
Tuberculosis
Study Questions
Practice Exercise 1
A nurse is obtaining a health history from a client suspected of having early tuberculosis. Which manifestations should the nurse ask the client about?
Explanation
Tuberculosis often presents with insidious, non-specific symptoms that can be easily overlooked or attributed to other minor illnesses. The causative agent, Mycobacterium tuberculosis, triggers a chronic systemic inflammatory response as the immune system attempts to sequester the bacteria within granulomas. Recognizing these subtle constitutional symptoms is critical for early diagnosis and preventing the further transmission of the infection within the community.
Rationale for correct answer
2. The nurse should specifically ask about fatigue, low-grade fever, and night sweats, as these are the classic hallmarks of early tuberculosis. The fever typically follows a diurnal pattern, often peaking in the late afternoon or evening, while the night sweats are frequently profound enough to require a change of bed linens. These symptoms reflect the body’s ongoing metabolic and immune struggle against the primary infection.
Rationale for incorrect answers
1. Manifestations such as chest pain, hemoptysis, and weight loss generally indicate more advanced or extensive pulmonary involvement. While these findings are associated with tuberculosis, they are rarely the very first signs reported by the client. Hemoptysis (coughing up blood) occurs when the infection causes cavitary lesions that erode into the bronchial arteries, signifying significant tissue destruction.
3. A cough with purulent mucus and high fever with chills are more characteristic of acute bacterial pneumonia rather than the chronic, slow-burning nature of TB. Tuberculosis typically begins with a dry, persistent cough that only becomes productive as the disease progresses. Chills and high-intensity fevers suggest a more rapid and acute infectious process than is usually seen in the early stages of a mycobacterial infection.
4. While temperature elevation at night is correct, the presence of pleuritic pain and a strictly nonproductive cough is not the most common early presentation. Pleuritic pain suggests that the infection has reached the pleural surface, causing inflammation (pleurisy). In early TB, the cough is often the most prominent respiratory symptom, and it gradually transitions from nonproductive to productive over several weeks.
Test-taking strategy
- Distinguish between constitutional symptoms (system-wide) and localized respiratory symptoms (chest pain, hemoptysis).
- Identify the typical timeline of tuberculosis, recognizing it as a chronic, slowly progressing disease rather than an acute one.
- Look for the cluster of symptoms that includes the classic triad: low-grade afternoon fever, night sweats, and unexplained fatigue.
- Recall that early manifestations are often subtle, whereas dramatic symptoms like coughing up blood signal advanced stages of the pathology.
Take home points
- A persistent cough lasting three weeks or longer should always be screened for tuberculosis.
- Weight loss in TB is often unintentional and occurs due to the high metabolic demand of the chronic infection.
- Night sweats in TB are typically drenching and occur during the early morning hours as the fever breaks.
- Early detection allows for the prompt initiation of Airborne Precautions to protect healthcare workers and other patients.
A nurse is reviewing the epidemiology of tuberculosis with a client. To what factor is the resurgence of TB, especially the emergence of multidrug-resistant (MDR) strains, most closely related?
Explanation
Tuberculosis management and epidemiological control depend heavily on the strict adherence to prolonged pharmaceutical regimens to eradicate the slow-growing bacteria. The rise of multidrug-resistant (MDR) strains is a direct consequence of intermittent or incomplete treatment, which allows the most resilient Mycobacterium tuberculosis organisms to survive and mutate. Addressing poor compliance is therefore the most critical factor in halting the global resurgence and evolution of resistant TB.
Rationale for correct answer
2. The emergence of MDR strains is most closely related to poor compliance with drug therapy. TB treatment typically lasts six to nine months; when patients stop taking medications prematurely or skip doses, the "weak" bacteria die while the stronger ones develop genetic resistance. These resistant strains are then transmitted to others, making standard treatments ineffective and leading to a significant public health crisis.
Rationale for incorrect answers
1. A lack of effective means to diagnose TB is not the primary driver of resurgence or resistance. Gold-standard diagnostics like sputum cultures, chest X-rays, and rapid molecular tests are widely available. The challenge lies not in the technology of diagnosis, but in the social and economic barriers that prevent patients from accessing care and completing the long-term therapeutic process.
3. The indiscriminate use of antitubercular drugs for other infections is extremely rare and not a significant factor. Unlike common antibiotics used for various ailments, medications like isoniazid and rifampin are highly specific and generally reserved for mycobacterial infections. Resistance develops within the treatment of TB itself due to non-adherence, rather than through the misuse of the drugs for unrelated conditions.
4. While the immunosuppressed population (including those with AIDS) has a much higher risk of contracting active TB, this does not inherently cause multidrug resistance. Immunosuppression increases the susceptibility and spread of the disease, but the actual biological development of MDR strains is a result of the selection pressure created by improper or inconsistent antibiotic dosing.
Test-taking strategy
- Identify the link between patient behavior (compliance) and the biological evolution of antibiotic resistance in chronic infections.
- Distinguish between factors that increase prevalence (like AIDS) and factors that cause resistance (like incomplete treatment).
- Recall that TB bacteria are exceptionally hardy and require a consistent, multi-drug approach over a long duration to be fully eliminated.
- Eliminate options that focus on diagnostic tools, as the resurgence of TB is primarily a socioeconomic and behavioral issue.
Take home points
- Directly Observed Therapy (DOT) is the most effective strategy to ensure compliance and prevent the development of MDR-TB.
- MDR-TB is defined as resistance to at least isoniazid and rifampin, the two most powerful first-line drugs.
- Non-compliance not only harms the individual but also creates a significant risk to the community through the spread of resistant bacteria.
- Patient education must emphasize that feeling better does not mean the infection is cured; the full course must be finished.
A nurse is assessing a client at risk for tuberculosis. Which of the following factors should the nurse recognize as increasing the likelihood of developing TB? Select all that apply
Explanation
Tuberculosis risk assessment involves identifying both environmental exposure and the host's physiological ability to contain the bacteria. While many people can be exposed to Mycobacterium tuberculosis, only those with specific risk factors typically progress from a latent state to active disease. Recognizing these constitutional symptoms and vulnerabilities is the first step in implementing infectious disease containment protocols.
Rationale for correct answer
1, 2, and 3. These three factors significantly increase TB risk. HIV infection is the strongest known risk factor because it depletes CD4+ T-cells, which are essential for forming the granulomas that keep TB dormant. Close contact with an active case provides the high-dose, prolonged exposure necessary for transmission via airborne droplets. Finally, recent travel to endemic regions increases the statistical probability of encountering resistant or highly virulent strains.
Rationale for incorrect answers
4. Maintaining a regular exercise and healthy diet actually serves as a protective factor rather than a risk factor. A robust immune system is more capable of sequestering the bacteria and preventing the progression to active disease. While physical health does not guarantee immunity to infection, it significantly improves the body's natural defenses and overall resilience against mycobacterial pathogens.
5. The BCG vaccine is used in many countries to prevent severe forms of TB in children. While it can cause a false-positive result on a TST (Tuberculin Skin Test), the vaccine itself does not increase the likelihood of developing the disease. In fact, its purpose is to provide a level of immunological protection, although its effectiveness in preventing adult pulmonary TB is variable and often limited.
Test-taking strategy
- Identify factors that weaken the immune system (immunosuppression) as primary risk markers for tuberculosis.
- Consider the mode of transmission (airborne) and prioritize settings where close, indoor contact is likely to occur.
- Distinguish between factors that cause a positive test result (BCG vaccine) and factors that actually cause the disease pathology.
- Use a systematic approach to "Select all that apply" questions by evaluating each option independently against the known risk criteria.
Take home points
- Homelessness and living in crowded environments (like prisons or shelters) are major social determinants of TB risk.
- Substance abuse and malnutrition significantly impair the immune response, making the individual more susceptible.
- Healthcare workers are at increased risk and must use N95 respirators when caring for suspected TB patients.
- Patients with diabetes or chronic kidney disease also have a higher risk of TB reactivation due to altered immunity.
A client asks the nurse how TB affects the lungs. The nurse explains that the disease primarily causes which pathological change?
Explanation
Early-stage tuberculosis involves a unique immune response where the body attempts to wall off the invading bacteria within the lung tissue. This process is driven by Mycobacterium tuberculosis, which triggers the migration of macrophages and T-cells to the site of infection. Understanding how the immune system creates granulomas to sequester the pathogen is essential for grasping the constitutional symptoms and the long-term structural changes that occur in the lungs.
Rationale for correct answer
1. The primary pathological change in TB is the formation of granulomas and caseating necrosis. When the immune system cannot immediately kill the bacteria, it forms a granuloma (Ghon complex) to contain them. The center of this mass undergoes a specific type of cell death called caseating necrosis, which has a soft, cheese-like appearance. If the immune system weakens, these areas can liquefy and rupture, allowing the infection to spread throughout the lungs.
Rationale for incorrect answers
2. Widespread alveolar collapse (atelectasis) is not the hallmark of tuberculosis. While localized collapse can occur if a large granuloma or lymph node obstructs a bronchus, it is not the defining pathological process of the disease. TB is characterized by chronic inflammation and tissue destruction rather than the acute loss of air pressure that typically causes generalized alveolar collapse.
3. Acute bronchospasm and airway edema are the primary features of asthma or acute allergic reactions, not tuberculosis. TB is a slow-growing bacterial infection that affects the lung parenchyma (the functional tissue). While a patient with TB may have a cough, the underlying issue is not the sudden constriction of the airways seen in reactive airway diseases, but rather the development of lesions within the tissue itself.
4. A pulmonary embolism is a vascular event caused by a blood clot traveling to the lungs, obstructing blood flow. It is a circulatory problem rather than an infectious one. While chronic illness can increase the risk of blood clots, a pulmonary embolism does not represent the pathological change caused by the mycobacteria. TB is an infectious process of the respiratory tissue, not a primary clotting disorder.
Test-taking strategy
- Associate the term "caseating" (cheese-like) exclusively with the necrosis found in tuberculosis infections.
- Recognize that TB is a granulomatous disease, a category shared with only a few other chronic conditions like sarcoidosis.
- Distinguish between parenchymal diseases (TB, pneumonia) and airway diseases (asthma, COPD) when selecting pathological changes.
- Remember that TB pathology is defined by the body's attempt to encapsulate the bacteria rather than an immediate systemic failure.
Take home points
- Granulomas can remain dormant for decades, a state known as latent tuberculosis infection.
- Calcification of these granulomas (Ghon complexes) is often visible on a chest X-ray as small, white spots.
- If the necrotic center of a granuloma liquefies, it creates a cavity where bacteria can multiply rapidly.
- The "cheese-like" appearance of caseous necrosis is a key diagnostic finding in pathology.
A nurse is educating a community group about tuberculosis. Which statements should the nurse include as true risk factors or causes of TB? Select all that apply
Explanation
Tuberculosis education focuses on understanding both the transmission mechanics and the host factors that facilitate infection. While the causative agent is strictly bacterial, the environmental and physiological state of the individual dictates whether an exposure results in active disease. Identifying these constitutional symptoms and risks allows the community to recognize that TB is a disease of social determinants as much as it is a biological one.
Rationale for correct answers
1. Tuberculosis is primarily transmitted via the airborne route, occurring when an individual with active pulmonary disease expels microscopic droplets through coughing, sneezing, or speaking. These droplets remain suspended in the air for extended periods, potentially being inhaled by others. Controlling the source of infection through respiratory etiquette is a key public health strategy.
3. People with weakened immune systems, particularly those with HIV/AIDS, are at significantly higher risk for progressing from latent to active tuberculosis. When the body's T-lymphocyte response is compromised, the immune system cannot effectively sequester the bacilli within granulomas. Other risk factors include the use of immunosuppressive medications and certain chronic illnesses like diabetes.
4. Proper nutrition is a vital component of the body's defense against infection; therefore, malnutrition severely weakens the cell-mediated immune response. In areas with high rates of food insecurity, individuals are more susceptible to becoming infected after exposure and are less likely to recover without significant nutritional support alongside pharmacological treatment.
Rationale for incorrect answers
2. Smoking and air pollution damage the ciliary clearance mechanisms and cause chronic inflammation of the respiratory tract. This damage makes the lungs more vulnerable to bacterial colonization and hinders the body's ability to expel infectious particles. Environmental toxins are well-documented contributors to increased TB susceptibility and poorer treatment outcomes.
5. The belief that TB cannot develop in vaccinated people is a dangerous misconception. The BCG vaccine provides partial protection, primarily against severe childhood forms of the disease like TB meningitis. It does not provide guaranteed, lifelong immunity against adult pulmonary tuberculosis. Many individuals who were vaccinated as children can still develop active disease if they are exposed to a high bacterial load or become immunosuppressed.
Test-taking strategy
- Apply the principle of airborne transmission to identify how the disease moves from person to person.
- Recognize that immunosuppression is the common denominator for almost all high-risk categories in infectious diseases.
- Be wary of "absolute" statements like "no effect" or "cannot develop," which are rarely true in clinical medicine.
- Connect socioeconomic factors (malnutrition, crowded living) to the biological success of the tuberculosis pathogen.
Take home points
- Airborne precautions require the use of a negative-pressure room and N95 respirators.
- TB is not spread by touching surfaces, sharing clothes, or sitting on a toilet seat.
- Improving ventilation in crowded areas is a key public health strategy for reducing transmission.
- Screening programs often target high-risk groups to catch cases before they become highly infectious.
Practice Exercise 2
A nurse is caring for a client diagnosed with tuberculosis. A sputum sample is requested for three consecutive days. At which of the following times should the nurse correctly schedule the collection of the sputum sample?
Explanation
Tuberculosis diagnosis relies heavily on the quality of the specimen collected for acid-fast bacilli (AFB) testing. Because the bacteria are slow-growing and can be scarce in the respiratory tract, a concentrated sample is necessary for accurate detection. Identifying the constitutional symptoms of the patient, combined with a properly timed sputum collection, ensures that the Mycobacterium tuberculosis can be identified and treated before the infection progresses further.
Rationale for correct answer
1. The nurse should schedule the collection immediately upon waking in the morning. During sleep, pulmonary secretions pool and concentrate in the lungs, making the first cough of the day the most likely to contain a high density of the bacteria. Collecting samples for three consecutive mornings increases the diagnostic yield and compensates for the fact that the bacteria are often released intermittently rather than in every single sputum expectoration.
Rationale for incorrect answers
2. Collecting a sample midmorning after breakfast is less ideal because food particles can contaminate the specimen and interfere with laboratory analysis. Additionally, physical activity and fluid intake throughout the morning may thin or dilute the secretions. For the most accurate microbiological results, the sample should be obtained before the patient eats, drinks, or performs oral hygiene that might introduce contaminants.
3. Sampling in the evening typically results in a less concentrated specimen. Throughout the day, regular breathing, talking, and occasional coughing prevent the significant accumulation of mucus seen overnight. An evening sample is more likely to consist of saliva or thin secretions rather than the deep, bronchial material required to confirm a diagnosis of active pulmonary tuberculosis.
