
Fertilization and Implantation, Fetal Environment
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- To describe the physiological processes of fertilization, including sperm and ovum transport, and the events leading to zygote formation.
- To explain the stages of early embryonic development from cleavage to blastocyst formation and the intricate process of implantation into the uterine wall.
- To identify the key components of the fetal environment, specifically the amnion, chorion, amniotic fluid, and placenta.
- To elucidate the structural characteristics and essential functions of the amnion, chorion, and amniotic fluid in supporting fetal growth and protection.
- To detail the comprehensive structure, development, and multifaceted functions of the placenta, emphasizing its critical roles in endocrine regulation, metabolism, and substance exchange between mother and fetus.
- To recognize potential deviations from normal amniotic fluid volume and placental variations that may impact maternal and fetal well-being.
Introduction
The journey from conception to the development of a viable fetus is an extraordinary biological marvel, orchestrated by a series of precise and coordinated cellular and molecular events. This intricate process commences with fertilization, the union of male and female gametes, followed by the crucial phase of implantation, where the nascent embryo establishes a vital connection with the maternal endometrium. Concurrently, a specialized fetal environment begins to form, encompassing the amnion, chorion, amniotic fluid, and the placenta. These structures collectively provide the necessary support, protection, and sustenance for the developing fetus throughout gestation. A profound understanding of these foundational maternal-newborn topics is paramount for nursing students, as it forms the basis for comprehending normal pregnancy progression, identifying potential complications, and delivering comprehensive, evidence-based care to both mother and child.
Fertilization
Fertilization is the fusion of male and female gametes (spermatozoon and ovum) to form a new individual, the zygote. This remarkable event typically occurs in the ampulla of the fallopian tube.
1. Sperm Transport and Capacitation
Spermatozoa are deposited in the vagina during coitus and must navigate a challenging journey through the cervix, uterus, and fallopian tubes to reach the ovum.
- Vaginal and Cervical Passage:
- The acidic environment of the vagina is hostile to sperm, with many being immobilized or killed.
- Cervical mucus, particularly around ovulation, becomes less viscous and forms channels, facilitating sperm passage into the uterus.
- Some sperm are stored in cervical crypts and released over several hours, contributing to sustained fertility.
- Uterine and Tubal Transport:
- Uterine contractions and the inherent motility of sperm aid their ascent through the uterine cavity and into the fallopian tubes.
- Only a small fraction of ejaculated sperm, typically a few hundred, reach the ampulla.
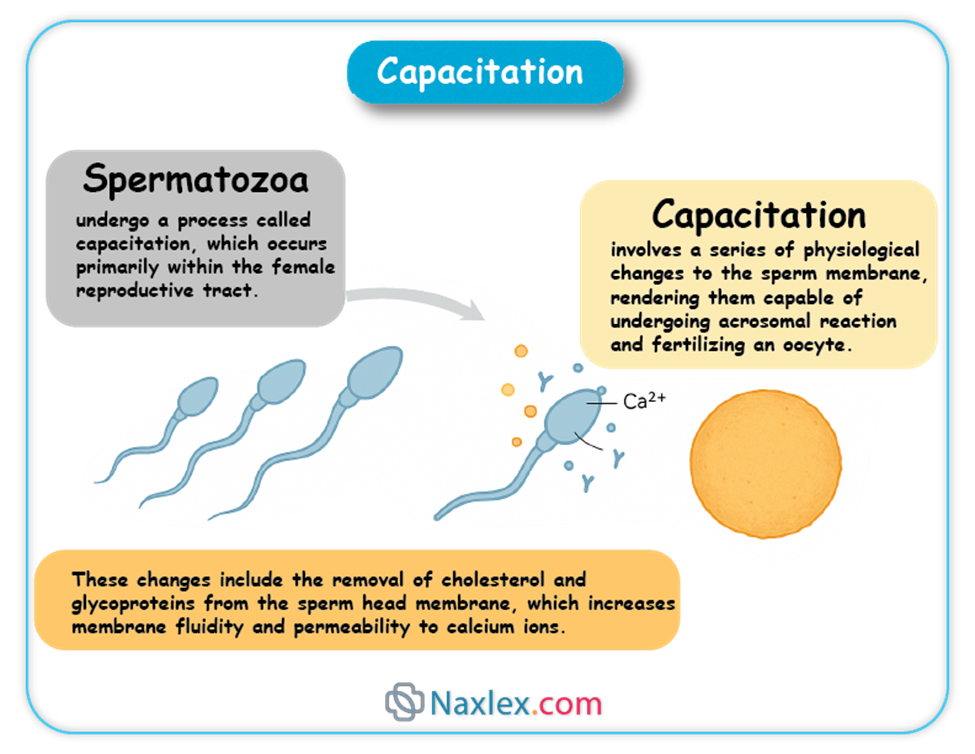
- Capacitation:
- Spermatozoa undergo a process called capacitation, which occurs primarily within the female reproductive tract.
- Capacitation involves a series of physiological changes to the sperm membrane, rendering them capable of undergoing the acrosomal reaction and fertilizing an oocyte.
- These changes include the removal of cholesterol and glycoproteins from the sperm head membrane, which increases membrane fluidity and permeability to calcium ions.
2. Ovum Transport
Ovulation typically releases a secondary oocyte, arrested in metaphase II of meiosis, from the graafian follicle.
- Fimbrial Capture:
- The fimbriae, finger-like projections at the end of the fallopian tube, sweep over the surface of the ovary and, through ciliary action, capture the released oocyte.
- Tubal Peristalsis and Ciliary Action:
- Once inside the fallopian tube, the oocyte is propelled towards the uterus by the rhythmic contractions (peristalsis) of the smooth muscle walls of the tube and the coordinated beating of cilia lining the tubal epithelium.
- Viability:
- The oocyte remains viable for fertilization for approximately 12-24 hours after ovulation.
3. The Process of Fertilization
Once capacitated sperm encounter the ovum, a series of events leads to the fusion of their genetic material.
3.1. Acrosomal Reaction
- Upon binding to the zona pellucida, the outer glycoprotein layer surrounding the ovum, capacitated sperm undergo the acrosomal reaction.
- This reaction involves the fusion of the outer acrosomal membrane with the sperm plasma membrane, leading to the release of hydrolytic enzymes, including hyaluronidase and acrosin.
- These enzymes are crucial for digesting the cumulus oophorus (granulosa cells surrounding the ovum) and creating a path through the zona pellucida for the sperm to reach the oocyte membrane.
3.2. Cortical Reaction (Block to Polyspermy)
- As soon as the first sperm makes contact with the oocyte plasma membrane, a rapid depolarization of the oocyte membrane occurs, known as the "fast block to polyspermy." This transient electrical change prevents immediate fusion by other sperm.
- Simultaneously, a more permanent "slow block to polyspermy" is initiated, called the cortical reaction.
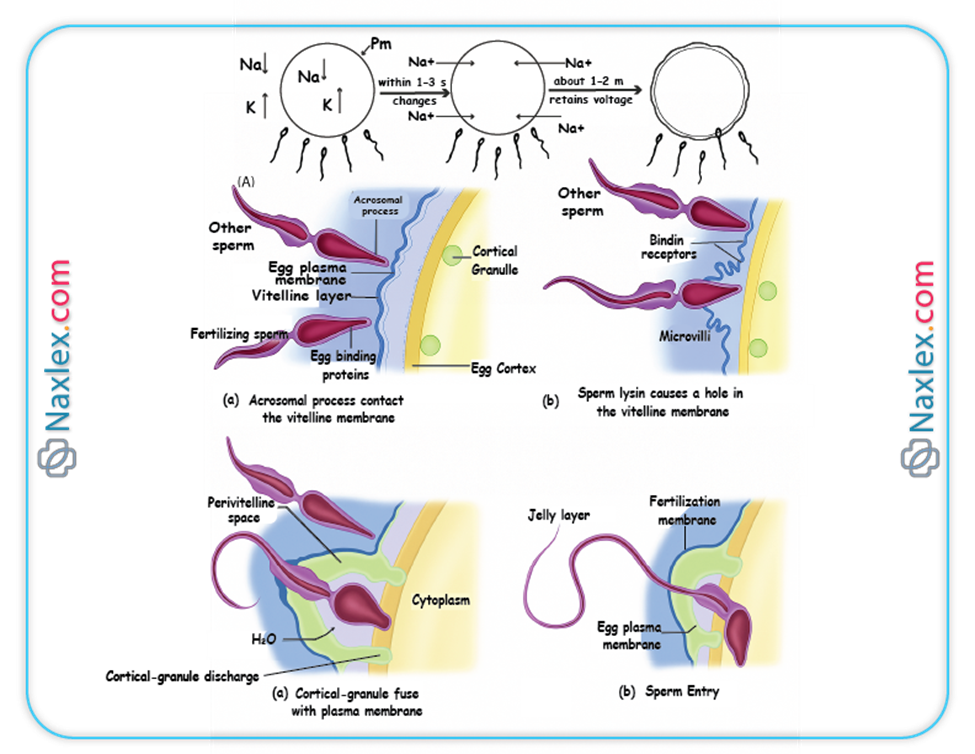
- The cortical reaction involves the release of cortical granules (lysosome-like vesicles located just beneath the oocyte membrane) into the perivitelline space (the space between the oocyte membrane and the zona pellucida).
