
Please set your exam date
Chronic Obstructive Pulmonary Disease
Study Questions
Practice Exercise 1
A nurse is teaching a client about the effects of tobacco smoke on the respiratory system and its impact. Which of the following represents a long-term effect of smoking?
Explanation
Chronic inhalation of tobacco smoke triggers a persistent inflammatory response within the tracheobronchial tree characterized by goblet cell proliferation. This sustained chemical insult results in the metaplasia of ciliated columnar epithelium into stratified squamous epithelium, significantly impairing the mucociliary escalator. Furthermore, the toxic constituents induce protease-antiprotease imbalance, leading to the destruction of alveolar walls and permanent capillary bed rarefaction.
Rationale for correct answer
4. Long-term exposure to cigarette smoke irritants induces mucous gland hyperplasia and goblet cell metaplasia, resulting in chronic hypersecretion of thick, tenacious sputum. These structural alterations, combined with impaired ciliary motility, create a stagnant environment that significantly elevates the infection risk for the patient.
Rationale for incorrect answers
1. Acute exposure to smoke irritants typically triggers immediate bronchospasm and laryngeal irritation, leading to transient hoarseness rather than permanent structural remodeling. While these symptoms are common in smokers, they represent acute physiological responses to chemical combustion products instead of the definitive long-term architectural changes of the lung.
2. Tobacco smoke actually increases secretions rather than causing decreased mucus, as the body attempts to protect the delicate mucosal lining from thermal and chemical injury. The characteristic chronic smoker's cough is a compensatory mechanism necessitated by the failure of the paralyzed cilia to effectively clear the resulting excessive secretions.
3. Chronic smoking significantly impairs rather than promotes the increased function of alveolar macrophages, which are the primary phagocytic cells of the distal airways. The heavy oxidative stress and particulate load from smoke lead to macrophage dysfunction, reducing their ability to phagocytize pathogens and increasing susceptibility to lower respiratory tract infections.
Test-taking strategy
- Identify the timeframe required by the question stem, specifically looking for long-term versus acute physiological changes.
- Apply knowledge of pathophysiology to recognize that chronic irritation leads to cellular hyperplasia and structural remodeling.
- Rule out options that describe diminished physiological responses or improved immune functions, as smoking is a known pathogenic immunosuppressant.
- Select the option that reflects permanent anatomical changes resulting from prolonged chemical exposure.
Take home points
- Chronic smoking causes hyperplasia of mucous glands and goblet cells leading to chronic bronchitis.
- Tobacco smoke paralyzes and eventually destroys cilia, severely compromising the mucociliary escalator.
- Alveolar macrophage activity is suppressed by tobacco toxins, directly increasing bacterial colonization risks.
- Metaplastic changes in the airway epithelium represent a precursor to the development of bronchogenic carcinoma.
A nurse is reviewing the pathophysiology of cystic fibrosis with a client. Which mechanism explains how cystic fibrosis leads to obstructive lung disease?
Explanation
Cystic fibrosis arises from a genetic mutation in the CFTR protein, which serves as a critical transmembrane regulator for chloride ion conductance in epithelial tissues. In the respiratory tract, this dysfunction inhibits the normal efflux of chloride into the airway lumen and causes the dysregulation of epithelial sodium channels, resulting in excessive sodium and water reabsorption. This pathological ion transport creates a depleted airway surface liquid layer, transforming the normal mucus blanket into an extremely dehydrated, viscid substance that adheres to the bronchial mucosa and initiates a cycle of obstruction and infection.
Rationale for correct answer
3. The primary biochemical defect in cystic fibrosis involves the production of airway secretions that are low in chloride, leading to secondary water depletion and the formation of thickened mucus. This hyperviscous state prevents normal mucociliary clearance, causing the secretions to remain trapped within the bronchi and acting as a physical nidus for chronic bacterial colonization.
Rationale for incorrect answers
1. Although chronic inflammation eventually leads to structural changes, fibrosis of the mucous glands is a late-stage complication rather than the initial mechanism that explains how the disease causes obstruction. The obstructive component is primarily driven by the inspissated secretions themselves, which fill the lumen long before the permanent destruction of the underlying bronchial walls occurs.
2. The hallmark of cystic fibrosis is obstructive airway disease, whereas the destruction of the lung parenchyma and significant interstitial scarring are more characteristic of restrictive or end-stage fibrotic lung processes. While parenchymal damage does occur over decades of infection, the fundamental obstructive mechanism is centered on the conductive airways rather than the primary gas-exchange units.
4. There is no physiological mechanism where pancreatic enzymes are transported through the systemic circulation and deposited into the respiratory tract to cause lung disease. While cystic fibrosis causes pancreatic duct obstruction, the bronchial symptoms are the result of the genetic defect existing independently within the respiratory epithelial cells themselves.
Test-taking strategy
- Analyze the biochemical basis of the disease, specifically how ion movement influences the rheology of respiratory secretions.
- Differentiate between the primary defect, which is the abnormal mucus consistency, and the secondary structural damage like bronchial wall destruction.
- Rule out options that suggest systemic enzyme deposition, as the pulmonary manifestations of cystic fibrosis are localized to the respiratory epithelium.
- Focus on the osmotic consequences of sodium and chloride imbalances that lead to the hallmark "thickened mucus" of the condition.
Take home points
- The CFTR mutation leads to defective chloride transport and excessive sodium uptake, dehydrating the airway surface.
- Obstructive lung disease in cystic fibrosis starts with mucus plugging of the small and medium-sized bronchi.
- Chronic endobronchial infection leads to a protease-rich environment that eventually causes bronchiectasis.
- Pancreatic insufficiency and respiratory disease in cystic fibrosis are both caused by the same cellular ion channel defect.
A nurse is assessing an adult client diagnosed with bronchiectasis. Which finding is the nurse most likely to observe in this client’s history?
Explanation
Bronchiectasis represents a pathological state of permanent, irreversible bronchial dilation resulting from a vicious cycle of inflammation and infection that destroys the muscular and elastic components of the airway walls. This condition typically evolves through the Cole hypothesis, where an initial insult leads to impaired mucociliary clearance, facilitating microbial colonization and a persistent neutrophilic response. The release of toxic mediators, including neutrophil elastase, causes extensive tissue degradation and replaces normal lung architecture with dilated, thick-walled bronchi that frequently sequester purulent secretions.
Rationale for correct answer
4. The clinical history of a patient with bronchiectasis is characteristically defined by recurrent episodes of pneumonia or bronchitis that initiate and perpetuate the inflammatory destruction of the airways. These frequent respiratory infections lead to the structural remodeling and permanent dilation of the bronchi, which is the hallmark of the disease process observed in this population.
Rationale for incorrect answers
1. While severe injuries can impact pulmonary function, isolated chest trauma is not a primary etiological factor for the chronic, diffuse bronchial remodeling seen in bronchiectasis. Most traumatic injuries result in localized issues such as pneumothorax or pulmonary contusion rather than the widespread airway dilation and chronic suppurative disease that characterizes this specific obstructive condition.
2. Although it involves airway inflammation, childhood asthma typically involves reversible bronchospasm and hyperreactivity rather than the permanent, necrotizing destruction of the bronchial walls. While severe, poorly controlled asthma can lead to airway remodeling, it is not the most common or definitive historical finding when compared to the chronic infective triggers of bronchiectasis.
3. Cigarette smoking is the primary driver for chronic obstructive pulmonary disease and emphysema, but it is not considered the direct cause of the localized bronchial wall destruction seen here. While smoking can exacerbate respiratory symptoms, the primary pathophysiological hallmark of bronchiectasis is linked to underlying ciliary dysfunction or prior severe infection rather than tobacco-induced alveolar wall destruction.
Test-taking strategy
- Focus on the hallmark of the disease, which is permanent airway destruction caused by a cycle of inflammation and infection.
- Evaluate the choices based on which factor provides the necessary pathological environment for chronic bronchial remodeling and dilation.
- Rule out conditions like smoking or asthma that have distinct pathophysiological profiles, such as alveolar destruction or reversible bronchoconstriction.
- Select the option that aligns with the "vicious cycle" theory of microbial colonization and subsequent tissue damage.
Take home points
- Bronchiectasis is characterized by permanent dilation of the bronchi due to destruction of elastic and muscular tissue.
- Recurrent lower respiratory tract infections are the most frequent cause and clinical finding in these patients.
- The classic presentation includes a chronic productive cough with large volumes of foul-smelling, purulent sputum.
- High-resolution computed tomography is the gold standard diagnostic tool to visualize the thickened, dilated airway walls.
A nurse is assessing a 30-year-old white female whose parent has a history of a genetic pulmonary disease. Which obstructive pulmonary disease is she most likely to be diagnosed with?
Explanation
Alpha1-Antitrypsin deficiency is an autosomal codominant genetic disorder characterized by a mutation in the SERPINA1 gene, leading to significantly reduced serum levels of the protease inhibitor Alpha1-Antitrypsin. Under normal physiological conditions, this protein is synthesized in the liver and functions to neutralize neutrophil elastase in the lower respiratory tract, thereby protecting the delicate alveolar connective tissue. A quantitative or functional deficiency results in an uncontrolled proteolytic attack on the pulmonary parenchyma, causing the premature development of panacinar emphysema, often occurring between the ages of 20 and 50 years.
Rationale for correct answer
4. The patient's age of 30 years and the specific mention of a parental genetic history strongly suggest Alpha1-Antitrypsin deficiency as the most probable diagnosis. This hereditary condition leads to early-onset obstructive disease by allowing protease-mediated alveolar destruction, which is clinically distinct from the typical smoking-related emphysema that usually manifests in much older populations.
Rationale for incorrect answers
1. While COPD encompasses emphysema and chronic bronchitis, it is primarily an acquired condition resulting from long-term inhalation of noxious particles, most commonly from tobacco smoke. A diagnosis of standard smoking-related COPD in a 30-year-old is statistically rare and would not be characterized primarily as a genetic disease inherited directly from a parent.
2. Although asthma has a strong polygenic component and often presents with a familial cluster, it is generally considered a multifactorial disease rather than a straightforward genetic pulmonary disorder. Furthermore, the question emphasizes a inherited pulmonary disease history in the parent, whereas asthma is typically associated with a broader atopic history including eczema or allergic rhinitis.
3. While cystic fibrosis is indeed a genetic obstructive disease, it is most commonly diagnosed during neonatal screening or early childhood due to severe multisystem involvement. A 30-year-old female presenting for an initial assessment is less likely to have undiagnosed fibrosis of the lungs from this specific mutation compared to the adult-onset presentation of Alpha1-Antitrypsin deficiency.
Test-taking strategy
- Identify the demographic data, specifically the young age of 30, which should trigger suspicion for a genetic predisposition to lung disease.
- Distinguish between multifactorial conditions like asthma and true Mendelian genetic disorders like Alpha1-Antitrypsin deficiency or cystic fibrosis.
- Recognize that panacinar emphysema in a young, non-smoking adult is the classic clinical vignette for a protease inhibitor deficiency.
- Rule out cystic fibrosis based on the typical age of onset, as most patients are symptomatic and diagnosed well before the third decade of life.
Take home points
- Alpha1-Antitrypsin deficiency should be suspected in any young adult presenting with signs of emphysema.
- The condition results from an imbalance where neutrophil elastase unchecked by antiprotease destroys alveolar walls.
- Unlike smoking-induced emphysema, Alpha1-Antitrypsin deficiency typically causes panacinar damage in the lower lung lobes.
- Genetic testing and serum level quantification are essential for confirming the diagnosis and determining the specific phenotype
A nurse is teaching a client about the effects of cigarette smoking on the respiratory system. Which of the following changes is typically caused by long-term smoking?
Explanation
Chronic exposure to tobacco smoke initiates a pervasive inflammatory cascade within the tracheobronchial tree characterized by profound structural remodeling of the airway epithelium. The primary pathological response involves the sustained metaplasia of ciliated columnar cells into stratified squamous cells, a transition that significantly compromises the mucociliary escalator. This toxic environment promotes the proliferation of inflammatory mediators and proteases that degrade the pulmonary extracellular matrix, leading to the irreversible enlargement of distal air spaces and the loss of elastic recoil. The chemical irritants induce significant alterations in glandular architecture, specifically targeting the mucosal lining of the conducting airways.
Rationale for correct answer
2. Long-term inhalation of cigarette smoke acts as a potent chronic irritant that triggers hyperplasia of the goblet cells and the submucosal glands. This cellular adaptation results in the persistent mucus production and hypersecretion characteristic of chronic bronchitis, which significantly obstructs the smaller airways and necessitates a chronic productive cough.
Rationale for incorrect answers
1. Smoking does not cause the hypertrophy of the pulmonary capillaries; rather, it typically leads to the destruction of the alveolar-capillary membrane and rarefaction of the vascular bed. While hemoptysis can occur in chronic smokers, it is usually secondary to airway inflammation, infection, or the development of a bronchogenic carcinoma rather than a primary hypertrophic vascular change.
3. Cigarette smoke is toxic to the respiratory epithelium and causes the paralysis and eventual destruction of the cilia rather than an increased proliferation of these structures. The loss of ciliary function, combined with the presence of thickened mucus, prevents the effective clearance of inhaled particulates and pathogens from the lower respiratory tract, predisposing the individual to chronic disease.
4. Although the number of macrophages may increase in response to inflammation, smoking actually impairs the macrophage function and reduces their phagocytic efficiency. This functional deficit, rather than a protective proliferation, leaves the smoker with a blunted immune response in the distal airways and a significantly higher susceptibility to frequent and severe pulmonary infections.
Test-taking strategy
- Identify the pathological cellular adaptations that occur in response to chronic chemical irritation, such as hyperplasia and metaplasia.
- Distinguish between proliferative changes that are protective versus those that are maladaptive, such as the increase in mucus-secreting cells.
