
Perioperative Nursing Care
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
To:
- Describe the surgical experience, including perioperative phases, classifications of surgery, types of anesthesia, informed consent and advance directives, and outpatient/same-day surgery.
- Conduct a preoperative nursing history and physical assessment to identify patient strengths as well as factors that increase risks for surgical and postoperative complications.
- Prepare a patient physically and psychologically for surgery.
- Identify assessments and interventions specific to the prevention of complications in the immediate and early postoperative phases.
- Use the nursing process to develop an individualized plan of care for the surgical patient during each phase of the perioperative period.
Introduction
Surgery may be done for a variety of reasons:
- to cure or minimize disease
- to diagnose the specific presence of a disease or condition
- to reconstruct or eliminate a defect
- to enhance form and function
- to prescribe appropriate postoperative treatment and prognosis
- to palliate, or offer comfort, when cure is not possible
- to follow up or monitor an incurable disease process
- to offer a preventative option when disease is inevitable, such as an elective, prophylactic mastectomy for a woman at high risk for breast cancer.
Surgery may be planned or unplanned, elective/optional or necessary, major or minor, and may involve any body part or system.
Nursing care provided for the patient before, during, and after surgery is called perioperative nursing.
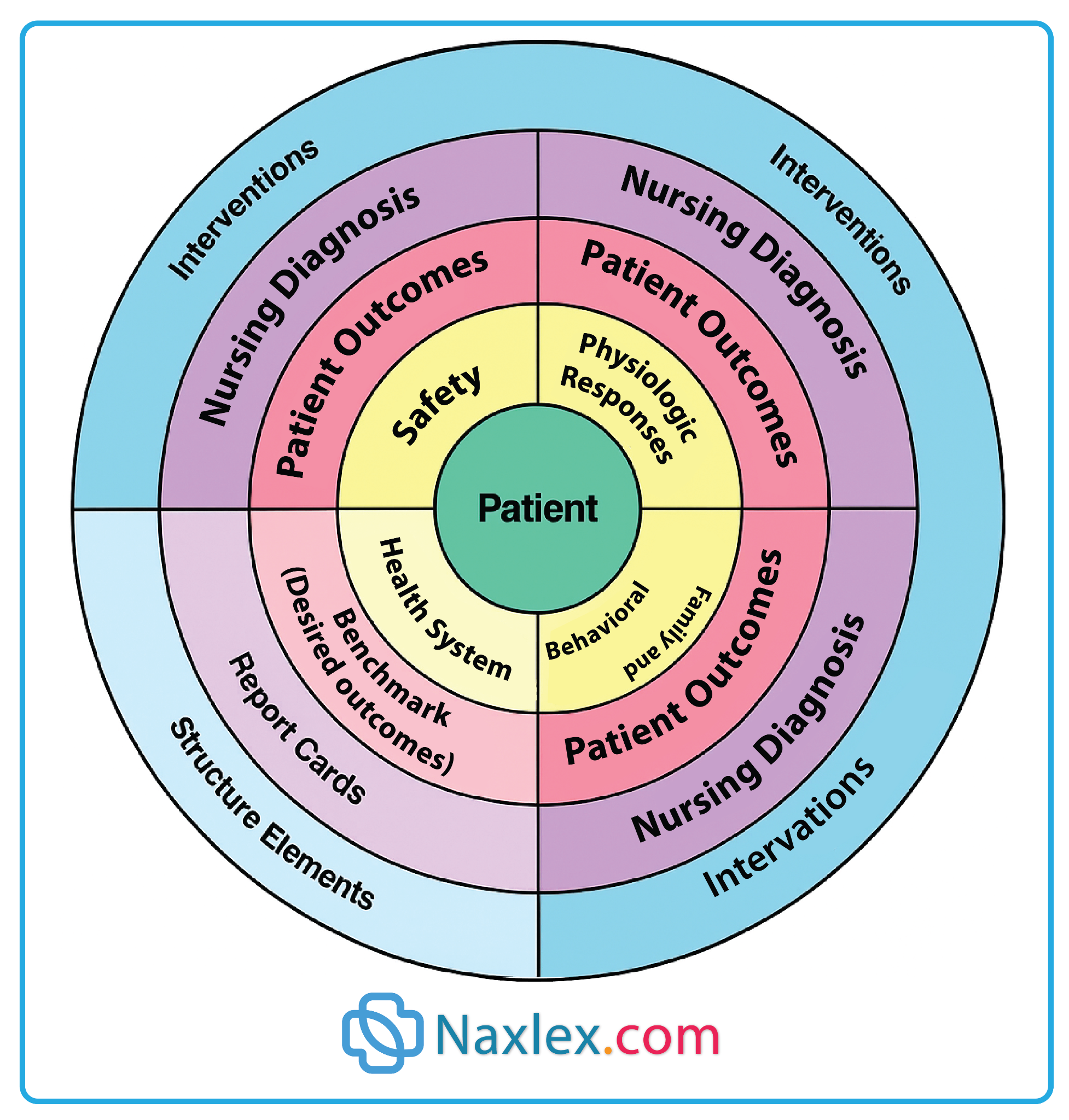
A conceptual model for perioperative nursing care is shown in the figure below. In this model, the patient is at the center of all care activities. Surrounding the patient are four domains. Three of these domains, safety, physiologic responses, and the patient and family behavioral responses, are critical for patient care. The fourth domain, health system, represents the structure elements and other system activities that must be present to support safe, effective, high-quality patient care.
The Surgical Experience
1.1 Phases of the Perioperative period
The patient who is having surgery progresses through several distinct phases, called the perioperative period. Include:
- The preoperative phase, beginning when the patient and surgeon mutually decide that surgery is necessary and will take place.
- The intraoperative phase, beginning when the patient is transferred to the OR bed, also called a table, until transfer to the postoperative recovery area.
- The postoperative phase, lasting from admission to the recovery area to complete recovery from surgery and the last follow-up physician visit. Further divided into:
- phase I - providing patient care from a totally anesthetized state to one requiring less acute nursing interventions
- phase II - preparing the patient for self or family care or for care in a phase III extended care environment
- phase III- providing ongoing care for patients requiring extended observation or intervention after transfer or discharge from phase I or II
1.2 Surgical procedure classification
Surgical procedures usually are classified according to urgency, risk, and purpose.
