
Hypertensive Disorders
Lessons
- Objectives
- Introduction
- Classification Of Hypertensive Disorders Of Pregnancy
- Practice Exercise 1
- Pathophysiology Of Hypertensive Disorders
- Practice Exercise 2
- Clinical Manifestations And Diagnostic Findings
- Practice Exercise 3
- Management Of Hypertensive Disorders In Pregnancy
- Practice Exercise 4
- Hellp Syndrome (Hemolysis, Elevated Liver Enzymes, Low Platelet Count)
- Practice Exercise 5
- Eclampsia: Seizure Management And Nursing Care
- Practice Exercise 6
- Maternal And Fetal Complications Of Hypertensive Disorders
- Practice Exercise 7
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Define and classify hypertensive disorders of pregnancy based on current obstetric standards, differentiating between gestational hypertension, preeclampsia (with and without severe features), eclampsia, chronic hypertension, and superimposed preeclampsia.
- Explain the pathophysiologic mechanisms underlying hypertensive disorders of pregnancy, including abnormal trophoblastic invasion, endothelial dysfunction, generalized vasospasm, coagulation activation, and the resultant multi-organ microangiopathy.
- Identify and interpret diagnostic criteria for hypertensive disorders in pregnancy, including blood pressure thresholds, proteinuria quantification, and laboratory parameters of organ involvement.
- Correlate fetal assessment findings such as growth restriction, oligohydramnios, and abnormal Doppler velocimetry with maternal disease severity and uteroplacental perfusion compromise.
- Describe the clinical manifestations of each hypertensive disorder, differentiating between mild and severe disease presentations and recognizing early warning signs of deterioration.
- Discuss pharmacologic management strategies, including the mechanisms of action, dosages, and nursing considerations for antihypertensive drugs (labetalol, hydralazine, nifedipine), anticonvulsant therapy (magnesium sulfate), and corticosteroids for fetal lung maturity.
- Explain the principles of magnesium sulfate therapy, including its pharmacodynamics, toxicity monitoring, therapeutic serum levels, and nursing interventions for prevention of magnesium toxicity.
- Discuss the obstetric management regarding timing and mode of delivery in patients with hypertensive disorders, considering maternal stability, gestational age, and fetal well-being.
- Explain the pathophysiology, diagnostic criteria, and management of HELLP Syndrome, emphasizing early recognition and the nursing priorities to prevent maternal morbidity and mortality.
- Describe the seizure mechanism in eclampsia, identify precipitating factors, and demonstrate step-by-step nursing care during and after a seizure to ensure maternal and fetal safety.
- Identify maternal and fetal complications arising from hypertensive disorders, including disseminated intravascular coagulation (DIC), placental abruption, intrauterine growth restriction (IUGR), preterm birth, and stillbirth.
- Provide patient-centered health education focusing on lifestyle modification, warning signs, adherence to medication, and follow-up care during the postpartum period.
Introduction
Hypertensive disorders of pregnancy (HDP) represent one of the most critical complications encountered in obstetrics, contributing substantially to maternal and perinatal morbidity and mortality worldwide. These disorders encompass a spectrum of clinical conditions characterized by elevated blood pressure during pregnancy, often accompanied by systemic involvement that affects multiple organ systems including the renal, hepatic, cerebral, and hematologic systems.
Definition
Hypertensive disorders of pregnancy are defined as conditions in which a pregnant woman develops systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg on at least two occasions, measured at least 4 hours apart after 20 weeks of gestation. These disorders are classified based on timing, severity, and the presence of proteinuria or end-organ dysfunction.
Epidemiology and Global Significance
HDPs occur in approximately 5%–10% of all pregnancies and are among the leading causes of maternal deaths globally, second only to hemorrhage. Preeclampsia and eclampsia together account for more than 70,000 maternal deaths and 500,000 perinatal deaths annually. The burden is particularly high in low-resource settings, where early detection and appropriate management are often limited.
Beyond immediate pregnancy outcomes, women who experience hypertensive disorders face an increased lifetime risk of chronic hypertension, cardiovascular disease, and renal impairment.
Etiologic Overview
The exact cause of hypertensive disorders of pregnancy remains multifactorial and incompletely understood. The most widely accepted theory implicates abnormal placentation during early gestation, leading to incomplete remodeling of the spiral arteries. This results in placental ischemia, endothelial dysfunction, and systemic vasospasm, which manifest clinically as hypertension and end-organ injury. Genetic, immunologic, and environmental factors also contribute to the pathogenesis.
