
Dementia And Alzheimer’s Disease
Lessons
- Objectives
- Introduction
- Definition And Classification Of Dementia
- Practice Exercise 1
- Alzheimer’s Disease
- Practice Excercise 2
- Differences Between Dementia And Alzheimer’s Disease
- Nursing Management Of Dementia
- Practice Excercise 3
- Pharmacological Management Of Dementia And Alzheimer’s Disease
- Psychosocial And Behavioral Management
- Practice Exercise 4
- Complications And Prognosis
- Ethical And Legal Considerations In Dementia Care
- Practice Exercise 5
- Prevention And Health Education
- Role Of The Nurse In Community And Institutional Care
- Practice Exercise 6
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
At the end of this topic, the learner should be able to:
- Define dementia and classify its types scientifically.
- Describe the epidemiology of dementia, including global and regional prevalence, incidence, and demographic patterns.
- Explain the etiology and major risk factors contributing to the development of dementia.
- Discuss the pathophysiological mechanisms underlying dementia.
- Differentiate between various forms of dementia based on their neuropathological and clinical features.
- Describe Alzheimer’s disease as the most common cause of dementia.
- Identify the stages, clinical manifestations, diagnostic criteria, and management strategies of Alzheimer’s disease.
- Explain the pharmacological and non-pharmacological approaches used in the treatment and nursing care of patients with dementia and Alzheimer’s disease.
- Discuss the nurse’s role in the management, rehabilitation, and health education of patients with dementia and Alzheimer’s disease.
- Demonstrate knowledge of ethical and legal principles guiding dementia care.
- Apply evidence-based nursing interventions in the care of individuals with cognitive decline and their families.
Introduction
- Dementia represents a syndrome of chronic and progressive deterioration in cognitive function, beyond what is expected from normal aging.
- It involves impairment in memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgment, often accompanied by deterioration in emotional control, social behavior, or motivation.
- Alzheimer’s disease (AD) is the most prevalent form of dementia, accounting for approximately 60–80% of all cases.
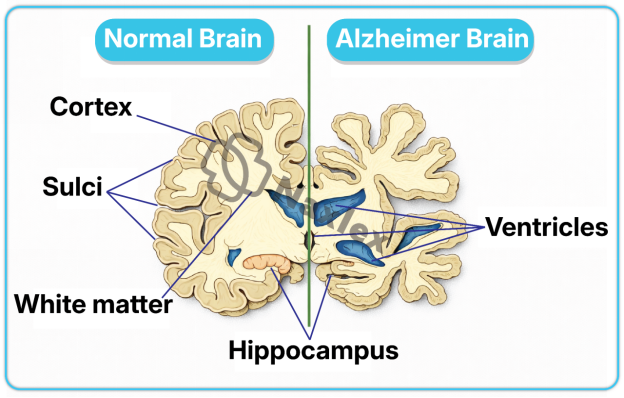
- It is characterized by neurodegenerative changes that lead to irreversible loss of neurons and synapses, especially in the cerebral cortex and hippocampus, resulting in progressive decline in cognitive and functional abilities.
- Dementia is a major public health concern with increasing global prevalence due to aging populations.
- According to the World Health Organization (WHO), more than 55 million people worldwide are currently living with dementia, with nearly 10 million new cases annually. It is a leading cause of disability and dependency among older adults.
- From a nursing perspective, dementia poses complex challenges that require multidisciplinary management, including accurate assessment, symptom control, psychological support, family education, and promotion of quality of life.
- Nurses play a vital role in early detection, compassionate care, prevention of complications, and maintaining patient dignity.
Definition And Classification Of Dementia
- Dementia is a chronic, acquired, and progressive syndrome characterized by impairment in multiple higher cortical functions such as memory, intellect, language, and executive functioning, severe enough to interfere with daily life and social functioning, in the absence of altered consciousness.
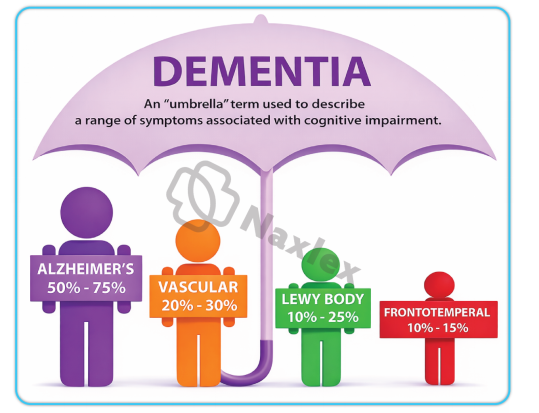
- Dementia is not a single disease but rather a clinical syndrome resulting from various brain disorders that affect cognition and behavior.
1.1 Types of Dementia
Dementias can be classified based on etiology, pathophysiological mechanisms, or clinical presentation.
A. Based on Etiology:
- Primary Dementias:
- The dementia itself is the main disorder, due to intrinsic neurodegenerative processes.
- Examples:
- Alzheimer’s disease
- Frontotemporal dementia (Pick’s disease)
- Lewy body dementia
- Parkinson’s disease dementia
- Huntington’s disease - Secondary Dementias:
- Cognitive impairment occurs as a consequence of another underlying systemic or cerebral disorder.
- Examples:
- Vascular dementia (post-stroke dementia)
- Dementia due to infections (HIV, neurosyphilis, Creutzfeldt-Jakob disease)
- Dementia due to toxins (chronic alcohol use, heavy metals)
- Dementia due to metabolic or endocrine disorders (hypothyroidism, vitamin B₁₂ deficiency)
Alzheimer’s Dementia
- Etiology:
- Caused by progressive neurodegeneration and neuronal loss.
- Associated with amyloid plaque accumulation and neurofibrillary tangles.
- Genetic factors, including APOE-e4 allele, increase risk.
- Key Features:
- Gradual, insidious onset of cognitive decline.
- Memory impairment is typically the earliest and most prominent symptom.
- Progressive decline in language, executive function, and visuospatial skills.
- Clinical Manifestations:
- Early-stage: mild memory loss, difficulty performing complex tasks, subtle personality changes.
- Middle-stage: increased disorientation, language impairments, behavioral disturbances such as agitation and wandering.
- Late-stage: profound cognitive loss, inability to communicate, total dependence for ADLs.
- Nursing Implications:
- Focus on safety, cognitive stimulation, structured routines, and caregiver education.
- Early intervention improves quality of life and slows functional decline.
Vascular Dementia
- Etiology:
- Results from cerebrovascular disease, including stroke, chronic ischemia, or microvascular injury.
- Cognitive decline is due to reduced cerebral blood flow and neuronal damage.
- Key Features:
- Onset may be abrupt or stepwise after a stroke or transient ischemic attack.
