
Please set your exam date
ATTENTION-DEFICIT/HYPERACTIVITY DISORDER (ADHD)
Study Questions
Practice Exercise 1
A nurse is educating a group of parents about the causes of attention-deficit/hyperactivity disorder (ADHD). Which of the following factors should the nurse include as being attributed to the etiology of the disorder? Select all that apply
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder characterized by persistent inattention, hyperactivity, and impulsivity. It involves geneticpredisposition, neurochemicaldysregulation, abnormal dopaminergicsignaling, and altered prefrontal cortexfunction. Symptoms include distractibility, poor executive function, and impaired working memory. Neuroimaging shows reduced cortical thickness and hypoactivity in fronto-striatal circuits. Environmental factors may exacerbate severity but are not primary etiologies.
Rationale for correct answers:
1.Genetic factors are strongly implicated, with heritability estimates ≥70%.Twin studies confirm familial aggregation. Specific polymorphisms in dopamine transporter and receptor genes increase vulnerability. The question stem highlights causative factors, making genetics a scientifically valid etiology. Geneticand heritabilityare central.
3.Neurochemical factors are critical, particularly dopamine and norepinephrine imbalance in fronto-striatal pathways. Reduced catecholamine activity impairs attention regulation. Pharmacologic evidence supports this, as stimulants normalize neurotransmission. The stem’s focus on etiology validates neurochemical dysregulation. Dopamineand norepinephrineare emphasized.
Rationale for incorrect answers:
2.Psychodynamic factors are not causative. They may explain behavioral manifestations but lack neurobiological evidence. ADHD is not rooted in unconscious conflict or early psychosexual stages. Reliance on psychodynamic theory misattributes etiology. Psychodynamicsand conflictare irrelevant.
4.Family dynamic factors influence symptom expression and management but are not etiologic. Dysfunctional parenting may worsen behavior but does not cause ADHD. Neurodevelopmental abnormalities precede environmental influences. Familyand environmentare contributory, not causal.
5.Dietary factors have limited evidence. Additives or sugar may exacerbate symptoms but are not primary causes. Controlled trials show inconsistent associations. Etiology remains neurobiological, not nutritional. Dietaryand additiveslack scientific causation.
Test-taking strategy
- Focus on etiologyrather than contributing or exacerbating factors.
- Rule out theories lacking neurobiological evidence such as psychodynamicexplanations.
- Distinguish between causativeversus influencingfactors.
- Use knowledge of geneticsand neurochemistryas established scientific bases.
- Eliminate options that describe environmental modifiers (family dynamics, diet) since they do not explain pathogenesis.
- Apply evidence-based reasoning: ADHD is a neurodevelopmental disorderwith strong heritability and neurotransmitter dysregulation.
- When faced with “select all that apply,” ensure each choice aligns with established pathophysiology.
- Avoid distractors that describe management or symptom exacerbation rather than causation.
- Remember that stimulant pharmacologysupports neurochemical etiology, reinforcing neurotransmitter imbalance as a correct answer.
- Genetic linkage studies provide definitive evidence, making genetics a reliable choice.
Take home points
- ADHD is a neurodevelopmental disorder with strong genetic heritability.
- Dopamine and norepinephrine dysregulation underlie attentional deficits and impulsivity.
- Family dynamics and diet may influence severity but are not causative.
- Psychodynamic theories lack scientific validity in explaining ADHD etiology.
A nurse is explaining the biological basis of attention-deficit/hyperactivity disorder (ADHD) to a group of nursing students. Which factor should the nurse identify as being associated with the genetic etiology of the disorder?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder with strong geneticpredisposition, involving abnormal dopaminergicsignaling, impairedprefrontal cortexregulation, and alteredcatecholaminepathways. Heritability is estimated at ≥70%, with family and twin studies confirming genetic transmission. Specific gene polymorphisms in dopamine transporter and receptor genes increase susceptibility.
Rationale for correct answer:
2.Having a sibling diagnosed with ADHD reflects familial aggregation and high heritability. Twin and family studies consistently show genetic transmission. The stem emphasizes genetic etiology, and sibling presence is a direct indicator of inherited vulnerability. Heritabilityand familiallinkage confirm this.
Rationale for incorrect answers:
1.Inborn error of metabolism is not implicated in ADHD pathogenesis. Metabolic disorders such as phenylketonuria cause cognitive impairment but do not specifically produce ADHD. ADHD is linked to neurotransmitter dysregulation, not metabolic enzyme defects. Metabolismand enzymeare irrelevant.
3.Dopamine neurotransmitter deficit is a neurochemical factor, not strictly genetic. While dopamine dysregulation contributes to symptoms, it represents biochemical imbalance rather than inherited etiology. The stem specifies genetic basis, making this option incorrect. Dopamineand neurochemicalare contributory, not genetic.
4.Arrested id development is a psychodynamic concept without biological evidence. ADHD is not explained by Freud’s structural theory of personality. Neurodevelopmental abnormalities, not unconscious conflict, underlie the disorder. Psychodynamicand idare scientifically invalid here.
Test-taking strategy
- Focus on the stem wording: it specifies genetic etiology, not biochemical or psychodynamic.
- Rule out options describing neurochemical imbalanceor psychodynamic theory, as these are not genetic.
- Eliminate distractors that describe unrelated conditions (inborn errors of metabolism).
- Recognize that family historyis the strongest genetic indicator.
- Use knowledge of heritability studies: ADHD shows sibling and twin concordance, confirming genetics.
- Apply principle: when asked about genetic basis, select familial aggregation rather than neurotransmitter imbalance.
- Remember that dopamine deficit is valid but belongs under neurochemical etiology, not genetic.
- Psychodynamic explanations are outdated and lack biological evidence, making them easy eliminations.
- Inborn errors of metabolism cause global cognitive deficits, not ADHD-specific pathology.
- Correct answer aligns with evidence-based geneticsin ADHD research.
Take home points
- ADHD has strong genetic heritability, with sibling concordance supporting familial transmission.
- Dopamine and norepinephrine dysregulation explain neurochemical basis but are not genetic causes.
- Psychodynamic theories do not explain ADHD etiology.
- Inborn errors of metabolism cause cognitive impairment but are not linked to ADHD.
A nurse reviews possible causes of attention-deficit/hyperactivity disorder (ADHD) with a parent. Which factor is most strongly associated with the development of ADHD?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder with strong geneticpredisposition, involving abnormal dopaminergicsignaling, impaired prefrontal cortexregulation, and altered catecholaminepathways. Heritability is estimated at ≥70%, with family and twin studies confirming genetic transmission. Specific gene polymorphisms in dopamine transporter and receptor genes increase susceptibility.
Rationale for correct answer:
1.Genetic predisposition involving first-degree relatives is the most stronglyassociated factor. Twin and family studies consistently demonstrate high heritability. The presence of ADHD in parents or siblings significantly increases risk. Geneticand heritabilityevidence confirm this as the primary etiology.
Rationale for incorrect answers:
2.Inconsistent parental discipline may exacerbate behavioral symptoms but does not cause ADHD. Parenting style influences symptom severity and management but lacks neurobiological causation. ADHD originates from neurodevelopmental abnormalities, not discipline patterns. Parenting and environment are contributory, not causal.
3.Exposure to stressful school environments may worsen inattention and hyperactivity but is not etiologic. Environmental stressors influence symptom expression but do not explain pathogenesis. ADHD develops from genetic and neurochemical abnormalities. Stressand schoolfactors are secondary.
4.Delayed toilet training during toddlerhood is unrelated to ADHD. Toilet training reflects developmental readiness and parental guidance, not neurobiological dysfunction. ADHD symptoms are linked to cortical and neurotransmitter dysregulation, not toileting milestones. Toilet and development are irrelevant.
Test-taking strategy
- Focus on the stem wording: it asks for the factor most strongly associated with ADHD development.
- Rule out options describing environmental influences or developmental milestones, as these are not causative.
- ADHD is a neurodevelopmental disorderwith high heritability; family history is the strongest predictor.
- Eliminate distractors that describe symptom exacerbation (school stress, parental discipline).
- Apply principle: when asked about strongest association, select genetic predispositionsupported by twin and family studies.
- Remember that neurotransmitter imbalance explains symptoms but the question specifies etiology, making genetics the correct choice.
- Use evidence-based reasoning: ADHD heritability ≥70% confirms genetic linkage.
- Distractors are environmental modifiers, not primary causes.
- Correct answer aligns with established scientific consensus on ADHD pathogenesis.
- Always prioritize biological evidencewhen asked about strongest associations.
Take home points
- ADHD is a neurodevelopmental disorder with strong genetic heritability.
- Family history, especially first-degree relatives, is the most significant risk factor.
- Environmental influences may worsen symptoms but are not causative.
- Developmental milestones such as toilet training are unrelated to ADHD etiology.
A nurse is providing an educational session for parents of children recently diagnosed with attention-deficit/hyperactivity disorder (ADHD). Which statement should the nurse include as an accurate description of the disorder?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder marked by inattention, hyperactivity, and impulsivity. It involves abnormal dopaminergicand noradrenergicsignaling within frontostriatal circuits, leading to impaired executive function. Symptoms persist ≥6 months, manifest before age 12, and cause functional impairment across settings.
Rationale for correct answer:
4.ADHD is characterized by a persistent pattern of inattention, often accompanied by hyperactivity and impulsivity. Diagnostic criteria require symptoms across ≥2 settings with significant impairment. The stem emphasizes accurate description, making this the correct choice. Inattentionand impulsivitydefine the disorder.
Rationale for incorrect answers:
1.Withdrawal into self describes autism spectrum disorder, not ADHD. ADHD involves externalizing behaviors such as distractibility and hyperactivity, not social withdrawal. Autismand withdrawalare distinct from ADHD pathology.
2.ADHD is not diagnosed before 2 years of age. Symptoms must be present before age 12, but reliable diagnosis typically occurs during school years. Ageand diagnosiscriteria exclude toddlers.
3.ADHD occurs more commonly in males than females, with a ratio of approximately 2:1 in childhood. Females often present with inattentive subtype, but prevalence is not equal. Genderand prevalencediffer.
Test-taking strategy
- Focus on DSM-5 diagnostic criteria: persistent inattention, hyperactivity, impulsivity.
- Rule out distractors describing other disorders (withdrawal → autism).
- Eliminate options inconsistent with diagnostic age criteria (<2 years).
- Apply epidemiology: ADHD is more common in males, not equal prevalence.
- Select the option that directly reflects the core symptom pattern.
- Use knowledge of diagnostic thresholds: symptoms ≥6 months, onset before 12 years, impairment in ≥2 settings.
- Remember that accurate descriptions must align with established definitions, not environmental or developmental factors.
- Distractors often describe associated conditions or misapplied features.
- Correct answer reflects the persistent symptom patterncentral to ADHD.
- Always prioritize evidence-based diagnostic language when evaluating descriptive statements.
Take home points
- ADHD is defined by persistent inattention, hyperactivity, and impulsivity.
- Diagnosis requires symptoms ≥6 months, onset before age 12, and impairment in multiple settings.
- Autism involves withdrawal into self, distinguishing it from ADHD.
- ADHD prevalence is higher in males, with females often showing inattentive subtype.
A nurse is performing a physical and behavioral assessment on a child. Which finding should the nurse recognize as a criterion for a diagnosis of attention-deficit/hyperactivity disorder (ADHD)?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder defined by inattention, hyperactivity, and impulsivity. It involves abnormal dopaminergicand noradrenergicsignaling in frontostriatal circuits, leading to impaired executive function. Symptoms must persist ≥6 months, begin before age 12, and cause impairment in ≥2 settings.
Rationale for correct answer:
1.Inattention is a DSM-5-TR diagnostic criterion for ADHD. It includes distractibility, difficulty sustaining tasks, forgetfulness, and disorganization. The stem specifies DSM-5-TR criteria, making inattention the accurate choice. Inattentionand disorganizationare core features.
Rationale for incorrect answers:
2.Recurrent intrusive thoughts are characteristic of obsessive-compulsive disorder, not ADHD. They involve unwanted, repetitive cognitions leading to compulsions. ADHD symptoms are attentional and behavioral, not intrusive thought patterns. Obsessionsand compulsionsare distinct.
3.Physical aggression is not a DSM-5-TR criterion for ADHD. Aggression may occur as a comorbidity with oppositional defiant disorder or conduct disorder but is not diagnostic. ADHD criteria focus on attention and activity regulation. Aggressionand conductare separate.
4.Anxiety and panic attacks are diagnostic of anxiety disorders, not ADHD. While ADHD may coexist with anxiety, panic attacks are not part of ADHD criteria. ADHD is defined by attentional and behavioral dysregulation. Anxietyand panicare unrelated.
Test-taking strategy
- Focus on DSM-5-TR diagnostic criteria: inattention, hyperactivity, impulsivity.
- Rule out distractors describing other psychiatric disorders (OCD, anxiety disorders, conduct disorders).
- Eliminate options that describe comorbidities rather than core diagnostic features.
- Apply principle: ADHD diagnosis requires symptoms ≥6 months, onset before 12 years, impairment in ≥2 settings.
- Select the option that directly reflects the core symptom pattern.
- Distractors often describe associated conditions but not diagnostic criteria.
- Correct answer aligns with established DSM-5-TR definitions.
- Always prioritize evidence-based diagnostic languagewhen evaluating descriptive statements.
- Use knowledge of comorbidities to rule out non-etiologic features.
- Inattention is the most accurate DSM-5-TR criterion in this context.
Take home points
- ADHD is diagnosed based on persistent inattention, hyperactivity, and impulsivity.
- DSM-5-TR requires symptoms ≥6 months, onset before age 12, impairment in multiple settings.
- Intrusive thoughts indicate OCD, not ADHD.
- Aggression and panic attacks are not diagnostic criteria but may occur as comorbidities.
Practice Excercise 2
A nurse obtains a health history for a client diagnosed with attention-deficit/hyperactivity disorder (ADHD). Which behaviors should the nurse expect? Select all that apply
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmentalcondition characterized by inattention, hyperactivity, and impulsivity. It results from dysregulation of dopamineand norepinephrinepathways in the prefrontal cortex. Symptoms include distractibility, poor task completion, excessive verbalization, and impulsive actions. Onset occurs before age 12, with prevalence higher in males.
Rationale for correct answers:
1.Impulsivity is a hallmark of ADHDdue to impaired inhibitory control in the prefrontal cortex. Clients act without forethought, interrupt conversations, and engage in risk-taking behaviors. This stems from deficient executive functioning and altered catecholamine signaling. Impulsivity and executive dysfunctiondefine the disorder.
2.Excessive talking reflects hyperactivityand poor self-regulation. Clients often dominate conversations, interrupt others, and struggle with quiet activities. This behavior arises from cortical disinhibition and impaired attention modulation. Hyperactivity and disinhibition make this a classic ADHD manifestation.
6.Failure to complete tasks is a core feature of inattention. Clients begin activities but leave them unfinished due to distractibility and poor sustained focus. This results from impaired working memory and deficient organizational skills. Inattention and distractibility explain this presentation.
Rationale for incorrect answers:
3.Spiteful behavior is more consistent with oppositional defiant disorder, not ADHD. ADHD involves impulsivity and distractibility, but not intentional hostility. The underlying pathology is attentional dysregulation, not deliberate aggression. Hostility and vindictiveness are not diagnostic features of ADHD.
4.Deliberately annoying others is typical of oppositional defiant disorder. ADHD clients may irritate others unintentionally due to impulsivity, but purposeful provocation is not characteristic. The neurobiology involves attentional deficits, not intentional defiance. Provocation and defiance distinguish ODD from ADHD.
5.Prolonged video gaming is a behavioral choice, not a diagnostic criterion. While ADHD clients may struggle with time management, excessive gaming is not a defining feature. It reflects environmental reinforcement, not intrinsic pathology. Behavioral addiction and environmental influence explain this, not ADHD.
Test-taking strategy
- Identify core symptomsof ADHD: inattention, hyperactivity, impulsivity.
- Rule out behaviors linked to other disorders: oppositional defiant disorder involves hostility and deliberate provocation.
- Distinguish environmental behaviors (gaming) from diagnostic features.
