
Please set your exam date
Process of Labor (4 Ps)
Study Questions
Practice Exercise 1
A nurse is assessing a client in active labor. Which of the following findings indicates effective uterine contractions?
Explanation
Active labor requires coordinated myometrial contractions stimulated by oxytocin to facilitate progressive cervical effacement and dilation. Effective patterns feature a frequency of 2–3 minutes, duration of 60–90 seconds, and adequate intensity with complete uterine muscle relaxation between cycles.
Rationale for correct answer:
2. Contractions every 2–3 minutes lasting 60–90 seconds demonstrate a therapeutic labor pattern. The definitive indicator of effective contractions is progressive cervical dilation and effacement. This frequency ensures adequate fetal oxygenation during the necessary uterine relaxation phase. This finding confirms appropriate labor progress.
Rationale for incorrect answers:
1. Contractions every 10 minutes lasting 20 seconds signify an inadequate pattern for active labor. This infrequent cycle is typical of the early latent phase rather than active labor. It lacks the mechanical force needed to induce cervical effacement or dilation. The nurse recognizes this requires ongoing monitoring to track labor changes.
3. Irregular contractions with no cervical change indicate false labor rather than active labor progress. True labor requires regular contractions that cause measurable cervical effacement and dilation. This finding shows the myometrium is not contracting effectively to advance delivery. The nurse anticipates further clinical evaluation regarding patient status.
4. Mild contractions every 15 minutes indicate hypotonic labor patterns that are ineffective for active labor. This low frequency and mild intensity cannot facilitate expected cervical change. The uterine force is insufficient to advance the fetal descent through the birth canal. The nurse documents this as inadequate labor progress.
Test-taking strategy:
- Analyze the scenario/question: The client is in active labor, and the nurse must identify signs of effective uterine contractions. This requires distinguishing optimal labor parameters from inadequate uterine activity or false labor signs.
- Apply Knowledge of Labor Progress: Assessment of labor requires monitoring the frequency, duration, intensity, and historical efficacy of myometrial contractions. Effective contractions in active labor must cause structural changes to the cervix while preserving uteroplacental blood flow. The nurse evaluates the frequency and duration to ensure the patient is progressing normally according to standard labor curves.
- Rule out Choice 1: This infrequent, brief pattern represents latent labor rather than active labor.
- Rule in Choice 2: A frequency of 2–3 minutes and duration of 60–90 seconds combined with progressive cervical dilation establishes true contraction efficacy.
- Rule out Choice 3: Irregularity and a lack of cervical modification are definitive biomarkers of false labor.
- Rule out Choice 4: This pattern is weak and infrequent, indicating hypotonic uterine dysfunction instead of effective labor.
Take home points
- Active labor contractions typically occur every 2–3 minutes and last 60–90 seconds.
- The definitive indicator of effective uterine contractions is progressive cervical dilation and effacement.
- Irregular contractions without cervical change indicate false labor rather than true labor.
- Inadequate or infrequent contractions during active labor signify hypotonic uterine dysfunction.
A nurse is monitoring uterine contractions using an intrauterine pressure catheter (IUPC). Which of the following findings should the nurse identify as adequate labor? Select all that apply
Explanation
Adequate labor requires coordinated myometrial activity to overcome resistance from the lower uterine segment. Quantitative evaluation utilizes an intrauterine pressure catheter to measure baseline uterine tonus and contraction intensity above baseline. Calculated Montevideo units (MVUs) provide an objective measure of adequate labor power necessary to advance cervical changes during active labor phases.
Rationale for correct answers:
1. Montevideo units calculated at 210 in 10 minutes signify adequate labor contractions. A range between 200 and 250 MVUs is the recognized physiologic threshold required for normal labor progression. This calculation validates that the uterine power is sufficient to induce cervical dilation and effacement.
2. A baseline resting tone of 10 mmHg falls perfectly within the normal physiologic range for labor. Normal resting tone should stay between 5 and 15 mmHg to maintain adequate perfusion to the fetus. This baseline confirms the myometrium relaxes completely between contractions to allow adequate oxygenation.
4. Regular contractions with an intensity greater than 50 mmHg are necessary to advance cervical dilation. True active labor requires peak contraction intensities to consistently exceed 40 to 50 mmHg above resting tone. This pressure provides the mechanical force needed for fetal descent through the birth canal.
Rationale for incorrect answers:
3. An average contraction intensity of 15 mmHg represents hypotonic dysfunction during active labor. This pressure is insufficient to alter cervical tissue or promote fetal descent since effective contractions must exceed 40 mmHg. The nurse identifies this as inadequate labor requiring clinical intervention.
5. Contractions occurring once every 15 minutes indicate severe uterine inertia during active labor. Effective labor progress requires a regular contraction frequency of 2 to 3 minutes to achieve progressive effacement. This extended interval will stall labor and represents inadequate contraction frequency.
Test-taking strategy:
- Analyze the scenario/question: The nurse is monitoring uterine contractions using an intrauterine pressure catheter to identify parameters that define adequate labor. This is a select-all-that-apply question requiring discrimination between normal physiological intrauterine pressure values and ineffective or hypertonic patterns.
- Apply Knowledge of Intrauterine Pressure Catheter Monitoring: Electronic fetal monitoring using internal pressure transducers allows for the precise quantification of uterine work. The nurse must calculate Montevideo units by summing the peak intensities of all contractions within a ten-minute window while ensuring the baseline pressure allows for normal intervillous space blood flow. Understanding these exact numbers prevents complications like uterine tachysystole or prolonged labor.
- Rule in Choice 1: A value of 210 MVUs meets the benchmark of 200 to 250 MVUs required for normal labor progress.
- Rule in Choice 2: A baseline pressure of 10 mmHg is within the normal limit of 5 to 15 mmHg, ensuring fetal safety.
- Rule out Choice 3: An intensity of 15 mmHg is too weak to cause cervical changes and indicates hypotonic labor.
- Rule in Choice 4: True active labor contractions must reach a minimum peak intensity of 50 mmHg to be effective.
- Rule out Choice 5: A frequency of once every 15 minutes is inadequate to maintain labor progress in the active phase.
Take home points
- Adequate uterine contraction power during active labor corresponds to a measurement of 200 to 250 Montevideo units.
- Normal uterine resting tone during internal monitoring must remain between 5 and 15 mmHg to preserve placental blood flow.
- Active labor contractions must exhibit a peak intensity greater than 50 mmHg to promote progressive cervical change.
- A contraction frequency of once every 15 minutes or an intensity of 15 mmHg indicates an inadequate, hypotonic labor pattern.
A nurse is caring for a client with hypertonic labor dysfunction. Which of the following should the nurse expect?
Explanation
Hypertonic labor dysfunction involves an uncoordinated myometrial hypertonicity where contractions originate outside the normal uterine pacemaker. This dysfunctional pattern produces painful uterine activity without contributing to effective mechanical force. The lack of synchronized relaxation results in elevated resting tone, which severely compromises uteroplacental perfusion and halts regular cervical progress.
Rationale for correct answer:
2. Painful, frequent contractions with minimal cervical dilation characterize hypertonic labor dysfunction. The primary defect is uncoordinated myometrial contraction that causes intense maternal pain without driving productive labor. Because these forces are erratic, they do not result in expected cervical dilation progress. The nurse expects this specific presentation during the early latent phase of labor.
Rationale for incorrect answers:
1. Regular contractions with strong intensity and rapid dilation describe a physiologic labor pattern or precipitous labor. Hypertonic dysfunction features uncoordinated, ineffective patterns rather than therapeutic or rapid dilation cycles. Strong, organized contractions indicate high uterine efficiency, which contradicts the uterine dysfunction seen in hypertonic labor states.
3. Weak contractions with prolonged labor progression describe hypotonic labor dysfunction. In hypotonic states, the contractions are regular but lack the needed amplitude and intensity to efface the cervix. The nurse differentiates this from hypertonic labor, which presents with elevated resting tone and painful, frequent contractions.
4. Complete absence of uterine contractions defines uterine atony or arrest lines. Hypertonic dysfunction represents an excess of erratic, uncoordinated muscle activity rather than a quiescent myometrium. The absolute lack of contractions is seen postpartum or during secondary uterine inertia states rather than hypertonic labor.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a client experiencing hypertonic labor dysfunction and needs to determine the expected clinical manifestations. This requires distinguishing between hypertonic patterns, hypotonic patterns, and normal labor progression.
- Apply Knowledge of Labor Progress: Assessment of dystocia requires the nurse to identify the specific phase of labor and the physiological nature of myometrial dysfunction. Hypertonic labor typically occurs in the latent phase and features elevated uterine resting tone due to multiple contraction pacemakers. Understanding these characteristics allows the nurse to prioritize appropriate therapeutic actions like promoting rest rather than administering oxytocin.
- Rule out Choice 1: Organized contractions that produce rapid dilation demonstrate normal or precipitous labor efficiency.
- Rule in Choice 2: Frequent, painful, and uncoordinated contractions that fail to change the cervix define hypertonic dysfunction.
- Rule out Choice 3: Weak, infrequent contractions that delay labor are classic indicators of hypotonic labor dysfunction.
- Rule out Choice 4: A total absence of contraction activity is not a hypertonic feature but represents uterine standstill.
Take home points
- Hypertonic labor dysfunction is characterized by frequent, uncoordinated, and painful contractions that do not produce progressive cervical dilation.
- This condition typically occurs during the early latent phase of labor and features an elevated uterine resting tone.
- Hypotonic labor dysfunction differs by presenting later in the active phase with weak, infrequent, and painless contractions.
- Therapeutic management for hypertonic labor focuses on therapeutic rest and sedation, whereas hypotonic labor often requires oxytocin augmentation.
A nurse is evaluating uterine activity. Which of the following findings indicate uterine tachysystole? Select all that apply
Explanation
Uterine tachysystole is characterized by an excessive myometrial contraction frequency that threatens fetal well-being. This condition involves shortened relaxation phases that elevate uterine resting tone, which rapidly compromises the maternal-fetal exchange. The continuous mechanical pressure reduces intervillous space perfusion during contractions, which can subsequently lead to progressive fetal hypoxemia if the pattern persists.
Rationale for correct answers:
1. More than 5 contractions in a 10-minute period satisfies the official clinical definition of uterine tachysystole. This excessive frequency prevents the placenta from refilling with freshly oxygenated maternal blood between cycles. The nurse recognizes this pattern requires immediate tracking to prevent fetal distress occurrences.
2. An internal resting tone greater than 25 mmHg indicates significant myometrial hypertonus. Normal baseline resting tone should stay between 5 and 15 mmHg to ensure adequate placental blood flow. Exceeding 25 mmHg confirms the uterus is not relaxing enough to maintain fetal oxygenation.
Rationale for incorrect answers:
3. Contractions lasting less than 30 seconds are brief and do not constitute a state of uterine hyperstimulation. Tachysystole typically involves prolonged or exceptionally frequent contractions rather than short duration cycles. Brief contractions are common in early labor and do not threaten fetal tolerance limits.
4. Decreased fetal heart rate variability is a potential clinical consequence of tachysystole rather than a component of uterine activity measurements. Tachysystole refers strictly to myometrial contraction patterns quantified via electronic monitoring, not the fetal heart monitor tracings. The nurse documents variability separately as a fetal status indicator.
5. Uterine contractions occurring every 8 minutes represent an infrequent and non-stressful labor pattern. Tachysystole requires a dense clustering of contractions, whereas an 8-minute interval provides ample time for uteroplacental perfusion. This frequency represents a normal latent or hypotonic labor phase.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing electronic fetal monitoring data to identify specific findings that meet the clinical diagnostic criteria for uterine tachysystole. This is a select-all-that-apply question requiring the nurse to differentiate between uterine contraction parameters and fetal heart rate responses.
- Apply Knowledge of Labor Progress: Evaluation of uterine contraction frequency, duration, and intensity is necessary to prevent hyperstimulation injuries. The nurse must assess the quantitative parameters of myometrial work independently from the fetal heart rate features to accurately document maternal labor patterns. Recognizing the strict boundary of 5 contractions in 10 minutes ensures safe titration of labor-inducing medications.
- Rule in Choice 1: A frequency exceeding 5 contractions in a 10-minute window matches the standard diagnostic definition of tachysystole.
- Rule in Choice 2: A resting tone greater than 25 mmHg represents hypertonus, which is an element of abnormal uterine activity.
- Rule out Choice 3: Short contractions lasting less than 30 seconds do not qualify as overstimulation or hyperactive labor.
- Rule out Choice 4: Reduced variability is a secondary fetal neurological response rather than a structural metric of uterine activity.
- Rule out Choice 5: A contraction interval of 8 minutes provides an excessive relaxation window, eliminating any risk of tachysystole.
Take home points
- Uterine tachysystole is strictly defined as more than 5 contractions within a rolling 10-minute monitoring window.
- An elevated uterine resting tone greater than 25 mmHg denotes uterine hypertonus and a lack of necessary muscle relaxation.
- Fetal heart rate changes like decreased variability are secondary outcomes of tachysystole rather than indicators of uterine activity itself.
- The primary danger of sustained tachysystole is the reduction of uteroplacental blood flow leading to progressive fetal hypoxia.
A nurse is educating a pregnant client about secondary powers. Which of the following statements indicates understanding?
Explanation
Secondary powers represent the voluntary maternal bearing-down efforts that complement primary involuntary uterine contractions during delivery. These expulsive forces utilize increased intra-abdominal pressure to successfully drive the fetus through the pelvic outlet. Proper execution of these maneuvers significantly optimizes fetal expulsion forces without prematurely depleting maternal physical reserves during the active pushing stage.
Rationale for correct answer:
2. Voluntary pushing efforts that assist in fetal expulsion accurately describe secondary powers during childbirth. Once the cervix reaches full dilation, the mother uses her abdominal muscles to enhance the expulsive forces of the uterus. This coordinated effort helps push the fetus through the birth canal during the second stage of labor. This statement confirms accurate understanding of labor physiology.
Rationale for incorrect answers:
1. Involuntary uterine contractions that occur during all stages of labor define the primary powers of childbirth. Secondary powers are strictly voluntary and do not assist until the second stage of labor begins. The involuntary contractions originate from the myometrial pacemakers and operate independently of maternal conscious effort or control.
3. Forces responsible for cervical effacement only describe the primary powers during the first stage of labor. Secondary powers have no role in thinning or dilating the cervix since they are only used after complete dilation is achieved. Their sole clinical purpose is to facilitate the mechanical descent and expulsion of the fetus.
4. Contractions occurring only before the onset of labor describe Braxton Hicks contractions or pre-labor warming signs. Secondary powers are active expulsive forces utilized exclusively during the second stage of labor to accomplish delivery. They are never present or useful prior to the true onset of labor phases.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a client's understanding of secondary powers during the labor process. The question requires identifying the statement that correctly matches the physiological definition and clinical function of secondary labor forces.
- Apply Knowledge of Labor Progress: Childbirth relies on two distinct forces known as primary and secondary powers to move the fetus through the pelvis. The nurse must differentiate between the involuntary myometrial contractions responsible for cervical preparation and the conscious abdominal pressures used for fetal delivery. Recognizing this distinction helps the nurse guide the patient on when to initiate pushing to avoid structural cervical damage.
- Rule out Choice 1: Involuntary contractions that span all labor stages represent primary powers rather than secondary powers.
- Rule in Choice 2: Conscious bearing-down maneuvers that assist in expelling the fetus correctly define secondary powers.
- Rule out Choice 3: Early mechanical changes like effacement are driven exclusively by involuntary primary uterine forces.
- Rule out Choice 4: Premature uterine tightening before active labor begins represents Braxton Hicks activity instead of expulsive powers.
Take home points
- Primary powers consist of involuntary uterine contractions that cause cervical effacement and dilation during the first stage of labor.
- Secondary powers comprise the voluntary maternal bearing-down efforts that assist in fetal expulsion during the second stage of labor.
- Initiating secondary powers before full cervical dilation can cause maternal exhaustion, cervical edema, or tissue tearing.
- Effective secondary powers utilize abdominal muscles to increase intra-abdominal pressure, enhancing the efficiency of uterine contractions.
Practice Exercise 2
A nurse is assessing a client in labor. Which of the following pelvic types is most favorable for vaginal delivery?
Explanation
The skeletal architecture of the maternal bony pelvis dictates the ease of fetal passage during parturition. Pelvic classification relies on structural variations of the pelvic inlet, midpelvis, and outlet that alter the available diameters. A wide, accommodative frame optimizes fetal presentation alignment and rotation, preventing mechanical dystocia and facilitating a normal spontaneous vaginal delivery without structural obstruction.
Rationale for correct answer:
2. A gynecoid pelvis with a rounded inlet and wide pubic arch is the most favorable anatomical shape for childbirth. This classic female pelvic type provides optimal anteroposterior and transverse diameters throughout the entire birth canal. The spacious dimensions accommodate normal fetal head rotation and descent during the second stage of labor. It occurs naturally in approximately fifty percent of women.
Rationale for incorrect answers:
1. An android pelvis with a narrow pubic arch is an unfavorable shape that mimics the male pelvic structure. The convergent side walls and narrow arch create a restricted outlet that hinders fetal descent. This shape frequently causes fetal position arrest during labor, significantly increasing the likelihood of a cesarean birth.
3. A platypelloid pelvis with a flattened inlet features a significantly shortened anteroposterior diameter that restricts entry. This rare, transverse-oval shape forces the fetal head to engage in a persistent transverse position, causing severe engagement delays at the inlet. It is highly unfavorable for standard vaginal delivery progression.
4. An anthropoid pelvis with a long anteroposterior diameter has an oval inlet that favors a persistent occiput posterior position. Although vaginal delivery is possible, the narrow transverse diameter makes it less favorable than the spacious gynecoid type. It requires extra fetal head rotation maneuvers to successfully pass through the midpelvis.
Test-taking strategy:
- Analyze the scenario/question: The nurse is identifying which maternal pelvic classification provides the most favorable anatomical dimensions for a successful vaginal delivery. This requires comparing the pelvic inlet shapes, pubic arch widths, and overall diameters of the four primary pelvic types.
- Apply Knowledge of Labor Progress: Assessment of the passenger-passage relationship requires an understanding of pelvic pelvimentry and pelvic architecture. The nurse must recognize how different bony boundaries influence fetal cardinal movements and rotation through the birth canal. Identifying the most spacious and rounded pelvis type allows the nurse to anticipate normal labor curves versus potential mechanical obstructions.
- Rule out Choice 1: The android pelvis features a heart-shaped, narrow layout that typically obstructs normal fetal descent.
- Rule in Choice 2: The gynecoid pelvis offers a completely rounded inlet and wide arch, making it anatomically ideal for delivery.
- Rule out Choice 3: The platypelloid pelvis is flattened from front to back, which prevents normal fetal head engagement.
- Rule out Choice 4: The anthropoid pelvis is elongated vertically and narrowed transversely, often leading to posterior fetal positioning.
Take home points
- The gynecoid pelvis is the most common and favorable pelvic type for vaginal delivery due to its rounded inlet and wide pubic arch.
- The android pelvis resembles the male anatomy and features a heart-shaped inlet that increases the risk of labor arrest.
- The platypelloid pelvis is flattened anteroposteriorly, which impairs the initial engagement of the fetal presenting part.
- The anthropoid pelvis features an elongated anteroposterior diameter that frequently causes the fetus to present in an occiput posterior position.
A nurse is evaluating factors affecting the passageway. Which of the following findings may impair labor progress? Select all that apply
Explanation
The birth passageway comprises the maternal bony pelvis and the distensible soft tissues of the birth canal. Structural obstructions or space-occupying masses within these boundaries compress the available diameters, creating mechanical resistance. These impediments prevent optimal fetal head engagement and descent, directly stalling labor progress and increasing the risk of dystocia during labor if uncorrected.
Rationale for correct answers:
1. A full urinary bladder creates a significant soft tissue obstruction within the anterior pelvic cavity. The distended organ physically displaces the lower uterine segment and prevents the fetus from advancing down the pelvic birth canal. The nurse anticipates this will stall cervical change progress and requires frequent bladder emptying.
2. The presence of uterine fibroids can physically distort the uterine cavity or lower segment architecture. These benign myometrial tumors reduce the functional space available for fetal descent pathways through the pelvis. Depending on their location, they can cause mechanical obstruction and prevent normal labor progression.
4. A narrow pelvic inlet imposes an immediate skeletal restriction at the very beginning of the passageway. If the initial anteroposterior or transverse diameters are inadequate, the fetal presenting part cannot achieve pelvic inlet engagement. This anatomical constraint frequently causes cephalopelvic disproportion and prolonged labor states.
Rationale for incorrect answers:
3. Multiparity typically leads to decreased soft tissue resistance and a more rapid, efficient labor progress cycle. Women who have had multiple births experience greater elasticity of the birth canal tissues, which accelerates descent. The nurse identifies this as a factor that facilitates rather than impairs fetal expulsion speeds.
5. Frequent maternal position changes optimize pelvic diameters and facilitate the mechanical rotation of the fetus. Altering positions uses gravity to expand pelvic dimensions and corrects minor fetal position misalignments during labor. This active nursing intervention promotes labor progress rather than causing any pelvic passage impairment.
Test-taking strategy:
- Analyze the scenario/question: The nurse is evaluating maternal factors affecting the passageway to identify specific findings that may impair labor progress. This is a select-all-that-apply question requiring discrimination between obstructive anatomical or soft tissue barriers and factors that facilitate normal labor.
- Apply Knowledge of Labor Progress: Assessment of the passageway requires evaluating both the rigid skeletal pelvic dimensions and the distensibility of adjacent soft tissue structures. The nurse must recognize that any mechanical obstruction within the true pelvis will disrupt the cardinal movements of labor by physically blocking the fetal presenting part. Identifying and correcting modifiable soft tissue obstructions, such as a distended bladder, is a priority nursing action to restore normal labor kinetics.
- Rule in Choice 1: A distended bladder mechanically blocks the pelvic cavity, obstructing the path of fetal descent.
- Rule in Choice 2: Myometrial fibroids create space-occupying lesions that restrict the available diameters of the birth canal.
- Rule out Choice 3: Having delivered multiple children reduces soft tissue resistance, which speeds up labor instead of hindering it.
- Rule in Choice 4: A restricted or narrow pelvic inlet directly prevents the initial engagement of the fetal head.
- Rule out Choice 5: Altering maternal positions utilizes gravitational forces to dynamically widen the pelvic outlet and enhance progress.