- Cognitive deficits often correlate with location and extent of vascular lesions.
- Memory may be less affected initially compared to Alzheimer’s, but executive dysfunction is prominent.
- Clinical Manifestations:
- Impaired judgment, slowed thinking, and difficulty with planning and decision-making.
- Emotional lability or depression is common.
- Focal neurological deficits (e.g., hemiparesis, visual field deficits) may be present.
- Nursing Implications:
- Focus on stroke prevention, management of cardiovascular risk factors, and safety planning.
- Cognitive and functional support should be individualized based on neurological deficits.
Lewy Body Dementia (LBD)
- Etiology:
- Caused by abnormal deposition of alpha-synuclein proteins (Lewy bodies) in cortical neurons.
- Key Features:
- Fluctuating cognition, pronounced attention deficits, and visual hallucinations.
- Parkinsonian motor symptoms (rigidity, bradykinesia) often appear.
- REM sleep behavior disorder may precede cognitive symptoms.
- Clinical Manifestations:
- Recurrent visual hallucinations and delusions.
- Variations in alertness and attention throughout the day.
- Parkinsonian signs including shuffling gait and tremor.
- Nursing Implications:
- Monitor for falls due to motor impairment.
- Avoid antipsychotics if possible, as clients with LBD are highly sensitive to extrapyramidal side effects.
- Focus on environmental modifications, reassurance, and caregiver support.
Frontotemporal Dementia (FTD)
- Etiology:
- Degeneration of frontal and/or temporal lobes of the brain.
- Genetic mutations in MAPT or progranulin genes may contribute.
- Key Features:
- Early behavioral changes or language deficits rather than memory loss.
- Two primary variants:
- Behavioral variant FTD: marked changes in personality, social conduct, and judgment.
- Primary progressive aphasia: progressive language and communication impairments.
- Clinical Manifestations:
- Socially inappropriate behaviors, impulsivity, and apathy.
- Loss of empathy and insight into own behavior.
- Difficulty naming objects, constructing sentences, or understanding language.
- Nursing Implications:
- Emphasize behavioral management, caregiver education, and environmental modifications.
- Support communication strategies for language deficits.
- Focus on safety due to impulsive or disinhibited behaviors.
Mixed Dementia
- Etiology:
- Combination of two or more types of dementia, most commonly Alzheimer’s disease and vascular dementia.
- Key Features:
- Cognitive decline reflects contributions from multiple pathologies.
- Symptoms may overlap and complicate diagnosis.
- Clinical Manifestations:
- Memory impairment, executive dysfunction, mood disturbances, and possible motor deficits.
- Fluctuating cognitive abilities may be observed.
- Nursing Implications:
- Care must address all contributing pathologies, including cardiovascular risk management.
- Tailored interventions for both cognitive and functional deficits are necessary.
B. Based on Affected Brain Regions:
- Cortical Dementias: Primarily involve the cerebral cortex.
- Manifested by language disturbances, memory loss, and reasoning difficulties.
- Examples: Alzheimer’s disease, frontotemporal dementia. - Subcortical Dementias: Affect basal ganglia, thalamus, and brainstem structures.
- Manifested by psychomotor slowing and mood changes.
- Examples: Parkinson’s disease dementia, Huntington’s disease dementia. - Mixed Dementias: Show features of both cortical and subcortical involvement.
- Example: Vascular dementia with Alzheimer’s pathology.
1.2 Epidemiology of Dementia
- Global Prevalence:
- >55 million people are living with dementia worldwide.
- Alzheimer’s disease accounts for ≈60–80% of all dementia cases.
- Prevalence increases exponentially with age:
- ~5% among people aged ≥65 years
- ~25–50% among those aged ≥85 years - Gender Distribution:
- Women are more commonly affected than men due to longer life expectancy and possible hormonal influences. - Geographic Variation:
- Higher prevalence in developed nations, but a growing burden in low- and middle-income countries due to increased life expectancy. - Mortality:
- Dementia is among the top 10 causes of death globally.
- Average survival after diagnosis ranges from 4–8 years, depending on type and severity. -
Nursing Insights:
- Nurses must recognize that early detection and diagnosis of dementia allow better planning and improved outcomes.
- Community health nurses play a key role in screening older adults for early cognitive impairment using tools such as the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA).
- Understanding epidemiological patterns helps nurses prioritize at-risk populations and educate families on preventive measures such as controlling vascular risk factors.
1.3 Etiology and Risk Factors of Dementia
A. Etiological Categories:
- Neurodegenerative causes: Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, and frontotemporal lobar degeneration.
- Vascular causes: Multi-infarct dementia, subcortical ischemic vascular dementia.
- Infectious causes: HIV-associated dementia, neurosyphilis, prion diseases.
- Metabolic and toxic causes: Chronic alcoholism, hypoglycemia, hepatic encephalopathy, thyroid disorders, vitamin deficiencies (e.g., B₁₂, thiamine).
- Traumatic causes: Chronic traumatic encephalopathy (CTE) in repetitive head injuries.
- Neoplastic causes: Primary brain tumors or metastases affecting cortical and limbic structures.
B. Major Risk Factors:
- Age: Risk doubles every 5 years after age 65.
- Genetics:
- APOE-ε4 allele increases risk of late-onset Alzheimer’s disease.
- Mutations in APP, PSEN1, PSEN2 genes cause early-onset familial Alzheimer’s disease. - Gender: Female sex is associated with a higher risk.
- Vascular risk factors: Hypertension, diabetes mellitus, hyperlipidemia, smoking, and obesity.
- Lifestyle factors: Physical inactivity, poor diet, social isolation, and low educational attainment.
- Head trauma: Repeated traumatic brain injuries increase dementia risk.
- Chronic stress and depression: Associated with neuroendocrine and inflammatory changes that promote cognitive decline.
Nursing Insights:
- Nurses should educate patients on modifiable risk factors, emphasizing the importance of controlling blood pressure, glucose, and cholesterol levels, and maintaining active mental and social engagement.
- During patient assessment, always take a comprehensive history, including family history, occupational exposure, and lifestyle habits to identify potential contributing factors.
- Nursing interventions should focus on primary prevention, such as community education on healthy brain aging.
1.4 Pathophysiology of Dementia
Dementia results from progressive neuronal loss and synaptic dysfunction in regions of the brain responsible for cognition, memory, and behavior.
Key Pathophysiological Mechanisms:
- Neuronal Degeneration: Loss of neurons and synapses in cortical and subcortical regions impairs signal transmission.
- Neurotransmitter Imbalance:
- ↓ Acetylcholine (ACh) is particularly important in Alzheimer’s disease, leading to memory impairment.
