
Health problems in children (infancy to adolescence)
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Analyze nutritional health problems in infancy, including the management of severe acute malnutrition and food sensitivities.
- Evaluate risk factors and preventive nursing interventions for sudden infant death syndrome (SIDS) and positional plagiocephaly.
- Outline the principles of emergency treatment for the ingestion of injurious agents, specifically focusing on lead and heavy metal poisoning.
- Identify clinical indicators of child maltreatment (neglect, physical, and sexual abuse) and the nurse's legal role as a mandatory reporter.
- Assess behavioral and mental health disorders in school-aged children, including ADHD, Tourette Syndrome, and childhood depression.
- Manage pediatric-specific disorders of continence and functional abdominal pain through behavioral and physiological interventions.
- Differentiate between acute reproductive emergencies, such as testicular torsion, and chronic conditions like endometriosis or varicocele.
- Formulate comprehensive care plans for adolescents facing behavioral health challenges, including eating disorders, substance abuse, and suicidal ideation.
Introduction
- Pediatric nursing requires a vigilant understanding of age-specific health problems that can alter a child’s developmental trajectory.
- From the fragility of infancy to the complex psychosocial landscape of adolescence, the nurse serves as the primary detector of physiological and behavioral deviations.
- In infancy, health problems are often rooted in nutritional imbalances or sleep-related risks. Severe acute malnutrition and food sensitivities require immediate dietary intervention to prevent long-term growth stunting.
- Nurses must also educate parents on "Safe to Sleep" practices to mitigate the risk of sudden infant death syndrome (SIDS) and address physical concerns like positional plagiocephaly.
- As children move into early childhood, the focus shifts toward environmental safety and protection. This stage is marked by an increased risk of accidental ingestion of toxins, with lead poisoning remaining a significant public health concern.
- The nurse plays a critical role in identifying child maltreatment. Recognizing the subtle signs of neglect or the specific patterns of physical and sexual abuse is a vital nursing competency that requires both clinical skill and ethical fortitude. In these cases, the nurse is not only a caregiver but a legal advocate for the child’s safety.
- During the school-aged and adolescent years, health problems become increasingly complex, often involving a combination of physical and behavioral components.
- The rise in childhood obesity and dental disorders necessitates early lifestyle intervention.
- Meanwhile, the emergence of disorders like ADHD, anxiety, and depression requires a multidisciplinary approach.
- In adolescence, reproductive health and behavioral risks, such as eating disorders and substance abuse, take center stage.
- By understanding the full spectrum of these health problems, the nurse can provide targeted, evidence-based care that addresses the unique vulnerabilities of each developmental stage.
Health problems of the infant
3.1. Nutritional Imbalances (Vitamin imbalances, mineral imbalances)
Infants are particularly vulnerable to nutritional deficiencies due to their rapid growth and dependence on caregivers for food.
- Vitamin D Deficiency: Can lead to rickets, characterized by soft bones and skeletal deformities. Nursing management involves educating parents on the importance of vitamin D supplementation for breastfed infants and those who consume less than 32 oz of formula daily.
- Iron-Deficiency Anemia: Common after 6 months of age when maternal iron stores are depleted. Manifests as pallor, fatigue, and irritability. Nursing care focuses on encouraging iron-rich foods and supplementing as prescribed.
- Vitamin K Deficiency: In newborns, this can cause vitamin K deficiency bleeding (VKDB), a serious and potentially fatal condition. The standard nursing practice of administering a vitamin K injection at birth is a critical preventative measure.
- Vitamin A Deficiency: Vitamin A is essential for the development and function of the immune system. It helps maintain the integrity of epithelial tissues (skin, respiratory, and gastrointestinal mucosa), which serve as the body’s first line of defense against infections. It enhances antibody responses and T-cell–mediated immunity, which are vital for fighting measles infection. Measles causes depletion of vitamin A stores, even in well-nourished children. Deficiency worsens measles by increasing the risk of severe diarrhea, pneumonia, and blindness (keratomalacia). Vitamin A supplementation during measles reduces the severity of complications, shortens disease duration, and lowers the risk of hospitalization.
3.2. Health Problems Related to Nutrition
3.2.1. Severe acute malnutrition
Severe acute malnutrition (SAM) is a life-threatening condition resulting from insufficient intake of nutrients.
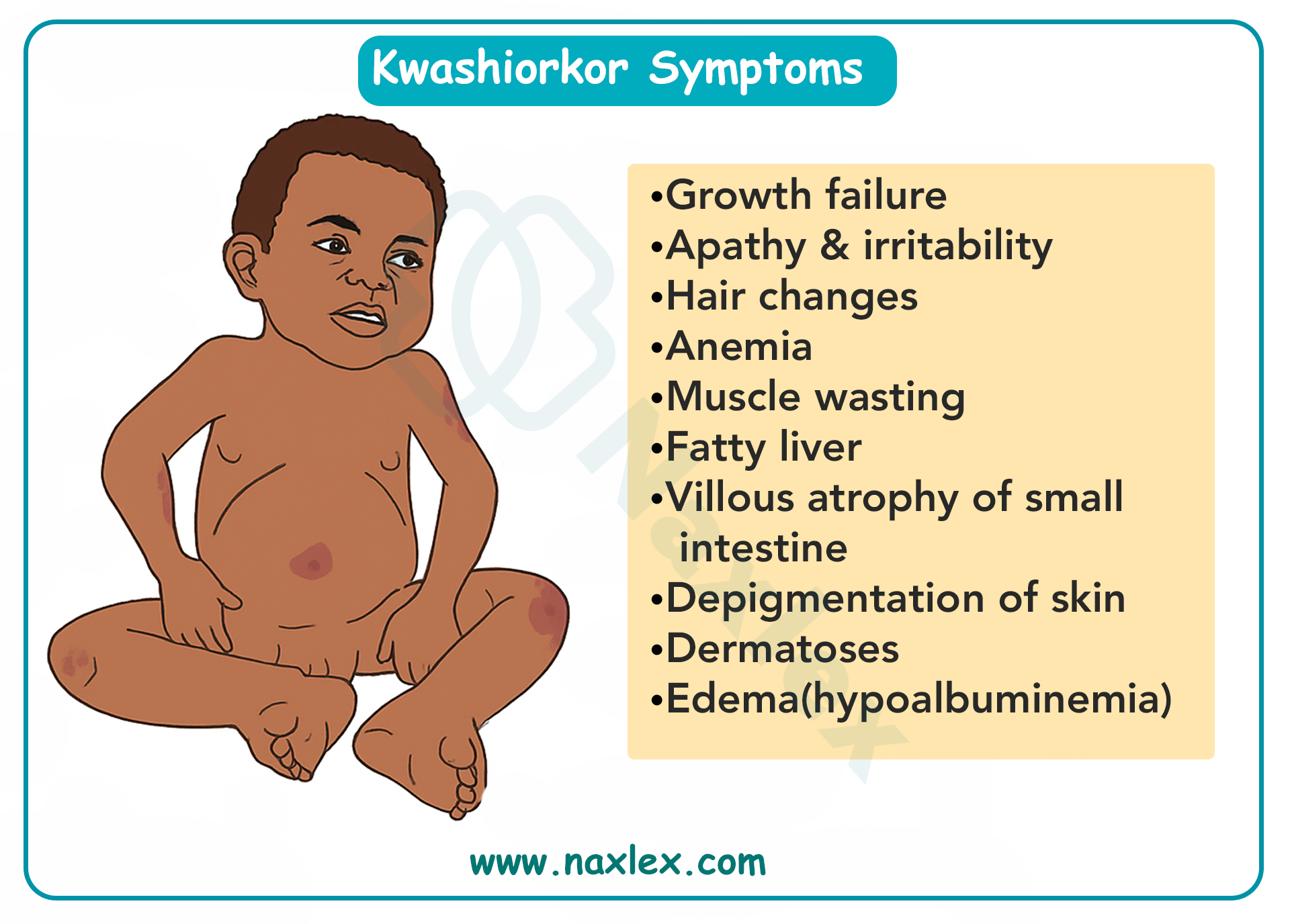
- Kwashiorkor: This form of SAM is caused by a severe protein deficiency. Symptoms include edema (swelling), particularly in the abdomen and face, giving the child a "pot belly" appearance, and thin, brittle hair. The child may be irritable and have a large, fatty liver.
- Marasmus: This is a severe deficiency of calories and protein. The child appears emaciated, with generalized muscle wasting and a thin, wrinkled face (often called an "old man" face). The skin hangs loosely in folds.
Nursing Management for Severe Acute Malnutrition (SAM):
- Fluid and Electrolyte Management: Carefully rehydrate the child using oral rehydration solution (ORS) to correct dehydration and electrolyte imbalances. Rapid rehydration can be dangerous, leading to refeeding syndrome.
- Nutritional Rehabilitation: The initial phase is slow and cautious to prevent refeeding syndrome. Start with small, frequent feedings of a high-protein, high-calorie formula. Gradually increase the quantity and concentration of feeds as the child stabilizes.
- Infection Control: Malnourished children are highly susceptible to infections due to a compromised immune system. Monitor for signs of sepsis and administer antibiotics as prescribed.
