
Pediatric Anatomy And Physiology Of The Respiratory Tract
Study Questions
Comprehensive Questions
A small degree of inflammation in a child's airway can lead to a disproportionately large increase in airway resistance compared to an adult. Which of the following is the primary reason for this?
Explanation
The primary reason a small degree of inflammation in a child’s airway causes a disproportionately large increase in airway resistance is the significantly narrower airway diameter. According to Poiseuille’s law, resistance to airflow is inversely proportional to the fourth power of the radius, meaning even a slight reduction in airway size greatly increases resistance.
Rationale for correct answer:
4. A child’s airway is much narrower than an adult’s, so swelling or mucus buildup reduces the radius substantially, causing a dramatic increase in resistance and work of breathing. This makes conditions like croup or bronchiolitis more severe in young children.
Rationale for incorrect answers:
1. While children do have higher metabolic rates and oxygen demands, this is not the main reason for the exaggerated effect of inflammation on airway resistance.
2. The cartilaginous and flexible trachea in infants contributes to collapsibility but does not explain the disproportionate rise in resistance from swelling.
3. Greater diaphragmatic reliance affects breathing mechanics but not the mathematical relationship between airway narrowing and resistance.
Take home points
- Airway resistance is highly sensitive to changes in radius, especially in children due to their small baseline diameters.
- Even minor airway swelling (e.g., 1 mm circumferential edema) can reduce the cross-sectional area by more than half in a child.
- Rapid recognition and management of pediatric airway inflammation is critical to prevent respiratory distress and hypoxia.
Which of the following are anatomical features that make infants and children more susceptible to respiratory distress and disease? Select all that apply
Explanation
Infants and children have multiple anatomical and physiological characteristics that increase their vulnerability to respiratory distress and disease. These features make them less able to compensate for airway compromise, infection, or increased oxygen demands.
Rationale for correct answers:
1. Fewer and smaller alveoli: At birth, the lungs have a limited number of alveoli, which grow in number and size over early childhood. This reduces the surface area for gas exchange, making them more prone to hypoxia during illness.
2. More compliant, cartilaginous chest wall: A softer chest wall can lead to retractions and inefficient ventilation when respiratory effort increases.
3. Higher, more anterior larynx: This anatomical position makes airway obstruction more likely and complicates airway management during resuscitation or intubation.
Rationale for incorrect answers:
4. Infants actually have a higher metabolic rate and oxygen consumption (about twice that of adults per kg body weight). This increases their vulnerability to hypoxia when breathing is compromised.
Take home points
- Pediatric airways are smaller, more collapsible, and more easily obstructed than adult airways.
- Immature lung development limits gas exchange capacity.
- High oxygen needs and low reserves mean children can deteriorate rapidly.
- Early recognition and intervention are essential to prevent severe hypoxia.
The primary function of the mucociliary clearance system is to:
Explanation
The mucociliary clearance system is a key innate defense mechanism of the respiratory tract, designed to trap and remove inhaled particles, pathogens, and debris before they reach the lower airways and alveoli.
Rationale for correct answer:
1. The respiratory epithelium contains mucus-producing goblet cells and ciliated cells. Mucus traps inhaled contaminants, and coordinated ciliary beating moves the mucus upward toward the pharynx, where it can be swallowed or expectorated. This process helps prevent infections and maintains airway cleanliness.
Rationale for incorrect answers:
2. While moisture in the alveoli facilitates gas exchange, this is not the main role of the mucociliary clearance system, alveolar moisture regulation is handled by surfactant and fluid balance mechanisms, not cilia and mucus.
3. Adaptive immunity involves lymphocytes and antigen-specific responses, which are separate from the mechanical clearance provided by the mucociliary system.
4. Angiotensin-converting enzyme (ACE) production occurs mainly in the pulmonary capillary endothelium, not as part of mucociliary clearance.
Take home points
- The mucociliary escalator is an essential first-line defense in the respiratory tract.
- Smoking, dehydration, and certain diseases (e.g., cystic fibrosis, primary ciliary dyskinesia) can impair this system, increasing infection risk.
- Efficient mucociliary function is especially important in children, whose immune systems are still developing.
Which statement about the defense mechanisms of the pediatric respiratory tract is correct?
Explanation
Lymphoid tissues such as the tonsils and adenoids form part of the Waldeyer’s ring and play a vital role in local immune surveillance of the upper respiratory tract, detecting and responding to inhaled or ingested pathogens.