Take home points
- Soft tissue obstructions, such as a full urinary bladder or low-lying uterine fibroids, can mechanically impede fetal descent.
- A narrow pelvic inlet restricts the initial skeletal diameter, preventing successful engagement of the fetal presenting part.
- Multiparity generally decreases soft tissue resistance within the birth canal, leading to shorter labor durations.
- Frequent maternal position changes are a therapeutic nursing intervention that dynamically optimizes pelvic diameters to advance labor.
A nurse is assessing pelvic diameters. Which of the following is the narrowest diameter of the pelvis?
Explanation
Pelvic pelvimentry requires precise clinical evaluation of the restrictive pelvic dimensions to assess vaginal delivery feasibility. The birth canal features several critical boundaries across the inlet, midpelvis, and pelvic outlet planes. The midpelvis contains the narrowest plane of the entire pelvic canal, where the transverse midpelvic measurement serves as a major determinant for successful fetal rotation and unobstructed fetal descent.
Rationale for correct answer:
3. The interspinous diameter represents the narrowest diameter of the maternal pelvis. This transverse measurement between the ischial spine landmarks typically averages 10.5 centimeters in a normal gynecoid pelvis. It forms the tightest structural constriction the fetus must navigate during the midpelvis descent phase. A restriction here can easily cause a persistent fetal position arrest.
Rationale for incorrect answers:
1. The transverse diameter of the inlet is the widest dimension at the pelvic entry plane. Measuring approximately 13.5 centimeters, it allows ample room for the fetal head to enter the superior pelvic border transversely. The nurse differentiates this spacious upper entry from the restricted lower midpelvis dimensions located further down the canal.
2. The anteroposterior diameter of the outlet is a flexible plane that widens during active delivery. Measuring roughly 11.5 centimeters, it can expand further as the maternal coccyx bone naturally deflects posteriorly during fetal expulsion. It does not present the rigid, narrow limitation seen at the ischial spine level.
4. The diagonal conjugate is an anteroposterior measurement of the pelvic inlet. It averages 12.5 centimeters or greater and can be manually measured during a pelvic exam procedure. Since it is significantly larger than the interspinous space, it does not represent the smallest pelvic diameter boundary.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing pelvic diameters to identify the narrowest dimension of the maternal pelvis. This requires comparing specific anatomical measurements across the inlet, midpelvis, and outlet planes.
- Apply Knowledge of Labor Progress: Evaluation of the birth passageway requires the nurse to recognize specific skeletal checkpoints that can cause mechanical dystocia. The midpelvis is a rigid bony ring, and its transverse width is limited by the prominent inward projection of the ischial spines. Understanding these precise dimensions allows the nurse to anticipate when a fetus might encounter structural resistance during the descent process.
- Rule out Choice 1: The transverse inlet diameter is the largest measurement at the pelvic entrance, accommodating initial engagement.
- Rule out Choice 2: The anteroposterior outlet diameter is larger and possesses mobility due to the flexible nature of the coccyx joints.
- Rule in Choice 3: The interspinous diameter represents the absolute smallest, most rigid transverse clearance inside the true pelvis.
- Rule out Choice 4: The diagonal conjugate is an inlet measurement that provides a significantly wider clearance than the midpelvis.
Take home points
- The interspinous diameter is the narrowest diameter of the pelvis, measuring approximately 10.5 centimeters at the midpelvis plane.
- The ischial spines serve as the primary anatomical landmarks for assessing this narrowest transverse space and determining fetal station.
- The transverse diameter of the inlet is the widest diameter of the pelvic entrance, measuring roughly 13.5 centimeters.
- The anteroposterior diameter of the outlet can expand during delivery because the coccyx is pushed back by the presenting part.
A nurse is assessing soft tissue structures during labor. Which of the following findings indicate normal labor progression? Select all that apply
Explanation
Normal labor progression relies on the orderly remodeling of maternal soft tissues to facilitate fetal passage. The biochemical alterations within the cervical matrix reduce collagen density, allowing for progressive tissue compliance under the influence of regular uterine forces. The vaginal canal and surrounding pelvic floor structures must exhibit significant elastic tissue expansion to prevent mechanical lacerations and accommodate the descending fetus during the birth process.
Rationale for correct answers:
1. Cervical dilation progressing from 4 cm to 6 cm indicates the transition into the active labor phase. This progressive change confirms that the soft tissue is successfully remodeling in response to effective uterine forces. The nurse documents this finding as a key biomarker of normal labor progress speed.
2. Cervical effacement increasing to 80% reflects normal thinning and shortening of the cervical soft tissue. In primigravidas, effacement typically precedes dilation, whereas in multiparas, both processes occur concurrently. This high percentage indicates the lower uterine segment is successfully withdrawing the cervix upward.
4. Elastic vaginal expansion is a necessary physiological adaptation that permits the fetal descent pathway to open completely. The vaginal rugae stretch and flatten out due to increased tissue hypertrophy and vascularity induced by pregnancy hormones. This compliance ensures the passage accommodates the widening fetal head diameters.
Rationale for incorrect answers:
3. A rigid cervix with no dilation indicates a state of cervical ripening failure during labor. A firm, unyielding cervix resists the mechanical pressures exerted by the presenting part and uterine contractions, which stalls progress. The nurse identifies this as an abnormal finding that often requires pharmacological ripening agents.
5. Perineal resistance with no stretching indicates a rigid pelvic floor that creates an obstruction at outlet levels. Normal delivery requires the perineal body to thin out, lengthen, and stretch substantially to allow for fetal crowning. A complete lack of stretching can lead to severe soft tissue tears or prolonged second-stage labor.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing the soft tissue structures of the birth canal to identify findings that indicate normal labor progression. This is a select-all-that-apply question requiring the nurse to differentiate between adaptive tissue compliance and abnormal rigidity or resistance.
- Apply Knowledge of Labor Progress: Evaluation of the soft tissue passageway requires monitoring structural changes in the cervix, vagina, and perineum. Under the influence of estrogen, progesterone, and prostaglandins, these tissues lose their baseline rigidity and become highly distendable to allow for fetal passage. Recognizing normal patterns of effacement, dilation, and vaginal elasticity allows the nurse to confirm normal labor curves and identify early signs of soft tissue dystocia.
- Rule in Choice 1: A change from 4 cm to 6 cm signifies appropriate progress into the active phase of labor.
- Rule in Choice 2: An increase to 80% effacement demonstrates effective thinning of the lower uterine segment.
- Rule out Choice 3: Uterine contractions matching a firm, unchanged cervix point toward a rigid cervix or a lack of ripening.
- Rule in Choice 4: The natural stretching and widening of the vaginal walls represent normal, expected soft tissue elasticity.
- Rule out Choice 5: A complete lack of perineal stretching creates an absolute soft tissue barrier that delays the expulsion stage.
Take home points
- Normal labor progress is characterized by progressive cervical dilation and effacement driven by regular uterine contractions.
- Hormonal changes during pregnancy increase the elasticity of the vaginal tissues, allowing the birth canal to expand during descent.
- A rigid, unyielding cervix that fails to dilate under contraction pressure represents a soft tissue barrier that can stall labor.
- The perineum must stretch and thin out during the second stage of labor to accommodate the fetal presenting part during crowning.
A nurse is educating a client about pelvic anatomy. Which of the following statements indicates understanding?
Explanation
Pelvic anatomy is divided by the linea terminalis into the superior false pelvis and the inferior true pelvis structure. While the upper portion supports the expanding pregnant uterus, only the lower bony basin acts as the restrictive birth canal. The anatomical dimensions of this inner ring determine the spatial constraints, guiding the fetal presentation alignment and rotation necessary for a successful spontaneous vaginal delivery.
Rationale for correct answer:
2. The statement that the true pelvis is the part involved in childbirth indicates accurate client understanding. This lower bony canal consists of the inlet, midpelvis, and outlet through which the fetus must successfully navigate. Its precise structural diameters dictate whether the passenger can pass safely during the second stage of labor. This boundary represents the true obstetrical birth canal.
Rationale for incorrect answers:
1. The statement that the false pelvis forms the birth canal reflects an incorrect anatomical understanding. The false pelvis is the shallow superior portion situated above the pelvic brim that merely supports the growing uterus. It plays no mechanical role in directing fetal descent pathways or forming the actual boundaries of the birth canal.
3. The statement that the pelvic inlet is the exit of the birth canal confuses the pelvic entry point with its exit. The pelvic inlet represents the upper boundary where the fetal head must first engage to enter the true pelvis. The actual exit of the birth canal is the pelvic outlet, located at the lowest plane.
4. The statement that the coccyx does not play a role in labor overlooks its physiological mobility attributes. During the expulsive phase of delivery, the coccyx naturally deflects posteriorly to increase the anteroposterior diameter of the outlet. If this bone is rigid or fused, it can cause mechanical outlet obstruction.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a client's understanding of pelvic anatomy relevant to the childbearing process. The question requires identifying the specific statement that correctly differentiates between the anatomical divisions and functional planes of the maternal pelvis.
- Apply Knowledge of Labor Progress: Evaluation of the birth passageway requires a clear structural distinction between the false pelvis and the true pelvis. The nurse must recognize that the true pelvis is the rigid, osseous ring that poses the actual mechanical challenge to the descending fetus during parturition. Educating the patient on how these structures operate helps clarify the physiological path the fetus takes during the cardinal movements of labor.
- Rule out Choice 1: The false pelvis sits above the pelvic brim and acts as a support basin rather than forming the birth canal.
- Rule in Choice 2: The true pelvis is the lower anatomical division that directly encompasses the path of childbirth.
- Rule out Choice 3: The pelvic inlet represents the superior entrance into the true pelvis, not the exit of the canal.
- Rule out Choice 4: The coccyx plays a vital role by moving backward during crowning to widen the available outlet diameter.
Take home points
- The true pelvis is the lower portion of the pelvis that forms the actual bony birth canal involved in childbirth.
- The false pelvis is the upper area above the linea terminalis that supports the pregnant uterus but does not affect fetal descent boundaries.
- The pelvic inlet serves as the upper entrance into the true pelvis, whereas the pelvic outlet forms the lower exit plane.
- The coccyx is a mobile bone that deflecting posteriorly during the second stage of labor to increase the outlet's diameter.
Practice Exercise 3
A nurse is assessing a client in labor. Which of the following fetal positions is most favorable for vaginal delivery?
Explanation
Optimal fetal positioning facilitates the efficient progression of labor by minimizing the presenting diameters of the fetal head configuration. The cephalic presentation allows the smallest vertex diameter to adapt directly to the maternal pelvis, promoting regular cervical mechanical pressure and effacement. Proper alignment of the fetal occiput with the anterior maternal pelvis prevents prolonged labor, reduces maternal back pain, and optimizes the cardinal movements pathway required for an uncomplicated vaginal birth.
Rationale for correct answer:
2. The left occiput anterior position is the most favorable anatomical alignment for vaginal delivery. In this position, the fetal occiput faces the left anterior quadrant of the maternal pelvis, allowing the smallest suboccipitobregmatic head diameter to enter the inlet. This alignment fits perfectly into the spacious gynecoid pelvic curves, which drastically reduces the risk of labor dystocia complications. It represents the most common and ideal delivery position.
Rationale for incorrect answers:
1. The occiput posterior position is an unfavorable alignment often referred to as a sunny-side-up presentation. In this layout, the fetal hard skull presses directly against the maternal sacrum, inducing severe back labor pain. This position features a wider presenting diameter that significantly prolongs the second stage of labor and increases cesarean rates.
3. The right occiput posterior position is a malposition that impairs normal fetal rotation mechanisms. The fetus must rotate a full 135 degrees to reach an anterior position, which frequently causes a persistent posterior arrest. The nurse anticipates this configuration will cause prolonged labor progression and extensive maternal exhaustion during pushing.
4. A transverse lie with shoulder presentation represents an impossible configuration for a standard spontaneous vaginal delivery. The long axis of the fetus lies perpendicular to the maternal spine, meaning the fetus cannot enter the pelvic inlet ring. The nurse recognizes this dangerous presentation requires an immediate cesarean section delivery.
Test-taking strategy:
- Analyze the scenario/question: The nurse is identifying the specific fetal position that is most anatomically favorable for a successful vaginal delivery. This requires evaluating different fetal orientations relative to the quadrants of the maternal pelvis.
- Apply Knowledge of Labor Progress: Assessment of the passenger-passageway relationship requires an understanding of fetal presentation, position, and lie. The nurse must recognize that anterior cephalic positions allow the fetal head to flex fully, presenting the smallest possible diameter to the pelvic brim. Identifying these optimal relationships allows the nurse to anticipate smooth labor progress versus mechanical obstructions that delay delivery.
- Rule out Choice 1: The occiput posterior orientation places the fetal head in an extended position, creating a wider presenting diameter and severe back pain.
- Rule in Choice 2: The left occiput anterior position aligns the fetus perfectly with maternal anatomy, making it the most favorable layout.
- Rule out Choice 3: A right occiput posterior position constitutes a malposition that requires extensive internal rotation, stalling labor.
- Rule out Choice 4: A transverse lie with a presenting shoulder is a mechanical impossibility for vaginal birth, requiring surgical intervention.
Take home points
- The left occiput anterior position is the most common and favorable fetal orientation for a smooth vaginal delivery.
- Occiput posterior positions cause intense maternal back labor due to the fetal skull pressing directly against the sacrum.
- Fetal malpositions like occiput posterior present wider head diameters to the pelvis, which significantly prolongs the labor process.
- A transverse lie with a shoulder presentation cannot be delivered vaginally and necessitates an immediate cesarean birth.
A nurse is evaluating fetal lie and presentation. Which of the following findings indicate abnormal conditions? Select all that apply
Explanation
Fetal orientation within the uterine cavity is determined by comparing the fetal long axis to the maternal spinal column. A misalignment of these structural lines creates mechanical barriers that impede normal engagement and descent. These variations establish malpresentation during labor, which prevents the smallest cranial diameters from adapting to the pelvic inlet, significantly increasing the risk of umbilical cord prolapse and mechanical dystocia.
Rationale for correct answers:
1. A transverse lie represents an abnormal condition where the fetus lies perpendicular to the maternal spine. The presenting part is typically the shoulder, making a spontaneous vaginal delivery mechanically impossible. The nurse recognizes that this dangerous configuration requires surgical intervention to prevent uterine rupture risks during active labor.
3. A breech presentation indicates an abnormal condition where the buttocks or feet enter the pelvic inlet first. This presentation creates significant risks because the largest fetal part, the head, is delivered last and can become trapped in the maternal bony pelvis. This trapping leads to severe fetal hypoxia complications due to umbilical cord compression.
5. An oblique lie is an unstable, abnormal condition where the fetal axis crosses the maternal spine at an angle. This position is usually transient and typically converts into either a longitudinal or transverse lie as active labor progresses. It prevents proper fetal head engagement and requires close monitoring by the medical team.
Rationale for incorrect answers:
2. A longitudinal lie is a normal physiological finding where the fetal spine runs parallel to the maternal spine. This alignment is standard for childbirth and allows the fetus to enter the pelvic inlet plane vertically. The nurse identifies this layout as a requirement for achieving a safe vaginal delivery progress path.
4. A cephalic presentation is the most common and favorable condition where the head presents to the birth canal. This orientation allows the fetal skull to exert even, constructive mechanical pressure against the cervix to promote dilation. It represents the ideal presentation pattern for an uncomplicated, normal delivery process.
Test-taking strategy:
- Analyze the scenario/question: The nurse is evaluating fetal lie and presentation to identify specific findings that indicate abnormal maternal-fetal conditions. This is a select-all-that-apply question requiring discrimination between physiological, delivery-compatible orientations and pathological malpresentations.
- Apply Knowledge of Labor Progress: Assessment of the passenger requires analyzing the spatial relationship between the fetal long axis and the maternal birth canal. The nurse must recognize that any deviation from a parallel longitudinal lie or a vertex cephalic presentation introduces a mechanical obstruction that halts standard delivery pathways. Identifying these malpositions early allows the nurse to anticipate specialized obstetric maneuvers, external cephalic versions, or preparation for operative delivery.
- Rule in Choice 1: A transverse lie positions the fetus horizontally across the uterus, which completely blocks the pelvic inlet.
- Rule out Choice 2: A longitudinal lie aligns the fetal spine parallel to the mother, which is the normal position for delivery.
- Rule in Choice 3: A breech presentation reverses the normal fetal poles, bringing the lower extremities or pelvis into the inlet first.
- Rule out Choice 4: A cephalic presentation positions the fetal head down toward the birth canal, representing normal labor anatomy.
- Rule in Choice 5: An oblique lie places the fetus at an un-engageable angle, making it an unstable and abnormal labor finding.
Take home points
- A longitudinal lie combined with a cephalic presentation represents the normal and most favorable configuration for vaginal delivery.
- A transverse lie places the fetus perpendicular to the maternal spine and necessitates a cesarean delivery because the shoulder blocks the airway.
- Breech presentations involve the fetal buttocks or feet presenting first, which carries a high risk of umbilical cord prolapse and head entrapment.
- An oblique lie features a diagonal fetal axis that is unstable and must convert to a longitudinal lie for a safe vaginal birth to occur.
A nurse is assessing fetal station. Which of the following findings indicates engagement?
Explanation
Fetal station measures the relative descent of the fetal presenting part through the maternal birth canal. This assessment utilizes the narrowest plane of the midpelvis to gauge spatial progress and track movement. Achieving fetal head engagement confirms that the largest biparietal diameter has successfully passed through the pelvic inlet, providing a key clinical benchmark that rules out cephalopelvic disproportion risks and indicates that the passenger is structurally committed to the true obstetric canal.
Rationale for correct answer:
2. Station 0 indicates that the fetal presenting part has reached the level of the ischial spines, confirming fetal head engagement. At this point, the narrowest transverse plane of the midpelvis has been navigated successfully. This finding represents a crucial milestone in labor because it demonstrates the fetus can fit through the pelvic inlet border. The nurse documents this position as engaged labor progress.
Rationale for incorrect answers:
1. Station -3 signifies that the presenting part is located 3 centimeters above the ischial spines, meaning the fetus remains unengaged and floating. The fetal head has not yet entered the midpelvis ring to begin its true descent. The nurse recognizes that the passenger is still high within the false pelvis basin at this monitoring stage.
3. Station -5 indicates that the fetal presenting part is positioned 5 centimeters above the ischial spines, reflecting a completely unengaged floating fetus. This finding is common prior to the onset of active labor or before cervical membranes rupture. It confirms the presenting part sits entirely above the entry level of the superior pelvic inlet.
4. Station -2 indicates that the presenting part is 2 centimeters above the ischial spines, which means the head is partially descended but not yet engaged. While progress has occurred from higher stations, the widest part of the skull has not cleared the pelvic brim. The fetus is still considered unengaged until it reaches the ischial spine level.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a client's fetal station during labor to identify the specific numerical finding that indicates engagement has occurred. This requires understanding the scoring system used to measure descent relative to maternal pelvic landmarks.
- Apply Knowledge of Labor Progress: Evaluation of fetal station uses the rigid ischial spines of the maternal midpelvis as the designated zero benchmark. Stations above these bony projections are assigned negative numbers from -1 down to -5, while stations below are designated with positive numbers from +1 up to +5. The nurse must recognize that engagement corresponds exactly to a station of zero, which confirms the largest transverse diameter of the fetal skull has cleared the inlet.
- Rule out Choice 1: A station of -3 indicates the fetus remains high and unengaged within the pelvic basin.
- Rule in Choice 2: A station of 0 confirms the presenting part aligns with the ischial spines, satisfying the criteria for engagement.
- Rule out Choice 3: A station of -5 demonstrates the fetus is completely floating and unengaged above the pelvic brim.
- Rule out Choice 4: A station of -2 shows the fetus has descended slightly but remains unengaged above the zero benchmark line.
Take home points
- Fetal station is evaluated in centimeters using the maternal ischial spines as the central anatomical zero landmark.
- Station 0 indicates that the fetal presenting part has reached the ischial spines, signaling that engagement has occurred.
- Negative station numbers indicate the fetus is unengaged and floating above the level of the midpelvis spines.
- Positive station numbers signify that the fetus is descending further through the true pelvis toward the vaginal outlet for birth.
A nurse is monitoring labor progress. Which of the following are cardinal movements of labor? Select all that apply
Explanation
The positional alterations that the fetus undergoes during its journey through the birth canal are defined as the cardinal movements pathway. These passive modifications allow the fetus to adapt its structural dimensions to the changing diameters of the maternal bony pelvis. This precise sequence of rotations and deflections minimizes mechanical friction, maximizing pelvic clearance efficiency and facilitating a smooth progression toward delivery.
Rationale for correct answers:
1. Internal rotation is a critical cardinal movement that aligns the long axis of the fetal head with the maternal pelvic outlet plane. The fetus typically turns from a transverse position to an occiput anterior position to clear the midpelvis. The nurse monitors this change as a requirement for successful fetal descent.
2. Flexion occurs as the descending fetal head meets resistance from the maternal soft tissues or pelvic floor muscles. This resistance forces the fetal chin to touch the chest, presenting the smallest cranial diameter to the birth canal. This mechanical adaptation is essential for unobstructed pelvic passage.
4. Extension takes place when the fetal occiput passes under the maternal pubic arch, allowing the head to emerge. The combined forces of the uterine contractions and pelvic floor resistance push the face upward and out of the vaginal outlet boundary. The nurse supports this movement to prevent perineal tissue tears.
5. External rotation occurs immediately after the head is born, as the shoulders rotate internally to align anteroposteriorly within the pelvis. The fetal head turns sideways to realign naturally with the fetal torso axis. This step allows the shoulders to clear the maternal pubic bone safely.
Rationale for incorrect answers:
3. Retraction describes a specialized behavior of the upper uterine muscle segment during contractions, not a positional change made by the fetus. Myometrial fibers permanently shorten during labor to pull the lower uterine segment upward and advance cervical effacement progress. The nurse documents this under uterine contraction mechanics.
Test-taking strategy:
- Analyze the scenario/question: The nurse is tracking labor progress and must identify which of the listed physical adaptations constitute true cardinal movements of labor. This is a select-all-that-apply question that requires distinguishing fetal positional changes from maternal uterine muscle behaviors.
- Apply Knowledge of Labor Progress: Assessment of the passenger during delivery involves understanding the exact chronological sequence of positional adjustments the fetus makes to escape the birth canal. The standard sequence encompasses engagement, descent, flexion, internal rotation, extension, external rotation, and expulsion. The nurse must recognize that these steps reflect the passive mechanical movement of the fetus adapting to the maternal pelvic geometry rather than active actions or uterine muscle properties.
