
Pain assessment and management in children
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Differentiate between acute, chronic, and mixed-pain conditions in pediatric patients.
- Identify appropriate observational pain tools for infants and non-verbal children.
- Select age-appropriate self-report pain rating scales for verbal children.
- Assess the unique challenges and strategies for measuring pain in special populations or those with cognitive impairments.
- Evaluate the role of biobehavioral interventions in a holistic pain management plan.
- Compare the indications and side effects of non-opioids, opioids, and coanalgesic medications.
- Analyze the benefits and risks of various delivery methods, including PCA and epidural analgesia.
- Determine the critical monitoring parameters for preventing and managing analgesic-related side effects.
Introduction
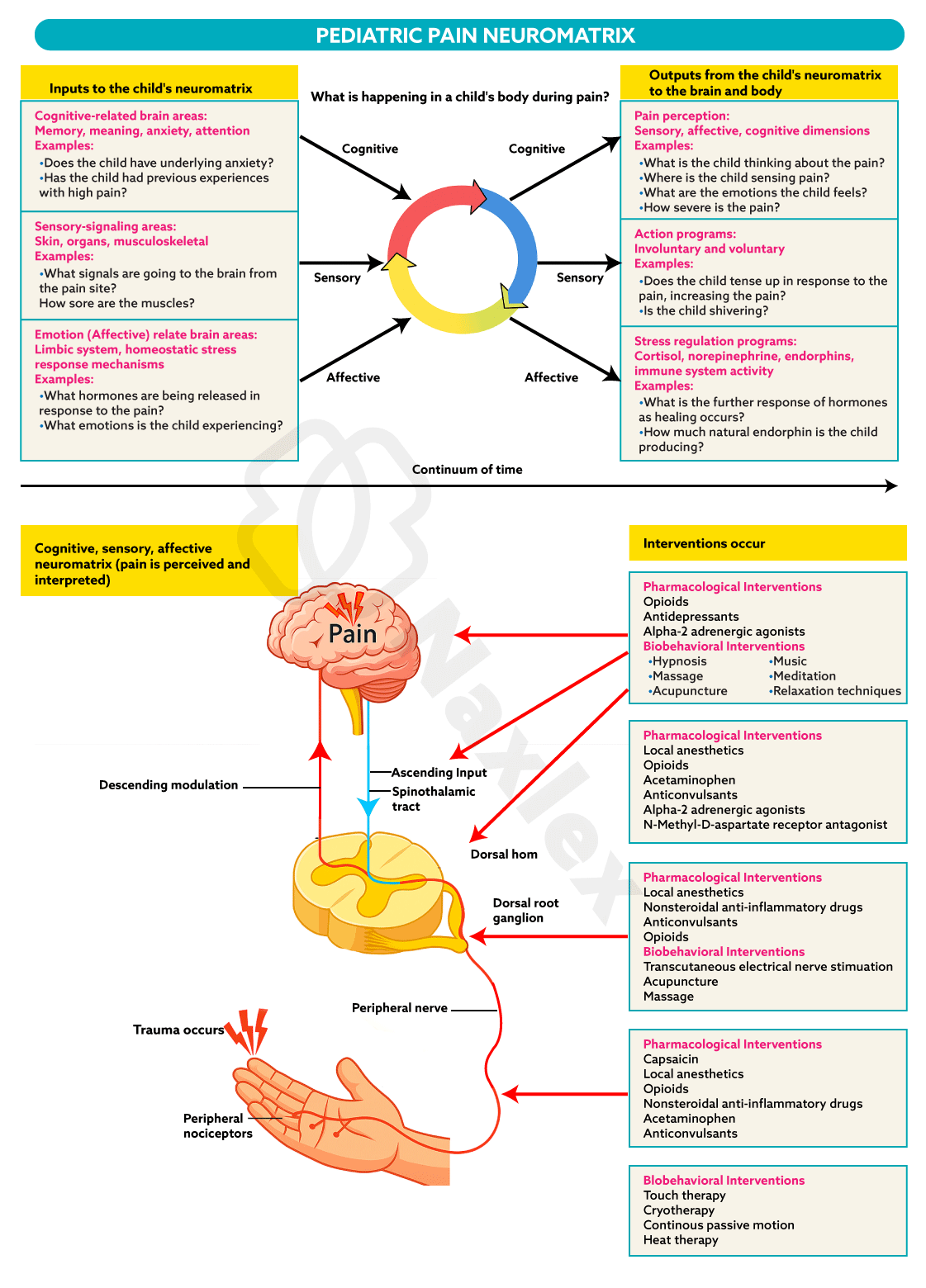
- Pain is a complex, subjective experience, and its assessment in children presents unique challenges such as requiring a sophisticated understanding of a child’s developmental stage, cognitive abilities, and emotional maturity.