- Dopamine and serotonin imbalances contribute to behavioral and psychotic symptoms. - Cerebrovascular Pathology: In vascular dementia, multiple infarctions or chronic ischemia cause white matter lesions and neuronal death.
- Amyloid Plaques and Neurofibrillary Tangles:
- Extracellular deposition of β-amyloid peptides and intracellular aggregation of hyperphosphorylated tau protein disrupt neuronal communication.
- These are hallmark features of Alzheimer’s disease. - Oxidative Stress and Inflammation:
- Excess reactive oxygen species (ROS) cause mitochondrial dysfunction and neuronal apoptosis.
- Microglial activation releases pro-inflammatory cytokines (IL-1β, TNF-α). - Synaptic Dysfunction:
- Progressive loss of dendritic spines impairs neuronal plasticity and learning.
Table: Major Pathophysiological Changes in Dementia
|
Mechanism |
Resulting Effect |
Example Disorder |
|
β-Amyloid accumulation |
Disrupts synaptic transmission |
Alzheimer’s disease |
|
Tau hyperphosphorylation |
Neuronal cytoskeletal collapse |
Alzheimer’s disease |
|
Ischemic injury |
White matter damage, infarcts |
Vascular dementia |
|
Lewy bodies (α-synuclein) |
Neuronal death in cortex |
Lewy body dementia |
|
Neurotransmitter depletion |
Cognitive and behavioral impairment |
Various dementias |
Nursing Insights:
- Understanding pathophysiology assists nurses in interpreting symptoms (e.g., memory loss due to hippocampal damage).
- It also guides pharmacologic care—cholinesterase inhibitors (e.g., donepezil) are prescribed to enhance acetylcholine levels in Alzheimer’s disease.
- Nurses should closely monitor adverse drug effects such as bradycardia, dizziness, and gastrointestinal disturbances.
- Patient and family education should include explaining the biological basis of symptoms, helping to reduce stigma and enhance cooperation with care.
Alzheimer’s Disease
1.1 Definition of Alzheimer’s Disease
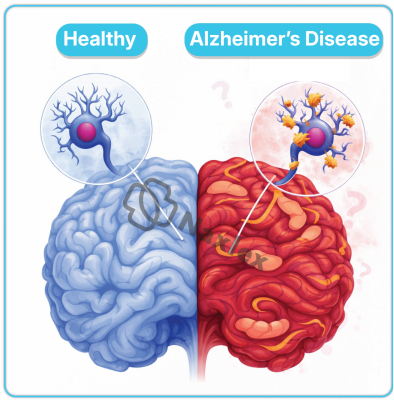
- Alzheimer’s disease (AD) is a progressive, irreversible neurodegenerative disorder characterized by cognitive decline, memory impairment, and behavioral disturbances due to widespread neuronal degeneration and synaptic loss, particularly in the cerebral cortex and hippocampus.
- It is the most common cause of dementia, accounting for approximately 60–80% of all dementia cases globally.
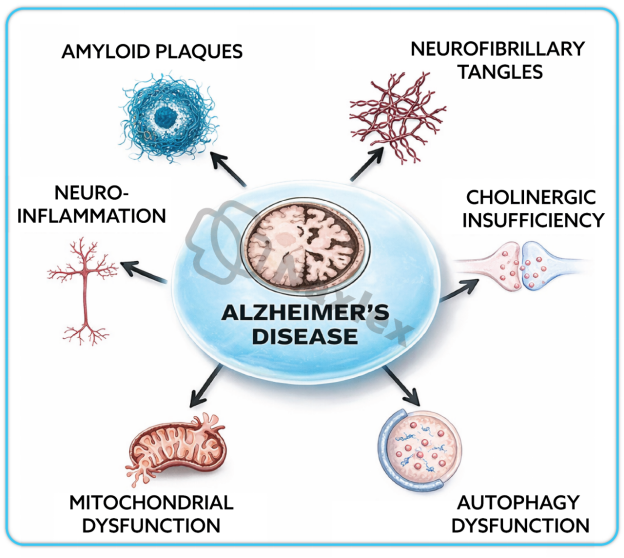
- Alzheimer’s disease results from the accumulation of abnormal proteins in the brain, specifically β-amyloid plaques and neurofibrillary tangles composed of hyperphosphorylated tau protein.
- The hallmark features include loss of cholinergic neurons, cerebral atrophy, and ventricular enlargement.
- Nurses should understand that Alzheimer’s disease leads to irreversible loss of cognitive and functional abilities and requires long-term multidisciplinary management.
- Early recognition and accurate diagnosis are crucial for planning appropriate interventions, supporting caregivers, and improving patient outcomes.
1.2 Epidemiology of Alzheimer’s Disease
- Prevalence:
- Alzheimer’s disease affects over 35 million people globally, with prevalence increasing sharply with age.
- Approximately 1 in 9 individuals aged ≥65 years and nearly one-third of those aged ≥85 years have Alzheimer’s disease. - Gender Distribution:
- Women are at higher risk than men, partly due to longer life expectancy and hormonal changes after menopause. - Geographic and Socioeconomic Factors:
- Higher prevalence in high-income countries due to longer lifespans, but incidence is rising rapidly in low- and middle-income countries. - Mortality:
- Alzheimer’s disease is among the top 5 causes of death in adults over 65 years.
- The average survival period after diagnosis is 4–8 years, though some may live up to 20 years. -
Nursing Insights:
- Nurses in geriatrics and community health should identify high-risk populations for early screening.
- Awareness programs should emphasize healthy aging, lifestyle modifications, and regular cognitive assessments in elderly patients.
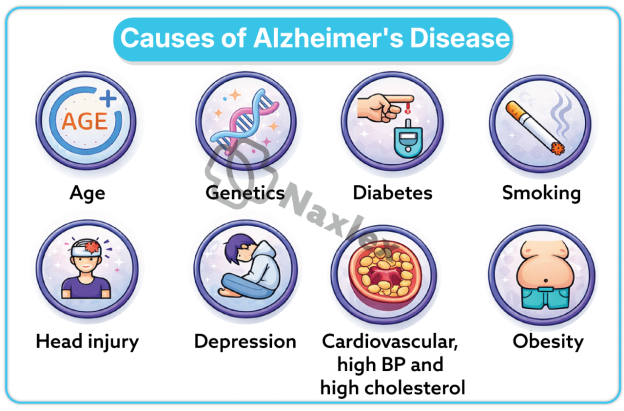
1.3 Etiology and Risk Factors of Alzheimer’s Disease
Alzheimer’s disease results from a complex interaction of genetic, environmental, and lifestyle factors leading to neuronal degeneration.
A. Genetic Factors:
- Familial (Early-Onset) Alzheimer’s Disease:
- Occurs before 65 years, accounting for <5% of cases.
