
CONGENITAL HEART DISEASES: MIXED DEFECTS
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Classify congenital heart diseases characterized by mixed blood flow, distinguishing them from simple left-to-right shunting mechanisms.
- Describe the anatomical defects and abnormal systemic-pulmonary connections in Transposition of the Great Vessels (TGV), Total Anomalous Pulmonary Venous Connection (TAPVC), Truncus Arteriosus, and Hypoplastic Left Heart Syndrome (HLHS).
- Identify the clinical manifestations of mixed blood defects, highlighting profound cyanosis, rapidly developing congestive heart failure (CHF), and differential oxygen saturations.
- Explain the vital role of transitional fetal structures, specifically the Patent Ductus Arteriosus (PDA) and Foramen Ovale, in maintaining life before surgical intervention.
- Interpret diagnostic findings from echocardiograms, chest X-rays (such as the "egg-on-a-string" or "snowman" signs), and cardiac catheterization.
- Outline urgent medical management (including Prostaglandin E1 infusion) and complex multi-stage surgical corrections.
- Develop a comprehensive nursing care plan for pediatric patients exhibiting critical cyanosis, metabolic stress, and poor perfusion.
- Recognize severe post-operative complications, including pulmonary hypertensive crises, low cardiac output syndrome, and arrhythmias.
Introduction
- Congenital Heart Diseases (CHDs): Mixed Defects represent a highly complex, critical category of cardiac anomalies characterized by the survival-dependent mixing of oxygenated and unoxygenated blood.
- Unlike simple lesions, mixed defects involve a profound anatomical restructuring where the systemic and pulmonary circulations function either as isolated, parallel loops or drain into a single, shared cardiac chamber.
- The defining pathophysiological hallmark of these defects, which include Transposition of the Great Vessels (TGV), Total Anomalous Pulmonary Venous Return (TAPVR), and Truncus Arteriosus, is bidirectional shunting.
- Because oxygen-rich and oxygen-poor blood completely blend within the heart or great vessels, the blood ejected into the systemic circulation is permanently desaturated. This results in progressive tissue hypoxia and profound, visible cyanosis that does not resolve with supplemental oxygen.
- In the neonatal period, these defects constitute a medical emergency. Survival is entirely dependent on the patency of fetal pathways, such as a Patent Ductus Arteriosus (PDA) or Foramen Ovale, which act as the sole channels for cross-mixing.
- As these fetal pathways naturally begin to close hours or days after birth, blood mixing drops catastrophically, triggering severe metabolic acidosis, respiratory distress, and rapid cardiovascular collapse.
- Advanced nursing and medical management center on keeping these vital mixing pathways open. The immediate initiation of a continuous prostaglandin E1 (PGE1) infusion is required to maintain ductal patency.
- Paradoxically, high-flow supplemental oxygen must be tightly restricted; because oxygen is a potent pulmonary vasodilator and ductal constrictor, over-oxygenation can flood the lungs, starve systemic organs, and close the life-sustaining PDA.
- Palliative interventions like a balloon atrial septostomy provide temporary stabilization until definitive, highly complex open-heart surgical correction can be performed.
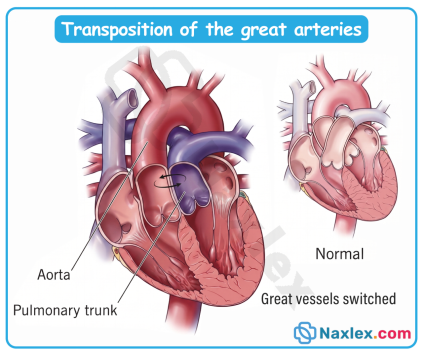
Transposition of the Great Vessels
Transposition of the Great Vessels (TGV) is a cyanotic congenital heart anomaly characterized by a complete reversal of the anatomical positions of the major outflow tracts. The aorta erroneously arises directly from the right ventricle, and the pulmonary artery arises from the left ventricle. This creates two separate, parallel circulatory loops rather than the normal series circuit, preventing oxygenated blood from reaching the systemic circulation unless a mixing shunt coexists.
Epidemiology
- TGV accounts for approximately 5% to 7% of all congenital heart defects.
- It is the most common cyanotic heart defect presenting in the immediate neonatal period.
- There is a distinct male-to-female predilection, with a ratio of approximately 3:1.
- Occurs in roughly 20 to 30 per 100,000 live births.
Etiology
- Genetic factors: Often isolated, but can be associated with specific gene mutations (such as PROSIT24 or GDF1) or chromosomal syndromes, though less frequently linked to Down syndrome than septal defects.
- Environmental factors: Strongly linked to maternal pre-gestational diabetes, maternal obesity, exposure to organic solvents, and advanced maternal age during the first trimester.
- Embryological failure: Results from the abnormal spiraling and partitioning of the truncus arteriosus by the aorticopulmonary septum during the 5th to 8th weeks of fetal development.
Pathophysiology
- Parallel Circulation: Unoxygenated systemic venous return enters the right atrium, passes to the right ventricle, and is pumped directly back out to the body via the transposed aorta. Simultaneously, oxygenated pulmonary venous return enters the left atrium, passes to the left ventricle, and is pumped back into the lungs via the transposed pulmonary artery.
- Survival Dependency: Life is incompatible with birth unless an anatomical communication exists to allow mixing of the two circuits. Mixing typically occurs via a Patent Ductus Arteriosus (PDA), Foramen Ovale/ Atrial Septal Defect (ASD), or Ventricular Septal Defect (VSD).
- Hypoxemia and Tissue Hypoxia: As the PDA begins to close postnatally, systemic oxygen saturation drops precipitously, leading to severe metabolic acidosis and tissue hypoxia.
Clinical Manifestations
Symptoms present immediately at birth or within the first hours of life, depending on the degree of mixing through fetal shunts.
- General: Profound, progressive cyanosis that does not improve with supplemental oxygen administration (unresponsive to hyperoxia challenge). Tachypnea and signs of respiratory distress (grunting, flaring, retractions) emerge as tissue hypoxia worsens.
- Growth/Feeding: Poor feeding performance and rapid fatigue during attempts to suckle.
- Cardiac Auscultation:
- S1: Normal.
- S2: Typically single and loud, because the anteriorly transposed aorta closes closer to the chest wall, obscuring the pulmonic closure sound.
- Murmur: Often completely absent if the interventricular septum is intact. If a VSD or PDA is present, a systolic murmur or continuous murmur may be heard, respectively.