- Focus on neurodevelopmental basis: ADHD arises from catecholamine dysregulation in the prefrontal cortex.
- Eliminate distractors by asking: Is this behavior intrinsic to attentional or inhibitory dysfunction?
- Correct answers must align with DSM-5 diagnostic criteria.
- Use elimination: spiteful and deliberately annoying behaviors → ODD; prolonged gaming → lifestyle, not pathology.
- Select impulsivity, excessive talking, and failure to complete tasks as they directly reflect ADHD’s triad of symptoms.
Take home points
- ADHD is defined by inattention, hyperactivity, and impulsivity.
- Oppositional defiant disorder involves deliberate hostility and provocation, not ADHD.
- Environmental behaviors like gaming are not diagnostic criteria.
- Differentiation requires understanding neurodevelopmental versus behavioral pathology.
A nurse assesses a client with the inattentive presentation of attention-deficit/hyperactivity disorder (ADHD). Which behavior is most consistent with this presentation?
Explanation
Attention-deficit/hyperactivity disorder, inattentive presentation, is defined by inattention, poor concentration, impaired working memory, and reduced organization. It is linked to dysfunction in prefrontal cortical circuits regulating dopamine and norepinephrine. Clients show distractibility, forgetfulness, and difficulty sustaining focus, without prominent hyperactivity or impulsivity.
Rationale for correct answer:
1.Difficulty sustaining attention during tasks is the hallmark of inattentive ADHD. Clients struggle with prolonged focus, make careless mistakes, and fail to follow through on instructions. This results from impaired executive functioning and deficient catecholamine signaling. Inattention and distractibilitydefine this subtype.
Rationale for incorrect answers:
2.Frequent physical restlessness is characteristic of hyperactive-impulsive ADHD. It involves fidgeting, inability to remain seated, and excessive motor activity. Inattentive presentation lacks prominent hyperactivity and motor agitation, making this inconsistent with the described subtype.
3.Excessive talking and interrupting others reflect hyperactive-impulsive ADHD. Clients with inattentive presentation do not display verbal overactivity. The pathology involves attentional deficits, not disinhibition or verbal impulsivity, so this is not consistent.
4.Engaging in risk-taking behaviors is linked to impulsivity and poor inhibitory control, typical of hyperactive-impulsive ADHD. Inattentive presentation is defined by distractibility and poor sustained focus, not impulsivity or risk-taking, making this incorrect.
Test-taking strategy
- Identify the presentation subtype: inattentive vs hyperactive-impulsive.
- Recall DSM-5 criteria: inattentive subtype requires ≥6 symptoms of inattention, such as poor focus, forgetfulness, and disorganization.
- Eliminate distractors by matching behaviors to hyperactive-impulsive features (restlessness, excessive talking, risk-taking).
- Focus on neurodevelopmental basis: inattentive ADHD stems from impaired prefrontal cortical regulation of attention, not motor or behavioral disinhibition.
- Correct answer must directly reflect attentional dysfunction, not hyperactivity or impulsivity.
- Use elimination: restlessness, talking, and risk-taking → hyperactive-impulsive; sustained attention difficulty → inattentive subtype.
Take home points
- Inattentive ADHD is defined by distractibility, poor focus, and disorganization.
- Hyperactive-impulsive ADHD involves restlessness, excessive talking, and impulsivity.
- Subtype differentiation is essential for accurate diagnosis and management.
- Neurobiology involves catecholamine dysregulation in prefrontal cortical circuits.
A nurse is assessing a client with the hyperactive-impulsive presentation of attention-deficit/hyperactivity disorder (ADHD). Which finding should the nurse expect?
Explanation
Attention-deficit/hyperactivity disorder, hyperactive-impulsive presentation, is characterized by hyperactivity, impulsivity, poor inhibitory control, and excessive motor activity. It results from dysregulation of catecholamine pathways in the prefrontal cortex and basal ganglia. Clients display restlessness, excessive talking, interrupting, and risk-taking behaviors without predominant inattention.
Rationale for correct answer:
1.Fidgeting and inability to remain seated are classic features of hyperactive-impulsive ADHD. Clients show constant movement, tapping, or squirming due to cortical disinhibition. This reflects impaired inhibitory control and excessive motor drive. Hyperactivityand restlessnessdefine this subtype.
Rationale for incorrect answers:
2.Daydreaming during conversations is typical of inattentive ADHD. It reflects distractibility and poor sustained focus, not hyperactivity. The pathology involves inattentionand cognitive drift, making this inconsistent with hyperactive-impulsive presentation.
3.Slow task completion is linked to inattentive ADHD due to poor organization and distractibility. Hyperactive-impulsive clients act quickly, often without forethought, but do not exhibit prolonged task delays. Disorganizationand inattentionexplain slow completion, not hyperactivity.
4.Avoidance of group activities is more consistent with social anxiety or autism spectrum disorder. Hyperactive-impulsive ADHD clients often seek stimulation and interaction, though disruptive. Social withdrawaland avoidanceare not defining features of this subtype.
Test-taking strategy
- Identify presentation subtype: hyperactive-impulsive vs inattentive.
- Recall DSM-5 criteria: hyperactive-impulsive requires ≥6 symptoms of hyperactivity/impulsivity such as fidgeting, excessive talking, interrupting, and inability to remain seated.
- Eliminate distractors by matching behaviors to inattentive features (daydreaming, slow task completion) or unrelated conditions (avoidance of group activities).
- Focus on motor restlessnessand impulsivityas diagnostic hallmarks.
- Correct answer must directly reflect excessive motor activity and poor inhibitory control.
- Use elimination: daydreaming and slow tasks → inattentive; avoidance → social withdrawal; fidgeting → hyperactive-impulsive.
Take home points
- Hyperactive-impulsive ADHD is defined by restlessness, impulsivity, and excessive motor activity.
- Inattentive ADHD involves distractibility, daydreaming, and poor task completion.
- Social withdrawal is not a feature of ADHD but may suggest other conditions.
- Subtype recognition is essential for accurate diagnosis and tailored interventions.
A nurse is selecting an intervention for a client with attention-deficit/hyperactivity disorder (ADHD). Which activity is most appropriate for a client with ADHD?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmentaldisorder marked by hyperactivity, impulsivity, and inattention. Clients benefit from structured activities with clear rules, short attention demands, and opportunities for physical activity. Such interventions channel excess energy, improve focus, and reduce disruptive behaviors.
Rationale for correct answer:
2.Volleyball is appropriate because it provides structured rules, teamwork, and continuous physical movement. The activity channels hyperactivity into organized play, enhances attention through rapid responses, and promotes social interaction. Structureand movementmake it ideal for ADHD management.
Rationale for incorrect answers:
1.Monopoly requires prolonged attention, strategic planning, and sustained focus, which ADHD clients struggle with. The slow pace and extended cognitive demand exacerbate distractibility. Inattentionand poor concentrationmake this unsuitable.
3.Pool swimming, while physically engaging, lacks the structured group interaction and rapid attention shifts that benefit ADHD clients. It may reduce hyperactivity but does not reinforce social skillsor teamwork, limiting therapeutic value.
4.Checkers demands sustained concentration and patience, which ADHD clients often lack. The sedentary nature fails to channel hyperactivity, and the cognitive load may increase frustration. Distractibilityand restlessnessmake this inappropriate.
Test-taking strategy
- Identify interventions that match ADHD symptomatology: hyperactivity, impulsivity, inattention.
- Apply principles: activities should be structured, short in duration, and involve physical movement.
- Rule out sedentary, prolonged, or cognitively demanding activities (Monopoly, Checkers).
- Consider therapeutic value: group sports enhance socializationand attention regulation.
- Eliminate options that do not address hyperactivity or require sustained focus.
- Select volleyball because it combines structure, movement, and teamwork, aligning with ADHD needs.
Take home points
- ADHD interventions should emphasize structure, movement, and short attention demands.
- Sedentary, prolonged activities worsen distractibility and frustration.
- Group sports enhance social skills and channel hyperactivity positively.
- Differentiating interventions requires matching activity demands to ADHD symptom profile.
A nurse anticipates that a client with attention-deficit/hyperactivity disorder (ADHD) may be learning-disabled. This means the client:
Explanation
Learning disability refers to perceptual difficultiesthat interfere with information processing, despite normal intelligenceand adequate opportunity. It involves dysfunction in brain regions responsible for language, reading, or mathematics. Clients may struggle with decoding, comprehension, or written expression, independent of intellectual impairment.
Rationale for correct answer:
3.Experiences perceptual difficulties that interfere with learning defines a learning disability. Clients have intact intelligence but impaired processing of auditory or visual input. This leads to difficulties in reading, writing, or mathematics. Perceptionand processing deficitsare central features.
Rationale for incorrect answers:
1.Not being self-directed reflects motivational or behavioral issues, not learning disability. Learning disability is neurologically based, involving processing deficits, not lack of initiative or independence.
2.Intellectual impairment is distinct from learning disability. Clients with learning disabilities have normal intelligence but specific deficits in processing. Cognitionand IQremain intact, differentiating it from intellectual disability.
4.Performing two grade levels below age norms may be a consequence of learning disability but is not its definition. The defining feature is impaired information processing, not academic performance alone.
Test-taking strategy
- Focus on the definitionof learning disability: intact intelligence with impaired perceptual processing.
- Rule out distractors that describe intellectual disability (choice 2) or behavioral issues (choice 1).
- Recognize that academic underperformance (choice 4) is a result, not the defining feature.
- Correct answer must directly reflect the neurological basis of learning disability.
- Use elimination: lack of self-direction → behavioral; intellectual impairment → separate disorder; grade-level deficit → consequence, not definition.
- Select perceptual difficulties interfering with learning as the precise definition.
Take home points
- Learning disability involves perceptual and processing deficits, not low intelligence.
- ADHD often coexists with learning disabilities, complicating academic performance.
- Intellectual disability differs by global cognitive impairment, not specific processing deficits.
- Academic underachievement may result from learning disability but is not diagnostic.
Practice Exercise 3
A nurse reviews the criteria for attention-deficit/hyperactivity disorder (ADHD). Which requirement must be met for diagnosis?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmentaldisorder characterized by inattention, hyperactivity, and impulsivity. According to DSM-5-TR, symptoms must be present before age 12, persist for ≥6 months, and cause impairment in multiple settings such as home, school, or work. Functional impairmentacross contexts is essential for diagnosis.
Rationale for correct answer:
1.Symptoms must be present in two or more settings is a DSM-5-TR requirement. ADHD must cause impairment in at least two domains (e.g., school and home) to confirm pervasive dysfunction. Cross-situationaland functional impairmentvalidate the diagnosis.
Rationale for incorrect answers:
2.Symptoms resolving with behavioral therapy alone is not a diagnostic requirement. ADHD often requires multimodal treatment including pharmacotherapy. Persistenceand neurobiologydefine the disorder, not treatment response.
3.Symptoms accompanied by psychosis are not part of ADHD criteria. Psychosis indicates a separate psychiatric disorder. ADHD involves attention deficitsand impulsivity, not hallucinations or delusions.
4.Symptoms beginning after school enrollment contradict DSM-5-TR. ADHD must present before age 12. Onset after school entry suggests other conditions. Early onsetand developmental trajectoryare required.
Test-taking strategy
- Recall DSM-5-TR diagnostic criteria: onset before age 12, persistence ≥6 months, impairment in ≥2 settings.
- Eliminate distractors: treatment response is not diagnostic, psychosis is unrelated, and onset after school enrollment is too late.
- Focus on cross-situational impairmentas the defining requirement.
- Correct answer must align with DSM-5-TR standards, not treatment outcomes or unrelated psychiatric features.
- Use elimination: therapy response → management, not diagnosis; psychosis → separate disorder; late onset → inconsistent.
Take home points
- ADHD requires symptoms in ≥2 settings for diagnosis.
- Onset must occur before age 12.
- Psychosis is not part of ADHD diagnostic criteria.
- Treatment response does not define diagnosis; persistence and impairment do.
A nurse uses assessment scales when evaluating a client for attention-deficit/hyperactivity disorder (ADHD). Which tool is commonly used to support diagnosis?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmentaldisorder characterized by persistent inattention, hyperactivity, and impulsivitybeginning before age 12. It involves dysfunction of dopaminergicand noradrenergic pathways, with genetic predisposition and environmental triggers. Symptoms include distractibility, poor task completion, fidgeting, and impulsive behaviors. ADHD is associated with academic underachievement, social impairment, and increased risk of comorbid psychiatric disorders.
Rationale for correct answer:
1.The Vanderbilt Assessment Scale is specifically designed to evaluate ADHD symptoms in children. It assesses both inattentionand hyperactivity, with teacher and parent input. It also screens for comorbidities such as oppositional defiant disorder and conduct disorder, making it clinically appropriate for diagnostic support.
Rationale for incorrect answers:
2.The Mini-Mental State Examination evaluatescognitionin adults, focusing on orientation, memory, and language. It is used for dementia and delirium screening, not ADHD. Its structure lacks sensitivity for attentional deficits in pediatric populations, making it unsuitable for ADHD diagnosis.
3.The Beck Depression Inventory measuresdepressivesymptomsincluding mood, guilt, and suicidal ideation. It is validated for major depressive disorder but does not assess hyperactivity or impulsivity. ADHD requires evaluation of attentional and behavioral domains, which this tool does not address.
4.The Glasgow Coma Scale assesses consciousness in acute neurological injury, measuring eye, verbal, and motor responses. It is used in trauma and critical care settings. ADHD is a chronic neurodevelopmental disorder, not an acute alteration of consciousness, so this scale is irrelevant.
Test-taking strategy
- Identify the main conditionin the stem: ADHD.
- Recall that ADHD requires specialized behavioral assessment tools.
- Rule out tools unrelated to ADHD:
- MMSE is for dementia.
- Beck Depression Inventory is for depression.
- Glasgow Coma Scale is for consciousness.
- Focus on the tool that specifically evaluates inattentionand hyperactivityin children.
- Use elimination methodology:
- Remove tools assessing cognition, mood, or consciousness.
- Retain the one validated for ADHD diagnosis.
- Correct answer emerges by matching the tool to the disorder’s core symptoms.
Take home points
- ADHD is a neurodevelopmental disorder with onset before age 12.
- Vanderbilt Assessment Scale is validated for ADHD diagnosis in children.
- MMSE, Beck Depression Inventory, and Glasgow Coma Scale assess other conditions.
- Differentiating ADHD from mood disorders and cognitive impairment is essential.
A nurse is differentiating combined presentation attention-deficit/hyperactivity disorder (ADHD) from other conditions. Which feature supports a combined presentation?
Explanation
Attention-deficit/hyperactivity disorder combined presentation involves both inattentionand hyperactivity-impulsivitypersisting ≥6 months, with onset before age 12, across ≥2 settings. Dysfunction in dopamineand norepinephrinepathways underlies impaired executive function, manifesting as distractibility, fidgeting, poor sustained attention, and impulsive behaviors.
Rationale for correct answer:
1.Combined presentation requires ≥6 months of both inattentionand hyperactivitysymptoms, present in multiple environments. This aligns with DSM-5 criteria, confirming diagnosis. The persistence and dual symptom clusters distinguish combined ADHD from inattentive or hyperactive-impulsive types.
Rationale for incorrect answers:
2.Symptoms limited to the classroom indicate situational behavioralissues, not ADHD. ADHD requires impairment in ≥2 settings (home, school, social). Restriction to one environment excludes diagnosis of combined presentation.
3.Onset after age 12 contradicts DSM-5 criteria. ADHD must begin before age 12. Later onset suggests other psychiatricor cognitive disorders, not combined ADHD.
4.Hallucinations and delusions are features of psychosis, not ADHD. ADHD involves attentional and behavioral dysregulation, not perceptual disturbances. Psychotic symptoms indicate schizophrenia or mood disorders with psychotic features.
Test-taking strategy
- Identify the main condition: ADHD combined presentation.
- Recall DSM-5 diagnostic criteria: onset before 12, symptoms ≥6 months, impairment in ≥2 settings.
- Rule out distractors:
- Classroom-only symptoms = situational.
- Onset after 12 = not ADHD.
- Hallucinations = psychosis.
- Focus on the option describing both inattentionand hyperactivitypersisting ≥6 months.