- Associated with mutations in genes encoding:
- Amyloid precursor protein (APP)
- Presenilin 1 (PSEN1)
- Presenilin 2 (PSEN2) - Sporadic (Late-Onset) Alzheimer’s Disease:
- Accounts for >95% of cases.
- The APOE-ε4 allele is the strongest genetic risk factor.
B. Non-Genetic Risk Factors:
- Age: Risk doubles every 5 years after age 65.
- Gender: Women more frequently affected.
- Vascular and Metabolic Conditions: Hypertension, diabetes, obesity, and dyslipidemia increase susceptibility.
- Head Trauma: Repeated concussions or severe brain injury accelerate pathology.
- Lifestyle Factors: Sedentary lifestyle, poor diet, smoking, and social isolation.
- Neuroinflammation: Chronic activation of microglia leads to progressive neuronal damage.
- Low Education Level: Reduced cognitive reserve predisposes to earlier symptom onset.
Nursing Insights:
- Nurses should perform comprehensive health assessments to identify modifiable risk factors.
- Patient education should focus on vascular health, dietary habits (Mediterranean diet), and physical and mental activity as preventive strategies.
1.4 Pathophysiology of Alzheimer’s Disease
The pathogenesis of Alzheimer’s disease involves accumulation of toxic proteins, neuronal death, and neurotransmitter depletion.
A. Amyloid Cascade Hypothesis:
- The β-amyloid (Aβ) peptide, derived from abnormal cleavage of amyloid precursor protein (APP), accumulates extracellularly forming amyloid plaques.
- These plaques disrupt synaptic communication and trigger neuroinflammation and oxidative stress.
B. Tau Protein Abnormality:
- Hyperphosphorylated tau protein aggregates intracellularly into neurofibrillary tangles (NFTs).
- This disrupts the neuronal cytoskeleton, leading to impaired axonal transport and neuronal death.
C. Neurotransmitter Deficiency:
- Marked reduction in acetylcholine (ACh) due to degeneration of cholinergic neurons in the basal forebrain.
- This correlates with severity of cognitive impairment.
D. Brain Structural Changes:
- Cortical atrophy, ventricular enlargement, and hippocampal degeneration are prominent features.
- Loss of synaptic density leads to decline in neural plasticity.
E. Neuroinflammation and Oxidative Stress:
Activated microglia release cytokines (IL-1β, TNF-α) and reactive oxygen species (ROS), perpetuating neuronal injury.
|
Pathological Feature |
Description |
Functional Consequence |
|
β-Amyloid plaques |
Extracellular aggregates |
Synaptic dysfunction |
|
Neurofibrillary tangles |
Intracellular tau accumulations |
Neuronal death |
|
Loss of cholinergic neurons |
Decreased acetylcholine |
Memory loss |
|
Cortical atrophy |
Shrinking of cerebral tissue |
Cognitive decline |
Nursing Insights:
- Understanding these mechanisms helps nurses correlate clinical symptoms with brain pathology.
- Explaining these changes to families can improve understanding and empathy for patient behavior.
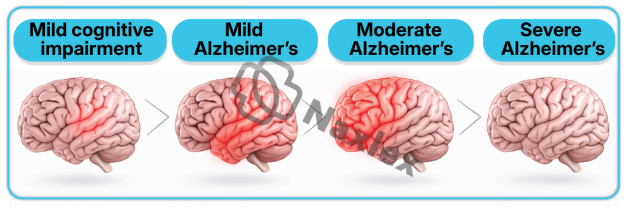
1.5 Stages of Alzheimer’s Disease
Alzheimer’s disease progresses through three major clinical stages:
1. Mild (Early Stage):
- Memory lapses, especially short-term memory.
- Difficulty with words, names, and recent events.
- Mild disorientation in familiar places.
- Preserved independence in basic activities of daily living (ADLs).
2. Moderate (Middle Stage):
- Increasing confusion and forgetfulness.
- Impairment in complex tasks (finances, meal preparation).
- Behavioral changes: agitation, wandering, aggression, hallucinations.
- Assistance required for most ADLs.
3. Severe (Late Stage):
- Loss of ability to communicate.
- Incontinence, inability to ambulate, and profound dependence.
- Dysphagia, muscle rigidity, and cachexia.
- Death often due to complications such as infections or aspiration pneumonia.
Nursing Insights:
- Nurses must tailor interventions to disease stage—safety and orientation in mild stages; behavioral management and full assistance in late stages.
- Family education on progressive care needs is essential.
1.6 Clinical Manifestations of Alzheimer’s Disease
A. Cognitive Symptoms:
- Memory loss (initially short-term, later long-term).
- Disorientation to time, place, and person.
- Impaired judgment and problem-solving.
- Aphasia (language difficulties).
- Apraxia (difficulty performing motor tasks).
- Agnosia (inability to recognize objects or people).
B. Behavioral and Psychological Symptoms:
- Agitation, irritability, depression, and anxiety.
- Paranoia, delusions, and hallucinations.
- Wandering, sundowning (worsening confusion at dusk).
C. Physical and Functional Changes:
- Gait disturbance, rigidity, and loss of coordination.
- Difficulty swallowing, leading to aspiration risk.
- Bladder and bowel incontinence.
Nursing Insights:
- Nurses should monitor for behavioral triggers (e.g., pain, overstimulation, fatigue).
- Gentle reorientation, calm tone, and consistent routine help minimize agitation.
1.7 Diagnostic Evaluation of Alzheimer’s Disease
A. Clinical Assessment:
- Detailed history from patient and caregivers.
- Cognitive screening:
- Mini-Mental State Examination (MMSE)
- Montreal Cognitive Assessment (MoCA)
- Clock drawing test - Functional status evaluation using Activities of Daily Living (ADL) and Instrumental ADL scales.
B. Laboratory Tests:
- Complete blood count (CBC), electrolytes, thyroid function, vitamin B₁₂ levels to rule out reversible causes.
C. Neuroimaging:
- MRI/CT Scan: Cortical atrophy, ventricular enlargement, hippocampal shrinkage.
- PET Scan: Decreased glucose metabolism in temporoparietal areas.
D. Biomarkers (advanced settings):
- CSF analysis for ↓Aβ42 and ↑tau proteins.
- Amyloid PET imaging to detect β-amyloid deposition.
Nursing Insights:
- Nurses play a vital role in preparing patients for neuroimaging, ensuring cooperation and comfort.
- During assessment, nurses should evaluate for delirium, depression, or medication effects which may mimic dementia.
1.8 Medical Management of Alzheimer’s Disease
A. Pharmacologic Management:
- Cholinesterase Inhibitors: Donepezil, Rivastigmine, Galantamine
- Increase acetylcholine levels, improving cognition and daily function. - NMDA Receptor Antagonist: Memantine
- Reduces excitotoxic neuronal damage. - Adjunctive Medications:
- Antidepressants (SSRIs) for mood disturbances.