Diagnostic Evaluation
- Echocardiography (ECHO): The gold standard diagnostic tool. It directly visualizes the ventriculoarterial discordance, confirming that the aorta arises from the right ventricle and the pulmonary artery from the left ventricle, while mapping out any concurrent mixing lesions (ASD, VSD, PDA).
- Electrocardiogram (ECG): Usually reveals right axis deviation and right ventricular hypertrophy (RVH) because the right ventricle continues to pump against high systemic vascular resistance.
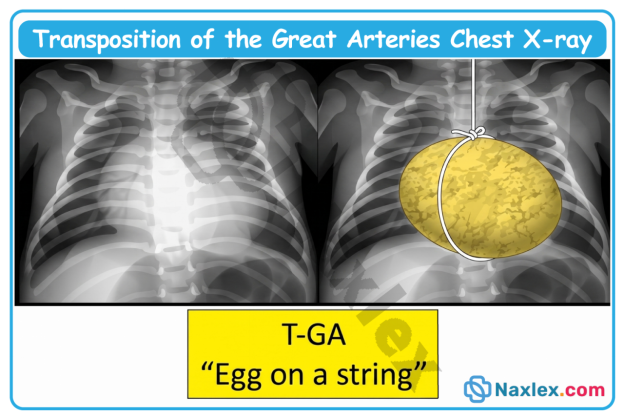
- Chest X-ray (CXR): Characteristically demonstrates cardiomegaly with a narrow mediastinal shadow, classically described as an "egg-on-a-string" appearance, along with increased pulmonary vascular markings.
Image Title: Transposition of the Great Arteries Chest X-ray
- Hyperoxia Test: Administering 100% fraction of inspired oxygen (FiO2) fails to significantly raise the partial pressure of arterial oxygen (PaO2), pointing directly to a right-to-left structural shunt.
Therapeutic Management
A. General & Medical Principles
- Prostaglandin E1 (PGE1) Infusion: Initiated immediately via a secure central or peripheral line. PGE1 prevents the physiological closure of the patent ductus arteriosus, maintaining critical mixing of systemic and pulmonary blood.
- Therapeutic Sub-ambient Oxygen/Minimal Handling: High oxygen concentrations reduce pulmonary vascular resistance and may hasten ductal closure; therefore, oxygen supplementation is kept minimal, targeting oxygen saturations between 75% and 85%.
- Emergency Balloon Atrial Septostomy (Rashkind Procedure): Performed in the cardiac catheterization lab or at the bedside under ECHO guidance if severe hypoxia persists despite PGE1. A balloon catheter is advanced into the right atrium, through the foramen ovale into the left atrium, inflated, and pulled back forcefully to tear the interatrial septum, creating a large ASD for blood mixing.
B. Surgical Management
- Indication: Definitively required for all neonates diagnosed with TGV, typically executed within the first 1 to 2 weeks of life.
- Procedure (Arterial Switch Operation / ASO): The definitive corrective surgery (Jatene procedure). The transposed aorta and pulmonary artery are transected above the valves and switched to their correct anatomical ventricles. Crucially, the coronary arteries must be meticulously excised from the native aorta and replanted into the neoaorta.
Post-Operative Nursing Interventions
Post-Op Day 0 to 1 (ICU Phase)
- Maintain continuous mechanical ventilation and closely analyze arterial blood gases (ABGs) to optimize acid-base balance and oxygenation.
- Monitor hourly chest tube output. Report drainage greater than 3 mL/kg/hr for 3 consecutive hours or greater than 5 mL/kg in any single hour, as this signals acute post-operative hemorrhage.
- Provide continuous ECG monitoring; closely watch for bradyarrhythmias, heart blocks, or ST-segment changes that indicate coronary artery compression or spasm following replantation.
- Maintain a strict fluid balance profile via an indwelling Foley catheter, ensuring a minimum urine output of 1 mL/kg/hr.
- Regularly check central and peripheral perfusion status (ensure capillary refill time remains less than 3 seconds).
Post-Op Day 2 to 3 (Transition Phase)
- Gradually wean from mechanical ventilation and supplemental oxygen as tolerated by the patient.
- Slowly advance nutrition from NPO status to clear liquids or specialized infant formula once bowel sounds return and extubation is successful.
- Implement respiratory therapy support (e.g., gentle chest physiotherapy or tactile stimulation to encourage deep crying) to prevent micro-atelectasis.
- Ensure multimodal pain management utilizing scheduled intravenous acetaminophen or ketorolac with low-dose opioid rescue choices.
Post-Op Day 4 to Discharge
- Regularly inspect the sternotomy surgical incision site for signs of localized infection (warmth, purulent drainage, erythema, or wound dehiscence).
- Assist the infant's caregivers with safe handling and holding techniques during gradual increases in ambient activity.
- Deliver comprehensive discharge and parent education, explicitly instructing caregivers never to lift the infant by their arms or under the armpits for 4 to 6 weeks to prevent structural mechanical stress on the healing sternum.
Nursing Diagnosis (Post-Op)
Post-Op Day 1
- Decreased Cardiac Output related to surgical myocardial ischemia, coronary artery translocation alterations, or arrhythmia development.
- Impaired Gas Exchange related to cardiopulmonary bypass effects, mechanical ventilation dependencies, or ventilation-perfusion mismatching.
- Risk for Fluid Volume Deficit related to chest tube blood loss, surgical hemorrhage, or aggressive post-bypass diuretic management.
Post-Op Day 2 to 3
- Acute Pain related to surgical sternotomy access, chest tube placement irritation, and frequent nursing manipulations.
- Ineffective Airway Clearance related to thick retained respiratory secretions, relative immobility, and post-extubation incisional splinting.
- Risk for Infection related to multiple indwelling lines (central venous lines, arterial lines) and the median sternotomy incision.
Post-Op Day 4+
- Deficient Knowledge (Caregiver) related to specialized infant home care routines, recognition of cardiac decompensation signs, and medication tracking.
- Activity Intolerance related to prolonged surgical recovery, decreased caloric intake during the acute illness, and generic physical weakness.
Complications
- Cardiac: Acute myocardial infarction or ischemia due to coronary artery kinking or stenosis at the surgical reimplantation sites; supraventricular arrhythmias, or neo-aortic root dilation.
- Pulmonary: Pulmonary artery stenosis at the site of the surgical anastomosis.