- Use elimination methodology: remove answers inconsistent with ADHD diagnostic framework.
- Correct answer emerges by matching DSM-5 criteria to combined presentation.
Take home points
- Combined ADHD requires both inattention and hyperactivity symptoms ≥6 months.
- Symptoms must occur in ≥2 settings, not restricted to one.
- Onset must be before age 12 for ADHD diagnosis.
- Psychotic features differentiate schizophrenia from ADHD.
A nurse differentiates attention-deficit/hyperactivity disorder (ADHD) from anxiety disorders. Which finding is more consistent with ADHD?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmentaldisorder characterized by persistent inattention, hyperactivity, and impulsivityacross multiple settings, with onset before age 12. Dysfunction in dopamineand norepinephrine pathways impairs executive function, leading to distractibility, poor sustained attention, fidgeting, and impulsive behaviors. ADHD differs from anxiety disorders, which are marked by excessive worry, fear, and autonomic hyperarousal.
Rationale for correct answer:
1.ADHD presents with persistent difficulty sustainingattentionacross settings such as home, school, and social environments. This impairment is not situational but pervasive. The presence of both attentional deficits and behavioral dysregulation supports ADHD rather than anxiety disorders.
Rationale for incorrect answers:
2.Excessive worry about future events is characteristic of generalized anxiety disorder. It reflects cognitive preoccupation with potential threats, not attentional deficits. ADHD involves distractibility and impulsivity, not chronic worry.
3.Fear of social situations indicates socialanxiety disorder. It involves avoidance due to fear of embarrassment or scrutiny. ADHD does not primarily manifest as social fear but as inattentive and hyperactive behaviors.
4.Avoidance of school due to panic reflects panicdisorderor school refusal linked to anxiety. ADHD does not cause panic attacks or avoidance behaviors; instead, it causes poor task completion and impulsivity across settings.
Test-taking strategy
- Identify the main condition: ADHD versus anxiety disorders.
- Recall ADHD diagnostic criteria: inattention, hyperactivity, impulsivity, onset before 12, symptoms ≥6 months, impairment in ≥2 settings.
- Rule out distractors:
- Excessive worry = generalized anxiety.
- Social fear = social anxiety.
- School avoidance due to panic = panic disorder.
- Focus on the option describing attention deficitsacross multiple environments.
- Use elimination methodology: remove answers linked to anxiety-specific features.
- Correct answer emerges by matching ADHD’s hallmark symptom of persistent inattentionacross settings.
Take home points
- ADHD involves persistent inattention and hyperactivity across ≥2 settings.
- Anxiety disorders are defined by excessive worry, fear, or panic.
- ADHD onset is before age 12, anxiety may occur later.
- Differentiating ADHD from anxiety requires focus on attentional versus emotional symptoms.
Practice Exercise 4
A nurse is caring for a 9-year-old client with attention-deficit/hyperactivity disorder. Which medication is most frequently prescribed for ADHD?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmentaldisorder treated primarily with stimulantmedications that enhance dopamineand norepinephrinetransmission in the prefrontal cortex, improving attention and impulse control. Methylphenidate is the most frequently prescribed stimulant for children, with proven efficacy in reducing hyperactivity and improving focus.
Rationale for correct answer:
3.Methylphenidate (Ritalin) is the first-line stimulant for ADHD. It increases synaptic dopamine and norepinephrine, improving attention span and reducing impulsivity. It is widely prescribed in pediatric ADHD due to strong evidence of efficacy and safety.
Rationale for incorrect answers:
1.Lorazepam (Ativan) is a benzodiazepineused for anxiety and acute agitation. It enhances GABA activity, causing sedation. It does not improve attention or hyperactivity, making it inappropriate for ADHD management.
2.Haloperidol (Haldol) is a typical antipsychoticused for schizophrenia and severe agitation. It blocks dopamine receptors, which may worsen attentional deficits. It is not indicated for ADHD and carries risk of extrapyramidal side effects.
4.Methocarbamol (Robaxin) is a muscle relaxantused for musculoskeletal pain. It acts centrally to reduce muscle spasms but has no role in ADHD treatment. It does not affect attention or impulsivity.
Test-taking strategy
- Identify the main condition: ADHD in a pediatric client.
- Recall first-line pharmacologic treatment: stimulants(methylphenidate, amphetamines).
- Rule out distractors:
- Benzodiazepines treat anxiety, not ADHD.
- Antipsychotics treat psychosis, not ADHD.
- Muscle relaxants treat musculoskeletal pain, not ADHD.
- Focus on the option that directly improves dopamineand norepinephrinesignaling in the prefrontal cortex.
- Use elimination methodology: remove drugs unrelated to attentional regulation.
- Correct answer emerges by matching stimulant therapy to ADHD pathophysiology.
Take home points
- Methylphenidate is the most frequently prescribed stimulant for ADHD in children.
- ADHD treatment targets dopamine and norepinephrine pathways to improve attention.
- Benzodiazepines, antipsychotics, and muscle relaxants are not indicated for ADHD.
- Differentiating ADHD pharmacotherapy from other psychiatric and neurologic drugs is essential.
A nurse is caring for a client with attention-deficit/hyperactivity disorder (ADHD) who is prescribed methylphenidate (Ritalin). Which symptoms should the nurse monitor as potential side effects? Select all that apply
Explanation
Methylphenidate is a stimulantmedication that enhances dopamineand norepinephrineactivity in the prefrontal cortex, improving attention and impulse control. Common adverse effects include insomnia, decreased appetite, headache, abdominal pain, and potential risk of seizures. Cardiovascular effects usually involve mild hypertension or tachycardia, not hypotension.
Rationale for correct answers:
2.Decreased appetite is a frequent side effect due to stimulant-induced suppression ofdopaminergicpathwaysregulating hunger. This can lead to weight loss in children, requiring monitoring of growth and nutritional intake.
4.Insomnia occurs because stimulantsincrease CNS activity. Evening dosing exacerbates sleep disturbance. Nurses should advise morning administration and monitor sleep hygiene to reduce impact on rest.
5.Headache is a common adverse effect linked to stimulant-induced changes inneurotransmitterbalance. It is usually mild but can interfere with adherence, requiring symptomatic management.
6.Seizures are a rare but serious adverse effect. Stimulants lower the seizure threshold, especially in clients with preexisting epilepsy. Monitoring neurological status is essential to detect early warning signs.
Rationale for incorrect answers:
1.Hypotension is not typical of methylphenidate. Stimulants usually cause hypertension or tachycardia due to sympathetic activation. Monitoring blood pressure is important, but hypotension is not expected.
3.Sedation is inconsistent with stimulant pharmacology. Methylphenidate increases alertness and activity, not drowsiness. Sedationwould suggest another drug effector comorbidity, not methylphenidate.
Test-taking strategy
- Identify the main drug: methylphenidate, a stimulant.
- Recall stimulant side effects: insomnia, appetite suppression, headache, abdominal pain, possible seizures.
- Rule out distractors:
- Hypotension is not expected; stimulants raise blood pressure.
- Sedation contradicts stimulant pharmacology.
- Focus on adverse effects consistent with CNS stimulationand appetite suppression.
- Use elimination methodology: remove options inconsistent with stimulant effects.
- Correct answers emerge by matching stimulant pharmacodynamics to expected clinical manifestations.
Take home points
- Methylphenidate commonly causes decreased appetite, insomnia, and headache.
- Seizures are rare but serious adverse effects requiring monitoring.
- Hypotension and sedation are not expected with stimulant therapy.
- Nurses must monitor growth, sleep, and neurological status in children on methylphenidate.
A nurse is caring for a 10-year-old client prescribed dextroamphetamine (Dexedrine) who has a nursing diagnosis of imbalanced nutrition: less than body requirements related to anorexia. Which nursing intervention addresses this problem?
Explanation
Dextroamphetamine is a stimulantthat enhances dopamineand norepinephrineactivity, improving attention and impulse control in ADHD. However, it frequently causes anorexiaand weight loss due to appetite suppression. Administering the drug after meals helps reduce nutritional impact by allowing adequate intake before appetite suppression begins.
Rationale for correct answer:
3.Administering dextroamphetamine after meals minimizesanorexiaby ensuring the child eats before appetite suppression occurs. This intervention directly addresses imbalanced nutrition and supports growth and weight maintenance in pediatric ADHD clients.
Rationale for incorrect answers:
1.Monitoring output and sleep patterns daily is important for stimulant therapy but does not directly addressnutrition. It helps detect insomnia or urinary changes, yet it fails to correct anorexia-related weight loss.
2.Administering medication with food prevents nausea, not anorexia. Stimulants primarily suppress appetite rather than cause gastrointestinal upset. This intervention does not resolve the nutritional deficit associated with dextroamphetamine.
4.Increasing fiber and fluid intake prevents constipation, a possible side effect of stimulants. While beneficial, it does not address anorexia or weight loss, which are the primary nutritional concerns in this scenario.
Test-taking strategy
- Identify the main issue: imbalanced nutrition due to anorexia from stimulant therapy.
- Recall stimulant side effects: appetite suppression, insomnia, headache, abdominal pain.
- Rule out distractors:
- Monitoring sleep/output = general care, not nutrition.
- With food = prevents nausea, not anorexia.
- Fiber/fluid = prevents constipation, not anorexia.
- Focus on the intervention that directly improves nutritional intake.
- Correct answer emerges by matching anorexia management with timing of medication administration.
Take home points
- Stimulants like dextroamphetamine suppress appetite, leading to anorexia and weight loss.
- Administering medication after meals helps preserve nutritional intake.
- Other interventions address side effects but not anorexia.
- Nurses must monitor growth and weight in children on stimulant therapy.
A nurse educates parents about non-stimulant medications used to treat attention-deficit/hyperactivity disorder (ADHD). Which medication is a non-stimulant option?
Explanation
Non-stimulant therapy for ADHD includes atomoxetine, a selective norepinephrinereuptake inhibitor. Unlike stimulants, it does not directly increase dopamine release but modulates norepinephrine transmission, improving attention and impulse control. Atomoxetine is useful in patients with contraindications to stimulants, comorbid anxiety, or risk of substance misuse.
Rationale for correct answer:
1.Atomoxetine (Strattera) is a non-stimulant norepinephrinereuptake inhibitor approved for ADHD. It improves attentional control without the abuse potential of stimulants. It is particularly beneficial in children with comorbid anxiety or those intolerant to stimulant side effects.
Rationale for incorrect answers:
2.Methylphenidate (Ritalin) is a stimulantthat blocks dopamine and norepinephrine reuptake. It is first-line therapy for ADHD but not classified as non-stimulant.
3.Dextroamphetamine (Dexedrine) is a stimulantthat increases dopamine and norepinephrine release. It is effective for ADHD but carries abuse potential, making it unsuitable as a non-stimulant option.
4.Lisdexamfetamine (Vyvanse) is a stimulantprodrug of dextroamphetamine. It is long-acting and effective for ADHD but remains a stimulant, not a non-stimulant medication.
Test-taking strategy
- Identify the main concept: non-stimulant ADHD medication.
- Recall that stimulants (methylphenidate, amphetamines) are first-line but not non-stimulant.
- Rule out distractors:
- Methylphenidate = stimulant.
- Dextroamphetamine = stimulant.
- Lisdexamfetamine = stimulant.
- Focus on the option that is FDA-approved as a non-stimulant.
- Correct answer emerges by matching atomoxetine to non-stimulant pharmacology.
Take home points
- Atomoxetine is the primary non-stimulant approved for ADHD.
- Stimulants include methylphenidate, dextroamphetamine, and lisdexamfetamine.
- Atomoxetine is preferred in patients with anxiety or substance misuse risk.
- Differentiating stimulant from non-stimulant therapy is essential in ADHD management.
A nurse monitors a client prescribed atomoxetine for attention-deficit/hyperactivity disorder (ADHD). Which adverse effect should the nurse assess for?
Explanation
Atomoxetine is a non-stimulantselective norepinephrinereuptake inhibitor used in ADHD management. Unlike stimulants, it lacks abuse potential but carries risk of liverinjury. Clinicians must monitor hepatic function, as atomoxetine can cause elevated transaminases, jaundice, and rare cases of hepatic failure.
Rationale for correct answer:
1.Atomoxetine may causeliver dysfunction, including hepatotoxicity with elevated ALT/AST and jaundice. Monitoring liver enzymes and clinical signs such as dark urine or right upper quadrant pain is essential to detect early hepatic injury.
Rationale for incorrect answers:
2.Severe hypoglycemia is not associated with atomoxetine. Hypoglycemia is linked toinsulinor oral hypoglycemics, not norepinephrine reuptake inhibition. Atomoxetine does not alter glucose metabolism significantly.
3.Respiratory depression is a risk with opioidsor sedatives, not atomoxetine. Atomoxetine does not depress respiratory drive, as it lacks GABAergic or opioid receptor activity.
4.Constipation is not a major adverse effect of atomoxetine. While mild gastrointestinalupset may occur, constipation is not a clinically significant or frequent finding compared to hepatic risk.
Test-taking strategy
- Identify the main drug: atomoxetine, a non-stimulant norepinephrine reuptake inhibitor.
- Recall its unique adverse effect profile: liver dysfunctionis the most clinically significant.
- Rule out distractors:
- Hypoglycemia = insulin-related.
- Respiratory depression = opioids/sedatives.
- Constipation = not common with atomoxetine.
- Focus on the adverse effect requiring routine monitoring.
- Correct answer emerges by matching atomoxetine’s pharmacology to its known hepatotoxic risk.
Take home points
- Atomoxetine is a non-stimulant ADHD medication acting via norepinephrine reuptake inhibition.
- Liver dysfunction is the most important adverse effect requiring monitoring.
- Hypoglycemia and respiratory depression are unrelated to atomoxetine.
- Differentiating stimulant versus non-stimulant adverse effects is essential in ADHD pharmacology.
Practice Exercise 5
A nurse is evaluating the effectiveness of parental teaching for a 10-year-old client diagnosed with attention-deficit/hyperactivity disorder (ADHD). Which parental statement indicates that further teaching is needed?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with functioning. Pathophysiology involves dysregulation of dopamine, norepinephrine, and prefrontal cortexcircuits. Symptoms include distractibility, poor organization, fidgeting, and impulsive actions. Diagnosis requires ≥6 symptoms persisting ≥6 months. Management includes behavioral therapy, structured routines, and pharmacologic agents such as stimulants.
Rationale for correct answer:
1.Restricting sugar and food-coloring additives is not evidence-basedin ADHD management. Scientific studies show no consistent link between dietary sugar or artificial coloring and hyperactivity. The parental statement reflects a misconception, requiring further teaching. The correct approach emphasizes behavioral interventionsand pharmacologic therapy.
Rationale for incorrect answers:
2.Behavioral contracts are effective in ADHD because they provide structured reinforcement and accountability. They help children with poor organizational skills by linking specific behaviors to rewards. This aligns with evidence-basedbehavioral modificationstrategies.
3.Goal charts with star rewards are appropriate positive reinforcement techniques. They enhance motivation and track progress, supporting executive function deficits in ADHD. This structured system is consistent with recommended behavioral therapyinterventions for pediatric ADHD.
4.Setting limits and encouraging recreational activities are valid strategies. Clear boundaries reduce impulsivity, while physical activity channels hyperactivity constructively. These interventions are consistent with non-pharmacologic management and improve behavioral regulationand social functioningin affected children.
Test-taking strategy
To answer this question, the nurse must differentiate between evidence-based interventions and misconceptions. The strategy involves:
- Identifying scientifically supported interventionssuch as behavioral contracts, reward charts, and structured recreational activities.
- Recognizing that dietary restrictionsinvolving sugar and food coloring lack empirical support in ADHD management.
- Applying elimination methodology: rule out options that align with behavioral therapy principles, leaving the one based on outdated or unsupported beliefs.
- Using clinical reasoning: ADHD requires structured behavioral interventions and pharmacologic therapy, not dietary elimination.
- Focus on patient education: nurses must correct misconceptions and reinforce evidence-based strategies to ensure effective parental teaching.
This systematic approach ensures accurate identification of the statement needing further teaching.
