
Abuse, Violence, Trauma, and Stressor Related Disorders
Lessons
- Objectives
- Introduction
- Clinical Picture of Abuse and Violence
- Child and Elder Abuse
- Child Abuse
- Elder Abuse
- Trauma and Stressor Related Disorders
- Post-Traumatic Stress Disorder (PTSD)
- Acute Stress Disorder (ASD)
- Adjustment Disorder (AD)
- Reactive Attachment Disorder (RAD)
- Disinhibited Social Engagement Disorder (DSED)
Notes Highlighting is available once you sign in. Login Here.
Objectives
-
Define abuse, violence, trauma, and stressor related disorders and their types, causes, risk factors, and effects.
-
Identify the clinical manifestations of abuse, violence, trauma, and stressor related disorders in different populations and settings.
-
Describe the nursing assessment and interventions for abuse, violence, trauma, and stressor related disorders, including prevention, screening, reporting, referral, education, support, and therapy.
-
Apply the nursing process and evidence-based practice to provide holistic and culturally sensitive care for clients with abuse, violence, trauma, and stressor related disorders.
-
Evaluate the outcomes of nursing care for clients with abuse, violence, trauma, and stressor related disorders and their families.
-
Demonstrate ethical, legal, and professional responsibilities in caring for clients with abuse, violence, trauma, and stressor related disorders.
Introduction
Introduction
-
Abuse is the intentional or unintentional infliction of physical, sexual, emotional, or financial harm or neglect on another person.
-
Violence is the use of physical force or power to threaten or harm oneself or others.
-
Trauma is the exposure to actual or threatened death, serious injury, or sexual violence.
-
Stressor-related disorders are a group of mental disorders that develop after exposure to a traumatic or stressful event.
-
Abuse, violence, trauma, and stressor-related disorders are major public health problems that affect millions of people worldwide.
-
Abuse, violence, trauma, and stressor-related disorders can have serious and long-lasting consequences for the physical, mental, emotional, social, and spiritual well-being of individuals, families, communities, and societies.
-
Nurses play a vital role in preventing, identifying, reporting, treating, and supporting clients with abuse, violence, trauma, and stressor-related disorders across the lifespan and in various settings.

Clinical Picture of Abuse and Violence
Abuse and violence can occur in different forms and contexts. Some of the common types of abuse and violence are:
Child abuse: any act or failure to act by a parent or caregiver that results in death, serious physical or emotional harm, sexual abuse, or exploitation of a child under 18 years of age. Child abuse can be physical, sexual, emotional, or neglectful.

Elder abuse: any act or failure to act by a person in a relationship of trust that results in harm or distress to an older person. Elder abuse can be physical, sexual, emotional, financial, or neglectful.
Intimate partner violence (IPV): any physical, sexual, psychological, or economic harm or threat of harm by a current or former partner or spouse. IPV can be physical, sexual, emotional, stalking, or coercive control.
Sexual assault: any unwanted sexual contact or activity without consent or under coercion. Sexual assault can include rape, attempted rape, fondling, groping, oral sex, anal sex, penetration with objects, or exposure to pornography.
Community violence: any intentional act of interpersonal violence that occurs in public or private spaces between individuals who are not related or intimate partners. Community violence can include homicide, assault, robbery, kidnapping, terrorism, hate crimes, gang violence, school violence, workplace violence, or mass shootings.
The causes of abuse and violence are complex and multifactorial. Some of the factors that contribute to abuse and violence are:
-
Individual factors: such as age, gender, race/ethnicity, personality traits, mental health status, substance use disorder, history of trauma or abuse, low self-esteem, poor impulse control, anger issues, cognitive impairment, disability.
-
Relationship factors: such as family dynamics, marital conflict, power imbalance, poor communication skills, lack of trust or respect, isolation from social support networks.
-
Community factors: such as poverty, unemployment, homelessness, crime rates, lack of access to education or health care services or legal protection or social welfare programs or resources for victims/survivors.
-
Societal factors: such as cultural norms or values or beliefs or attitudes that condone or justify or tolerate or minimize or deny abuse or violence or discrimination or oppression based on gender or sexuality or race/ethnicity or religion or age or disability.
-
The effects of abuse and violence can be devastating and lasting for the victims/survivors, perpetrators, witnesses, and bystanders. Some of the effects of abuse and violence are:
-
Physical effects: such as injuries, bruises, cuts, burns, fractures, internal bleeding, organ damage, sexually transmitted infections (STIs), unwanted pregnancy, chronic pain, headaches, gastrointestinal problems, cardiovascular problems, respiratory problems, immune system dysfunction.
-
Psychological effects: such as post-traumatic stress disorder (PTSD), acute stress disorder (ASD), adjustment disorder (AD), depression, anxiety, panic disorder, phobias, obsessive-compulsive disorder (OCD), dissociative disorders, personality disorders, eating disorders, sleep disorders, substance use disorder, suicidal ideation or behavior.
-
Emotional effects: such as fear, anger, guilt, shame, sadness, grief, loneliness, hopelessness, helplessness, low self-esteem, low self-confidence, low self-worth, distrust, resentment, bitterness.
-
-
Social effects: such as isolation, withdrawal, avoidance, detachment, alienation, rejection, stigma, discrimination, bullying, harassment, violence, abuse, exploitation, homelessness, unemployment, poverty.
-
Spiritual effects: such as loss of faith, meaning, purpose, values, morals, ethics, hope.
Child and Elder Abuse
-
Child and elder abuse are serious forms of abuse that affect vulnerable populations who may have difficulty in protecting themselves or seeking help.
-
Child and elder abuse can have severe and long-term consequences for the physical, mental, emotional, social, and spiritual health and development of the victims/survivors.
-
Child and elder abuse can occur in various settings such as home, school, work, community, or institutional care.
-
Child and elder abuse can be perpetrated by various people such as parents, caregivers, relatives, friends, neighbors, teachers, co-workers, strangers, or professionals.
-
Child and elder abuse can be influenced by various factors such as individual characteristics of the victim/survivor or perpetrator; relationship dynamics; family structure; cultural norms; social support; economic status; legal system; and health care system.
Child Abuse
-
Child abuse can be classified into four main types: physical abuse; sexual abuse; emotional abuse; neglect.
-
Physical abuse is the intentional use of physical force that results in or has the potential to result in physical injury to a child. Examples of physical abuse are hitting; kicking; punching; slapping; shaking; throwing; burning; biting; choking; poisoning; using weapons.
-
Sexual abuse is the involvement of a child in sexual activity that he or she does not fully comprehend or consent to or is not developmentally prepared for or violates the laws or social taboos of society. Examples of sexual abuse are fondling; oral sex; anal sex; vaginal sex; penetration with objects; exposure to pornography; prostitution; trafficking; incest; rape.
-
Emotional abuse is the persistent emotional maltreatment of a child that causes severe and adverse effects on the child’s emotional development. Examples of emotional abuse are verbal insults; threats; humiliation; rejection; isolation; ignoring; blaming; manipulating; intimidating; controlling; withholding affection; denying emotional responsiveness.
-
Neglect is the failure to provide for a child’s basic physical or emotional or educational or medical or dental needs. Examples of neglect are inadequate food or clothing or shelter or hygiene or supervision or protection or stimulation or affection or education or health care or dental care.
-
Child Abuse
-
Child abuse can be classified into four main types: physical abuse; sexual abuse; emotional abuse; neglect.
-
Physical abuse is the intentional use of physical force that results in or has the potential to result in physical injury to a child. Examples of physical abuse are hitting; kicking; punching; slapping; shaking; throwing; burning; biting; choking; poisoning; using weapons.
-
Sexual abuse is the involvement of a child in sexual activity that he or she does not fully comprehend or consent to or is not developmentally prepared for or violates the laws or social taboos of society. Examples of sexual abuse are fondling; oral sex; anal sex; vaginal sex; penetration with objects; exposure to pornography; prostitution; trafficking; incest; rape.
-
Emotional abuse is the persistent emotional maltreatment of a child that causes severe and adverse effects on the child’s emotional development. Examples of emotional abuse are verbal insults; threats; humiliation; rejection; isolation; ignoring; blaming; manipulating; intimidating; controlling; withholding affection; denying emotional responsiveness.
-
Neglect is the failure to provide for a child’s basic physical or emotional or educational or medical or dental needs. Examples of neglect are inadequate food or clothing or shelter or hygiene or supervision or protection or stimulation or affection or education or health care or dental care.
-
Clinical Manifestations of Child Abuse
-
The clinical manifestations of child abuse may vary depending on the type and severity and duration and frequency of the abuse and the age and developmental stage and personality and coping skills of the child.
-
Behavioral signs: such as fear or anxiety or depression or aggression or withdrawal or low self-esteem or poor social skills or difficulty trusting others or difficulty forming attachments or difficulty expressing emotions or difficulty coping with stress or difficulty concentrating or learning or memory problems or nightmares or sleep problems or eating problems or substance use problems or self-harm or suicidal thoughts or behaviors.
-
Sexual signs: such as sexualized behavior or language or knowledge that is inappropriate for the child’s age or developmental level. The child may also show signs of genital or anal trauma or irritation or infection or pain or bleeding or discharge or pregnancy or STIs.
-
Nursing Assessment of Child Abuse
-
The nursing assessment of child abuse involves collecting subjective and objective data from the child and the caregiver and other sources such as family members, teachers, social workers, or health care providers.
-
The nursing assessment of child abuse should be done in a safe, private, and comfortable environment with the child’s consent and cooperation. The nurse should use a calm, gentle, and supportive approach and avoid leading, suggestive, or judgmental questions. The nurse should also use developmentally appropriate language and tools such as dolls, drawings, or games to facilitate communication with the child.
-
The nursing assessment of child abuse should include the following components:
-
History: The nurse should obtain a comprehensive history of the child’s physical, mental, emotional, social, and spiritual health and development; family structure and dynamics; cultural background and beliefs; exposure to abuse or violence; current situation and concerns; coping strategies and support systems; strengths and resources.
-
Physical examination: The nurse should perform a thorough physical examination of the child’s head, neck, chest, abdomen, back, extremities, genitals, anus, and skin. The nurse should document any signs of injury or trauma such as location, size, shape, color, pattern, stage of healing, and consistency with the history given by the child or caregiver. The nurse should also assess the child’s vital signs, growth parameters, nutritional status, developmental milestones, and immunization status.
-
Laboratory tests: The nurse should order laboratory tests as indicated by the history and physical examination. Some of the common laboratory tests for child abuse are complete blood count (CBC), coagulation studies, electrolytes, liver function tests (LFTs), renal function tests (RFTs), urine analysis (UA), urine toxicology screen (UTS), blood alcohol level (BAL), blood cultures, wound cultures, STI tests, pregnancy tests.
-
Diagnostic tests: The nurse should order diagnostic tests as indicated by the history and physical examination. Some of the common diagnostic tests for child abuse are x-rays, computed tomography (CT) scan, magnetic resonance imaging (MRI) scan, ultrasound, electroencephalogram (EEG), electrocardiogram (EKG), echocardiogram, bone scan, skeletal survey.
