
Diagnostic testing
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
To:
- Describe the nurse’s role for each of the phases involved in diagnostic testing.
- List common blood tests.
- Discuss the nursing responsibilities for specimen collection.
- Explain the rationale for the collection of each type of specimen.
- Compare and contrast CT, MRI, and nuclear imaging studies.
- Describe the nurse’s role in caring for clients undergoing aspiration/biopsy procedures.
- Demonstrate appropriate documentation and reporting of diagnostic testing information.
Introduction
Diagnostic and laboratory tests are tools that provide information about clients.
- Tests may be used for basic screening as part of a wellness check.
- Frequently tests are used to help confirm a diagnosis, monitor an illness, and provide valuable information about the client’s response to treatment.
Nurses require knowledge of the most common laboratory and diagnostic tests because one primary role of the nurse is to teach the client and family or significant other how to prepare for the test and the care that may be required following the test.
Diagnostic Testing Phases
Diagnostic testing involves three phases: pretest, intratest, and post-test.
Pretest:
The major focus of the pretest phase is client preparation. A thorough assessment and data collection (e.g., biologic, psychological, sociologic, cultural, and spiritual) assist the nurse in determining communication and teaching strategies.
Examples of questions:
- What type of sample will be needed and how will it be collected?
- Does the client need to stop oral intake for a certain number of hours prior to the test?
- Does the test include administration of dye (contrast media) and, if so, is it injected or swallowed?
- Are fluids restricted or forced?
- Are medications given or withheld?
- How long is the test?
- Is a consent form required?
Intratest:
This phase focuses on specimen collection and performing or assisting with certain diagnostic testing. The nurse ensures correct labeling, storage, and transportation of the specimen to avoid invalid test results.
Post-Test:
The focus of this phase is on nursing care of the client and follow-up activities and observations. The nurse also reports the results to appropriate health team members.
Blood Tests
A phlebotomist, a person from a laboratory who performs venipuncture, usually collects the blood specimen for the tests ordered by the primary care provider.
- Complete Blood Count
The CBC is a basic screening test and one of the most frequently ordered blood tests
|
Component |
Normal Findings (Adult) |
Possible Causes: Increased |
Possible Causes: Decreased |
|
RED BLOOD CELL (RBC) COUNT The number of RBCs per cubic millimeter (mm3 )
|
Men: 4.6–6.0 million/ mm3 Women: 4.0–5.0 million/ mm3
|
Dehydration, Polycythemia vera, High altitude, cardiovascular disease |
Blood loss, Anemias, Overhydration, Leukemias, Chronic renal failure, Pregnancy |
|
HEMOGLOBIN (HGB)
Composed of a pigment (heme), which contains iron, and a protein (globin). |
Men: 13.5–18 g/dL
Women: 12–15 g/dL |
Polycythemia, Dehydration, Chronic obstructive pulmonary disease, Heart failure |
Blood loss, Anemias, Kidney diseases, Cancers |
|
HEMATOCRIT (HCT) The hematocrit or packed cell volume (Hct, PCV, or crit) is a fast way to determine the percentage of RBCs in the plasma. Reported as a percentage because it is the concentration of RBCs in the blood. |
Men: 40–54% Women: 36–46% |
Dehydration, Burns, Hypovolemia |
Acute blood loss, Pregnancy, Dietary deficiencies, Anemias |
|
RBC INDICES: Mean corpuscular volume (MCV) The mean or average size of the individual RBC. |
Men: 80–98 μm3 Women: 78–102 μm3 |
Chronic liver disease, Pernicious anemia |
Microcytic iron deficiency anemia, Lead poisoning |
|
Mean corpuscular hemoglobin (MCH) Amount of Hgb present in one cell. |
25–35 pg |
Macrocytic anemias |
Radiation |
|
Mean corpuscular hemoglobin concentration (MCHC) The proportion of each cell occupied by Hgb. |
31–37% |
Rarely seen |
Microcytic, hypochromic anemia |
|
WHITE BLOOD CELL (WBC) COUNT Count of the total number of WBCs in a cubic millimeter of blood. |
4,500–11,000 mm3 |
Acute infections, Tissue necrosis (e.g., myocardial infarction), Collagen diseases |
Viral infections, Hematopoietic diseases, Rheumatoid arthritis |
|
DIFFERENTIAL COUNT The proportion of each of the five types of WBCs in a sample of 100 WBCs. Neutrophils |
50–70% |
Acute infections |
Viral diseases, Leukemias, Aplastic and iron deficiency anemia |
|
Lymphocytes |
25–35% |
Viral infection, Chronic infections, Lymphocytic leukemia |
Cancers, Leukemia, Multiple sclerosis, Renal failure |
|
Monocytes |
4–6% |
Viral diseases, Parasitic diseases, Collagen diseases, Cancer |
Lymphocytic leukemia, Aplastic anemia |
|
Eosinophils |
1–3% |
Allergic reactions Phlebitis Thrombophlebitis Parasitic infestations |
Stress (burns, shock) Adrenocortical hyperfunction |
|
Basophils |
0.4–1.0% |
Leukemia Inflammatory process |
Hypersensitivity reaction Stress Pregnancy |
|
PLATELET COUNT Platelets are basic elements in the blood that promote coagulation. |
150,000–400,000/mm3 |
Infections Polycythemia vera Acute blood loss Splenectomy |
Idiopathic thrombocytopenic purpura Cancer, Systemic lupus erythematosus (SLE) Some types of anemias |
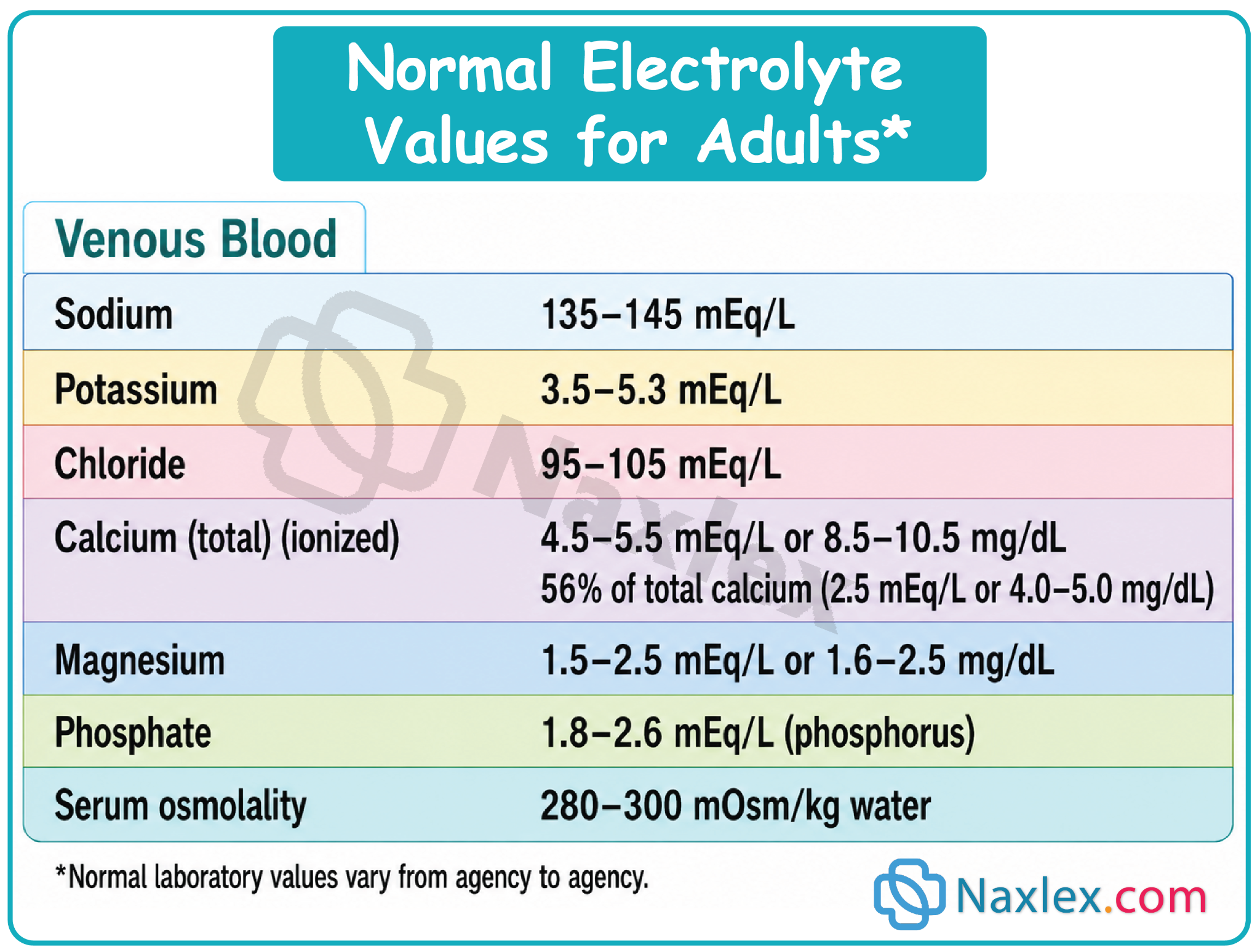
- Serum Electrolytes
The most commonly ordered serum tests are for sodium, potassium, chloride, and bicarbonate ions.