4. Obtaining a sample at bedtime presents the same issues as an evening collection. The patient has been upright and active for many hours, which means the secretions are not as stagnant or concentrated as they are after a full night of rest. To ensure the highest sensitivity of the AFB smear and culture, the early morning hours remain the "gold standard" for clinical specimen collection.
Test-taking strategy
- Always prioritize the first-morning specimen for tests involving respiratory secretions or urinalysis when concentration is required.
- Distinguish between sputum (from the deep lungs) and saliva (from the mouth), noting that the former is required for TB testing.
- Recall that three consecutive days of collection is the standard protocol to overcome the "intermittent shedding" of mycobacteria.
- Look for the timing that minimizes contamination from food, drink, or oral care products.
Take home points
- Patients should be instructed to perform several deep breaths and a forceful "huff" cough to produce a deep-lung specimen.
- If a patient cannot produce sputum spontaneously, an induced sputum may be ordered using hypertonic saline via a nebulizer.
- Sputum samples must be sent to the laboratory immediately to ensure the viability of the organisms for culture.
- Negative results on three consecutive morning smears are often required before a patient can be released from airborne precautions.
A nurse is reviewing diagnostic tests with a client at risk for infectious diseases. What condition can a Mantoux test identify?
Explanation
Mycobacterium tuberculosis exposure is detected through a specialized immunological skin test that measures the body's delayed-type hypersensitivity reaction. This screening tool is essential for identifying asymptomatic individuals who carry the bacteria in a latent state. Recognizing the constitutional symptoms along with a positive test result allows clinicians to initiate prophylactic treatment.

Rationale for correct answer
4. The Mantoux test, also known as the Tuberculin Skin Test (TST), is specifically used to identify infection with Tuberculosis. It involves the intradermal injection of 0.1 mL of Purified Protein Derivative (PPD). If a person has been exposed, their T-cells will recognize the protein and cause a local inflammatory response, resulting in a firm, raised area called an induration within 48 to 72 hours.
Rationale for incorrect answers
1. Herpes is a viral infection (HSV-1 or HSV-2) that is typically diagnosed through physical examination of lesions, viral cultures, or Polymerase Chain Reaction (PCR) testing. The Mantoux test is designed solely to detect a bacterial immune response specific to mycobacteria and has no diagnostic value for identifying viral pathogens or the integumentary outbreaks associated with herpes.
2. Sarcoma is a type of malignant tumor that arises from connective tissues like bone, muscle, or fat. Diagnosis for such neoplasms requires imaging studies (MRI, CT) and a definitive tissue biopsy for histological analysis. A skin test measuring delayed-type hypersensitivity is not an appropriate or effective method for detecting oncological processes or cellular mutations.
3. Emphysema is a chronic obstructive pulmonary disease characterized by the destruction of the alveolar walls and permanent enlargement of the airspaces. It is a structural and obstructive disease rather than an infectious one. Diagnosis is primarily achieved through Pulmonary Function Tests (PFTs), specifically measuring forced expiratory volume and total lung capacity, rather than an immunological skin reaction.
Test-taking strategy
- Memorize the specific "eponym" tests for common diseases, linking Mantoux directly to Tuberculosis.
- Distinguish between screening tests (like the TST) and confirmatory tests (like a sputum culture or chest X-ray).
- Recognize that the Mantoux test measures an immune response to a bacterial protein, not a physical structural change in the lungs.
- Recall that a positive Mantoux test does not distinguish between latent and active disease; it only indicates that infection has occurred.
Take home points
- The test result is based on the diameter of the induration (hardness) in millimeters, not the presence of redness (erythema).
- A positive result is defined by different thresholds (5mm, 10mm, or 15mm) based on the patient's specific risk factors and immune status.
- If a TST is positive, the next clinical steps are a chest X-ray and a sputum assessment to rule out active disease.
- Patients who have received the BCG vaccine may show a false positive and may require an Interferon-Gamma Release Assay (IGRA) blood test instead.
A nurse is caring for a client with active TB. Which of the following are common signs and symptoms of the disease? Select all that apply
Explanation
Mycobacterium tuberculosis induces a localized pulmonary infection that triggers a systemic metabolic shift and granulomatous inflammation. Activated macrophages release tumor necrosis factor-alpha, causing the constitutional symptoms of nocturnal diaphoresis and cachexia. If cavitary lesions erode into bronchial arteries, life-threatening hemorrhage occurs, while untreated bacilli may disseminate hematogenously.
Rationale for correct answers
1. The phenomenon of nocturnal diaphoresis occurs as the body attempts to regulate core temperature during the diurnal fever cycle associated with tuberculosis. This symptom typically emerges in the late evening or early morning hours as the cytokine-induced thermoregulatory set point resets. It remains a hallmark of active disease and requires immediate diagnostic evaluation through sputum cultures.
2. Significant and unintentional reduction in body mass occurs due to the high metabolic demand of the chronic inflammatory response. The pathogen induces a state of hypermetabolism and anorexia through the sustained release of specific pro-inflammatory cytokines. Patients often present with cachexia which correlates with the severity and duration of the untreated bacterial infection.
3. This symptom indicates that the infection has progressed to the point of causing tissue necrosis and vascular erosion within the lung parenchyma. Rupture of a Rasmussen aneurysm or erosion into the bronchial circulation results in the expectoration of blood-streaked sputum. The presence of hemoptysis necessitates urgent intervention to maintain airway patency and prevent hemorrhagic shock in the patient.
5. Profound lethargy is a frequent complaint in those with mycobacterial infections due to the energy redirected toward the immune system. This systemic depletion occurs alongside chronic hypoxia and the nutritional deficiencies caused by the long-term metabolic strain of the infectious process. Addressing fatigue involves both treating the underlying pathogen and providing comprehensive nutritional support to the client.
Rationale for incorrect answers
4. Yellowing of the sclera or skin is not a direct clinical manifestation of a primary pulmonary tuberculosis infection. This finding typically indicates hepatic dysfunction or biliary obstruction rather than the typical parenchymal damage seen in lung disease. While hepatotoxicity can occur as a side effect of antitubercular medications, it is not an inherent sign of TB.
Test-taking strategy
- Categorize signs and symptoms into systemic/constitutional versus organ-specific manifestations to identify the broad impact of the infection.
- Differentiate between the natural history of the disease and the potential adverse effects of pharmacological interventions like isoniazid.
- Prioritize symptoms that reflect chronic inflammation and tissue destruction, such as drenching sweats and coughing up blood.
- Eliminate options that suggest extrapulmonary involvement not typical of the primary respiratory presentation unless systemic dissemination is specified.
Take home points
- The classic clinical triad for pulmonary tuberculosis includes night sweats, low-grade afternoon fevers, and unintentional weight loss.
- Hemoptysis signals advanced cavitary disease and requires monitoring for respiratory distress or significant blood loss.
- Constitutional symptoms like fatigue and anorexia are driven by cytokine release during the chronic immune response to the bacilli.
- Nurses must differentiate primary disease symptoms from medication-induced side effects like jaundice to ensure appropriate clinical management.
A client asks the nurse how TB is diagnosed. The nurse explains that which test provides a definitive diagnosis of active tuberculosis?
Explanation
Tuberculosis is diagnosed through a combination of clinical assessment, radiologic findings, and laboratory testing. Clients commonly present with chronic cough, fever, night sweats, and weight loss, prompting further evaluation. A chest X-ray may show infiltrates or cavitation, while definitive diagnosis requires sputum microscopy, culture, or nucleic acid amplification tests (NAATs) to detect Mycobacterium tuberculosis and confirm active infection.
Rationale for correct answer
1. A sputum culture is the only method that provides a definitive diagnosis by identifying the actual growth of Mycobacterium tuberculosis. While smears can show acid-fast bacilli, the culture confirms the species and allows for sensitivity testing. This ensures the medical team selects the most effective antibiotics to treat the specific bacterial strain.
Rationale for incorrect answers
2. A chest X-ray is a suggestive diagnostic tool that identifies pulmonary infiltrates, cavities, or granulomas characteristic of the disease. However, it cannot distinguish between active tuberculosis and other lung conditions like pneumonia or fungal infections. It is used to support the diagnosis but lacks the microbiological specificity to confirm the presence of the bacilli.
3. The tuberculin skin test only indicates that a person has been exposed to the bacteria and has developed a cell-mediated immune response. It cannot differentiate between latent infection and active disease, nor can it confirm if the person is currently infectious. Many people with a positive TST never develop the active pulmonary symptoms of tuberculosis.
4. A complete blood count (CBC) is a general diagnostic test used to monitor for signs of systemic infection or anemia. While an elevated white blood cell count might suggest an inflammatory process, it is not specific to tuberculosis in any way. It provides no information regarding the presence or location of mycobacterial pathogens within the body.
Test-taking strategy
- Distinguish between screening (TST), supportive (X-ray), and definitive (Culture) diagnostic procedures.
- Remember that "Definitive" in microbiology almost always refers to a culture that grows the specific offending organism.
- Rule out general laboratory tests like a CBC that do not provide site-specific or pathogen-specific information.
- Use the "Gold Standard" rule: for TB, the gold standard for confirmation is always the sputum culture.
Take home points
- Sputum cultures can take 2 to 6 weeks to provide results because TB is a slow-growing bacterium.
- Three consecutive morning sputum specimens are typically required to increase the diagnostic yield.
- Nucleic Acid Amplification Tests (NAAT) are faster than cultures but are often used alongside them for rapid screening.
- Once a culture is positive, it is used throughout treatment to monitor the patient's transition to a non-infectious state.
A nurse is assessing a client suspected of having tuberculosis. Which clinical manifestation should the nurse expect to observe?
Explanation
Mycobacterium tuberculosis induces a localized pulmonary infection that triggers a systemic metabolic shift and granulomatous inflammation. Activated macrophages release tumor necrosis factor-alpha, causing the constitutional symptoms of nocturnal diaphoresis and cachexia. If cavitary lesions erode into bronchial arteries, life-threatening hemorrhage occurs, while untreated bacilli may disseminate hematogenously.
Rationale for correct answer
1. A persistent cough is the most frequent symptom of pulmonary tuberculosis because the bacteria cause direct irritation and inflammation of the respiratory mucosa. As the infection progresses and tissue necrosis occurs, the cough typically transitions from nonproductive to producing purulent sputum. Clinical guidelines mandate that any productive cough lasting longer than 3 weeks must be investigated for mycobacterial infection to prevent transmission.
Rationale for incorrect answers
2. The rapid development of intense thoracic discomfort is more characteristic of acute conditions such as pulmonary embolism or spontaneous pneumothorax. Tuberculosis is a chronic, slow-burning disease that typically causes dull or pleuritic pain only after significant parenchymal involvement. The sudden onset described here contradicts the typical insidious progression of a mycobacterial infection which develops over several weeks.
3. Fever associated with tuberculosis is generally a chronic, low-grade occurrence that characteristically peaks in the late afternoon or evening hours. A febrile state that completely resolves within 24 hours suggests an acute viral or bacterial process rather than the persistent inflammatory state of TB. The diurnal fever pattern in tuberculosis is sustained over many days or weeks until effective antitubercular therapy is initiated.
4. Changes in bowel habits are not a standard clinical manifestation of primary pulmonary tuberculosis which targets the respiratory system. While extrapulmonary TB can affect the gastrointestinal tract, watery diarrhea is much more likely to indicate a primary enteric infection or a medication side effect. Focus remains on respiratory symptoms and systemic wasting when assessing a client for the most common form of this disease.
Test-taking strategy
- Apply the chronicity principle by selecting symptoms that reflect a long-term, slow-moving infectious process rather than acute changes.
- Link the specific duration of 3 weeks to standard public health screening protocols for identifying potential tuberculosis cases in clinical settings.
- Eliminate symptoms that are not system-specific to the respiratory tract, such as gastrointestinal distress, unless systemic dissemination is specifically mentioned.
- Recognize that insidious onset is a hallmark of TB, making sudden-onset symptoms statistically less likely to be the correct answer.
Take home points
- A productive cough for over 3 weeks is the primary clinical indicator used to trigger airborne precautions and diagnostic testing.
- Clinical manifestations of TB are often subtle initially and may be mistaken for a common cold or bronchitis.
- Systemic symptoms like weight loss and night sweats often accompany the respiratory symptoms in active disease.
- Sputum for acid-fast bacilli (AFB) remains the priority diagnostic intervention for any patient presenting with a chronic productive cough.
Practice Exercise 3
A nurse is caring for a client with active tuberculosis who continues to have positive sputum cultures after 6 months of treatment. What is the best action to help ensure the client adheres to the prescribed medication regimen?
Explanation
The clinical management of Mycobacterium tuberculosis requires a rigorous pharmacological approach to overcome the metabolic resilience of the bacilli. Failure to achieve sputum conversion within 6 months often indicates treatment non-adherence or the development of resistance. Implementing Directly Observed Therapy ensures that the prolonged drug regimen effectively eradicates the pathogen and prevents the further community transmission of potentially resistant bacterial strains.
Rationale for correct answer
4. The implementation of Directly Observed Therapy is the primary clinical strategy for managing patients who fail to adhere to their medication. By having a designated professional witness the patient swallow each dose, the healthcare team guarantees medication compliance and minimizes the risk of treatment failure. This method is the most reliable way to ensure that the prescribed regimen is followed exactly as required for bacterial eradication.
Rationale for incorrect answers
1. Mandating that a patient come to the clinic daily creates significant socioeconomic barriers that may actually decrease overall adherence. Travel costs and time constraints often interfere with the patient’s ability to maintain employment or fulfill family obligations during the long treatment course. Providing care within the patient's community or home environment is a much more sustainable approach for long-term infectious disease management.
2. Although peer support may improve a patient's psychological outlook, it does not provide the objective verification needed for medical safety. Success stories cannot replace the clinical oversight necessary to ensure that the patient is actually ingesting the potent antitubercular drugs. When sputum cultures remain positive after 6 months, the nurse must prioritize verifiable adherence over purely motivational or anecdotal interventions.
3. Conducting more teaching sessions is often an insufficient response to documented treatment failure because it ignores the practical obstacles to adherence. While education is vital, patients often understand the risks but struggle with the logistics or side effects of the medications. The focus must shift from theoretical knowledge to active surveillance of drug administration to stop the progression of the disease.
Test-taking strategy
- Select Directly Observed Therapy as the priority intervention whenever a patient with tuberculosis demonstrates a history of or potential for non-compliance.
- Distinguish between educational strategies and regulatory strategies, choosing the latter when objective evidence of treatment failure (positive cultures) is present.
- Look for the answer that provides the highest level of certainty regarding medication ingestion while maintaining a patient-centered focus.
- Rule out options that place excessive logistical burdens on the client, as these are known to decrease rather than increase long-term adherence.
Take home points
- Directly Observed Therapy is the global standard of care for preventing the emergence of multidrug-resistant tuberculosis.
