
Please set your exam date
Growth And Development In Preschoolers
Study Questions
Practice Exercise 1
The nurse is caring for a hospitalized 4-year-old who insists on having the nurse perform every assessment and intervention on her imaginary friend first. She then agrees to have the assessment or intervention done to herself. The nurse identifies this preschooler’s behavior as
Explanation
Preschoolers (ages 3–5) are in Piaget’s preoperational stage of cognitive development, characterized by egocentric thinking, fantasy play, and magical thinking. Imaginary friends are common and developmentally appropriate, often helping children express emotions, cope with new experiences, or gain a sense of control, especially in unfamiliar or stressful environments like hospitals.
Rationale for correct answer:
3. Pretend play and imaginary companions are a normal and healthy part of preschool development. These behaviors are a reflection of the child’s imagination and help them understand the world around them. In stressful settings such as hospitalization, imaginary friends can offer comfort and security.
Rationale for incorrect answers:
1. Preschoolers are still developing their sense of reality. Expecting them to fully distinguish between reality and fantasy is unrealistic at this age. The behavior is not problematic, but expected.
2. While hospitalization can increase stress and lead to regressive behaviors, this type of fantasy play is not abnormal only because the child is out of routine, it’s developmentally typical regardless of setting.
4. This behavior does not interfere with care, in fact, it can facilitate cooperation if the nurse respects the child’s developmental needs and plays along with the imaginary friend briefly to gain trust and reduce anxiety.
Take home points:
- Imaginary friends are normal for preschool-aged children and aid in emotional expression and coping.
- Nurses should respect and incorporate fantasy play into care when possible to reduce anxiety and foster trust.
- Avoid labeling fantasy behaviors as problematic unless they interfere significantly with functioning or persist beyond the expected developmental window.
- Supportive, playful interaction can enhance cooperation and comfort in pediatric care settings.
A nurse is preparing a 4-year-old boy for surgery. Which nursing action is appropriate for preoperative teaching based on Erikson’s developmental stages?
Explanation
A 4-year-old is in Erikson’s stage of Initiative vs. Guilt and Piaget’s preoperational stage. At this developmental stage, children learn through play, imitation, and visual demonstration. They have active imaginations and limited ability to understand abstract explanations, but they respond well to hands-on, concrete teaching methods that reduce fear and promote a sense of control.
Rationale for correct answer:
2. Using a doll to demonstrate surgical equipment allows the child to learn through play and familiar actions. This approach respects the child’s developmental level, supports understanding, and helps reduce anxiety by making unfamiliar concepts more concrete and less threatening.
Rationale for Incorrect Answers:
1. Making a project may be appropriate for older school-age children, but a 4-year-old may lack the attention span or fine motor skills for a meaningful project tied to surgery. It’s also too abstract for effective preparation.
3. Asking about feelings is developmentally too advanced for a 4-year-old. While it’s important to be emotionally supportive, preschoolers may not be able to articulate their feelings clearly or respond meaningfully to open-ended emotional questions.
4. Listening to music without further instructions does not engage the child in a developmentally appropriate way for preoperative preparation. While music can calm anxiety, it does not address the child’s need for active, visual, and play-based learning.
Take home points
- Preschoolers learn best through hands-on, play-based activities that involve modeling and imitation.
- Preparing children for procedures should include demonstration on dolls or use of familiar objects to reduce anxiety.
- Avoid abstract explanations or expecting preschoolers to verbalize complex emotions.
- Nurses should use developmentally appropriate strategies based on Erikson and Piaget’s stages to reduce fear and promote cooperation.
A parent asks the nurse the following question: “My son plays with his penis all the time. What should I do?” Which of the following responses is appropriate for the nurse to give the parent? “Advise your child that:
Explanation
Preschool children often engage in genital exploration as a normal part of their development. It is typically motivated by curiosity and not sexual in nature. The goal is to teach appropriate boundaries, not to shame the behavior.
Rationale for correct answer:
2. Telling the child to only touch his genitals in a private place acknowledges that the behavior is developmentally normal while also teaching the child about social norms and privacy. It helps the child understand where and when such behavior is acceptable, promoting healthy body awareness without instilling shame or fear.
Rationale for Incorrect Answers:
1. Limiting genital touching only to urination may imply that natural curiosity is wrong, leading to confusion or shame. This does not help the child learn about privacy or autonomy.
3. Telling the child that only boys "old enough to have sex" can touch themselves is developmentally inappropriate, confusing, and introduces adult concepts prematurely.
4. Warning the child that “bad men” may try to hurt him for touching his penis is frightening, misleading, and potentially traumatizing. It uses fear rather than education and does not teach healthy or appropriate boundaries.
Take home points
- Genital exploration is normal in preschoolers and is not typically a cause for concern.
- Parents should set calm, age-appropriate boundaries by teaching children that some behaviors are private.
- Avoid shaming, scolding, or using fear-based messages, which can lead to guilt, confusion, or anxiety about the body.
- Encourage open, honest communication about bodies, privacy, and safety in a developmentally appropriate manner.
When a preschooler believes that their stuffed animal is "sad" because it fell off the bed, this is an example of which cognitive characteristic according to Piaget?
Explanation
Preschoolers (ages 3–6) are in Piaget’s preoperational stage of cognitive development. This stage is marked by symbolic thinking, limited logic, and the tendency to assign human qualities to inanimate objects, a characteristic known as animism.
Rationale for correct answer:
3. Animism is the belief that non-living objects have feelings, thoughts, or intentions, just like people. When a preschooler says their stuffed animal is "sad" after falling, they are projecting emotions onto an inanimate object, which is a classic sign of animism in Piaget’s theory.
Rationale for incorrect answers:
1. Egocentrism refers to a child's inability to see things from another person’s perspective. While also common in the preoperational stage, it does not explain assigning emotions to objects.
2. Centration is when a child focuses on one aspect of a situation and ignores others such as focusing only on the height of liquid in a glass, not the width. It doesn’t relate to attributing feelings to objects.
4. Irreversibility is the child’s difficulty in understanding that actions can be reversed such as not realizing that if you pour the water back into the original cup, it’s the same amount. It’s unrelated to believing an object has feelings.
Take home points
- Animism is a normal part of preschool cognitive development in Piaget’s preoperational stage.
- Children may attribute life-like qualities (e.g., feelings, intentions) to toys or objects as a way of understanding the world.
- Nurses and caregivers should recognize this as age-appropriate imagination, not a sign of confusion or concern.
- Supportive, imaginative play helps preschoolers process emotions and experiences safely.
Which of the following gross motor skills would a typical 3-year-old be expected to perform?
Explanation
A typical 3-year-old is in the early preschool stage of development. At this age, children are refining gross motor skills, gaining balance and coordination, and increasing independence in physical play.
Rationale for correct answer:
2. By age 3, most children have developed the leg strength, coordination, and balance to ride a tricycle. This is a well-established milestone for 3-year-olds and supports physical activity and exploration.
Rationale for incorrect answers:
1. Skipping with alternate feet typically emerges around age 5. It requires advanced coordination and rhythm beyond the motor abilities of a typical 3-year-old.
3. Jumping rope is a more advanced gross motor skill that involves timing, coordination, and strength, and is generally expected around age 5 to 6.
4. Tying shoelaces is a fine motor skill, not a gross motor one, and typically develops closer to age 5 to 6 due to the need for dexterity and sequencing.
Take home points
- Gross motor skills for 3-year-olds include running, climbing stairs with alternating feet, jumping in place, and riding a tricycle.
- Skipping, jumping rope, and tying shoelaces develop later in the preschool or early school-age years.
- Understanding motor milestones helps in assessing age-appropriate development and identifying any delays early.
Practice Exercise 2
A nurse is educating a group of parents regarding disciplinary actions that they can take if their preschool child disobeys. Which of the following recommendations should the nurse make?
Explanation
Preschool children (ages 3–5) are in Erikson’s stage of Initiative vs. Guilt and Piaget’s preoperational stage, where they are beginning to understand rules but still have limited logical thinking. Discipline at this age should aim to teach appropriate behavior, not shame or instill fear. Time-outs offer a brief, developmentally appropriate way to help children calm down and reflect, reinforcing boundaries without harsh consequences.
Rationale for correct answer:
1. Time-outs are effective for preschoolers when used appropriately, one minute per year of age is a commonly recommended guideline (e.g., 3 minutes for a 3-year-old). Time-outs help children regulate emotions and learn that certain behaviors have immediate but fair consequences. This method is nonviolent, structured, and reinforces boundaries in a developmentally appropriate way.
Rationale for incorrect answers:
2. Spanking, even if described as “light,” is not recommended by major health organizations such as the American Academy of Pediatrics due to its association with increased aggression, antisocial behavior, and mental health issues. It does not teach alternative positive behaviors.
3. Withholding meals as punishment is inappropriate and may harm the child's sense of security, emotional health, and nutrition. It also uses a basic need as a disciplinary tool, which is not recommended.
4. Taking away a favorite toy for days may be too abstract and delayed for preschoolers to connect the consequence with the behavior. Preschoolers require immediate and clear consequences to understand the relationship between action and outcome.
Take home points
- Preschoolers need clear boundaries and consistent consequences that are brief and immediate.