Blood levels of two metabolically produced substances, urea and creatinine, are routinely used to evaluate renal function. The kidneys, through filtration and tubular secretion, normally eliminate both.
- Urea, the end product of protein metabolism, is measured as blood urea nitrogen (BUN).
- Creatinine is produced in relatively constant quantities by the muscles and is excreted by the kidneys. Thus the amount of creatinine in the blood relates to renal excretory function.
- Serum Osmolality
Serum osmolality is a measure of the solute concentration of the blood. The particles included are sodium ions, glucose, and urea (BUN).
Serum osmolality can be estimated by doubling the serum sodium, because sodium and its associated chloride ions are the major determinants of serum osmolality. Normal values are 280 to 300 mOsm/kg.
- Drug Monitoring
Therapeutic drug monitoring is often conducted when a client is taking a medication with a narrow therapeutic range (e.g., digoxin, theophylline, aminoglycosides).
Peak and trough levels to determine if the blood serum levels of a specific drug are at a therapeutic level and not a subtherapeutic or toxic level.
- Arterial Blood Gases
Specimens of arterial blood from the radial, brachial, or femoral arteries.
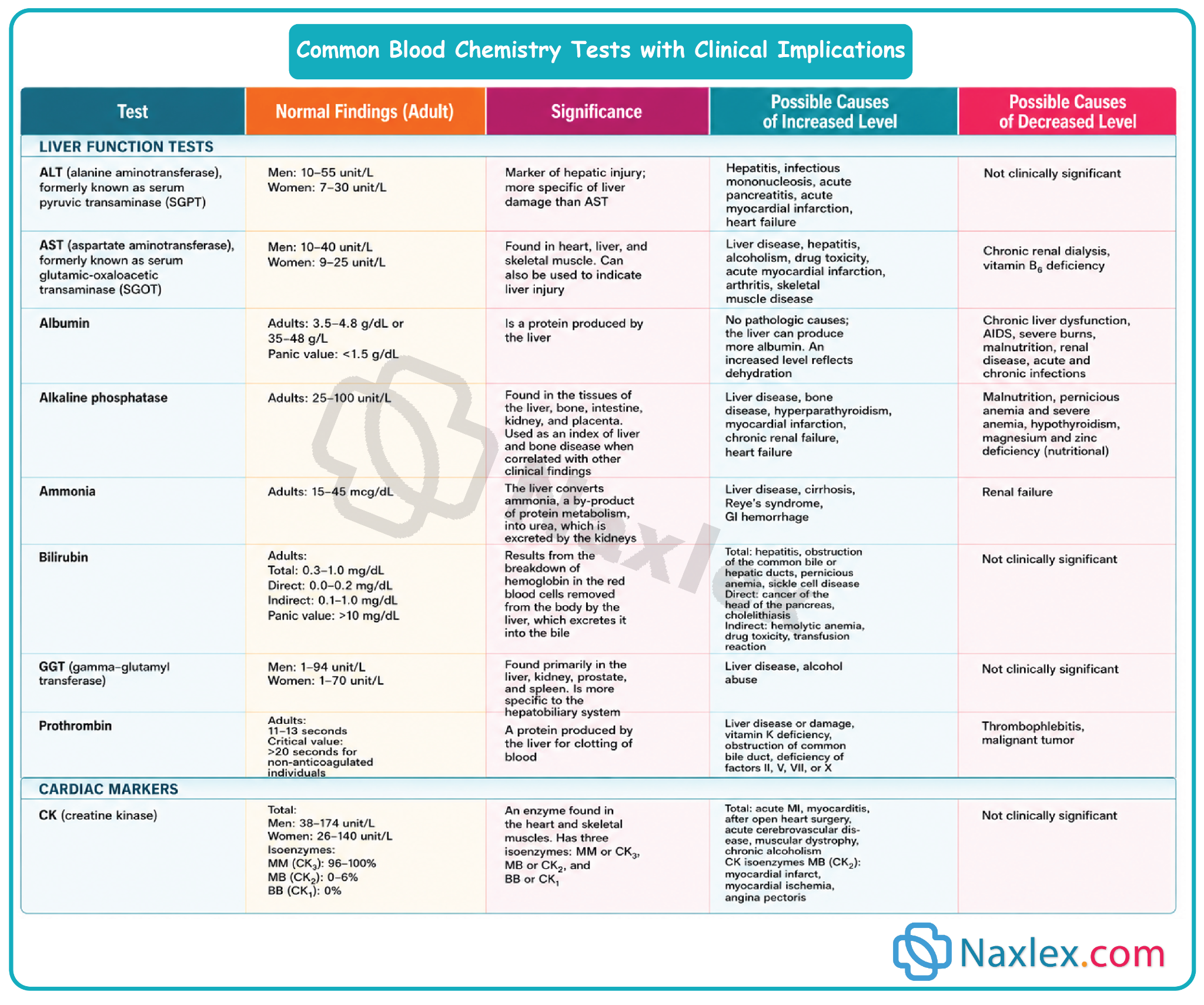
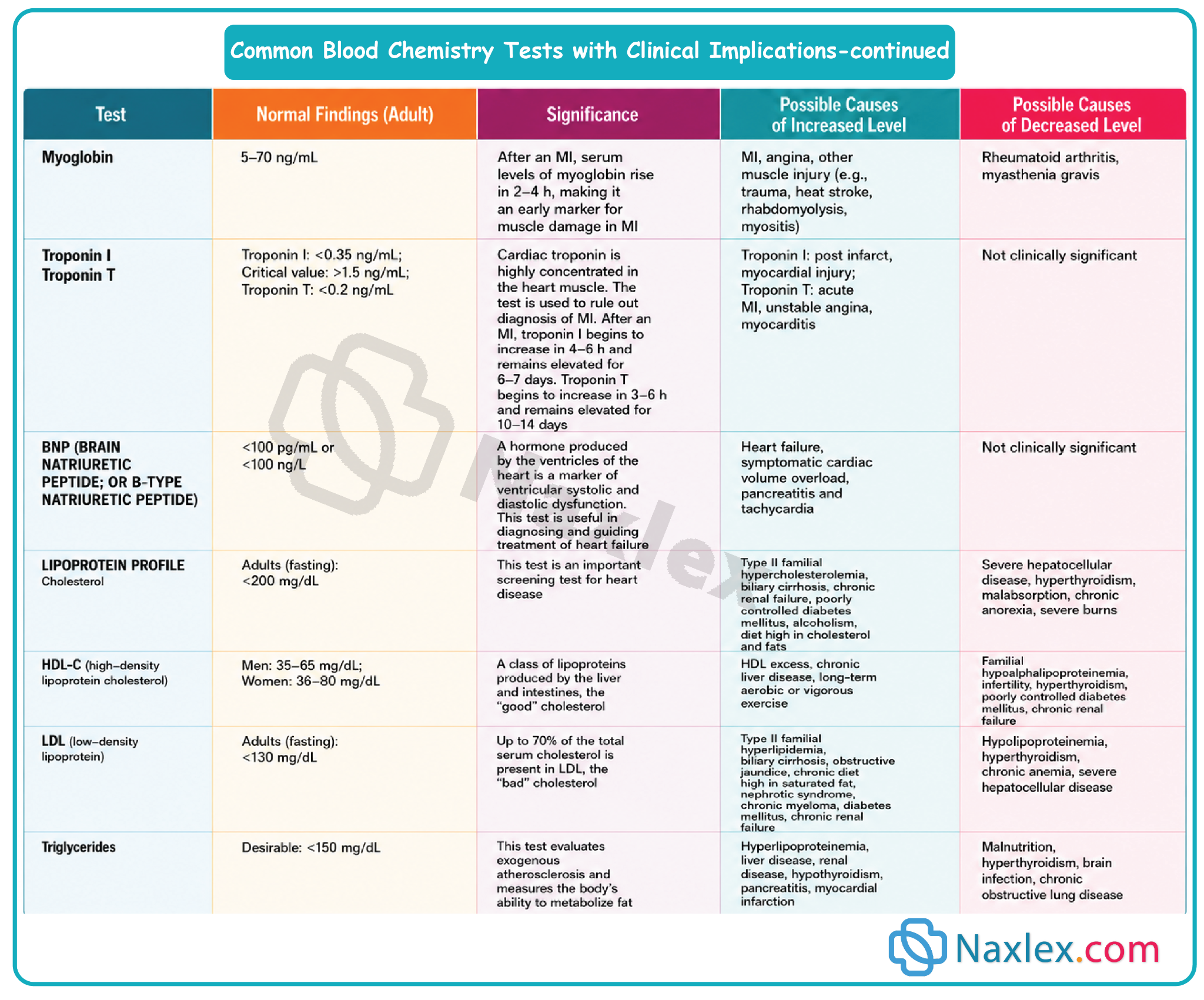
- Blood Chemistry
These are tests that may be performed on blood serum (the liquid portion of the blood).