- The enzymes released from these granules alter the structure of the zona pellucida (zona reaction), hardening it and inactivating sperm receptors, thereby preventing additional sperm from penetrating the oocyte. This ensures monospermy (fertilization by only one sperm).
3.3. Formation of the Zygote
- Once a single sperm enters the oocyte cytoplasm, it triggers the completion of meiosis II by the secondary oocyte, resulting in a mature ovum and the second polar body.
- The nucleus of the sperm decondenses and forms the male pronucleus.
- The nucleus of the mature ovum forms the female pronucleus.
- Both pronuclei replicate their DNA, and then their nuclear envelopes break down, allowing the chromosomes to combine, forming a single diploid nucleus.
- The cell containing this new diploid nucleus is now called a zygote, marking the successful completion of fertilization.
Nursing Insights: The understanding of fertilization is critical for nurses, especially in reproductive health and infertility. Explaining the timing of ovulation and the importance of sperm viability aids in patient education regarding conception. Recognizing that polyspermy is a lethal condition for the embryo highlights the precision of natural biological processes.
Implantation
Implantation is the process by which the blastocyst, the early stage of embryonic development, attaches to and invades the maternal endometrium. This crucial event typically occurs around 6-10 days after fertilization.
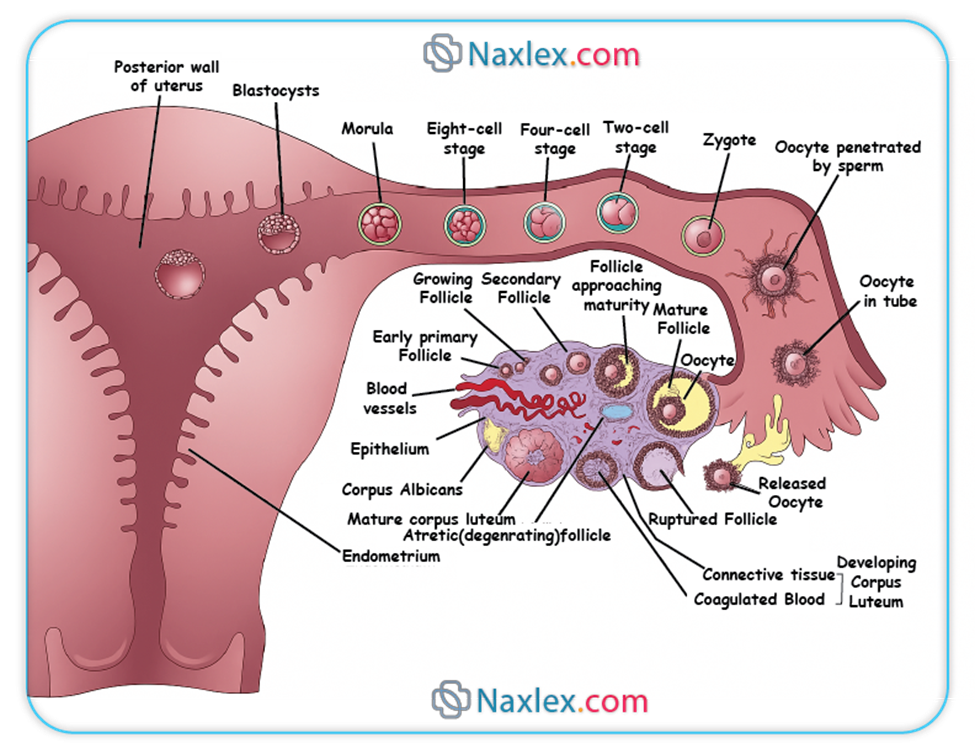
1. Cleavage and Morula Formation
- Following fertilization, the zygote undergoes a series of rapid mitotic divisions called cleavage.
- These divisions occur without significant growth of the overall cell mass, meaning the daughter cells (blastomeres) become progressively smaller with each division.
- Day 1-2: The zygote divides into two blastomeres, then four.
- Day 3: The embryo consists of 8-16 blastomeres and is termed a morula (resembling a mulberry). The morula is still encased within the zona pellucida and is transported through the fallopian tube towards the uterus.
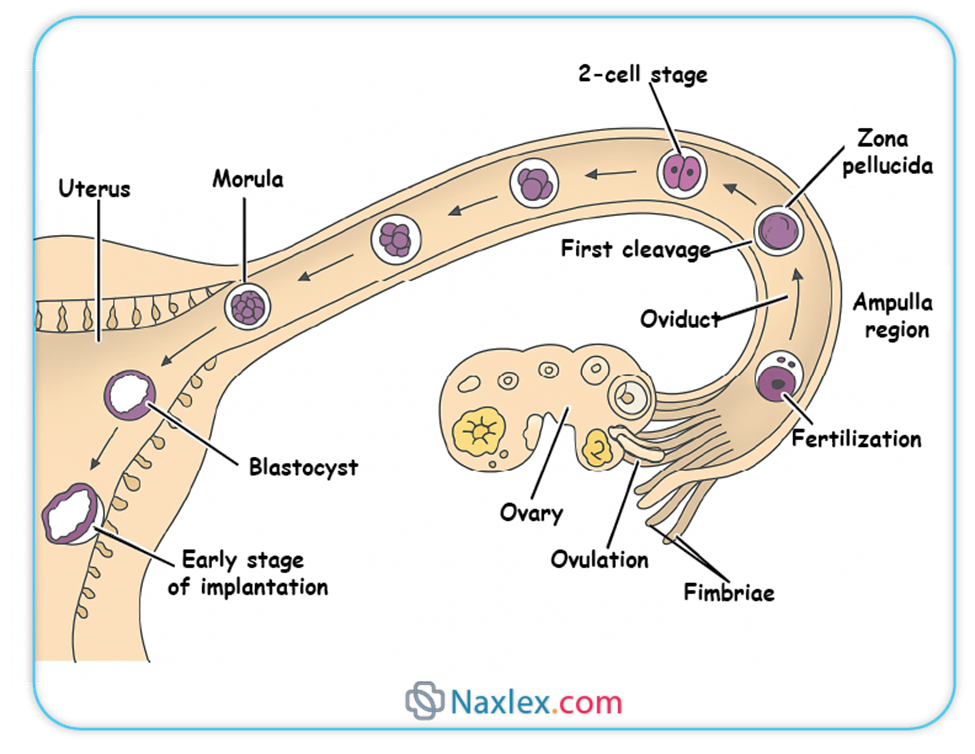
2. Blastocyst Formation
- As the morula enters the uterine cavity around day 4, fluid begins to penetrate the zona pellucida and accumulate within the intercellular spaces of the morula.
- This fluid coalesces to form a single fluid-filled cavity called the blastocoel (or blastocyst cavity).
- The cells of the morula differentiate into two distinct cell populations:
- Inner Cell Mass (ICM) or Embryoblast: A group of cells clustered at one pole of the blastocyst. These cells will give rise to the embryo proper and some extraembryonic membranes.
- Trophoblast: An outer layer of flattened cells surrounding the blastocoel and the inner cell mass. The trophoblast plays a crucial role in implantation and the formation of the placenta.
- At this stage, the embryo is called a blastocyst. Around day 5, the blastocyst "hatches" from the zona pellucida, allowing it to directly interact with the endometrial lining.
3. Process of Implantation
Implantation is a complex process involving several stages:
- Apposition:
- The blastocyst comes into close proximity with the endometrial lining. This is a transient and unstable adhesion.
- Adhesion (Attachment):
- The trophoblast cells of the blastocyst firmly attach to the endometrial epithelium.
- This attachment is mediated by various adhesion molecules, including integrins, selectins, and cadherins, expressed on both the trophoblast and endometrial cells.
- Invasion (Penetration):
- The trophoblast differentiates into two layers:
- Cytotrophoblast: The inner layer, composed of distinct cells with mitotic activity.
- Syncytiotrophoblast: The outer multinucleated layer formed by the fusion of cytotrophoblast cells. The syncytiotrophoblast lacks distinct cell boundaries and directly invades the maternal endometrium.
- The syncytiotrophoblast produces proteolytic enzymes (e.g., matrix metalloproteinases) that degrade the extracellular matrix of the endometrial tissue, allowing the blastocyst to burrow into the uterine wall.
- Lacunae (spaces) form within the syncytiotrophoblast, which will eventually fill with maternal blood, establishing the uteroplacental circulation.
- The trophoblast differentiates into two layers:
- Embedding:
- The blastocyst becomes completely embedded within the endometrial stroma, and the defect in the endometrial surface is sealed by a fibrin coagulum. This typically occurs by day 10-12 post-fertilization.