- Eliminate options that suggest an improvement in physiological function, as tobacco smoke is universally deleterious to the mucociliary and immune defenses.
- Focus on the structural hallmarks of chronic bronchitis, which is the quintessential long-term obstructive consequence of prolonged tobacco use.
Take home points
- Chronic smoking causes a shift in the cellular population of the airway, favoring mucus-producing goblet cells.
- Tobacco toxins paralyze and destroy the cilia, leading to the failure of the mucociliary clearance mechanism.
- The chronic hypersecretion of mucus is the primary driver for the productive cough seen in obstructive lung disease.
- Smoking-induced inflammation leads to a protease-antiprotease imbalance that destroys the alveolar walls and elastic tissue
Practice Exercise 2
A nurse is teaching a client about pulmonary rehabilitation (PR) for COPD. The nurse wants to explain the anticipated outcomes of PR in addition to improved exercise capacity. Which of the following are expected results? Select all that apply
Explanation
Pulmonary rehabilitation (PR) is a comprehensive, evidence-based intervention designed to optimize the physical and psychological condition of patients with chronic respiratory impairment. The program integrates aerobic conditioning, strength training, nutritional counseling, and psychosocial support to address the extrapulmonary manifestations of chronic obstructive pulmonary disease. While PR cannot reverse the anatomical airflow limitation or modify the fixed airway obstruction, it significantly improves peripheral muscle oxidative capacity and desensitizes the patient to the sensation of dyspnea.
Rationale for correct answers
2. Participation in pulmonary rehabilitation provides patients with coping mechanisms and controlled breathing techniques that directly lead to decreased anxiety levels. By improving the patient’s confidence in managing breathlessness, the psychological burden of the disease is reduced, breaking the cycle of dyspnea-induced panic that often exacerbates respiratory distress.
3. The combination of social interaction and physical exercise within a peer-supported environment results in decreased depression for many COPD patients. Regular physical activity increases the release of endogenous opioids and neurotrophic factors, which helps stabilize mood and improves the overall mental health status of those with chronic illness.
5. Comprehensive pulmonary rehabilitation programs have been clinically proven to result in decreased hospitalizations and fewer emergency department visits. Improved self-management skills and better physical conditioning allow patients to recognize early signs of exacerbation and maintain stability, thereby reducing the frequency of acute medical interventions.
Rationale for incorrect answers
1. Pulmonary rehabilitation focuses on functional status and does not result in a decreased FEV₁, nor does it significantly increase this value. The forced expiratory volume in 1 second is a measure of fixed physiological obstruction, which typically remains stable or follows its natural disease trajectory despite the improvements in exercise tolerance.
4. An expected outcome of successful pulmonary rehabilitation is improved ventilatory efficiency, which does not lead to an increased oxygen requirement for the patient. In fact, many patients demonstrate an enhanced ability to perform activities of daily living with their current support, rather than requiring supplemental escalation as a result of the rehabilitation process.
Test-taking strategy
- Identify the intervention as a holistic program that targets functional and psychological outcomes rather than anatomical lung repair.
- Distinguish between physiological markers of disease (like FEV₁) which are relatively fixed, and functional markers (like quality of life) which are modifiable.
- Apply the principle of holistic care to recognize that pulmonary rehabilitation addresses the "whole person," including mental health and social functioning.
- Eliminate options that suggest a worsening of the clinical condition, such as increased oxygen needs or further declines in lung function parameters.
Take home points
- Pulmonary rehabilitation improves exercise tolerance despite having minimal impact on objective pulmonary function tests.
- Psychosocial benefits include significant reductions in the symptoms of clinical anxiety and depression.
- Program completion is associated with a decrease in the frequency and duration of hospital admissions.
- Education on energy conservation and breathing techniques is a core component of effective pulmonary rehabilitation.
A nurse is reviewing arterial blood gas (ABG) results for a client with long-standing COPD who typically has hypoxia and hypercapnia. Which ABG results show movement toward respiratory acidosis and further hypoxia indicating respiratory failure?
Explanation
Acute respiratory failure in chronic obstructive pulmonary disease occurs when the gas exchange system fails to maintain adequate oxygenation or carbon dioxide elimination. This clinical state is defined by a rapid decline in arterial oxygen tension below 60 mm Hg or an increase in arterial carbon dioxide tension above 50 mm Hg with an associated decrease in pH. The pathophysiology involves severe ventilation-perfusion mismatching and alveolar hypoventilation, leading to a profound accumulation of dissolved carbon dioxide and the formation of carbonic acid.
Rationale for correct answer
2. The values of pH 7.34 and PaCO₂ 65 mm Hg indicate a state of respiratory acidosis where the lungs are failing to eliminate carbon dioxide efficiently. This finding, coupled with a PaO₂ of 45 mm Hg, represents further hypoxia and confirms the patient has progressed into acute-on-chronic respiratory failure requiring immediate intervention.
Rationale for incorrect answers
1. These results reflect a pH of 7.35 and a PaCO₂ of 45 mm Hg which are essentially within normal limits for a patient with chronic lung disease. While the PaO₂ of 62 mm Hg shows mild hypoxemia, it does not represent the acute respiratory failure or the significant acidotic shift described in the question stem.
3. A pH of 7.42 and a PaO₂ of 90 mm Hg indicate that the patient is currently well-oxygenated and maintaining a normal acid-base balance. The PaCO₂ of 43 mm Hg is within the standard reference range, suggesting that there is no hypercapnia or movement toward respiratory acidosis in this specific clinical scenario.
4. The pH of 7.46 and PaCO₂ of 32 mm Hg demonstrate a state of respiratory alkalosis, which is typically caused by hyperventilation rather than hypoventilation. This profile is the opposite of the requested acidotic shift and shows a high oxygen level of 92 mm Hg, which is inconsistent with respiratory failure.
Test-taking strategy
- Identify the baseline characteristics of the patient, specifically the tendency toward chronic hypercapnia and hypoxia.
- Look for the direction of change required: "toward respiratory acidosis" means a lower pH and a higher PaCO₂ level.
- Use the numeric criteria for respiratory failure, which generally includes a PaO₂ < 60 mm Hg and a PaCO₂ > 50 mm Hg.
- Rule out options that show alkalotic pH values or normal oxygenation levels, as these do not fit the failure criteria.
Take home points
- Respiratory failure is defined by a PaO₂ ≤ 60 mm Hg or a PaCO₂ ≥ 50 mm Hg with pH < 7.35.
- Chronic COPD patients often have compensated respiratory acidosis where the pH remains in the low-normal range.
- An acute rise in PaCO₂ without a corresponding rise in bicarbonate results in a dangerous drop in pH.
- Severe hypoxia in COPD is often driven by V/Q mismatch and increased dead space ventilation.
A nurse is teaching a client with moderate COPD strategies to improve breathing. The nurse wants to show a technique that promotes effective exhalation. Which of the following interventions should the nurse recommend?
Explanation
Effective exhalation in the setting of obstructive pulmonary disease is frequently compromised by premature airway collapse during the expiratory phase of the respiratory cycle. This phenomenon occurs because the loss of elastic recoil and increased airway resistance shift the equal pressure point toward the smaller, non-cartilaginous bronchioles. By increasing the back pressure within the tracheobronchial tree, patients can mechanically stent these airways open for a longer duration. This physiologic adjustment facilitates the evacuation of trapped air.
Rationale for correct answer
3. The technique of pursed lip breathing is specifically designed to create positive expiratory pressure that prevents the early closure of terminal bronchioles. This prolonged effective exhalation allows for a more complete emptying of the alveoli, which directly reduces the work of breathing and improves the overall oxygenation status of the client.
Rationale for incorrect answers
1. The technique known as huff coughing is a forced expiratory maneuver primarily used to mobilize and expectorate secretions from the central airways rather than to promote steady exhalation. While it is an essential part of airway clearance therapy, it does not provide the continuous back pressure needed to prevent the alveolar air trapping seen in chronic obstructive lung conditions.
2. Utilizing thoracic breathing is generally discouraged in patients with chronic lung disease because it relies heavily on accessory muscles and is often inefficient. This shallow, upper-chest movement increases the energy expenditure of the patient without effectively addressing the need for prolonged expiration or the reduction of hyperinflation within the lower lung lobes.
4. While diaphragmatic breathing is a helpful strategy for improving the efficiency of the primary respiratory muscle and reducing the use of accessory muscles, it focuses primarily on the inspiratory phase. It does not provide the specific pressure gradient at the lips necessary to stent the airways open during exhalation, which is the functional goal described in the question.
Test-taking strategy
- Focus on the specific goal identified in the question, which is "effective exhalation" and the prevention of airway collapse.
- Connect the pathophysiology of air trapping in COPD to the mechanical solution of providing back pressure through the mouth.
- Differentiate between clearing secretions (huff coughing), muscle efficiency (diaphragmatic), and airway stenting (pursed lip).
- Select the intervention that directly counteracts the dynamic compression of airways that occurs when a patient with COPD exhales too quickly.
Take home points
- Pursed lip breathing increases airway pressure during expiration to prevent premature airway collapse.
- This technique effectively reduces the respiratory rate and helps control the sensation of dyspnea.
- Diaphragmatic breathing focuses on strengthening the diaphragm and improving the depth of inspiration.
- Effective exhalation is critical for reducing hyperinflation and improving the exchange of fresh atmospheric gases.
A nurse is reviewing the pathophysiology of COPD with a client and discussing potential complications. The nurse explains that certain physiological changes can lead to cor pulmonale. What causes the pulmonary vasoconstriction that may result in this condition?
Explanation
Cor pulmonale is defined as right ventricular hypertrophy and eventual failure resulting from primary disorders of the respiratory system or the pulmonary vasculature. In chronic obstructive pulmonary disease, the progressive destruction of the alveolar-capillary membrane reduces the total cross-sectional area of the vascular bed, increasing resistance to blood flow. This anatomical loss is compounded by a potent physiological reflex known as hypoxic vasoconstriction, where the precapillary sphincters constrict to divert blood away from poorly ventilated areas. This sustained increase in afterload forces the right ventricle to work against higher pressures, eventually leading to myocardial remodeling and clinical signs of systemic venous congestion.
Rationale for correct answer
2. The presence of sustained alveolar hypoxia and significant hypercapnia triggers the myogenic response of the pulmonary arterial smooth muscle, leading to widespread vasoconstriction. This physiological mechanism, intended to optimize ventilation-perfusion matching, becomes maladaptive when it occurs globally, resulting in pulmonary hypertension and the subsequent development of right-sided heart failure.
Rationale for incorrect answers
1. While chronic hypoxemia stimulates erythropoietin production and causes polycythemia, the increased viscosity of the blood is a secondary factor that contributes to workload rather than the primary cause of vasoconstriction. The actual narrowing of the vascular lumen is a direct response to gas exchange abnormalities rather than the thickness of the blood flowing through the vessels.
3. Utilizing long-term low-flow oxygen therapy is actually a treatment modality intended to prevent or mitigate the progression of cor pulmonale by reducing hypoxic pulmonary vasoconstriction. By improving the oxygen tension within the alveoli, this therapy helps to relax the pulmonary vasculature and decrease the workload placed upon the right ventricle.
4. The administration of high concentrations of oxygen to a patient with chronic hypercapnia may suppress the respiratory drive, but it does not cause pulmonary vasoconstriction. In fact, oxygen acts as a pulmonary vasodilator, and the primary risk of high-flow oxygen in this population is the worsening of respiratory acidosis rather than the induction of cor pulmonale.
Test-taking strategy
- Identify the trigger for right-sided heart failure in lung disease, focusing on what happens to the pulmonary arteries.
- Differentiate between the mechanical cause of the problem (vasoconstriction) and the secondary compensatory mechanisms (polycythemia).
- Recognize that hypoxia is the most powerful natural stimulus for the constriction of pulmonary vessels.
- Rule out treatments (oxygen therapy) as the cause of the pathology, as these are typically implemented to reverse the underlying vasoconstrictive state.
Take home points
- Cor pulmonale is right heart failure caused by pulmonary hypertension secondary to lung disease.
- Alveolar hypoxia is the primary stimulus for the vasoconstriction that increases pulmonary vascular resistance.
- Chronic hypercapnia and acidosis further sensitize the pulmonary vasculature to the effects of hypoxia.
- Management focuses on improving oxygenation to reduce pulmonary arterial pressures and unloading the right ventricle.
A nurse plans to teach a client how to perform pursed-lip breathing. Which instruction should be included?
Explanation
Pursed-lip breathing creates a resistive orifice, maintaining positive pressure throughout the expiratory phase. This technique prevents early airway collapse by stenting open non-cartilaginous bronchioles. Consequently, it facilitates the evacuation of trapped gas, effectively reducing dynamic hyperinflation and the overall sensation of dyspnea during physical exertion or acute respiratory distress.
Rationale for correct answer
3. The nurse must instruct the client to inhale slowly through the nose to ensure the air is properly warmed and filtered while preventing the turbulent flow associated with rapid gasping. This controlled inspiratory phase sets the appropriate respiratory rhythm necessary to transition into the prolonged, resistive expiratory phase that defines the therapeutic benefit of this specific breathing maneuver.
Rationale for incorrect answers
1. The client should be taught to avoid the instruction to breathe in through the mouth, especially when performed quickly, as this can lead to shallow ventilation and increased aerophagia. Inhaling through the nasal passages is preferred because it utilizes the natural humidification and filtration functions of the upper respiratory tract while promoting a more relaxed breathing pattern.
2. Instructing the client to place one hand over the abdomen is the hallmark of teaching diaphragmatic or abdominal breathing rather than the specific technique of pursed-lip breathing. While both methods are often used together in pulmonary rehabilitation, the abdominal hand placement is specifically intended to provide sensory feedback for diaphragm excursion rather than controlling expiratory airway pressures.