- Skin Care: Protect the skin, especially in marasmus patients, from breakdown and infection.
- Family Education: Teach parents about proper nutrition, hygiene, and the importance of follow-up care to prevent recurrence.
3.2.2. Food sensitivity
- Cow's Milk Allergy (CMA): This is an immune system reaction to the protein in cow's milk. Symptoms can be immediate (hives, wheezing, vomiting) or delayed (nausea, diarrhea, blood in stool, poor weight gain). Management involves eliminating cow's milk and using a hypoallergenic or amino acid-based formula.
- Lactose Intolerance: This is the inability to digest lactose, the sugar in milk, due to a deficiency of the lactase enzyme. Symptoms include gas, bloating, and diarrhea after consuming milk products. It is managed by using lactose-free formulas or products.
- Failure to Thrive (FTT): This describes inadequate weight gain and growth, falling below the 5th percentile for age. It can be organic (caused by an underlying medical condition like a metabolic disorder or congenital heart defect) or non-organic (related to psychosocial factors like neglect, poverty, or feeding problems). Nursing management includes a detailed feeding assessment, nutritional education for parents, and collaboration with social work if psychosocial factors are suspected.
Nursing Insight: When assessing an infant with suspected FTT, it is crucial to perform a detailed feeding history. This includes asking about the type of formula/breast milk, frequency of feedings, amount consumed, and the parent-infant interaction during feeding. This information can reveal a lot about the potential cause of FTT.
3.3. Special Health Problems
3.3.1. Colic
Colic is a condition in which an otherwise healthy infant cries inconsolably for an extended period, often at the same time each day, usually in the late afternoon or evening.
- The "Rule of Threes": Crying for more than 3 hours a day, at least 3 days a week, for more than 3 weeks.
- Causes: The exact cause is unknown, but theories include an immature digestive system, gas, or a hypersensitive temperament.
- Management: Reassurance for parents is key. Strategies include soothing techniques like swaddling, gentle rocking, "white noise" from a fan or machine, and pacifier use. Dietary changes may be explored, but their effectiveness is debated.
3.3.2. Sudden infant death syndrome (SIDS)
SIDS is the sudden, unexplained death of an infant under one year of age. It typically occurs during sleep.
- Risk Factors: Prone or side sleeping position, co-sleeping, soft bedding in the crib, overheating, maternal smoking during pregnancy, and a family history of SIDS.
- Prevention: The "Back to Sleep" campaign has significantly reduced SIDS rates. Infants should always be placed on their backs to sleep, on a firm surface, in a crib free of pillows, blankets, and stuffed animals.
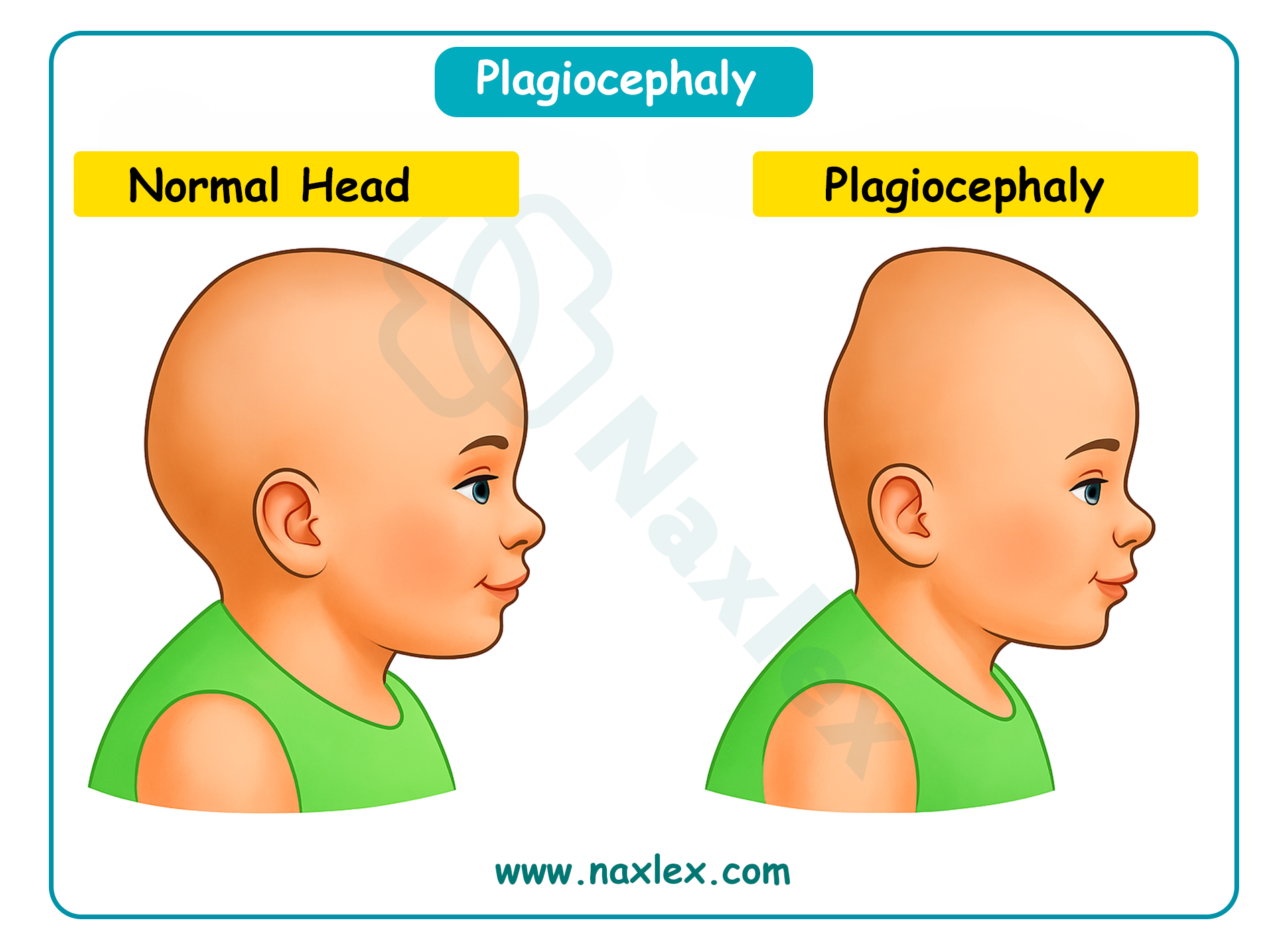
3.3.3. Positional plagiocephaly
Also known as "flat head syndrome," this is a condition where an infant's head becomes flattened on one side. It is most prevalent between 2 and 4 months of age.
- Causes: Occurs when an infant spends too much time in one position, such as sleeping on their back, resulting in pressure on the same part of the skull.
- Prevention: "Tummy time" while the infant is awake and supervised is a crucial preventative measure. Changing the infant's head position during sleep and holding the infant frequently can also help. In severe cases, a custom-fitted helmet may be used to promote resolution of cranial asymmetry while the infant’s head is still rapidly growing. Orthotic helmets do not actively mold the skull; instead, they protect the areas that are flattened and allow the child to “grow into” the flat spots.
3.3.4. Apparent life-threatening event (ALTE)
An ALTE is an episode in an infant that is frightening to the observer and is characterized by a combination of apnea (no breathing), a change in color (cyanosis or pallor), a change in muscle tone, and/or choking or gagging.
- Evaluation: An ALTE is a diagnosis of exclusion. A thorough medical evaluation is needed to rule out underlying medical conditions, such as gastroesophageal reflux, seizures, or heart problems.
- Management: Often involves hospitalization for monitoring and a comprehensive workup. Parents are taught CPR and how to use an apnea monitor if it's deemed necessary.
Health problems of early childhood
5.1. Sleep Problems
Sleep problems are common in early childhood and can affect both the child and the family. They range from difficulty falling or staying asleep to more complex sleep disorders.
- Sleep-Onset Association Disorder: This occurs when a child needs a specific object or routine (like being rocked, held, or having a bottle) to fall asleep. When they wake up during the night, they can't go back to sleep without that same association.
- Limit-Setting Sleep Disorder: This involves a child's resistance to bedtime or a parent's inability to set consistent sleep boundaries. This often leads to a long, drawn-out bedtime routine.
- Night Terrors: A child may suddenly wake up screaming or thrashing but remains in a sleep-like state and won't be able to recall the event in the morning. They're different from nightmares because the child isn't actually awake. Night terrors usually resolve on their own as the child matures, but supportive measures such as ensuring adequate sleep can help reduce frequency and severity.
- Nightmares: Nightmares are frightening dreams that a child can remember upon waking. They're common and usually occur during the second half of the night.
- Obstructive Sleep Apnea (OSA): A condition where a child's breathing is temporarily blocked during sleep, often due to enlarged tonsils or adenoids. This can lead to snoring, restless sleep, and daytime fatigue.