- Children, especially infants and toddlers, may be unable to verbalize their pain, requiring nurses to rely on behavioral and physiological cues.
- The primary goal of effective assessment is to bridge the communication gap between the young patient and the healthcare provider. For neonates and infants, nurses rely on physiological indicators and behavioral markers, such as crying patterns and facial grimacing, captured through validated observational tools.
- As children grow, the focus shifts toward self-report scales, which empower the child to quantify their own experience using visual aids like faces or numerical lines.
- Pain assessment in children is a critical nursing skill that requires a blend of observational and self-report techniques tailored to the child's age and developmental stage.
- The key goal of pain management is not just to relieve pain, but to do so in a way that is safe and supports the child's overall well-being and development.
- Effective pain management improves healing, reduces stress, and fosters trust between the child, family, and healthcare team.
- Understanding the different types of pain, acute, chronic, and mixed, is essential for accurate diagnosis and management.
- Accurate pain assessment is the essential precursor to any successful intervention; without a precise measurement of intensity and character, the implementation of pharmacological or biobehavioral therapies remains a matter of guesswork rather than evidence-based care.
Types of pain
3.1. Acute Pain Conditions
Acute pain is sudden in onset and typically short-lived, with a clear cause. It serves as a warning signal of actual or potential tissue damage.
- Needlestick Pain: A common cause of acute pain and anxiety in children, often associated with immunizations or blood draws. The pain is sharp and localized, and the associated fear can be a significant barrier to care.
- Postoperative Pain: Pain that occurs after a surgical procedure. It is a predictable and often severe type of acute pain, which, if not managed effectively, can delay recovery, prolong hospital stays, and increase the risk of developing chronic pain.
- Nursing Insight: Proactive pain management for acute pain, especially post-op, is crucial. Administering analgesics on a schedule prevents the pain from escalating, making it easier to manage.
3.2. Chronic Pain Conditions
Chronic pain persists for more than three months or beyond the expected period of healing. It can significantly impact a child's quality of life, school attendance, and emotional health.
- Headaches: Common in children and can be classified as migraines or tension-type headaches. Assessment includes identifying triggers, frequency, and severity.
- Abdominal Pain: Often functional in nature, meaning there is no underlying organic cause, though it requires thorough medical evaluation to rule out conditions like inflammatory bowel disease.
- Musculoskeletal Pain: Includes conditions like juvenile idiopathic arthritis (JIA) or growing pains. The pain can affect mobility and daily activities.
- Neuropathic Pain Syndromes: Result from damage to the nervous system. The pain is often described as burning, shooting, or tingling. Conditions include complex regional pain syndrome (CRPS).
- Nursing Insight: Chronic pain management requires a holistic, multidisciplinary approach. Nursing care extends beyond medication to include emotional support, education on coping mechanisms, and collaboration with physical therapists and psychologists.
3.3. Mixed-Pain Conditions
Mixed-pain conditions involve elements of both acute and chronic pain. The pain is often severe, persistent, and challenging to manage.
- Burn Pain: This is a combination of acute pain from the initial injury, ongoing pain from dressing changes and debridement, and chronic neuropathic pain as the skin heals.
- Cancer Pain: Can be acute (e.g., from surgery or a procedure) or chronic (e.g., from tumor growth or treatments like chemotherapy and radiation).
- Sickle Cell Pain: Characterized by episodic, severe, acute pain crises (vaso-occlusive crises) that can also lead to chronic pain over time.