- Use time-outs as an immediate, short, and structured discipline technique for preschool-aged children.
- Avoid physical punishment and withholding basic needs, as these approaches are ineffective and potentially harmful.
The mother of a 3-year-old is concerned about her child’s speech. She describes her preschooler as hesitating at the beginning of sentences and repeating consonant sounds. What is the nurse’s best response?
Explanation
Preschoolers, especially between ages 3 to 5, often experience normal dysfluency or "developmental stuttering" as their language skills rapidly expand. During this stage, children are learning to coordinate thinking with speech, which can lead to temporary repetitions, pauses, and hesitations, especially when excited or trying to express complex ideas.
Rationale for correct answer:
1. Normal dysfluency is expected in early preschool years, often peaking around age 3. It typically resolves on its own without intervention. The nurse should reassure the parent that this is common and usually not a sign of a speech disorder unless it persists beyond age 5, worsens, or includes signs of struggle such as facial tension and frustration.
Rationale for incorrect answers:
2. Reading to the child is always encouraged and supports language development, but it is not the most direct or reassuring response to a concern about dysfluency. It may be offered as a supportive strategy, but not as the primary response.
3. Developmental evaluation is not warranted at this point unless there are other concerns such as regression, incomprehensible speech, and social withdrawal. Hesitation and repeated consonants alone are typical for this age.
3. A speech therapy referral would be premature. Most children outgrow normal dysfluency without intervention. Only if the dysfluency persists, worsens, or interferes with communication should a formal evaluation be recommended.
Take home points:
- Speech dysfluency is common and usually resolves naturally in preschool-aged children.
- Nurses should reassure and educate caregivers on normal language development patterns.
- Red flags include prolonged stuttering beyond age 5, frustration during speech, or loss of language skills, in which case, referral is appropriate.
- Encourage reading, modeling clear speech, and avoiding correction or pressure to speak perfectly.
The mother of a 4-year-old asks for advice on using time-out for discipline with her child. What advice should the nurse give the mother?
Explanation
Time-out is an effective, age-appropriate discipline technique for preschoolers when used consistently, calmly, and immediately after inappropriate behavior. The recommended duration is 1 minute per year of age, helping the child understand consequences without physical punishment. This aligns with the preschooler’s developmental stage of Initiative vs. Guilt stage in which they are learning boundaries and testing limits.
Rationale for correct answer:
2. A 4-year-old should have a 4-minute time-out. This short duration is developmentally appropriate, easy for the child to understand, and ensures the technique is effective without becoming punitive. Time-out gives the child space to calm down and reflect, reinforcing boundaries.
Rationale for incorrect answers:
1. Saying "if spanking is not working, time-out won’t help either" is incorrect and not evidence-based. Spanking is discouraged due to its association with increased aggression and negative outcomes, while time-out is endorsed by pediatric experts as a safe and effective behavioral tool.
3. Time-out should not be a last resort. It is often the first-line discipline strategy for preschoolers. Removing privileges can be helpful too, but time-out offers a clearer, immediate consequence that aligns with a young child’s developmental understanding.
4. Forcing a child to stay in time-out until crying stops is not appropriate. The goal of time-out is not emotional suppression but brief, structured removal from a situation. Some children may still be emotional when time-out ends, and that’s okay, as long as the time is consistent and calmly enforced.
Take home points
- Time-out should last 1 minute per year of age, applied immediately and consistently after misbehavior.
- It is a recommended, non-punitive discipline method that helps young children learn limits.
- Spanking and overly harsh methods are discouraged; emotional regulation is a developmental skill, not a discipline goal.
- Nurses should educate caregivers on the proper use of time-out, including remaining calm and avoiding prolonged punishment.
A 4-year-old child is hospitalized with a high fever. While the child is in bed, the child comforts himself by sucking the thumb. The mother of the child becomes concerned because her child has not sucked his thumb for 6 months. Which nursing response to the mother’s concerns is most appropriate?
Explanation
Developmental regression is a common and temporary behavioral response in young children when faced with stressful events, such as illness, hospitalization, or changes in routine. In preschoolers, behaviors like thumb-sucking, bed-wetting, or clinginess may reappear even after being previously outgrown. These actions serve as self-soothing mechanisms during times of anxiety or discomfort.
Rationale for correct answer:
2. This response is supportive, reassuring, and developmentally informed. It validates the mother’s concern while educating her that regressive behaviors during hospitalization are expected in preschoolers. Encouraging continued love and support helps the child feel secure, which can aid recovery and eventual return to age-appropriate behaviors.
Rationale for incorrect answers:
1. Saying “maybe your child just needs more attention” is dismissive and lacks developmental insight. It may also make the mother feel blamed or criticized.
3. While family stressors can contribute to regression, this question shifts focus away from the current illness and hospitalization, which are likely the immediate cause. It’s less appropriate than directly addressing the behavior in context.
4. Asking “Where is the father?” is speculative, assumes family structure plays a role without evidence, and does not address the mother’s concern directly or offer appropriate support.
Take home points
- Regression is a normal response to stress in preschool-aged children, especially during hospitalization.
- Nurses should provide reassurance and education to caregivers, helping them understand that such behaviors are temporary.
- Supportive caregiving including comfort, routine, and presence helps children return to normal developmental patterns.
- Avoid blaming or speculative responses; instead, respond with developmentally appropriate education and empathy.
When preparing a 4-year-old for their first day of kindergarten, which of the following nursing interventions would be most beneficial?
Explanation
Starting kindergarten is a major developmental milestone for a 4-year-old child. It often brings a mix of excitement and anxiety, both for the child and the caregivers. Nurses play an essential role in supporting families during this transition by providing guidance that fosters emotional readiness, reduces fear, and promotes a positive attitude toward school.
Rationale for correct answer:
3. Visiting the school allows the child to become familiar with the environment, and talking about what to expect helps them visualize the routine, increasing comfort and confidence. This aligns with Erikson’s stage of initiative vs. guilt, where children thrive when encouraged to explore new experiences in a supportive environment.
Rationale for incorrect answers:
1. While this may seem reassuring, it's inaccurate and dismissive. Kindergarten has more structure, academic expectations, and new routines compared to daycare, and oversimplifying it might cause confusion or distrust.
2. Telling the child that they must remain quiet creates unnecessary fear and places unrealistic expectations on a preschooler. It can discourage the child and promote anxiety about failing to meet strict standards.
4. Warning about potential difficulties focuses on possible challenges or problems which can overwhelm and frighten the child. At this age, it's more helpful to frame the transition as a positive adventure, not a source of stress.
Take home points
- Use positive, honest, and developmentally appropriate language when preparing a child for transitions.
- Familiarization visits, storybooks about school, and involving the child in school preparation (e.g., shopping for supplies) can boost confidence.
- Always validate feelings but provide reassurance and support, especially when entering a new environment.
Practice Exercise 3
A nurse is educating the parents of a 4½-year-old child regarding personal safety issues. Which of the following statements should the nurse include in the teaching? Select all that apply
The parents should:
Explanation
Child safety is the practice of protecting children from harm, injury, and dangerous situations, whether at home, in the community, online, or in healthcare settings. It’s a broad concept that spans physical, emotional, and developmental well-being.
Rationale for correct answers:
1. Choosing a safety word is a widely recommended personal safety strategy. It helps a child verify that a person is safe if sent by a parent. If the adult doesn’t know the word, the child should not go with them.
2. Teaching children to report unfamiliar adults offering treats is a core part of “stranger danger” education. Children must be empowered to recognize and avoid luring tactics.
5. Educating the child about 911 is essential. Children should know how and when to call, and be able to provide their name, address, and a brief description of the emergency.
Rationale for incorrect answers:
3. It is unsafe to tell children that any of the parents' friends or neighbors are automatically safe. Abuse often occurs by individuals known to the family. Children should be taught to trust their instincts and always report uncomfortable situations, even with familiar people.
4. Teaching a child to only report touching of shoulders and back is too limited. Safe-touch education should include instruction on private body parts and boundaries, using correct anatomical terms, and the message that any uncomfortable or inappropriate touch, regardless of the area, should be reported.
Take home points
- Personal safety teaching for preschool-aged children should include safe people, safe situations, and how to get help.
- Safety plans should empower children while avoiding fear-based messaging.
- Parents should teach children that anyone can be a danger, even familiar people, and that their body boundaries deserve respect.
- Children should know their full name, address, and how to dial 911 for emergencies.
A 5-year-old child is not gaining weight appropriately. Organic problems have been ruled out. What is the priority action by the nurse?
Explanation
Inadequate weight gain in a preschool-aged child with no organic cause may suggest issues such as inadequate caloric intake, feeding dynamics, or psychosocial factors such as family stress, food insecurity, or behavioral feeding problems. Understanding the child's actual intake patterns and mealtime environment is crucial for identifying the root of the problem and tailoring appropriate interventions.
Rationale for correct answer:
4. Assessment is the priority nursing action in the absence of an identified physical cause. A detailed dietary and feeding history, including types of food offered, portion sizes, mealtime behaviors, caregiver-child interaction, and feeding frequency, provides the foundation for identifying behavioral or environmental contributors to poor weight gain.