|
CLASSIFICATION OF SURGICAL PROCEDURES |
||
|
Classification |
Purpose |
Examples |
|
Based on Urgency Elective: Delay of surgery has no ill effects; can be scheduled in advance based on patient’s choice. Urgent: Usually done within 24-48 hours Emergency: Done immediately |
• To remove or repair a body part • To restore function • To improve health • To improve self-concept • To remove or repair a body part • To preserve or restore health • To prevent further tissue damage • To preserve life |
Elective: Tonsillectomy, hernia repair, cataract extraction and lens implantation
Urgent: Removal of gallbladder, coronary artery bypass, surgical removal of a malignant tumor
Emergency: Control of hemorrhage; repair of trauma, perforated ulcer, intestinal obstruction; tracheostomy |
|
Based on Degree of Risk Major: May be elective, urgent, or emergency Minor: Primarily elective |
To preserve life • To remove or repair a body part • To restore function • To improve or maintain health • To remove skin lesions • To correct deformities |
Major: Carotid endarterectomy, cholecystectomy, nephrectomy
Minor: Teeth extraction, removal of warts, skin biopsy, dilation and curettage, |
|
Based on Purpose
Diagnostic
Ablative
Palliative
Reconstructive
Transplantation
Constructive |
• To make or confirm a diagnosis
• To remove a diseased body part
• To relieve or reduce intensity of an illness; is not curative
• To restore function to traumatized or malfunctioning tissue • To improve self-concept
• To replace organs or structures that are diseased or malfunctioning
• To restore function in congenital anomalies |
Breast biopsy, laparoscopy, bronchoscopy, exploratory laparotomy Appendectomy, subtotal thyroidectomy, partial gastrectomy, colon resection, amputation
Colostomy, nerve root resection, debridement of necrotic tissue, balloon angioplasties, arthroscopy
Scar revision, plastic surgery, skin graft, internal fixation of a fracture, breast reconstruction
Kidney, liver, cornea, heart, joints
Cleft palate repair, closure of atrial–septal defect |
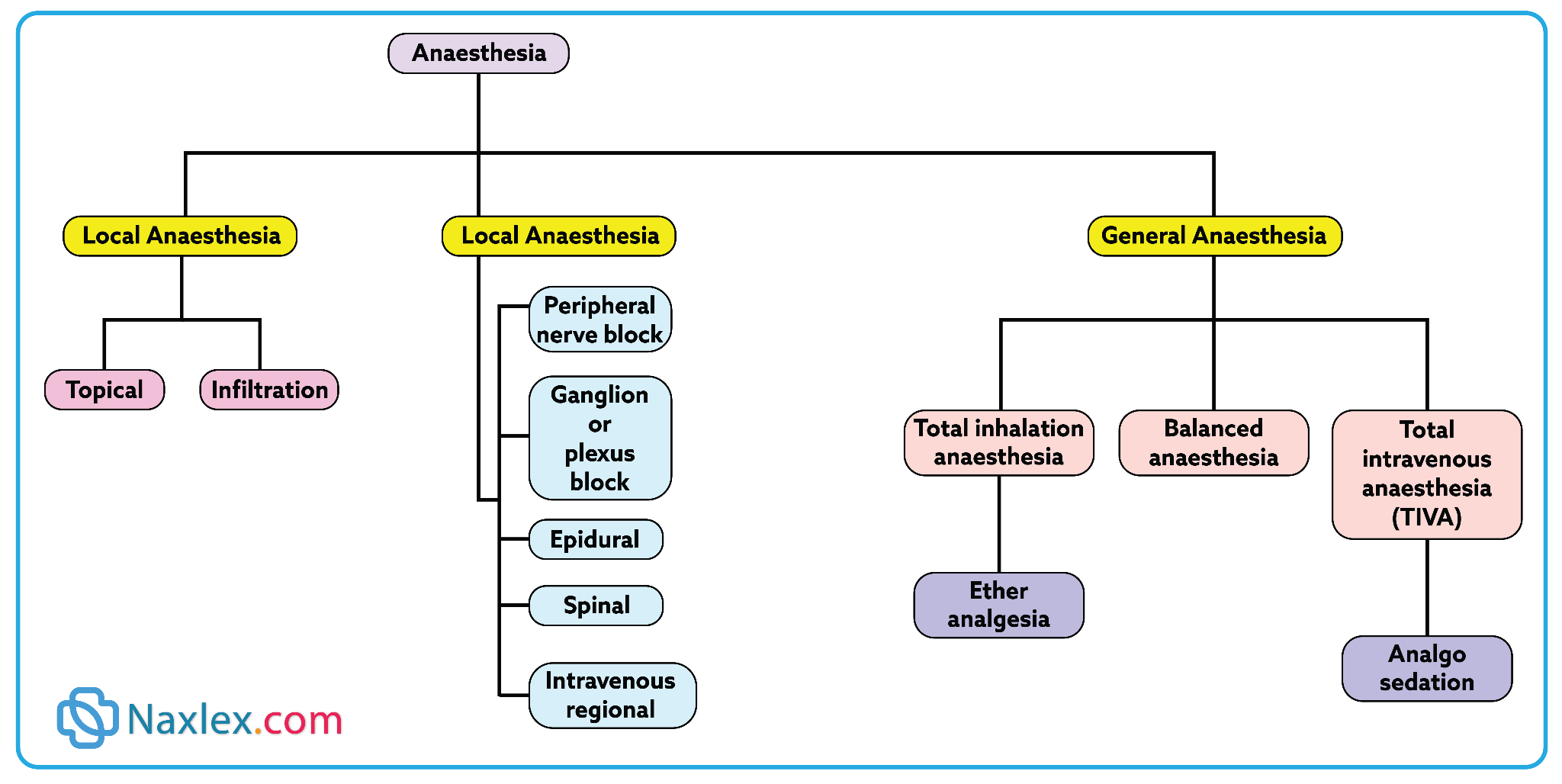
1.3 Anesthesia
Anesthesia is a method and technique of making potentially uncomfortable interventions tolerable and safe. Anesthetic agents can be administered systemically, to the whole body, or regionally to block nerve conduction.
Anesthesiologists (medical doctors) or certified registered nurse anesthetists (CRNA) administer anesthetic agents while monitoring the patient’s physiologic response and maintaining homeostasis
General anesthesia:
General anesthesia involves the administration of drugs by the inhalation or intravenous (IV) route to produce central nervous system depression.
The three phases of general anesthesia are induction, maintenance, and emergence.
- Induction begins with administration of the anesthetic agent and continues until the patient is ready for the incision.
- Maintenance continues from this point until near the completion of the procedure.
- Emergence starts as the patient begins to awaken from the altered state induced by the anesthesia and usually ends when the patient is ready to leave the operating room
Regional Anesthesia:
Regional anesthesia occurs when an anesthetic agent is injected near a nerve or nerve pathway in or around the operative site, inhibiting the transmission of sensory stimuli to central nervous system receptors. Accomplished through:
- Nerve blocks are accomplished by injecting a local anesthetic around a nerve trunk supplying the area of surgery such as the jaw, face, and extremities
- Spinal anesthesia is achieved by injecting a local anesthetic into the subarachnoid space through a lumbar puncture, causing sensory, motor, and autonomic blockage.
- Caudal anesthesia is the injection of the local anesthetic into the epidural space through the caudal canal in the sacrum.
- Epidural anesthesia involves the injection of the anesthetic through the intervertebral spaces, usually in the lumbar region.
Topical and Local Anesthesia
Topical anesthesia is used on mucous membranes, open skin surfaces, wounds, and burns. Topical anesthetics may be sprayed, spread, or applied with a compress of drug-saturated gauze or cotton tipped applicators.
Local anesthesia is the injection of an anesthetic agent such as lidocaine, bupivicaine, or tetracaine to a specific area of the body.
Moderate Sedation/Analgesia
Moderate sedation/analgesia, also called conscious or procedural sedation, is used for short-term and minimally invasive procedures.
1.4 Informed Consent and Advance Directives
Informed consent:
Informed consent is the patient’s voluntary agreement to undergo a particular procedure or treatment after having received the following information by the procedural physician:
- Description of the procedure or treatment along with potential alternative therapies.
- The underlying disease process and its natural course
- Name and qualifications of the person performing the procedure or treatment.
- Explanation of the risks involved, including risk for damage, disfigurement, or death, and how often they occur.
- Explanation that the patient has the right to refuse treatment and that consent can be withdrawn.
- Explanation of expected outcome, recovery, and rehabilitation plan and course.
The responsibility for securing informed consent from the patient lies with the person who will perform the procedure. This is usually the physician. The nurse may sign as a witness, signifying that the patient signed the consent form without coercion and was alert and aware of the act. The patient always has the right to refuse treatment.
Consent forms are not legal if the patient is confused, unconscious, sedated, mentally incompetent, or a minor (as determined by state laws). Consent may be given in those instances by a parent, spouse, next of kin, or legal guardian.
Note: In emergency situations, the physician may obtain consent over the telephone or by court order
Advanced directives:
Advance directives, also legal documents, allow the patient to specify instructions for healthcare treatment should he or she be unable to communicate these wishes postoperatively.
Two common forms of advance directive include living wills and durable power of attorney for healthcare.
It is important to discuss and document the exact wishes of the patient and family members before surgery, especially related to resuscitation (do-not-resuscitate [DNR]).
1.5 Outpatient/Same-day Surgery
Surgical procedures performed in outpatient or same-day (also referred to as ambulatory) surgical settings have become common.
Typically, patients are admitted to the healthcare setting the morning of surgery. Allowing the patient to spend the night before surgery at home and to return to his or her own home to recover, reduces much of the stress associated with surgery.
Preoperative information for outpatient/same-day surgery
Provide verbal and written instructions for patients having outpatient/same-day surgery as follows:
- List medications routinely taken, and ask the physician which should be taken or omitted the morning of surgery.
- Notify the surgeon’s office if a cold or infection develops before surgery.
- List allergies, and be sure the operating staff is aware of these.
- Remove nail polish and do not wear makeup for the procedure.
- Leave all jewelry and valuables at home.
- Wear clothing that buttons in front; short-sleeved garments are better for surgery on the hands.
- Have someone available for transportation home after recovery from anesthesia.
Inform patient of:
- Limitations on eating or drinking before surgery, with a specific time to begin the limitations.
- When and where to arrive for the procedure, as well as the estimated time when the procedure will be performed.
Preoperative Care: The Nursing Process
Surgical patients may be of any age and at any point on the health–illness continuum. It is the nurse’s responsibility to identify factors that affect the risk of a surgical procedure.