Rationale for correct answer:
2. Lymphoid tissue like tonsils and adenoids provide local immune surveillance and defense. These structures contain immune cells (B and T lymphocytes) that detect antigens entering through the nose and mouth, initiating immune responses to help prevent infection spread.
Rationale for incorrect answers:
1. Alveolar macrophages are part of the innate immune system, not adaptive immunity. They engulf and destroy pathogens and debris but do not produce specific antibodies.
3. Infants’ cough and sneeze reflexes are actually less forceful and less coordinated than adults’, making clearance of secretions less efficient.
4. Secretory Immunoglobulin A (sIgA) is part of the active mucosal immune system, not passive immunity. Passive immunity is typically acquired via maternal antibodies (e.g., IgG via placenta, IgA via breast milk).
Take home points
- The pediatric respiratory tract uses multiple defense layers: mechanical (mucociliary clearance), reflexive (cough/sneeze), and immune (lymphoid tissue, sIgA, macrophages).
- Tonsils and adenoids are particularly important in early childhood but can also be a site of chronic infection or hypertrophy leading to obstruction.
What is the primary muscle of respiration in a newborn infant, and why is this significant?
Explanation
The diaphragm is the primary muscle of respiration in newborn infants. This is significant because their intercostal muscles are underdeveloped, and their rib cages are highly compliant, so they rely almost entirely on diaphragmatic movement for ventilation.
Rationale for correct answer:
3. In newborns, diaphragmatic contraction creates negative pressure to draw air into the lungs. If the diaphragm tires due to illness, hypoxia, or increased work of breathing, ventilation can rapidly deteriorate since accessory muscle use is limited.
Rationale for incorrect answers:
1. Sternocleidomastoid muscles are accessory muscles used during respiratory distress, not for quiet breathing in healthy infants.
2. Intercostal muscles are not fully developed in newborns and provide minimal contribution to chest wall stability or ventilation.
4. Abdominal muscles assist in forced exhalation and coughing but are not the primary drivers of quiet respiration.
Take home points
- Infants’ dependence on the diaphragm makes them vulnerable to respiratory fatigue in prolonged distress.
- Conditions that impair diaphragmatic function (e.g., sepsis, neuromuscular disorders, fatigue from tachypnea) can cause rapid deterioration.
- Early recognition of increased work of breathing is essential, as infants have limited reserves.
Which of these factors contributes to infants’ and children's increased risk for upper airway obstruction as compared with adults?
Explanation
Infants and young children have anatomical and physiological differences in their upper airways compared to adults that increase their risk for airway obstruction. These differences include a smaller and more flexible airway structure and narrower passages, which make them more vulnerable to swelling and obstruction.
Rationale for correct answer:
1. Underdeveloped cricoid cartilage and narrow nasal passages contribute significantly to the increased risk of upper airway obstruction in infants and children. The cricoid cartilage is the narrowest part of a child’s airway and is less rigid than in adults, making it more prone to collapse or swelling. Narrow nasal passages can become easily blocked by secretions or inflammation, further compromising airflow.
Rationale for incorrect answers:
2. Tonsils in children tend to be relatively large, not small, and can contribute to obstruction. The nasal passages are narrow, but this option misses the critical role of cricoid cartilage development.
3. The child’s larynx is funnel-shaped, not cylindrical, with the narrowest point at the cricoid cartilage. While sinuses develop over time, their underdevelopment doesn’t directly increase risk of upper airway obstruction.
4. Children actually have proportionally larger tongues relative to their oral cavity, which can contribute to obstruction, so “smaller tongue” is inaccurate.
Take home points
- Infants and children have a funnel-shaped, narrower airway with a less rigid cricoid cartilage, making them more susceptible to airway obstruction.
- Narrow nasal passages add to the risk by limiting airflow, especially during inflammation.
- Understanding these anatomical differences is critical when assessing respiratory distress in pediatric patients.