- Rule in Choice 1: Internal rotation alters the fetal head alignment from transverse to anteroposterior within the maternal midpelvis.
- Rule in Choice 2: Flexion minimizes the presenting skull dimensions by tucking the chin down against the chest.
- Rule out Choice 3: Retraction is a physiological property of myometrial muscle fibers that thins the lower uterine segment.
- Rule in Choice 4: Extension allows the fetal head to sweep upward over the perineum using the pubic bone as a pivot point.
- Rule in Choice 5: External rotation occurs after delivery of the head to align the biacromial diameter with the pelvic outlet.
Take home points
- The cardinal movements of labor represent the passive positional changes that the fetus undergoes to navigate the birth canal.
- Flexion reduces the presenting diameter of the fetal skull, while extension allows the head to exit under the pubic arch.
- Internal and external rotations align the fetal head and shoulders with the widest available diameters of the maternal pelvis.
- Uterine retraction is a maternal muscular property that shortens myometrial fibers and must not be confused with fetal positional movements.
A nurse is palpating fetal skull sutures during labor. Which of the following is the significance of sutures?
Explanation
The unossified cranial bones of the fetal skull configuration are separated by membranous spaces called sutures. These flexible connections eliminate structural rigidity, permitting the shifting of cranial plates under the influence of regular uterine forces. This protective mechanism enables fetal head molding to compress the presenting diameters, successfully reducing mechanical resistance and facilitating an unobstructed transit through the narrow maternal bony pelvis during delivery.
Rationale for correct answer:
2. The primary significance of sutures is that they allow molding of the fetal head to facilitate passage. The flexible, membranous pathways permit the cranial bones to overlap slightly when subjected to pressure from the birth canal walls. This adaptation temporarily reduces the skull diameter, enabling the passenger to safely navigate the bony pelvic ring. This finding represents a vital protective neonatal birth mechanism.
Rationale for incorrect answers:
1. Sutures do not prevent fetal head movement during labor; rather, they directly enhance structural flexibility. If the cranial bones were rigidly fused, the head could not flex or rotate within the maternal pelvic space. The nurse knows that fixed plates would result in permanent mechanical labor arrest complications.
3. Sutures are designed to decrease rather than increase fetal head rigidity during the birthing process. Their physiological elasticity ensures the skull can change shape safely without causing damage to the fetal brain tissue. Increased rigidity is a pathological state seen in premature craniosynostosis conditions before delivery.
4. Cranial sutures are universal anatomical structures that cannot determine fetal gender under any clinical circumstances. The palpable patterns of the fontanels and sutures help the nurse identify fetal position orientations instead of sex characteristics. Gender is determined exclusively by genetic factors and verified via ultrasound visualization methods.
Test-taking strategy:
- Analyze the scenario/question: The nurse is palpating the fetal skull sutures during an internal exam to identify the physiological significance of these structures. This requires understanding how neonatal cranial anatomy adapts dynamically to the birth canal.
- Apply Knowledge of Labor Progress: Assessment of the passenger requires an understanding of how the fetal skull interacts with the maternal pelvis. The skull contains multiple bones separated by sagittal, frontal, coronal, and lambdoidal sutures that intersect at the fontanels. The nurse must recognize that these pliable gaps allow the head to mold and change shape to match the pelvic diameters, reducing maternal-fetal trauma during the descent phase.
- Rule out Choice 1: Gaps between the skull bones increase rather than prevent the mobility required for positional adjustments.
- Rule in Choice 2: Sutures provide the structural pliability needed for molding, which reduces the presenting diameter of the head.
- Rule out Choice 3: Rigidity would act as a severe mechanical barrier, whereas sutures provide necessary compliance during labor.
- Rule out Choice 4: Palpating cranial landmarks serves to identify fetal position and station, having no link to fetal gender.
Take home points
- Cranial sutures are membranous spaces that separate the bones of the fetal skull, allowing the head to change shape during labor.
- Molding is the temporary overlapping of fetal skull bones that reduces head diameters to facilitate passage through the pelvis.
- Palpation of the sutures and fontanels during a vaginal examination helps the nurse identify fetal presentation and position.
- Increased rigidity of the fetal skull due to premature fusion of sutures can result in cephalopelvic disproportion and delayed labor progress.
Practice Exercise 4
A nurse is caring for a client in labor. Which of the following maternal responses indicates a positive psychological state?
Explanation
Maternal adaptation to parturition relies heavily on effective emotional coping and positive psychological response mechanisms. High anxiety levels induce a sympathetic fight-or-flight reaction, causing an excessive release of maternal catecholamine secretions like epinephrine and cortisol. This hormonal surge diverts blood flow away from the uterus, which subsequently impairs myometrial contraction efficiency and reduces overall placental perfusion during labor progress.
Rationale for correct answer:
2. Demonstrating controlled breathing and cooperative behavior indicates a positive psychological state during childbirth. This structured focus shows that the client is successfully utilizing cognitive coping strategies to manage labor discomfort. Maintaining behavioral control reduces the overall stress response, which preserves uterine tissue perfusion and facilitates normal labor progression.
Rationale for incorrect answers:
1. Expressing fear and inability to cope signifies a state of emotional distress and maternal exhaustion development. Uncontrolled anxiety triggers muscle tensing, which intensifies pain perception and disrupts normal labor rhythms. The nurse identifies this as a barrier that often requires therapeutic nursing interventions to restore calm.
3. Refusing all assistance from the health care team indicates withdrawal or a profound loss of control. This protective reaction frequently masks severe fear, panic, or a lack of trust in the environment. The nurse recognizes that a complete refusal of care compromises patient safety and reflects ineffective coping styles.
4. Exhibiting increased muscle tension and panic demonstrates severe psychological distress and physiological hyperarousal. Panic states cause hyperventilation, which disturbs maternal acid-base balance parameters and reduces fetal oxygenation. This somatic response directly hinders progress by increasing systemic resistance against fetal descent pathways.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a laboring client to identify a maternal response that indicates a positive psychological state. This requires distinguishing adaptive, organized coping mechanisms from maladaptive emotional responses like panic or withdrawal.
- Apply Knowledge of Labor Progress: Evaluation of the psychological power during labor involves assessing maternal anxiety levels, coping behaviors, and support structures. The nurse must recognize that excessive maternal stress triggers a profound neuroendocrine cascade that can stall active labor progress. Confirming that a patient remains calm and follows structured breathing patterns allows the nurse to validate that the psychological component of labor is supporting rather than hindering delivery.
- Rule out Choice 1: Vocalizing an inability to handle contractions is a classic sign of severe distress and coping failure.
- Rule in Choice 2: Exhibiting regulated breathing and working with the staff directly signals excellent psychological adaptation.
- Rule out Choice 3: Defiant withdrawal or a total rejection of clinical support points to an overwhelmed emotional state.
- Rule out Choice 4: Tonic muscle contraction and visible panic indicate a high sympathetic response that impairs labor kinetics.
Take home points
- A positive maternal psychological state is characterized by controlled coping behaviors, relaxation between contractions, and active collaboration with care providers.
- High maternal anxiety causes an overproduction of catecholamines, which can weaken uterine contractions and prolong labor duration.
- Emotional distress can decrease blood flow through the placenta, leading to a higher incidence of non-reassuring fetal heart rate patterns.
- Providing continuous labor support, encouraging breathing techniques, and maintaining a calm environment are essential to optimize psychological outcomes.
A nurse is assessing the effects of anxiety during labor. Which of the following findings should the nurse expect? Select all that apply
Explanation
Severe anxiety during labor triggers a profound sympathetic nervous system response that disrupts normal parturition physiology curves. The resulting neuroendocrine cascade activates the adrenal medulla, leading to an immediate surge in maternal catecholamine levels. This systemic chemical response alters systemic vascular resistance, redirecting blood away from reproductive organs, which subsequently impairs myometrial contraction patterns and degrades the overall intrauterine environment.
Rationale for correct answers:
1. Increased catecholamine release occurs as a direct physiological consequence of maternal anxiety and fear. The body treats labor distress as a fight-or-flight crisis, flooding the circulation with epinephrine and norepinephrine. The nurse expects this hormonal shift to disrupt normal uterine efficiency and elevate maternal heart rate metrics.
2. Decreased uterine blood flow happens because elevated norepinephrine triggers widespread vasoconstriction of the uterine arterioles. This vascular tightening restricts blood movement through the intervillous space pathways, directly reducing the supply of essential nutrients. This reduction impairs the placenta's ability to support the metabolic demands of active labor progress.
4. Increased perception of pain is a well-documented psychological and somatic result of high anxiety states. Fear lowers the baseline maternal pain threshold and limits the production of natural endorphin secretions. This amplification makes each contraction feel significantly more intense, accelerating physical and maternal emotional exhaustion.
Rationale for incorrect answers:
3. Enhanced oxytocin activity is not expected; instead, high adrenaline levels directly inhibit endogenous oxytocin hormone release. The uncoordinated sympathetic firing interferes with the regular uterine pacemakers, stalling normal cervical dilation progress. This inhibition leads to prolonged labor or secondary uterine inertia states.
5. Improved fetal oxygenation is incorrect because maternal vasoconstriction directly causes a decline in fetal oxygen status. The restriction of blood flow through the umbilical vessels compromises gas exchange, predisposing the fetus to hypoxic stress. The nurse frequently notes this decline as non-reassuring heart decelerations.
Test-taking strategy:
- Analyze the scenario/question: The nurse is analyzing the physiological and psychological impacts of severe maternal anxiety on the labor process. This is a select-all-that-apply question requiring the identification of the negative systemic changes associated with a high-stress sympathetic response.
- Apply Knowledge of Labor Progress: Assessment of psychological factors requires the nurse to understand how maternal emotions influence neuroendocrine pathways. Severe anxiety shifts the body's metabolic priorities, using catecholamines to clamp down pelvic vasculature while suppressing the posterior pituitary gland's regular hormone secretion. Recognizing these maladaptive changes allows the nurse to prioritize therapeutic calming techniques to restore normal uterine perfusion.
- Rule in Choice 1: High stress states immediately activate the maternal adrenal glands, causing an overproduction of catecholamines.
- Rule in Choice 2: Sympathetic vasoconstriction reduces blood volume passing through the uterine vessels, threatening placental function.
- Rule out Choice 3: Adrenaline acts as a direct physiological antagonist to oxytocin, reducing rather than enhancing contraction power.
- Rule in Choice 4: Anxiety amplifies the central nervous system's processing of nociceptive signals, worsening the maternal pain experience.
- Rule out Choice 5: Reduced placental blood flow inevitably diminishes rather than improves the available fetal oxygen supply.
Take home points
- Maternal anxiety triggers a sympathetic fight-or-flight response, causing an excessive release of epinephrine and norepinephrine.
- High catecholamine levels cause pelvic vasoconstriction, which directly decreases uterine blood flow and placental perfusion.
- Stress hormones inhibit endogenous oxytocin secretion, which can lead to uncoordinated or ineffective uterine contraction patterns.
- Elevated anxiety lowers maternal pain tolerance and compromises fetal oxygenation, increasing the risk of non-reassuring fetal heart rates.
A nurse is providing culturally competent care. Which of the following actions is most appropriate?
Explanation
Culturally competent care requires an adaptive approach to maternal healthcare delivery that respects the diverse values of the laboring client. Culturally specific rituals, modesty requirements, and gender preferences profoundly influence how a patient experiences pain and interacts with medical staff. Incorporating these variations into the care plan reduces maternal psychological stress, enhances trust, and fosters a supportive environment that optimizes labor coping efficiency.
Rationale for correct answer:
2. Assessing the client's individual cultural preferences is the most appropriate nursing action to provide tailored care. Every patient possesses unique cultural beliefs regarding support persons, pain expression, and postpartum healing rituals. Rather than relying on generalizations, the nurse must perform an individual assessment to safely modify the care plan. This inquiry ensures culturally congruent interventions that enhance the patient's labor experience.
Rationale for incorrect answers:
1. Applying standard care regardless of cultural beliefs represents a prescriptive approach that results in cultural blindness complications. Ignoring unique traditions can alienate the childbearing family and increase maternal anxiety levels during delivery. The nurse must balance clinical safety protocols with individualized care rather than practicing completely inflexible nursing care.
3. Ignoring family involvement in labor violates the social structure and support networks common in many diverse cultural groups. Many traditions designate specific family members to manage the birthing environment and offer essential emotional strength. Disregarding these support persons strips the client of her chosen coping assistance resources.
4. Enforcing hospital routines without explanation demonstrates institutional ethnocentrism and disregards maternal autonomy rights. Demanding strict compliance with rigid, unexplained protocols can induce panic and feelings of helplessness in the patient. The nurse must communicate transparently to bridge gaps between clinical necessities and personal cultural practices.
Test-taking strategy:
- Analyze the scenario/question: The question asks the nurse to select the most appropriate action for providing culturally competent care to a client in labor. This requires identifying an action that prioritizes individualized assessment over rigid institutional compliance or cultural assumptions.
- Apply Knowledge of Labor Progress: Providing holistic care during labor requires balancing critical clinical milestones with the patient's psychosocial and cultural needs. The nurse must recognize that cultural beliefs directly dictate maternal pain expression, position choices, and the preferred role of support persons in the delivery room. Conducting a targeted cultural assessment on admission allows the nurse to co-create a safe, respectful environment that minimizes catecholamine-induced labor delays.
- Rule out Choice 1: Utilizing a uniform approach to care disregards individual client needs and compromises the therapeutic relationship.
- Rule in Choice 2: Performing an individualized cultural assessment is the essential first step to delivering customized, respectful maternity care.
- Rule out Choice 3: Shunning family support blocks vital emotional resources that are central to many cultural birthing practices.
- Rule out Choice 4: Imposing clinical routines without dialogue creates an adversarial atmosphere that increases maternal stress and resistance.
Take home points
- Cultural competence in maternity nursing begins with a direct, individualized assessment of the client's specific birthing preferences and values.
- Cultural practices profoundly influence maternal pain expression, the choice of support persons, and desired postpartum rituals.
- Imposing rigid hospital routines without explaining the clinical rationale can cause cultural conflict and increase maternal anxiety.
- Integrating safe cultural traditions into the labor plan promotes emotional comfort, lowers stress hormones, and supports physiologic labor progress.
A nurse is implementing interventions to promote a positive psyche. Which of the following actions should the nurse include? Select all that apply
Explanation
Promoting a positive maternal psyche requires targeted nursing interventions aimed at reducing stress-induced sympathetic nervous system activation. By keeping maternal anxiety at bay, the nurse prevents the excessive release of catecholamines (epinephrine and norepinephrine), which are known to cause uterine vasoconstriction and weaken contractions. Providing structured coping mechanisms and a supportive environment helps maintain normal uterine blood flow, preserves oxytocin efficiency, and fosters an empowering birth experience.
Rationale for correct answers:
1. Encouraging relaxation breathing techniques gives the client an active, structured focus to navigate contractions. Controlled breathing patterns stimulate the parasympathetic nervous system, lowering the heart rate and reducing muscle tension. This directly alters the central processing of labor discomfort, decreasing the overall perception of pain.
2. Providing continuous reassurance builds a strong therapeutic alliance and directly counters feelings of helplessness or fear. Ongoing verbal and emotional support validates the client's efforts, lowering anxiety levels and stabilizing her psychological coping mechanisms during challenging phases of labor.
4. Maintaining a calm and quiet environment minimizes external sensory triggers that can exacerbate a panic or stress response. Dimming lights, controlling room traffic, and reducing noise preserve a peaceful space that encourages natural endorphin production and allows the client to rest effectively between contractions.
Rationale for incorrect answers:
3. Limiting communication to avoid overstimulation is inappropriate because it can cause the client to feel isolated, abandoned, or uninformed. While communication should be clear and calm, maintaining open, supportive dialogue is essential for answering questions, offering guidance, and ensuring the client feels safe.
5. Using authoritative communication to ensure compliance fosters an adversarial environment and strips the client of her maternal autonomy. Dominant, demanding tones increase psychological distress, elevate stress hormone levels, and can cause a client to withdraw or experience a loss of control.
Test-taking strategy:
- Analyze the scenario/question: The nurse is selecting interventions specifically designed to promote a positive psychological state (psyche) for a laboring client. This is a select-all-that-apply question requiring the identification of supportive, calming, and anxiety-reducing care techniques.
- Apply Knowledge of Labor Progress: Managing the psychological "power" of labor involves reducing the maternal fight-or-flight response. The nurse must recognize that interventions enhancing a patient's sense of safety, control, and comfort will directly optimize physiological labor progress by preventing catecholamine-induced uterine inertia.
- Rule in Choice 1: Regulated breathing patterns actively reduce muscle tension and soothe the central nervous system.
- Rule in Choice 2: Consistent, positive feedback preserves maternal confidence and prevents emotional exhaustion.
- Rule out Choice 3: Cutting off communication isolates the patient and can breed further anxiety and confusion.
- Rule in Choice 4: A serene physical environment reduces external stressors, supporting focus and relaxation.
- Rule out Choice 5: Demanding compliance through strict authority increases client stress and triggers a defensive emotional response.
Take home points
- Nursing actions that promote a positive psyche directly improve labor physiology by mitigating the vasoconstrictive effects of maternal stress hormones.
- Continuous emotional support and reassurance help the client maintain behavioral control and reduce overall pain perception.
- Relaxation breathing techniques serve as an effective cognitive-behavioral tool that lowers systemic tension during contractions.
- Creating a calm, predictable environment supports the natural, rhythmic progression of labor by enhancing comfort and safety.
A nurse is explaining the role of support systems during labor. Which of the following statements indicates understanding?
Explanation
The presence of a continuous support system—whether a partner, family member, or doula—exerts a powerful influence on the neuroendocrine regulation of labor. Continuous labor support significantly lowers maternal stress, which limits the production of catecholamines (epinephrine and norepinephrine). Because high levels of these stress hormones can disrupt normal uterine contractility and intensify nociceptive (pain) signaling, an effective support system helps preserve physiological labor efficiency and enhances the laboring client's natural pain tolerance.
Rationale for correct answer:
2. The statement that continuous support can reduce the need for analgesia indicates an accurate understanding of labor support. Clinical evidence consistently demonstrates that one-on-one emotional and physical support lowers the client's anxiety and alters their central perception of pain. This psychological buffering frequently decreases the maternal demand for pharmacological interventions, including epidurals and systemic opioid analgesics.
Rationale for incorrect answers:
1. The statement that support persons increase labor duration is fictional. Continuous support is associated with shorter labor durations. By fostering relaxation and maintaining a calm environment, support systems help optimize endogenous oxytocin secretion, which facilitates steady cervical dilation and efficient fetal descent.
3. The statement that support systems have no effect on labor outcomes ignores established obstetric data. Continuous intrapartum support is linked to improved clinical metrics, including a reduced incidence of instrumental vaginal deliveries (forceps or vacuum assistance), lower cesarean birth rates, and higher five-minute Apgar scores for the newborn.
4. The statement that only medical staff should provide support during labor represents an outdated and restrictive approach to maternity care. While clinical staff manage safety and medical interventions, they often have split responsibilities across multiple patients. Lay support persons provide uninterrupted, personalized companionship that fulfills distinct psychosocial comfort needs that medical personnel cannot always supply.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a client's or family member's understanding of how support systems alter the labor experience. The question requires selecting the option that correctly identifies the positive clinical and psychological impacts of continuous labor support.
- Apply Knowledge of Labor Progress: Evaluating the "psyche" component of labor requires the nurse to recognize that emotional safety directly translates to physiological ease. Uninterrupted labor support mitigates the fight-or-flight cascade, ensuring that uterine blood flow remains uncompromised. Recognizing the evidence-based benefits of doulas and birth partners allows the nurse to seamlessly integrate these support figures into the active care plan.
- Rule out Choice 1: Continuous support actively streamlines and shortens the labor curve rather than extending it.
- Rule in Choice 2: Emotional and physical comfort measures significantly boost the maternal coping threshold, reducing the reliance on pain medications.
- Rule out Choice 3: Support systems drastically improve both subjective satisfaction scores and objective obstetrical birth outcomes.
- Rule out Choice 4: Family and lay birth workers offer unique, non-clinical presence and advocacy that complements the medical team's role.
Take home points
- Continuous labor support is an evidence-based intervention linked to shorter labor durations and a decreased need for pharmacological pain relief.
- Having a dedicated support person present minimizes maternal anxiety, preserving optimal uterine blood flow and endogenous oxytocin release.
- One-on-one intrapartum companion care reduces the likelihood of operative interventions, such as cesarean sections or vacuum-assisted deliveries.
- The nursing team should actively collaborate with lay support persons to cultivate an empowering, stress-minimizing environment for the laboring client.
Comprehensive Questions
A nurse is assessing uterine contractions. Which of the following findings indicates adequate labor?
Explanation
Adequate labor requires effective uterine activity that drives progressive cervical effacement and dilation. True labor contractions originate in the fundus, build intensity, and occur at regular intervals. This synchronized myometrial contractility relies on gap junction formation and oxytocin receptor up-regulation to ensure optimal fetal descent through the birth canal, facilitating cervical change and preventing hypotonic uterine dysfunction.
Rationale for correct answer:
2. The presence of regular contractions every 2–3 min lasting 60–90 sec with cervical change defines effective uterine activity. This frequency and duration optimize uterine efficiency while preserving essential placental perfusion between contractions. Documented cervical dilation or effacement provides definitive physiological validation that the contractions are adequate to progress labor.
Rationale for incorrect answers:
1. Contractions occurring every 10 min lasting 20 sec are insufficient to alter cervical architecture. This infrequent and brief pattern is typical of the latent phase or prodromal labor rather than active, effective contractions. Without increased frequency and duration, these contractions fail to provide the mechanical force needed for myometrial contractility.
3. Irregular contractions with no cervical dilation describe false labor, commonly referred to as Braxton Hicks contractions. These contractions do not increase in intensity, often subside with ambulation or hydration, and lack fundal dominance. Because they fail to induce cervical effacement or dilation, they are classified as inadequate.
4. Mild contractions occurring every 15 min represent an inadequate uterine pattern that cannot support progressive labor. This low-frequency tracking is often observed in uterine inertia or early pre-labor states. It lacks the sustained intrauterine pressure necessary to facilitate engagement and fetal descent.
Test-taking strategy:
- Analyze the scenario/question: The question asks the nurse to identify which uterine contraction pattern indicates adequate labor. This requires distinguishing effective, productive labor contractions from ineffective, false, or early prodromal patterns based on objective physiological parameters.