Rationale for incorrect answers:
1. Unlimited access to a sippy cup, especially with milk or juice, may decrease appetite for solid foods and lead to poor nutritional balance. Grazing or constant sipping can disrupt hunger cues and is discouraged.
2. Encouraging sweets for calories is inappropriate. While extra calories are needed, they should come from nutrient-dense foods such as whole milk, peanut butter, avocados, or full-fat yogurt, not from low-nutrient, sugary foods that can displace healthier options.
3. Teaching about nutrition is important, but it comes after assessment. Without understanding the child's current intake, teaching may be unfocused or irrelevant to the family's actual challenges or routines.
Take home points
- In cases of poor weight gain with no organic cause, nutritional assessment is the first priority.
- Feeding history should include what, when, how, and with whom the child eats.
- Avoid over-reliance on liquids or sweets; focus on nutrient-dense foods.
- Nurses play a key role in identifying behavioral and environmental barriers to nutrition and guiding families toward healthy feeding practices.
The mother of a 5½-year-old child who is 36 inches tall and who weighs 42 pounds states that the child complains every time she attempts to strap her child into the car seat. The nurse searches the Internet and finds the specifications of the child’s car seat are as follows:
• Maximum weight forward facing: 40 lb
• Minimum weight forward facing: 22 lb
• Maximum weight rear facing: 40 lb
• Minimum weight rear facing: 5 lb
• Maximum height forward facing: 40 in.
• Minimum height forward facing: 28 in.
Which of the following statements would be appropriate for the nurse to make at this time?
Explanation
According to car seat safety guidelines, once a child exceeds the weight or height limit for their current car seat, they should transition to the next appropriate restraint system. In this case, the child weighs 42 pounds, exceeding the car seat’s maximum forward-facing weight limit of 40 pounds, and should therefore move to a booster seat.
Rationale for correct answer:
2. The child has outgrown the weight limit for the current forward-facing car seat (40 lb max). Booster seats are recommended for children who outgrow their forward-facing harnessed car seat but are not yet tall enough (typically 4 feet 9 inches) to use a regular seatbelt alone. A booster seat helps position the seatbelt correctly over the child's body for safety.
Rationale for incorrect answers:
1. While the child is not yet 40 inches tall, height alone does not determine when to switch to a booster. Weight limits are equally critical. Since the child exceeds the weight limit, staying in the car seat may now be unsafe.
3. The minimum height is not the issue. The child already exceeds both the minimum weight and height requirements. The maximum weight is what disqualifies the child from continuing in this seat.
4. The minimum weight for forward-facing (22 lb) is not relevant here. The child is already well above that threshold. The focus needs to be on the maximum weight, which has been exceeded.
Take home points
- Children must be transitioned out of a car seat when they exceed its maximum height or weight limits, whichever comes first.
- Booster seats are the next step after outgrowing a forward-facing car seat and are essential for proper seatbelt positioning.
- Nurses should counsel parents on using manufacturer guidelines and AAP car seat safety recommendations to ensure optimal child passenger safety.
- Safety always outweighs convenience or complaints, if a child has outgrown a seat, continuing to use it can be dangerous.
How many hours of sleep per 24 hours does a typical preschooler require?
Explanation
Sleep hygiene includes routines, behaviors, and environmental conditions that support consistent, high-quality sleep. Adequate sleep is essential for growth hormone release, immune function, behavior regulation, and memory and learning
Rationale for correct answer:
3. Preschoolers typically need 10 to 13 hours of total sleep per 24-hour period, including both nighttime sleep and naps. This amount of sleep supports critical physical, emotional, and cognitive development during these formative years.
Rationale for incorrect answers:
1. 6–8 hours is insufficient for a preschooler and is more appropriate for adults or adolescents.
2. 8–10 hours is too little for most preschoolers. While some older children might function on the lower end of this range, preschoolers need more to support rapid growth.
4. 13–15 hours is more typical of infants or toddlers, not preschool-aged children.
Take home points
- The recommended sleep for preschoolers is 10–13 hours in 24 hours (including naps).
- Sleep disturbances such as night terrors or nightmares are common in this age group and should be addressed with consistent bedtime routines.
Comprehensive Questions
The nurse caring for a preschool child understands which of the following developmental concepts? Select all that apply
Explanation
Preschoolers (ages 3–5) are in Piaget’s preoperational stage, where they exhibit egocentrism, magical thinking, and limited logical reasoning. Understanding these concepts helps nurses and caregivers approach communication and education effectively.
Rationale for correct answers:
1. Egocentric thought is a hallmark of preschoolers. They often assume others see, think, and feel exactly as they do. This is a normal part of early cognitive development and limits their ability to adopt other perspectives.
2. Play as a tool is powerful in this age group. Through imaginative play and role-playing, preschoolers express feelings and demonstrate what they comprehend about the world around them. Nurses often use therapeutic play to reduce anxiety or assess a child's perception of illness or hospitalization.
5. Magical thinking is common in preschoolers. They may believe their thoughts or wishes cause real events. This can lead to feelings of guilt if something bad happens, as they might believe they caused it. Nurses must provide reassurance and clarification.
Rationale for incorrect answers:
3. Explanations with detail may be overwhelming. Preschoolers benefit from simple, concrete explanations. Using too much detail or abstract reasoning may increase confusion and stress rather than reduce it.
4. Understanding inferences and empathy is limited in this stage. While preschoolers may show basic concern if someone is sad, they do not yet fully grasp abstract feelings or make emotional inferences as older children or adults can. Their empathy is emerging but not mature.
Take home points
- Preschoolers are egocentric and view the world from their own perspective.
- Magical thinking can lead to misunderstandings about illness, death, or punishment.
- Play is not just recreational, it’s a window into their cognitive and emotional world.
- Explanations should be concrete, visual, and brief, avoiding abstract reasoning.
When her preschool son is in the hospital, the parent tells the nurse, “I think there is something wrong with him because he is so skinny.” The most appropriate answer by the nurse is:
Explanation
Growth is the increase in body size, including height, weight, and head circumference. It reflects changes in the skeletal system, muscle mass, and organ development. Growth is influenced by factors such as genetics, nutrition, health status, environmental and emotional well-being.
Rationale for correct answer:
2. Between ages 3 to 5, body fat decreases, the legs lengthen, and the preschooler loses the toddler’s characteristic pot-bellied look. This can cause concern for caregivers who are used to a rounder appearance. The child may look thinner, but this is normal and expected with proportional growth.
Rationale for incorrect answers:
1. While the average weight of a preschooler may fall within this range, giving a numerical estimate doesn’t directly address the parent’s concern or explain the reason for the perceived slimness. It may also seem dismissive.
3. The pot-bellied appearance typically starts to fade by age 3, not extend until age 4. Preschoolers begin developing a straighter posture and tighter abdominal muscles earlier than this answer implies.
4. Although it’s true that preschoolers gain about 2 to 3 pounds per year, stating this doesn’t address the visual change in body shape that concerns the parent.
Take home points
- Preschool growth involves changes in body proportions; longer legs, straighter posture, and reduced abdominal prominence.
- It’s normal for preschoolers to appear leaner as they grow, which may seem concerning to parents accustomed to toddler roundness.
- Nurses should provide reassurance by explaining expected developmental changes in simple, supportive terms.
- Education should focus on how children grow, not just how much, to support caregiver understanding and reduce unnecessary worry.
At the clinic appointment, a 4-year-old’s mother wants to discuss several concerns. Which statements require more teaching by the nurse? Select all that apply
Explanation
Preschool years are critical for cognitive, social, and emotional development. While creativity and play are important, certain misconceptions, especially about learning and developmentally appropriate behavior, require clarification and teaching from the nurse.
Rationale for correct answers:
1. Although some educational TV content can be beneficial in small doses, the American Academy of Pediatrics recommends limiting screen time for preschoolers to no more than 1 hour per day of high-quality programming. Passive watching, even of educational programs, can reduce time spent in active, imaginative, or social play, which is more developmentally enriching.
3. Imaginary friends are a normal and healthy part of preschool development. They serve various purposes, such as practicing social roles, expressing feelings, and coping with fears. Discouraging or dismissing this behavior may interfere with emotional development or creativity.
5. While formal academics should not be pushed aggressively, preschoolers are naturally curious and ready for age-appropriate early literacy and numeracy. Using flash cards in a playful, engaging manner can support pre-academic skills and should not be entirely dismissed. This response reflects a missed opportunity for developmentally appropriate learning.
Rationale for incorrect answers:
2. Playing dress-up is an important part of preschool play, supporting creativity, social development, and gender exploration. It is perfectly normal and healthy for boys to engage in pretend play alongside girls. No additional teaching is needed here.
4. The parent’s statement reflects an appropriate understanding of the importance of parent-child interaction and play in early childhood. Unstructured playtime with a parent promotes bonding, emotional regulation, and social skills.
Take home points
- Imaginary play and creativity are essential parts of preschool development and should be supported, not discouraged.
- Screen time should be limited, and interactive, imaginative play should be prioritized.
- Early exposure to learning tools like flash cards can be beneficial if used in a playful, pressure-free way.
- Nurses should guide parents on recognizing developmentally appropriate behaviors and encourage balanced support for learning, play, and creativity.