Take home points
• ADHD is a neurodevelopmental disorder involving dopamine and norepinephrine dysregulation.
• Evidence-based management includes behavioral therapy, structured routines, and stimulant medications.
• Dietary sugar and food-coloring restrictions are not scientifically supported interventions.
• Differentiation from conditions like oppositional defiant disorder and anxiety disorders is essential in clinical practice.
A nurse is counseling the parent of a client with attention-deficit/hyperactivity disorder (ADHD). The parent demonstrates understanding of the teaching when stating:
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder marked by impaired executive function, poor attention regulation, excessive hyperactivity, and impulsivity. Pathophysiology involves altered catecholamine signaling in the prefrontal cortex. Children struggle with organization, task completion, and sustaining focus. Evidence-based management includes structured routines, behavioral therapy, and stimulant medications.
Rationale for correct answer:
1.Completing homework immediately after school reflects structured routineand prioritization of tasks before distractions. This approach supports executive function deficits, enhances consistency, and reduces procrastination. It aligns with evidence-based behavioral strategies for ADHD, emphasizingstructureand consistencyin daily activities.
Rationale for incorrect answers:
2.Taking the child to play in the park first delays academic tasks, increasing risk of distraction and poor task completion. While physical activity is beneficial, it should follow structured responsibilities. Lack of immediatetask focusundermineseffective ADHD management.
3.Allowing television after school promotes passive activity and distractibility. Screen time exacerbates attention difficulties and delays homework completion. This approach fails to reinforce structured routines and does not addressexecutive dysfunctioninherent in ADHD.
4.Reading a favorite book after school encourages leisure before responsibilities. Although reading is constructive, prioritizing non-academic activities over homework undermines structured task completion. ADHD management requires consistentroutine adherenceand reinforcement of responsibility before recreation.
Test-taking strategy
To answer this question, the nurse must identify the parental statement that reflects evidence-based ADHD management. The strategy involves:
- Recognizing that structure and routineare essential for children with ADHD.
- Applying elimination methodology: rule out options that prioritize recreation or passive activities before responsibilities.
- Identifying the statement that emphasizes task completion first, which directly supports executive function deficits.
- Using clinical reasoning: ADHD requires reinforcement of responsibility before leisure to prevent distraction and incomplete tasks.
- Focusing on behavioral interventions: structured routines, prioritization, and consistency are the foundation of non-pharmacologic ADHD management.
This systematic approach ensures the correct identification of the parental statement demonstrating understanding.
Take home points
• ADHD requires structured routines to compensate for executive dysfunction.
• Homework and responsibilities should be prioritized before recreational activities.
• Passive activities like television worsen distractibility and delay task completion.
• Differentiation from learning disorders is essential, as ADHD primarily affects attention and impulse control.
A nurse is developing a care plan for a client with attention-deficit/hyperactivity disorder (ADHD) who is at high risk for self-harm due to impulsivity and poor judgment. Which intervention is the priority?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder characterized by impaired impulse control, poor judgment, excessive hyperactivity, and deficits in executive function. These impairments increase risk for self-harm behaviors, particularly when impulsivity overrides safety awareness. Clinical management requires prioritizing immediate safety through close observation, followed by behavioral interventions and pharmacologic therapy.
Rationale for correct answer:
3.One-to-one close observation is the priority intervention for a client at high risk of self-harm. Continuous monitoring ensures immediate safety, prevents impulsive acts, and allows rapid intervention. This approach directly addresses impulsivityand risk reduction, which are critical in acute care planning.
Rationale for incorrect answers:
1.Daily sessions to explore stressors provide therapeutic support but do not ensure immediate safety. Exploration of stressors is a long-term intervention, not suitable as the priority when acute riskof self-harm is present.
2.A no self-harm contract and unit activities promote accountability and engagement but lack immediate protective measures. Contracts are not reliable for impulsive clients, as judgment deficitslimit adherence. Safety requires direct observation, not verbal agreements.
4.Hospital-issued clothing and staff view increase visibility but do not guarantee continuous monitoring. Clients may still engage in impulsive self-harm behaviors when not directly observed. This intervention is supportive but insufficient compared to constant observation.
Test-taking strategy
To answer this question, apply prioritization principles:
- Use ABCs and safety first: immediate risk of self-harm requires direct protective measures.
- Apply Maslow’s Hierarchy of Needs: physiological safety precedes psychological exploration.
- Eliminate options that provide long-term support but fail to address acute risk.
- Identify interventions that directly mitigate impulsivity and poor judgment, which are core ADHD risks.
- Select the option that ensures continuous monitoring, as this is the most effective method to prevent harm in high-risk clients.
This systematic approach ensures the correct prioritization of interventions in acute psychiatric care.
Take home points
• ADHD increases self-harm risk due to impulsivity and poor judgment.
• Priority intervention in acute risk is continuous one-to-one observation.
• Contracts and therapy sessions are supportive but not sufficient for immediate safety.
• Differentiation from mood disorders is essential, as impulsivity in ADHD requires distinct safety planning.
A nurse is providing discharge instructions to parents of a child with attention-deficit/hyperactivity disorder (ADHD). Which management strategy should be included?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired attention, poor impulse control, excessive hyperactivity, and deficits in executive function. Pathophysiology includes altered catecholamine signaling in the prefrontal cortex. Children often struggle with organization, task completion, and emotional regulation. Evidence-based management emphasizes structured routines, behavioral therapy, and pharmacologic agents such as stimulants.
Rationale for correct answer:
2.Rewarding appropriate behavior is a cornerstone of behavioral therapy in ADHD. Positive reinforcement strengthens desired behaviors, improves compliance, and enhances self-esteem. This strategy directly addresses impulsivityand supports behavioral modification, making it an essential discharge teaching point for parents.
Rationale for incorrect answers:
1.Orienting the client to reality is appropriate for psychotic disorders but not ADHD. ADHD is not characterized by hallucinations or delusions. The focusshould be onbehavioral reinforcement, not reality orientation.
3.Suppressing frustration expressions is counterproductive. Emotional regulation is impaired in ADHD, and suppression increases stress and behavioral outbursts. Effective management involves teaching coping strategies and encouraging healthy emotional expression, not suppression.
4.Physical restraints during loss of control are inappropriateand potentially harmful. Restraints increase trauma risk and do not address impulsivity. ADHD management emphasizes positive reinforcement and structured routines, not coercive measures.
Test-taking strategy
To answer this question, apply principles of evidence-based ADHD management:
- Identify interventions that emphasize positive reinforcementand structured behavioral therapy.
- Eliminate options that apply to other psychiatric conditions (e.g., reality orientation for psychosis).
- Rule out harmful or non-therapeutic strategies such as restraintsor emotional suppression.
- Focus on interventions that enhance self-regulationand promote adaptive behaviors.
- Select the option that aligns with discharge teaching goals: empowering parents to use reinforcement strategies at home.
This systematic approach ensures accurate identification of the correct management strategy.
Take home points
• ADHD requires behavioral therapy emphasizing positive reinforcement.
• Reality orientation is not relevant, as ADHD does not involve psychosis.
• Emotional suppression worsens behavioral outcomes; coping strategies are preferred.
• Physical restraints are contraindicated; structured routines and reinforcement are safer and effective.
A nurse is developing a behavioral plan for a client with attention-deficit/hyperactivity disorder (ADHD). Which strategy is most effective for encouraging a new desired behavior?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder characterized by impaired attention, poor impulse control, excessive hyperactivity, and deficits in executive function. Children with ADHD struggle to sustain focus, complete tasks, and regulate behavior. Evidence-based management emphasizes structured routines, positive reinforcement, and pharmacologic therapy. Immediate reinforcement is most effective because delayed rewards fail to sustain motivation in children with impaired executive functioning.
Rationale for correct answer:
2.Immediate verbal praise and tangible rewards after task completion directlyreinforce desired behavior.Children with ADHD respond best to positive reinforcementdelivered promptly, as delayed rewards lose effectiveness due to impaired attention span and poor impulse regulation.
Rationale for incorrect answers:
1.Weekly rewards are too delayed for childrenwith ADHD. Executive dysfunction prevents sustained motivation over long intervals. Reinforcement must be immediate to strengthen behavior consistently and effectively. Lack of timely feedback reduces behavioral improvement.
3.Threatening to remove privileges relies on punishmentrather than reinforcement. Punitive strategies increase frustration and resistance, failing to promote adaptive behavior. ADHD management emphasizes positive reinforcement, not negative consequences, to encourage compliance and task completion.
4.Ignoring behavior until improvement occurs is ineffective. ADHD requiresstructured interventions and immediate reinforcement. Passive approaches fail to address impulsivity and poor self-regulation, allowing maladaptive behaviors to persist without correction or guidance.
Test-taking strategy
To answer this question, apply behavioral principles:
- Identify interventions that emphasize positive reinforcementrather than punishment or passive approaches.
- Eliminate options that rely on delayed rewards, as ADHD requires immediate feedback.
- Rule out punitive strategies, which worsen frustration and do not build adaptive behaviors.
- Recognize that ignoring behavior is ineffective in ADHD due to persistent impulsivity and poor self-regulation.
- Select the option that provides immediate reinforcement, which is scientifically proven to be the most effective strategy for encouraging new behaviors in ADHD.
This systematic approach ensures accurate identification of the most effective behavioral plan.
Take home points
• ADHD requires immediate reinforcement to strengthen desired behaviors.
• Delayed rewards are ineffective due to impaired executive function.
• Punitive strategies worsen frustration and do not promote adaptive behavior.
• Ignoring maladaptive behavior fails to address impulsivity and poor regulation.
Comprehensive Questions
A nurse is performing a health history on a client who is being evaluated for attention-deficit/hyperactivity disorder (ADHD). Regarding the likelihood of management with psychostimulant medications, which area is critical to document in the review of systems?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder characterized by impaired dopaminergicand noradrenergicneurotransmission, leading to inattention, hyperactivity, and impulsivity. Psychostimulants such as methylphenidate and amphetamines increase synaptic dopamine and norepinephrine. These agents can cause tachyarrhythmias, hypertension, and sudden cardiac events, making cardiovascular screening essential before initiation. Baseline blood pressure, heart rate, and history of structural heart disease must be documented. Electrocardiogram is recommended in patients with known cardiac pathology. Contraindications include structural cardiac abnormalities, cardiomyopathy, and serious arrhythmias.
Rationale for correct answer:
4.Psychostimulants elevate catecholamine activity, increasing myocardial oxygen demand and risk of arrhythmia. Documenting cardiovascularhistory ensures safe prescribing. Hypertension, congenital heart disease, or prior myocardial infarction are critical contraindications. The question stem emphasizes stimulant use, making cardiovascular assessment the most relevant system to review.
Rationale for incorrect answers:
1.Musculoskeletal history is not directly relevantto stimulant safety. Stimulants do not exacerbate arthritis, fractures, or muscular disorders. While musculoskeletal complaints may affect functioning, they do not contraindicate stimulant therapy. The absenceof cardiovascularriskmakes this option incorrect.
2.Genitourinary history is not critical for stimulant prescribing. Stimulants do not cause renal impairment or urinary retention. Although dehydration may worsen urinary symptoms, stimulant pharmacodynamics are unrelated to genitourinary pathology. Thus, documenting this system does not influence stimulant safety or efficacy.
3.Immunization history is unrelated to stimulant therapy. Vaccination status does not alter pharmacokineticsor pharmacodynamicsof psychostimulants. While immunization is important for general health, it does not determine stimulant eligibility or contraindications. Therefore, this option is not relevant to stimulant prescribing.
Test-taking strategy
- Focus on the main idea: psychostimulant medications for ADHD.
- Identify the system most affected by stimulant side effects.
- Rule out distractors:
- Musculoskeletal: unrelated to stimulant safety.
- Genitourinary: no pharmacologic link.
- Immunization: irrelevant to drug metabolism.
- Apply risk reduction principles: prioritize systems where adverse drug effects can be life-threatening. Cardiovascular complications such as arrhythmia or hypertension are serious risks.
- Use elimination method: only cardiovascular history directly impacts stimulant prescribing.
- Remember: in pharmacology questions, always connect drug mechanism of action to organ system risk. Stimulants increase catecholamines, stressing the heart.
- Therefore, cardiovascular history is the critical documentation area.
Take home points
- ADHD management with stimulants requires cardiovascular risk assessment.
- Psychostimulants increase catecholamine activity, predisposing to arrhythmias and hypertension.
- Musculoskeletal, genitourinary, and immunization histories do not influence stimulant safety.
- Always differentiate ADHD stimulant contraindications from unrelated systemic histories.
A client diagnosed with bipolar disorder also has attention-deficit/hyperactivity disorder (ADHD). How are these comorbid conditions most appropriately treated?
Explanation
Bipolar disorder is a chronic mood disorder characterized by recurrent episodes of mania, hypomania, and depression, with pathophysiology involving dysregulation of dopamine, serotonin, and glutamate. ADHD is a neurodevelopmental disorder with impaired dopaminergic and noradrenergic signaling. When comorbid, stimulant therapy for ADHD can precipitate manic episodes if bipolar disorder is not stabilized. Mood stabilization with lithium, valproate, or atypical antipsychotics must precede stimulant initiation to prevent destabilization.
Rationale for correct answer:
3.Stabilizing bipolar disorder first prevents stimulant-induced mania. Mood stabilizers such as lithium or valproate reduce risk of destabilization. Only after stabilization can ADHD be safely treated with stimulants or non-stimulants. This sequence ensures safe and effective management of both conditions.
Rationale for incorrect answers:
1.Withholding all medication ignores evidence-based treatment. Untreated bipolar disorder leads to recurrent mania and depression, while untreated ADHD impairs functioning. Pharmacologic therapy is essential for both conditions, making this option clinically inappropriate.
2.Simultaneous treatment risks stimulant-inducedmaniabefore mood stabilization. Administering stimulants without prior stabilization can exacerbate bipolar symptoms, leading to rapid cycling or hospitalization. This approach disregards the need for sequential management.
4.Treating ADHD first with stimulants destabilizes bipolar disorder. Stimulants increase dopaminergic activity, precipitating manic episodes. Without prior stabilization, this approach worsenspsychiatric morbidityand is contraindicated in comorbid presentations.
Test-taking strategy
- Identify the main idea: comorbid bipolar disorder and ADHD.
- Recall that stimulants can precipitate mania in unstable bipolar disorder.
- Apply risk reduction principles: stabilize life-threatening or destabilizing conditions first.
- Rule out distractors:
- No medication: inappropriate, both conditions require treatment.
- Simultaneous treatment: unsafe, risks mania.
- ADHD first: contraindicated, stimulant-induced mania risk.
- Correct approach: stabilize bipolar disorder first, then treat ADHD.
- Use sequential management principle: mood stabilization precedes stimulant therapy.
- This ensures safety and efficacy in comorbid psychiatric conditions.
Take home points
- Bipolar disorder must be stabilized before ADHD treatment.
- Stimulants can precipitate mania if bipolar disorder is untreated.
- Mood stabilizers such as lithium or valproate are first-line in bipolar disorder.
- Sequential management prevents destabilization and optimizes outcomes in comorbid presentations.
A client with attention-deficit/hyperactivity disorder (ADHD) and juvenile diabetes is prescribed methylphenidate (Ritalin). Which nursing intervention related to both diagnoses is the priority?
Explanation
Methylphenidate is a central nervous system stimulant that enhances dopaminergicand noradrenergictransmission, improving attention and reducing hyperactivity. In clients with juvenile diabetes, stimulants can increase glucoselevels due to catecholamine-mediated glycogenolysis and gluconeogenesis. Monitoring fasting blood glucose is critical to prevent hyperglycemiaand diabetic complications.
Rationale for correct answer:
3.Stimulants elevate catecholamineactivity, increasing hepatic glucose output and impairing glycemic control. Regular monitoring of fasting glucoseensures early detection of hyperglycemia. This intervention directly addresses the interaction between ADHD pharmacotherapy and juvenile diabetes management.
Rationale for incorrect answers:
1.Morning administration reducesinsomnia, but this is a general ADHD management principle. It does not address the metabolic risks posed by methylphenidate in a diabetic client, making it less critical compared to glucose monitoring.
