formulate health promotion strategies for nutrition, physical activity, and sleep hygiene tailored to the school-aged child.
- Prioritize injury prevention education, focusing on bicycle safety, sports protection, and motor vehicle safety.
Introduction
- The school-aged period, spanning from approximately 6 to 12 years, is often described as a time of gradual growth and significant social expansion.
- Unlike the rapid physical transformations of infancy or the emotional volatility of toddlerhood, the school years represent a period of relative physiologic calm before the storm of adolescence.
- For the pediatric nurse, this stage is characterized by the child’s entry into a larger world where the peer group becomes a secondary but powerful influence alongside the family.
- Growth is steady where children typically gain about 2 to 3 kilograms and grow 5 centimeters per year, with a noticeable shift in body proportions as legs lengthen and the "baby fat" of earlier years disappears.
- Psychosocially, the school-aged child is immersed in Erikson’s stage of Industry vs. Inferiority. The primary goal is the mastery of skills, whether academic, athletic, or social.
- Success in these endeavors fosters a sense of competence, while repeated failures can lead to feelings of inadequacy. This is mirrored by Piaget’s Concrete Operational stage, where children move away from magical thinking and begin to apply logic to physical objects.
- They learn the concept of conservation that is understanding that the quantity of a substance remains the same even if its shape changes.
- This cognitive shift allows the nurse to communicate more effectively; the child can now understand the "why" behind treatments and participate more actively in their own care.
- Socially, this period is marked by the development of "best friends" and the emergence of structured play, such as organized sports or board games with complex rules.
- The school-aged child also begins to refine their self-concept, which is heavily tied to their perceived abilities and physical appearance.
- As a nurse, assessing a child in this age group requires acknowledging their desire for autonomy and privacy while providing clear, logical explanations that respect their growing intellectual capacity.
Promoting Optimum Growth And Development
3.1. Biologic Development
- Height and Weight: Growth is slower and more gradual than in early childhood.
- Average weight gain: 2-3 kg (4.4-6.6 lbs) per year.
- Average height gain: 5-7.5 cm (2-3 inches) per year.
- Boys and girls are similar in size until prepubescence, when girls typically experience a growth spurt earlier.
- Physical Changes:
- Skeletal lengthening and muscle mass increase.
- Loss of primary teeth and eruption of permanent teeth (around age 6, first molar appears, followed by incisors).
- Immune system matures; fewer infections than preschoolers.
- Body proportions change: legs lengthen, body becomes more slender.
- Maturation of Systems:
- Respiratory System: Lung capacity increases.
- Cardiovascular System: Heart grows more slowly, blood pressure gradually increases, pulse rate decreases.
- Gastrointestinal System: Digestive system becomes more mature; stomach capacity increases.
- Urinary System: Bladder capacity increases, allowing for longer periods between voiding.
- Nervous System: Brain growth slows, but myelination continues, improving fine motor skills and coordination.
- Immune System: Lymphoid tissue reaches maximum size, improving immune response.
- Sensory Development:
- By the school-age years, all of a child's senses are well-developed.
- Vision is typically 20/20 by this age, with mature ocular muscular control, peripheral vision, and color discrimination by age 7. Good vision is crucial for a child's physical and educational development. School vision screenings often identify issues like amblyopia (lazy eye), uncorrected refractive errors, and strabismus (misaligned eyes). Amblyopia, the leading cause of visual impairment in children, is reduced vision in an eye not adequately used during early development, often due to conditions like strabismus or significant differences in vision between the eyes. If left untreated by age 9, amblyopia can lead to irreversible vision loss, though recent studies suggest older children (7-17) can still benefit from treatments like glasses or patching.
- Hearing sense: While severe hearing deficits are usually diagnosed in infancy, less severe issues might not be detected until school, when a child experiences learning or speech difficulties. Regular hearing screenings are vital for ensuring proper educational and social progress. There's also growing concern about the impact of prolonged exposure to loud music on the hearing of school-aged children and adolescents.
- The senses of smell and touch are also mature in school-aged children. Smell can be tested using familiar scents, and touch discrimination (e.g., hot/cold, soft/hard, blunt/sharp) can also be assessed.
- Prepubescence (Preadolescence):
- Typically occurs 9-12 years for girls and 10-14 years for boys.
- Defined as the 2 years preceding puberty.
- Characterized by initial physiological changes that herald puberty, such as the growth spurt, appearance of secondary sexual characteristics (breast budding in girls, testicular enlargement in boys), and hormonal changes.
- Girls usually begin prepubescence earlier than boys.
- Nursing Insight: Nurses should be sensitive to the diverse range of pubertal onset and development. Reassure children and parents that variations are normal. Provide accurate information about body changes to alleviate anxiety and promote positive body image.
3.2. Psychosocial Development (Erikson: Industry vs. Inferiority)
- Children develop a sense of industry by achieving a sense of competence and mastery in various activities (schoolwork, sports, hobbies).
- They strive to complete tasks and receive recognition for their accomplishments.
- If children are not encouraged or are constantly criticized, they may develop a sense of inferiority, doubting their abilities.
- Nursing Insight: Encourage participation in age-appropriate tasks and activities, celebrating efforts and successes. Provide opportunities for children to contribute and feel useful, especially during illness or hospitalization.
3.3. Cognitive Development (Piaget: Concrete Operational Stage)
- Key Characteristics:
- Conservation: Ability to understand that a quantity remains the same despite changes in its appearance (e.g., volume of liquid in different-shaped containers).
-
- Classification: Ability to group objects by common characteristics.
- Seriation: Ability to order objects along a quantitative dimension (e.g., by length or weight).
- Decentration: Ability to consider multiple aspects of a situation simultaneously (moving away from egocentrism).
- Reversibility: Ability to mentally reverse a sequence of events or operations.
- Logic and Reasoning: Begin to think more logically about concrete events, but still struggle with abstract concepts.