Classification Of Hypertensive Disorders Of Pregnancy
1.1 Gestational Hypertension
- Definition and Diagnostic Criteria
- Gestational hypertension is defined as new-onset systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg documented on two occasions at least 4 hours apart that occurs at >20 weeks of gestation in a previously normotensive woman, without proteinuria or other signs of end-organ dysfunction at the time of diagnosis.
- Blood pressure elevations that first appear before 20 weeks of gestation should prompt evaluation for chronic hypertension rather than gestational hypertension.
- If hypertension develops after 20 weeks and proteinuria or end-organ dysfunction subsequently appears, the diagnosis is reclassified to preeclampsia.

- Epidemiology and Clinical Course
- Gestational hypertension may represent a transient hypertensive response to pregnancy in some women or may be a precursor to preeclampsia in others; approximately 15%–25% of women with gestational hypertension progress to preeclampsia.
- Onset is typically in the second half of pregnancy; resolution usually occurs by 6 weeks postpartum, but persistent hypertension beyond 12 weeks postpartum suggests chronic hypertension.
- Key Clinical Features
- Elevated blood pressure readings as described above, in the absence of proteinuria or systemic manifestations (e.g., thrombocytopenia, elevated liver enzymes, renal insufficiency, pulmonary edema, neurological symptoms).
- May be accompanied by mild peripheral edema, but generalized edema alone is not diagnostic.

- Differential Diagnosis
- Distinguish from chronic hypertension (preexisting or diagnosed before 20 weeks gestation), white coat hypertension, and masked hypertension.
- Confirm accurate measurement technique and consider ambulatory or home BP monitoring if readings are inconsistent.
- Nursing Insights
- Accurate blood pressure measurement technique is essential: use an appropriately sized cuff, ensure the patient is seated with back supported and legs uncrossed, arm at heart level, and allow 5 minutes of rest before measurement; document position and cuff size.
- Re-evaluate elevated readings with repeated measurements at least 4 hours apart; do not diagnose based on a single elevated value.
- Educate the patient on home blood pressure monitoring: instruct on frequency (e.g., twice daily), proper technique, and threshold values for reporting (report readings ≥140/90 mm Hg).
- Recognize gestational hypertension as a dynamic diagnosis that requires close follow-up because progression to preeclampsia may be sudden; establish a surveillance plan including BP checks and symptom review.
- Prepare patient education materials that explain warning signs (headache, visual changes, epigastric pain, oliguria, decreased fetal movement) and emergency contact instructions.
1.2 Preeclampsia
- Definition and Diagnostic Criteria
- Preeclampsia is a multisystem disorder of pregnancy defined by new-onset hypertension (systolic ≥140 mm Hg or diastolic ≥90 mm Hg on two occasions ≥4 hours apart) at >20 weeks gestation accompanied by either:
- Proteinuria defined as ≥300 mg protein in a 24-hour urine collection, protein/creatinine ratio ≥0.3, or dipstick reading ≥1+ when quantitative methods are unavailable; or
- In the absence of proteinuria, new-onset end-organ dysfunction including thrombocytopenia (platelets <100,000/µL), renal insufficiency (serum creatinine >1.1 mg/dL or doubling of baseline), impaired liver function (elevated transaminases), pulmonary edema, or new-onset cerebral or visual disturbances.
- Preeclampsia is a multisystem disorder of pregnancy defined by new-onset hypertension (systolic ≥140 mm Hg or diastolic ≥90 mm Hg on two occasions ≥4 hours apart) at >20 weeks gestation accompanied by either:
- Pathophysiologic Overview (brief, to orient classification)
- The central pathophysiologic process involves abnormal placentation with inadequate remodeling of the spiral arteries, resulting in placental hypoperfusion and ischemia; the ischemic placenta releases antiangiogenic factors (e.g., sFlt-1) and inflammatory mediators that provoke widespread maternal endothelial dysfunction, vasoconstriction, and a prothrombotic state.
- Clinical Spectrum
- Preeclampsia is a spectrum ranging from mild disease (preeclampsia without severe features) to severe disease (preeclampsia with severe features), and in its extreme form can lead to HELLP syndrome or eclampsia.
- Nursing Insights
- Assess for and document symptoms that indicate systemic involvement: persistent or severe headache, visual disturbances (scotomata, blurred vision), right upper quadrant or epigastric pain, sudden weight gain, and oliguria. These symptoms indicate progressive or severe disease and warrant urgent escalation.