-
-
Nursing Interventions for Child Abuse
-
The nursing interventions for child abuse are based on the nursing process and evidence-based practice. The nursing interventions for child abuse aim to prevent further harm; protect the child’s rights; promote the child’s safety; report the suspected or confirmed abuse; refer the child and the caregiver to appropriate services; educate the child and the caregiver about abuse prevention and treatment; support the child’s physical, mental, emotional, social, and spiritual healing; and evaluate the outcomes of care.
-
Some of the common nursing interventions for child abuse are:
-
Prevention: The nurse should implement primary, secondary, and tertiary prevention strategies to reduce the risk of child abuse. Primary prevention strategies include providing education, information, and resources to parents, caregivers, children, and communities about child development, parenting skills, stress management, conflict resolution, anger management, substance use prevention, and abuse prevention. Secondary prevention strategies include screening children and caregivers for risk factors or signs of abuse; providing counseling, therapy, support groups, home visits, crisis intervention, and respite care to families at risk of abuse; and monitoring children and caregivers for changes in behavior or health status. Tertiary prevention strategies include reporting suspected or confirmed abuse to the appropriate authorities; providing medical care, legal assistance, social services, shelter, protection orders, and advocacy to children and caregivers who have experienced abuse; and facilitating reunification or alternative placement for children who have been removed from their homes due to abuse.
-
Protection: The nurse should protect the child’s rights according to the United Nations Convention on the Rights of the Child. The nurse should respect the child’s dignity, autonomy, privacy, confidentiality, and participation in decision-making. The nurse should also protect the child from further harm by ensuring a safe and secure environment; removing or minimizing any potential sources of danger; and providing appropriate equipment, supplies, and medications to prevent or treat complications or infections. The nurse should also protect the child from re-traumatization by avoiding unnecessary or repeated examinations or procedures; using a trauma-informed approach; and providing emotional support and comfort to the child.
-
Reporting: The nurse should report any suspected or confirmed cases of child abuse to the appropriate authorities as mandated by the law and the professional code of ethics. The nurse should follow the reporting protocol of the institution or agency where he or she works. The nurse should document the facts and evidence of the abuse in a clear, concise, and objective manner. The nurse should also inform the child and the caregiver about the reporting process and their rights and responsibilities. The nurse should cooperate with the investigation and provide any additional information or testimony as required.
-
Referral: The nurse should refer the child and the caregiver to appropriate services that can provide further assessment, treatment, support, and follow-up. Some of the common services that the nurse can refer to are:
-
Medical services: such as pediatrician, surgeon, dentist, ophthalmologist, otolaryngologist, dermatologist, gynecologist, urologist, endocrinologist, neurologist, psychiatrist, psychologist, nurse practitioner, physician assistant, nurse, social worker, pharmacist.
-
Legal services: such as lawyer, judge, prosecutor, defense attorney, police officer, detective, forensic examiner, child advocate, guardian ad litem, court-appointed special advocate (CASA).
-
Social services: such as child protective services (CPS), foster care, adoption, kinship care, group home, residential treatment center, shelter, transitional housing, independent living program.
-
Educational services: such as teacher, counselor, tutor, special education teacher, speech therapist, occupational therapist, physical therapist, school nurse, school social worker.
-
Community services: such as child abuse prevention program, family resource center, crisis hotline, helpline, support group, peer mentor, mentor, volunteer, faith-based organization.
-
-
Education: The nurse should educate the child and the caregiver about abuse prevention and treatment. The nurse should provide accurate, relevant, and understandable information about the causes, types, effects, and signs of abuse; the reporting process and legal implications; the available services and resources; the treatment options and outcomes; the coping strategies and self-care techniques; the safety planning and protection measures; the rights and responsibilities of the child and the caregiver; and the importance of follow-up and adherence to care.
-
Support: The nurse should support the child’s physical, mental, emotional, social, and spiritual healing. The nurse should provide holistic and culturally sensitive care that meets the individual needs and preferences and goals of the child. The nurse should also provide therapeutic communication and active listening and empathy and validation and encouragement and praise to the child. The nurse should also facilitate the development of a trusting and respectful and collaborative relationship with the child. The nurse should also promote the empowerment and resilience and recovery of the child. The nurse should also involve the family or significant others or community members in the care of the child as appropriate.
-
Evaluation: The nurse should evaluate the outcomes of care for the child and the caregiver. The nurse should use standardized tools or scales or questionnaires or interviews or observations to measure the progress or improvement or achievement of the expected outcomes. The expected outcomes may include:
-
The child is free from further harm or injury.
-
The child reports or demonstrates reduced pain or discomfort.
-
The child’s physical wounds or infections are healed or treated.
-
The child’s vital signs or laboratory tests or diagnostic tests are within normal limits or show improvement.
-
The child’s growth parameters or developmental milestones are appropriate for age or show improvement.
-
The child reports or demonstrates reduced fear or anxiety or depression or aggression or withdrawal or low self-esteem or poor social skills or difficulty trusting others or difficulty forming attachments or difficulty expressing emotions or difficulty coping with stress or difficulty concentrating or learning or memory problems or nightmares or sleep problems or eating problems or substance use problems or self-harm or suicidal thoughts or behaviors.
-
The child reports or demonstrates increased happiness or confidence or self-worth or self-esteem or social skills or trust in others or attachment to others or expression of emotions or coping with stress or concentration or learning or memory skills.
-
The child reports having a positive outlook on life and a sense of meaning and purpose.
-
The child reports having a supportive network of family members, friends, peers, mentors, professionals, and community members.
-
The child reports having a safe and secure environment at home, school, work, community or institutional care. The child reports having a safety plan and protection measures in place.
-
- The child reports or demonstrates reduced involvement or exposure to abuse or violence or trauma or stressors.
-
- The child reports or demonstrates increased involvement or participation in positive activities or hobbies or interests or goals.
-
- The child reports or demonstrates increased adherence to medical care, legal assistance, social services, educational services, community services, and follow-up appointments.
-
- The child reports or demonstrates increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
- The caregiver reports or demonstrates reduced risk factors or signs of abuse; increased protective factors or signs of support; increased knowledge and skills about child development, parenting, stress management, conflict resolution, anger management, substance use prevention, and abuse prevention; increased awareness and acceptance of the child’s needs and feelings; increased communication and cooperation with the child and other professionals; increased adherence to medical care, legal assistance, social services, educational services, community services, and follow-up appointments; increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
-
-
-
The nurse should also monitor for any complications or adverse effects of the abuse or the treatment such as infection, bleeding, shock, organ failure, sepsis, death, re-injury, re-victimization, re-traumatization, non-compliance, relapse, recurrence, dissatisfaction, dissatisfaction.
-
The nurse should also modify the plan of care as needed based on the evaluation of the outcomes and the feedback from the child and the caregiver. The nurse should also collaborate with other members of the interdisciplinary team to ensure continuity and coordination of care. The nurse should also document the evaluation of the outcomes and any changes in the plan of care in a clear, concise, and objective manner.
-
Some of the common clinical manifestations of child abuse are:
-
Physical signs: such as injuries or bruises or burns or fractures or scars or bites or infections or bleeding or pain or swelling or marks from objects or cords or belts. The injuries may be in various stages of healing or inconsistent with the history given by the child or caregiver or located in unusual places such as genitals or buttocks or back or face. The child may also show signs of malnutrition or dehydration or poor growth or developmental delay or failure to thrive.
-

Elder Abuse
-
Elder abuse is any act or failure to act by a person in a relationship of trust that results in harm or distress to an older person. Elder abuse can be physical, sexual, emotional, financial, or neglectful.
-
Physical abuse is the intentional use of physical force that results in or has the potential to result in physical injury to an older person. Examples of physical abuse are hitting; kicking; punching; slapping; shaking; pushing; pulling; dragging; burning; biting; choking; poisoning; using weapons.
-
Sexual abuse is any unwanted sexual contact or activity without consent or under coercion. Examples of sexual abuse are fondling; oral sex; anal sex; vaginal sex; penetration with objects; exposure to pornography; prostitution; trafficking.
-
Emotional abuse is the intentional infliction of mental pain or anguish or distress on an older person. Examples of emotional abuse are verbal insults; threats; humiliation; intimidation; isolation; ignoring; blaming; manipulating; controlling; withholding affection; denying emotional responsiveness.
-
Financial abuse is the illegal or improper or unauthorized use or exploitation or mismanagement of an older person’s money or property or assets or benefits. Examples of financial abuse are stealing; forging; coercing; deceiving; undue influencing; withholding; misappropriating; overcharging; fraud; scam.
-
Neglect is the failure to provide for an older person’s basic physical or emotional or social or medical needs. Examples of neglect are inadequate food or clothing or shelter or hygiene or supervision or protection or stimulation or affection or health care.

Clinical Manifestations of Elder Abuse
-
The clinical manifestations of elder abuse may vary depending on the type and severity and duration and frequency of the abuse and the age and health status and cognitive function and personality and coping skills of the older person.
-
Some of the common clinical manifestations of elder abuse are:
-
Physical signs: such as injuries or bruises or burns or fractures or scars or bites or infections or bleeding or pain or swelling or marks from objects or cords or belts. The injuries may be in various stages of healing or inconsistent with the history given by the older person or caregiver or located in unusual places such as genitals or buttocks or back or face. The older person may also show signs of malnutrition or dehydration or poor hygiene or pressure ulcers or contractures or infections.
-
-
Behavioral signs: such as fear or anxiety or depression or aggression or withdrawal or confusion or dementia or delirium or hallucinations or paranoia or low self-esteem or poor social skills or difficulty trusting others or difficulty expressing emotions or difficulty coping with stress or difficulty concentrating or memory problems or sleep problems or eating problems or substance use problems or self-harm or suicidal thoughts or behaviors.
-
Sexual signs: such as sexualized behavior or language that is inappropriate for the older person’s age or cognitive level. The older person may also show signs of genital or anal trauma or irritation or infection or pain or bleeding or discharge or STIs.
-
Financial signs: such as unexplained changes in the older person’s financial situation or status such as missing money or property or assets or benefits; unpaid bills or debts or taxes; forged checks or signatures; unauthorized transactions or withdrawals; unusual purchases or donations; exploitation by family members, caregivers, friends, neighbors, strangers, professionals, or organizations.
-
Neglect signs: such as inadequate food or clothing or shelter or hygiene or supervision or protection or stimulation or affection; lack of access to health care services or medications or assistive devices; lack of participation in social activities or hobbies or interests; lack of respect or dignity; lack of autonomy or choice.
Nursing Interventions for Elder Abuse
-
The nursing interventions for elder abuse are based on the nursing process and evidence-based practice. The nursing interventions for elder abuse aim to prevent further harm; protect the older person’s rights; promote the older person’s safety; report the suspected or confirmed abuse; refer the older person and the caregiver to appropriate services; educate the older person and the caregiver about abuse prevention and treatment; support the older person’s physical, mental, emotional, social, and spiritual healing; and evaluate the outcomes of care.