- Continued positive sputum cultures after 6 months of therapy necessitate immediate drug susceptibility testing and adherence review.
- DOT can be performed by public health nurses, trained community health workers, or designated responsible individuals.
- Successful tuberculosis treatment requires a multidisciplinary approach to address the social and economic barriers to consistent medication use.
A nurse is reviewing pharmacologic therapy for a client with newly diagnosed tuberculosis. Which medications are included in the standard four-drug regimen used during the initial phase of treatment? Select all that apply
Explanation
The pharmacological eradication of Mycobacterium tuberculosis requires a multi-drug approach to target bacilli in different metabolic states and prevent selective resistance. Standard protocols utilize a combination of bactericidal and bacteriostatic agents to ensure complete sterilization of pulmonary lesions. This initial phase typically lasts 2 months and is designed to rapidly reduce the bacterial load and decrease the risk of infectious transmission.
Rationale for correct answers
1. This agent is a primary bactericidal drug that inhibits the synthesis of mycolic acids, which are essential components of the mycobacterial cell wall. It is highly effective against rapidly dividing organisms and remains a cornerstone of first-line therapy. Nurses must monitor for peripheral neuropathy and hepatotoxicity while ensuring the client receives supplemental pyridoxine to prevent neurological complications.
2. As a potent macrocyclic antibiotic, this medication inhibits bacterial RNA synthesis by binding to the beta subunit of DNA-dependent RNA polymerase. It possesses significant sterilizing activity against semi-dormant bacilli, which helps shorten the total duration of the prescribed treatment. Patients should be educated that this drug commonly causes a benign orange-red discoloration of body fluids.
3. This drug is a pyrazine analogue that exhibits potent bactericidal activity specifically within the acidic environment of intracellular macrophages. It is exceptionally effective during the first 2 months of therapy for killing persistent organisms that other drugs may miss. Its use is associated with potential hyperuricemia, which may precipitate acute gouty arthritis in susceptible individuals during the treatment course.
4. This bacteriostatic agent functions by inhibiting arabinosyl transferase, thereby disrupting the assembly of the mycobacterial cell wall polysaccharide layer. It is primarily included in the initial regimen to provide additional coverage in the event of isoniazid resistance. The most critical nursing priority is monitoring for optic neuritis, which manifests as decreased visual acuity.
Rationale for incorrect answers
5. This medication is a rifamycin derivative typically reserved for patients who cannot tolerate rifampin due to drug-drug interactions. It is frequently utilized in the management of tuberculosis among individuals with HIV/AIDS who are receiving specific protease inhibitors. While effective, it is not part of the standard four-drug RIPE regimen used for uncomplicated cases.
6. As a second-generation fluoroquinolone, this drug is classified as a second-line agent rather than a standard first-line medication. It is generally indicated for the treatment of multidrug-resistant tuberculosis or when a patient has documented intolerance to primary drugs. Indiscriminate use is avoided to prevent the development of resistance within the broader class of quinolone antibiotics.
Test-taking strategy
- Memorize the RIPE acronym (Rifampin, Isoniazid, Pyrazinamide, Ethambutol) to quickly identify the standard first-line antitubercular drug combination.
- Distinguish between first-line agents used for initial therapy and second-line agents reserved for resistant or complicated infectious cases.
- Recognize that combination therapy is mandatory in tuberculosis management to prevent the survival of mutated, resistant bacterial strains.
- Focus on the unique side effects of each drug, such as visual changes for Ethambutol and orange secretions for Rifampin.
Take home points
- The initial phase of TB treatment uses four drugs for 2 months to achieve rapid sputum conversion.
- Liver function tests must be monitored regularly as INH, Rifampin, and PZA are all potentially hepatotoxic.
- Ethambutol requires baseline and monthly visual acuity and color discrimination screening to detect optic nerve damage.
- Adherence to the full course of combination therapy is the only way to prevent the emergence of MDR-TB.
A nurse is reviewing medications for a client on long-term TB therapy with rifampicin and isoniazid. Which of the following are potential complications of the drugs? Select all that apply
Explanation
Pharmacological management of Mycobacterium tuberculosis utilizes potent antimicrobial agents that require extensive hepatic metabolism and systemic distribution. The prolonged duration of the initial phase and continuation phase increases the cumulative risk of metabolic disruptions and drug-induced cellular damage. Monitoring for adverse reactions is a critical nursing responsibility to ensure patient safety and prevent the permanent neurological complications associated with long-term antitubercular therapy.
Rationale for correct answers
1. Both isoniazid and rifampin are primary antitubercular agents that undergo significant biotransformation in the liver and can cause chemical hepatitis. Nurses must perform serial assessments for clinical signs such as jaundice, dark urine, or upper quadrant pain which indicate hepatotoxicity. Baseline and periodic elevations in liver transaminases (AST/ALT) serve as the primary laboratory markers for evaluating this common metabolic complication.
2. This complication is most frequently associated with the use of isoniazid due to the drug interfering with the normal metabolism of pyridoxine. Clients typically report symmetrical paresthesia, tingling, or burning sensations in the distal extremities as the peripheral neuropathy progresses. Administration of daily vitamin B6 supplements is the standard preventative intervention utilized to maintain the integrity of the nervous system.
Rationale for incorrect answers
3. Impairment of the sensory pathways in the eye is a well-documented adverse effect of ethambutol, but it is not typically associated with isoniazid or rifampin. Since the question specifies a regimen consisting only of INH and rifampin, the nurse would not expect visual disturbances as a primary complication. Regular ophthalmologic screening is mandatory only for clients on ethambutol to detect early signs of optic nerve damage.
4. A significant reduction in blood glucose levels is not a recognized or typical complication of the standard first-line antitubercular regimen. While some drugs may interact with oral antidiabetic agents, they do not inherently trigger hypoglycemia in the average patient. Metabolic monitoring in TB focuses primarily on hepatic function and uric acid levels rather than the pancreatic regulation of glucose.
5. Auditory and vestibular damage is caused by aminoglycosides like streptomycin and is not a side effect of isoniazid or rifampin. These injectable second-line medications damage the hair cells in the cochlea and the vestibular apparatus, leading to permanent ototoxicity. Because the client is only receiving INH and rifampin, they are not at risk for the eighth cranial nerve damage associated with aminoglycoside therapy.
Test-taking strategy
- Focus strictly on the specific medications listed in the stem (INH and rifampin) rather than the entire RIPE acronym.
- Apply the organ-based approach to recall complications: liver (hepatitis) for both and nerves (neuropathy) specifically for isoniazid.
- Distinguish between the unique toxicities of individual drugs, noting that ethambutol affects eyes and streptomycin affects ears.
- Recognize that hepatotoxicity is a shared risk for almost all first-line TB medications except for ethambutol.
Take home points
- Peripheral neuropathy from isoniazid is preventable with daily pyridoxine (Vitamin B6) supplementation.
- Patients must be taught to report any yellowing of the skin or eyes immediately due to the risk of drug-induced hepatitis.
- Rifampin is a potent enzyme inducer and can significantly decrease the effectiveness of oral contraceptives and warfarin.
- Alcohol consumption must be strictly avoided during TB therapy to minimize the risk of additive liver damage.
A nurse is teaching a client newly diagnosed with TB about preventing transmission. Which statement by the client indicates understanding?
Explanation
Prevention of tuberculosis (TB) focuses on breaking transmission and protecting vulnerable populations. Key strategies include BCG vaccination in high-risk groups, early screening and diagnosis, prompt initiation of effective treatment, and strict treatment adherence to prevent drug resistance. Improving ventilation, reducing overcrowding, and using respiratory masks in healthcare settings limit airborne spread. Ongoing contact tracing and public health education further reduce TB incidence and support strong infection control policies worldwide consistently.
Rationale for correct answer
1. This statement reflects a correct understanding of respiratory hygiene and source control. Using a tissue to contain droplets and wearing a surgical mask in public spaces physically prevents the aerosolization of bacilli. The client correctly identifies that these precautions must remain in place until the healthcare provider confirms they are no longer infectious, typically after three negative sputum smears.
Rationale for incorrect answers
2. Discontinuing medication prematurely is the leading cause of treatment failure and the development of drug-resistant strains. While symptoms like cough and fever often improve within the first few weeks, the mycobacteria are not yet eradicated. The client must be educated that "feeling better" does not mean they are cured or unable to transmit the disease to others.
3. Tuberculosis is not spread through fomites (inanimate objects) such as utensils, dishes, or linens. While general hygiene is important, the client’s focus on washing utensils as a primary TB prevention strategy is a misconception. Education should redirect the client's efforts toward ventilation and respiratory cover, which are the true methods of preventing airborne transmission.
4. The absence of a fever does not correlate with a lack of infectiousness. Many patients remain highly contagious even when they are afebrile, as long as they are still coughing up active bacilli. Staying home is a requirement based on the duration of therapy and sputum results, not on the presence or absence of a single systemic symptom like a fever.
Test-taking strategy
- Identify the mode of transmission (airborne) to rule out answers focusing on contact precautions like utensil washing.
- Look for "Safety and Public Health" answers that emphasize source control (tissues and masks) and professional clearance.
- Eliminate any options that suggest patient-led changes to the medication schedule, as adherence is a non-negotiable priority.
- Associate non-infectiousness with medical criteria (negative smears) rather than subjective feelings or isolated symptoms.
Take home points
- The most effective way to prevent transmission is for the patient to strictly adhere to their medication regimen.
- Households should be well-ventilated; opening windows helps dilute the concentration of airborne bacilli.
- Surgical masks are worn by the patient to contain droplets, while N95 masks are worn by healthcare workers to filter them.
- Close contacts should be identified and screened with a tuberculin skin test or IGRA blood test.
A nurse is providing discharge teaching to a client with active TB. Which instructions should the nurse include to ensure safe management and treatment adherence? Select all that apply
Explanation
Effective eradication of Mycobacterium tuberculosis depends on meticulous adherence to a long-term antimicrobial regimen to prevent the selection of resistant strains. Clients must understand that active tuberculosis requires a combination of bactericidal agents administered over 6 to 9 months to achieve biological sterilization. Proper discharge teaching focuses on medication compliance and the early identification of adverse effects to ensure both individual recovery and the protection of public health.
Rationale for correct answers
1. Consistency in drug administration is essential to maintain steady serum levels of antitubercular agents and effectively suppress bacterial replication. Patients must understand that stopping the prescribed course prematurely allows surviving bacilli to mutate into multidrug-resistant forms. Completing the full course is the only way to ensure the infection is entirely eradicated from the pulmonary tissue.
2. Routine monitoring through laboratory analysis is the only objective method to verify that the pharmacological therapy is successfully clearing the infection. Clients must attend follow-up appointments to provide specimens for acid-fast bacilli (AFB) smears and cultures. These tests provide the necessary diagnostic evidence to determine when the patient is no longer a transmission risk to the community.
3. First-line medications such as isoniazid and rifampin carry a significant risk of drug-induced hepatitis due to hepatic metabolism. Clients are instructed to monitor for liver toxicity markers, including dark-colored urine, clay-colored stools, and scleral icterus. Early reporting of jaundice allows the provider to adjust the regimen before irreversible hepatic damage or failure occurs.
5. Until a client provides 3 consecutive negative sputum smears, they remain potentially infectious and can transmit the pathogen via airborne droplets. Maintaining respiratory isolation and avoiding crowded indoor environments prevents the spread of the bacilli to susceptible individuals. Only a healthcare provider can officially lift these restrictions based on specific clinical and microbiological criteria.
Rationale for incorrect answers
4. Encouraging a patient to skip doses is dangerous and directly contributes to the failure of therapy and the development of resistance. Clinical improvement often occurs long before the bacteria are fully eliminated, leading to a false sense of security. Adherence must be maintained regardless of symptomatic relief to prevent a relapse of the active infectious process.
Test-taking strategy
- Apply the Directly Observed Therapy (DOT) principles by prioritizing total adherence and consistent timing of all medication doses.
- Focus on safety and infection control by selecting options that emphasize monitoring for organ toxicity and preventing community transmission.
- Rule out any options that suggest self-adjustment of medications, as TB protocols are strictly standardized and monitored by public health authorities.
- Link the clinical markers of hepatotoxicity (jaundice, nausea) directly to the known side effect profiles of the primary TB drug regimen.
Take home points
- Medication adherence is the single most important factor in preventing the development of multidrug-resistant tuberculosis.
- Patients are typically considered non-infectious after 2 to 3 weeks of continuous therapy and 3 negative sputum smears.
- Alcohol must be completely avoided during treatment due to the high risk of additive hepatotoxicity from TB drugs.
- Household members should be screened for latent TB infection following the diagnosis of an active case in the home.
Comprehensive Questions
A nurse is providing teaching to a client prescribed the following medication regimen: isoniazid (Nydrazid) 250 mg PO daily, rifampin (Rifadin) 500 mg PO daily, pyrazinamide 750 mg PO daily, and ethambutol (Myambutol) 1 mg PO daily. Which client statements demonstrate understanding of the teaching? Select all that apply
Explanation
Effective eradication of Mycobacterium tuberculosis requires a synergistic multi-drug protocol to suppress diverse bacterial populations and prevent acquired resistance. Patients must strictly adhere to airborne precautions and meticulous hygiene during the early phase of treatment to interrupt the aerosolized transmission of bacilli. Public health safety relies on the patient's understanding of source control and the necessity of prolonged pharmacological compliance to achieve a definitive cure.
Rationale for correct answers
2. Frequent hand hygiene reduces the secondary transfer of respiratory secretions from the hands to surfaces. While Mycobacterium tuberculosis is primarily airborne, mechanical removal via hand washing lowers the risk of environmental contamination. This statement reflects comprehension of respiratory hygiene as a tool for protecting the community.
3. A surgical mask serves as essential source control by containing infectious droplets at their origin. Because the patient is in the initial phase, they can still exhale aerosolized bacilli during normal speech. Utilizing a protective barrier in public mitigates the risk of transmission to susceptible individuals.
Rationale for incorrect answers
1. Antitubercular agents are not interchangeable because each component of the RIPE regimen targets different metabolic states. Substituting drugs would compromise the synergistic effect required to prevent resistance. Success depends on the simultaneous and consistent administration of all four prescribed medications.
4. Sputum collection is mandatory for evaluating clinical efficacy and determining infectious status throughout treatment. The patient must provide sputum specimens at regular intervals until bacterial clearance is documented. Symptomatic improvement does not negate the need for laboratory verification of the pharmacological intervention.
5. Initiating therapy does not grant immediate permission to interact in crowded settings without restrictions. Patients must maintain isolation measures until achieving 3 consecutive negative smears as per CDC guidelines. Assuming total freedom ignores the reality that the patient may still be an infectious source.
Test-taking strategy
- Focus on infection control principles, prioritizing behaviors that physically limit the spread of droplets to the environment or other people.
- Distinguish between the patient's role in source control (surgical mask) and the nurse's role in protection (N95 respirator).
- Reject any statements that imply medication flexibility or the premature cessation of diagnostic monitoring like sputum collection.