One of the concerns of the preschool period is adequate nutrition. What can the nurse say to give anticipatory guidance to parents?
Explanation
Preschoolers typically exhibit unpredictable eating patterns. It’s important for parents to understand that occasional variations in intake are normal, and healthy children often balance their nutritional needs over the course of a day or week.
Rationale for correct answer:
2. Research supports that preschoolers have an innate ability to self-regulate food intake when offered a variety of nutritious options. They may eat little at one meal and make up for it at another. This anticipatory guidance reassures parents and prevents unnecessary anxiety or pressure around eating.
Rationale for incorrect answers:
1. Preschoolers need about 90–100 kcal/kg/day, not 110 kcal/kg. The average total intake is closer to 1,200–1,800 calories/day, depending on age, size, and activity, not 2,200 calories, which is more appropriate for adolescents or very active older children.
3. While it is true that fat intake should be moderated, dairy and meat are important sources of protein, calcium, iron, and other nutrients. Limiting them to twice a day may undermine adequate nutritional intake unless replaced with high-quality alternatives. Instead, the focus should be on choosing lean meats and low-fat dairy rather than reducing frequency.
4. Fruit juice is not a healthy alternative to milk. Juice lacks the protein, fat, and calcium found in milk and is high in sugar. The American Academy of Pediatrics recommends limiting juice to 4–6 ounces per day for preschoolers, and water or calcium-fortified plant-based milks (e.g., almond or soy) may be better alternatives for children who dislike cow’s milk.
Take home points
- Preschoolers often self-regulate food intake and should not be forced to eat when not hungry.
- Parental anxiety about eating can lead to power struggles; offering a variety of healthy choices is more effective.
- Nutrient-dense foods are more important than calorie quantity, quality over quantity matters.
- Limit juice consumption and avoid using it as a milk substitute; consider other calcium-rich options if milk is refused.
At an appointment at the pediatrician’s office, a patient’s mother states, “My son gets rough with some of the neighborhood kids. I am worried that he is becoming a bully.” Which statements by the mother need more teaching? Select all that apply
Explanation
Aggressive behaviors in preschoolers are quite common and often developmentally typical, though they can be distressing for caregivers. These behaviors usually stem from limited emotional regulation, impulse control, and communication skills. These behaviors in preschoolers require supportive, developmentally appropriate interventions that teach emotional regulation, not harsh discipline or normalization of harmful behavior.
Rationale for correct answers:
1. The idea that aggressive behavior must be punished reflects a misunderstanding of effective behavior management. Punishment often increases fear or resentment without teaching appropriate alternatives. Positive discipline strategies, like time-outs, redirection, and emotional coaching, are more effective in helping children learn self-control.
2. While bonding with a parent is beneficial, passive screen time, especially involving violent or aggressive content, has been linked to increased aggression in children. Watching TV together without discussing content or modeling healthy behavior may reinforce negative actions.
4. Saying “boys will be boys” minimizes and normalizes aggression, which discourages healthy behavior correction. Aggression is not an acceptable or inevitable stage of development. Children need to be taught empathy, communication, and boundaries.
Rationale for incorrect answers:
3. Teaching a preschooler to express feelings in words rather than through physical actions helps build emotional intelligence and social skills. This statement reflects a developmentally appropriate strategy.
5. Time-outs are a recommended discipline technique for preschoolers. They provide a cooling-off period and are more constructive than spanking, which can lead to increased aggression and emotional harm.
Take home points
- Preschool aggression should be addressed through positive behavior strategies, not punishment or minimization.
- Parental modeling, including screen content and reactions to conflict, strongly influences child behavior.
- Statements like “boys will be boys” can undermine the importance of teaching empathy and respectful behavior.
- Encourage emotional expression, clear boundaries, and age-appropriate consequences like time-outs or loss of privileges.
A 4-year-old child, who is hospitalized with pneumonia, tells the nurse, “I got sick because I was bad. I yelled at my little sister yesterday.” The nurse determines that which of the following is an accurate explanation for the child’s comment? The child is:
Explanation
Preschoolers are in Piaget’s preoperational stage, where magical thinking is prominent. They believe that their thoughts, wishes, or behaviors can cause real-world events, even illness or injury, because they cannot yet separate cause from coincidence.
Rationale for correct answer:
2. Magical thinking is a normal cognitive feature of preschool-aged children. They may believe that bad behavior causes bad outcomes, like getting sick. This stems from limited understanding of causality and can lead to feelings of guilt. Nurses must correct these misconceptions gently and provide reassurance.
Rationale for incorrect answers:
1. Preschoolers may seek comfort when ill, but this statement is not a form of manipulation or sympathy-seeking. It reflects a sincere belief shaped by their developmental stage.
3. While preschoolers enjoy imaginative stories, this comment is not a playful fabrication, it reveals a misunderstanding of illness due to magical thinking.
4. Though the child may feel some regret, the belief that being “bad” caused the illness goes beyond simple remorse. It is an example of flawed logic rather than true emotional processing.
Take home points
- Magical thinking in preschoolers can lead them to believe their thoughts or actions cause illness or misfortune.
- Nurses should provide age-appropriate explanations and reassure the child that illness is not a punishment for behavior.
- Understanding developmental psychology helps nurses address emotional needs as well as physical ones.
- Encouraging open conversation and correcting misunderstandings fosters emotional resilience and trust in healthcare settings.
A kindergarten child, who has developed a fever since arriving at school, is resting in the school nurse’s office. It is 11:30 a.m. The child asks, “When is my mommy going to get me?” The nurse knows that the mother will arrive in approximately 30 minutes. Which is the best response for the nurse to give to the child? “Your mommy should get here:
Explanation
Preschool and early school-age children often do not yet fully grasp the concept of clock time. They understand time better when it is related to familiar daily routines like lunch, snack time, or nap time.
Rationale for correct answer:
3. Linking the mother's arrival to a concrete, familiar routine such as lunch time, helps the child feel more secure and better understand the timing. This approach is developmentally appropriate for kindergarten-age children, who typically cannot yet tell time or interpret abstract time intervals.
Rationale for incorrect answers:
1. “In about a half hour” is too abstract for most 5-year-olds. They do not have a reliable sense of what "30 minutes" feels like.
2. “When both hands on the clock reach 12” assumes the child knows how to read an analog clock, which most kindergarteners cannot do yet.
4. “At 12 o’clock noon” uses formal clock language, which is generally not meaningful to children at this stage of development.
Take home points
- Young children understand time in relation to routines, not numbers on a clock.
- Nurses should provide concrete, relatable explanations to reduce anxiety and promote understanding.
- Developmentally appropriate communication builds trust and emotional comfort, especially when a child is sick or upset.
- Avoid using abstract time language like minutes or hours when talking to young children.
The nurse is giving a 5-year-old child a vaccine injection. The child cries loudly during the procedure. Which of the following interventions would be appropriate for the nurse to perform after the injection?
Explanation
After a painful or stressful procedure, emotional support and positive reinforcement are essential for young children. Providing comfort and a small reward, such as a sticker, helps reduce fear and build resilience for future healthcare experiences.
Rationale for correct answer:
4. Comforting the child and offering a sticker provides positive reinforcement and acknowledges the child’s bravery. This developmentally appropriate response helps the child associate medical procedures with support and care, rather than fear and punishment.
Rationale for incorrect answers:
1. Telling a child that "big children are quiet" is shaming and dismissive. It implies that the child did something wrong by crying, which is a normal emotional reaction at this age.
2. Explaining why vaccines are given may be more appropriate before the procedure, but afterward, the child is likely focused on the pain or distress, not the rationale. At 5 years old, the child may not fully comprehend the explanation either.
3. Informing the child that the provider ordered the vaccine may seem like an attempt to deflect responsibility and does nothing to comfort or validate the child's feelings.
Take home points
- Preschool and early school-age children benefit from comfort, reassurance, and tangible rewards after stressful events.
- Crying is a normal, age-appropriate reaction to pain; it should not be shamed or discouraged.
- Focus post-procedure care on emotional recovery, not explanation or discipline.
- Positive reinforcement builds cooperation and trust in medical settings, making future encounters easier for both the child and the caregiver.
A nurse is preparing to give a 5-year-old child preoperative teaching for abdominal surgery. Which of the nurse’s actions is most appropriate?
Explanation
A 5-year-old child is in Erikson’s stage of Initiative vs. Guilt and Piaget’s preoperational stage. At this age, children learn best through play, imitation, and sensory engagement. They have active imaginations and may fear unfamiliar environments like operating rooms.
Rationale for correct answer:
2. Dressing up in surgical attire is a form of medical play, which is effective for preparing preschoolers for procedures. It helps the child become familiar with the hospital environment, reduces anxiety, and gives the child a sense of participation and control. This kind of interactive teaching is ideal for their developmental stage.
Rationale for incorrect answers:
1. Explaining the procedures is helpful but must be very concrete and simplified. Preschoolers do not possess the conceptual ability to understand from an explanation what procedure will be performed. If done alone without hands-on involvement, it may not be effective for a 5-year-old who still has limited abstract thinking.
3. Telling the child why the surgery will make them healthier is too abstract for this developmental age. Preschoolers do not fully understand future health benefits and are more focused on immediate experiences and sensations.