4. Decidua Formation
- In response to the invading blastocyst and hormonal influences (primarily progesterone), the endometrial stromal cells undergo a process called decidualization.
- Decidualization transforms the endometrial stromal cells into large, polyhedral decidual cells, rich in glycogen and lipids.
- The decidua provides an immunologically privileged environment for the developing embryo and plays a vital role in regulating trophoblast invasion and subsequent placental development.
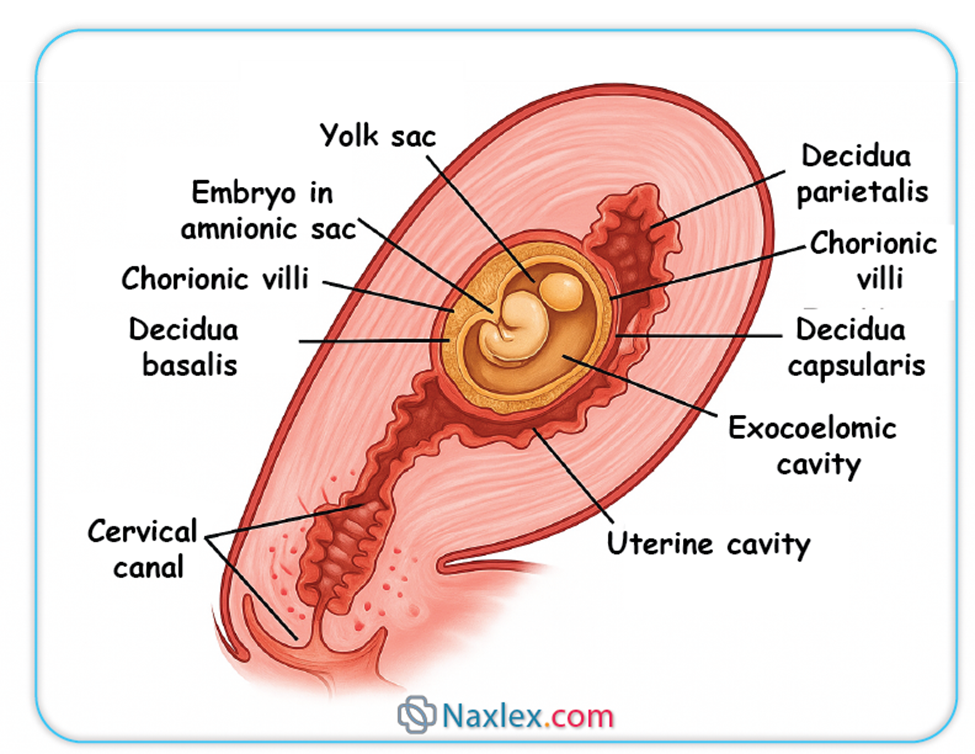
- Three regions of the decidua are recognized:
- Decidua Basalis: The portion of the decidua located beneath the implanted blastocyst, forming the maternal component of the placenta.
- Decidua Capsularis: The portion of the decidua overlying the implanted blastocyst, separating it from the uterine lumen. As the embryo grows, this layer becomes thin and eventually fuses with the decidua parietalis.
- Decidua Parietalis (Vera): The remaining part of the decidua lining the rest of the uterine cavity.
Nursing Insights: The timing and location of implantation are crucial. Ectopic pregnancies, where implantation occurs outside the uterus (most commonly in the fallopian tube), are a significant concern. Nurses must be aware of the signs and symptoms of ectopic pregnancy to ensure timely intervention, as it can be life-threatening. Understanding decidua formation also provides context for interpreting early pregnancy ultrasound findings.
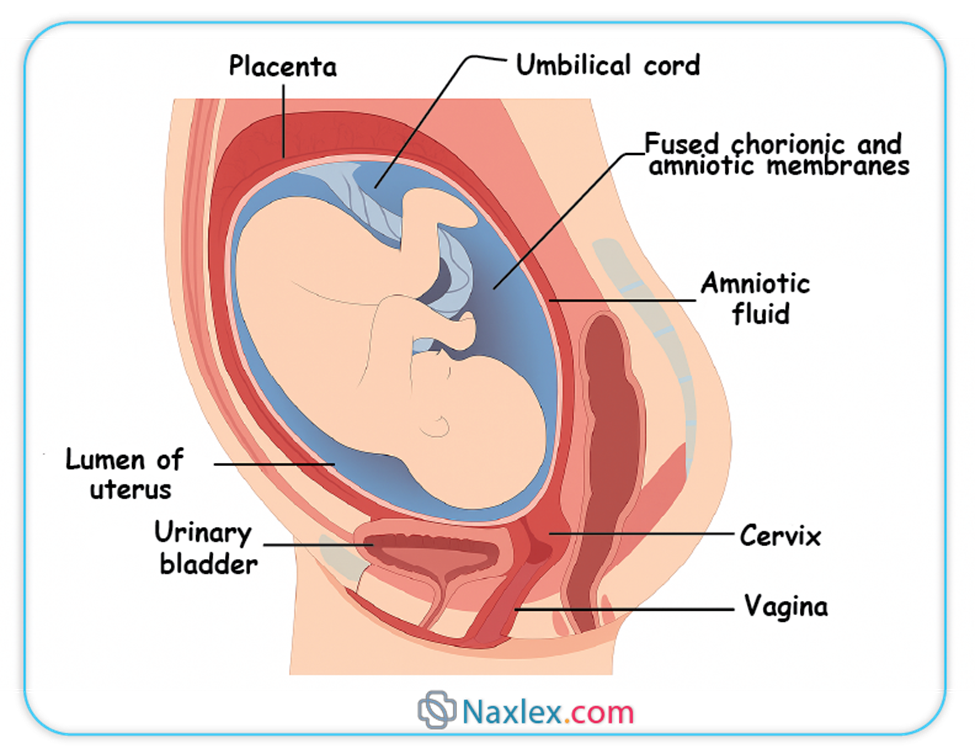
Fetal Environment
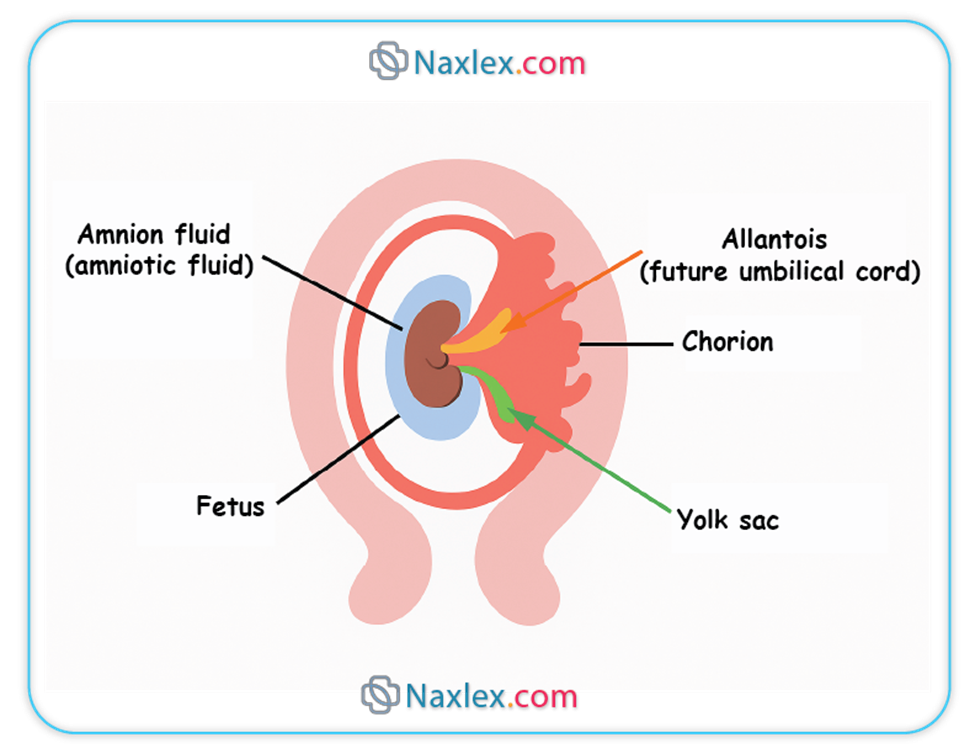
The fetal environment refers to the structures that surround and support the developing fetus within the uterus. These include the amnion, chorion, amniotic fluid, and the placenta.
1. AMNION
The amnion is the innermost fetal membrane, forming a fluid-filled sac that directly encloses the embryo and later the fetus.