- Recall the timeline for non-infectivity, which requires both time (usually 2 to 3 weeks) and objective microbiological evidence (negative smears).
Take home points
- Hand washing and covering the mouth when coughing are critical to prevent the spread of infectious respiratory droplets.
- Patients must wear a surgical mask when leaving their room or going into public until cleared by a healthcare provider.
- Adherence to the exact four-drug regimen is the only way to ensure cure and prevent the development of resistant TB.
- Monthly sputum samples are required until two consecutive cultures are negative to confirm the successful end of treatment.
A nurse is educating a client diagnosed with tuberculosis. Which statement should the nurse include in the teaching?
Explanation
The clinical management of Mycobacterium tuberculosis necessitates a prolonged antimicrobial course to effectively eradicate slow-growing bacilli and prevent bacterial recrudescence. Pharmacological success is measured by the transition of the sputum from a positive to a negative state, indicating a reduction in the infectious load. Continuous microbiological monitoring is the gold standard for validating the efficacy of the intensive and continuation phases of the therapeutic regimen.
Rationale for correct answer
2. Consistent evaluation of sputum specimens every 4 weeks is mandatory to track the patient's response to the antitubercular therapy. This frequency allows the healthcare team to objectively document the conversion from an infectious to a non-infectious state through bacteriological clearance. Obtaining 2 consecutive negative cultures at the end of treatment serves as the definitive marker for a successful cure.
Rationale for incorrect answers
1. The standard duration for treating active pulmonary tuberculosis is typically 6 to 9 months, rather than only 4 months. Treatment must be sustained long enough to ensure the elimination of dormant bacilli that could otherwise cause a disease relapse. Shortening the duration of the pharmacological course significantly increases the risk of treatment failure and the development of drug-resistant strains.
3. Most patients with tuberculosis are managed in the outpatient setting once they are clinically stable and have a safe environment for isolation. Hospitalization is generally reserved for individuals with severe respiratory distress, those requiring initial stabilization, or those with complex comorbidities. Effective treatment focuses on Directly Observed Therapy within the community to facilitate long-term adherence and social reintegration.
4. Patients are only required to wear a surgical mask when they are in public spaces or around others while still in the infectious stage. It is unnecessary for the client to wear a mask at all times, especially when alone in a well-ventilated room. Once the healthcare provider confirms non-infectious status via negative smears, the requirement for source control barriers is lifted.
Test-taking strategy
- Prioritize answers that emphasize objective diagnostic monitoring, such as regular sputum testing, to evaluate treatment progress and efficacy.
- Distinguish between the standard treatment duration (6 to 9 months) and shorter, inadequate timeframes that might be presented as distractors.
- Recognize the shift toward community-based care for TB, eliminating the misconception that long-term hospitalization is required for all active cases.
- Identify that respiratory precautions are situational and temporary, lasting only until the patient is no longer considered a public health risk.
Take home points
- Sputum specimens must be collected monthly until two consecutive cultures are negative to confirm treatment success.
- Standard TB treatment lasts a minimum of 6 months to ensure complete eradication of the Mycobacterium tuberculosis bacilli.
- Non-infectivity is usually achieved after 2 to 3 weeks of consistent medication and 3 negative sputum smears.
- Outpatient management using Directly Observed Therapy is the preferred method for ensuring patient adherence and community safety.
A nurse is caring for a client newly diagnosed with tuberculosis who has been started on a multi-medication regimen. Which instruction should the nurse provide regarding ethambutol (Myambutol)?
Explanation
Ethambutol acts by inhibiting arabinosyl transferase, thereby disrupting the assembly of the mycobacterial cell wall polysaccharide layer. This bacteriostatic agent can penetrate the blood-brain barrier and the optic nerve, leading to potential ophthalmic toxicity. Regular clinical screening for alterations in visual acuity and color discrimination is essential to detect early manifestations of medication-induced sensory impairment.
Rationale for correct answer
3. The most significant adverse effect of ethambutol is optic neuritis, which requires the patient to report any changes in their sight immediately. This condition typically manifests as blurred vision, decreased acuity, or a loss of red-green discrimination. Because this complication can become irreversible if the drug is continued, patients must undergo baseline and monthly ophthalmological evaluations.
Rationale for incorrect answers
1. Benign orange-red discoloration of urine, sweat, and tears is a classic side effect of rifampin, not ethambutol. This occurs because rifampin is a pigmented compound that is excreted through various body fluids. While harmless, it can be alarming to patients, and it must be distinguished from the signs of icterus or hematuria.
2. Monitoring for icterus, or the yellowing of the whites of your eyes, is a priority for patients taking isoniazid, rifampin, or pyrazinamide. These medications are associated with significant hepatotoxicity and potential drug-induced hepatitis. Ethambutol is the only first-line TB drug that is generally not considered to be hepatotoxic in standard doses.
4. Daily supplementation of vitamin B6, or pyridoxine, is specifically indicated for patients taking isoniazid to prevent peripheral neuropathy. Isoniazid competes with pyridoxine for binding sites, leading to nerve damage in the distal extremities. Ethambutol does not interfere with vitamin B6 metabolism and therefore does not require this specific preventative intervention.
Test-taking strategy
- Use the mnemonic E for Eyes to link ethambutol directly to its primary adverse effect of optic neuritis.
- Differentiate between the pigment changes caused by rifampin and the neurological changes caused by isoniazid and ethambutol.
- Recognize that while most TB drugs affect the liver, ethambutol is unique in its focus on ocular toxicity.
- Prioritize symptoms that indicate irreversible organ damage, such as changes in vision or hearing, as urgent nursing concerns.
Take home points
- Patients on ethambutol must have a baseline vision test for acuity and color perception before starting therapy.
- Optic neuritis is usually dose-related and often reversible if the medication is discontinued promptly.
- Red-green color blindness is a specific early sign of ethambutol-induced optic nerve inflammation.
- Unlike other first-line TB medications, ethambutol does not typically cause liver enzyme elevations.
A nurse is preparing to give a client with tuberculosis a newly prescribed dose of isoniazid (INH). Which statement by the nurse is appropriate when discussing this medication?
Explanation
Isoniazid serves as a cornerstone of antitubercular therapy by inhibiting the synthesis of mycolic acids, which are essential components of the mycobacterial cell wall. This bactericidal agent frequently interferes with the metabolic activation of pyridoxine, leading to a functional deficiency within the peripheral nervous system. Maintaining adequate levels of vitamin B6 is the primary clinical strategy to prevent the development of drug-induced neurological deficits during the treatment course.
Rationale for correct answer
3. Peripheral neuropathy is a frequent adverse effect of isoniazid caused by the depletion of intracellular vitamin B6. Patients often report a tingling sensation or paresthesia in their distal extremities as the first sign of nerve fiber dysfunction. Providing daily pyridoxine supplements is the standard nursing intervention to mitigate these neurological complications during the prolonged therapeutic regimen.
Rationale for incorrect answers
1. Yellow discoloration of the skin indicates icterus, a clinical sign of severe hepatotoxicity rather than a direct side effect of isoniazid. While the drug is hepatotoxic, the nurse should instruct the patient to report jaundice as a serious complication rather than an expected finding. This manifestation requires immediate medical evaluation and potential discontinuation of the pharmacological therapy to prevent liver failure.
2. Joint discomfort or arthralgia is specifically associated with the use of pyrazinamide, which can cause hyperuricemia by inhibiting the renal excretion of uric acid. Isoniazid does not typically affect uric acid metabolism or precipitate acute gouty symptoms in the joints of the patient. Nurses must differentiate between the unique side effect profiles of each drug in the multi-drug regimen.
4. While systemic infections can cause anorexia, a decreased appetite is not a specific or hallmark side effect attributed to isoniazid administration. The most critical gastrointestinal monitoring for this drug involves detecting signs of hepatic distress rather than general nutritional intake changes. Gastrointestinal upset is more commonly linked to the broad-spectrum effects of rifampin or pyrazinamide during the initial phase.
Test-taking strategy
- Pair Isoniazid with its specific neurological side effect of peripheral neuropathy and its antidote, vitamin B6.
- Recognize that jaundice is a toxic complication of many TB drugs but is not considered a benign "side effect" to be expected.
- Distinguish between the metabolic side effects of pyrazinamide (gout) and the neurological side effects of isoniazid (paresthesia).
- Prioritize the assessment of the nervous system when evaluating a client who is starting or maintaining a regimen containing INH.
Take home points
- Peripheral neuropathy from isoniazid is caused by a deficiency in pyridoxine (Vitamin B6).
- Patients should be instructed to report any numbness or tingling in the hands and feet immediately.
- Alcohol must be avoided while taking INH due to the significantly increased risk of drug-induced hepatitis.
- Daily vitamin B6 supplementation is the gold standard for preventing isoniazid-related nerve damage.
A nurse is educating a group of individuals at a community center about tuberculosis. Which clinical manifestations should the nurse include in the teaching? Select all that apply
Explanation
Mycobacterium tuberculosis induces a localized pulmonary infection that triggers a systemic metabolic shift and granulomatous inflammation. Activated macrophages release tumor necrosis factor-alpha, causing the constitutional symptoms of nocturnal diaphoresis and cachexia. If cavitary lesions erode into bronchial arteries, life-threatening hemorrhage occurs, while untreated bacilli may disseminate hematogenously.
Rationale for correct answers
1. A persistent cough is the primary symptom of pulmonary tuberculosis due to the chronic irritation of the respiratory mucosa. This cough typically lasts for more than 3 weeks and reflects the ongoing infectious process within the lungs. It serves as the main mechanism for the aerosolization of bacilli into the immediate environment.
3. Profound lethargy occurs as the body's metabolic resources are diverted to the immune system to fight the chronic infection. This generalized exhaustion is a hallmark of the constitutional symptoms that accompany active disease states in the patient. Fatigue often correlates with the severity of the underlying inflammatory response and nutritional depletion.
4. Nocturnal diaphoresis results from the body's attempt to regulate temperature during the classic diurnal fever cycle of tuberculosis. These drenching sweats typically occur in the late evening or early morning as the cytokine-induced set point resets. It is a highly specific clinical marker used to differentiate TB from other respiratory infections.
5. The expectoration of thick, discolored mucus indicates that the infection has progressed to cause tissue necrosis. As the bacteria destroy lung parenchyma, the body produces purulent sputum consisting of cellular debris, leukocytes, and active mycobacteria. This manifestation is often accompanied by hemoptysis if vascular erosion occurs within the pulmonary cavities.
Rationale for incorrect answers
2. An unexplained increase in mass is inconsistent with the high metabolic demand and anorexia associated with active tuberculosis. Most patients experience significant and unintentional weight loss as the body enters a catabolic state driven by chronic inflammation. Weight gain would only be expected once effective therapy has been established and the infection is controlled.
Test-taking strategy
- Group the symptoms into respiratory and constitutional categories to ensure all systemic effects of the infection are captured.
- Use the catabolic nature of chronic infections to rule out options like weight gain that imply a positive energy balance.
- Link the chronicity of TB to the specific duration of symptoms, such as a cough lasting specifically over three weeks.
- Prioritize symptoms that reflect granulomatous destruction of the lungs, such as the production of purulent or bloody sputum.
Take home points
- The classic triad for screening active TB consists of a chronic cough, night sweats, and unintentional weight loss.
- Productive coughs lasting longer than three weeks require immediate evaluation with chest radiography and sputum cultures.
- Constitutional symptoms like fatigue and low-grade fevers are often the first subtle signs of a burgeoning mycobacterial infection.
- Purulent or blood-tinged sputum indicates advanced parenchymal damage and a high risk of transmission to the community.
A hospitalized client is receiving treatment for tuberculosis (TB). When reviewing the client’s medication administration record (MAR), which medication should the nurse recognize as being used to treat TB?
Explanation
The pharmacological eradication of Mycobacterium tuberculosis requires a multi-drug approach to target bacilli in different metabolic states and prevent selective resistance. Standard protocols utilize a combination of bactericidal and bacteriostatic agents to ensure complete sterilization of pulmonary lesions. This initial phase typically lasts 2 months and is designed to rapidly reduce the bacterial load and decrease the risk of infectious transmission.
Rationale for correct answer
1. This agent is a primary bactericidal drug that inhibits the synthesis of mycolic acids, which are essential components of the mycobacterial cell wall. It is highly effective against rapidly dividing organisms and remains a cornerstone of first-line therapy. Nurses must monitor for peripheral neuropathy and hepatotoxicity while ensuring the client receives supplemental pyridoxine to prevent neurological complications.
Rationale for incorrect answers
2. This medication is a triazole derivative used for the treatment of systemic and superficial fungal infections. It functions by inhibiting the synthesis of ergosterol, a vital component of the fungal cell membrane, rather than affecting mycobacterial growth. Consequently, it has no therapeutic utility in the management of active or latent pulmonary tuberculosis cases.
3. This macrolide antibiotic is primarily utilized for typical and atypical bacterial respiratory infections, such as those caused by Streptococcus pneumoniae. While it inhibits protein synthesis by binding to the 50S ribosomal subunit, it is not part of the standard antitubercular regimen. It lacks the specific bactericidal activity required to penetrate and sterilize the granulomatous lesions characteristic of TB.
4. This antiviral agent is specifically designed to treat infections caused by members of the herpesvirus family. It functions as a nucleoside analogue to inhibit viral DNA polymerase, but it has no effect on prokaryotic cells like bacteria. It is clinically indicated for conditions such as herpes simplex or varicella-zoster rather than pulmonary infections caused by acid-fast bacilli.
Test-taking strategy
- Memorize the RIPE acronym (Rifampin, Isoniazid, Pyrazinamide, Ethambutol) to quickly identify the standard first-line antitubercular drug combination.
- Distinguish between antibacterial, antifungal, and antiviral classes to rule out medications that do not target mycobacteria.
- Recognize that Isoniazid is often the first drug listed in any primary treatment protocol for both active and latent disease.
- Focus on the suffix or drug class of distractors to identify them as inappropriate for treating a mycobacterial infection.
Take home points
- Isoniazid is a cornerstone of tuberculosis treatment and acts by disrupting mycobacterial cell wall synthesis.
- First-line TB therapy always requires multiple medications to prevent the development of multidrug-resistant strains.
- Fluconazole, Azithromycin, and Acyclovir are used for fungal, general bacterial, and viral infections respectively.
- Patients on Isoniazid require frequent monitoring of liver function tests and assessment for peripheral nerve damage.
A client with a positive tuberculin skin test is prescribed an initial treatment regimen of isoniazid (Laniazid®), rifampin (Rifadin®), and ethambutol (Myambutol®). The client shares that she may be pregnant and asks whether she should continue taking the medication. On what rationale should the nurse base a response?
Explanation
The management of Mycobacterium tuberculosis during gestation requires a careful balance between maternal health and fetal safety. Untreated active disease presents a substantial risk of congenital tuberculosis, low birth weight, and increased maternal-fetal mortality. Standard pharmacological protocols are modified to include agents with proven safety profiles while ensuring the bacterial load is effectively suppressed to protect the developing intrauterine environment.
