
Please set your exam date
Critical thinking, decision making, and the nursing process
Study Questions
Practice Exercise 1
A nurse is assigned to care for a woman who is expecting her first child. The nurse organizes herself and plans to gather data about the client by applying Pender’s health promotion model, including the client’s characteristics and experiences and situational influences. She plans to observe client behavior and consider the client’s psychosocial issues. Such data will offer a clear understanding to help the nurse identify the client’s needs. This is an example of which of the following concepts? Select all that apply
Explanation
Applying an overarching conceptual framework to guide data collection exemplifies deductive reasoning within clinical practice. Constructing a systematic nursing assessment around specific theoretical constructs ensures that data tracking remains comprehensive and goal-directed. Utilizing this top-down approach allows clinicians to organize raw observations into coherent categories defined by the theory. This process transforms fragmented patient signals into an evidence-based framework tailored to individual wellness promotion.
Rationale for correct answers:
B. Deductive reasoning is demonstrated when a clinician applies a general theory or model to a specific patient scenario. By utilizing Pender's Health Promotion Model, the nurse moves from abstract theoretical premises to concrete, individualized data gathering. This top-down cognitive strategy provides structure to the clinical inquiry. It ensures that the practitioner systematically screens for specific theoretical variables and predictable behavioral influences.
D. Assessment is the foundational phase of the nursing process focused on systematic, comprehensive data collection. Planning to observe physical behavior and gather qualitative psychosocial data directly defines this operational step. The nurse is actively collecting baseline information rather than formulating final nursing diagnoses or testing clinical interventions. This deliberate gathering establishes the empirical database necessary for subsequent clinical analysis.
Rationale for incorrect answers:
A. Diagnostic reasoning involves assigning clinical meaning to collected data by clustering cues to identify specific health problems. In this scenario, the nurse is strictly in the planning and information-gathering stage, not yet analyzing or labeling a distinct pathological or wellness state. Prematurely declaring diagnostic conclusions before data collection is complete violates the sequence of clinical processing and structured data synthesis.
C. Inductive reasoning moves in the opposite direction, from specific localized observations to the formation of a generalized conclusion or theory. Since the nurse is starting with an already established, universal framework and applying it downward to one primigravida patient, the cognitive trajectory is not bottom-up. Misclassifying this process ignores the fundamental distinction between theory generation and local theory application.
E. Problem solving focuses on identifying an active clinical malfunction or deficit and implementing an immediate corrective intervention. The scenario centers on health promotion, behavioral observation, and baseline wellness assessment rather than correcting an active physiologic or psychological failure. Selecting this option confuses preventive, framework-driven wellness tracking with reactive, deficit-focused troubleshooting or crisis mitigation strategies.
Test-taking strategy
- Analyze the scenario/question: The question asks to identify the critical thinking and clinical process concepts demonstrated when a nurse utilizes Pender's Health Promotion Model to guide data collection and behavioral observation for a pregnant client.
- Apply concepts of logical direction and clinical phase: Evaluate whether the nurse's actions represent a top-down or bottom-up logical flow, and map the action to the correct stage of the nursing process.
- Choice 2 is correct because starting with a general theory (Pender's model) and looking for specific client clues matches the definition of deductive reasoning. Rule in B.
- Choice 4 is correct because organizing, planning, and gathering raw behavioral and psychosocial data describes the assessment phase. Rule in D.
- Choice 1 and Choice 5 are ruled out because the nurse has not yet clustered the data into diagnoses or implemented steps to fix an active clinical deficit. Rule out 1 and E.
- Choice 3 is ruled out because the cognitive direction is top-down (theory to facts), not bottom-up (facts to theory). Rule out C.
Take home points
- Deductive reasoning in nursing involves using an established theoretical model to guide the collection and organization of specific patient data.
- The assessment phase of the nursing process focuses entirely on planning, observing, and gathering objective and subjective baseline information.
- Health promotion models direct the clinical focus toward behavioral, situational, and psychosocial influences rather than purely reactive problem-solving.
- Diagnostic reasoning can only occur after sufficient assessment data has been systematically gathered, verified, and clustered.
A nurse is caring for a client who has poor pain control. The client has a history of opioid abuse. During the day, the client made frequent requests for a pain medication. To make an effective clinical decision about this client, the nurse needs to ask questions about the data available on the client to make a thorough and thoughtful decision. The nurse asks herself, “How does my view about the client’s pain tolerance compare with the client’s, and does that pose a problem?” This is an example of:
Explanation
Analgesic management in patients with a history of substance use disorder requires careful metacognitive monitoring to prevent personal biases from compromising care. Clinicians must actively examine their own interpretive lenses regarding pain behaviors and chemical dependency to avoid undertreating legitimate physical suffering. Examining how one's professional viewpoint contrasts with the patient's subjective reality constitutes a deliberate cognitive re-framing exercise. This self-appraisal ensures that clinical decisions remain grounded in objective clinical need rather than unexamined professional prejudices.
Rationale for correct answers:
D. Asking how one's personal view compares with the patient's viewpoint directly represents a question about perspective. This critical thinking habit involves recognizing that multiple distinct viewpoints exist surrounding complex clinical phenomena like pain and addiction. The nurse actively analyzes potential conflicts between her own interpretive framework and the patient's internal experience. This specific evaluation targets clinical viewpoint alignment and reflexive bias identification.
Rationale for incorrect answers:
A. Questions about assumptions focus on identifying unstated, taken-for-granted beliefs or premises that are accepted as true without empirical proof. While biased viewpoints often rest upon hidden assumptions, the explicit phrasing of the question compares two distinct viewpoints or mental models. The immediate action is contrasting divergent viewpoints rather than dissecting an unverified underlying premise or unproven claim.
B. Questions about evidence center on evaluating the quality, reliability, source, and clinical precision of objective and subjective assessment data. The nurse's internal inquiry does not evaluate diagnostic lab numbers, physical assessment scales, or the validity of historical medical documentation. Her analysis targets the cognitive interpretation of data rather than checking the integrity of the empirical evidence or factual statistics.
C. Questions about procedure examine the operational steps, institutional protocols, or technical methodologies utilized to execute a specific clinical task. Reviewing one's subjective attitude toward an individual experiencing chemical dependency does not involve evaluating clinical algorithms or drug titrations. The nurse is practicing internal, psychological reflection rather than reviewing an operational workflow or technical protocol.
Test-taking strategy
- Analyze the scenario/question: The question asks to identify the critical thinking concept demonstrated when a nurse internally asks, “How does my view about the client’s pain tolerance compare with the client’s, and does that pose a problem?”
- Apply concepts of critical thinking elements: Evaluate the key words used in the internal question ("my view" vs. "the client's") to determine which cognitive element is being examined.
- Choice 4 is correct because comparing one "view" or framework against another directly matches the definition of exploring perspectives. Rule in D.
- Choice 1 is ruled out because the question does not focus on uncovering hidden, unverified premises accepted blindly as truth. Rule out A.
- Choice 2 is ruled out because the nurse is not questioning the validity or source of objective data or clinical signs. Rule out B.
- Choice 3 is ruled out because the inquiry does not address institutional pathways or technical steps for drug administration. Rule out C.
Take home points
- Questions about perspective involve identifying and contrasting different viewpoints between the healthcare provider and the patient.
- Effective pain management in patients with substance use histories requires continuous self-reflection to mitigate personal biases.
- Critical thinking frameworks differentiate between the data itself (evidence) and the mental lens through which that data is viewed (perspective).
- Identifying a mismatch between provider assumptions and patient experiences prevents the clinical undertreatment of acute or chronic pain.
A client in a cardiac rehabilitation program says to the nurse, “I have to eat a low-sodium diet for the rest of my life, and I hate it!” Which is the most appropriate response by the nurse?
Explanation
The nursing process relies on targeted therapeutic communication to uncover and resolve psychological and behavioral barriers to treatment compliance. When a patient expresses strong frustration or negative emotions regarding a required therapeutic lifestyle change, the nurse must employ open-ended communication to explore the underlying cause. Dietary restrictions, such as a low-sodium restriction, are essential in managing cardiovascular diseases to lower blood pressure, reduce ventricular workload, and prevent fluid retention, but their long-term success depends entirely on addressing the client's subjective challenges.
Rationale for correct answer:
B. The nursing activity involves utilizing an open-ended communication technique to explore the client's underlying resistance to a mandatory lifestyle modification. Asking what makes the regimen difficult directly promotes client emotional exploration by providing a non-judgmental space to express frustration. Gathering this subjective assessment data is required before the nurse can design realistic, individualized dietary coping strategies.
Rationale for incorrect answers:
A. This option is inappropriate because it prematurely passes off the therapeutic relationship responsibility to another department without addressing the client's immediate distress. Requesting an immediate dietary consult is a collaborative intervention that should occur only after the nurse has completed an initial focused assessment of the patient's specific concerns. Bypassing the immediate conversation delays therapeutic rapport and problem exploration.
C. This option is unsafe and non-therapeutic because it completely dismisses the client's valid feelings and forces an unwanted perspective shift. Making statements that start with "at least" represents a patronizing communication failure that invalidates maternal and patient concerns, shutting down any further honest verbalization. Minimizing a patient's daily lifestyle frustrations destroys trust and increases the risk of complete treatment non-compliance.
D. This option is clinically dangerous because it provides false reassurance and inaccurate medical information regarding chronic cardiovascular management. Telling a cardiac rehabilitation patient they might not need a low-sodium diet long-term creates false reassurance and undercuts the mandatory lifelong nature of their therapeutic regimen. Giving misleading information leads to confusion and severe fluid overload complications down the road.
The nurse is caring for a client and reflects on the concept of blended skills in nursing practice. Which statement best describes this concept?
Explanation
The nursing process requires the synchronized application of diverse cognitive, behavioral, and technical proficiencies to provide safe, holistic client care. Blended skills represent an integrated framework comprising cognitive, technical, interpersonal, and ethical/legal competencies. These four domains must be dynamically adapted to meet the specific requirements of each clinical encounter, ensuring that professional actions are scientifically sound, technically precise, relationally compassionate, and legally accountable.
Rationale for correct answer:
B. The nursing activity of delivering comprehensive care depends on the fluid integration of all four competency domains tailored to individual client scenarios. Utilizing cognitive, interpersonal, technical, and ethical/legal skills in a situation-specific manner defines the concept of blended skills. This balanced mastery ensures the clinician addresses both the technical and humanistic dimensions of healthcare.
Rationale for incorrect answers:
A. Professional nursing rejects the notion that relational care and compassion are outdated concepts that can be delegated to untrained individuals. Devaluing interpersonal skills compromises the therapeutic alliance and undermines holistic patient recovery. Interpersonal competence is a specialized, non-negotiable professional skill required to assess emotional and psychological human responses.
C. Every professional nurse is legally and ethically required to achieve baseline competency in all four skill domains rather than being completely deficient in any single area. Being utterly deficient in any competency domain poses an immediate threat to patient safety and violates professional standards of care. A deficit in one area cannot be compensated for by an excellence in another.
D. Clinical scenarios are highly fluid and variable, meaning they do not all demand the exact same proportion or blend of basic nursing competencies. For example, a cardiac arrest requires a heavy emphasis on immediate technical and cognitive skills, whereas end-of-life care demands profound interpersonal and ethical skills. The combination must match the unique situation.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the statement that best describes the concept of blended skills within professional nursing practice.
- Evaluate competency frameworks: Apply knowledge of the four essential nursing competencies: cognitive (intellectual), technical, interpersonal, and ethical/legal.
- Recognize that these skills are interdependent and mandatory for every professional clinician to master.
- Identify that Choice 2 accurately captures the necessity of using all four skills as demanded dynamically by each unique patient situation.
- Eliminate imbalanced or rigid options: Rule out choices that minimize compassion, excuse severe skill deficiencies, or claim that care is completely static.
- Rule out Choice 1 because it inappropriately dismisses interpersonal care as an outdated, non-professional task.
- Rule out Choice 3 because professional practice acts do not permit a nurse to be completely deficient in any foundational core competency.
- Rule out Choice 4 because it incorrectly implies that a rigid, identical blend of skills is applied to every single clinical scenario.
Take home points
- Blended skills consist of cognitive, technical, interpersonal, and ethical/legal competencies that every nurse must possess.
- The specific proportion and application of blended skills must change dynamically based on the unique demands of each clinical situation.
- Interpersonal skills and compassionate communication are specialized professional competencies that cannot be dismissed or treated as optional.
- Deficiency in any single blended skill domain compromises patient safety and violates mandatory professional standards of practice.
A client complains of shortness of breath. During assessment the nurse observes that the client has edema of the left leg only. The nurse reviews evidence-based practice literature and reflects on a previous client with the same clinical manifestations. What do these actions represent?
Explanation
The nursing process relies on an active, fluid cognitive journey to synthesize raw clinical information and guide bedside decision-making. Clinical reasoning represents the comprehensive mental process where a nurse actively gathers data, analyzes physiological relationships, incorporates evidence-based literature, and recalls past experiential knowledge. unilateral lower extremity swelling paired with acute dyspnea demands rapid analytical tracking to evaluate for life-threatening conditions like a pulmonary embolism secondary to a deep vein thrombosis.
Rationale for correct answer:
B. The nursing activity involves actively collecting physical data, retrieving empirical research, and drawing parallels to a past clinical case. This multi-layered cognitive processing defines clinical reasoning, which is the actual thought journey used to interpret patient status. It encompasses both the analytical search for evidence and the integration of personal experiential knowledge.
Rationale for incorrect answers:
A. This option is incorrect because it describes the final outcome or conclusion rather than the active thinking process itself. A definitive clinical judgment represents the final decision, opinion, or clinical conclusion reached as a result of thorough reasoning. Because the nurse is still reviewing literature and analyzing data, they are engaged in the process rather than the final decision.
C. This option is incorrect because it isolates a single component of the nurse's thought process instead of capturing the whole activity. While recalling a previous client represents reflection, it does not account for the concurrent physical assessment or active literature review. Reflection is merely a subset of the broader clinical reasoning framework being displayed.
D. This option is incorrect because the nurse's current actions are driven by explicit empirical data and structured scientific investigation. Expert intuition involves immediate, non-conscious pattern recognition that occurs without a conscious, step-by-step logical analysis or literature search. The nurse's deliberate review of evidence-based literature directly contradicts a purely intuitive approach.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the overarching cognitive concept demonstrated when a nurse assesses a patient, searches scientific literature, and reflects on past clinical experiences.
- Differentiate cognitive processes: Distinguish between the active thinking process, the final decision, and individual components of thought within clinical judgment models.
- Recognize that searching literature and comparing cases represents the dynamic, ongoing cognitive journey of analyzing a situation.
- Select Choice 2 because clinical reasoning is the specific term for the active mental process of translating data into clinical understanding.
- Eliminate overly narrow or final-state terms: Rule out choices that describe only a single aspect of thinking or represent a completed conclusion.
- Rule out Clinical judgment (Choice 1) because it is the final product, not the active process.
- Rule out Reflection (Choice 3) because it only covers looking backward, ignoring the active data collection and literature search.
- Rule out Intuition (Choice 4) because the nurse is using deliberate, analytical steps rather than instantaneous, unguided insights.
Take home points
- Clinical reasoning is the active, multi-dimensional cognitive process used by nurses to analyze and interpret changing patient data.
- Clinical judgment is distinct from clinical reasoning, representing the final conclusion or decision reached at the end of the thought process.
- Unilateral leg edema combined with dyspnea is a critical clinical finding requiring immediate tracking for deep vein thrombosis and pulmonary embolism.
- Integrating evidence-based literature and past clinical reflections are core activities that strengthen accuracy during clinical reasoning.
Practice Exercise 2
A nurse has been caring for a client with a chronic wound that has not been healing. The nurse talks with a nurse specialist in wound care to find alternative approaches from what the health care provider ordered for dressing the wound. The two decide that because of the client’s allergy to tape, a nonallergenic dressing will be used. The nurse obtains an order from the health care provider for the new dressing. After 2 days there is improvement in the wound. This is an example of which critical thinking standards? Select all that apply
Explanation
Clinical problem-solving requires integrating specific intellectual standards alongside dynamic behavioral attitudes to alter ineffective care plans. Applying customized cognitive strategies allows clinicians to overcome clinical impasses, driving innovative interventions that optimize physiological tissue healing.
Rationale for correct answers:
C. Relevance requires that all selected clinical facts and interventions relate directly to the central medical problem. Identifying the patient's tape allergy is highly relevant to resolving the non-healing wound. This specific information allows the nurse to choose a safe, effective dressing material. It ensures that the diagnostic plan directly targets essential data and contextual facts.
D. Risk taking is a critical thinking attitude demonstrated when a nurse explores unconventional paths to improve patient outcomes. Standing up for the patient by questioning an ineffective standard order involves calculated risk. This action moves beyond routine habits to find better therapeutic solutions. It balances professional independence with accountable advocacy.