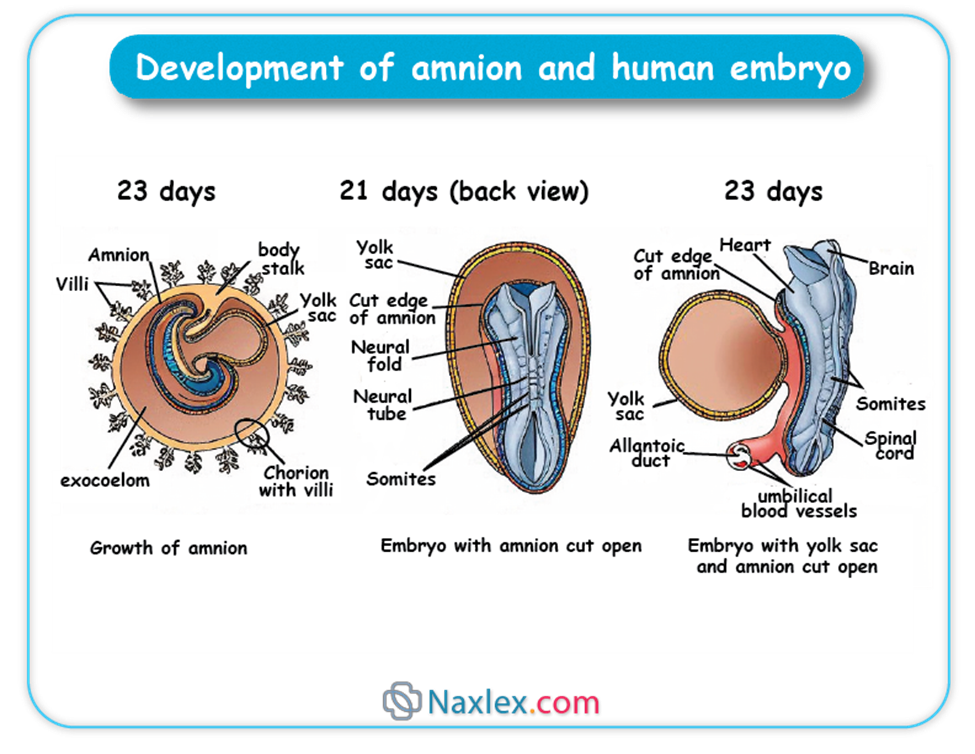
1.1. Structure and Development
- The amnion develops from the epiblast during the second week of embryonic development, forming a thin, transparent membrane.
- Initially, the amnion is small and closely surrounds the embryonic disc.
- As the embryo grows and folds, the amnion expands rapidly to enclose the entire embryo, forming the amniotic cavity.
- The amniotic cavity eventually obliterates the chorionic cavity by fusing with the chorion, typically by the end of the first trimester.
- The amnion is composed of two layers:
- Amniotic Epithelium: An inner layer of simple cuboidal or columnar epithelial cells that face the amniotic fluid. These cells are responsible for secreting and absorbing amniotic fluid.
- Amniotic Mesoderm: An outer layer of connective tissue that is continuous with the chorion.
1.2. Functions of the Amnion
The amnion plays several vital roles in protecting and supporting the developing fetus:
- Formation of the Amniotic Cavity: It creates the space in which the fetus can grow and move freely.
- Production of Amniotic Fluid: The amniotic epithelial cells contribute to the secretion of amniotic fluid.
- Protection:
- Shock Absorber: The fluid-filled sac acts as a buffer against external mechanical trauma or pressure on the uterus.
- Temperature Regulation: It helps maintain a relatively constant temperature for the fetus.
- Prevents Adhesion: It prevents the amnion from adhering to the fetal skin, which could lead to congenital anomalies (amniotic band syndrome).
- Facilitates Fetal Movement and Growth:
- Allows for symmetrical musculoskeletal development by providing space for limb movement and preventing compression.
- Facilitates fetal swallowing and respiratory movements, contributing to the development of the gastrointestinal and respiratory systems, respectively.
Nursing Insights: Understanding the amnion's protective role helps nurses explain the importance of preventing abdominal trauma during pregnancy. Awareness of amniotic band syndrome, though rare, underscores the delicate nature of fetal development and the potential for mechanical forces to impact it.
2. CHORION
The chorion is the outermost fetal membrane, forming the protective sac that surrounds the amnion and the developing embryo/fetus.
2.1. Structure and Development
- The chorion develops from the trophoblast and extraembryonic mesoderm.
- It consists of two layers:
- Trophoblast: The outer layer, which further differentiates into cytotrophoblast and syncytiotrophoblast.
- Somatic Layer of Extraembryonic Mesoderm: An inner layer that lies beneath the trophoblast.
- Initially, the chorion is covered by chorionic villi all around its surface.
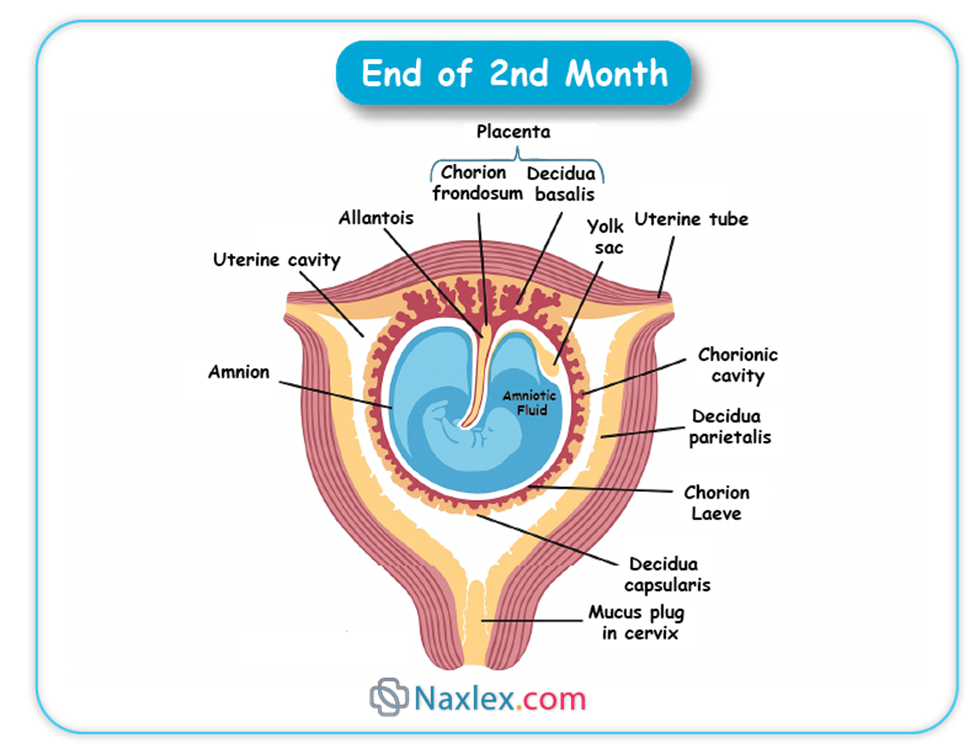
- As pregnancy progresses, the villi associated with the decidua capsularis degenerate, forming the smooth chorion (chorion laeve).
- The villi adjacent to the decidua basalis proliferate and branch extensively, forming the bushy chorion (chorion frondosum), which contributes to the fetal part of the placenta.
- The chorion encloses the amniotic sac, the yolk sac, and the connecting stalk.
2.2. Functions of the Chorion
The chorion serves several critical functions:
- Formation of the Placenta: The chorion frondosum is the primary fetal component of the placenta.
- Exchange of Substances: Through the chorionic villi, it facilitates the exchange of nutrients, gases, and waste products between the maternal and fetal circulations.
- Hormone Production: The syncytiotrophoblast of the chorion produces various hormones essential for maintaining pregnancy, including human chorionic gonadotropin (hCG), progesterone, and estrogen.
- Protection: Along with the amnion, it forms a protective barrier around the fetus.
- Immunological Role: It helps to modulate the maternal immune response to prevent rejection of the fetal allograft.
Nursing Insights: The chorion's role in placenta formation is fundamental to understanding nutrient and waste exchange, which is directly relevant to fetal growth and well-being. The production of hCG by the chorion is the basis for most pregnancy tests, a key nursing assessment tool.
3. AMNIOTIC FLUID
Amniotic fluid is the clear, yellowish fluid that fills the amniotic sac, surrounding and protecting the developing fetus.
3.1. Origin and Composition
The origin and composition of amniotic fluid change throughout gestation:
- Early Pregnancy (First Trimester):
- Primarily derived from maternal plasma by diffusion across the amniotic membrane and fetal skin.
- A small amount is also contributed by secretion from the amniotic epithelial cells.
- Mid-to-Late Pregnancy (Second and Third Trimesters):
- Fetal Urine: Becomes the major contributor to amniotic fluid volume, starting around 10-12 weeks of gestation. The fetus swallows amniotic fluid, absorbs it into the bloodstream, and then excretes dilute urine into the amniotic cavity.
- Fetal Lung Fluid: Secretions from the fetal lungs also contribute to the fluid volume.
- Transudation Across Fetal Skin: Prior to keratinization (around 20-25 weeks), water and solutes can diffuse across the fetal skin. After keratinization, this contribution significantly decreases.
- Maternal Sources: Some fluid continues to transudate from the maternal circulation across the uteroplacental membranes.
