
Acquired Cardiovascular Disorders: Acute Rheumatic Fever
Study Questions
Practice Exercise 1
A nurse has attended a staff education program on streptococcal infection of the throat. The most serious complication of this infection is:
Explanation
Streptococcal pharyngitis,caused by Streptococcus pyogenes,can trigger non-suppurative sequelae through molecular mimicry.Bacterial M-proteins cross-react with human tissues, inducing a systemic inflammatory response affecting the joints, skin, and central nervous system, leading to permanent structural injuries.
Rationale for correct answer:
4.Rheumatic heart diseaseis the most critical consequence because immune-mediated pancarditis leads to chronic valvular stenosisand insufficiency. Recurrent inflammation causes scarring, heart failure, and permanent structural damage, requiring lifelong secondary antibiotic prophylaxis.
Rationale for incorrect answers:
1.Lymphadenopathyrepresents a localized, acute lymphatic response rather than a life-threatening systemic complication. The enlargement ofcervical nodesis a typical symptom of active inflammation during the acute phase of infection.
2.Scarlet feveris an acute cutaneous manifestation driven by erythrogenic exotoxins rather than a permanent destructive complication. It presents as a diffuse erythematous rashand strawberry tongue, resolving completely with appropriate courses of standard antibiotics.
3.Encephalitisis an inflammation of the brain parenchyma that is not typically caused by Group A streptococcal infections. Neurological sequelae are instead associated with chorea orautoimmune disorderslike PANDAS, rather than primary viral-like encephalitis.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the most serious, life-threatening complication resulting from a streptococcal infection of the throat.
- Evaluate severity and pathophysiology:
- Rule outChoice 1:Lymphadenopathy is a localized, expected symptom during acute infection rather than a long-term chronic threat.
- Rule outChoice 2:Scarlet fever is a toxin-mediated acute systemic illness, but it resolves cleanly with standard antimicrobial therapy.
- Rule outChoice 3:Encephalitis is not a recognized direct consequence of streptococcal pharyngitis infections.
- Select Choice 4:Rheumatic heart disease causes irreversible, progressive cardiac damage, making it the most severe long-term sequela.
Take home points
- Rheumatic heart disease is an autoimmune sequela of Streptococcus pyogenes pharyngitis caused by cross-reactive antibodies attacking cardiac tissue.
- The chronic phase is characterized by progressive valvular scarring, most frequently targeting the mitral valve, leading to stenosis.
- Prompt treatment of streptococcal pharyngitis with penicillin within 9 days of onset is highly effective in preventing rheumatic fever.
- Acute clinical features of the underlying rheumatic fever include migratory polyarthritis, erythema marginatum, subcutaneous nodules, and Sydenham chorea.
The nurse is reviewing the medical record of an 8-year-old child suspected of having acute rheumatic fever. Which historical finding is most critical to confirm the etiology of this disease?
Explanation
Acute rheumatic feverdevelops exclusively as a delayed, non-suppurative autoimmune response following a streptococcal pharyngitisinfection. The immune system generates cross-reactive antibodies against bacterial M proteins that mistakenly attack host tissues, causing diffuse inflammatory lesions within the connective tissues.
Rationale for correct answer:
2.A documented untreated upper respiratory infectionis the definitive prequalifying criterion required by the modified Jones criteria. The latent period between the pharyngeal infection and the onset of rheumatic symptoms typically spans 2 to 3 weeks.
Rationale for incorrect answers:
1.A history of superficial pyoderma or impetigois associated with post-streptococcal glomerulonephritis but does not trigger acute rheumatic fever.Skin strains of Group A Streptococcus lack the specific rheumatogenic properties needed to cause systemic pancarditis.
3.A genetic family history of structural cardiac anomaliessuch as congenital aortic stenosis does not provide the required infectious etiology needed to precipitate this condition. Congenital aortic stenosis is a localized structural defectpresent at birth, unrelated to acquired post-infectious inflammatory diseases.
4.Exposure to infectious mononucleosisinvolves the Epstein-Barr virus, which causes entirely different clinical manifestations and long-term sequelae. Viral pharyngitis does not stimulate the molecular mimicrypathways that lead to the cross-reactive antibodies seen in rheumatogenic disease.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the most critical historical finding to confirm the specific etiology of acute rheumatic fever in an 8-year-old child.
- Evaluate pathophysiological links:
- Rule outChoice 1:Impetigo is a cutaneous streptococcal infection that causes renal complications, never cardiac rheumatic sequelae.
- Rule inChoice 2:Untreated streptococcal pharyngitis is the mandatory primary antecedent event required to establish a valid diagnosis.
- Rule outChoice 3:Congenital conditions represent inherited anatomical defects rather than an acquired, post-infectious inflammatory response.
- Rule outChoice 4:Viral exposures explain standard mononucleosis symptoms but bear no causal relationship to post-streptococcal autoimmune disease.
Take home points
- Acute rheumatic fever occurs only after upper respiratory tract infections caused by Group A beta-hemolytic streptococci, never after skin infections.
- Confirmation of the antecedent infection requires a positive throat culture, rapid antigen test, or elevated antistreptolysin O antibody titers.
- The inflammatory process targets the endocardium, myocardium, and pericardium, frequently causing acute mitral valve regurgitation during the initial illness.
- Eradication of the initial pharyngeal infection with appropriate antibiotic courses prevents the subsequent development of the autoimmune cascade completely.
The nurse understands that the tissue damage seen in acute rheumatic fever is not caused by a direct bacterial invasion of the tissues, but rather by which mechanism?
Explanation
Acute rheumatic feverrepresents a post-infectious, non-suppurative sequela driven by a type II hypersensitivityreaction. Structural similarities between bacterial cell wall components and human connective tissues cause the immune system to inadvertently target self-antigens, leading to widespread inflammatory damage across multiple organ systems.
Rationale for correct answer:
3.Molecular mimicryoccurs when antibodies generated against streptococcal M proteinsmistakenly attack host tissues sharing similar antigenic determinants. This cross-reactivity targets cardiac myosin, valvular endothelium, joint synovium, and basal ganglia neurons, causing the clinical manifestations.
Rationale for incorrect answers:
1.A type I immediate hypersensitivity reactionis an allergic response driven by allergen cross-linking of IgE antibodieson mast cells. This pathway triggers anaphylaxis, asthma, and urticaria, rather than the delayed, tissue-destructive autoimmune response seen here.
2.Direct cytotoxicity from circulating bacterial exotoxinscauses acute illnesses like toxic shock syndrome or scarlet fever rather than delayed autoimmunity.Rheumatic manifestations appear weeks after the active pharyngeal infection has already been cleared from the body.
4.Microvascular occlusioncaused by bacterial emboli describes the mechanical damage pathway seen in infective endocarditis during active bacterial seeding.Rheumatic fever is strictly a sterile, immune-mediated inflammatory process without live bacterial colonization in affected tissues.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the specific immunological mechanism responsible for tissue damage in acute rheumatic fever, emphasizing it is not a direct bacterial invasion.
- Evaluate Immunological Pathways:
- Rule outChoice 1:IgE-mediated reactions govern immediate allergies and anaphylaxis, not delayed organ-specific autoimmune destruction.
- Rule outChoice 2:Exotoxins cause acute localized or systemic toxic signs, not the delayed sterile inflammation characteristic of this sequela.
- Rule inChoice 3:Cross-reactive antibody binding via molecular mimicry perfectly describes the true underlying autoimmune pathophysiology.
- Rule outChoice 4:Bacterial emboli imply active, septic thromboembolic events which occur in endocarditis, not rheumatic fever.
Take home points
- The pathogenesis of acute rheumatic fever centers on a type II hypersensitivity reaction where antibodies cross-react with endogenous tissue antigens.
- Streptococcal M protein is the primary virulence factor responsible for triggering the cross-reactive humoral and cellular immune responses.
- Affected organs remain sterile during the disease process, meaning live bacteria cannot be cultured from the heart, joints, or brain.
- The Aschoff body is the pathognomonic histological lesion found in myocardial tissue, representing localized granulomatous inflammation.
A 12-year-old child presents with symptoms of ARF. While taking the history, the parents mention that the child lives in a crowded, multi-generational household with limited access to consistent medical care. How should the nurse interpret this information?
Explanation
Acute rheumatic feverexhibits a strong epidemiological correlation with poor socioeconomic conditions that promote the spread of upper respiratory pathogens. Widespread social determinantsof health,including dense housing and inadequate healthcare access, directly accelerate the replication and transmission of rheumatogenic strains within vulnerable pediatric populations.
Rationale for correct answer:
2.Crowded households and restricted healthcare accessrepresent classic socioeconomic risk factors that dramatically increase GABHS transmissionrates among children. Overcrowding facilitates close-contact droplet spread, while sparse medical care leaves primary pharyngeal infections untreated, allowing the autoimmune cascade to initiate.
Rationale for incorrect answers:
1.Environmental factors like housing density or medical accessdo not alter the inherited genetic composition of an individual's HLA markers.Human leukocyte antigens are genetically predetermined structures that influence susceptibility, rather than dynamic variables modified by external living arrangements.
3.Living in a crowded multi-generational homedoes not specifically indicate that the child is experiencing a concurrent viral co-infection.While crowding increases exposure to all respiratory pathogens, the presenting pathology is strictly a post-streptococcal bacterial sequela.
4.Widespread socioeconomic disadvantagesdo not alter the underlying sterile, immune-mediated nature of the disease into a suppurative infection.The disease process remains an autoimmune, non-suppurative complication regardless of the patient's background or the environment where transmission occurred.
Test-taking strategy:
- Analyze the scenario/question:The question describes a 12-year-old child with acute rheumatic fever living in a crowded household with poor healthcare access, asking the nurse to interpret these environmental findings.
- Evaluate epidemiological principles:
- Rule outChoice 1:Genetic markers are inherited at birth and cannot be rewritten or modified by crowded living conditions.
- Rule inChoice 2:Overcrowding and lack of treatment directly maximize the spread and duration of streptococcal pharyngitis infections.
- Rule outChoice 3:The presentation is a specific bacterial sequela; crowding does not dictate or imply a viral co-infection.
- Rule outChoice 4:Socioeconomic status affects disease transmission dynamics but never alters the fundamental autoimmune pathophysiology.
Take home points
- Acute rheumatic fever is considered a disease of poverty because its incidence tracks closely with overcrowding and sub-standard housing.
- Crowded environments optimize the droplet transmission of Group A beta-hemolytic streptococcus among school-aged children and family members.
- Inadequate access to timely primary healthcare prevents the administration of early antibiotic therapy, which is required to clear pharyngeal infections.
- Public health interventions targeting housing quality and accessible penicillin clinics are vital to lowering the global burden of rheumatic heart disease.
Practice Excercise 2
A 7-year-old child has been diagnosed with rheumatic fever. Which of the following physical findings would the nurse expect to assess?
Explanation
Acute rheumatic fevertypically manifests with key inflammatory signs across multiple organ systems, with migratory arthritis being the most common clinical feature. The systemic inflammationtargeted at connective tissues primarily affects large joints, producing temporary, reversible manifestations that clear without causing permanent joint deformities.
Rationale for correct answer:
2.Migratory polyarthritisclassically causes warm, painful, and swollen knees and elbowsas a primary major Jones criterion. The inflammation typically moves from one large joint to another sequentially, responding dramatically to standard anti-inflammatory therapeutic regimens.
Rationale for incorrect answers:
1.A vesicular rash over the face and chestis typical of varicella or herpes zoster infectionsrather than acute rheumatic fever. The dermatological manifestation specific to this condition is erythema marginatum, which presents as non-pruritic, erythematous macules with pale centers.
3.A palpable mass in the upper right quadrant of the abdomenindicates hepatomegaly or gallbladder pathologyrather than typical rheumatic lesions. While severe carditis can cause congestive hepatomegaly, a distinct palpable mass is not a standard expected finding.
4.Yellow pigmentation of the scleraeindicates jaundice, signifying hepatic dysfunction or hemolysisrather than localized post-streptococcal connective tissue inflammation. The disease process does not target the biliary system or induce significant red blood cell destruction.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the expected physical assessment finding in a 7-year-old child diagnosed with acute rheumatic fever.
- Evaluate diagnostic criteria:
- Rule outChoice 1:Vesicular rashes indicate viral processes, whereas rheumatic fever features distinct, non-vesicular erythema marginatum.
- Rule inChoice 2:Large joint polyarthritis is the most frequent major clinical manifestation observed during the acute phase.
- Rule outChoice 3:Abdominal masses point toward localized visceral pathology or tumors, not transient systemic autoimmune inflammation.
- Rule outChoice 4:Scleral icterus points to hepatobiliary issues or hemolysis, which are unrelated to the sterile autoimmune cascade.
Take home points
- Migratory polyarthritis affects approximately 75% of patients during the acute phase, characteristically involving large joints like knees, ankles, and elbows.
- Joint pain is typically disproportionately severe compared to the objective physical signs of swelling and redness observed during examination.
- Erythema marginatum is a transient, non-pruritic rash with elevated margins that typically appears on the trunk and proximal extremities.
- Subcutaneous nodules are firm, painless lumps found over bony prominences that usually correlate with the presence of severe carditis.
The nurse in the pediatric unit is assessing a 7-year-old client. What manifestations most strongly support a diagnosis of acute rheumatic fever?
Explanation
The clinical confirmation of acute rheumatic feverrelies heavily on the structured application of the modified Jones criteria.Establishing a definitive diagnosis requires objective evidence of a preceding group A streptococcal infection paired with specific combinations of major and minor systemic inflammatory manifestations.
Rationale for correct answer:
1.Carditis, polyarthritis, and erythema marginatumrepresent three definitive major clinical signs that provide the most robust diagnostic validation. Presenting with multiple major criteria fulfills the clinical threshold required to confirm the presence of this active post-streptococcal autoimmune process.