- Monitor laboratory trends: serial platelet counts, AST/ALT, serum creatinine, and LDH when clinically indicated; create clear protocols for frequency of labs based on disease severity.
- Coordinate multidisciplinary care early (obstetrics, maternal-fetal medicine, anesthesia, critical care) when preeclampsia is diagnosed, as rapid deterioration is possible.
- Implement fetal surveillance appropriate to severity and gestational age: non-stress tests, biophysical profiles, and ultrasound growth assessments to detect fetal growth restriction and oligohydramnios.
- Ensure documentation includes baseline blood pressures, times of measurement, symptoms, urine protein quantification, and all nursing interventions.
1.2.1 Preeclampsia Without Severe Features
- Definition and Diagnostic Criteria
- Preeclampsia without severe features is characterized by new-onset hypertension (≥140/90 mm Hg) after 20 weeks of gestation plus proteinuria (≥300 mg/24 h or equivalent) or other diagnostic criteria for preeclampsia without evidence of severe features such as severe-range blood pressures, significant thrombocytopenia, impaired liver function, renal insufficiency, pulmonary edema, or neurological symptoms.
- Clinical Presentation
- Patients typically have asymptomatic or mildly symptomatic disease: mild headache responsive to acetaminophen, mild peripheral edema, and modest proteinuria.
- Blood pressure generally in the range of 140–159 systolic or 90–109 diastolic.
- Monitoring and Management Principles
- Conservative management may be appropriate depending on gestational age and maternal/fetal status: outpatient management with frequent blood pressure checks, activity modification, serial laboratory assessment, and fetal surveillance can be considered for stable patients at or beyond a threshold gestational age.
- Consider antenatal corticosteroids if delivery is anticipated before 34 weeks and maternal/fetal status warrants it.
- Antihypertensive therapy is instituted when BP is persistently ≥150–160/100–110 mm Hg depending on institutional policy and maternal risk; thresholds vary but aim to prevent severe-range pressures.
- Nursing Insights
- For ambulatory patients, set up a structured follow-up schedule: BP checks (clinic or home), symptom diary (headache, vision changes, RUQ pain), and clear escalation criteria for urgent evaluation.
- Educate on activity and diet: no evidence supports strict bed rest; encourage moderate activity as tolerated and balanced nutrition; advise against high-sodium or fad diets.
- Teach accurate home urine protein testing only as adjunct; emphasize that quantitative testing (protein/creatinine ratio or 24-hour collection) is definitive.
- Recognize that even “without severe features” can rapidly evolve; instruct patients to present urgently for any concerning symptoms.
1.2.2 Preeclampsia With Severe Features
- Definition and Diagnostic Criteria
- Preeclampsia with severe features is defined as new-onset hypertension after 20 weeks gestation plus one or more of the following:
- Systolic blood pressure ≥160 mm Hg or diastolic ≥110 mm Hg on two occasions at least 4 hours apart (unless antihypertensive therapy is initiated), or
- Thrombocytopenia (platelets <100,000/µL), or
- Serum transaminases at least twice normal concentration, or
- Progressive renal insufficiency (serum creatinine >1.1 mg/dL or doubling of baseline), or
- Pulmonary edema, or
- New-onset cerebral or visual disturbances (e.g., severe headache, visual scotomata), or
- Persistent or severe epigastric or right upper quadrant pain.
- Preeclampsia with severe features is defined as new-onset hypertension after 20 weeks gestation plus one or more of the following:

- Clinical Implications
- Severe features signal significant end-organ involvement and substantially increase the risk of maternal morbidity (e.g., intracranial hemorrhage, pulmonary edema, hepatic rupture, DIC) and fetal compromise (IUGR, oligohydramnios, preterm birth).
- Immediate medical management and frequently expedited delivery are often indicated, depending on gestational age and stability.
- Management Priorities
- Stabilize maternal airway, breathing, and circulation; treat severe-range hypertension with rapid-acting antihypertensives (e.g., IV labetalol, IV hydralazine, or oral/NG nifedipine per protocol) to reduce risk of stroke.
- Initiate magnesium sulfate for seizure prophylaxis when indicated (generally for severe features) and continue per protocol post-delivery for a recommended period.