- Apply Knowledge of Labor Progress: To determine adequacy, the nurse must assess the frequency, duration, intensity, and structural impact of contractions on the cervix. True, adequate labor must demonstrate an organized pattern that physically alters the cervix. The nurse must recognize that uterine contractions alone do not equal labor; there must be definitive data indicating that the structural components of the reproductive tract are responding dynamically to the mechanical work being performed.
- Rule out Choice 1: A frequency of 10 minutes and a duration of 20 seconds are too weak and far apart to cause structural change. This represents ineffective uterine activity.
- Rule in Choice 2: The pattern of every 2–3 minutes lasting 60–90 seconds perfectly matches active labor guidelines, and the presence of cervical change confirms adequacy.
- Rule out Choice 3: Irregular contractions that fail to cause cervical dilation are clinical markers of false labor rather than adequate active labor.
- Rule out Choice 4: Mild contractions every 15 minutes are insufficient in both frequency and mechanical strength to progress a patient through the stages of parturition.
Take home points
- Adequate labor is clinically defined by regular uterine contractions that result in progressive cervical effacement and dilation.
- True labor contractions typically occur every 2–3 minutes, last 60–90 seconds, and manifest with strong fundal intensity.
- Braxton Hicks contractions are irregular, do not intensify with time, and are characterized by an absence of cervical dilation.
- Hypotonic uterine contractions are too infrequent or weak to facilitate proper fetal descent and require ongoing clinical assessment.
A nurse is monitoring uterine activity. Which of the following findings indicate uterine tachysystole? Select all that apply
Explanation
Uterine tachysystole represents a critical hyperstimulation state characterized by an excessive frequency or elevated baseline pressure of myometrial contractions. This condition compromises uteroplacental perfusion by severely limiting the relaxation phases necessary for adequate maternal-fetal gas exchange across the intervillous spaces. Prolonged or untreated overactivity can rapidly trigger functional myometrial fatigue, leading to progressive fetal hypoxia, metabolic acidosis, and subsequent operational fetal distress requiring immediate therapeutic or surgical intervention.
Rationale for correct answers:
1. A contraction frequency exceeding 5 contractions within a standard 10-minute window averaged over a 30-minute period explicitly meets the diagnostic criteria for uterine tachysystole. This rapid cycling prevents the necessary physiological relaxation phase, directly accelerating maternal myometrial exhaustion and compromising fetal oxygenation. The nurse must identify this pattern promptly to initiate corrective actions, such as discontinuing oxytocin infusions or administering tocolytics.
2. An elevated resting intrauterine pressure exceeding 25 mmHg measured via an intrauterine pressure catheter indicates an abnormally high resting tone. This lack of complete baseline relaxation maintains constant mechanical compression on the intramyometrial blood vessels, severely diminishing the vital placental blood flow that normally occurs between contractions. Prolonged elevation of this base pressure leads directly to intrapartum hypoxia and progressive fetal heart rate decelerations.
Rationale for incorrect answers:
3. Contractions occurring every 8 min represent a hypotonic or infrequent uterine pattern that is entirely inconsistent with hyperstimulation syndromes. This low frequency is insufficient to cause structural labor progression and is commonly associated with early prodromal labor or underlying uterine inertia. Because it poses no risk of restricting essential perfusion pathways, it cannot be classified as an overactive or tachysystolic state.
4. A reduction in fetal heart rate variability is a pathological clinical consequence or sign of worsening fetal hypoxia rather than a direct defining finding of uterine activity itself. While this ominous finding frequently occurs secondary to sustained hyperstimulation, it remains a distinct hemodynamic marker of fetal compromise. Tachysystole is strictly quantified by measuring mechanical contractions and intrauterine pressures rather than monitoring the autonomic responses of the fetal heart rate.
5. Contractions lasting less than 30 sec are considered brief and clinically ineffective, representing the opposite structural presentation of a hyperstimulated uterus. True tachysystole often involves prolonged durations that exceed 90 seconds, which maximizes intrauterine pressure and extends the ischemic phase. Short, weak contraction patterns are characteristically benign markers of early latent labor or functional hypotonic dysfunction.
Test-taking strategy:
- Analyze the scenario/question: The question requires the nurse to identify the specific clinical findings that indicate the presence of uterine tachysystole from a select-all-that-apply list. This necessitates distinguishing normal or hypotonic contraction characteristics from quantified metrics of uterine hyperstimulation and hypertonicity.
- Apply Knowledge of Uterine Monitoring: To determine tachysystole, the nurse must analyze mechanical parameters such as frequency, duration, and baseline resting tone. The nurse must recognize that tachysystole is strictly defined by excessive quantification of uterine contractions themselves over a specific time frame, rather than the secondary fetal physiological responses that result from the condition.
- Rule in Choice 1: More than 5 contractions in 10 minutes matches the formal diagnostic definition of tachysystole, which requires immediate intervention to protect maternal and fetal well-being.
- Rule in Choice 2: A resting tone greater than 25 mmHg reflects uterine hypertonus, confirming that the muscle is failing to relax between contraction peaks.
- Rule out Choice 3: Contractions occurring every 8 minutes describe an underactive, hypotonic labor pattern rather than a hyperstimulated or tachysystolic state.
- Rule out Choice 4: Decreased fetal heart rate variability is a secondary fetal neurological response to hypoxia and does not constitute a direct measurement of uterine activity.
- Rule out Choice 5: A contraction duration under 30 seconds signifies weak, inadequate uterine activity, which contradicts the prolonged contraction profiles seen in hyperstimulation.
Take home points
- Uterine tachysystole is formally defined as more than 5 contractions in 10 minutes averaged over a 30-minute window.
- A normal uterine resting tone should remain below 20-25 mmHg to ensure adequate intervillous space perfusion between contractions.
- Fetal heart rate decelerations and decreased variability are secondary consequences of tachysystole, not diagnostic criteria of uterine activity.
- Primary nursing interventions for tachysystole include stopping oxytocin, repositioning the client, and administering oxygen or tocolytics.
A nurse is assessing fetal position. Which of the following is most favorable for vaginal delivery?
Explanation
Fetal positioning plays a critical role in determining the efficiency and safety of cephalic presentation during labor. The ideal orientation minimizes the presenting diameters of the fetal skull as it traverses the maternal pelvis, reducing the risk of cephalic disproportions and labor dystocia. The fetal cranium accommodates best when it enters the pelvic inlet via an optimal pelvic diameter, which facilitates smooth fetal descent, rotational adaptation, internal rotation, and progressive cervical change while preventing prolonged maternal exhaustion or mechanical uterine inertia.
Rationale for correct answer:
2. The left occiput anterior position places the fetal occiput toward the left anterior quadrant of the maternal pelvis, which represents the most common and optimal orientation for an uncomplicated vertex delivery. This alignment allows the smallest suboccipital-bregmatic diameter of the skull to present, facilitating rapid fetal descent and efficient rotational maneuvers through the vaginal canal. It ensures ideal application of the vertex to the cervix, which maximizes uterine efficiency and accelerates progressive cervical dilation.
Rationale for incorrect answers:
1. The occiput posterior orientation places the fetal skull facing the maternal symphysis pubis, which significantly delays normal cardinal movements. This maladaptive positioning causes severe back pain, commonly known as back labor, due to direct sacral compression by the rigid fetal cranium. It increases the likelihood of prolonged active phase labor and often requires operational maneuvers or cesarean birth to resolve mechanical labor arrest.
3. The right occiput posterior alignment represents a malposition where the fetus faces anteriorly toward the maternal right side, forcing a wider skull diameter through the pelvis. This presentation frequently induces severe back labor and extends the second stage of labor due to the extensive rotation required to reach an anterior state. It significantly increases maternal risk for pelvic floor trauma, deep perineal lacerations, and functional myometrial fatigue.
4. A shoulder presentation occurs when the fetus is in a transverse lie, making a normal vaginal delivery physically impossible. This malpresentation poses an immediate risk for severe intrapartum complications, including umbilical cord prolapse or acute uterine rupture if labor progresses without intervention. The structural misalignment completely prevents engagement into the pelvic inlet, necessitating an immediate cesarean birth to preserve maternal and fetal safety.
Test-taking strategy:
- Analyze the scenario/question: The question asks the nurse to identify which fetal position is most favorable for a successful and uncomplicated vaginal delivery. This requires evaluating the anatomical relationships between the fetal presenting part and the maternal pelvic quadrants to determine the path of least resistance.
- Apply Knowledge of Labor Progress: To identify the most favorable position, the nurse must analyze how different cephalic and non-cephalic positions affect the mechanics of labor and cardinal movements. The nurse must recognize that anterior cephalic positions optimize pelvic diameters, whereas posterior or transverse positions impede descent and drastically increase the risk of maternal and fetal intrapartum complications.
- Rule out Choice 1: The occiput posterior position is a malposition that leads to prolonged labor, severe sacral pain, and an increased incidence of instrumental or surgical intervention.
- Rule in Choice 2: The left occiput anterior position is the ideal obstetric alignment because it presents the narrowest cranial diameter to the pelvic inlet, promoting efficient labor.
- Rule out Choice 3: The right occiput posterior position causes mechanical dystocia and severe back labor due to the fetal occiput compressing the maternal sacrum during descent.
- Rule out Choice 4: A shoulder presentation indicates a transverse lie, which is an absolute contraindication to vaginal delivery and carries a high risk of umbilical cord prolapse.
Take home points
- Occiput anterior positions are the most favorable for vaginal delivery because they minimize the presenting diameter of the fetal head.
- Occiput posterior positions frequently cause prolonged labor, severe maternal back pain, and an increased risk of assisted delivery interventions.
- A transverse lie resulting in a shoulder presentation cannot be delivered vaginally and requires an immediate cesarean delivery.
- Accurate assessment of fetal position via Leopold maneuvers allows the nurse to anticipate labor dystocia and implement corrective maternal positioning.
A nurse is evaluating pelvic adequacy. Which of the following findings may contribute to cephalopelvic disproportion (CPD)? Select all that apply
Explanation
Cephalopelvic disproportion represents a critical mechanical mismatch where the structural dimensions of the maternal bony pelvis cannot accommodate the presenting diameters of the fetal head. This anatomical conflict completely impedes normal fetal descent, stalls internal rotation maneuvers, and arrests progressive cervical dilation despite strong, coordinated uterine contractions. Prolonged engagement against an impassable pelvic boundary can rapidly trigger severe myometrial fatigue, elevate risks of uterine rupture, or cause acute fetal hypoxemia, which ultimately leads to operational arrest and mandates an emergent cesarean birth.
Rationale for correct answers:
1. A narrow interspinous diameter restricts the midpelvis plane, which represents the most common site of mechanical pelvic contraction. This reduced transverse space prevents the fetal head from completing vital internal rotation maneuvers, directly stalling downward fetal descent during the second stage of labor. Because the rigid ischial spines cannot expand, an inadequate diameter creates an unyielding structural barrier that contributes significantly to labor dystocia.
2. An abnormally large fetal size, such as macrosomia, introduces a primary fetal factor that directly disrupts pelvic proportionality. When the biparietal diameter of the fetal cranium exceeds the maximum available space within the pelvic inlet, cephalopelvic disproportion occurs regardless of maternal pelvic shape. This volume mismatch prevents proper engagement into the superior strait, rendering successful vaginal delivery highly improbable and increasing risks of shoulder dystocia.
4. A full urinary bladder creates a temporary, space-occupying soft tissue mass directly anterior to the uterus and cervix. This mechanical displacement physically pushes the lower uterine segment upward, which directly inhibits the necessary engagement and fetal descent into the true pelvis. If left uncatheterized, the distended bladder non-physiologically narrows the available pelvic inlet space, weakens contraction efficiency, and induces secondary uterine inertia.
Rationale for incorrect answers:
3. A gynecoid pelvis features a wide, rounded pelvic inlet, blunt ischial spines, and an unyielding pubic arch that represents the ideal architectural shape for childbearing. This structural morphology maximizes all internal diameters, allowing the fetal head to flex and rotate with minimal resistance. Because it provides the most room for passage, it is highly protective against disproportion and promotes optimal uterine efficiency.
5. A soft and compliant perineum describes highly distensible pelvic floor musculature that easily expands during the crowning phase of labor. Because the perineum is an external soft tissue structure, its compliance has no influence on the rigid osseous boundaries of the true pelvis where mechanical disproportion occurs. A compliant perineum prevents lacerations during expulsion but cannot mitigate an underlying restriction within the maternal pelvis.
Test-taking strategy:
- Analyze the scenario/question: The question asks the nurse to select all findings that could mechanically contribute to the development of cephalopelvic disproportion (CPD). This requires identifying both fixed osseous restrictions, temporary soft-tissue obstructions, and fetal mass variations that disrupt the passage-passenger relationship.
- Apply Knowledge of Pelvic Adequacy: To determine factors contributing to CPD, the nurse must analyze the components of the birthing process, specifically separating factors that contract or obstruct the pelvis from those that facilitate smooth passage. The nurse must recognize that CPD can be caused by absolute pelvic restrictions, excessive fetal dimensions, or reversible soft-tissue obstructions that narrow the birth canal.
- Rule in Choice 1: A narrow interspinous diameter represents a contraction of the midpelvis plane that physically blocks the fetus from descending past the ischial spines.
- Rule in Choice 2: A large fetal size introduces a passenger-related mismatch where the fetal head is too large for an otherwise normal maternal pelvis, causing disproportion.
- Rule out Choice 3: A gynecoid pelvis is the classic, most favorable female pelvic type and is characterized by adequate diameters that decrease the risk of CPD.
- Rule in Choice 4: A full urinary bladder acts as an obstructing soft-tissue mass that displaces the uterus, prevents fetal engagement, and effectively reduces available pelvic space.
- Rule out Choice 5: A soft and compliant perineum relates to external soft tissue elasticity at delivery and has no bearing on the internal bony constraints that define true CPD.
Take home points
- Cephalopelvic disproportion is caused by an architectural mismatch between maternal pelvic diameters and the presenting part of the fetus.
- The interspinous diameter evaluates midpelvis adequacy, and contraction of this space is a frequent cause of instrumental or operational labor arrest.
- Maternal soft-tissue obstructions, such as a full urinary bladder or a uterine fibroid, can transiently mimic CPD by blocking fetal descent.
- A gynecoid pelvis offers the most favorable dimensions for vaginal birth, whereas platypelloid and android shapes carry much higher risks of disproportion.
A nurse is assessing fetal station. Which of the following indicates engagement?
Explanation
Fetal station measures the relative descent of the presenting part through the maternal pelvis, quantified in centimeters above or below the ischial spines. True engagement signifies that the largest transverse diameter of the fetal presenting part, typically the biparietal diameter in cephalic presentations, has successfully passed through the pelvic inlet into the true pelvis. This crucial mechanical milestone confirms that the pelvic inlet plane is adequate to accommodate the fetus, paving the way for progressive fetal descent, internal rotational movements, and effective cervical change while protecting against maternal uterine inertia.
Rationale for correct answer:
3. A 0 station indicates that the leading bony edge of the fetal presenting part has reached the level of the maternal ischial spines. In a vertex presentation, this anatomical alignment demonstrates that the widest part of the fetal head has entered the pelvic inlet, confirming true fetal engagement. Achieving this station provides essential clinical validation that the superior pelvic plane is adequate, allowing the nurse to anticipate subsequent cardinal movements of labor.
Rationale for incorrect answers:
1. A -3 station indicates that the presenting part remains 3 centimeters floating above the level of the ischial spines. This highly unengaged position reflects a high, mobile fetus that has not yet entered the pelvic inlet, which is common in early primigravid labor or latent labor. If this tracking persists despite strong, regular contractions, it may point toward an underlying anatomical mismatch like cephalopelvic disproportion.
2. A -5 station represents a completely unengaged fetus floating high above the pelvic inlet, often referred to as being ballotable. This high position carries a significant risk for immediate cord prolapse if the amniotic membranes rupture prematurely or spontaneously before the head fixes in the inlet. Because the vertex has made no structural progress into the true pelvis, it reflects an inadequate labor or pre-labor state.
4. A -2 station means the presenting part is situated 2 centimeters above the ischial spines, showing that engagement has not yet occurred. While this indicates a minor degree of downward mobility compared to higher stations, the head remains unengaged within the upper pelvic strait. The nurse must continue to monitor uterine contractions to ensure they have the mechanical force required to achieve pelvic engagement.
Test-taking strategy:
- Analyze the scenario/question: The question asks the nurse to identify which fetal station indicates that engagement has occurred. This requires understanding the numerical scoring system used to track fetal descent relative to the landmark of the maternal pelvis.
- Apply Knowledge of Fetal Station: To determine engagement, the nurse must evaluate the positional relationship between the presenting part and the maternal ischial spines. The nurse must recognize that negative numbers represent a floating or unengaged fetus above the spines, positive numbers indicate progressive descent below the spines, and the zero point serves as the definitive boundary for engagement.
- Rule out Choice 1: A -3 station describes a high, floating presenting part situated well above the ischial spines, indicating that the fetus is completely unengaged.
- Rule out Choice 2: A -5 station represents a presentation that is completely ballotable and unengaged at the superior border of the pelvic inlet.
- Rule in Choice 3: A 0 station is the precise clinical definition of engagement, indicating that the widest diameter of the fetal head has successfully navigated the pelvic inlet.
- Rule out Choice 4: A -2 station indicates that the fetus is descending but remains floating above the ischial spines, meaning engagement has not yet been achieved.
Take home points
- Fetal engagement is clinically defined as a station of 0, where the presenting part is level with the maternal ischial spines.
- Negative stations (-1 to -5) indicate that the presenting part is floating above the ischial spines and is not yet engaged.
- Positive stations (+1 to +5) confirm that the fetus is descending through the midpelvis toward delivery at the perineal floor.
- Rupture of membranes when the fetus is at a high negative station (-3 to -5) significantly increases the emergency risk of umbilical cord prolapse.
A nurse is assessing fetal skull features. Which of the following statements are correct? Select all that apply
Explanation
The structural architecture of the fetal skull is uniquely adapted to navigate the rigid constraints of the maternal bony pelvis during parturition. This anatomical flexibility is primarily facilitated by the non-ossified membranous spaces separating the cranial bones, which allow for adaptive modifications in head shape. This dynamic system coordinates with uterine forces to optimize fetal descent, prevent prolonged mechanical labor dystocia, and reduce intracranial pressure variations during engagement, thereby ensuring efficient passage through the birth canal and mitigating the risk of myometrial fatigue.
Rationale for correct answers:
1. Cranial sutures are flexible, fibrous joints that separate the individual bones of the fetal skull, directly permitting cranial molding during labor. This structural pliability enables the skull bones to shift and temporarily overlap in response to mechanical pressures exerted by the birth canal. The nurse must recognize that this shifting reduces the overall presenting diameter of the vertex, which prevents cephalopelvic disproportion and facilitates a safer delivery.
2. Fontanelles are the wider, membrane-filled spaces located at the intersections of cranial sutures, serving as critical landmarks to determine fetal position. By performing a digital vaginal examination, the clinician can palpate the triangular posterior fontanelle and the diamond-shaped anterior fontanelle relative to the quadrants of the maternal pelvis. Identifying these specific structures allows the nurse to accurately map the fetal orientation, such as identifying an optimal occiput anterior alignment.
4. Molding is the physiological process of cranial shaping that directly facilitates the passenger's navigation through the unyielding pelvic straits. This transient overlapping reduces the biparietal and occipitofrontal diameters of the cranium, allowing the vertex to conform to the precise contours of the maternal pelvis. Without this critical capacity for mechanical adaptation, the incidence of prolonged second-stage arrest and secondary uterine inertia would rise significantly.
Rationale for incorrect answers:
3. Sutures function to provide necessary elasticity and movement rather than acting to increase the structural rigidity of the cranium. If these fibrous joints were rigid or fused prematurely, a condition known as craniosynostosis, the fetal head would be completely incapable of shifting shape during labor. This lack of compliance would present an unyielding mechanical barrier to delivery, rapidly precipitating severe fetal distress.
5. Fontanelles serve to allow extensive, protective cranial deformation and reshaping rather than acting to prevent head movement. These membranous gaps provide the essential space required for the skull bones to overlap safely without compressing vital underlying cerebral structures. Restricting this mobility would negate the skull's primary evolutionary adaptation for childbearing, leading to absolute obstruction and mandatory cesarean birth.
Test-taking strategy:
- Analyze the scenario/question: The question requires the nurse to identify correct statements regarding the physiological features and clinical relevance of the fetal skull during labor from a select-all-that-apply list. This requires understanding how cranial bones, sutures, and fontanelles interact to allow mechanical adaptation.
- Apply Knowledge of Fetal Skull Adaptations: To evaluate each statement, the nurse must analyze the mechanics of passage through the birth canal, specifically focusing on how structural flexibility aids delivery while rigid configurations impede it. The nurse must recognize that the fetal skull is anatomically designed to be dynamic and compressible rather than static, and that its surface markings provide vital diagnostic clues during labor assessment.
- Rule in Choice 1: Sutures are non-ossified junctions that explicitly permit the skull bones to shift, allowing the essential process of molding to occur.
- Rule in Choice 2: Fontanelles possess distinct geometric shapes that allow clinicians to palpate and accurately identify the presentation and position of the fetus.
- Rule out Choice 3: Sutures are designed to decrease rigidity and increase pliability during delivery, making the assertion of increased rigidity false.
- Rule in Choice 4: Molding reduces the presenting cranial diameters, which directly helps the fetus squeeze through the tight dimensions of the pelvic canal.
- Rule out Choice 5: Fontanelles facilitate cranial compression and flexibility rather than preventing movement, rendering this choice biologically incorrect.
Take home points
- Cranial molding is a protective physiological adaptation that temporarily reduces fetal head diameters to facilitate pelvic passage.
- The anterior fontanelle is diamond-shaped and closes by 18 months, while the posterior fontanelle is triangular and closes by 2 months.
- Palpation of the sagittal suture and fontanelles during vaginal exams is the primary method for tracking internal fetal rotation.
- Premature fusion of cranial sutures eliminates skull elasticity, significantly increasing the risk of mechanical birth dystocia.
A nurse is caring for a client with hypertonic labor. Which of the following findings should the nurse expect?