Measuring pain in children
5.1. Observational Pain Measures
For infants and nonverbal children, nurses must rely on observational pain measures. These scales assess a child's behavioral and physiological responses to pain.
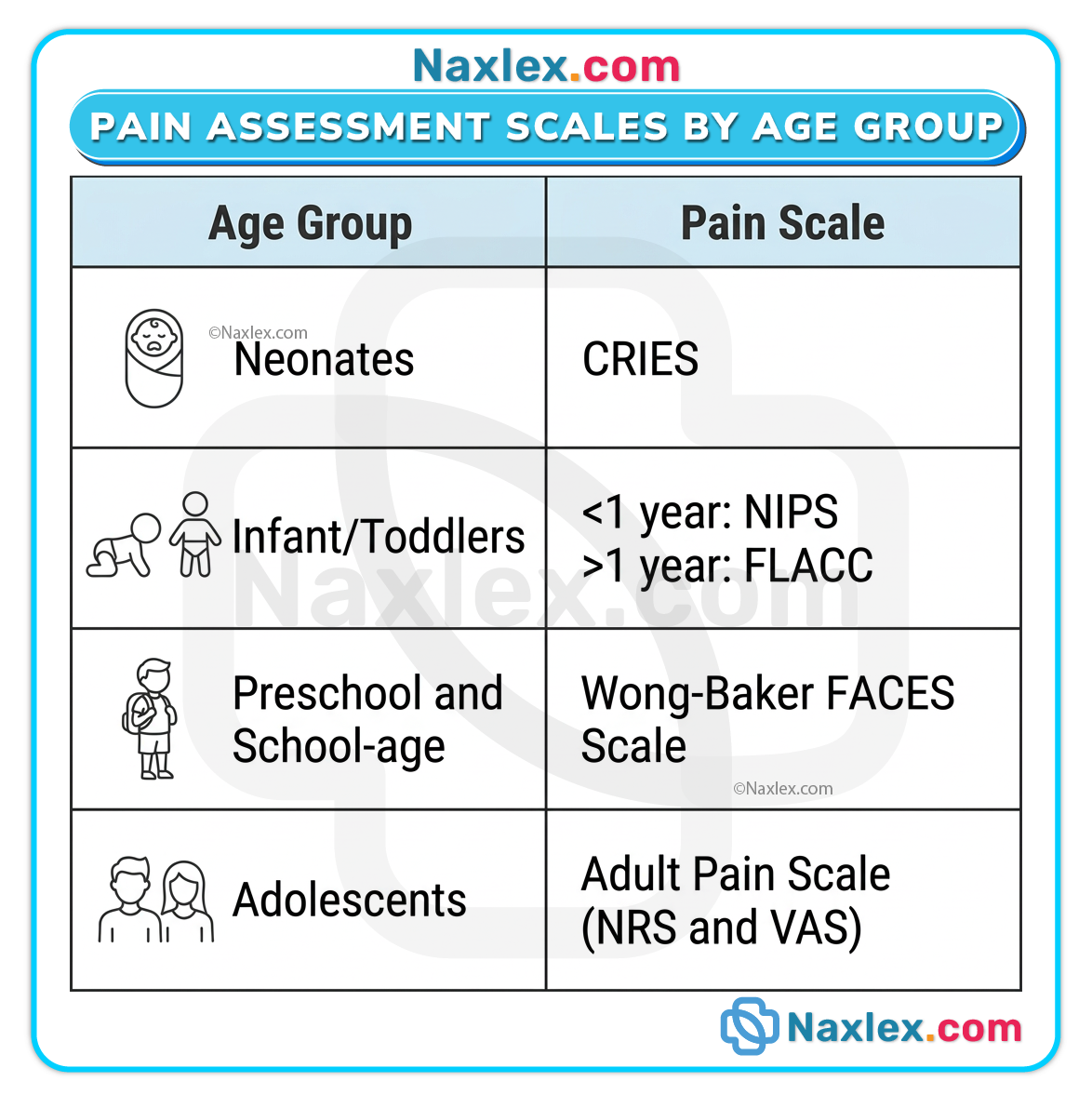
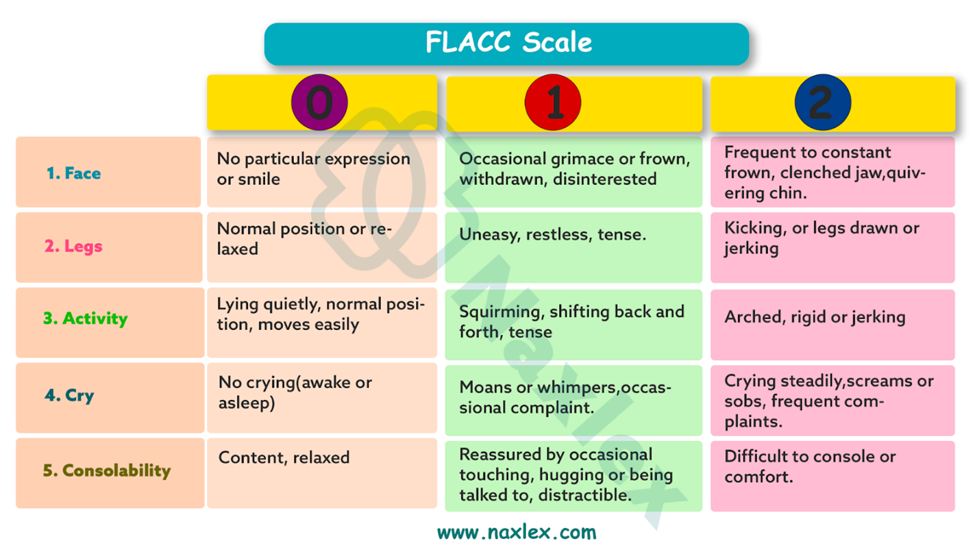
- FLACC Scale: Used for children from 2 months to 7 years. It stands for Face, Legs, Activity, Cry, and Consolability. The nurse rates each category from 0-2, with a total score from 0-10.
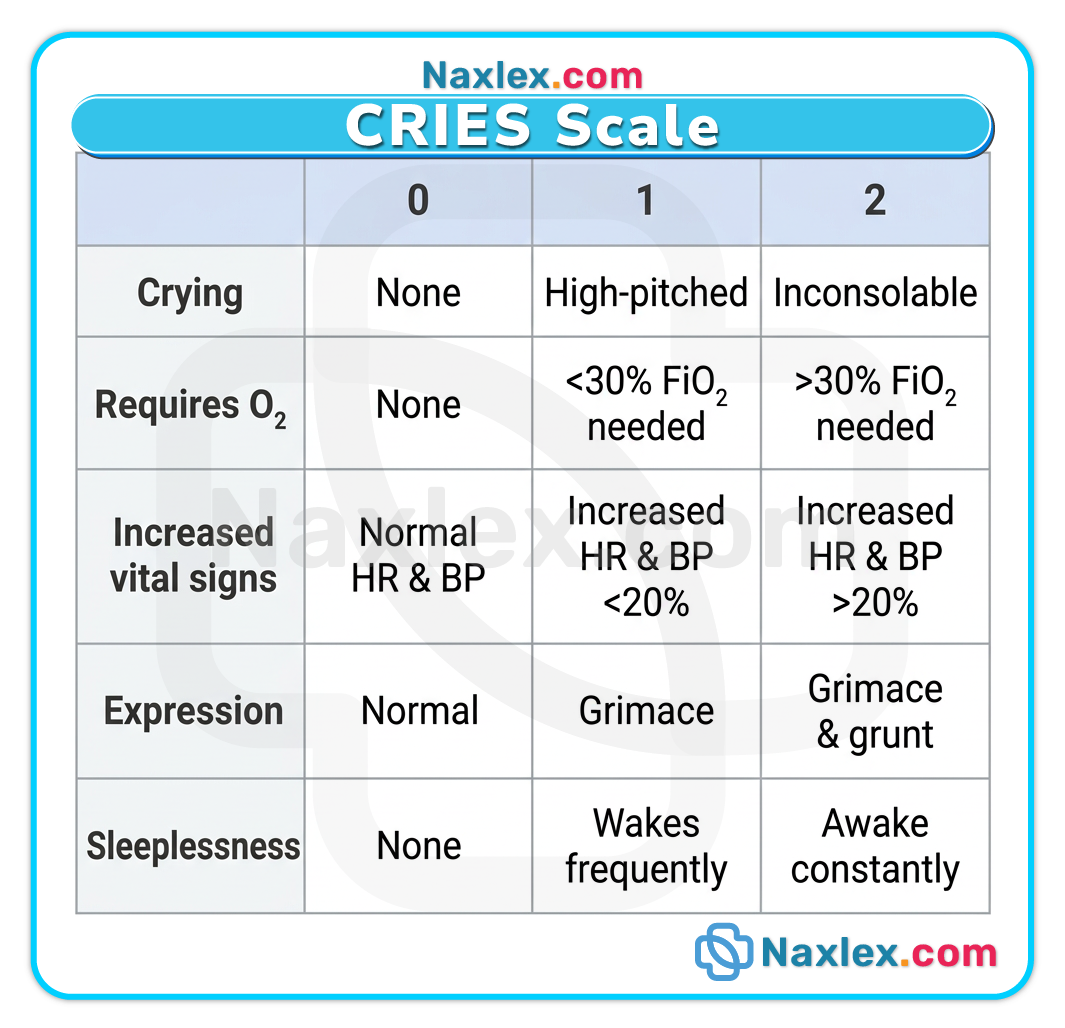
- CRIES Scale: Used for neonates. It assesses Crying, Requires O2, Increased vital signs, Expression, and Sleeplessness.