- Antipsychotics (Risperidone, Quetiapine) for agitation or psychosis.
- Benzodiazepines used cautiously for anxiety. -
B. Non-Pharmacologic Management:
- Cognitive stimulation therapy and memory training.
- Reality orientation and reminiscence therapy.
- Physical activity, balanced diet, and structured routines.
- Environmental modifications to prevent wandering and injury.
-
Nursing Insights:
- Nurses should monitor for adverse drug reactions (bradycardia, dizziness, GI upset).
- Encourage caregiver support programs to prevent burnout.
- Regularly evaluate medication efficacy and side effects.
1.9 Nursing Management of Alzheimer’s Disease
1.9.1 Nursing Assessment
- Assess level of consciousness, orientation, and cognitive status.
- Evaluate memory, judgment, speech, and emotional status.
- Assess ability to perform ADLs.
- Observe for behavioral and psychotic symptoms.
- Review medications, nutrition, sleep patterns, and safety risks.
1.9.2 Nursing Diagnosis
- Impaired memory related to neuronal degeneration.
- Risk for injury related to confusion and wandering.
- Self-care deficit related to cognitive decline.
- Caregiver role strain related to patient dependency.
1.9.3 Nursing Planning and Implementation
- Promote Safety:
- Remove hazardous objects, use identification bracelets.
- Maintain a consistent, familiar environment. - Enhance Orientation:
- Display clocks, calendars, and labels on rooms.
- Use simple, clear communication. - Promote Independence:
- Encourage participation in self-care within ability limits.
- Provide step-by-step instructions for tasks. - Support Family and Caregivers:
- Offer education on disease progression and coping strategies.
- Facilitate support group referrals. - Manage Behavioral Symptoms:
- Use distraction, reassurance, and avoid confrontation.
- Provide activities that reduce restlessness.
1.9.4 Nursing Evaluation
- Patient demonstrates improved orientation and reduced agitation.
- ADLs maintained to maximum ability.
- Safety maintained with no falls or injuries.
- Caregiver demonstrates understanding and coping skills.
2.0 Complications of Alzheimer’s Disease
- Medical Complications:
- Malnutrition and dehydration
→ Due to dysphagia and neglect of self-care.
- Aspiration pneumonia
→ From impaired swallowing reflex.
- Pressure ulcers
→ Due to immobility and incontinence.
- Falls and fractures
→ From disorientation and poor coordination. - Psychological Complications:
- Depression, psychosis, social withdrawal. - Caregiver Complications:
- Fatigue, depression, and emotional exhaustion. -
Nursing Insights:
- Nurses must anticipate complications and initiate preventive measures, such as regular repositioning, nutritional monitoring, and fall prevention strategies.
-
Continuous caregiver assessment and support are essential to sustain effective long-term care.
Differences Between Dementia And Alzheimer’s Disease
- ementia and Alzheimer’s disease are closely related but not synonymous.
- Dementia is a broad clinical syndrome characterized by impairment in cognitive function severe enough to interfere with daily activities, while Alzheimer’s disease (AD) is a specific neurodegenerative disorder and the most common cause of dementia.
- Understanding their differences is crucial for accurate diagnosis, appropriate management, and nursing care planning.
1.1 Comparative Table: Dementia vs. Alzheimer’s Disease
|
Feature |
Dementia |
Alzheimer’s Disease |
|
Definition |
A clinical syndrome involving decline in cognitive function affecting memory, thinking, and social abilities due to various brain disorders. |
A specific neurodegenerative disease that causes 60–80% of all dementia cases, characterized by β-amyloid plaques and neurofibrillary tangles. |
|
Nature |
A symptom complex or umbrella term. |
A distinct pathological condition. |
|
Causes |
Multiple causes: Alzheimer’s, vascular, Lewy body, Parkinson’s, frontotemporal, infections, toxins, etc. |
Caused by accumulation of β-amyloid and tau proteins leading to neuronal death. |
|
Onset |
May be sudden (vascular) or gradual (degenerative). |
Gradual and insidious onset. |
|
Progression |
Depends on underlying cause; may be stable or progressive. |
Always progressive and irreversible. |
|
Memory Impairment |
Variable depending on cause; not always early. |
Early and prominent symptom. |
|
Reversibility |
Some forms are reversible (e.g., metabolic, drug-induced). |
Irreversible. |
|
Diagnosis |
Based on identifying the underlying cause. |
Confirmed by clinical evaluation, neuroimaging, and biomarkers. |
|
Treatment |
Depends on etiology; may include treating underlying condition. |
Symptomatic management only; no cure available. |
|
Prognosis |
Varies with cause. |
Chronic progressive deterioration leading to death. |
Nursing Insights:
- Nurses must recognize that all Alzheimer’s disease causes dementia, but not all dementia is Alzheimer’s disease.
- Accurate differentiation helps direct appropriate care strategies and medication use.
- During assessment, always rule out reversible causes of dementia before diagnosing Alzheimer’s disease.
Nursing Management Of Dementia
Nursing management of dementia focuses on maintaining patient safety, preserving functional abilities, supporting cognitive function, and providing emotional and psychosocial support to both patients and caregivers.
1.1 Nursing Assessment of Dementia
The nurse performs a comprehensive and holistic assessment to determine the degree of cognitive impairment and the impact on daily living.
- Cognitive Function:
- Assess orientation to time, place, person, and situation.
- Evaluate memory (short-term, long-term), attention, and problem-solving abilities. - Behavioral and Psychological Symptoms:
- Observe for agitation, aggression, delusions, hallucinations, wandering, or sleep disturbances. - Functional Status:
- Determine ability to perform Activities of Daily Living (ADLs) and Instrumental ADLs. - Physical Examination:
- Assess for neurological deficits, nutrition, hydration, mobility, and continence status. - Environmental Assessment:
- Evaluate home safety, fall hazards, lighting, and noise levels. - Family and Social Support:
- Assess caregiver burden, coping mechanisms, and available support systems.
Nursing Insights:
- Nurses should recognize behavioral changes as a form of communication rather than intentional defiance.
- Early detection of functional decline can guide interventions to maintain independence longer.
1.2 Nursing Diagnoses in Dementia
Common nursing diagnoses include:
- Impaired memory related to progressive neuronal degeneration.
- Chronic confusion related to disorientation and cognitive decline.
- Risk for injury related to impaired judgment and wandering.
- Impaired verbal communication related to aphasia.
- Self-care deficit related to impaired cognitive function.
- Caregiver role strain related to continuous supervision demands.