Explanation
Hypertonic labor represents a dysfunctional uterine state characterized by uncoordinated, high-frequency myometrial contractions originating outside the normal fundal pacemaker. This baseline hypertonicity elevates resting intrauterine pressure, which prevents the complete relaxation phase necessary to restore vital maternal-fetal intervillous gas exchange between contraction peaks. The erratic contractility leads to premature myometrial fatigue and severe ischemia, resulting in intense maternal pain, minimal structural advancement, and acute operational fetal distress requiring urgent therapeutic or pharmacological tocolysis.
Rationale for correct answer:
2. The presence of painful frequent contractions with minimal cervical change is the classic clinical hallmark of hypertonic uterine dysfunction. Because these contractions are erratic, localized, and lack fundal dominance, they expend immense metabolic energy without generating the synchronized mechanical force required to efface or dilate the cervix. The constant muscle tension leads to severe ischemic pain and rapid maternal exhaustion without contributing to productive labor progress.
Rationale for incorrect answers:
1. Strong coordinated contractions with rapid dilation describe an optimal, highly efficient uterine pattern or a precipitate labor state. This synchronized contractility originates correctly in the fundus and sweeps downward, promoting rapid cervical change and smooth fetal descent. This highly effective mechanism represents the physiological opposite of the uncoordinated, non-productive tracking that defines hypertonic labor.
3. Weak contractions with prolonged labor describe hypotonic uterine dysfunction, which is characterized by inadequate mechanical pressure during the active phase of labor. In hypotonic states, the uterus relaxes completely between cycles, but the contractions lack the intensity needed to achieve cervical dilation. This is a distinct form of labor dystocia that typically responds well to oxytocin augmentation, which is strictly contraindicated in hypertonic labor.
4. An absence of contractions indicates a state of uterine quiescence, which is typical of late pregnancy before the onset of true or false labor. This lack of myometrial activity poses no immediate threat to uteroplacental perfusion and does not involve the severe, agonizing pain associated with hypertonus. Dysfunctional labor requires the presence of abnormal contractility rather than a complete absence of contractions.
Test-taking strategy:
- Analyze the scenario/question: The question asks the nurse to identify the expected clinical findings associated with a client experiencing hypertonic labor. This requires distinguishing the characteristic presentation of uncoordinated, overactive uterine patterns from normal, underactive, or completely absent contractility.
- Apply Knowledge of Uterine Dysfunction: To determine the correct finding, the nurse must analyze the physiological differences between hypertonic and hypotonic labor states, focusing on how contraction coordination impacts cervical work and maternal pain. The nurse must recognize that "hyper" denotes excess frequency and tone, but because the contractions are uncoordinated, they result in severe pain and maternal exhaustion without producing effective structural progress.
- Rule out Choice 1: Strong, coordinated contractions that produce rapid dilation indicate effective uterine activity or precipitate labor, not a dysfunctional hypertonic state.
- Rule in Choice 2: Painful, frequent contractions paired with a lack of cervical progress perfectly match the diagnostic criteria for hypertonic labor due to elevated resting tone and poor coordination.
- Rule out Choice 3: Weak contractions that prolong labor describe a hypotonic uterine pattern, which is a separate class of mechanical dystocia characterized by low intrauterine pressure.
- Rule out Choice 4: An absence of contractions indicates a resting pre-labor or postpartum state rather than an active, hyperstimulated, and dysfunctional labor pattern.
Take home points
- Hypertonic labor is characterized by frequent, uncoordinated, and highly painful contractions that fail to produce progressive cervical dilation.
- Therapeutic rest utilizing sedatives or tocolytics is the primary intervention for hypertonic labor to stop abnormal signaling and allow the uterus to reset.
- Oxytocin administration is strictly contraindicated in hypertonic labor because it can worsen myometrial hypertonus and induce severe fetal hypoxia.
- Hypotonic labor features weak, infrequent contractions with a low resting tone and is treated with amniotomy or oxytocin augmentation.
A nurse is evaluating psychological factors. Which of the following are effects of maternal anxiety during labor? Select all that apply
Explanation
Maternal anxiety during parturition triggers a profound sympathetic nervous system response that directly compromises the mechanical and physiological efficiency of labor. This psychological stress state accelerates catecholamine release, including epinephrine and norepinephrine, which activates systemic alpha and beta-adrenergic receptors. This neuroendocrine cascade causes peripheral vasoconstriction, diverts essential maternal cardiac output away from the reproductive tract, alters normal myometrial contractility patterns, and directly increases the risk of prolonged labor dystocia and secondary fetal compromise.
Rationale for correct answers:
1. High levels of anxiety stimulate the adrenal medulla, resulting in a marked catecholamine release into the maternal circulation. Epinephrine acts as a potent beta-adrenergic receptor agonist that inhibits normal myometrial activity, while norepinephrine induces generalized vasoconstriction. This hormonal surge disrupts the synchronized pacemaker signaling of the fundus, leading directly to uncoordinated uterine contractions and functional uterine inertia.
2. The severe vasoconstriction triggered by sympathetic nervous system activation leads directly to a decreased uterine blood flow. As maternal systemic vascular resistance rises, blood is shunted away from the splanchnic bed and reproductive organs toward major skeletal muscles. This reduced perfusion impairs the essential exchange of gases across the intervillous spaces, directly lowering baseline uteroplacental perfusion during contraction cycles.
4. Psychological stress lowers the maternal threshold for discomfort, causing a significant increased pain perception. Anxiety amplifies central nervous system processing of nociceptive signals from the stretching cervix and contracting uterus, creating a maladaptive cycle of fear, tension, and agony. This heightened neurological response depletes maternal coping mechanisms, accelerating early exhaustional states and myometrial fatigue.
Rationale for incorrect answers:
3. Maternal anxiety results in a marked inhibition of posterior pituitary function, causing a drop rather than an increased oxytocin activity. Endogenous catecholamines actively block the systemic release and myometrial binding of oxytocin, which is required to drive progressive effacement and dilation. This hormonal suppression slows down the active phase of labor, necessitating medical interventions like oxytocin augmentation.
5. The physiological changes associated with maternal panic severely compromise rather than lead to improved fetal oxygenation. Because uterine artery vasoconstriction limits the volume of oxygenated blood reaching the placenta, the fetus faces a higher risk of intrapartum hypoxemia. This restricted perfusion manifests clinically as late decelerations, bradycardia, or loss of normal fetal heart rate variability.
Test-taking strategy:
- Analyze the scenario/question: The question requires the nurse to identify the physiological and psychological effects of maternal anxiety during labor from a select-all-that-apply list. This requires understanding how the sympathetic "fight-or-flight" response alters maternal hemodynamics and uterine efficiency.
- Apply Knowledge of Psychological Factors: To evaluate each choice, the nurse must analyze the systemic effects of stress hormones on smooth muscle contractility and pelvic blood flow. The nurse must recognize that anxiety releases stress chemicals that naturally inhibit normal labor hormones, constrict blood vessels supplying the fetus, and lower the maternal pain tolerance threshold.
- Rule in Choice 1: Increased catecholamine release is a direct physiological consequence of anxiety, as the body floods the system with epinephrine and norepinephrine under stress.
- Rule in Choice 2: Decreased uterine blood flow occurs because sympathetic vasoconstriction shunts maternal blood away from the uterus to feed skeletal muscles.
- Rule out Choice 3: Increased oxytocin activity is incorrect because stress hormones actively suppress posterior pituitary oxytocin release, slowing labor progress.
- Rule in Choice 4: Increased pain perception is a well-documented psychological effect of anxiety, which amplifies nociceptive pathways and worsens the fear-tension-pain cycle.
- Rule out Choice 5: Improved fetal oxygenation is biologically false; the reduction in uteroplacental blood flow directly lowers fetal oxygen levels, causing distress.
Take home points
- Severe maternal anxiety induces a fight-or-flight response that releases epinephrine and norepinephrine, disrupting normal labor progress.
- High catecholamine levels cause significant vasoconstriction of the uterine artery, which decreases placental perfusion and risks fetal hypoxia.
- Emotional support, proper labor coaching, and pharmacological analgesia help lower maternal anxiety, thereby improving myometrial efficiency.
- Anxiety slows labor progression by actively suppressing endogenous oxytocin release, frequently leading to secondary hypotonic dysfunction.
A nurse is teaching about secondary powers. Which of the following statements indicates understanding?
Explanation
Secondary powers involve the conscious, coordinated expulsion efforts initiated by the maternal abdominal musculature during the second stage of labor. These voluntary forces supplement the primary powers, which consist of involuntary myometrial contractions, to generate the intra-abdominal pressure needed to drive the presenting part through the lower birth canal. This combined mechanical push maximizes fetal expulsion forces, overcomes perineal floor resistance, and assists in achieving successful fetal descent, minimizing the risk of prolonged positional arrest, pelvic tissue trauma, or severe myometrial fatigue.
Rationale for correct answer:
2. The statement that secondary powers assist in fetal expulsion through maternal pushing indicates a correct clinical understanding of intrapartum mechanics. Once the cervix achieves full dilation, the maternal bearing-down reflex is triggered as the fetal head compresses the pelvic floor. This voluntary recruitment of the diaphragm and abdominal wall increases intra-abdominal pressure, working in synergy with contractions to accomplish fetal expulsion.
Rationale for incorrect answers:
1. Describing secondary powers as involuntary uterine contractions is incorrect because it confuses them with primary powers. Primary powers are the automatic, involuntary contractions of the myometrium driven by pacemaker cells in the fundus that perform cervical change. Secondary powers are entirely voluntary and require active, conscious maternal physical effort during the expulsive phase.
3. Stating that these forces occur only before labor begins represents a fundamental misunderstanding of labor physiology. Secondary powers are strictly utilized during the second stage of labor, after full dilation is achieved, to actively deliver the fetus. Pre-labor contractions, such as Braxton Hicks patterns, are part of the primary spectrum and serve to ripen the cervix, rather than acting as expulsive forces.
4. Asserting that secondary powers are responsible for cervical dilation only is incorrect because these forces play no role in opening the cervix. Attempting to push before full cervical dilation can cause severe cervical lacerations, edema, and subsequent labor dystocia. Dilating forces are exclusively driven by primary involuntary contractions that pull the lower uterine segment upward over the fetal vertex.
Test-taking strategy:
- Analyze the scenario/question: The question asks the nurse to identify the statement that demonstrates an accurate understanding of secondary powers during labor. This requires distinguishing the mechanisms and timing of primary involuntary uterine forces from secondary voluntary bearing-down efforts.
- Apply Knowledge of Forces of Labor: To select the correct statement, the nurse must analyze the two distinct forces that drive parturition: primary powers and secondary powers. The nurse must recognize that primary powers open the cervix involuntarily, whereas secondary powers are the maternal voluntary pushes required to expel the fetus once the cervix is completely open.
- Rule out Choice 1: Involuntary uterine contractions define the primary powers of labor, which are driven autonomously by the myometrium, not the secondary powers.
- Rule in Choice 2: Secondary powers refer precisely to the voluntary maternal bearing-down efforts that provide the secondary mechanical force necessary for fetal expulsion.
- Rule out Choice 3: Secondary powers are only initiated during active, second-stage labor and are completely absent before true labor begins.
- Rule out Choice 4: Cervical dilation is achieved solely through primary involuntary contractions; pushing against an undilated cervix is dangerous and ineffective.
Take home points
- Primary powers are involuntary uterine contractions responsible for effacement and dilation of the cervix during the first stage of labor.
- Secondary powers are voluntary bearing-down efforts by the mother that increase intra-abdominal pressure to expel the fetus during the second stage.
- Premature pushing before full cervical dilation must be discouraged because it can cause cervical edema, tearing, and maternal exhaustion.
- The Ferguson reflex is the neuroendocrine response triggered by fetal head pressure on the pelvic floor that stimulates the urge to use secondary powers.
A nurse is assessing factors affecting the passageway. Which of the following findings may impair labor? Select all that apply
Explanation
The passageway encompasses the rigid maternal bony pelvis and the distensible soft tissues of the birth canal through which the fetus must navigate. Anatomical obstructions or structural restrictions within these components can significantly impair labor progression by blocking the path of travel. These barriers prevent optimal fetal descent, arrest cardinal rotational movements, and stall cervical effacement, which directly leads to prolonged labor dystocia, mechanical arrest, or acute maternal-fetal injury if the mechanical obstruction is not promptly identified and managed.
Rationale for correct answers:
1. Uterine fibroids located in the lower uterine segment or cervix act as benign, space-occupying muscular tumors that narrow the reproductive tract. These physical masses alter normal myometrial architecture, disrupting synchronized myometrial contractility and mechanically blocking the fetus from entering the true pelvis. The presence of these tumors can permanently arrest descent, necessitating structural changes in the delivery plan, such as a cesarean birth.
2. A full bladder creates a dynamic soft-tissue obstruction directly anterior to the lower uterine segment and vaginal canal. This localized fluid accumulation physically pushes the uterus upward and backward, preventing the fetal vertex from establishing proper engagement against the cervix. This lack of appropriate contact weakens mechanical feedback loops, resulting in diminished contraction intensity and secondary uterine inertia.
4. A narrow pelvic inlet imposes a rigid osseous restriction at the superior strait of the maternal skeletal pelvis. When the inlet diameters are contracted, the widest transverse part of the fetal skull cannot enter the true pelvis, causing an absolute failure of pelvic engagement. This structural disproportion serves as a primary mechanical cause of cephalopelvic disproportion that cannot be overcome by manual positioning.
Rationale for incorrect answers:
3. Multiparity generally facilitates rather than impairs the passage of the fetus due to residual changes from previous deliveries. Women who have given birth multiple times typically exhibit more relaxed pelvic floor musculature and a more compliant cervix, which accelerates both the first and second stages of labor. This anatomical compliance enhances uterine efficiency and lowers the overall statistical risk for developing labor dystocia.
5. Frequent position changes during labor actively support rather than impair the physical mechanics of the birth canal. Altering maternal postures, such as moving from upright to side-lying positions, dynamically shifts pelvic joints and expands internal diameters to favor optimal fetal rotation. This mobility reduces maternal fatigue, increases comfort, and helps prevent positional arrest by utilizing gravity to assist fetal descent.
Test-taking strategy:
- Analyze the scenario/question: The question requires the nurse to select all findings that may impair labor by negatively affecting the passageway. This requires distinguishing structural anomalies and soft-tissue obstructions from factors that facilitate or normalize the mechanical process of childbirth.
- Apply Knowledge of the Passageway: To evaluate each finding, the nurse must analyze the components of the birth canal, differentiating between immovable bony constraints, reversible soft-tissue mass effects, and functional maternal behaviors. The nurse must recognize that any factor that reduces the internal diameter of the bony pelvis or physically occupies space within the soft-tissue tract will impede the mechanical descent of the passenger.
- Rule in Choice 1: Uterine fibroids introduce an obstructive soft-tissue mass within the lower uterine segment that physically blocks the pelvic inlet.
- Rule in Choice 2: A full bladder acts as a transient soft-tissue barrier that shifts the uterus anatomically and prevents proper fetal engagement.
- Rule out Choice 3: Multiparity reduces soft-tissue resistance from the pelvic floor, which typically shortens labor duration rather than impairing it.
- Rule in Choice 4: A narrow pelvic inlet represents a fixed bony contraction that directly prevents the fetal head from entering the birth canal.
- Rule out Choice 5: Frequent position changes are a beneficial nursing intervention that helps optimize pelvic diameters and promotes smooth fetal rotation.
Take home points
- The passageway consists of both the rigid maternal bony pelvis and soft tissues, including the cervix, pelvic floor, vagina, and bladder.
- Structural obstructions like lower-segment uterine fibroids can physically block the birth canal, causing mechanical labor arrest.
- Maintaining an empty urinary bladder via regular voiding or catheterization is essential to prevent transient soft-tissue obstruction and uterine displacement.
- Bony pelvic contractions, such as a narrow inlet or midpelvis, represent absolute barriers that frequently cause cephalopelvic disproportion.
A nurse is identifying cardinal movements. Which of the following occurs after internal rotation?
Explanation
The cardinal movements of labor represent a highly coordinated sequence of passive positional adjustments that the fetus must undergo to successfully navigate the rigid geometric constraints of the maternal bony pelvis. These positional changes are driven by the mechanical forces of uterine contractions and maternal expulsive efforts against the changing resistance of the pelvic floor musculature. This kinematic progression optimizes fetal diameters relative to pelvic planes, ensuring continuous fetal descent, minimizing the risk of mechanical labor dystocia, and preventing maternal myometrial exhaustion or secondary uterine inertia.
Rationale for correct answer:
2. Extension occurs immediately after internal rotation as the fetal head reaches the level of the maternal perineum and symphysis pubis. During internal rotation, the fetus aligns its long occipital diameter with the anteroposterior diameter of the pelvis, placing the occiput directly beneath the pubic arch. As downward forces continue, the unyielding pelvic floor drives the fetal head upward and outward, pivoting the occiput against the pubic bone to achieve fetal extension.
Rationale for incorrect answers:
1. Flexion occurs much earlier in the cardinal sequence, long before internal rotation is initiated. As the descending head meets resistance from the cervix or pelvic walls, the fetal chin is forced down toward the chest, which minimizes the presenting cranial diameter. This early adaptation converts the presentation to the highly favorable suboccipitobregmatic diameter, which facilitates subsequent pelvic engagement.
3. Engagement is an early mechanical milestone that must be achieved before internal rotation or extension can take place. It is defined as the arrival of the widest biparietal diameter of the fetal head at the level of the maternal ischial spines. This entry confirms that the superior pelvic inlet plane is adequate to accommodate the passenger, serving as a prerequisite for all subsequent cardinal movements.
4. Descent is an overarching, continuous process that occurs throughout the entire duration of labor rather than acting as a single step following internal rotation. It represents the steady downward movement of the presenting part through the birth canal, measured via fetal station. While descent accelerates during the expulsive stage, it serves as the mechanical engine that drives individual structural rotations rather than a distinct subsequent movement.
Test-taking strategy:
- Analyze the scenario/question: The question asks the nurse to identify which specific cardinal movement of labor occurs immediately after internal rotation has been completed. This requires mapping the chronological sequence of mechanical maneuvers performed by the fetus during birth.
- Apply Knowledge of Cardinal Movements: To determine the correct subsequent movement, the nurse must analyze the exact chronological order of positional changes: engagement, descent, flexion, internal rotation, extension, restitution, external rotation, and expulsion. The nurse must recognize that internal rotation places the occiput directly under the symphysis pubis, and the only path for further progress out of the curved birth canal is for the head to extend upward.
- Rule out Choice 1: Flexion is an early adaptation that occurs during initial descent when the head meets soft-tissue resistance, long before internal rotation.
- Rule in Choice 2: Extension follows internal rotation because the fetal head must pivot under the pubic arch to emerge from the vaginal introitus.
- Rule out Choice 3: Engagement is a foundational early step that establishes the fetus at a 0 station, serving as a prerequisite for internal rotation.
- Rule out Choice 4: Descent is a continuous mechanism that operates across all stages of labor rather than a discrete step that follows internal rotation.
Take home points
- The standard chronological sequence of cardinal movements is engagement, descent, flexion, internal rotation, extension, restitution, external rotation, and expulsion.
- Internal rotation aligns the long diameter of the fetal head with the anteroposterior diameter of the maternal pelvis.
- Extension occurs as the fetal head pivots under the symphysis pubis, allowing the brow, nose, mouth, and chin to be born over the perineum.
- Failure to progress through the cardinal movements in sequence results in labor arrest and frequently indicates an underlying cephalopelvic disproportion.
A nurse is assessing fetal presentation. Which of the following are abnormal presentations? Select all that apply
Explanation
Fetal presentation specifies the anatomical part of the passenger that leads into the pelvic inlet and arrives first at the cervix during digital examination. Deviation from the ideal vertex configuration introduces a non-cephalic arrangement that mechanically alters the shape of the presenting mass against the maternal birth canal. These atypical configurations prevent uniform application of the presenting part to the cervix, disrupt normal myometrial contractility pathways, extend the duration of labor, and drastically elevate the risks of mechanical labor dystocia, umbilical cord prolapse, or acute traumatic fetal distress necessitating operational intervention.
Rationale for correct answers:
1. A breech presentation occurs when the fetal buttocks or lower extremities present into the maternal pelvic inlet instead of the cranium. This malpresentation lacks the heavy, rigid structure of the skull needed to effectively dilate the cervix, which directly predisposes the client to prolonged uterine inertia. Delivering a breech fetus vaginally carries an exceptionally high risk of head entrapment and umbilical cord compression, which frequently mandates a cesarean birth.
3. A shoulder presentation arises when the fetus settles into a transverse orientation, making the acromion process the leading anatomical feature. This structural configuration is completely incompatible with a normal vaginal birth because the fetus cannot engage or pass through the pelvic planes in this position. If labor progresses with a shoulder presentation, it can rapidly precipitate an emergency umbilical cord prolapse or catastrophic uterine rupture.
4. A transverse lie describes an anatomical relationship where the long axis of the fetus is perpendicular to the long axis of the mother, leading directly to a shoulder or arm presentation. This orientation prevents the fetus from entering the superior strait of the pelvis, completely arresting normal fetal descent. Because the passenger cannot navigate the birth canal horizontally, a transverse lie represents an absolute mechanical barrier to delivery that requires surgical intervention.
Rationale for incorrect answers:
2. A cephalic presentation represents the ideal, most frequent orientation where the fetal head enters the pelvic inlet first. When the head is well-flexed, this vertex presentation allows the narrowest diameter of the skull to apply flatly against the cervix, maximizing uterine efficiency. This optimal alignment promotes steady cervical effacement and dilation, ensuring a lower statistical probability of developing a mechanical disproportion.
5. A longitudinal lie indicates that the long axis of the fetus is completely parallel with the long axis of the mother, which is the necessary spatial orientation for a standard delivery. This axis alignment accommodates both normal cephalic and breech presentations, establishing the basic structural pathway for downward fetal descent. While a breech presentation within a longitudinal lie is abnormal, the longitudinal lie itself is the preferred fetal lie.
Test-taking strategy:
- Analyze the scenario/question: The question requires the nurse to select all options from the list that represent abnormal fetal presentations or lies that would complicate or prevent a normal vaginal delivery. This requires distinguishing normal cephalic and longitudinal orientations from pathological malpresentations.
- Apply Knowledge of Fetal Presentation: To evaluate each choice, the nurse must analyze the spatial relationship between the passenger and the passageway, separating configurations that flow through pelvic diameters from those that create mechanical obstructions. The nurse must recognize that any presentation that does not feature the head leading the way parallel to the maternal spine will disrupt the normal mechanics of labor and significantly increase delivery risks.