E. Creativity involves developing unique, customized solutions to circumvent specific clinical barriers or patient contraindications. Modifying a standard dressing regimen to accommodate a severe hypersensitivity reaction requires creative thinking. This tailored adaptation provides an alternative method when standard algorithms fail. It demonstrates clinical ingenuity and original customization.
Rationale for incorrect answers:
A. Clarity focuses on ensuring that clinical data, communication, and orders are clear, precise, and completely unambiguous. While clear communication is needed to update the provider's order, the scenario doesn't describe resolving vague language. The nurse is focused on finding alternative therapies rather than improving linguistic precision or semantic accuracy.
B. Broadness requires looking at a problem from multiple viewpoints and incorporating diverse clinical perspectives. While consulting a wound specialist gathers outside input, the question focuses on the specific acts of identifying an allergy and changing materials. The core standard demonstrated here is targeting the allergy rather than exploring comprehensive viewpoints or global approaches.
Test-taking strategy
- Analyze the scenario/question: The question asks to identify the critical thinking concepts demonstrated when a nurse recognizes a tape allergy, consults a specialist, and takes the initiative to change a dressing protocol.
- Apply concepts of standards and attitudes: Evaluate the choices to identify which terms accurately match the actions of applying relevant data, taking initiative, and customizing care.
- Choice 3 is correct because focusing on the tape allergy addresses a highly relevant piece of clinical information. Rule in C.
- Choice 4 is correct because moving away from an established provider order to advocate for change represents clinical risk taking. Rule in D.
- Choice 5 is correct because adapting the dressing to bypass a specific allergy barrier demonstrates clear creativity. Rule in E.
- Choice 1 and Choice 2 are ruled out because the scenario does not focus on correcting ambiguous phrasing or examining broad, macro-level viewpoints. Rule out 1 and B.
Take home points
- Relevance ensures that clinical interventions are directly connected to specific patient data like allergies.
- Risk taking involves the willingness to question standard, ineffective orders to advocate for better patient outcomes.
- Creativity allows clinicians to adapt standardized medical protocols to overcome unique patient barriers.
- Combining intellectual standards with behavioral attitudes is essential for resolving complex, non-healing clinical issues.
A nurse is preparing medications for a client. The nurse checks the name of the medication on the label with the name of the medication on the health care provider’s order. At the bedside, the nurse checks the client’s name against the medication order as well. The nurse is following which critical thinking attitude?
Explanation
Medication safety protocols rely strictly on individual clinician accountability during the preparation and administration phases. Demonstrating nursing responsibility requires executing mandatory cross-checks to ensure the right medication is delivered safely to the right patient. This systematic verification process forms an essential risk reduction framework designed to intercept adverse drug events before they reach the bedside. Cultivating this diligent professional accountability protects patient welfare and maintains high standards of clinical practice.
Rationale for correct answers:
A. Checking the medication label against the prescription order and validating the patient's identity directly fulfills professional responsibility. This critical thinking attitude involves holding oneself personally accountable for executing safe, standard medical practices. The nurse actively minimizes the risk of harm by adhering strictly to these safety checks. This rigorous verification embodies clinical personal accountability and defensive safety compliance.
Rationale for incorrect answers:
B. Humility involves recognizing the limitations of one's own clinical knowledge and asking for expert assistance when necessary. While a humble mindset is valuable when clarifying confusing or illegible orders, performing routine cross-checks does not represent an admission of knowledge gaps. The action described is a standard execution of duty rather than intellectual modesty or limitation recognition.
C. Accuracy is a critical thinking intellectual standard used to evaluate data precision, but it is not classified as a critical thinking attitude. Attitudes describe the underlying behavioral dispositions and moral motivations that drive a clinician to perform safe actions. Choosing this option represents a fundamental category mistake by confusing an analytical benchmark with a behavioral disposition.
D. Fairness requires delivering medical interventions equitably, justly, and completely free from personal prejudice or bias. While all patients deserve safe medication administration, checking labels does not involve managing social equity or distributing healthcare resources. The nurse is practicing focused bedside safety rather than demonstrating impartial distribution or egalitarian care.
Test-taking strategy
- Analyze the scenario/question: The question asks to identify the specific critical thinking attitude demonstrated when a nurse double-checks a drug label and verifies a client's identity at the bedside.
- Apply concept of critical thinking attitudes: Differentiate between behavioral attitudes (dispositions) and intellectual standards (benchmarks like accuracy).
- Choice 1 directly reflects the attitude of responsibility, which demands that the clinician accept personal accountability for following safety rules. Rule in A.
- Choice 3 must be eliminated because accuracy is an intellectual standard, not a behavioral attitude. Rule out C.
- Choice 2 and Choice 4 represent different attitudes entirely, focusing on admitting ignorance and practicing non-discrimination respectively. Rule out 2 and D.
Take home points
- Responsibility as a critical thinking attitude means accepting personal accountability for executing mandatory patient safety protocols.
- Medication verification at the bedside requires checking the drug label against the order and confirming the client's identity.
- Critical thinking concepts are divided into behavioral attitudes and intellectual standards; accuracy is a standard, while responsibility is an attitude.
- Diligent execution of the rights of medication administration serves as a primary defense mechanism against clinical errors.
A nurse has seen many cancer clients struggle with pain management because they are afraid of becoming addicted to the medicine. Pain control is a priority for cancer care. By helping clients focus on their values and beliefs about pain control, a nurse can best make clinical decisions. This is an example of:
Explanation
Oncology pain management often intersects with deep-seated client fears regarding opioid dependence. Addressing these concerns requires a framework of values clarification, which allows the clinician to align therapeutic goals with the patient's moral and personal belief systems. Utilizing ethical criteria ensures that clinical decisions honor patient autonomy while maximizing the ethical duty of beneficence through effective analgesia. This specialized focus shifts clinical decision-making from a purely technical exercise to an exercise in bioethical evaluation and person-centered care.
Rationale for correct answers:
D. Focusing on a client's individual values and beliefs regarding pain medication directly represents the application of ethical criteria. This practice respects the core bioethical principle of patient autonomy by honoring their unique perspective. It allows the nurse to make therapeutic decisions that balance effective pain relief with the patient's personal moral framework. This targeted approach ensures that the delivery of palliative care remains deeply ethically aligned with the client's worldview.
Rationale for incorrect answers:
A. Creativity involves developing novel, unconventional solutions to unique clinical problems. While resolving an analgesic impasse requires clinical ingenuity, exploring established personal beliefs does not constitute an act of original invention. The nurse is relying on structured ethical frameworks rather than inventing a completely unorthodox strategy or novel intervention.
B. Fairness dictates that clinical care is delivered equitably and without personal bias to all individuals. While the nurse acts justly by not judging the client's fear, the core action described is the active exploration of personal belief systems. Fairness focuses on impartial distribution of medical resources rather than the qualitative exploration of individual maternal values.
C. Clinical reasoning is the broad, overarching cognitive process used to analyze patient data and choose interventions. While clinical reasoning is definitely occurring here, it is too general an option to be the best answer. The question specifically highlights a nurse focusing on values and beliefs, making the application of ethical benchmarks the more precise subcomponent and specific definition required.
Test-taking strategy
- Analyze the scenario/question: The question asks to identify the critical thinking concept demonstrated when a nurse explores a client's internal values and beliefs regarding opioid addiction to guide oncological pain management decisions.
- Apply concepts of bioethics and specificity: Evaluate the choices based on their exact definitions within critical thinking frameworks to find the most precise match.
- Choice 4 directly links the exploration of patient beliefs, morals, and values to clinical choices, which matches the definition of utilizing ethical standards. Rule in D.
- Choice 3 is an umbrella term that encompasses all thinking processes but lacks the specificity required by the question's explicit focus on values. Rule out C.
- Choice 1 and Choice 2 represent different intellectual standards entirely, focusing on uniqueness and non-discriminatory care respectively. Rule out 1 and B.
Take home points
- Applying ethical criteria in nursing care requires integrating the patient's personal values, morals, and belief systems into the diagnostic plan.
- Effective oncology pain management must proactively address psychological barriers like phobia of addiction through collaborative discussion.
- Autonomy and beneficence are balanced when clinical actions are customized to align with the client's clarified healthcare goals.
- Critical thinking frameworks contain distinct subcomponents, and questions focusing on values specifically test ethical criteria over broad reasoning.
The nurse evaluates possible solutions for care of an infected wound for optimal client outcomes. Which reasoning process describes the nurse’s actions?
Explanation
The nursing process relies on structured cognitive methods to resolve clinical challenges and achieve optimal patient outcomes. Problem solving represents a systematic, goal-directed intellectual process where the clinician identifies an issue, analyzes multiple potential interventions, evaluates possible solutions, and executes a planned strategy. Managing an infected wound demands an organized analytical approach to evaluate variables such as microbial burden, exudate volume, and tissue viability, ensuring that selected treatments are grounded in evidence-based wound care rather than unguided, random choices.
Rationale for correct answer:
D. The nursing activity involves systematically assessing a clinical complication, generating multiple potential interventions, and comparing them to find the most effective path forward. Engaging in this focused analytical behavior defines the core of clinical problem solving. This deliberate cognitive approach ensures that care modifications are logical, goal-oriented, and structured to optimize wound healing outcomes.
Rationale for incorrect answers:
A. The nurse is actively evaluating and weighing explicit, structured solutions rather than relying on an unguided feeling. Expert intuition involves an immediate, non-conscious pattern recognition that occurs instantaneously without any conscious, step-by-step logical breakdown or consideration of alternatives. The deliberate analysis of solutions directly contradicts a purely intuitive response.
B. The nurse's immediate goal is to optimize care for an individual client rather than to generate generalized scientific data. The research process is a highly disciplined, formal investigation that involves controlled variables, institutional review boards, and extensive literature replication to create universal nursing knowledge. Individual clinical adjustments fall under daily problem-solving frameworks rather than formal research.
C. The nurse is analyzing and evaluating the merits of solutions before execution rather than acting randomly. The trial and error method is an unstructured, unscientific approach where multiple random interventions are blindly attempted one after another until something accidentally succeeds. Using this disorganized technique on an infected wound creates severe risks of unchecked sepsis.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the specific cognitive reasoning process a nurse is using when systematically evaluating multiple possible solutions to manage an infected wound effectively.
- Differentiate problem-solving methods: Evaluate the distinct characteristics of problem solving, intuition, trial and error, and research within clinical practice models.
- Identify that the nurse is facing a specific clinical challenge and is weighing structured alternatives to achieve a targeted patient goal.
- Select Choice 4 because the structured evaluation of alternatives to resolve a localized clinical issue fits the definition of standard problem solving.
- Eliminate inappropriately structured or non-analytical options: Rule out choices that represent unguided interventions, immediate non-conscious insight, or large-scale scientific studies.
- Rule out Intuition (Choice 1) and Trial and error (Choice 3) because they lack the conscious, systematic evaluation of explicit solutions described in the prompt.
- Rule out Research process (Choice 2) because the nurse is adjusting care for a single patient scenario rather than conducting a formal, generalized scientific study.
Take home points
- Clinical problem solving is a systematic, goal-directed cognitive process used to identify issues and evaluate the best solutions for individual patient scenarios.
- Evaluating wound care solutions requires analyzing specific physical parameters such as exudate characteristics, bacterial load, and localized tissue perfusion.
- Relying on structured problem solving rather than random trial and error protects clients from severe systemic complications like worsening sepsis.
- The research process focuses on generating generalized, universal knowledge, whereas clinical problem solving targets individual patient care optimization.
The charge nurse tells the nurse not to bother studying too hard, since most clinical reasoning becomes “second nature” and “intuitive” once you start practicing. What thinking below should underlie the nurse’s response?
Explanation
The nursing process and modern clinical judgment rely on an integrated cognitive framework combining evidence-based science with experiential knowledge. While intuitive reasoning develops over years of clinical practice, it represents a recognition of patterns rather than an unguided guess. Relying on intuition without balancing it against systematic, objective verification creates significant vulnerabilities, potentially leading to diagnostic errors or fragmented, unscientific patient care.
Rationale for correct answer:
A. The nursing activity of clinical reasoning requires a balance between rapid pattern recognition and objective data validation. Relying on intuition alone significantly amplifies the risk of clinical errors and forces reliance on unscientific trial-and-error approaches. Validating intuitive feelings with evidence-based data ensures safe, predictable, and high-quality patient care.
Rationale for incorrect answers:
B. Professional nursing acknowledges that intuition is a valid component of expert clinical judgment that should not be eradicated. Benner's novice-to-expert framework establishes that intuitive pattern recognition naturally develops with experience. Instead of stamping out intuition, nurses must learn to critically validate it with objective clinical evidence.
C. Advancements in evidence-based practice and logical, scientific frameworks have elevated nursing care outcomes and professional autonomy. Claiming that scientific reasoning has held nursing back directly contradicts the core principles of modern, safe clinical practice. Championing unvalidated creativity over empirical science compromises patient safety and objective clinical standards.
D. Clinical decision-making is governed by rigorous professional, legal, and ethical standards rather than individual cognitive matters of preference. Every professional nurse is legally required to utilize logical, systematic, and evidence-based frameworks to justify clinical actions. Personal thinking styles can complement but never substitute for mandatory scientific reasoning.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the correct scientific thinking that should guide a nurse's perspective when a colleague suggests relying solely on intuition and "second nature" clinical reasoning.
- Evaluate clinical judgment frameworks: Apply established nursing theories regarding evidence-based practice, critical thinking, and Benner's stages of clinical competence.
- Identify that while intuition exists in expert practice, it is highly unsafe when used as an independent, unverified problem-solving method.
- Recognize that Choice 1 correctly identifies the operational speed of intuition while accurately warning against its high-risk, trial-and-error limitations.
- Eliminate extreme or non-scientific viewpoints: Rule out options that either completely reject intuition or inappropriately minimize the necessity of rigorous scientific logic.
- Rule out Choice 2 because it takes an extreme stance of completely erasing an inherent cognitive aspect of expert practice.
- Rule out Choice 3 and Choice 4 because they degrade the mandatory legal and scientific foundations of professional nursing practice to mere personal preferences.
Take home points
- Intuitive reasoning is a valid asset born of clinical experience, but it must always be verified with objective, evidence-based data.
- Relying exclusively on unvalidated intuition increases patient safety risks and often leads to inefficient trial-and-error clinical interventions.
- Expert nurses utilize fluid pattern recognition automatically, but they can always rationalize their final decisions using objective, scientific principles.
- Evidence-based practice and systematic critical thinking remain the non-negotiable legal and professional foundations of all nursing actions.
Practice Exercise 3
The nurse is aware that one element of clinical decision making is knowing the client. Which of the following activities affect a nurse’s ability to know clients better? Select all that apply
Explanation
Deeply knowing the client serves as a foundational component of expert clinical decision-making within healthcare. This multi-dimensional process involves cultivating a highly attuned clinical grasp through direct, immersive patient interactions and continuous exposure to specific clinical populations. Building this intuitive pattern recognition allows clinicians to instantly differentiate between a patient's normal individual variations and early signs of acute physiological decline. Engaging in experiential learning ensures that healthcare providers move beyond abstract, formulaic rule-following into nuanced, context-dependent person-centered care.
Rationale for correct answers:
A. Caring for similar cohorts of patients over time builds an expansive clinical repository of experiential knowledge. This structural exposure allows the nurse to compare current presentations against a deeply ingrained population baseline. It directly fosters the development of specialized clinical expertise and intuitive diagnostic forecasting. This long-term repetition refines experiential expertise and population-specific pattern recognition.
C. Learning a client's typical coping responses to illness provides a baseline for behavioral and physiological normality. This insight allows the clinician to detect subtle deviations that standardized assessment tools often miss. Understanding these habitual trends prevents misinterpreting idiosyncratic patient responses as new pathological developments. This understanding supports behavioral profiling and individualized baseline tracking.
D. Observing clients through continuous, deliberate physical assessment uncovers subtle non-verbal cues and qualitative clinical trends. This active sensory vigilance tracks immediate changes in patient status, such as work of breathing or psychological withdrawal. Direct observation provides the raw empirical data needed to guide subsequent diagnostic interventions. This step maximizes objective surveillance and rapid clinical detection.
E. Engaging with clients directly during their illness experience builds a deep understanding of their unique values and preferences. This collaborative interaction allows the nurse to look past the medical diagnosis to understand the human response to suffering. It transforms standard technical interventions into tailored, highly individualized healthcare plans. This dialogue enhances therapeutic engagement and holistic interpersonal immersion.
Rationale for incorrect answers:
B. Reading external evidence-based literature provides generalized, non-specific population data rather than specific insight into an individual client. While research updates theoretical knowledge, it cannot provide the experiential or contextual familiarity required to "know" a specific person. Universal guidelines offer abstract frameworks rather than localized, patient-centered understanding. This tool provides generalized knowledge rather than individual contextual intimacy.
Test-taking strategy
- Analyze the scenario/question: The question asks for specific activities that directly improve a clinician's capacity to "know the client," which is a specific element of clinical decision-making that emphasizes experiential familiarity and individual baseline tracking.