- Surgical: Postpericardiotomy syndrome, phrenic nerve injury causing diaphragmatic paralysis, or paradoxical systemic emboli.
Prognosis
- Without surgical intervention, the mortality rate is approximately 30% within the first week of life, and exceeds 90% by 1 year of age.
- Following a successful Arterial Switch Operation (ASO), the long-term prognosis is excellent, boasting a survival rate greater than 95% at 20 years.
- Most survivors enjoy a completely normal life span and normal exercise tolerance, requiring only lifelong periodic follow-up with a pediatric cardiologist.
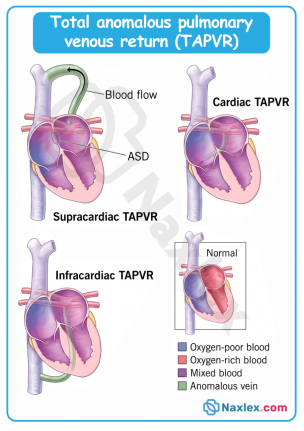
Total Anomalous Pulmonary Venous Connection
Total anomalous pulmonary venous connection (TAPVC) is a critical cyanotic congenital heart defect in which none of the four pulmonary veins connect directly to the left atrium. Instead, all oxygenated pulmonary venous return drains abnormally into the right atrium or systemic venous circulation (such as the superior vena cava, inferior vena cava, or coronary sinus). Survival is strictly dependent on a right-to-left interatrial shunt, typically an atrial septal defect (ASD) or patent foramen ovale (PFO), to deliver oxygenated blood to the left side of the heart and the rest of the body.
Epidemiology
- TAPVC is rare, accounting for approximately 1% to 3% of all congenital heart anomalies.
- The overall incidence is roughly 1 in 10,000 to 15,000 live births.
- Unlike ASD, there is no significant female predilection; however, the infracardiac type shows a distinct male predominance (up to a 4:1 male-to-female ratio).
- Supracardiac TAPVC is the most common anatomical variant, representing roughly 45% to 50% of all presentations.
Etiology
- Genetic factors: Can be isolated or occur in association with heterotaxy syndromes (asplenia or polysplenia), Trisomy 21, or specific genetic mutations altering early cardiac looping.
- Environmental factors: Maternal exposure to specific environmental toxins, metabolic conditions (uncontrolled maternal diabetes), or organic solvent exposure during the early weeks of embryogenesis.
- Embryological failure: Results from an developmental arrest during the first month of gestation. The common pulmonary vein fails to sprout from the posterior wall of the left atrium or prematurely undergoes atresia before connecting to the pulmonary venous plexus, forcing primitive systemic venous channels to persist.
Pathophysiology
- Total Mixing: Because all pulmonary veins dump into the right side of the heart, the right atrium becomes a common mixing chamber for completely deoxygenated systemic venous return and highly oxygenated pulmonary venous return.
- Obligatory Shunt: The mixed blood in the right atrium can only reach the left side of the heart and systemic circulation via a right-to-left shunt across an ASD or PFO.
- Volume Overload: The right atrium and right ventricle must accommodate the entire systemic venous return plus the entire pulmonary venous return, leading to severe right-sided heart volume overload and hypertrophy.
- Obstruction vs. Non-obstruction:
- Non-obstructed TAPVC: Pulmonary blood flow is massive, leading to early congestive heart failure and mild-to-moderate cyanosis.
- Obstructed TAPVC: If the anomalous venous pathway is compressed (classic in Infracardiac types passing through the diaphragm), pulmonary venous pressures skyrocket, causing severe pulmonary edema, profound hypoxemia, and neonatal shock.
Clinical Manifestations
Clinical presentation varies dramatically based on whether pulmonary venous drainage is obstructed.
- General: Profound, early cyanosis and tachypnea in newborns with obstruction. Infants with non-obstructed pathways present with poor feeding, diaphoresis during feeds, and failure to thrive.
- Respiratory: Severe respiratory distress, retractions, and grunting if obstruction is present; frequent lower respiratory tract infections due to pulmonary hypercirculation if non-obstructed.
- Cardiac auscultation:
- S1: Normal or prominent.
- S2: Widely split with a loud, accentuated pulmonic component due to pulmonary hypertension.
- Murmur: Usually a soft, hyperdynamic midsystolic ejection murmur at the upper left sternal border due to increased flow across the pulmonic valve. A mid-diastolic rumble may be noted at the lower left sternal border due to tricuspid overcirculation.
- Quadruple Rhythm: A distinctive 3rd or 4th heart sound can sometimes create a galloping quadruple rhythm in non-obstructed states.
Diagnostic Evaluation
- Echocardiography (ECHO): The definitive gold standard diagnostic tool. It visualizes the common pulmonary venous confluence, tracks the anomalous pathway, determines the direction of the right-to-left shunt across the atrial septum, and evaluates for the presence of venous obstruction.
- Electrocardiogram (ECG): Demonstrates severe right axis deviation, right atrial enlargement (tall, peaked P waves), and right ventricular hypertrophy.
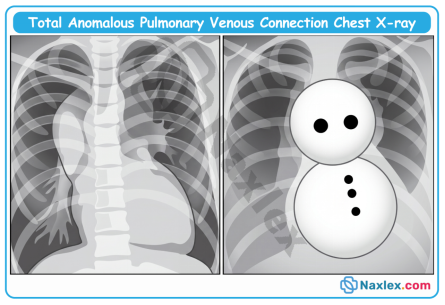
- Chest X-ray (CXR): In non-obstructed older infants, it reveals the classic "snowman" or "figure-of-8" appearance caused by a dilated vertical vein and superior vena cava. In obstructed neonates, it reveals a normal-sized heart with severe, diffuse reticular patterns mimicking respiratory distress syndrome.
Image Title: Total Anomalous Pulmonary Venous Connection Chest X-ray
- Cardiac catheterization: Historically utilized but now largely reserved for emergency transcatheter decompression or when echocardiographic views are inconclusive regarding individual pulmonary vein entries.
Therapeutic Management
A. General Principles
- Stabilization: Obstructed TAPVC is a profound surgical emergency. Intubation, mechanical ventilation, and continuous inotropic support are implemented immediately.
- Prostagladin E1 (PGE1): May be infused to maintain ductal patency, though its therapeutic benefit is variable and depends heavily on the specific anatomical subtype.