Rationale for incorrect answers:
2.Although polyarthritis and Sydenham choreaare recognized major signs, a decreased antistreptolysin O titer directly contradicts the diagnostic requirements. Confirming this condition requires laboratory evidence of an elevated titerto prove the mandatory antecedent group A streptococcal exposure.
3.Organic heart murmurssignify carditis, but fever and an elevated erythrocyte sedimentation rate are classified only as weaker minor criteria. A combination consisting of one major sign and two minor signs is insufficient unless accompanied by documented preceding infection.
4.A positive C-reactive protein and elevated white blood cell countsare non-specific systemic inflammatory markers categorized as minor signs. While subcutaneous nodules represent a major manifestation, these non-specific laboratory values cannot independently substantiate the diagnosis.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the group of manifestations that most strongly support and validate a diagnosis of acute rheumatic fever in a pediatric client.
- Apply diagnostic frameworks:
- Rule inChoice 1:This option contains three distinct major criteria, which represents the strongest possible diagnostic grouping.
- Rule outChoice 2:A low or decreasing serological antibody titer disproves the mandatory requirement of a recent streptococcal infection.
- Rule outChoice 3:This cluster relies too heavily on non-specific systemic inflammatory markers that represent minor diagnostic components.
- Rule outChoice 4:Laboratory values like leukocytosis are non-specific minor criteria that cannot replace multiple distinct major physical findings.
Take home points
- A definitive diagnosis of acute rheumatic fever requires evidence of preceding streptococcal infection plus two major criteria, or one major and two minor criteria.
- The five major Jones criteria consist of carditis, migratory polyarthritis, Sydenham chorea, erythema marginatum, and firm subcutaneous nodules.
- Minor diagnostic criteria include clinical findings such as fever and arthralgia, alongside laboratory findings of elevated acute-phase reactants.
- Electrocardiographic identification of a prolonged PR interval serves as a minor cardiac criterion, reflecting transient conduction delays through the atrioventricular node.
An 11-year-old child is admitted with suspected acute rheumatic fever. The nurse notes objective swelling, redness, and severe pain in the left knee, which seems to improve the next day as the right wrist becomes similarly inflamed. How should the nurse document this pattern?
Explanation
Acute rheumatic feverclassically presents with a specific pattern of articular inflammation that targets multiple large joints sequentially. The inflammatory cascadeshifts rapidly between limbs, leaving previously affected joints completely undamaged while causing acute, reversible functional impairment in newly involved anatomical sites.
Rationale for correct answer:
3.Migratory polyarthritisaccurately describes the classic hallmark finding where inflammation resolves in one large joint while simultaneously developing in another. This shifting pattern is a key major Jones criterionthat reflects the systemic, transient nature of the post-streptococcal autoimmune response in connective tissues.
Rationale for incorrect answers:
1.Chronic osteoarthritisis a degenerative joint disease characterized by the progressive, long-term mechanical breakdown of articular cartilage. It is extremely rare in pediatric populations and does not present with an acute, rapidly shifting patternof inflammatory signs.
2.Symmetrical small-joint arthralgiarefers to bilateral pain without objective inflammatory signs occurring in the minor joints of the hands or feet. Rheumatic joint involvement characteristically targets large joints asymmetricly and presents with explicit objective findings like erythema and swelling.
4.Fixed monoarticular synovitisdefines a persistent, non-shifting inflammation confined entirely to a single isolated joint capsule over time. This fixed presentation is typical of septic arthritis or localized juvenile idiopathic arthritisrather than the mobile pattern seen here.
Test-taking strategy:
- Analyze the scenario/question:The question describes an 11-year-old child whose joint inflammation shifts from the left knee to the right wrist within 24 hours, asking for the correct clinical documentation term.
- Evaluate clinical terminology:
- Rule outChoice 1:Degenerative conditions imply chronic wear and tear, not acute, transient, post-infectious inflammatory shifts.
- Rule outChoice 2:The presentation involves clear objective inflammation rather than simple pain, and targets large joints asymmetricly.
- Rule inChoice 3:The rapid movement of objective inflammation from a knee to a wrist perfectly illustrates migratory polyarthritis.
- Rule outChoice 4:The joint involvement is explicitly mobile and involves multiple joints rather than remaining fixed in one location.
Take home points
- Migratory polyarthritis is the most common major manifestation of acute rheumatic fever, affecting the large joints sequentially rather than simultaneously.
- Each involved joint typically remains inflamed for a brief period ranging from a few days to a week before resolving completely without residual deformity.
- The joint inflammation is exquisitely sensitive to anti-inflammatory therapies, particularly salicylates, which can rapidly suppress the joint symptoms.
- Clinical documentation must precisely detail the onset, location, severity, and moving nature of the joint inflammation to support diagnostic tracking.
The nurse is conducting a staff education program on acute rheumatic fever (ARF). According to the Revised Jones Criteria, which combination of findings confirms a diagnosis of primary ARF when combined with evidence of a recent GABHS infection?
Explanation
The diagnostic framework for acute rheumatic feverrequires a strict combination of clinical and laboratory findings to prevent misdiagnosis. Under the Revised Jones Criteria,the presence of an antecedent group A streptococcal infection provides the mandatory etiologic foundation, which must then be accompanied by specific combinations of major and minor cardiovascular and systemicmanifestations.
Rationale for correct answer:
2.Two major criteriaprovide the definitive clinical weight necessary to confirm a primary diagnosis when paired with preceding streptococcal evidence. These major signs reflect high-specificity organ involvement, including rheumatic carditisand Sydenham chorea,which are highly characteristic of this post-infectious autoimmune cascade.
Rationale for incorrect answers:
1.One major and one minor criterionfail to meet the required diagnostic threshold because this combination lacks sufficient clinical specificity. Minor signs like fever or arthralgia are highly non-specific, meaning this paring could easily lead to an incorrect diagnosis of a mimicking condition.
3.Three minor criteria aloneare insufficient to secure a diagnosis of primary acute rheumatic fever regardless of streptococcal status. Without at least one major manifestation demonstrating specific target-organ inflammation, non-specific findings like acute-phase reactantscannot substantiate the diagnosis.
4.Elevated ESR and a prolonged PR intervalrepresent two distinct minor criteria that cannot independently confirm the disease. These two isolated findings merely indicate generalized systemic inflammation and transientatrioventricular delay,which can occur in numerous other pediatric infectious states.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the correct combination of Revised Jones Criteria required to confirm a primary diagnosis of acute rheumatic fever alongside evidence of a recent GABHS infection.
- Apply diagnostic rule thresholds:
- Rule outChoice 1:A single major finding paired with only one minor finding falls short of the validated diagnostic requirement.
- Rule inChoice 2:The presence of two major criteria satisfies the primary diagnostic pathway established by the American Heart Association.
- Rule outChoice 3:Minor criteria represent low-specificity signs that can never independently confirm a diagnosis without major organ involvement.
- Rule outChoice 4:This option pairs two minor criteria, which is diagnostically insufficient and fails to demonstrate primary major organ pathology.
Take home points
- A primary diagnosis of acute rheumatic fever requires either two major criteria, or one major and two minor criteria, plus evidence of GABHS.
- Documenting the preceding streptococcal infection is mandatory except in cases of isolated Sydenham chorea or long-standing insidious carditis.
- Major criteria carry high diagnostic specificity and include carditis, polyarthritis, chorea, erythema marginatum, and subcutaneous nodules.
- Minor criteria reflect systemic inflammation and include fever, polyarthralgia, elevated ESR or C-reactive protein, and prolonged PR interval.
A child diagnosed with ARF exhibits involuntary, aimless, jerky movements of the arms and legs, grimacing, and sudden emotional outbursts. The nurse recognizes this as Sydenham chorea. Which nursing intervention is a priority for this manifestation?
Explanation
Sydenham choreais a delayed neurological manifestation of acute rheumatic fever caused by autoimmune inflammation within the basal ganglia.The resulting involuntary hyperkinetic movements, muscle weakness, and emotional lability compromise the patient's coordination, making the prevention of accidental physical trauma the primary focus of nursing care.
Rationale for correct answer:
3.Implementing environmental safety precautionsis the priority to protect the child from accidental self-injuryduring involuntary movements. Modifying the surroundings by padding side rails, removing sharp objects, and assisting with ambulation directly addresses the neurological deficits without causing physical or psychological stress.
Rationale for incorrect answers:
1.Encouraging the child to sit stillis counterproductive and will worsen the involuntary movements and emotional distress.The purposeless jerking movements are completely involuntary and driven by basal ganglia dysfunction, meaning voluntary suppression is physiologically impossible and trying to do so increases anxiety.
2.Applying mechanical restraintsis strictly contraindicated as forcing immobilization against active, involuntary hyperkinetic movements can cause severe musculoskeletal trauma. Restraining an uncoordinated child increases agitation, exacerbates emotional lability,and elevates the risk of skin breakdown or joint dislocations.
4.Ordering immediate physical therapy for muscle retrainingis inappropriate during the acute, uncoordinated phase of the illness. Sydenham chorea is a transient, self-limiting autoimmune condition that resolves spontaneously over weeks or months, requiringrest and protectionrather than aggressive physical exertion.
Test-taking strategy:
- Analyze the scenario/question:The question describes a child with acute rheumatic fever exhibiting Sydenham chorea and asks the nurse to identify the priority nursing intervention.
- Evaluate safety and feasibility:
- Rule outChoice 1:Involuntary movements cannot be controlled through willpower, and demanding stillness increases stress and choreic activity.
- Rule outChoice 2:Restraints cause resistance against involuntary muscle contractions, directly increasing the risk of physical injury.
- Rule inChoice 3:Proactive environmental modifications keep the patient safe while allowing the self-limiting neurological process to run its course.
- Rule outChoice 4:Active muscle retraining is ineffective during acute central nervous system inflammation and does not address immediate safety needs.
Take home points
- Sydenham chorea is a major Jones criterion that manifests weeks to months after a streptococcal infection due to cross-reactive antibodies targeting the basal ganglia.
- Clinical features include involuntary choreiform movements, facial grimacing, hypotonia, deterioration in fine motor skills, and transient behavioral changes.
- The condition is completely reversible and self-limiting, though symptoms can persist for several months before resolving fully without permanent deficits.
- Nursing care focuses on creating a calm, low-stimulus environment, providing emotional support for outbursts, and implementing strict seizure-like safety precautions.
The nurse is reviewing laboratory results for a client suspected of having ARF. Which diagnostic result serves as the required evidence of a preceding streptococcal infection?
Explanation
An acute rheumatic fever diagnosiscannot be clinically validated without definitive objective confirmation of a prior group A streptococcal exposure. Because the active upper respiratory tract infection has typically cleared by the time systemic autoimmune symptoms appear, doctors rely on specificserological biomarkersto confirm that the patient experienced a recent bacterial infection.
Rationale for correct answer:
2.An elevated anti-streptolysin O titerserves as the definitive diagnostic evidence proving a preceding group A streptococcal infection.This assay measures circulating antibodies directed against streptolysin O, a toxic exotoxin secreted by the bacteria, providing the required etiologic link under the Jones criteria.
Rationale for incorrect answers:
1.An elevated C-reactive proteinis a non-specific acute-phase reactant that indicates systemic inflammation but cannot identify a specific infectious agent. It is classified as a minor diagnostic criterion that tracks disease activity rather than confirming the mandatory streptococcal etiology.
3.A prolonged PR intervalon an electrocardiogram represents a minor cardiac criterion indicating a transient delay in atrioventricular conduction.While it reflects active rheumatic myocardial inflammation, it is not an infectious biomarker and can occur in many non-streptococcal conditions.
4.Leukocytosis with a left shiftindicates an active immunologic response characterized by an increased proportion of immature neutrophilic bands. This finding represents a generalized response to any acute bacterial process or stressor and lacks the specificity needed to confirm a streptococcal infection.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the specific diagnostic result that satisfies the mandatory requirement of proving a preceding streptococcal infection in a patient suspected of having acute rheumatic fever.
- Differentiate specificity from inflammation:
- Rule outChoice 1:This laboratory value measures generalized inflammation and is categorized as a minor diagnostic criterion.
- Rule inChoice 2:This specific antibody titer provides direct, objective evidence of a host immune response to a recent streptococcal exposure.
- Rule outChoice 3:This electrocardiographic finding demonstrates cardiac conduction delays rather than proving an underlying infectious etiology.
- Rule outChoice 4:General elevations in white blood cell counts occur across numerous infectious states and lack etiology-specific diagnostic weight.
Take home points
- Confirming a preceding group A streptococcal infection is a mandatory element of the Jones criteria required to diagnose acute rheumatic fever.
- Antistreptolysin O titers peak approximately 3 to 5 weeks after the initial pharyngeal infection, coinciding perfectly with the onset of rheumatic symptoms.
- A single elevated titer or a rising serial titer over time provides valid diagnostic evidence of the antecedent bacterial exposure.
- In cases where the anti-streptolysin O titer is normal, an anti-DNase B titer may be ordered to check for past streptococcal exposure.
Practice Excercise 3
The nurse is educating caregivers about the early recognition of streptococcal throat infections. What is the most important role of the nurse in preventing rheumatic fever?
Explanation
The primary prevention of acute rheumatic feverrelies entirely on the timely eradication of the primary pharyngeal pathogenbefore the autoimmune cascade can initiate. Nurses serve as critical public health advocates by recognizing clinical indicators of upper respiratory infections and ensuring adherence to validated antimicrobials, which prevents the development of cross-reactive anti-streptococcal antibodies.
Rationale for correct answer:
4.Promoting early diagnosis and immediate treatment of group A streptococcal pharyngitisis the most important intervention to eliminate the bacterial trigger.Administering a full course of penicillin within 9 days of symptom onset achieves complete bacterial eradication, preventing the post-infectious inflammatory response entirely.