- Apply concepts of experiential familiarity: Evaluate each choice to distinguish between generalized textbook knowledge and direct, patient-specific experiential learning.
- Choice 1, Choice 3, Choice 4, and Choice 5 involve direct, immersive contact with patients or specific populations, which builds pattern recognition. Rule in 1, 3, 4, and E.
- Choice 2 involves abstract literature review, which informs general practice but does not provide specific clinical grasp of individual patient dynamics. Rule out B.
- Eliminate non-specific frameworks: Rule out choices that prioritize theoretical data over direct clinical observation and experiential tracking.
Take home points
- Knowing the client is an experiential process driven by direct interaction, deliberate observation, and pattern recognition over time.
- Population familiarity achieved through caring for similar groups allows nurses to anticipate common clinical trajectories and needs.
- General evidence-based guidelines inform broad clinical protocols but cannot substitute for patient-specific contextual baseline tracking.
- Attuned observation and therapeutic engagement reveal qualitative behavioral and physiological data that checklists fail to capture.
The nurse is concerned about a client who begins to breathe very rapidly. Which action by the nurse reflects clinical reasoning?
Explanation
The nursing process dictates that comprehensive data collection must always precede clinical analysis and medical notification. Clinical reasoning requires the nurse to gather immediate objective parameters to identify the underlying cause of an acute change in status. When a patient exhibits sudden tachypnea (rapid breathing), the clinician must immediately evaluate physiological indicators, such as oxygen saturation and full vital signs, to differentiate between respiratory distress, metabolic abnormalities, or acute cardiovascular instability before initiating external communication.
Rationale for correct answer:
B. The nursing activity involves gathering immediate objective data to analyze the severity and cause of the patient's sudden tachypnea. Obtaining full vital signs and oxygen saturation reflects accurate clinical reasoning by prioritizing immediate physiological assessment. This critical data collection provides the necessary baseline information required to determine the urgency of subsequent interventions.
Rationale for incorrect answers:
A. This option is premature because the nurse lacks the essential physiological data required to deliver a comprehensive clinical report. Notifying the primary care provider before assessing vital signs and oxygenation prevents an effective SBAR (Situation-Background-Assessment-Recommendation) communication. The nurse must collect baseline clinical findings to provide a meaningful situation update.
C. This option is incorrect because ordering diagnostic imaging falls outside the independent legal scope of professional nursing practice. Requesting a chest x-ray requires a specific diagnostic provider order and cannot be initiated autonomously by the nurse. Furthermore, executing an imaging study takes precedence only after completing an immediate bedside assessment.
D. This option is premature because the nurse has not yet established whether the client is experiencing a life-threatening physiological emergency. Activating the rapid response team should be reserved for specific, documented clinical deterioration criteria, such as severe, uncorrectable hypoxemia or hemodynamic collapse. The nurse must assess the patient first to justify this escalation.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the action that best reflects clinical reasoning when a nurse encounters a client who suddenly begins to breathe very rapidly.
- Apply nursing process and prioritization rules: Use the foundational principle that assessment and data collection must always occur before implementing an intervention or notifying a provider.
- Identify that tachypnea is a clinical sign that requires immediate, deeper investigation to determine the patient's oxygenation and hemodynamic status.
- Select Choice 2 because obtaining vital signs and pulse oximetry represents the mandatory assessment step needed to drive safe clinical reasoning.
- Eliminate premature escalations: Rule out options that involve notifying other team members or ordering tests before bedside data has been gathered.
- Rule out Choice 1 and Choice 4 because calling a provider or a crisis team without vital sign data represents an unvalidated panic response rather than structured reasoning.
- Rule out Choice 3 because it is a dependent intervention that cannot be done autonomously and delays immediate bedside evaluation.
Take home points
- Clinical reasoning dictates that a rapid bedside assessment must always occur before escalating care or notifying a physician.
- Gathering vital signs and oxygen saturation provides the objective data needed to structure an effective, professional SBAR report.
- Independent nursing assessment must be prioritized during acute respiratory changes to ensure patient safety and rule out immediate danger.
- Escalating care to a rapid response team requires clear, documented objective criteria gathered during a preliminary physical assessment.
The nurse considers that a client is from a developing country and may have a positive tuberculosis test due to a prior vaccination. Which critical thinking attitude and skill is the nurse practicing?
Explanation
The nursing process dictates that comprehensive data collection must always precede clinical analysis and medical notification. Clinical reasoning requires the nurse to gather immediate objective parameters to identify the underlying cause of an acute change in status. When a patient exhibits sudden tachypnea (rapid breathing), the clinician must immediately evaluate physiological indicators, such as oxygen saturation and full vital signs, to differentiate between respiratory distress, metabolic abnormalities, or acute cardiovascular instability before initiating external communication.
Rationale for correct answer:
B. The nursing activity involves gathering immediate objective data to analyze the severity and cause of the patient's sudden tachypnea. Obtaining full vital signs and oxygen saturation reflects accurate clinical reasoning by prioritizing immediate physiological assessment. This critical data collection provides the necessary baseline information required to determine the urgency of subsequent interventions.
Rationale for incorrect answers:
A. This option is premature because the nurse lacks the essential physiological data required to deliver a comprehensive clinical report. Notifying the primary care provider before assessing vital signs and oxygenation prevents an effective SBAR (Situation-Background-Assessment-Recommendation) communication. The nurse must collect baseline clinical findings to provide a meaningful situation update.
C. This option is incorrect because ordering diagnostic imaging falls outside the independent legal scope of professional nursing practice. Requesting a chest x-ray requires a specific diagnostic provider order and cannot be initiated autonomously by the nurse. Furthermore, executing an imaging study takes precedence only after completing an immediate bedside assessment.
D. This option is premature because the nurse has not yet established whether the client is experiencing a life-threatening physiological emergency. Activating the rapid response team should be reserved for specific, documented clinical deterioration criteria, such as severe, uncorrectable hypoxemia or hemodynamic collapse. The nurse must assess the patient first to justify this escalation.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the action that best reflects clinical reasoning when a nurse encounters a client who suddenly begins to breathe very rapidly.
- Apply nursing process and prioritization rules: Use the foundational principle that assessment and data collection must always occur before implementing an intervention or notifying a provider.
- Identify that tachypnea is a clinical sign that requires immediate, deeper investigation to determine the patient's oxygenation and hemodynamic status.
- Select Choice 2 because obtaining vital signs and pulse oximetry represents the mandatory assessment step needed to drive safe clinical reasoning.
- Eliminate premature escalations: Rule out options that involve notifying other team members or ordering tests before bedside data has been gathered.
- Rule out Choice 1 and Choice 4 because calling a provider or a crisis team without vital sign data represents an unvalidated panic response rather than structured reasoning.
- Rule out Choice 3 because it is a dependent intervention that cannot be done autonomously and delays immediate bedside evaluation.
Take home points
- Clinical reasoning dictates that a rapid bedside assessment must always occur before escalating care or notifying a physician.
- Gathering vital signs and oxygen saturation provides the objective data needed to structure an effective, professional SBAR report.
- Independent nursing assessment must be prioritized during acute respiratory changes to ensure patient safety and rule out immediate danger.
- Escalating care to a rapid response team requires clear, documented objective criteria gathered during a preliminary physical assessment.
A client reports feeling hungry, but does not eat when food is served. Using clinical reasoning skills, the nurse should perform which of the following?
Explanation
The nursing process relies on continuous, objective data validation to guide clinical decision-making and resolve discrepancies in patient behavior. When a conflict arises between a client's verbal report and their physical actions, the nurse must avoid assumptions. A client may refuse food due to physiological barriers such as dysphagia (difficulty swallowing), nausea, or dental pain, as well as sociocultural or psychological factors. Systematic nursing assessment must always precede any clinical intervention or modification to the plan of care.
Rationale for correct answer:
A. The nursing activity requires resolving the immediate contradiction between the client's stated hunger and their actual refusal to eat. Conducting an immediate focused assessment identifies the underlying physiological, psychological, or cultural barriers preventing nutritional intake. Gathering this essential data is the mandatory initial step required to formulate safe, effective, and targeted nursing interventions.
Rationale for incorrect answers:
B. This option is dangerous because leaving food at the bedside indefinitely introduces severe risks of bacterial proliferation and food contamination. Neglecting to investigate the cause of food refusal can lead to progressive nutritional decline and muscle wasting. Simply waiting for hunger to increase ignores potential acute physical barriers like worsening dysphagia or severe nausea.
C. This option is premature because it jumps to an invasive, high-risk intervention before any baseline problem identification has occurred. Recommending enteral tube feeding without assessing simpler barriers, such as unpalatable food or temporary nausea, violates the principle of least-restrictive care. It bypasses the mandatory diagnostic steps of the clinical framework.
D. This option is unsafe because it dismisses the client's subjective communication based on a subjective, unverified personal assumption. Labeling the patient's statement as untruthful demonstrates a severe cognitive bias that destroys the therapeutic relationship. Critical thinking demands validating discrepancies through objective assessment rather than adopting personal disbelief.
Test-taking strategy
- Analyze the scenario and question: The question requires determining the most appropriate action when a client displays a direct contradiction between a subjective complaint (feeling hungry) and an objective behavior (not eating).
- Apply prioritization and process frameworks: Use the foundational rule of the nursing process: assessment must always precede intervention.
- Identify that the nurse lacks sufficient data to understand why the client is refusing the food tray.
- Select Choice 1 because it is the only option focused on systematic data collection and problem exploration before implementing a solution.
- Eliminate premature or defusal options: Rule out choices that either implement premature interventions, dismiss the patient, or pass the responsibility to another provider.
- Rule out Choice 2 and Choice 4 because they ignore the patient's nutritional safety and rely on unverified assumptions.
- Rule out Choice 3 because recommending an invasive intervention before completing a comprehensive nursing assessment is clinically unsound.
Take home points
- Comprehensive assessment and data validation must always occur before the nurse plans or implements a clinical intervention.
- Discrepancies between a patient's verbal statements and their physical behaviors require immediate, focused clinical investigation.
- Nutritional barriers can stem from diverse physiological issues like dysphagia or nausea, as well as psychological or cultural preferences.
- Dismissing a client's subjective reports or assuming their intent introduces dangerous cognitive biases that compromise client safety.
In the clinical reasoning process, the nurse sets and weighs the criteria, examines alternatives, and performs which of the following before implementing a plan?
Explanation
The nursing process requires a highly disciplined cognitive framework during the planning and decision-making phase to minimize clinical errors. When selecting a specific course of action, the nurse sets criteria, weighs alternatives, and systematically reexamines the purpose of the decision before execution. This critical step ensures that the chosen nursing intervention remains strictly aligned with the core therapeutic goal and the patient's primary pathological or psychological needs, preventing cognitive drift or misdirected clinical care.
Rationale for correct answer:
A. The nursing activity of clinical decision-making demands a final metacognitive check to ensure the chosen strategy directly matches the original goal. Having set criteria and weighed alternatives, the nurse must reexamine the purpose of the decision before final implementation. This step verifies that the selected path remains appropriate and directly solves the primary clinical problem.
Rationale for incorrect answers:
B. This option is incorrect because checking client and family preferences should occur much earlier when establishing the initial criteria. Waiting until after alternatives have already been generated and weighed to consult on the view of the criteria disrupts the logical sequence of planning. It represents an inappropriately timed communication step in the decision-making model.
C. This option is incorrect because identifying alternative methods is an action that has already been completed in the scenario. The stem explicitly states that the nurse has already examined alternatives as part of the cognitive workflow. Re-engaging in identifying various means at this point creates an unnecessary, redundant loop that stalls the execution of care.
D. This option is incorrect because anticipating future secondary complications occurs during a different phase of the clinical framework. Formulating contingency plans for should intervening problems arise is a component of risk management and proactive evaluation. It is not the immediate, mandatory cognitive step required to finalize the primary choice of action.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the precise next step in the structured clinical decision-making process after a nurse has set criteria and examined alternatives, but before a plan is implemented.
- Apply decision-making frameworks: Analyze the logical, sequential phases of cognitive problem-solving within nursing models.
- Recognize that after weighing options, the thinker must perform a final quality-control check to ensure the path matches the original objective.
- Select Choice 1 because re-evaluating the central purpose of the decision serves as the vital final verification step before putting a plan into action.
- Eliminate completed or out-of-sequence options: Rule out actions that describe steps already accomplished in the prompt or those that fall outside the immediate sequence.
- Rule out Choice 3 because examining alternatives has already occurred according to the question stem.
- Rule out Choice 2 and Choice 4 because they represent either early baseline input gathering or distant contingency planning rather than the immediate pre-implementation check.
Take home points
- Reexamining the central purpose of a decision before implementation ensures clinical actions remain perfectly aligned with patient goals.
- Clinical decision-making is a structured cognitive process that requires setting clear criteria and systematically weighing all available alternatives.
- Consulting the client and family regarding care criteria must occur during the initial phases of planning rather than immediately before execution.
- Meta-cognition, or actively thinking about one's own reasoning process, is essential for reducing diagnostic errors and optimizing care outcomes.
Comprehensive Questions
The nurse is caring for a client and reviews the concept of the nursing process. Which statement is most accurate?
Explanation
The nursing process represents a universally recognized professional framework designed to deliver continuous, goal-oriented care. This cognitive model evolves dynamically to ensure professional nursing practice remains distinct from medical specialties, anchoring clinical decision-making within an interpersonal and humanistic paradigm.
Rationale for correct answer:
D. National licensing bodies structured professional examinations around the nursing process to establish a standardized framework for evaluating clinical competence. This organizing framework replaced historic medical specialties testing divisions. It ensures evaluation focuses on clinical reasoning rather than rote anatomical memorization.
Rationale for incorrect answers:
A. The nursing process utilizes a five-step cyclical sequence rather than a limited four-step process protocol. It consists of assessing, diagnosing, planning, implementing, and evaluating. Omiting any stage disrupts the essential clinical feedback mechanism. Therefore, this numerical description remains fundamentally inaccurate.
B. Historical records confirm that Florence Nightingale did not utilize or practice this formalized modern framework. The structural methodology was introduced in the mid-twentieth century by professional nursing theorists. Nightingale focused instead on environmental hygiene and sanitation. Thus, this statement represents historical anachronism.
C. Utilizing this standardized scientific method is a mandatory legal requirement rather than an optional clinical preference. State practice acts and professional scopes of practice institutionalize the framework. It ensures uniform quality and legal accountability across healthcare institutions. Consequently, professional compliance remains compulsory.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the most accurate statement regarding the professional evolution, structure, and legal definition of the nursing process.
- Evaluate professional and structural frameworks: Apply historical and contemporary knowledge of nursing education, legal scopes of practice, and licensing criteria to evaluate each statement.
- Identify that the modern framework features five steps, making Choice 1 factually incorrect.
- Recognize that state board examinations transitioned away from traditional medical models to evaluate universal nursing behaviors, validating Choice 4 as the correct professional trend.
- Differentiate practice realities from myths: Rule out choices that claim the process is non-compulsory or historically tied to nineteenth-century nursing.
- Rule out Choice 3 because the nursing process is legally mandated by nurse practice acts and is never optional.
- Rule out Choice 2 because the framework was developed in the mid-twentieth century, long after Nightingale's era.
Take home points
- The nursing process is an organized, five-step clinical framework mandatory for professional practice rather than an optional workflow.
- State board examinations utilize client needs and the nursing process as an organizing concept to test analytical reasoning instead of medical specialties.
- Modern nursing frameworks were developed by twentieth-century theorists and were not part of the nineteenth-century curriculum of Florence Nightingale.
- Every phase of the five-step process is interdependent, requiring precise execution to maintain professional and legal standards of care.
The nursing process ensures that nurses are patient centered rather than task centered. Rather than simply approaching a client to take vital signs, the nurse thinks “How is Mrs. Barclay today? Are our nursing actions helping her to achieve her goals? How can we better help her?” This demonstrates which characteristic of the nursing process?
Explanation
The nursing process establishes a humanistic framework that prioritizes the client's holistic experience over routine clinical tasks. An interpersonal approach demands that the nurse views the client as a dynamic partner in care rather than a passive recipient of interventions. This relational core forms the foundation for therapeutic communication, ensuring that all subsequent nursing phases directly reflect the unique values, goals, and psychosocial needs of the individual.
Rationale for correct answer:
B. The nursing process establishes a direct human connection that prioritizes client-centered care over purely routine physical tasks. This specific approach exemplifies the foundational interpersonal characteristic of clinical practice. It ensures the client is actively engaged as a partner rather than an object of care.
Rationale for incorrect answers:
A. A systematic characteristic implies that clinical activities follow a highly ordered, predictable, and logical sequence. While the care delivery follows a sequence, the specific thoughts regarding the client's holistic well-being express person-centered philosophy. It does not illustrate sequential task organization. Therefore, this description is inappropriate.
C. The dynamic characteristic indicates that the five steps possess a great deal of overlapping fluidity. This features a continuous movement back and forth between assessments and active interventions. While the thought pattern shows clinical flexibility, it specifically emphasizes relationship-centered values. Hence, it represents fluidity rather than partnership.