- ECMO: Extracorporeal Membrane Oxygenation may be required as a bridge to surgery for infants presenting in extremis with severe pulmonary edema and refractory hypoxia.
B. Surgical Management
- Indication: All cases of TAPVC require definitive surgical repair. Obstructed variants undergo immediate emergent surgery, while non-obstructed forms are scheduled semi-urgently within the first few weeks or months of life.
- Procedure: Completed via open-heart surgery utilizing cardiopulmonary bypass. The common pulmonary venous confluence is anastomosed directly to the posterior wall of the left atrium, the anomalous vertical connecting channels are ligated, and the accompanying ASD or PFO is surgically closed.
Post-Operative Nursing Interventions
Post-Op Day 0 to 1 (ICU Phase):
- Maintain mechanical ventilation and strictly monitor arterial blood gases (ABGs) to manage volatile pulmonary vascular resistance.
- Monitor hourly chest tube output; report drainage greater than 3 mL/kg/hr for 3 consecutive hours or 5 mL/kg in any single hour to catch acute post-operative hemorrhage early.
- Continuously monitor ECG for tachyarrhythmias, junctional ectopic tachycardia (JET), or heart blocks resulting from suture lines near the conduction system.
- Maintain strict fluid balance and intake/output (I&O) tracking; monitor urinary output hourly through a Foley catheter (maintain greater than 1 mL/kg/hr).
- Assess peripheral perfusion, core-to-peripheral temperature gradients, and capillary refill time (normal less than 3 seconds) to ensure adequate cardiac output.
Post-Op Day 2 to 3 (Transition Phase):
- Encourage gradual weaning from mechanical ventilation and transition to supplemental oxygen as tolerated.
- Advance diet slowly from NPO to clear liquids or breast milk as active bowel sounds return and extubation goals are met.
- Utilize age-appropriate chest physiotherapy, gentle repositioning, or bubble blowing to prevent atelectasis and maximize recruitment of functional lung volumes.
- Provide aggressive pain management via scheduled IV multi-modal regimens (e.g., acetaminophen or ketorolac) combined with opioid rescue doses to minimize sympathetic surges.
Post-Op Day 4 to Discharge:
- Inspect the sternotomy incision daily for signs of infection, such as progressive erythema, warmth, or purulent drainage.
- Promote progressive, age-appropriate ambulation and holding to prevent standard post-surgical deconditioning.
- Deliver comprehensive caregiver education on handling restrictions, explicitly reinforcing that the infant must not be lifted by the arms or under the armpits for 4 to 6 weeks to ensure proper sternal healing.
Nursing Diagnosis (Post-Op)
Post-Op Day 1:
- Decreased Cardiac Output related to myocardial stunning, post-operative arrhythmias, or acute alterations in right-to-left fluid volume shifts.
- Impaired Gas Exchange related to cardiopulmonary bypass exposure, mechanical ventilation dependencies, or transient pulmonary venous congestion.
- Risk for Fluid Volume Deficit related to mediastinal bleeding or aggressive post-operative diuretic therapy.
Post-Op Day 2 to 3:
- Acute Pain related to the midline sternotomy site, mediastinal chest tube placement, and required nursing manipulations.
- Ineffective Airway Clearance related to thick retained secretions, transient diaphragm weakness, or splinting due to thoracic pain.
- Risk for Infection related to multiple indwelling central venous lines, arterial monitoring lines, and a healing surgical wound.
Post-Op Day 4+:
- Deficient Knowledge (Caregiver) related to specialized home medication schedules, post-surgical warning signs, and specific activity restrictions.
- Activity Intolerance related to surgical recovery, residual cardiopulmonary imbalances, and prolonged bed rest.
Complications
- Cardiac: Left ventricular dysfunction (due to a chronically underfilled left ventricle suddenly managing total systemic load), atrial flutter/fibrillation, and persistent pulmonary hypertension.
- Pulmonary: Recurrent pulmonary venous obstruction at the surgical anastomosis site, occurring in 5% to 15% of patients and presenting as late-onset respiratory distress.
- Surgical: Postpericardiotomy syndrome, structural phrenic nerve injury resulting in diaphragmatic paralysis, or localized wound infections.
Prognosis
- Surgical repair provides an excellent long-term survival rate exceeding 85% to 90% for uncomplicated, non-obstructed variants.
- Surgical mortality remains higher (up to 10% to 15%) in neonates presenting with severe infracardiac obstruction and preoperative cardiogenic shock.
- If the patient completes the first post-operative year without developing recurrent pulmonary venous stenosis or anastomotic narrowing, the long-term prognosis is outstanding, and most children achieve catch-up growth and lead active lives.
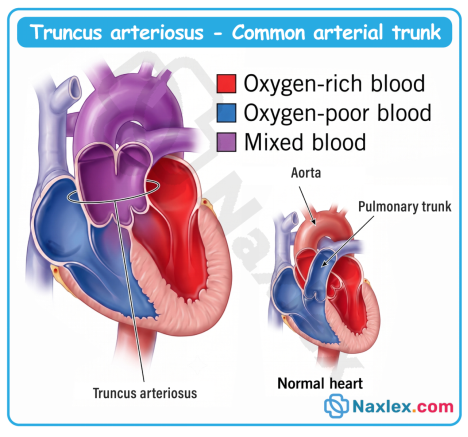
Truncus Arteriosus
Truncus arteriosus (TA) is a rare, complex, and cyanotic congenital heart anomaly characterized by a single large primitive arterial trunk that overrides a large ventricular septal defect (VSD). Instead of dividing into a distinct aorta and main pulmonary artery during fetal development, this single trunk serves as the sole outlet for both the right and left ventricles, supplying the systemic, pulmonary, and coronary circulations simultaneously.
Epidemiology
- Truncus arteriosus is uncommon, accounting for approximately 1% to 2% of all congenital heart defects.
- The incidence is approximately 1 in 10,000 live births.
- Unlike ASD, there is no significant gender predilection; it affects males and females relatively equally.
- It carries an extremely high mortality rate if left untreated, with the majority of infants dying within the first year of life due to severe congestive heart failure.
Etiology
- Genetic factors: Highly associated with microdeletions of chromosome 22q11.2 (DiGeorge Syndrome and Velocardiofacial Syndrome), which impacts normal conotruncal development.
- Environmental factors: Maternal exposure to rubella, poorly controlled pregestational maternal diabetes, advanced maternal age, smoking, and alcohol consumption during the first trimester.