5.2. Ingestion of Injurious Agents
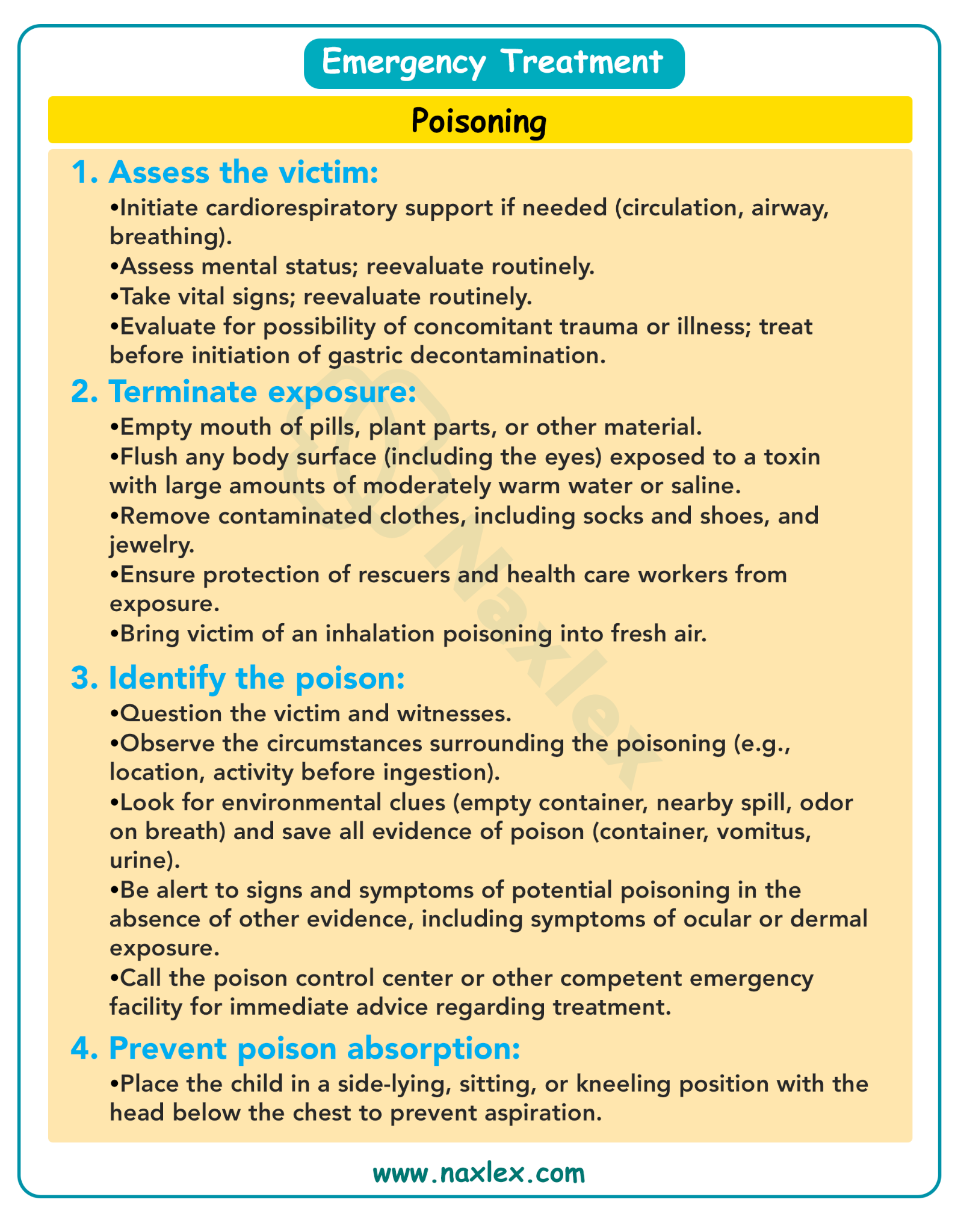
5.2.1. Principles of emergency treatment
- Assess and Stabilize: The first priority is to assess the child's airway, breathing, and circulation (the ABCs). Provide support as needed.
- Identify the Poison: If possible, determine what the child ingested, the amount, and when it happened. Call a poison control center immediately for expert guidance. Do not induce vomiting unless instructed to do so by a medical professional.
- Prevent Absorption: Depending on the substance, interventions like activated charcoal may be given to prevent the body from absorbing the poison.
- Elimination: Measures to enhance the elimination of the poison, such as forced diuresis or hemodialysis, may be necessary in severe cases.
5.2.2. Heavy metal poisoning
Heavy metal poisoning, particularly from lead, is a serious concern for young children due to their rapid development and tendency to put objects in their mouths.
Lead poisoning
Lead poisoning is a condition caused by the accumulation of lead in the body, which can be toxic.
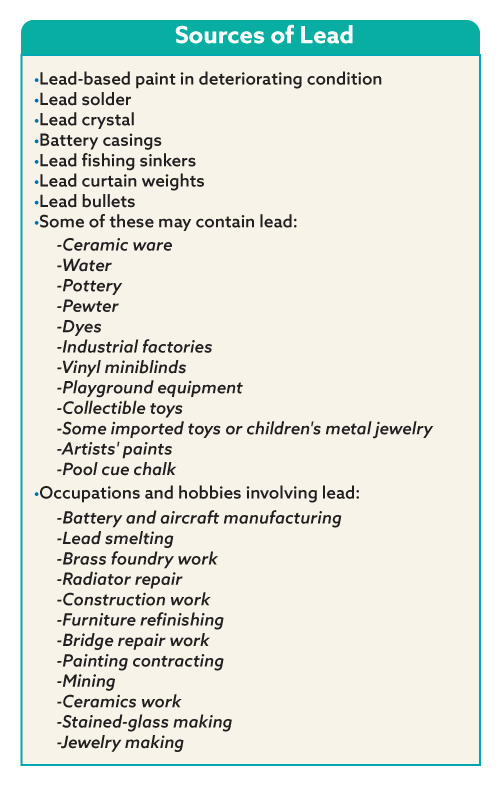
- Sources: The most common sources include lead-based paint in older homes, contaminated soil, certain toys, and some traditional remedies.
- Symptoms: High levels of lead can cause developmental delays, learning disabilities, seizures, coma, and even death. Low levels may cause subtle symptoms like irritability, abdominal pain, and fatigue.
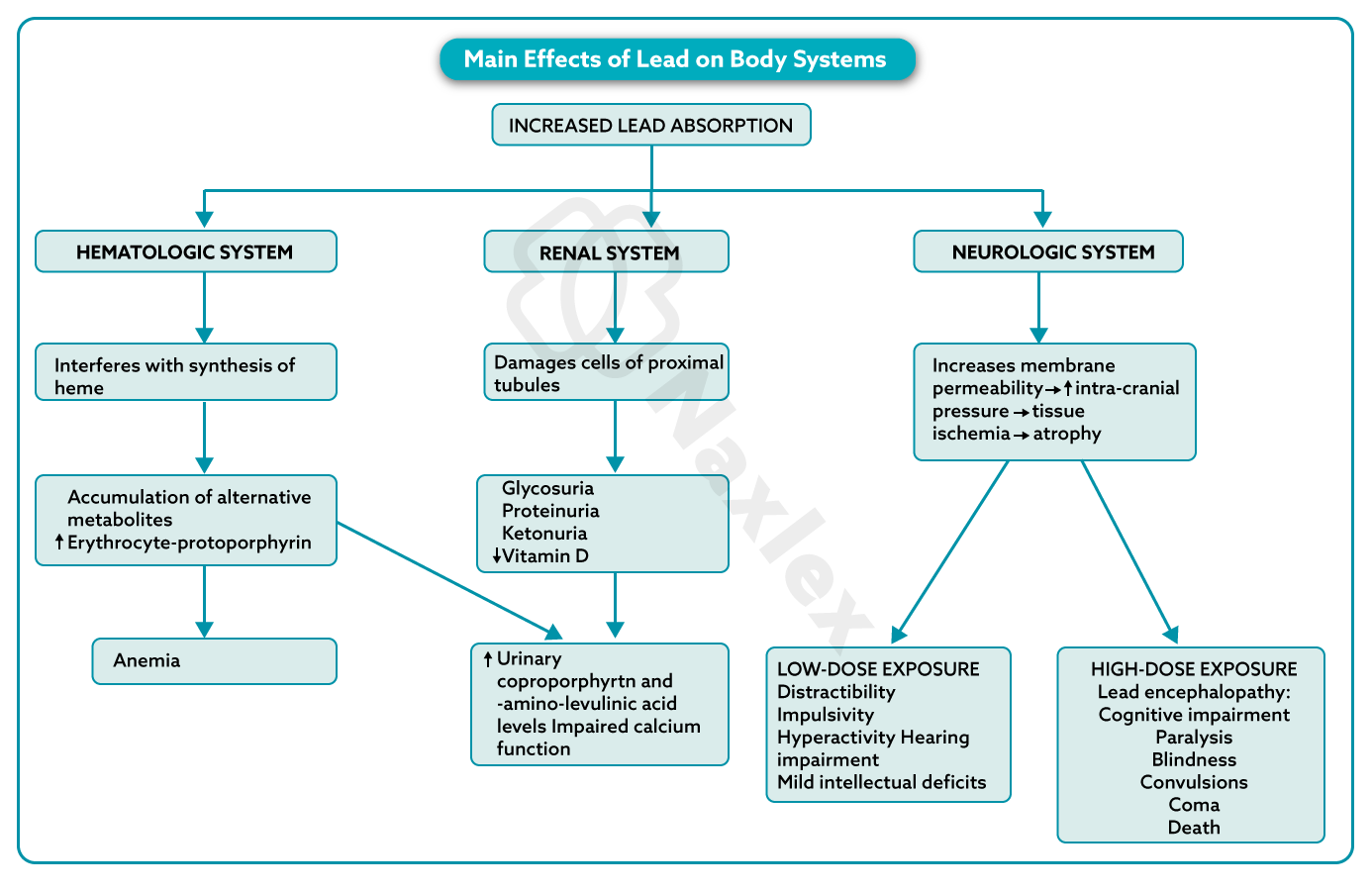
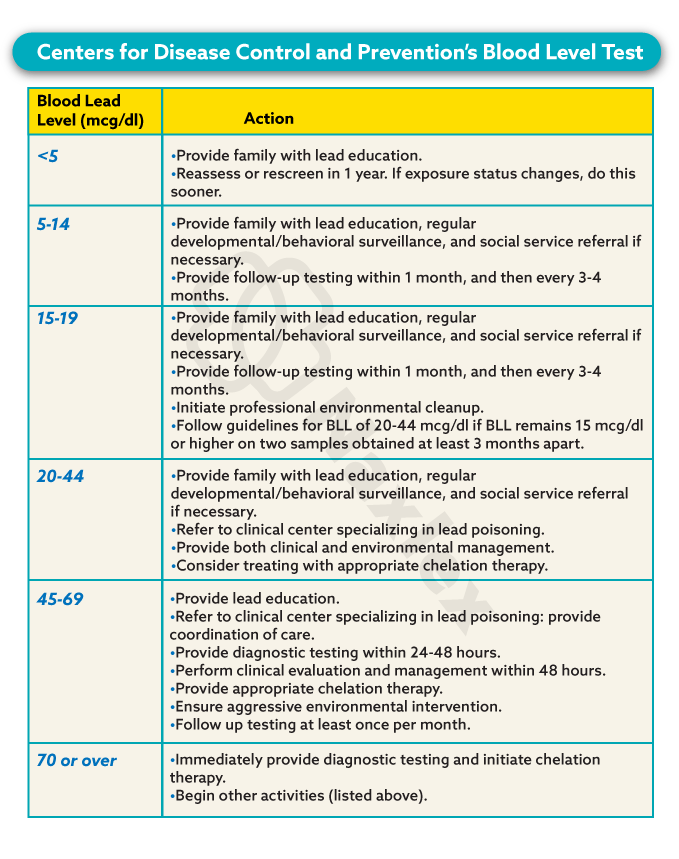
- Treatment: The primary goal is to remove the source of lead exposure. For high lead levels, chelation therapy is used. This involves administering a medication that binds to lead and helps the body excrete it.
Nursing Insight: Lead poisoning can mimic other common childhood illnesses. A comprehensive nursing assessment, including a detailed environmental history, is key to identifying children at risk. Always ask about the age of the home and any renovation activities.
5.3. Child Maltreatment
5.3.1. Child Neglect
Child neglect is the failure to provide for a child's basic needs. It is the most common form of child maltreatment.
- Types:
- Physical neglect: Failure to provide adequate food, clothing, shelter, or medical care.
- Emotional neglect: Inattention to a child's emotional needs, often leading to attachment issues and behavioral problems.
- Educational neglect: Failure to ensure a child receives an adequate education, such as chronic truancy.
5.3.2. Physical Abuse