D. Universal applicability means the clinical framework can be applied effectively across all age groups, settings, and health conditions. This addresses the scope of practice rather than the specific philosophical shift from tasks to persons. It highlights operational versatility rather than therapeutic relationship dimensions.
Test-taking strategy
- Analyze the scenario and question: The question asks to identify the specific nursing process characteristic demonstrated when a clinician prioritizes a patient's goals and well-being over standard physical tasks.
- Identify core practice characteristics: Analyze the underlying clinical philosophy expressed in the Mrs. Barclay scenario, distinguishing between structural, temporal, and relational attributes.
- Recognize that focusing on the patient as a unique individual rather than a vital sign task emphasizes the human-to-human connection.
- Select Choice 2 because it directly aligns with the defined interpersonal characteristic that places the human being at the heart of nursing care.
- Differentiate other process attributes: Rule out definitions that describe the order, flexibility, or environment of care delivery.
- Rule out Systematic (Choice 1) because the focus is on relationships, not an ordered workflow.
- Rule out Dynamic (Choice 3) and Universally applicable (Choice 4) because they describe process movement and systemic scope rather than person-centered engagement.
Take home points
- The interpersonal characteristic ensures that nursing care remains holistically patient-centered rather than focused on isolated technical tasks.
- Collaborating with patients as active partners honors their autonomy and directly enhances the therapeutic relationship.
- While the nursing process is systematic and ordered, its execution must always be adjusted to fit humanistic, individual needs.
- Shifting focus from task completion to goal achievement is the defining element of professional, person-centered nursing care.
The nurse is caring for a client and reviews the concept of critical thinking indicators (CTIs). Which statement best describes CTIs?
Explanation
The nursing process relies on the intentional application of critical thinking to ensure accurate clinical reasoning and optimal patient outcomes. Critical thinking indicators (CTIs) serve as an operational framework to measure and develop this intellectual capacity. These indicators provide clear, evidence-based behaviors that illustrate the specific personal characteristics, foundational knowledge, and intellectual skills required to safely analyze complex clinical scenarios and make sound diagnostic decisions.
Rationale for correct answer:
C. The nursing activity of evaluating clinical judgment requires a multi-dimensional framework that incorporates personal attributes alongside intellectual capabilities. CTIs provide explicit descriptions of behaviors that demonstrate the necessary knowledge, characteristics, and skills that promote critical thinking in clinical practice. This definition encompasses the affective traits, such as open-mindedness, that are essential for accurate clinical reasoning.
Rationale for incorrect answers:
A. This option is incomplete because it restricts critical thinking indicators solely to the cognitive acquisition of theoretical concepts. Focusing entirely on the knowledge ignores the critical behavioral skills and personal dispositions required to apply that knowledge at the bedside. Therefore, this narrow scope fails to reflect the holistic nature of clinical critical thinking.
B. This option remains overly restrictive by omitting the personal traits and attitudes that dictate how a clinician approaches problems. While combining knowledge and skills captures the intellectual and psychomotor dimensions, it leaves out vital personal attributes like intellectual humility and integrity. Consequently, it represents an incomplete operational definition of the concept.
D. This option introduces an incorrect structural element that does not belong within the standard behavioral definition of the concept. Professional standards refer to external legal, ethical, or institutional benchmarks that govern practice rather than an individual's personal, observable clinical behaviors. Including them conflates external regulatory guidelines with internal cognitive indicators.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the most accurate and comprehensive definition of critical thinking indicators (CTIs) within professional nursing practice.
- Evaluate critical thinking frameworks: Apply established nursing education models, specifically Alfaro-LeFevre's critical thinking indicators framework, which categorizes indicators into distinct human dimensions.
- Recognize that true critical thinking requires a combination of what you know (knowledge), how you act (skills), and who you are as a thinker (personal characteristics/dispositions).
- Identify that Choice 3 completely captures these three core dimensions—knowledge, characteristics, and skills—in an integrated, evidence-based behavioral definition.
- Eliminate incomplete or inflated options: Rule out choices that either oversimplify the concept by dropping key human dimensions or overcomplicate it by adding inappropriate external elements.
- Rule out Choice 1 and Choice 2 because they are too limited, ignoring the vital personal dispositions that drive critical thinking behavior.
- Rule out Choice 4 because external professional standards are distinct regulatory rules, not individual behavioral indicators.
Take home points
- Critical thinking indicators are evidence-based, observable behaviors that demonstrate a clinician's capacity for sound clinical judgment.
- Comprehensive critical thinking requires a combination of three domains: personal characteristics, foundational knowledge, and intellectual skills.
- Personal characteristics like curiosity, intellectual humility, and fair-mindedness are essential components of an effective critical thinker.
- CTIs are used as an objective framework in clinical education to assess, self-regulate, and systematically improve clinical reasoning behaviors.
A client with diarrhea also has a primary care provider’s order for a bulk laxative daily. The nurse, not realizing that bulk laxatives can help solidify certain types of diarrhea, concludes, “The primary care provider does not know the client has diarrhea.” What type of statement is this?
Explanation
The nursing process demands precise information processing to avoid clinical reasoning errors during data interpretation. An inference represents a cognitive leap where a clinician links an observation to a conclusion without sufficient factual verification. In pharmacology, hydrophilic bulk-forming laxatives absorb excess fluid to solidify fecal consistency in specific diarrheal states. Jumping to conclusions regarding a provider's awareness without validating the clinical rationale illustrates an unverified cognitive deduction.
Rationale for correct answer:
B. The nursing activity involves making a subjective deduction based on an incomplete understanding of a pharmacological mechanism. Labeling the provider's awareness based purely on a perceived contradiction constitutes a premature inference. This cognitive step bridges an observation to a conclusion before gathering all necessary facts or verifying the underlying clinical rationale.
Rationale for incorrect answers:
A. This option is incorrect because the nurse's statement lacks objective verification and empirical confirmation. A baseline fact represents information that can be definitively proven true through direct observation or undeniable evidence. Because the provider may fully know the client's status and intended to treat the diarrhea, the nurse's statement is not factual.
C. This option is incorrect because the statement does not assign a moral, ethical, or qualitative value to the provider's behavior. A formal judgment involves evaluating data against an established standard to declare something right or wrong, good or bad. Saying the provider does not know is an unverified deduction rather than a qualitative critique.
D. This option is incorrect because the nurse's conclusion is structured as an assumed statement of reality rather than a personal preference. An individual opinion reflects a deeply held personal belief, taste, or attitude that does not require objective, empirical proof. The nurse is attempting to deduce a factual circumstance rather than expressing a subjective preference.
Test-taking strategy
- Analyze the scenario and question: The question requires classifying the specific type of cognitive statement made by a nurse who assumes a provider is unaware of a client's diarrhea due to a bulk laxative order.
- Apply cognitive and critical thinking frameworks: Differentiate between facts, inferences, judgments, and opinions within clinical reasoning models.
- Identify that the nurse observes a situation and immediately creates a logical bridge to an unverified conclusion.
- Recognize that drawing a conclusion from an observation without factual confirmation matches the definition of making an inference, validating Choice B.
- Rule out distortions and alternative definitions: Evaluate the remaining choices based on their strict semantic definitions in critical thinking.
- Rule out Fact (Choice 1) because the statement is factually unsupported and clinically incorrect regarding bulk laxative pharmacology.
- Rule out Judgment (Choice 3) and Opinion (Choice 4) because the statement is a deduction of a situational circumstance rather than a moral evaluation or personal preference.
Take home points
- An inference is an unverified conclusion drawn from an observation that requires systematic validation before taking clinical action.
- Bulk-forming laxatives can absorb excess intestinal water to solidify stool, making them a valid treatment option for certain types of diarrhea.
- Making unverified clinical inferences without checking rationales introduces significant cognitive bias and compromises collaborative healthcare.
- Critical thinkers must actively separate objective facts from subjective deductions to ensure accurate clinical reasoning and safe care.
The client who is short of breath benefits from the head of the bed being elevated. Because this position can result in skin breakdown in the sacral area, the nurse decides to study the amount of sacral pressure occurring in other positions. What decision making is the nurse engaging in?
Explanation
The nursing process and modern clinical practice heavily rely on evidence-based problem-solving frameworks to minimize patient complications. The research method represents a rigorous, disciplined, and systematic study designed to generate or validate empirical knowledge that refines healthcare protocols. High-Fowler position (elevating the head of the bed 60 to 90 degrees) improves ventilation by lowering the diaphragm, but it creates mechanical shearing forces and concentrated sacral pressure, necessitating formal scientific investigation to optimize skin integrity.
Rationale for correct answer:
A. The nursing activity involves identifying a specific clinical problem, formulating a study topic, and systematically analyzing sacral tissue forces across multiple variables. Engaging in a structured study to gather empirical evidence defines the research method. This disciplined scientific inquiry generates reliable, generalizable data that advances nursing science beyond basic routine protocols.
Rationale for incorrect answers:
B. This option is incorrect because the nurse is designing a structured study rather than randomly applying unverified solutions to a single patient. The trial-and-error method is an undisciplined, unsystematic approach where multiple random interventions are attempted sequentially until one haphazardly works. This unscientific technique carries high risk and lacks empirical control.
C. This option is incorrect because the nurse's decision is driven by objective physiological data and deliberate, structured measurement. Expert intuition involves immediate, non-conscious pattern recognition that occurs without any conscious, step-by-step logical analysis or formal scientific data collection. Designing a structured investigation directly contradicts an intuitive approach.
D. This option is incorrect because the nurse's scope of action extends beyond managing an individual care plan to studying a broader clinical phenomenon. While the nursing process is a systematic framework used to assess, diagnose, plan, implement, and evaluate care for a specific patient, it is not an expansive research study meant to measure generalized physiological data.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the specific type of decision-making method a nurse is using when deciding to systematically study sacral pressure across different positions to solve a broader clinical problem.
- Differentiate problem-solving methods: Evaluate the distinct characteristics of research, trial-and-error, intuition, and the nursing process within clinical practice.
- Identify that the nurse is moving past individual patient care to conduct a structured, comparative analysis of a physical phenomenon.
- Select Choice 1 because initiating a structured study to evaluate variables and gather empirical evidence matches the definition of the research method.
- Eliminate individual or unscientific frameworks: Rule out options that represent unguided interventions, individual clinical loops, or immediate pattern recognition.
- Rule out trial-and-error (Choice 2) and Intuition (Choice 3) because they lack the structured, systematic, and empirical nature of the nurse's intended action.
- Rule out the nursing process (Choice 4) because it is a tool for managing an individual client's daily care cycle rather than conducting a generalized scientific study.
Take home points
- The research method is a systematic, controlled inquiry used to generate generalizable, evidence-based data that refines clinical nursing standards.
- Elevating the head of the bed optimizes respiratory mechanics but dramatically elevates tissue interface pressure and shearing forces over the sacrum.
- The nursing process focuses on the individualized care cycle of a specific patient, whereas nursing research seeks broader, generalizable scientific truths.
- Relying on systematic research over unguided trial-and-error drastically enhances patient safety and protects against hospital-acquired pressure injuries.
The nurse is teaching a client about wound care during a follow up visit in the client’s home. Which critical thinking attitude causes the nurse to reconsider the plan and supports evidence-based practice when the client states, “I just don’t know how I can afford these dressings”?
Explanation
The nursing process requires continuous modification of care plans when socioeconomic barriers threaten therapeutic compliance. Intellectual humility represents a critical thinking attitude where the clinician acknowledges the limitations of their own knowledge and recognizes that their assumptions may not match the client's reality. While evidence-based guidelines dictate specific advanced wound care dressings, an expert nurse must maintain open-mindedness to modify interventions when economic constraints or financial barriers make the prescribed regimen impossible for the client to execute.
Rationale for correct answer:
B. The nursing activity involves recognizing that a pre-planned medical regimen is unfeasible due to the client's socioeconomic reality. Demonstrating intellectual humility allows the nurse to accept that an otherwise perfect care plan must be re-evaluated based on the patient's input. Admitting that the plan fails to address financial barriers is the first step toward finding realistic, cost-effective alternatives.
Rationale for incorrect answers:
A. This option is incorrect because the scenario does not involve a conflict of personal ethics or admitting a lapse in professional standards. Intellectual integrity requires clinicians to hold themselves to the same rigorous standards of proof and behavior that they expect from others. While important for overall practice, it is not the primary attitude driving care plan adaptation due to a patient's financial constraints.
C. This option is incorrect because relying on an unyielding belief in one's initial plan would lead the nurse to dismiss the client's financial concerns. Having confidence in reasoning implies a well-founded trust in one's own critical thinking and instructional abilities. Overconfidence without humility can cause a nurse to push an unaffordable plan, resulting in complete non-compliance.
D. This option is incorrect because the nurse's primary need here is collaboration with the client rather than autonomous separation from the healthcare team. Critical thinking independence involves thinking autonomously and questioning traditional care models rather than blindly following routines. It does not specifically address the internal openness required to modify a care plan based on patient-reported financial barriers.
Test-taking strategy
- Analyze the scenario and question: The question requires identifying the specific critical thinking attitude that enables a home-health nurse to reconsider a wound care plan when a client reveals they cannot afford the required dressings.
- Apply critical thinking attitudes: Evaluate the definitions of standard critical thinking dispositions (integrity, humility, confidence, independence) within nursing models.
- Recognize that the nurse must overcome the assumption that "the current plan is best" and accept the client's reality as a valid reason to change course.
- Select Choice 2 because intellectual humility is the defining trait that allows a professional to admit the limitations of their plan and adjust it to fit the patient's actual life circumstances.
- Eliminate inapplicable dispositions: Rule out choices that focus on moral consistency, self-assurance, or independent reasoning.
- Rule out Choice 1 and Choice 4 because neither integrity nor independence specifically addresses the willingness to yield a planned protocol to a patient's financial limitations.
- Rule out Choice 3 because excessive confidence would lead to ignoring or minimizing the client's stated financial barriers.
Take home points
- Intellectual humility enables nurses to recognize the limitations of their plans and adapt them to match client socioeconomic realities.
- Evidence-based wound care practice must balance optimal physiological dressing requirements with real-world patient financial accessibility.
- When a client states they cannot afford medical supplies, the nurse must immediately pause implementation and reassess alternative care strategies.
- Overlooking economic barriers during discharge or home teaching directly leads to care non-compliance and poor wound healing outcomes.
A nurse enters a client’s room at the beginning of a shift to assess his condition following a blood transfusion. The nurse cared for the client on the previous day as well. The client has several issues he wishes to share with the nurse, who takes time to explore each issue. The nurse also assesses the client and finds no signs or symptoms of a reaction to the blood product. The nurse observed the client the prior day and sees a change in his behavior—a reluctance to get out of bed and ambulate. Which of the following actions improve the nurse’s ability to make clinical decisions about this client? Select all that apply
Explanation
Clinical decision-making in nursing relies heavily on contextual awareness, structural knowledge, and experiential familiarity with the patient. Developing clinical grasp requires intentional observation and continuity of care to detect subtle deviations from baseline physiologic or behavioral status. Expertise development is enhanced when clinicians engage in deep situational assessment rather than superficial task execution. Understanding a patient's habitual patterns allows for early identification of functional decline or psychological distress.
Rationale for correct answers:
B. Spending adequate time during a formal assessment allows for deep exploration of patient concerns. This comprehensive approach uncovers qualitative data that structured checklists frequently miss. The nurse detects subtle changes by engaging in active observation. This thoroughness directly enhances the accuracy of subsequent clinical judgments.
D. Caring for the individual on consecutive days establishes essential continuity of care. This structural arrangement allows the clinician to establish a clear baseline of patient function. Deviations from this baseline become immediately apparent during subsequent shifts. Continuity minimizes clinical errors resulting from fragmented patient information.
E. Recognizing the established behavioral baseline regarding physical activity enables rapid identification of new reluctance. A shift from previous compliance to sudden resistance signals an underlying physiological or psychological complication. This pattern recognition guides targeted diagnostic reasoning. The nurse can immediately investigate specific barriers to early ambulation.
Rationale for incorrect answers:
A. Working the identical shift daily does not inherently improve clinical decision-making capabilities. While schedule consistency offers personal routine, it does not guarantee clinical continuity or improved patient insight. The quality of the interaction matters more than the time of day. Clinicians can make excellent decisions across varying shift configurations.
C. Memorizing institutional guidelines provides an abstract framework but does not enhance client-specific clinical insights. Guidelines offer generalized, non-specific recommendations rather than individualized diagnostic data. The clinical problem in this scenario is identifying why this specific patient's behavior changed. Universal protocols cannot substitute for direct, individualized clinical assessment.
Test-taking strategy
- Analyze the scenario and question: The question asks for specific actions that enhance a nurse's capacity to make accurate clinical judgments regarding a patient showing a sudden behavioral change. The core concept tested is clinical decision-making, which relies on continuity, pattern recognition, and comprehensive assessment rather than rigid scheduling or generic protocols.