- Embryological failure: Occurs due to a failure of the neural crest-derived conotruncal ridges to fuse and spiral, which prevents the normal embryonic truncus arteriosus from dividing into the ascending aorta and the main pulmonary trunk.
Pathophysiology
- Mixing of blood: Deoxygenated systemic venous return enters the right ventricle, while oxygenated pulmonary venous return enters the left ventricle. Both streams meet and freely mix through the large, obligatory ventricular septal defect (VSD) directly underneath the truncal valve.
- Common ejection pathway: This mixed, desaturated blood is ejected out of both ventricles into the single massive truncal vessel.
- Shifting fluid dynamics: Blood flow divides into the systemic and pulmonary pathways based entirely on the path of least resistance. Initially, newborn pulmonary vascular resistance (PVR) is high, balancing flow.
- Pulmonary overcirculation: As PVR drops sharply over the first few weeks of life, blood preferentially floods the low-pressure pulmonary bed. This leads to massive pulmonary overcirculation, systemic hypoperfusion, and rapid volume overload of the left atrium and left ventricle.
- Vessel remodeling: Chronic volume and pressure overload damage the pulmonary vascular bed. If surgical intervention is delayed, irreversible pulmonary hypertension and pulmonary vascular obstructive disease will establish rapidly.
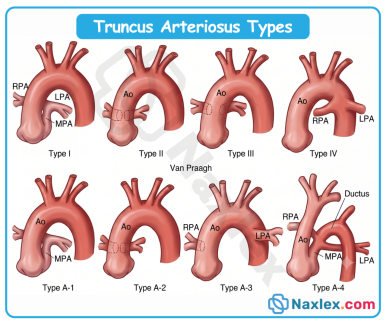
Anatomical Classifications
Anatomical variants are universally classified using two major systems based on how the pulmonary arteries arise from the common truncal vessel:
|
Type |
Collett and Edwards System (1949) |
Van Praagh System (1965 / 2000 Mod) |
|
Type I / A1 |
A single short pulmonary trunk arises from the common trunk and then branches into the right and left pulmonary arteries. (Most common, ~50-60% of cases). |
Identical to Collett & Edwards Type I; single pulmonary trunk arises from the left posterolateral side of the main truncus. |
|
Type II / A2 |
The right and left pulmonary arteries arise separately and directly from the posterior wall of the common trunk close to each other. |
The right and left branch pulmonary arteries have separate origins from the posterolateral portion of the common trunk (combines C&E Types II and III). |
|
Type III / A3 |
The right and left pulmonary arteries arise separately from the lateral aspects of the common trunk, widely spaced. |
Unilateral branch pulmonary artery atresia or absence; one lung is supplied by a branch from the truncus, while the other is fed by collaterals/PDA. |
|
Type IV / A4 |
No pulmonary arteries arise from the common trunk; pulmonary flow is supplied by major collateral arteries from the descending aorta (now classified as Tetralogy of Fallot with pulmonary atresia). |
Common trunk coexists with an underdeveloped, hypoplastic, or completely interrupted aortic arch. |
Image Title: Truncus Arteriosus Types
Clinical Manifestations
Infants may appear deceptively normal at birth while PVR remains elevated, but symptoms escalate rapidly over the first few weeks of life as pulmonary resistance plummets.
- General: Persistent mild-to-moderate cyanosis or duskiness that does not resolve with oxygen therapy, profound fatigue, lethargy, poor feeding patterns, and sweating during feeds leading to failure to thrive.
- Respiratory: Signs of severe congestive heart failure and pulmonary edema including tachypnea, grunting, nasal flaring, costosternal retractions, and persistent rales.
- Cardiac auscultation:
- S1: Normal.
- S2: Characteristically single, loud, and pounding because there is only one functioning semilunar valve closing (the truncal valve).
- Ejection Click: A sharp systolic ejection click is frequently heard immediately after S1 at the apex and left sternal border, caused by the opening of the large, often dysplastic truncal valve.
- Murmur: A harsh, loud pansystolic murmur (Grade/ III-IV/VI) is heard best at the lower left sternal border due to the VSD. A mid-diastolic low-pitched rumble may be heard at the apex due to excessive, increased blood flow returning across the mitral valve.
Diagnostic Evaluation
- Echocardiography (ECHO): The primary diagnostic tool. Confirms a single overriding arterial trunk, delineates the origin of the branch pulmonary arteries, measures the size of the VSD, and assesses the structure and competence of the truncal valve (which is frequently regurgitant or stenotic).
- Electrocardiogram (ECG): Demonstrates biventricular hypertrophy as both lower chambers adapt to systemic pressures. Right axis deviation and prominent P-waves indicating biatrial enlargement may be present.
- Chest X-ray (CXR): Typically reveals profound cardiomegaly, a prominent or absent pulmonary artery segment, an abnormally high right-sided aortic arch (present in ~30% of cases), and massively increased pulmonary vascular markings.
- Genetic Testing: Indicated in all presentations to confirm or rule out a 22q11.2 microdeletion (DiGeorge Syndrome).
Therapeutic Management
A. General Pre-Operative Principles
- Medical Stabilization: Aggressive management of congestive heart failure using loop diuretics (e.g., furosemide) and afterload reducers (e.g., ACE inhibitors) to ease systemic output.
- Inotropic Support: Digoxin or low-dose milrinone may be initiated to maximize myocardial contractility and lower systemic vascular resistance.
- Oxygen Delivery Balancing: Supplemental oxygen must be used with extreme caution. Oxygen is a potent pulmonary vasodilator; administering high concentrations drops PVR further, causing massive pulmonary flooding and dangerous systemic hypoperfusion. Target oxygen saturations are deliberately maintained at tight sub-normal parameters (75% to 85%).
B. Surgical Management
- Indication: Mandatory for survival. Performed early in infancy, typically within the first 2 to 6 weeks of life, before irreversible pulmonary vascular changes set in.
- Procedure (Complete Repair / Rastelli-type variant):
- The branch pulmonary arteries are surgically detached from the common truncal vessel.
- The remaining common trunk is repaired and remodeled to serve exclusively as the new ascending aorta.
- The large ventricular septal defect is closed using a synthetic patch (Dacron or pericardial), ensuring the left ventricle vents directly into the remodeled aorta.
- A valved Right Ventricle-to-Pulmonary Artery (RV-PA) conduit (allograft or synthetic tube) is placed to establish a brand-new pathway for right ventricular outflow to the lungs.