Some of the desired outcomes that frame the plan of care for the surgical patient, state that the patient will meet the following goals:
- Be free from injury and adverse effects related to positioning, retained foreign objects, or chemical, physical, or electrical hazards
- Be free from infection
- Maintain fluid and electrolyte balance and skin integrity
- Maintain normal body temperature
- Be free from deep vein thrombosis (DVT, formation of a blood clot [“thrombus”] in a deep vein)
- Have their pain managed
- Demonstrate an understanding of the physiologic and psychological responses to the planned surgery
- Participate in a rehabilitation process following surgery
1.1 Assessing
Assessment of the surgical patient includes:
- Obtaining a health history and performing a physical assessment to establish a baseline data base
- Identifying risk factors and allergies that could pose surgical complications
- Identifying medications and treatments the patient is currently receiving
- Determining the teaching and psychosocial needs of the patient and family
- Determining postsurgical support and referral needs for recovery
HEALTH HISTORY:
Developmental Level
- Infants: increased surgical risk due to small blood volume, immature liver/kidneys, unstable temperature, small airway, increased risk of hypoxia/bronchospasm. Surgery postponed if respiratory infection present.
- Older adults: Physiologic changes decreased stress response, affect meds/anesthesia, slow wound healing. Chronic illnesses (e.g., CHF, diabetes) increased risk.
Medical History
- Cardiovascular disease - risk of bleeding, shock, arrhythmias, venous stasis.
- Respiratory disorders - risk of anesthesia depression, pneumonia, atelectasis.
- Renal/Liver disease - impaired drug metabolism/excretion, wound healing issues.
- Endocrine (especially Diabetes) - hypoglycemia, acidosis, delayed healing, CV risk.
Medications
- Risks:
- Anticoagulants - bleeding.
- Diuretics - electrolyte imbalance, resp. depression.
- Tranquilizers - hypotension with anesthesia.
- Steroids - withdrawal - Cardiovascular collapse.
- Antibiotics (mycins) - resp. paralysis with muscle relaxants.
- Oral antidiabetics (e.g., metformin) - renal failure with contrast dyes.
- Some meds continued with sips of water (e.g., cardiac/diabetic drugs).
Previous Surgeries
- Complications (e.g., malignant hyperthermia, latex allergy, pneumonia, thrombophlebitis) increased current surgical risk.
- Past experiences (positive/negative) influence anxiety and teaching needs.
- Children: most stressful- admission, tests, transport, recovery.
Nutritional Status
- Malnutrition - delayed healing, infection, fluid/electrolyte imbalance.
- Obesity - risks: DVT, GI issues, respiratory compromise (OSA, GERD, aspiration), delayed wound healing, infection.
Substance Use
- Alcohol: increased anesthetic/analgesic needs, drug complications.
- Illicit drugs: unsafe anesthesia interactions, poor IV access.
- Smoking: increased mucus, decreased ciliary action - pneumonia, hypoxia, poor wound healing.
ADLs & Occupation
- Exercise: improves surgical recovery.
- Rest/Sleep: essential for recovery.
- Occupation: may affect rehab, return-to-work needs.
Coping Patterns & Support Systems
- Surgery is a major psychological stressor.
- Common fears: anesthesia, death, pain, disfigurement, finances.
- Anxiety may show as anger, withdrawal, apathy.
- Nursing role: therapeutic communication, teaching, involve family, encourage support, address spiritual needs.
Sociocultural Needs
- Influenced by family beliefs, culture, economics.
- May affect views on surgery, pain expression, response to teaching, ambulation, diet.
- Care must be culturally sensitive (e.g., language, family roles, rituals).
PHYSICAL ASSESSMENT
Assessing the patient’s current physical status provides data for interventions to decrease surgical risk and potential postoperative complications.
|
PREOPERATIVE PHYSICAL ASSESSMENT |
|
|
Factors to Assess |
Questions and Approaches |
|
General survey |
• Note general state of health. • Note body posture and stature. • Take and record vital signs. |
|
Skin |
• Inspect skin for color, characteristics, and location and appearance of lesions. • Assess skin over bony prominences. • Palpate skin turgor |
|
Chest and lungs |
• Observe chest excursion and diameter and shape of thorax. • Auscultate breath sounds. • Palpate for any pain or tenderness. |
|
Cardiovascular system |
• Inspect for jugular vein distention. • Auscultate apical rate, rhythm, and character. • Auscultate heart sounds. • Assess for peripheral edema. • Palpate character of peripheral pulses. |
|
Abdomen |
• Ask time of last bowel movement. • Inspect abdominal contour. • Auscultate bowel sounds |
|
Neurologic system |
• Note orientation, level of consciousness, awareness, and speech. • Assess reflexes. • Assess motor and sensory ability. • Assess visual and hearing ability. |
|
Musculoskeletal system |
• Inspect and note joint range of motion. • Palpate muscle strength. • Assess ability to ambulate. |
Usual presurgical screening tests include chest x-ray, electrocardiography, complete blood count, electrolyte levels, and urinalysis.
1.2 Diagnosing
Nursing diagnoses for patients in the preoperative phase may be identified for various actual or potential problems for which a patient is at risk.
Many diagnoses reflect assessment of risk and are made to guide interventions for patient needs in the intraoperative and postoperative phases.
Examples of NANDA Nursing Diagnoses:
- Grieving
- Anxiety
- Risk for Infection
1.3 Outcome Identification and Planning
Outcomes are standard for all patients having surgery, but nursing interventions are designed to meet the priority needs of individual patients and situations.
Specific appropriate outcomes include that the patient:
- Is physically and emotionally prepared for surgery
- Demonstrates turning, coughing, and deep-breathing exercises
- Verbalizes understanding of postoperative pain management
- Maintains fluid intake and nutritional balance to meet needs
1.4 Implementing
1. Preparing the Patient Psychologically
a. Communication
- Surgery - life crisis - evokes anxiety/fear.
- Use therapeutic communication to build trust and psychological safety.
- Avoid false reassurance - denies patient’s emotions & blocks trust.
b. Teaching
- Preoperative teaching - decreases complications, decreases length of stay, increases recovery outcomes.
- Should be individualized (depends on timing, type of surgery, support system).
- Teaching checklist helps ensure thorough education.
Key Teaching topics:
- Surgical events & sensations
- What to expect before/during/after surgery.
- Sensations: dry mouth, sore throat, cool environment, drowsiness, bright lights, incision pain.
- Emphasize: “You are the most important person in the room.”
- Pain management
- Pain - normal but treatable; uncontrolled pain delays recovery.
- Assess every 2 hours after major surgery.
- Teach use of pain scales, request meds before pain becomes severe.
- Techniques: relaxation (deep breathing, music, imagery), PCA, TENS, local anesthetic pumps, epidurals.
- Low risk of addiction in postoperative use.
- Physical activities
- Prevent respiratory & circulatory complications.
- Must be taught & practiced before surgery.
- Techniques:
- Deep breathing - expands lungs, clears anesthesia, prevents atelectasis.