2.Restlessnessand dry mouthare common stimulantside effects, but they are not life-threatening. While important to report, these do not pose the same immediate risk as uncontrolled hyperglycemia in a client with juvenile diabetes.
4.Reinforcing adherence ensures therapeutic efficacy, but it does not specifically addressthe metabolic riskin diabetes. Without glucose monitoring, strict adherence could still result in hyperglycemia complications, making this option less urgent than blood glucose surveillance.
Test-taking strategy
- Identify the main idea: ADHD treatment with methylphenidate in a client with juvenile diabetes.
- Apply risk reduction principles: prioritize interventions that prevent life-threatening complications.
- Rule out distractors:
- Morning dosing: addresses insomnia, not diabetes.
- Side effect reporting: important but not critical.
- Adherence: general principle, not diabetes-specific.
- Focus on the comorbidity: stimulant-induced hyperglycemia risk in diabetes.
- Correct intervention: monitoring fasting blood glucose to prevent acute and chronic complications.
- Use elimination method: only option 3 directly addresses both ADHD treatment and diabetes management.
Take home points
- Methylphenidate can increase blood glucose via catecholamine effects.
- Juvenile diabetes requires strict monitoring of fasting glucose when stimulants are prescribed.
- ADHD side effects like insomnia and restlessness are secondary concerns compared to metabolic risks.
- Priority nursing intervention is glucose monitoring to prevent hyperglycemia complications.
A parent insists on medication for a client with suspected attention-deficit/hyperactivity disorder (ADHD). What is the nurse’s best response?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired dopaminergicand noradrenergicsignaling, manifesting as inattention, hyperactivity, and impulsivity. Management requires comprehensive assessment, including behavioral interventions and pharmacotherapy. Parents often experience significant stress managing symptoms. The nurse’s role includes providing empathy, validating concerns, and fostering therapeutic alliance before discussing treatment options. Establishing rapport ensures effective collaboration in care planning.
Rationale for correct answer:
1.Expressing empathy validatesparental frustrationand builds trust. This response acknowledges the difficulty of managing ADHD behaviors without judgment. Establishing rapport is essential before discussing pharmacologic or non-pharmacologic interventions, making this the best therapeutic communication choice.
Rationale for incorrect answers:
2.Asking about alternatives prematurely shifts focusaway from parental concerns. While nonpharmacologic strategies are important, this response lacks empathy and may appear dismissive, weakening therapeutic communication and rapport.
3.Suggesting the parent seeks an “easy solution” isjudgmentaland undermines trust. This response conveys criticism rather than support, which is inappropriate in therapeutic communication and may damage the nurse-parent relationship.
4.Explaining medicationside effectsis educational but not the priority. Without first validating parental feelings, this response risks appearing dismissive. Effective communication begins with empathy before providing information.
Test-taking strategy
- Identify the main idea: therapeutic communication in ADHD management.
- Apply principles: empathy and validation precede education or problem-solving.
- Rule out distractors:
- Alternatives: premature, lacks empathy.
- Easy solution: judgmental, non-therapeutic.
- Side effects: informative but not empathetic.
- Correct choice: empathetic statement that validates parental frustration.
- Use Maslow’s hierarchy: address emotional needs (trust, support) before cognitive needs (information).
- Apply therapeutic communication principle: empathy first, education second.
Take home points
- ADHD management requires empathy toward parental stress.
- Therapeutic communication begins with validating feelings before education.
- Judgmental or dismissive responses undermine rapport.
- Empathy builds trust and facilitates collaborative care planning.
A nurse evaluates long-term outcomes for a client with attention-deficit/hyperactivity disorder (ADHD). Which factor is associated with improved prognosis?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired dopaminergicand noradrenergicsignaling, manifesting as inattention, impulsivity, and hyperactivity. Long-term prognosis improves with early diagnosisand consistent treatment, which include stimulant or non-stimulant medications, behavioral interventions, and educational support. Early intervention reduces academic failure, social impairment, and psychiatric comorbidities, while delayed or punitive approaches worsen outcomes.
Rationale for correct answer:
1.Early diagnosisand consistent treatment allow timely initiationof pharmacologic and behavioral interventions. This reduces symptom severity, improves academic performance, and lowers risk of comorbid mood or conduct disorders. Prognosis is significantly better with early, structured management.
Rationale for incorrect answers:
2.Delayed interventionuntil adulthood prolongs impairment, increasing risk of academic failure, substance use, and psychiatric comorbidities. Late treatment reduces effectiveness and worsens long-term outcomes.
3.Absence of educational support exacerbates academic difficulties. ADHD clients require structured accommodations such as extended test time and behavioral reinforcement. Without support, prognosis worsens due to persistent academic and social challenges.
4.Reliance on punishment increases frustrationand impulsivity. Punitive strategies do not teach adaptive behaviors and worsen emotional regulation, leading to poor long-term outcomes.
Test-taking strategy
- Identify the main idea: factors improving ADHD prognosis.
- Apply risk reduction principles: interventions must reduce long-term impairment.
- Rule out distractors:
- Delayed intervention: worsens prognosis.
- No educational support: increases academic failure.
- Punishment: ineffective, worsens symptoms.
- Correct choice: early diagnosis and consistent treatment, which directly improve functioning and reduce comorbidities.
- Use developmental principle: early intervention yields better outcomes in neurodevelopmental disorders.
Take home points
- Early diagnosis and consistent treatment improve ADHD prognosis.
- Delayed intervention increases risk of academic and psychiatric complications.
- Educational support is essential for long-term functioning.
Punishment-based discipline worsens impulsivity and emotional regulation.
A nurse promotes quality of life for a client with attention-deficit/hyperactivity disorder (ADHD). Which intervention best supports community integration?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired dopaminergicand noradrenergicsignaling, leading to inattention, impulsivity, and hyperactivity. Promoting quality of life requires interventions that enhance social skills, community participation, and structured engagement. Encouraging participation in structured extracurricular activities provides opportunities for peer interaction, skill development, and positive reinforcement, supporting long-term integration and psychosocial functioning.
Rationale for correct answer:
1.Structured extracurricular activities foster peer relationships, improve social skills, and provide consistent routines. These activities enhancecommunity integrationby promoting inclusion, reducing isolation, and reinforcing adaptive behaviors in a supportive environment.
Rationale for incorrect answers:
2.Limiting social interaction to family restricts opportunities for peer learningand community engagement. ADHD clients benefit from broader social exposure, making this option counterproductive.
3.Avoiding peer relationships worsens social isolationand impairs development of interpersonal skills. ADHD management emphasizes structured peer interaction, not avoidance.
4.Discouraging independent decision-making undermines autonomyand adaptive functioning.Adolescents and adults with ADHD require support in developing independence, not restriction, making this option inappropriate.
Test-taking strategy
- Identify the main idea: promoting quality of life and community integration in ADHD.
- Apply psychosocial principles: inclusion, structured engagement, skill development.
- Rule out distractors:
- Family-only interaction: limits integration.
- Avoiding peers: increases isolation.
- Discouraging independence: reduces autonomy.
- Correct choice: structured extracurricular activities, which balance routine with social engagement.
- Use risk reduction principle: interventions must enhance functioning, not restrict growth.
Take home points
- Structured extracurricular activities support social skills and community integration in ADHD.
- Limiting social interaction impairs development and increases isolation.
- Peer relationships are essential for psychosocial growth.
- Independence and autonomy must be encouraged for long-term quality of life.
A nurse provides discharge teaching to parents of a client with attention-deficit/hyperactivity disorder (ADHD). Which instruction is most important to include?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired dopaminergicand noradrenergicsignaling, leading to inattention, impulsivity, and hyperactivity. Long-term management requires multidisciplinary collaboration, including healthcare providers, school staff, and family. Consistent follow-up ensures monitoring of medication effects, behavioral progress, and academic functioning. Discontinuing medication prematurely, avoiding therapy, or restricting activity worsens outcomes.
Rationale for correct answer:
1.Maintaining consistent follow-up with healthcare and school providers ensures ongoing monitoring of treatment efficacy, side effects, and academic performance. This collaborative approach supports optimal functioning and long-term stability in ADHD management.
Rationale for incorrect answers:
2.Discontinuing medication once symptoms improve risks relapse. ADHD requires long-term management, and premature cessation undermines therapeutic progress and symptom control.
3.Avoiding behavioral therapy eliminates a critical component of ADHD management. Behavioral interventions complement pharmacotherapy, improving attention, impulse control, and social functioning.
4.Restricting physical activity is inappropriate. Structured activity improves focus, reduces hyperactivity, and supports overall health. Limiting activity worsens restlessness and impairs psychosocial development.
Test-taking strategy
- Identify the main idea: discharge teaching for ADHD management.
- Apply risk reduction principles: prioritize interventions that ensure continuity of care.
- Rule out distractors:
- Discontinuing medication: unsafe, risks relapse.
- Avoiding therapy: removes essential intervention.
- Restricting activity: counterproductive, worsens symptoms.
- Correct choice: consistent follow-up with healthcare and school providers, ensuring multidisciplinary support.
- Use elimination method: only option 1 promotes safe, comprehensive long-term management.
Take home points
- ADHD requires consistent follow-up with healthcare and school providers.
- Premature discontinuation of medication risks symptom recurrence.
- Behavioral therapy is essential alongside pharmacologic treatment.
- Structured physical activity supports focus and overall health in ADHD.
A nurse provides teaching about stimulant medications prescribed for attention-deficit/hyperactivity disorder (ADHD). Which medication belongs to this class?
Explanation
Stimulant medications are the first-line pharmacologic treatment for attention-deficit/hyperactivity disorder, acting primarily by increasing dopamineand norepinephrineavailability in the prefrontal cortex. This enhances executive functioning, attention, and impulse control. Methylphenidateis the prototypical stimulant, widely used in pediatric and adult ADHD. It can cause insomnia, appetite suppression, and cardiovascular effects such as tachycardia and hypertension. Contraindications include structural cardiac abnormalities and severe anxiety disorders.
Rationale for correct answer:
1.Methylphenidateis a central nervous system (CNS) stimulantthat increases catecholamine activity, improving attention and reducing hyperactivity. It is FDA-approved for ADHD and represents the primary pharmacologic class used in management. Its mechanism directly addresses the neurochemical deficits in ADHD.
Rationale for incorrect answers:
2.Fluoxetine is a selective serotonin reuptake inhibitorused for depression and anxiety disorders. It does not enhance dopaminergic or noradrenergic transmission and is not indicated for ADHD treatment, making it inappropriate in this context.
3.Risperidone is an atypical antipsychoticused for schizophrenia, bipolar disorder, and irritability in autism. It acts on dopamine and serotonin receptors but does not improve ADHD core symptoms. It is not classified as a stimulant medication.
4.Valproic acid is an anticonvulsant and mood stabilizerused in epilepsy and bipolar disorder. It modulates GABA activity but has no role in ADHD treatment. It is not a stimulant and does not address ADHD pathophysiology.
Test-taking strategy
- Identify the main idea: stimulant medications for ADHD.
- Recall pharmacologic classes: stimulants (methylphenidate, amphetamines) are first-line.
- Rule out distractors:
- SSRIs (fluoxetine): depression, not ADHD.
- Antipsychotics (risperidone): psychosis, not ADHD.
- Anticonvulsants (valproic acid): seizures, not ADHD.
- Apply elimination method: only methylphenidate belongs to stimulant class.
- Use drug classification principle: match mechanism of action to ADHD neurobiology.
- Correct choice: methylphenidate, the prototypical stimulant for ADHD.
Take home points
- Methylphenidate is the prototypical stimulant used in ADHD.
- Stimulants act by increasing dopamine and norepinephrine in the prefrontal cortex.
- SSRIs, antipsychotics, and anticonvulsants are not indicated for ADHD.
- ADHD pharmacotherapy requires careful monitoring for cardiovascular and psychiatric side effects.
A nurse monitors a client receiving stimulant therapy for attention-deficit/hyperactivity disorder (ADHD). Which findings should the nurse report? Select all that apply
Explanation
Attention-deficit/hyperactivity disorder is managed with stimulantmedications such as methylphenidate and amphetamines, which increase dopamineand norepinephrineactivity in the central nervous system. These agents improve attention and impulse control but can cause adverse effects including weight loss, insomnia, and tachycardiadue to appetite suppression, CNS stimulation, and catecholamine-mediated cardiovascular effects. Monitoring and reporting these findings is essential to prevent complications.
Rationale for correct answers:
1.Stimulants suppress appetite, leading to weight loss. Persistent weight reduction can impair growth in children and nutritional status, requiring monitoring and possible dose adjustment. This adverse effect must be reported promptly.
2.CNS stimulation often causesinsomnia, especially if medication is taken late in the day. Sleep disturbance can worsen ADHD symptoms and overall functioning, making this a reportable adverse effect.
4.Increased catecholamineactivity can cause tachycardiaand elevated blood pressure. Cardiovascular monitoring is critical, as stimulants may precipitate arrhythmias or exacerbate underlying cardiac disease. This finding must be reported immediately.
Rationale for incorrect answers:
3.Stimulants do not cause increased appetite; instead, they suppress appetite. Reporting increased appetite would be irrelevant, as it is not a typical adverse effect of stimulant therapy.
5.Improved concentrationis a desired therapeutic effect of stimulant therapy. It indicates medication efficacy, not an adverse effect. This finding should be documented as a positive outcome, not reported as a problem.
Test-taking strategy
- Identify the main idea: adverse effects of stimulant therapy in ADHD.
- Recall common stimulant side effects: appetite suppression, insomnia, cardiovascular stimulation.
- Rule out distractors:
- Increased appetite: opposite of expected effect.
- Improved concentration: therapeutic outcome, not adverse.
- Apply risk reduction principles: report findings that can impair growth, sleep, or cardiovascular stability.
- Correct answers are those representing adverse effects requiring monitoring and intervention: weight loss, insomnia, tachycardia.
Take home points
- Stimulants commonly cause weight loss, insomnia, and tachycardia.
- Appetite suppression is a hallmark adverse effect, not increased appetite.
- Improved concentration is a therapeutic goal, not a complication.
- Nurses must monitor growth, sleep, and cardiovascular status in clients receiving stimulant therapy.
A nurse plans behavioral interventions for a client with attention-deficit/hyperactivity disorder (ADHD). Which approach is most effective?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder characterized by impaired dopaminergicand noradrenergicsignaling, resulting in inattention, impulsivity, and hyperactivity. Behavioral interventions are essential alongside pharmacotherapy. The most effective approach is positive reinforcement, which strengthens adaptive behaviors by rewarding desired actions immediately and consistently. This method enhances motivation, improves compliance, and reduces disruptive behaviors. Punishment or ignoring behaviors is less effective and may worsen symptoms.
Rationale for correct answer:
1.Immediate and consistentpositive reinforcementstrengthens desired behaviors in ADHD. Rewarding adaptive actions increases dopamine release, enhancing motivation and attention. This approach is evidence-based and improves long-term behavioral outcomes, making it the most effective intervention.
Rationale for incorrect answers:
2.Ignoring both positive and negative behaviors fails to reinforce adaptive actions. Without reinforcement, children with ADHD lack motivation to sustain attention or control impulses, leading to persistence of maladaptive behaviors.
3.Applying punishment after repeated behaviors may suppress actions temporarily but does not teach adaptive alternatives. Punishment increases frustration and can worsen impulsivity, making it ineffective as a primary intervention.
4.Allowing unrestricted activity choices exacerbates hyperactivityand distractibility. ADHD clients require structured environments with clear expectations. Unrestricted activity undermines behavioral control and worsens symptoms.
Test-taking strategy
- Identify the main idea: behavioral interventions for ADHD.
- Recall evidence-based practice: reinforcement is more effective than punishment or ignoring.
- Rule out distractors:
- Ignoring: no reinforcement, ineffective.
- Punishment: increases frustration, not therapeutic.
- Unrestricted activity: worsens hyperactivity.
- Apply behavioral psychology principle: reinforcement strengthens desired behaviors.
- Correct choice: immediate and consistent positive reinforcement.
Take home points
- ADHD behavioral management relies on positive reinforcement.
- Punishment is less effective and may worsen impulsivity.
- Ignoring behaviors fails to promote adaptive functioning.