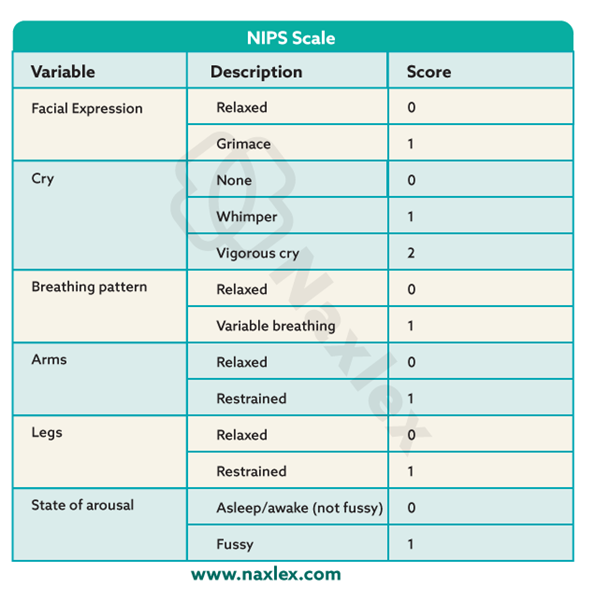
- NIPS Scale: Used for infants up to 1 year. It assesses facial expression, crying, breathing patterns, arm and leg movements, and state of arousal.
Nursing Insight: Consistent use of a single, validated observational tool by all healthcare providers ensures reliable and accurate pain assessment.
5.2. Special Populations
- Preterm Infants: Use specialized scales like the Premature Infant Pain Profile (PIPP), which considers gestational age and behavioral states.
- Cognitively Impaired Children: May not be able to use self-report scales. Nurses should use observational tools and rely on caregivers who know the child's typical behaviors. The Non-Communicating Children's Pain Checklist (NCCPC) is a useful tool.
- Children Postanesthesia: Nurses must monitor for signs of pain as the child emerges from anesthesia and is unable to self-report.
- Children in the Pediatric Intensive Care Unit (PICU): Pain assessment can be complicated by sedation, mechanical ventilation, and multiple procedures. Use tools like the Critical-Care Pain Observation Tool (CPOT).
5.3. Self-Report Pain Rating Scales
For children over 3-4 years old, self-report is the gold standard for pain assessment.