- Physical Abuse: Non-accidental injury to a child. Suspicious injuries include multiple fractures in different stages of healing, bruises in patterns (e.g., belt marks), or burns with distinct shapes.
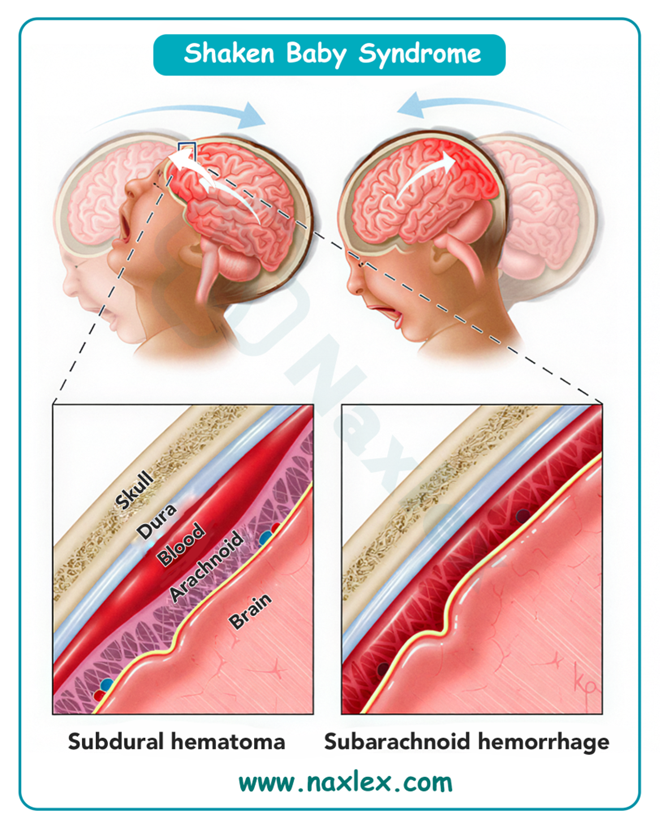
- Abusive Head Trauma (AHT): Also known as Shaken Baby Syndrome. Caused by violently shaking an infant, leading to brain hemorrhages, retinal hemorrhages, and often permanent brain damage, blindness, or death. Nurses should educate parents on coping with a crying baby.
- Munchausen Syndrome by Proxy (MSBP): A caregiver, usually the mother, fabricates or induces illness in a child. The nurse's role is to act as the child's advocate, identifying inconsistent signs and symptoms and reporting suspicions to child protective services.
5.3.3. Sexual Abuse
Sexual abuse is any sexual act or exploitation imposed on a child by an adult or an older child. It can be physical, emotional, or psychological. It's often difficult to identify because children may not disclose the abuse, and physical signs aren't always present.
5.3.4. Nursing Care of the Maltreated Child
- Recognize and Report: Nurses are mandatory reporters and must be able to recognize the signs and symptoms of abuse and neglect. These can include unexplained injuries, a delay in seeking medical care, or a child's fear of a caregiver.
- Create a Safe Environment: Provide a safe, non-judgmental space for the child to be examined and interviewed.
- Document: Document all injuries, observations, and conversations with the child and family in a detailed, objective manner.
- Support the Child: Provide comfort and emotional support to the child.
- Collaborate: Work with a multidisciplinary team, including social workers, child protective services, and law enforcement, to ensure the child's safety and well-being.
Nursing Insight: When documenting injuries, use objective, non-judgmental language. Instead of writing "The father's story doesn't make sense," document the specific details of the father's explanation and the discrepancy with the physical findings. For example, "Father states the child fell from a chair, but the child has a spiral fracture of the femur."
Health problems of the school-aged child
7.1. Obesity
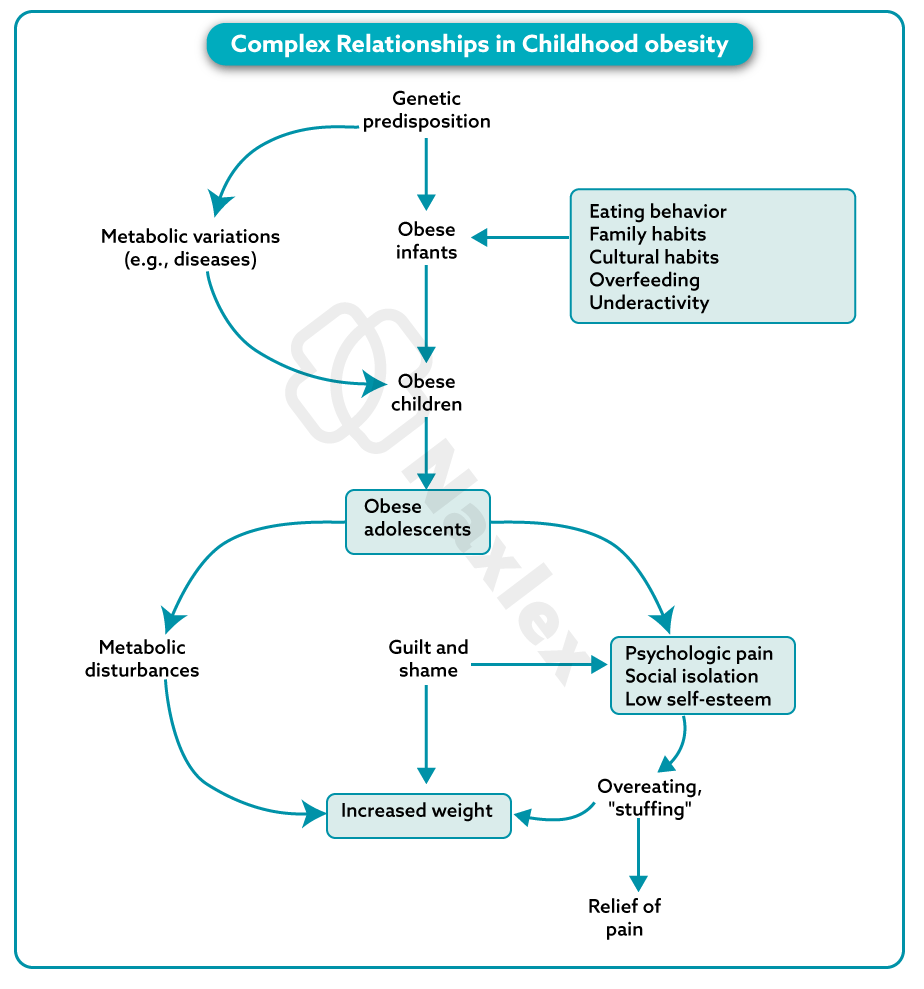
Obesity is a serious health problem characterized by an excessive accumulation of body fat. In school-age children, it's typically defined as having a Body Mass Index (BMI) at or above the 95th percentile for their age and sex. Childhood obesity is a significant predictor of adult obesity and is linked to numerous health complications.