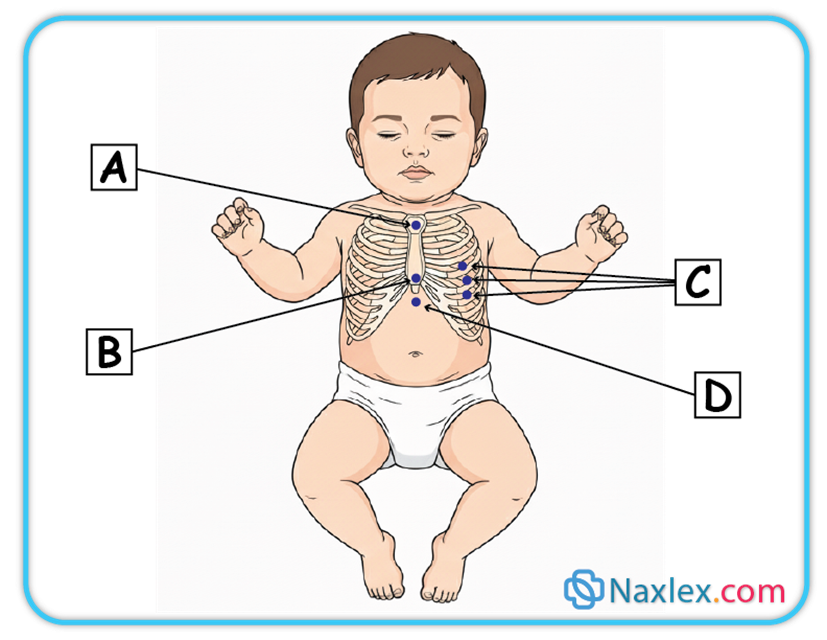
A nurse notes substernal retractions when assessing a child. At which area on the illustration did the nurse make this observation?
Explanation
Retractions are a clinical sign of increased work of breathing, often seen in infants and children. They occur when soft tissues around the chest wall are pulled inward during inspiration due to negative intrathoracic pressure, usually because the child is struggling to get enough air into the lungs.
Rationale for correct answer:
4. D: Substernal retractions are inward pulling of the soft tissue just beneath the sternum/xiphoid (subxiphoid/epigastric area). This reflects increased negative intrathoracic pressure and is common in moderate- severe respiratory distress.
Rationale for incorrect answers:
1. A: This represents suprasternal retractions, typically seen at the sternal notch with upper-airway obstruction (e.g., croup, laryngomalacia). Not “substernal.”
2. B: The xiphoid itself is the bony tip; retractions are named for the soft tissue below it (subxiphoid/substernal). At the xiphisternum isn’t the same as below the sternum.
3. C: Those are intercostal retractions along the lateral chest wall, not beneath the sternum.
Take home points
- Retractions are classified by location: suprasternal (above sternum), intercostal (between ribs), subcostal (below ribs), and substernal (below sternum).
- The more severe the respiratory distress, the more locations you may see retractions in simultaneously.
- Substernal retractions often point to lower airway or lung pathology (e.g., bronchiolitis, asthma, pneumonia).
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Analyze the anatomical differences between the pediatric and adult respiratory systems, focusing on airway diameter and tongue size.
- Evaluate the physiological implications of the infant’s compliant chest wall and reliance on diaphragmatic breathing.
- Identify the structural components of the upper and lower respiratory tracts in children and their susceptibility to obstruction.
- Explain the primary and secondary functions of the respiratory tract, including gas exchange and acid-base balance.
- Assess respiratory function in children using objective data such as breath sounds, work of breathing, and pulse oximetry.
- Interpret diagnostic procedures commonly used in pediatric pulmonology, including blood gas analysis and pulmonary function tests.
- Describe the innate defenses of the pediatric respiratory tract, such as the mucociliary escalator and alveolar macrophages.
- Formulate nursing interventions that prioritize airway patency based on pediatric-specific anatomical vulnerabilities.
Introduction
- Understanding the pediatric respiratory system is the most critical skill for a pediatric nurse, as respiratory failure is the primary cause of cardiac arrest in children.
- Unlike adults, children are not merely smaller versions of grown-ups since they possess unique anatomical and physiological variations that make them highly susceptible to respiratory distress.
- The pediatric airway is significantly smaller in diameter, roughly the size of the child's pinky finger, meaning that even a small amount of edema or mucus can cause a catastrophic increase in airway resistance.
- Furthermore, infants are "obligate nose breathers" until approximately 4 to 6 months of age, meaning nasal congestion alone can lead to significant respiratory compromise.
- Physiologically, the child's respiratory system is in a constant state of development. The chest wall is highly compliant due to the cartilaginous nature of the ribs, which allows for retractions during distress rather than the effective expansion of the lungs.
- Because the intercostal muscles are immature, infants rely heavily on the diaphragm for ventilation. This "diaphragmatic breathing" makes them vulnerable to abdominal distension, which can impede the diaphragm's movement and decrease tidal volume.
- Children also have a higher metabolic rate and oxygen consumption than adults but fewer alveoli for gas exchange, leaving them with very little "respiratory reserve" during illness.