1.3 Nursing Interventions and Rationales
A. Promote Safety:
- Provide a secure and hazard-free environment.
- Install door alarms, remove clutter, and use nightlights.
- Ensure supervision during ambulation and meals to prevent falls and choking.
B. Enhance Cognitive Function:
- Provide structured routines to reduce confusion.
- Use calendars, clocks, and labeled items for orientation.
- Encourage memory exercises and familiar activities.
C. Manage Behavioral Symptoms:
- Maintain calm, reassuring communication; avoid arguing.
- Use distraction and redirection when agitation occurs.
- Provide rest periods to prevent fatigue and irritability.
D. Support Daily Functioning:
- Encourage self-care with assistance as needed.
- Simplify tasks into small, achievable steps.
- Provide adaptive devices to foster independence.
E. Promote Nutrition and Hydration:
- Offer finger foods if utensils are difficult to use.
- Monitor intake to prevent malnutrition and dehydration.
F. Provide Emotional and Family Support:
- Educate caregivers about disease progression and coping strategies.
- Encourage participation in support groups.
- Provide information on respite care services.
Nursing Insights:
- Nurses should adopt a patient-centered approach, focusing on dignity, respect, and comfort.
- Avoid overstimulation—use calm environments and familiar caregivers.
- Recognize caregiver fatigue early and provide resources for stress management.
1.4 Nursing Evaluation of Dementia Care
- Patient demonstrates improved orientation and reduced episodes of agitation.
- Safety maintained with no falls or injuries.
- Nutritional and hydration status stable.
- Family verbalizes understanding of disease and demonstrates coping ability.
- Patient maintains optimal level of independence in ADLs.
Pharmacological Management Of Dementia And Alzheimer’s Disease
- Pharmacologic treatment aims to slow disease progression, stabilize symptoms, and improve quality of life.
- Medications are primarily symptomatic, addressing neurotransmitter imbalances and behavioral disturbances.
1.1 Cholinesterase Inhibitors
- Mechanism of Action:
- Inhibit acetylcholinesterase enzyme, increasing acetylcholine levels in synaptic clefts.
- Enhance communication between neurons, improving memory and cognition. - Common Agents:
- Donepezil (Aricept): Used in mild to severe AD; once daily dosing.
→ Adverse effects: nausea, bradycardia, diarrhea.
- Rivastigmine (Exelon): Available as oral or transdermal patch; reduces GI effects.
- Galantamine (Razadyne): Also enhances nicotinic receptor activity. - Nursing Responsibilities:
- Monitor heart rate for bradycardia.
- Administer with food to minimize GI upset.
- Assess cognitive function periodically for drug effectiveness.
Nursing Insights:
- Early initiation improves outcomes; however, these drugs do not halt disease progression.
- Nurses should educate families on adherence and expected benefits (symptom stabilization, not cure).
1.2 NMDA Receptor Antagonists
- Agent: Memantine (Namenda)
- Mechanism:
- Blocks excessive glutamate activity at NMDA receptors, preventing excitotoxicity and neuronal death. - Indication: Moderate to severe Alzheimer’s disease, alone or combined with cholinesterase inhibitors.
- Side Effects: Dizziness, headache, constipation, confusion.
- Nursing Responsibilities:
- Monitor for cognitive changes and side effects.
- Ensure adequate hydration and slow dosage titration.
Nursing Insights:
- Combination therapy (Memantine + Donepezil) often provides greater functional stability in moderate to severe disease.
1.3 Adjunctive Medications (Antidepressants, Antipsychotics, etc.)
- Antidepressants (SSRIs):
- For depressive symptoms; e.g., sertraline, citalopram. - Antipsychotics:
- Used cautiously for severe agitation, hallucinations, or aggression (e.g., risperidone, quetiapine).
- Monitor for extrapyramidal symptoms and sedation. - Anxiolytics:
- Short-term use for anxiety or restlessness (avoid long-term benzodiazepines). - Sleep Aids:
- Non-pharmacologic sleep hygiene preferred; melatonin may be used.
Nursing Insights:
- Nurses should prioritize non-drug behavioral interventions before pharmacologic options.
- Always monitor for adverse reactions, particularly in elderly patients with comorbidities.
Psychosocial And Behavioral Management
Psychosocial interventions aim to preserve cognitive abilities, reduce behavioral disturbances, and enhance emotional well-being.
1.1 Cognitive Stimulation Therapy
- Involves structured group activities designed to improve thinking, concentration, and memory.
- Activities may include word games, music, puzzles, and discussion of current events.
- Evidence shows it improves quality of life and cognitive function in mild to moderate dementia.
Nursing Insights:
- Nurses can facilitate sessions in day-care or residential settings.
- Participation should be voluntary and enjoyable to promote engagement.
1.2 Reality Orientation
- A therapeutic approach using verbal and visual cues to reinforce person, place, and time orientation.
- Tools include clocks, calendars, labeled objects, and regular reminders.
- Enhances environmental familiarity and reduces confusion.
Nursing Insights:
- Should be applied gently; avoid correcting the patient harshly.
- Consistent caregivers help reinforce stability and trust.
1.3 Reminiscence Therapy
- Uses past experiences, photographs, and music to stimulate long-term memory.
- Strengthens identity, reduces anxiety, and improves social interaction.
Nursing Insights:
- Particularly beneficial in later stages when short-term memory is impaired.
- Nurses can use old songs, family albums, or cultural stories to elicit positive emotions.
1.4 Family and Caregiver Support
- Provide education on disease process, prognosis, and care strategies.
- Encourage respite care and support groups to prevent caregiver burnout.
- Offer guidance on managing financial, ethical, and legal aspects of long-term care.
Nursing Insights:
- Nurses serve as primary educators, advocates, and emotional support for caregivers.
- Recognizing caregiver stress early prevents neglect and improves patient care outcomes.
Complications And Prognosis
- Dementia and Alzheimer’s disease are chronic, progressive neurodegenerative disorders that lead to a multitude of complications affecting multiple systems.
- As the disease advances, patients experience deterioration in cognitive, functional, behavioral, and physiological domains.
- Understanding the potential complications and overall prognosis enables nurses to plan anticipatory care and provide holistic, evidence-based management.
1.1 Short-Term and Long-Term Complications
A. Short-Term Complications
Short-term complications commonly arise during the early to moderate stages of the disease due to impaired cognition and behavioral instability.
- Falls and Injuries:
- Disorientation, poor balance, and wandering behavior increase fall risk.
- Visual-perceptual deficits cause difficulty navigating environments.
- Fractures, head injuries, and soft tissue damage are common outcomes. - Nutritional Deficiencies:
- Forgetfulness and inability to recognize hunger or thirst lead to poor intake.