Complications
Obesity in childhood can lead to a wide range of short-term and long-term health problems affecting nearly every body system. These include:
- Cardiovascular: High blood pressure (hypertension), high cholesterol, and early development of atherosclerosis.
- Metabolic: Type 2 diabetes, insulin resistance, and non-alcoholic fatty liver disease (NAFLD).
- Musculoskeletal: Increased risk of fractures, flat feet, and joint pain, particularly in the hips and knees (e.g., slipped capital femoral epiphysis).
- Respiratory: Sleep apnea and asthma.
- Psychosocial: Low self-esteem, depression, anxiety, social isolation, and bullying.
Treatment
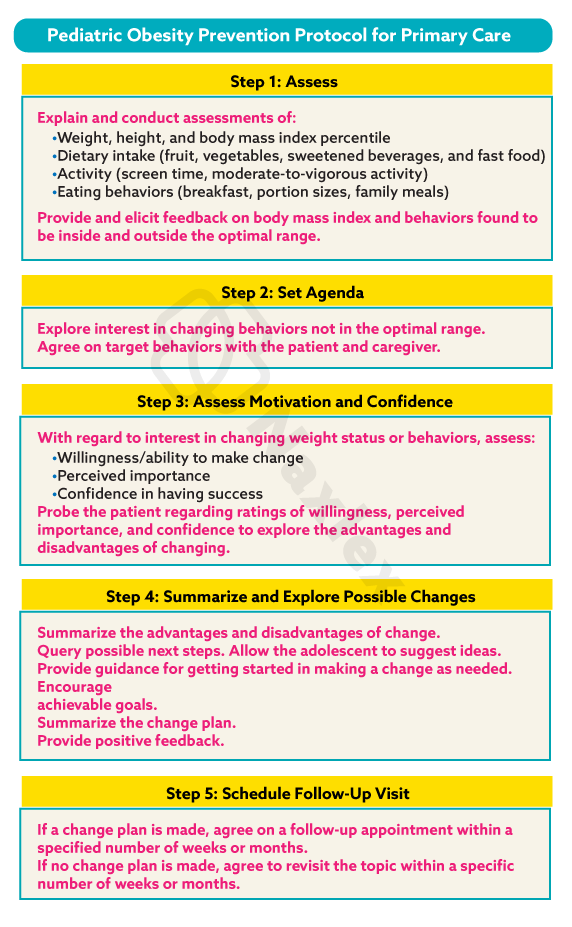
Treatment for childhood obesity is a multifaceted approach that involves the child, family, and healthcare providers. It focuses on lifestyle changes rather than rapid weight loss.
- Dietary Changes: Emphasize a balanced diet rich in fruits, vegetables, and whole grains while limiting sugary drinks, processed foods, and high-fat snacks. A registered dietitian can provide personalized guidance.
- Physical Activity: Encourage at least 60 minutes of moderate-to-vigorous physical activity daily. This can include sports, active play, or family activities. Screen time should be limited to less than two hours per day.
- Behavioral Therapy: Cognitive-behavioral therapy (CBT) can help children and families address emotional eating, build problem-solving skills, and develop a positive body image. Family involvement is crucial for long-term success.
Prevention
Preventing childhood obesity starts early and is a community-wide effort.
- Healthy Habits: Promote healthy eating and regular physical activity from a young age.
- Parental Modeling: Parents and caregivers should model healthy behaviors, such as eating nutritious meals and being physically active.
- Community Support: Schools, community centers, and healthcare providers should offer resources and programs that support healthy lifestyles.
- Policy: Policies that promote healthy food choices and safe places to play are essential for creating a supportive environment.
Nursing Insight: When discussing weight with a child and their family, use a positive, non-judgmental approach. Focus on "healthy choices" and "being strong and active" rather than "losing weight." This helps prevent the development of body image issues.
7.2. Dental Disorders
Dental health is a key component of a child's overall well-being. Poor oral hygiene and diet can lead to several common dental disorders.
Dental Caries (Cavities)
Dental caries is the irreversible breakdown of tooth enamel due to acid-producing bacteria in plaque. These bacteria metabolize sugars from food, creating acids that demineralize the tooth surface.
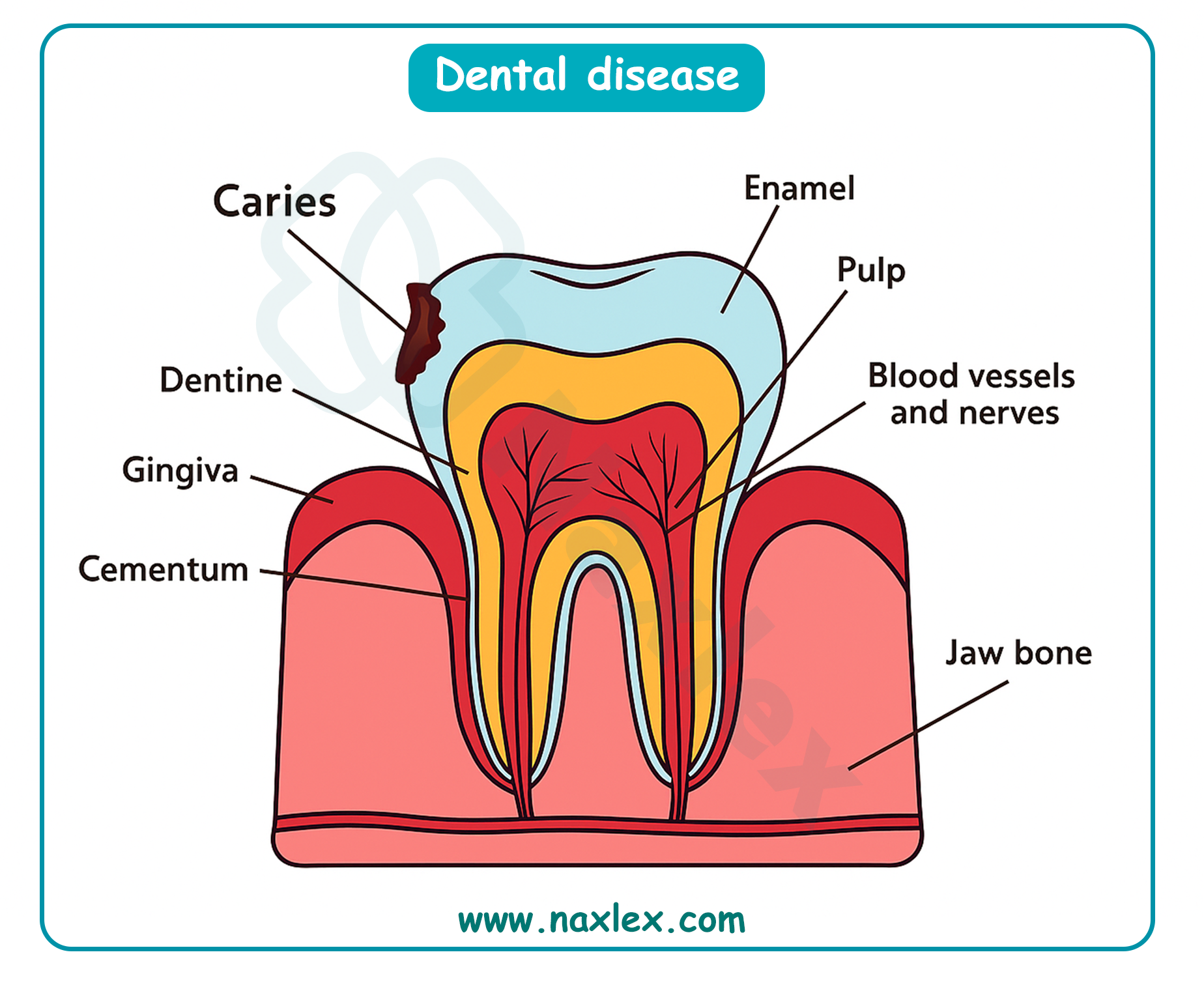
- Causes: Poor oral hygiene, a diet high in sugar and carbohydrates, and inadequate fluoride exposure.