- Understanding of Time and Space: Develop a clearer understanding of time (past, present, future) and spatial relationships.
- Nursing Insight: Explain procedures in a clear, concrete, and literal manner, avoiding abstract terms. Use visual aids and demonstrations. Allow children to manipulate equipment when appropriate to foster understanding and cooperation.
3.4. Moral Development (Kohlberg: Conventional Level)
- Stage 3: Good Interpersonal Relationships (Good Boy/Good Girl Orientation):
- Children act to gain approval from others and avoid disapproval.
- Focus on being "nice" and conforming to social expectations.
- Stage 4: Maintaining the Social Order (Law and Order Orientation):
- Children understand the importance of rules and laws for maintaining social order.
- Obedience is based on respect for authority and the desire to avoid guilt.
- Nursing Insight: Discuss rules and expectations clearly and consistently. Help children understand the reasoning behind rules, promoting a sense of fairness and justice. Encourage empathy and understanding of others' perspectives.
3.5. Spiritual Development
- School-age children often have a concrete understanding of God or a higher power.
- They may attribute human characteristics to divine beings.
- Prayer and religious rituals may be important.
- They begin to question and internalize religious beliefs from their families and community.
- Nursing Insight: Respect and support the child's and family's spiritual beliefs. Provide opportunities for spiritual practices if desired (e.g., quiet time for prayer, access to religious materials).
3.6. Language Development
- Vocabulary expands significantly.
- Improved grammar and sentence structure.
- Use of jokes, riddles, and puns demonstrates growing understanding of wordplay and multiple meanings.
- Can understand and use more complex language structures, including passive voice and conditional clauses.
- Nursing Insight: Use clear, age-appropriate language. Encourage verbalization of feelings and thoughts. Listen actively to build rapport.
3.7. Development of Self-Concept
- Self-Concept: The mental picture one has of oneself, including one's abilities, appearance, and values.
- Body Image: How one perceives and feels about their physical appearance. Influenced by peer opinions and media.
- Self-Esteem: The overall evaluation of one's worth or value. Strongly influenced by competence in various areas (academics, sports, social skills) and perceived acceptance by peers and adults.
- Nursing Insight: Foster positive self-esteem by emphasizing the child's strengths and efforts. Provide opportunities for success. Help children develop coping strategies for perceived limitations. Address body image concerns sensitively, especially during prepubescence. Encourage healthy lifestyle choices that promote a positive body image.
3.8. Development of Sexuality
- School-age children are curious about sex and reproduction.
- They begin to distinguish between sex and gender.
- Awareness of sexual identity (who they are attracted to) may begin.
- Sex Education:
- Should be age-appropriate and delivered in a factual, open, and non-judgmental manner.
- Starts with basic anatomy and physiology.
- Progresses to reproduction, puberty, healthy relationships, personal safety, and boundaries.
- Emphasize body privacy and the concept of "good touch" and "bad touch."
- Parents often struggle to teach their children accurate sexual terminology and information, frequently leading to children associating reproductive organs with excretory functions and thus, "dirtiness."
- This lack of parental guidance often results in children acquiring sexual information from peers, which can be misleading and cause anxiety.
- Although middle childhood is an ideal time for formal sex education, it remains a controversial topic.
- Nurse’s Role in Sex Education:
- Provide accurate, evidence-based information.
- Answer questions openly and honestly.
- Address misconceptions and fears.
- Emphasize that sex is a normal and healthy part of human development.
- Promote healthy sexual decision-making and safe practices.
- Encourage open communication between children and their parents/guardians.
- Assess for signs of sexual abuse and report as mandated.
3.9. Social Development
- Social Relationships and Cooperation:
- Shift from egocentric play to cooperative play.
- Develop an understanding of social rules and expectations.
- Increased desire for peer acceptance and belonging.
- Clubs and Peer Groups:
- Form strong friendships and "best friends."
- Peer groups become increasingly influential in shaping behaviors, attitudes, and values.
- "Cliques" and social hierarchies may begin to emerge.
- Participation in organized activities (sports, scouts, clubs) provides opportunities for social skill development and positive peer interactions.
- Relationships with Families:
- While peer influence increases, family remains the primary source of security, guidance, and values.
- Children still seek approval from parents.
- More independence, but still need parental supervision and boundaries.
- Family routines and rituals provide stability.
- Nursing Insight: Support positive peer relationships and involvement in extracurricular activities. Counsel parents on balancing independence with appropriate supervision. Encourage family communication and quality time.
3.10. Play
- Play evolves from solitary and parallel play to highly organized, cooperative play.
- Rules and Rituals: Children enjoy games with clear rules and often invent their own. This helps them understand fairness, negotiation, and strategy.
- Team Play: Participation in team sports teaches cooperation, division of labor, competition, and sportsmanship.
- Quiet Games and Activities: Puzzles, board games, reading, and creative activities (drawing, crafting) are popular and foster cognitive skills and concentration.
- Ego Mastery: Through play, children master new skills, develop a sense of competence, and cope with anxieties and conflicts.
- Nursing Insight: Encourage age-appropriate play, even in healthcare settings, as it aids in coping and recovery. Utilize therapeutic play to help children express feelings and understand medical procedures.
Temperament
- In the school-aged population, temperament that is the "how" of behavior, continues to play a major role in how a child adapts to new environments.
- While the basic categories (easy, difficult, slow-to-warm-up) persist, they are now expressed through the child's reaction to school demands, peer pressure, and authority figures.
- The "easy" school-ager typically adapts well to the structure of the classroom and transitions smoothly between activities. Conversely, the "slow-to-warm-up" child may experience significant anxiety when starting a new school year or joining a new sports team. Nurses can help by recommending "gradual exposure" and extra preparation for new situations.