Rationale for correct answer
4. Untreated tuberculosis carries a higher risk of adverse outcomes for the mother and fetus than the standard drug regimen. Failure to treat active infection can lead to hematogenous spread to the placenta, resulting in congenital infection. Modern antitubercular therapy using isoniazid and rifampin is considered safe and essential for preventing maternal-fetal complications.
Rationale for incorrect answers
1. While it is true that these medications cross the placental barrier, they have not been proven to be teratogenic in humans. Delaying treatment until after delivery would allow the infection to progress, significantly endangering the life of the mother and the fetus. The benefits of achieving microbiological control far outweigh the theoretical risks of fetal drug exposure.
2. A diagnosis of tuberculosis is never a medical indication for the termination of pregnancy as the disease is treatable. With appropriate pharmacological intervention and clinical monitoring, women can successfully carry a pregnancy to term while undergoing treatment for the infection. Suggesting termination is both medically inaccurate and an inappropriate violation of patient autonomy.
3. Although the risk of isoniazid-induced hepatitis may be slightly higher in the postpartum period, it is not a reason to postpone therapy. Pregnancy itself does not contraindicate the use of these life-saving medications provided that frequent liver function tests are performed. Delaying treatment based on potential side effects would ignore the immediate lethality of untreated active disease.
Test-taking strategy
- Prioritize the life-over-limb principle, recognizing that untreated active tuberculosis is a life-threatening condition for both mother and child.
- Identify that isoniazid and rifampin are the gold standard for TB in pregnancy and are not classified as teratogenic.
- Eliminate options that suggest delaying treatment for a communicable and progressive disease, as this violates public health and safety standards.
- Recognize that ethambutol is also considered safe in pregnancy, making the three-drug regimen appropriate for initial management.
Take home points
- Untreated tuberculosis in pregnancy is associated with a high risk of spontaneous abortion and preterm labor.
- Isoniazid, rifampin, and ethambutol form the core of safe antitubercular therapy for pregnant women.
- Pyridoxine (Vitamin B6) supplementation is mandatory for pregnant women taking isoniazid to prevent fetal and maternal neuropathy.
- Streptomycin is the only major antitubercular drug strictly contraindicated in pregnancy due to the risk of fetal ototoxicity.
A normally healthy client shows a 5-mm induration 72 hours after receiving a tuberculin skin test. What should the nurse conclude about the test results?
Explanation
A tuberculin skin test (TST) is a diagnostic tool used to detect Mycobacterium tuberculosis infection. A small amount of purified protein derivative (PPD) is injected intradermally into the forearm. The site is evaluated after 48–72 hours for induration, not redness. Results depend on induration size and individual risk factors, such as immunosuppression or recent TB exposure. False positives may occur after BCG vaccination, and false negatives in severe illness states.
Rationale for correct answer
1. For a normally healthy individual with no known risk factors, an induration must be 15 mm or greater to be considered positive. A 5-mm induration is categorized as negative for this specific population. This threshold ensures that the nurse does not initiate unnecessary pharmacological interventions or further diagnostic testing for clients who are at minimal risk for tuberculosis infection.
Rationale for incorrect answers
2. A 5-mm induration only indicates a positive result in high-risk groups, such as those with HIV infection or recent contact with an active TB case. Furthermore, a positive TST never confirms active tuberculosis; it only indicates exposure or latent infection. Definitive diagnosis of active disease requires a chest X-ray and microbiological sputum analysis to identify the presence of the bacilli.
3. This result is not inconclusive but is a definitive negative based on CDC diagnostic criteria for a healthy person. A chest X-ray is typically reserved for those who have a positive skin test or present with classic constitutional symptoms like night sweats or chronic cough. Performing an X-ray on a healthy person with a 5-mm reaction would be an unnecessary use of diagnostic resources.
4. The assessment window for a tuberculin skin test is strictly defined as 48 to 72 hours after the initial intradermal injection. Since the nurse performed the reading exactly 72 hours later, the result is considered highly accurate and valid. Reading the test after 72 hours could lead to an inaccurate measurement as the inflammatory response begins to dissipate.
Test-taking strategy
- Memorize the three-tier system for TST: 5 mm (high risk/HIV), 10 mm (moderate risk/healthcare workers), and 15 mm (low risk/healthy).
- Distinguish between induration (hard, palpable area) and erythema (redness), as only the induration is measured for the result.
- Recognize that a positive skin test alone never diagnoses active disease, only exposure or latent tuberculosis infection (LTBI).
- Use the timing of the reading (48-72 hours) as a key indicator of the validity of the diagnostic procedure.
Take home points
- A 15-mm induration is the standard cutoff for a positive TST in a person with no known risk factors for TB.
- Immunosuppressed patients, such as those with HIV, are considered positive at only 5 mm of induration.
- TB skin tests must be read between 48 and 72 hours; if the patient returns after 72 hours, the test must be repeated.
- A positive TST requires a follow-up chest X-ray to rule out active pulmonary tuberculosis before starting latent TB treatment.
A nurse is planning care for a client admitted with newly diagnosed active tuberculosis (TB) secondary to AIDS. Which intervention should the nurse prioritize?
Explanation
The clinical management of active tuberculosis in the presence of AIDS requires an immediate focus on preventing the transmission of aerosolized pathogens. Because Mycobacterium tuberculosis is spread via minute droplets that remain suspended in the air, the priority is to protect the healthcare team and other vulnerable clients. Establishing a controlled environment is the first step in the nursing process before addressing the long-term immunological or secondary complications of the infection.
Rationale for correct answer
3. Prioritizing airborne precautions is essential to prevent the spread of the infection to healthcare workers and other immunocompromised patients. The nurse must place the client in a negative-pressure room and ensure all staff wear N95 or higher-level respirators during care. This intervention takes precedence because it addresses the immediate public health risk posed by the highly infectious nature of the disease.
Rationale for incorrect answers
1. While some TB medications or comorbid conditions could theoretically influence coagulation, monitoring for signs of bleeding is not the primary concern for a new TB diagnosis. The nurse should focus on respiratory and hepatic assessments rather than routine hemorrhage checks. Bleeding risk is a significantly lower priority compared to the containment of an airborne pathogen.
2. Although clients with AIDS are at risk for various opportunistic skin infections, providing skin care strategies is a supportive rather than an urgent intervention. In the acute phase of active tuberculosis, the respiratory status and infection control measures are the life-saving priorities. Skin integrity does not pose an immediate threat to the client or the clinical environment.
4. Assessing CD4 and T-lymphocyte counts is necessary for managing AIDS, but it does not address the immediate safety risks of active tuberculosis. While these values help determine the degree of immunisuppression, they are diagnostic markers rather than an active intervention. The nurse must first ensure infection control before analyzing the long-term progression of the underlying viral disease.
Test-taking strategy
- Apply Maslow’s Hierarchy and the principles of infection control, where safety and the prevention of transmission often take priority.
- Recognize the "Select the First" or "Priority" rule: look for the action that protects the greatest number of people or addresses the most immediate threat.
- Associate Active TB immediately with Airborne Precautions (Negative pressure, N95 mask, 6–12 air exchanges per hour).
- Distinguish between the long-term management of AIDS (CD4 counts) and the acute crisis of an active, communicable respiratory infection.
Take home points
- Airborne precautions must be initiated immediately upon suspicion or diagnosis of active pulmonary tuberculosis.
- The client must be placed in a private room with monitored negative airflow (AIIR - Airborne Infection Isolation Room).
- Healthcare workers must perform a "fit test" for their N95 respirator to ensure a proper seal against microscopic bacilli.
- Precautions can generally be discontinued only after three consecutive negative sputum smears are obtained.
A nurse is caring for a client diagnosed with class 3 tuberculosis one week ago who is admitted with chest pain and coughing. Which nursing action is the priority for this client?
Explanation
Prevention of tuberculosis (TB) focuses on breaking transmission and protecting vulnerable populations. Key strategies include BCG vaccination in high-risk groups, early screening and diagnosis, prompt initiation of effective treatment, and strict treatment adherence to prevent drug resistance. Improving ventilation, reducing overcrowding, and using respiratory masks in healthcare settings limit airborne spread. Ongoing contact tracing and public health education further reduce TB incidence and support strong infection control policies worldwide consistently.
Rationale for correct answer
2. Placing the client in an airborne infection isolation room (AIIR) is the highest priority to prevent the spread of the disease within the hospital. This specialized environment utilizes negative pressure to ensure that air does not flow from the patient's room into the hallways. This intervention takes precedence because it addresses the immediate public health risk and protects the safety of the entire clinical facility.
Rationale for incorrect answers
1. While antitubercular drugs are essential for the long-term cure of the disease, their administration is secondary to immediate infection control. One week of therapy is generally insufficient to render a patient non-infectious, meaning they still pose an active transmission risk upon admission. The nurse must first ensure that the bacilli are contained before entering the room to provide pharmacological interventions.
3. Preparing the room with suction equipment and extra linens are supportive nursing tasks but do not address the lethal risk of airborne transmission. While these items may be necessary for managing sputum production or patient comfort, they do not provide protection against the inhalation of infectious particles. These actions are considered part of routine care rather than a high-priority safety intervention.
4. Admitting the patient to an intensive care unit (ICU) is not strictly necessary unless the patient is experiencing severe respiratory failure or hemodynamic instability. Most TB patients can be safely managed in a standard medical unit provided that airborne precautions are strictly maintained. Unnecessarily transferring an infectious patient to an ICU increases the number of staff members potentially exposed to the pathogenic aerosols.
Test-taking strategy
- Apply the safety and infection control priority: when a patient is highly infectious, the first action must be to protect others from exposure.
- Recall that a patient is considered infectious until they have completed 2 to 3 weeks of therapy and have 3 negative sputum smears.
- Distinguish between source control (the isolation room) and treatment (medications), prioritizing the former in an acute hospital admission.
- Identify that the "highest priority" in TB management almost always involves the implementation of airborne precautions (Negative pressure, N95 respirator).
Take home points
- Airborne infection isolation rooms must have at least 6 to 12 air exchanges per hour to be effective.
- Healthcare workers must wear a fit-tested N95 respirator every time they enter the isolation room of a TB patient.
- The door to the isolation room must remain closed at all times to maintain the negative pressure gradient.
- If the patient must be transported to another department, they must wear a surgical mask to contain their respiratory secretions.
A client on long-term TB therapy reports numbness and tingling in the hands and feet. Which medication is most likely responsible?
Explanation
The management of Mycobacterium tuberculosis utilizes a multi-drug regimen where specific agents can interfere with vital metabolic pathways. Isoniazid, a core bactericidal drug, often depletes the body's levels of pyridoxine, which is essential for maintaining the integrity of the peripheral nervous system. This functional deficiency leads to axonal degeneration and the subsequent development of the sensory symptoms reported by the client during long-term therapy.
Rationale for correct answer
1. This medication is the most likely cause of the client's symptoms because it interferes with the metabolic activation of vitamin B6. The resulting deficiency manifests as peripheral neuropathy, characterized by symmetrical numbness and a "pins and needles" tingling sensation in the distal extremities. To prevent this neurological complication, clinicians routinely prescribe daily pyridoxine supplements alongside this specific antitubercular agent.
Rationale for incorrect answers
2. This drug is primarily associated with the benign, reddish-orange discoloration of body fluids and significant hepatotoxicity. It functions by inhibiting bacterial RNA polymerase but does not typically cause paresthesia or nerve damage in the hands and feet. Nurses should prioritize monitoring liver enzymes and educating the patient about harmless changes in urine color rather than neurological deficits.
3. This agent is known for causing hyperuricemia, which can lead to acute joint pain or gouty arthritis in susceptible individuals. While it is also hepatotoxic, it does not have a documented association with peripheral nerve impairment or sensory disturbances. Assessment should focus on the client's joints and uric acid levels rather than the tingling sensations mentioned in the prompt.
4. This bacteriostatic medication is uniquely linked to optic neuritis, which results in visual disturbances and loss of red-green color discrimination. It does not negatively impact the peripheral nerves of the extremities or interfere with pyridoxine metabolism. The nursing priority for this drug is ensuring the client receives regular ophthalmologic exams to monitor for ocular toxicity.
Test-taking strategy
- Pair Isoniazid directly with its "partner" Vitamin B6 to remember that it is the primary cause of nerve-related side effects.
- Use the organ-based system: Isoniazid affects nerves, Ethambutol affects eyes, Rifampin affects secretions/liver, and Pyrazinamide affects joints.
- Recognize that numbness and tingling are the classic descriptors for peripheral neuropathy in medical-surgical nursing questions.
- Distinguish between the intended therapeutic effect (killing TB) and the collateral metabolic effect (B6 depletion).
Take home points
- Peripheral neuropathy is a dose-related side effect of isoniazid that can be prevented with 10–50 mg of daily Vitamin B6.
- Patients at high risk for this complication include those with diabetes, alcoholism, or severe malnutrition.
- If a patient reports paresthesia, the nurse must assess for coordination and gait changes that may indicate advancing nerve damage.
- Isoniazid must still be taken consistently despite these side effects; the priority is adding the supplement rather than stopping the TB treatment.
A client asks the nurse how long pulmonary TB treatment typically lasts. Which is the nurse’s best response?
Explanation
Tuberculosis treatment requires combination antibiotics to cure infection and prevent resistance. The standard regimen includes isoniazid, rifampin, pyrazinamide, and ethambutol. Treatment usually lasts 6 months, with an intensive phase followed by continuation. Adherence, monitoring, and support are essential to ensure cure and reduce transmission. Public health follow-up is critical globally.
Rationale for correct answer
1. The standard duration for treating uncomplicated active pulmonary tuberculosis is 6 to 9 months, which may be extended significantly for multidrug-resistant (MDR) cases. This prolonged timeframe is necessary because Mycobacterium tuberculosis is a slow-growing pathogen that requires extended exposure to antimicrobials for complete sterilization. Providing this information ensures the client understands that pharmacological persistence is the only way to prevent disease relapse.
Rationale for incorrect answers
2. While a patient may become non-infectious after two to three weeks of therapy, the bacteria are far from being eradicated from the body. Stopping treatment at this early stage would lead to an immediate return of the infection and the selection of resistant strains. This timeframe is only relevant for determining when isolation precautions might be lifted, not for the total duration of the cure.
3. Clinical symptoms often improve significantly within the first few weeks of therapy, but this does not indicate that the infection is cleared. Instructing a patient to stop medication once they "feel better" is a dangerous practice that directly causes treatment failure. Adherence must be maintained through the entire prescribed course, regardless of the absence of cough or fever.
4. Tuberculosis treatment is not lifelong; it is a curative regimen with a defined end point once microbiological clearance is documented. Lifelong therapy is more characteristic of chronic viral infections like HIV, whereas TB is a bacterial infection that can be completely eliminated. Suggesting that the treatment never ends could unnecessarily discourage the client from initiating the standard therapeutic course.