- Symptoms: White spots on the teeth (early sign), brown or black spots, tooth sensitivity, and pain.
- Prevention: Brushing with a fluoride toothpaste twice daily, flossing, limiting sugary foods and drinks, regular dental check-ups, and dental appointments.
Periodontal Disease (Gum Disease)
Periodontal disease is an inflammation of the gums and supporting structures of the teeth. It's rare in its severe form in children but gingivitis (mild gum inflammation) is very common.
- Causes: Plaque buildup, poor oral hygiene, and genetic factors.
- Symptoms: Red, swollen, and bleeding gums.
- Prevention: Proper brushing and flossing to remove plaque and regular dental cleanings.
Malocclusion
Malocclusion refers to an improper alignment of the teeth and jaws. This can be hereditary or caused by habits like thumb-sucking or prolonged pacifier use.
- Types:
- Class I: The bite is normal, but teeth are crowded, spaced, or rotated.
- Class II (Overbite): The upper jaw and teeth protrude over the lower jaw.
- Class III (Underbite): The lower jaw and teeth protrude past the upper jaw.
- Treatment: Orthodontic treatment, such as braces or retainers.
Dental Trauma
Dental trauma is an injury to the teeth, gums, or supporting structures. It's common in school-age children due to falls, sports injuries, or accidents.
- Common Injuries: Fractured teeth, luxated (displaced) teeth, or avulsed (knocked-out) teeth.
- Action: Immediate dental care is essential. For a knocked-out permanent tooth, it's crucial to find the tooth, rinse it gently with milk or saline, and attempt to re-implant it or transport it to the dentist in a container of milk.
7.3. Disorders of Continence
These disorders involve the involuntary loss of urine or feces and can be a source of significant distress for children and their families.
Enuresis (Bedwetting)
Enuresis is the involuntary urination by a child who is past the age of toilet training. It's classified as primary (the child has never been consistently dry) or secondary (the child has a period of dryness lasting at least six months before the onset of enuresis).
- Causes: A combination of factors, including a small bladder capacity, a delay in the maturation of the nervous system, a family history of enuresis, and deep sleep patterns. Psychological factors can also play a role, especially in secondary enuresis.
- Treatment:
- Behavioral: Motivational therapy (e.g., star charts), fluid restriction before bedtime, and bladder training.
- Enuresis Alarms: These devices are highly effective and wake the child at the first sign of wetness, helping to condition them to wake up and use the toilet.
- Medication: Desmopressin, which reduces urine production at night, may be used for short-term management.
Encopresis (Fecal Incontinence)
Encopresis is the voluntary or involuntary passage of feces into inappropriate places by a child older than four years. It's often associated with chronic constipation.
- Causes: Chronic constipation leads to a buildup of hard stool in the rectum (impaction). This stretches the rectum, causing a loss of sensation. Liquid stool from higher up in the colon leaks around the impacted stool, resulting in soiling.
- Treatment:
- Stool Removal: The first step is to clear the impacted stool using laxatives or enemas.
- Maintenance: A long-term regimen of high-fiber diet, increased fluids, and laxatives is needed to prevent re-impaction.
- Behavioral: Positive reinforcement and a regular toileting schedule are important.
7.4. Disorders With Behavioral Components
7.4.1. Attention-Deficit/Hyperactivity Disorder (ADHD)
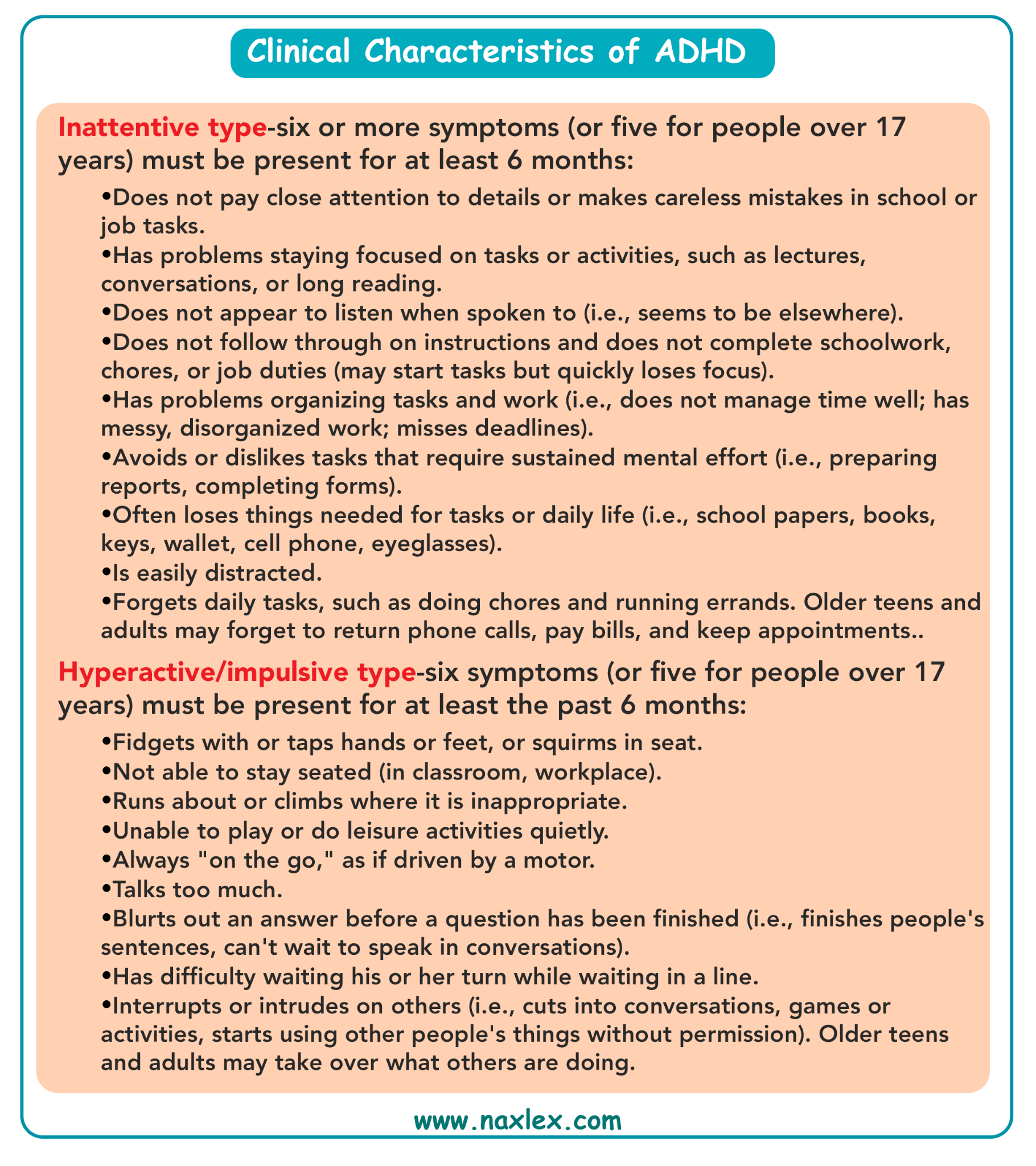
Description: A neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with functioning or development.
- Symptoms:
- Inattention: Difficulty sustaining attention, is easily distracted, seems not to listen, and struggles with organization.
- Hyperactivity: Fidgets, talks excessively, can't sit still, and has trouble engaging in quiet activities.
- Impulsivity: Acts without thinking, interrupts others, and has difficulty waiting their turn.
- Management:
- Medication: CNS stimulants (e.g., methylphenidate, amphetamine) are often used to improve focus and reduce hyperactivity.
- Behavioral Therapy: Strategies include creating a structured environment, using clear and consistent rules, providing positive reinforcement, and teaching social skills.
- Nursing Care: Educate parents and teachers on the disorder, administer medications, and monitor for side effects. Advocate for school accommodations (e.g., extended time on tests).
7.4.2 Learning Disability
A Learning Disability is a neurological disorder that affects a person's ability to receive, process, analyze, or store information. It's not a sign of low intelligence.
- Types:
- Dyslexia: Difficulty with reading, including decoding words, reading fluency, and comprehension.
- Dysgraphia: Difficulty with writing, including handwriting, spelling, and organizing thoughts on paper.
- Dyscalculia: Difficulty with math, including understanding number concepts and performing calculations.
- Intervention: Specialized educational programs, accommodations in the classroom (e.g., extra time on tests), and one-on-one tutoring.
7.4.3. Tic Disorders
Tics are sudden, rapid, recurrent, non-rhythmic movements or vocalizations. They can be simple (e.g., eye blinking, throat clearing) or complex (e.g., jumping, repeating phrases).
- Treatment: In most cases, tics are mild and don't require treatment. However, when tics are disruptive, behavioral therapies (e.g., habit reversal training) and sometimes medication may be used.