- Structured reinforcement strategies improve compliance and symptom control.
A nurse teaches parents strategies for homework completion in a client with attention-deficit/hyperactivity disorder (ADHD). Which recommendation is most appropriate?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder marked by impaired dopaminergicand noradrenergicsignaling, resulting in inattention, impulsivity, and hyperactivity. Effective behavioral strategies must accommodate limited attention span and need for structure. Breaking tasks into short, manageablesegments reduces cognitive overload, enhances focus, and improves task completion. Structured reinforcement and scheduled breaks further optimize performance.
Rationale for correct answer:
1.Dividing tasks into short, manageablesegments aligns with the limited attentioncapacity in ADHD. This method reduces frustration, enhances focus, and promotes successful completion of assignments. It is evidence-based and widely recommended in pediatric ADHD management.
Rationale for incorrect answers:
2.Completing homework late at night worsensinsomniaand reduces attention. ADHD clients benefit from structured routines and early task completion. Nighttime study increases fatigue and impairs learning, making this approach inappropriate.
3.Eliminating all breaks increases restlessnessand reduces productivity. ADHD clients require short, scheduled breaks to sustain attention. Continuous study without breaks leads to frustration and poor task performance.
4.Assigning multiple tasks simultaneously overwhelmsworking memoryand exacerbates distractibility. ADHD clients require sequential tasking with clear instructions. Multitasking worsens inattention and reduces overall productivity, making this option ineffective.
Test-taking strategy
- Identify the main idea: strategies for homework completion in ADHD.
- Recall ADHD characteristics: short attention span, distractibility, need for structure.
- Rule out distractors:
- Late-night study: worsens sleep and attention.
- No breaks: increases restlessness.
- Multiple tasks: overwhelms working memory.
- Apply behavioral psychology principle: breaking tasks into smaller segments improves compliance and reduces frustration.
- Correct choice: short, manageable segments tailored to ADHD cognitive limitations.
Take home points
- ADHD clients benefit from structured, short tasks with reinforcement.
- Breaks are necessary to sustain attention and reduce restlessness.
- Multitasking worsens distractibility and impairs performance.
- Early, structured routines optimize homework completion in ADHD.
A nurse collaborates with school staff to support a client with attention-deficit/hyperactivity disorder (ADHD). Which accommodation is most appropriate?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired dopaminergicand noradrenergicsignaling, leading to inattention, impulsivity, and hyperactivity. School accommodations must support academic performance, reduce frustration, and promote engagement. Extended time for tests allows students to compensate for distractibility and slower task completion without lowering expectations. This intervention supports learning while maintaining academic standards.
Rationale for correct answer:
1.Providing extended timefor tests accommodates attention deficitsand reduces performance anxiety. It allows students to demonstrate knowledge without being penalized for slower processing. This evidence-based intervention promotes academic successwhile maintaining expectations.
Rationale for incorrect answers:
2.Removal from all group activities isolates the student sociallyand undermines peer interaction. ADHD management emphasizes inclusion and structured participation, not exclusion. This option worsens social development and is inappropriate.
3.Permanent classroom isolation stigmatizes the studentand impairs social learning. ADHD requires structured support, not segregation. Isolation exacerbates behavioral issues and reduces engagement, making this option harmful.
4.Elimination of academic expectations denies the student educational opportunities. ADHD accommodations should support learning, not remove standards. Lowering expectations undermines achievement and self-esteem, making this option inappropriate.
Test-taking strategy
- Identify the main idea: school accommodations for ADHD.
- Apply risk reduction principles: interventions must support learning without stigmatization.
- Rule out distractors:
- Removal from group activities: socially harmful.
- Isolation: stigmatizing.
- Elimination of expectations: denies education.
- Correct choice: extended time for tests, which supports academic performance while maintaining standards.
- Use educational psychology principle: accommodations should enhance success without lowering expectations.
Take home points
- Extended time for tests is an effective ADHD school accommodation.
- Isolation or removal from group activities worsens social development.
- Eliminating academic expectations undermines achievement and self-esteem.
- ADHD accommodations must balance support with maintaining educational standards.
A nurse evaluates parent training effectiveness for a client with attention-deficit/hyperactivity disorder (ADHD). Which statement indicates understanding?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired dopaminergicand noradrenergicsignaling, leading to inattention, impulsivity, and hyperactivity. Behavioral management emphasizes structured routines, clear expectations, and positive reinforcement. Immediate rewards strengthen adaptive behaviors by enhancing motivation and sustaining attention. Punishment or passive waiting is ineffective and may worsen symptoms.
Rationale for correct answer:
1.Immediate positive reinforcementstrengthens desired behaviorsby increasing dopamine release, improving motivation and compliance. This evidence-based approach is the cornerstone of ADHD behavioral management and reflects effective parent training.
Rationale for incorrect answers:
2.Consistent punishment suppresses behavior temporarily but does not teach adaptive alternatives.It increases frustration and impulsivity, making it ineffective as a primary intervention in ADHD.
3.Avoiding clear rules creates inconsistencyand worsens distractibility. ADHD clients require structured expectations to reduce impulsivity and enhance functioning. Lack of rules undermines behavioral control.
4.Waiting for behaviors to improve on their own ignores the need forintervention. ADHD symptoms persist without structured management, and passive approaches delay progress and worsen outcomes.
Test-taking strategy
- Identify the main idea: evaluating parent training effectiveness in ADHD.
- Recall evidence-based practice: reinforcement is more effective than punishment or passive approaches.
- Rule out distractors:
- Punishment: ineffective, increases frustration.
- No rules: worsens distractibility.
- Waiting: passive, delays improvement.
- Apply behavioral psychology principle: immediate reinforcement strengthens adaptive behaviors.
- Correct choice: rewarding positive behaviors immediately.
Take home points
- ADHD behavioral management relies on immediate positive reinforcement.
- Punishment does not teach adaptive behaviors and worsens impulsivity.
- Clear rules and structured routines are essential for ADHD management.
- Passive approaches fail; active reinforcement strategies improve outcomes.
A nurse teaches parents psychosocial interventions for attention-deficit/hyperactivity disorder (ADHD). Which strategies are appropriate? Select all that apply
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired dopaminergicand noradrenergicsignaling, leading to inattention, impulsivity, and hyperactivity. Psychosocial interventions focus on structured environments, consistent reinforcement, and clear communication. Effective strategies include predictable routines, behavioral charts, and concise instructions, which reduce distractibility and improve compliance. Unlimited screen time and ignoring unsafe behaviors worsen symptoms and increase risk.
Rationale for correct answers:
1.Establishing predictable routines provides structure and reduces impulsivity. Consistent schedules enhance attention and minimize behavioral disruptions, making this an effective psychosocial intervention.
2.Using behavioral charts reinforces positive behaviorsthrough visual trackingand rewards. This strategy strengthens adaptive actions and improves compliance in children with ADHD.
4.Providing clear instructions reduces confusionand distractibility. Concise communication enhances understanding and supports task completion, directly addressing ADHD-related deficits in attention.
Rationale for incorrect answers:
3.Allowing unlimited screen time increases overstimulationand worsens distractibility. Excessive screen exposure is linked to poor sleep and impaired attention, making this strategy inappropriate.
5.Ignoring unsafe behaviors places the childat risk of harm. Safety concerns must always be addressed directly. Therapeutic interventions cannot neglect dangerous actions, making this option unacceptable.
Test-taking strategy
- Identify the main idea: psychosocial interventions for ADHD.
- Recall evidence-based strategies: structure, reinforcement, clear communication.
- Rule out distractors:
- Unlimited screen time: worsens symptoms.
- Ignoring unsafe behaviors: violates safety principles.
- Apply risk reduction principles: prioritize interventions that enhance safety and functioning.
- Correct answers are those that provide structure, reinforcement, and clarity.
Take home points
- ADHD management benefits from predictable routines and structured environments.
- Behavioral charts reinforce positive actions through visual and reward systems.
- Clear, concise instructions reduce distractibility and improve compliance.
- Unlimited screen time and ignoring unsafe behaviors worsen ADHD outcomes and compromise safety.
A nurse assists with transition planning for an adolescent with attention-deficit/hyperactivity disorder (ADHD). Which focus is most important?
Explanation
Attention-deficit/hyperactivity disorder is a neurodevelopmental disorder involving impaired dopaminergicand noradrenergicsignaling, resulting in inattention, impulsivity, and hyperactivity. Transition planning for adolescents requires emphasis on self-management, organizational skills, and independenceto prepare for adult responsibilities. These skills improve academic performance, vocational readiness, and psychosocial functioning. Medication decisions, parental involvement, and academic challenges must be addressed, but the priority is equipping the adolescent with lifelong adaptive strategies.
Rationale for correct answer:
1.Developing self-managementand organizational skillsis criticalforsuccessful transition into adulthood. These skills enhance independence, improve academic and vocational outcomes, and reduce reliance on external supports. This focus directly addresses ADHD-related deficits and ensures long-term functioning.
Rationale for incorrect answers:
2.Eliminating all medication use disregards evidence-based treatment. Many adolescents continue to benefit from stimulants or non-stimulants into adulthood. Medication decisions should be individualized, not universally discontinued.
3.Reducing parental involvement completely is inappropriate. Gradual transition toward independence is necessary, but ongoing support remains important. Abrupt withdrawalof parental guidance mayworsen functioning.
4.Avoiding future academic challenges undermines growthand achievement. Transition planning should encourage skill development and resilience, not avoidance. Shielding adolescents from challenges prevents adaptive coping and success.
Test-taking strategy
- Identify the main idea: transition planning for adolescents with ADHD.
- Apply Maslow’s hierarchyand developmental principles: focus on independence and skill acquisition.
- Rule out distractors:
- Eliminating medication: unsafe, not evidence-based.
- Reducing parental involvement: inappropriate, requires gradual transition.
- Avoiding challenges: counterproductive, prevents growth.
- Correct choice: developing self-management and organizational skills, which directly address ADHD deficits and prepare for adulthood.
Take home points
- Transition planning in ADHD emphasizes self-management and organizational skills.
- Medication should not be eliminated universally; decisions must be individualized.
- Parental involvement should taper gradually, not abruptly.
- Adolescents must be encouraged to face academic challenges with structured support.
Exams on ATTENTION-DEFICIT/HYPERACTIVITY DISORDER (ADHD)
Custom Exams
Login to Create a Quiz
Click here to loginLessons
- Objectives
- Introduction
- Etiology And Pathophysiology Of Adhd
- Practice Exercise 1
- Clinical Manifestations And Diagnostic Criteria
- Practice Excercise 2
- Diagnostic Evaluation And Differential Diagnosis
- Practice Exercise 3
- Pharmacological Interventions
- Practice Exercise 4
- Nursing Management And Psychosocial Interventions
- Practice Exercise 5
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Analyze the complex interplay of genetic, neurobiological, and environmental factors in the etiology of Attention-Deficit/Hyperactivity Disorder to understand its chronic nature.
- Evaluate the specific neuroanatomical structures and neurotransmitter pathways, specifically dopamine and norepinephrine, involved in the pathophysiology of executive dysfunction.
- Assess the impact of prenatal, perinatal, and environmental risk factors on the developing neonatal brain and their subsequent contribution to ADHD symptoms.
- Synthesize the relationship between hereditary transmission and clinical presentation to facilitate accurate family history taking during nursing assessments.
- Formulate a foundational scientific understanding of ADHD to provide high-level patient education regarding the biological basis of the disorder, reducing stigma for the patient and family.
- Distinguish between the behavioral manifestations of ADHD and other neurodevelopmental or psychiatric mimics to ensure diagnostic accuracy.
- Compare the mechanisms of action between various pharmacological classes to anticipate potential side effects and therapeutic outcomes.
- Design nursing interventions that utilize environmental modification and behavioral reinforcement to bridge the gap in executive functioning.
- Integrate legal and ethical considerations regarding the administration of controlled substances in the pediatric population.
Introduction
- Attention-Deficit/Hyperactivity Disorder (ADHD) is classified as a persistent, chronic neurodevelopmental disorder.
- The condition is characterized by an age-inappropriate and pervasive pattern of inattention, hyperactivity, and impulsivity.
- Symptoms must result in significant functional impairment across multiple domains, including social, academic, or occupational settings.
- Longitudinal data confirms that ADHD is not exclusively a childhood disorder; it persists into adulthood for approximately 50% to 60% of patients.
- In adults, the presentation often shifts from overt physical hyperactivity to internal restlessness and profound executive dysfunction.
- The disorder is rooted in physiological dysfunction of the prefrontal cortex and associated subcortical structures rather than being a mere "behavioral problem."
- Global prevalence is estimated at 5% to 7% in school-aged children, with a higher diagnostic frequency in males (3:1 ratio).
- Females are frequently underdiagnosed as they often present with predominantly inattentive symptoms rather than disruptive hyperactive behaviors.
- Multimodal management is the gold standard, requiring a combination of pharmacological therapy, behavioral modification, and environmental restructuring.
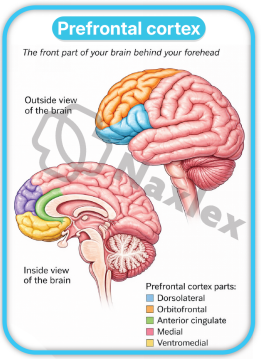
Etiology And Pathophysiology Of Adhd
- The etiology of ADHD is multifactorial, involving a sophisticated interaction between high heritability and environmental "hits" during critical periods of neurodevelopment.
- It is categorized as a neurobiological condition where the brain's "brakes" (inhibitory control) fail to regulate the "accelerator" (impulses and motor activity).
1 Genetic Predisposition and Hereditability
ADHD is among the most heritable psychiatric conditions, often showing strong familial clustering.
- Heritability Coefficients:
- Scientific studies indicate a heritability rate of approximately 75% to 91%.
- This suggests that genetic factors play a predominant role in the manifestation of the disorder compared to environmental factors alone.
- Polygenic Inheritance:
- ADHD is not caused by a single "ADHD gene" but rather by the cumulative effect of multiple risk alleles.
- DRD4 and DRD5 Genes: These genes code for dopamine receptors; variations here are linked to reduced receptor sensitivity in the reward centers of the brain.
- DAT1 (SLC6A3): This gene encodes the dopamine transporter protein, which is responsible for the reuptake of dopamine from the synaptic cleft.
- Familial Risk:
- A child with a parent or sibling diagnosed with ADHD has a 2 to 8 times higher risk of developing the disorder.
- Twin studies show significantly higher concordance rates in monozygotic (identical) twins compared to dizygotic (fraternal) twins.
Nursing Insights
- When conducting a health history, the nurse must meticulously document the psychiatric history of first-degree relatives.
- If a parent exhibits signs of undiagnosed ADHD (e.g., constant interrupting, inability to sit still during the interview, or poor follow-through), the nurse must adapt education materials.
- Education should be concise, written, and delivered in "chunks" as the parent may struggle to process long, complex verbal instructions.
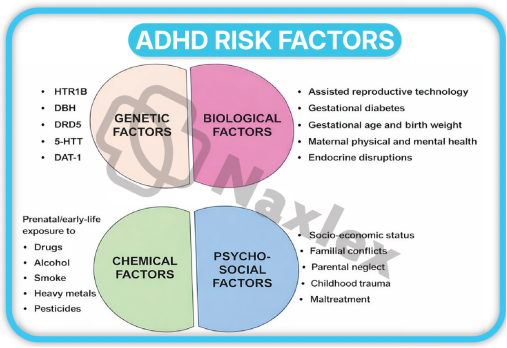
2 Neuroanatomical Disruption and Neurotransmitter Dysregulation
The core of ADHD pathology lies in the structural and functional deficiencies of the circuits connecting the prefrontal cortex to the basal ganglia.
- The Prefrontal Cortex (PFC):
- This area is the "CEO" of the brain, responsible for "Executive Functions."
- Functions include working memory, impulse inhibition, and organization.
- Patients with ADHD often show delayed cortical thickening and reduced metabolic activity in this region.
- The Basal Ganglia and Cerebellum:
- These subcortical structures regulate motor control and timing.
- Reduced volume in the caudate nucleus is frequently observed in neuroimaging, which correlates strongly with hyperactive symptoms.