Include determining certain enzymes that may be present (including lactic dehydrogenase [LDH], creatine kinase [CK], aspartate aminotransferase [AST], and alanine aminotransferase [ALT]), serum glucose, hemoglobin A1C (HbA1C) test, hormones such as thyroid hormone, and other substances such as cholesterol and triglycerides.
- Metabolic screening:
Newborns are routinely screened for congenital metabolic conditions- Tests for phenylketonuria (PKU), congenital hypothyroidism, sickle cell disease and galactosemia.
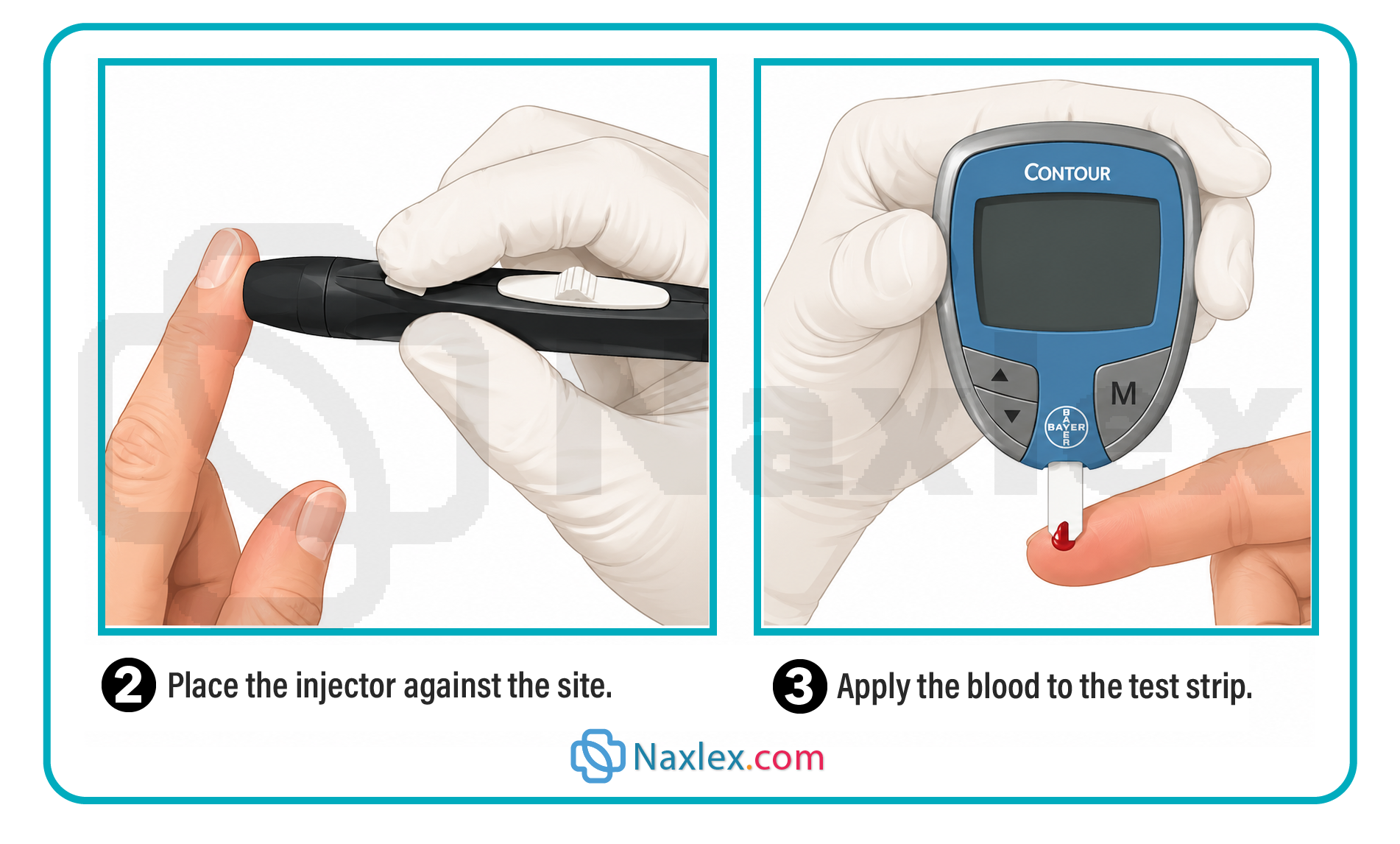
- Capillary Blood Glucose:
A capillary blood specimen is taken to measure the current blood glucose level when frequent tests are required or when a venipuncture cannot be performed.
Steps for obtaining a capillary blood specimen to measure blood glucose:
1. Preparation & Setup
- Review the specific manufacturer instructions for your glucose meter.
- Assemble all necessary equipment right at the client's bedside.
2. Implementation Procedure
Patient Intro & Hygiene
- Verify the client's identity, introduce yourself, and explain the procedure, its purpose, and how the results will impact their care.
- Perform hand hygiene, apply gloves, and ensure client privacy.
Site & Equipment Prep
- Turn on and prepare the meter (insert the test strip or calibrate/confirm the code if using an older model).
- Select the site: Choose the side of an adult's finger (avoiding bone) or an earlobe.
- Increase blood flow: Hold the finger below heart level, wrap it in a warm cloth, or gently rub the earlobe.
- Clean: Clean with soap and water or an antiseptic swab, allowing it to dry completely so alcohol doesn't alter the accuracy or cause stinging.
Sampling & Reading
- Puncture: Place the lancet perpendicular to the skin and pierce it using a quick darting motion.
- Collect: Gently squeeze for a drop of blood. Hold the strip to the drop to let it absorb or wick the blood without smearing it.
- Post-puncture: Have the client apply pressure to the site with gauze.
- Analyze: Leave the blood on the strip for the manufacturer's designated time. The meter will automatically display the glucose reading.
Cleanup & Documentation
- Dispose of the strip and gauze in a biohazard container, place the lancet in a sharps container, remove gloves, and wash hands.
- Document the results, testing method, and patient understanding on the client's record or diabetic flow sheet.
- Check for sliding scale insulin orders and administer medication as prescribed.
3. Evaluation
- Analyze Results: Compare the reading against normal ranges, previous results, and the client's current health status.
- Report & Follow-Up: Report abnormal results to the provider (confirming via venipuncture if required by agency policy).
- Patient Education: Assess the client's skin puncture site, evaluate their motivation and ability to self-test, and prepare them for home monitoring (frequency, record-keeping, and insulin administration).
Specimen Collection and Testing
Laboratory examination of specimens such as urine, blood, stool, sputum, and wound drainage provides important adjunct information for diagnosing health care problems and also provides a measure of the responses to therapy.
Nurses often assume the responsibility for specimen collection:
- Provide client comfort, privacy, and safety.
- Explain the purpose of the specimen collection and the procedure for obtaining the specimen.
- Use the correct procedure for obtaining a specimen or ensure that the client or staff follows the correct procedure.
- Note relevant information on the laboratory requisition slip, for example, medications the client is taking that may affect the results.
- Transport the specimen to the laboratory promptly. Fresh specimens provide more accurate results.
- Report abnormal laboratory findings to the health care provider in a timely manner consistent with the severity of the abnormal results.
6.1 Stool specimen collection and testing
1. Purposes of Fecal Analysis
|
Test Type |
Purpose / Clinical Significance |
Special Requirements |
|
Occult Blood (Guaiac) |
Detects hidden blood from ulcers, inflammatory disease, or tumors. |
Small smear on a card; sensitive to hemoglobin peroxidase. |
|
Dietary / Secretion |
Steatorrhea (excess fat) - absorption issue. Decreased bile - liver/gallbladder obstruction. |
Must collect the total quantity of a single bowel movement, not a small sample. |
|
Ova & Parasites (O&P) |
Identifies parasites and eggs. Requires 3 specimens over consecutive days. |
Must transport immediately while still warm. |
|
Bacteria / Viruses |
Cultures small amounts of feces to pinpoint infections. |
Must use sterile container/swab and aseptic technique. Note current antibiotics on lab form. |
2. Collection Guidelines & Patient Teaching
Patient Instructions (Crucial for Accuracy)
- Location: Defecate into a clean bedpan or bedside commode.
- No contamination: Void urine before the test. Do not contaminate the sample with urine or menstrual discharge.
- No toilet paper: Do not throw toilet tissue into the collection pan (chemicals alter lab results).
- Preparation: Remove toilet cleaners and flush twice before home collection.
Nursing Actions & Technique
- Safety & Hygiene: Wear clean gloves. Use 1–2 clean tongue blades to transfer the specimen; wrap sticks in paper towels and discard in regular waste (do not flush).
- Sample Size: Send ~2.5 cm (1 inch) of formed stool, or 15–30 mL of liquid stool.
- Target Selection: Intentionally include areas with visible pus, mucus, or blood.
- Timing & storage: Send to the lab immediately. If delayed, check container directions; some samples require refrigeration (never store in a fridge with food/meds).
- Delegation to UAP: Random collection and occult blood testing can be delegated. The nurse must perform sterile stool cultures. Instruct UAP to save positive cards for the nurse to verify.