- Dysphagia and motor dysfunction may cause aspiration pneumonia. - Infections:
- Poor hygiene, urinary retention, and immobility predispose to urinary tract infections (UTIs) and respiratory infections. - Behavioral and Psychological Disturbances (BPSD):
- Includes agitation, aggression, anxiety, hallucinations, and depression.
- May lead to social isolation and caregiver burnout. - Sleep Disturbances:
- Fragmented sleep and nocturnal wandering increase fatigue and confusion. - Medication Side Effects:
- Polypharmacy heightens the risk of adverse drug reactions and delirium.
B. Long-Term Complications
These occur in the advanced stages when the patient becomes fully dependent and physiological systems decline.
- Severe Malnutrition and Dehydration:
- Progressive dysphagia and anorexia reduce intake, leading to cachexia. - Aspiration Pneumonia:
- Loss of gag reflex and poor swallowing coordination cause aspiration. - Pressure Ulcers:
- Immobility, incontinence, and poor nutrition lead to skin breakdown. - Sepsis:
- Secondary to pressure ulcers, pneumonia, or urinary infections. - Contractures and Muscle Wasting:
- Prolonged immobility leads to atrophy and deformities. - Functional Incontinence:
- Due to lack of awareness or inability to locate restrooms. - Social Isolation and Institutionalization:
- Family caregivers may be unable to manage advanced cases, resulting in long-term care placement.
Nursing Insights:
- Nurses must vigilantly monitor for early signs of infection, aspiration, and nutritional decline, which are major causes of morbidity.
- Preventive measures such as frequent repositioning, assisted feeding, fall precautions, and infection control are essential in advanced care.
- Emotional support to families during the terminal stage is crucial in providing compassionate, dignified end-of-life care.
1.2 Prognosis of Dementia and Alzheimer’s Disease
- Disease Course:
- Alzheimer’s disease is progressive and irreversible, typically spanning 8–12 years after diagnosis.
- The course may vary depending on comorbidities, genetics, and quality of care. - Mortality:
- Leading causes of death include pneumonia, sepsis, and malnutrition.
- Advanced dementia is a terminal condition with gradual decline in all body functions. - Factors Influencing Prognosis:
- Age: Older patients deteriorate faster.
- Sex: Women show higher prevalence and slightly slower decline.
- Comorbidities: Diabetes, hypertension, and cardiovascular disease accelerate progression.
- Early Diagnosis and Intervention: Early initiation of cholinesterase inhibitors may prolong function and delay institutionalization. - Functional Decline:
- Cognitive and physical abilities deteriorate progressively until complete dependency is reached.
Nursing Insights:
- Nurses should counsel families that dementia is a life-limiting illness requiring palliative and supportive care approaches.
The focus of care should shift gradually from curative to comfort, dignity, and quality of life.
Ethical And Legal Considerations In Dementia Care
- Ethical and legal challenges frequently arise in dementia care due to cognitive impairment, loss of decision-making capacity, and dependence on others for daily needs.
- Nurses play a key role in upholding ethical principles—autonomy, beneficence, nonmaleficence, and justice—while ensuring the patient’s rights are respected.
1.1 Informed Consent
- Definition:
- Informed consent refers to a patient’s voluntary agreement to treatment after receiving adequate information about the procedure, benefits, risks, and alternatives. - Challenges in Dementia:
- As cognitive function declines, the patient’s capacity to understand and consent diminishes.
- Consent may need to be obtained from a legally authorized representative or next of kin. - Nurse’s Role:
- Ensure that the patient is informed in a manner consistent with their cognitive level.
- Verify comprehension by asking the patient to restate the information.
- Document all discussions related to consent.
- Advocate for patient rights if coercion or misunderstanding is suspected.
Nursing Insights:
- Nurses should always assess for fluctuating levels of capacity, as mild dementia patients may still be capable of making simple decisions.
- Involve family members, but prioritize the patient’s preferences wherever possible.
1.2 Patient Autonomy and Capacity Assessment
- Patient Autonomy:
- Refers to the right of individuals to make decisions regarding their care and treatment.
- Dementia progressively impairs autonomy due to cognitive decline. - Capacity Assessment:
- Must be task-specific and time-specific, evaluated for each decision.
- A competent patient should be able to:
→ Understand relevant information.
→ Appreciate the consequences of decisions.
→ Communicate a consistent choice.
→ Reason about treatment options. - Legal Provisions:
- When capacity is lost, legal mechanisms such as power of attorney, guardianship, or advance directives are implemented.
Nurse’s Role:
- Collaborate with physicians and legal representatives in capacity evaluation.
- Support patient participation in decisions to the fullest extent possible.
- Respect cultural and individual values regarding autonomy and dependence.
Nursing Insights:
- Nurses should be familiar with local laws and institutional policies governing capacity and guardianship.
- Advocacy for the patient’s best interests is paramount, especially in cases of neglect or exploitation.
1.3 End-of-Life Decision-Making
End-of-life care in dementia involves making decisions about resuscitation, artificial nutrition, hydration, and life-prolonging interventions as cognitive decline progresses.
- Advance Directives:
- Legal documents expressing the patient’s wishes regarding treatment when they lose decision-making capacity.
- May include Do Not Resuscitate (DNR) orders and preferences for comfort-focused care. - Palliative and Hospice Care:
- Focus on symptom control, comfort, and dignity rather than curative treatment.
- Prioritizes management of pain, dyspnea, and agitation. - Ethical Dilemmas:
- Conflicts may arise between family desires for aggressive treatment and professional recommendations for comfort care.
- Nurses must balance beneficence (doing good) and nonmaleficence (avoiding harm).
Nurse’s Role:
- Facilitate discussions between healthcare providers and families regarding goals of care.
- Ensure that the patient’s prior wishes, cultural beliefs, and dignity are respected.
- Provide emotional support to families during bereavement.
Nursing Insights:
- Nurses are critical in ensuring that end-of-life care aligns with ethical principles and the patient’s known or presumed wishes.
- Compassionate communication and empathy are key to helping families accept the natural course of dementia.
Prevention And Health Education
- Dementia and Alzheimer’s disease are major global public health issues with no definitive cure, making prevention and health education critical in reducing incidence, delaying onset, and mitigating complications.
- Nurses have a central role in educating individuals, families, and communities about risk reduction strategies, early detection, and maintenance of brain health.
1.1 Primary Prevention
Primary prevention targets individuals before disease onset to minimize risk factors that predispose to dementia and Alzheimer’s disease.
A. Lifestyle Modifications:
- Cognitive Stimulation:
- Encourage mental exercises such as reading, puzzles, crosswords, and learning new languages to enhance neuroplasticity. - Physical Activity:
- Regular aerobic and resistance exercises improve cerebral circulation and reduce vascular dementia risk.