- Prepare for delivery when maternal or fetal condition indicates; coordinate anesthesia consult early because coagulopathy and thrombocytopenia may affect neuraxial anesthesia decisions.
- Nursing Insights
- Prioritize frequent vital signs and continuous maternal-fetal monitoring; document BP every 15 minutes during acute management, then at intervals per protocol.
- Perform and document neurological assessments frequently: level of consciousness, headache severity, visual changes, deep tendon reflexes, and presence of clonus. Escalate care immediately for signs of neurological deterioration.
- Monitor intake and output hourly and report oliguria (<30 mL/h) as this may indicate renal compromise or magnesium toxicity in the setting of magnesium therapy.
- Prepare blood products and have transfusion protocols ready if HELLP or DIC is suspected; obtain baseline coagulation studies and crossmatch as ordered.
- Ensure bedrest in a lateral position when feasible to enhance uteroplacental perfusion; implement seizure precautions including padded side rails and suction at bedside.
1.3 Eclampsia
- Definition
- Eclampsia is the occurrence of new-onset generalized tonic-clonic seizures or coma in a woman with preeclampsia that cannot be attributed to other neurologic conditions (e.g., epilepsy, cerebral hemorrhage, intoxication).
- Epidemiology and Clinical Course
- Eclampsia is less common in high-resource settings due to prophylactic use of magnesium sulfate and improved surveillance, but it remains a major contributor to maternal mortality in regions with limited access to care.
- Seizures may occur antepartum, intrapartum, or postpartum; up to one-third of eclamptic seizures occur postpartum.
- Pathophysiology
- Seizures in eclampsia are believed to result from severe cerebral vasospasm, endothelial disruption, and vasogenic cerebral edema leading to decreased seizure threshold and focal or generalized neuronal hyperexcitability.
- Clinical Features
- Prodromal symptoms may include severe headache, visual disturbances, agitation, or altered mental status, but seizures can also be abrupt and without warning.
- Nursing Insights
- During a seizure, the immediate nursing priorities are airway protection, maternal safety, and prevention of aspiration: position on the side once feasible, clear airway, do not place objects in mouth, and ensure oxygen and suction are available.
- Administer magnesium sulfate as first-line anticonvulsant therapy per protocol; have calcium gluconate available as the antidote for magnesium toxicity.
- After the seizure, perform a rapid assessment for injury, vaginal bleeding/placental abruption, cervical status, and fetal distress; continuous fetal monitoring is essential.
- Communicate rapidly with the multidisciplinary team to prepare for potential urgent delivery, intubation, imaging (CT/MRI if intracranial hemorrhage suspected), and critical care transfer.
1.4 Chronic Hypertension
- Definition
- Chronic hypertension is hypertension diagnosed prior to pregnancy or detected before 20 weeks of gestation; it includes women with preexisting essential hypertension and those with secondary causes of hypertension.
- Clinical Considerations
- Women with chronic hypertension are at increased risk of superimposed preeclampsia, fetal growth restriction, preterm birth, and placental abruption.
- Baseline antihypertensive therapies may require adjustment because certain antihypertensive agents (e.g., ACE inhibitors, ARBs) are contraindicated in pregnancy.
- Management Principles
- Optimize blood pressure control prior to conception when possible; during pregnancy, use pregnancy-safe antihypertensives (e.g., labetalol, nifedipine, methyldopa) and monitor for signs of superimposed preeclampsia.
- Monitor fetal growth and placental function with serial ultrasound and consider increased antenatal surveillance.
- Nursing Insights
- Obtain a thorough preconception/antepartum medication history and reconcile medications; educate patients about teratogenic drugs and the need for changes before or immediately after conception.
- Monitor for signs of superimposed preeclampsia: new or worsening proteinuria, sudden increase in BP, development of severe features—escalate care promptly.
- Educate on lifestyle modifications to support BP control: sodium moderation, weight management, smoking cessation, and adherence to prescribed medications.
- Coordinate care with primary care and cardiology when appropriate for complex or secondary hypertension.
1.5 Superimposed Preeclampsia
- Definition
- Superimposed preeclampsia occurs when a woman with chronic hypertension develops new-onset proteinuria or sudden worsening of hypertension with features consistent with preeclampsia after 20 weeks gestation, or when preexisting hypertension becomes accompanied by end-organ dysfunction typical of preeclampsia.