- Composition:
- Primarily water (98-99%).
- Contains electrolytes, proteins, carbohydrates, lipids, urea, creatinine, hormones, enzymes, fetal cells (skin, genitourinary, gastrointestinal), vernix caseosa, and lanugo.
- The specific gravity is typically 1.008-1.010.
3.2. Functions of Amniotic Fluid
Amniotic fluid performs numerous vital functions for fetal development and protection:
- Protection from Trauma:
- Acts as a shock absorber, cushioning the fetus from external blows or pressure on the maternal abdomen.
- Temperature Regulation:
- Helps maintain a stable fetal body temperature, buffering against abrupt thermal changes.
- Musculoskeletal Development:
- Provides space for symmetrical growth and development of the fetal limbs and musculoskeletal system, allowing for freedom of movement.
- Prevents compression of the umbilical cord.
- Lung Development:
- Fetal breathing movements, involving the aspiration and expulsion of amniotic fluid, are essential for lung maturation and development of the pulmonary system.
- Gastrointestinal Development:
- Fetal swallowing of amniotic fluid contributes to the development and maturation of the gastrointestinal tract and aids in fluid and electrolyte balance.
- Prevents Adhesions:
- Keeps the fetal skin from adhering to the amnion.
- Antibacterial Properties:
- Contains some antibacterial substances that offer a minor degree of protection against infection.
- Diagnostic Tool:
- Amniocentesis (sampling of amniotic fluid) can be used to assess fetal chromosomal abnormalities, genetic disorders, and lung maturity.
3.3. Amniotic Fluid Volume
The volume of amniotic fluid fluctuates throughout pregnancy, typically increasing until 34-36 weeks gestation and then slightly decreasing. Normal volume is generally considered to be 800-1000 mL at term. Abnormalities in volume can indicate underlying fetal or maternal issues.
3.3.1. Polyhydramnios (Hydramnios)
- Definition: Excessive accumulation of amniotic fluid, typically defined as an amniotic fluid index (AFI) greater than 24-25 cm or a single deepest pocket (SDP) greater than 8 cm.
- Causes:
- Fetal Factors (most common):
- Fetal Dysphagia/Anencephaly: Inability of the fetus to swallow amniotic fluid (e.g., esophageal atresia, anencephaly, other CNS anomalies affecting swallowing reflex).
- Fetal Hydrops: Generalized edema in the fetus, leading to increased fluid accumulation.
- Chromosomal Abnormalities: Trisomy 18, 21.
- Fetal Tumors: Rarely, can obstruct swallowing or increase fluid production.
- Maternal Factors:
- Maternal Diabetes Mellitus: Poorly controlled maternal hyperglycemia can lead to fetal polyuria.
- Idiopathic: In many cases, no specific cause is identified.
- Placental Factors:
- Chorioangioma: A benign placental tumor that can lead to increased fluid production.
- Multiple Gestation: Especially in twin-twin transfusion syndrome.
- Fetal Factors (most common):
- Clinical Significance:
- Increased risk of preterm labor and premature rupture of membranes (PROM).
- Maternal discomfort (dyspnea, abdominal distension).
- Increased risk of postpartum hemorrhage due to uterine overdistension.
- Fetal malpresentation (breech, transverse lie).
- Umbilical cord prolapse upon rupture of membranes.
3.3.2. Oligohydramnios
- Definition: Insufficient amount of amniotic fluid, typically defined as an AFI less than 5 cm or an SDP less than 2 cm.
- Causes:
- Fetal Factors (most common):
- Renal Agenesis (Potter's Syndrome): Absence or severe underdevelopment of fetal kidneys, leading to absence or severely reduced urine production.
- Urinary Tract Obstruction: Blockage in the fetal urinary tract (e.g., posterior urethral valves), preventing urine excretion.
- Fetal Growth Restriction (FGR): Redistribution of blood flow away from non-essential organs, including the kidneys, in compromised fetuses.
- Premature Rupture of Membranes (PROM): Leakage of amniotic fluid.
- Maternal Factors:
- Dehydration.
- Placental Insufficiency: Reduced blood flow to the placenta, impacting fetal renal perfusion.
- Medications: Certain drugs, especially NSAIDs (e.g., indomethacin) used for preterm labor, can reduce fetal urine output.
- Post-term Pregnancy: Decreased placental function can lead to reduced fluid production.
- Fetal Factors (most common):
- Clinical Significance:
- Increased risk of fetal lung hypoplasia (underdevelopment of lungs) due to lack of fluid for breathing movements.
- Skeletal deformities (e.g., clubfoot, facial compression) due to uterine compression.
- Umbilical cord compression, leading to variable decelerations and fetal hypoxia.
- Fetal growth restriction.
- Increased risk of stillbirth.
Nursing Insights: Nurses play a crucial role in assessing amniotic fluid volume through physical examination (fundal height) and monitoring ultrasound reports. Explaining the implications of abnormal fluid volumes to expectant parents is essential, as is preparing them for potential interventions or complications associated with polyhydramnios or oligohydramnios.
Placenta
The placenta is a remarkable temporary organ that serves as the primary interface between the mother and the developing fetus, facilitating crucial exchange processes and hormone production essential for pregnancy maintenance.
1. Structure and Development
- Development:
- Begins to form during implantation from the trophoblast of the blastocyst and the decidua basalis of the uterus.
- The chorion frondosum (bushy chorion) forms the fetal component, while the decidua basalis forms the maternal component.
- By the end of the first trimester (approximately 12 weeks), the placenta is fully formed and functional.
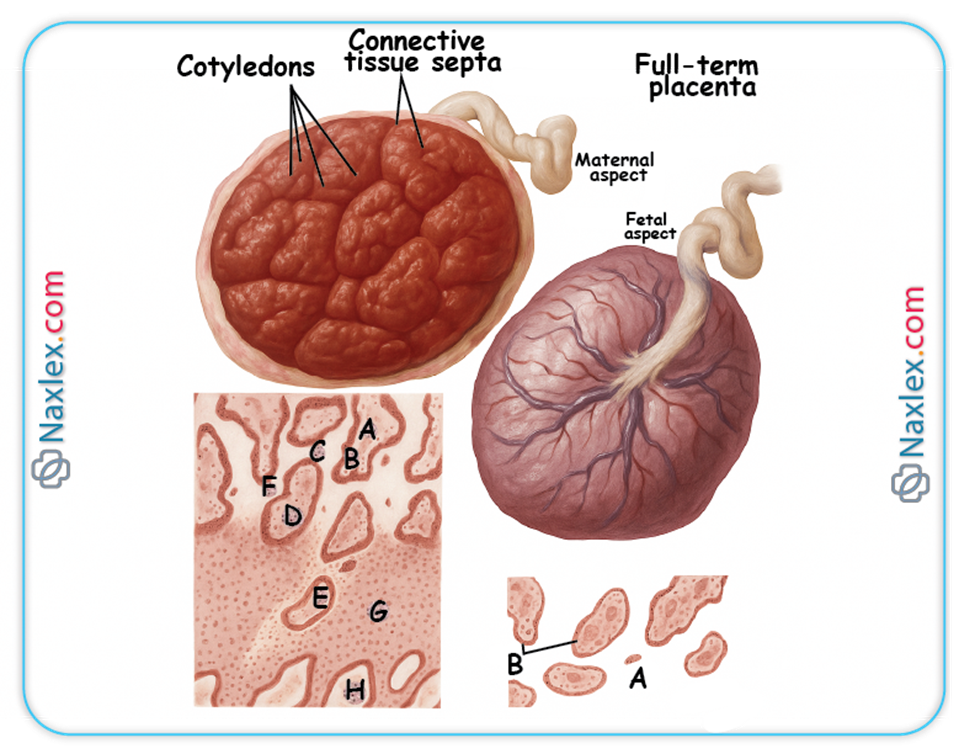
- Gross Structure at Term:
- Shape: Typically discoid or disc-shaped.
- Size: Approximately 15-20 cm in diameter, 2-3 cm thick at the center.
- Weight: Around 500-600 grams (about 1/6th of the fetal weight).
- Two Surfaces:
- Maternal Surface (Cotyledons): Appears rough and irregular, divided into 15-20 convex areas called cotyledons, which are formed by decidual septa. The cotyledons represent the lobes of the placenta, each containing a main stem villus and its branches.