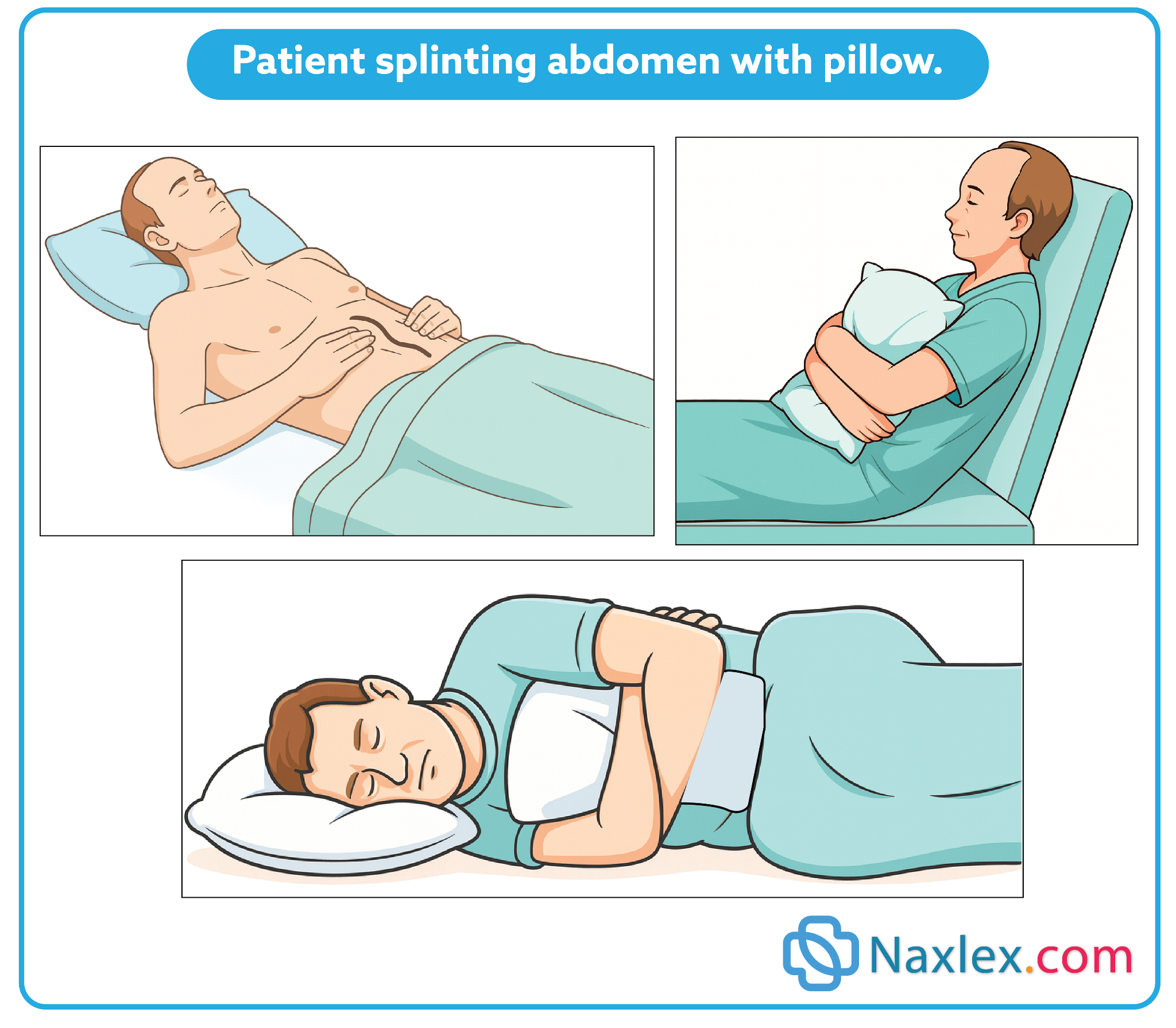
- Coughing - clears mucus; splint incision with pillow/blanket.
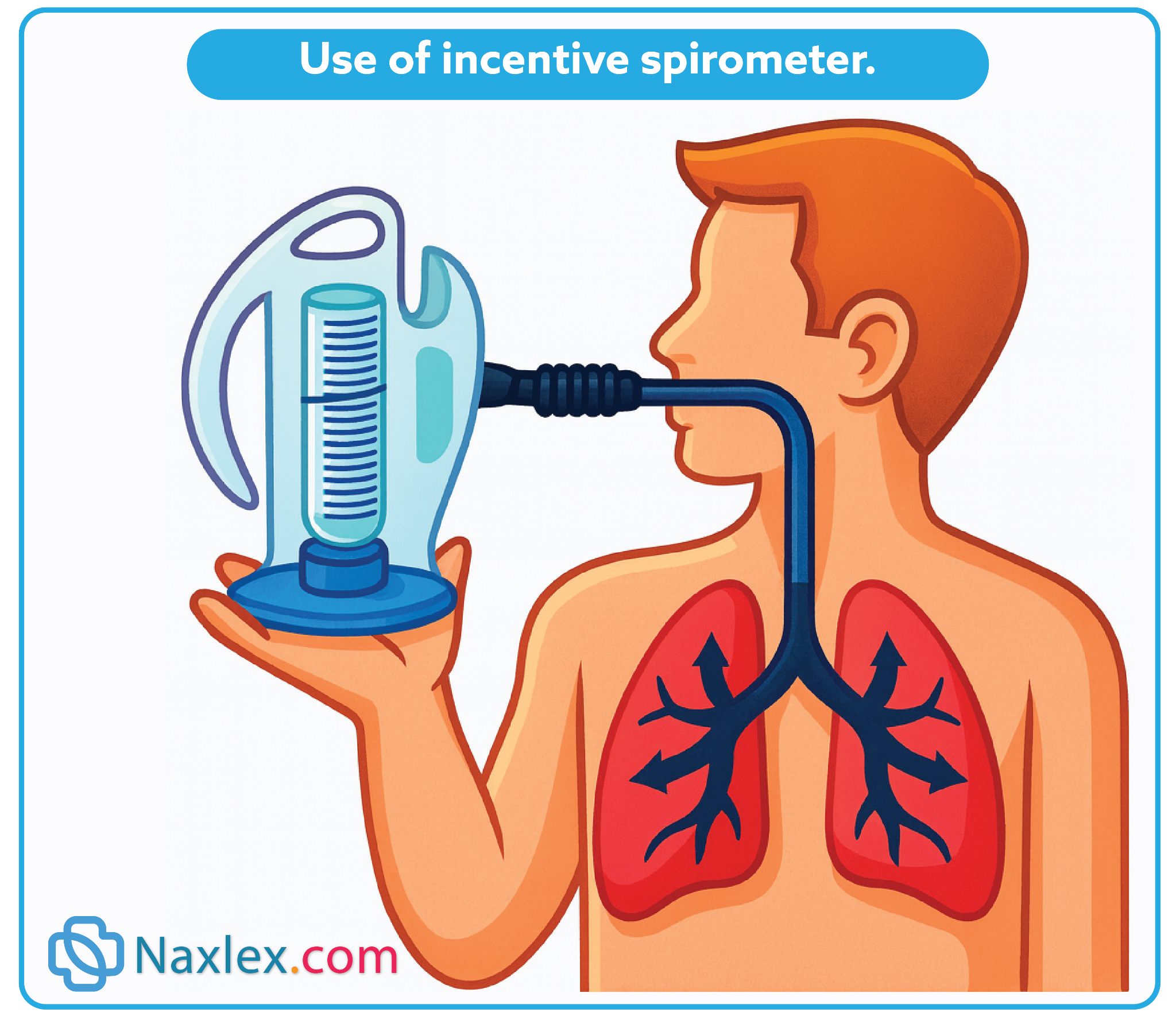
- Incentive spirometry - improves lung inflation, encourages progress.
- Leg exercises - improve venous return, decreases DVT risk.
- Turning in bed - prevents skin breakdown, increases circulation & peristalsis; practice with splinting for comfort.
2. Preparing the Patient Physically
a. Hygiene & Skin Prep
- Clean skin reduces infection risk.
- Shower night before/morning of surgery (often with chlorhexidine).
- Hair removal: clippers preferred, not shaving.
- Document method & skin condition.
b. Nutrition & Fluids
- Good nutrition/hydration supports healing.
- Blood transfusion if Hgb < 10 g/dL or Hct < 33%.
- NPO guidelines:
- Clear fluids up to 2 hours before surgery (unless contraindicated).
- Examples: water, pulp-free juice, clear tea/coffee, soda.
- Explain purpose of NPO & enforce strictly.
c. Elimination
- Bowel prep not routine - depends on type of surgery.
- May require enema/cleansing for GI surgeries.
- Encourage voiding before pre-op meds; catheter may be inserted for pelvic surgery.
d. Rest & Sleep
- Rest reduces stress & aids healing.
- Support with teaching, quiet environment, relaxation measures, or sedatives.
3. Preparing the Patient on the Day of Surgery
- Pre-op checklist ensures completion of tasks: consent, teaching, NPO, skin prep, elimination, tests.
- Check that preoperative consent forms are signed, witnessed, and correct; that advance directives are in the medical record (as applicable); and that the patient’s chart is in order.
- Gather the needed equipment and supplies.
- Perform hand hygiene.
- Check vital signs. Notify physician of any pertinent changes (i.e., rise or drop in blood pressure, elevated temperature, cough, symptoms of infection).
- Provide hygiene and oral care. Assess for loose teeth. Remind patient of food and fluid restrictions before surgery.
- Instruct the patient to remove all personal clothing including underwear and put on a hospital gown.
- Ask patient to remove cosmetics, jewelry including body piercing, nail polish, and prostheses (e.g., contact lenses, false eyelashes, dentures). Some facilities allow a wedding band to be left in place, depending on the type of surgery, provided it is secured to the finger with tape.