7.4.4 Gilles De La Tourette Syndrome
Tourette's Syndrome is a complex tic disorder characterized by the presence of both multiple motor tics and at least one vocal tic for more than one year.
- Associated Conditions: Tourette's is often associated with other conditions, including ADHD, Obsessive-Compulsive Disorder (OCD), and anxiety.
- Treatment: Primarily symptomatic. Behavioral therapies like Habit Reversal Training (HRT) and Comprehensive Behavioral Intervention for Tics (CBIT) are the first-line treatment. Medications are used when tics are severe and interfere with daily functioning.
7.4.5 Post-Traumatic Stress Disorder (PTSD)
PTSD is a disorder that develops in some people who have experienced a shocking, scary, or dangerous event. In children, it may present differently than in adults.
- Symptoms:
- Re-experiencing: Flashbacks, nightmares, and intrusive thoughts about the event.
- Avoidance: Avoiding places, people, or activities that remind them of the trauma.
- Negative Changes in Mood/Thinking: Negative beliefs about themselves, difficulty with positive emotions, and memory problems.
- Increased Arousal: Irritability, difficulty sleeping, and being easily startled.
- Treatment: Trauma-focused cognitive-behavioral therapy (TF-CBT) is a highly effective treatment for children with PTSD. Family therapy and play therapy are also used.
7.4.6 School Phobia
School phobia, or school refusal, is an extreme, irrational fear of attending school. It's often a symptom of an underlying anxiety disorder, such as separation anxiety or social anxiety.
- Symptoms: Physical complaints (stomachaches, headaches) that disappear on weekends or school breaks, panic attacks, and crying spells before school.
- Treatment: The goal is a gradual return to school. Treatment involves a multi-pronged approach with the child, family, and school. Cognitive-behavioral therapy (CBT) helps the child understand and manage their anxiety.
7.4.7 Functional Abdominal Pain (FAP)
FAP is a chronic or recurrent abdominal pain that has no identifiable organic cause. It's often linked to psychological stress or anxiety.
- Symptoms: Diffuse, crampy pain around the belly button, with no other signs of illness. It doesn't typically wake the child at night.
- Treatment: Reassurance and education are key. Treatment focuses on managing the pain and coping with the symptoms, often using CBT, relaxation techniques, and sometimes dietary changes.
7.4.8 Childhood Depression
Childhood depression is a serious mood disorder that can affect how a child feels, thinks, and behaves. It's more than just a passing sadness.
- Symptoms: Persistent sadness or irritability, loss of interest in activities they once enjoyed, changes in appetite or sleep, fatigue, feelings of worthlessness or guilt, and thoughts of self-harm or suicide.
- Treatment: Cognitive-behavioral therapy (CBT) and Interpersonal Therapy (IPT) are effective. In moderate-to-severe cases, medication (antidepressants) may be used in combination with therapy, with careful monitoring.
7.4.9 Childhood Schizophrenia
Childhood schizophrenia is a rare but severe psychiatric disorder characterized by psychosis, including hallucinations and delusions. Its onset is typically later in adolescence, but in rare cases, it can begin in childhood.
- Symptoms: Hallucinations (e.g., hearing voices), delusions (false beliefs), disorganized thinking, and social withdrawal.
- Treatment: A combination of antipsychotic medication, psychotherapy (individual and family), and social skills training. Early intervention is crucial for a better prognosis.
7.4.10. Anxiety Disorders
Anxiety disorders are the most common mental health problems in children. They are characterized by excessive fear, worry, and avoidance behaviors.
- Types:
- Separation Anxiety: Excessive worry about being away from home or attachment figures.
- Generalized Anxiety Disorder (GAD): Persistent and excessive worry about multiple things (e.g., school performance, future events).
- Social Anxiety Disorder: Intense fear of social situations and being judged by others.
- Specific Phobias: Irrational fear of a specific object or situation (e.g., dogs, needles, heights).
- Treatment: Cognitive-behavioral therapy (CBT) is the gold standard for treating anxiety disorders in children. It helps them identify and challenge anxious thoughts and gradually face their fears.
7.4.11 Conduct Disorders
Conduct Disorder is a behavioral disorder characterized by a persistent pattern of violating the rights of others or major age-appropriate societal norms or rules.
- Symptoms: Aggression toward people and animals, destruction of property, deceitfulness or theft, and serious violations of rules.
- Treatment: Parent Management Training (PMT), in which parents learn techniques to manage their child's behavior, and Multisystemic Therapy (MST), which addresses the child's entire social environment (family, school, community).
Nursing Insight: When a child presents with somatic symptoms like stomachaches or headaches with no organic cause, always consider psychosocial stressors like school phobia, anxiety, or bullying. A thorough psychosocial assessment is as important as a physical one.
Health problems of the adolescent
9.1. Health Conditions of the Male Reproductive System
9.1.1. Penile Conditions
Adolescent males may experience various penile conditions. Phimosis is a condition where the foreskin can't be retracted, while paraphimosis is a medical emergency where the retracted foreskin is trapped behind the glans, causing swelling. Balanitis is an inflammation of the head of the penis, often caused by poor hygiene.
9.1.2. Varicocele
A varicocele is an enlargement of the veins within the scrotum, similar to a varicose vein in the leg.
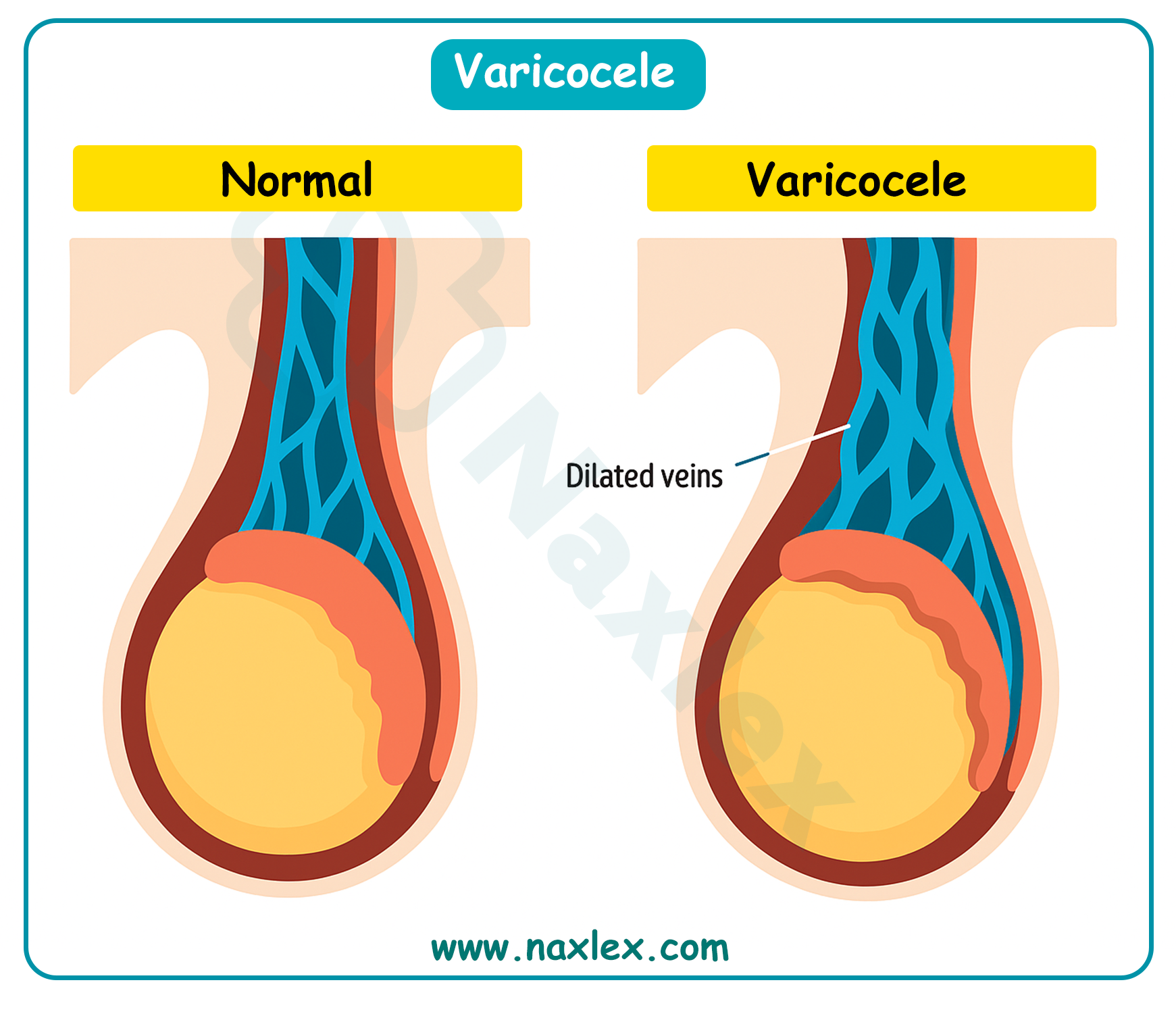
It's a common cause of low sperm production and decreased sperm quality, which can lead to infertility. It often feels like a "bag of worms." Treatment is usually only necessary if the varicocele causes pain, testicular atrophy, or infertility.