- Rule in Choice 1: Breech presentation is an abnormal presentation where the buttocks or feet lead into the pelvis, increasing risks of cord compression and head entrapment.
- Rule out Choice 2: Cephalic presentation is the normal, most common presentation where the fetal head enters the pelvis first, which is ideal for delivery.
- Rule in Choice 3: Shoulder presentation is an abnormal presentation associated with a transverse lie that physically cannot be delivered through the vaginal canal.
- Rule in Choice 4: Transverse lie is an abnormal fetal lie where the fetus is positioned horizontally across the uterus, preventing engagement into the pelvic inlet.
- Rule out Choice 5: Longitudinal lie is the normal orientation where the maternal and fetal spines are parallel, which is required for a safe vaginal delivery path.
Take home points
- Cephalic presentation, specifically the vertex position, is the most common and favorable orientation for an uncomplicated vaginal birth.
- Breech presentations involve the buttocks or feet presenting first and are associated with a high incidence of umbilical cord prolapse during membrane rupture.
- A transverse lie results in a shoulder presentation and represents an absolute contraindication to vaginal delivery, requiring a cesarean section.
- Accurate tracking of fetal lie and presentation via Leopold maneuvers allows the nurse to anticipate delivery complications and coordinate alternative delivery modes.
Exams on Process of Labor (4 Ps)
Custom Exams
Login to Create a Quiz
Click here to loginLessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Explain the physiological mechanisms underlying uterine contractions, including myometrial activity, hormonal regulation, and cellular changes during labor
- Differentiate between primary powers (uterine contractions) and secondary powers (maternal pushing efforts) and describe their coordinated role in labor progression
- Analyze the characteristics of effective uterine contractions including frequency, duration, intensity, and resting tone, and correlate these with labor progress
- Evaluate methods of uterine contraction monitoring, including external tocodynamometry and internal intrauterine pressure catheter (IUPC), with interpretation of findings
- Identify and differentiate dysfunctional labor patterns such as hypotonic and hypertonic uterine dysfunction and their clinical implications
- Apply nursing interventions and clinical judgment in managing labor abnormalities related to uterine powers
- Integrate theoretical knowledge into clinical decision-making to optimize maternal and fetal outcomes during labor
Introduction
- Labor is a physiological process involving a series of coordinated events that lead to the expulsion of the fetus, placenta, and membranes from the uterus
- The Process of Labor is classically explained using the 4 Ps:
- Powers → Uterine contractions and maternal pushing efforts
- Passageway → Maternal pelvis and soft tissues
- Passenger → Fetus and placenta
- Psyche → Maternal psychological state
- Powers are the primary driving force of labor, responsible for:
- Cervical effacement (thinning)
- Cervical dilation (opening)
- Fetal descent through the birth canal
- Labor progression depends on the synchronization between uterine contractility and maternal expulsive efforts
- Hormonal influences regulating labor include:
- Oxytocin → stimulates uterine contractions
- Prostaglandins → enhance uterine activity and cervical ripening
- Estrogen → increases uterine sensitivity to oxytocin
- Progesterone withdrawal → facilitates initiation of labor
- Cellular basis of uterine contractions:
- Myometrial cells exhibit electrical excitability and coordinated contraction
- Presence of gap junctions allows synchronized contraction waves
Nursing Insights
- Effective labor is not determined by contraction presence alone, but by quality and coordination of uterine activity
- A nurse must assess not just contraction pattern but also cervical change and fetal response
- In clinical practice, failure of powers is one of the most common causes of prolonged labor
Powers (Uterine Forces And Maternal Efforts)
3.1 Physiology Of Uterine Contractions
- Uterine contractions originate from pacemaker areas located near the fundus of the uterus
- Contractions follow a fundal dominance pattern:
- Begin at fundus
- Spread downward
- Result in downward fetal movement
- Mechanism of contraction:
- Myometrial cells contract through actin-myosin interaction
- Triggered by calcium ion influx (Ca²⁺)
- Energy provided by ATP hydrolysis
- Unique features of uterine contractions:
- Involuntary and rhythmic
- Exhibit polarity (fundus contracts strongly, lower segment relaxes)
- Retraction:
- Muscle fibers shorten permanently after contraction
- Leads to progressive cervical dilation and fetal descent
- Phases of contraction:
- Increment → buildup phase
- Acme → peak intensity
- Decrement → relaxation phase
Nursing Insights
- Retraction is clinically important because it prevents reversal of cervical dilation
- Lack of coordinated contractions may indicate uterine inertia
- Continuous monitoring is necessary to assess fetal tolerance to contractions
3.2 Types Of Uterine Forces: Primary And Secondary Powers
Primary Powers
- Involuntary uterine contractions
- Responsible for:
- Cervical effacement
- Cervical dilation
- Initial fetal descent
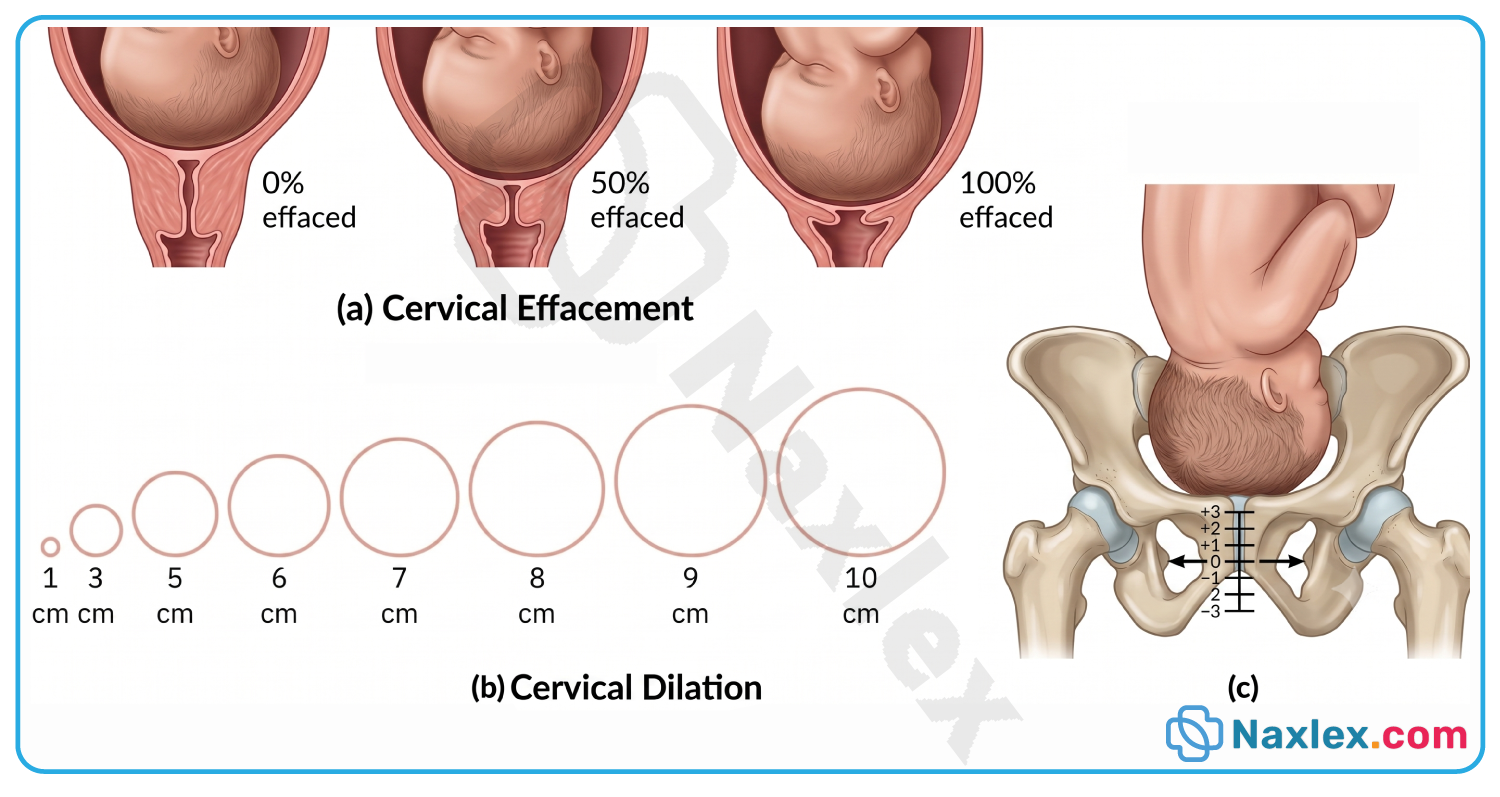
Secondary Powers
- Voluntary pushing efforts by the client
- Occur during second stage of labor
- Enhance fetal descent and expulsion
- Mechanism:
- Increased intra-abdominal pressure via:
- Diaphragm contraction
- Abdominal muscle contraction
- Increased intra-abdominal pressure via:
Comparison Table
|
Feature |
Primary Powers |
Secondary Powers |
|
Control |
Involuntary |
Voluntary |
|
Origin |
Uterus |
Maternal muscles |
|
Function |
Dilatation & effacement |
Fetal expulsion |
|
Timing |
Entire labor |
Second stage |
Nursing Insights
- Ineffective pushing may result from:
- Epidural anesthesia
- Maternal exhaustion
- Coaching the client on proper pushing techniques improves outcomes
- Avoid prolonged Valsalva maneuver due to risk of fetal hypoxia
3.3 Characteristics Of Effective Contractions (Frequency, Duration, Intensity)
- Frequency:
- Time from beginning of one contraction to beginning of next
- Normal:
- Early labor: 5–30 min
- Active labor: 2–5 min
- Duration:
- Length of each contraction
- Normal:
- Early labor: 30–45 sec
- Active labor: 60–90 sec
- Intensity:
- Strength of contraction
- Measured via:
- Palpation (mild, moderate, strong)
- Internal monitor (mmHg)
- Resting Tone:
- Pressure between contractions
- Should be <20 mmHg
Nursing Insights
- Adequate uterine perfusion occurs between contractions, not during contractions
- Excessively frequent contractions (>5 in 10 min) can cause uteroplacental insufficiency
- Nurses must monitor for tachysystole (>5 contractions in 10 min)
3.4 Uterine Contraction Monitoring (External And Internal Methods)
External Monitoring (Tocodynamometer)
- Placed on abdomen
- Measures:
- Frequency
- Duration
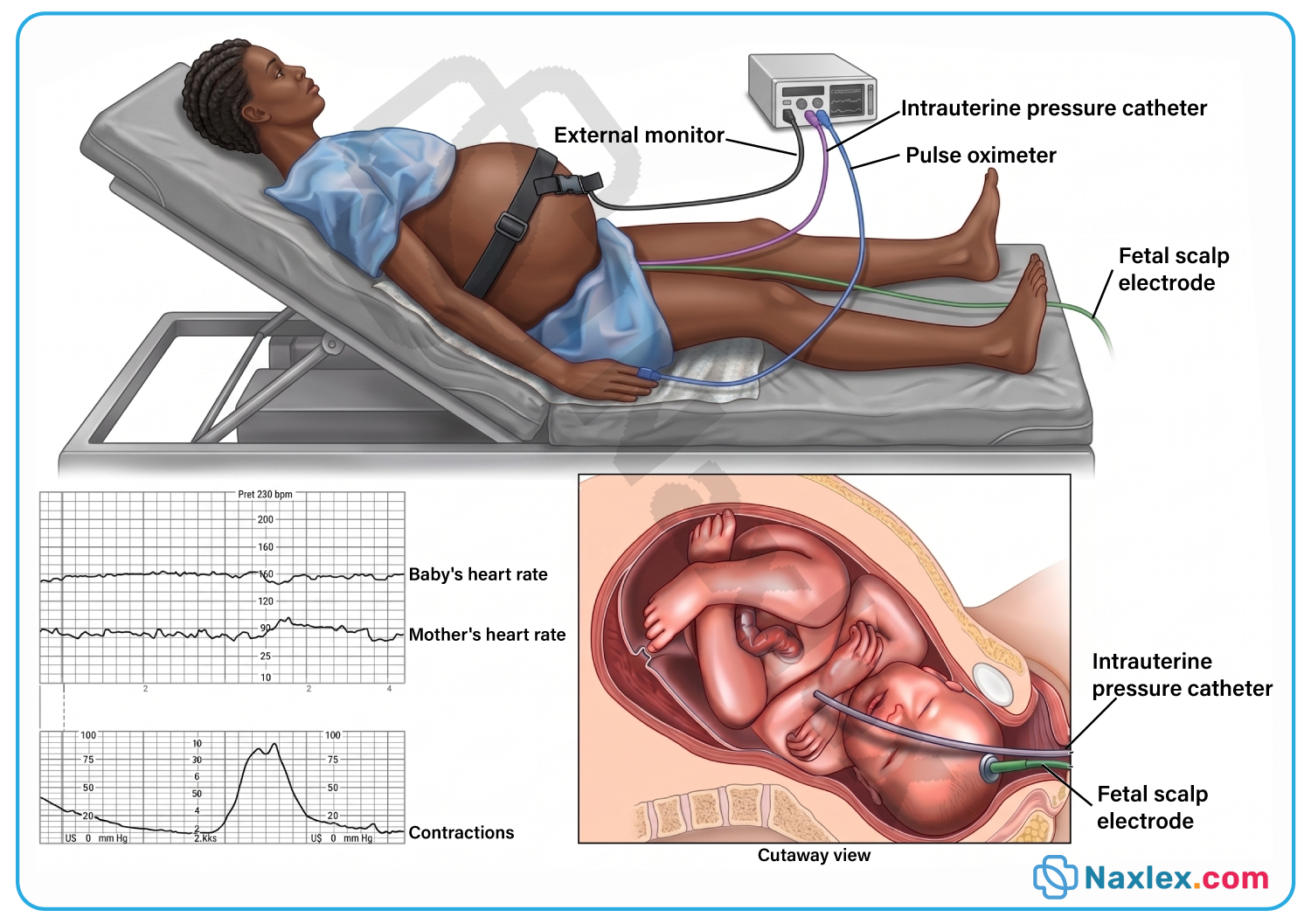
- Limitations:
- Cannot measure intensity accurately
Internal Monitoring (Intrauterine Pressure Catheter – IUPC)
- Inserted into uterine cavity
- Measures:
- Frequency
- Duration
- Intensity (mmHg)
- Montevideo Units (MVU):
- Sum of contraction intensities in 10 min
- Adequate labor: ≥200 MVU
Nursing Insights
- Internal monitoring requires:
- Ruptured membranes
- Cervical dilation