4. The patient should specifically avoid the instruction to puff out the cheeks during the expiratory phase of the exercise, as this indicates unnecessary facial muscle tension. Proper technique involves keeping the cheeks relaxed while the air is firmly exhaled through tightly pressed lips, ensuring that the resistance is generated at the orolabial interface rather than within the buccal cavity.
Test-taking strategy
- Identify the specific technique being taught and recall the exact procedural steps required for its correct execution.
- Distinguish between pursed-lip breathing (focused on expiration and airway stenting) and diaphragmatic breathing (focused on inspiration and muscle efficiency).
- Eliminate options that describe incorrect mechanics, such as breathing through the mouth or using improper facial muscle tension.
- Select the step that represents the standardized beginning of a controlled respiratory cycle for patients with obstructive disease.
Take home points
- Pursed-lip breathing should begin with a slow, deep inhalation through the nose with the mouth closed.
- The exhalation phase should be at least twice as long as the inhalation phase to maximize air evacuation.
- This technique prevents the collapse of small airways by maintaining positive pressure during the expiratory cycle.
- Clients should be coached to exhale as if they are whistling or flickering a candle flame without blowing it out
Practice Exercise 3
A nurse is teaching a client with COPD about a newly prescribed albuterol (Proventil). Which statement by the client demonstrates correct understanding of the medication?
Explanation
Albuterol is a selective beta2-adrenergic agonist that induces bronchial smooth muscle relaxation. It works by stimulating adenyl cyclase to increase cyclic AMP levels, effectively reversing bronchoconstriction during acute exacerbations. However, higher doses can lose selectivity, affecting cardiac receptors and causing transient systemic side effects during clinical respiratory therapy.
Rationale for correct answer
3. Albuterol primarily targets beta2 receptors but can stimulate beta1 receptors in the heart, leading to a faster heart rate or palpitations. This is a common and expected sympathomimetic side effect that the nurse must include in the patient education to prevent unnecessary anxiety during medication use.
Rationale for incorrect answers
1. Systemic corticosteroids are well-known to increase blood glucose levels, but short-acting beta2 agonists like albuterol do not typically have this metabolic effect. Therefore, the client's statement regarding hyperglycemia is clinically incorrect for this specific rescue inhaler and would indicate a need for further medication clarification.
2. Unlike inhaled or systemic corticosteroids which can cause localized or systemic immune suppression, albuterol does not impair the body’s defenses. It is a bronchodilator with no anti-inflammatory or immunosuppressive properties, making this statement an incorrect understanding of how the drug affects the client's overall health.
4. Development of mouth sores or oral candidiasis is a classic side effect associated with inhaled corticosteroids, not bronchodilators like albuterol. These fungal infections occur due to local immunosuppression in the oropharynx, whereas albuterol’s side effect profile is primarily related to nervous system and cardiovascular stimulation.
Test-taking strategy
- Identify the drug class of albuterol as a sympathomimetic bronchodilator and recall its common side effects.
- Differentiate between the effects of bronchodilators (tachycardia, tremors) and inhaled corticosteroids (thrush, immune suppression).
- Recognize that sympathetic nervous system activation naturally results in an increased heart rate and potentially mild tremors.
- Rule out metabolic or immunological changes that are characteristic of different classes of respiratory medications like steroids.
Take home points
- Albuterol is a rescue medication used for rapid relief of acute bronchospasm in obstructive lung diseases.
- Common side effects include tachycardia, palpitations, tremors, and occasionally a sense of nervousness or anxiety.
- Use of albuterol can cause a temporary shift of potassium into cells, potentially leading to mild hypokalemia.
- Clients should be taught to monitor their pulse and report any significant or persistent cardiac palpitations.
A nurse is educating a client on the proper use of an incentive spirometer. Which statement made by the client indicates correct understanding of the instructions?
Explanation
Incentive spirometry utilizes sustained maximal inspiration to increase transpulmonary pressure and inspiratory volumes. This mechanical intervention promotes alveolar expansion, effectively reversing atelectasis by facilitating collateral ventilation through the pores of Kohn. Improved surfactant distribution and gas exchange make it a critical tool in postoperative pulmonary hygiene.
Rationale for correct answer
4. The client must inhale deeply and perform a brief end-inspiratory pause to stabilize the distal air spaces for maximal recruitment. This hold of the breath ensures the inspired air distributes evenly throughout the lung parenchyma. Such action maximizes the therapeutic effect on pulmonary expansion.
Rationale for incorrect answers
1. The client is confusing the incentive spirometer with a pulse oximeter, which non-invasively monitors arterial oxygen saturation. An incentive spirometer is a mechanical breathing tool requiring active patient participation through inhalation. It is not a passive sensor attached to the finger or earlobe.
2. Patients should be positioned in a high-Fowler or semi-Fowler position to allow for maximum diaphragmatic excursion and chest wall expansion. Recumbent positioning increases abdominal pressure against the diaphragm. This significantly hinders the patient's ability to achieve the deep inspiratory volumes required for effective therapy.
3. Placing a hand over the abdomen is a technique used in diaphragmatic breathing to monitor muscle movement. It does not add resistance to the incentive spirometer. The device provides visual feedback for flow, and manual resistance would be counterproductive to achieving a slow, deep inspiratory effort.
Test-taking strategy
- Identify the primary goal of the incentive spirometer as encouraging deep inhalation to prevent or treat atelectasis.
- Distinguish between inhalation (correct for spirometry) and exhalation (correct for peak flow meters or pursed-lip breathing).
- Rule out positioning errors because upright posture is essential for optimal lung expansion and diaphragmatic movement.
- Connect the concept of collateral ventilation to the need for a sustained breath-hold at the peak of inspiration.
Take home points
- The incentive spirometer is used to encourage voluntary, deep, and sustained inhalation.
- Patients should be instructed to perform 5 to 10 repetitions every hour while awake to prevent respiratory complications.
- A visual indicator on the device helps the patient maintain a slow and steady inspiratory flow rate.
- Effective use requires an upright sitting position and a tight seal around the mouthpiece to ensure accurate volume measurement.
A nurse is teaching a client about oxygen delivery systems. The nurse asks which feature is characteristic of a partial rebreathing mask.
Explanation
A partial rebreathing mask is an oxygen-delivery device that provides moderate to high concentrations of oxygen (≈40–70%) at flow rates of 6–10 L/min. It has a reservoir bag without one-way valves, allowing the client to rebreathe the first portion of exhaled air (rich in oxygen) while preventing carbon dioxide accumulation when used correctly.
Rationale for correct answer
2. The defining characteristic of a partial rebreathing mask is the reservoir bag, which collects the first third of the client's exhaled air. Because this initial portion of exhaled air comes from the anatomic dead space, it is rich in oxygen and lacks carbon dioxide, allowing it to be re-inhaled alongside fresh oxygen. This mechanism significantly increases the inspired oxygen concentration compared to a standard simple mask.
Rationale for incorrect answers
1. Partial rebreathing masks are generally used for short-term therapy in patients who require higher oxygen concentrations during acute respiratory distress. They are not suitable for long-term therapy because the mask is hot, confining, and interferes with essential activities like eating and talking. Long-term management typically utilizes more stable and comfortable devices like a nasal cannula.
3. The non-rebreather mask, not the partial rebreather, provides the highest oxygen concentrations (up to 90% to 100%). The non-rebreather is equipped with one-way valves that prevent any exhaled air from entering the reservoir bag and prevent room air from entering the mask. The partial rebreather allows some mixing of air, resulting in a lower fraction of inspired oxygen (FiO2).
4. The nasal cannula is the device that is most comfortable and causes the least restriction on the patient's activities. It allows the client to eat, drink, and speak without interrupting the oxygen flow. Masks, by contrast, are more restrictive and can cause skin breakdown over the bridge of the nose and behind the ears during prolonged use.
Test-taking strategy
- Differentiate between the Partial Rebreather (no valves) and the Non-Rebreather (one-way valves) to identify which provides higher FiO2.
- Associate the term "Reservoir" with masks designed to deliver oxygen concentrations between 40% and 70%.
- Evaluate the patient's activity level; if they need to eat, a mask is never the "most comfortable" or "least restrictive" choice.
- Remember that any device with a bag must have the flow rate high enough (usually 6 to 15 L/min) to keep the bag from collapsing during inspiration.
Take home points
- A partial rebreather delivers an FiO2 of approximately 40% to 70%.
- The reservoir bag must remain at least one-third to one-half full on inspiration to ensure the patient receives the intended dose.
- Partial rebreathers do not have the one-way valves found on non-rebreather masks, allowing the "partial rebreathing" of dead-space air.
- Close monitoring for skin irritation and proper mask seal is required to maintain therapeutic oxygen levels.
A nurse is planning postural drainage for a client with COPD. The nurse considers which actions are essential to ensure safety and effectiveness during the procedure.
Explanation
Postural drainage utilizes specific body positions to harness gravity for the clearance of tracheobronchial secretions. Segmental bronchi are aligned vertically to facilitate the movement of mucus from peripheral lung fields toward the central airways. This mechanical intervention is essential for managing mucus hypersecretion and preventing secondary bacterial colonization in patients with impaired mucociliary clearance or chronic obstructive lung disease.
Rationale for correct answer
3. The nurse must prioritize the assessment of the patient's tolerance for Trendelenburg or head-down positions to prevent dangerous complications. Significant physiological stress from these positions can increase intracranial pressure or cause severe dyspnea. This safety evaluation is the most critical step before beginning the drainage procedure for a compromised client.
Rationale for incorrect answers
1. Standard nursing protocols typically recommend scheduling the procedure at least 2 hours after meals to minimize the risk of vomiting or aspiration. A timeframe of only 1 hour after a meal is insufficient and could lead to gastric distress. Positional changes require an empty stomach to ensure patient safety and comfort.
2. Effective airway clearance requires the patient to remain in the drainage position for several minutes to allow gravity to mobilize the secretions. A cough before positioning is counterproductive because the mucus has not yet moved into the larger, central airways. The final step of the procedure should be expectoration once secretions have migrated.
4. The correct clinical sequence requires the nurse to place the patient in the appropriate positioning first before applying manual techniques like percussion or vibration. These adjunctive maneuvers are specifically designed to shake secretions loose while the lung segment is superior to the carina. This ensures that the loosened mucus moves toward the trachea immediately.
Test-taking strategy
- Identify the safety priority among the options, as nursing questions often emphasize the assessment of patient stability and risk reduction.
- Recognize that gravity is the primary driver of postural drainage, meaning positioning must occur before manual techniques like vibration.
- Apply knowledge of gastric emptying to rule out timing that occurs too soon after a meal.
- Distinguish between the functional goal of the procedure and the final step of coughing to expectorate.
Take home points
- Postural drainage positions are held for 3 to 15 minutes to allow gravity to mobilize secretions.
- Head-down positions are contraindicated in patients with increased intracranial pressure, heart failure, or severe hypertension.
- Percussion and vibration should be performed during the drainage session to enhance mucus movement.
- Always encourage the patient to perform huff coughing or a deep cough after the drainage is complete.
A nurse is caring for a client experiencing an acute exacerbation of mild COPD. The nurse identifies ineffective breathing pattern related to airway obstruction and anxiety. What is the best immediate action for the nurse to take?
Explanation
Acute exacerbations induce severe airway resistance and dynamic hyperinflation, significantly increasing the work of breathing. Patients often adopt the tripod position to optimize the mechanical advantage of the diaphragm and accessory muscles. This posture stabilizes the pectoralis muscles to assist in thoracic expansion while reducing the metabolic demand of ventilation.
Rationale for correct answer
4. Upright positioning with the elbows resting on an over-the-bed table facilitates the use of accessory muscles and improves diaphragmatic excursion. This immediate intervention provides the fastest mechanical relief for dyspnea by maximizing thoracic volume. Correct posture also helps stabilize the patient and reduces the anxiety associated with the feeling of suffocation.
Rationale for incorrect answers
1. Administration of routine medications is a necessary component of long-term management but does not address the immediate, acute distress. The nurse must prioritize non-pharmacological stabilization techniques that offer instant relief before waiting for the onset of pharmacological agents. Routine orders may not be sufficient during an acute exacerbation requiring rapid stabilization.
2. Chest physiotherapy is an intensive procedure that can actually increase the oxygen demand and worsen the anxiety of a patient. Such techniques are generally reserved for periods of stability to manage chronic secretions. Performing percussion during an active dyspneic episode can further compromise the patient’s limited respiratory reserve and increase the physical workload.
3. Delivery of oxygen at 5 L/min is inappropriately high for a COPD patient and carries the risk of suppressing the hypoxic respiratory drive. Excessive oxygenation can lead to carbon dioxide retention and worsening respiratory acidosis. Oxygen therapy must be titrated carefully to maintain a saturation between 88% and 92% rather than using high flow rates.
Test-taking strategy
- Identify the immediate nursing action that provides the fastest relief for an ineffective breathing pattern and anxiety.
- Choose the least invasive and most rapid physiological intervention, which is typically repositioning the patient.
- Recall the contraindications of high-flow oxygen in COPD patients to eliminate unsafe interventions.
- Distinguish between acute stabilization maneuvers and chronic maintenance therapies like chest physiotherapy.
Take home points
- The tripod position helps stabilize the shoulder girdle to allow accessory muscles to assist in ventilation.
- Upright positioning reduces the pressure of abdominal organs against the diaphragm to improve tidal volume.
- High-flow oxygen is avoided in COPD to prevent the loss of the stimulus to breathe.
- Immediate nursing care focuses on reducing the work of breathing and calming the patient’s anxiety.