-
Some of the common nursing interventions for elder abuse are:
-
Prevention: The nurse should implement primary, secondary, and tertiary prevention strategies to reduce the risk of elder abuse. Primary prevention strategies include providing education, information, and resources to older persons, caregivers, families, and communities about aging, health care needs, legal rights, financial management, and abuse prevention. Secondary prevention strategies include screening older persons and caregivers for risk factors or signs of abuse; providing counseling, therapy, support groups, home visits, crisis intervention, and respite care to older persons and caregivers at risk of abuse; and monitoring older persons and caregivers for changes in behavior or health status. Tertiary prevention strategies include reporting suspected or confirmed abuse to the appropriate authorities; providing medical care or legal assistance or social services or shelter or protection orders or advocacy to older persons who have experienced abuse; and facilitating reunification or alternative placement for older persons who have been removed from their homes due to abuse.
-
Protection: The nurse should protect the older person’s rights according to the United Nations Principles for Older Persons. The nurse should respect the older person’s dignity or independence or participation or care or self-fulfillment. The nurse should also protect the older person from further harm by ensuring a safe and secure environment; removing or minimizing any potential sources of danger; and providing appropriate equipment or supplies or medications to prevent or treat complications or infections. The nurse should also protect the older person from re-traumatization by avoiding unnecessary or repeated examinations or procedures; using a trauma-informed approach; and providing emotional support and comfort to the older person.
-
Reporting: The nurse should report any suspected or confirmed cases of elder abuse to the appropriate authorities as mandated by the law and the professional code of ethics. The nurse should follow the reporting protocol of the institution or agency where he or she works. The nurse should document the facts and evidence of the abuse in a clear, concise, and objective manner. The nurse should also inform the older person and the caregiver about the reporting process and their rights and responsibilities. The nurse should cooperate with the investigation and provide any additional information or testimony as required.
-
Referral: The nurse should refer the older person and the caregiver to appropriate services that can provide further assessment, treatment, support, and follow-up. Some of the common services that the nurse can refer to are:
-
Medical services: such as geriatrician, surgeon, dentist, ophthalmologist, otolaryngologist, dermatologist, gynecologist, urologist, endocrinologist, neurologist, psychiatrist, psychologist, nurse practitioner, physician assistant, nurse, social worker, pharmacist.
-
Legal services: such as lawyer, judge, prosecutor, defense attorney, police officer, detective, forensic examiner, elder advocate, guardian ad litem, court-appointed special advocate (CASA).
-
Social services: such as adult protective services (APS), foster care, adoption, kinship care, group home, residential treatment center, shelter, transitional housing, independent living program.
-
Educational services: such as teacher, counselor, tutor, special education teacher, speech therapist, occupational therapist, physical therapist, school nurse, school social worker.
-
Community services: such as elder abuse prevention program, senior center, crisis hotline, helpline, support group, peer mentor, mentor, volunteer, faith-based organization.
-
-
Education: The nurse should educate the older person and the caregiver about abuse prevention and treatment. The nurse should provide accurate or relevant or understandable information about the causes or types or effects or signs of abuse; the reporting process and legal implications; the available services and resources; the treatment options and outcomes; the coping strategies and self-care techniques; the safety planning and protection measures; the rights and responsibilities of the older person and the caregiver; and the importance of follow-up and adherence to care.
-
Support: The nurse should support the older person’s physical or mental or emotional or social or spiritual healing. The nurse should provide holistic and culturally sensitive care that meets the individual needs or preferences or goals of the older person. The nurse should also provide therapeutic communication or active listening or empathy or validation or encouragement or praise to the older person. The nurse should also facilitate the development of a trusting or respectful or collaborative relationship with the older person. The nurse should also promote the empowerment or resilience or
Nursing Interventions for Elder Abuse
-
The nursing interventions for elder abuse are based on the nursing process and evidence-based practice. The nursing interventions for elder abuse aim to prevent further harm; protect the older person’s rights; promote the older person’s safety; report the suspected or confirmed abuse; refer the older person and the caregiver to appropriate services; educate the older person and the caregiver about abuse prevention and treatment; support the older person’s physical, mental, emotional, social, and spiritual healing; and evaluate the outcomes of care.
-
Some of the common nursing interventions for elder abuse are:
-
Prevention: The nurse should implement primary, secondary, and tertiary prevention strategies to reduce the risk of elder abuse. Primary prevention strategies include providing education, information, and resources to older persons, caregivers, families, and communities about aging, health care needs, legal rights, financial management, and abuse prevention. Secondary prevention strategies include screening older persons and caregivers for risk factors or signs of abuse; providing counseling, therapy, support groups, home visits, crisis intervention, and respite care to older persons and caregivers at risk of abuse; and monitoring older persons and caregivers for changes in behavior or health status. Tertiary prevention strategies include reporting suspected or confirmed abuse to the appropriate authorities; providing medical care or legal assistance or social services or shelter or protection orders or advocacy to older persons who have experienced abuse; and facilitating reunification or alternative placement for older persons who have been removed from their homes due to abuse.
-
Protection: The nurse should protect the older person’s rights according to the United Nations Principles for Older Persons. The nurse should respect the older person’s dignity or independence or participation or care or self-fulfillment. The nurse should also protect the older person from further harm by ensuring a safe and secure environment; removing or minimizing any potential sources of danger; and providing appropriate equipment or supplies or medications to prevent or treat complications or infections. The nurse should also protect the older person from re-traumatization by avoiding unnecessary or repeated examinations or procedures; using a trauma-informed approach; and providing emotional support and comfort to the older person.
-
Reporting: The nurse should report any suspected or confirmed cases of elder abuse to the appropriate authorities as mandated by the law and the professional code of ethics. The nurse should follow the reporting protocol of the institution or agency where he or she works. The nurse should document the facts and evidence of the abuse in a clear, concise, and objective manner. The nurse should also inform the older person and the caregiver about the reporting process and their rights and responsibilities. The nurse should cooperate with the investigation and provide any additional information or testimony as required.
-
Referral: The nurse should refer the older person and the caregiver to appropriate services that can provide further assessment, treatment, support, and follow-up. Some of the common services that the nurse can refer to are:
-
Medical services: such as geriatrician, surgeon, dentist, ophthalmologist, otolaryngologist, dermatologist, gynecologist, urologist, endocrinologist, neurologist, psychiatrist, psychologist, nurse practitioner, physician assistant, nurse, social worker, pharmacist.
-
Legal services: such as lawyer, judge, prosecutor, defense attorney, police officer, detective, forensic examiner, elder advocate, guardian ad litem, court-appointed special advocate (CASA).
-
Social services: such as adult protective services (APS), foster care, adoption, kinship care, group home, residential treatment center, shelter, transitional housing, independent living program.
-
Educational services: such as teacher, counselor, tutor, special education teacher, speech therapist, occupational therapist, physical therapist, school nurse, school social worker.
-
Community services: such as elder abuse prevention program, senior center, crisis hotline, helpline, support group, peer mentor, mentor, volunteer, faith-based organization.
-
-
Education: The nurse should educate the older person and the caregiver about abuse prevention and treatment. The nurse should provide accurate or relevant or understandable information about the causes or types or effects or signs of abuse; the reporting process and legal implications; the available services and resources; the treatment options and outcomes; the coping strategies and self-care techniques; the safety planning and protection measures; the rights and responsibilities of the older person and the caregiver; and the importance of follow-up and adherence to care.
-
Support: The nurse should support the older person’s physical or mental or emotional or social or spiritual healing. The nurse should provide holistic and culturally sensitive care that meets the individual needs or preferences or goals of the older person. The nurse should also provide therapeutic communication or active listening or empathy or validation or encouragement or praise to the older person. The nurse should also facilitate the development of a trusting or respectful or collaborative relationship with the older person. The nurse should also promote the empowerment or resilience or recovery of the older person. The nurse should also involve the family or significant others or community members in the care of the older person as appropriate.
-
Evaluation: The nurse should evaluate the outcomes of care for the older person and the caregiver. The nurse should use standardized tools or scales or questionnaires or interviews or observations to measure the progress or improvement or achievement of the expected outcomes. The expected outcomes may include:
-
The older person is free from further harm or injury.
-
The older person reports or demonstrates reduced pain or discomfort.
-
The older person’s physical wounds or infections are healed or treated.
-
The older person’s vital signs or laboratory tests or diagnostic tests are within normal limits or show improvement.
-
The older person’s functional status or nutritional status or cognitive function or mental status or mood or affect or behavior or pain level are appropriate for age or show improvement.
-
The older person reports or demonstrates reduced fear or anxiety or depression or aggression or withdrawal or confusion or dementia or delirium or hallucinations or paranoia or low self-esteem or poor social skills or difficulty trusting others or difficulty expressing emotions or difficulty coping with stress or difficulty concentrating or memory problems or sleep problems or eating problems or substance use problems or self-harm or suicidal thoughts or behaviors.
-
The older person reports or demonstrates increased happiness or confidence or self-worth or self-esteem or social skills or trust in others or expression of emotions or coping with stress or concentration or memory skills.
-
The older person reports having a positive outlook on life and a sense of meaning and purpose.
-
The older person reports having a supportive network of family members, friends, peers, mentors, professionals, and community members.
-
The older person reports having a safe and secure environment at home, work, community, or institutional care. The older person reports having a safety plan and protection measures in place.
-
The older person reports or demonstrates reduced involvement or exposure to abuse or violence or trauma or stressors.
-
The older person reports or demonstrates increased involvement or participation in positive activities or hobbies or interests or goals.
-
- The older person reports or demonstrates increased adherence to medical care, legal assistance, social services, educational services, community services, and follow-up appointments.
-
- The older person reports or demonstrates increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
- The caregiver reports or demonstrates reduced risk factors or signs of abuse; increased protective factors or signs of support; increased knowledge and skills about aging, health care needs, legal rights, financial management, and abuse prevention; increased awareness and acceptance of the older person’s needs and feelings; increased communication and cooperation with the older person and other professionals; increased adherence to medical care, legal assistance, social services, educational services, community services, and follow-up appointments; increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
-
-
-
The nurse should also monitor for any complications or adverse effects of the abuse or the treatment such as infection, bleeding, shock, organ failure, sepsis, death, re-injury, re-victimization, re-traumatization, non-compliance, relapse, recurrence, dissatisfaction.
-
The nurse should also modify the plan of care as needed based on the evaluation of the outcomes and the feedback from the older person and the caregiver. The nurse should also collaborate with other members of the interdisciplinary team to ensure continuity and coordination of care. The nurse should also document the evaluation of the outcomes and any changes in the plan of care in a clear, concise, and objective manner.
Trauma and Stressor Related Disorders
-
Trauma and stressor-related disorders are a group of mental disorders that develop after exposure to a traumatic or stressful event. Trauma and stressor-related disorders include post-traumatic stress disorder (PTSD), acute stress disorder (ASD), adjustment disorder (AD), reactive attachment disorder (RAD), disinhibited social engagement disorder (DSED), and other specified trauma and stressor-related disorder (OSTSD).