- Diagnostic Criteria
- New-onset proteinuria in a woman with chronic hypertension, or a sudden and sustained increase in blood pressure or development of severe features (thrombocytopenia, elevated transaminases, renal insufficiency, pulmonary edema, neurological symptoms) that cannot be explained by chronic hypertension alone.
- Clinical Importance
- Superimposed preeclampsia carries a higher risk of adverse maternal and fetal outcomes compared with preeclampsia or chronic hypertension alone, including higher rates of HELLP syndrome, placental abruption, and preterm delivery.
- Management Considerations
- Management is similar to preeclampsia with severe features when severe features are present; more intense surveillance is required including frequent laboratory monitoring and fetal assessment.
- Antihypertensive regimens may need to be intensified and magnesium sulfate initiated if severe features develop.
- Nursing Insights
- Maintain a high index of suspicion in women with chronic hypertension for new proteinuria or abrupt changes in BP; institute prompt urine protein testing and laboratory evaluation when indicated.
- Establish baseline laboratory values early in pregnancy for women with chronic hypertension to aid in detection of superimposed disease.
- Provide anticipatory guidance regarding the increased risk of adverse outcomes and the potential need for earlier delivery; discuss implications for anesthesia and possible blood product availability.
- Educate women and family about the signs of deterioration and ensure rapid access to care; arrange closer follow-up schedules.
Pathophysiology Of Hypertensive Disorders
Hypertensive disorders of pregnancy (HDP), particularly preeclampsia and eclampsia, arise from a complex interplay of placental, vascular, immunologic, and genetic factors. The underlying event is abnormal placentation that leads to endothelial dysfunction, vasospasm, and multi-organ microangiopathy. These processes compromise maternal perfusion and cause characteristic signs such as hypertension, proteinuria, and systemic involvement.
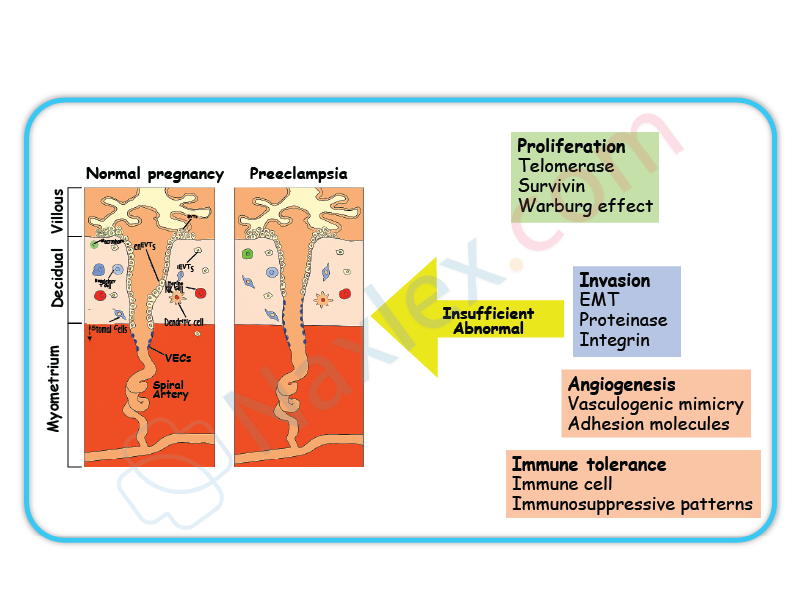
1.1 Abnormal Trophoblastic Invasion
In normal pregnancy, the cytotrophoblasts invade the maternal spiral arteries during early gestation (8–18 weeks). This physiologic remodeling transforms the small, high-resistance vessels into large, low-resistance channels to ensure adequate uteroplacental blood flow.
In preeclampsia:
- Trophoblastic invasion is incomplete.
- Spiral arteries remain narrow, muscular, and responsive to vasomotor stimuli.
- This results in reduced uteroplacental perfusion and relative placental ischemia.
Key cellular events:
- Impaired differentiation of endovascular cytotrophoblasts prevents normal vascular remodeling.
- The placental bed shows fibrinoid necrosis, atherosis, and inflammatory infiltration.
- The ischemic placenta releases antiangiogenic factors such as sFlt-1 and endoglin, which antagonize VEGF (vascular endothelial growth factor) and placental growth factor (PlGF).
Pathophysiologic consequence:
Placental hypoxia → oxidative stress → systemic endothelial activation → vasoconstriction → hypertension.