Rationale for incorrect answers:
1.Teaching patients with infective endocarditis to adhere to antibiotic prophylaxisfocuses on preventing endovascular infection recurrence rather than primary rheumatic fever. While both conditions involve cardiac valves, endocarditis is an active bacteremic seeding process with distinct pathophysiological mechanisms and prevention guidelines.
2.Identifying patients with existing valvular heart diseaseaddresses secondary prevention or tracking of chronic complications rather than stopping disease onset. While these patients require aggressive monitoring to prevent recurrent episodes, primary prevention focuses on stopping the initial development of valvular damage.
3.Encouraging the use of antibiotics for all infectionsinvolving a sore throat promotes inappropriate antimicrobial utilization and acceleratesbacterial resistance. The majority of pharyngitis cases in pediatric populations are viral in origin, meaning antibiotics are indicated only after confirming a streptococcal etiology.
Test-taking strategy:
- Analyze the scenario/question:The question asks for the nurse's most important role in preventing the development of acute rheumatic fever when educating caregivers.
- Evaluate preventive tiers:
- Rule outChoice 1:This addresses infective endocarditis management, which represents a separate cardiac infectious process.
- Rule outChoice 2:This focuses on secondary tracking of existing damage rather than primary prevention of the underlying disease.
- Rule outChoice 3:Broad antibiotic use for all sore throats violates stewardship principles since most upper respiratory tract infections are viral.
- Rule inChoice 4:Targeted, timely eradication of confirmed group A streptococcal pharyngitis is the absolute gold standard for primary prevention.
Take home points
- Primary prevention of rheumatic fever is achieved only by diagnosing and treating group A streptococcal pharyngitis effectively with appropriate antibiotics.
- Antimicrobial therapy must be initiated within 9 days of the onset of pharyngeal symptoms to successfully block the subsequent autoimmune response.
- Viral pharyngitis presents with cough, rhinorrhea, and hoarseness, and must be differentiated from streptococcal infections to avoid unnecessary antibiotic use.
- Complete adherence to the entire prescribed course of antibiotics is essential to ensure total eradication of the rheumatogenic bacterial strains.
The nurse is caring for a 10-year-old client with acute rheumatic fever. Which is a priority nursing intervention for a client during the acute phase of this disease?
Explanation
The acute phase of acute rheumatic feverdemands immediate pharmacological intervention to eradicate any residual bacterial reservoir and suppress systemic inflammation. Eliminating the primary pathogen stops the ongoing production of rheumatogenic antigens, halting the progression of the autoimmune cascadethat targets cardiac, articular, and neurological tissues.
Rationale for correct answer:
1.Administration of antibiotics as orderedis the priority intervention to achieve completebacterial eradicationwithin the pharynx. Even if the active pharyngitis has clinically resolved, eliminating residual group A streptococci is essential to terminate the antigenic stimulus driving the destructive inflammatory response.
Rationale for incorrect answers:
2.Management of pain with opioid analgesicsis inappropriate because the intense joint pain responds dramatically to standard anti-inflammatory agents.High-dose salicylates or nonsteroidal anti-inflammatory drugs are the first-line therapies used to manage arthralgia, making heavy central nervous system depressants unnecessary.
3.Encouraging fluid intake for hydrationis a supportive measure but can be hazardous if the client has developed severe rheumatic carditis.Fluid overload risks precipitating acute congestive heart failure in a heart compromised by pancarditis, meaning fluid balance must be monitored with extreme caution.
4.Performance of frequent active range-of-motion exercisesis strictly contraindicated due to the severe pain and inflammation affecting the joints and heart. The acute phase requires strict bed rest to minimize myocardial workload and reduce metabolic demands on a compromised myocardium.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the priority nursing intervention for a 10-year-old client during the acute phase of acute rheumatic fever.
- Evaluate safety and hierarchy of needs:
- Rule inChoice 1:Eliminating the underlying infectious trigger is the definitive initial step to stop the progressive autoimmune destruction.
- Rule outChoice 2:Rheumatic joint pain is highly responsive to salicylates and nonsteroidal anti-inflammatory drugs rather than narcotic options.
- Rule outChoice 3:Aggressive fluid loading poses a significant fluid overload risk if active carditis has weakened the patient's myocardial function.
- Rule outChoice 4:Active joint exercises worsen severe migratory arthritis and unsafely increase metabolic strain on an inflamed heart.
Take home points
- Antibiotic therapy with penicillin remains the immediate priority during the acute phase to eliminate any remaining group A streptococcal organisms.
- Strict bed rest is enforced during the acute phase of carditis to reduce cardiac workload and minimize permanent structural valvular damage.
- High-dose aspirin or nonsteroidal anti-inflammatory drugs are utilized for rapid, effective management of severe migratory polyarthritis symptoms.
- Cardiovascular assessment, including frequent monitoring of heart rates, sounds, and fluid balances, is critical to detect early signs of heart failure.
The nurse is discharging a 10-year-old child who was treated for ARF without carditis. Which statement by the parent indicates a correct understanding of the secondary prevention plan?
Explanation
Secondary prevention of acute rheumatic feveris a critical public health strategy aimed at preventing recurrent group A streptococcal infections. Because each recurrence increases the risk and severity of permanent valvular damage,long-term continuous antimicrobial prophylaxis is mandated for all individuals with a documented history of the disease, with the duration determined by the presence and severity of cardiac involvement.
Rationale for correct answer:
2.Returning every 3 to 4 weeks for a penicillin injection for at least 5 years or until turning 21represents the exact standard guideline for a child without rheumatic carditis. Intramuscular penicillin G benzathine provides continuous, reliable serum levels that shield the patient from recurrent subclinical infections.
Rationale for incorrect answers:
1.Administering antibiotics only when the child develops another sore throatdescribes an outdated primary prevention approach rather than the required continuous secondary prophylaxis.Recurrent infections can be asymptomatic or subclinical but still trigger an autoimmune reactivation, making intermittent therapy completely ineffective.
3.Believing the child is completely cured and requires no further medication after a standard 10-day coursereflects a hazardous misunderstanding of disease recurrence. The initial 10-day regimen merely eradicates the primary triggering infection, but it leaves the patient immunologically primed for severe recurrent attacks if exposed again.
4.Taking aspirin daily until adulthoodis inappropriate because salicylates are utilized only during the acute inflammatory phase to manage migratory arthritis.Long-term maintenance therapy relies strictly on antimicrobial regimens to prevent infection rather than chronic anti-inflammatory suppression, which carries significant toxic risks.
Test-taking strategy:
- Analyze the scenario/question:The question describes a 10-year-old child being discharged after treatment for acute rheumatic fever without carditis, asking for the statement that confirms correct understanding of secondary prophylaxis.
- Apply professional guidelines:
- Rule outChoice 1:Intermittent treatment fails to protect against asymptomatic streptococcal exposures that can cause severe rheumatic recurrences.
- Rule inChoice 2:This statement precisely matches the American Heart Association criteria for secondary prevention duration in patients without carditis.
- Rule outChoice 3:Stopping all treatment after 10 days leaves the child highly vulnerable to recurrent episodes and progressive heart damage.
- Rule outChoice 4:Chronic aspirin therapy is not indicated for secondary prophylaxis and increases the risk of bleeding and Reye syndrome.
Take home points
- Secondary prevention guidelines mandate continuous antibiotic prophylaxis for patients with a history of acute rheumatic fever to prevent recurrent attacks.
- For individuals who experienced rheumatic fever without carditis, prophylaxis must continue for 5 years or until age 21, whichever period is longer.
- Intramuscular injection of penicillin G benzathine every 3 to 4 weeks is the most effective and preferred method of secondary prophylaxis.
- Oral penicillin V or sulfadiazine daily can be utilized as alternative secondary preventive regimens for patients who refuse or cannot tolerate injections.
The nurse is conducting a staff education program on chronic rheumatic heart disease. Which cardiac valve is most vulnerable to permanent structural damage and scarring as a complication of this disease?
Explanation
Chronic rheumatic heart diseaseis characterized by permanent structural alterations within the endocardium resulting from repetitive, severe autoimmune inflammation. High hemodynamic stressacross the left-sided chambers accelerates tissue scarring, leading to classic chordae tendineae shortening, leaflet thickening, and commissural fusion that permanently alters valvular function.
Rationale for correct answer:
3.The mitral valveis the most vulnerable structure because it experiences the highest mechanical closure pressures within the left side of the heart.This persistent hemodynamic workload exacerbates the immune-mediated valvulitis, making it the primary site for permanent valvular stenosis and chronic regurgitation.
Rationale for incorrect answers:
1.The tricuspid valveis a low-pressure structure located on the right side of the heart that is rarely damaged by chronic rheumatic carditis. Right-sided valvular involvement typically occurs only as a late, secondary complication in the context of severe, multi-valvular pancarditis.
2.The pulmonic valveis the least likely cardiac structure to sustain permanent scarring or calcification from this post-streptococcal disease process. Low right-sided ventricular pressures shield the pulmonic leaflets from the heavy mechanical deformation needed to accelerate chronic fibrotic remodeling.
4.The aortic valveis the second most frequently affected structure, but it is less commonly deformed in isolation than the upstream left-sided gateway. Although aortic insufficiency often coexists with mitral disease, it is rarely the exclusive or primary site of chronic post-rheumatic fibrous scarring.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify which of the four human cardiac valves is most frequently and severely damaged by chronic rheumatic heart disease.
- Evaluate hemodynamic pressures:
- Rule outChoice 1:Low-pressure right-sided heart structures are mechanically protected from significant post-inflammatory fibrotic scarring.
- Rule outChoice 2:The pulmonic gateway operates under minimal mechanical strain and is rarely affected by chronic rheumatic sequelae.
- Rule inChoice 3:The mitral gateway bears the highest closing stress in the left ventricle, making it the single most common site of structural injury.
- Rule outChoice 4:The aortic structure is frequently involved, but it ranks strictly second behind the mitral valve in clinical frequency and severity.
Take home points
- Chronic rheumatic heart disease is the leading cause of acquired mitral stenosis in pediatric and young adult populations worldwide.
- Pathological changes include fibrous thickening of the valve leaflets, fusion of the baseline commissures, and calcification over multiple decades.
- Chronic valvular stenosis restricts left atrial emptying, elevating pulmonary pressures and potentially inducing right-sided heart failure over time.
- Prophylactic adherence to secondary antibiotics is vital to stop recurrent inflammatory episodes that cause cumulative, irreversible valvular damage.
A child with severe rheumatic carditis is prescribed prednisone. The nurse understands that corticosteroids are added to the therapeutic regimen for which primary purpose?
Explanation
Corticosteroidsare reserved for patients with severe rheumatic carditis,particularly those presenting with cardiomegaly, pericarditis, or active congestive heart failure. These agents exert powerful anti-inflammatory effects that target the endocardium, myocardium, and pericardium, rapidly stabilizing themyocardial functionand limiting the progression of permanent structural scarring.
Rationale for correct answer:
2.Rapidly suppressing severe myocardial inflammationis crucial to reduce the risk of acute cardiac failure and minimize permanent valvular integrity loss.Prednisone suppresses the intense, destructive immune response directed at cardiac structures during the life-threatening phase of acute pancarditis.
Rationale for incorrect answers:
1.Eradicating remaining streptococcal colonies in the bloodstreamrequires targeted antimicrobial agentssuch as penicillin rather than systemic corticosteroids. Prednisone has zero antimicrobial properties and acts exclusively as an immunosuppressant, which temporarily reduces the host immune response.
3.Alleviating the choreiform movements of Sydenham choreais not the primary purpose for adding prednisone to this specific client's carditis regimen. While severe, debilitating chorea can sometimes respond to immunomodulatory therapy, the presence of severe carditis is the definitive life-saving indication here.
4.Acting as an analgesic for severe migratory polyarthritisis incorrect because joint inflammation is managed effectively using standard high-dose salicylates.Aspirin or nonsteroidal anti-inflammatory drugs are the first-line therapies for joint symptoms, making corticosteroids unnecessary for uncomplicated arthritis.
Test-taking strategy:
- Analyze the scenario/question:The question describes a child with severe rheumatic carditis prescribed prednisone and asks for the primary purpose of this corticosteroid therapy.
- Prioritize life-threatening manifestations:
- Rule outChoice 1:Antibiotics are required for bacterial eradication; steroids do not have bactericidal or bacteriostatic capabilities.
- Rule inChoice 2:Severe carditis threatens immediate cardiac output and long-term valvular health, making rapid anti-inflammatory suppression the priority.
- Rule outChoice 3:Chorea is a self-limiting neurological complication; severe carditis is a far more critical, high-acuity therapeutic target.
- Rule outChoice 4:Joint pain and swelling respond beautifully to salicylates, meaning steroids are never indicated for isolated arthritis.
Take home points
- Corticosteroids are indicated in acute rheumatic fever only when severe carditis is present, especially if it leads to congestive heart failure.
- Prednisone acts by inhibiting inflammatory cytokine production, decreasing capillary permeability, and preventing progressive granulomatous lesion formation.
- Nursing care during systemic steroid therapy must include frequent monitoring for hypertension, hyperglycemia, electrolyte imbalances, and increased infection risk.
- Abrupt withdrawal of corticosteroids can cause a rebound of rheumatic symptoms, necessitating a gradual, closely monitored tapering schedule.
A school nurse is teaching parents about primary prevention of acute rheumatic fever. Which message is most critical to convey?
Explanation
The primary prevention of acute rheumatic feverdepends entirely on the complete eradication of the underlying pharyngeal bacterial reservoirbefore the host immune system initiates a post-infectious autoimmune response. Incomplete antibiotic therapy allows surviving bacteria to propagate, extending the antigenic stimulation that drives the production of cross-reactive anti-streptococcal antibodies.