3. Fecal Occult Blood Testing (FOBT)
Guaiac Smear (Hemoccult)
- Mechanism: Detects the enzyme peroxidase in hemoglobin.
- Interpretation: A blue color indicates a positive result (blood is present).
Nursing Alert: Color-blind nurses should not read these results.
- Interferences (The 3-to-7 Day Rule):
- False-Positives: Caused by red meat, raw vegetables/fruits (radishes, turnips, melons), and irritating medications (NSAIDs, aspirin, steroids, iron, anticoagulants). Restrict foods rich in Vit C for 3 days and meds for 7 days before testing.
- False-Negatives: Caused by taking >250 mg/day of Vitamin C up to 3 days before the test.
Fecal Immunochemical Test (FIT)
- Advantages over Guaiac: Higher sensitivity/specificity for colorectal cancer, no dietary or medication restrictions, and only requires 2 samples (instead of 3).
- Methods: Available as a liquid-based method (stored in a buffer solution) or a dry-slide method (collected via a long-handled brush).
Stool DNA Testing (Cologuard)
- A non-invasive screening tool for colorectal cancer that measures both human hemoglobin and specific cancer-related gene mutations.
4. Documentation Checklist
- Date, time, and specific collection method.
- Stool Characteristics: Color, odor, consistency, amount, and abnormal findings (mucus, blood).
- FOBT results (if performed).
- Patient tolerance (anal bleeding, discomfort during/after defecation) and perianal skin status.
- Patient/family education and ability to self-test.
Nursing insights:
LIFESPAN CONSIDERATIONS: Stool Specimen
INFANTS
- To collect a stool specimen for an infant, the stool is scraped from the diaper, being careful not to contaminate the stool with urine.
CHILDREN
- A child who is toilet trained should be able to provide a fecal specimen, but may prefer being assisted by a parent.
- When explaining the procedure to the child, use words appropriate for the child’s age rather than medical terms.
- Ask the parent what words the family normally uses to describe a bowel movement.
- A specimen for pinworms is collected by the parent early in the morning, after sleep and before the child has a bowel movement. Scotch tape is attached to a tongue blade and the sticky side is laid flat against the perineum and anus to pick up any eggs or small worms. The tongue blade is then examined under a microscope.
OLDER ADULTS
- Older adults may need assistance if serial stool specimens are required.
6.2 Urine specimens
Kidney function is directly dependent on cardiac output. Any systemic alteration that reduces cardiac output will inherently compromise renal perfusion and decrease urine output.
The nurse is responsible for collecting urine specimens for a number of tests:
- clean voided urine specimens for routine urinalysis
- clean-catch or midstream urine specimens for urine culture
- timed urine specimens for a variety of tests that depend on the client’s specific health problem
1. Routine & Culture Collection Methods
Clean Voided Specimen (Routine Urinalysis)
Used for general screening and non-culture testing.
- Optimal sample: First morning void. It has a higher, more uniform solute concentration and a more acidic pH.
- Volume required: A minimum of 10 mL is generally required for a standard urinalysis (UA).
- Contamination controls: Must be strictly free of fecal matter. Instruct female clients to discard toilet tissue in the toilet or waste bag, never in the collection pan (tissue fibers degrade lab analysis).
- Delegation: Collection can be delegated to Unlicensed Assistive Personnel (UAP) with clear instructions regarding client assistance or bedpan use.
Clean-Catch / Midstream Specimen (Culture & Sensitivity)
Ordered to identify specific uropathogens causing a Urinary Tract Infection (UTI).
-
- Perineal pre-wash:
Wash the external genitalia with soap and water to clear transient surface bacteria, then assess for any allergies to antiseptic cleansers.
-
- Targeted antiseptic cleansing:
Clean the urinary meatus using specific anatomical protocols, using each provided towelette exactly once.
- Female: Spread labia minora; cleanse front to back.
- Male: Retract foreskin if uncircumcised; cleanse in a circular motion from the meatus outward and down the shaft.
-
- Initiate voiding (initial flush):
Instruct the client to start urinating into the toilet or commode first. This initial stream clears out normal flora residing in the distal urethra and meatus.
-
- Midstream collection:
Without stopping the stream, pass the sterile specimen cup into the path of the running urine. Avoid letting the cup touch the penis, perineum, or labia.
2. Indwelling catheter specimen collection
Sterile urine specimens must be obtained from a closed drainage system using the built-in sampling port. Never collect a sample from the dependent drainage bag, as stagnant urine undergoes biochemical changes and bacterial overgrowth.
Structural Requirements
- Needleless Systems (Modern Standard): Utilize a Luer-Lok syringe inserted at a 90-degree angle perpendicular to the needleless port. Twist and lock to aspirate. The port self-seals upon removal.
- Traditional Rubber Catheters: Can only be performed on self-sealing rubber tubing (never on plastic, silicone, or Silastic). Insert a sterile needle at a 30- to 45-degree angle directly into the designated patch/port to facilitate self-sealing.
Procedure Sequence
- Apply clean gloves.
- Clamp the tubing: If fresh urine is not present in the tubing, clamp it at least 8 cm (3 inches) below the sampling port for up to 30 minutes to allow fresh urine to pool.
- Disinfect: Scrub the sampling port with a disinfectant swab. Ensure the site is distal to the balloon inflation tube to prevent accidental puncture of the balloon channel.
- Aspirate sample: Unclamp the tubing and withdraw the required volume:
- 3 mL for a sterile urine culture.
- 30 mL for a routine urinalysis.
- Transfer & clean: Transfer to a sterile container without touching the rim. Wipe the exterior of the container with disinfectant if contaminated.
- Transit: Unclamp the catheter line and send the sample to the lab immediately (or refrigerate).
3. Timed urine specimen
Some urine examinations require collection of all urine produced and voided over a specific period of time, ranging from 1 to 2 hours to 24 hours.
Timed specimens generally either are refrigerated or contain a preservative to prevent bacterial growth or decomposition of urine components. Each voiding of urine is collected in a small, clean container and then emptied immediately into the large refrigerated bottle or carton.
Timed urine specimens tests are performed for the following purposes:
- To assess the ability of the kidney to concentrate and dilute urine.
- To determine disorders of glucose metabolism, for example, diabetes mellitus.
- To determine levels of specific constituents, for example, albumin, amylase, creatinine, urobilinogen, or certain hormones (e.g., e striol or corticosteroids), in the urine.
Point-of-Care Urine Testing (Reagent Strips/Dipsticks)
Nurses or trained UAP can perform bedside reagent strip testing. Ensure strips are not outdated, follow exact manufacturer timing blocks for color reactions, and have UAP save positive samples for nursing verification.
|
Testing Parameter |
Clinical Range / Values |
Clinical Significance & Pathophysiology |
|
Specific Gravity |
1.010 to 1.025
|
Measures concentration/solute density.
• High (>1.025): Dehydration/fluid volume deficit, or excess solutes (glucose). • Low (<1.010): Fluid volume excess, high fluid intake, or renal inability to concentrate urine. |
|
Urinary pH |
Average: 6 (Slightly acidic; range 4.5–8.0) |
Reflects systemic acid-base regulation. • Metabolic Acidosis: Expected renal compensation drops pH (excreting H+ ions). • Metabolic Alkalosis: Expected renal compensation elevates pH. |
|
Glucose |
Negligible / Negative |
Screens for diabetes mellitus or gestational glucose intolerance. Inadequate for active glycemic monitoring; only indicated if blood glucose testing is refused or impossible. |
|
Ketones |
Negative |
Products of fatty acid catabolism. • Positive findings: Poorly controlled Type 1 diabetes (indicated during illness, fever, or BG consistently over 300 mg/dL), starvation, fasting, alcoholism, or strict high-protein diets. |
|
Protein |
Negative |
Plasma proteins are normally too large to pass the glomerular filtration barrier. • Positive findings: Indicates damage/increased permeability of the glomerular membrane (e.g., glomerulonephritis). |
|
Occult Blood |
Negative |
Highly sensitive indicator of micro/macro-hematuria. • > Clinical Alert: Indicates structural damage to the kidney parenchyma or the urinary tract lining. |
|
Osmolality |
50 to 1,200 mOsm/kg
|
Note: This is a laboratory test, not a bedside dipstick. Measures exact particle concentration (urea, creatinine, uric acid). • Elevated: Fluid volume deficit. • Decreased: Fluid volume excess. |
Documentation Checklist
- Exact date, time, and collection method (e.g., midstream vs. needleless catheter aspiration).
- Physical Characteristics: Color, clarity, presence of sediment, and distinct odors.
- Client tolerance, dysuria, or specific difficulties voiding.
- Lab Requisition Notations: Explicitly note if the client is currently on antibiotic therapy or is menstruating, as both alter diagnostic accuracy.
6.3 Sputum specimens
Sputum is a mucous secretion from the deep lower airways (lungs, bronchi, trachea). It must be strictly differentiated from saliva, which is clear oral secretions. Healthy individuals do not produce sputum.
Clinical indications & rationale
- Culture & Sensitivity (C&S): Identifies specific lower airway pathogens and determines targeted antimicrobial therapies.