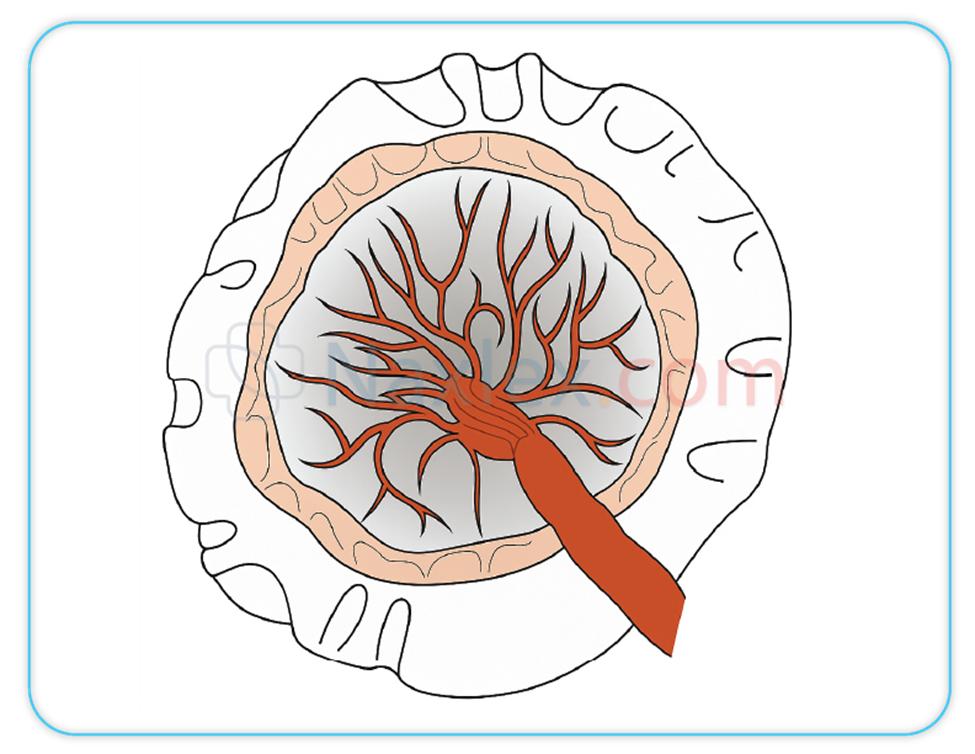
- Fetal Surface (Shiny Schultze): Appears smooth and shiny, covered by the amnion. The umbilical cord typically inserts near the center, and blood vessels (umbilical arteries and vein) can be seen radiating from the cord insertion site.
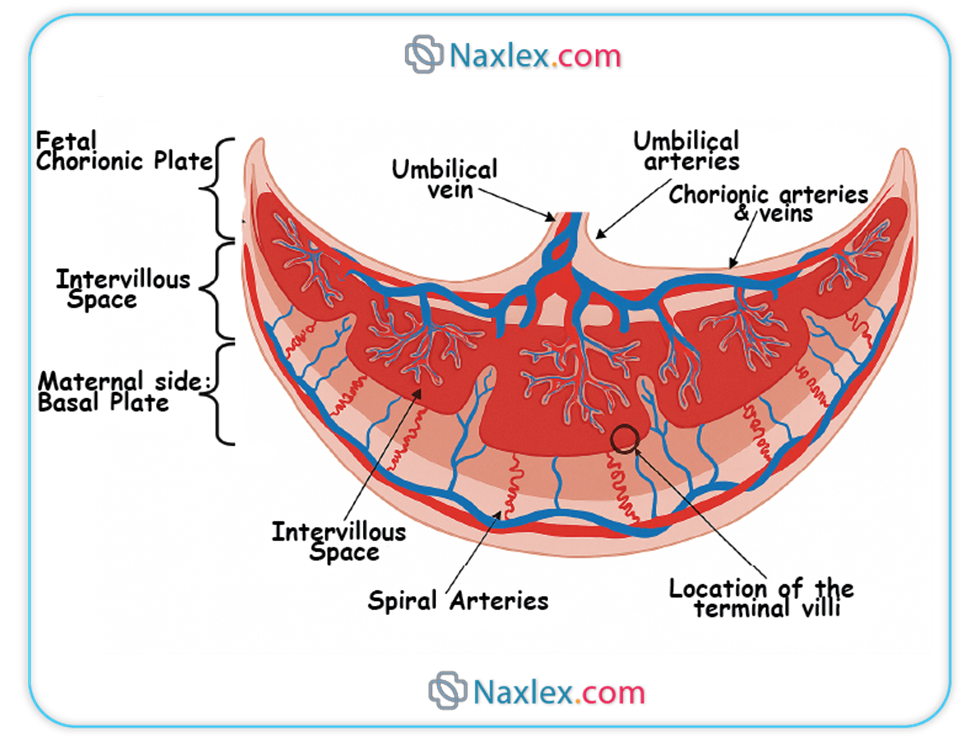
- Microscopic Structure (Placental Barrier):
- The functional unit of the placenta is the chorionic villus. These villi project into the intervillous space, which is filled with maternal blood.
- The "placental barrier" or "placental membrane" is a misnomer, as it is not an impermeable barrier. It represents the layers of tissue that separate maternal and fetal blood.
- In early pregnancy, this barrier is thicker, consisting of:
- Syncytiotrophoblast
- Cytotrophoblast
- Connective tissue of the villus (stroma)
- Endothelium of the fetal capillary
- As pregnancy progresses, the cytotrophoblast layer thins and largely disappears, and the syncytiotrophoblast thins significantly, bringing the fetal capillaries closer to the maternal blood in the intervillous space. This thinning facilitates more efficient exchange.
2. Functions of the Placenta
The placenta is a multifunctional organ critical for sustaining pregnancy.
2.1. Endocrine Functions
The syncytiotrophoblast is a major endocrine organ, producing numerous hormones essential for maintaining pregnancy:
- Human Chorionic Gonadotropin (hCG):
- Secreted shortly after implantation.
- Maintains the corpus luteum in the ovary during early pregnancy, ensuring continued production of progesterone and estrogen until the placenta is mature enough to take over.
- Is the hormone detected in pregnancy tests.
- Progesterone:
- Produced in increasing amounts by the placenta from approximately 7-8 weeks gestation, eventually becoming the primary source.
- Functions:
- Maintains the decidua.
- Relaxes uterine smooth muscle, preventing contractions and preterm labor.
- Suppresses maternal immune response to prevent rejection of the fetus.
- Inhibits synthesis of prostaglandins.
- Prepares mammary glands for lactation.
- Estrogens (primarily Estriol):
- Produced by the placenta using androgen precursors from the fetal adrenal glands and maternal cholesterol. This unique fetoplacental unit interaction is essential for estrogen synthesis.
- Functions:
- Stimulates uterine growth and uteroplacental blood flow.
- Contributes to the development of maternal mammary glands.
- Increases uterine contractility towards term.
- Human Placental Lactogen (hPL) / Human Chorionic Somatomammotropin (hCS):
- Produced by the syncytiotrophoblast.
- Functions:
- Modifies maternal metabolism to provide more nutrients for fetal growth (e.g., increases maternal insulin resistance, promotes lipolysis).
- Stimulates mammary gland development for lactation.
- Relaxin:
- Produced by the decidua and placenta.
- Relaxes pelvic ligaments and softens the cervix, preparing for labor.
2.2. Metabolic Functions
The placenta also performs various metabolic activities:
- Glycogen Synthesis: Stores glycogen, providing a readily available energy source for the fetus.
- Fatty Acid Synthesis: Synthesizes fatty acids, which are important for fetal growth and development.
- Protein Synthesis: Can synthesize some proteins.
- Nutrient Storage: Stores iron, glycogen, and fat-soluble vitamins.
2.3. Transfer Functions
The placenta facilitates the transfer of substances between the mother and fetus through various mechanisms:
2.3.1. Gas Exchange
- Oxygen and carbon dioxide are transferred across the placental membrane primarily by simple diffusion.
- Fetal hemoglobin has a higher affinity for oxygen than adult hemoglobin, facilitating oxygen uptake.
2.3.2. Nutrient Transfer
- Glucose: Transferred by facilitated diffusion via glucose transporters (GLUTs). It is the primary energy source for the fetus.
- Amino Acids: Transferred by active transport, leading to higher concentrations in fetal blood than maternal blood. Essential for fetal protein synthesis.
- Fatty Acids: Primarily transferred by simple diffusion, especially free fatty acids.
- Vitamins and Minerals: Transferred by various mechanisms, including active transport (e.g., iron, calcium, folate) and facilitated diffusion.
2.3.3. Waste Product Excretion
- Urea, Creatinine, Uric Acid: Transferred from fetal to maternal blood by simple diffusion for excretion by the maternal kidneys.
2.3.4. Antibody Transfer
- Immunoglobulin G (IgG): Actively transported across the placenta, primarily in the third trimester.
- Provides passive immunity to the fetus against various maternal infections (e.g., measles, rubella, tetanus, diphtheria), offering protection during the first few months of life. Other immunoglobulins (IgA, IgM) do not cross the placenta significantly.
2.3.5. Drug Transfer
- Most drugs with a molecular weight less than 1000 Da can cross the placenta.
- Transfer depends on factors like lipid solubility, molecular size, protein binding, and concentration gradient.
- This is a critical concern as many medications and illicit substances can have teratogenic or adverse effects on the fetus.