- Assessment in the pediatric population requires the nurse to be a keen observer of subtle shifts. A child’s "work of breathing" is a primary indicator of their clinical status.
- Nurses must be proficient at identifying nasal flaring, grunting, and various types of retractions (substernal, intercostal, suprasternal) that signal the use of accessory muscles.
- By mastering the structural and functional nuances of the pediatric respiratory tract, the nurse can intervene early, preventing the rapid progression from respiratory distress to failure.
Variation In Pediatric Anatomy And Physiology
Children are not just "small adults." Their distinct anatomy and physiology predispose them to respiratory issues:
|
Feature |
Pediatric Variation |
Clinical Implication |
|
Airway Size |
Narrower diameter, especially the trachea and bronchi. |
Smaller decrease in radius causes a much greater increase in airway resistance (Poiseuille's Law: resistance is inversely proportional to r4). Quickly prone to obstruction from edema or mucus. Even mild swelling can compromise a baby's airway significantly. |
|
Larynx & Glottis |
Higher in the neck (C3-C4 vs. C5-C6 in adults); funnel-shaped (narrowest point is the cricoid ring in infants). |
This shape makes them prone to subglottic stenosis and makes intubation challenging. |
|
Tongue |
Proportionately larger than in adults. |
Easily occludes the pharynx when muscle tone is decreased (e.g., during sleep, sedation, or illness). |
|
Epiglottis |
Longer, floppier, and more U-shaped. |
Greater risk for acute epiglottitis and obstruction. |
|
Chest Wall |
More cartilaginous, compliant, and less rigid (ribs are horizontal). |
Offers poor leverage for the intercostal muscles; chest wall retractions are common during distress and are a sign of respiratory effort. |
|
Diaphragm |
Primary muscle of respiration; muscle fibers are less fatigue-resistant. |
Fatigue occurs faster, leading to respiratory failure. Monitor for signs of diaphragmatic fatigue (e.g., reduced grunting, paradoxical breathing). |
|
Metabolic Rate & O2 Consumption |
Higher (about 2x that of an adult per kg of body weight). |
They require more O2; any compromise leads to hypoxia faster. |
|
Alveoli |
Fewer in number and smaller at birth; increase rapidly up to age 8. |
Less surface area for gas exchange, reducing reserve capacity. |
|
Obligate Nose Breathers |
Infants (especially those under 4-6 months) |
Nasal congestion (e.g., from a common cold) is a major problem causing significant feeding and respiratory distress. Nasal suctioning (e.g., with a bulb syringe) and saline drops before feeds/sleep are vital interventions. |
Respiratory Tract Structure
The respiratory tract is divided into upper and lower sections:
A. Upper Respiratory Tract (Above the Larynx)
- Nose and Nasal Cavity: Filters, warms, and humidifies air. Contains ciliated mucosa.
- Pharynx: Passageway for air and food (nasopharynx, oropharynx, laryngopharynx).
- Tonsils and Adenoids: Lymphoid tissue; prominent in children, providing immune defense but can obstruct the airway when hypertrophied.
- Larynx (Voice Box): Contains the vocal cords; separates the upper and lower tract.
B. Lower Respiratory Tract (Below the Larynx)
- Trachea (Windpipe): Cartilaginous tube extending to the carina (bifurcation point). In children, it is shorter.
- Bronchi: The right main bronchus is shorter, wider, and straighter than the left, making it the more common site for aspiration of foreign bodies.
- Bronchioles: Small air passages lacking cartilage; rely on surrounding tissue for support. Prone to collapse and spasm (e.g., in asthma/bronchiolitis).
- Alveoli: Microscopic air sacs where gas exchange occurs.
Functions Of The Respiratory Tract
1. Gas Exchange
This is the fundamental biological purpose of breathing. It occurs at the microscopic level within the alveoli, which are tiny air sacs wrapped in a dense network of capillaries.
- Oxygenation: Oxygen (O2) is inhaled into the alveoli, where it crosses a thin membrane into the blood to be transported to cells for energy production.
- Carbon Dioxide Removal: As a byproduct of metabolism, carbon dioxide (CO2) moves from the blood into the alveoli to be exhaled.
2. Air Conditioning
The lungs are delicate; cold, dry, or dirty air can damage the underlying tissues. The upper respiratory tract (nose and pharynx) prepares the air before it reaches the deep lungs:
- Warming: Blood flowing through the nasal mucosa acts like a radiator, bringing air closer to body temperature.
- Humidifying: Mucus and moisture from the respiratory lining add water vapor to the air to prevent the lungs from drying out.