4. Having the child meet another child who had surgery introduces unpredictability. The peer may share frightening or confusing information, which could increase anxiety instead of alleviating it.
Take home points
- Medical play is an ideal teaching method for preschoolers because it uses imagination and sensory involvement to reduce fear.
- Children at this age benefit from active participation, not just verbal explanations.
- Concrete, familiarization strategies, like dressing up, using dolls, or exploring safe medical tools, help children feel more in control.
- Nurses should tailor preoperative education to the developmental stage, hands-on, play-based learning is best for age 5.
A nurse is having difficulty communicating with a hospitalized 5-year-old child. Which of the following techniques is appropriate for the nurse to use to improve communication?
Explanation
Preschoolers communicate best through play, storytelling, and symbolic expression, not through direct verbal explanation. Puppetry is a developmentally appropriate technique that allows the child to express feelings and fears indirectly and safely.
Rationale for correct answer:
4. Using puppets enables non-threatening, imaginative communication, which is ideal for 5-year-olds. It helps the child express thoughts and emotions while feeling safe and engaged. The puppets can also model procedures or hospital routines, promoting understanding and emotional processing.
Rationale for incorrect answers:
1. Keeping a diary is not appropriate for a 5-year-old, who is likely still learning basic writing skills. At this age, children express themselves better through non-written forms such as drawing, play, and verbal storytelling.
2. Reading a fairy tale about scary adventures could intensify anxiety, especially in a hospitalized child. Preschoolers may interpret fiction as reality and internalize frightening stories, worsening their fears.
3. While parental insight is helpful, relying solely on the mother to interpret the child’s emotions does not build communication between the nurse and child. Direct interaction with the child, using developmentally appropriate methods, is crucial for trust and rapport.
Take home points
- Play-based communication, such as puppetry, is highly effective for preschoolers.
- Avoid techniques that are too advanced such as diaries or emotionally confusing such as scary stories.
- Nurses should aim to connect with the child directly, using imaginative and familiar tools.
- Understanding a child’s cognitive and emotional stage enhances therapeutic communication and reduces anxiety in the healthcare setting.
A mother tells the nurse that it is difficult to get her 4-year-old child to bed at night. Which of the following should the nurse suggest that the mother do?
Explanation
Sleep hygiene includes routines, behaviors, and environmental conditions that support consistent, high-quality sleep. For preschoolers, ages 3–5, the goal is to help them get 10–13 hours of sleep per 24 hours, including naps.
Rationale for correct answer:
3. Preschoolers thrive on consistency and routine. A predictable sequence, such as taking a bath, brushing teeth, reading a story, and then going to bed, helps signal to the child that it’s time to wind down. Over time, this ritual becomes a behavioral cue that prepares the body and mind for sleep.
Rationale for incorrect answers:
1. Offering a present or material reward can undermine intrinsic motivation and does not address the root cause of bedtime resistance. It may also promote a pattern where the child expects a reward for basic routines.
2. Playing a running game before bedtime is stimulating, not calming. Physical activity close to bedtime increases alertness and adrenaline, making it harder for the child to settle down and fall asleep.
4. Allowing late weekend bedtimes disrupts the child’s internal sleep-wake rhythm and makes weekday bedtime more difficult. Sleep routines should be consistent across all days to maintain healthy patterns.
Take home points
- Establishing a consistent, calming bedtime routine is the most effective strategy for preschoolers with sleep difficulties.
- Avoid stimulating activities before bed, opt for quiet time, stories, or gentle music instead.
- Material rewards should not be the basis for sleep compliance; focus on nurturing habits, not transactional behavior.
- Consistency is key, routine sleep and wake times help regulate the child's biological clock and improve overall behavior and mood.
Parents inform the nurse that their 4½-year-old daughter “stutters a lot.” The nurse should advise the parents to do which of the following? Select all that apply
Explanation
Mild stuttering is common in children aged 3–5 years as they experience rapid language development. This developmental disfluency often resolves on its own. The goal is to support the child’s confidence and reduce any anxiety or pressure around speaking.
Rationale for correct answers:
1. Waiting patiently shows the child that her words are valued. Interrupting or rushing can increase anxiety and worsen stuttering.
3. Making eye contact while listening conveys attention, acceptance, and support, helping the child feel understood and confident.
4. Speaking slowly and clearly models fluent speech and creates a calm environment. It encourages the child to slow down without needing direct correction.
5. Avoiding comments about stuttering prevents the child from becoming self-conscious, which can exacerbate the problem. Keeping communication natural and pressure-free is key.
Rationale for incorrect answer:
2. Giving treats for clear speech turns normal communication into a performance and may cause the child to feel pressure or shame when stuttering occurs. This approach is counterproductive and may lead to increased anxiety or reluctance to speak.
Take home points
- Developmental stuttering is common and usually temporary in preschoolers.
- Encourage speech by being attentive, patient, and supportive, not by correcting or rewarding.
- Avoid drawing attention to the stuttering, pressure can worsen disfluency.
- If stuttering persists beyond age 6, worsens, or is accompanied by physical tension or frustration, referral to a speech-language pathologist is appropriate.
A nurse is planning to use the Denver Articulation Screening Examination (DASE) for a 4-year-old child. To properly use the DASE, the nurse should plan to ask the child to:
Explanation
The Denver Articulation Screening Examination (DASE) is a standardized tool used to assess articulation and speech sound development in children ages 2½ to 7 years. It helps identify children who may have articulation delays or disorders by evaluating their ability to produce specific speech sounds correctly. The test involves repeating familiar words that the examiner reads aloud, allowing the nurse to assess for misarticulations or omissions.
Rationale for correct answer:
3. The DASE is administered by having the child repeat words spoken by the examiner, allowing evaluation of speech sound production. This method is appropriate for preschoolers, aligns with the purpose of the tool, and does not require reading skills, which are typically undeveloped at age 4.
Rationale for incorrect answers:
1. Reading a favorite book is not part of the DASE and requires reading ability that most 4-year-olds do not yet have. It also assesses comprehension, not articulation.
2. Reading a phrase and explaining its meaning assesses comprehension and vocabulary, not articulation. This exceeds the expected verbal skill level for a 4-year-old and is outside the DASE’s scope.
4. Stating letters of the alphabet assesses letter recognition or memory, not speech articulation. It is unrelated to the test’s purpose.
Take home points:
- The DASE evaluates speech articulation by having children repeat spoken words.
- It is appropriate for children ages 2½–7 years, especially when assessing concerns about unclear or delayed speech.
- Reading or defining phrases is not developmentally appropriate for 4-year-olds in this context.
- Nurses should use age-appropriate, validated tools like the DASE to screen for speech delays and guide referrals.
A parent telephones the nurse in the primary health-care provider’s office and states, “My 4½-year-old child was screaming and kicking in her sleep. She really scared me, but by the time I got into her bedroom, she seemed to be quiet again. What should I do if that happens again?” Which of the following responses by the nurse is appropriate?
Explanation
Night terrors are a type of sleep disturbance common in preschool-aged children, usually occurring in the first few hours of sleep during deep (non-REM) stages. Unlike nightmares, the child is not fully awake and typically does not remember the event. The best approach is to let the episode pass without waking the child, while ensuring the environment is safe.
Rationale for correct answer:
3. Night terrors are self-limiting and usually resolve as the child matures. Waking the child during a night terror can be confusing or distressing and may prolong the episode. Offering reassurance afterward, if the child does wake up, is appropriate. Otherwise, observe quietly and ensure safety.
Rationale for incorrect answers:
1. Talking about fears during the day is more helpful for nightmares, not night terrors. Night terrors are not typically linked to daytime anxiety or specific fears, and the child does not remember the episode, so discussing it may be unhelpful.
2. A night light may help children afraid of the dark or experiencing nightmares, but it does not prevent night terrors, which occur during non-REM sleep and are not related to external stimuli like lighting.
4. Waking the child up and telling them they are safe is suited for nightmares, not night terrors. In a nightmare, the child wakes up and seeks comfort. In a night terror, the child appears awake but is actually in a deep sleep and will often not recognize or respond to others.
Take home points
- Night terrors are common in preschoolers and usually go away without intervention.
- During a night terror, the child is not fully awake and typically doesn’t recall the event.
- Do not try to wake the child; instead, observe, ensure safety, and allow the episode to pass.
- Distinguish between nightmares where the child wakes and remembers the dream, and night terrors where the child remains asleep and is unaware.
Which result should a nurse expect if a 4-year-old child’s visual acuity test is normal for the child’s developmental age?
Explanation
Visual acuity refers to the clarity or sharpness of vision. Visual acuity improves with age, reaching 20/20 by approximately age 6–7. Early detection of vision problems is important to prevent conditions like amblyopia, which can be treated more effectively when caught early.
Rationale for correct answer:
3. At age 4, 20/40 vision is developmentally normal. This means the child can see at 20 feet what a person with perfect vision sees at 40 feet. It reflects typical visual development at this age.
Rationale for incorrect answers:
1. 10/10 is not a standard measurement in vision testing and is not used clinically in the U.S.
2. 20/20 vision is ideal but not expected for most 4-year-olds. While some may achieve it, it is more typical for older children, around 6 years and above.