Nursing Insights: The placenta's role as a major endocrine organ explains the hormonal changes observed in pregnancy. Its transfer functions underscore the importance of maternal nutrition and avoidance of harmful substances. The transfer of maternal antibodies highlights the natural protection afforded to newborns, influencing vaccination schedules and disease susceptibility.
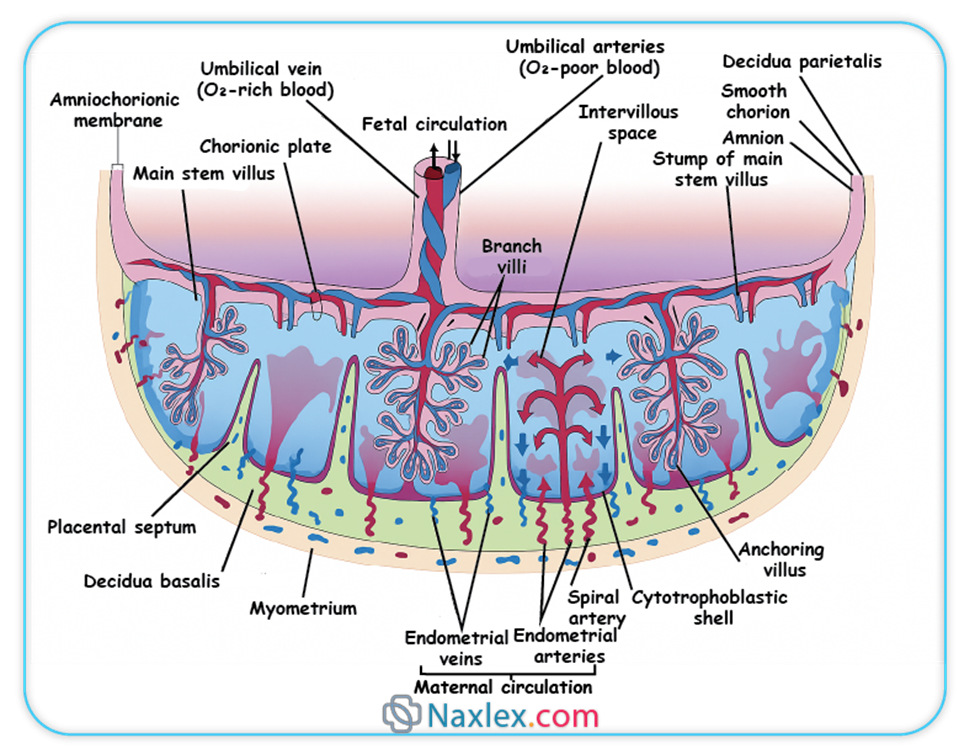
3. Placental Circulation
The placenta serves as the interface for two separate circulatory systems: maternal and fetal.
- Maternal Placental Circulation:
- Maternal blood enters the intervillous space from the uterine arteries, which are branches of the internal iliac arteries.
- These spiral arteries pierce the decidua basalis and open directly into the intervillous space.
- Maternal blood then bathes the chorionic villi, facilitating exchange.
- Deoxygenated and waste-laden blood drains from the intervillous space through the endometrial veins back into the maternal systemic circulation.
- Crucially, there is no direct mixing of maternal and fetal blood under normal physiological conditions.
- Fetal Placental Circulation:
- Deoxygenated blood and waste products are carried from the fetus to the placenta via two umbilical arteries (branches of the fetal internal iliac arteries).
- These arteries enter the placenta, branch extensively, and supply the capillary networks within the chorionic villi.
- Within the villi, exchange of gases, nutrients, and waste products occurs between fetal capillary blood and maternal blood in the intervillous space.
- Oxygenated and nutrient-rich blood is returned to the fetus via a single umbilical vein.
- The umbilical cord typically contains two umbilical arteries and one umbilical vein, embedded in Wharton's jelly (a gelatinous connective tissue that protects the vessels).
Nursing Insights: Understanding placental circulation is fundamental to interpreting fetal monitoring (e.g., non-stress tests, biophysical profiles) and recognizing signs of placental insufficiency, which can lead to fetal hypoxia and growth restriction. The presence of two arteries and one vein in the umbilical cord is a normal finding, and deviations (e.g., single umbilical artery) warrant further investigation for potential fetal anomalies.
4. Variations and Abnormalities of the Placenta
Variations in placental structure and position can affect pregnancy outcomes:
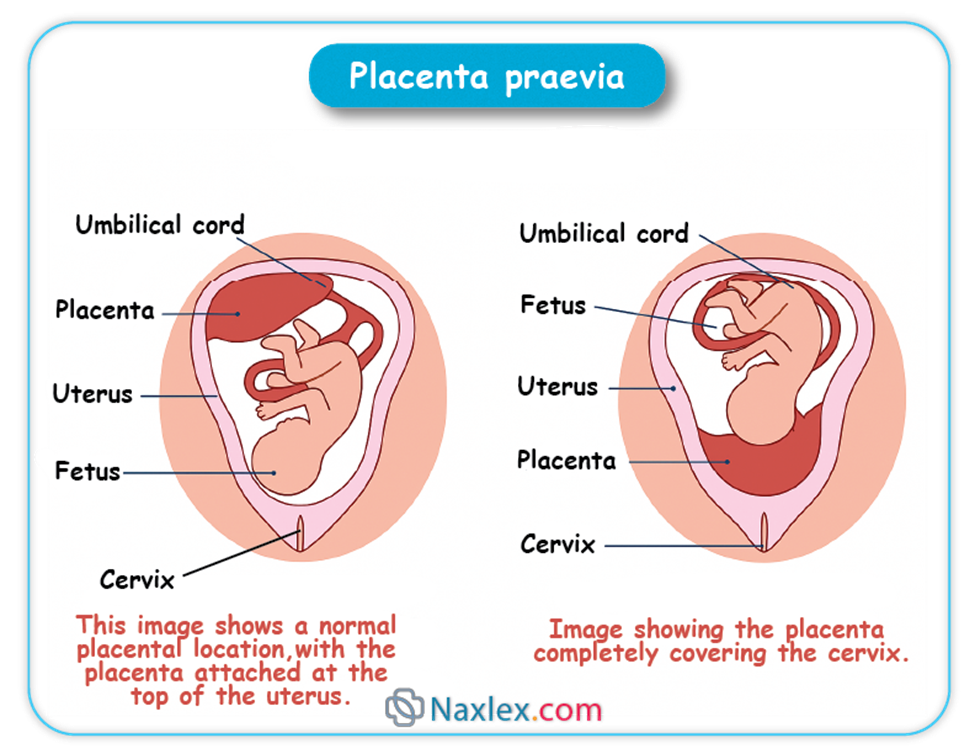
- Placenta Previa:
- Definition: Implantation of the placenta over or near the internal os of the cervix.
- Types: Complete/Total (covers the entire os), Partial (partially covers), Marginal (edge reaches the os), Low-lying (near but not covering).
- Clinical Significance: Painless vaginal bleeding in the second or third trimester, increased risk of hemorrhage, preterm birth, need for Cesarean section.
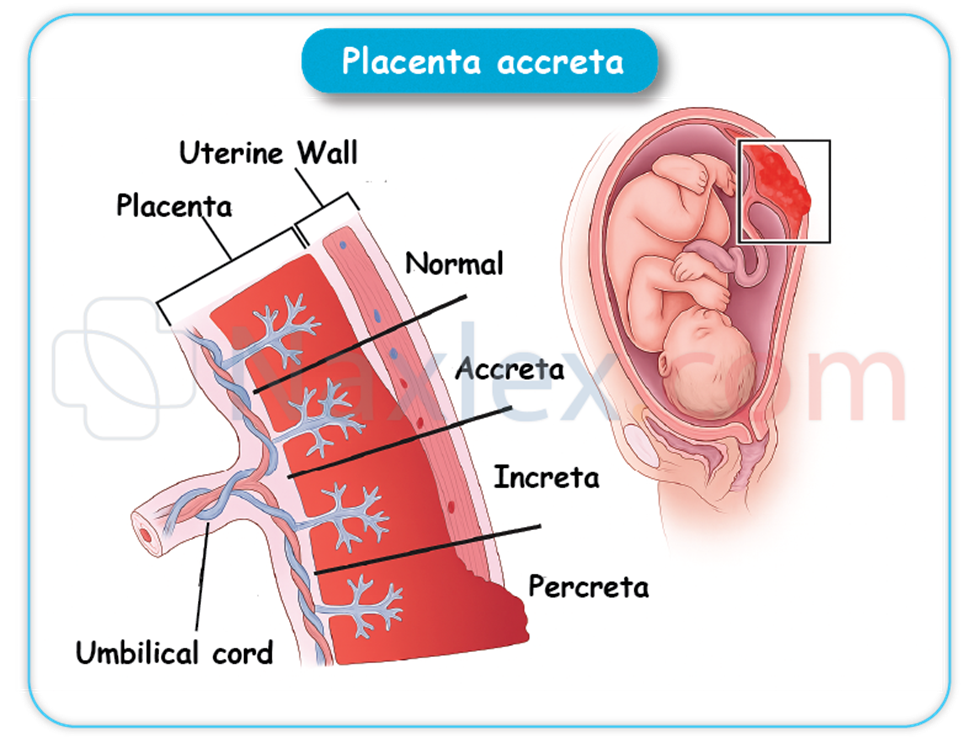
- Placenta Accreta/Increta/Percreta:
- Definition: Abnormal adherence of the placenta to the uterine wall due to defective decidua basalis.