- Filtering: Large particles are trapped by nasal hairs, while smaller particles stick to the mucous membranes.
3. Acid-Base Balance
The respiratory system works alongside the kidneys to maintain the body's pH level (ideally around 7.4). Because CO2 dissolves in the blood to form carbonic acid (H2CO3), the rate of breathing directly impacts blood acidity:
- Hyperventilation: Breathing faster/deeper flushes out CO2. Since there is less acid, the blood pH become more alkaline.
- Hypoventilation: Breathing slower/shallower allows CO2 to build up. This creates more acid, causing the blood pH to become more acidic.
4. Speech and Olfaction
While essential for survival, the respiratory tract also facilitates communication and sensory input:
- Speech: As air is exhaled, it passes through the larynx (voice box). The controlled vibration of the vocal cords, combined with the movement of the tongue and lips, produces sound.
- Olfaction: Inhaled air carries odor molecules to the olfactory epithelium at the roof of the nasal cavity. These signals are sent directly to the brain, allowing us to perceive smells.
5. Defense Mechanisms
The respiratory system is constantly exposed to the external environment, requiring a robust defense strategy:
- The Mucociliary Escalator: Cilia line the airways and move in a rhythmic "wave" to push trapped dust and pathogens upward toward the throat to be swallowed or coughed out.
- Immune Cells: Alveolar macrophages "patrol" the deep lungs to ingest and destroy any bacteria or viruses that bypass the upper filters.
Assessment Of Respiration Function
A rapid, systematic assessment is critical for identifying impending respiratory failure.
A. Physical Assessment Components
|
Observation |
Explanation |
Significance |
|
Respiration |
Rate (Tachypnea is often the first sign of distress). Depth (shallow or deep). Rhythm (regular or irregular). |
Count respirations for a full minute in infants/young children due to their irregular patterns. |
|
Retractions |
Visible sinking of the chest wall with inspiration due to the use of accessory muscles to overcome high airway resistance or poor lung compliance. Types: Suprasternal, Supraclavicular, Intercostal, Subcostal.
|
Mild: Intercostal only. Severe: Multiple areas, including supraclavicular/suprasternal. Indicates significant respiratory effort. |
|
Nasal Flaring |
Widening of the nostrils on inspiration. |
An attempt to decrease nasal airway resistance and increase the amount of air inhaled. A significant sign of distress, especially in infants. |
|
Head Bobbing |
Accessory muscle use where the head lifts with inspiration and falls with exhalation. |
Sign of severe distress and exhaustion, often seen in infants. |
|
Noisy Breathing |
Any sound other than clear breath sounds (e.g., stridor, grunting, wheezing). |
Localizes the problem (upper vs. lower airway). |
|
Stridor |
A high-pitched, harsh sound heard primarily on inspiration. |
Indicative of upper airway obstruction (e.g., Croup, foreign body, epiglottitis). Requires immediate attention. |
|
Grunting |
A short, low-pitched sound heard on expiration as the child attempts to keep the alveoli open. |
Sign of alveolar collapse/poor lung compliance (e.g., pneumonia, RDS). Self-preservation mechanism (like PEEP). |
|
Wheezing |
A high-pitched, musical whistling sound heard primarily on expiration. |
Indicative of lower airway obstruction/narrowing (e.g., Asthma, Bronchiolitis). Due to air attempting to pass through constricted bronchioles. |
|
Color Changes (Skin/Mucous Membranes) |
Pallor (early sign due to vasoconstriction). Cyanosis (late sign of O2 deprivation; central cyanosis in the lips/mucous membranes is an emergency). Cyanosis
|
Cyanosis is often a very late sign in children because they have a high Hgb concentration. Do not wait for cyanosis! |
|
Chest Pain |
Pain in the chest, often sharp and worse with deep breaths/cough (pleuritic). |
Can be related to coughing, infection (pleurisy), or inflammation. |
|
Clubbing |
Bulbous enlargement of the fingertips/toes. |
Sign of chronic hypoxia (e.g., Cystic Fibrosis, congenital heart disease). Takes time to develop. |
|
Cough |
Reflex to clear the airway. Characterized by quality (dry, wet/productive, "seal-like" in Croup) and timing. |
A sudden onset of a non-productive cough, especially in a toddler, suggests foreign body aspiration until proven otherwise. |
Diagnostic Procedures
A. Pulmonary Function Tests (PFTs)
- Purpose: Measure lung volumes, capacities, flow rates, and gas exchange.