- Apply concepts of continuity and assessment: Evaluate each choice to determine if it directly provides the nurse with patient-specific data or contextual baseline knowledge.
- Choice 2 increases the depth of data collection during the physical and psychological assessment. Rule in B.
- Choice 4 and Choice 5 provide historical context and baseline behavioral patterns necessary to recognize anomalies. Rule in 4 and E.
- Choice 1 focuses on administrative scheduling rather than patient-centered care or continuity. Rule out A.
- Choice 3 introduces generic institutional rules rather than patient-specific analytical tools. Rule out C.
Take home points
- Continuity of care directly enhances clinical grasp by allowing nurses to establish a reliable behavioral and physiological baseline.
- Thorough assessment techniques provide qualitative insights that standard quantitative vital sign tracking may overlook.
- Pattern recognition involves comparing current patient presentations against known prior behaviors to detect early functional decline.
- Institutional protocols provide standardized frameworks but cannot replace individualized clinical reasoning and direct patient observation.
A nurse is giving a client a medication and notices the dosage. From the nurse’s experience, the dosage is higher than what is normally given. Which of the following steps should the nurse take to ensure a safe outcome for the client? Select all that apply
Explanation
Safe medication administration requires active validation and interprofessional collaboration when a potential error is detected. Clinicians must apply experiential knowledge to question prescriptions that deviate significantly from standard therapeutic ranges, serving as a critical safeguard. Exercising clinical accountability overrides blind protocol compliance, preventing the administration of potentially toxic drug quantities. Gathering immediate subjective verification from the patient regarding chronic dosing regimens stabilizes situational awareness before executing or modifying care.
Rationale for correct answers:
B. Recognizing communication patterns within the medical team and consulting the charge nurse utilizes the established clinical chain of command. This collaborative step allows for peer verification of the suspected pharmacological variance. It introduces an objective clinical perspective to help validate the nurse's initial safety concerns. This action maximizes resource utilization and unit-based collaborative consultation.
C. Holding the medication dose and immediately conferring with the prescribing healthcare provider prevents potential patient injury from an overdose. The nurse is legally and ethically obligated to clarify ambiguous, unusual, or potentially unsafe medical orders before administration. Intercepting a suspected error at the pre-administration stage represents an essential safety baseline. This intervention demonstrates proactive interception and independent injury prevention.
D. Assessing the patient's existing knowledge regarding their routine medication schedule provides valuable historical context. Patients with chronic conditions often possess exact insights into their specific home maintenance doses and individual tolerances. This baseline interview helps determine if the high dose is an intentional titration or an administrative transcription error. This step supports patient-centered verification and baseline history tracking.
Rationale for incorrect answers:
A. Waiting until the end of the shift to verify a suspicious drug order exposes the patient to severe, immediate physiological harm. Medication safety queries must be resolved dynamically in real time before the substance is introduced into the patient's system. Delaying necessary research to prioritize administrative convenience violates core nursing safety duties. This delay represents a hazardous omission and unsafe time management.
E. Administering an unusually high medication dose with the intention of merely monitoring the subsequent reaction is a profound clinical error. Monitoring a patient after administering a suspected overdose does not mitigate the initial negligence if an adverse event occurs. Clinicians must never deliberately expose a patient to known pharmacological hazards to test a physiological response. This choice reflects negligent execution and dangerous malpractice exposure.
Test-taking strategy
- Analyze the scenario/question: The question asks for the immediate, multi-faceted safety steps a clinician must take when encountering a medication prescription that exceeds normal therapeutic dosage ranges based on past clinical experience.
- Apply concepts of risk mitigation and communication: Evaluate each intervention to determine if it proactively prevents patient harm and utilizes appropriate communication networks.
- Choice 3 is the primary safety action; holding the drug and contacting the prescriber stops the error from reaching the patient. Rule in C.
- Choice 2 and Choice 4 are valuable secondary actions that gather expert peer input and verify patient baseline histories to clarify the order. Rule in 2 and D.
- Choice 1 introduces an unacceptable delay that leaves the patient unprotected during the shift. Rule out A.
- Choice 5 involves executing an unsafe action, which directly violates the ethical duty of non-maleficence. Rule out E.
Take home points
- Suspicious or unusually high medication dosages must be held immediately until absolute safety verification is obtained from the prescriber.
- Utilizing the internal chain of command and consulting the charge nurse provides a critical peer-review safety net during dosage disputes.
- Interviewing patients about their established home maintenance doses helps identify transcription errors versus intentional therapeutic titrations.
- Administering an unverified, potentially hazardous medication dose with the plan to monitor for toxic side effects constitutes professional negligence.
Read the client scenario below and then match each numbered and boldfaced nursing activity with the correct step of the nursing process.
Annie seeks your help in the student health clinic because she suspects that her roommate Angela suffered date rape. She is concerned because Angela chose not to report the rape and does not seem to be coping well. (1) After talking with Annie, you learn that although Angela blurted out that she had been raped when she first came home, since then she has refused verbalization about the rape (“I don’t want to think or talk about it”), has stopped attending all college social activities (a marked change in behavior), and seems to be having nightmares. After analyzing the data, you believe that Angela might be experiencing (2) rape-trauma syndrome: silent reaction. Fortunately, Angela trusts Annie and is willing to come to the student health center for help. After a conversation with Angela confirms your suspicions and problem identification, you talk with Angela (3) to develop some treatment goals that you formulate as outcomes and begin to think about the types of nursing interventions most likely to yield the outcomes you both seek. In your initial meeting with Angela, (4) you encourage her expression of feelings and help her to identify personal coping strategies and strengths. You and Angela decide to meet in 1 week (5) to assess her progress toward achieving targeted outcomes. If she is not making progress, you might need to modify the plan of care.
The nursing activity represented as (1) is an example of which step of the nursing process?
Explanation
The nursing process is a systematic, patient-centered scientific method comprising five sequential phases designed to optimize clinical outcomes. Assessment forms the foundational step, requiring structured data collection regarding physiological, psychological, and sociocultural stressors. Objective and subjective parameters are systematically gathered during this baseline phase to establish a comprehensive clinical profile before formulating subsequent diagnostic hypotheses.
Rationale for correct answer:
A. The nursing activity involves systematic data collection regarding Angela's behavior, speech patterns, and sleep disturbances through a secondary reporter. Gathering baseline clinical information is the defining characteristic of the assessing phase of the nursing process. This step is required to identify client problems before any clinical analysis or intervention can occur.
Rationale for incorrect answers:
B. This option represents the diagnosing phase, where the clinician analyzes the gathered clinical database to identify actual or potential health problems. Statement 2 explicitly labels the problem as rape-trauma syndrome, which represents clinical judgment rather than data gathering. Therefore, this does not represent the initial collection of baseline assessment information.
C. This option signifies the evaluating phase, which measures the client's behavioral and physiological responses against pre-established therapeutic outcomes. Statement 5 explicitly denotes reviewing the client's progress after 1 week to determine if care plan modifications are necessary. It is a terminal or continuous loop step, not the primary data-gathering phase.
D. This option embodies the implementing phase, where the clinician executes specific, action-oriented nursing interventions designed to achieve targeted goals. Statement 4 illustrates the actual deployment of therapeutic communication techniques and coping strategy identification during the session. It represents active intervention rather than the baseline diagnostic data collection phase.
E. This option represents the planning phase, which focuses on formulating measurable, client-centered goals and selecting appropriate nursing orders. Statement 3 describes the collaborative formulation of targeted clinical outcomes and behavioral goals with the client. This occurs after a problem is diagnosed but before direct action is implemented.
Test-taking strategy
- Analyze the scenario and question: The question requires the identification of the specific nursing process step represented by the nursing activity labeled as 1 in the text.
- Apply steps of the nursing process: Evaluate the actions performed in the specified text segment using the sequential framework of assessing, diagnosing, planning, implementing, and evaluating.
- Identify that segment 1 involves listening, observing behavior changes, and documenting specific statements like "I don't want to think or talk about it."
- Recognize that these activities constitute the systematic collection of subjective and objective data from primary or secondary sources.
- Differentiate data collection from analysis and action: Rule out options that involve clinical judgment, goal setting, or direct action.
- Rule out Diagnosing (Choice 2) because no problem is being formally analyzed or labeled in segment A.
- Rule out Planning (Choice 5) and Implementing (Choice 4) because no goals are being set and no therapeutic techniques are being actively deployed yet.
- Rule out Evaluating (Choice 3) because there are no pre-established outcomes to measure progress against at this baseline stage.
Take home points
- Assessing is the initial, systematic phase of the nursing process focused on comprehensive data collection from primary and secondary sources.
- Data gathered during the assessment phase must be purely objective and subjective observations, free from premature diagnostic labeling or clinical conclusions.
- The five steps of the nursing process operate in a progressive, dynamic sequence where each phase depends entirely on the accuracy of the preceding step.
- Secondary informants, such as roommates or family members, provide valid assessment data when the primary client is unable or hesitant to communicate.
Read the client scenario below and then match each numbered and boldfaced nursing activity with the correct step of the nursing process.
Annie seeks your help in the student health clinic because she suspects that her roommate Angela suffered date rape. She is concerned because Angela chose not to report the rape and does not seem to be coping well. (1) After talking with Annie, you learn that although Angela blurted out that she had been raped when she first came home, since then she has refused verbalization about the rape (“I don’t want to think or talk about it”), has stopped attending all college social activities (a marked change in behavior), and seems to be having nightmares. After analyzing the data, you believe that Angela might be experiencing (2) rape-trauma syndrome: silent reaction. Fortunately, Angela trusts Annie and is willing to come to the student health center for help. After a conversation with Angela confirms your suspicions and problem identification, you talk with Angela (3) to develop some treatment goals that you formulate as outcomes and begin to think about the types of nursing interventions most likely to yield the outcomes you both seek. In your initial meeting with Angela, (4) you encourage her expression of feelings and help her to identify personal coping strategies and strengths. You and Angela decide to meet in 1 week (5) to assess her progress toward achieving targeted outcomes. If she is not making progress, you might need to modify the plan of care.
The nursing activity represented as (2) is an example of which step of the nursing process?
Explanation
The nursing process utilizes a progressive clinical framework to identify and manage human responses to actual or potential health problems. Diagnosing represents the secondary phase, where the clinician performs intensive data analysis to identify specific health patterns. During this critical analytical step, clinical data is clustered, validated, and interpreted to formulate a formal diagnostic label that directly directs the subsequent development of targeted patient outcomes.
Rationale for correct answer:
B. The nursing activity involves interpreting clustered assessment data to formulate a specific clinical judgment regarding Angela's condition. Labeling the response as rape-trauma syndrome represents the formal diagnosing step of the nursing process. This analytical conclusion establishes the exact clinical focus needed to guide subsequent care planning and targeted outcome identification.
Rationale for incorrect answers:
A. This option represents the assessing phase, which focuses strictly on the baseline collection of subjective and objective clinical information. Statement 1 illustrates gathering historical details and behavioral observations from a secondary reporter rather than analyzing that data. Therefore, statement 2 represents clinical analysis, which goes beyond simple raw data collection.
C. This option signifies the evaluating phase, which measures the client's behavioral and physiological responses against pre-established therapeutic outcomes. Statement 5 explicitly denotes reviewing the client's progress after 1 week to determine if care plan modifications are necessary. It is a terminal or continuous loop step, not the secondary diagnostic phase.
D. This option embodies the implementing phase, where the clinician executes specific, action-oriented nursing interventions designed to achieve targeted goals. Statement 4 illustrates the actual deployment of therapeutic communication techniques and coping strategy identification during the session. It represents active intervention rather than the clinical interpretation of clustered baseline data.
E. This option represents the planning phase, which focuses on formulating measurable, client-centered goals and selecting appropriate nursing orders. Statement 3 describes the collaborative formulation of targeted clinical outcomes and behavioral goals with the client. This occurs after a problem is diagnosed but before direct action is implemented.
Test-taking strategy
- Analyze the scenario and question: The question requires the identification of the specific nursing process step represented by the nursing activity labeled as 2 in the text.
- Apply steps of the nursing process: Evaluate the actions performed in the specified text segment using the sequential framework of assessing, diagnosing, planning, implementing, and evaluating.
- Identify that segment 2 involves analyzing clustered clinical data to formulate a standard problem statement.
- Recognize that naming a specific human response like rape-trauma syndrome constitutes the formal diagnostic phase of clinical reasoning.
- Differentiate diagnosis from data collection and intervention: Rule out options that involve raw data gathering, planning, or direct therapeutic action.
- Rule out Assessing (Choice 1) because the clinician has moved past gathering observations to interpreting the meaning of those accumulated findings.
- Rule out Planning (Choice 5) and Implementing (Choice 4) because labeling the problem must precede setting goals or performing therapeutic nursing actions.
- Rule out Evaluating (Choice 3) because no care plan has been executed yet to measure outcomes against.
Take home points
- Diagnosing involves analyzing clustered assessment findings to identify a clear clinical label for a client's response to stressors.
- Nanda International taxomony terms like rape-trauma syndrome provide standardized professional communication to direct specific, evidence-based nursing interventions.
- The diagnostic phase requires clinical reasoning to differentiate between distinct pathological states based on defining characteristics and related factors.
- An accurate diagnosis is dependent on a comprehensive assessment and serves as the absolute foundation for planning client care.
Read the client scenario below and then match each numbered and boldfaced nursing activity with the correct step of the nursing process.
Annie seeks your help in the student health clinic because she suspects that her roommate Angela suffered date rape. She is concerned because Angela chose not to report the rape and does not seem to be coping well. (1) After talking with Annie, you learn that although Angela blurted out that she had been raped when she first came home, since then she has refused verbalization about the rape (“I don’t want to think or talk about it”), has stopped attending all college social activities (a marked change in behavior), and seems to be having nightmares. After analyzing the data, you believe that Angela might be experiencing (2) rape-trauma syndrome: silent reaction. Fortunately, Angela trusts Annie and is willing to come to the student health center for help. After a conversation with Angela confirms your suspicions and problem identification, you talk with Angela (3) to develop some treatment goals that you formulate as outcomes and begin to think about the types of nursing interventions most likely to yield the outcomes you both seek. In your initial meeting with Angela, (4) you encourage her expression of feelings and help her to identify personal coping strategies and strengths. You and Angela decide to meet in 1 week (5) to assess her progress toward achieving targeted outcomes. If she is not making progress, you might need to modify the plan of care.
The nursing activity represented as (3) is an example of which step of the nursing process?
Explanation
The nursing process utilizes a progressive clinical framework to identify and manage human responses to actual or potential health problems. Diagnosing represents the secondary phase, where the clinician performs intensive data analysis to identify specific health patterns. During this critical analytical step, clinical data is clustered, validated, and interpreted to formulate a formal diagnostic label that directly directs the subsequent development of targeted patient outcomes.
Rationale for correct answer:
B. The nursing activity involves interpreting clustered assessment data to formulate a specific clinical judgment regarding Angela's condition. Labeling the response as rape-trauma syndrome represents the formal diagnosing step of the nursing process. This analytical conclusion establishes the exact clinical focus needed to guide subsequent care planning and targeted outcome identification.
Rationale for incorrect answers:
A. This option represents the assessing phase, which focuses strictly on the baseline collection of subjective and objective clinical information. Statement 1 illustrates gathering historical details and behavioral observations from a secondary reporter rather than analyzing that data. Therefore, statement 2 represents clinical analysis, which goes beyond simple raw data collection.
C. This option signifies the evaluating phase, which measures the client's behavioral and physiological responses against pre-established therapeutic outcomes. Statement 5 explicitly denotes reviewing the client's progress after 1 week to determine if care plan modifications are necessary. It is a terminal or continuous loop step, not the secondary diagnostic phase.
D. This option embodies the implementing phase, where the clinician executes specific, action-oriented nursing interventions designed to achieve targeted goals. Statement 4 illustrates the actual deployment of therapeutic communication techniques and coping strategy identification during the session. It represents active intervention rather than the clinical interpretation of clustered baseline data.
E. This option represents the planning phase, which focuses on formulating measurable, client-centered goals and selecting appropriate nursing orders. Statement 3 describes the collaborative formulation of targeted clinical outcomes and behavioral goals with the client. This occurs after a problem is diagnosed but before direct action is implemented.
Test-taking strategy
- Analyze the scenario and question: The question requires the identification of the specific nursing process step represented by the nursing activity labeled as 2 in the text.
- Apply steps of the nursing process: Evaluate the actions performed in the specified text segment using the sequential framework of assessing, diagnosing, planning, implementing, and evaluating.
- Identify that segment 2 involves analyzing clustered clinical data to formulate a standard problem statement.
- Recognize that naming a specific human response like rape-trauma syndrome constitutes the formal diagnostic phase of clinical reasoning.
- Differentiate diagnosis from data collection and intervention: Rule out options that involve raw data gathering, planning, or direct therapeutic action.
- Rule out Assessing (Choice 1) because the clinician has moved past gathering observations to interpreting the meaning of those accumulated findings.