Comprehensive Questions
A nurse is preparing to give a newly prescribed dose of prednisone (Deltasone) to a client with COPD. Which findings should the nurse assess for? Select all that apply
Explanation
Prednisone is a potent glucocorticoid utilized to reduce the significant airway inflammation associated with acute pulmonary exacerbations. These systemic steroids mimic endogenous cortisol, influencing the metabolism of carbohydrates, proteins, and fats while suppressing the immune response. High-dose administration often results in mineralocorticoid effects, leading to significant shifts in fluid and electrolyte balances.
Rationale for correct answers
1. The nurse must assess the client for low potassium levels because glucocorticoids promote the renal excretion of potassium. This kaliuretic effect can lead to hypokalemia, which increases the risk of cardiac arrhythmias and muscle weakness, especially in patients also taking potassium-wasting diuretics or beta-agonists.
3. Clinical monitoring for fluid retention is essential due to the sodium-retaining properties of systemic corticosteroids. Prednisone causes the kidneys to reabsorb sodium and water, potentially leading to edema, weight gain, and hypertension. These complications can further strain the cardiovascular system of a patient with chronic lung disease.
5. Clients must be instructed to report dark, tarry stools as prednisone increases the risk of gastrointestinal ulceration and occult bleeding. Glucocorticoids inhibit the synthesis of protective prostaglandins in the gastric mucosa. Such inhibition makes the patient highly susceptible to peptic ulcers and subsequent hemorrhage.
Rationale for incorrect answers
2. An increased heart rate is not a primary side effect of prednisone; rather, it is more commonly associated with bronchodilators like albuterol. Fluid overload from steroid-induced retention could eventually increase cardiac work, but tachycardia is not a direct pharmacological expectation of glucocorticoid administration.
4. Some gastric irritation may occur, but nausea is not a classic hallmark or a priority assessment finding specifically linked to the systemic action of prednisone. The more critical gastrointestinal concern involves the actual ulceration and bleeding of the mucosal lining rather than transient feelings of nausea.
Test-taking strategy
- Focus on the multi-system impact of steroids, particularly the "S" side effects: sugar, salt, and stomach.
- Connect the mineralocorticoid effect of prednisone to the renal handling of electrolytes like sodium and potassium.
- Identify that bleeding risks are a major priority in pharmacological nursing assessments, making the monitoring of stool color a critical intervention.
- Distinguish between the cardiovascular stimulants (beta-agonists) and the metabolic agents (corticosteroids) to avoid misattributing tachycardia.
Take home points
- Prednisone should be taken with food to minimize the risk of gastric irritation and potential ulcer formation.
- Regular monitoring of serum glucose is necessary, as steroids can induce or worsen diabetes mellitus.
- Tapering the dose is required after long-term use to prevent acute adrenal insufficiency or "addisonian crisis."
- Daily weights are a practical way for patients to monitor for significant fluid retention and edema at home.
A nurse is developing a plan of care for a client with COPD. Which interventions should be included to help manage symptoms and maintain lung function? Select all that apply
Explanation
Comprehensive management of chronic obstructive pulmonary disease focuses on optimizing functional status and minimizing airway collapse. Physical conditioning improves peripheral muscle efficiency, reducing the ventilatory demand during exertion. Targeted breathing techniques provide the mechanical backpressure necessary to stent open smaller airways, which effectively mitigates the destructive consequences of dynamic hyperinflation.
Rationale for correct answers
1. Regular exercise, particularly walking, is essential to prevent physical deconditioning and improve the oxidative capacity of skeletal muscles. This intervention enhances the patient's functional independence and quality of life, as better-conditioned muscles require less oxygen for the same amount of physical work, thereby reducing the workload on the heart and lungs.
5. Targeted breathing exercises, such as pursed-lip breathing, are fundamental for managing the expiratory airflow limitation characteristic of the disease. These techniques prolong the expiratory phase, facilitating more complete alveolar emptying and reducing the residual volume that leads to the distressing sensation of breathlessness during activities of daily living.
Rationale for incorrect answers
2. Delivery of oxygen at a high flow rate is contraindicated for most patients with chronic obstructive disease due to the risk of oxygen-induced hypercapnia. Excessive oxygen can dampen the hypoxic drive to breathe, leading to dangerous levels of carbon dioxide retention and acute respiratory acidosis rather than maintaining stable lung function.
3. Routine use of long-term oral corticosteroids is generally avoided because the risk of systemic side effects outweighs the clinical benefits for stable patients. These medications cause osteoporosis, hyperglycemia, and muscle wasting; therefore, clinicians typically reserve them for the management of acute exacerbations rather than using them as a maintenance therapy.
4. Monitoring with a peak flow meter is primarily a strategy for managing asthma rather than assessing the slow, progressive decline of COPD. Clinicians utilize spirometry to track disease progression, as peak flow measurements focus on the initial burst of expiration and do not accurately reflect the overall airflow limitation present in chronic obstructive patients.
Test-taking strategy
- Identify interventions that improve functional capacity without introducing significant systemic risks or side effects.
- Differentiate between asthma monitoring tools (peak flow) and COPD assessment standards (spirometry).
- Recall the respiratory drive physiology in chronic lung disease to recognize the dangers of high-flow oxygen administration.
- Select treatments that address the underlying mechanical issues of the disease, such as air trapping and muscle deconditioning.
Take home points
- Exercise training remains the cornerstone of pulmonary rehabilitation to improve cardiovascular and muscular efficiency.
- Pursed-lip breathing helps maintain positive airway pressure, preventing premature closure of the bronchioles during exhalation.
- Systemic steroids are restricted to short-term use during exacerbations to avoid multi-system complications.
- Oxygen therapy should be carefully titrated to target a saturation of 88% to 92% in chronic CO2 retainers.
A client with COPD is being discharged and expresses concern that continuous oxygen therapy will prevent them from leaving home. Which response by the nurse is most appropriate?
Explanation
Modern pulmonary rehabilitation emphasizes maintaining social engagement and physical mobility for patients with chronic lung disease. Continuous oxygen therapy is often prescribed to maintain arterial saturation and reduce the cardiac workload associated with chronic hypoxemia. Technological advancements in medical equipment now provide options that accommodate an active lifestyle while ensuring the delivery of necessary supplemental oxygen.
Rationale for correct answer
1. Portable oxygen systems, including lightweight cylinders and portable oxygen concentrators, are specifically designed to allow clients to maintain their independence. The nurse must provide this information to alleviate the client's anxiety and promote psychosocial well-being. Informing the client about these resources ensures they understand that life-sustaining therapy does not necessitate total home confinement.
Rationale for incorrect answers
2. Instructing a client that they can simply remove your oxygen when leaving home is dangerous and medically unsound advice. For those requiring continuous therapy, even brief periods of desaturation can lead to significant hypoxemia, increased pulmonary hypertension, and cardiac strain. The therapy must be maintained as prescribed by the healthcare provider to remain effective and safe.
3. Telling a client they will not be able to go out as often is a discouraging and potentially inaccurate statement that can lead to depression and social isolation. Such a response ignores the existence of modern mobility aids and fails to address the client's need for a quality of life that includes community participation. This approach does not fulfill the nurse's role in health promotion.
4. Suggesting that home health care replaces the need to leave the house inappropriately limits the client's autonomy and social life. While home health services are valuable for monitoring, they do not satisfy the client's desire for recreational or social outings. The nurse should focus on empowering the client to navigate the world with their equipment rather than encouraging a sedentary, housebound existence.
Test-taking strategy
- Prioritize responses that promote independence and quality of life while adhering to the medical treatment plan.
- Eliminate options that suggest non-compliance with a physician's orders, such as removing oxygen during activity.
- Avoid answers that are pessimistic or dismissive of the client's concerns regarding their lifestyle and social integration.
- Recognize that technological solutions are often the key to balancing medical needs with personal freedom in chronic disease management.
Take home points
- Portable oxygen concentrators (POCs) can run on battery power and are approved for use in cars and on airplanes.
- Liquid oxygen systems provide a high volume of oxygen in a small, lightweight container for longer outings.
- Patients should be taught to plan their trips by checking battery life or tank duration before leaving home.
- Social interaction and moderate physical activity are essential components of a successful COPD management plan.
A nurse is caring for a client diagnosed with COPD. The nurse reviews the client’s treatment plan and considers interventions beyond smoking cessation. Which treatment is included to help slow the progression of the disease?
Explanation
Chronic obstructive pulmonary disease involves a cycle of inflammation and structural damage that worsens over time. Frequent acute exacerbations accelerate the decline in lung function by triggering systemic inflammatory responses and further damaging the lung parenchyma. Infection prevention strategies are fundamental because they reduce the frequency of these destructive clinical events and preserve existing respiratory reserve.
Rationale for correct answer
4. The prevention of respiratory tract infections through vaccinations and hygiene is a primary intervention to slow disease progression. Each exacerbation caused by a viral or bacterial infection leads to a permanent loss of FEV1 and lung capacity. Reducing the incidence of these infections directly protects the remaining healthy tissue and stabilizes the overall clinical course.
Rationale for incorrect answers
1. Routine bronchodilator drugs are essential for symptom management and improving the patient's daily quality of life. These medications do not alter the underlying inflammatory process or prevent the progressive destruction of the alveolar walls. While they make breathing easier by relaxing smooth muscles, they do not stop the long-term decline in pulmonary function.
2. Regular inhaled corticosteroids help manage chronic inflammation and are often used to reduce the frequency of exacerbations in severe cases. These agents do not provide a cure or definitively stop the natural history of the disease's progression. Their role is focused more on stability and symptom control rather than reversing the permanent structural changes typical of obstructive disease.
3. Selected patients may undergo lung volume–reduction surgery to improve chest wall mechanics and reduce air trapping. This procedure is a palliative intervention designed to improve functional status and reduce the work of breathing in specific disease phenotypes. It does not stop the underlying pathological process or prevent the disease from advancing in the remaining lung tissue.
Test-taking strategy
- Distinguish between symptomatic relief (bronchodilators) and interventions that address the causes of rapid decline (infections).
- Identify exacerbations as the major driver of disease acceleration in chronic obstructive pulmonary disorders.
- Recognize that prevention of secondary complications is often the most effective way to preserve organ function over time.
- Rule out surgical or pharmacological treatments that focus on mechanics rather than the biological progression of the pathology.
Take home points
- Annual influenza and regular pneumococcal vaccinations are critical for all patients with chronic lung disease.
- Prompt treatment of respiratory symptoms can prevent a mild infection from becoming a severe exacerbation.
- Hand hygiene and avoiding large crowds during flu season are simple yet effective preventative measures.
- Maintaining overall health through nutrition and hydration supports the immune system in fighting off potential pathogens.
A nurse is caring for a client with COPD. The nurse wants to determine which oxygen delivery system is safest for this client. Which oxygen delivery method is most appropriate?
Explanation
Precise oxygen delivery is vital for patients whose respiratory drive depends on low arterial oxygen levels rather than carbon dioxide. Excessive oxygenation can cause hypercapnia by blunting this hypoxic drive and worsening ventilation-perfusion mismatch. This specific delivery system ensures a consistent fraction of inspired oxygen (FiO2) despite varying patient respiratory rates or tidal volumes.
Rationale for correct answer
1. The Venturi mask is considered the safest system because it delivers a precise, high-flow concentration of oxygen. Large volumes of room air mix with a specific oxygen flow to provide an exact FiO2 through entrainment ports. This accuracy prevents the accidental administration of excessive oxygen. Such precision protects the client from CO2 retention and respiratory depression.
Rationale for incorrect answers
2. A nasal cannula is commonly used for stable patients but is less precise than a Venturi mask. Flow rates of 1 to 6 liters per minute result in an estimated oxygen concentration that varies significantly based on the patient's breathing pattern. Mouth breathing or rapid respirations change the actual percentage of oxygen delivered. This variability makes it less ideal for those requiring strict titration.
3. Use of a simple face mask is generally avoided in this population due to the lack of precision and the higher flow rates required. These masks must operate at 5 to 10 liters per minute to prevent the rebreathing of exhaled carbon dioxide. This flow often exceeds the safe limit for a client who is a chronic CO2 retainer.
4. The non-rebreathing mask delivers the highest possible oxygen concentration, often between 60% and 90%. Such high levels are typically reserved for emergencies or acute respiratory failure rather than routine COPD management. Administering this much oxygen to a COPD client would likely suppress their drive to breathe and cause dangerous carbon dioxide narcosis.
Test-taking strategy
- Select the device that offers the most precise control over oxygen concentration for patients with chronic lung disease.
- Recall that the Venturi effect allows for specific FiO2 settings that remain stable regardless of how the patient breathes.
- Recognize that high-flow devices like non-rebreathers are dangerous for chronic retainers unless an emergency occurs.
- Differentiate between low-flow systems (cannula) and high-flow precision systems (Venturi) when accuracy is the priority.
Take home points
- The Venturi mask is the gold standard for delivering precise oxygen to patients with COPD.
- Proper function requires the entrainment ports to remain unobstructed by bed linens or clothing.
- Oxygen concentrations for a Venturi mask typically range from 24% to 50% depending on the adapter used.
- Monitoring arterial blood gases remains the most accurate way to assess the patient's response to oxygen therapy.
A nurse is preparing a client for discharge with home oxygen therapy using an O₂ concentrator and a portable O₂-conserving unit. The nurse wants to teach the client how to use the equipment safely and effectively. What should the nurse include in the teaching?
Explanation
Home oxygen concentrators provide a reliable solution for long-term respiratory support by filtering nitrogen from ambient air. This technology ensures an uninterrupted supply of medical-grade oxygen without the need for frequent heavy tank deliveries. Effective education empowers the client to manage their chronic condition independently while ensuring the safety and efficiency of the prescribed therapy.
Rationale for correct answer
3. The nurse must explain that the unit concentrates O2 from the room air to provide a continuous and virtually limitless supply of oxygen. This eliminates the anxiety and logistical burden of managing heavy pressurized tanks. Understanding the mechanical function helps the client realize why the machine must remain plugged in and situated in a well-ventilated area for optimal performance.