- If possible, give valuables to a family member or place valuables in an appropriate area, such as the hospital safe if this is not possible.
- Have patient empty bladder before surgery.
- Attend to any special preoperative orders, such as starting an IV line.
- Complete preoperative checklist and record of patient’s preoperative preparation.
- Administer preoperative medication as prescribed by physician/anesthesia provider.
- Preoperative medications may include:
- Sedatives (e.g., diazepam, midazolam, lorazepam) -decreases anxiety, amnesia.
- Anticholinergics (e.g., atropine, glycopyrrolate) -decreases secretions, prevent laryngospasm.
- Narcotic analgesics (e.g., morphine, meperidine) - relaxation, decreases anesthetic needs.
- Neuroleptanalgesics (e.g., fentanyl + droperidol) - calmness/sleepiness.
- H2 receptor blockers (e.g., cimetidine, ranitidine) -decreases gastric acidity.
- Raise side rails of bed; place bed in lowest position. Instruct patient to remain in bed or on stretcher. If necessary, a safety belt may be used.
- Tell the family of the patient where the patient will be taken after surgery and the location of the waiting area where the surgeon will come to explain the outcome of the surgery.
1.5 Evaluating
Evaluating the plan of care for the preoperative phase is based on the expected outcomes. The plan is effective if the patient is physically and emotionally prepared for surgery, verbalizes expected events and sensations of the perioperative period, and demonstrates postoperative exercises and activities.
Nursing insights:
General Considerations
• Obese patients are at greater risk of surgical complications and death compared to optimal weight patients. In taking this patient’s history, the nurse needs to be alert for other medical conditions such as diabetes, hypertension, and sleep apnea.
Infant and Child Considerations
• Children have special needs related to their overall health, age, and size. Easing preoperative anxiety of the child is crucial and includes using simple and concrete terms when providing information.
• The nurse needs to be sensitive to the anxiety level of the parent and provide support, explanations, and patient teaching as needed.
• Accurate weights are essential for correct medication dosages.
• Developmentally appropriate pain assessment and therapy needs to be followed to ensure adequate pain management.
Older Adult Considerations
• Age-related changes and preexisting chronic conditions can affect the postoperative course of the older adult patient.
• It is important to present preoperative teaching information slowly with reinforcement, since processing of information can be slower.
• Pain assessment and therapy may be suboptimal due to communication barriers and comorbidities present in many older adult patients. These patients may respond differently to pain medication, therefore, careful and individualized attention is required in this more vulnerable age group.
Intraoperative Care: The Nursing Process
The intraoperative phase of surgery begins with admission of the patient to the surgical area and lasts until the patient is transferred to the PACU.
1.1 Assessing
Nurses in surgical scrub attire identify the surgical patient, assess the patient’s emotional and physical status, and verify the information on the preoperative checklist including assessment data, lab reports, and consents for surgery and blood transfusion.
They may also carry out required immediate preoperative care, including performing skin preparation, starting IV fluids, placing sequential compression devices to prevent deep vein thrombosis (DVT), determining pain level, assuring patient and family, providing comfort, and giving preoperative medications.
The patient’s response to the procedures is assessed, and the events of surgery are explained.
In the operating room, the patient is positioned on the operating bed, identified again with the operative team using at least two identifiers (such as name, birth date, medical record number), and then anesthetized and draped.
1.2 Diagnosing
Patient problems in the intraoperative period may occur as a result of the position of the patient during the procedure, the effects of the anesthesia, equipment used and potential hazards, disruption of tissues during surgery, and the incision.
Examples of NANDA Nursing Diagnoses:
- Risk for Imbalanced Fluid Volume
- Risk for Perioperative Positioning Injury
1.3 Outcome Identification and Planning
Some expected outcomes are that the patient will:
- Remain free of neuromuscular injury
- Remain free from wrong site, wrong side, wrong procedure surgery
- Maintain fluid and electrolyte balance
- Maintain skin integrity (other than for the incision)
- Have symmetric breathing patterns
- Be free of injury from burns, retained foreign objects (inaccurate count of supplies), and medication errors
- Remain free from surgical site infection
- Maintain normothermia
1.4 Implementing
The scrub nurse is a member of the sterile team who maintains surgical asepsis while draping and handling instruments and supplies.
The circulating nurse identifies and assesses the patient on admission to the operating room, collaborates in safely positioning the patient on the operating bed, assists with monitoring the patient during surgery, provides additional supplies, maintains environmental safety, and counts the number of instruments, needles, and sponges used during the surgery to prevent the accidental loss of an item in the open incision.
The RNFA (registered nurse first assistants) actively assists the surgeon by providing exposure of the operative area, hemostasis (blood clotting), and wound closure.
The APN (Advanced Practice Nurses) coordinates care activities, collaborates with physicians and nurses in all phases of perioperative and post anesthesia care, and integrates case management, critical paths, and research into care of the surgical patient.
Positioning:
The risk for skin injury is avoided by lifting, rather than rolling or pulling, the patient into the surgical position. Perioperative nurses need to know the position to be used and significant nursing considerations for that position. Examples:
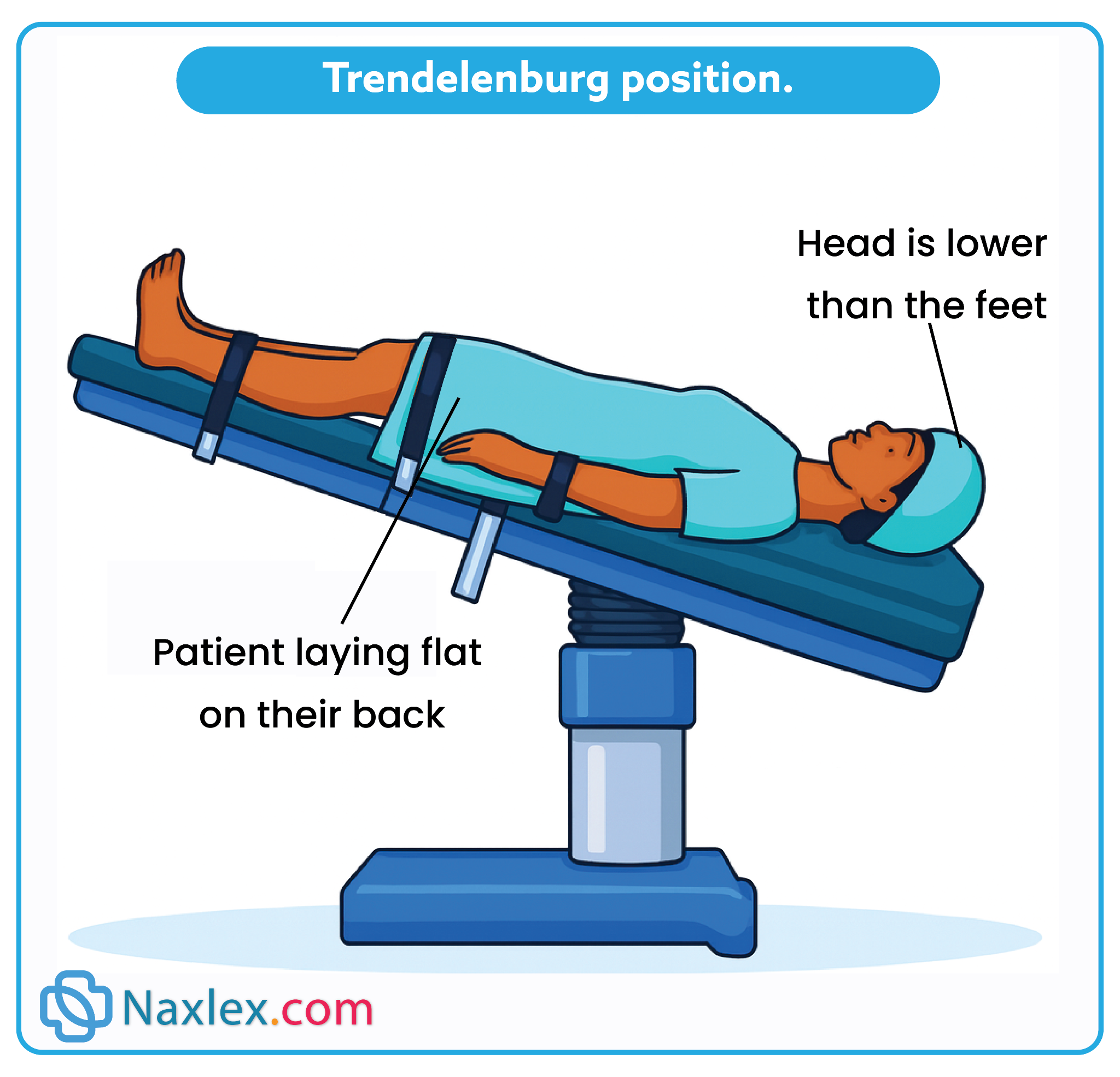
The Trendelenburg position requires lowering the upper torso and raising the feet.