-
A traumatic event is an event that involves actual or threatened death, serious injury, or sexual violence to oneself or others. Examples of traumatic events are natural disasters, war, terrorism, violence, abuse, rape, accidents, illnesses, injuries, and losses.
-
A stressful event is an event that involves a significant change or disruption in one’s life that causes distress or difficulty in coping. Examples of stressful events are divorce, separation, marriage, birth, death, moving, school, work, retirement, financial problems, and legal problems. Trauma and stressor-related disorders can affect anyone regardless of age, gender, race/ethnicity, culture, or background. Trauma and stressor-related disorders can have serious and long-lasting consequences for the physical, mental, emotional, social, and spiritual well-being of individuals, families, communities, and societies.
Clinical Manifestations of PTSD
The clinical manifestations of PTSD may vary depending on the type and severity and duration and frequency of the traumatic event; the age and developmental stage and personality and coping skills of the individual; the availability of social support; the presence of comorbid conditions.
-
Some of the common clinical manifestations of PTSD are:
-
Physical signs: such as headaches; gastrointestinal problems; cardiovascular problems; respiratory problems; immune system dysfunction; chronic pain; fatigue; substance use disorder; suicidal ideation or behavior.
-
Psychological signs: such as depression; anxiety; panic disorder; phobias; obsessive-compulsive disorder (OCD); dissociative disorders; personality disorders; eating disorders; and sleep disorders.
-
Emotional signs: such as fear; anger; guilt; shame; sadness; grief; loneliness; hopelessness; helplessness; low self-esteem; low self-confidence; low self-worth; distrust; resentment; and bitterness.
-
Social signs: such as isolation or withdrawal or avoidance detachment alienation or rejection or stigma discrimination or bullying harassment or violence or abuse or exploitation.
-
Spiritual signs: such as loss of faith or meaning or purpose or values or morals or ethics or hope.
-
Nursing Interventions for PTSD
-
The nursing interventions for PTSD are based on the nursing process and evidence-based practice. The nursing interventions for PTSD aim to prevent further harm; protect the individual’s rights; promote the individual’s safety; report the suspected or confirmed trauma; refer the individual to appropriate services; educate the individual about trauma prevention and treatment; support the individual’s physical, mental, emotional, social, and spiritual healing; and evaluate the outcomes of care.
-
Some of the common nursing interventions for PTSD are:
-
Prevention: The nurse should implement primary, secondary, and tertiary prevention strategies to reduce the risk of PTSD. Primary prevention strategies include providing education, information, and resources to individuals, families, and communities about trauma, its causes, types, effects, and signs; the available services and resources; and coping strategies and self-care techniques. Secondary prevention strategies include screening individuals for risk factors or signs of PTSD; providing counseling, therapy, support groups, crisis intervention, and debriefing to individuals who have been exposed to trauma or are at risk of developing PTSD; and monitoring individuals for changes in behavior or health status. Tertiary prevention strategies include providing medical care, legal assistance, social services, shelter, protection orders, and advocacy to individuals who have developed PTSD; and facilitating recovery or rehabilitation or reintegration for individuals who have been affected by trauma.
-
Protection: The nurse should protect the individual’s rights according to the United Nations Declaration of Human Rights. The nurse should respect the individual’s dignity, autonomy, privacy, confidentiality, and participation in decision-making. The nurse should also protect the individual from further harm by ensuring a safe and secure environment; removing or minimizing any potential sources of danger; and providing appropriate equipment, supplies, and medications to prevent or treat complications or infections. The nurse should also protect the individual from re-traumatization by avoiding unnecessary or repeated examinations or procedures; using a trauma-informed approach; and providing emotional support and comfort to the individual.
-
Reporting: The nurse should report any suspected or confirmed cases of trauma to the appropriate authorities as mandated by the law and the professional code of ethics. The nurse should follow the reporting protocol of the institution or agency where he or she works. The nurse should document the facts and evidence of the trauma in a clear, concise, and objective manner. The nurse should also inform the individual about the reporting process and their rights and responsibilities. The nurse should cooperate with the investigation and provide any additional information or testimony as required.
-
Referral: The nurse should refer the individual to appropriate services that can provide further assessment, treatment, support, and follow-up. Some of the common services that the nurse can refer to are:
-
Medical services: such as physician, surgeon, nurse practitioner, physician assistant, nurse, social worker, pharmacist, psychiatrist, and psychologist.
-
Legal services: such as lawyer, judge, prosecutor, defense attorney, police officer, detective, forensic examiner, victim advocate, guardian ad litem, and court-appointed special advocate (CASA).
-
Social services: such as social worker, case manager, counselor, therapist, support group facilitator, crisis intervention worker, debriefing worker.
-
Community services: such as trauma prevention programs, crisis hotlines, helplines, support groups, peer mentors, mentors, volunteers, and faith-based organizations.
-
-
Education: The nurse should educate the individual about trauma prevention and treatment. The nurse should provide accurate or relevant or understandable information about trauma or its causes or types or effects or signs; the reporting process and legal implications; the available services and resources; the treatment options and outcomes; the coping strategies and self-care techniques; the safety planning and protection measures; the rights and responsibilities of the individual; and the importance of follow-up and adherence to care.
-
Support: The nurse should support the individual’s physical or mental or emotional or social or spiritual healing. The nurse should provide holistic and culturally sensitive care that meets the individual needs or preferences or goals of the individual. The nurse should also provide therapeutic communication or active listening or empathy or validation or encouragement or praise to the individual. The nurse should also facilitate the development of a trusting or respectful or collaborative relationship with the individual. The nurse should also promote the empowerment or resilience or recovery of the individual. The nurse should also involve the family or significant others or community members in the care of the individual as appropriate.
-
Evaluation: The nurse should evaluate the outcomes of care for the individual. The nurse should use standardized tools or scales or questionnaires or interviews or observations to measure the progress or improvement or achievement of the expected outcomes. The expected outcomes may include:
-
The individual is free from further harm or injury.
-
The individual reports or demonstrates reduced pain or discomfort.
-
The individual’s physical wounds or infections are healed or treated.
-
The individual’s vital signs or laboratory tests or diagnostic tests are within normal limits or show improvement.
-
The individual reports or demonstrates reduced intrusion symptoms or avoidance symptoms or negative alterations in cognition and mood or alterations in arousal and reactivity.
-
The individual reports or demonstrates increased happiness or confidence or self-worth or self-esteem or social skills or trust in others or expression of emotions or coping with stress or concentration or memory skills.
-
The individual reports having a positive outlook on life and a sense of meaning and purpose.
-
The individual reports having a supportive network of family members, friends, peers, mentors, professionals, and community members.
-
The individual reports having a safe and secure environment at home, work, community, or institutional care. The individual reports having a safety plan and protection measures in place.
-
The individual reports or demonstrates reduced involvement or exposure to trauma or stressors.
-
The individual reports or demonstrates increased involvement or participation in positive activities or hobbies interests or goals.
-
The individual reports or demonstrates increased adherence to medical care, legal assistance, social services, community services, and follow-up appointments.
-
The individual reports or demonstrates increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
-
-
The nurse should also monitor for any complications or adverse effects of the trauma or the treatment such as infection, bleeding, shock, organ failure, sepsis, death, re-injury, re-victimization, re-traumatization, non-compliance, relapse, recurrence, and dissatisfaction.
-
The nurse should also modify the plan of care as needed based on the evaluation of the outcomes and the feedback from the individual. The nurse should also collaborate with other members of the interdisciplinary team to ensure continuity and coordination of care. The nurse should also document the evaluation of the outcomes and any changes in the plan of care in a clear, concise, and objective manner.
Post-Traumatic Stress Disorder (PTSD)

-
Post-traumatic stress disorder (PTSD) is a mental disorder that develops after exposure to a traumatic event that causes intense fear or horror or helplessness.
-
PTSD is characterized by four main symptom clusters: intrusion symptoms; avoidance symptoms; negative alterations in cognition and mood; and alterations in arousal and reactivity.
-
Intrusion symptoms are recurrent and involuntary and intrusive memories or dreams flashbacks or distressing thoughts or feelings related to the traumatic event.
-
Avoidance symptoms are persistent and deliberate efforts to avoid or escape from reminders of the traumatic event such as people or places objects activities situations thoughts or feelings.
-
Negative alterations in cognition and mood are persistent and pervasive changes in the way one thinks or feels about oneself others or the world after the traumatic event such as negative beliefs or expectations of self-blame guilt shame anger or fear; diminished interest or participation in activities; detachment or estrangement from others; inability to experience positive emotions.
-
Alterations in arousal and reactivity are persistent and excessive increases in one’s level of alertness or responsiveness after the traumatic event such as irritability or aggression; recklessness or impulsivity; hypervigilance; exaggerated startle response; difficulty concentrating; and difficulty sleeping.
Acute Stress Disorder (ASD)

-
Acute stress disorder (ASD) is a mental disorder that develops after exposure to a traumatic event that causes intense fear or horror or helplessness.
-
ASD is characterized by nine or more symptoms from any of the five categories of intrusion, negative mood, dissociation, avoidance, and arousal, occurring within one month of the traumatic event and lasting for at least three days and up to one month.
-
Intrusion symptoms are recurrent and involuntary and intrusive memories or dreams or flashbacks or distressing thoughts or feelings related to the traumatic event.
-
Negative mood symptoms are persistent and pervasive inability to experience positive emotions such as happiness, satisfaction, or love after the traumatic event.
-
Dissociation symptoms are altered sense of reality or detachment from oneself or one’s surroundings or inability to remember important aspects of the traumatic event.
-
Avoidance symptoms are persistent and deliberate efforts to avoid or escape from reminders of the traumatic event such as people, places, objects, activities, situations, thoughts, or feelings.
-
Arousal symptoms are persistent and excessive increases in one’s level of alertness or responsiveness after the traumatic event such as irritability or aggression; recklessness or impulsivity; hypervigilance; exaggerated startle response; difficulty concentrating; difficulty sleeping.
Clinical Manifestations of ASD
-
The clinical manifestations of ASD may vary depending on the type and severity and duration and frequency of the traumatic event; the age and developmental stage and personality and coping skills of the individual; the availability of social support; the presence of comorbid conditions.
-
Some of the common clinical manifestations of ASD are:
-
Physical signs: such as headaches; gastrointestinal problems; cardiovascular problems; respiratory problems; immune system dysfunction; chronic pain; fatigue; substance use disorder; suicidal ideation or behavior.
-
Psychological signs: such as depression; anxiety; panic disorder; phobias; obsessive-compulsive disorder (OCD); dissociative disorders; personality disorders; eating disorders; sleep disorders.
-
Emotional signs: such as fear; anger; guilt; shame; sadness; grief; loneliness; hopelessness; helplessness; low self-esteem; low self-confidence; low self-worth; distrust; resentment; bitterness.
-
Social signs: such as isolation or withdrawal or avoidance or detachment or alienation or rejection or stigma or discrimination or bullying or harassment or violence or abuse or exploitation.
-
Spiritual signs: such as loss of faith or meaning or purpose or values or morals or ethics or hope.
-
Nursing Assessment of ASD
-
The nursing assessment of ASD involves collecting subjective and objective data from the individual and other sources such as family members, friends, peers, professionals, or records.