- Rule out Planning (Choice 5) and Implementing (Choice 4) because labeling the problem must precede setting goals or performing therapeutic nursing actions.
- Rule out Evaluating (Choice 3) because no care plan has been executed yet to measure outcomes against.
Take home points
- Diagnosing involves analyzing clustered assessment findings to identify a clear clinical label for a client's response to stressors.
- Nanda International taxomony terms like rape-trauma syndrome provide standardized professional communication to direct specific, evidence-based nursing interventions.
- The diagnostic phase requires clinical reasoning to differentiate between distinct pathological states based on defining characteristics and related factors.
- An accurate diagnosis is dependent on a comprehensive assessment and serves as the absolute foundation for planning client care.
Read the client scenario below and then match each numbered and boldfaced nursing activity with the correct step of the nursing process.
Annie seeks your help in the student health clinic because she suspects that her roommate Angela suffered date rape. She is concerned because Angela chose not to report the rape and does not seem to be coping well. (1) After talking with Annie, you learn that although Angela blurted out that she had been raped when she first came home, since then she has refused verbalization about the rape (“I don’t want to think or talk about it”), has stopped attending all college social activities (a marked change in behavior), and seems to be having nightmares. After analyzing the data, you believe that Angela might be experiencing (2) rape-trauma syndrome: silent reaction. Fortunately, Angela trusts Annie and is willing to come to the student health center for help. After a conversation with Angela confirms your suspicions and problem identification, you talk with Angela (3) to develop some treatment goals that you formulate as outcomes and begin to think about the types of nursing interventions most likely to yield the outcomes you both seek. In your initial meeting with Angela, (4) you encourage her expression of feelings and help her to identify personal coping strategies and strengths. You and Angela decide to meet in 1 week (5) to assess her progress toward achieving targeted outcomes. If she is not making progress, you might need to modify the plan of care.
The nursing activity represented as (4) is an example of which step of the nursing process?
Explanation
The nursing process operates as an action-oriented framework to deliver targeted clinical care that addresses identified human responses. Implementing constitutes the quaternary phase, focusing on the actual execution of interventions designed to achieve desired outcomes. During this dynamic stage, the clinician performs specific therapeutic actions, deploys psychological support mechanisms, and facilitates active coping strategies to directly assist the client in meeting established behavioral benchmarks.
Rationale for correct answer:
D. The nursing activity involves actively encouraging the expression of feelings and directly helping Angela identify her personal coping strategies and strengths. Performing therapeutic actions to address an identified problem defines the implementing phase of the nursing process. This step translates the theoretical care plan into direct clinical action to promote patient healing.
Rationale for incorrect answers:
A. This option represents the assessing phase, which focuses strictly on the baseline collection of subjective and objective clinical information. Statement 1 illustrates gathering historical details and behavioral observations from a secondary reporter rather than executing therapeutic actions. Therefore, statement 4 represents an active intervention phase, which occurs well after baseline data accumulation.
B. This option represents the diagnosing phase, where the clinician analyzes the gathered clinical database to identify actual or potential health problems. Statement 2 explicitly labels the problem as rape-trauma syndrome, which represents clinical judgment and problem identification. Therefore, statement 4 represents a subsequent action phase that builds upon that diagnosis.
C. This option signifies the evaluating phase, which measures the client's behavioral and physiological responses against pre-established therapeutic outcomes. Statement 5 explicitly denotes reviewing the client's progress after 1 week to determine if care plan modifications are necessary. It is a terminal or continuous loop step, not the active intervention phase.
E. This option represents the planning phase, which focuses on formulating measurable, client-centered goals and selecting appropriate nursing orders. Statement 3 describes the collaborative formulation of targeted clinical outcomes and behavioral goals with the client. This occurs before direct therapeutic action is implemented during the clinical session.
Test-taking strategy
- Analyze the scenario and question: The question requires the identification of the specific nursing process step represented by the nursing activity labeled as 4 in the text.
- Apply steps of the nursing process: Evaluate the actions performed in the specified text segment using the sequential framework of assessing, diagnosing, planning, implementing, and evaluating.
- Identify that segment 4 involves actively encouraging verbalization and guiding the client to discover personal internal coping mechanisms.
- Recognize that executing specific therapeutic techniques and nursing care behaviors constitutes the implementing phase of the framework.
- Differentiate action from goal formulation and outcome assessment: Rule out options that involve problem identification, goal setting, or subsequent progress monitoring.
- Rule out Diagnosing (Choice 2) because the problem statement has already been formulated and labeled in a previous phase.
- Rule out Planning (Choice 5) because the clinician has progressed past simply designing strategies to actually executing them during the encounter.
- Rule out Evaluating (Choice 3) because the clinician is actively delivering care rather than measuring long-term progress against a baseline.
Take home points
- Implementing is the action-focused phase where the established nursing care plan is directly put into clinical practice.
- Nursing interventions must be continuous with the assessment data and directly aligned with the pre-formulated client outcomes.
- Therapeutic communication and fostering client coping strengths represent autonomous nursing interventions critical for psychological trauma recovery.
- Independent reassessment must occur continuously during the implementation phase to ensure client safety and tolerability of interventions.
Read the client scenario below and then match each numbered and boldfaced nursing activity with the correct step of the nursing process.
Annie seeks your help in the student health clinic because she suspects that her roommate Angela suffered date rape. She is concerned because Angela chose not to report the rape and does not seem to be coping well. (1) After talking with Annie, you learn that although Angela blurted out that she had been raped when she first came home, since then she has refused verbalization about the rape (“I don’t want to think or talk about it”), has stopped attending all college social activities (a marked change in behavior), and seems to be having nightmares. After analyzing the data, you believe that Angela might be experiencing (2) rape-trauma syndrome: silent reaction. Fortunately, Angela trusts Annie and is willing to come to the student health center for help. After a conversation with Angela confirms your suspicions and problem identification, you talk with Angela (3) to develop some treatment goals that you formulate as outcomes and begin to think about the types of nursing interventions most likely to yield the outcomes you both seek. In your initial meeting with Angela, (4) you encourage her expression of feelings and help her to identify personal coping strategies and strengths. You and Angela decide to meet in 1 week (5) to assess her progress toward achieving targeted outcomes. If she is not making progress, you might need to modify the plan of care.
The nursing activity represented as (5) is an example of which step of the nursing process?
Explanation
The nursing process relies on a continuous feedback loop to ensure the delivery of safe, effective, and responsive clinical care. Evaluating represents the final or cyclical phase, focusing on the structured appraisal of outcomes to determine therapeutic efficacy. During this critical analytical step, the clinician measures the client's behavioral and physiological responses against pre-established criteria to determine whether to terminate, continue, or modify the plan of care.
Rationale for correct answer:
C. The nursing activity involves scheduling a specific future session to measure Angela's clinical progress against her pre-established goals. Planning to systematically review goal achievement defines the core function of the evaluating phase of the nursing process. This step closes the feedback loop and dictates whether the care plan must be modified due to insufficient progress.
Rationale for incorrect answers:
A. This option represents the assessing phase, which focuses strictly on the initial baseline collection of subjective and objective clinical information. Statement 1 illustrates gathering historical details and behavioral observations from a secondary reporter rather than measuring goal achievement. Therefore, statement 5 represents a subsequent appraisal step rather than raw data collection.
B. This option represents the diagnosing phase, where the clinician analyzes the gathered clinical database to identify actual or potential health problems. Statement 2 explicitly labels the problem as rape-trauma syndrome, which represents clinical judgment and problem identification. Therefore, statement 5 represents a terminal evaluation step rather than initial diagnostic labeling.
D. This option embodies the implementing phase, where the clinician executes specific, action-oriented nursing interventions designed to achieve targeted goals. Statement 4 illustrates the actual deployment of therapeutic communication techniques and coping strategy identification during the session. It represents active intervention rather than the subsequent measurement of its overall effectiveness.
E. This option represents the planning phase, which focuses on formulating measurable, client-centered goals and selecting appropriate nursing orders. Statement 3 describes the collaborative formulation of targeted clinical outcomes and behavioral goals with the client. While planning sets up the benchmarks, statement 5 represents the distinct process of scheduled outcome measurement.
Test-taking strategy
- Analyze the scenario and question: The question requires the identification of the specific nursing process step represented by the nursing activity labeled as 5 in the text.
- Apply steps of the nursing process: Evaluate the actions performed in the specified text segment using the sequential framework of assessing, diagnosing, planning, implementing, and evaluating.
- Identify that segment 5 involves meeting in 1 week specifically to assess progress toward targeted outcomes and modify care if needed.
- Recognize that measuring actual behavioral responses against pre-established goals constitutes the evaluating phase of the framework.
- Differentiate evaluation from data collection and active intervention: Rule out options that involve baseline data gathering, diagnostic analysis, or active therapeutic execution.
- Rule out Assessing (Choice 1) because the subsequent data gathering is specifically structured to measure established goal achievement rather than baseline state.
- Rule out Diagnosing (Choice 2) and Planning (Choice 5) because the clinical problem has already been labeled and the benchmarks have been established.
- Rule out Implementing (Choice 4) because scheduling a review session is an act of appraisal rather than the direct execution of a therapeutic coping intervention.
Take home points
- Evaluating is the systematic process of comparing the client's current health status against pre-established, measurable behavioral outcomes.
- The evaluation phase directly dictates whether a nursing care plan should be successfully terminated, maintained, or fundamentally modified.
- Continuous evaluation ensures clinical safety by rapidly identifying non-responsive client patterns and ineffective nursing interventions.
- Client-centered outcomes must be written in measurable terms during the planning phase to allow for objective evaluation during follow-up.
Exams on Critical thinking, decision making, and the nursing process
Custom Exams
Login to Create a Quiz
Click here to loginLessons
- Objectives
- Introduction
- Purpose of Critical Thinking
- Techniques in Critical Thinking
- Practice Exercise 1
- Applying Critical Thinking to Nursing Practice
- Components of Clinical Reasoning
- Practice Exercise 2
- Integration of Critical Thinking and Clinical Reasoning
- Concept Mapping
- Practice Exercise 3
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
To:
- Describe the significance of developing critical thinking abilities in order to practice safe, effective, and professional nursing care.
- Describe the actions of clinical reasoning in the implementation of the nursing process.
- Discuss the attitudes and skills needed to develop critical thinking and clinical reasoning.
- Describe the components of clinical reasoning.
- Integrate strategies to enhance critical thinking and clinical reasoning as the provider of nursing care.
- Describe the process of concept mapping to enhance critical thinking and clinical reasoning for the provision of nursing care.
Introduction
Critical thinking is the process of intentional higher-level thinking to define a client’s problem, examine the evidence-based practice in caring for the client, and make choices in the delivery of care.
Clinical reasoning is the cognitive process that uses thinking strategies to gather and analyze client information, evaluate the relevance of the information, and decide on possible nursing actions to improve the client’s physiological and psychosocial outcomes.
Clinical reasoning requires the integration of critical thinking in the identification of the most appropriate interventions that will improve the client’s condition.
The nursing process is described by the American Nurses Association (ANA) as the framework nurses use to apply critical thinking in nursing practice for making clinical decisions. The ANA describes the process as including six steps: assessment, diagnosis, outcome identification, planning, implementation, and evaluation.

Six cognitive skills interact, enabling nurses to apply the nursing process in clinical decision making. The six cognitive skills are: recognize cues, analyze cues, prioritize problems/diagnoses, generate solutions, take actions, and evaluate outcomes.
Purpose of Critical Thinking
Critical thinking involves the differentiation of statements of fact, judgment, and opinion. The process of critical thinking requires the nurse to think creatively, use reflection, and engage in analytical thinking.
Alfaro-LeFevre’s 4-circle critical thinking model provides a visual representation of critical thinking abilities and promotes making meaningful connections between nursing research and critical thinking and practice.
In 2000, Scheffer and Rubenfeld conducted a landmark study in which internationally diverse expert nurses from nine countries defined ten habits of the mind (affective components) and seven skills (cognitive components) of critical thinking in nursing.
The ten affective components are:
- Confidence
- Contextual perspective
- Creativity
- Flexibility
- Inquisitiveness
- Intellectual integrity
- Intuition
- Open-mindedness
- Perseverance
- Reflection
The seven skills are:
- Analyzing
- Applying standards
- Discriminating
- Information seeking
- Logical reasoning
- Predicting
- Transforming knowledge
Nurses use critical thinking skills in a variety of ways:
- Nurses use knowledge from other subjects and fields in order to provide holistic nursing care.
- Nurses deal with change in stressful environments - Critical thinking enables the nurse to recognize important cues, respond quickly, and adapt interventions to meet specific client needs at the right time.
- Nurses make important decisions - use critical thinking skills and clinical reasoning to make judgments about a client’s care.
- Generate many ideas rapidly.
- Be generally flexible and natural; that is, able to change viewpoints or directions in thinking rapidly and easily.
- Create original solutions to problems.
- Be independent and self-confident, even when under pressure.
- Demonstrate individuality.
Creativity is thinking that results in the development of new ideas and products. Creativity in problem solving and decision making is the ability to develop and implement new and better solutions for health care outcomes.
Creativity is required when the nurse encounters a new situation or a client situation in which traditional interventions are not effective.
Techniques in Critical Thinking
These techniques include critical analysis, inductive and deductive reasoning, making valid inferences, differentiating facts from opinions, evaluating the credibility of information sources, clarifying concepts, and recognizing assumptions.
1. Critical Analysis & Socratic Questioning
- Critical Analysis: The application of a non-sequential set of questions/criteria to a situation or idea to isolate essential information and discard the irrelevant.
- Socratic Questioning: A technique used to dig beneath the surface, examine assumptions, spot inconsistencies, and differentiate true knowledge from mere belief.
- Nursing Application: Use when reporting client status, reviewing charts/progress notes, and planning care.
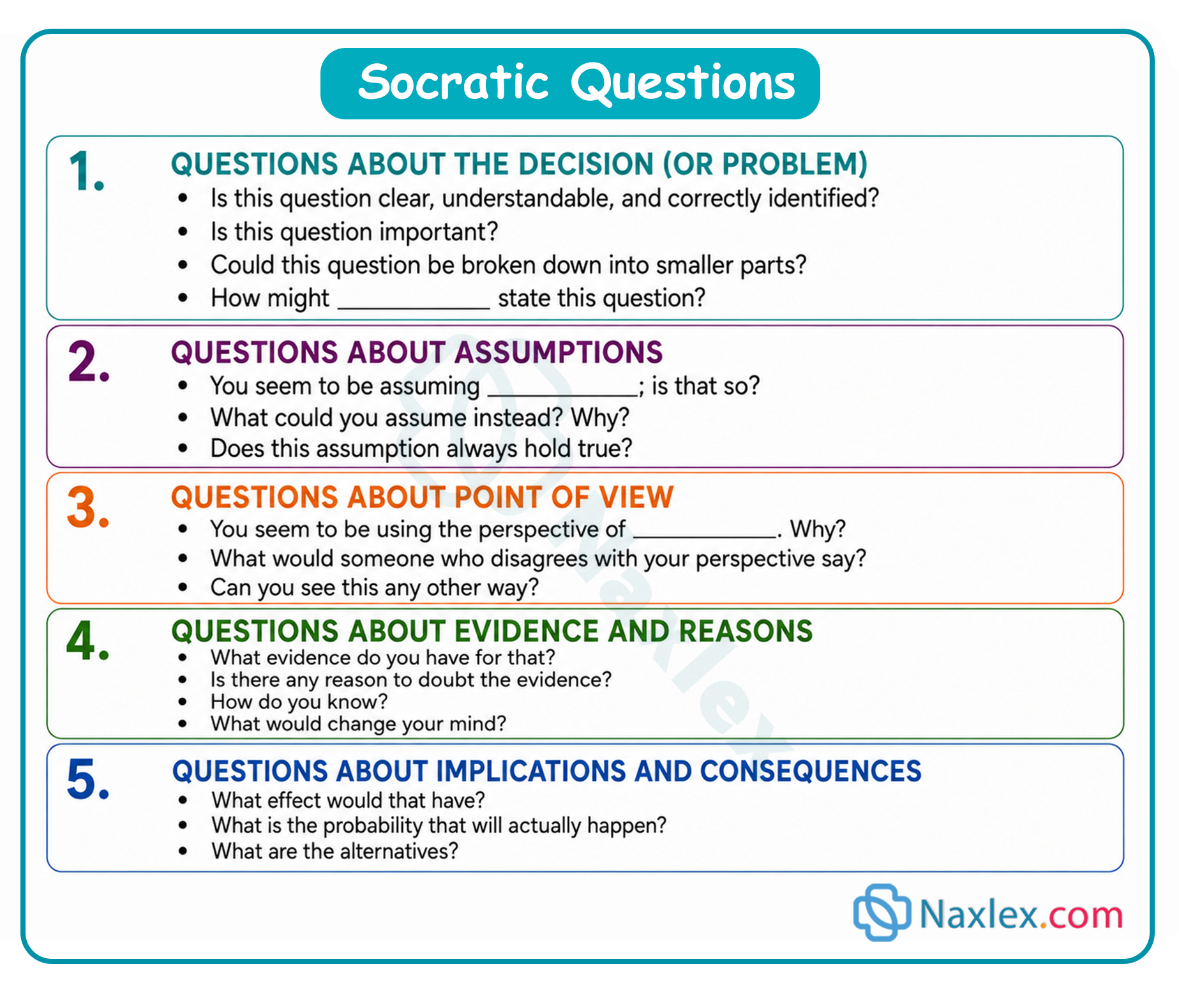
2. Reasoning modes: Inductive vs. Deductive
|
Type |
Direction |
Example |
Risk |
|
Inductive |
Specific 🡪 General (Forming a generalization from specific facts/observations) |
Observing dry skin, poor turgor, and dark urine in a patient, and concluding these signs indicate dehydration in general. |
Overgeneralizing from limited observations. |
|
Deductive |
General 🡪 Specific (Applying a general premise to a specific conclusion) |
Starting with the premise that "all children love peanut butter" and offering one to a child who refuses to eat. |
If the initial premise is false or invalid, the final conclusion will be false. |
Core nursing role: Nurses must use critical thinking to continuously verify that their starting premises are actually valid.