- The "difficult" or "spirited" child may struggle with the rigid rules of a classroom, often being labeled as "problematic" when they are simply reacting to a mismatch between their high-intensity temperament and the environment. These children may require may require more patience and consistent routines.
- Nurses should assess for "Goodness of Fit" between the child's temperament and the expectations of both parents and teachers. A mismatch here is often a hidden source of stress and "somatic complaints" like stomach aches or headaches used to avoid school.
- By identifying these temperamental traits, nurses can provide anticipatory guidance on discipline and coping mechanisms that work with the child's nature rather than against it.
Coping With Concerns Related To Normal Growth And Development
6.1. School Experience
- Anticipatory Socialization: Children learn about and prepare for future roles and social situations, such as going to school. This involves developing skills like following instructions, sharing, and interacting with non-family adults and peers.
- Role of the Teacher: Teachers become significant adults outside the family, providing guidance, instruction, and opportunities for learning and social development. They are key figures in the child's development of industry.
- Role of Parents: Parents remain crucial for support, encouragement, and ensuring school readiness. They need to communicate with teachers, monitor academic progress, and provide a conducive learning environment at home.
- Encourage parents to visit schools with their children before enrollment, participate in school events, and communicate openly with teachers. Address school refusal or anxiety with a holistic approach, considering underlying fears, learning difficulties, or social challenges.
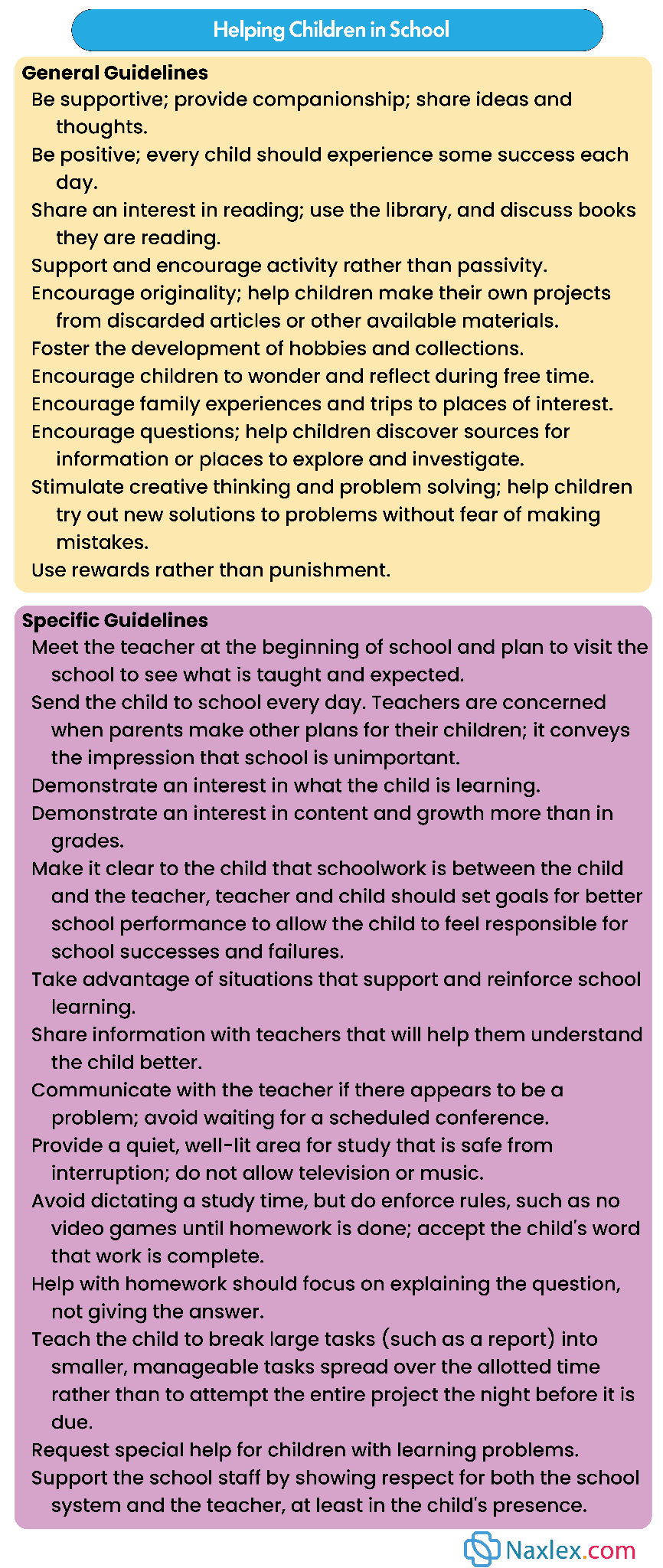
6.2. Discipline
- Effective discipline for school-age children focuses on teaching self-control, responsibility, and understanding consequences.
- Should be consistent, fair, and clearly communicated.
- Techniques include:
- Logical Consequences: Directly related to the misbehavior (e.g., if a toy is broken, the child helps repair or replace it).
- Natural Consequences: Occur without adult intervention (e.g., if a child doesn't wear a coat, they get cold).
- Time-out: Brief period of isolation to allow the child to calm down and reflect.
- Privilege Removal: Temporarily taking away a desired item or activity.
- Positive Reinforcement: Praising and rewarding desired behaviors.
- Dishonest Behavior (Lying, Cheating, Stealing):
Common behaviors that emerge as children test boundaries and understand rules are lying, cheating, and stealing.
- Lying
- Children lie for various reasons, and the motivations evolve with age. Preschoolers often struggle to differentiate between fact and fantasy, so their "lies" may simply be misperceptions or imaginative stories. As they reach school age, most children can distinguish reality from make-believe, but may still exaggerate to impress others.