Rationale for incorrect answers
1. Stating that the portable unit will last exactly 6 to 8 hours is potentially inaccurate and unsafe because the duration depends entirely on the flow rate and the client's activity level. Battery life for portable concentrators or the volume of small cylinders varies significantly. The nurse should teach the client how to calculate duration based on their specific equipment and prescribed settings.
2. Defining the unit as strictly for portable or emergency use is incorrect for a home concentrator, which serves as the primary source of stationary oxygen. While portable oxygen-conserving devices are for travel, the main concentrator is the stationary hub of the home therapy system. This statement would confuse the client regarding which device provides their routine daily oxygen.
4. Expecting a weekly delivery of a large cylinder is unnecessary when using a concentrator, as the machine generates its own supply. This description applies to traditional compressed gas systems rather than the modern concentrator technology being discussed. One of the primary advantages of a concentrator is the removal of the need for frequent cylinder exchanges or bulk deliveries.
Test-taking strategy
- Identify the specific technology mentioned in the question—the oxygen concentrator—and recall its unique operational characteristics.
- Distinguish between compressed gas systems (tanks) and extraction systems (concentrators) to rule out delivery-based answers.
- Recognize that duration of oxygen is variable and dependent on usage patterns rather than a fixed number of hours.
- Focus on the environmental source of oxygen for these machines, which is always the surrounding atmospheric air.
Take home points
- Oxygen concentrators require electricity to function and should have a backup power source or emergency tank.
- The intake filter on the concentrator should be cleaned weekly with warm, soapy water to maintain air quality.
- Portable oxygen-conserving devices (PCDs) save oxygen by only delivering a bolus during the inspiratory phase.
- Clients should notify their local power company that life-sustaining medical equipment is in use at their residence.
A nurse is teaching a client with COPD about nutrition to support respiratory function. The nurse wants to identify which dietary modification helps meet the client’s nutritional needs. Which of the following should be included?
Explanation
Chronic obstructive pulmonary disease significantly increases caloric requirements due to the high energy cost of labored breathing. Patients often experience profound dyspnea while eating, which can lead to inadequate intake and progressive weight loss. Nutritional interventions focus on reducing physical exertion during meals and optimizing the metabolic efficiency of the fuels consumed by the body.
Rationale for correct answer
2. The nurse must recommend avoiding foods that require extensive chewing to minimize physical fatigue during the meal. Chewing increases oxygen consumption and can worsen the sensation of breathlessness, leading the client to stop eating before meeting their caloric needs. Providing soft, easy-to-consume foods allows the patient to conserve energy for the vital process of ventilation.
Rationale for incorrect answers
1. A high-carbohydrate diet is generally avoided because the metabolism of carbohydrates produces a higher respiratory quotient compared to fats. This results in the production of more carbon dioxide, which can further strain the respiratory system of a client who already struggles to exhale gas. A higher fat content is often preferred to provide dense calories with less CO2 byproduct.
3. Serving hot foods can actually increase the patient's sense of congestion and trigger coughing or dyspnea due to the steam and intense aromas. Many patients find that cool or room-temperature foods are easier to tolerate and less likely to provoke a respiratory response. This preference helps maintain a steady intake by avoiding triggers that interrupt the eating process.
4. To prevent gastric distension, clients should avoid drinking fluids during their actual meals. A full stomach can push upward against the diaphragm, limiting its movement and making breathing much more difficult during and after eating. Fluids should be consumed between meals to ensure adequate hydration without compromising the space needed for lung expansion.
Test-taking strategy
- Focus on the energy conservation needs of the client, recognizing that even the act of eating can be exhausting.
- Recall the respiratory quotient of different macronutrients to identify why high-fat, low-carbohydrate diets are often beneficial.
- Apply principles of mechanics, knowing that anything increasing abdominal pressure (like fluids with meals) hinders diaphragmatic excursion.
- Choose the option that reduces the physical workload of consuming food while maintaining high nutrient density.
Take home points
- Small, frequent meals (5-6 per day) are better tolerated than three large, heavy meals.
- Resting for 30 minutes before eating can help reduce fatigue and dyspnea during the meal.
- High-protein options help maintain the strength of the respiratory muscles and the immune system.
- Supplemental oxygen may be used during meals if the client's saturation drops significantly while eating.
A nurse is caring for a client with COPD. The nurse wants to determine which intervention can safely be delegated to unlicensed assistive personnel (UAP).
Explanation
Effective clinical management requires the nurse to distinguish between tasks requiring specialized professional judgment and those involving routine physical support. Professional nursing responsibilities include complex assessment, diagnostic reasoning, and the formal education of the patient. Delegation of non-invasive tasks to assistive staff allows the registered nurse to focus on the hemodynamic and respiratory stability of the compromised patient.
Rationale for correct answer
1. The nurse may safely delegate the task to assist the patient out of bed to the unlicensed assistive personnel. This action is a routine part of daily care that does not require clinical assessment or the development of a complex care plan. UAPs are trained to help with ambulation and transfers, provided the patient is hemodynamically stable and the nurse has already assessed the initial risk.
Rationale for incorrect answers
2. To auscultate breath sounds is a component of physical assessment that requires the specialized knowledge of a licensed nurse. Distinguishing between crackles, wheezes, and diminished air entry is a critical skill used to evaluate the pathophysiology of the disease. Unlicensed personnel do not have the training to interpret these sounds or make decisions based on respiratory changes.
3. The nurse must plan patient activities to ensure that the workload does not exceed the patient's limited oxygen supply. This coordination involves evaluating the patient's current endurance levels and medical status to prevent an exacerbation. Such strategic planning is a core nursing function that cannot be assigned to staff who lack a deep understanding of pulmonary physiology.
4. To teach the patient a clinical skill like pursed-lip breathing is a formal educational intervention that belongs solely to the licensed nurse. Education requires assessing the patient's readiness to learn and evaluating the effectiveness of the teaching. These steps are integral to the nursing process and must be performed by a professional capable of modifying the plan based on patient response.
Test-taking strategy
- Apply the five rights of delegation: right task, right circumstance, right person, right direction, and right supervision.
- Remember the acronym TAPE (Teaching, Assessment, Planning, Evaluation) to identify tasks that should never be delegated to a UAP.
- Focus on routine and repetitive tasks like hygiene, feeding, or simple mobility for assistive personnel.
- Recognize that any intervention involving clinical judgment or the interpretation of data must remain with the registered nurse.
Take home points
- UAPs can perform vital signs and document them, but the nurse must interpret the results.
- Delegation requires clear communication regarding the specific limits of the task and when to report findings.
- Safe delegation depends on the nurse first ensuring the patient is medically stable for the activity.
- Activities of daily living (ADLs) are the most common tasks appropriate for unlicensed assistive staff.
A nurse is reviewing medications for a client with COPD. The nurse wants to identify which drug is a dry powder inhaler (DPI) specifically used for COPD.
Explanation
Dry powder inhalers require a forceful, deep inhalation to aerosolize the medication without the use of chemical propellants. This delivery method is highly dependent on the patient's inspiratory flow rate to ensure the drug reaches the peripheral airways. Effective management involves selecting the appropriate device interface to match the patient's physical ability and the specific requirements of the prescribed bronchodilator therapy.
Rationale for correct answer
4. Indacaterol is a long-acting beta2-agonist (LABA) formulated specifically as a dry powder inhaler for the maintenance treatment of airflow obstruction. The Arcapta Neohaler system requires the client to place a capsule into the device, pierce it, and then inhale the powder. This specific DPI technology provides 24-hour bronchodilation and is indicated solely for the treatment of chronic obstructive pulmonary disease.
Rationale for incorrect answers
1. Roflumilast is an oral phosphodiesterase-4 (PDE4) inhibitor rather than an inhaled medication. It is used to reduce the frequency of exacerbations in patients with severe disease associated with chronic bronchitis. Because it is administered as a tablet, it does not utilize any inhaler technology or dry powder delivery systems.
2. While Salmeterol is a LABA that can be delivered via a DPI (Diskus), it is not exclusively used for COPD. It is frequently prescribed for the long-term maintenance of asthma in both pediatric and adult populations. The question asks for a drug specifically used for COPD, whereas salmeterol has broader indications across multiple respiratory conditions.
3. Ipratropium (Atrovent HFA) is a short-acting muscarinic antagonist delivered via a metered-dose inhaler (MDI) rather than a dry powder inhaler. The "HFA" designation indicates the use of hydrofluoroalkane as a propellant to spray the medication. This delivery method is fundamentally different from a DPI, which relies entirely on the patient's own inspiratory effort.
Test-taking strategy
- Identify the delivery system mentioned in the stem (DPI) and eliminate any oral or MDI medications.
- Recognize the "Neohaler" and "Handihaler" suffixes as common indicators of capsule-based dry powder systems.
- Distinguish between drugs that have dual indications (asthma and COPD) and those marketed specifically for one disease.
- Recall that HFA versions of medications always refer to metered-dose inhalers rather than dry powder devices.
Take home points
- Dry powder inhalers do not require the coordination of "press and breathe" associated with MDIs.
- Patients must have sufficient inspiratory flow to effectively draw the powder out of the inhaler.
- Moisture can cause the powder to clump, so DPI devices should never be stored in humid environments like bathrooms.
- Rinsing the mouth after using any inhaler helps prevent local irritation and reduces systemic absorption.
A nurse is counseling the husband of a client with severe COPD who reports that they have not had sexual activity since her diagnosis due to shortness of breath. What is the nurse’s best response to address intimacy concerns?
Explanation
Chronic obstructive pulmonary disease introduces significant physical and psychological barriers to intimacy through decreased stamina and fear of breathlessness. Patients often experience exertional dyspnea that causes them to avoid physical closeness, leading to emotional distance within the relationship. Professional guidance focuses on validating these concerns while offering evidence-based strategies to facilitate continued physical connection and improve the psychosocial quality of life.
Rationale for correct answer
4. The nurse’s best response is to offer a joint consultation to discuss practical modifications that can maintain sexual activity. This approach is holistic and non-judgmental, addressing both the physical limitations and the emotional needs of the couple. By suggesting modifications, the nurse provides hope and professional support. Such a response encourages open communication about a sensitive topic while ensuring that both partners are included in the educational process.
Rationale for incorrect answers
1. Telling the husband to discuss his expectations with his wife is an insensitive approach that places undue pressure on a chronically ill patient. This could increase the wife's anxiety and feelings of inadequacy, potentially worsening her respiratory symptoms. Effective counseling should focus on mutual adaptation and support rather than individual demands or one-sided expectations within the relationship.
2. Suggesting that there are other ways to maintain intimacy is a common but dismissive response that avoids addressing the specific concern about sexual activity. While true, this statement may make the couple feel that their desire for a normal sexual life is being minimized. The nurse should address the actual problem of intercourse directly before pivoting to alternative forms of intimacy.
3. Stating that the wife is no longer capable of sexual activity is factually incorrect and clinically inappropriate. This response reinforces a "sick role" and can lead to unnecessary social and emotional isolation for the patient. Many clients with severe disease can remain sexually active with proper positioning, timing of medications, and the use of supplemental oxygen during physical exertion.
Test-taking strategy
- Select the answer that is the most inclusive of both partners and promotes open communication.
- Avoid responses that are judgmental, dismissive, or medically inaccurate regarding the client's capabilities.
- Look for options that offer specific interventions (modifications) rather than general or vague advice.
- Recognize that sexual health is a legitimate part of a comprehensive nursing assessment and plan of care for chronic conditions.
Take home points
- Couples can schedule sexual activity for times when energy levels are highest, such as during the late morning.
- Using a bronchodilator approximately 30 minutes before activity can help minimize shortness of breath.
- Positions that require less energy and do not put pressure on the chest facilitate better breathing.
- Some patients may benefit from using supplemental oxygen during intimacy to maintain adequate saturation.
A nurse is teaching a client with COPD about physical exercise. Which statement should the nurse include in the teaching?
Explanation
Physical conditioning is a primary component of pulmonary rehabilitation that improves skeletal muscle efficiency and reduces the subjective sensation of dyspnea. Patients with chronic lung disease often avoid exertion due to fear of breathlessness, leading to a cycle of deconditioning and worsening respiratory function. Effective training focuses on pacing and setting realistic expectations for symptom recovery during active movement.
Rationale for correct answer
3. The nurse must explain that shortness of breath is a normal physiological response to exercise but should resolve within five minutes of rest. This guideline helps the patient distinguish between a healthy level of exertion and overexertion. Understanding this recovery window reduces anxiety and provides a practical metric for the patient to use when gauging the intensity of their physical activity.
Rationale for incorrect answers
1. Stating that all patients should be able to walk 20 minutes per day is an overgeneralization that does not account for individual disease severity. Some clients with very severe airflow obstruction may only tolerate a few minutes of activity. Goals must be individualized based on the patient's baseline FEV1 and overall functional status rather than a fixed time limit applied to everyone.
2. A bronchodilator inhaler is typically used before exercise as a prophylactic measure to prevent or minimize broncho-constriction during activity. Using it only after exercise does not help the patient tolerate the physical work while it is occurring. Pre-medication is the preferred strategy to optimize airway patency and increase the patient's overall exercise capacity.
4. Monitoring the heart rate is less effective for COPD patients than assessing the Borg Dyspnea Scale or perceived exertion. Heart rate may be influenced by medications like beta-agonists or the presence of pulmonary hypertension. The most reliable indicator of tolerance in this population is the severity of breathlessness and the time it takes to return to a baseline respiratory state.
Test-taking strategy
- Avoid "absolute" statements that include words like all or always, as medical care must be tailored to the individual.
- Prioritize answers that provide a specific timeframe for evaluating the normal physiological response to stress.