Deductive reasoning moves from the general to the specific. A nurse will start analysis of the facts and observations from a conceptual viewpoint, such as prioritization of needs according to Nola Pender’s health promotion model. After collecting data based on the conceptual view, the nurse forms an inference and eventually interprets the patient’s condition with respect to that conceptual view.
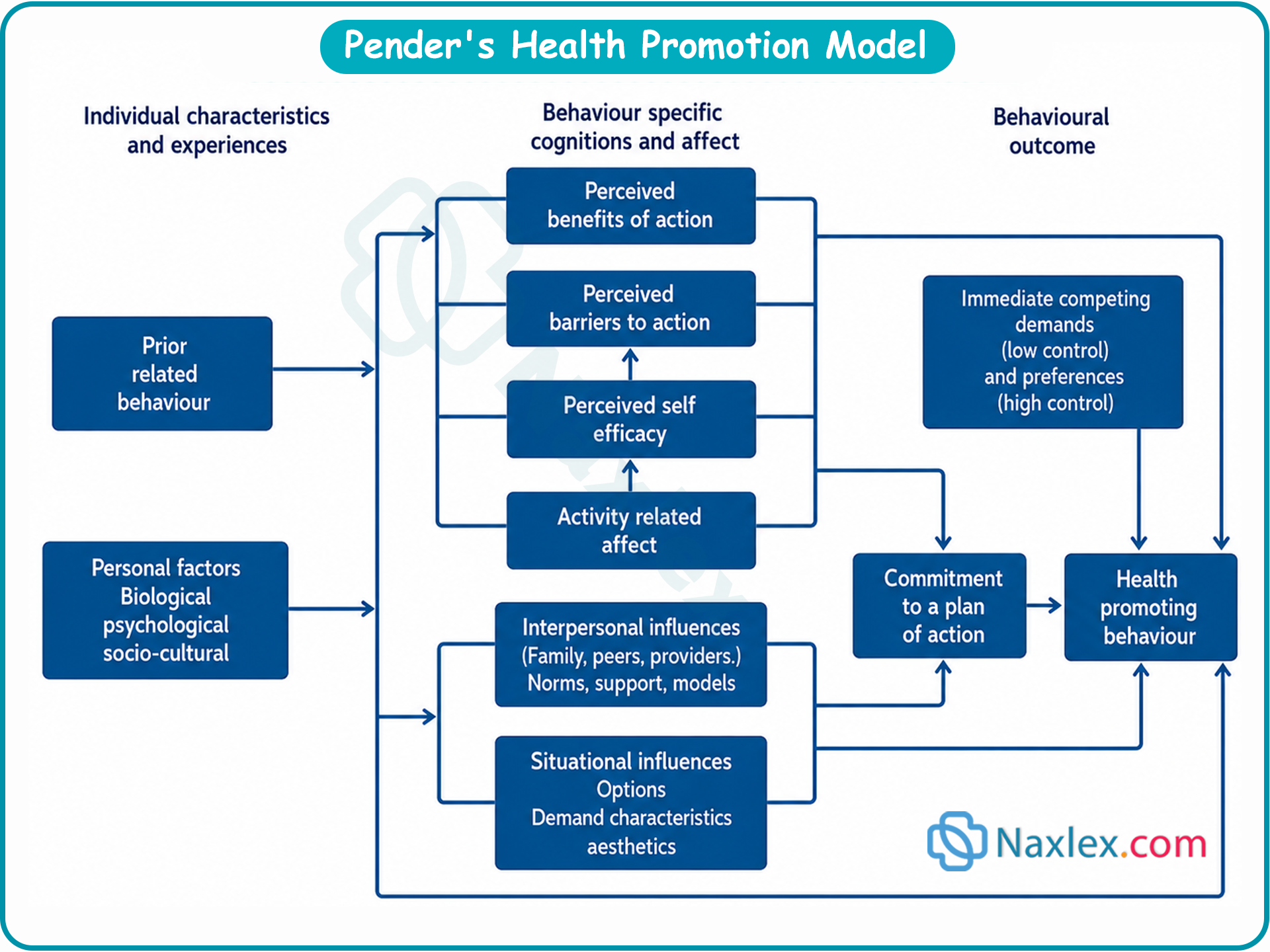
3. Differentiating types of statements
To accurately analyze data, a nurse must categorize information into four distinct types of statements:
- Facts: Information that can be verified through objective investigation.
- Inferences: Conclusions drawn from facts; going beyond what is immediately known to make a logical leap.
- Judgments: Evaluations of facts or information that reflect specific values or criteria (a subset of opinion).
- Opinions: Beliefs formed over time that may either align perfectly with facts or be completely erroneous.
4. Source credibility & Evidence-based practice
- Information evaluation: Nurses cannot accept all documentation or verbal reports at face value.
- Verification: Accuracy must be cross-checked with other documents or informants. This critical verification process drives the expanding need for evidence-based nursing practice.
5. Clarifying concepts & recognizing assumptions
- Concept clarification: The nurse and client must agree on the definition of terms to prevent critical misunderstandings.
- Example: Clarifying if a patient's use of the word "tumor" means a generic solid mass (medical definition) or cancer (lay definition).
- Recognizing assumptions: Underlying beliefs dictate how both nurses and clients view the world (e.g., valuing quality of life vs. quantity of life).
- Takeaway: Problems arise when individuals fail to identify the assumptions underlying their actions. Recognizing these divergent assumptions allows the nurse and client to collaborate on an acceptable plan of care.
Applying Critical Thinking to Nursing Practice
When a nurse uses intentional thinking, a dynamic relationship forms between:
- Critical thinking & clinical reasoning (Knowledge, skills, and attitudes).
- The nursing process (A systematic, rational, and creative 5-phase method to assess, diagnose, plan, implement, and evaluate individualized client care).
- The problem-solving process (A mental activity aimed at identifying an unsteady state and finding solutions to return the client to a steady state).
Approaches to Problem Solving
The nurse evaluates possible solutions, implements the best one, and holds alternatives in reserve. Three common approaches include:
1. Trial and Error
- Definition: Trying multiple approaches until a solution is found, without systematic consideration of alternatives.
- Clinical Warning: Can be dangerous in hospital settings because the client might suffer harm from inappropriate actions.
- Contextual Exception: Frequently used in home settings due to logistical or lifestyle constraints (e.g., using a bent coat hanger on a shower rod for colostomy irrigation when an IV pole isn't available).
2. Intuition
- Definition: Understanding or learning things without the conscious use of reasoning; also called a "sixth sense," hunch, or instinct.
- Mechanism: Derived from deep knowledge and clinical experience, allowing seasoned nurses to quickly recognize cues, notice patterns, and act rapidly on limited evidence.
- User Restriction: Not recommended for novices or students, as they lack the foundational knowledge base and clinical experience required to make valid intuitive judgments.
3. Research Process
- Definition: A formalized, logical, and systematic approach to gathering evidence.
- Application: While strict quantitative research requires controlled environments, nurses use a modified approach to identify evidence-based data that supports effective nursing care in complex, uncontrolled human environments.
Attitudes fostering critical thinking
Critical thinkers assume that rational people are motivated to learn and grow. They actively cultivate these nine essential traits:
|
Attitude |
Definition |
Clinical Example |
|
Independence |
Thinking for oneself; examining beliefs in the light of new evidence rather than just following instructions. |
Being open-minded about trying different methods to perform a technical skill, not just the single way taught in school. |
|
Fair-Mindedness |
Making impartial judgments; assessing all viewpoints using the same standards without personal or group bias. |
Listening to all family members (young and old) and ensuring a clear, objective rationale exists for whatever action is taken. |
|
Insight into Egocentricity |
Actively examining and identifying one's own personal biases, customs, or social pressures to avoid wrong conclusions. |
Avoiding the assumption that a client shares your exact health motivations, preventing wasted teaching time. |
|
Intellectual Humility |
Having an awareness of the limits of one's own knowledge and willingly admitting what you do not know. |
Recognizing that you cannot assume or predict what an elderly wife can achieve when caring for her post-stroke husband at home. |
|
Intellectual Courage |
Willingness to fairly examine and challenge the status quo, rituals, or deeply held traditions. |
Initiating research on allowing families to witness CPR, proving it can be done safely despite historical opposition. |
|
Integrity |
Applying the same rigorous standards of proof and questioning to your own beliefs as you do to the beliefs of others. |
Reconsidering your belief that wound care always requires sterile technique after reading new data on clean technique outcomes. |
|
Perseverance |
Showing determination to clarify complex issues and find effective solutions despite frustration and confusion. |
Spending months collaborating across departments to slowly build a new hospital day-pass policy instead of giving up. |
|
Confidence |
Trusting that well-reasoned, logical thinking (inductive and deductive) leads to the most trustworthy conclusions. |
Systematically assessing the fairest way to allocate holiday time off (e.g., lottery vs. seniority) rather than rushing to a quick agreement. |
|
Curiosity |
Maintaining a mind filled with questions (Why? What causes that? Could something else work?) to challenge stagnant traditions. |
Questioning which hospital department (nursing, lab, or respiratory) is truly best suited to draw arterial blood samples. |
Components of Clinical Reasoning
Clinical reasoning is the analysis of a clinical situation as it unfolds or develops. It requires the nurse to use cognitive and metacognitive processes.
- Cognitive processes are the thinking processes based on the knowledge of aspects of client care. Cognitive skills are learned through reading and applying health-related literature. Cognitive skills are enhanced through the use of critical thought to understand and apply content the nurse has previously learned.
- Metacognitive processes include reflective thinking and awareness of the skills learned by the nurse in caring for the client. The nurse reflects on the client’s status, and through the use of critical thinking skills determines the most effective plan of care.
Five core components of clinical reasoning
Benner et al. outline specific components that shift a nurse from a task-oriented mindset to an analytical one:
1. Setting priorities
- The reality: The clinical environment is fast-paced. Nurses must constantly decide which assessments, tasks, and requests must be handled first.
- The shift: Novice students often view all tasks as equally important and remain highly task-oriented. Experience teaches them how to filter out irrelevant data and identify what is most critical.
- Flexibility: While preclinical preparation helps students set initial priorities, these priorities must remain dynamic and change immediately if the live client situation shifts.
2. Developing rationales
- The "Why": After identifying urgent needs and choosing interventions, the nurse must transfer their theoretical knowledge to justify the plan of care.
- Purpose: Verbally stating the underlying rationale acts as a safeguard against errors, justifies clinical actions, ensures client safety, and trains the brain to think like an expert.
3. Learning how to act
- Proactive planning: The nurse translates medical and nursing knowledge into action by anticipating potential complications before they happen.
- Result: By knowing what complications are possible given a specific diagnosis, the nurse knows exactly what to look for, recognizes significant cues instantly, and initiates swift rescue interventions to promote safety.
4. Clinical reasoning-in-transition
- Trend tracking: The ability to recognize subtle, creeping changes in a client's condition over time.
- Mechanism: This requires continuous evaluation of ongoing nursing interventions and the tracking/trending of relevant assessment data over a timeline, keeping the client's well-being as the primary anchor.
5. Responding to changes in the client's condition
- Vigilance: Because nurses spend the most time with clients, they bear the responsibility to detect status changes, adjust care plans on the fly, and alert the primary care provider before adverse outcomes occur. This relies heavily on comparing current data against baseline history.
Reflection: The key to success
Reflection is the final, crucial loop in clinical reasoning. It is the act of looking back to assess:
- Was the assessment accurate and timely?
- Were the implemented interventions effective?
- What was the final outcome of care?
- How does this case compare to similar past experiences?
REFLECT:
This model can be used individually or as a process shared with others.
- R—Recall the events. Review the facts about a situation and describe what happened.
- E—Examine your responses. Think about or discuss your thoughts and actions at the time of the situation.
- F—Acknowledge feelings: Identify any feelings you had during the situation.
- L—Learn from the experience: Review and highlight what you learned from the situation—for example, your patient’s responses and your actions.
- E—Explore options: Think about or discuss your options for similar situations in the future.
- C—Create a plan of action: Create a plan for how to act in future similar situations.
- T—Set a time: Set a time by which your plan of action will be completed.
Integration of Critical Thinking and Clinical Reasoning
Clinical reasoning cannot be separated from the cultural, logical, and educational context of the nurse.
Multi-client prioritization
Nurses do not think in a vacuum; they must simultaneously prioritize the competing needs of multiple clients, deciding who needs immediate assistance and who can safely wait.
Environment & context assessment
- Home care decisions: A home health nurse must accurately judge whether a client can be safely managed at home or requires emergency hospitalization. This requires assessing whether the caregiver truly understands and can follow the medical discharge teaching.
- Cultural competence: True critical thought demands looking at the client's cultural and religious practices.
Example: In the Muslim tradition, female relatives typically care for a newborn so the mother can rest. A nurse who fails to assess this and aggressively insists the exhausted mother perform all immediate parenting tasks has failed to apply clinical reasoning to the client's real context.
Evidence-based practice & lifelong learning
- Logical reasoning: Nurses must constantly question whether their current practices align with the newest evidence. They are expected to consult current nursing literature rather than relying blindly on "the way it has always been done."
- The experience factor: Research (Andersson, Klang, & Petersson, 2012) confirms that professional competence and clinical reasoning are directly enhanced by two factors: clinical experience and continuous education/training.
Concept Mapping
Concept mapping is a technique that uses a graphic depiction of nonlinear and linear relationships to represent critical thinking.
Also known as mind mapping, concept maps are context dependent and can be used to develop analytical skills.
Types of Concept Maps
Hierarchical maps: Concept and attributes arranged in a hierarchical pattern and typically constructed in a descending order of importance. Relationships are identified between and among a concept and its attributes.
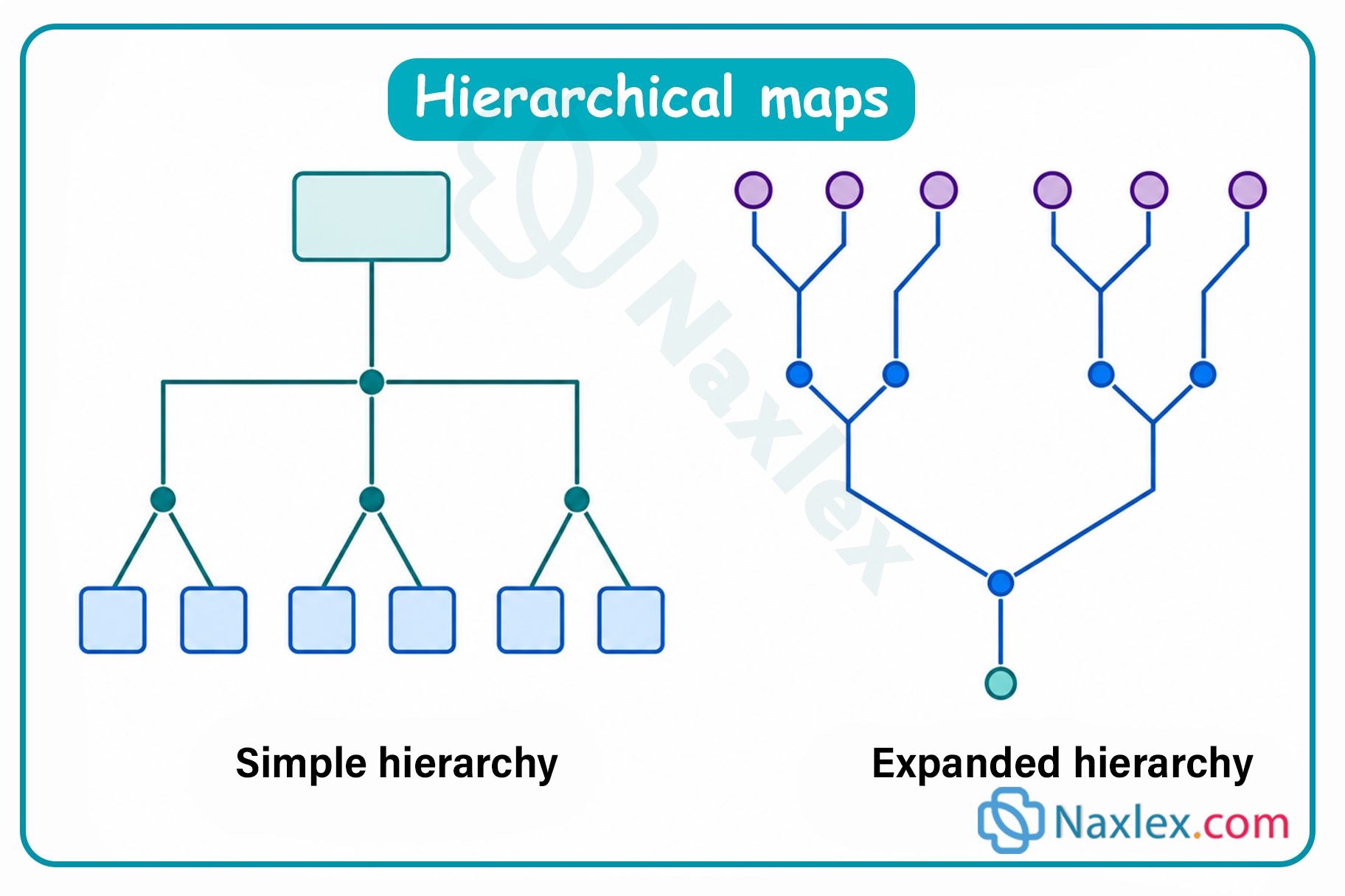
Spider maps - depict the interrelatedness of the concept and its attributes in the map.