- Accreta: Villi attach to the myometrium.
- Increta: Villi invade the myometrium.
- Percreta: Villi penetrate through the myometrium and possibly into adjacent organs (e.g., bladder).
- Clinical Significance: Severe postpartum hemorrhage, often requiring hysterectomy. Risk factors include previous Cesarean sections, placenta previa, and uterine surgery.
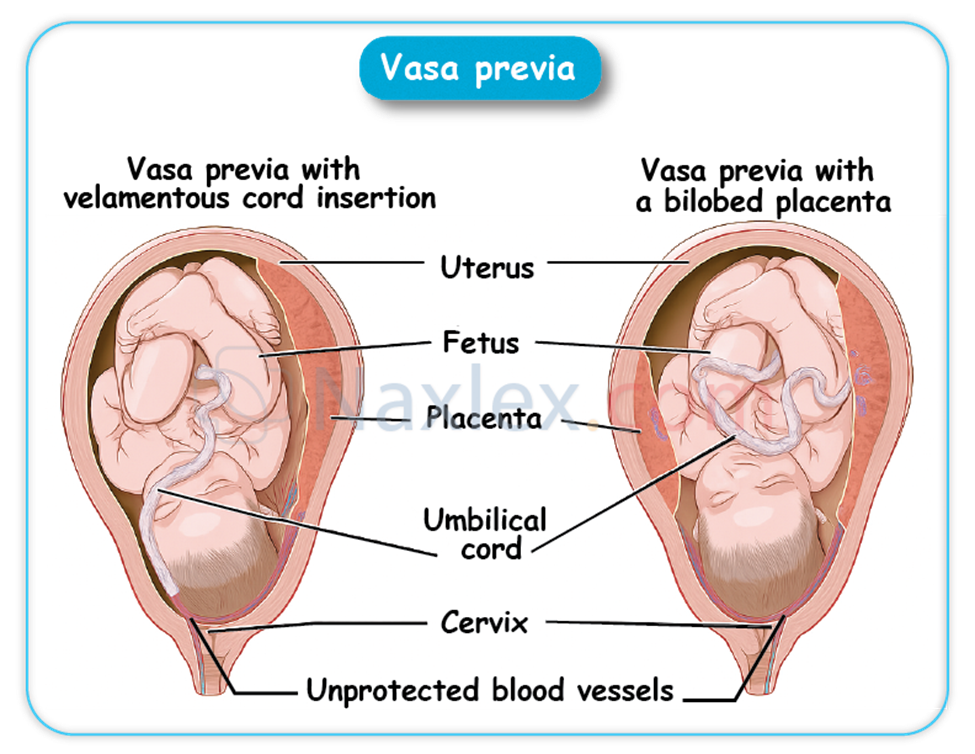
- Vasa Previa:
- Definition: Fetal blood vessels (umbilical vessels) traverse the membranes unprotected by placental tissue or umbilical cord, lying in front of the presenting part.
- Clinical Significance: High risk of fetal exsanguination (hemorrhage) if membranes rupture and vessels are compressed or torn, particularly during labor.
- Battledore Placenta (Marginal Cord Insertion):
- The umbilical cord inserts at the margin or periphery of the placenta rather than centrally. Usually of no clinical significance unless the insertion site is compromised.
- Velamentous Cord Insertion:
- Umbilical vessels separate in the membranes some distance from the placental margin and then travel within the membranes to insert into the placenta.
- Increases risk of vasa previa and vessel compression/rupture.
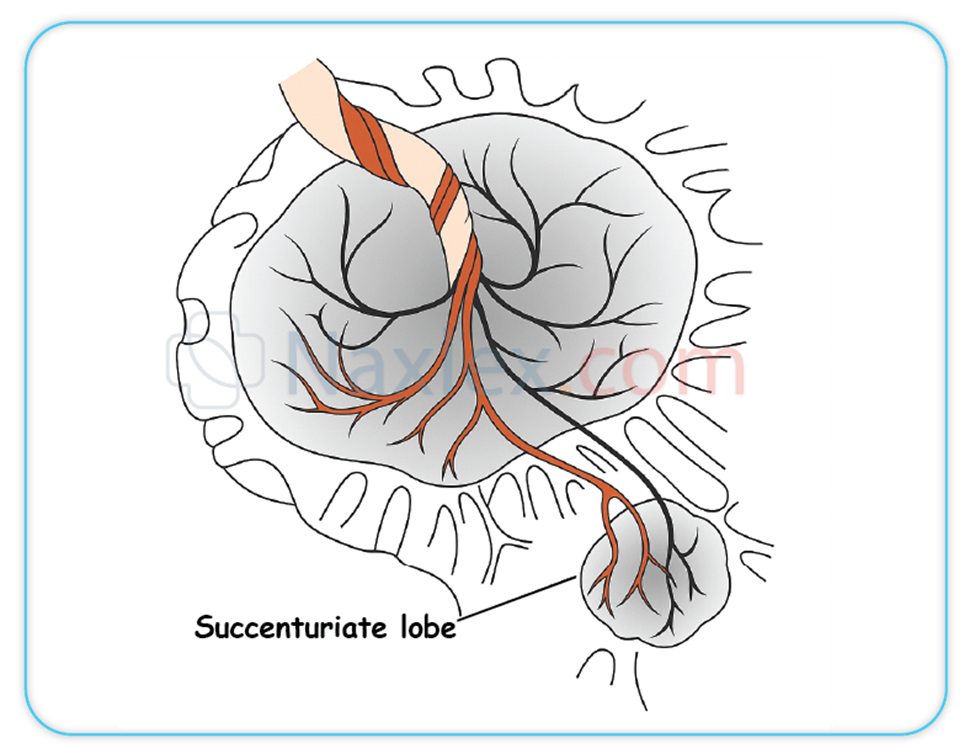
- Succenturiate Lobe:
- One or more accessory lobes of placental tissue are connected to the main placenta by blood vessels.
- Risk of a retained succenturiate lobe after delivery, leading to postpartum hemorrhage or infection.
- Circumvallate Placenta:
- A double fold of amnion and chorion forms a ring around the periphery of the placenta on the fetal surface, with vessels extending beyond this ring.
- Associated with preterm birth, hemorrhage, and placental abruption.
Nursing Insights: Nurses must be vigilant for signs and symptoms of placental abnormalities, especially bleeding. Understanding these conditions informs patient education, prepares for potential emergencies (e.g., massive transfusion protocols for accreta), and ensures appropriate monitoring and interventions to optimize maternal and fetal outcomes.
Summary
The initiation and progression of human pregnancy are founded upon a series of remarkably coordinated biological events, beginning with the precise union of gametes. Fertilization, typically occurring in the fallopian tube, involves the intricate journey of sperm, their capacitation, and the subsequent penetration of the ovum, culminating in the formation of a diploid zygote. Following fertilization, the zygote undergoes rapid cleavage divisions to form a morula, which then transforms into a blastocyst with distinct inner cell mass and trophoblast components. This blastocyst subsequently undergoes implantation into the prepared decidua of the maternal endometrium, establishing the critical connection for pregnancy.
Concurrently with early embryonic development, the fetal environment begins to take shape. The amnion, the innermost membrane, forms the amniotic cavity, which fills with amniotic fluid. This fluid, primarily composed of fetal urine in later stages, serves numerous vital functions: providing mechanical protection, maintaining thermal stability, facilitating musculoskeletal and organ development (especially lungs and GI tract), and preventing adhesions. Abnormalities in amniotic fluid volume, such as polyhydramnios (excess) or oligohydramnios (deficient), indicate potential fetal or maternal complications. The chorion, the outermost fetal membrane, plays a crucial role in forming the fetal component of the placenta.
The placenta is a temporary yet indispensable organ, serving as the interface for maternal-fetal exchange. Structurally, it comprises both maternal (decidua basalis) and fetal (chorion frondosum) components. Functionally, the placenta acts as a multifaceted organ: performing crucial endocrine functions by producing hormones like hCG, progesterone, estrogens, and hPL to maintain pregnancy; facilitating essential metabolic functions for fetal growth; and mediating vital transfer functions of gases, nutrients, waste products, and maternal antibodies between the two circulations. The unique placental circulation ensures efficient exchange without direct mixing of maternal and fetal blood. Variations and abnormalities of the placenta, such as placenta previa or accreta, carry significant risks and necessitate diligent nursing assessment and intervention. A comprehensive understanding of these interconnected processes is paramount for nurses to provide high-quality, evidence-based care throughout the maternal-newborn continuum.