4. 40/40 is not a valid or recognized measure of visual acuity. Standard measurements use 20 as the baseline.
Take home points
- 20/40 is normal visual acuity for a 4-year-old, with gradual improvement expected as the child grows.
- Routine vision screening begins in the preschool years to identify early issues.
- Nurses should recognize age-based norms to properly evaluate developmental progress and guide parental expectations.
- Referral is needed if visual acuity is worse than age norms or if there's evidence of strabismus or other visual concerns.
Exams on Growth And Development In Preschoolers
Custom Exams
Login to Create a Quiz
Click here to loginLessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Analyze the physical growth patterns of the preschooler, noting the shift from the "pot-bellied" toddler to a more slender, agile body proportions.
- Evaluate the psychosocial stage of Initiative vs. Guilt, identifying how preschoolers explore their environment and develop a sense of purpose.
- Identify cognitive milestones within the preoperational phase, specifically focusing on magical thinking, animism, and egocentrism.
- Discuss the development of body image and sexuality, including the child's natural curiosity about anatomical differences.
- Interpret the preschooler's moral and spiritual development, characterized by an understanding of "good" and "bad" based on parental rewards and punishment.
- Formulate nursing strategies to manage common developmental concerns affecting preschoolers.
- Educate caregivers on health promotion, including nutritional requirements, sleep hygiene, and dental care.
- Prioritize safety interventions for the preschool age group.
Introduction
- The preschool period, encompassing ages three to five, is a transformative era where the child transitions from the home-centered life of a toddler to the social world of peers and school.
- For the pediatric nurse, this stage is marked by a significant refinement of motor skills and a dramatic expansion of language and imagination.
- Biologic development becomes more stabilized; the rapid growth of infancy slows, and the child’s physical appearance changes as the trunk and limbs lengthen. This physical readiness allows the preschooler to engage in more complex activities, such as hopping, skipping, and using scissors, reflecting the maturation of both gross and fine motor coordination.
- Psychosocially, the preschooler is navigating Erikson’s stage of Initiative vs. Guilt. This is a time of intense "doing" and "trying."
- Children at this age are eager to help with chores and engage in "associative play," where they begin to interact and share with others, though their play remains largely unorganized. This initiative is heavily influenced by their cognitive state, the Piaget’s preoperational phase.
- The nurse must understand that the preschooler’s world is governed by magical thinking and "animism," where inanimate objects are believed to have lifelike qualities. This has direct implications for nursing care, for instance, a blood pressure cuff might be seen as a "pinching monster," requiring the nurse to use therapeutic play to demystify medical equipment.
- The preschooler also begins to develop a more concrete body image and a curiosity about sexuality and gender identity.
- They become acutely aware of physical differences and may exhibit "doctor play" as a way to understand their bodies.
- Socially, the child is learning to regulate emotions, though they may still struggle with aggression and various developmental fears, such as fear of the dark or "monsters."
- By understanding these foundational concepts, the nurse can provide a supportive environment that encourages the child's blossoming independence while providing the structure they still desperately need.
Promoting Optimum Growth And Development
3.1. Biologic Development
Preschoolers experience continued but slower physical growth compared to infancy and toddlerhood. Growth is more proportional, with a decrease in the prominence of the abdomen. Motor skills become increasingly refined.
- Gross Motor Behavior:
- 3 years: Rides a tricycle, stands on one foot for a few seconds, jumps off bottom step, broad jumps.
- 4 years: Hops on one foot, throws ball overhead, catches ball reliably, climbs and descends stairs with alternate feet.
-
- 5 years: Skips with alternate feet, jumps rope, ice skates/roller skates, swims, climbs trees, walks backward heel-to-toe.
- Nursing Insight: Encourage active play, provide safe environments for gross motor skill practice (e.g., playgrounds, open spaces), and emphasize the importance of physical activity for overall health.
- Fine Motor Behavior:
- 3 years: Builds tower of 9-10 cubes, imitates vertical and horizontal strokes, copies a circle, dresses and undresses self (with some help).
- 4 years: Uses scissors successfully, copies a square, draws a person with 2-4 parts, laces shoes, dresses self completely.

-
- 5 years: Ties shoelaces, copies a diamond and triangle, draws a person with 6 parts, prints first name, learns to write letters and numbers.
- Nursing Insight: Provide opportunities for drawing, coloring, cutting, building blocks, and other activities that promote fine motor coordination. Encourage self-feeding and dressing to foster independence.
3.2. Psychosocial Development
- Sense of Initiative vs. Guilt (Erikson): Preschoolers are in Erikson's third stage of psychosocial development. They are eager to try new things and master new skills. They enjoy imaginative play and exploring their environment. Successfully navigating this stage leads to a sense of purpose and direction. If their initiative is stifled by overly critical parents or excessive control, they may develop a sense of guilt.
- Nursing Insight: Encourage imaginative play, offer choices, allow for safe exploration, praise efforts and accomplishments, avoid excessive criticism, and provide opportunities for the child to take on responsibilities.

- Oedipal Stage/Phallic Stage (Freud): According to Freud, preschoolers are in the phallic stage, characterized by a focus on the genital area and the development of the Oedipus (boys) or Electra (girls) complex. This involves unconscious sexual desires toward the parent of the opposite sex and rivalry with the parent of the same sex. Resolution of these complexes is crucial for gender identity development.
- Nursing Insight: Be aware of this theoretical stage, but focus on providing a safe and non-judgmental environment. Answer questions about bodies and sexuality simply and honestly at the child's developmental level. Promote healthy gender identity and self-esteem.
3.3. Cognitive Development (Preoperational Stage - Piaget)
Preschoolers are in Piaget's preoperational stage, which is characterized by:
- Egocentrism: Difficulty seeing things from another person's perspective.
- Magical Thinking: Belief that thoughts or actions can influence events in the real world (e.g., believing they caused a sibling's illness).
- Animism: Attributing lifelike qualities to inanimate objects (e.g., a doll is "sad").
- Centration: Focusing on only one aspect of a situation at a time.
- Irreversibility: Difficulty understanding that an action can be reversed.
- Transductive Reasoning: Connecting two events that occur close in time, without understanding cause and effect.
- Symbolic Thought: Development of language and the ability to use symbols (words, objects) to represent other things, evident in pretend play.

-
- Nursing Implications: Use concrete examples and simple language when explaining procedures or concepts. Engage in play as a teaching tool. Acknowledge and validate their feelings, even if based on magical thinking. Avoid abstract concepts.
3.4. Moral Development
Preschoolers are typically in the preconventional level of Kohlberg's theory of moral development. Their moral reasoning is based on:
- Punishment and Obedience Orientation: Good and bad are defined by what is punished or rewarded.
- Naïve Hedonism/Instrumental Relativist Orientation: Actions are chosen based on what satisfies their own needs or results in a reward.
- Nursing Insight: Set clear, consistent rules with simple explanations. Use positive reinforcement for desired behaviors. Emphasize the impact of their actions on others in a concrete way. Help them understand the concept of fairness.
3.5. Spiritual Development
- Preschoolers' understanding of spirituality is influenced by their egocentrism and concrete thinking. They may see God or a higher power as a "super-person" who grants wishes or punishes bad behavior. They often imitate religious practices observed in their families.
- Nursing Implications: Respect family spiritual practices. Answer questions about spirituality honestly and simply, based on the child's understanding. Avoid imposing personal beliefs.
3.6. Development of Sexuality
- Preschoolers become increasingly aware of their own bodies and the differences between boys and girls. They may engage in "doctor games" or ask questions about where babies come from. They often show curiosity about nudity.
- Nursing Implications: Provide factual, age-appropriate information in response to questions. Use correct anatomical terms. Teach about "good touch" and "bad touch." Foster a healthy and positive view of their bodies.
3.7. Development of Body Image
- Preschoolers begin to form a basic understanding of their body parts and how they function. They may express preferences for certain clothing or hairstyles. Their body image is largely influenced by what they see and hear from adults.
- Nursing Implications: Promote a positive body image by focusing on what the body can do rather than its appearance. Avoid negative comments about body size or shape. Encourage healthy habits.
3.8. Social Development
- Language:
- Rapid vocabulary growth (from ~900 words at 3 years to ~2100 words at 5 years).
- Increased sentence length and complexity.
- Begins to use prepositions, adverbs, and conjunctions.
- Engages in longer conversations.
- Nursing Insight: Read aloud regularly, engage in conversations, ask open-ended questions, correct grammatical errors gently, and encourage storytelling.
- Personal-Social Behavior:
- Increased independence in self-care (dressing, toileting, feeding).
- Develops friendships and enjoys cooperative play.
- Learns to share and take turns (though still challenging at times).
- Expresses emotions more effectively.
- Nursing Implications: Encourage independence in self-care, facilitate social interactions, teach sharing and turn-taking, help them identify and express emotions in healthy ways.
- Play:
- Associative Play: Children play together, engaging in similar activities but without a shared goal (e.g., two children building separate towers next to each other).
- Cooperative Play: Children play together with a shared goal and division of labor (e.g., building a sandcastle together).
- Imaginative Play/Pretend Play: Essential for cognitive and social development, allowing children to explore roles, solve problems, and express emotions.