- Common reasons for lying in younger children include avoiding punishment or getting out of trouble, especially in families with severe disciplinary practices. Children often emulate their parents' behavior; if parents lie, their children are more likely to do the same. Older children might lie due to low self-esteem, to meet unrealistic expectations, or to gain something with minimal effort. Interestingly, most children are concerned about the wrongfulness of lying and cheating, particularly when observed in their friends. Parents should understand that occasional lying is normal and that their own honesty serves as a crucial role model. Discussing the importance of truthfulness and how it impacts trust and respect can be beneficial.
- Cheating
- Cheating is common in young children, particularly between the ages of 5 and 8. They often find it difficult to lose games or contests and may cheat almost automatically, not yet fully grasping the wrongfulness of the behavior. This usually fades as they mature. However, children learn from their environment; if parents boast about cheating (e.g., on taxes), children may perceive such behavior as acceptable. Therefore, parents modeling honest behavior is essential in discouraging cheating.
- Stealing
- Stealing in younger children (5 to 8 years old) is not uncommon and is often linked to a limited sense of property rights. They might take items because they're attracted to them or for what money can buy, and they may even give away their own valuable possessions. When caught, young children are typically remorseful, promising not to repeat the act, but they may do so the next day, sometimes also lying to cover up the theft or offer excuses. Directly trapping them into an admission is seldom helpful, as they don't grasp full responsibility until later in middle childhood.
- Children steal for various reasons, including a lack of understanding of property rights, an attempt to bribe peers, a strong desire for a coveted item, or as a form of revenge against perceived unfair treatment, often from a parent. Older children might steal to supplement inadequate income, or it could signal deeper issues or unmet needs in their lives.
- Factors like crowded living arrangements, lack of privacy, and communal family property can hinder a child's development of property rights. Inconsistent messages from parents, such as forcing children to share everything or taking items from children's private spaces, can also cause confusion. Parents should provide children with a private space and respect their personal belongings to foster respect for the property rights of others.
- For most cases of stealing, a reprimand and a reasonable consequence, such as returning the item or paying restitution, are usually effective. While temptations exist, most children can learn to respect others' property rights, though some may need more time to internalize these cultural rules.
6.3. Coping with Stress
- School-age children experience various stressors: academic pressure, peer conflict, family changes (divorce, new sibling), moving.
- Signs of Stress: Changes in behavior (irritability, withdrawal), sleep disturbances, appetite changes, physical complaints (headaches, stomachaches), decline in school performance.
- Coping Strategies: Talking about feelings, engaging in hobbies, physical activity, problem-solving, seeking support from trusted adults.
- Nursing Insight: Help children identify sources of stress. Teach and model healthy coping mechanisms. Encourage open communication with parents and other supportive adults. Refer for counseling if stress is overwhelming or prolonged.
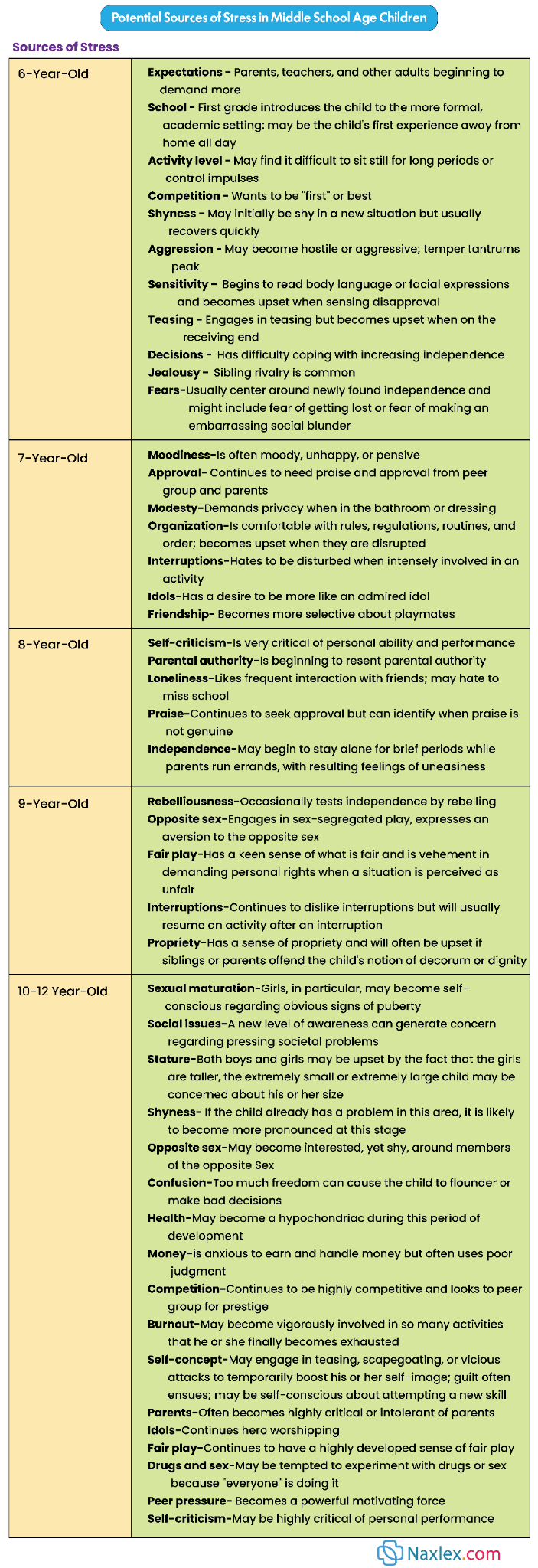
6.4. Latchkey Children
- Children who care for themselves after school until a parent or guardian returns home.
- May experience feelings of loneliness, fear, boredom, or increased responsibility.
- Risks: Increased risk of injury, unsupervised online activity, exposure to risky behaviors.
- Provide anticipatory guidance to parents on safe practices for latchkey children (e.g., emergency plans, "safe" adults to contact, clear rules for screen time and visitors). Encourage enrollment in after-school programs if feasible.