- The Catecholamine Hypothesis:
- The primary biochemical theory involves a deficit in the transmission of Dopamine and Norepinephrine.
- Dopamine (DA): Essential for reward, motivation, and attention. Low levels in the nucleus accumbens lead to "reward deficiency," where the patient seeks high-stimulation activities to achieve a normal level of arousal.
- Norepinephrine (NE): Crucial for modulating the "signal-to-noise" ratio. Deficient NE prevents the brain from filtering out irrelevant environmental stimuli, leading to distractibility.
- Default Mode Network (DMN) Interference:
- In a healthy brain, the DMN deactivates when a person focuses on a task.
- In ADHD, the DMN stays active, causing internal "mind-wandering" even when the patient is attempting to concentrate on a specific task.
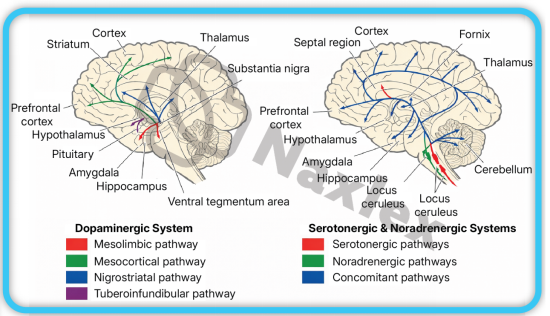
Nursing Insights
- It is vital for the nurse to explain to parents that ADHD is a "performance disorder," not a "knowledge disorder."
- The child often knows what to do but their brain lacks the chemical "bridge" (Dopamine/Norepinephrine) to execute the action in the moment.
- Nurses should advocate for the use of external cues—such as timers, checklists, and visual prompts—to compensate for these internal neurological deficits.
- Recognize that "laziness" is a misnomer; the patient's brain requires a higher threshold of stimulation to engage in mundane tasks.
3 Environmental and Psychosocial Influences
-
While genetics set the stage, environmental "insults" can trigger or exacerbate the severity of ADHD symptoms.
- Prenatal Exposures:
- Maternal Substance Use: Exposure to nicotine, alcohol, or cocaine in utero is strongly correlated with disrupted neurogenesis and subsequent ADHD.
- Maternal Stress: High levels of maternal cortisol during pregnancy can affect fetal brain development, particularly the hypothalamic-pituitary-adrenal (HPA) axis.
- Perinatal and Postnatal Factors:
- Prematurity and Low Birth Weight: Infants born < 32 weeks gestation or < 1500g have a significantly increased risk due to potential hypoxic-ischemic brain injury to the white matter.
- Lead Exposure: Even low levels of lead (Pb) in the blood are neurotoxic and specifically interfere with the development of the prefrontal cortex and synaptic pruning.
- Psychosocial Stressors:
- Severe early deprivation (e.g., institutionalization) can lead to "ADHD-like" symptoms.
- Family discord or low socioeconomic status do not "cause" ADHD in a vacuum but can worsen the clinical trajectory and increase the risk of comorbid conduct disorders.
- Nurses working in community health or pediatric clinics should prioritize screening for environmental toxins like lead.
- Assess the home environment for stability and routine; while chaos doesn't cause ADHD, a structured environment is the primary non-pharmacological treatment.
- Identifying these secondary contributors allows for a more comprehensive treatment plan that addresses the patient's environment alongside their biology.
Clinical Manifestations And Diagnostic Criteria
- The clinical presentation of ADHD is heterogeneous and categorized into three distinct presentations based on the predominance of symptoms over the previous 6 months.
- To meet diagnostic thresholds, symptoms must be present before age 12, occur in two or more settings (e.g., home and school), and clearly interfere with social, academic, or occupational functioning.
1. Inattentive Presentation
This presentation is characterized by a primary failure in the brain's "filtering" system, where the individual cannot prioritize relevant stimuli over irrelevant distractions.
- Diagnostic Requirements:
- For children up to age 16, at least 6 symptoms of inattention must be present.
- For adolescents 17 and older and adults, at least 5 symptoms are required.
- Key Clinical Manifestations:
- Failure to Give Close Attention to Detail: The patient makes "careless" mistakes in schoolwork or professional tasks because the brain does not sustain focus on the minutiae of the assignment.
- Difficulty Sustaining Attention: Inability to remain focused during lengthy lectures, conversations, or long reading assignments.
- Apparent Listening Deficits: The individual often seems "elsewhere" or as if their mind is wandering, even in the absence of obvious external distraction.
- Poor Follow-through: Failure to finish schoolwork, chores, or workplace duties; the patient starts tasks but quickly loses focus and becomes easily sidetracked.
- Executive Dysfunction in Organization: Significant difficulty managing sequential tasks, keeping materials/belongings in order, and poor time management (missing deadlines).
- Avoidance of Mentally Effortful Tasks: A persistent reluctance to engage in tasks that require sustained mental effort (e.g., preparing reports, completing forms, or long-term projects).
- Frequent Loss of Items: Losing essential tools such as school assignments, wallets, keys, eyeglasses, or mobile phones.
- Distractibility: Easily diverted by extraneous stimuli (e.g., a car driving by, a conversation in the hallway).
- Forgetfulness in Daily Activities: Missing appointments, forgetting to return calls, or neglecting daily chores/obligations.
Nursing Insights
- Recognize that Inattentive Presentation is the most common form in females and is frequently misidentified as "daydreaming," "shyness," or "lack of motivation."
- When providing patient education, use the "TEACH-BACK" method to ensure the patient has processed the information, as their internal distractibility may prevent them from encoding the entire conversation.
- Nurses should assess for "masking" in older students, where they expend massive amounts of energy to appear focused, leading to extreme fatigue and burnout after the school day.
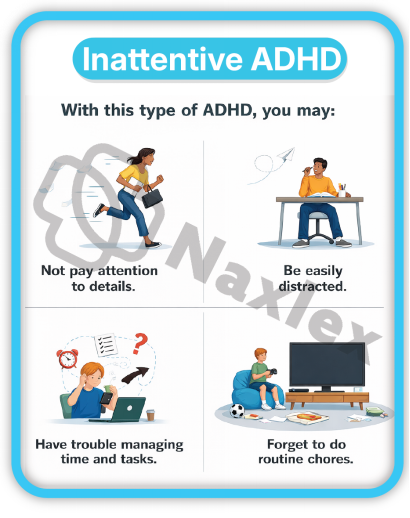
2. Hyperactive-Impulsive Presentation
This presentation involves a lack of behavioral inhibition and "top-down" regulation of motor activity and verbal output.
- Diagnostic Requirements:
- Similar to inattention, 6 or more symptoms are required for children.
- 5 or more for individuals 17 and older.
- Key Clinical Manifestations of Hyperactivity:
- Fidgeting and Squirming: Constant movement of hands or feet; inability to sit still in a chair.
- Inability to Remain Seated: Leaving the seat in situations where remaining seated is expected (e.g., classroom, office, or dinner table).
- Inappropriate Physical Activity: Running or climbing in situations where it is inappropriate (in adolescents or adults, this may manifest as a subjective feeling of "internal restlessness").
- Inability to Play Quietly: Difficulty engaging in leisure activities or hobbies in a calm manner.
- "Driven by a Motor": Appearing to be constantly on the go; the patient is uncomfortable being still for extended periods.
- Excessive Volubility: Talking excessively regardless of social cues or the need for silence.
- Key Clinical Manifestations of Impulsivity:
- Blurting Out Answers: Completing people's sentences or answering before a question has been fully asked.
- Difficulty Waiting Turns: Demonstrating profound impatience in lines or during group games.
- Intrusiveness: Interrupting or intruding on others' conversations, games, or activities; may start using other people's things without asking.
- In the clinical setting, the hyperactive patient is at a higher risk for accidental injury. The nurse must prioritize safety assessments and environment-proofing.
- Impulsivity can lead to "social rejection" by peers. The nurse should assess the patient's self-esteem, as repeated negative feedback from teachers and peers regarding their behavior can lead to comorbid depression or anxiety.
- In adults, physical hyperactivity often transforms into "verbal hyperactivity" or a constant need to be busy, which can be misdiagnosed as mania or high-energy anxiety.
3. Combined Presentation
- Definition: This is the most common clinical presentation. It occurs when the individual meets the diagnostic threshold (6 symptoms for children, 5 for adults) for both Inattention and Hyperactivity-Impulsivity.
- Clinical Profile: These patients represent the "classic" ADHD case. They struggle simultaneously with staying focused and remaining physically still.
- Functional Impact: Because both domains are affected, these individuals often face the highest level of impairment in academic settings and social relationships.
- Developmental Shift: It is common for a child to be diagnosed with Combined Presentation in elementary school, but as they age, the hyperactive symptoms may diminish, leaving them with a predominantly Inattentive Presentation in adulthood.
|
Feature |
Inattentive |
Hyperactive-Impulsive |
Combined |
|
Primary Deficit |
Selective Attention & Working Memory |
Behavioral Inhibition & Motor Control |
Both Cognitive & Motor Regulation |
|
Common Misnomer |
"Spacey" or "Lazy" |
"Disruptive" or "Wild" |
"Difficult" or "Uncontrollable" |
|
Gender Trend |
More common in Females |
More common in Males |
Most common clinical diagnosis |
|
Academic Impact |
Missed instructions, incomplete work |
Classroom disruption, unfinished tests |
Severe global academic impairment |
Nursing Insights
- For the Combined Presentation, the nurse must coordinate a "multimodal" plan. Medication often targets the physiological hyperactivity, but behavioral therapy is necessary to teach the organizational skills missed due to inattention.
- Nurses should monitor for "rebound" symptoms in the late afternoon when medication wears off; the combined symptoms may return with increased intensity, leading to "meltdowns" or high-risk impulsive behaviors during evening hours.
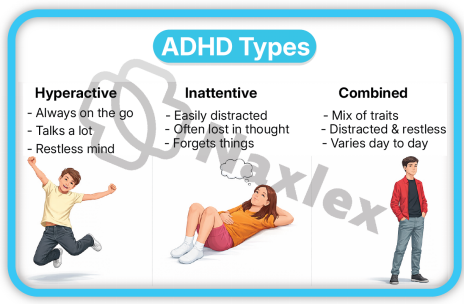
Diagnostic Evaluation And Differential Diagnosis
- The diagnostic process for ADHD is a meticulous clinical synthesis rather than a singular laboratory event.
- Because there is no definitive biological marker, such as a blood test or neuroimaging scan, for a definitive diagnosis, the clinician relies on a comprehensive history, objective data from multiple informants, and the exclusion of other medical and psychiatric conditions.
1. DSM-5-TR Diagnostic Criteria
The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision (DSM-5-TR) establishes the standardized gold standard for diagnosis, emphasizing chronicity, pervasiveness, and impairment.
- Symptom Thresholds and Age Adjustments:
- Pediatric Population (<17 years): Requires the presence of at least 6 symptoms of inattention or 6 symptoms of hyperactivity-impulsivity.
- Adolescent/Adult Population (≥17 years): Requires a minimum of 5 symptoms in either category, acknowledging that hyperactivity often attenuates with age.
- Chronicity Requirements:
- Symptoms must have been persistent for at least 6 months to a degree that is maladaptive and inconsistent with the individual’s developmental level.
- Early Onset:
- Several inattentive or hyperactive-impulsive symptoms must have been present prior to the age of 12 years. This distinguishes ADHD from adult-onset conditions like Generalized Anxiety Disorder (GAD).
- Pervasiveness Across Environments:
- Symptoms must be manifest in two or more settings (e.g., home and school; work and social gatherings).
- If symptoms are localized to only one environment, the nurse must investigate environmental stressors, such as an abusive home or a specific learning disability at school.
- Functional Interference:
- There must be clear evidence that the symptoms interfere with, or reduce the quality of, social, academic, or occupational functioning.
Nursing Insights
- When gathering a history, the nurse should specifically ask parents for "archival data" such as elementary school report cards.
- Common red flags in early records include comments like "talks too much," "does not follow directions," or "frequently loses materials," which provide the objective evidence of symptoms before age 12 required by the DSM-5-TR.
- Nurses must be aware of "masking" in high-IQ patients who may use sheer cognitive effort to compensate for executive deficits until the complexity of higher education or professional life exceeds their coping mechanisms.
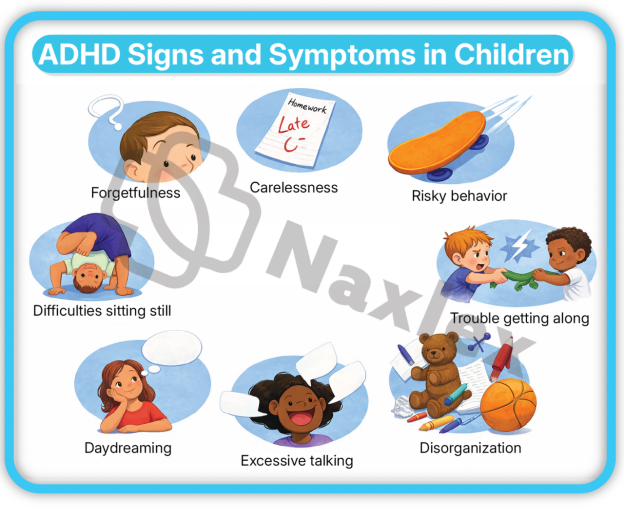
2 Assessment Scales and Clinical Observation
Objective measurement tools are utilized to quantify the severity of behaviors and compare them to age-matched norms.
- Standardized Rating Scales:
- Vanderbilt Assessment Scales: These are the most common primary care tools; they include parent and teacher versions and screen for comorbidities such as Oppositional Defiant Disorder (ODD), Conduct Disorder (CD), and Anxiety/Depression.
- Conners Rating Scales: A highly detailed tool used often in neuropsychological evaluations to assess specific domains like cognitive instability and restlessness.
- Adult ADHD Self-Report Scale (ASRS): A validated 6-item screening tool for adults used to identify the likelihood of adult ADHD.
- Clinical Observation Strategies:
- Clinic Behavior: The nurse should observe the patient's behavior in the waiting room and during the interview. Does the child climb on furniture? Does the adult interrupt the nurse or lose the thread of the conversation?
- The "One-on-One" Effect: Note that children with ADHD often perform well in the novelty of a doctor's office or a one-on-one setting. A lack of symptoms during a 20-minute office visit does not rule out ADHD.
- Neuropsychological and Cognitive Testing:
- Continuous Performance Test (CPT): A computerized task measuring sustained attention and impulsivity (omission and commission errors).
- IQ and Achievement Testing: Vital for identifying a "discrepancy" between a child's potential (IQ) and their actual academic performance.
-
Nursing Insights
- The nurse is the "Coordinator of Information." Ensure that rating scales are collected from all primary environments. If only a parent completes the form, the diagnosis is incomplete.
- Nurses must verify that the teacher completing the form has known the child for at least 2 to 3 months to ensure the observations are representative of the child's baseline.
- Be cautious of "Symptom Over-reporting" by parents seeking a specific diagnosis or "Under-reporting" by teachers who may have a very high tolerance for disruptive behavior.
-
7.3 Differential Diagnosis: Ruling Out Mimics
ADHD symptoms are non-specific; therefore, the nurse must assist the provider in ruling out "The Great Mimics" to avoid misdiagnosis.
- Physiological and Medical Mimics:
- Sleep-Disordered Breathing (SDB): Chronic hypoxia from enlarged tonsils or sleep apnea leads to daytime irritability and "brain fog" that mimics ADHD.
- Absence Seizures (Petit Mal): Brief episodes of staring and unresponsiveness can be mistaken for "inattentive" daydreaming.
- Thyroid Dysfunction: Hyperthyroidism presents with restlessness and tachycardia; Hypothyroidism presents with cognitive sluggishness.
- Iron Deficiency Anemia: Low ferritin levels are associated with restless leg symptoms and decreased cognitive focus.
- Lead Poisoning: Chronic exposure to lead (Pb) is neurotoxic to the prefrontal cortex, causing permanent deficits in impulse control.
- Psychiatric and Psychosocial Mimics:
- Anxiety Disorders: A child who is "worried" may appear inattentive because they are ruminating on fears rather than the teacher's lesson.