- Cytology: Evaluates cellular structure to identify lung cancer and specific malignant cell types. Requires 3 serial early-morning specimens.
- Acid-Fast Bacillus (AFB): Screens for Mycobacterium tuberculosis (TB). Requires 3 consecutive daily early-morning collections, often using dedicated glass containers.
- Therapeutic Evaluation: Used to track if current respiratory therapies are resolving an infection.
Procedural mechanics & collection timing
- Optimal Timing: Early morning upon awakening (captures pooled nocturnal secretions) or immediately following postural drainage treatments.
- Volume Target: 1 to 2 teaspoons (4 to 10 mL) of thick expectorated sputum.
Step 1: Pre-Collection Oral Care:
Provide the client with fresh water to rinse the mouth. This clears residual food and transient oral microorganisms without altering lower airway flora.
Step 2: Airborne & droplet isolation setup:
If tuberculosis is suspected, perform collection in a negative-airflow isolation room, under UV lighting, or outdoors. If unavailable, wear a fitted respirator mask (capable of filtering droplet nuclei) along with standard gloves and PPE.
Step 3: Deep breathing & expectorated puncture:
Instruct the client to take deep breaths to expand the lungs, then perform a deep, productive cough to expectorate mucus directly into a sterile container. Prevent sputum from touching the container's exterior.
Step 4: Post-procedure hygiene & transit:
Offer mouthwash to alleviate an unpleasant taste. If the container's exterior is contaminated, wipe it down with disinfectant. Send the labeled sample to the lab immediately or refrigerate it to prevent normal contaminant overgrowth.
Nursing Scope & Delegation:
Expectorated collection can be delegated to UAP with directions on positioning and timing. However, if a client cannot cough, the nurse must perform an invasive pharyngeal suctioning procedure using a sterile sputum trap.
6.4 Throat culture
A throat culture samples the mucosa of the oropharynx and tonsillar pillars to isolate pathogenic microorganisms. This is an invasive procedure requiring nurse implementation to protect client safety and navigate airway reflexes.
Minimizing the gag reflex
The gag reflex is triggered by touching the pharyngeal walls or soft palate, causing the constrictor muscles of the pharynx to contract. To suppress this response and expose the target tissue, guide the patient through these steps:
- Positioning: Sit upright (if tolerated) to facilitate optimal visual alignment.
- Anatomical exposure: Have the client open their mouth wide and fully extend their tongue forward.
- Vocal relaxation: Instruct the client to say "ah." This vocalization lowers the back of the tongue, elevates the soft palate, and relaxes the pharyngeal constrictor muscles.
Collection technique
- Apply clean gloves.
- If the posterior wall is obscured, utilize a localized light source and gently depress the tongue with a clean tongue blade.
- Insert the sterile swab swiftly. Firmly run it across the tonsillar pillars and posterior pharynx, targeting areas that are explicitly reddened, inflamed, or contain purulent exudate.
- Remove the swab quickly without touching the teeth, gums, or buccal mucosa to prevent contamination. Secure it into the transport medium.
Documentation & Lab Requisition Checklist
- Exact date, time, and specific collection method utilized (e.g., expectorated vs. suctioned trap).
- Sputum Metrics: Record total volume, color (e.g., rust, green, clear), consistency (thick, tenacious, watery, mucoid), distinct odors, and any signs of hemoptysis (blood streaks).
- Auxiliary therapies used to assist collection (e.g., chest physiotherapy, postural drainage).
- Client comfort and tolerance of the procedure.
- Lab Requisition Entry: Explicitly note current or newly initiated antibiotic therapies on the laboratory requisition form, as this directly affects culture growth interpretation.
Nursing insights:
LIFESPAN CONSIDERATIONS: Sputum and Throat Specimens
INFANTS
- When taking a throat swab, avoid occluding an infant’s nose because infants normally breathe only through the nose.
CHILDREN
- Have a parent stand the young child between the parent’s legs with the child’s back to the parent and the parent’s arms gently but firmly around the child. As the parent tips the child’s head back, ask the child to open wide and stick the tongue out.
- Assure the child that the procedure will be over quickly and may “tickle” but should not hurt.
OLDER ADULTS
- Older adults may need encouragement to cough because a decreased cough reflex occurs with aging.
- Allow time for older adults to rest and recover between coughs when obtaining a sputum specimen.
Visualization Procedures
Diagnostic visualization splits into two primary modalities:
- Direct visualization (Invasive): Inside-the-body viewing via an inserted scope. Requires specialized consent, infection control, and post-procedural monitoring (e.g., perforation, bleeding, return of gag reflex).
- Indirect visualization (Noninvasive): Exterior imaging using structural or functional scanning modalities (X-ray, ultrasound, CT, MRI, Nuclear medicine).
1. Gastrointestinal (GI) System
Direct Visualization (Invasive)
Uses specialized scopes to view the luminal mucosal lining. All require post-procedural monitoring for complications like perforation or hemorrhage.
- Anoscopy: Visualizes the anal canal.
- Proctoscopy: Visualizes the rectum.
- Proctosigmoidoscopy: Visualizes the rectum and sigmoid colon.
- Colonoscopy: Visualizes the entire large intestine.
Indirect Visualization (Noninvasive)
Roentgenography (X-Ray & Fluoroscopy): Uses structural imaging to detect strictures, obstructions, tumors, ulcers, inflammatory disease, or hiatal hernias. Enhanced via radiopaque contrast (Barium Sulfate). Continuous flow is monitored in real-time via fluoroscopy.
|
Procedure |
Technique |
Nursing Implications |
|
Barium Swallow |
Patient drinks barium sulfate to image the upper GI tract/small bowel. |
Pre-op preparation; Post-op fluid management to avoid barium impaction (chalky white stools are expected). |
|
Barium Enema |
Barium enema is administered rectally to image the lower GI tract. |
Clear liquid diet/laxatives pre-procedure; evacuative clearance post-procedure. |
2. Urinary System
Direct Visualization (Invasive)
- Cystoscopy: Direct mucosal examination of the bladder, ureteral orifices, and urethra using a lighted cystoscope inserted transurethrally. Requires sterile technique.
Indirect Visualization (Noninvasive)
- KUB: Plain structural X-ray of the Kidneys, Ureters, and Bladder without contrast.
- Renal Ultrasonography: High-frequency reflected sound waves used to evaluate renal structures noninvasively.
- Intravenous Pyelography (IVP): Radiographic assessment of the urinary tract where contrast medium is injected intravenously and cleared renally.
- Retrograde Pyelography: Contrast medium is instilled directly into the renal pelvis via transurethral catheterization of the bladder and ureters.
3. Cardiopulmonary System
Cardiovascular Assessments
- Electrocardiography (ECG): Graphic recording of cardiac electrical activity using skin-surface electrodes.
- Echocardiogram: Noninvasive cardiac ultrasound assessing structural integrity and left ventricular ejection fraction. Nursing Note: Reassure the patient it is painless, though the conductive gel feels cold.
- Angiography: Invasive structural mapping of vascular patency using injected radiopaque dye under fluoroscopy.
- Coronary Angiography: Assesses the extent of coronary artery disease (CAD).
- Pulmonary Angiography: Evaluates the pulmonary vasculature, primarily to confirm a pulmonary embolism (PE).
- Other Sites: Carotid, cerebral, renal, and lower extremity vessels.
Respiratory assessments
- Chest X-Ray (CXR): Basic noninvasive structural imaging to diagnose and track pulmonary disease. Nursing Note: Ensure all jewelry and waist-up clothing are removed.
- Lung Scan (V/Q Scan): Nuclear imaging measuring gas and blood distribution. Used primarily to identify mismatch anomalies like pulmonary emboli.
- Perfusion Scan (Q Scan): Measures pulmonary blood flow via IV radioisotopes.
- Ventilation Scan (V Scan): Evaluates airway distribution (e.g., in emphysema) via inhaled radioactive gas.
- Nursing Note: Patient stays under a mask or exhales into room air. Scan takes 20 to 40 minutes. No radiation isolation precautions are needed (the dose is nominal).