9.1.3. Epididymitis
- Epididymitis is an inflammation of the epididymis, the coiled tube at the back of the testicle that stores and carries sperm.
- It's often caused by a bacterial infection, including sexually transmitted infections (STIs) like chlamydia or gonorrhea.
- Symptoms include testicular pain, redness, and swelling, often accompanied by fever. Treatment involves antibiotics and supportive care.
9.1.4. Testicular Torsion
- Testicular torsion is a medical emergency where the spermatic cord, which provides blood to the testicle, twists. This cuts off blood supply and can lead to the death of the testicle.
- Symptoms include a sudden onset of severe testicular pain, swelling, and redness. It requires immediate surgical intervention to save the testicle.
9.1.5. Gynecomastia
Gynecomastia is the benign enlargement of male breast tissue. It's common during puberty due to hormonal imbalances. It usually resolves on its own, but in some cases, it can persist and cause psychological distress. In such cases, surgical removal of the excess tissue may be considered.
9.2. Health Conditions of the Female Reproductive System
9.2.1. Gynecologic Examination
- The first gynecologic exam for an adolescent is typically recommended between ages 13 and 15, unless there's a specific health concern. The first exam usually doesn't include a Pap test unless the adolescent is sexually active. The exam focuses on providing education about reproductive health, menstrual cycles, and contraception.
Nursing Insight: To make the gynecologic exam less intimidating for an adolescent, a nurse should explain each step of the process clearly and respectfully. Offering the option of a chaperone and ensuring privacy are also vital.
9.2.2. Menstrual Disorders
- Amenorrhea: The absence of menstruation. Primary amenorrhea is when menstruation hasn't started by age 16. Secondary amenorrhea is the cessation of menstruation for more than three to six months in someone who has previously had periods. Causes can include hormonal imbalances, excessive exercise, or eating disorders.
- Dysmenorrhea: Painful menstruation. Primary dysmenorrhea is common and caused by prostaglandins, which cause uterine contractions. It's treated with NSAIDs. Secondary dysmenorrhea is caused by an underlying medical condition, such as endometriosis or fibroids.
9.2.3. Endometriosis
Endometriosis is a condition in which tissue similar to the lining of the uterus grows outside the uterus. This can cause severe pelvic pain, especially during menstruation, and may lead to infertility. Diagnosis often involves a laparoscopy.
9.2.4. Premenstrual Syndrome (PMS)
PMS is a group of physical and emotional symptoms that occur in the one to two weeks before menstruation. Symptoms can include bloating, breast tenderness, mood swings, and irritability. Lifestyle changes, such as diet and exercise, can help manage symptoms.
9.2.5. Abnormal Uterine Bleeding
This refers to any deviation from a normal menstrual cycle, including bleeding between periods, a very heavy flow, or an unusually long period. It can be caused by hormonal imbalances, uterine fibroids, or infections.
9.2.6. Vaginal Infections
- Bacterial Vaginosis (BV): An imbalance of bacteria in the vagina, characterized by a thin, gray discharge with a "fishy" odor. It's treated with antibiotics.
- Candidiasis (Yeast Infection): An overgrowth of the Candida fungus, causing itching, burning, and a thick, white discharge. It's treated with antifungal medications.
9.2.7. Sexually Transmitted Infections (STIs)
Adolescents are a high-risk group for STIs.
- HIV: A virus that attacks the immune system.
- Trichomoniasis: A parasitic infection causing a foul-smelling, greenish-yellow discharge.
- Chlamydia and Gonorrhea: Both are bacterial infections that often have no symptoms, making them easy to spread. They can lead to pelvic inflammatory disease (PID).
- Syphilis: A bacterial infection that progresses through stages and can cause serious long-term complications if left untreated.
- Pelvic Inflammatory Disease (PID): An infection of the female reproductive organs, often a complication of untreated chlamydia or gonorrhea.
- HPV (Human Papillomavirus): The most common STI. Some strains cause genital warts, while others can lead to cervical cancer. A vaccine is available for prevention.
- Herpes Simplex Virus (HSV): Causes painful blisters on the genitals, mouth, or surrounding areas. It's a lifelong infection.
- Hepatitis: A viral infection of the liver, with types B and C being transmitted sexually.
Nursing Insight: When discussing sexual health with adolescents, use a non-judgmental, confidential, and straightforward approach. Use the "5 P's" as a framework for your assessment: Partners, Practices, Protection from STIs, Past history of STIs, and Pregnancy plans.
9.3. Health Conditions Related to Reproduction
9.3.1. Adolescent Pregnancy
Teen pregnancy is associated with higher risks for both the mother and the infant, including pre-term birth, low birth weight, and higher infant mortality rates. Social and economic consequences for the mother are also significant.
9.3.2. Adolescent Abortion
Adolescents may seek abortion due to lack of support, financial instability, or wanting to continue their education. They require compassionate, non-judgmental care and counseling.
9.3.3. Contraception
Adolescents need access to comprehensive education about contraception, including methods like condoms, birth control pills, and long-acting reversible contraception (LARC) such as IUDs and implants. Condoms are the only method that also protects against STIs.
9.3.4. Sexual Assault
Sexual assault is a serious crime and a devastating experience for an adolescent. Nurses must provide sensitive, trauma-informed care. This includes providing a safe space, physical assessment, and collection of forensic evidence, as well as offering emotional support and resources for counseling.
9.4. Health Conditions with a Behavioral Component
9.4.1. Anorexia Nervosa and Bulimia Nervosa
Description: Eating disorders characterized by a distorted body image.
- Anorexia Nervosa: Involves a refusal to maintain a healthy body weight, an intense fear of gaining weight, and a distorted perception of body shape.
- Bulimia Nervosa: Involves cycles of binge eating followed by compensatory behaviors like self-induced vomiting, excessive exercise, or laxative abuse.
- Management: Requires a multidisciplinary team approach including medical stabilization, nutritional counseling, and psychotherapy.
9.4.2. Substance Abuse
Substance abuse is the harmful use of psychoactive substances. Adolescents may be particularly vulnerable due to peer pressure and a developing brain.
- Tobacco: Nicotine is highly addictive. Vaping and e-cigarettes are also a major concern.
- Alcohol: Can impair judgment and lead to risky behaviors, as well as long-term health problems.
- Cocaine: A powerful stimulant that can be highly addictive.
- Narcotics: Opioids like heroin and prescription painkillers are highly addictive and carry a high risk of overdose.
- CNS Depressants: Drugs like benzodiazepines that slow brain activity.
- CNS Stimulants: Drugs like amphetamines that speed up brain activity.
- Mind-altering drugs: Hallucinogens like LSD and PCP.
9.4.3. Self-Harm
Description: A coping mechanism for intense emotional pain, not necessarily a suicide attempt. It includes cutting, burning, or scratching oneself.
- Management: Nurses must assess for suicidal ideation and provide a safe environment. Teaching alternative coping strategies and referring the adolescent to a mental health professional is crucial.
9.4.4. Suicide
Description: Suicide is a leading cause of death in adolescents.
- Risk factors: Depression, substance abuse, previous suicide attempts, and a family history of suicide.
- Management:
- Nursing Insight: If an adolescent discloses thoughts of self-harm or suicide, the nurse's priority is to assess the immediate risk. Ask direct questions like, "Are you thinking about hurting yourself?" and "Do you have a plan?" If a plan exists, the adolescent is at high risk and should not be left alone. Initiate a safety contract and contact the appropriate mental health services.
Summary
- The management of health problems across the pediatric lifespan demands a transition from acute physical care to long-term behavioral advocacy.
- In infancy and early childhood, nursing interventions are heavily weighted toward prevention and emergency stabilization.
- Whether managing a "Brief Resolved Unexplained Event" (formerly ALTE) or treating a child who has ingested a caustic substance, the nurse must act with speed and precision. A deep understanding of lead poisoning protocols and the principles of emergency toxicology is essential for protecting the developing nervous system of the young child.
- As children reach school age, the nursing focus expands to include behavioral health and disorders of functional maturity.
- Conditions like ADHD and Tourette Syndrome require the nurse to coordinate care between the home, school, and clinical setting.
- Behavioral components also manifest physically through disorders of continence (enuresis/encopresis) and functional abdominal pain, often linked to school phobia or anxiety.
- Nurses must be adept at using screening tools for childhood depression and schizophrenia, ensuring that mental health is prioritized alongside physical growth.
- In the adolescent population, the nurse navigates the sensitive domains of reproductive and behavioral health.
- Acute conditions like testicular torsion represent surgical emergencies that require rapid identification to save the organ. Conversely, managing menstrual disorders, STIs, or adolescent pregnancy requires a high degree of empathy and confidentiality.
- The summary of adolescent care is often dominated by behavioral crises such as anorexia nervosa, bulimia, substance abuse, and the tragic rise in self-harm and suicide.
- By integrating physical assessments with robust psychosocial screening, nurses can identify the warning signs of these life-threatening conditions early, providing the necessary intervention to guide the patient toward a healthy adulthood.