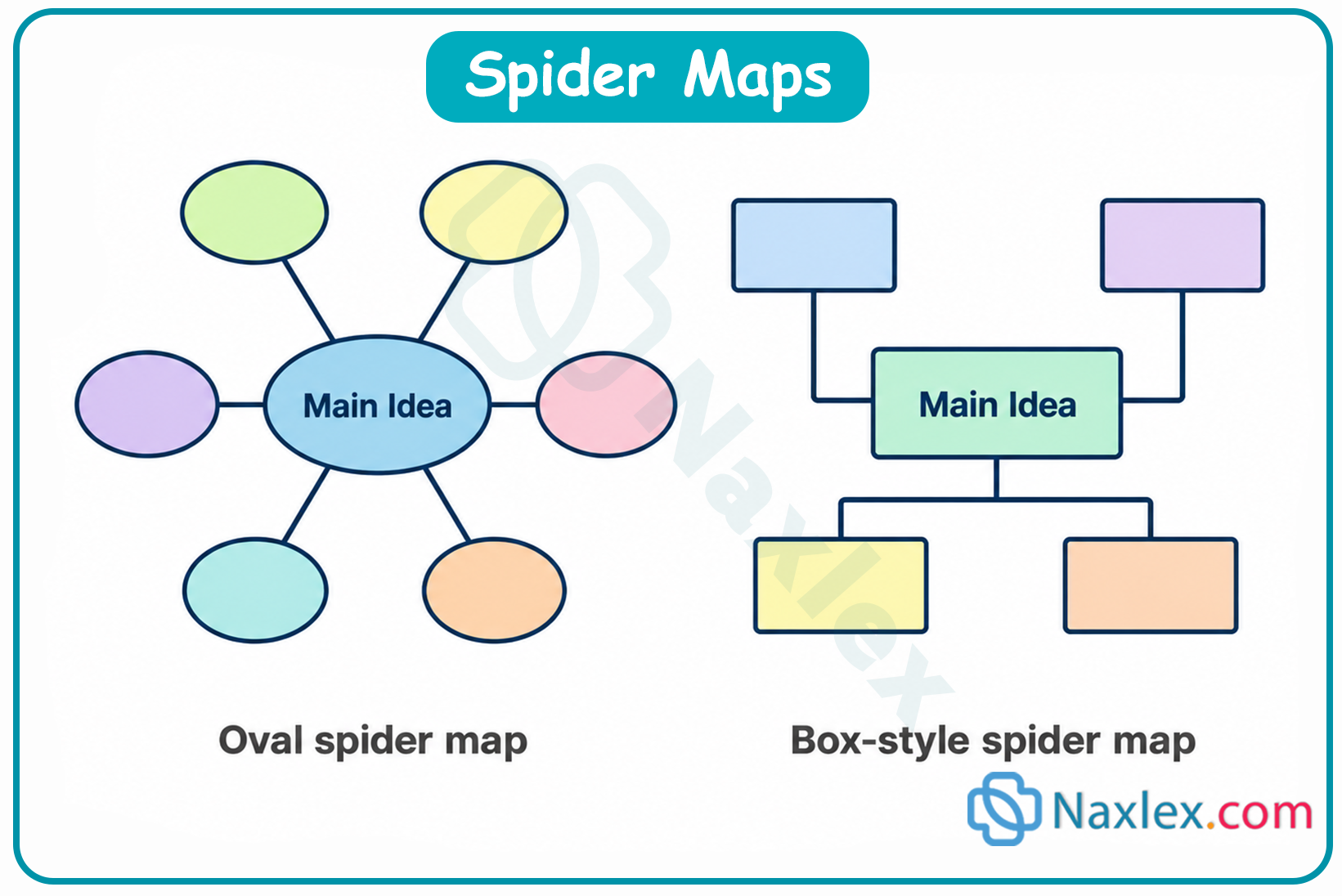
Flowchart maps-linear diagrams demonstrating sequence or cause-and-effect relations.

Systems maps-inputs and outputs illustrate relationships among the concept and its attributes.
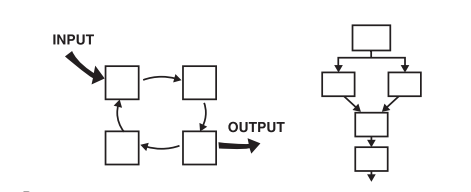
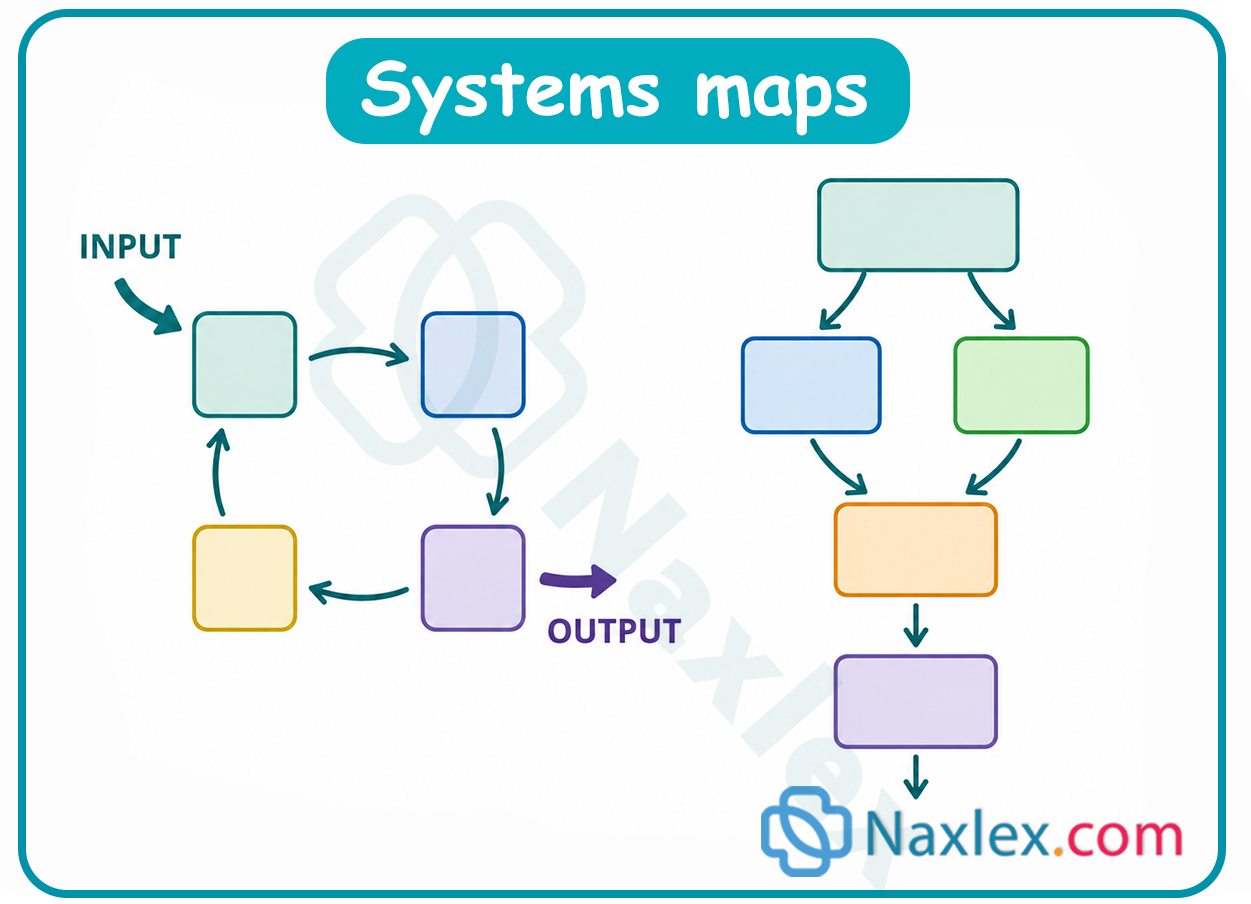
Concept mapping provides nurses with a link between existing nursing knowledge and new information. This learning strategy enhances the critical thinking process and can assist the nursing student in understanding complex concepts.
Rather than address one single client problem, the concept map can incorporate multiple problems. This allows the nurse to demonstrate interrelationships among a client’s problems and determine care based on the complexity of those problems.
Thus, concept mapping may be a valuable tool to improve critical thinking.
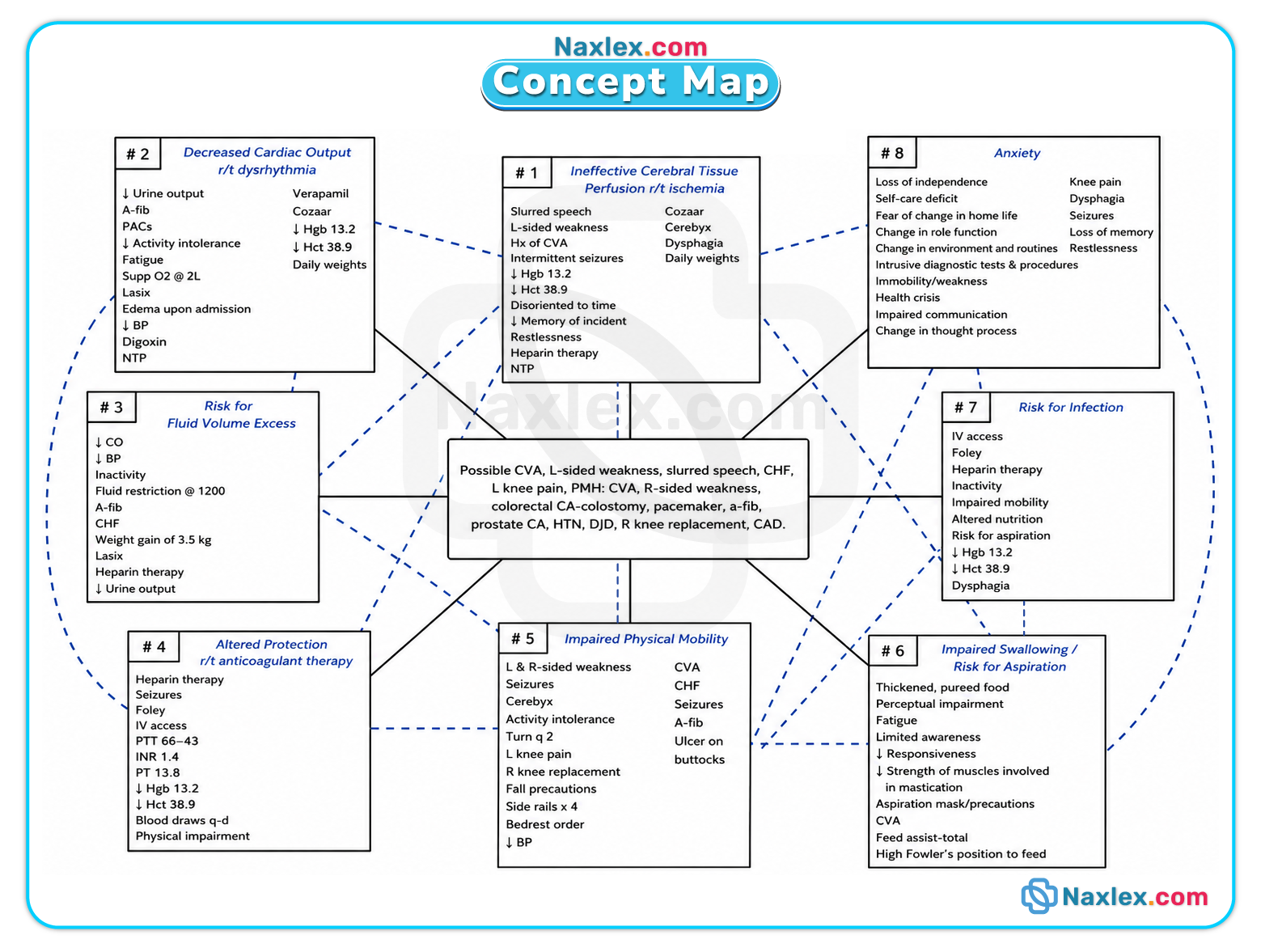
Lifespan considerations in healthcare decisions
1. Children: Developmentally appropriate involvement
While parents typically make the final healthcare decisions for minors, children should be involved in age-appropriate ways. A child's ability to reason critically matures gradually through distinct stages:
Infants
- Cognitive state: Progress from reflexive to simple, repetitive, and imitative behaviors. They are developing concepts of cause-and-effect and object permanence.
- Involvement: Cannot participate in decisions.
- Nursing Focus: Prioritize comforting techniques and establishing a sense of security during care.
Toddlers & Preschoolers
- Cognitive state: Highly egocentric; engage in magical thinking. They cannot rationally understand the long-term implications of healthcare.
- Involvement: Provide simple explanations in words they understand. Offer structured, low-stakes choices to grant them a sense of control.
Example: "Do you want your dressing changed before breakfast or after?"
- Nursing focus: Use play therapy, dolls, and toys to help them visually adjust to and process procedures.
School-age children
- Cognitive State: Concrete thinkers.
- Involvement: Benefit from simple, direct explanations. They can be invited to help the nurse with minor, safe tasks during a procedure.
- Nursing Focus: Allow hands-on exploration of safe equipment. Active involvement reduces their anxiety and increases clinical cooperation.
Adolescents
- Cognitive state: Increasingly capable of abstract thinking.
- Involvement: Capable of making many of their own healthcare decisions.
- Nursing focus: Actively consult them as vital, maturing individuals within the broader family system.
2. Older adults: Preserving autonomy amid cognitive decline
While all adult clients must be included in their care planning, working with older adults experiencing cognitive impairments (e.g., Alzheimer's disease) requires specific modifications to maximize their input.
|
Goal |
Clinical Strategy |
|
Maximize Control |
Allow them as much input and autonomy as possible over their daily care choices. |
|
Accommodate Cognitive Load |
Keep information simple, direct, and focused. Impaired adults often struggle to process multiple tasks or multi-step commands at once. Break instructions down into one step at a time. |
|
Maintain Communication |
Practice patience. Be prepared to calmly repeat instructions in basic terms without sounding patronizing. |
|
Preserve Dignity |
Discuss clinical issues respectfully. Keeping them involved helps maintain self-worth and prolongs their participation in self-care. |
|
Adapt Care Delivery |
If the client becomes completely unable to perform physical self-care (e.g., bathing or dressing changes), the nurse must seek alternative, creative methods to assist them while minimizing distress. |
Summary
- Nurses need critical thinking skills and attitudes to be safe, competent, skillful practitioners.
- Nurses use clinical reasoning skills to assess each client’s condition and identify interventions that improve clients’ physiological and psychosocial outcomes.
- Creativity enhances critical thinking. Creative nurses generate many ideas rapidly, are flexible and natural, create original solutions to problems, tend to be independent and self-confident, and demonstrate individuality.
- Critical thinking skills include the ability to do critical analysis, perform inductive and deductive reasoning, make valid inferences, differentiate facts and opinions, evaluate the credibility of information sources, clarify concepts, and recognize assumptions.
- Critical thinkers have certain attitudes: independence, fair-mindedness, insight, intellectual humility, intellectual courage to challenge the status quo and rituals, integrity, perseverance, confidence, and curiosity.
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Critical thinking, decision making, and the nursing process
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