Rationale for correct answer:
2.Completing the entire prescribed course of antibioticsis the most critical public health instruction to achieve complete bacterial eradication.Eliminating group A streptococci completely from the upper respiratory tract prevents the initiation of the molecular mimicry cascade that damages cardiac valves.
Rationale for incorrect answers:
1.Avoiding playing in the mudto prevent superficial cutaneous pyodermas will not reduce the incidence of acute rheumatic fever. Although skin infections like impetigo can lead to post-streptococcal glomerulonephritis, only pharyngeal infections are rheumatogenic and capable of causing carditis.
3.Administering aspirinimmediately to any child who develops a high fever is dangerous and strictly contraindicated in pediatric populations due to Reye syndrome.Salicylates are reserved for confirmed inflammatory conditions like rheumatic arthritis and should never be given empirically for simple undifferentiated fevers.
4.Stating that a throat culture is unnecessary based on viral symptomsdoes not represent a safe primary prevention message regarding disease detection. While a runny nose and cough suggest a viral etiology, healthcare providers must perform objective screening whenever streptococcal pharyngitis cannot be definitively ruled out.
Test-taking strategy:
- Analyze the scenario/question:The question asks the school nurse for the most critical primary prevention message to convey to parents to prevent the development of acute rheumatic fever.
- Evaluate primary prevention thresholds:
- Rule outChoice 1:Skin infections do not trigger the specific cross-reactive autoimmune pathways that cause rheumatic heart disease.
- Rule inChoice 2:Complete antibiotic compliance is the absolute gold standard required to prevent the post-streptococcal autoimmune cascade.
- Rule outChoice 3:Empiric aspirin use for pediatric fevers is highly dangerous due to its known association with fatal Reye syndrome.
- Rule outChoice 4:This statement focuses on ruling out testing rather than proactively guiding parents on how to prevent the disease.
Take home points
- Primary prevention of rheumatic fever requires a full 10-day course of oral penicillin or amoxicillin to ensure total eradication of the bacteria.
- Parents must be educated to continue administering antibiotics even after the child's acute sore throat and fever symptoms resolve completely.
- Group A beta-hemolytic streptococcus is transmitted readily via respiratory droplets in crowded environments like schools and childcare centers.
- Eradication of the pharyngeal infection is highly effective at preventing rheumatic fever if initiated within 9 days of symptom onset.
Comprehensive Questions
A 6-year-old client is diagnosed with rheumatic heart disease and the parent questions the nurse following the doctor’s statement that the child has a heart murmur. The nurse explains that a heart murmur is an abnormal or extra heart sound produced by which malfunctioning structure of the heart?
Explanation
A heart murmurrepresents an acoustic manifestation of turbulent blood flow within the cardiovascular system,most frequently caused by structural alterations of the endocardium. In post-streptococcal disease, chronic inflammation induces scarring, commissural fusion, and leaflet deformation, which permanently compromisesvalvular functionand disrupts the normal laminar flow of blood through the cardiac chambers.
Rationale for correct answer:
1.A heart murmur is an abnormal sound produced directly by a malfunctioning heart valve that fails to open or close properly.Rheumatic endocarditis creates structural abnormalities like mitral stenosis or regurgitation, which forces blood through narrowed orifices or backward through leaking leaflets, generating audible turbulence.
Rationale for incorrect answers:
2.A malfunctioning major heart vesselcan produce abnormal sounds like bruits or continuous murmurs in conditions like patent ductus arteriosus, but it is not the primary site of rheumatic scarring.The structural damage characteristic of rheumatic heart disease is located within the intracardiac endocardial architecture.
3.A malfunctioning heart chambercan experience hypertrophy or dilation as a secondary hemodynamic consequence of valvular disease, but the chamber wall itself does not generate a heart murmur. The chamber changes represent long-term structural remodeling rather than the primary mechanism of acoustic flow turbulence.
4.A malfunctioning heart conduction systemresults in dysrhythmias, heart blocks, or a prolonged PR interval due to inflammatory delays in the atrioventricular node. These electrical impairments alter the rhythm and rate of cardiac contractions but do not directly create structural, turbulent fluid murmurs.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the specific anatomical structure of the heart responsible for producing a heart murmur in a 6-year-old client with rheumatic heart disease.
- Correlate pathophysiology with acoustics:
- Rule inChoice 1:Murmurs are the definitive clinical acoustic sign of turbulent blood flow caused by stenotic or regurgitant valvular leaflets.
- Rule outChoice 2:Large blood vessels can cause specialized extra-cardiac sounds, but they are not the primary target of chronic rheumatic endocarditis.
- Rule outChoice 3:Ventricular or atrial chambers reshape in response to workload shifts but are not the source of the audible murmur sound.
- Rule outChoice 4:Conduction abnormalities cause electrical rate or rhythm defects, which are distinct from mechanical fluid turbulence.
Take home points
- A heart murmur is the classic clinical sign of rheumatic endocarditis, reflecting turbulent blood flow through damaged, scarred cardiac valves.
- The mitral valve is the most frequently affected structure in pediatric rheumatic heart disease, often presenting initially as acute mitral regurgitation.
- Regurgitant murmurs occur when damaged leaflets fail to close completely, allowing blood to flow backward into a chamber during systole or diastole.
- Stenotic murmurs are generated when progressive fibrous tissue scarring and calcification narrow the valve orifice, restricting normal forward blood flow.
A nurse is preparing to discharge a 10-year-old male client who is hospitalized with the diagnosis of rheumatic fever. The nurse’s priority during the client’s discharge teaching should be:
Explanation
The primary goal of discharge managementfollowing acute rheumatic fever is the absolute prevention of recurrent group A streptococcal infections.Because the immune system remains permanently primed against host tissues, any subsequent streptococcal exposure can trigger a severe secondary autoimmune response, exponentially increasing the risk of permanentvalvular destructionand chronic heart failure.
Rationale for correct answer:
4.Emphasizing the need for long-term prophylactic antibiotic therapyis the absolute priority to prevent cumulative, permanent cardiac damage.Compliance with continuous, regular penicillin regimens represents the single most effective intervention to safeguard the child's long-term cardiovascular health and survival.
Rationale for incorrect answers:
1.Providing an avenue for verbalization of feelings regarding illnessis a valuable psychosocial intervention that addresses the client's emotional adjustment. Although essential for holistic pediatric nursing care, it represents a lower-tier priority compared to life-saving, infection-preventing medical therapies.
2.Providing adequate and appropriate pain medicationsis less critical at discharge because joint inflammation typically resolves completely during the acute phase. Migratory polyarthritis responds rapidly to early salicylate regimens, meaning ongoing severe pain is rarely a primary issue at the time of discharge.
3.Ensuring awareness of activity restrictions and complianceis important if the child experienced active carditis, but it represents a secondary focus.Restricting physical exertion minimizes immediate myocardial workload, but it cannot prevent the devastating long-term structural recurrences caused by new streptococcal infections.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the highest priority discharge teaching point for a 10-year-old male client hospitalized with acute rheumatic fever.
- Apply prioritization frameworks:
- Rule outChoice 1:Psychosocial needs are important for emotional well-being but rank below physiological safety and life-prolonging interventions.
- Rule outChoice 2:Joint pain is transient and highly responsive to early acute treatments, making chronic pain management a lower priority at discharge.
- Rule outChoice 3:Activity restriction protects an actively inflamed heart, but it does not prevent the primary threat of disease recurrence.
- Rule inChoice 4:Continuous secondary antibiotic prophylaxis directly prevents recurrent streptococcal infections, making it the most critical, life-saving instruction.
Take home points
- Adherence to secondary antibiotic prophylaxis is the single most critical intervention to prevent recurrent episodes of acute rheumatic fever.
- Recurrent episodes of the disease cause cumulative, irreversible scarring of the endocardium, most frequently targeting the mitral valve leaflets.
- Prophylaxis must be maintained continuously for a minimum of 5 years or until age 21 for patients who did not experience carditis.
- The preferred method of prevention is an intramuscular injection of long-acting penicillin G benzathine administered every 3 to 4 weeks.
An 11-year-old client has a diagnosis of rheumatic fever and has missed school for a week. What is the most likely cause of this problem?
Explanation
Acute rheumatic feverdevelops exclusively as a delayed, non-suppurative inflammatory complication following an upper respiratory infection. The host immune response generates cross-reactive antibodies that target self-antigens within theconnective tissues,leading to systemic manifestations such as carditis, chorea, and polyarthritisthat cause significant pediatric illness and school absenteeism.
Rationale for correct answer:
1.A previous streptococcal throat infectionis the mandatory triggering event that initiates the autoimmune cascadeleading to rheumatic fever. Inadequate eradication of group A beta-hemolytic streptococcus allows for molecular mimicry to occur, producing systemic symptoms that cause the child to miss school.
Rationale for incorrect answers:
2.A history of open heart surgery at 5 years of ageindicates a pre-existing structural anomaly but is not the etiologic trigger for this acute inflammatory condition. Rheumatic fever is an acquired, post-infectious autoimmune disease rather than a late-stage mechanical complication of congenital heart surgery.
3.Playing too much soccer and not getting enough restrepresents physical overexertion, which causes transient fatigue or simple muscular strains rather than systemic autoimmunity. While physical exertion must be restricted during active carditis, lifestyle exhaustion never acts as the primary cause of this disease.
4.Exposure to a sibling with pneumoniainvolves distinct respiratory pathogens like Streptococcus pneumoniae or viruses, which do not express rheumatogenic M proteins. Only pharyngeal infections caused by group A Streptococcus can induce the specific cross-reactive antibodies required to precipitate this disease.
Test-taking strategy:
- Analyze the scenario/question:The question notes an 11-year-old client diagnosed with rheumatic fever who has missed school for a week, asking for the most likely cause of this underlying problem.
- Identify the mandatory etiology:
- Rule inChoice 1:Acute rheumatic fever requires a preceding group A streptococcal pharyngitis infection as its absolute, mandatory causative event.
- Rule outChoice 2:Prior surgical histories point toward congenital or anatomical corrections rather than the acquisition of a post-infectious autoimmune disorder.
- Rule outChoice 3:Lifestyle factors and lack of sleep can lower generalized immunity but never independently generate specific cross-reactive autoantibodies.
- Rule outChoice 4:Other respiratory infections like pneumonia do not share the specific antigenic structure necessary to trigger the rheumatic cascade.
Take home points
- Acute rheumatic fever is caused exclusively by an untreated or inadequately treated pharyngeal infection with group A beta-hemolytic streptococcus.
- Clinical manifestations like migratory polyarthritis and Sydenham chorea cause acute physical impairments that lead to significant school absenteeism.
- The systemic inflammatory response typically manifests after a latent period spanning 2 to 3 weeks following the initial sore throat.
- Skin infections caused by the same bacteria, such as impetigo, do not trigger the autoimmune pathways responsible for causing rheumatic fever.
A toddler has been diagnosed with streptococcal pharyngitis. When explaining to caregivers the importance of finishing the full course of oral antibiotic therapy, the nurse should include which potential complications of inadequately treated streptococcal infection? Select all that apply
Explanation
Infection with Streptococcus pyogenescan lead to suppurative and non-suppurative complications via direct bacterial extension or immune-mediated mechanisms.Inadequate eradication triggers local tissue destruction, presenting with fever, exudates, and widespread systemic inflammatory sequelae.
Rationale for correct answers:
1.Otitis mediarepresents a common suppurative complication. The pathogen spreads directly through the eustachian tube into the middle ear cavity.This localized bacterial invasion causes severe otalgia. It presents with fever and distinct tympanic membrane erythema.
4.Acute rheumatic feveris a critical non-suppurative complication. It arises from a delayed autoimmune response following pharyngeal infection. Cross-reactive antibodies target host tissues through molecular mimicry.This cascade triggers severe systemic pancarditis and permanent valvular damage.
5.Glomerulonephritisis a classic post-infectious non-suppurative complication. Circulating antigen-antibody aggregates deposit inside the glomerular basement membrane, activating complement pathways. This inflammatory injury disrupts renal filtration. It induces sudden hematuria, oliguria, and acute nephritic syndrome.
Rationale for incorrect answers:
2.Diabetes insipidusis a neuroendocrine disorder. It involves a deficiency of or resistance to antidiuretic hormone. This condition stems from central hypothalamus trauma or genetic defects rather than bacterial pharyngitis. It produces severe polyuria, completely unrelated to post-streptococcal autoimmune sequelae.
3.Nephrotic syndromeis a distinct glomerular disorder. It is characterized by massive proteinuria and generalized edema. Streptococcal infections trigger acute nephritic conditions rather than primary nephrotic pathology. The structural podocyte injuries involve entirely separate, non-streptococcal immunological mechanisms.
Test-taking strategy:
- Analyze the scenario/question:The question requires the nurse to identify the potential suppurativeand non-suppurativecomplications resulting from an inadequately treated group A streptococcal pharyngitis infection in a toddler.
- Evaluate clinical pathophysiology:
- Rule inChoice 1:Otitis media is a classic complication caused by local bacterial migration.
- Rule outChoice 2:Diabetes insipidus involves antidiuretic hormone pathology, which lacks any infectious link.
- Rule outChoice 3:Streptococcal sequelae cause acute nephritic manifestations, not classic primary nephrotic conditions.
- Select Choice 4:Acute rheumatic fever is a major complication prevented by completing antibiotic therapy.
- Rule inChoice 5:Glomerulonephritis is a well-documented immune-complex renal complication of this bacterial infection.
Take home points
- Group A streptococcal infections can cause suppurative complications like otitis media and peritonsillar abscesses through direct regional tissue invasion.
- Acute rheumatic fever is a non-suppurative sequela that damages cardiac valves and is entirely preventable with timely antibiotic administration.
- Post-streptococcal glomerulonephritis is an immune-complex mediated kidney injury that presents with hematuria, hypertension, and periorbital edema.