- Dramatic Play: Acting out roles and scenarios.
- Nursing Implications: Provide a variety of toys that encourage imaginative and cooperative play. Create opportunities for dramatic play. Recognize the importance of play as a learning tool.
Temperament
Temperament refers to an individual's innate behavioral style and characteristic way of responding to stimuli. It is thought to be largely genetic and remains relatively stable over time. Understanding a child's temperament can help parents and caregivers adapt their parenting strategies and avoid power struggles.
- Categories of Temperament (Chess & Thomas):
- Easy Child: Generally positive mood, adaptable, regular in bodily functions, mild-to-moderate intensity of reactions.
- Difficult Child: Irregular bodily functions, negative mood, slow to adapt, intense reactions, withdraws from new situations.
- Slow-to-Warm-Up Child: Low activity level, somewhat negative mood, slow adaptability, mild-to-moderate intensity of reactions, initial withdrawal followed by gradual acceptance of new situations.
- Goodness of Fit: The congruence between the child's temperament and the demands and expectations of the environment. A good fit promotes healthy development, while a poor fit can lead to behavioral problems.
- Nursing Implications: Help parents identify their child's temperament. Educate parents on "goodness of fit" and how to adapt their parenting style to their child's temperament. Provide strategies for managing challenging temperaments (e.g., providing predictability for a difficult child, allowing a slow-to-warm-up child time to adjust). Reassure parents that temperament is not a reflection of their parenting skills.
Coping With Concerns Related To Normal Growth And Development
1.1. Preschool and Kindergarten Experience
- Preparing the Child:
- Visitation: Visit the school together beforehand.
- Talk about it: Discuss what to expect in a positive and reassuring way.
- Read books: Read books about starting school.
- Practice: Practice routines (e.g., packing a backpack, opening lunchbox).
- Address fears: Acknowledge and validate any fears the child may have.
- Positive reinforcement: Focus on the fun aspects of school and new friends.
- Nursing Implications: Provide anticipatory guidance to parents regarding school readiness. Discuss common anxieties and coping strategies. Emphasize the importance of clear communication with school staff.
1.2. Sex Education
- Age-appropriate information: Provide simple, factual answers to questions as they arise. Use correct anatomical terms.
- "Good Touch" / "Bad Touch": Teach children about personal boundaries and that their body belongs to them. Emphasize that they should tell a trusted adult if someone makes them feel uncomfortable.
- Source of information: Parents are the primary educators.
- Nursing Insight: Encourage open communication between parents and children about sexuality. Provide resources for parents on age-appropriate sex education. Reinforce the message of body safety.
1.3. Gifted Child
- Characteristics: Advanced vocabulary, intense curiosity, long attention span for topics of interest, highly imaginative, strong memory, early reading or mathematical abilities.
- Challenges: May become bored in traditional classrooms, social isolation if peers don't share their interests, perfectionism, anxiety.
- Nursing Implications: Advise parents to seek intellectual stimulation (e.g., special programs, challenging activities at home). Emphasize the importance of social and emotional development alongside academic advancement. Advocate for individualized educational plans.
1.4. Aggression
- Normal vs. Concerning: Some aggression (e.g., temper tantrums, occasional hitting) is common in preschoolers as they learn to regulate emotions and socialize. Persistent, severe, or escalating aggression requires intervention.
- Causes: Frustration, limited language skills, seeking attention, modeling aggressive behavior, underlying developmental issues.
- Interventions:
- Time-out: Brief, consistent time-outs for aggressive behavior.
- Redirection: Divert attention to a more appropriate activity.
- Teaching alternative behaviors: Model and teach prosocial behaviors (e.g., "use your words," "share").
- Ignoring attention-seeking behavior (when safe): For mild attention-seeking aggression.
- Consistency: Consistent consequences from all caregivers.
- Identifying triggers: Help children understand what makes them angry.
- Nursing Insight: Educate parents on normal vs. concerning aggression. Provide strategies for managing aggressive behavior. Screen for underlying developmental or emotional issues. Refer to specialists if aggression is persistent or severe.
1.5. Speech Problems
- Common issues: Stuttering, lisping, articulation errors, difficulty with sentence structure.
- When to be concerned: If speech is not understood by strangers by age 4-5, significant difficulty forming sentences, persistent stuttering, or lack of progress.
- Nursing Implications: Conduct developmental screenings, including speech and language. Encourage parents to seek early intervention from a speech-language pathologist if concerns arise. Advise parents to talk to their child clearly and listen attentively.
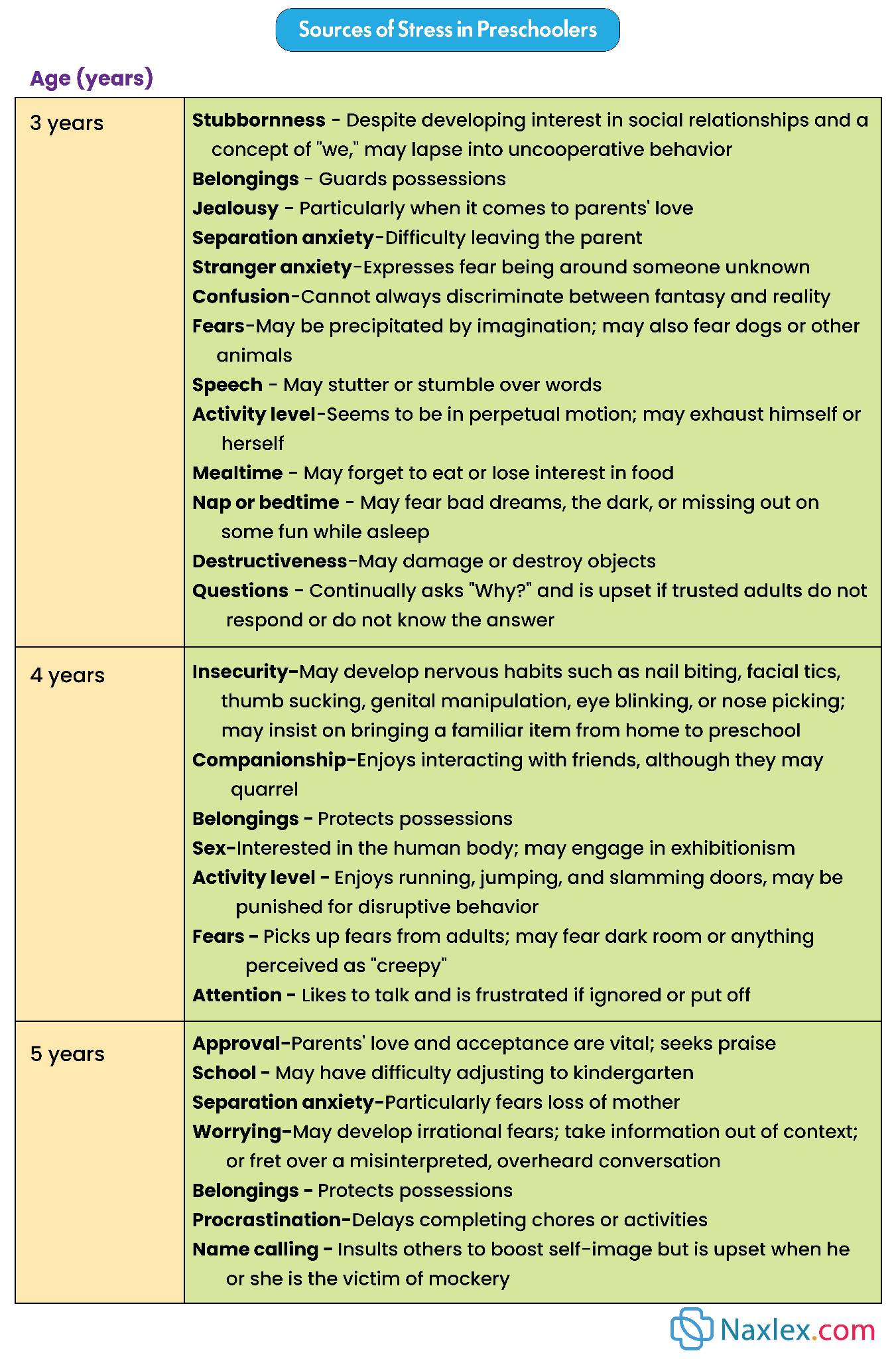
1.6. Stress
- Sources of stress: Changes in routine, new siblings, parental conflict, illness, starting school, too many activities, media exposure.
- Signs of stress: Regression (e.g., bedwetting), increased irritability, sleep disturbances, changes in eating habits, withdrawal, clinginess, somatic complaints (e.g., stomachaches).
- Coping strategies: Providing a consistent routine, open communication, validating feelings, encouraging play, relaxation techniques (e.g., deep breaths), limiting screen time.
- Nursing Implications: Help parents identify sources of stress in their child's life. Educate on the signs of stress and healthy coping mechanisms. Encourage parents to prioritize family time and a calm home environment.
1.7. Fears
- Common fears: Imaginary creatures, the dark, loud noises, strangers, separation from parents. These are normal parts of development.
- Interventions:
- Validate feelings: Acknowledge and respect the child's fear.
- Reassurance: Provide comfort and reassurance.