- It is commonly used in minimally invasive surgery of the lower abdomen or pelvis.
- The displacement of the abdominal viscera toward the head decreases diaphragmatic movement and respiratory exchange; blood pools in the upper torso, and blood pressure increases; hypotension can result with return to the supine position.
- Shearing with resultant tissue damage is also a significant risk in this position
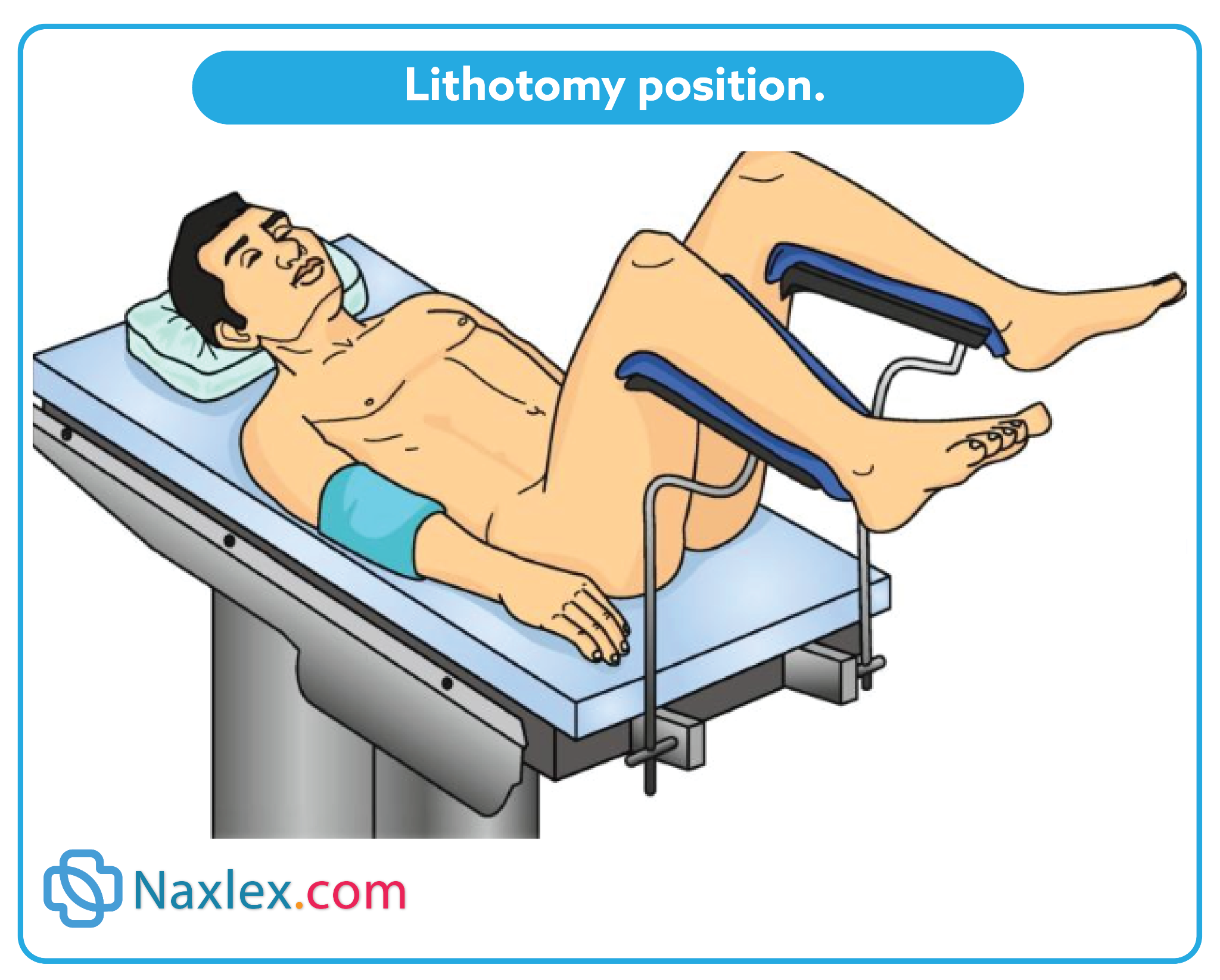
The lithotomy position is used for gynecologic, rectal, and urologic procedures.
- The placement of legs in stirrups causes pooling of blood in the legs increasing the risk of thrombophlebitis.
- Pressure can also damage the peroneal nerve, with resultant foot drop.
Draping:
Drapes are used to create and maintain a sterile field around the operative site, preventing the passage of microorganisms, particulate matter, and fluids between sterile and nonsterile areas.
Documenting:
Throughout surgery, the perioperative nurse documents ongoing patient assessment, item counts (sponges, sharps, instruments), monitoring data (e.g., vital signs, urine output, blood loss, pulse oximetry results), positioning, medications, dressings and drains, specimens, and responses to care on the intraoperative record.
Transferring to the Post anesthesia Care Unit:
This is a critical time: Sudden or rough handling can cause severe hypotension or potentially lethal cardiac or respiratory arrest.
The primary objective of the hand-off report from OR nurse to PACU nurse is to provide accurate information about the patient’s care, procedure, presenting condition, and any important events that occurred during the procedure.
1.5 Evaluating
Evaluation of the effectiveness of the plan of care for the intraoperative phase is based on the expected outcomes. If met, the plan was effective.
Postoperative Nursing Care
The postoperative phase can be divided into two stages:
- immediate care (usually provided in the PACU in both in hospital and outpatient/same-day surgery centers)
- ongoing postoperative care (lasting from return to the unit through convalescence).
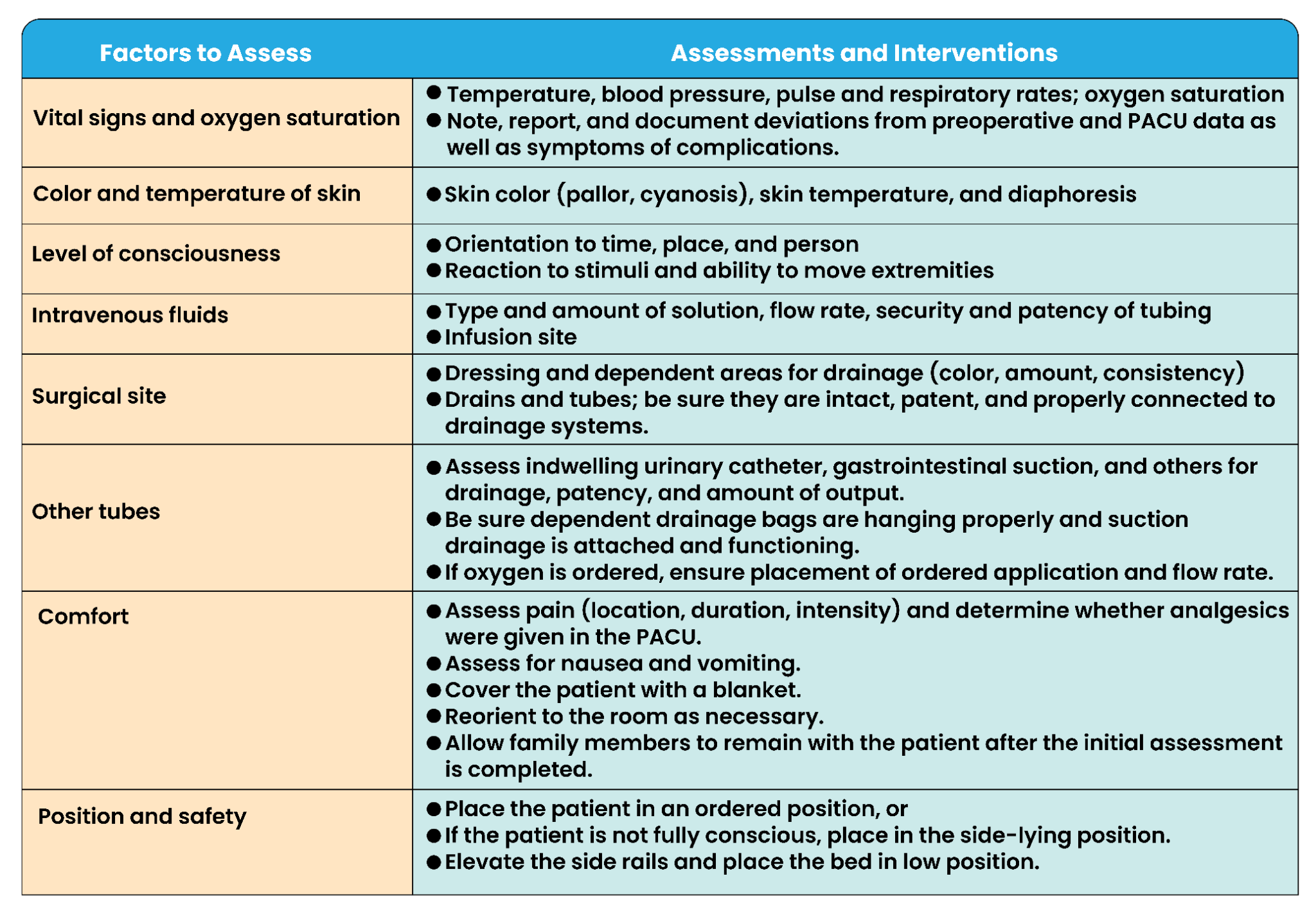
1.1 Immediate Postoperative Assessment and Care
Purpose of PACU Care
- Continuous monitoring to prevent complications from anesthesia/surgery.