-
The nursing assessment of ASD should be done in a safe, private, and comfortable environment with the individual’s consent and cooperation. The nurse should use a calm, gentle, and supportive approach and avoid leading, suggestive, or judgmental questions. The nurse should also use developmentally appropriate language and tools such as pictures, charts, or scales to facilitate communication with the individual.
-
The nursing assessment of ASD should include the following components:
-
History: The nurse should obtain a comprehensive history of the individual’s physical, mental, emotional, social, and spiritual health and well-being; exposure to traumatic events; current situation and concerns; coping strategies and support systems; strengths and resources.
-
Physical examination: The nurse should perform a thorough physical examination of the individual’s head, neck, chest, abdomen, back, extremities, genitals, anus, and skin. The nurse should document any signs of injury or trauma or infection or pain or discomfort. The nurse should also assess the individual’s vital signs, nutritional status, pain level, and substance use status.
-
Laboratory tests: The nurse should order laboratory tests as indicated by the history and physical examination. Some of the common laboratory tests for ASD are complete blood count (CBC), coagulation studies, electrolytes, liver function tests (LFTs), renal function tests (RFTs), urine analysis (UA), urine toxicology screen (UTS), blood alcohol level (BAL), blood cultures, wound cultures, STI tests.
-
Diagnostic tests: The nurse should order diagnostic tests as indicated by the history and physical examination. Some of the common diagnostic tests for ASD are x-rays, computed tomography (CT) scan, magnetic resonance imaging (MRI) scan, ultrasound, electroencephalogram (EEG), electrocardiogram (EKG), echocardiogram.
-
Psychological tests: The nurse should administer psychological tests as indicated by the history and physical examination. Some of the common psychological tests for ASD are Acute Stress Disorder Scale (ASDS), Acute Stress Disorder Interview (ASDI), Structured Clinical Interview for DSM-5 Disorders (SCID-5), Beck Depression Inventory-II (BDI-II), Beck Anxiety Inventory (BAI), Impact of Event Scale-Revised (IES-R), Dissociative Experiences Scale (DES), Personality Assessment Inventory (PAI).
-
Nursing Interventions for ASD
-
The nursing interventions for ASD are based on the nursing process and evidence-based practice. The nursing interventions for ASD aim to prevent further harm; protect the individual’s rights; promote the individual’s safety; report the suspected or confirmed trauma; refer the individual to appropriate services; educate the individual about trauma prevention and treatment; support the individual’s physical, mental, emotional, social, and spiritual healing; and evaluate the outcomes of care.
-
Some of the common nursing interventions for ASD are:
-
Prevention: The nurse should implement primary, secondary, and tertiary prevention strategies to reduce the risk of ASD. Primary prevention strategies include providing education, information, and resources to individuals, families, and communities about trauma, its causes, types, effects, and signs; the available services and resources; and the coping strategies and self-care techniques. Secondary prevention strategies include screening individuals for risk factors or signs of ASD; providing counseling, therapy, support groups, crisis intervention, and debriefing to individuals who have been exposed to trauma or are at risk of developing ASD; and monitoring individuals for changes in behavior or health status. Tertiary prevention strategies include providing medical care, legal assistance, social services, shelter, protection orders, and advocacy to individuals who have developed ASD; and facilitating recovery or rehabilitation or reintegration for individuals who have been affected by trauma.
-
Protection: The nurse should protect the individual’s rights according to the United Nations Declaration of Human Rights. The nurse should respect the individual’s dignity, autonomy, privacy, confidentiality, and participation in decision-making. The nurse should also protect the individual from further harm by ensuring a safe and secure environment; removing or minimizing any potential sources of danger; and providing appropriate equipment, supplies, and medications to prevent or treat complications or infections. The nurse should also protect the individual from re-traumatization by avoiding unnecessary or repeated examinations or procedures; using a trauma-informed approach; and providing emotional support and comfort to the individual.
-
Reporting: The nurse should report any suspected or confirmed cases of trauma to the appropriate authorities as mandated by the law and the professional code of ethics. The nurse should follow the reporting protocol of the institution or agency where he or she works. The nurse should document the facts and evidence of the trauma in a clear, concise, and objective manner. The nurse should also inform the individual about the reporting process and their rights and responsibilities. The nurse should cooperate with the investigation and provide any additional information or testimony as required.
-
Referral: The nurse should refer the individual to appropriate services that can provide further assessment, treatment, support, and follow-up. Some of the common services that the nurse can refer to are:
-
Medical services: such as physician, surgeon, nurse practitioner, physician assistant, nurse, social worker, pharmacist, psychiatrist, psychologist.
-
Legal services: such as lawyer, judge, prosecutor, defense attorney, police officer, detective, forensic examiner, victim advocate, guardian ad litem, court-appointed special advocate (CASA).
-
Social services: such as social worker, case manager, counselor, therapist, support group facilitator, crisis intervention worker, debriefing worker.
-
Community services: such as trauma prevention program or crisis hotline or helpline or support group or peer mentor or mentor or volunteer or faith-based organization.
-
-
Education: The nurse should educate the individual about trauma prevention and treatment. The nurse should provide accurate or relevant or understandable information about trauma or its causes or types or effects or signs; the reporting process and legal implications; the available services and resources; the treatment options and outcomes; the coping strategies and self-care techniques; the safety planning and protection measures; the rights and responsibilities of the individual; and the importance of follow-up and adherence to care.
-
Support: The nurse should support the individual’s physical or mental or emotional or social or spiritual healing. The nurse should provide holistic and culturally sensitive care that meets the individual needs or preferences or goals of the individual. The nurse should also provide therapeutic communication or active listening or empathy or validation or encouragement or praise to the individual. The nurse should also facilitate the development of a trusting or respectful or collaborative relationship with the individual. The nurse should also promote the empowerment or resilience or recovery of the individual. The nurse should also involve the family or significant others or community members in the care of the individual as appropriate.
-
Evaluation: The nurse should evaluate the outcomes of care for the individual. The nurse should use standardized tools or scales or questionnaires or interviews or observations to measure the progress or improvement or achievement of the expected outcomes. The expected outcomes may include:
-
-
The individual is free from further harm or injury.
-
The individual reports or demonstrates reduced pain or discomfort.
-
The individual’s physical wounds or infections are healed or treated.
-
The individual’s vital signs or laboratory tests or diagnostic tests are within normal limits or show improvement.
-
The individual reports or demonstrates reduced intrusion symptoms or avoidance symptoms or negative mood symptoms or dissociation symptoms or arousal symptoms.
-
The individual reports or demonstrates increased happiness or confidence or self-worth or self-esteem or social skills or trust in others or expression of emotions or coping with stress or concentration or memory skills.
-
The individual reports having a positive outlook on life and a sense of meaning and purpose.
-
The individual reports having a supportive network of family members, friends, peers, mentors, professionals, and community members.
-
The individual reports having a safe and secure environment at home, work, community, or institutional care. The individual reports having a safety plan and protection measures in place.
-
The individual reports or demonstrates reduced involvement or exposure to trauma or stressors.
-
The individual reports or demonstrates increased involvement or participation in positive activities or hobbies or interests or goals.
-
The individual reports or demonstrates increased adherence to medical care, legal assistance, social services, community services, and follow-up appointments.
-
The individual reports or demonstrates increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
The nurse should also monitor for any complications or adverse effects of the trauma or the treatment such as infection, bleeding, shock, organ failure, sepsis, death, re-injury, re-victimization, re-traumatization, non-compliance, relapse, recurrence, dissatisfaction.
-
The nurse should also modify the plan of care as needed based on the evaluation of the outcomes and the feedback from the individual. The nurse should also collaborate with other members of the interdisciplinary team to ensure continuity and coordination of care. The nurse should also document the evaluation of the outcomes and any changes in the plan of care in a clear, concise, and objective manner.
Adjustment Disorder (AD)

-
Adjustment disorder (AD) is a mental disorder that develops after exposure to a stressful event that causes significant distress or difficulty in coping. AD is characterized by emotional or behavioral symptoms that are out of proportion to the severity or intensity of the stressor or that impair one’s functioning or relationships.
-
AD can be classified into six subtypes based on the predominant symptom: depressed mood; anxiety; mixed anxiety and depressed mood; disturbance of conduct; mixed disturbance of emotions and conduct; unspecified.
-
A stressful event is an event that involves a significant change or disruption in one’s life that causes distress or difficulty in coping. Examples of stressful events are divorce, separation, marriage, birth, death, moving, school, work, retirement, financial problems, legal problems.
Clinical Manifestations of AD
-
The clinical manifestations of AD may vary depending on the type and severity and duration and frequency of the stressful event; the age and developmental stage and personality and coping skills of the individual; the availability of social support; the presence of comorbid conditions.
-
Some of the common clinical manifestations of AD are:
-
Physical signs: such as headaches; gastrointestinal problems; cardiovascular problems; respiratory problems; immune system dysfunction; chronic pain; fatigue; substance use disorder; suicidal ideation or behavior.
-
Psychological signs: such as depression; anxiety; panic disorder; phobias; obsessive-compulsive disorder (OCD); eating disorders; sleep disorders.
-
Emotional signs: such as sadness; grief; loneliness; hopelessness; helplessness; anger; guilt; shame; fear; anxiety; low self-esteem; low self-confidence; low self-worth; distrust; resentment; bitterness.
-
Behavioral signs: such as withdrawal or isolation or avoidance or detachment or alienation or rejection; aggression or violence or vandalism or theft or lying or cheating or truancy or running away; recklessness or impulsivity or risk-taking; poor performance or attendance or participation in school or work; poor hygiene or grooming; changes in appetite or weight; changes in sleep patterns; substance use disorder; self-harm; suicidal thoughts or behaviors.
-
Nursing Assessment of AD
-
The nursing assessment of AD involves collecting subjective and objective data from the individual and other sources such as family members, friends, peers, professionals, or records.
-
The nursing assessment of AD should be done in a safe, private, and comfortable environment with the individual’s consent and cooperation. The nurse should use a calm, gentle, and supportive approach and avoid leading, suggestive, or judgmental questions. The nurse should also use developmentally appropriate language and tools such as pictures, charts, or scales to facilitate communication with the individual.
-
The nursing assessment of AD should include the following components:
-
History: The nurse should obtain a comprehensive history of the individual’s physical, mental, emotional, social, and spiritual health and well-being; exposure to stressful events; current situation and concerns; coping strategies and support systems; strengths and resources.
-
Physical examination: The nurse should perform a thorough physical examination of the individual’s head, neck, chest, abdomen, back, extremities, genitals, anus, and skin. The nurse should document any signs of injury or infection or pain or discomfort. The nurse should also assess the individual’s vital signs, nutritional status, pain level, and substance use status.
-
Laboratory tests: The nurse should order laboratory tests as indicated by the history and physical examination. Some of the common laboratory tests for AD are complete blood count (CBC), coagulation studies, electrolytes, liver function tests (LFTs), renal function tests (RFTs), urine analysis (UA), urine toxicology screen (UTS), blood alcohol level (BAL), blood cultures, wound cultures.