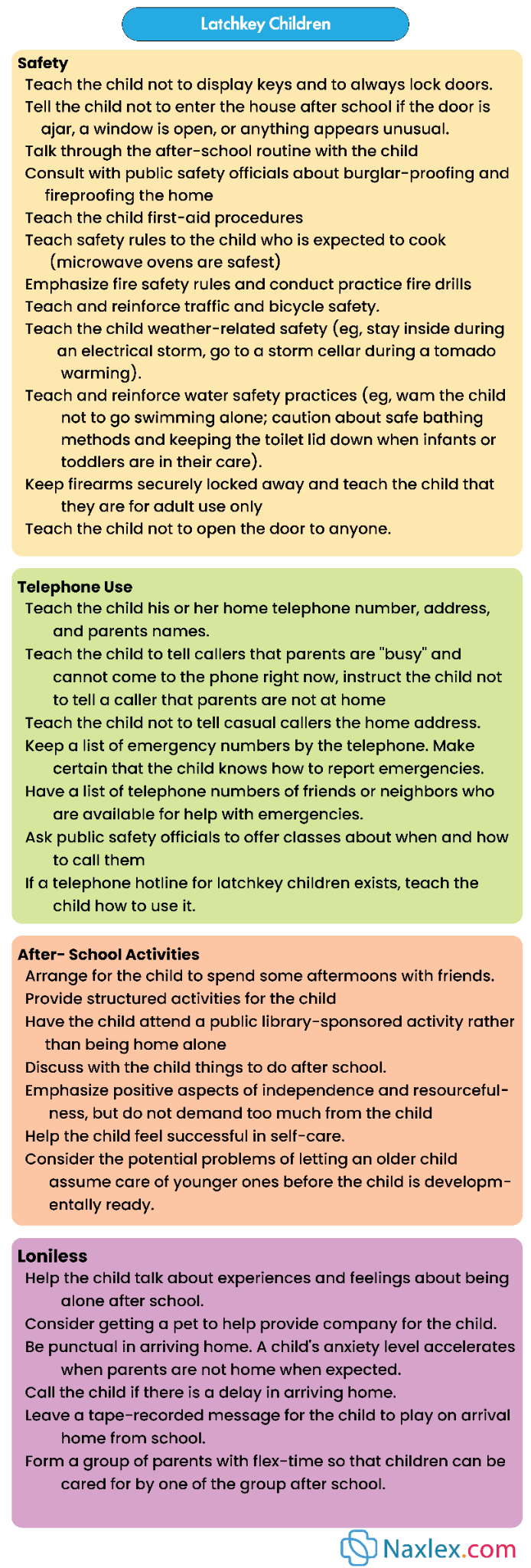
6.5. Fears
- Common fears include:
- Bodily harm/injury: Falls, accidents.
- Darkness: Fear of the unknown.
- Being alone: Especially at night.
- School failure/tests: Performance anxiety.
- Social rejection: Not being liked by peers.
- Natural disasters, war, crime: Influenced by media and adult conversations.
- Nursing Insight: Validate the child's feelings. Help them articulate their fears. Provide reassurance and strategies for coping (e.g., nightlights, problem-solving for school anxiety). Avoid dismissing or ridiculing fears.
Promoting Optimum Health During The School Years
8.1. Health Behaviors
- School-age children begin to internalize health behaviors and habits.
- Emphasis on developing personal responsibility for health.
- Provide health education that is practical and relevant to their daily lives. Empower children to make healthy choices.
8.2. Nutrition
- Nutritional Needs: Energy needs vary based on age, gender, and activity level. Balanced diet with adequate protein, carbohydrates, healthy fats, vitamins, and minerals is crucial for growth and development.
- Outside Influences: Peer pressure, advertising, and availability of unhealthy snacks.
- School Programs: School lunch and breakfast programs are vital for ensuring adequate nutrition, especially for low-income families.
- Nutrition Education: Teaching children about healthy food choices, portion sizes, and the benefits of a balanced diet.
- Assess dietary intake and identify nutritional deficiencies or excesses. Provide education on healthy eating habits to children and families. Advocate for healthy school lunch programs and nutrition education in schools. Address picky eating, obesity, and disordered eating patterns.
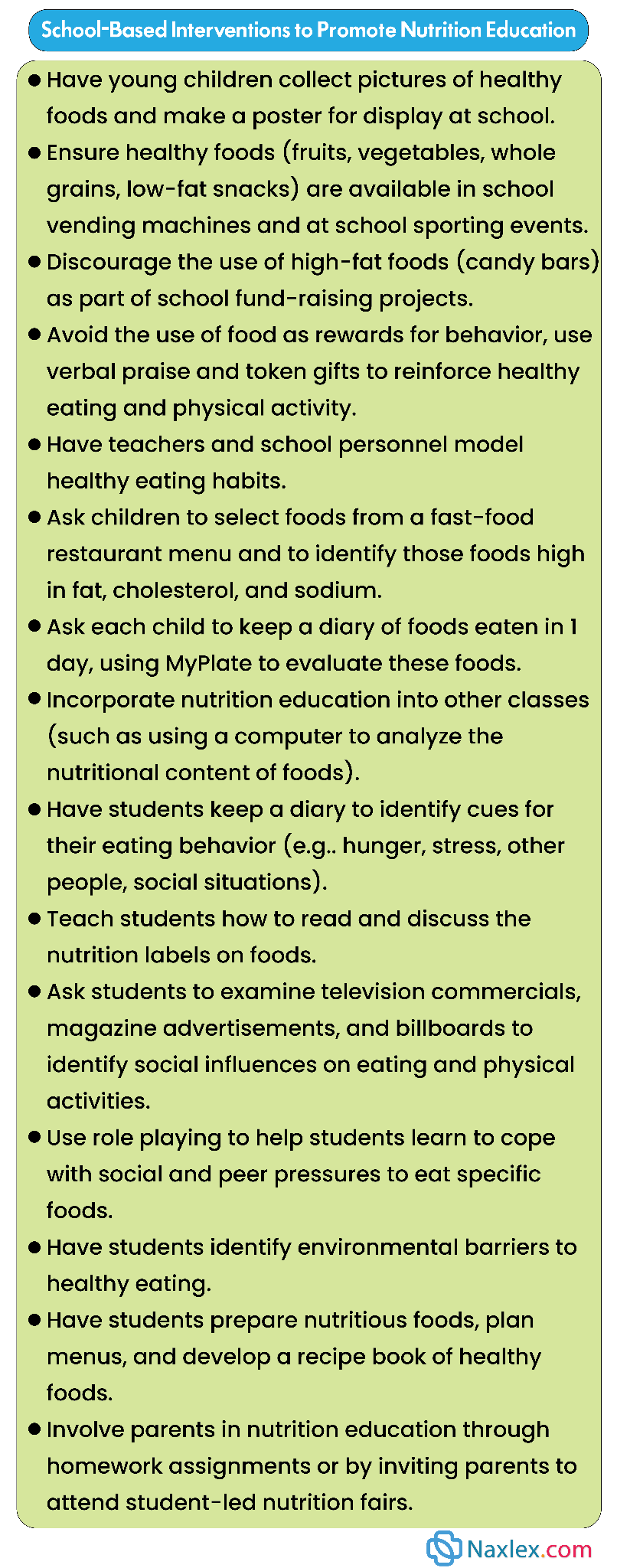
8.3. Sleep and Rest
- School-age children need approximately 9-12 hours of sleep per night.