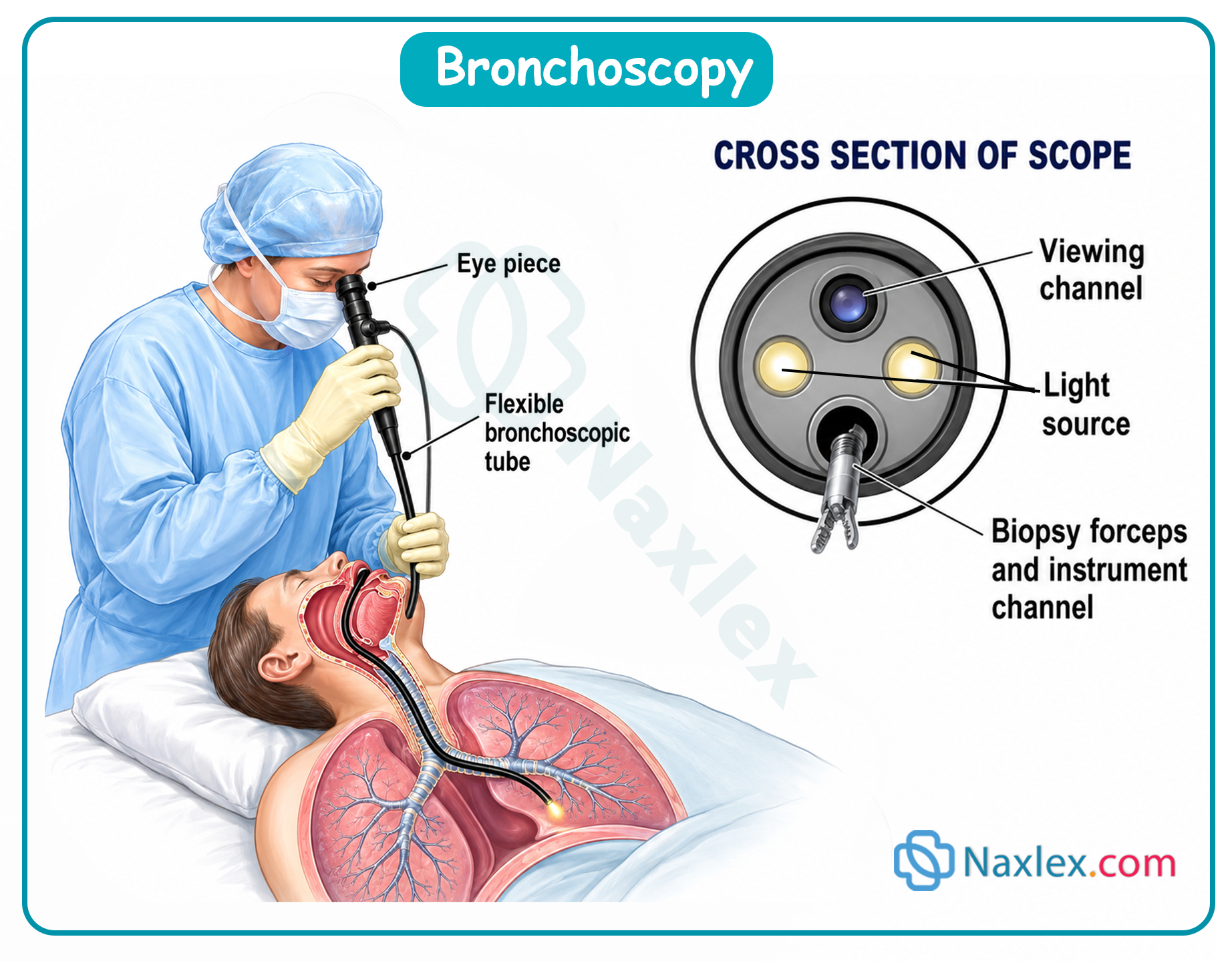
Direct airway visualization (Invasive)
- Laryngoscopy & Bronchoscopy: Sterile visualization of the larynx and tracheobronchial tree. Used for diagnostic examination or tissue biopsy.
- Nursing & Safety Protocols:
- Informed consent is mandatory.
- Administer local anesthetic spray or gargle to the pharynx to completely abolish the gag reflex.
- Strictly NPO post-procedure until a positive gag reflex returns to prevent aspiration.
4. Advanced Advanced Cross-Sectional Imaging
Computed Tomography (CT)
- Mechanism: Multi-angle, high-sensitivity X-ray imaging creating three-dimensional structural reconstructions. Very sensitive to minor differences in tissue density.
Magnetic Resonance Imaging (MRI)
- Mechanism: Noninvasive scanning leveraging high-energy magnetic fields to align atomic nuclei. Avoids ionizing radiation. Provides superior soft-tissue contrast compared to CT.
MRI Safety Screen Checklist
- Implanted medical devices: Strictly contraindicated for ferromagnetically active implants (e.g., older pacemakers, specific metal hip prostheses).
- Removable metal: Remove all rings, watches, phones, and body jewelry. Exception: Titanium, niobium, and true surgical stainless steel are non-ferromagnetic and safe.
- Transdermal Patches: Remove all patches containing foil or metallic backings prior to scanning to prevent local thermal skin burns. Advise the patient to reapply a fresh patch post-procedure.
- Tattoos & Permanent Makeup: Screen for body tattoos (especially red pigments). Remind patients they may feel localized warming or mild edema and should report unusual sensations immediately to the operator.
- Environment/Comfort: High-magnet closed tunnels can trigger severe claustrophobia. Utilize the internal two-way communication system for constant monitoring. Provide earplugs to attenuate the loud acoustic noises during the 60–90 minute scan.
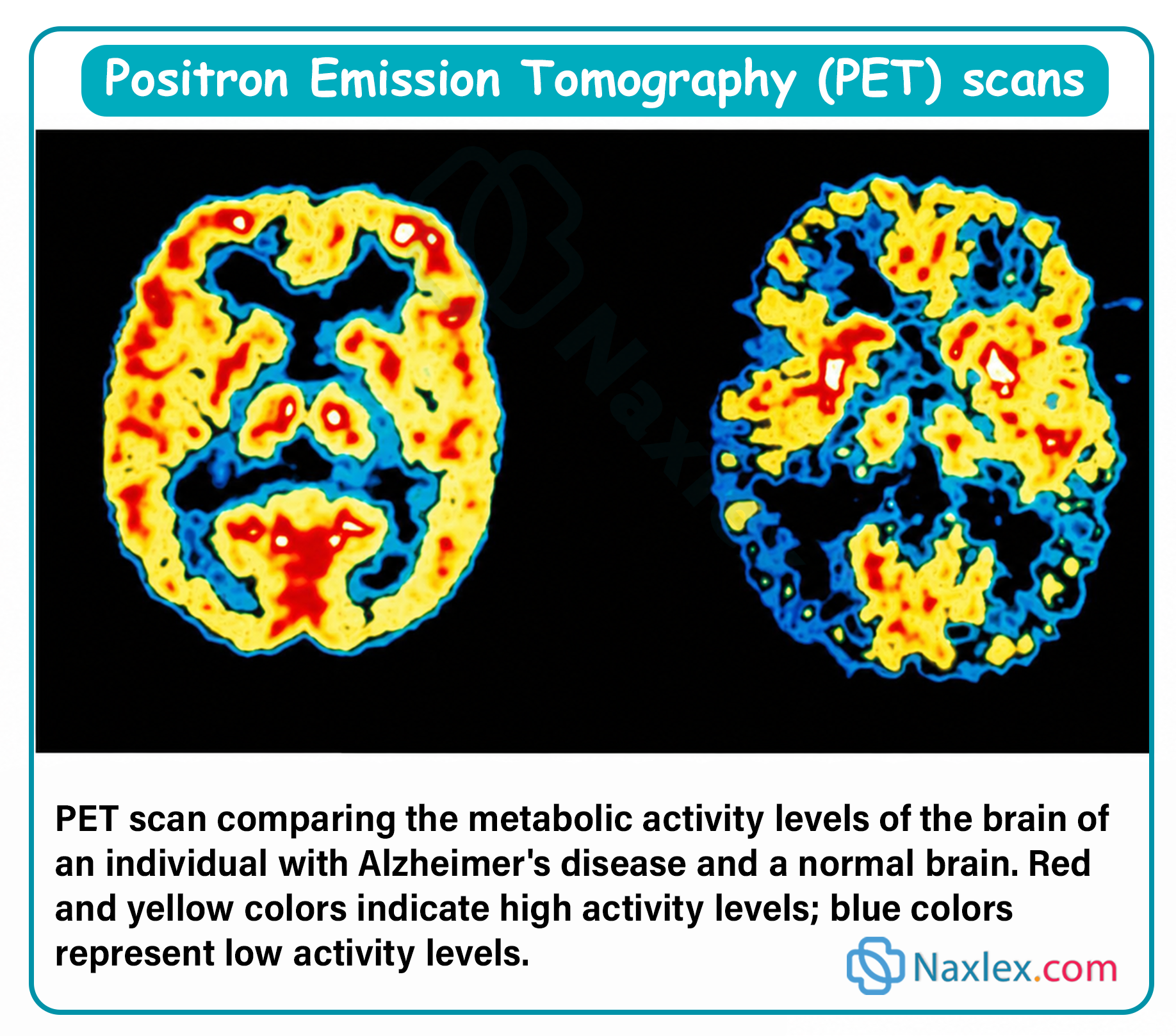
5. Nuclear Imaging
Nuclear medicine tracks organ physiological dynamics using targeted radiopharmaceuticals. Tissue uptake patterns showcase metabolic activity:
- Normal tissue- uniform, equal gray distribution
- Hyperfunctioning tissue- increased uptake; darker images (hot spots)
- Hypo functioning tissue- decreased uptake; lighter images (cold spots)
Positron Emission Tomography (PET): A functional nuclear study using an inhaled or injected radioisotope to dynamically track organ perfusion, cellular metabolic activity, and malignant tumor growth patterns.
Aspiration/Biopsy
Aspiration is the withdrawal of fluid that has abnormally collected (e.g., pleural cavity, abdominal cavity) or the obtaining of a specimen (e.g., cerebrospinal fluid).