-
Diagnostic tests: The nurse should order diagnostic tests as indicated by the history and physical examination. Some of the common diagnostic tests for AD are x-rays, computed tomography (CT) scan, magnetic resonance imaging (MRI) scan, ultrasound, electroencephalogram (EEG), electrocardiogram (EKG), echocardiogram.
-
Psychological tests: The nurse should administer psychological tests as indicated by the history and physical examination. Some of the common psychological tests for AD are Structured Clinical Interview for DSM-5 Disorders (SCID-5), Beck Depression Inventory-II (BDI-II), Beck Anxiety Inventory (BAI), Eating Disorder Inventory-3 (EDI-3), Pittsburgh Sleep Quality Index (PSQI).
-
Nursing Interventions for AD
-
The nursing interventions for AD are based on the nursing process and evidence-based practice. The nursing interventions for AD aim to prevent further harm; protect the individual’s rights; promote the individual’s safety; report the suspected or confirmed stressor; refer the individual to appropriate services; educate the individual about stress prevention and treatment; support the individual’s physical, mental, emotional, social, and spiritual healing; and evaluate the outcomes of care.
-
Some of the common nursing interventions for AD are:
-
Prevention: The nurse should implement primary, secondary, and tertiary prevention strategies to reduce the risk of AD. Primary prevention strategies include providing education, information, and resources to individuals, families, and communities about stress, its causes, types, effects, and signs; the available services and resources; and the coping strategies and self-care techniques. Secondary prevention strategies include screening individuals for risk factors or signs of AD; providing counseling, therapy, support groups, crisis intervention, and debriefing to individuals who have been exposed to stress or are at risk of developing AD; and monitoring individuals for changes in behavior or health status. Tertiary prevention strategies include providing medical care, legal assistance, social services, shelter, protection orders, and advocacy to individuals who have developed AD; and facilitating recovery or rehabilitation or reintegration for individuals who have been affected by stress.
-
Protection: The nurse should protect the individual’s rights according to the United Nations Declaration of Human Rights. The nurse should respect the individual’s dignity, autonomy, privacy, confidentiality, and participation in decision-making. The nurse should also protect the individual from further harm by ensuring a safe and secure environment; removing or minimizing any potential sources of danger; and providing appropriate equipment or supplies or medications to prevent or treat complications or infections. The nurse should also protect the individual from re-traumatization by avoiding unnecessary or repeated examinations or procedures; using a trauma-informed approach; and providing emotional support and comfort to the individual.
-
Reporting: The nurse should report any suspected or confirmed cases of stress to the appropriate authorities as mandated by the law and the professional code of ethics. The nurse should follow the reporting protocol of the institution or agency where he or she works. The nurse should document the facts and evidence of the stress in a clear or concise or objective manner. The nurse should also inform the individual about the reporting process and their rights and responsibilities. The nurse should cooperate with the investigation and provide any additional information or testimony as required.
-
Referral: The nurse should refer the individual to appropriate services that can provide further assessment, treatment, support, and follow-up. Some of the common services that the nurse can refer to are:
-
-
Medical services: such as physician, surgeon, nurse practitioner, physician assistant, nurse, social worker, pharmacist, psychiatrist, psychologist.
-
Legal services: such as lawyer, judge, prosecutor, defense attorney, police officer, detective, forensic examiner, victim advocate, guardian ad litem, court-appointed special advocate (CASA).
-
Social services: such as social worker, case manager, counselor, therapist, support group facilitator, crisis intervention worker, debriefing worker.
-
Community services: such as stress prevention program, crisis hotline, helpline, support group, peer mentor, mentor, volunteer, faith-based organization.
-
Education: The nurse should educate the individual about stress prevention and treatment. The nurse should provide accurate or relevant or understandable information about stress or its causes or types or effects or signs; the reporting process and legal implications; the available services and resources; the treatment options and outcomes; the coping strategies and self-care techniques; the safety planning and protection measures; the rights and responsibilities of the individual; and the importance of follow-up and adherence to care.
-
Support: The nurse should support the individual’s physical or mental or emotional or social or spiritual healing. The nurse should provide holistic and culturally sensitive care that meets the individual needs or preferences or goals of the individual. The nurse should also provide therapeutic communication or active listening or empathy or validation or encouragement or praise to the individual. The nurse should also facilitate the development of a trusting or respectful or collaborative relationship with the individual. The nurse should also promote the empowerment or resilience or recovery of the individual. The nurse should also involve the family or significant others or community members in the care of the individual as appropriate.
-
Evaluation: The nurse should evaluate the outcomes of care for the individual. The nurse should use standardized tools or scales or questionnaires or interviews or observations to measure the progress or improvement or achievement of the expected outcomes. The expected outcomes may include:
-
The individual is free from further harm or injury.
-
The individual reports or demonstrates reduced pain or discomfort.
-
The individual’s physical wounds or infections are healed or treated.
-
The individual’s vital signs or laboratory tests or diagnostic tests are within normal limits or show improvement.
-
The individual reports or demonstrates reduced emotional or behavioral symptoms that are out of proportion to the severity or intensity of the stressor or that impair one’s functioning or relationships.
-
The individual reports or demonstrates increased happiness or confidence or self-worth or self-esteem or social skills or trust in others or expression of emotions or coping with stress.
-
The individual reports having a positive outlook on life and a sense of meaning and purpose.
-
The individual reports having a supportive network of family members, friends, peers, mentors, professionals, and community members.
-
The individual reports having a safe and secure environment at home, work, community, or institutional care. The individual reports having a safety plan and protection measures in place.
-
The individual reports or demonstrates reduced involvement or exposure to stressors.
-
The individual reports or demonstrates increased involvement or participation in positive activities or hobbies or interests or goals.
-
The individual reports or demonstrates increased adherence to medical care, legal assistance, social services, community services, and follow-up appointments.
-
The individual reports or demonstrates increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
-
The nurse should also monitor for any complications or adverse effects of the stress or the treatment such as infection, bleeding, shock, organ failure, sepsis, death, re-injury, re-victimization, re-traumatization, non-compliance, relapse, recurrence, dissatisfaction.
-
The nurse should also modify the plan of care as needed based on the evaluation of the outcomes and the feedback from the individual. The nurse should also collaborate with other members of the interdisciplinary team to ensure continuity and coordination of care. The nurse should also document the evaluation of the outcomes and any changes in the plan of care in a clear, concise, and objective manner.
Reactive Attachment Disorder (RAD)
-
Reactive attachment disorder (RAD) is a mental disorder that develops in early childhood after exposure to severe neglect or abuse or frequent changes in caregivers that prevent the formation of a secure attachment bond with a primary caregiver. RAD is characterized by a consistent pattern of inhibited or emotionally withdrawn behavior toward adult caregivers; a persistent social and emotional disturbance; and an evident lack of having typical childhood experiences of comfort, stimulation, and affection from adult caregivers.
-
RAD can be classified into two subtypes based on the predominant behavioral pattern: inhibited type and disinhibited type. Inhibited type is marked by a consistent pattern of emotionally withdrawn behavior toward adult caregivers, such as rarely seeking or responding to comfort when distressed, showing minimal social and emotional responsiveness to others, and having a limited positive affect. Disinhibited type is marked by a consistent pattern of indiscriminate social behavior toward adult caregivers, such as showing excessive familiarity or lack of selectivity in choosing attachment figures, approaching strangers in an overly friendly or inappropriate manner, and having difficulty maintaining appropriate boundaries with others.
Clinical Manifestations of RAD
-
The clinical manifestations of RAD may vary depending on the type and severity and duration and frequency of the neglect or abuse or caregiver changes; the age and developmental stage and personality and coping skills of the child; the availability of social support; the presence of comorbid conditions.
-
Some of the common clinical manifestations of RAD are:
-
Physical signs: such as failure to thrive; growth retardation; developmental delay; malnutrition; dehydration; poor hygiene; chronic illness; infection; injury; pain; fatigue; substance use disorder; suicidal ideation or behavior.
-
Psychological signs: such as depression; anxiety; panic disorder; phobias; obsessive-compulsive disorder (OCD); dissociative disorders; personality disorders; eating disorders; sleep disorders.
-
Emotional signs: such as fear; anger; guilt; shame; sadness; grief; loneliness; hopelessness; helplessness; low self-esteem; low self-confidence; low self-worth; distrust; resentment; bitterness.
-
Behavioral signs: such as withdrawal or isolation or avoidance or detachment or alienation or rejection; aggression or violence or vandalism or theft or lying or cheating or truancy or running away; recklessness or impulsivity or risk-taking; poor performance or attendance or participation in school or work; poor hygiene or grooming; changes in appetite or weight; changes in sleep patterns; substance use disorder; self-harm; suicidal thoughts or behaviors.
-
Social signs: such as lack of attachment or bonding or affection or trust or empathy with adult caregivers; lack of social skills or communication skills or interpersonal skills; lack of peer relationships or friendships; lack of involvement or participation in social activities or hobbies or interests; lack of respect or dignity; lack of autonomy or choice.
-
Spiritual signs: such as loss of faith or meaning or purpose or values or morals or ethics or hope.
-
-
The nursing assessment of RAD involves collecting subjective and objective data from the child and the caregiver and other sources such as family members, friends, neighbors, teachers, social workers, or health care providers.
-
The nursing assessment of RAD should be done in a safe, private, and comfortable environment with the child’s consent and cooperation. The nurse should use a calm, gentle, and supportive approach and avoid leading, suggestive, or judgmental questions. The nurse should also use developmentally appropriate language and tools such as dolls, drawings, or games to facilitate communication with the child.
-
The nursing assessment of RAD should include the following components:
-
History: The nurse should obtain a comprehensive history of the child’s physical, mental, emotional, social, and spiritual health and well-being; exposure to neglect or abuse or caregiver changes; current situation and concerns; coping strategies and support systems; strengths and resources.
-
Physical examination: The nurse should perform a thorough physical examination of the child’s head, neck, chest, abdomen, back, extremities, genitals, anus, and skin. The nurse should document any signs of injury or trauma or infection or pain or discomfort. The nurse should also assess the child’s vital signs, growth parameters, nutritional status, developmental milestones, pain level, and substance use status.
-
Laboratory tests: The nurse should order laboratory tests as indicated by the history and physical examination. Some of the common laboratory tests for RAD are complete blood count (CBC), coagulation studies, electrolytes, liver function tests (LFTs), renal function tests (RFTs), urine analysis (UA), urine toxicology screen (UTS), blood alcohol level (BAL), blood cultures, wound cultures.
-
Diagnostic tests: The nurse should order diagnostic tests as indicated by the history and physical examination. Some of the common diagnostic tests for RAD are x-rays, computed tomography (CT) scan, magnetic resonance imaging (MRI) scan, ultrasound, electroencephalogram (EEG), electrocardiogram (EKG), echocardiogram.