Test-taking strategy
- Memorize the standard "6 to 9 months" window as the baseline for all modern, first-line tuberculosis treatment regimens.
- Distinguish between the infectious period (weeks) and the curative period (months) to avoid selecting inadequate treatment durations.
- Rule out any options that encourage self-discontinuation of antibiotics, as this is always a red flag in nursing pharmacology questions.
- Focus on the biological nature of the bacteria (slow-growing, acid-fast) to understand why short-term therapy is never sufficient for a cure.
Take home points
- The "intensive phase" usually involves four drugs for 2 months, followed by a "continuation phase" of two drugs for 4 to 7 months.
- Treatment for multidrug-resistant TB (MDR-TB) can last up to 20 months or longer with second-line agents.
- Directly Observed Therapy (DOT) is often used to ensure patients complete the full 6-to-9-month course.
- Sputum cultures are used at the end of treatment to officially confirm that the patient is cured.
A nurse is teaching a client about directly observed therapy (DOT) for TB. Which statements should the nurse include? Select all that apply
Explanation
Directly Observed Therapy (DOT) is a cornerstone of public health management for tuberculosis, designed to maximize adherence and ensure treatment success. By providing a structured framework for medication administration, DOT addresses the social and clinical barriers that often lead to premature discontinuation of the multi-drug regimen. This strategy is essential for achieving individual cure and protecting the community from the threat of untreated transmission.
Rationale for correct answers
1. The defining feature of DOT is that a trained healthcare worker physically watches the client swallow every dose of their medication. This ensures 100% compliance and allows for immediate identification of any adverse reactions or side effects. This direct supervision removes the burden of self-management, ensuring the clinical protocol is followed exactly as prescribed.
2. Inconsistent dosing is the primary driver of multidrug-resistant TB (MDR-TB). By guaranteeing that every dose is consumed, DOT prevents the bacilli from being exposed to sub-therapeutic levels of antibiotics, which would otherwise allow for the selection of resistant strains. This protective measure is vital for maintaining the efficacy of standard first-line agents.
4. To promote adherence, DOT is designed to be highly accessible and can be performed in various settings, including the client's home, workplace, or a local clinic. This flexibility reduces the logistical and financial barriers to treatment, making it easier for the patient to integrate the long-term regimen into their daily life.
Rationale for incorrect answers
3. DOT is a standard of care typically recommended for all clients with active tuberculosis, regardless of their initial compliance history. It is not a punitive measure reserved only for those who "miss a dose," but a proactive strategy to prevent failure. Implementing DOT early ensures that the intensive phase of treatment is completed successfully.
5. While DOT ensures medication is swallowed, it does not replace the necessity for routine laboratory monitoring. Patients must still undergo regular liver function tests, sputum cultures, and vision screenings to monitor for drug-induced toxicities and confirm bacterial clearance. DOT is a delivery strategy, not a substitute for the comprehensive clinical surveillance required during treatment.
Test-taking strategy
- Identify DOT as a public health intervention aimed at compliance and the prevention of drug-resistant bacteria.
- Associate DOT with flexibility and observation, rather than punishment or a lack of clinical monitoring.
- Rule out any options that suggest a decrease in monitoring, as TB therapy always requires ongoing biological verification.
- Recognize that "Directly Observed" literally means a person must see the medication being consumed to satisfy the requirement.
Take home points
- DOT is the "Gold Standard" recommended by the CDC and WHO for all patients being treated for active TB.
- The observer must be a trained person; a family member is usually not recommended to avoid issues with accountability.
- DOT can significantly shorten the overall time spent in the public health system by preventing treatment relapses.
- Successful completion of a DOT program is the most effective way to ensure a patient is cured and can return to normal activities.
A nurse is caring for a client with TB and HIV. Which consideration is most important when planning care?
Explanation
The management of patients with a dual diagnosis of Tuberculosis and HIV is complex due to the immunological suppression and the potential for life-threatening drug-drug interactions. Because many antitubercular agents induce hepatic enzymes, they can significantly alter the metabolic clearance of antiretroviral drugs. Harmonizing these two therapeutic regimens requires precise clinical timing and intensive monitoring to ensure both the viral load is suppressed and the bacterial infection is eradicated.
Rationale for correct answer
1. Rifamycins, particularly rifampin, are potent inducers of the cytochrome P450 enzyme system, which can drastically reduce the blood levels of various antiretroviral medications. This interaction risks therapeutic failure of the HIV regimen and the development of viral resistance. Nurses must coordinate with the healthcare team to monitor drug levels closely and potentially adjust dosages or substitute agents to maintain the efficacy of both treatments.
Rationale for incorrect answers
2. The statement that TB medications have no impact on HIV treatment is medically inaccurate and dangerous. As noted, rifampin significantly lowers the concentration of protease inhibitors and non-nucleoside reverse transcriptase inhibitors in the systemic circulation. Ignoring these interactions would compromise the patient's immune recovery and allow both the virus and the bacteria to proliferate unchecked.
3. A patient's HIV status has a profound negative impact on the prognosis of tuberculosis. Immunosuppression increases the likelihood of disseminated (extrapulmonary) TB, treatment failure, and higher mortality rates compared to HIV-negative individuals. The synergy between these two pathogens creates a "syndemic" where the progression of AIDS is accelerated by the inflammatory response to the TB infection.
4. Tuberculosis therapy for individuals with HIV can never be shortened to reduce the pill burden; in fact, it may sometimes be extended. Shortening the course of treatment for a patient with a weakened immune system significantly increases the risk of disease relapse and the emergence of drug resistance. Managing "pill burden" is addressed through supportive care and patient education, not by compromising the pharmacological protocol.
Test-taking strategy
- Prioritize "Safety and Drug Interaction" options when a question involves two complex, multi-drug therapeutic regimens.
- Recall that Rifampin is the "master inducer" of liver enzymes, making it the most likely culprit for drug interactions in TB care.
- Recognize that immunocompromised status (HIV) always complicates the prognosis and treatment of bacterial infections.
- Reject any answer that suggests shortening an antibiotic course for a high-risk patient, as this contradicts standard infectious disease principles.
Take home points
- HIV and TB are considered a "deadly duo" as each disease accelerates the progression of the other.
- Rifabutin is often used as a substitute for Rifampin in HIV patients because it has fewer drug interactions with antiretrovirals.
- Immune Reconstitution Inflammatory Syndrome (IRIS) is a potential complication when starting HIV meds shortly after TB treatment.
- Strict adherence to both regimens is required to prevent the development of multidrug-resistant TB and drug-resistant HIV.
A nurse is counseling a client newly diagnosed with TB. Which strategies should the nurse include to support adherence and mental health? Select all that apply
Explanation
The management of active tuberculosis extends beyond pharmacological intervention, requiring a holistic approach to address the psychosocial and emotional barriers to recovery. Because the treatment involves a prolonged regimen, patients often experience isolation, anxiety, and social marginalization. Nursing strategies must prioritize health literacy and psychological resilience to ensure the client remains engaged with the clinical team throughout the multi-month curative process.
Rationale for correct answers
1. Support groups provide a vital platform for patients to share experiences with others navigating the same long-term therapy. This social connection reduces feelings of alienation and provides a sense of community during the infectious phase. Peer support is a proven intervention for improving mental health outcomes and fostering the commitment necessary to finish the entire treatment course.
2. Comprehensive education on the rationale for completing therapy empowers the client to participate actively in their own care. Understanding that the disappearance of symptoms does not equal the eradication of the pathogen helps prevent premature discontinuation. Clear communication about the risks of relapse and resistance reinforces the necessity of the full 6-to-9-month pharmacological commitment.
4. Tuberculosis carries a significant social stigma that can lead to depression, non-adherence, and social withdrawal. By discussing these challenges openly, the nurse helps the client develop coping mechanisms and prepares them for potential interactions with friends or employers. Addressing stigma directly reduces the psychological burden and encourages the client to seek help rather than hiding their diagnosis.
Rationale for incorrect answers
3. Instructing a client to remain in isolation for the entire duration of treatment is medically unnecessary and psychologically damaging. Most patients become non-infectious after several weeks of therapy and can return to normal social activities once cleared by negative sputum smears. Imposing an "exceptions-free" isolation for six months would lead to severe emotional distress and likely result in treatment non-compliance.
5. Avoiding the discussion of side effects is an unsafe nursing practice that increases patient anxiety when unexpected symptoms occur. Clients must be informed of what to expect, such as orange urine from rifampin or tingling from isoniazid, to prevent them from stopping the medication out of fear. Open dialogue about adverse effects builds trust and allows for early intervention before complications become severe.
Test-taking strategy
- Select interventions that promote patient empowerment and address the holistic (emotional/social) needs of the client.
- Rule out any "extremes" in nursing care, such as "isolation for the entire duration" or "avoiding discussions" of important clinical information.
- Prioritize therapeutic communication strategies that identify and mitigate barriers to compliance, like stigma and lack of social support.
- Recognize that education is the primary tool for fostering adherence in any chronic or long-term disease management plan.
Take home points
- Adherence is highest when patients feel supported and understand the "why" behind their long treatment journey.
- Mental health screenings should be part of routine TB follow-up appointments to catch signs of depression early.
- Social workers and community health workers are essential members of the TB care team for addressing housing and financial barriers.
- Education must be culturally sensitive and provided at an appropriate literacy level to be truly effective.
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Define tuberculosis and explain its causative agent and modes of transmission.
- Describe the pathophysiology of tuberculosis and how it affects the body.
- Identify common risk factors and populations at increased risk for TB infection.
- Recognize the clinical manifestations of latent and active tuberculosis.
- Explain the diagnostic methods used to detect tuberculosis, including screening tests.
- Discuss pharmacologic management of tuberculosis, including first-line anti-TB medications.
- Describe nursing interventions and infection-control measures for patients with TB.
- Explain prevention strategies, including patient education, adherence to treatment, and public health measures.
Introduction
Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis. It usually involves the lungs, but any organ can be infected. TB is a primary cause of death worldwide from a potentially curable infectious disease. It is the leading cause of mortality in patients with HIV infection. The incidence of TB worldwide declined until the mid-1980s when HIV disease emerged. The major factors contributing to the resurgence of TB were high rates of TB among patients with HIV infection and the emergence of MDR strains of M. tuberculosis. Worldwide, more than two billion people (one third of the population) are currently infected with TB. Although the prevalence of TB has increased in Europe, in the United States it has steadily declined since reaching a resurgence peak in 1992. TB occurs disproportionately in the poor, the underserved, and minorities. In the United States, people at risk include the homeless, residents of inner-city neighborhoods, foreign-born people, those living or working in institutions (long-term care facilities, prisons, shelters, hospitals), IV injecting drug users, people at poverty level, and those with poor access to health care. Immunosuppression from any etiology (e.g., HIV infection, malignancy, long-term corticosteroid use) increases the risk of active TB infection. The prevalence of TB in the United States is highest in those of Asian descent.
Epidemiology
- United States
The incidence of TB infection in the US has been slowly declining.
The incidence rate for 2018 was 2.8 cases per 100,000 population.
Two-thirds of new TB cases reported in the US in 2019 were in individuals born outside the US.
The prevalence of LTBI in the United States is estimated to be 5%.
- Worldwide
A leading cause of death from a single infectious agent.
The overall incidence and prevalence have been declining.
The incidence rate for 2018 was 132 cases per 100,000 population.
One-fourth of the world's population has latent TB.
The sex ratio varies across countries and communities and largely depends on social and cultural factors.
Countries with the highest incidence of TB: India, Indonesia, China, the Philippines, Bangladesh, Nigeria, Pakistan, and South Africa.
The incidence of multidrug-resistant TB is steadily rising.
Etiology
Mycobacteria species
|
Category |
Details |
|
Mycobacterium Species |
Mycobacterium tuberculosis complex |
|
Mycobacterium tuberculosis |
Mode of transmission: aerosol droplet nuclei Reservoir: predominantly humans Disease: all forms of tuberculosis |
|
Mycobacterium bovis |
Mode of transmission: ingestion of contaminated cow's milk Reservoir: predominantly cattle Disease: gastrointestinal tuberculosis in humans |
|
Mycobacterium africanum |
Common cause of tuberculosis in West, Central, and East Africa |
|
Mycobacterium microti |
No specific details provided |
Risk factors
- Working in the health care industry
- Migration from countries with a high TB incidence (≥ 100 cases per 100,000 population)
- Frequent travel to countries with a high TB burden
- Close contact with a patient with active TB infection
- Crowded living conditions (e.g., prisons)
- Homelessness
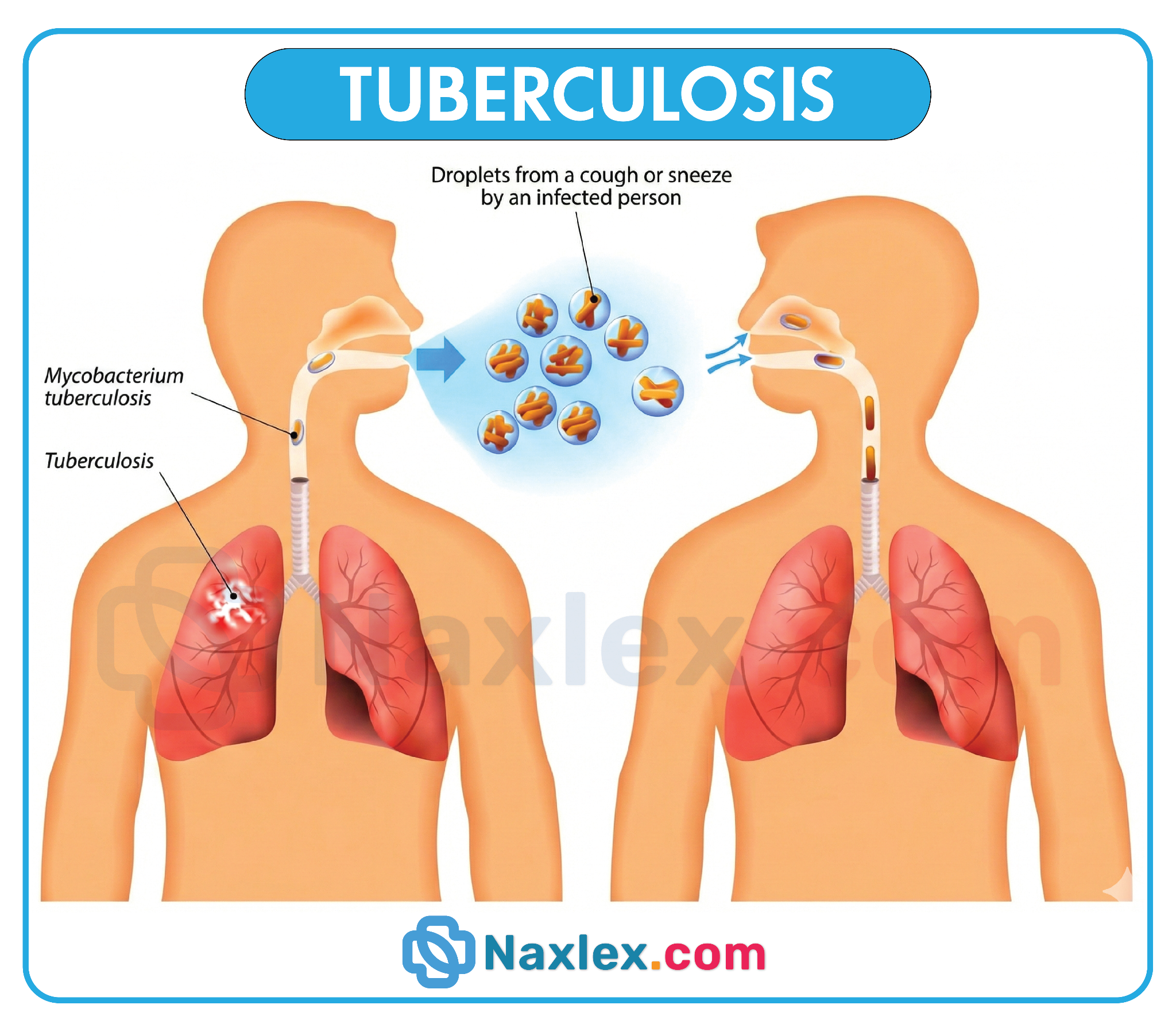
Pathophysiology
Primary tuberculosis
Innate immune response
Exposure to M. tuberculosis
- Individuals with M. tuberculosis infection disperse droplet nuclei via sneezing or coughing.