- Recommendations: ≥150 minutes of moderate exercise weekly. - Balanced Diet:
- Adoption of the Mediterranean diet rich in fruits, vegetables, whole grains, nuts, fish, and olive oil.
- Limit saturated fats, refined sugars, and processed foods. - Social Interaction:
- Promote regular engagement in social activities and community participation to prevent isolation and depression. - Cardiovascular Health:
- Manage hypertension, diabetes, obesity, and dyslipidemia to reduce cerebrovascular injury. - Avoidance of Neurotoxins:
- Discourage smoking, excessive alcohol consumption, and exposure to environmental toxins (e.g., heavy metals).
B. Public Health Measures:
- Conduct community education programs on maintaining brain health.
- Encourage periodic screening for cognitive decline in older adults.
- Support vaccination programs against infections that may precipitate delirium (e.g., influenza, pneumococcal vaccines).
Nursing Insights:
- Nurses should integrate brain health education into community outreach and primary care consultations.
- Early identification of at-risk individuals enables preventive interventions before irreversible neuronal damage occurs.
1.2 Secondary Prevention
Secondary prevention aims to detect early disease and slow its progression through timely diagnosis and intervention.
A. Early Detection:
- Utilize cognitive screening tools such as MMSE, MoCA, and Clock Drawing Test in routine assessments for elderly clients.
- Recognize early warning signs such as forgetfulness, apathy, irritability, and decreased problem-solving ability.
B. Prompt Intervention:
- Initiate cholinesterase inhibitors (Donepezil, Rivastigmine, Galantamine) early in mild cases.
- Start cognitive stimulation therapy and structured routines to maintain independence.
C. Management of Comorbidities:
- Optimize control of hypertension, diabetes, dyslipidemia, and heart disease.
- Encourage smoking cessation and moderate alcohol use.
D. Family Education:
- Provide teaching on the significance of early consultation and regular follow-up.
- Direct families to support services, day-care programs, and local memory clinics.
Nursing Insights:
- Nurses are instrumental in detecting subtle cognitive changes that may go unnoticed in clinical settings.
- Early intervention can delay institutionalization and preserve patient autonomy longer.
1.3 Tertiary Prevention
Tertiary prevention seeks to reduce disability, prevent complications, and improve quality of life for patients with established dementia or Alzheimer’s disease.
A. Supportive and Rehabilitative Care:
- Maintain patient mobility through physiotherapy and regular ambulation.
- Provide occupational therapy to promote independence in daily activities.
B. Complication Prevention:
- Prevent falls by using bed alarms, clear pathways, and proper footwear.
- Prevent aspiration by ensuring correct positioning during meals and providing texture-modified diets.
- Implement turning schedules to avoid pressure injuries.
C. Caregiver and Family Support:
- Offer psychological support, respite care, and education on symptom management.
- Teach stress reduction and coping strategies to prevent burnout.
D. Long-Term Planning:
- Assist families in planning for advanced disease stages, including palliative care options.
- Collaborate with social services for long-term care placement when necessary.
Nursing Insights:
- The focus in tertiary prevention should shift toward comfort, dignity, and functional maintenance.
- Nurses must regularly assess for caregiver fatigue and connect families to community-based resources.
Role Of The Nurse In Community And Institutional Care
- Nurses function as educators, caregivers, advocates, and coordinators across all settings of dementia care.
- Their role spans prevention, clinical management, rehabilitation, and support for patients and caregivers both in the community and institutional environments.
1.1 Health Promotion in the Community
A. Community Health Education:
- Conduct awareness campaigns about dementia risk factors, symptoms, and prevention strategies.
- Dispel myths and stigma surrounding mental health and aging.
B. Screening and Early Detection:
- Participate in community outreach programs offering cognitive assessments for older adults.
- Facilitate referrals to specialized memory clinics.
C. Support Group Initiatives:
- Establish and facilitate caregiver support groups to share experiences and coping techniques.
- Promote social interaction for both patients and caregivers.
D. Advocacy:
- Advocate for accessible mental health services, dementia-friendly environments, and policies that protect elderly rights.
E. Home-Based Care and Follow-Up:
- Conduct home visits to assess environmental safety, nutrition, and caregiver competency.
- Provide education on behavioral management and medication adherence.
Nursing Insights:
- Community nurses are essential in maintaining continuity of care between hospital and home.
- Empathy and effective communication foster trust, adherence, and improved outcomes.
1.2 Institutional Support and Multidisciplinary Team Role
A. Institutional Care Settings:
- Ensure a safe, structured, and supportive environment tailored to dementia patients.
- Incorporate therapeutic activities such as music therapy, reminiscence, and reality orientation.
B. Multidisciplinary Collaboration:
- Physician: Diagnosis, medical treatment, and disease monitoring.
- Psychiatrist/Psychologist: Manage behavioral and emotional issues.
- Physiotherapist/Occupational Therapist: Support functional mobility and independence.
- Dietitian: Develop nutrition plans preventing malnutrition and dehydration.
- Social Worker: Provide counseling, coordinate financial and social resources.
- Nurse: Monitor daily health status, administer medications, educate families, and coordinate team communication.
C. Role of the Nurse:
- Implement individualized care plans and ensure holistic attention to physical, emotional, and spiritual needs.
- Prevent complications through vigilant observation and early intervention.
- Serve as the primary advocate for patient dignity, respect, and comfort.
Nursing Insights:
- Nurses bridge communication gaps between the patient, family, and multidisciplinary team, ensuring seamless and compassionate care.
- Institutional nurses must regularly reassess care goals and adapt interventions as the disease progresses.
Summary
- Dementia is a progressive, irreversible cognitive decline impairing memory, reasoning, and daily functioning.
- Alzheimer’s disease is the leading cause of dementia, characterized by β-amyloid plaque accumulation and neurofibrillary tangles leading to neuronal loss.
- Pathophysiology involves acetylcholine deficiency, synaptic degeneration, and cortical atrophy.
- Clinical presentation includes progressive memory loss, disorientation, behavioral changes, and eventual dependency.
- Diagnosis utilizes cognitive tests, neuroimaging, and laboratory assessments to exclude reversible causes.
- Management combines pharmacologic therapy (cholinesterase inhibitors, NMDA antagonists) with psychosocial and nursing interventions.
- Complications such as aspiration, infections, pressure ulcers, and caregiver burnout require proactive nursing care.
- Ethical and legal aspects involve respecting autonomy, ensuring informed consent, and guiding end-of-life decisions.
- Preventive measures—primary, secondary, and tertiary—are essential to reduce disease burden.
- Nurses serve as advocates, educators, and caregivers in both community and institutional contexts, ensuring holistic, compassionate, and patient-centered dementia care.