-
Psychological tests: The nurse should administer psychological tests as indicated by the history and physical examination. Some of the common psychological tests for RAD are Reactive Attachment Disorder Questionnaire (RADQ), Randolph Attachment Disorder Questionnaire (RADS), Attachment Behavior Q-Set (ABQ), Attachment Q-Sort (AQS), Strange Situation Procedure (SSP), Attachment Story Completion Task (ASCT), Separation Anxiety Test (SAT), Child Behavior Checklist (CBCL), Teacher Report Form (TRF), Youth Self-Report (YSR).
-
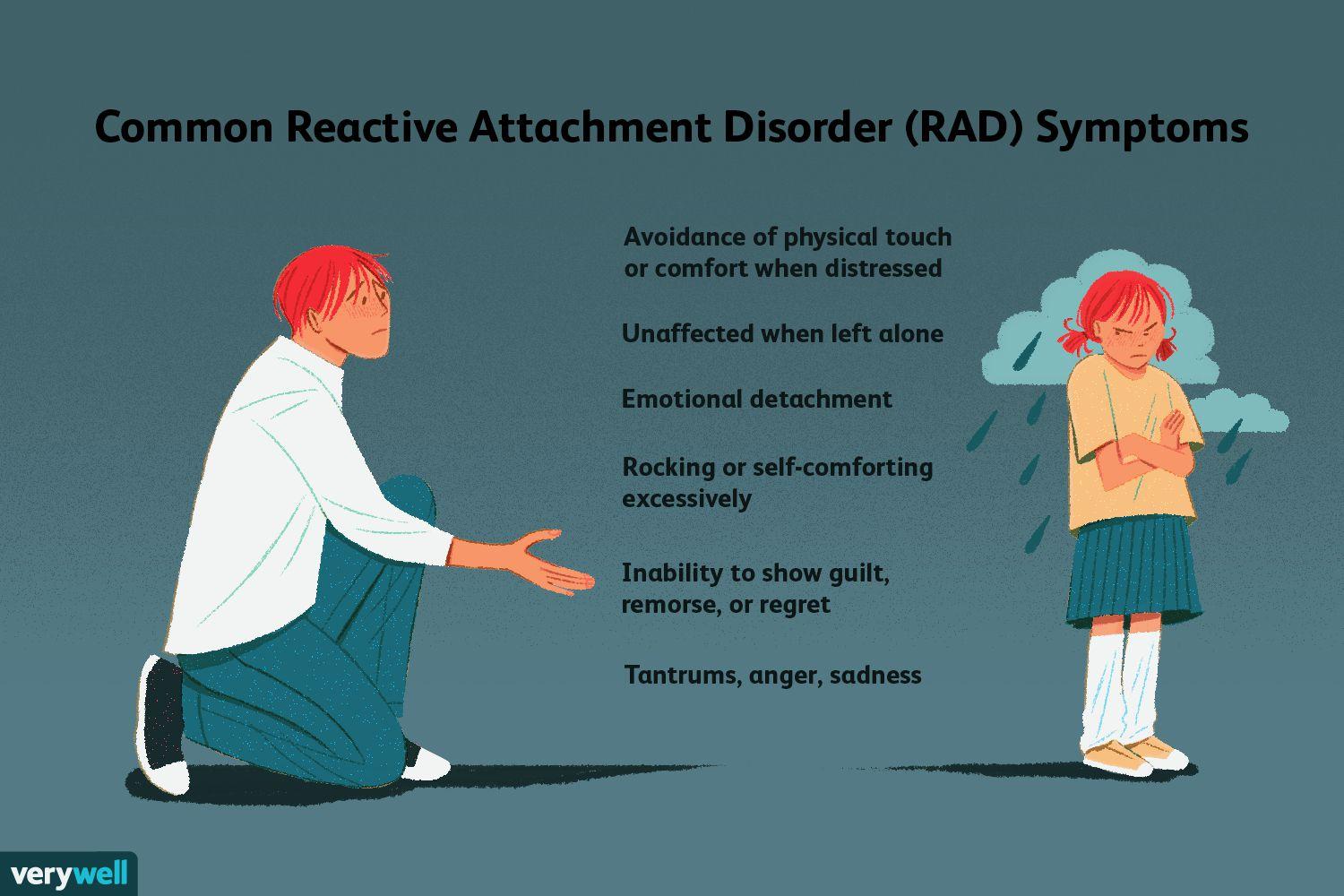
Nursing Assessment of RAD
Nursing Assessment of RAD
-
The nursing interventions for RAD are based on the nursing process and evidence-based practice. The nursing interventions for RAD aim to prevent further harm; protect the child’s rights; promote the child’s safety; report the suspected or confirmed neglect or abuse or caregiver changes; refer the child and the caregiver to appropriate services; educate the child and the caregiver about attachment development and disorder; support the child’s physical, mental, emotional, social, and spiritual healing; and evaluate the outcomes of care.
-
Some of the common nursing interventions for RAD are:
-
Prevention: The nurse should implement primary, secondary, and tertiary prevention strategies to reduce the risk of RAD. Primary prevention strategies include providing education, information, and resources to children, caregivers, families, and communities about attachment, its development, importance, types, and signs; the available services and resources; and the coping strategies and self-care techniques. Secondary prevention strategies include screening children and caregivers for risk factors or signs of RAD; providing counseling, therapy, support groups, home visits, crisis intervention, and respite care to children and caregivers who have been exposed to neglect or abuse or caregiver changes or are at risk of developing RAD; and monitoring children and caregivers for changes in behavior or health status. Tertiary prevention strategies include providing medical care, legal assistance, social services, foster care, adoption, kinship care, group homes, residential treatment centers, shelters, protection orders, and advocacy to children who have developed RAD; and facilitating reunification or alternative placement for children who have been removed from their homes due to neglect or abuse or caregiver changes.
-
Protection: The nurse should protect the child’s rights according to the United Nations Convention on the Rights of the Child. The nurse should respect the child’s dignity, autonomy, privacy, confidentiality, and participation in decision-making. The nurse should also protect the child from further harm by ensuring a safe and secure environment; removing or minimizing any potential sources of danger; and providing appropriate equipment, supplies, and medications to prevent or treat complications or infections. The nurse should also protect the child from re-traumatization by avoiding unnecessary or repeated examinations or procedures; using a trauma-informed approach; and providing emotional support and comfort to the child.
-
Reporting: The nurse should report any suspected or confirmed cases of neglect or abuse or caregiver changes to the appropriate authorities as mandated by the law and the professional code of ethics. The nurse should follow the reporting protocol of the institution or agency where he or she works. The nurse should document the facts and evidence of the neglect or abuse or caregiver changes in a clear, concise, and objective manner. The nurse should also inform the child and the caregiver about the reporting process and their rights and responsibilities. The nurse should cooperate with the investigation and provide any additional information or testimony as required.
-
Referral: The nurse should refer the child and the caregiver to appropriate services that can provide further assessment, treatment, support, and follow-up. Some of the common services that the nurse can refer to are:
-
Medical services: such as pediatrician, surgeon, dentist, ophthalmologist, otolaryngologist, dermatologist, gynecologist, urologist, endocrinologist, neurologist, psychiatrist, psychologist, nurse practitioner, physician assistant, nurse, social worker, pharmacist.
-
Legal services: such as lawyer, judge, prosecutor, defense attorney, police officer, detective, forensic examiner, child advocate, guardian ad litem, and court-appointed special advocate (CASA).
-
Social services: such as social worker, case manager, counselor, therapist, support group facilitator, home visitor, crisis intervention worker, respite care worker.
-
Educational services: such as teacher, counselor, tutor, special education teacher, speech therapist, occupational therapist, physical therapist, school nurse, school social worker.
-
Community services: such as attachment disorder prevention program or crisis hotline or helpline or support group or peer mentor or mentor or volunteer or faith-based organization.
-
-
Education: The nurse should educate the child and the caregiver about attachment development and disorder. The nurse should provide accurate or relevant or understandable information about attachment or its development or importance or types or signs; the causes or effects or signs of neglect or abuse or caregiver changes; the reporting process and legal implications; the available services and resources; the treatment options and outcomes; the coping strategies and self-care techniques; the safety planning and protection measures; the rights and responsibilities of the child and the caregiver; and the importance of follow-up and adherence to care.
-
Support: The nurse should support the child’s physical or mental or emotional or social or spiritual healing. The nurse should provide holistic and culturally sensitive care that meets the child’s needs or preferences or goals. The nurse should also provide therapeutic communication or active listening or empathy or validation or encouragement or praise to the child. The nurse should also facilitate the development of a trusting or respectful or collaborative relationship with the child. The nurse should also promote the empowerment or resilience or recovery of the child. The nurse should also involve the family or significant others or community members in the care of the child as appropriate.
-
Evaluation: The nurse should evaluate the outcomes of care for the child and the caregiver. The nurse should use standardized tools or scales or questionnaires or interviews or observations to measure the progress or improvement or achievement of the expected outcomes. The expected outcomes may include:
-
The child is free from further harm or injury.
-
The child reports or demonstrates reduced pain or discomfort.
-
The child’s physical wounds or infections are healed or treated.
-
The child’s vital signs or laboratory tests or diagnostic tests are within normal limits or show improvement.
-
The child reports or demonstrates a consistent pattern of inhibited or emotionally withdrawn behavior toward adult caregivers; a persistent social and emotional disturbance; and an evident lack of having typical childhood experiences of comfort, stimulation, and affection from adult caregivers (inhibited type) OR a consistent pattern of indiscriminate social behavior toward adult caregivers; showing excessive familiarity or lack of selectivity in choosing attachment figures; approaching strangers in an overly friendly or inappropriate manner; and having difficulty maintaining appropriate boundaries with others (disinhibited type).
-
The child reports or demonstrates increased happiness or confidence or self-worth or self-esteem or social skills or trust in others or expression of emotions or coping with stress.
-
The child reports having a positive outlook on life and a sense of meaning and purpose.
-
The child reports having a supportive network of family members, friends, peers, mentors, professionals, and community members.
-
The child reports having a safe and secure environment at home, school, community, or institutional care. The child reports having a safety plan and protection measures in place.
-
The child reports or demonstrates reduced involvement or exposure to neglect or abuse or caregiver changes.
-
-
-
The child reports or demonstrates increased involvement or participation in positive activities or hobbies or interests or goals.
-
The child reports or demonstrates increased adherence to medical care, legal assistance, social services, educational services, community services, and follow-up appointments.
-
The child reports or demonstrates increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
The nurse should also monitor for any complications or adverse effects of the neglect or abuse or caregiver changes or the treatment such as infection, bleeding, shock, organ failure, sepsis, death, re-injury, re-victimization, re-traumatization, non-compliance, relapse, recurrence, dissatisfaction.
-
The nurse should also modify the plan of care as needed based on the evaluation of the outcomes and the feedback from the child and the caregiver. The nurse should also collaborate with other members of the interdisciplinary team to ensure continuity and coordination of care. The nurse should also document the evaluation of the outcomes and any changes in the plan of care in a clear, concise, and objective manner.