- Assessments compared with preoperative & intraoperative data.
- Frequency: every 10–15 minutes initially.
- Children: high risk for airway loss; emergence delirium common.
- Average PACU stay: ~1 hour (varies by surgery, anesthesia, patient response).
- PACU nurse role: vigilant monitoring, pain control, fluid/electrolyte balance, physiologic stabilization, prepare for next level of care.
Key Assessment Areas
1. Respiratory Status
- Monitor: rate, rhythm, depth, breath sounds, O₂ saturation, skin color, cardiovascular & mental status.
- Airway: patent, humidified O₂, pulse oximetry. Remove ET tube only after reflexes return.
- Signs of ineffective breathing: restlessness, anxiety, unequal chest expansion, noisy/shallow respirations, cyanosis, tachycardia.
- Common emergency: respiratory obstruction (from tongue, secretions, laryngospasm, or edema).
- Management: positioning, suctioning, O₂, encourage deep breaths.
2. Cardiovascular Status
- Monitor: vital signs, ECG, skin color/condition, compare BP with baseline.
- Hypertension causes: anesthetics, respiratory issues, surgical stress, recovery excitement.
- Hypotension causes: anesthesia, blood loss, positioning, pooling, meds.
- Interventions: O₂, deep breathing, leg exercises, verbal stimulation, accurate IV rates.
- Temperature regulation:
- Risk for inadvertent hypothermia (<35.5°C / 96°F).
- Complications: poor healing, cardiac disturbances, coagulopathy, delayed emergence.
- Interventions: warmed blankets, forced-air warming.
- Shock signs: tachycardia, decreased BP, cyanosis, cool skin, decreased urine output.
3. Central Nervous System Status
- Monitor return of consciousness:
- Unconscious
- Response to touch/sound
- Drowsy
- Awake, not oriented
- Awake, oriented
- Provide reorientation (touch, name, reassurance).
4. Fluid Status
- Risks: restriction, intraoperative loss, wound drainage, stress response (Na⁺/H₂O retention).
- High risk: children, older adults.
- Assess: skin turgor, vitals, urine output, wound drainage, IV intake.
- IV care: check type, rate, insertion site, tubing patency.
5. Wound Status
- Assess incision dressing for amount, color, consistency of drainage.
- Check drains/tubes output.
- Warning signs: large bright-red drainage and restlessness, pallor, cool moist skin, decreased BP, increased pulse/RR - possible hemorrhage/hypovolemic shock (report immediately).
6. Pain Management
- Use pain scales (verbal, numeric 0–10, or faces).
- Administer analgesia early: NSAIDs, opioids (PCA possible).
- Nonpharmacologic: positioning, reassurance, touch.
- Use preoperative pain-preference info for individualized care.
7. General Condition & Safety
- Maintain psychological comfort with reorientation and reassurance.
- Ensure physical safety: proper positioning, side rails.
- Discharge criteria: stable vitals & consciousness.
- PACU nurse communicates a handoff report to unit nurse upon transfer.
1.2 Ongoing Postoperative Care
Ongoing postoperative care is planned to facilitate recovery from surgery and coping with alterations.
THE NURSING PROCESS FOR ONGOING POSTOPERATIVE CARE
Assessing:
The nurse on the unit assists PACU personnel in transferring the patient to the bed in the unit and makes an initial assessment using data from the preoperative and intraoperative phases. A postoperative checklist or flow sheet may be used.
Common time frames are every 15 minutes until stable, changing to every 1 to 2 hours for the first 24 hours, and every 4 hours thereafter.
Diagnosing:
Nursing diagnoses in the postoperative phase may represent actual problems or those for which the patient is at risk.
Examples:
- Risk for Infection
- Disturbed Body Image
- Acute Pain
- Urinary Retention
Outcome Identification and Planning
Examples of desired postoperative outcomes for a patient after major surgery are as follows: The patient will:
- Carry out leg exercises every 2 to 4 hours.
- Deep breathe and cough effectively every 2 hours.
- Verbalize decreasing levels of pain.
- Have a balanced intake and output.
- Regain normal bowel and bladder elimination.
- Exhibit a healing surgical incision.
- Remain free of infection.
- Verbalize any concerns about appearance of wound.
- Verbalize and demonstrate wound self-care
Implementing:
Nursing care is discussed to prevent complications, promote a return to health, and facilitate coping with alterations.
1. Preventing Cardiovascular Complications
Hemorrhage
- Cause: slipped suture, dislodged clot, stress on site, meds, conditions
- Signs: restlessness, anxiety, frank bleeding, hypotension, cold/clammy skin, weak rapid pulse, mottled extremities, decreased urine, thirst
- Care: stop bleeding, replace blood volume, apply pressure dressing, notify surgeon, prepare for OR if uncontrolled.
Shock (usually hypovolemic)
- Cause: blood/fluid loss, circulatory failure
- Signs: same as hemorrhage
- Care: airway, flat with legs elevated 30–45°, O₂, cover for warmth, monitor vitals/Hct/ABGs, start IV lines, fluids/blood, meds, notify surgeon.
Thrombophlebitis
- Cause: venous stasis, clot in leg vein
- Signs: calf/thigh pain & cramping, redness, swelling, increased temperature, increased limb diameter
- Care: prevent embolus, give meds (anticoagulants, anti-inflammatory, analgesics), bed rest, apply heat, compression devices, measure calf/thigh circumference, do not massage legs.
2. Preventing Respiratory Complications
- General measures: monitor vitals, deep breathing, coughing, incentive spirometry, turning q2h, ambulation, hydration, semi-Fowler’s position, monitor narcotic response.
Pulmonary Embolus
- Cause: clot lodges in pulmonary vessels
- Signs: dyspnea, chest pain, cough, cyanosis, tachypnea, tachycardia, anxiety
- Care: emergency! Notify physician, semi-Fowler’s, O₂, bed rest, meds (anticoagulants, analgesics), avoid Valsalva.
Pneumonia
- Cause: aspiration, infection, weak cough, anesthesia secretions, dehydration, immobility
- Signs: fever, chills, cough with or without purulent or rusty sputum, crackles, wheezes, dyspnea, chest pain
- Care: semi-Fowler’s/Fowler’s, O₂, antibiotics, expectorants, analgesics, oral hygiene, rest.
Atelectasis
- Cause: alveoli collapse from mucus retention leading to poor gas exchange
- Signs: decreased breath sounds, dyspnea, cyanosis, crackles, restlessness, apprehension
- Care: O₂, semi-Fowler’s, pain relief, lung expansion interventions.
3. Preventing Surgical Site Complications
- Risks: infection, dehiscence (separation), evisceration (organ protrusion)
- Care: monitor vitals (fever), hydration, nutrition (protein, carbs, calories, vitamins), aseptic dressing changes, hand hygiene, proper disposal of soiled materials.