Post-Operative Nursing Interventions
Post-Op Day 0 to 1 (ICU Phase)
- Ventilatory Architecture & Gas Exchange: Maintain mechanical ventilation with precise sedation/paralysis to prevent pulmonary hypertensive crises. Closely monitor arterial blood gases (ABGs). Avoid hypercapnia and acidosis, which act as triggers for pulmonary vasoconstriction.
- Hemorrhage Tracking: Monitor hourly chest tube output. Report drainage greater than 3 mL/kg/hr for 3 consecutive hours OR greater than 5 mL/kg in any single hour, as this indicates acute surgical hemorrhage.
- Hemodynamic Core Parameters: Monitor mean arterial pressures (MAP) and central venous pressures (CVP). Assess peripheral perfusion markers (capillary refill time less than 3 seconds, core-to-peripheral temperature gradients, and strong pedal pulses).
- Rhythm Surveillance: Continuous ECG monitoring for conduction delays or lethal arrhythmias. Watch for Junctional Ectopic Tachycardia (JET) or varying degrees of Atrioventricular (AV) blocks caused by surgical manipulation near the AV node during VSD patch placement.
- Fluid & Metabolism Balancing: Strict intake and output (I&O) recording. Monitor urinary output hourly via an indwelling Foley catheter; report values dropping below 1 mL/kg/hr (signaling low cardiac output or early acute kidney injury).
Post-Op Day 2 to 3 (Transition Phase)
- Pulmonary Toilet and Weaning: Support gradual weaning from mechanical ventilation to supplemental oxygen as tolerated. Perform gentle endotracheal or oral suctioning accompanied by pre-oxygenation. Initiate active atelectasis prevention measures (bubble-blowing or infant repositioning shifts).
- Metabolic Escalation: Advance gastrointestinal intake from NPO to clear liquids or specialized formulas via a nasogastric/orogastric tube as bowel sounds recover. Monitor closely for abdominal distension or feeding intolerance.
- Analgesic Titration: Administer scheduled multi-modal pain therapies (IV ketorolac or acetaminophen) coupled with continuous or scheduled opioid infusions (fentanyl or morphine) to minimize sympathetic stress responses.
Post-Op Day 4 to Discharge
- Integumentary Inspection: Assess the median sternotomy incision site hourly then daily for early indicators of deep or superficial wound infections (erythema, localized warmth, edema, or purulent drainage).
- Caregiver Empowerment: Provide intensive education regarding activity restrictions. Instruct caregivers never to lift the infant under the arms/axillae for 4 to 6 weeks to prevent sheer forces across the healing bony sternum; demonstrate scooping techniques supporting the neck and bottom.
- Conduit Longevity Counseling: Educate parents that the RV-PA conduit does not grow with the child. Emphasize the absolute necessity of long-term pediatric cardiology follow-ups, as future surgical or transcatheter conduit replacements will be required as the child grows.
Nursing Diagnosis (Post-Op)
Post-Op Day 1
- Decreased Cardiac Output related to structural surgical trauma, altered pre/afterload parameters, transient myocardial dysfunction, or dysrhythmias.
- Impaired Gas Exchange related to ventilation-perfusion (V/Q) mismatching, high pulmonary vascular resistance, residual anesthesia effects, or surgical pain.
- Risk for Altered Trigeminal/Systemic Perfusion related to fluid shifts, chest tube losses, or rapid changes in vascular circuit resistance.
Post-Op Day 2 to 3
- Acute Pain related to invasive chest tubes, continuous tissue retraction, and a median sternotomy incision.
- Ineffective Airway Clearance related to viscous retained secretions, post-extubation glottic edema, and a pain-induced reluctance to cough or sigh deep.
- Risk for Infection related to indwelling central venous lines, arterial monitoring lines, temporary pacing wires, and an open surgical field.
Post-Op Day 4+
- Deficient Knowledge (Caregiver) related to specialized home medication management (diuretics, digoxin safety parameters), wound care tracking, and red flag clinical signs.
- Activity Intolerance related to surgical convalescence, compromised cardiopulmonary reserves, and generalized physical deconditioning.
Complications
- Cardiac: Pulmonary hypertensive crises (abrupt spiking of PVR leading to right-heart collapse), residual ventricular septal leaks, persistent truncal (aortic) valve regurgitation, and refractory tachyarrhythmias (JET, atrial flutter).
- Pulmonary: Chronic atelectasis, diaphragmatic paralysis due to phrenic nerve injury during thoracic dissection, and pleural effusions.
- Surgical/Systemic: Conduit stenosis or calcification, postpericardiotomy syndrome, infective endocarditis, or thromboembolic neurological events (stroke).
Prognosis
- Surgical survival rates for early primary repair range between 80% and 97% in high-volume pediatric cardiac centers.
- Long-term data reveals roughly 75% of survivors are alive 20 years post-op.
- Re-intervention is a mathematical certainty; nearly 100% of infants will outgrow or experience structural degeneration of their RV-PA conduit, requiring successive surgical replacements or transcatheter balloon/stent dilations throughout late childhood and adolescence.
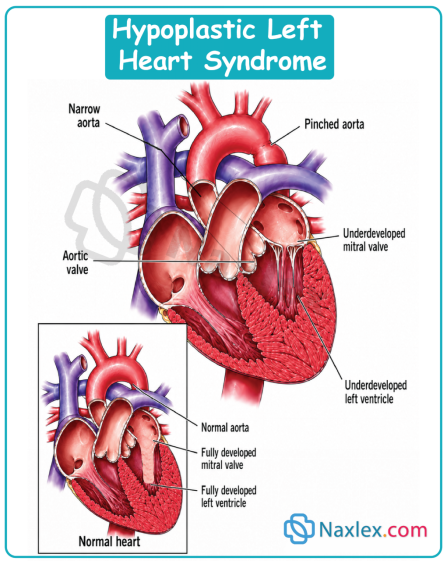
Hypoplastic Left Heart Syndrome
Hypoplastic left heart syndrome (HLHS) is a severe, complex congenital heart anomaly characterized by the marked underdevelopment of the left-sided cardiac structures. This includes a hypoplastic left ventricle, atresia or severe stenosis of the aortic and mitral valves, and hypoplasia of the ascending aorta and aortic arch. As a result, the left side of the heart is completely incapable of supporting systemic circulation, rendering systemic perfusion entirely dependent on a patent ductus arteriosus (PDA) after birth.