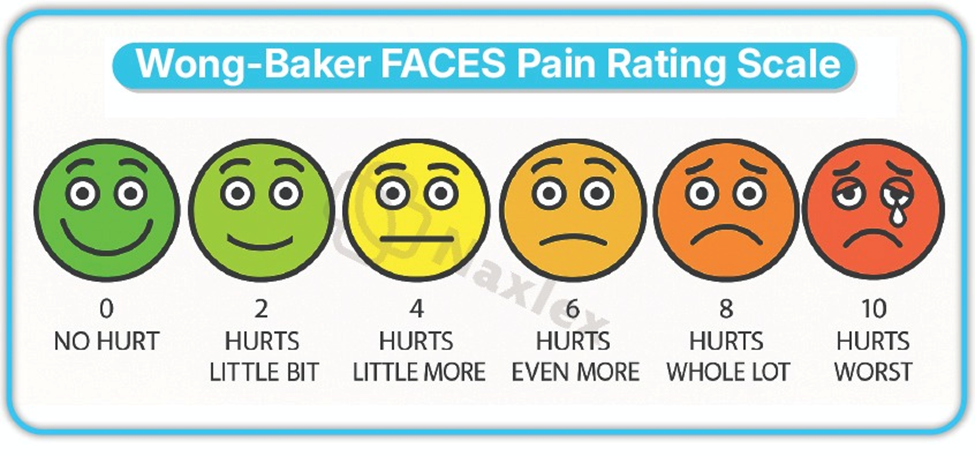
- Wong-Baker Faces Pain Rating Scale: Consists of six faces ranging from a smiling face for "no pain" to a crying face for "worst pain." It is suitable for children as young as 3.
- Faces Pain Scale-Revised (FPS-R): A similar scale with seven faces, but without the smile or tears. It is anchored with a 0-10 numerical scale and is considered more neutral.
- Word-Graphic Rating Scale: Uses a series of descriptive words (e.g., "no pain," "a little pain," "worst pain") for children who can read.
- The NCCPC (Non-Communicating Children's Pain Checklist) is a behavioral pain scale used by parents and caregivers to assess acute and chronic pain in children who are unable to express their pain verbally. It is particularly useful for children with cognitive impairments, developmental disabilities, or severe neurological conditions.
- Nursing Insight: Take the time to explain the scale to the child, ensuring they understand how to use it correctly to represent their pain level.
5.4. Multidimensional Measures
These scales assess pain from multiple perspectives, including location, quality, intensity, and impact on a child's life.
- Pediatric Pain Questionnaire (PPQ): Assesses the child's and parent's perception of the pain.
- Functional Disability Inventory (FDI): Measures how pain impacts a child's daily functioning.
- Pediatric Quality of Life Inventory (PedsQL): Assesses the child's health-related quality of life.
- Pediatric Migraine Disability Assessment Scale (PedMIDAS): Specifically for children with migraines, it measures the impact of headaches on school, home, and social activities.
Prevention and treatment of pain in children
6.1. Biobehavioral Interventions
These are non-pharmacologic strategies that focus on the child's psychological and behavioral responses to pain.
- Distraction: Using toys, games, bubbles, or music to divert a child's attention from a painful procedure.
- Relaxation Techniques: Deep breathing exercises, guided imagery, or muscle relaxation.
- Massage and Positioning: Gentle touch can reduce muscle tension and provide comfort. Proper positioning in infants can reduce procedural pain.
- Sweet-Tasting Solutions: For infants, a few drops of sucrose solution on the tongue before a procedure (e.g., heel stick) can provide a calming, analgesic effect.