- Adequate sleep supports cognitive function, mood regulation, and physical health.
- Nursing Insight: Encourage consistent bedtimes and wake times, even on weekends. Promote a relaxing bedtime routine. Limit screen time before bed. Discuss the impact of insufficient sleep on school performance and behavior.
8.4. Physical Activity
- Physical Fitness: Essential for healthy weight, cardiovascular health, bone development, and muscle strength.
- Sports: Participation in organized sports promotes physical fitness, teamwork, sportsmanship, and skill acquisition.
- Acquisition of Skills: Development of fine and gross motor skills through various activities (e.g., throwing, catching, running, writing, drawing).
- Television, Video Games, and the Internet:
- Can be beneficial for learning and entertainment but excessive use can lead to sedentary lifestyles, sleep disturbances, exposure to inappropriate content, and cyberbullying.
- Screen Time Recommendations: Limit recreational screen time to 1-2 hours per day.
- Nursing Insight: Encourage daily physical activity (at least 60 minutes of moderate-to-vigorous activity). Promote diverse activities to develop a range of skills. Educate parents and children on healthy screen time habits, including setting limits, co-viewing, and monitoring content.
8.5. Dental Health
- Loss of primary teeth and eruption of permanent teeth.
- Brushing: Emphasize proper brushing technique (at least twice daily) and flossing.
- Regular dental check-ups (every 6 months) for cleaning, fluoride application, and cavity detection.
- Dental sealants are recommended to protect molars.
- Parents should be counseled regarding food items that place children at high risk of dental caries including:
- Those that are quickly consumed and swallowed pose the least threat, such as: Soda, chocolate, and cookies.
- Those that stick to the teeth after chewing pose the greatest threat, such as: caramel, jelly beans, and raisins.
- Nurses should provide dental health education. Encourage parents to supervise brushing and flossing. Reinforce the importance of regular dental visits.
8.6. School Health
- Health Education: Schools play a critical role in providing comprehensive health education, including nutrition, hygiene, safety, substance abuse prevention, and mental health awareness.
- School Nursing Services: School nurses are vital for:
- Providing first aid and managing chronic conditions (e.g., asthma, diabetes).
- Administering medications.
- Conducting health screenings (vision, hearing, scoliosis).
- Identifying and reporting child abuse and neglect.
- Promoting a healthy school environment.
- Acting as a liaison between home, school, and healthcare providers.
- Providing individual and group health counseling.
- Collaborate with school nurses and educators to promote student health and well-being. Advocate for adequate funding and resources for school health programs.
8.7. Injury Prevention
- Leading cause of morbidity and mortality in school-age children.
- Increased independence and exploration lead to greater risk-taking behavior.
- Risk-Taking Behavior: Children may overestimate their abilities and underestimate risks.
- Motor Vehicle Injury:
- Proper use of booster seats until they reach 4 feet 9 inches (145 cm) tall and are 8-12 years old.
- Always use seatbelts in the back seat.
- Pedestrian safety education (looking both ways, crossing at crosswalks).
- Bicycle Injury:
- Always wear a properly fitted helmet.
- Follow traffic rules.
- Ride in safe areas.