Epidemiology
- HLHS accounts for approximately 1% to 3% of all congenital heart defects, but it is responsible for nearly 25% of all cardiac-related deaths in the first week of life if left untreated.
- The incidence is approximately 1 in 3,000 to 4,300 live births.
- There is a slight male predilection, with a male-to-female ratio of approximately 1.5:1.
- It represents one of the most challenging and high-risk conditions in pediatric cardiology.
Etiology
- Genetic factors: Highly heritable with a complex multi-genic inheritance pattern. It is associated with specific genetic syndromes like Turner syndrome, Trisomy 13, Trisomy 18, and mutations in genes such as NOTCH1 and NKX2.5.
- Environmental factors: Maternal exposure to specific industrial solvents, maternal diabetes, or advanced maternal age have been noted as potential contributing risks.
- Embryological failure: Result of restricted blood flow through the left side of the developing heart during fetal life, leading to the failure of left ventricular and valvular growth (the "no flow, no grow" hypothesis).
Pathophysiology
- Underdeveloped Left Ventricle: The left ventricle is tiny, non-functional, and unable to pump blood to the body.
- Ductal-Dependent Systemic Circulation: Oxygenated blood returning from the lungs to the left atrium cannot pass normally into the left ventricle. Instead, it crosses an atrial communication (PFO or ASD) into the right atrium, mixing with deoxygenated systemic venous return.
- Single Ventricle Function: The right ventricle must perform double duty: pumping mixed blood into the pulmonary artery to the lungs, and simultaneously redirecting a portion of that blood through the patent ductus arteriosus (PDA) into the aorta to supply the brain and coronary arteries.
- Ductal Closure Crisis: As the PDA begins to constrict naturally within the first hours or days of life, systemic blood flow drops rapidly. This leads to systemic hypoperfusion, severe metabolic acidosis, hypovolemic-cardiogenic shock, and organ failure unless the ductus is medically forced open.
Clinical Manifestations
Infants often appear healthy and stable at birth while the ductus arteriosus remains open, but deteriorate rapidly as it closes.
- General: Progressive, profound cyanosis, cold extremities, weak peripheral pulses, and a grayish skin color as systemic perfusion collapses.
- Respiratory: Tachypnea, dyspnea, grunting, and retractions due to severe pulmonary overcirculation and congestive heart failure.
- Cardiac auscultation:
- S1: Normal.
- S2: Typically single and loud because the aortic valve component is faint or entirely absent.
- Murmur: A non-specific, soft systolic ejection murmur may be heard at the left sternal border, or a continuous machinery-like murmur if a patent ductus arteriosus is present, though murmurs can be surprisingly quiet or absent.
- Shock/Metabolic: Hypotension, delayed capillary refill (> 3 seconds), oliguria, and profound metabolic acidosis.
Diagnostic Evaluation
- Echocardiography (ECHO): The gold standard diagnostic tool. It definitively shows a diminutive left ventricle, atretic/stenotic aortic and mitral valves, a hypoplastic ascending aorta, and confirms the size and patency of the PDA and atrial communication.
- Electrocardiogram (ECG): Demonstrates right axis deviation and right ventricular hypertrophy (RVH) due to chronic right-sided volume and pressure workload.
- Chest X-ray (CXR): Typically reveals cardiomegaly and marked pulmonary venous congestion or increased pulmonary vascular markings.
- Cardiac Catheterization: Rarely needed for initial diagnosis, but may be used emergently to perform an atrial septostomy if the interatrial communication is severely restrictive.
Therapeutic Management
A. Pre-Operative General Principles
- Prostaglandin E1 (Alprostadil) Infusion: Continuous IV infusion is started immediately to prevent the closure of, or reopen, the ductus arteriosus. This maintains essential systemic blood flow.
- Balancing the Qp:Qs Ratio: Careful management of the balance between pulmonary blood flow (Qp) and systemic blood flow (Qs).
- Avoid hyperoxemia: Keep targeted SpO2 tight between 75% to 85%. High supplemental oxygen acts as a potent pulmonary vasodilator, which steals blood from the systemic loop and floods the lungs.
- Permissive Hypercapnia: Sub-ambient oxygen environment or mild hypoventilation on a mechanical ventilator may be used to elevate pulmonary vascular resistance (PVR) slightly, shifting blood flow safely back toward systemic circulation.
- Avoid Inadvertent Over-oxygenation: Maintain room air (FiO2 21%) or precise blending; avoid high-flow or 100% oxygen therapies unless directed.
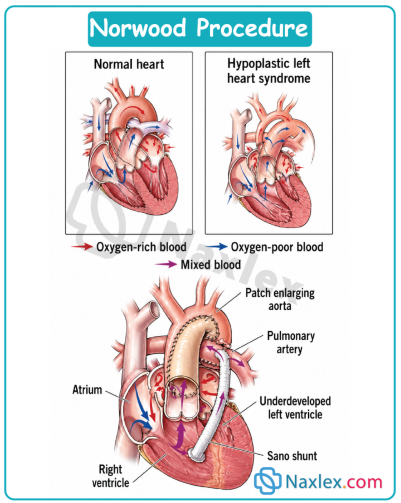
B. Surgical Management (Staged Palliation)
HLHS cannot be cured, but it is palliated through a series of three highly complex surgeries to convert the heart into a single-ventricle system where the right ventricle acts as the systemic pump.
Stage 1: The Norwood Procedure: First 1-2 weeks of life.
The hypoplastic aorta is reconstructed and connected directly to the right ventricle so it can pump blood to the body. A shunt (either a modified Blalock-Taussig [BT] shunt or a Sano shunt) is placed to provide a controlled source of blood flow to the lungs. The atrial septum is completely removed to ensure unhindered flow from the lungs to the right side of the heart.
Stage 2: The Bidirectional Glenn Procedure: Age 4-6 months.
The superior vena cava (SVC) is disconnected from the heart and sutured directly to the pulmonary artery. This routes deoxygenated blood from the upper body straight to the lungs without passing through the ventricle, reducing the volume workload on the right ventricle. The previous BT or Sano shunt is removed.
Stage 3: The Fontan Procedure: Age 2-4 years.
The inferior vena cava (IVC) is connected to the pulmonary artery, often via an extracardiac conduit. This completely separates systemic and pulmonary circulations. The single right ventricle now functions exclusively as the systemic pump, driving oxygenated blood to the body, while systemic venous blood flows passively into the lungs.