- Recognize that pre-treatment is almost always superior to post-event rescue for predictable triggers like physical exertion.
- Understand that subjective breathlessness is the primary limiting factor for COPD patients, making it a better assessment tool than heart rate.
Take home points
- Patients should be taught to use pursed-lip and diaphragmatic breathing during periods of physical activity.
- Exercise should be performed at least three times a week to maintain the benefits of muscle conditioning.
- Stopping to rest when dyspnea becomes severe is encouraged to prevent total exhaustion or panic.
- Stationary cycling or treadmill walking are excellent low-impact options for improving cardiovascular endurance.
A nurse is reviewing treatment options with a client who has cystic fibrosis. Which intervention is considered the most effective in managing the disease?
Explanation
Cystic fibrosis is a genetic disorder characterized by the production of abnormally thick and tenacious mucus. This viscous secretion obstructs the small airways, leading to chronic infection and progressive bronchiectasis. Airway clearance remains the cornerstone of clinical management because it addresses the fundamental mechanical failure of mucus transport. Regular removal of these secretions significantly reduces the bacterial load and slows the rate of pulmonary decline.
Rationale for correct answer
4. Vigorous and consistent chest physiotherapy is the most effective daily intervention for managing the clinical manifestations of the disease. Percussion, vibration, and postural drainage help move thick mucus from the peripheral lungs into the central airways for expectoration. Such meticulous pulmonary hygiene is essential to prevent the chronic inflammatory cycles that cause permanent tissue destruction and respiratory failure.
Rationale for incorrect answers
1. A heart-lung transplant is an extreme measure reserved for patients in the end stages of respiratory failure. While life-saving for some, it is not a routine management strategy and carries high risks of organ rejection and complications from immunosuppression. It does not treat the underlying genetic defect in other organ systems affected by the disease.
2. The administration of prophylactic antibiotics is controversial and not universally recommended for all patients. While treating active infections is vital, continuous use of antibiotics can lead to the development of multi-drug resistant organisms. Most clinicians prefer to treat acute pulmonary exacerbations with targeted therapy based on culture results rather than relying on chronic prophylaxis.
3. Using nebulized bronchodilators helps relax the smooth muscles of the airways and can improve flow before physiotherapy. These medications do not address the primary problem of mucus viscosity and accumulation. While they are a helpful adjunct, they are not as effective as mechanical clearance techniques in preserving long-term lung function and preventing infectious complications.
Test-taking strategy
- Focus on the underlying pathology of the disease, which is the production of thick, obstructive secretions.
- Select the intervention that most directly addresses the mechanical cause of airway obstruction.
- Distinguish between daily maintenance therapies (physiotherapy) and late-stage or emergency interventions (transplant).
- Recognize that non-pharmacological clearing of the airways is the most critical factor in extending the lifespan of these patients.
Take home points
- Airway clearance should be performed at least twice a day and increased during times of illness.
- Aerobic exercise is an excellent supplement to traditional chest physiotherapy as it helps loosen secretions.
- Newer devices like high-frequency chest wall oscillation vests provide a more independent method of clearance.
- Proper nutrition and pancreatic enzyme replacement are also vital to support the high energy demands of the body.
A nurse is discussing developmental challenges with a young adult client who has cystic fibrosis. Why does meeting the typical developmental tasks of young adulthood become especially difficult for these clients?
Explanation
The transition into young adulthood involves achieving independence, establishing a career, and forming intimate relationships. For individuals with cystic fibrosis, these milestones are complicated by the demanding daily treatment regimen and the physical limitations of their condition. Balancing the developmental goals of autonomy with the necessary reliance on healthcare systems creates a unique psychological and social burden that distinguishes their experience from that of their peers.
Rationale for correct answer
2. Young adults with cystic fibrosis must also adapt to a chronic disease while navigating the standard challenges of their age group. The time-consuming nature of chest physiotherapy, frequent hospitalizations, and the need for meticulous nutritional management can interfere with social activities and career progression. This "dual transition" requires significant emotional resilience and complex time-management skills to integrate medical necessity with a normal adult lifestyle.
Rationale for incorrect answers
1. While some patients may eventually need a lung transplant, this is a specific medical event rather than a broad developmental challenge. The fear or reality of a transplant is a major stressor, but the daily difficulty of young adulthood stems more from the chronic management of the disease and its impact on everyday life choices rather than a single surgical intervention.
3. It is medically inaccurate to state that any children they have will develop cystic fibrosis. Cystic fibrosis is an autosomal recessive disorder; a child only develops the disease if they inherit a mutated gene from both parents. While males with CF are often sterile and females may have decreased fertility, genetic counseling allows for a clearer understanding of reproductive risks rather than a guarantee of transmission.
4. While the illness presents challenges, it is not true that it keeps them from becoming financially independent. Many individuals with cystic fibrosis successfully complete higher education and maintain productive careers. Modern treatments and workplace accommodations allow many patients to achieve financial autonomy, though it may require more strategic planning and energy conservation than for a healthy individual.
Test-taking strategy
- Focus on the psychosocial impact of balancing normal life stages with the burden of a chronic, life-limiting illness.
- Identify and eliminate absolute or factually incorrect statements regarding genetics and financial outcomes.
- Look for the answer that encompasses the broadest range of developmental struggles, such as the overall adaptation to the disease.
- Recognize that the primary challenge for young adults with chronic illness is the integration of their "patient identity" with their "adult identity."
Take home points
- Transition programs help adolescents move from pediatric to adult-centered care to foster independence.
- Support groups provide a vital social outlet for young adults to share experiences regarding dating and career planning.
- Adherence to treatment often declines during young adulthood as individuals prioritize social integration over medical routines.
- Mental health screening is essential, as the stress of managing a chronic illness increases the risk of depression and anxiety.
A nurse is planning care for a client diagnosed with bronchiectasis. Which nursing intervention should be included to support airway clearance and symptom management?
Explanation
Bronchiectasis is a chronic condition characterized by the permanent, abnormal dilation of the bronchi, resulting from recurring inflammation and infection. This structural damage impairs the mucociliary escalator, leading to the pooling of thick, purulent secretions in the weakened airways. Effective clinical management focuses on aggressive bronchial hygiene to prevent the stasis of mucus, which serves as a breeding ground for pathogenic bacteria.
Rationale for correct answer
4. The priority intervention is to promote drainage and removal of mucus to prevent further airway obstruction and secondary infections. Techniques such as chest physiotherapy, postural drainage, and the use of positive expiratory pressure (PEP) devices are essential. Effective clearance of these voluminous secretions reduces the bacterial colonization of the lungs and minimizes the progressive inflammatory damage to the bronchial walls.
Rationale for incorrect answers
1. While comfort is important, the need to relieve or reduce pain is not typically the primary focus for stable bronchiectasis. The disease is characterized more by productive coughing and dyspnea than by acute pain. Nursing care must prioritize the mechanical clearance of the airways, as untreated mucus accumulation is the actual driver of the disease's complications.
2. It is counterproductive to prevent paroxysmal coughing in these clients because coughing is a vital compensatory mechanism for clearing the excessive secretions. Instead of suppressing the cough, the nurse should teach controlled coughing techniques, such as huff coughing. Suppressing the cough reflex would lead to significant mucus retention and an increased risk of pneumonia.
3. Bronchiectasis is a structural lung disease and is not contagious, so the nurse does not need to prevent the spread of the disease to others. Unlike tuberculosis or influenza, the chronic inflammation and bronchial dilation cannot be transmitted between individuals. The nurse should focus on the patient's internal infection control and hygiene rather than public health isolation measures.
Test-taking strategy
- Focus on the structural defect of the disease: dilated, "floppy" airways that cannot clear mucus effectively.
- Choose the intervention that addresses the root cause of the patient's symptoms (mucus stasis).
- Eliminate options that suggest the disease is communicable or that involve suppressing the body's natural clearing mechanisms (the cough).
- Identify that airway clearance is the "gold standard" of care for any obstructive or bronchiectatic pulmonary condition.
Take home points
- Postural drainage utilizes gravity to help move secretions from specific lung segments into the central airways.
- Increased fluid intake (hydration) is necessary to thin thick secretions, making them easier to expectorate.
- Patients with bronchiectasis often require long-term monitoring for colonization by Pseudomonas aeruginosa.
- Smoking cessation is mandatory to prevent further damage to the remaining healthy ciliary function.
A nurse is reviewing airway clearance devices with a client who has difficulty clearing pulmonary secretions. What is the primary principle used by these devices to help mobilize secretions?
Explanation
Airway clearance devices are engineered to overcome the mechanical challenges of thick, retained secretions by modulating intrathoracic pressure. When a patient exhales against a resistance within the device, it creates a backpressure that prevents premature airway closure and stents the bronchioles open. This physiological stabilization allows air to move behind the mucus plugs, effectively pushing them toward the central airways where they can be successfully expectorated.
Rationale for correct answer
4. The primary principle used by these devices is positive expiratory pressure (PEP). As the client exhales into the device, the resistance generates a constant pressure that keeps the airways from collapsing during the expiratory phase. This pressure facilitates the movement of air into collateral ventilation channels, which assists in dislodging and mobilizing mucus from the distal to the proximal airways for easier clearance.
Rationale for incorrect answers
1. While some devices (like the Flutter or Acapella) incorporate vibration or oscillation, this is often a secondary feature rather than the universal primary principle of all such devices. Vibration helps thin the mucus, but without the underlying pressure to keep the airways open, the vibration alone would be significantly less effective at transporting the secretions out of the smaller lung segments.
2. Inhalation therapy, such as the use of nebulized saline or bronchodilators, is a complementary treatment rather than the mechanical principle of the clearance device itself. Inhalation therapy focuses on liquefying secretions or dilating the airways to prepare them for clearance, whereas the devices themselves are specifically designed to manipulate the expiratory flow.
3. Chest physiotherapy (CPT) is a broad clinical category that includes various manual and mechanical techniques, including percussion and postural drainage. While airway clearance devices are often used as a component of CPT, they are not the physiotherapy itself; rather, they are the specific tools that utilize pressure to achieve the goal of pulmonary hygiene.
Test-taking strategy
- Identify the mechanical action that occurs when a patient uses a handheld clearance device (breathing out against resistance).
- Recognize that PEP therapy is the standard physiological term for the pressure generated during forced expiration through a device.
- Distinguish between manual techniques (percussion) and mechanical principles (pressure and flow) used in respiratory equipment.
- Choose the answer that explains the physics of how the device prevents airway collapse during the breathing cycle.
Take home points
- PEP devices allow patients to perform airway clearance independently without the need for an assistant.
- Oscillating PEP devices combine pressure with high-frequency vibrations to further loosen tenacious mucus.
- Patients should be taught to perform "huff" coughs (forced expiratory maneuvers) after using the device.
- Consistency is key; these devices are most effective when used daily as part of a routine maintenance plan.
Exams on Chronic Obstructive Pulmonary Disease
Custom Exams
Login to Create a Quiz
Click here to loginLessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Define chronic obstructive pulmonary disease (COPD) and distinguish between chronic bronchitis and emphysema
- Identify common risk factors and causes of COPD, including smoking and environmental exposures
- Describe the pathophysiology of COPD and how airflow limitation occurs
- Recognize common signs, symptoms, and disease progression associated with COPD
- Interpret diagnostic tests used in COPD management, including spirometry, ABGs, and chest imaging
- Explain pharmacologic treatments for COPD, including bronchodilators, corticosteroids, and oxygen therapy
- Apply nursing interventions to manage acute exacerbations and promote effective airway clearance
- Demonstrate patient education strategies to improve self-management, prevent exacerbations, and enhance quality of life
Introduction
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable respiratory disorder characterized by persistent, slowly progressive airflow limitation. The disease is associated with an enhanced chronic inflammatory response in the airways and lungs to noxious particles or gases, most commonly resulting from cigarette smoking. Episodes of acute exacerbations and the presence of comorbid conditions significantly contribute to disease severity, functional decline, and overall health outcomes.
Historically, COPD encompassed two primary obstructive airway conditions: chronic bronchitis and emphysema. Chronic bronchitis is clinically defined as a productive cough lasting at least three months in two consecutive years, after excluding other causes of chronic cough. Emphysema involves the permanent enlargement of air spaces distal to the terminal bronchioles, accompanied by destruction of alveolar walls without fibrosis. While patients may exhibit a predominance of either condition, these pathologies frequently coexist, making clear differentiation difficult. Notably, only approximately 10% of patients present with pure emphysema, supporting the current view of COPD as a single disease entity in terms of pathophysiology and management.
Asthma may coexist with COPD, and although evidence remains inconclusive, it is considered a potential risk factor for COPD development. The public health burden of COPD is substantial and often underestimated due to delayed diagnosis, with many individuals identified only after the disease has reached a moderate or advanced stage. In the United States alone, an estimated 12.7 million adults have been diagnosed with COPD, while an additional 24 million individuals demonstrate impaired lung function. COPD is currently the third leading cause of death, accounting for more than 133,000 deaths annually, underscoring its significant impact on population health.