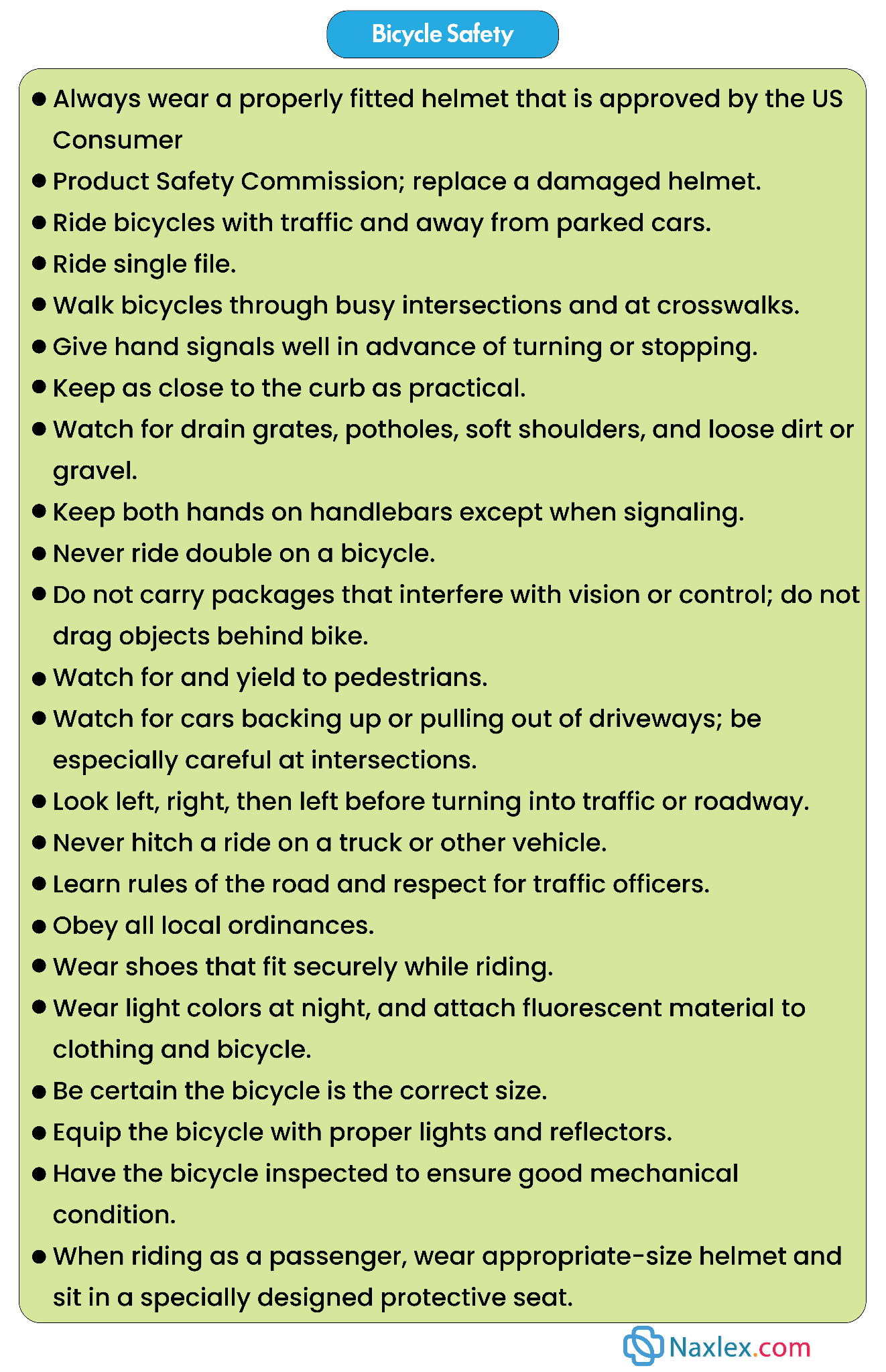
- Other Vehicle-Related Injuries:
- Ride-on toys, whether child-powered or motorized, are popular for their ability to help children develop balance, coordination, and physical fitness. However, they also pose significant safety risks.
- Between 1990 and 2011, ride-on toys were responsible for 35% of all toy-related injuries and 43% of hospital admissions for children under 10 years old. These toys were also three times more likely to cause fractures or dislocations compared to other types of toys. While most injuries affect the upper extremities, severe head and neck injuries are also possible.
- School-aged children using these toys on streets and highways face an increased risk of collisions with objects or vehicles. Parents should carefully assess their child's skill level before allowing them to use any ride-on toy.
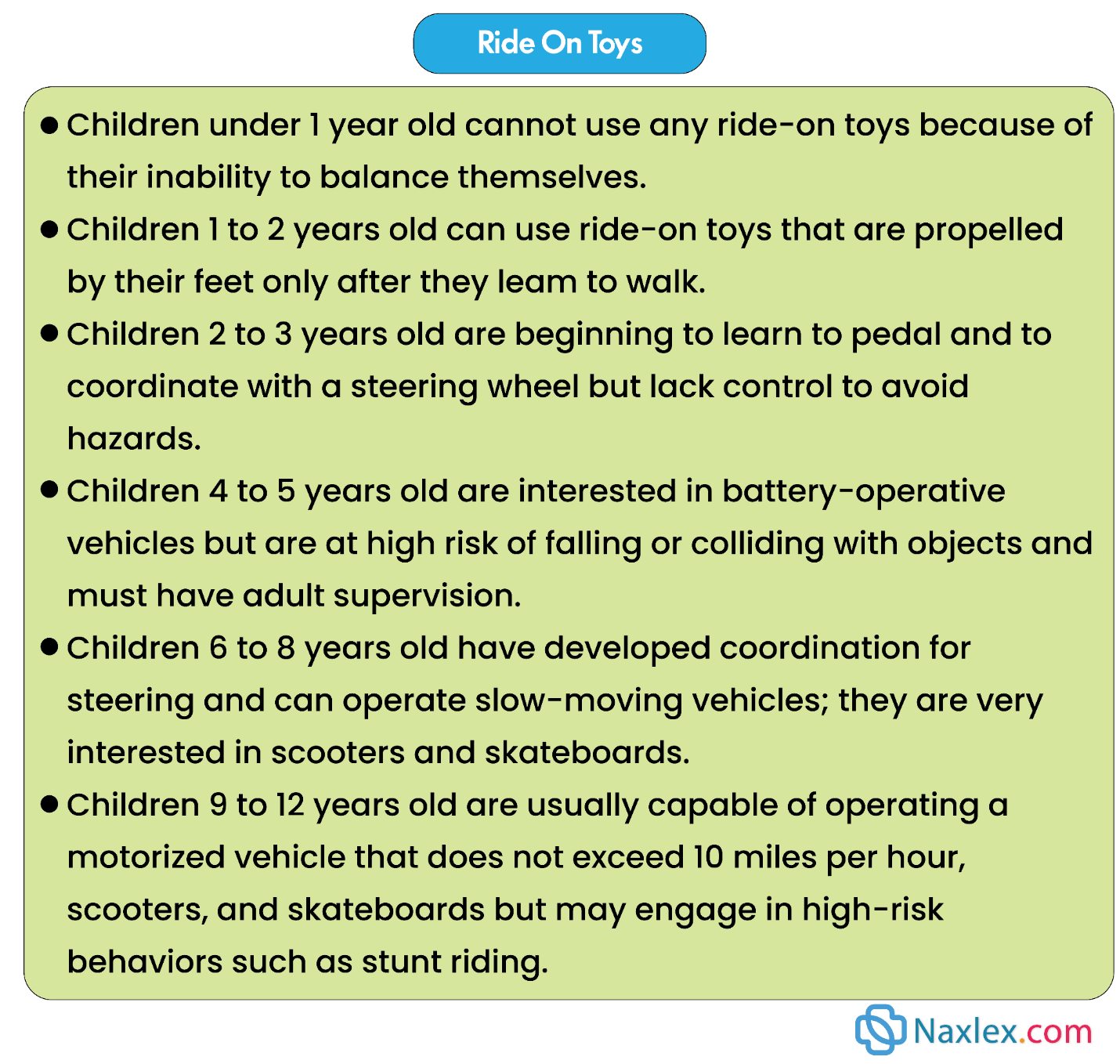
- Injuries at School: Playground injuries, sports injuries, falls.