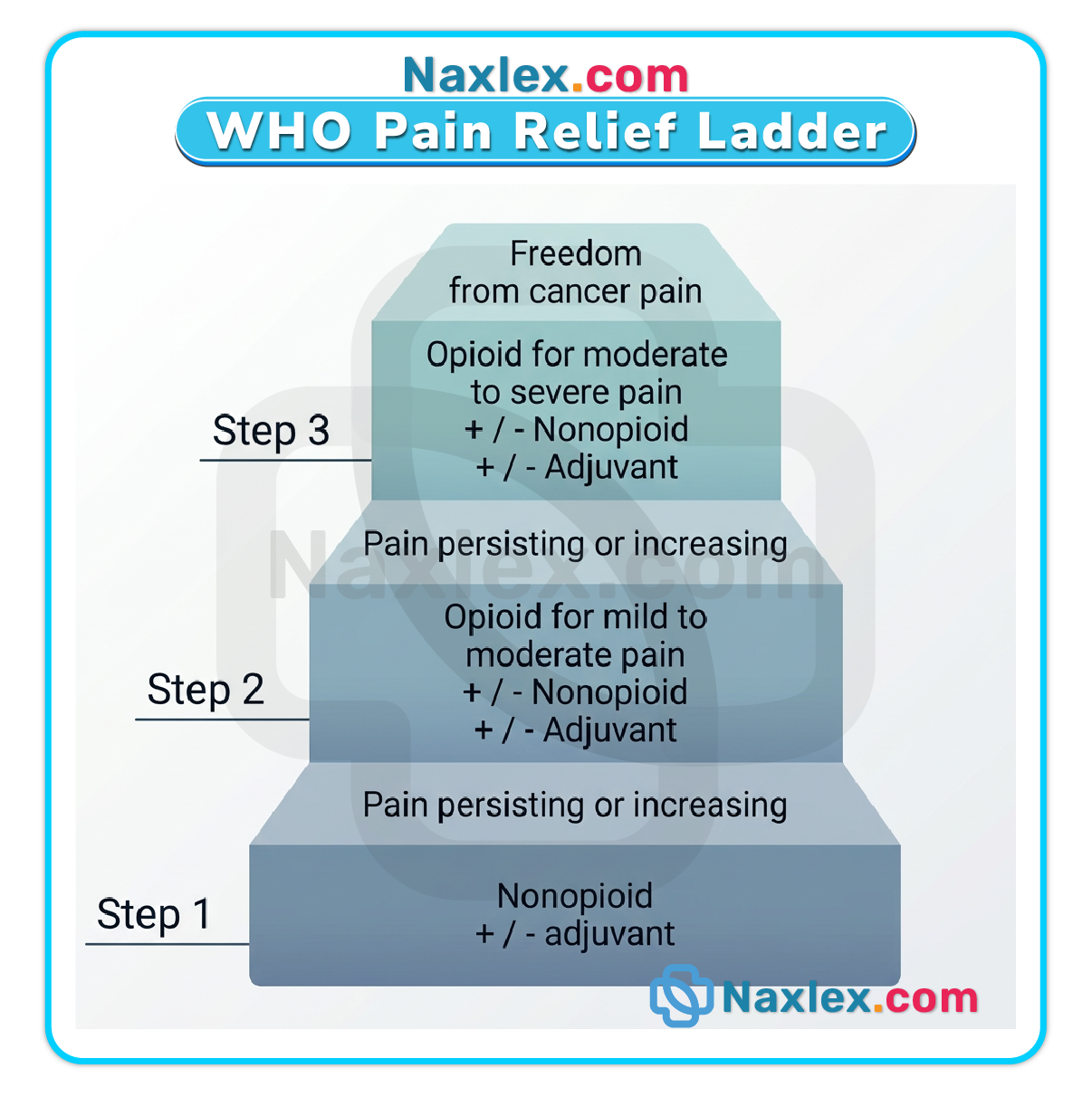
6.2. Pharmacologic Management of Pain
- Pharmacologic management follows the World Health Organization (WHO) pain ladder, starting with non-opioids and escalating as needed.
Non-opioids:
- Acetaminophen: A first-line agent for mild-to-moderate pain. It is an effective antipyretic and analgesic.
- Nonsteroidal Anti-inflammatory Drugs (NSAIDs): (e.g., ibuprofen, naproxen). Useful for inflammatory pain.
Opioids:
- Used for moderate-to-severe pain. Morphine is the gold standard. Fentanyl is often used for short procedures. Hydromorphone is another potent option.
Coanalgesic Drugs:
- Medications used to enhance the effect of primary analgesics or treat specific types of pain. Examples include anxiolytics, antidepressants, and anti-seizure medications (for neuropathic pain).