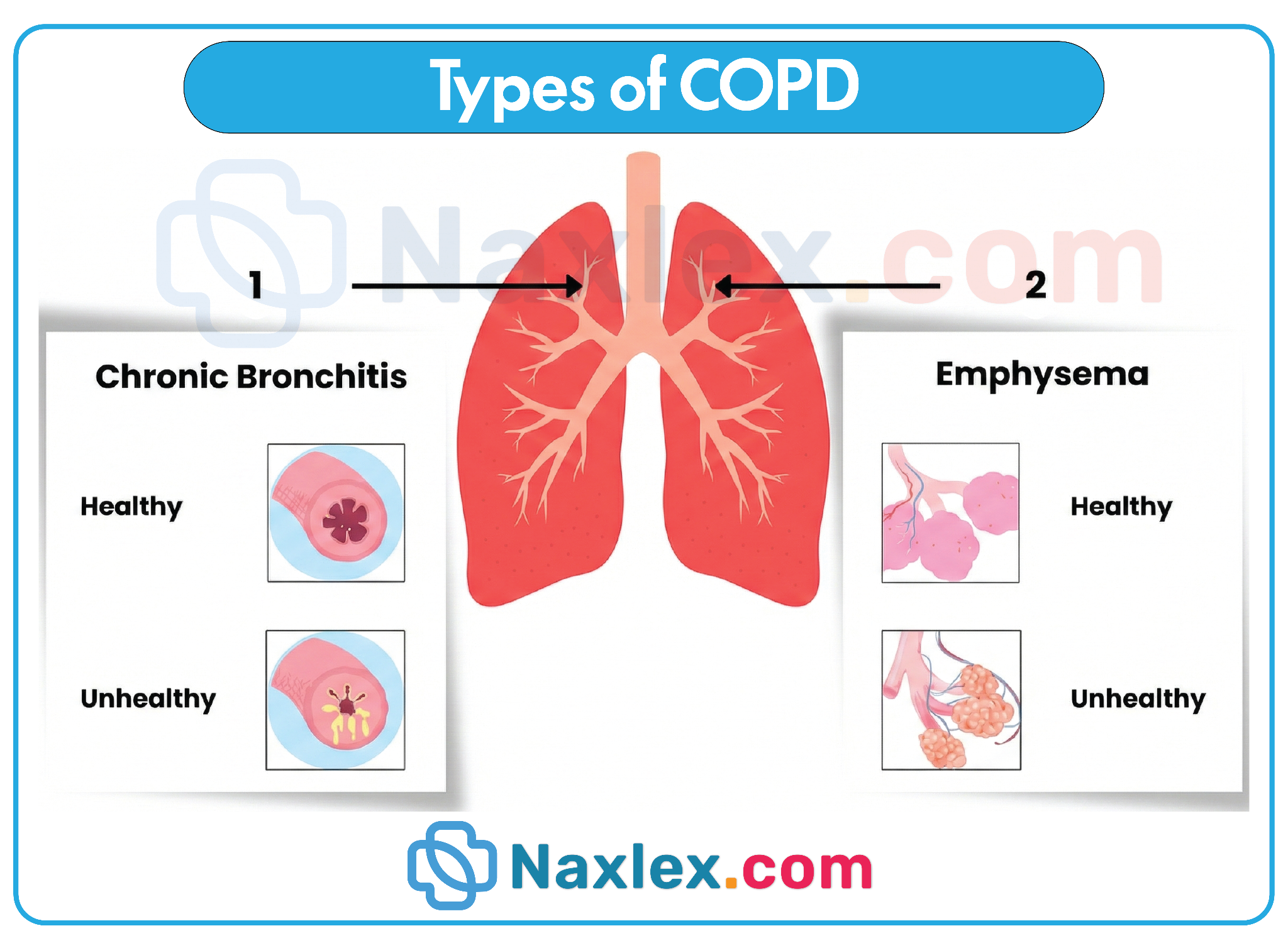
Risk Factors
Exogenous factors
- Tobacco use
- Cigarette smoking is the primary risk factor for COPD
- Individuals who stopped smoking ≥ 10 years ago are not at increased risk
- Passive smoking
- Exposure to air pollution or fine particulate matter
- Nonorganic dust exposure
- Occupational exposure such as industrial bronchitis in coal miners
- Organic dust exposure
- Increased COPD incidence in regions where biomass fuels (e.g., wood, animal dung) are routinely burned indoors
Endogenous factors
- Abnormal lung growth and development
- Recurrent pulmonary infections, including tuberculosis
- Premature birth
- α1-antitrypsin deficiency
- Airway hyperresponsiveness
- Antibody deficiency syndromes
- Examples include IgA deficiency
- Primary ciliary dyskinesia
- Includes Kartagener syndrome
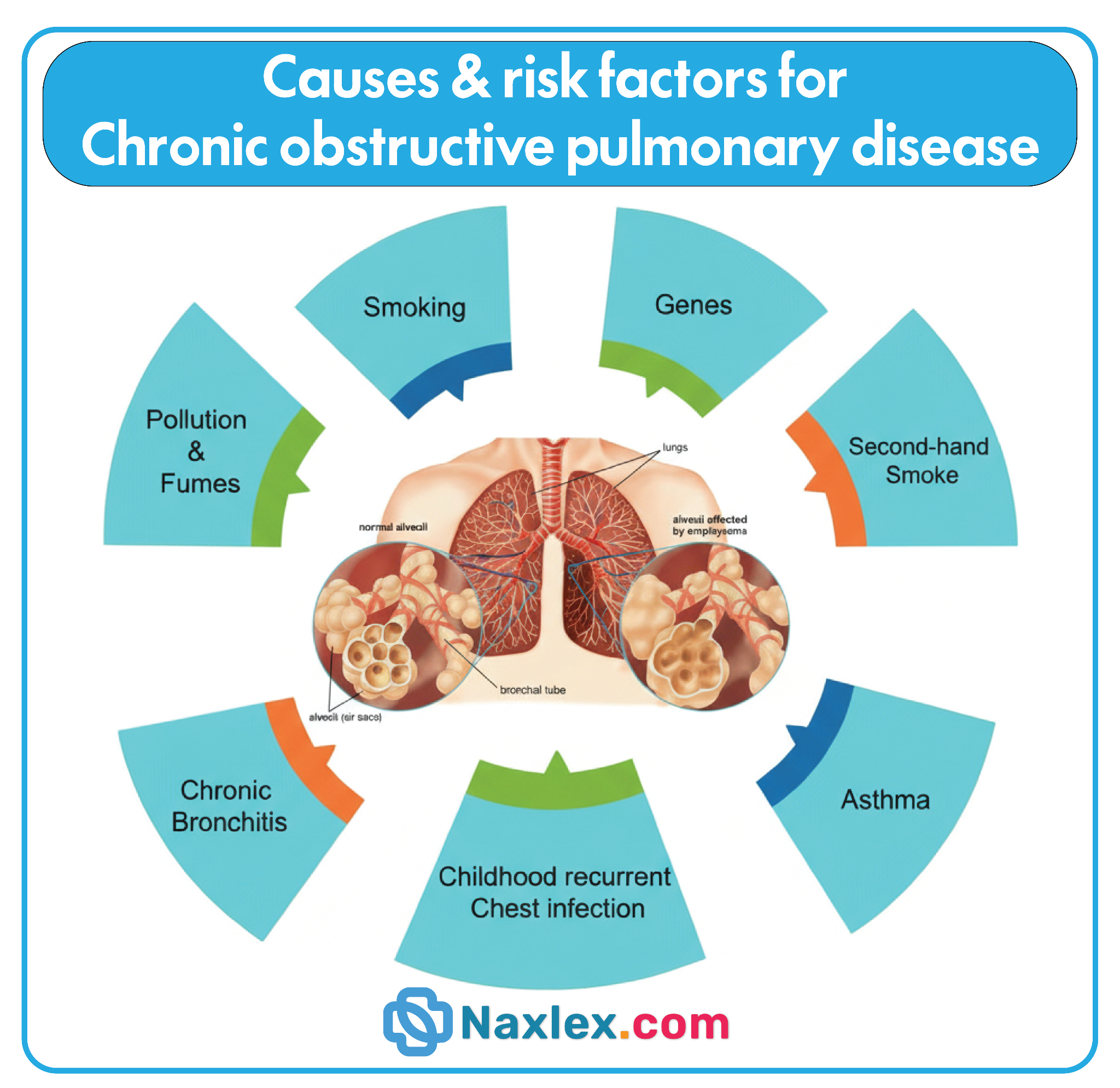
Classification
GOLD classification
- GOLD spirometric grades help inform the prognosis of a patient.
- GOLD groups guide pharmacological management.
GOLD grades
GOLD spirometric grades
|
Grade |
Post-bronchodilator FEV₁ (% predicted) |
|
GOLD 1: mild |
≥ 80% |
|
GOLD 2: moderate |
50–79% |
|
GOLD 3: severe |
30–49% |
|
GOLD 4: very severe |
< 30% |
- Cutoff points between GOLD spirometric grades (based on FEV₁ % predicted): 30 + 50 = 80
GOLD groups
GOLD group assessment
|
Group |
Exacerbations in the past year |
Severity of symptoms |
mMRC dyspnea scale |
CAT score |
|
GOLD group A |
0 or 1 not leading to hospital admission |
Mild |
0–1 |
0–9 |
|
GOLD group B |
≥ 2 |
Moderate |
2–4 |
≥ 10 |
|
GOLD group E |
≥ 2 moderate exacerbations or ≥ 1 leading to hospital admission |
Any severity |
Any |
Any |
Clinical Features
Presenting findings
- Chronic cough with expectoration
- Expectoration typically occurs in the morning
- Dyspnea and tachypnea
- Early stages: occurs only with exertion
- Advanced stages: occurs continuously
- Pursed-lip breathing
- Inhalation through the nose and slow exhalation through pursed lips
- Increases airway pressure and prevents bronchial collapse during late expiration
- More commonly observed in emphysema
- Auscultatory findings
- Prolonged expiratory phase
- End-expiratory wheezing
- Crackles
- Muffled breath sounds and/or coarse rhonchi
- Cyanosis due to hypoxemia
- Tachycardia
Features of advanced COPD
- Congested neck veins
- Barrel chest
- Most commonly seen in emphysema
- Asynchronous chest and abdominal movement during respiration
- Use of accessory respiratory muscles
- Due to diaphragmatic dysfunction
- Percussion findings
- Hyperresonant lung fields
- Reduced diaphragmatic excursion
- Relative cardiac dullness
- Decreased breath sounds on auscultation
- Referred to as a “silent lung”
- Peripheral edema
- Typically involving the ankles
- Right ventricular hypertrophy
- Evidence of right-sided heart failure and cor pulmonale
- Hepatomegaly
- Weight loss and cachexia
- Secondary polycythemia
- Confusion
- Resulting from hypoxemia and hypercapnia
- Nail clubbing
- Suggests comorbidities such as bronchiectasis, pulmonary fibrosis, or lung cancer
- Not specific to COPD
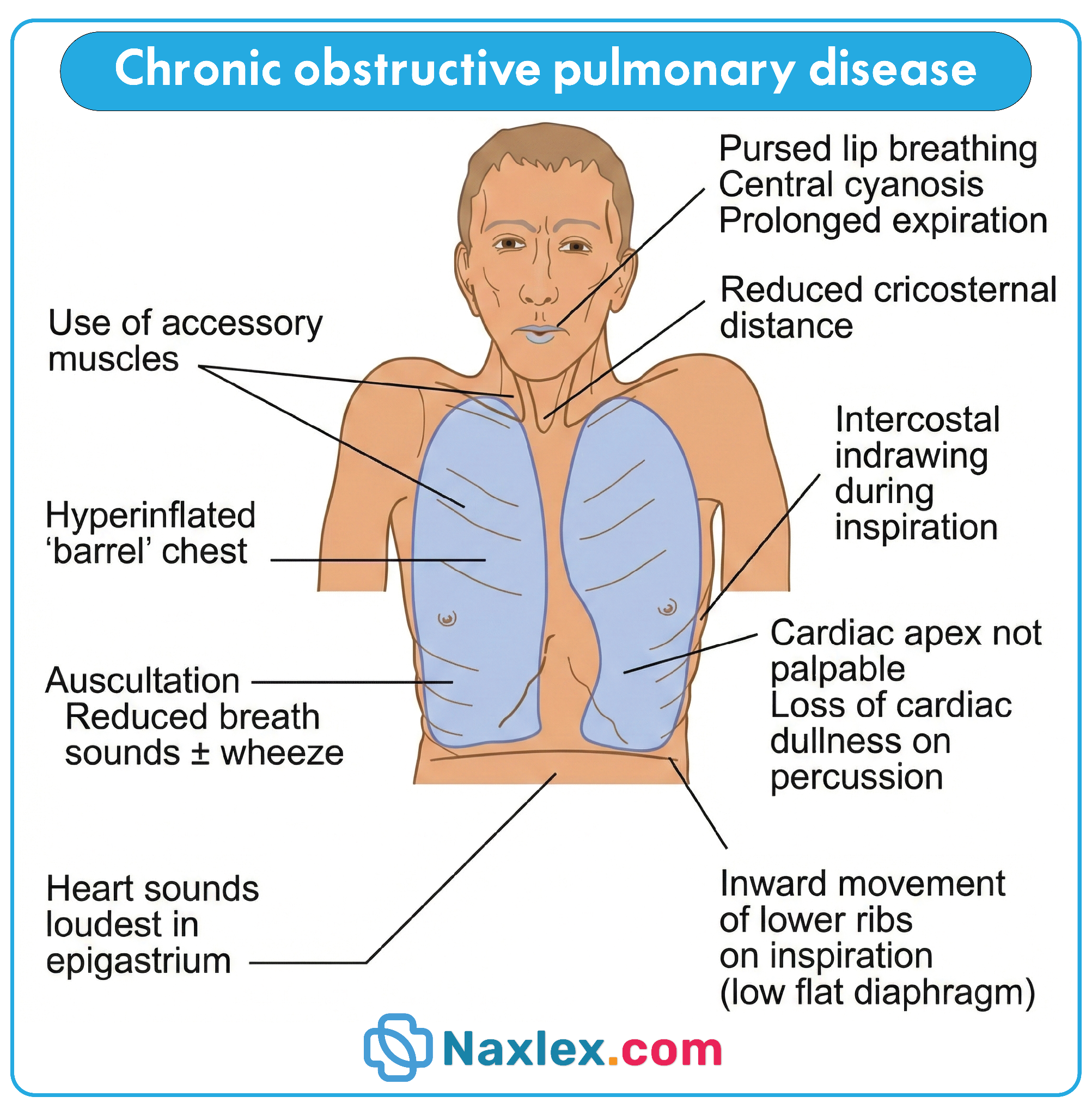
Pink puffer vs. blue bloater
|
Feature |
Pink Puffer |
Blue Bloater |
|
Main pathomechanism |
Emphysema |
Chronic bronchitis |
|
Cyanosis |
Absent |
Present |
|
Body habitus |
Cachectic |
Overweight |
|
Breathing pattern |
Pursed-lip breathing |
Normal or labored |
|
Cough |
Mild |
Productive |
|
Peripheral edema |
Absent |
Present |
|
PaO₂ |
Slightly reduced |
Markedly reduced |
|
PaCO₂ |
Normal (late hypercapnia possible) |
Increased (early hypercapnia) |
Features of COPD due to α1-antitrypsin deficiency (AATD)
- Earlier age of onset
- Typically < 60 years
- Associated hepatic involvement
- Jaundice
- Hepatitis or cirrhosis
Diagnostics
- Spirometry (gold standard for diagnosis)
- Required to confirm COPD in patients with suggestive symptoms
- Confirms the presence of airflow obstruction and determines disease severity
- Performed after administration of a short-acting bronchodilator
- COPD is diagnosed when FEV₁/FVC < 70% with appropriate clinical symptoms
- FEV₁ (% predicted) is used to grade severity
- Lower FEV₁ values indicate more severe disease
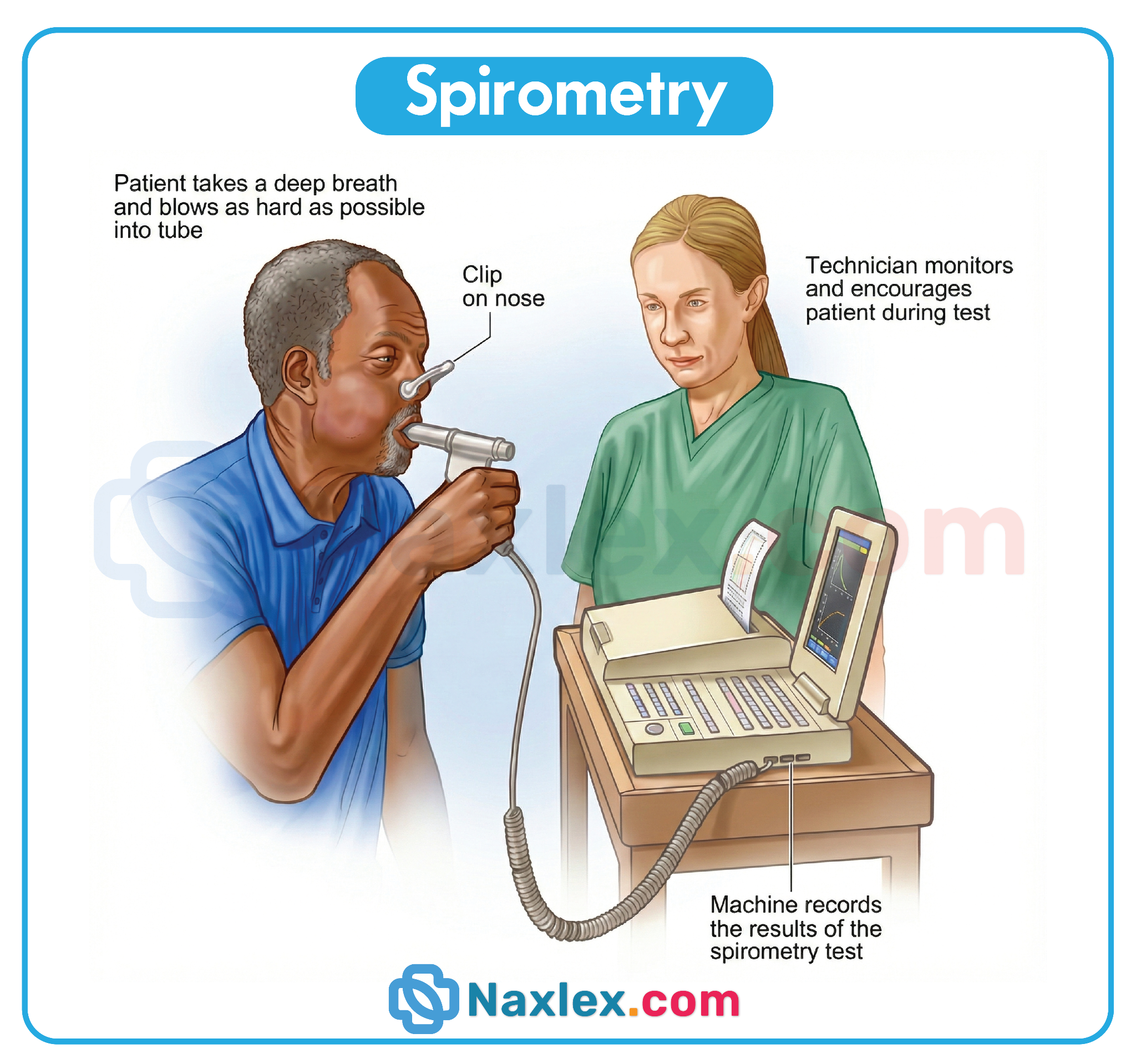
- Chest X-ray
- Not diagnostic for COPD
- May demonstrate hyperinflated lungs and a flattened diaphragm
- Computed tomography (CT) scan
- Not routinely used for diagnosis
- Useful in patients with predominant emphysema
- May show enlarged air spaces, particularly in the lung apices
- COPD Assessment Test (CAT)
- Validated questionnaire measuring the daily impact of COPD on quality of life
- Helps guide management and monitor response to therapy
- Modified Medical Research Council (mMRC) Dyspnea Scale
- Measures the severity of dyspnea
- 6-minute walk test
- Assesses exercise tolerance and detects exercise-induced hypoxemia
- Pulse oximetry is measured at rest and during ambulation
- Resting SpO₂ ≤ 88% on room air qualifies the patient for supplemental oxygen
- Arterial blood gases (ABGs)
- Evaluated in severe COPD (FEV₁ < 50%) and during acute exacerbations
- Early COPD: normal or mildly decreased PaO₂, normal PaCO₂
- Advanced COPD: decreased PaO₂, increased PaCO₂, low or low-normal pH, elevated HCO₃⁻
- Electrocardiogram (ECG)
- May be normal
- Can show evidence of right ventricular hypertrophy or failure
- Echocardiogram or MUGA scan
- Assesses right- and left-sided ventricular function
- Useful in evaluating cor pulmonale or coexisting heart disease
- Sputum culture and sensitivity
- Obtained during hospitalization for acute exacerbations
- Guides appropriate antibiotic therapy
Management
Pharmacological treatment
General principles
- Bronchodilators are the cornerstone of pharmacologic management in COPD.
- Inhaled corticosteroids (ICS) (e.g., budesonide, fluticasone, beclomethasone) should only be used in combination with long-acting bronchodilators and are not recommended as monotherapy.
Initial pharmacological treatment of stable COPD
|
GOLD group |
Daily regimen |
Rescue medication |
|
GOLD group A |
Long-acting bronchodilator (preferred if available and affordable) • Long-acting beta agonist (LABA), e.g., salmeterol, formoterol OR long-acting muscarinic antagonist (LAMA), e.g., tiotropium bromide OR consider a rescue medication alone for patients with very infrequent dyspnea |
Short-acting bronchodilator for immediate symptom relief • Short-acting beta agonist (SABA), e.g., albuterol, levalbuterol OR short-acting muscarinic antagonist (SAMA), e.g., ipratropium bromide |