- Risk of infection increases with invasive monitoring
- Nurses must ensure aseptic technique
3.5 Dysfunctional Labor Patterns Related To Powers
Hypotonic Labor Dysfunction
- Weak, ineffective contractions
- Occurs in active phase
- Causes:
- Uterine overdistention
- Maternal exhaustion
- Effects:
- Slow cervical dilation
- Prolonged labor
Hypertonic Labor Dysfunction
- Uncoordinated, frequent contractions
- Occurs in latent phase
- Effects:
- Painful contractions
- Minimal cervical change
Tachysystole
- 5 contractions in 10 min
- Risks:
- Fetal hypoxia
- Decreased placental perfusion
Nursing Insights
- Hypotonic labor may require oxytocin augmentation
- Hypertonic labor often requires rest, sedation, or hydration
- Immediate intervention is required if fetal distress occurs
Passageway (Maternal Pelvis And Soft Tissues)
- The passageway refers to the anatomical structures through which the fetus passes during labor
- It includes:
- Bony pelvis → rigid structure forming the birth canal
- Soft tissues → cervix, pelvic floor muscles, vagina, and perineum
- The adequacy of the passageway is critical in determining:
- Ease of fetal descent
- Progress of labor
- Likelihood of vaginal birth vs operative delivery
5.1 Anatomy Of The Bony Pelvis
- The pelvis is composed of:
- 2 innominate bones (hip bones)
- Sacrum
- Coccyx
- Each innominate bone consists of:
- Ilium
- Ischium
- Pubis
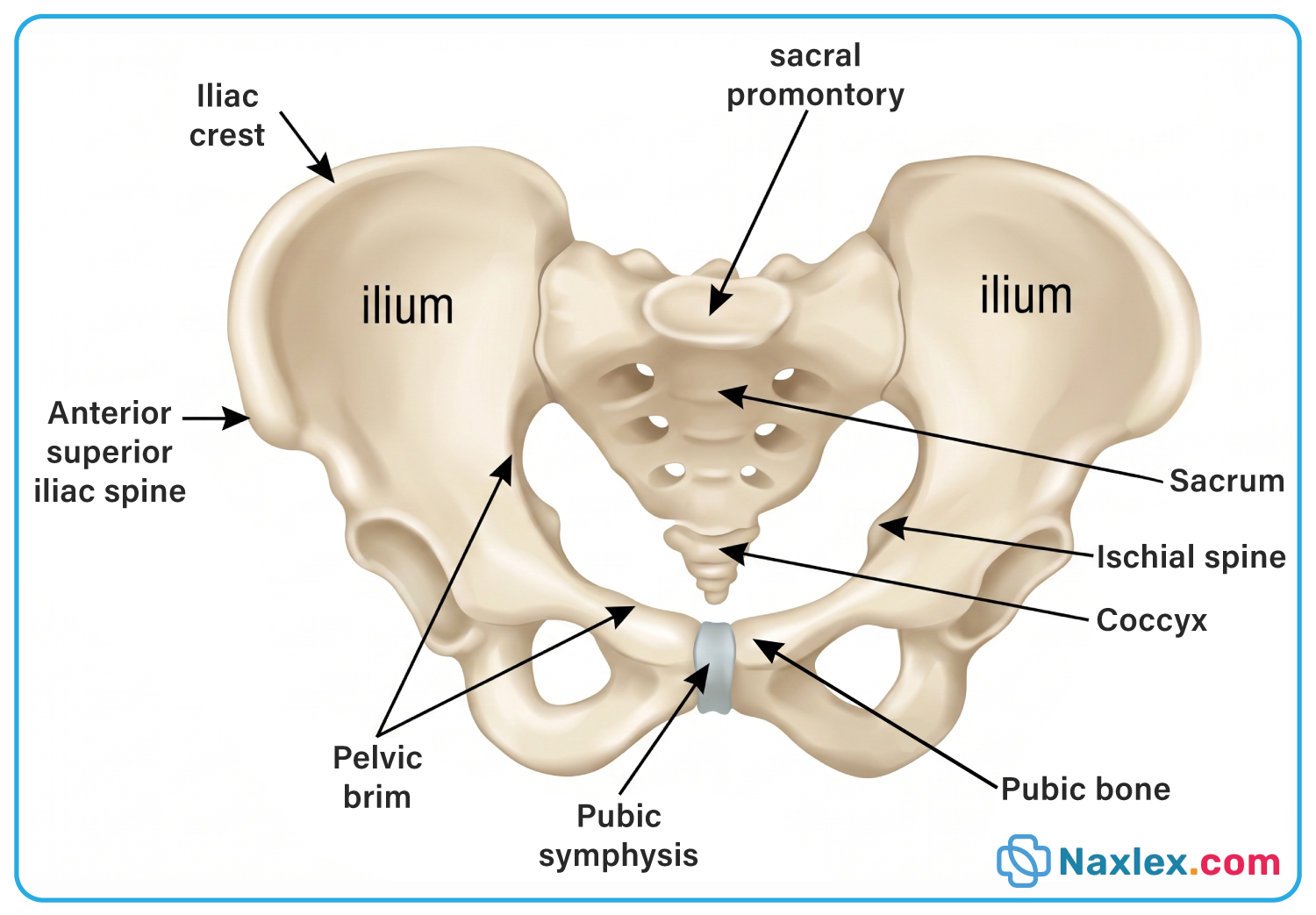
Divisions Of The Pelvis
- False Pelvis (Greater Pelvis):
- Located above pelvic brim
- Supports abdominal organs
- Not directly involved in childbirth
- True Pelvis (Lesser Pelvis):
- Located below pelvic brim
- Forms the birth canal
Pelvic Planes
- Pelvic Inlet:
- Upper opening of true pelvis
- Determines fetal entry
- Midpelvis:
- Area between inlet and outlet
- Critical for fetal descent
- Pelvic Outlet:
- Lower opening
- Determines fetal exit
Nursing Insights
- The midpelvis is the narrowest portion, making it a common site for labor arrest
- A prominent ischial spine may indicate potential obstruction
- Assessment of pelvis is done clinically via pelvimetry, though rarely used routinely
5.2 Types Of Female Pelvis (Gynecoid, Android, Anthropoid, Platypelloid)
Gynecoid Pelvis (Ideal for Childbirth)
- Rounded inlet
- Wide pubic arch (>90°)
- Straight sidewalls
- Most favorable for vaginal delivery
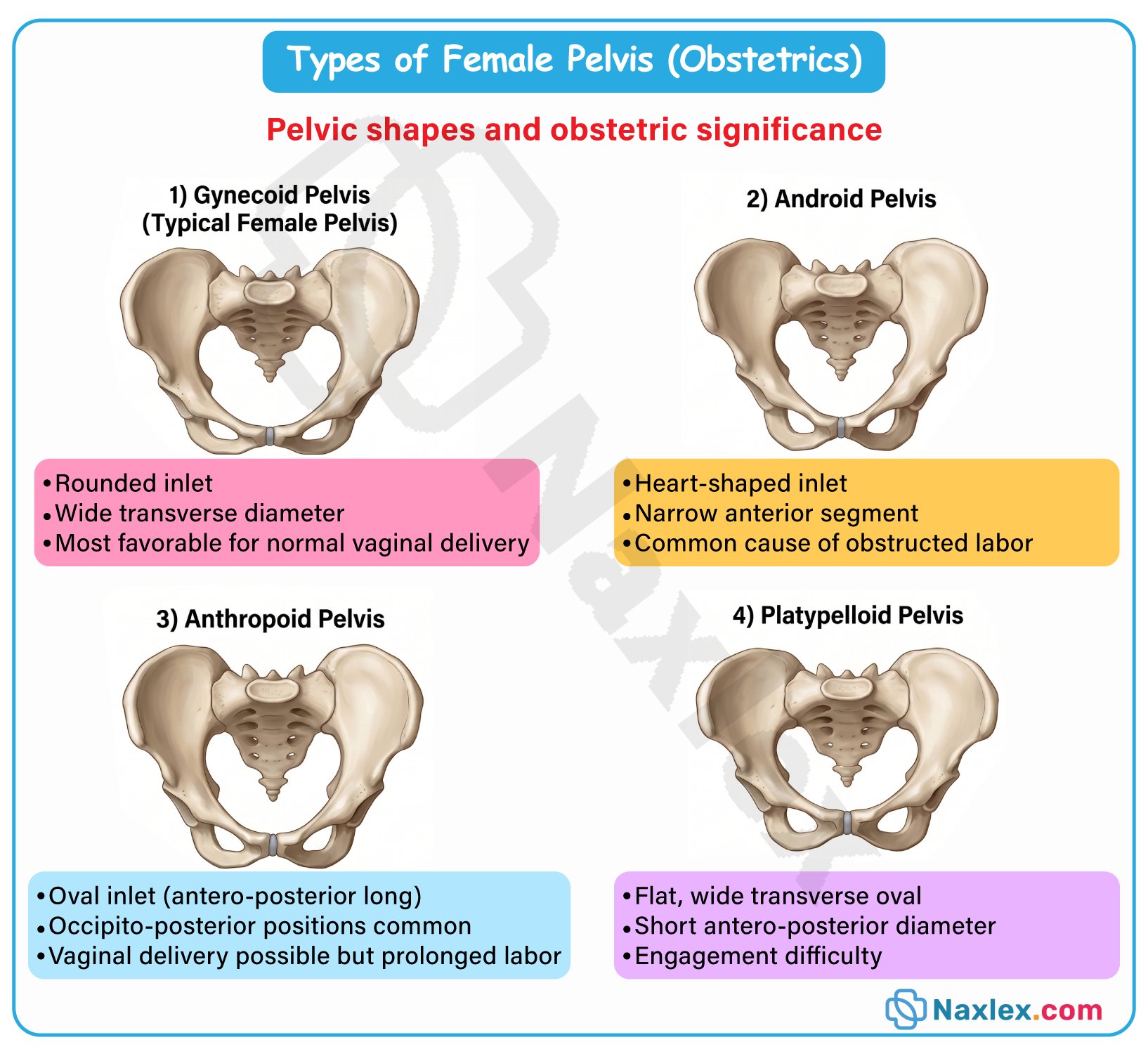
Android Pelvis
- Heart-shaped inlet
- Narrow pubic arch (<70°)
- Prominent ischial spines
- Associated with:
- Arrest of descent
- Increased operative deliveries
Anthropoid Pelvis
- Oval shape (anteroposterior diameter > transverse)
- Long narrow inlet
- Associated with:
- Occiput posterior positions
Platypelloid Pelvis
- Flattened shape
- Wide transverse diameter
- Short anteroposterior diameter
- Associated with:
- Difficulty in fetal engagement
Comparison Table
|
Pelvis Type |
Shape |
Obstetric Outcome |
|
Gynecoid |
Round |
Favorable |
|
Android |
Heart-shaped |
Difficult labor |
|
Anthropoid |
Oval |
OP positions |
|
Platypelloid |
Flat |
Delayed engagement |
Nursing Insights
- Most women have mixed pelvic types
- Pelvic shape influences:
- Fetal position
- Labor duration
- Nurses must anticipate complications based on pelvic type
5.3 Pelvic Diameters And Their Obstetric Significance
Pelvic Inlet Diameters
- Anteroposterior (True Conjugate):
- From sacral promontory to symphysis pubis
- Critical for fetal head entry
- Diagonal Conjugate:
- Clinically measurable
- Used to estimate true conjugate
- Transverse Diameter:
- Widest diameter of inlet
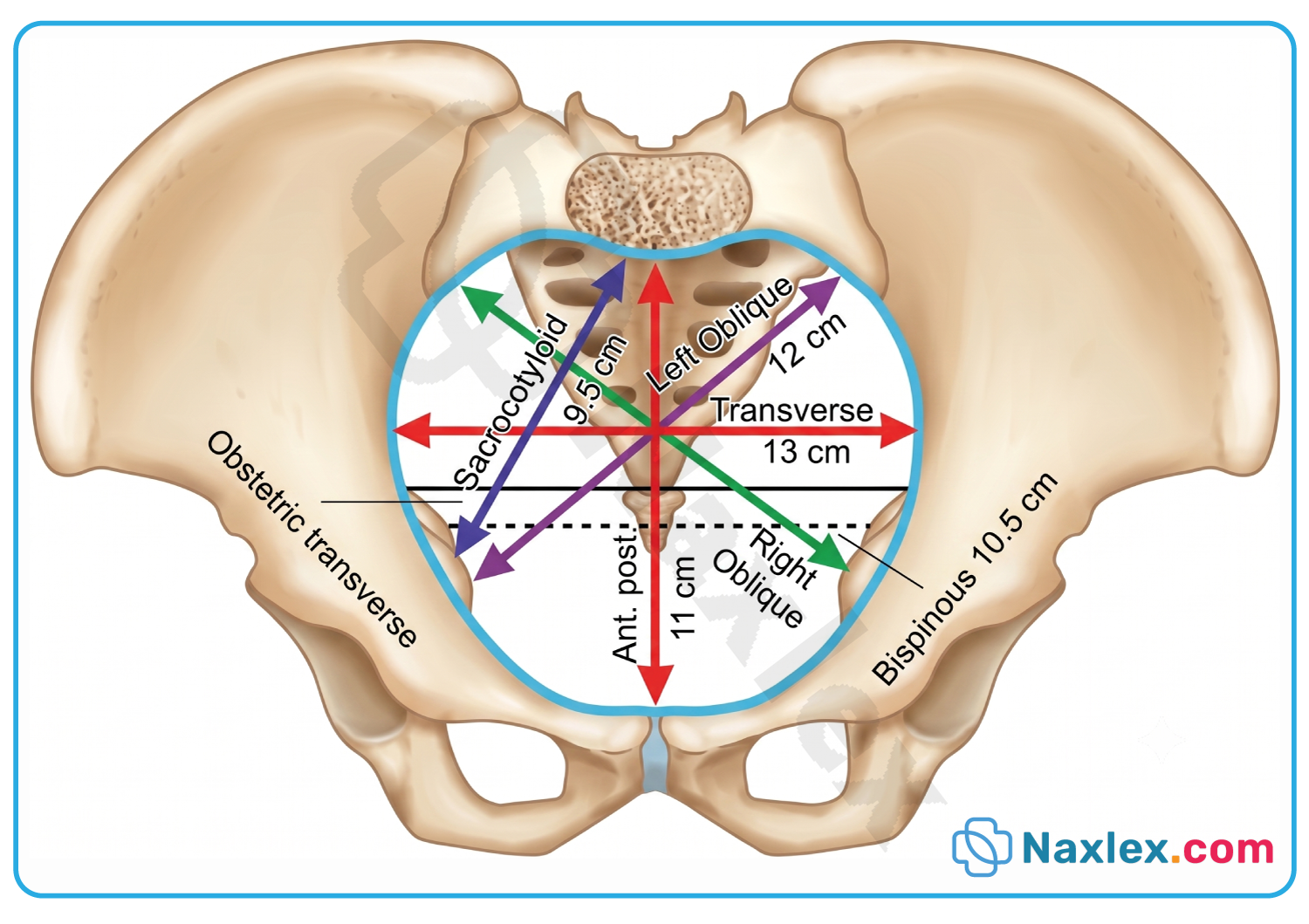
Midpelvis Diameter
- Interspinous Diameter:
- Distance between ischial spines
- Narrowest pelvic diameter
Pelvic Outlet Diameters
- Anteroposterior Diameter:
- From symphysis pubis to coccyx
- Transverse Diameter:
- Between ischial tuberosities
Nursing Insights
- Adequate diameters are essential for cephalopelvic compatibility
- Narrow diameters may result in:
- Cephalopelvic disproportion (CPD)
- CPD leads to:
- Prolonged labor
- Need for cesarean delivery
5.4 Soft Tissue Structures Affecting Labor (Cervix, Vagina, Perineum)
Cervix
- Undergoes:
- Effacement (0–100%)
- Dilation (0–10 cm)
- Softening due to:
- Prostaglandins
- Hormonal changes
Vagina
- Highly elastic structure
- Expands to accommodate fetal passage
Perineum
- Area between vaginal opening and anus
- Stretches during delivery
- May require:
- Episiotomy (rare in modern practice)
Nursing Insights
- Cervical change is the primary indicator of labor progress
- A rigid cervix may indicate:
- Ineffective labor
- Perineal support reduces:
- Risk of lacerations
5.5 Factors Affecting Passageway Adequacy
- Pelvic size and shape
- Soft tissue compliance
- Presence of obstruction:
- Fibroids
- Full bladder
- Tumors
- Maternal positioning:
- Upright positions improve pelvic dimensions
- Parity:
- Multiparous clients have more compliant tissues
Nursing Insights
- Encourage frequent voiding to prevent bladder obstruction
- Position changes can:
- Increase pelvic diameter
- Facilitate fetal descent
- Continuous assessment is needed for:
- Signs of obstructed labor
Passenger (Fetus And Placenta)
- The passenger refers to the fetus and placenta, which must successfully navigate the maternal passageway under the influence of uterine powers
- The characteristics of the passenger significantly influence:
- Labor progress
- Type of delivery
- Maternal and fetal outcomes
- Critical fetal factors include:
- Lie
- Attitude
- Presentation
- Position
- Size and skull adaptability
7.1 Fetal Lie, Attitude, Presentation, And Position
Fetal Lie
- Relationship between the long axis of the fetus and the long axis of the uterus
- Types:
- Longitudinal lie → most common
- Transverse lie → shoulder presentation
- Oblique lie → unstable, intermediate position
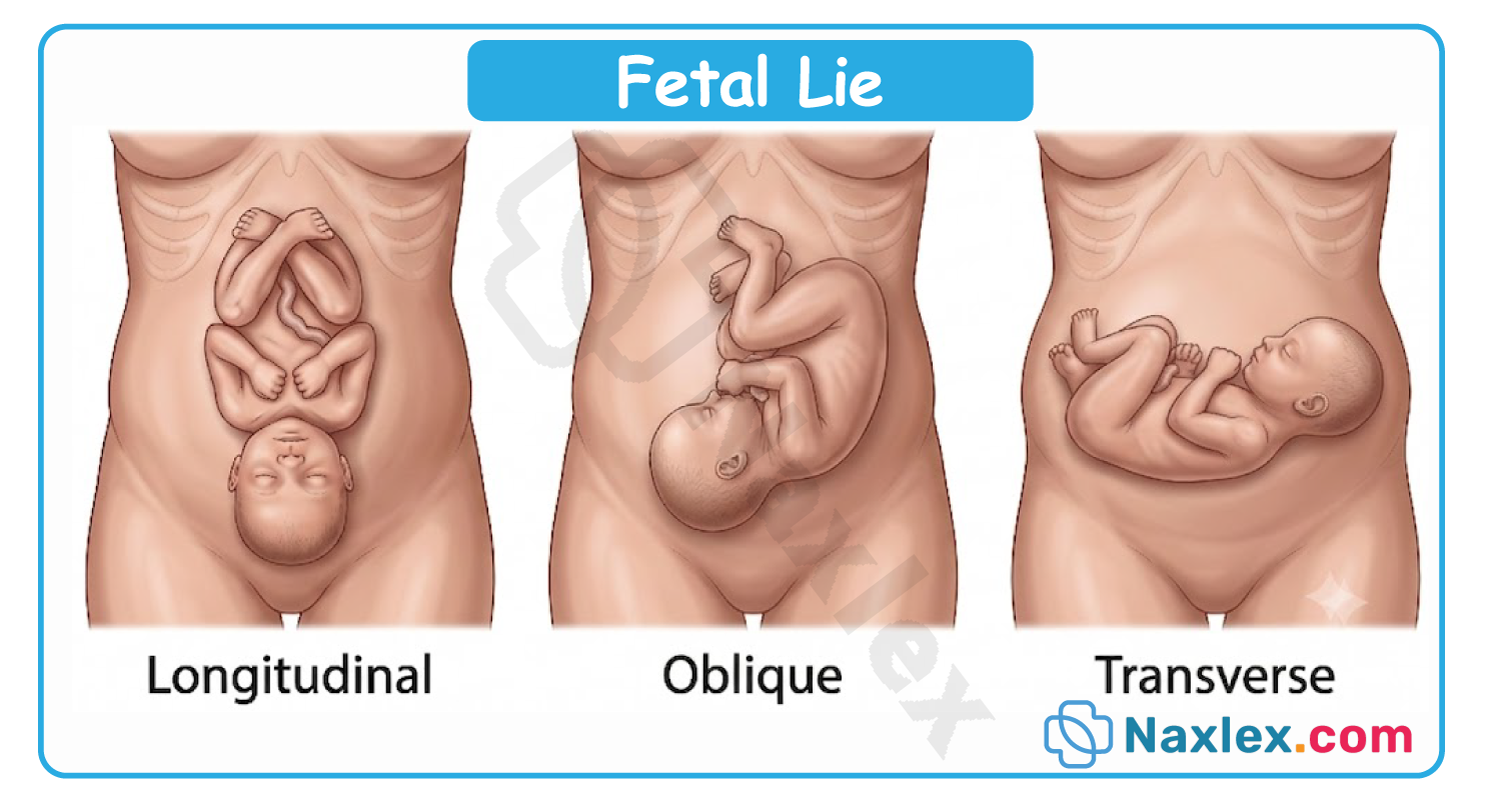
Fetal Attitude
- Relationship of fetal parts to one another
- Normal:
- Flexion → chin to chest, arms and legs flexed
- Abnormal:
- Extension → leads to larger presenting diameters
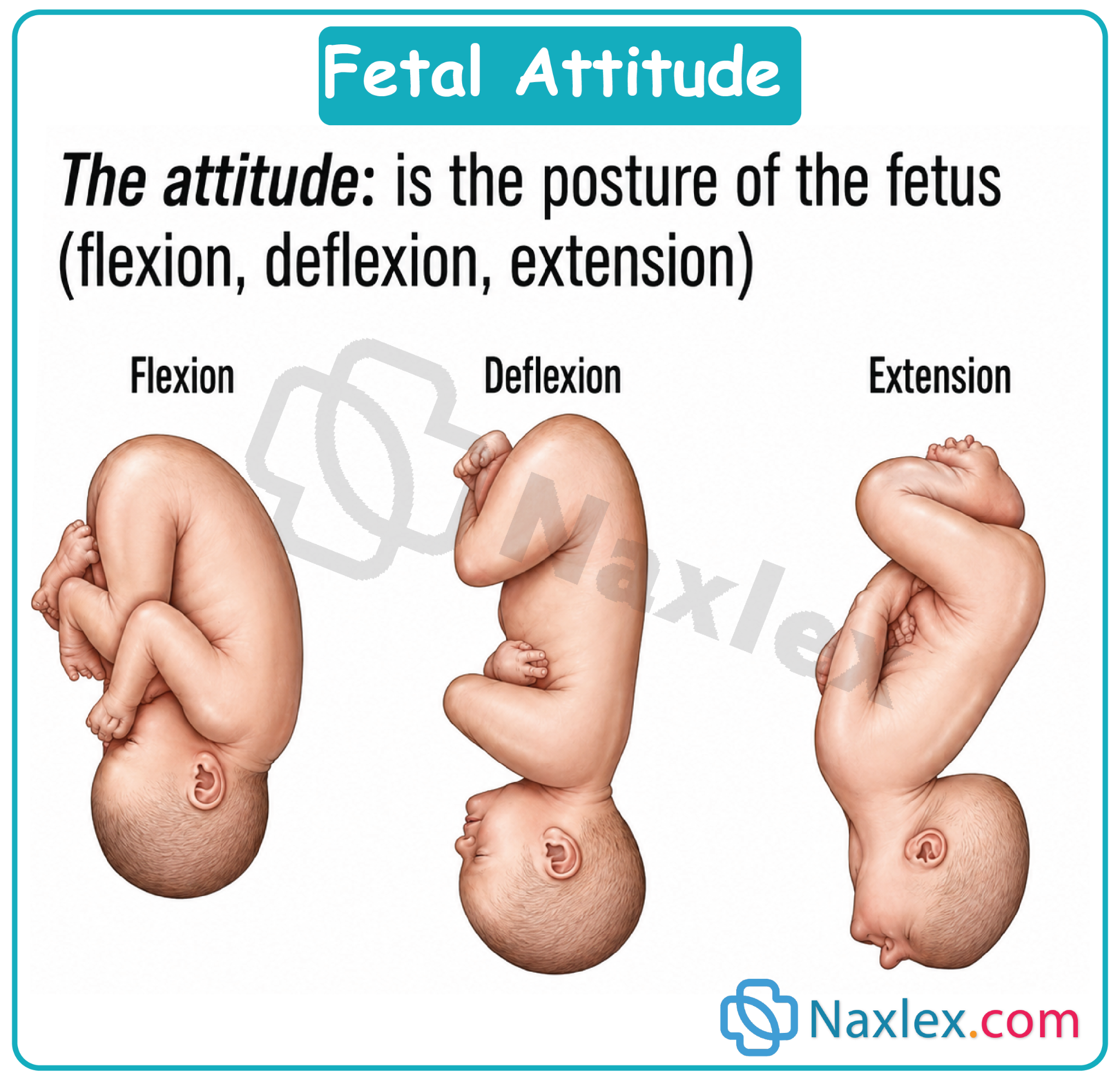
Fetal Presentation
- Part of fetus entering pelvic inlet
- Types:
- Cephalic (head) → most common
- Breech (buttocks/feet)
- Shoulder (transverse lie)
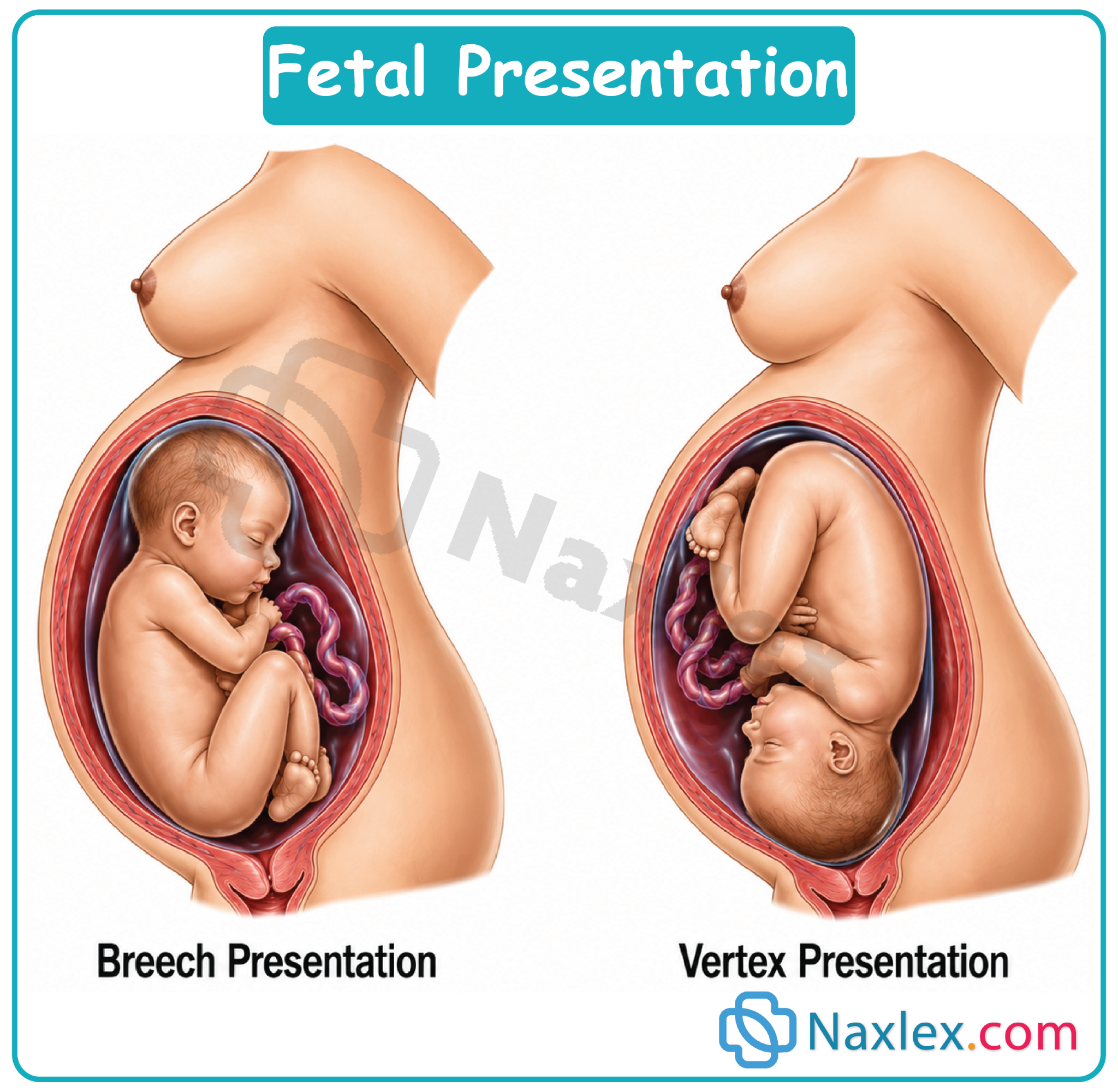
Fetal Position
- Relationship of presenting part to maternal pelvis
- Landmarks:
- Occiput (cephalic)
- Sacrum (breech)
- Example:
- Left Occiput Anterior (LOA) → most favorable
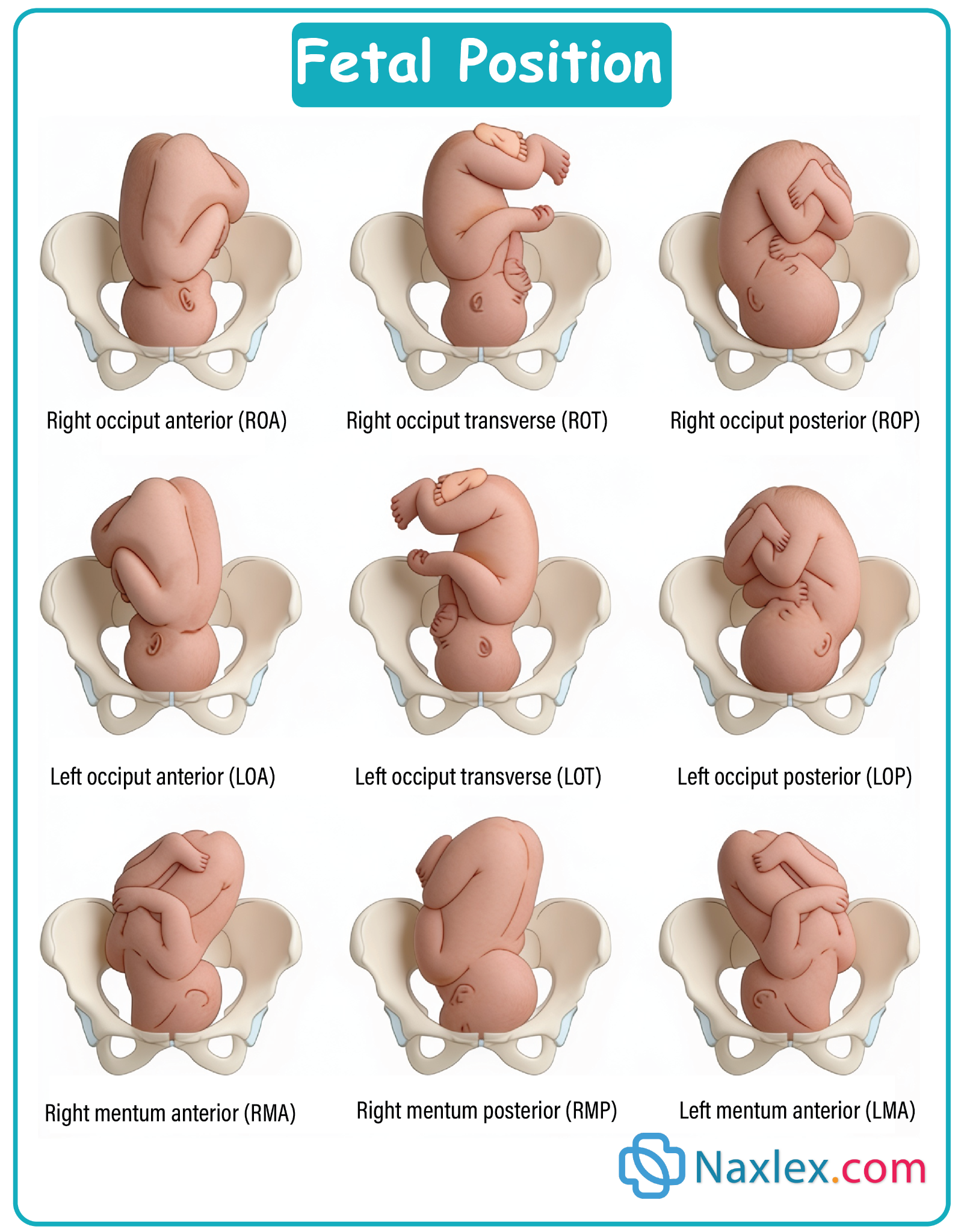
Nursing Insights
- LOA position allows optimal fetal descent and rotation
- Persistent occiput posterior (OP) leads to:
- Back labor
- Prolonged second stage
- Transverse lie is incompatible with vaginal delivery
7.2 Fetal Station And Engagement
Fetal Station
- Degree of descent of presenting part in relation to ischial spines
- Measurement:
- 0 station → at ischial spines
- Negative (-) → above spines
- Positive (+) → below spines
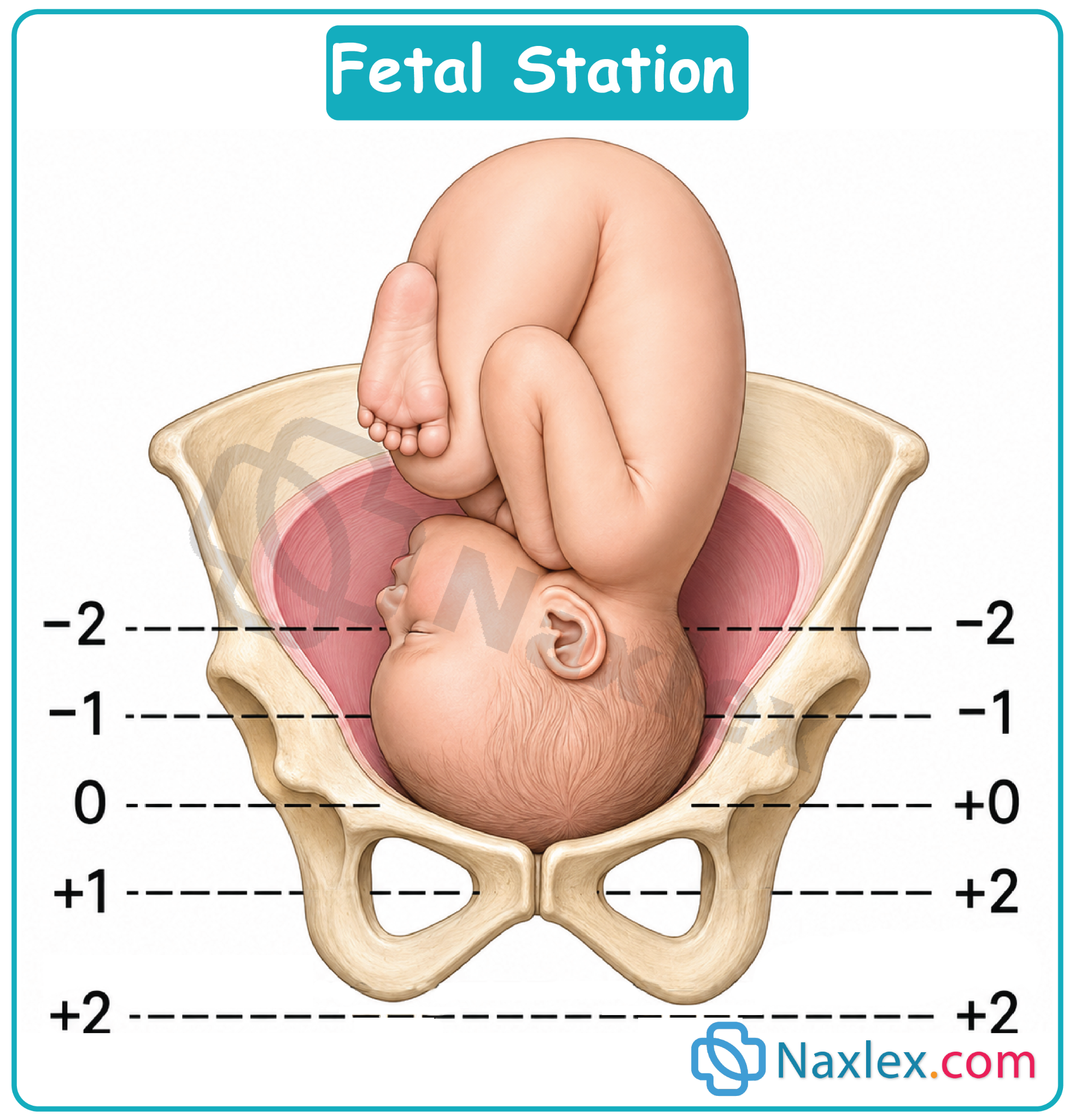
Engagement
- Occurs when:
- Largest diameter of fetal head passes pelvic inlet
- Typically at:
- 0 station
Nursing Insights
- Engagement in primigravida often occurs before labor onset
- Lack of engagement may indicate:
- Cephalopelvic disproportion (CPD)
- Station assessment helps determine labor progress
7.3 Cardinal Movements Of Labor
- Sequence of movements that fetus undergoes to navigate the birth canal:
- Engagement
- Descent
- Flexion
- Internal Rotation
- Extension
- External Rotation (Restitution)
- Expulsion
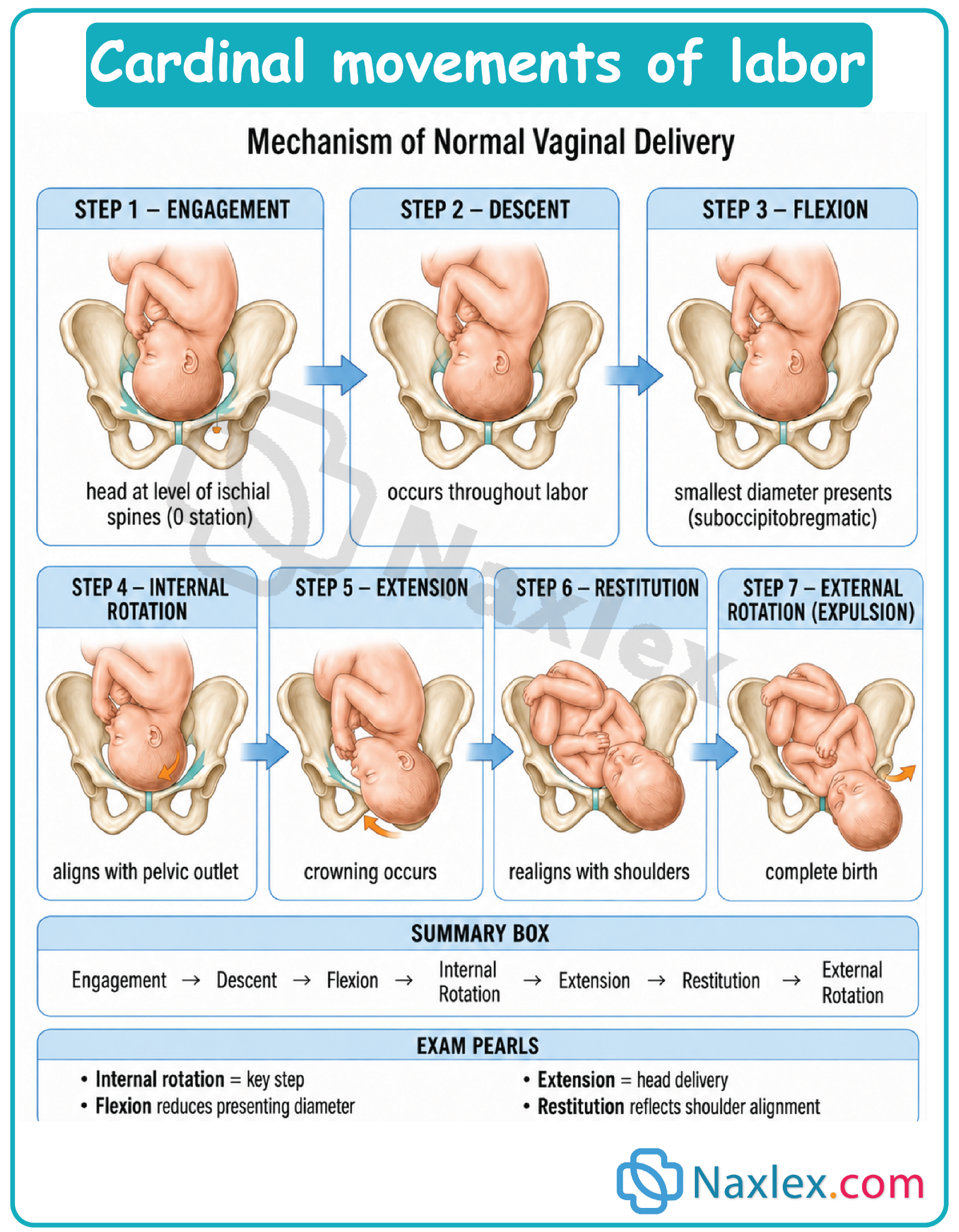
Detailed Breakdown