- Compliance with the full 10-day course of prescribed oral antibiotics is mandatory to ensure complete eradication of the bacteria.
A school-aged client admitted with a diagnosis of “Rule out rheumatic fever” has all of the following laboratory findings. Which finding supports the diagnosis of rheumatic fever?
Explanation
An acute rheumatic fever diagnosisrequires objective verification of a preceding group A beta-hemolytic streptococcal infection.Because the acute upper respiratory tract symptoms have typically resolved by the time systemic autoimmune manifestations surface, clinicians rely on specific serological antibody markersto confirm the mandatory antecedent exposure.
Rationale for correct answer:
1.An elevated antistreptolysin-O titerprovides the definitive diagnostic evidence proving a recent group A streptococcal infection.This laboratory assay measures circulating antibodies directed against streptolysin O, a cytolytic exotoxin secreted by the bacteria, satisfying the essential etiologic requirement under the Jones criteria.
Rationale for incorrect answers:
2.An elevated hematocritindicates hemoconcentration,which is typically secondary to dehydration rather than active rheumatic inflammation. Rheumatic fever is more commonly associated with mild to moderate anemia of chronic disease, driven by systemic inflammatory suppression of erythropoiesis.
3.Negative blood culturessimply rule out an active endovascular or systemic bacterial infection like septicaemia or infective endocarditis. Rheumatic fever is a sterile, post-infectious autoimmune complication, meaning live bacteria are not circulating in the bloodstream during the disease process.
4.A white blood cell count within the normal rangerepresents a neutral finding that does not actively support a diagnosis of active rheumatic fever. The acute phase of this systemic inflammatory disease is characteristically accompanied by leukocytosis, mirroring the active host immune cascade.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to select the specific laboratory finding that actively supports a diagnosis of acute rheumatic fever in a child admitted to "Rule out" the condition.
- Correlate etiology with serology:
- Rule inChoice 1:The ASO titer measures the specific host antibody response to the mandatory triggering pathogen, making it essential for diagnostic confirmation.
- Rule outChoice 2:Elevated hematocrit values reflect fluid balance alterations rather than post-streptococcal inflammatory cascades.
- Rule outChoice 3:Negative blood cultures are helpful to exclude active bacteremia, but they serve as a baseline rule-out test rather than positive diagnostic proof of ARF.
- Rule outChoice 4:Normal leukocyte ranges lack the expected indicators of an active, high-acuity systemic inflammatory process.
Take home points
- Confirming a preceding group A streptococcal exposure using serological antibody testing is a mandatory component of the Revised Jones Criteria.
- Antistreptolysin-O titers begin rising 1 week after the initial pharyngitis, peak at 3 to 5 weeks, and can remain elevated for several months.
- If the initial ASO titer returns within normal limits, alternative assays such as anti-DNase B testing should be utilized to investigate past streptococcal exposure.
- Systemic acute-phase reactants, including an elevated erythrocyte sedimentation rate and C-reactive protein, serve as supporting minor diagnostic criteria.
A pediatric client with rheumatic fever is admitted to the nursing unit. The nurse should prioritize which nursing intervention as most important at this time?
Explanation
Acute rheumatic feverleads to widespread connective tissue inflammation,characteristically presenting with migratory polyarthritisthat targets the large joints. The severe joint pain and swelling during this acute phase are debilitating for a pediatric client, making the rapid optimization of physical comfort and pain control a primary focal point of immediate nursing care.
Rationale for correct answer:
2.Providing comfort measures for arthralgiais the immediate priority during the initial admission phase. Implementing gentle handling, supporting inflamed joints with proper alignment, and administering prescribed high-dosesalicylates or NSAIDsdirectly addresses the child's acute pain and reduces the physiological stress associated with intense inflammatory arthritis.
Rationale for incorrect answers:
1.Preventing the spread of rheumatic feveris an incorrect nursing goal because the disease itself is a non-communicable, post-infectious autoimmune response.While the preceding group A streptococcal pharyngitis is highly contagious, the subsequent systemic rheumatic inflammatory cascade cannot be transmitted from person to person.
3.Evaluating for nervous system complicationsis an essential element of ongoing clinical tracking but represents a lower immediate priority compared to acute pain management. Sydenham chorea typically manifests as a delayed sign weeks or months after the initial infection, presenting as gradual uncoordination rather than a sudden life-threatening emergency.
4.Teaching parents about cardiopulmonary resuscitationis an important discharge intervention for children with permanent, severe valvular damage, but it is premature upon initial admission. The immediate focus during the acute, high-acuity phase must remain centered on active symptom stabilization and patient comfort.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the highest priority nursing intervention for a pediatric client with acute rheumatic fever immediately upon admission to the nursing unit.
- Assess high-acuity physiological needs:
- Rule outChoice 1:This choice relies on misinformation; rheumatic fever is an autoimmune phenomenon and is not a transmissible disease.
- Rule inChoice 2:Managing acute, debilitating inflammatory joint pain directly fulfills immediate comfort and physiological stabilization needs during early admission.
- Rule outChoice 3:Neurological manifestations like chorea are typically delayed and self-limiting, making active pain management a higher initial priority.
- Rule outChoice 4:CPR education is a long-term safety intervention appropriate for discharge planning rather than the initial acute stabilization phase.
Take home points
- Migratory polyarthritis is a major Jones criterion that causes severe, agonizing pain in large joints such as the knees, ankles, elbows, and wrists.
- The joint inflammation is typically transient and does not cause permanent orthopedic deformities, resolving rapidly once appropriate therapy begins.
- High-dose aspirin or nonsteroidal anti-inflammatory drugs are highly effective, providing dramatic relief from joint pain within 24 to 48 hours.
- Nursing comfort measures include keeping the weight of bed linens off inflamed joints, maintaining strict bed rest, and avoiding unnecessary joint manipulation.
An adolescent is admitted with a diagnosis of “Rule out rheumatic fever.” Based on Jones criteria, for which findings should the nurse assess?
Explanation
The diagnosis of acute rheumatic fever (ARF)relies on the Revised Jones Criteria,which categorizes clinical and laboratory findings into major and minor criteria. To confirm a primary diagnosis, the patient must meet either two major criteriaOR one major and two minor criteria,plus verified diagnostic evidence of a preceding group A streptococcal infection.
Rationale for correct answer:
4.Assessing for erythema, specifically erythema marginatum, a major criterion, polyarthritis,a major criterion), and an elevated ASO titer, the required evidence of a preceding streptococcal infection aligns perfectly with the diagnostic frameworks of the Jones Criteria.
Rationale for incorrect answers:
1.Dental cariesare entirely unrelated to the pathogenesis of rheumatic fever. While oral health is an important indicator of general pediatric health, it carries no diagnostic weight within the Jones framework.
2.Fever is a valid minor criterion,but headache and a low red blood cell count(anemia) are generalized, non-specific constitutional findings that are not formal diagnostic pillars of the Jones Criteria.
3.Chorea and muscle weaknessare appropriate neurological indicators (Sydenham chorea is a major criterion), but a decreased erythrocyte sedimentation rateis incorrect. ARF causes systemic inflammation, which results in an elevated erythrocyte sedimentation rate (ESR), a minor diagnostic criterion.
Test-taking strategy:
- Analyze the scenario/question:The question asks the nurse to identify the group of findings that should be assessed based directly on the classic Jones Criteria for diagnosing acute rheumatic fever.
- Recall the Jones Criteria pillars:
- Major: Joints (migratory polyarthritis), O(carditis, shaped like a heart), Nodules (subcutaneous), Erythema marginatum, Sydenham chorea.
- Evidence:Mandatory confirmation of a recent strep infection (e.g., ASO titer).
- Eliminate inaccuracies:
- Rule out Choice 1due to the inclusion of dental caries.
- Rule out Choice 2because headache and anemia are not formal Jones criteria elements.
- Rule out Choice 3because the ESR must be elevated, not decreased.
- Rule in Choice 4as it includes two major clinical findings alongside the mandatory serological validation.
Take home points
- The Jones Criteria requires a strict combination of major signs, minor signs, and confirmed laboratory proof of a recent group A streptococcal exposure.
- Erythema marginatum manifests as a transient, non-pruritic, macular rash with distinct erythematous rings and pale centers, typically distributed across the trunk.
- Migratory polyarthritis characteristically moves sequentially from one large joint to another, causing temporary heat, redness, and excruciating pain.
- Documenting an elevated or rising anti-streptolysin O (ASO) titer satisfies the mandatory prerequisite requirement of proving a preceding bacterial infection.
A 12-year-old child has been diagnosed with group A strep pharyngitis. The primary health-care provider has ordered penicillin V 500 mg PO tid for 10 days. Which of the following questions is important for the nurse to ask the parents and the child before giving them the prescription?
Explanation
Before releasing a prescription for a multi-day oral medication regimen,the nurse must evaluate potential barriers to compliance.Eradicating group A streptococcus requires strict adherence to the full length of the therapy; failing to complete the course allows the remaining bacteria to multiply, substantially rising the risk of acute rheumatic fever.
Rationale for correct answer:
1.Asking if there is any reason they cannot take the medicine 3 times a day for 10 daysdirectly assessestreatment adherence potential.Factors like complex school schedules, financial constraints, or past difficulties swallowing pills can immediately derail oral therapy, making it critical to catch and address these issues before the family leaves the clinic.
Rationale for incorrect answers:
2.Asking "Would you rather get 1 shot or take 40 pills?"uses unprofessional, biased phrasing that can create unnecessarypatient anxietyregarding intramuscular treatments. While penicillin G benzathine is a valid single-dose injection alternative, the choice should be presented as an objective medical option rather than a threatening comparison.
3.Asking "Have you ever had strep throat before?"provides baseline data regarding the child's medical history, but it does not change the active management of the current acute infection. While useful for long-term health tracking, it is far less critical than ensuring immediate compliance with the newly ordered antibiotic regimen.
4.Asking about other children in the school with sore throatsserves a general epidemiological purpose for tracking community spread. While this helps identify local outbreaks, it has no direct impact on the treatment safety, medication adherence, or immediate safety of the individual child being discharged.
Test-taking strategy:
- Analyze the scenario/question:The provider has ordered a complex oral regimen (3 times daily for 10 days) for a school-aged child with confirmed strep pharyngitis. The nurse needs to identify the most critical pre-discharge question.
- Prioritize clinical outcomes:
- Rule inChoice 1:Uncovering adherence limitations before the family leaves allows the team to pivot to an alternative (like a single intramuscular injection) if 30 doses are unrealistic for their schedule.
- Rule outChoice 2:The wording is manipulative and non-therapeutic, violating professional communication standards.
- Rule outChoice 3:Past history does not override the immediate necessity of ensuring compliance with the present prescription.
- Rule outChoice 4:Community tracking is a secondary public health task that ranks below securing direct therapeutic adherence for the patient.
Take home points
- Complete eradication of group A streptococcus requires finishing the entire 10-day antibiotic course, even if symptoms vanish after a few days.
- Prematurely discontinuing antibiotics leaves the child vulnerable to serious post-streptococcal sequelae, including acute rheumatic fever.
- Assessing family schedules, school hours, and medication access before discharge is a primary nursing responsibility to verify that an oral regimen is practical.
- For families facing clear compliance barriers, a single intramuscular injection of penicillin G benzathine offers a highly effective alternative.
A child who has been diagnosed with chorea has been admitted to the pediatric unit with a diagnosis of rheumatic fever. Immediately prior to admission, the child’s throat culture was positive for group A strep. Which of the following actions should the nurse perform when admitting the child? Select all that apply
Explanation
Admitting a pediatric client with acute rheumatic feverpresenting with Sydenham chorea requires simultaneous management of neurological involuntary movements, active bacterial containment, and vigilant cardiovascular screening.
Rationale for correct answers:
1.Covering the headboard with a soft materialis a vital neurological safety intervention. Sydenham chorea causes sudden, involuntary, purposeless hyperkinetic movements of the limbs and face. Padding the headboard and bed rails protects the child from sustaining accidental soft tissue trauma or bruising during severe choreiform episodes.
2.Putting the child on droplet precautionsis mandatory because the child has an actively positive throat culture for group A streptococcus.While rheumatic fever itself is an autoimmune reaction and not contagious, the live pharyngeal streptococcal infectionis highly transmissible via respiratory secretions, necessitating droplet isolation until effective antibiotic therapy has been established for at least 24 hours.
5.Assessing the child's apical heart rate for one full minuteis the priority cardiovascular assessment standard.Rheumatic carditis can cause hidden pancarditis, leading to myocardial inflammation,structural valvular damage, or atrioventricular conduction delays (such as a prolonged PR interval). A full-minute apical auscultation allows the nurse to detect subtle murmurs, extra heart sounds (S3 or S4), or rhythm irregularities.
Rationale for incorrect answers:
3.Placing a tracheostomy tray in the child's roomis unnecessary because Sydenham chorea affects the basal ganglia and voluntary skeletal muscles, but it does not compromise the upper airwayor cause acute laryngospasm. This emergency equipment is reserved for severe obstructive upper airway conditions like acute epiglottitis.
4.Having the child perform active range of motion exercisesis strictly contraindicated. The acute phase of rheumatic fever demands strict bed restto reduce metabolic demandsand minimize the workload on a potentially inflamed myocardium. Furthermore, forcing purposeful movements can exacerbate the frustration and physical exhaustion associated with involuntary chorea.
Test-taking strategy:
- Analyze the scenario/question:The client is a child admitted with acute rheumatic fever, presenting with both involuntary neurological movements (chorea) and a laboratory-confirmed, active group A strep pharyngeal infection.
- Evaluate priority interventions:
- Rule inChoice 1:Involuntary movements create a high risk for injury, making environmental padding a clear safety priority.
- Rule inChoice 2:The active, culture-positive strep infection demands immediate droplet isolation to prevent nosocomial spread.