- Inhaled droplet nuclei reach the terminal alveoli and are taken up by alveolar macrophages.
Entry into macrophages
- Mycobacterial cell wall contains pathogen-associated molecular patterns (PAMPs) such as lipoarabinomannan and lipomannan.
- Alveolar macrophages recognize M. tuberculosis PAMPs via toll-like receptors (TLRs).
- Activation of TLRs leads to production of proinflammatory cytokines (e.g., IL-1, IL-12, TNF-α) and phagocytosis of mycobacteria.
Replication within macrophages
- Phagocytosed organisms reside within a phagosome for intracellular killing via:
- Phagosome maturation: acidification using a proton pump system
- Fusion of phagosome and lysosome: mediated by increased intracellular calcium levels
- Killing of bacteria by reactive oxygen species (ROS), reactive nitrogen intermediates (RNI), and lysosomal enzymes
- M. tuberculosis survives within macrophages by inhibiting phagosome maturation and phagolysosome fusion
Virulence factors
- Cord factor (trehalose-6,6'-dimycolate): surface glycolipid causing serpentine cord-like growth, inhibits neutrophil migration, induces TNF-α release to stimulate granuloma formation
- Sulfatides: inhibit phagolysosome fusion
- Lipoarabinomannan: induces TNF-α release from macrophages and scavenges ROS
- Catalase-peroxidase: destroys ROS and H2O2
Macrophage lysis and release of bacteria
- Replicated bacteria attack uninfected macrophages to spread infection.
- Dendritic cells migrate to the site of infection and process mycobacterial antigens.
- Some bacteria enter the bloodstream, causing bacteremia and seeding multiple organs.
Cellular immune response
Th1 cell activation
- Dendritic cells present mycobacterial antigens with MHC 2 to naive T cells
- Activated CD4+ T cells migrate to infection sites (type IV HSR)
Macrophage activation and bacterial killing
- Activated CD4+ T cells release IFN-γ
- IFN-γ promotes phagosome maturation, enhanced RNI production, autophagy
Granulomatous inflammation and tissue destruction
- IFN-γ-activated macrophages secrete TNF-α
- TNF-α promotes aggregation of macrophages and T cells to form granulomas
- Destruction of infected macrophages causes central caseous necrosis and tissue damage
- Granuloma limits infection spread
- Ghon focus: granuloma typically in middle/lower lung lobes
- Ghon complex: Ghon focus, regional lymph node, and linking lymphatic vessels
Disease progression
- Sufficient immune response: most bacteria are killed; some persist causing LTBI; granulomas undergo fibrosis and calcification to form Ranke complex
- Deficient immune response (HIV, malnutrition): failure of granulomas to limit infection; progressive primary TB; bacteremia; miliary TB
Secondary tuberculosis
- Latent TB: dynamic equilibrium between host immune response and M. tuberculosis
- Reactivation: due to immune weakening (e.g., HIV, TNF-α inhibitor therapy)
- Disease progression: caseating granulomas with central necrosis and Langhans giant cells; usually affects upper lobes of lungs; can affect other organs
- Prior sensitization results in stronger inflammatory response, extensive tissue destruction, cavitation, and scarring
Clinical Features
Latent tuberculosis infection
- Typically asymptomatic
Pulmonary tuberculosis
Systemic
- Low-grade fever with night sweats
- Weight loss, anorexia, decreased appetite
- Malaise, weakness
Pulmonary
- Non-productive cough initially
- Symptoms of progression: productive cough with purulent sputum, hemoptysis
- Shortness of breath
- Pleuritic chest pain
Clinical examination
- Findings nonspecific; general: pallor, clubbing (advanced disease), generalized wasting
- Chest: varies depending on involvement
- Consolidation: dullness on percussion, crackles, diminished breath sounds
- Cavitation: hyperresonance on percussion, amphoric breath sounds
- Bronchial obstruction: rhonchi
- Pleural effusion/empyema: dullness on percussion, diminished breath sounds
- Other findings: erythema nodosum, phlyctenular conjunctivitis
- TB in HIV-positive individuals may progress atypically or rapidly
Extrapulmonary tuberculosis
- Clinical features vary depending on organ involvement
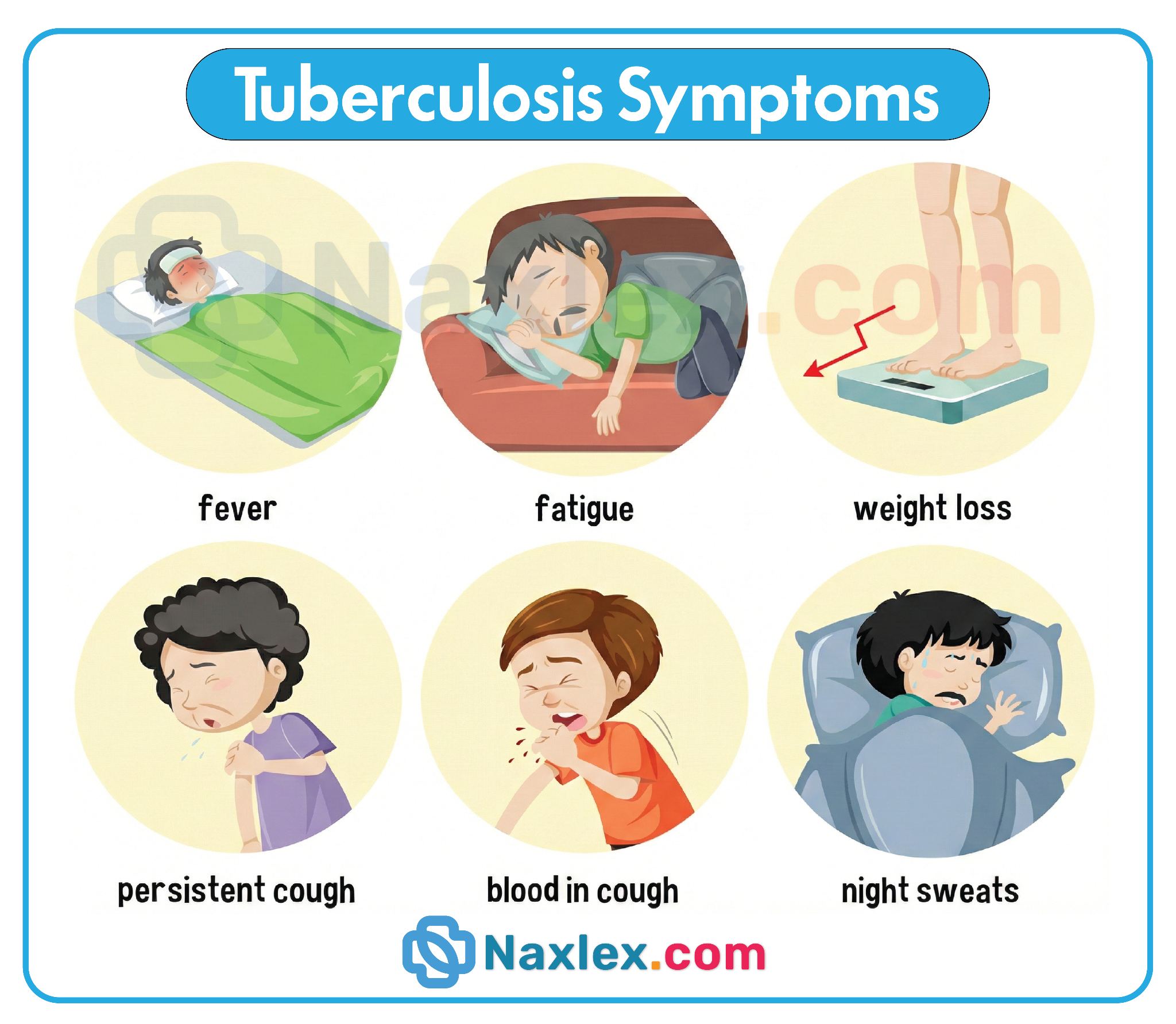
Diagnosis
Microbiological studies
- Confirmation by direct visualization, culture, or genetic detection
- Samples:
- Sputum: ≥ 3 samples at 8–24 hour intervals (at least one early morning)
- Induced sputum
- Gastric lavage
- Bronchoalveolar lavage
- Extrapulmonary TB: fluid or tissue samples for cell count, chemistries, AFB smear, NAAT
Mantoux test
- An intradermal injection of an extract of the tubercle bacillus is made.
- An induration (palpable, raised, hardened area) of 10 mm or greater in diameter indicates a positive skin test.
- An induration of 5 mm is considered a positive test for immunocompromised clients.
- A positive Mantoux test indicates that the client has developed an immune response to TB. It does not confirm that active disease is present. Clients who have been treated for TB may retain a positive reaction.
- Individuals who have latent TB may have a positive Mantoux test and may receive treatment to prevent development of an active form of the disease.
- Clients who have received a Bacillus Calmette-Guerin (BCG) vaccine within the past 10 years may have a false-positive Mantoux test. These clients will need a chest x-ray to evaluate the presence of active TB infection.
- Clients who are immunocompromised (such as those who have HIV) and the elderly should be tested for TB.
- Client Education: Reinforce to the client the importance of returning for a reading of the injection site by a health care personnel within 48 to 72 hr.