- Flexion:
- Reduces fetal head diameter
- Internal Rotation:
- Aligns fetal head with pelvic outlet
- Extension:
- Head emerges under pubic symphysis
- External Rotation:
- Realignment of head with shoulders
Nursing Insights
- Arrest at any stage indicates:
- Labor dysfunction
- Failure of rotation may require:
- Operative intervention
- Nurses must recognize normal vs abnormal progression
7.4 Fetal Size, Skull Sutures, And Fontanelles
Fetal Size
- Average term fetus:
- Weight: 2.5–4 kg
- Larger fetus increases risk of:
- Shoulder dystocia
- CPD
Fetal Skull Anatomy
- Bones:
- Frontal
- Parietal
- Occipital
- Sutures:
- Sagittal
- Coronal
- Lambdoid
- Allow:
- Molding → overlapping of bones
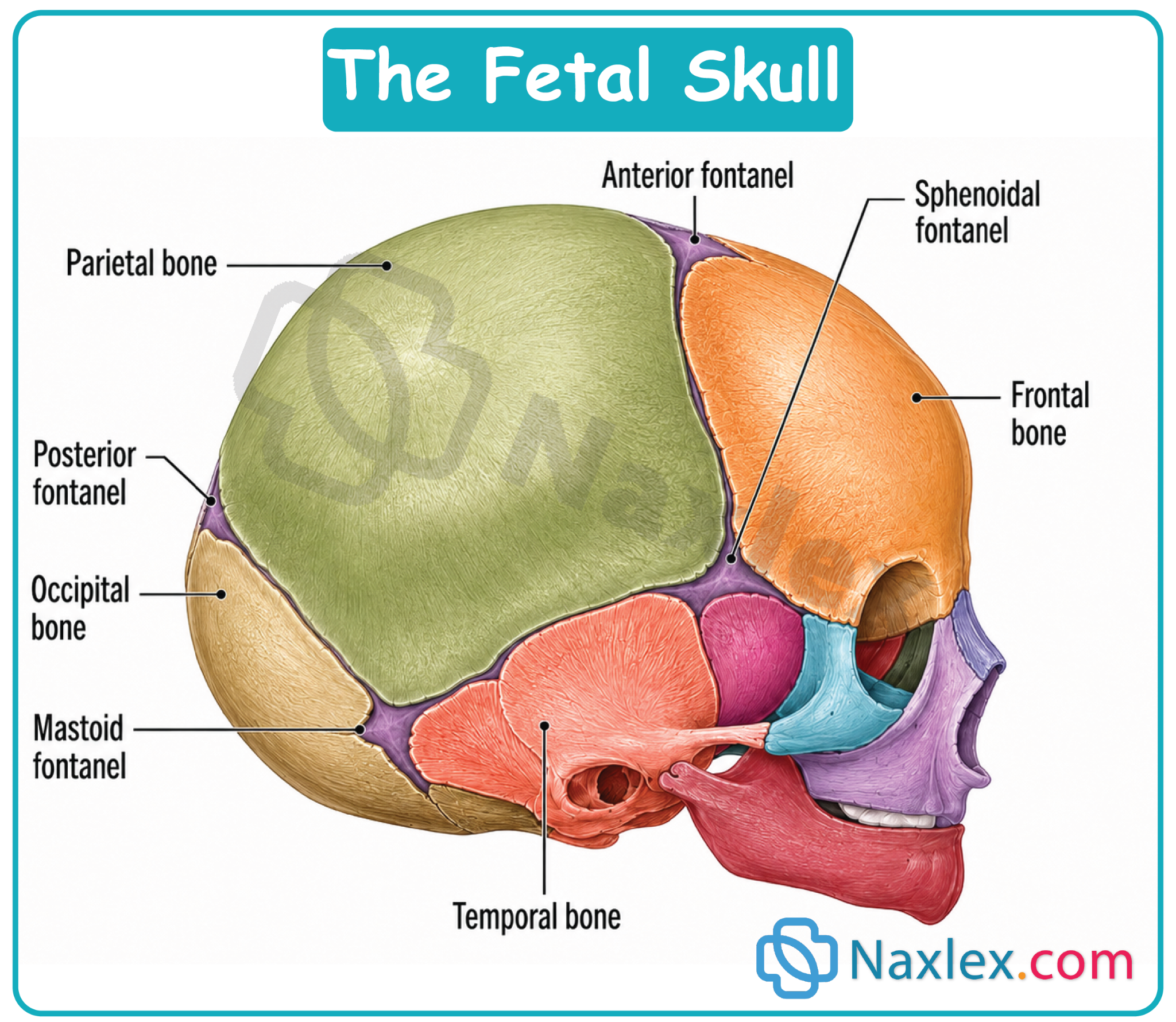
Fontanelles
- Anterior fontanelle:
- Diamond-shaped
- Posterior fontanelle:
- Triangular
- Used to determine:
- Fetal position
Nursing Insights
- Molding is a normal adaptation but excessive molding may indicate:
- Obstructed labor
- Palpation of sutures helps identify:
- Fetal orientation
7.5 Placental Factors Affecting Labor
- Placenta plays a key role in:
- Oxygen and nutrient exchange
Placental Position
- Normal → upper uterine segment
- Abnormal:
- Placenta previa → obstructs cervical opening
- Placental abruption → premature separation
Umbilical Cord Factors
- Cord compression may cause:
- Fetal distress
Nursing Insights
- Placenta previa is a contraindication to vaginal delivery
- Monitor for:
- Bleeding
- Fetal heart rate abnormalities
- Prompt intervention is critical
Psyche (Maternal Psychological Response)
- The psyche refers to the maternal psychological and emotional state during labor
- It is a critical determinant of:
- Labor progression
- Pain perception
- Maternal coping ability
- Fetal well-being
- Psychological responses influence physiological processes through:
- Neuroendocrine pathways
- Autonomic nervous system activation
9.1 Maternal Emotional State And Labor Progress
- Maternal emotional states include:
- Calmness
- Anxiety
- Fear
- Excitement
- Positive emotional state leads to:
- Efficient uterine contractions
- Shorter labor duration
- Improved maternal cooperation
- Negative emotional state leads to:
- Increased catecholamine release
- Inhibition of uterine contractions
- Prolonged labor
Nursing Insights
- Emotional distress can manifest as:
- Increased pain perception
- Ineffective pushing
- Nurses must continuously assess:
- Verbal cues
- Non-verbal behaviors (restlessness, tension)
- Emotional support directly improves labor outcomes
9.2 Influence Of Anxiety, Fear, And Stress Hormones
- Anxiety and fear activate:
- Sympathetic nervous system
- Release of stress hormones:
- Epinephrine
- Norepinephrine
- Cortisol
Physiological Effects
- Decreased uterine blood flow
- Reduced oxytocin effectiveness
- Increased uterine dysfunction
- Effects on fetus:
- Reduced oxygen supply
- Risk of fetal distress
Pain Perception
- Anxiety lowers pain threshold
- Leads to:
- Increased perception of contraction pain
- Exhaustion
Nursing Insights
- Fear–tension–pain cycle:
- Fear → muscle tension → increased pain → more fear
- Breaking this cycle is essential:
- Relaxation techniques
- Breathing exercises
- Nurses must recognize early signs of:
- Panic
- Hyperventilation
9.3 Cultural And Social Influences On Labor
- Cultural beliefs influence:
- Pain expression
- Labor practices
- Acceptance of interventions
Examples
- Some cultures:
- Encourage vocal expression of pain
- Others:
- Promote stoicism
Cultural Considerations
- Beliefs about:
- Modesty
- Gender roles
- Presence of family members
Nursing Insights
- Provide culturally competent care:
- Respect beliefs
- Avoid assumptions
- Assess individual preferences rather than generalizing
- Incorporate cultural practices when safe
9.4 Support Systems And Their Role In Labor Outcomes
- Support systems include:
- Partner
- Family members
- Doula
- Health care team
Benefits Of Continuous Support
- Shorter labor duration
- Reduced need for:
- Analgesia
- Operative delivery
- Improved maternal satisfaction
Types Of Support
- Emotional:
- Reassurance
- Encouragement
- Physical:
- Positioning
- Massage
- Informational:
- Explaining procedures
Nursing Insights
- Continuous presence of a support person:
- Decreases anxiety
- Improves coping
- Nurses play a key role when:
- Support system is absent
9.5 Nursing Interventions To Promote Positive Psyche
Assessment
- Evaluate:
- Anxiety level
- Coping mechanisms
- Support availability
Interventions
- Provide:
- Clear explanations of procedures
- Continuous reassurance
- Promote:
- Relaxation techniques
- Breathing exercises
- Encourage:
- Mobility and positioning
Environment Optimization
- Reduce:
- Noise
- Bright lights
- Maintain:
- Privacy
- Comfort
Communication
- Use:
- Therapeutic communication
- Active listening
Nursing Insights
- A calm environment enhances oxytocin release
- Avoid negative language that may increase fear
- Empower the client to:
- Participate in decision-making
Summary
- The process of labor is governed by the coordinated interaction of the 4 Ps:
- Powers
- Passageway
- Passenger
- Psyche
Powers
- Represent the forces of labor:
- Primary powers → involuntary uterine contractions responsible for:
- Cervical effacement and dilation
- Initial fetal descent
- Secondary powers → voluntary maternal pushing efforts aiding fetal expulsion
- Primary powers → involuntary uterine contractions responsible for:
- Effective contractions are characterized by:
- Frequency: 2–5 min apart in active labor
- Duration: 60–90 sec
- Intensity: sufficient to achieve ≥200 Montevideo Units (MVU)
- Dysfunctional labor patterns include:
- Hypotonic labor → weak contractions
- Hypertonic labor → uncoordinated contractions
- Tachysystole → >5 contractions in 10 min
Passageway
- Composed of:
- Bony pelvis
- Soft tissues (cervix, vagina, perineum)
- Pelvic types influence labor:
- Gynecoid → most favorable
- Android → associated with difficult labor
- Anthropoid → posterior positions
- Platypelloid → delayed engagement
- The interspinous diameter is the narrowest pelvic diameter
- Soft tissue changes include:
- Cervical dilation (0–10 cm)
- Effacement (0–100%)
Passenger
- Includes the fetus and placenta
- Key fetal characteristics:
- Lie → longitudinal most favorable
- Attitude → flexion reduces presenting diameter
- Presentation → cephalic preferred
- Position → LOA (Left Occiput Anterior) most optimal
- Fetal station indicates descent:
- 0 station = engagement
- Cardinal movements of labor:
- Engagement
- Descent
- Flexion
- Internal rotation
- Extension
- External rotation
- Expulsion
- Fetal skull:
- Sutures allow molding
- Fontanelles help determine position
Psyche
- Refers to maternal psychological state
- Positive psyche:
- Enhances oxytocin release
- Improves labor efficiency
- Negative psyche:
- Activates sympathetic nervous system
- Increases catecholamines, leading to:
- Decreased uterine perfusion
- Prolonged labor
- Support systems:
- Improve outcomes
- Reduce need for interventions
- Nursing interventions:
- Emotional support
- Education
- Relaxation techniques
- Cultural sensitivity
Nursing Insights
- The nurse must continuously evaluate all 4 Ps simultaneously, not in isolation
- Any imbalance among the 4 Ps may lead to:
- Labor dystocia
- Fetal compromise
- Early identification and intervention are critical to:
- Prevent complications
- Promote safe delivery
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Process of Labor (4 Ps)
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