- Rule outChoice 3:The airway is not acutely threatened by chorea, making a tracheostomy tray an inappropriate use of emergency resources here.
- Rule outChoice 4:Active physical exertion is unsafely contraindicated during the acute carditis risk window.
- Rule inChoice 5:Carditis is the most dangerous complication of ARF; a full-minute apical pulse check is essential to catch early cardiac dysfunction.
Take home points
- Sydenham chorea is a major Jones criterion characterized by involuntary, aimless movements, facial grimacing, muscle weakness, and emotional lability.
- Pediatric safety protocols for severe chorea require a quiet environment, padded bed frames, and assistance with fine-motor activities like eating to prevent injury.
- Droplet isolation precautions must be maintained for any client with a positive group A streptococcal culture until 24 hours of effective antibiotic therapy are completed.
- Carditis is the only manifestation of acute rheumatic fever that leads to permanent structural damage, requiring meticulous daily cardiac assessments.
The nurse is assessing a child diagnosed with rheumatic fever whose EKG is shown below.
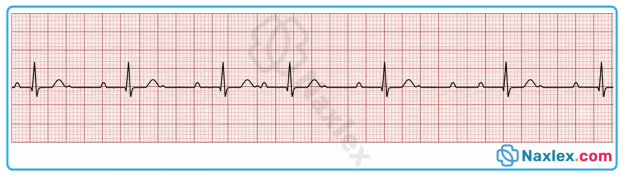
After examining the strip, which of the following conclusions would the nurse make? The strip shows evidence of:
Explanation
Rheumatic carditiscauses inflammation within the cardiac conduction pathways. Edema slows atrioventricular node conduction, producing a prolonged PR intervalrepresenting delayed atrial depolarization transmissionto ventricles, serving as a minor Jones criterionfor active myocardial tissue inflammation.
Rationale for correct answer:
3.The strip demonstrates an increased duration between the onset of atrial and ventricular activation.This baseline measurement exceeds the upper physiological limit of 0.16 seconds for pediatric cohorts. The delay directly indicates atrioventricular nodal inflammationduring acute carditis. This transient first-degree heart blockconfirms active carditis.
Rationale for incorrect answers:
1.The tracing reveals regular, identifiable sinus P waves preceding every QRS complex at consistent intervals. Atrial fibrillation would instead exhibit a total absence of P waves replaced by disorganized fibrillatory waves. Additionally, the ventricular response would manifest as a highly irregular rhythm. This specimen shows a completely regular rhythmruling out atrial fibrillation pathology.
2.The rhythm demonstrates uniform QRS complexes of normal duration under 0.08 seconds without early beats. A premature ventricular contraction would display an early, wide, distorted QRS complex exceeding normal limits. It would also lack a preceding P wave and be followed by a compensatory pause. This EKG shows normal QRS morphologywithout any ectopic ventricular beats.
4.The repolarization phase displays upright, rounded, asymmetrical waves that possess appropriate amplitude relative to the preceding complexes. Flattened repolarization waves typically indicate electrolyte imbalances like hypokalemia or generalized myocardial ischemia. Myocardial inflammation in rheumatic fever characteristically alters conduction transit times rather than causing isolated repolarization flattening.This normal appearance rules out acute ventricular repolarizationimpairment.
Test-taking strategy:
- Analyze the scenario/question:The nurse is analyzing an electrocardiogram strip from a pediatric client diagnosed with acute rheumatic fever to identify specific diagnostic features.
- Apply diagnostic frameworks:
- Rule in Choice 3:Recall that a prolonged PR intervalis a classic minor Jones criterion indicating atrioventricular conduction delay due to carditis.
- Evaluate rhythm regularity:
- Rule out Choice 1:Note the presence of organized P waves and constant R-R intervals, which eliminates the disorganized rhythm typical of atrial fibrillation.
- Analyze complex morphology:
- Rule out Choice 2:Observe that all ventricular complexes are narrow and uniform, excluding premature ventricular contractionsthat present with wide, aberrant shapes.
- Rule out Choice 4:Inspect the ST-T segment to confirm that T waves maintain normal amplitude and contour, ruling out flattened T wavesoften tied to electrolyte imbalances.
Take home points
- A prolonged PR interval represents a first-degree atrioventricular block caused by inflammatory edema within the cardiac conduction system during acute rheumatic fever.
- This conduction delay is classified as a minor criterion under the revised Jones criteria used to establish a diagnosis of rheumatic fever.
- Unlike valvular damage, the atrioventricular nodal conduction delay seen in these patients is typically transient and resolves as the acute inflammation subsides.
- Electrocardiographic monitoring in acute rheumatic fever is essential to track the progression of carditis and detect higher degrees of heart block.
A 10-year-old child is in the hospital on bedrest with a diagnosis of rheumatic fever complicated by carditis. When the nurse responds to the child’s call bell, the child states, “I hate this! I want to get up and play!” Which of the following responses is appropriate for the nurse to make at this time?
Explanation
When caring for a pediatric client on strict bed restdue to acute carditis,the nurse must maintain standard therapeutic boundaries while proactively addressing the child's developmental and emotional needs. Active myocardial inflammation increases the risk of heart failure and permanent structural damage if physical activity increases cardiac workload. The nurse's role is to enforce necessary physical limitations safely while offering age-appropriate diversionary activitiesto ease the frustration of confinement.
Rationale for correct answer:
4."I am so sorry that you are unhappy, but what if I contact the play lady and have her bring you a selection of video games to play with?"is the most appropriate response. It validates the child's emotional frustration with genuine empathy, strictly maintains the mandatory cardiac bed rest protocol,and immediately provides an engaging, low-energy substitute activity (video games) that fits the developmental needs of a 10-year-old.
Rationale for incorrect answers:
1."I know that you are unhappy, but you must stay in bed so that you can get better and go home"acknowledges the child's feelings but uses a rigid, dismissive communication style. It fails to offer any immediate diversionary solutionsor coping mechanisms, which can leave a school-aged child feeling powerless and more inclined to resist bed rest.
2."What if we make a deal and I promise to let you get up for 10 minutes every 2 hours if you are very good the rest of the day?"is dangerous and unscientific. The nurse cannot negotiate away a critical medical restriction; allowing an active carditis patient to ambulate repeatedly introduces severe myocardial strainthat can worsen valvular damage.
3."I am sure that I can get the doctor to let you go to the playroom for 1 to 2 hours this afternoon"offers false hope and misrepresents the standard of care for severe rheumatic carditis. The provider will not approve active playroom access during the acute phase, and making this promise damages therapeutic trustonce the request is denied.
Test-taking strategy:
- Analyze the scenario/question:The client is a 10-year-old child hospitalized on strict bed rest for rheumatic fever complicated by carditis. The child is frustrated by the physical confinement, and the nurse must choose the best response.
- Identify the physiological boundary:Carditis requires strict bed rest to prevent heart failure. Any answer choice that permits or promises ambulation (Choices 2 and 3) must be eliminated immediately for patient safety.
- Evaluate communication and development:
- Rule outChoice 1: This choice is overly authoritarian and fails to address the underlying problem of boredom.
- Rule inChoice 4:This response combines active empathy with a safe, developmentally appropriate, low-energy distraction that preserves cardiac rest.
Take home points
- Strict bed rest is an absolute requirement during the acute phase of rheumatic carditis to reduce myocardial oxygen demands and minimize permanent valvular scarring.
- School-aged children (ages 6 to 12) value industry and peer connection; long periods of immobilization can cause significant frustration, behavioral regression, or anger.
- Nurses should substitute physical activities with quiet, intellectually stimulating diversions such as board games, video games, books, or crafts to encourage compliance.
- Clear, empathetic communication that explains the biological reason for bed rest helps the child understand restrictions without feeling punished.
An 8-year-old client, who is complaining of a “really bad” sore throat and whose temperature is 102.2°F, is seen in the school nurse’s office. The nurse has the child lie down in a room away from other children. Which of the following statements is most important for the nurse to convey when calling the child’s parents?
Explanation
When managing a school-aged child with a sudden onset of a high fever (102.2oF/ 39oC) and a severe sore throat,the school nurse's primary public health and clinical responsibility is to secure a definitive diagnosis.These symptoms are classic indicators of group A beta-hemolytic streptococcal pharyngitis, which requires objective testing and prompt antibiotic intervention to eliminate the risk of severe post-infectious sequelae like acute rheumatic fever.
Rationale for correct answer:
1.Stating that the child needs to be seen by her primary care provideris the most critical message because it establishes a direct path toward definitive diagnostic testing(throat culture or rapid antigen test). Advancing the child to a clinical setting ensures that if strep is present, targeted antibiotic therapy will be initiated within the crucial 9-day windowrequired to prevent the onset of rheumatic heart disease.
Rationale for incorrect answers:
2.Conveying that the child is very uncomfortable with a sore throatprovides descriptive sensory information about the child's comfort level. While validating the child's distress is standard practice, this statement focuses on transient symptoms rather than guiding the parents toward the medical evaluation needed to prevent long-term systemic complications.
3.Reporting that the child is crying and asking for her parentshighlights an expected emotional and behavioral response for an ill 8-year-old child. While communicating emotional status is helpful for parental reassurance, it does not address the underlying clinical urgency or outline the necessary steps to manage a potentially severe bacterial infection.
4.Stating that the child may be contagious to other childrenaddresses a valid epidemiological concern that justifies the nurse's decision to isolate the child. However, emphasizing transmission risks to the parents is secondary to securing immediate, individualized clinical care and treatment for their own child.
Test-taking strategy:
- Analyze the scenario/question:An 8-year-old child presents with a severe sore throat and a high fever (102.2oF/ 39oC). The school nurse has isolated the child and needs to identify the most critical piece of information to communicate to the parents.
- Prioritize clinical actions:
- Rule inChoice 1:Directing the parents to a primary care provider ensures the child receives the diagnostic swabbing and narrow-spectrum antibiotics required for primary prevention of rheumatic fever.
- Rule outChoice 2:Documenting symptom severity describes the presentation but does not offer a proactive clinical solution.
- Rule outChoice 3:Psychosocial and comfort tracking is an ongoing care element but lacks the urgency of directing medical intervention.
- Rule outChoice 4:Highlighting contagion status addresses community spread but does not prioritize the immediate diagnostic needs of the patient.
Take home points
- School nurses play a frontline role in the primary prevention of acute rheumatic fever by identifying high-risk pharyngitis presentations and directing families to definitive care.
- Group A streptococcal pharyngitis typically presents abruptly with high fever, severe sore throat, tonsillar exudates, and an absence of viral symptoms like coryza or cough.
- Parents must be educated that a physical examination alone cannot differentiate between viral and bacterial pharyngitis; an objective throat swab is mandatory.
- Initiating appropriate antibiotic therapy within 9 days of the onset of streptococcal pharyngitis is nearly 100% effective at preventing the development of rheumatic fever.
A child who had rheumatic fever now has a complication of mild mitral valve prolapse. What information should be included in the child’s discharge instructions?
Explanation
The primary goal of discharge management for a child with a history of rheumatic feverand subsequent structural valvular damage, such as mitral valve prolapse, is the prevention of infective endocarditis.The scarred and deformed endothelial surfaces of the heart valves serve as prime sites for bacterial attachment. During invasive procedures, transient bacteremia can occur, risking colonization of these vulnerable leaflets.
Rationale for correct answer:
4.Complying with antibiotic therapy during dental surgeries or proceduresrepresents the critical infective endocarditis prophylaxisstandard. Prophylactic antibiotics (typically amoxicillin given one hour prior to the procedure) eradicate transient oral bacteria introduced into the bloodstream, safeguarding the deformed mitral valve from bacterial colonization and subsequent endocardial destruction.
Rationale for incorrect answers:
1.Reporting bruising and bleeding to the physicianis an important nursing instruction for patients receiving active anticoagulant therapy(such as warfarin) for mechanical valves or chronic atrial fibrillation. However, a child with simple, mild mitral valve prolapse does not require routine anticoagulation, making this warning unnecessary.
2.Increasing the intake of fruits and vegetablesrepresents excellent, generalized advice for baselinenutritional healthand cardiac wellness. While a nutrient-dense diet is always encouraged for growing children, it lacks the targeted, life-saving specificity required to prevent acute infectious destruction of a deformed valve.
3.Encouraging strenuous exercisemust be approached with caution and individualized based on recent clinical evaluations. While mild, asymptomatic mitral valve prolapse generally permits normal physical activity, an unguided recommendation to increase exercise is secondary to the immediate, high-priority need for infection prevention guidelines.
Test-taking strategy:
- Analyze the scenario/question:The client is a child with a history of rheumatic fever who has developed mild mitral valve prolapse. The nurse must identify the most critical piece of discharge instruction.
- Correlate pathology with clinical risk:
- Rule outChoice 1:Bleeding precautions are reserved for patients on therapeutic anticoagulants, which are not indicated for mild prolapse.
- Rule outChoice 2:Dietary advice supports general wellness but does not address the primary structural risk of the condition.
- Rule outChoice 3:Activity guidelines are essential, but they do not take priority over mitigating life-threatening infectious risks.
- Rule inChoice 4:Deformed endocardial tissue creates an absolute susceptibility to bacterial seeding during bacteremia, making dental antibiotic prophylaxis the definitive safety priority.
Take home points
- A history of rheumatic endocarditis permanently primes the valvular tissue for secondary complications, including bacterial colonization.
- Transient bacteremia caused by routine dental manipulations (like cleanings or extractions) is a leading trigger for infective endocarditis in susceptible hosts.
- Caregivers must maintain transparent communication, informing all dentists, surgeons, and specialists of the child's specific rheumatic and valvular history.
Standard prophylactic protocols utilize a single oral dose of amoxicillin administered 30 to 60 minutes before the scheduled tissue-disrupting procedure.