- Methods: Spirometry is the most common, measuring Forced Vital Capacity (FVC) and Forced Expiratory Volume in 1 second (FEV1).
- Pediatric Consideration: Requires cooperation, so reliable PFTs are typically performed in children over age 6.
B. Radiology
- Chest X-ray (CXR): Provides an image of the lungs, heart, and bony structures. Used to diagnose pneumonia, atelectasis, pneumothorax, and view foreign bodies.
- CT/MRI: Used for more detailed imaging of masses, congenital anomalies, or complex infections.
C. Blood Gas Determination (Arterial Blood Gas - ABG or Venous Blood Gas - VBG)
- Purpose: Assesses the adequacy of O2, ventilation, and acid-base status (pH, HCO3).
- Interpretation: A rising PaCO2 (hypercapnia) indicates impending respiratory failure in a child who is tiring out.
D. Non-Invasive Monitoring
- Pulse Oximetry (SpO2): Measures the percentage of hemoglobin saturated with oxygen. The easiest and most common method to monitor O2 status. Ensure proper probe placement (fingers, toes, earlobe) for an accurate reading. Movement or poor circulation can cause false low readings.
- Capnography (End-Tidal CO2 - EtCO2): Measures the maximum CO2 concentration at the end of exhalation. Excellent for monitoring ventilation status and is a reliable, continuous indicator of breathing adequacy.
E. Other Diagnostic Procedures
- Sputum/Nasal Swabs: To identify pathogens (e.g., RSV, Influenza, Mycoplasma).
- Bronchoscopy: Direct visualization of the airway, often used for removing foreign bodies or for biopsies.
Defenses Of The Respiratory Tract
The respiratory tract has multiple lines of defense to protect the delicate gas exchange surfaces:
- Lymphoid Tissues (Tonsils & Adenoids): Located at the entrance of the pharynx, they trap inhaled pathogens and produce immune cells.
- Epiglottis: A flap of cartilage that covers the entrance to the trachea during swallowing, preventing aspiration of food/liquid into the lungs.
- Mucous Blanket: A sticky layer secreted by goblet cells that lines the airway, trapping dust, pollen, and microorganisms.
- Ciliary Action (Mucociliary Escalator): Tiny hair-like projections (cilia) beat rhythmically, pushing the mucus blanket (and trapped debris) up and out of the lower airway toward the pharynx to be swallowed or coughed out.
- Cough: A vital involuntary reflex that clears the lower airways of mucus and foreign materials.
- Position Changes (Movement): Mobilization and frequent turning help to redistribute air and promote the drainage of secretions, preventing atelectasis and pneumonia.
- Lymphatics: A network of vessels and nodes that filter and trap pathogens and fluid from the lungs, promoting systemic immunity.
- Humoral Defenses: Immune components found in the blood and secretions, including:
- Immunoglobulin A (IgA): Found in respiratory secretions, providing localized immunity.
- Macrophages: Immune cells that engulf and destroy foreign particles, especially in the alveoli.
Summary
- The pediatric respiratory system is a dynamic and vulnerable system that requires specialized nursing vigilance.
- The anatomical variations, such as a larger tongue in a smaller oropharynx, a more cephalad larynx, and a funnel-shaped airway, create a high risk for obstruction.
- Nurses must integrate these anatomical facts into every assessment, recognizing that a child’s airway is most narrowed at the cricoid cartilage.
- When performing diagnostic procedures, such as pulse oximetry or arterial blood gases, the nurse must interpret results through the lens of age-specific norms, acknowledging that children desaturate much faster than adults due to their high metabolic demands.
- In clinical practice, the assessment of respiratory function must be holistic. Nurses should look for the "triple threat" of pediatric respiratory distress: tachypnea, retractions, and altered mental status (irritability or lethargy).
- Understanding the defenses of the respiratory tract allows the nurse to support the child’s natural immunity, such as encouraging hydration to keep the mucociliary escalator functioning effectively.
- Diagnostic tools like chest X-rays or peak flow meters are utilized to monitor structural changes and airway patency, but they never replace the nurse's clinical observation of the child’s color, effort, and breath sounds.
- The goal of pediatric respiratory nursing is the maintenance of an effective airway and adequate oxygenation.
- By anticipating the rapid transition from distress to failure, nurses can implement life-saving interventions such as positioning, oxygen administration, and suctioning.
- By understanding the fragility of the child's anatomy and the limitations of their physiology, the nurse acts as the critical safeguard for the child's most basic life-sustaining function.