Nursing Insight:
Early recognition of abnormal placental perfusion (via Doppler studies showing reduced diastolic flow) predicts the risk of preeclampsia. Nursing interventions should focus on monitoring fetal growth restriction and maternal symptoms early in high-risk pregnancies.
1.2 Endothelial Dysfunction
Endothelial cells normally produce vasodilators such as nitric oxide (NO) and prostacyclin (PGI₂), maintaining vascular tone and preventing platelet aggregation. In preeclampsia, endothelial injury shifts this balance toward vasoconstriction and coagulation.
Mechanisms:
- ↓ Nitric oxide and prostacyclin → vasoconstriction.
- ↑ Endothelin and thromboxane A₂ → increased vascular resistance.
- ↑ Capillary permeability → plasma leakage → edema and hemoconcentration.
- Activation of platelets and coagulation cascade → microthrombi formation.
|
Normal Endothelium |
Endothelial Dysfunction in Preeclampsia |
|
Balanced vasodilators (NO, PGI₂) |
Decreased NO and PGI₂ |
|
Minimal vascular reactivity |
Increased vascular sensitivity to angiotensin II |
|
Low platelet activation |
Platelet aggregation and thrombocytopenia |
|
Stable oncotic pressure |
Capillary leak → edema, proteinuria |
Clinical correlation:
- Elevated BP due to systemic vasoconstriction.
- Proteinuria from glomerular endotheliosis.
- Hemoconcentration and edema due to plasma leakage.
Nursing Insight:
Monitor blood pressure at consistent intervals, use appropriate cuff size, and assess for dependent and facial edema. Persistent headache and visual disturbances reflect endothelial dysfunction affecting cerebral circulation.
1.3 Vasospasm and Multisystem Involvement
The hallmark of preeclampsia is widespread vasospasm, which leads to ischemia and hypoperfusion of major organs.
Renal System
- Glomerular endotheliosis causes reduced glomerular filtration rate (GFR).
- Proteinuria ≥ 300 mg/24h results from leaky glomerular capillaries.
- Sodium and water retention → edema and increased BP.
Hepatic System
- Hepatic vasospasm leads to periportal necrosis and subcapsular hematoma.
- Elevated AST and ALT, right upper quadrant or epigastric pain.
- May progress to HELLP Syndrome (Hemolysis, Elevated Liver Enzymes, Low Platelet count).
Cerebral and Visual System
- Vasospasm causes cerebral edema and ischemia → headaches, hyperreflexia, visual disturbances, seizures (eclampsia).
- Retinal arteriolar spasm causes blurred vision and scotoma.
Cardiovascular System
- Increased systemic vascular resistance.
- Reduced plasma volume despite edema (third spacing).
- Hemoconcentration increases risk of thrombosis.
|
Organ System |
Effect of Vasospasm |
Clinical Manifestation |
|
Kidneys |
↓ GFR, proteinuria |
Oliguria, elevated creatinine |
|
Liver |
Ischemia, necrosis |
Epigastric pain, ↑ liver enzymes |
|
Brain |
Edema, ischemia |
Headache, seizures |
|
Eyes |
Retinal spasm |
Blurred vision |
|
Placenta |
Hypoperfusion |
IUGR, fetal distress |
Nursing Insight:
Monitor urine output (≥30 mL/hr), deep tendon reflexes, and neurologic signs. Deterioration suggests progression toward severe preeclampsia or impending eclampsia.
1.4 Coagulation Abnormalities
Endothelial injury exposes subendothelial collagen, triggering platelet aggregation and activation of the coagulation cascade.
Pathophysiologic outcomes:
- Platelet consumption → thrombocytopenia (<100,000/μL).
- Fibrin deposition in small vessels → microangiopathic hemolysis.
- Excessive activation may evolve into disseminated intravascular coagulation (DIC).
Clinical Indicators:
- Petechiae, bleeding gums, hematuria.
- Prolonged PT, aPTT, and decreased fibrinogen.
- Elevated D-dimers indicating fibrinolysis.
Nursing Insight:
Monitor platelet counts and coagulation profiles regularly. Avoid invasive procedures (e.g., IM injections) if platelet count is <100,000/μL.
1.5 Summary of Pathophysiologic Cascade
- Abnormal placentation → placental ischemia.
- Placenta releases antiangiogenic factors → endothelial injury.
- Endothelial dysfunction → vasospasm and capillary leak.
- Vasospasm → organ hypoperfusion and hypertension.
- Coagulation activation → thrombocytopenia and hemolysis.