A biopsy is the removal and examination of tissue. Biopsies are usually performed to determine a diagnosis or to detect malignancy.
Both aspiration and biopsy are invasive procedures and require strict sterile technique.
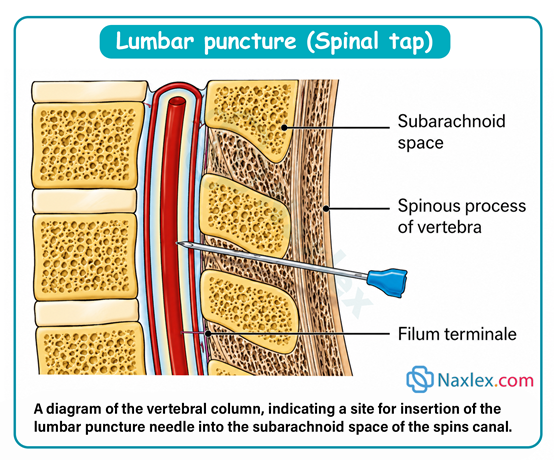
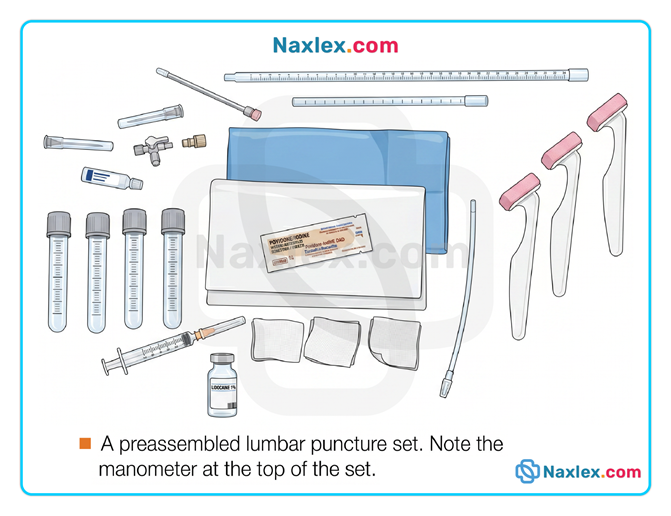
10.1 Lumbar puncture (Spinal tap)
- Purpose: Withdraw cerebrospinal fluid (CSF) from the subarachnoid space for diagnostics or pressure readings via a manometer.
- Anatomical Site: Between L3–L4 or L4–L5 (avoids the spinal cord and major nerve roots).
Clinical Workflow
- Pre-procedure: Explain that they must remain still for ~15 minutes; they will feel a local anesthetic pinprick and insertion pressure. Have the client empty their bladder and bowels before starting to optimize comfort.
- Positioning: Lateral (side-lying) with head bent toward the chest and knees flexed up to the abdomen (arches the back to widen intervertebral spaces).
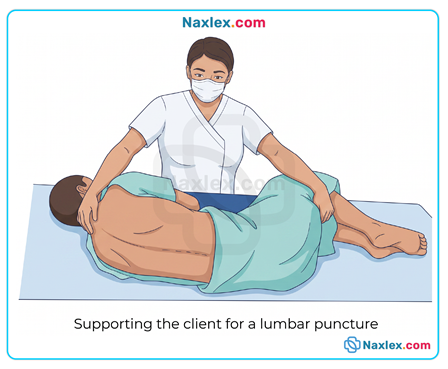
- During: Stand in front of the client to help them stay still. Monitor color, respirations, and pulse. Label specimen tubes in exact sequence and wear gloves.
- Post-procedure:
- Place a small sterile dressing over the site.
- Position client flat in dorsal recumbent with only one head pillow for 1 to 12 hours (per provider orders) to prevent spinal headaches.
- Encourage frequent oral fluids to help restore CSF volume.
- Monitor neurologic status and check for numbness, tingling, or radiating leg pain.
Nursing insights:
LIFESPAN CONSIDERATIONS: Lumbar Puncture
CHILDREN
- Briefly demonstrate the procedure on a doll or stuffed animal. Allow time to answer questions.
- One member of the health care team should stay in close physical contact with the child, maintain eye contact, and talk to and reassure the child during the procedure.
OLDER ADULTS
- Some clients need help maintaining the flexed position due to arthritis, weakness, or tremors.
- Provide an extra blanket to keep the client warm during the procedure. Older adults have a decreased metabolism and less subcutaneous fat.
- If the client has a hearing loss, speak slowly, distinctly, and loud enough, especially when unable to make eye contact.
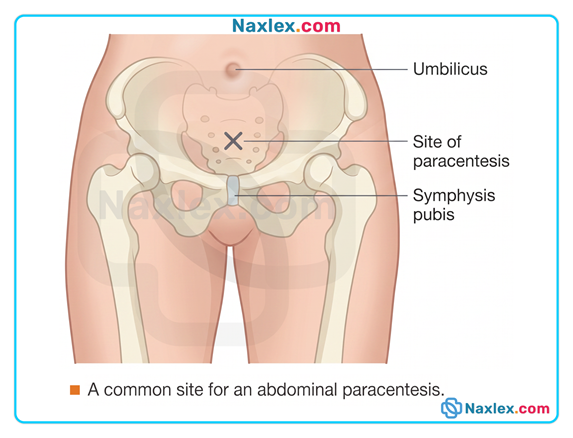
10.2 Abdominal paracentesis
- Purpose: To drain excess peritoneal fluid (ascites) to relieve abdominal organ pressure or collect fluid samples. Normal ascitic fluid is serous, clear, and light yellow.
- Anatomical Site: Midway between the umbilicus and the symphysis pubis on the abdominal midline.
Clinical Workflow
- Pre-procedure: Have the client void immediately before the procedure to empty the bladder and prevent accidental puncture.
- Positioning: Sitting position up in bed, in a chair, or at the edge of the bed supported by pillows.
- During: Observe closely for distress and signs of hypovolemic shock due to rapid fluid shifts (pallor, dyspnea, diaphoresis, dropping blood pressure, anxiety).
- Post-procedure:
- Apply a small sterile dressing.
- Monitor vital signs, urine output, and site drainage every 15 minutes for the first 2 hours, then hourly for 4 hours.
- Measure abdominal girth at the level of the umbilicus before and after.
- For male clients: Check specifically for scrotal edema.
Critical Safety Limit: Drain fluid very slowly and cap the maximum volume at 1,500 mL at one time to avoid hypovolemic shock. Older adults have an even lower tolerance for rapid fluid loss.
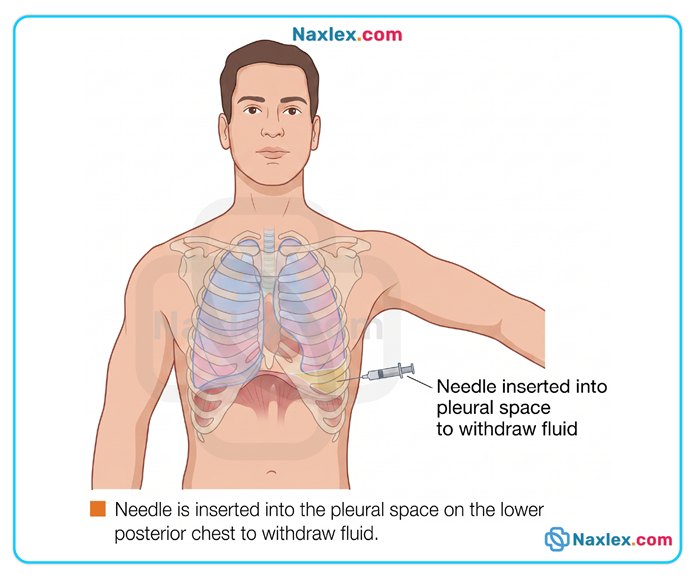
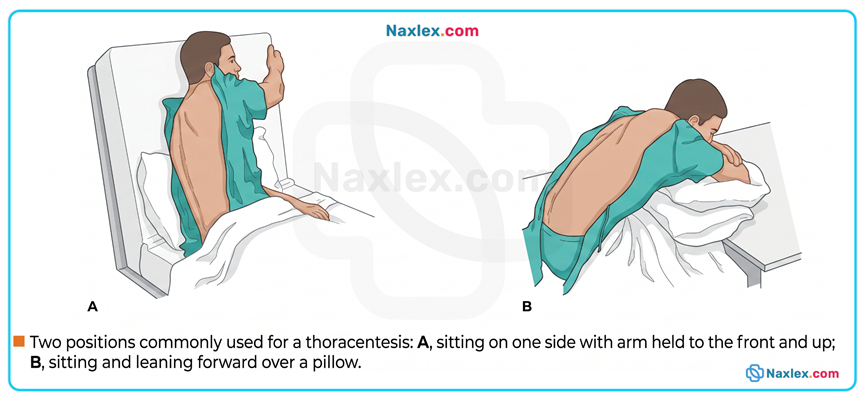
10.3 Thoracentesis
- Purpose: Remove excess fluid or air from the pleural cavity to ease breathing, or to introduce intrapleural chemotherapy.