|
GOLD group B |
LABA/LAMA combination therapy, e.g., umeclidinium/vilanterol |
Short-acting bronchodilator |
|
GOLD group E |
LABA/LAMA combination therapy OR, in patients with an eosinophil count ≥ 300 cells/mcL, consider LABA/LAMA/ICS triple therapy, e.g., fluticasone furoate/umeclidinium/vilanterol |
Short-acting bronchodilator |
- If the initial response to treatment is inadequate, assess for poor inhaler technique and/or poor medication adherence as potential contributing factors.
Follow-up treatment in COPD
|
Predominant trait |
Current treatment |
Follow-up treatment |
|
Persistent dyspnea |
LABA or LAMA monotherapy OR LABA/ICS combination therapy |
LAMA/LABA combination therapy, e.g., umeclidinium/vilanterol Consider switching inhaler device or medication within the same class Evaluate for alternative causes of dyspnea Consider adding ensifentrine (if available) |
|
Persistent exacerbations |
LABA or LAMA monotherapy OR LABA/ICS combination therapy |
Escalate therapy based on blood eosinophil count: • < 300 cells/mcL: LAMA/LABA combination therapy • ≥ 300 cells/mcL: LAMA/LABA/ICS triple therapy, e.g., fluticasone furoate/umeclidinium/vilanterol |
|
|
LABA/LAMA combination therapy |
Based on blood eosinophil count: • < 100 cells/mcL: consider adding either a macrolide antibiotic (e.g., azithromycin) or a PDE4 inhibitor (e.g., roflumilast) • ≥ 100 cells/mcL: add ICS (e.g., budesonide) or escalate to LAMA/LABA/ICS triple therapy |
|
|
LABA/LAMA/ICS triple therapy |
Consider adding: • Macrolide antibiotic • PDE4 inhibitor • IL-4 receptor alpha antagonist, e.g., dupilumab |
- Consider reducing or discontinuing ICS if adverse effects occur, such as pneumonia.
- Follow-up treatment decisions are guided by treatable traits (dyspnea and exacerbation frequency) and are made regardless of initial GOLD group (A, B, or E).
Other drugs
- Methylxanthines (e.g., theophylline)
- Nonselectively antagonize adenosine receptors and inhibit phosphodiesterase
- May be considered if other bronchodilators are unavailable
- Clinical benefit remains unproven
- Mucolytics (e.g., N-acetylcysteine, erdosteine)
- Reduce mucus viscosity by breaking disulfide bonds in mucoproteins
- May help reduce exacerbation frequency in selected patients
Non-pharmacological interventions
Lifestyle modifications
- Provide counseling on smoking cessation and available pharmacologic options, such as varenicline
- Encourage regular physical activity to lower the risk of acute exacerbations
- Recommend maintaining a healthy nutritional status
- Educate patients on:
- Reducing indoor air pollution, including the use of nonpolluting cooking stoves
- Use of personal protective equipment to prevent occupational lung disease
- Smoking cessation is the single most effective intervention to slow the decline in lung function in patients with COPD
Supportive care
- Recommended immunizations for patients with COPD:
- Influenza vaccine (annually)
- Pneumococcal vaccine for patients ≥ 19 years of age
- COVID-19 vaccine
- Tdap vaccine if not received during adolescence
- Zoster vaccine for patients > 50 years of age
- RSV vaccine for patients ≥ 60 years of age and/or those with chronic lung or heart disease
- Refer to the ACIP immunization schedule for detailed guidance
- Pulmonary rehabilitation
- Particularly beneficial for patients with moderate to severe COPD
- Vaccinations against influenza and pneumococcus
- Reduce the risk of respiratory infections and associated complications in patients with COPD
Complications
- Chronic respiratory failure
- Long-standing partial respiratory failure characterized by a resting PaO₂ < 60 mm Hg
- May progress to combined hypoxemic and hypercapnic respiratory failure, defined by PaO₂ < 60 mm Hg and PaCO₂ > 45 mm Hg
- Occurs in advanced COPD as a result of progressive emphysematous destruction and loss of alveolar diffusion surface area
- Acute exacerbations of COPD
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is a clinical diagnosis characterized by worsening respiratory symptoms within a period of 14 days. The most common trigger is a viral upper respiratory tract infection (URTI). Cardinal symptoms of AECOPD are worsening dyspnea, increased frequency and severity of cough, and increased volume and/or purulence of sputum. Testing is aimed at assessing severity, evaluating for underlying triggers, and identifying coexisting conditions (e.g., pneumonia). Respiratory support (e.g., oxygen therapy, noninvasive positive pressure ventilation) may be required to treat hypoxemia and hypercapnia. The mainstays of pharmacological therapy are bronchodilators and systemic glucocorticoids. Antibiotics should be considered in certain patients with cardinal symptoms of AECOPD (especially an increase in the purulence of sputum) and those who require mechanical ventilation.
- Cor pulmonale (right-sided heart failure)
- Secondary spontaneous pneumothorax: Caused by rupture of bullae, particularly in bullous emphysema
Summary
- COPD is a chronic lung disease that causes long-term airflow limitation and is not fully reversible.
- The two main types of COPD are chronic bronchitis and emphysema.
- Smoking is the leading cause of COPD, though pollution, occupational exposure, and genetics can also contribute.
- Chronic inflammation in COPD leads to airway narrowing, excess mucus production, and impaired gas exchange.
- Risk factors for COPD include smoking history, older age, environmental irritants, and family history.
- Common symptoms of COPD include chronic cough, sputum production, shortness of breath, wheezing, and fatigue.
- COPD is diagnosed primarily through spirometry, which shows a reduced FEV₁/FVC ratio.
- The disease is progressive and often includes periods of acute exacerbations triggered by infections or irritants.
- Medications for COPD include bronchodilators, inhaled corticosteroids, and combination inhalers.
- Non-pharmacologic management includes smoking cessation, pulmonary rehabilitation, oxygen therapy, and breathing exercises.
- Nursing care focuses on monitoring respiratory status, promoting airway clearance, and teaching proper inhaler use.
- Prevention includes vaccinations, avoidance of triggers, medication adherence, and early recognition of worsening symptoms.
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Chronic Obstructive Pulmonary Disease
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