- Burn safety and sun exposure:
a. Sun exposure: Children must be reminded to reapply sunscreen at least every 2 hours and more frequently if they become wet.
b. Fire and burns: Because of their increasing abilities, school-age children, especially those who are older, often are asked to assist in such activities as lighting fires and food preparation. Children must be taught regarding appropriate safe use of matches, stoves, ovens, and grills. The misuse of fireworks can be dangerous. Fireworks, if lawful, should only be used in the presence and guidance of an adult.
- School phobias and bullying.
a. Parents should be forewarned that even though school is usually a positive experience for the child, fostering children’s psychosocial, cognitive, and moral development, some children find the school
experience difficult.
b. School refusal: also called school phobia or school avoidance.
When children complain of vague symptoms (e.g., stomachaches and headaches that resolve once the parents allow the children to stay home from school), school refusal should be suspected.
Etiologies of school refusal include:
- Bullying by another student.
- Poor school performance.
- Boredom.
- Fear of teacher.
- Embarrassment, for example, over how he or she is dressed.
c. Parent education.
When school refusal is suspected, parents should be encouraged to:
- Solicit the assistance of school personnel to determine the specific problem that is leading to the refusal.
- Deal with bullying or other potentially dangerous issues as quickly as possible, if necessary.
- Inform the child that the parent understands the child’s discomfort.
- Gently, but firmly, require the child to attend school.
d. Bullying: Children may be victims of bullying by others who they are in face-to-face contact with or, because of the many electronic communication devices now available, via the Internet.
Parent education: Parents should be encouraged to query their children periodically regarding the children’s relationships, both positive and negative. If a child does report being a victim of bullying, the parent should:
- Immediately report the problem to the school and/or legal authorities, if appropriate.
- Educate the child regarding actions that he or she can take in response to the bullying (e.g., reporting the episodes to an appropriate adult, avoiding contact with the bully when possible, clearly telling the bully that the behavior is inappropriate).
- Nurse’s Role in Injury Prevention:
- Provide anticipatory guidance to parents and children on age-appropriate safety measures.
- Educate on proper use of safety equipment (helmets, seatbelts, booster seats).
- Promote safe play environments.
- Advocate for community safety initiatives (e.g., safe walking routes to school, playground safety standards).
- Discuss the dangers of substance abuse and risky behaviors.
- Assess for risk factors for injury in the home and community.
8.8. Immunizations
Vaccinations are recommended to be administered between age 7 and 12 years. They should be administered:
- Throughout childhood: yearly influenza vaccines.
- From 11 to 12 years of age.
- Tdap (tetanus, diphtheria, acellular pertussis).
- Three-dose series of human papillomavirus vaccines.
- First dose of meningococcal vaccine.
Nursing Insight: Any recommended vaccines that the child has yet to receive should be administered per the Advisory Committee on Immunization Practices catch-up vaccine schedule.
Summary
- Nursing care for the school-aged child focuses on supporting the transition from home to the broader community.
- The school experience is the central focus of the child's life, and nurses must assess for school-related stress, bullying, or learning disabilities that may impact the child’s self-esteem.
- For "latchkey children" who spend time at home unsupervised, the nurse must provide guidance on safety and emergency protocols.
- Discipline at this age shifts from physical control to the use of reasoning and natural consequences, helping the child internalize a sense of moral responsibility.
- Health promotion during these years is centered on preventing the "new morbidities," such as childhood obesity and dental caries.
- Nutrition education should focus on balanced meals and the dangers of excessive screen time versus the benefits of at least 60 minutes of daily physical activity.
- Dental health is critical, as this is the period when permanent teeth erupt. Nurses should also emphasize the importance of sleep, typically 9 to 12 hours, to support cognitive function and physical growth.
- School health programs play a vital role here, offering a platform for vision and hearing screenings, as well as the administration of booster immunizations (such as Tdap and HPV).
- Safety remains a priority, but the focus shifts to injuries related to increased independence. Pedestrian accidents, bicycle injuries, and sports-related trauma are the leading causes of morbidity.
- Nurses should advocate for "concussion awareness" in sports and ensure that parents are aware of current motor vehicle safety laws.
- By fostering a collaborative relationship with the child and family, the nurse ensures that the school-aged child develops the healthy habits and psychological resilience necessary to navigate the upcoming challenges of adolescence.
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Growth And Development In School-age Children
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