4. Promoting a Return to Health
Elimination Needs
- May be altered by anesthesia, surgery, inactivity, altered intake.
- Assess urine and bowel function, encourage mobility and fluids.
Fluid & Nutrition Needs
- Monitor I&O, IV rates, skin turgor, mucous membranes.
- Nutrition: advance diet as tolerated (clear then full liquids then soft then regular), monitor weight, oral hygiene, clean environment, upright position for meals, involve family.
Comfort & Rest
- Address nausea, vomiting, thirst, hiccups, pain.
- Provide hygiene, clean linens, quiet rest periods, allow family presence.
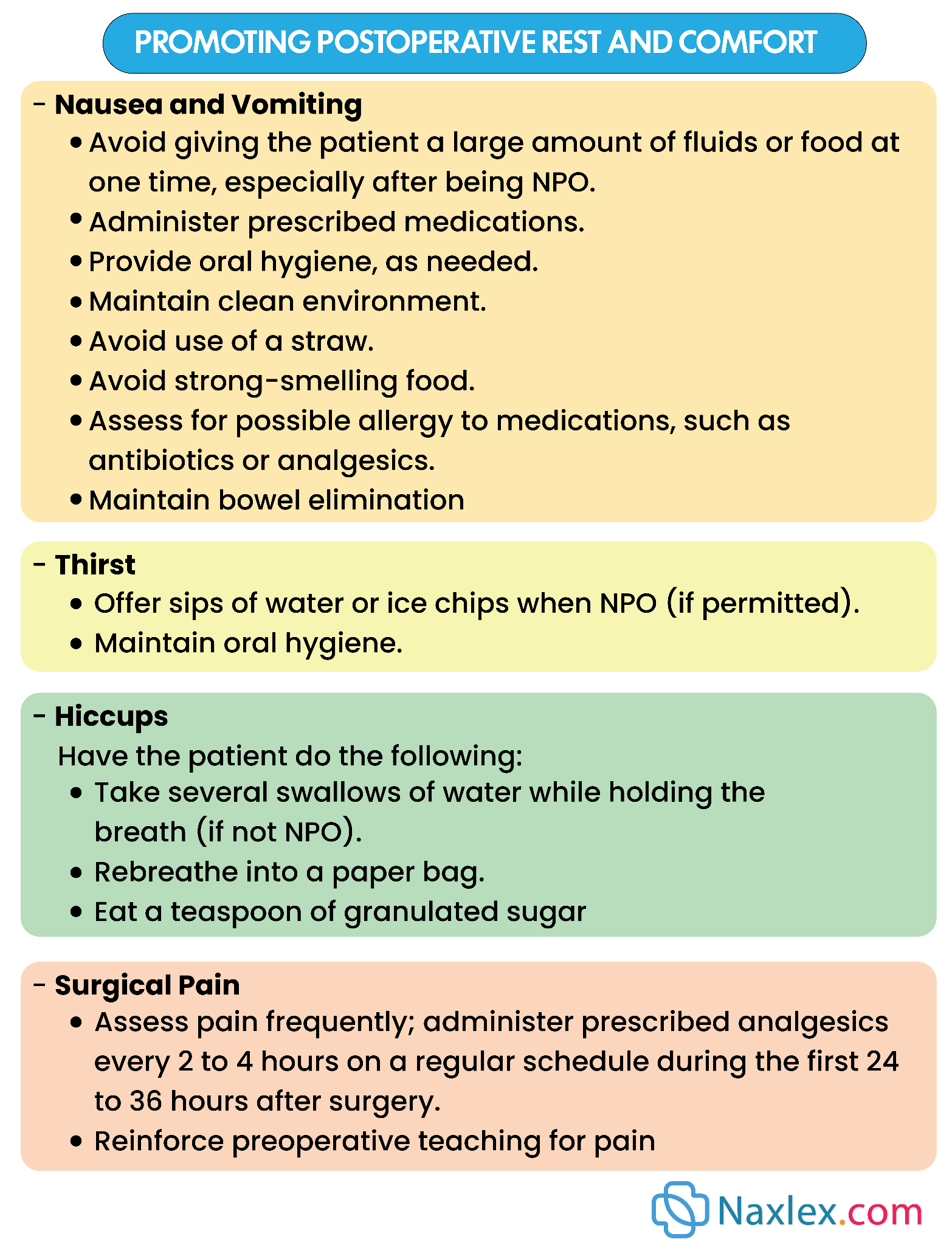
|
NURSING INSIGHTS: PROMOTING POSTOPERATIVE REST AND COMFORT Nausea and Vomiting Avoid giving the patient a large amount of fluids or food at one time, especially after being NPO. Administer prescribed medications. Provide oral hygiene, as needed. Maintain clean environment. Avoid use of a straw. Avoid strong-smelling food. Assess for possible allergy to medications, such as antibiotics or analgesics. Maintain bowel elimination
Thirst Offer sips of water or ice chips when NPO (if permitted). Maintain oral hygiene.
Hiccups Have the patient do the following: Take several swallows of water while holding the breath (if not NPO). Rebreathe into a paper bag. Eat a teaspoon of granulated sugar
Surgical Pain Assess pain frequently; administer prescribed analgesics every 2 to 4 hours on a regular schedule during the first 24 to 36 hours after surgery. Reinforce preoperative teaching for pain management. Offer nonpharmacologic measures to supplement medications: massage, position changes, relaxation, guided imagery, meditation, music. |
5. Helping the Patient Cope
- Surgery can affect body image and self-concept.
- Reactions may resemble grief; coping depends on age, culture, visibility of change, support system.
- Nurses provide emotional support, facilitate adaptation, respect cultural values, and acknowledge grief as normal.
6. Outpatient/Same-Day Surgery Care
- Discharge criteria: awake, alert, stable vitals, voided, tolerated oral fluids, not dizzy/drowsy.
- Must leave with responsible adult (no driving or solo public transport).
- Discharge usually 1-3 hours after surgery.
- Provide written and verbal home care instructions.
UNEXPECTED SITUATIONS AND ASSOCIATED INTERVENTIONS
• Vital signs are progressively increasing or decreasing from baseline: Notify primary care provider. A continued decrease in blood pressure or an increase in heart rate could indicate internal bleeding.
• Dressing was clean before but now has large amount of fresh blood: Do not remove dressing. Reinforce dressing with more bandages. Removing the bandage could dislodge any clot that is forming and lead to further blood loss. Notify primary care provider.
• Patient reports pain that is not relieved by ordered medication: After fully assessing pain (location, description, alleviating factors, causal factors), notify primary care provider. Pain can be a clue to other problems, such as hemorrhage.
• Patient is febrile within 12 hours of surgery: Assist patient with coughing and deep breathing. If ordered, begin incentive spirometry. Continue to monitor vital signs and laboratory values, such as complete blood count (CBC).
Nursing insights:
Older Adult Considerations:
In the older adult patient, postoperative pneumonia can be a very serious complication resulting in death. Therefore, it is especially important to encourage and assist the patient in using the incentive spirometer and with deep-breathing exercises.
Older patients may take longer to return to their level of orientation before surgery. Drugs and anesthetics will delay this return.
Infant and Child Considerations:
Postoperative complications are related to the respiratory system in this age group. After receiving general anesthesia, premature infants are at greater risk for apnea.
Infants and children are at great risk for temperature-related complications since their body temperature can change rapidly. It is essential to have warmed blankets and other warming equipment available to avoid this complication.
Summary
- Perioperative nursing includes the preoperative, intraoperative, and postoperative phases. Each phase focuses on different aspects of a patient’s surgical experience.
- The assessment of risk factors such as history of smoking, obesity, and obstructive sleep apnea allows a nurse to anticipate patient needs and the types of preparation required preoperatively to prevent intraoperative and postoperative complications.
- Malnutrition, diabetes, obesity, smoking, age, obstructive sleep apnea, and cardiac disorders increase patients’ risks for perioperative complications.
- A nurse assesses a patient’s potential psychological response by identifying the patient’s previous experiences with surgery to anticipate needs, providing teaching, addressing fears, and clarifying concerns.
- Postoperative patient education should be relevant and specific, culturally appropriate, and accurate to enhance the ability of patients to care for themselves at home.
- When caring for patients who are undergoing ambulatory surgery, prioritize education because of the limited time available, and involve the patient’s family or support system.