- Post-Traumatic Stress Disorder (PTSD): Hypervigilance and a "startle response" can be mistaken for hyperactivity.
- Bipolar Disorder: Mania involves high energy and impulsivity, but unlike the chronic, daily nature of ADHD, Bipolar symptoms occur in distinct, cyclical "episodes."
|
Condition |
Distinguishing Clinical Feature |
|
Learning Disability (LD) |
Struggle is task-specific (e.g., only with reading or math). |
|
Absence Seizures |
Sudden "stare" with lip-smacking or eyelid fluttering; no memory of the gap. |
|
Chronic Sleep Deprivation |
Symptoms resolve entirely when the child gets 10+ hours of sleep. |
|
Fetal Alcohol Syndrome |
Associated with distinct facial dysmorphology and global cognitive delay. |
Nursing Insights
- The Vision and Hearing Rule: No child should be diagnosed with ADHD until the nurse confirms a recent vision and hearing screening. A child who cannot see the board or hear instructions will invariably appear "off-task."
- The Snore Question: Always ask parents, "Does your child snore loudly or gasp for air at night?" If yes, refer to an ENT or Sleep Study before initiating stimulants.
- Trauma Screening: Always assess for "Adverse Childhood Experiences" (ACEs). Toxic stress in the home environment can over-activate the amygdala, leading to a state of constant "Fight or Flight" that perfectly mimics ADHD hyperactivity.
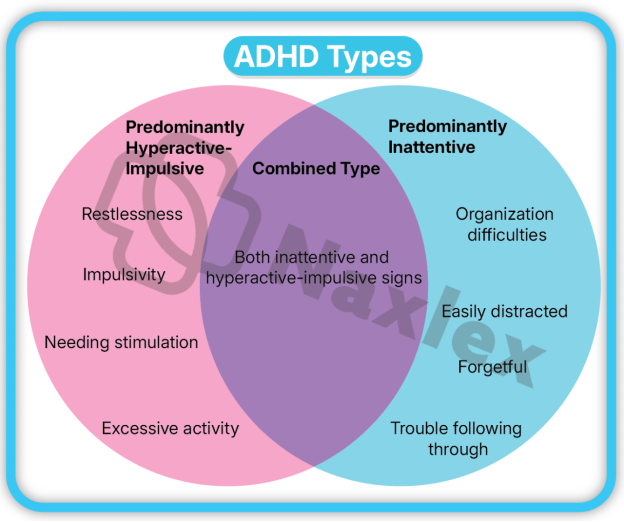
Pharmacological Interventions
- Pharmacotherapy is considered the first-line treatment for moderate to severe ADHD in school-aged children, adolescents, and adults.
- The primary goal of pharmacological intervention is to normalize the catecholaminergic neurotransmission within the prefrontal cortex and basal ganglia to enhance executive function and behavioral inhibition.
1. Stimulant Medications: Methylphenidates and Amphetamines
Stimulants are the most widely researched and frequently prescribed medications for ADHD, demonstrating a high effect size (approximately 1.0) in symptom reduction.
- Mechanism of Action (MOA):
- Methylphenidates: Block the reuptake of Dopamine (DA) and Norepinephrine (NE) by inhibiting the transport proteins (DAT and NET), thereby increasing the concentration of these neurotransmitters in the synaptic cleft.
- Amphetamines: Act as both reuptake inhibitors and "releasers." They enter the presynaptic neuron and induce the release of DA and NE from storage vesicles into the synapse, making them slightly more potent than methylphenidates.
- Classification by Duration:
- Short-Acting (Immediate Release): Effective for 3 to 5 hours (e.g., Ritalin, Focalin, Adderall IR). Requires multiple daily dosing, which can lead to "peaks and valleys" in focus and poor school-day compliance.
- Intermediate-Acting: Effective for 6 to 8 hours (e.g., Ritalin SR, Metadate ER).
- Long-Acting (Extended Release): Effective for 8 to 12+ hours (e.g., Concerta, Adderall XR, Vyvanse). These utilize sophisticated delivery systems like OROS (osmotic release) or prodrug technology to provide a steady therapeutic level.
- Common Compounds:
- Methylphenidate (MPH): Ritalin, Concerta, Daytrana (transdermal patch), Quillivant XR (liquid).
- Amphetamine Salts (AMP): Adderall, Vyvanse (Lisdexamfetamine—a prodrug that must be metabolized in the blood to become active, reducing abuse potential).
Nursing Insights
- Educate parents that stimulants are "Schedule II" controlled substances; they require a new hard-copy or secure electronic prescription every 30 days and cannot be refilled via telephone.
- For the "Daytrana" patch, teach the family to apply it to the hip 2 hours before the effect is needed and to rotate sites daily to prevent skin irritation.
- Explain the "Holiday" or "Medication Break" concept: Some providers recommend stopping stimulants during summer or school breaks to allow for "catch-up" growth, although this is debated if the child has severe social impairment.
2. Non-Stimulant Medications: Alpha-2 Agonists and SNRIs
Non-stimulants are indicated for patients who do not tolerate stimulants, have a history of substance abuse, or have comorbid conditions like Tic disorders or severe aggression.
- Selective Norepinephrine Reuptake Inhibitors (SNRIs):
- Atomoxetine (Strattera): The first non-stimulant FDA-approved for ADHD.
- MOA: Specifically inhibits the reuptake of Norepinephrine. Unlike stimulants, it is not a controlled substance and takes 2 to 4 weeks to reach full therapeutic effect.
- Alpha-2 Adrenergic Agonists:
- Guanfacine (Intuniv) and Clonidine (Kapvay):
- MOA: These were originally antihypertensives. They stimulate Alpha-2A receptors in the prefrontal cortex, strengthening the "signal" of neurotransmission to improve working memory and impulse control.
- Utility: Particularly effective for "Hyperactive-Impulsive" symptoms and for patients with co-occurring sleep disturbances or Tourette’s syndrome.
- Atomoxetine carries a "Black Box Warning" for increased suicidal ideation in children and adolescents; the nurse must monitor for mood changes and "dark" thoughts during the first month of therapy.
- Alpha-2 agonists can cause significant hypotension and bradycardia. Nurses must check blood pressure and heart rate before titration and educate parents not to discontinue these medications abruptly, as this can cause "rebound hypertension."
3. Side Effect Management and Monitoring
Effective nursing care involves the proactive identification and mitigation of adverse effects to ensure long-term treatment adherence.
- Anorexia and Weight Loss: Stimulants suppress the appetite center in the hypothalamus.
- Nursing Intervention: Monitor height and weight on a growth chart at every visit. Encourage "mechanical eating" (eating by the clock, not by hunger) and provide high-calorie, nutrient-dense "Power Breakfasts" before the medication kicks in.
- Insomnia: Especially common if long-acting stimulants are taken too late in the day.
- Nursing Intervention: Administer the dose early in the morning (e.g., 0700). Assess for "rebound" hyperactivity in the evening which may be mistaken for insomnia.
- Cardiovascular Effects: Increased heart rate and blood pressure.
- Nursing Intervention: Screen for family history of sudden cardiac death or arrhythmias. Baseline and periodic ECGs may be required for high-risk patients.
- Growth Suppression: Some studies show a temporary slowing of growth velocity in children on long-term stimulants.
- Nursing Intervention: Document growth trajectories meticulously. Most children eventually reach their predicted adult height.
- Tics and Agitation: Stimulants can unmask underlying motor tics.
- Nursing Intervention: Observe for repetitive eye-blinking, shoulder-shrugging, or throat-clearing.
|
Side Effect |
Management Strategy |
|
Appetite Suppression |
Dose after meals; offer calorie-dense snacks in the evening when the med wears off. |
|
Gastrointestinal Upset |
Administer medication with food. |
|
"Zombie-like" Affect |
Indicates the dose is too high; report to the provider for a dose reduction. |
|
Dry Mouth (Xerostomia) |
Encourage frequent sips of water or sugar-free gum (common with Atomoxetine). |
Nursing Insights
- Teach the "Concerta Ghost": In the Concerta OROS delivery system, the tablet shell may appear in the stool after the medication has been absorbed.
- Parents should be warned so they do not think the pill was not digested.
- Stimulants may lower the seizure threshold. If a patient has a known seizure disorder, the nurse must monitor for increased seizure frequency during titration.
Nursing Management And Psychosocial Interventions
- Nursing management of ADHD involves a multi-dimensional approach that extends beyond the clinical setting. The nurse acts as a liaison between the family, the school, and the medical provider, ensuring that the patient’s environment is optimized to compensate for their neurobiological deficits.
1. Behavioral Therapy and Parent Training
Behavioral therapy is the first-line recommendation for preschool-aged children (ages 4–5) before initiating medication, and it remains a core component of "Multimodal Treatment" for older children and adults.
- Principles of Behavior Modification: * Positive Reinforcement: Immediate rewards for desired behaviors (e.g., staying seated for 10 minutes).
- Token Economies: A systematic use of points or stickers that can be exchanged for larger privileges (e.g., extra screen time).
- Time-Outs/Response Cost: Consistent consequences for non-compliance or aggressive behaviors.
- Parent Management Training (PMT): * Nurses teach parents to shift from a "reactive" parenting style to a "proactive" one.
- Focus on "The 3 Cs": Clear, Concise, and Consistent commands.
- Emphasis on maintaining a highly structured daily routine (fixed times for meals, homework, and sleep).
- Social Skills Training: Group-based interventions to help the patient recognize social cues, practice turn-taking, and manage frustration without impulsivity.
Nursing Insights
- Explain to parents that behavioral therapy does not "cure" the ADHD brain; rather, it creates an "external prosthetic" for the child's missing executive functions.
- Nurses must encourage parents to "Catch the child being good." Children with ADHD receive significantly more negative feedback than their peers, which destroys self-esteem.
- The nurse should help parents identify "High-Yield Rewards." A child with ADHD has a low dopamine response; therefore, rewards must be frequent, immediate, and meaningful to be effective.
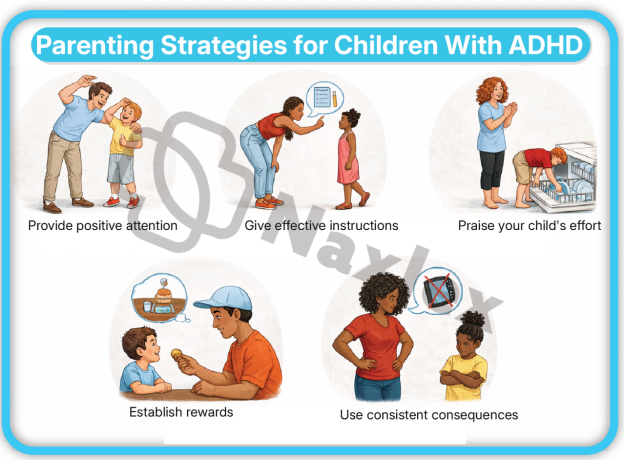
2. Classroom Management and Academic Accommodations
The school environment is often the most challenging domain for the ADHD patient due to the requirement for sustained mental effort and physical stillness.
- Environmental Restructuring:
- Preferential Seating: Seating the student near the teacher and away from high-distraction areas like windows, pencil sharpeners, or busy hallways.
- "Wiggle Room": Allowing for "planned movement breaks" (e.g., the student is assigned the job of taking a note to the office) to expend excess motor energy.
- Academic Modifications (Individualized Education Program - IEP or 504 Plan):
- Extended Time: Providing 50% to 100% more time on tests to account for slow processing and distractibility.
- Reduced Workload: Focusing on "quality over quantity" (e.g., having the student complete only every second math problem to demonstrate mastery).
- Visual Aids: Using graphic organizers, color-coded folders, and daily planners to assist with organizational deficits.
- Instructional Strategies:
- Breaking down long-term projects into "micro-goals" with individual deadlines.
- Providing written instructions to supplement verbal directions.
Nursing Insights
- The nurse should advocate for the "504 Plan" or "IEP." These are legally binding documents under the Individuals with Disabilities Education Act (IDEA).
- Advise teachers and parents to use a "Home-School Communication Log." Consistency across both environments is the strongest predictor of academic success.
- Nurses should educate school staff that ADHD is a disability of "self-regulation," not "disrespect." A child blurting out an answer is a symptom of poor impulse control, not an intentional act of defiance.
3. Nursing Process: Assessment, Nursing Diagnosis, and Interventions
The nursing process provides a systematic framework for managing the care of a patient with ADHD, focusing on safety, compliance, and functional improvement.
- Nursing Assessment:
- Subjective Data: Reports from parents/teachers regarding attention span, activity levels, and social interactions. Assessment of the patient's self-perception.
- Objective Data: Vital signs (BP/HR), height/weight growth velocity, and observation of motor activity during the exam.
- Common Nursing Diagnoses:
- Risk for Injury: Related to impulsive behaviors and lack of danger awareness.
- Impaired Social Interaction: Related to intrusiveness, inability to wait turns, and verbal impulsivity.
- Ineffective Coping (Family): Related to the chronic stress of managing a child with disruptive behavior.
- Non-compliance (Therapeutic Regimen): Related to medication side effects or forgetfulness.
- Nursing Interventions:
- Promote Safety: Instruct the family to keep medications locked away (due to stimulant abuse potential) and provide a supervised, clutter-free environment.
- Enhance Self-Esteem: Assist the child in identifying a "strength" (e.g., art, sports, or computers) to build confidence outside of academics.
- Medication Education: Teach the patient and family about the importance of morning dosing and the management of "rebound" symptoms.
|
Phase |
Nursing Action |
|
Assessment |
Check baseline BMI and EKG if indicated before starting stimulants. |
|
Planning |
Establish a "Behavior Contract" with the child with clear, attainable goals. |
|
Implementation |
Administer stimulants with or immediately after breakfast to mitigate appetite suppression. |
|
Evaluation |
Monitor the Vanderbilt Scale scores every 3–6 months to assess treatment efficacy. |
Nursing Insights
- The 1800-Rule: Stimulants should generally not be administered after 1800 (6:00 PM) to prevent severe insomnia, unless a very small "booster" dose is prescribed for evening homework.
- During follow-up appointments, always ask the child: "How do you feel on the medicine?" Listen for reports of "feeling like a robot" or "losing my personality," which indicates the dose is too high.
- For the nursing student: Remember that Safety is always the priority. If a question asks about an impulsive child running toward a street, the nursing intervention is immediate physical intervention/supervision.
Summary
- Neurobiological Foundation: Attention-Deficit/Hyperactivity Disorder (ADHD) is a chronic, highly heritable neurodevelopmental condition characterized by structural and functional deficits in the prefrontal cortex and basal ganglia.
- Neurochemical Basis: The pathophysiology primarily involves a deficiency in the synaptic availability of Dopamine (linked to motivation and reward) and Norepinephrine (linked to attention and executive filtering).
- Clinical Presentations: Diagnosis is categorized into three types—Predominantly Inattentive, Predominantly Hyperactive-Impulsive, and Combined—each requiring at least 6 symptoms in children (5 in adults) for a minimum of 6 months.
- Diagnostic Rigor: As a clinical diagnosis, it requires symptoms to manifest before age 12, persist in at least two separate environments, and result in clear functional impairment. The nurse must rule out "mimics" like sleep apnea, absence seizures, and trauma.
- Pharmacotherapy: * Stimulants (Methylphenidate/Amphetamines) are first-line, acting to increase catecholamine levels.
- Non-stimulants (Atomoxetine/Alpha-2 Agonists) are utilized for patients who cannot tolerate stimulants or have specific comorbidities like tics.
- Side Effect Vigilance: Nursing care is centered on monitoring for growth suppression, anorexia, insomnia, and cardiovascular changes. Strategies include "power breakfasts" and meticulous height/weight tracking.
- Multimodal Approach: Optimal outcomes are achieved when medication is paired with Behavioral Therapy, Parent Management Training, and Classroom Accommodations (504/IEP plans).
- The Nursing Role: The nurse acts as the central coordinator, educator, and advocate, ensuring the patient's self-esteem is protected while navigating a healthcare system that manages controlled substances.
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on ATTENTION-DEFICIT/HYPERACTIVITY DISORDER (ADHD)
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