A 12-year-old child is in the urgent care clinic presents with a complaint of fever, headache, and sore throat. A diagnosis of group A β-hemolytic streptococcus (GABHS) pharyngitis is established with a rapid-strep test, and oral penicillin is prescribed. The nurse knows that which of the following statements about GABHS is correct?
Explanation
Group A beta-hemolytic streptococcus (GABHS),or Streptococcus pyogenes, is a virulent bacterial pathogen responsible for the vast majority of acute bacterial pharyngitisin school-aged children. When left untreated or inadequately treated, GABHS can trigger severe, immune-mediated systemic diseases that carry high morbidity.
Rationale for correct answer:
3. GABHS possesses potent surface antigens, most notably M protein,that provoke a strong host immune response. In some individuals, the antibodies produced to fight the bacteria cross-react with human connective tissues through a process known as molecular mimicry,leading to acute rheumatic fever(affecting the heart, joints, and brain). Additionally, circulating antigen-antibody complexes can deposit within the renal filtration barriers, activating complement pathways and resulting in acute post-streptococcal glomerulonephritis.
Rationale for incorrect answers:
1. GABHS pharyngitis does not confer long-term immunity. There are over 200 distinct serotypes of group A streptococcus based on variations in the M protein. A child can easily contract a new GABHS infection if exposed to a different strain or if the previous exposure did not stimulate a strong protective antibody response.
2. Routine post-treatment throat culturesare not recommended for asymptomatic individuals who have completed a standard 10-day course of penicillin. Follow-up testing is reserved only for children who remain symptomatic, have a personal history of rheumatic fever, or live in high-risk households during an outbreak.
4. GABHS is the definitive trigger for rheumatic fever (which causes transient, migratory polyarthritis in children), but it has no causal or epidemiological link to rheumatoid arthritis.Rheumatoid arthritis is a completely separate, chronic autoimmune disorder characterized by symmetric destructive joint changes, driven by distinct genetic and environmental factors in adulthood.
Test-taking strategy:
- Analyze the core question:The prompt asks for a factually correct statement regarding the clinical trajectory or risks associated with a confirmed GABHS pharyngitis infection.
- Differentiate autoimmune sequelae:
- Rule out Choice 4:Do not confuse rheumatic fever (post-streptococcal) with rheumatoid arthritis (chronic, unrelated adult pathology).
- Rule out Choice 2:Standard guidelines emphasize that routine reswab plots waste clinical resources if the child is asymptomatic.
- Rule out Choice 1:Bacterial pharyngitis allows for frequent repeat infections due to strain diversity.
- Rule inChoice 3:This highlights the classic non-suppurative, immune-mediated multi-system complications that define post-streptococcal disease risks.
Take Home Points
- Acute rheumatic fever is a post-infectious sequela that follows pharyngeal GABHS infections exclusively, whereas post-streptococcal glomerulonephritis can follow either pharyngeal or cutaneous (impetigo) infections.
- While antibiotic therapy is highly effective at preventing acute rheumatic fever if initiated within 9 days of symptom onset, it does not reliably prevent the development of post-streptococcal glomerulonephritis.
- A standard 10-day oral penicillin V potassium or amoxicillin regimen remains the gold standard choice for GABHS pharyngitis due to narrow-spectrum targeting and lack of documented resistance.
The nurse is teaching the parents of a 6-year-old client about the long-term consequences of rheumatic fever. The nurse should discuss the possibility of:
Explanation
Rheumatic feveris an inflammatory disease following Streptococcus pyogenesinfection that causes autoimmune cross-reactivityagainst human tissues. It classically manifests with carditis, polyarthritis, erythema marginatum, subcutaneous nodules, and Sydenham chorea, potentially leading to chronic cardiac structural damage.
Rationale for correct answer:
1. Rheumatic carditiscauses progressive valvular fibrosisand scarring, primarily targeting the mitral valve. The chronic deformation results in valvular regurgitation or stenosis decades later. The question stem emphasizes long-term consequences, which specifically aligns with this permanent valvular architecturedisruption.
Rationale for incorrect answers:
2. Chronic left-sided valvular dysfunctioncan eventually cause pulmonary congestionas a secondary mechanism. However, primary pulmonary arterial hypertension is not a direct, characteristic complication of acute rheumatic carditis pathognomonic features. This option represents a secondary hemodynamic sequelarather than the primary structural lesion.
3. Obstruction of the superior vena cavausually arises from mediastinal malignancies or intravascular thrombosisassociated with central catheters. Rheumatic fever pathologically affects the endocardium, myocardium, and pericardium. It does not induce extrinsic venous compressionor occlusion within the superior mediastinum.
4. Chronic mitral stenosiseventually leads to right ventricular enlargementdue to increased afterload from pulmonary backward pressure. However, right ventricular remodeling is a late, tertiary adaptation to systemic pulmonary congestion. The primary, direct long-term structural consequence remains localized to left-sided endocardialstructures.
Test-taking strategy:
- Analyze the scenario/question:The nurse is providing discharge education to the parents of a 6-year-old child regarding the definitive long-term complications associated with a history of rheumatic fever.
- Evaluate pathophysiology standards:
- Rule in Choice 1:The molecular mimicry of rheumatic fever specifically targets endocardial tissues. Chronic valvular heart disease is the classic, definitive long-term structural complication of this disease process.
- Identify structural anatomy hazards:
- Rule out Choice 3:Superior vena cava syndrome involves systemic venous drainage obstruction. This is entirely unrelated to the carditis, asymmetrical polyarthritis, or dermatological manifestations seen in rheumatic fever sequences.
- Differentiate primary versus secondary lesions:
- Rule out Choice 2:Elevated pulmonary pressures occur only as a tertiary hemodynamic result of advanced, uncompensated left ventricular or valvular failure over many years.
- Rule out Choice 4:Right ventricular wall thickening is a late compensatory response to chronic pulmonary hypertension caused by severe left-sided valvular disease rather than a direct acute rheumatic lesion.
Take home points
- Rheumatic fever results from an untreated pharyngeal infection with group A beta-hemolytic streptococcus that triggers an immune-mediated attack on connective tissues.
- The most significant long-term complication of rheumatic carditis is chronic valvular heart disease, which most frequently damages the mitral and aortic valves.
- Right-sided cardiac remodeling and pulmonary venous congestion are late secondary complications resulting from chronic, uncompensated left-sided valvular stenosis or regurgitation.
- Prevention of recurrent episodes and subsequent structural cardiac damage requires adherence to long-term prophylactic antibiotic therapy, often lasting for several years or into adulthood.
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Analyze the relationship between Group A Beta-Hemolytic Streptococcal (GABHS) pharyngeal infections and the subsequent autoimmune development of acute rheumatic fever (ARF).
- Apply the Revised Jones Criteria accurately to differentiate major and minor manifestations for diagnosing primary and recurrent episodes of ARF.
- Identify key clinical manifestations of ARF, focusing on carditis, migratory polyarthritis, Sydenham chorea, erythema marginatum, and subcutaneous nodules.
- Interpret diagnostic findings, including anti-streptolysin O (ASO) titers, acute-phase reactants (ESR, CRP), and echocardiography, to confirm a diagnosis and assess carditis severity.
- Outline the therapeutic management for ARF, focusing on antibiotic eradication therapy, anti-inflammatory medications, and supportive care for chorea and heart failure.
- Develop a comprehensive nursing care plan prioritizing bed rest, pain management for joint pain, neurological safety for chorea, and monitoring for cardiac decompensation.
- Formulate a long-term secondary prevention strategy including appropriate choices, dosages, and duration of prophylactic antibiotic therapy to prevent recurrent ARF and chronic rheumatic heart disease (RHD).
Introduction
- Acute rheumatic fever (ARF) is a multi-system, nonsuppurative inflammatory disease that occurs as a delayed sequela to an untreated or inadequately treated pharyngeal infection caused by Group A Beta-Hemolytic Streptococcus (GABHS), specifically Streptococcus pyogenes.
- Unlike direct bacterial infections where pathogens tissue-invade local structures, ARF is a classic example of an autoimmune reaction driven by molecular mimicry. The body's immune system, while attempting to eliminate the streptococcal bacteria, mistakenly mounts an attack against its own healthy tissues due to structural similarities between bacterial antigens and human proteins.
- This inflammatory storm target-seeks specific organ systems, predominantly affecting the heart, joints, central nervous system, skin, and subcutaneous tissues.
- Although the manifestations in the joints, skin, and brain are typically transient and resolve without permanent damage, the impact on the heart can be profound and permanent.
- Carditis, or inflammation of the heart tissue, can involve the endocardium, myocardium, and pericardium (pancarditis).
- Acute valvular inflammation can progress over years or decades into chronic rheumatic heart disease (RHD), characterized by permanent valvular scarring, deformity, and subsequent heart failure.
- From a nursing perspective, patients presenting with ARF require vigilant, holistic care. Because ARF primarily strikes school-aged children and young adults, the psychological and physical impact can be severe.
- The nurse plays an indispensable role in recognizing early signs of cardiac stress, managing the extreme discomfort of migratory polyarthritis, and implementing strict safety measures for the involuntary movements of Sydenham chorea.
- Beyond acute stabilization, the nurse serves as a critical educator, ensuring families understand the absolute necessity of long-term secondary antibiotic prophylaxis to safeguard the heart from devastating recurrent attacks.
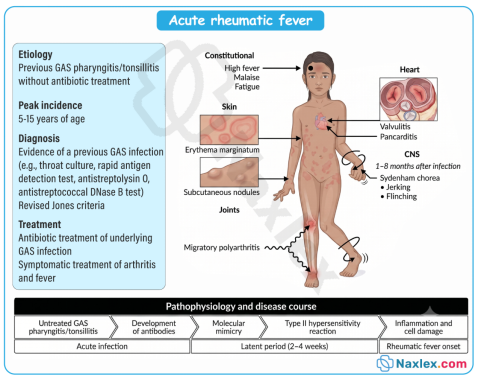
Epidemiology, Etiology, Risk Factors, And Pathophysiology
Epidemiology
- Age Group: ARF primarily affects children and adolescents aged 5 to 15 years. It is rare in children under 3 years and decreases significantly in frequency after late adolescence.
- Socioeconomic Impact: Although the incidence has drastically declined in high-income countries due to routine antibiotic treatment for strep throat, it remains a massive public health crisis in low- and middle-income countries, indigenous populations, and areas with crowded living conditions.
Etiology & Risk Factors
- Primary Pathogen: Streptococcus pyogenes (Group A Beta-Hemolytic Streptococcus or GABHS). Notably, only upper respiratory tract GABHS infections (pharyngitis) trigger ARF; streptococcal skin infections (impetigo, pyoderma) do not.
- Environmental Triggers: Overcrowding, substandard housing, poverty, and limited access to healthcare drastically increase transmission rates of streptococcal pharyngitis.
- Host Susceptibility: A genetic predisposition is linked to specific human leukocyte antigen (HLA) class II types, influencing how an individual's immune system responds to streptococcal antigens.
Pathophysiology
The underlying mechanism of ARF is molecular mimicry, a form of autoimmune cross-reactivity.
- Antigen Presentation: During a GABHS infection, the body creates antibodies against virulence factors on the bacterial cell wall, most notably the M-protein.
- Cross-Reactivity: The structural configuration of the streptococcal M-protein closely resembles human host proteins. The antibodies fail to distinguish between the two:
- Heart: Antibodies bind to cardiac myosin and valvular endothelium, initiating a cascade of inflammatory T-cells.
- Brain: Antibodies cross-react with lysogangliosides in the basal ganglia, disrupting dopaminergic pathways.
- Joints & Skin: Immune complexes deposit in the synovium and dermal layers, sparking acute, localized inflammation.
- Histopathology: The hallmark histological feature found in the myocardium during the acute phase is the Aschoff body, a localized area of tissue necrosis surrounded by immune cells (lymphocytes, plasma cells, and large, activated macrophages known as Anitschkow cells or "caterpillar cells").
Image Title: Acute Rheumatic Fever Pathophysiology
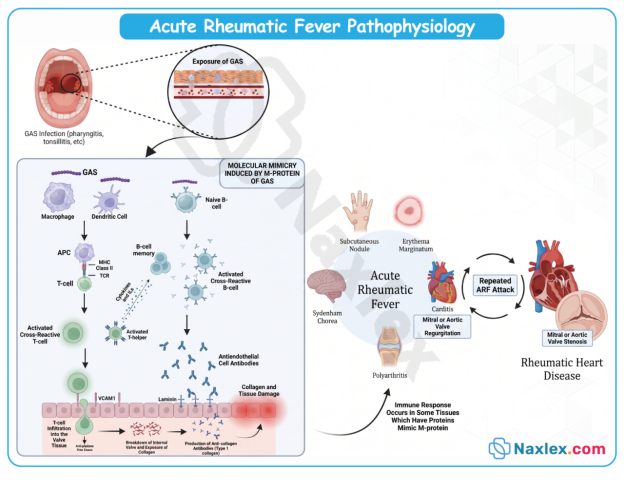
Clinical Manifestations
The clinical expression of ARF appears after a latent period of approximately 2 to 4 weeks following the initial strep infection. Signs are traditionally categorized into Major and Minor criteria.
Major Manifestations
- Carditis (50-70% of cases): The most serious manifestation. It presents as a pancarditis affecting the endocardium (causing valvular regurgitation, typically mitral or aortic), myocardium (causing tachycardia, cardiomegaly, or heart failure), and pericardium (causing a friction rub or chest pain).
- Migratory Polyarthritis (approx. 75% of cases): Intense inflammation affecting the large joints (knees, ankles, elbows, wrists). It is distinctively migratory, one joint becomes red, hot, swollen, and excruciatingly painful for a few days, and as it resolves, another joint becomes involved. It leaves no permanent joint damage.