Post-Operative Nursing Interventions
Post-Op Day 0 to 1 (ICU Phase)
- Monitor Hemodynamic Balance: Maintain SpO2 precisely between 75% and 85%. Watch for signs of pulmonary overcirculation (SpO2 > 85%, widening pulse pressures, hypotension) which indicates blood is stealing away from the body to the lungs.
- Monitor Chest Tube Output: Assess hourly drainage. Report immediately if output is greater than 3 mL/kg/hr for 3 consecutive hours or greater than 5 mL/kg in any single hour (indicates surgical hemorrhage).
- Vigilant ECG Monitoring: Watch for arrhythmias, especially Junctional Ectopic Tachycardia (JET) or heart blocks, which can quickly drop cardiac output.
- Strict Intake and Output (I&O): Monitor fluid balances hourly. Maintain a patent Foley catheter; target urine output at a minimum of 1 mL/kg/hr to preserve renal perfusion.
- Perfusion and Pulse Checks: Assess capillary refill times (normal < 3 seconds) and evaluate core-to-peripheral temperature gradients alongside central and peripheral pulses.
Post-Op Day 2 to 3 (Transition Phase)
- Weaning Ventilation: Carefully monitor respiratory mechanics during weaning from mechanical ventilation to prevent hypoxemia or respiratory acidosis.
- Nutritional Advancement: Keep NPO status until bowel sounds return and hemodynamic status is completely stable; advance from clear liquids to specialized high-calorie formulas as tolerated.
- Pulmonary Hygiene: Utilize gentle suctioning, passive repositioning, or bubble blowing/age-appropriate techniques in older stages to prevent atelectasis.
- Structured Pain Management: Administer scheduled multi-modal analgesia (e.g., IV acetaminophen or ketorolac) combined with titrated intravenous opioids for rescue to prevent stress-induced hypertensive crises.
Post-Op Day 4 to Discharge
- Incision Site Assessment: Monitor the sternotomy line and previous chest tube sites daily for signs of infection (erythema, warmth, edema, or drainage).
- Ambulation and Handling: Promote gentle handling and cluster care; facilitate gradual ambulation for older toddlers recovering from later-stage surgeries.
- Caregiver Education: Extensive training on feeding strategies (often requiring nasogastric tubes due to high caloric needs), infection prevention, strict medication adherence, and sternal precautions (avoid lifting the child under the arms for 4 to 6 weeks).
Nursing Diagnosis (Post-Op)
Post-Op Day 1
- Decreased Cardiac Output related to complex single-ventricle physiology, myocardial surgical trauma, or altered systemic/pulmonary vascular resistance balances.
- Impaired Gas Exchange related to mechanical ventilation dependency, altered pulmonary blood perfusion pathways, or ventilation-perfusion mismatching.
- Risk for Fluid Volume Deficit related to chest tube blood loss, surgical third-spacing shifts, or intensive diuretic therapy.
Post-Op Day 2 to 3
- Acute Pain related to sternotomy incision, mediastinal chest tube irritation, and invasive central lines.
- Ineffective Airway Clearance related to thick respiratory secretions, mechanical ventilation trauma, or reluctance to clear airway secondary to surgical pain.
- Risk for Infection related to multiple indwelling invasive lines (arterial, central venous lines) and a large median sternotomy incision.
Post-Op Day 4+
- Deficient Knowledge (Caregiver) related to highly complex home care protocols, multiple critical medication regimens, feeding challenges, and subtle red-flag identification.
- Activity Intolerance related to prolonged surgical recovery, baseline cardiac status, and generalized physical deconditioning.
Complications
- Cardiac: Single-ventricle pump failure, severe arrhythmias (especially during Fontan transition), thromboembolism, and progressive tricuspid valve regurgitation.
- Pulmonary: Pulmonary hypertension, plastic bronchitis (a rare proteinaceous cast complication post-Fontan), or pleural effusions.
- Surgical/Systemic: Interstage mortality (sudden death between Stage 1 and Stage 2), developmental delays, protein-losing enteropathy (PLE), renal insufficiency, or postpericardiotomy syndrome.
Prognosis
- Without surgical intervention, HLHS is fatal, typically within the first few days to weeks of life.
- With staged palliation, 5-year survival rates range between 60% and 70%, depending on center experience and underlying anatomical variations.
- Long-term survivors face unique, ongoing morbidities, and many may ultimately require a orthotopic heart transplantation later in childhood or adulthood due to eventual single-ventricle heart failure.
Summary
- Mixed congenital heart defects represent a high-acuity category of cardiac anomalies where survival depends on the deliberate blending of oxygenated and deoxygenated blood within the heart's chambers or great vessels.
- Unlike simple acyanotic shunts, these defects alter the traditional serial configuration of the circulatory system into parallel loops or single-chamber mixing pools.
- Consequently, the blood delivered to the systemic organs is invariably desaturated, manifesting clinically as cyanosis that is largely unresponsive to supplemental oxygen therapy.
- A definitive hallmark of critical mixed lesions, such as Transposition of the Great Vessels (TGV) and Hypoplastic Left Heart Syndrome (HLHS), is their absolute reliance on fetal transitional pathways, namely the Patent Ductus Arteriosus (PDA) and Patent Foramen Ovale (PFO).
- When these structures begin their natural closure shortly after birth, systemic perfusion or pulmonary mixing drops to zero, triggering swift metabolic acidosis, cardiogenic shock, and cardiovascular collapse.
- From a nursing perspective, managing these neonates requires maintaining a delicate equilibrium between pulmonary vascular resistance (PVR) and systemic vascular resistance (SVR).
- Because oxygen acts as a potent pulmonary vasodilator, administering excessive supplemental oxygen drastically drops PVR, causing blood to rush into the lungs and steal essential perfusion from the rest of the body.
- Nurses must target a lower baseline oxygen saturation (typically 75% to 85%) and maintain continuous, secure intravenous access for immediate prostaglandin E1 (PGE1) infusions to guarantee ductal patency.
- Definitive management involves complex surgical repairs, varying from the early neonatal arterial switch operation for TGV to the high-risk, three-stage palliative tracking (Norwood, Glenn, and Fontan procedures) required to reshape the right ventricle into a systemic pump for HLHS.
- Post-operative nursing care focuses on monitoring for low cardiac output syndrome, arrhythmias, and acute pulmonary hypertensive crises.