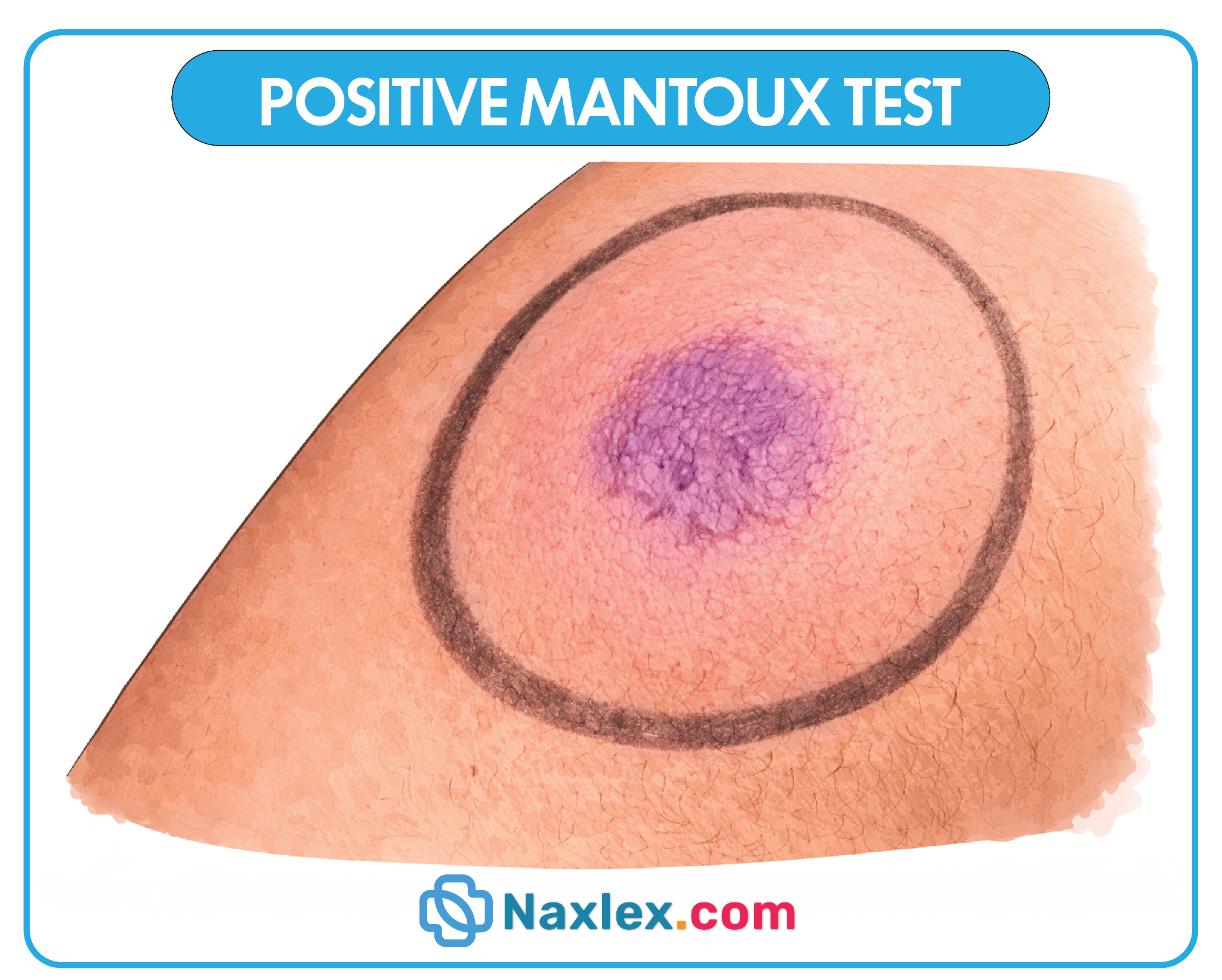
Microbiological tests for active TB
|
Test |
Description |
Advantages |
Disadvantages |
|
Acid-fast bacilli smear microscopy |
Ziehl-Neelsen or auramine rhodamine stain |
Rapid, inexpensive |
Low sensitivity; cannot differentiate from nontuberculous mycobacteria; stains viable and nonviable bacteria |
|
Nucleic acid amplification test |
Used for initial testing with AFB smear/culture |
High specificity & sensitivity; rapid diagnosis; detects drug-resistant strains; low cross-reactivity |
Requires equipment & trained staff; viable and nonviable bacteria detectable |
|
Culture |
Gold standard diagnostic test; provides drug susceptibility |
High sensitivity; species identification; identifies drug resistance |
Takes 2–6 weeks; delays initiation of treatment |
Drug susceptibility testing
- Standard culture: results in several weeks
- Rapid molecular testing: for high-risk patients
- Negative AFB smear does not rule out pulmonary TB; confirmatory culture recommended
Imaging
|
Imaging |
Primary TB |
Postprimary TB |
|
Chest x-ray |
Consolidation (homogeneous, ill-defined), hilar lymphadenopathy, Ghon complex, pleural effusion, cavitation (rare) |
Consolidation (patchy/confluent), fibrocaseous cavitary lesions in upper lobes, calcifications |
|
CT chest |
Enlarged lymph nodes with central necrosis |
Thick-walled cavities, tree-in-bud pattern, extensive cavitation; aspergillomas possible |
- Normal imaging does not rule out TB
- Immunocompromised individuals may have normal imaging findings
HIV and TB coinfection
- Diagnosing TB in HIV patients is challenging: negative AFB smear, atypical imaging due to paucibacillary disease
- Measures to increase diagnostic sensitivity: fluorescent AFB smear, specialized culture mediums
- Severe disease or CD4 < 100 cells/mm³: lateral flow urine lipoarabinomannan assay
- Resource-limited settings: lower threshold for smear positivity; empiric treatment may be necessary
- HIV testing recommended in all patients with suspected TB
Treatment
Pretreatment evaluation
Clinical assessment
- Weight
- Nutritional assessment
- Symptom review
- Eye exam: visual acuity and color discrimination
- Microbiology: sputum smear microscopy and culture, drug susceptibility testing
- Imaging: chest x-ray or other chest imaging
Laboratory studies
- All patients: liver chemistries, platelet count, BMP, HIV screening
- Depending on risk: hepatitis B and hepatitis C screening, diabetes screening
Antituberculosis therapy
RIPE TB regimen
- Intensive phase: 8 weeks (~2 months) of rifampin PLUS isoniazid, pyrazinamide, and ethambutol
- Continuation phase: 18 weeks (~4 months) of rifampin PLUS isoniazid
- Adjuvant treatment: pyridoxine to prevent vitamin B6 deficiency from isoniazid (for all individuals at risk of neuropathy)
Additional considerations
- Self-administered and daily dosages are preferred
- Directly observed therapy (DOT; standard practice): health care personnel observe the patient taking the medication
- Restart full treatment if there is an interruption of ≥ 14 days during the intensive phase
- RIPE TB regimen consists of 6 months of rifampin and isoniazid plus pyrazinamide and ethambutol during the first 2 months
- "RIPE": Rifampin, Isoniazid, Pyrazinamide, and Ethambutol
- The long duration of treatment for active TB requires patient-centered coordination with primary care and specialist services and DOT to ensure adherence
Treatment of drug-resistant TB disease
- Includes MDR-TB and XDR-TB
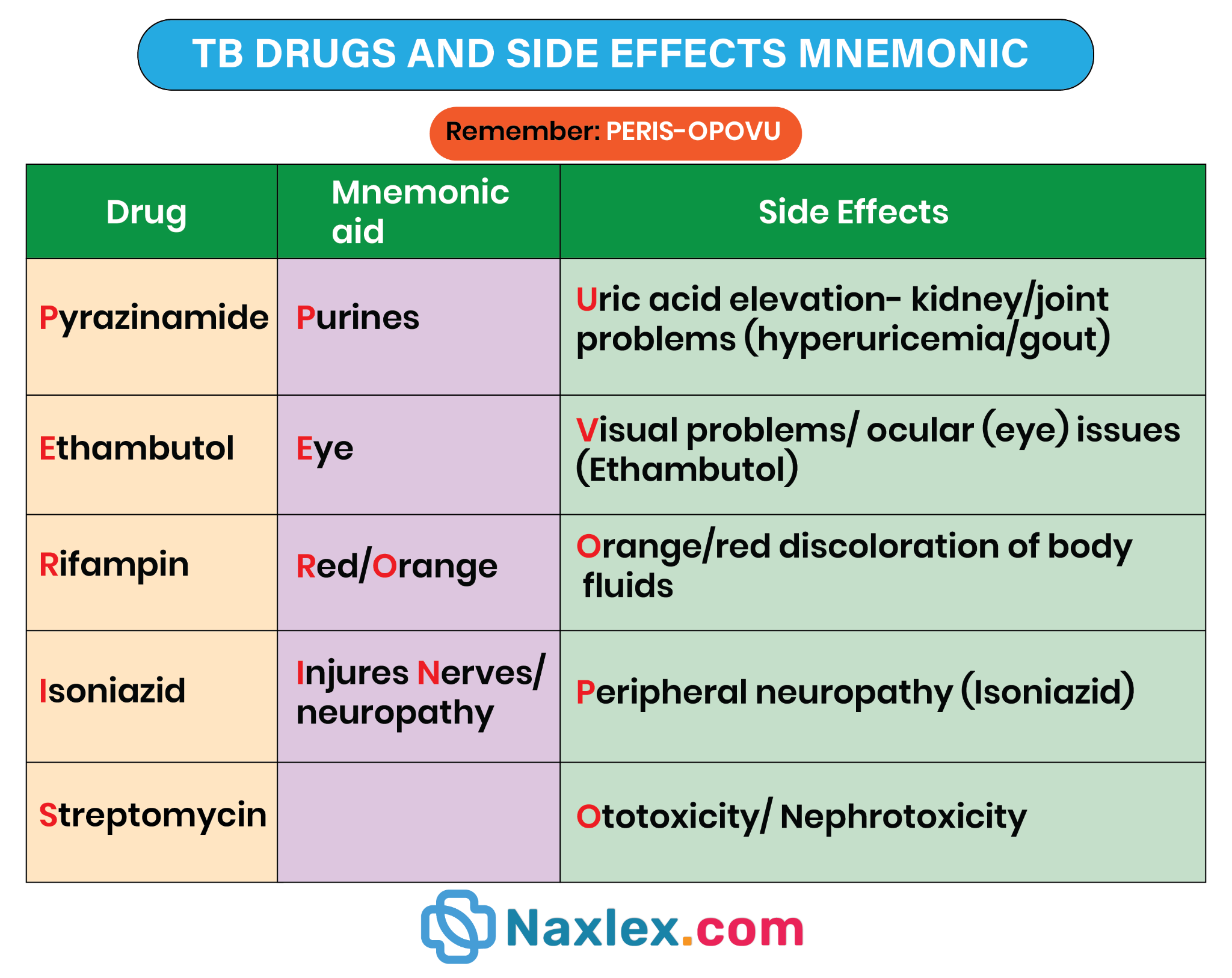
Agents
- Oral: later-generation fluoroquinolone (e.g., moxifloxacin), bedaquiline, linezolid, clofazimine, cycloserine
- IV: amikacin, streptomycin, carbapenem with amoxicillin-clavulanic acid
Treatment of extrapulmonary TB
- Choose antimicrobials under specialist guidance
- Tailor choice and duration of therapy to the infection site, severity, and response
Side effects of antituberculosis agents
|
Drug |
Side effects |
|
Isoniazid |
Asymptomatic elevation of transaminases; cytochrome P450 inhibition (drug interactions including ART, cardiovascular agents, antibiotics); less common: drug-induced lupus, vitamin B6 deficiency (sideroblastic anemia, peripheral neuropathy), CNS toxicity (benzodiazepine-refractory seizures at high doses, psychosis, ataxia); others: anion gap metabolic acidosis, pellagra, optic neuritis |
|
Rifampin |
Transient asymptomatic elevation of bilirubin, clinical hepatitis with cholestatic pattern; cytochrome P450 induction (drug interactions); orange discoloration of body fluids (urine, tears); thrombocytopenia; false-positive urine opiate screening |
|
Pyrazinamide |
Greatest hepatotoxicity potential; hyperuricemia; arthralgia; photosensitivity |
|
Ethambutol |
Optic neuritis (reversible red-green color blindness); hyperuricemia |
- Rifampin and isoniazid alter efficacy of drugs metabolized by cytochrome P450 (e.g., protease inhibitors, NNRTIs, OCPs, warfarin, sulfonylureas)
- Orange urine is common secondary to rifampin therapy
Monitoring
- Monthly follow-ups are recommended in all patients receiving antituberculosis treatment for active TB or LTBI
All patients
- Assess adherence to therapy
- Perform symptom review and screen for clinical features of active TB
- Monitor for side effects
Patients with active TB
- Sputum smear microscopy and culture
- Weight and vision assessment
- Laboratory studies: as indicated, including liver chemistries, platelet count, creatinine
- Advise patients to self-monitor for features suggesting hepatitis (e.g., jaundice, fatigue, anorexia, abdominal pain) and seek prompt medical attention if any arise
Complications
- Rasmussen aneurysm: inflammatory pseudoaneurysm of a branch of the pulmonary artery lying adjacent to a tuberculous cavity and manifesting with hemoptysis
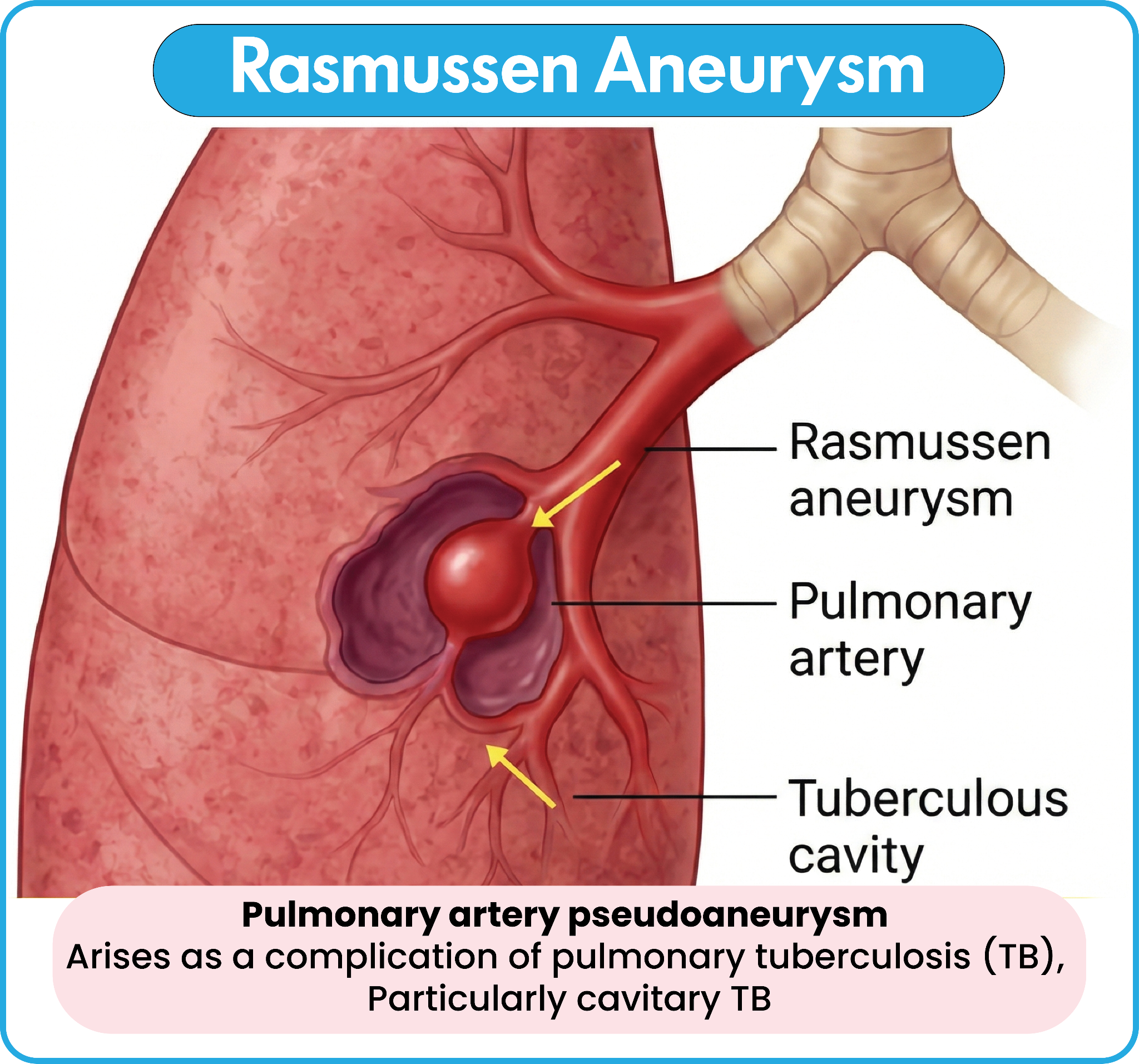
- Massive hemoptysis: due to erosion of blood vessels overlying a lung cavity, Rasmussen aneurysm, or aspergilloma
- Lung cavitation
- Lung fibrosis
- Aspergilloma
- Pneumothorax
- Bronchiectasis
- Fibrosing mediastinitis
- Venous thromboembolism
Client Education
- Provide the client and family education because TB is often treated in the home setting.
- Exposed family members should be tested for TB.
- Educate the client and family to continue medication therapy for its full duration of 6 to 12 months. Emphasize that failure to take the medications may lead to a resistant strain of TB.
- Instruct the client to continue with follow-up care for 1 full year.
- Inform the client that sputum samples are needed every 2 to 4 weeks to monitor therapy effectiveness. Clients are no longer considered infectious after three negative sputum cultures.
- Encourage proper hand hygiene.
- Instruct the client to cover mouth and nose when coughing or sneezing.
- Inform the client that contaminated tissues should be disposed of in plastic bags.
- Advise clients who have active TB to wear an N95 or HEPA respirator when in public places.
Summary
- Tuberculosis is a contagious infectious disease caused by Mycobacterium tuberculosis.
- TB is transmitted through airborne droplets when an infected person coughs, sneezes, or talks.
- There are two forms of TB: latent TB infection and active TB disease.
- People with latent TB have no symptoms and are not contagious, but the infection can become active.
- Active TB commonly affects the lungs and may cause a persistent cough, fever, night sweats, and weight loss.
- Individuals at higher risk for TB include those with weakened immune systems, close contacts of infected persons, and people living in crowded conditions.
- TB is diagnosed using skin tests or blood tests, chest X-rays, and sputum cultures.
- Treatment of TB requires a long course of multiple antibiotics taken exactly as prescribed.
- First-line TB medications may include isoniazid, rifampin, ethambutol, and pyrazinamide.
- Inadequate or incomplete treatment can lead to drug-resistant tuberculosis.
- Nursing care includes administering medications, monitoring for side effects, and promoting adherence to therapy.
- Prevention strategies include early detection, respiratory isolation, patient education, and public health reporting.