Choosing the Pain Medication Dose:
- Doses are based on the child's weight and are often calculated in milligrams per kilogram (mg/kg).
Choosing the Timing of Analgesic:
- Medications should be given on a scheduled basis (around the clock) for continuous pain, rather than waiting for the child to report pain.
Choosing the Method of Administration:
- Oral: Preferred route when possible.
- Intravenous (IV): Used for moderate-to-severe pain or when the oral route is not feasible.
- Intramuscular (IM): Avoided due to pain and unreliable absorption.
Patient-Controlled Analgesia (PCA):
- Allows the child to self-administer small, preset doses of pain medication (usually an opioid) by pressing a button. This is suitable for children as young as 5-6 years old who understand the concept.
Epidural Analgesia:
- A catheter is placed in the epidural space to deliver a continuous infusion of local anesthetics and/or opioids. Provides excellent regional pain control, especially for lower body and abdominal surgeries.
Transmucosal and Transdermal Analgesia:
- Transmucosal: Fentanyl lollipops or lozenges are used for acute procedural pain.
- Transdermal: Fentanyl patches are used for chronic pain management. EMLA cream (a topical anesthetic) is applied to the skin before needlesticks to numb the area.
Monitoring Side Effects:
- For opioids, nurses must closely monitor for respiratory depression, sedation, constipation, nausea, and vomiting. Use of a sedation scale is essential.
Specific Strategies for Special Populations:
- Pain Prevention for Needlestick: Use EMLA cream, distraction, and sweet-tasting solutions.
- Care During Painful and Invasive Procedures: Provide procedural sedation, use comfort positioning, and involve child life specialists.
- Biobehavioral Interventions with Postsurgical Pain: Combine pharmacologic agents with distraction and relaxation to enhance pain relief and reduce anxiety.
- Pain Management in Obese and Overweight Children: Use ideal body weight for dosing certain medications (e.g., opioids) to prevent overdosing.
- Treatment of Chronic Pain: Requires a multidisciplinary approach involving pharmacologic, physical therapy, and psychological interventions.
- Pain with Pediatric Cancer: Often requires potent opioids and coanalgesics.
- Pain Prevention and Treatment for Children with Sickle Cell Disease: Involves both chronic pain management and acute crisis management with hydration, warmth, and opioids.
- Pain Treatment During End-of-Life Care: The focus shifts to providing comfort and relieving suffering, often with higher doses of opioids.
Nursing Insight: Always verify medication dosages, especially weight-based calculations, with another nurse. Monitor for side effects and be prepared to intervene, particularly for respiratory depression with opioids.
Summary
- Effective pediatric pain management is a critical component of compassionate healthcare, requiring a nuanced understanding of how children experience and communicate distress.
- Because children vary significantly in their developmental stages and verbal abilities, nurses must move beyond a "one size fits all" approach.
- The clinical management of pediatric pain begins with identifying its nature, which is generally categorized into acute, chronic, or mixed conditions.
- Acute pain is typically sudden and time-limited, often resulting from injury or surgery, whereas chronic pain persists beyond the expected healing time, as seen in juvenile idiopathic arthritis.
- Mixed conditions, such as sickle cell anemia, often involve elements of both.
- To quantify this experience, providers utilize observational measures for infants and non-verbal children, focusing on facial expressions and body movements, while relying on self-report scales for older children who can articulate their discomfort.
- Special populations, including children with cognitive impairments, require tailored observational tools to ensure their distress is not overlooked.
- Comprehensive assessments may also include multidimensional measures that evaluate how pain impacts a child's sleep, mood, and daily activities.
- Treatment involves a synergy of biobehavioral interventions, such as distraction and relaxation, and a robust pharmacological framework. This framework ranges from non-opioids like acetaminophen to opioids for severe pain, supplemented by coanalgesic drugs to enhance relief.
- Safe administration is paramount and nurses must carefully choose the dose, timing, and route, whether via patient-controlled analgesia (PCA), epidural, or transdermal patches, while strictly monitoring for side effects.
- For special populations, these strategies are further refined to balance maximum efficacy with the highest safety standards, ensuring that every child receives individualized and humane care.