- Sydenham Chorea (10-15% of cases): Also known as "St. Vitus Dance," this is a delayed CNS manifestation occurring up to several months after infection. It is characterized by sudden, involuntary, purposeless, jerky movements, accompanied by muscle weakness and emotional lability. It is more common in females and resolves completely over weeks to months.
- Erythema Marginatum (<5% of cases): A distinct, non-pruritic, erythematous rash. It features pink macules with clear centers and elevated, wavy borders, typically found on the trunk and proximal extremities. It is transient and can be accentuated by heat (e.g., a warm bath).
- Subcutaneous Nodules (<2% of cases): Small, firm, painless, mobile nodules measuring 0.5 to 2 cm. They appear in crops over bony prominences (extensor surfaces of elbows, knees, knuckles, spine) and are almost always associated with severe carditis.
Minor Manifestations
- Arthralgia: Joint pain without objective findings of inflammation (swelling, redness, warmth). Cannot be used if polyarthritis is already counted as a major criterion.
- Fever: Characteristically high-grade at the onset of acute illness (>38.5∘C or >101.3∘F).
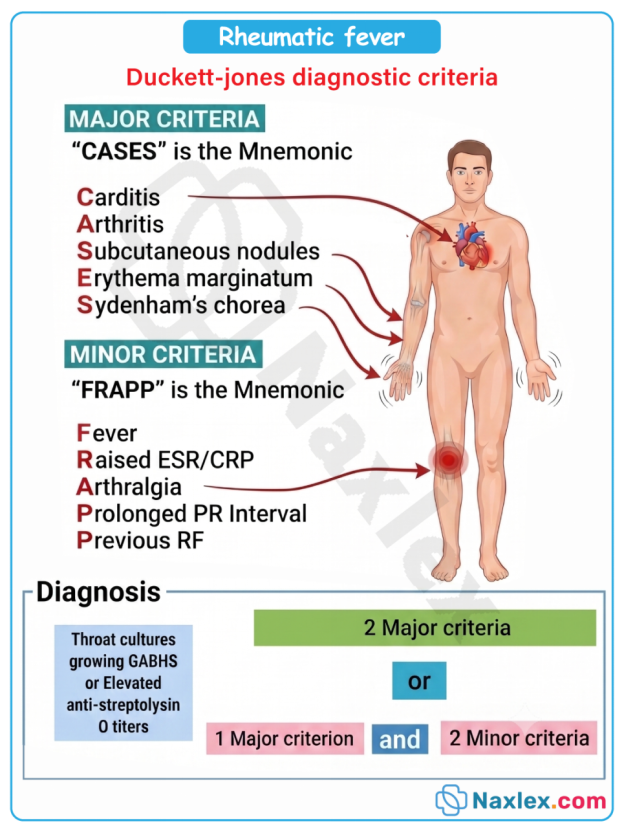
Diagnostic Evaluation
No single clinical symptom or laboratory marker is diagnostic of ARF. Clinicians rely on the Revised Jones Criteria, which requires evidence of a preceding GABHS infection PLUS either 2 major criteria OR 1 major and 2 minor criteria.
Essential Evidence of Preceding GABHS Infection
- Positive throat culture or rapid streptococcal antigen test.
- Elevated or rising streptococcal antibody titers: Anti-streptolysin O (ASO) titer (most common) or Anti-DNase B titer.
Laboratory Findings (Minor Criteria)
- Acute-Phase Reactants: Elevated Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP), reflecting systemic inflammation.
Objective Assessment Tools
- Electrocardiogram (ECG): Demonstrates a prolonged PR interval (first-degree atrioventricular block), reflecting inflammatory delay in cardiac conduction.
- Echocardiography (Echo): Essential for detecting subclinical carditis, evaluating mitral/aortic valve regurgitation, and assessing ventricular function.
Therapeutic Management
Therapeutic goals are aimed at eradicating any remaining streptococcal bacteria, controlling systemic inflammation, protecting the heart, and mitigating symptoms.
Antibiotic Therapy
- Primary Eradication: A single intramuscular injection of Penicillin G Benzathine is the treatment of choice. Alternatively, a 10-day course of oral Penicillin V or Amoxicillin is prescribed. For penicillin-allergic patients, Erythromycin, Azithromycin, or Cephalexin are used.
Anti-inflammatory Medications
- Salicylates (Aspirin): Highly effective at suppressing the joint pain and inflammation of polyarthritis.
Nursing Insight: Aspirin is used cautiously in pediatrics due to the risk of Reye's syndrome, but ARF is a specific indication where its anti-inflammatory benefits outweigh the risks under close monitoring.
- Corticosteroids (Prednisone): Reserved for patients with severe carditis or cardiomegaly to rapidly control myocardial inflammation and protect valvular function.
Supportive Therapy
- Chorea Management: For severe Sydenham chorea, anticonvulsants or sedatives such as Phenobarbital, Haloperidol, or Valproic acid may be utilized to minimize involuntary motor activity.
- Heart Failure Management: If carditis leads to heart failure, therapy includes fluid restriction, a low-sodium diet, diuretics (Furosemide), and inotropic agents (Digoxin).
Nursing Care Plan
Nursing Diagnosis 1: Decreased Cardiac Output
- Related To: Myocardial and valvular inflammation associated with acute rheumatic carditis.
- Evidenced By: Tachycardia disproportionate to fever, tachypnea, gallop rhythm, new or changing heart murmurs, orthopnea, or peripheral edema.
- Expected Outcome: The patient will maintain adequate cardiac output as evidenced by stable vital signs, clear lung fields, and strong peripheral pulses.
Nursing Interventions & Rationales
- Enforce Strict Bed Rest: Minimize metabolic demand and cardiac workload during the acute inflammatory phase. Slowly advance activity as acute-phase reactants (ESR, CRP) normalize.
- Monitor Vital Signs Continuously: Assess for resting tachycardia (a key indicator of carditis) and changes in respiratory rate or blood pressure.
- Perform Focused Cardiac Assessment: Auscultate for new murmurs (mitral regurgitation), muffled heart sounds, or a pericardial friction rub.
- Administer Prescribed Medications Safely: Give corticosteroids or diuretics as ordered; closely track intake/output and daily weights to monitor for fluid retention.
Nursing Diagnosis 2: Acute Pain
- Related To: Inflammatory immune complex deposition in the large joints (polyarthritis).
- Evidenced By: Guarding behavior, crying, reluctance to move limbs, and swollen, warm, erythematous joints.
- Expected Outcome: The patient will report a significant reduction in joint pain and display improved mobility within 24 to 48 hours of starting anti-inflammatory therapy.
Nursing Interventions & Rationales
- Administer Scheduled Salicylates (Aspirin): Provide aspirin with food or milk to minimize gastric distress; monitor closely for salicylic acid toxicity (tinnitus, tachypnea).
- Handle Joints with Extreme Gentleness: Avoid sudden movements or jerking the bed; support joints during repositioning.
- Utilize Non-Pharmacological Comfort Measures: Use bed cradles to keep heavy blankets off tender joints; apply warm compresses if tolerated.
Nursing Diagnosis 3: Risk for Injury
- Related To: Involuntary, uncoordinated motor movements associated with Sydenham chorea.
- Expected Outcome: The patient will remain free from physical trauma or injury during episodes of choreiform movements.
Nursing Interventions & Rationales
- Modify the Environment for Safety: Keep the bed in the lowest position with padded side rails up. Eliminate sharp objects from the immediate surroundings.
- Assist with Activities of Daily Living (ADLs): Provide finger foods and use unbreakable utensils to prevent injury during meals; assist with ambulation.
- Provide Emotional Support and Reassurance: Inform the child and family that these movements are temporary and will resolve completely, helping to alleviate anxiety and frustration.
Complications
Chronic Rheumatic Heart Disease (RHD)
The most significant and devastating long-term complication of ARF. Repeated or severe bouts of rheumatic carditis lead to structural remodeling, scarring, and calcification of the cardiac valves.
- Mitral Valve Deformity: The mitral valve is the most frequently damaged structure (followed by the aortic valve). Valvular inflammation leads to mitral regurgitation in the acute phase, which can evolve over decades into mitral stenosis as the valve leaflets become rigid, thickened, and fused.
- Clinical Sequelae: RHD leads to chronic heart failure, pulmonary hypertension, and atrial fibrillation (due to left atrial enlargement from mitral stenosis), which significantly elevates stroke risk.
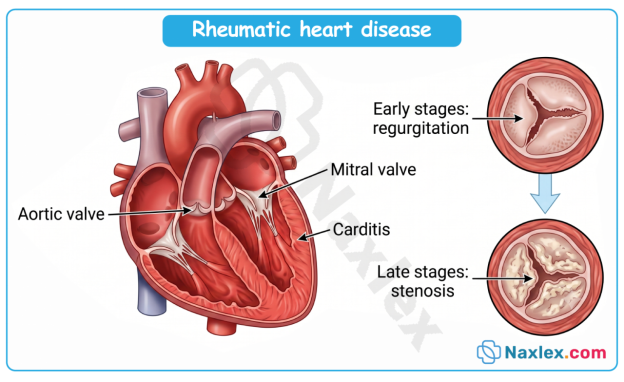
Other Complications
- Cardiac Arrhythmias: High-degree heart blocks or atrial tachyarrhythmias caused by conduction pathway inflammation.
Thromboembolism: Systemic emboli originating from thrombi formed in an enlarged, fibrillating left atrium.
Prognosis
The immediate prognosis of an ARF episode is generally favorable, with joint manifestations, rash, and chorea completely resolving without residual deficits. However, the overall long-term prognosis depends entirely on two primary variables:
- The Severity of the Initial Carditis: Individuals who escape the initial attack without cardiac involvement rarely develop subsequent valvular disease, provided they do not experience recurrences.
- Prevention of Recurrent Episodes: Each recurrent episode of ARF compounds previous cardiac damage. The heart becomes increasingly vulnerable with each subsequent streptococcal infection.
If recurrent infections are completely prevented through consistent antibiotic prophylaxis, even mild-to-moderate valvular damage can stabilize or improve over time.
Prevention
Prevention strategies are categorized into Primary and Secondary interventions, forming the cornerstone of global rheumatic fever control.
Primary Prevention
- Goal: Prevent the initial attack of ARF.
- Intervention: Promptly diagnose and properly treat all cases of GABHS pharyngitis using a full 10-day course of oral penicillin (or an appropriate alternative) or a single injection of Benzathine Penicillin G. If antibiotic therapy is initiated within 9 days of the onset of strep throat symptoms, the risk of developing ARF is virtually eliminated.
Secondary Prevention (Long-Term Prophylaxis)
- Goal: Prevent recurrent GABHS infections that trigger recurrent episodes of ARF and worsen RHD.
- Standard Regimen: Intramuscular Penicillin G Benzathine administered every 3 to 4 weeks is the most reliable method. Oral Penicillin V or Sulfadiazine daily are alternatives but are highly dependent on patient compliance.
- Duration of Prophylaxis:
|
Patient Clinical Status |
Standard Duration of Prophylaxis |
|
ARF without Carditis |
For 5 years or until age 21 (whichever is longer) |
|
ARF with Carditis (No Residual Valve Disease) |
For 10 years or until age 21 (whichever is longer) |
|
ARF with Carditis + Residual Valvular Disease |
For 10 years or until age 40 (whichever is longer); sometimes lifelong |
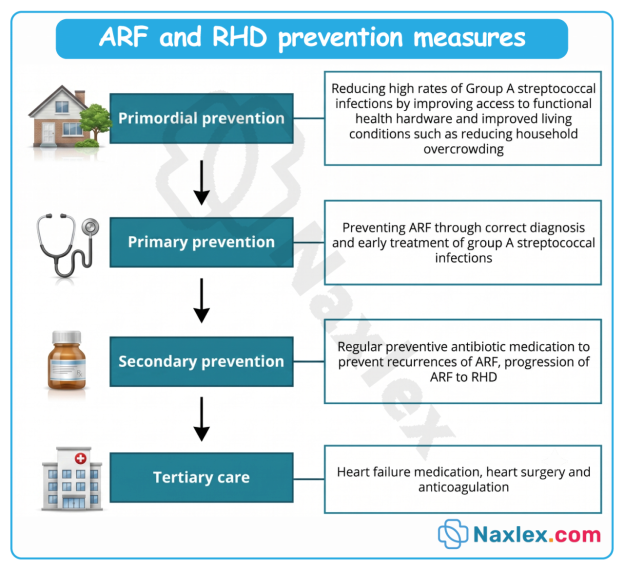
Summary
- Acute rheumatic fever (ARF) represents a critical, preventable public health challenge highlighting the severe consequences of an unregulated immune response.
- Driven by molecular mimicry, anti-streptococcal antibodies intended to combat a routine Group A Beta-Hemolytic Streptococcal (GABHS) pharyngeal infection cross-react with native human proteins.
- This autoimmune attack causes profound, systemic inflammation across multiple organ systems, most notably affecting the joints, skin, brain, and heart tissues.
- Although manifestations such as migratory polyarthritis, erythema marginatum, and Sydenham chorea are distressing to patients and families, they are transient and resolve without permanent disability. The true morbidity of ARF lies in its cardiac impact.
- Acute carditis can evolve into chronic rheumatic heart disease (RHD), causing permanent mechanical damage, fibrosis, and stenosis of the cardiac valves, most frequently the mitral valve. This structural damage places individuals at high risk for future heart failure, arrhythmias, and thromboembolic events later in life.
- The nursing care of a patient with ARF requires a multi-faceted approach. In the acute phase, nurses prioritize cardiac rest, gentle pain management, and environmental safety modifications for involuntary movements. In the long term, the nursing focus shifts toward education and advocacy.
- By ensuring strict adherence to secondary antibiotic prophylaxis regimens, nurses play a key role in preventing the recurrent GABHS infections that drive progressive, permanent valvular damage.