- Anatomical Site: Tailored by chest X-ray, percussion, and palpation. Typically, the lower posterior chest is selected to remove fluid, while the upper anterior chest is used to remove air.
Clinical Workflow
- Pre-procedure: Advise the client that they will feel pressure. Instruct them absolutely not to cough during needle insertion to avoid lung puncture.
- Positioning: Sitting up with arms raised above the head or leaning forward over a bedside pillow table. This spreads the ribs and enlarges the intercostal spaces.
- During: Monitor for respiratory distress (dyspnea, pallor, coughing). Ensure the stopcock attached to the aspirating needle stays closed when not actively draining so air cannot enter the pleural space. Keep collection containers below lung level.
- Post-procedure:
- Apply a sterile dressing. Do not remove more than 1,000 mL of fluid within the first 30 minutes.
- Assess breath sounds, respiratory rate/depth, chest pain, and changes in cough or sputum.
- Position the client on their unaffected side with the head of the bed elevated 30° for at least 30 minutes to facilitate lung expansion.
Nursing insights:
LIFESPAN CONSIDERATIONS: Thoracentesis
OLDER ADULTS
- Some older clients will need help maintaining the proper position due to arthritis, tremors, or weakness.
- Provide support with pillows during the procedure.
- Absence of body fat in older adults can help the primary care provider locate the intercostal spaces.
- Provide an extra blanket to keep your client warm during the procedure. Older adults have a decreased metabolism and less subcutaneous fat.
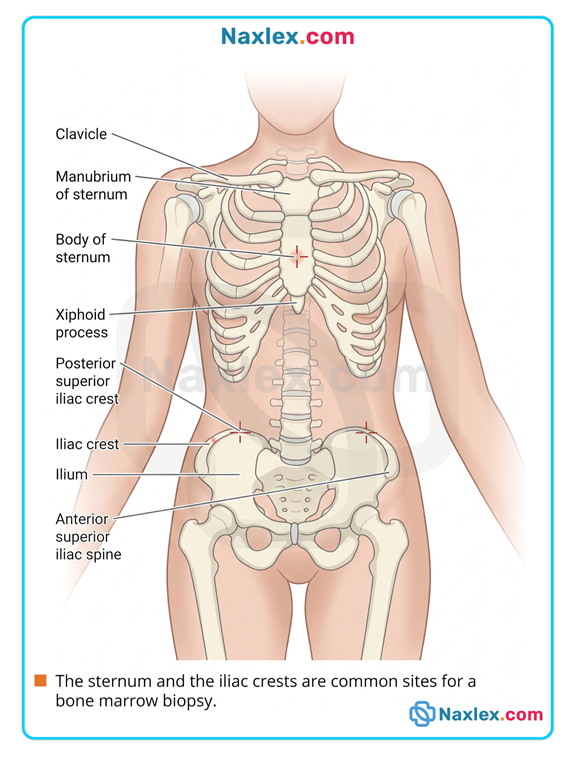
10.4 Bone marrow biopsy
- Purpose: Remove a sample of red bone marrow to diagnose blood disorders like leukemia or pernicious anemia.
- Anatomical Site: Sternum, iliac crests, anterior/posterior iliac spines. The posterior superior iliac crest is preferred.
Clinical Workflow
- Pre-procedure: Warn the client they may hear a "crunching" sound as the needle passes through the bone cortex and feel brief pain during marrow aspiration (1–2 mL collected). Administer sedatives as ordered.
- Positioning: Supine for a sternal biopsy; prone or side-lying for an iliac crest biopsy.
- During: Monitor for pallor, sweating (diaphoresis), or faintness from pain or bleeding.
- Post-procedure:
- Apply a small dressing. Many protocols require direct pressure for 5–10 minutes to prevent bleeding.
- Assess the site closely for bleeding and hematoma formation for several days.
- Provide prescribed analgesics for bone tenderness.
Nursing insights
LIFESPAN CONSIDERATIONS: Bone Marrow Biopsy
CHILDREN
- Young clients need emotional support due to the pain and pressure associated with this procedure.
- Young clients may require gentle restraint to prevent movement during the procedure.
OLDER ADULTS
- Older adults with osteoporosis will experience less needle pressure.
- Ask the client to empty the bladder for comfort before the procedure.
- Provide pillows and blankets to help older adults remain comfortable during the procedure.
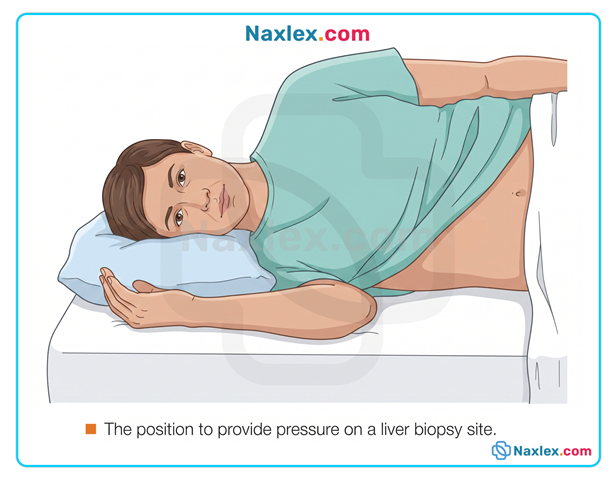
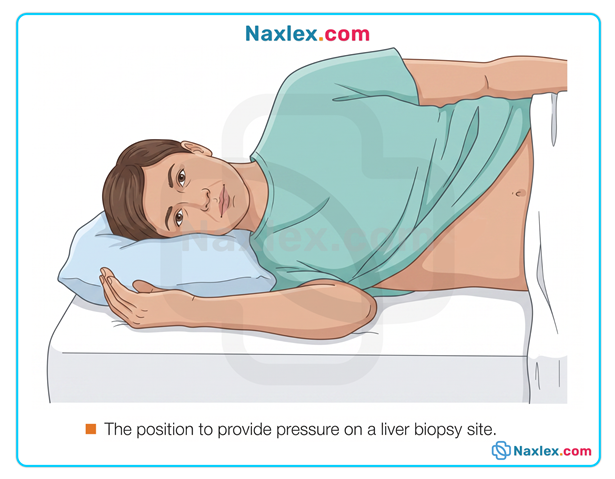
10.5 Liver biopsy
- Purpose: Aspirate a small sample of liver tissue at the bedside.
- Anatomical Site: Through the intercostal space between the two right lower ribs or subcostally (below the right rib cage).
Clinical Workflow
- Pre-procedure: Verify prothrombin time and platelet counts well in advance (abnormal clotting speeds make this highly contraindicated). Ensure the client fasts for at least 2 hours. Administer ordered sedatives or Vitamin K (given days prior to minimize hemorrhage risk).
- Positioning: Supine with the upper right quadrant exposed.
- During:
- Crucial breathing command: Instruct the client to take a few deep breaths, exhale completely, and hold their breath for up to 10 seconds during needle insertion and withdrawal. This immobilizes the chest wall and holds the diaphragm at its highest position, avoiding lung or liver laceration.
- Post-procedure:
- Apply immediate pressure and a small dressing.
- Positioning: Turn the client onto a right side-lying position with a small pillow or folded towel directly under the biopsy site for several hours to compress the liver against the chest wall and prevent bleeding.
-
- Monitor vital signs every 15 minutes for the first hour, then hourly for 24 hours.
- Assess for severe abdominal pain, which can indicate bile peritonitis (bile leaking into the abdominal cavity).
Nursing insights
LIFESPAN CONSIDERATIONS: Liver Biopsy
OLDER ADULTS
- Observe for skin irritation from tape applied to the sterile dressing. Older adults often have fragile skin.
- Ask the client to empty the bladder before the procedure. Older adults may need to void more often and in smaller amounts.
10.6 Core charting requirements for all procedures
For every procedure, the nurse must explicitly document:
- Date, time, and the performing provider's name.
- Fluid/tissue characteristics: Exact volume, color, and clarity/character of any fluid drained.
- Total number of specimens obtained and confirmation of immediate, correctly labeled transport to the lab.
- Specific measurements (e.g., pre/post abdominal girth for paracentesis, CSF pressure readings for LP).
- Detailed nursing interventions and client tolerance (vital signs, pain levels, and neuro/respiratory checks).
Summary
- Diagnostic testing involves three phases.
- Client preparation is the focus during the pretest phase.
- During the intratest phase, the nurse performs or assists with the diagnostic test and collects the specimen.
- Providing nursing care of the client and follow-up activities and observations are the role of the nurse during the post-test phase.
- Nursing responsibilities associated with specimen collection include
- providing client comfort, privacy, and safety
- explaining the purpose of and procedure for the specimen collection
- using correct procedure for obtaining the specimen
- noting relevant information on the laboratory requisition slip
- transporting the specimen promptly
- reporting abnormal findings.
- Visualization procedures include indirect visualization or noninvasive procedures such as lung scan, echocardiogram, electrocardiography, x-ray, CT, and MRI.
- In contrast, direct visualization or invasive techniques visualize body organs and system functions. Examples of invasive procedures include colonoscopy, barium enema, intravenous pyelography, and angiography.