- Avoid ridicule: Never belittle or make fun of fears.
- Gradual exposure: Slowly introduce the feared object or situation in a safe environment.
- Problem-solving: Help the child develop strategies to cope with the fear (e.g., "monster spray").
- Nursing Implications: Help parents identify stress sources and signs, and teach healthy coping mechanisms like consistent routines, open communication, and validating feelings. For fears, advise parents to validate feelings, offer reassurance, and avoid ridicule, considering gradual exposure when appropriate.
Promoting Optimum Health During Preschool Years
1.1. Nutrition
- Dietary Needs: Preschoolers need a balanced diet with adequate protein, carbohydrates, healthy fats, vitamins, and minerals to support their growth and activity levels.
- Portion Sizes: Offer smaller, age-appropriate portions. Allow children to self-regulate their intake.
- Picky Eaters: Common in this age group. Continue to offer a variety of foods. Avoid battles over food. Make mealtimes pleasant.
- Mealtime Routines: Establish regular meal and snack times. Eat together as a family.
- Fluid Intake: Encourage water. Limit sugary drinks and excessive milk intake.
- Nursing Insight: Provide nutritional counseling to parents. Discuss healthy food choices, portion control, and strategies for managing picky eaters. Reinforce the importance of family meals.
1.2. Sleep and Activity
- Sleep Requirements: Preschoolers typically need 10-13 hours of sleep per 24 hours, often including a daytime nap (which may be phased out by age 5).
- Sleep Routines: Establish a consistent bedtime routine (e.g., bath, story, quiet time).
- Night Terrors/Nightmares: Common. Differentiate between them and provide guidance to parents. (Night terrors: child is not fully awake, inconsolable; Nightmares: child wakes up, remembers dream, can be comforted).
- Activity: Encourage at least 60 minutes of moderate to vigorous physical activity daily. Limit screen time to no more than 1-2 hours per day.
- Nursing Implications: Assess sleep patterns and offer strategies for improving sleep hygiene. Educate parents on the importance of regular physical activity and limiting screen time.
1.3. Dental Health
- Eruption of Primary Teeth: Most primary teeth have erupted by age 3.
- Brushing: Parents should brush the child's teeth twice daily with a pea-sized amount of fluoride toothpaste (once the child can spit effectively).
- Dental Visits: First dental visit by age 1 or within 6 months of the first tooth eruption, then regular check-ups every 6 months.
- Fluoride: Discuss appropriate fluoride intake (water fluoridation, fluoride supplements if needed).
- Diet: Limit sugary snacks and drinks.
- Nursing Insight: Provide anticipatory guidance on dental hygiene. Emphasize the importance of regular dental check-ups and fluoride.
1.4. Safety Promotion and Injury Prevention
- Leading causes of injury: Motor vehicle accidents (MVA), drowning, burns, falls, poisoning.
- Motor vehicle accidents:
- Car seats: Use forward-facing car seats with a harness until the child outgrows the weight/height limits (typically around age 4-7), then booster seats until 4'9" tall.
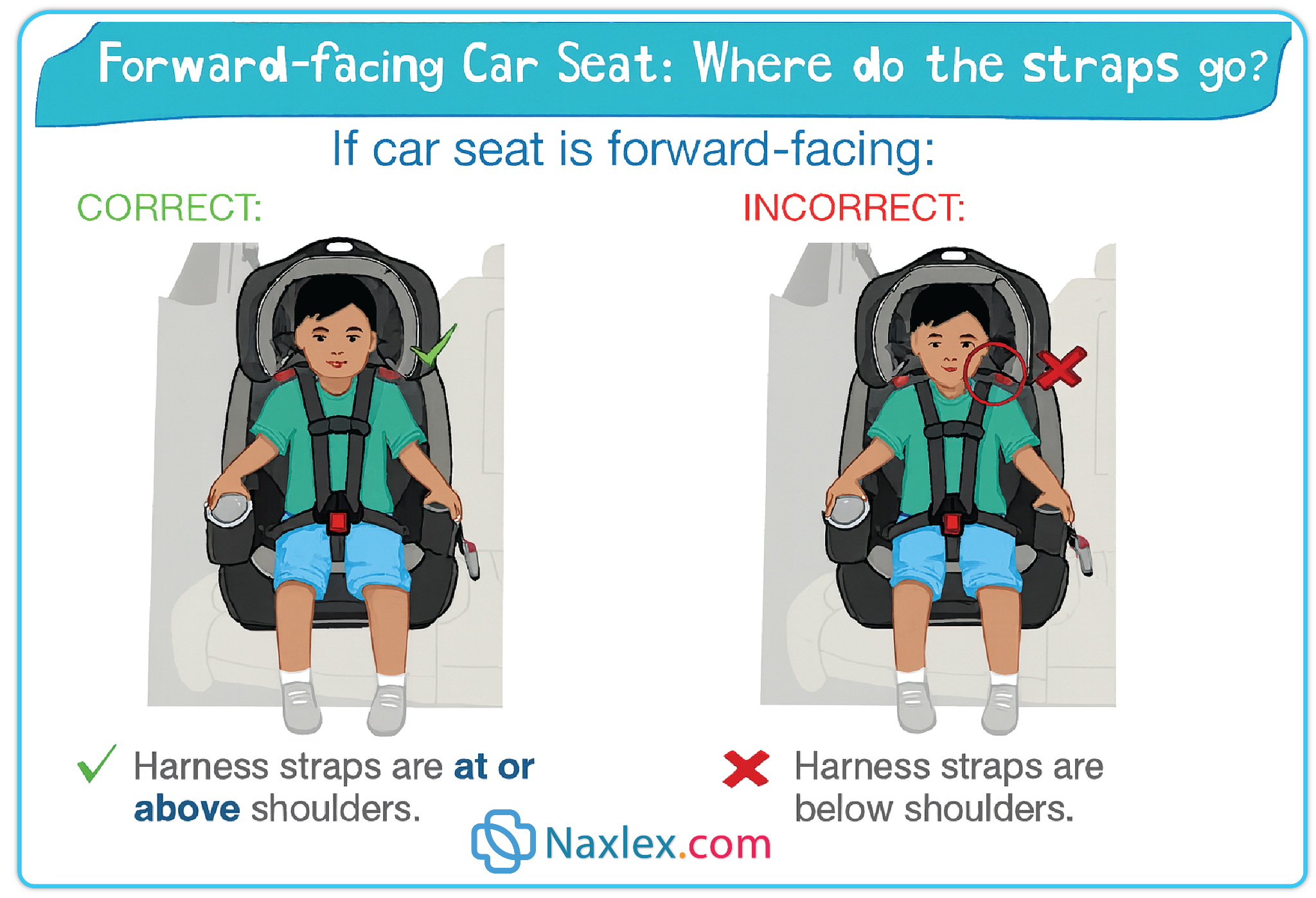
- Back seat: Children under 13 should always ride in the back seat.
- Drowning: Close supervision around water (bathtubs, pools, open water). Fence pools. Teach water safety.
- Burns: Keep hot liquids and appliances out of reach. Check water temperature. Fire safety education.
- Falls: Secure furniture. Use gates on stairs. Supervise climbing.
- Poisoning: Store all medications, cleaning products, and toxic substances in locked cabinets out of reach. Have Poison Control number readily available.
- Choking: Avoid small, hard foods. Supervise eating.
- Pedestrian/Bicycle Safety: Teach "stop, look, and listen." Supervise outdoor play. Use helmets when cycling/scootering.
- Nursing Implications: Provide comprehensive safety education to parents. Emphasize the importance of constant supervision. Model safe behaviors. Screen for home safety hazards.
Summary
- Nursing care for the preschooler involves a delicate balance of screening for developmental delays and providing anticipatory guidance to families.
- As the child prepares for the preschool and kindergarten experience, the nurse plays a pivotal role in assessing "school readiness," which includes social-emotional maturity as much as cognitive ability.
- Common concerns such as speech problems (stuttering) or the management of aggression require the nurse to distinguish between normal developmental variations and issues requiring intervention.
- Additionally, as the child's imagination grows, so do their fears hence nurses should educate parents on how to validate a child’s feelings without reinforcing their irrational anxieties.
- Promoting optimum health during these years focuses on establishing lifelong habits.
- Nutrition shifts toward ensuring a balanced intake of nutrients while avoiding the "food jags" common in earlier years.
- The nurse must also address sleep and activity, as preschoolers are prone to sleep-onset issues and night terrors due to their active imaginations.
- Dental health remains a priority, with the emphasis moving toward independent brushing with parental supervision and regular fluoride treatments.
- Safety promotion is perhaps the most critical nursing intervention. Because preschoolers are more mobile and adventurous but still lack a true sense of danger, they are at high risk for "accidental" injuries. Nurses should teach parents about the importance of bicycle helmets, pedestrian safety (looking both ways), and the continued need for supervision around water.
- By integrating evidence-based sex education such as using correct anatomical terms and answering questions simply and honestly, the nurse helps the child develop a healthy body image.
- The nurse serves as a coach for the family, ensuring the preschooler’s environment is safe, stimulating, and conducive to the successful mastery of early childhood milestones.
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Growth And Development In Preschoolers
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