Disinhibited Social Engagement Disorder (DSED)
-
Disinhibited social engagement disorder (DSED) is a mental disorder that develops in early childhood after exposure to severe neglect or abuse or frequent changes in caregivers that prevent the formation of a secure attachment bond with a primary caregiver. DSED is characterized by a consistent pattern of indiscriminate social behavior toward adult caregivers; showing excessive familiarity or lack of selectivity in choosing attachment figures; approaching strangers in an overly friendly or inappropriate manner; and having difficulty maintaining appropriate boundaries with others.
-
DSED is a subtype of reactive attachment disorder (RAD) and shares some common features with it. However, DSED differs from RAD in that children with DSED do not show inhibited or emotionally withdrawn behavior toward adult caregivers; do not have a persistent social and emotional disturbance; and do not lack typical childhood experiences of comfort, stimulation, and affection from adult caregivers.
Clinical Manifestations of DSED
-
The clinical manifestations of DSED may vary depending on the type and severity and duration and frequency of the neglect or abuse or caregiver changes; the age and developmental stage and personality and coping skills of the child; the availability of social support; the presence of comorbid conditions.
-
Some of the common clinical manifestations of DSED are:
-
Physical signs: such as failure to thrive; growth retardation; developmental delay; malnutrition; dehydration; poor hygiene; chronic illness; infection; injury; pain; fatigue; substance use disorder; suicidal ideation or behavior.
-
Psychological signs: such as depression; anxiety; panic disorder; phobias; obsessive-compulsive disorder (OCD); dissociative disorders; personality disorders; eating disorders; sleep disorders.
-
Emotional signs: such as fear; anger; guilt; shame; sadness; grief; loneliness; hopelessness; helplessness; low self-esteem; low self-confidence; low self-worth; distrust; resentment; bitterness.
-
Behavioral signs: such as withdrawal or isolation or avoidance or detachment or alienation or rejection; aggression or violence or vandalism or theft or lying or cheating or truancy or running away; recklessness or impulsivity or risk-taking; poor performance or attendance or participation in school or work; poor hygiene or grooming; changes in appetite or weight; changes in sleep patterns; substance use disorder; self-harm; suicidal thoughts or behaviors.
-
Social signs: such as lack of attachment or bonding or affection or trust or empathy with adult caregivers; lack of social skills or communication skills or interpersonal skills; lack of peer relationships or friendships; lack of involvement or participation in social activities or hobbies or interests; lack of respect or dignity; lack of autonomy or choice.
-
Spiritual signs: such as loss of faith or meaning or purpose or values or morals or ethics or hope.
-
Nursing Assessment of DSED
-
The nursing assessment of DSED involves collecting subjective and objective data from the child and the caregiver and other sources such as family members, friends, neighbors, teachers, social workers, or health care providers.
-
The nursing assessment of DSED should be done in a safe, private, and comfortable environment with the child’s consent and cooperation. The nurse should use a calm, gentle, and supportive approach and avoid leading, suggestive, or judgmental questions. The nurse should also use developmentally appropriate language and tools such as dolls, drawings, or games to facilitate communication with the child.
-
The nursing assessment of DSED should include the following components:
-
History: The nurse should obtain a comprehensive history of the child’s physical, mental, emotional, social, and spiritual health and well-being; exposure to neglect or abuse or caregiver changes; current situation and concerns; coping strategies and support systems; strengths and resources.
-
Physical examination: The nurse should perform a thorough physical examination of the child’s head, neck, chest, abdomen, back, extremities, genitals, anus, and skin. The nurse should document any signs of injury trauma or infection pain or discomfort. The nurse should also assess the child’s vital signs, growth parameters, nutritional status, developmental milestones, pain level, and substance use status.
-
Laboratory tests: The nurse should order laboratory tests as indicated by the history and physical examination. Some of the common laboratory tests for DSED are complete blood count (CBC), coagulation studies, electrolytes, liver function tests (LFTs), renal function tests (RFTs), urine analysis (UA), urine toxicology screen (UTS), blood alcohol level (BAL), blood cultures, wound cultures.
-
Diagnostic tests: The nurse should order diagnostic tests as indicated by the history and physical examination. Some of the common diagnostic tests for DSED are X-rays, computed tomography (CT) scans, magnetic resonance imaging (MRI) scans, ultrasound, electroencephalogram (EEG), electrocardiogram (EKG), and echocardiogram.
-
Psychological tests: The nurse should administer psychological tests as indicated by the history and physical examination. Some of the common psychological tests for DSED are Disinhibited Social Engagement Disorder Questionnaire (DSEDQ), Disinhibited Social Engagement Disorder Interview (DSEDI), Structured Clinical Interview for DSM-5 Disorders (SCID-5), Child Behavior Checklist (CBCL), Teacher Report Form (TRF), Youth Self-Report (YSR).
-
Nursing Interventions for DSED
-
The nursing interventions for DSED are based on the nursing process and evidence-based practice. The nursing interventions for DSED aim to prevent further harm; protect the child’s rights; promote the child’s safety; report the suspected or confirmed neglect or abuse or caregiver changes; refer the child and the caregiver to appropriate services; educate the child and the caregiver about attachment development and disorder; support the child’s physical, mental, emotional, social, and spiritual healing; and evaluate the outcomes of care.
-
Some of the common nursing interventions for DSED are:
-
Prevention: The nurse should implement primary, secondary, and tertiary prevention strategies to reduce the risk of DSED. Primary prevention strategies include providing education, information, and resources to children, caregivers, families, and communities about attachment, its development, importance, types, and signs; the available services and resources; and the coping strategies and self-care techniques. Secondary prevention strategies include screening children and caregivers for risk factors or signs of DSED; providing counseling, therapy, support groups, home visits, crisis intervention, and respite care to children and caregivers who have been exposed to neglect or abuse or caregiver changes or are at risk of developing DSED; and monitoring children and caregivers for changes in behavior or health status. Tertiary prevention strategies include providing medical care, legal assistance, social services, foster care, adoption, kinship care, group home, residential treatment center, shelter, protection orders, and advocacy to children who have developed DSED; and facilitating reunification or alternative placement for children who have been removed from their homes due to neglect or abuse or caregiver changes.
-
Protection: The nurse should protect the child’s rights according to the United Nations Convention on the Rights of the Child. The nurse should respect the child’s dignity, autonomy, privacy, confidentiality, and participation in decision-making. The nurse should also protect the child from further harm by ensuring a safe and secure environment; removing or minimizing any potential sources of danger; and providing appropriate equipment or supplies or medications to prevent or treat complications or infections. The nurse should also protect the child from re-traumatization by avoiding unnecessary or repeated examinations or procedures; using a trauma-informed approach; and providing emotional support and comfort to the child.
-
Reporting: The nurse should report any suspected or confirmed cases of neglect or abuse or caregiver changes to the appropriate authorities as mandated by the law and the professional code of ethics. The nurse should follow the reporting protocol of the institution or agency where he or she works. The nurse should document the facts and evidence of the neglect or abuse or caregiver changes in a clear, concise, and objective manner. The nurse should also inform the child and the caregiver about the reporting process and their rights and responsibilities. The nurse should cooperate with the investigation and provide any additional information or testimony as required.
-
Referral: The nurse should refer the child and the caregiver to appropriate services that can provide further assessment, treatment, support, and follow-up. Some of the common services that the nurse can refer to are:
-
Medical services: such as pediatrician, surgeon, dentist, ophthalmologist, otolaryngologist, dermatologist, gynecologist, urologist, endocrinologist, neurologist, psychiatrist, psychologist, nurse practitioner, physician assistant, nurse, social worker, pharmacist.
-
Legal services: such as lawyer, judge, prosecutor, defense attorney, police officer, detective, forensic examiner, child advocate, guardian ad litem, court-appointed special advocate (CASA).
-
Social services: such as social worker, case manager, counselor, therapist, support group facilitator, home visitor, crisis intervention worker, respite care worker.
-
Educational services: such as teacher, counselor, tutor, special education teacher, speech therapist, occupational therapist, physical therapist, school nurse, school social worker.
-
Community services: such as attachment disorder prevention program or crisis hotline or helpline or support group or peer mentor or mentor or volunteer or faith-based organization.
-
-
Education: The nurse should educate the child and the caregiver about attachment development and disorder. The nurse should provide accurate or relevant or understandable information about attachment or its development or importance or types or signs; the causes or effects or signs of neglect or abuse or caregiver changes; the reporting process and legal implications; the available services and resources; the treatment options and outcomes; the coping strategies and self-care techniques; the safety planning and protection measures; the rights and responsibilities of the child and the caregiver; and the importance of follow-up and adherence to care.
-
Support: The nurse should support the child’s physical or mental or emotional or social or spiritual healing. The nurse should provide holistic and culturally sensitive care that meets the child’s needs or preferences or goals. The nurse should also provide therapeutic communication or active listening or empathy or validation or encouragement or praise to the child. The nurse should also facilitate the development of a trusting or respectful or collaborative relationship with the child. The nurse should also promote the empowerment or resilience or recovery of the child. The nurse should also involve the family or significant others or community members in the care of the child as appropriate.
-
Evaluation: The nurse should evaluate the outcomes of care for the child and the caregiver. The nurse should use standardized tools or scales or questionnaires or interviews or observations to measure the progress or improvement or achievement of the expected outcomes. The expected outcomes may include:
-
The child is free from further harm or injury.
-
The child reports or demonstrates reduced pain or discomfort.
-
The child’s physical wounds or infections are healed or treated.
-
The child’s vital signs or laboratory tests or diagnostic tests are within normal limits or show improvement.
-
The child reports or demonstrates a consistent pattern of indiscriminate social behavior toward adult caregivers; showing excessive familiarity or lack of selectivity in choosing attachment figures; approaching strangers in an overly friendly or inappropriate manner; and having difficulty maintaining appropriate boundaries with others.
-
The child reports or demonstrates increased happiness or confidence or self-worth or self-esteem or social skills or trust in others or expression of emotions or coping with stress.
-
The child reports having a positive outlook on life and a sense of meaning and purpose.
-
The child reports having a supportive network of family members, friends, peers, mentors, professionals, and community members.
-
The child reports having a safe and secure environment at home, school, community, or institutional care. The child reports having a safety plan and protection measures in place.
-
The child reports or demonstrates reduced involvement or exposure to neglect or abuse or caregiver changes.
-
-
-
The child reports or demonstrates increased involvement or participation in positive activities or hobbies or interests or goals.
-
The child reports or demonstrates increased adherence to medical care, legal assistance, social services, educational services, community services, and follow-up appointments.
-
The child reports or demonstrates increased satisfaction with the quality of care and the relationship with the nurse and other professionals.
-
The nurse should also monitor for any complications or adverse effects of the neglect or abuse or caregiver changes or the treatment such as infection, bleeding, shock, organ failure, sepsis, death, re-injury, re-victimization, re-traumatization, non-compliance, relapse, recurrence, dissatisfaction.
-
The nurse should also modify the plan of care as needed based on the evaluation of the outcomes and the feedback from the child and the caregiver. The nurse should also collaborate with other members of the interdisciplinary team to ensure continuity and coordination of care. The nurse should also document the evaluation of the outcomes and any changes in the plan of care in a clear, concise, and objective manner.