- Resulting clinical picture → hypertension, proteinuria, edema, and multi-organ involvement.
Overall Conceptual Map:
Abnormal Placentation
↓
Placental Ischemia
↓
Endothelial Dysfunction
↓
Systemic Vasospasm
↓
↓ Organ Perfusion → Hypertension + Proteinuria + Multi-Organ Damage
Nursing Insight:
Pathophysiologic understanding guides timely nursing interventions — maintaining strict fluid balance, monitoring BP, observing for neurologic changes, and preventing seizure and renal complications.
Clinical Manifestations And Diagnostic Findings
1.1 Clinical Manifestations
Hypertensive disorders of pregnancy—gestational hypertension, preeclampsia, eclampsia, and HELLP syndrome—present a spectrum of clinical findings that evolve with the severity of endothelial dysfunction, vasospasm, and multiorgan involvement.
Key Clinical Manifestations:
- Elevated Blood Pressure
- Defined as systolic BP ≥140 mmHg and/or diastolic BP ≥90 mmHg on two occasions ≥4 hours apart after 20 weeks gestation in a previously normotensive woman.
- Severe features: Systolic ≥160 mmHg or diastolic ≥110 mmHg.
- Generalized Edema
- Pathological edema due to increased capillary permeability and decreased colloid osmotic pressure.
- Pitting edema, especially in the face, hands, and lower extremities.
- Proteinuria
- A hallmark of preeclampsia due to glomerular endotheliosis and increased glomerular permeability.
- Neurological Symptoms
- Headache (persistent, severe, frontal or occipital).
- Visual disturbances: blurred vision, scotomata, photophobia.
- Hyperreflexia and clonus due to CNS irritability.
- Gastrointestinal and Hepatic Symptoms
- Epigastric or right upper quadrant pain (due to hepatic capsule distention or subcapsular hematoma).
- Nausea and vomiting from hepatic involvement.
- Renal Manifestations
- Oliguria (<500 mL/24h) from renal vasospasm and reduced perfusion.
- Elevated serum creatinine and uric acid levels.
- Respiratory Manifestations
- Dyspnea from pulmonary edema due to capillary leak and left ventricular dysfunction.
- Hematologic Manifestations
- Thrombocytopenia and hemolysis (especially in HELLP syndrome).
- Fetal Manifestations
- Decreased uteroplacental perfusion leading to intrauterine growth restriction (IUGR) or fetal hypoxia.
Nursing Insights
- Persistent headache, visual disturbances, or epigastric pain are ominous warning signs of disease progression.
- Always assess deep tendon reflexes and clonus—increased neuromuscular irritability indicates risk of seizure onset.
- Report decreased fetal movement, which may indicate uteroplacental insufficiency.
1.2 Blood Pressure Criteria and Diagnostic Thresholds
|
Category |
Systolic (mmHg) |
Diastolic (mmHg) |
Timing |
Proteinuria |
Other Features |
|
Chronic Hypertension |
≥140 |
≥90 |
Before 20 weeks |
None |
|
|
Gestational Hypertension |
≥140 |
≥90 |
After 20 weeks |
None |
BP normalizes postpartum |
|
Preeclampsia (without severe features) |
≥140 but <160 |
≥90 but <110 |
After 20 weeks |
≥300 mg/24h or Protein/Creatinine ≥0.3 |
No organ dysfunction |
|
Preeclampsia with severe features |
≥160 |
≥110 |
After 20 weeks |
May or may not be present |
Evidence of organ damage |
|
Eclampsia |
Variable |
Variable |
After 20 weeks or postpartum |
Variable |
Seizures not due to other causes |
|
HELLP Syndrome |
Variable |
Variable |
Any time (usually 27–37 wks) |
Variable |
Hemolysis, Elevated Liver enzymes, Low Platelets |
Interpretation:
- Two readings, ≥4 hours apart, are required for diagnosis.
- Severe hypertension (≥160/110 mmHg) warrants immediate intervention to prevent maternal stroke.
Nursing Insights
- Always use the right cuff size; small cuffs overestimate BP.
- BP should be taken with the patient seated or in left lateral recumbent to avoid supine hypotension.
- Do not rely on a single BP reading for diagnosis; repeated accurate measurements are mandatory.
1.3 Proteinuria and Renal Assessment
Proteinuria Criteria:
- ≥300 mg protein in a 24-hour urine collection.
- Protein/creatinine ratio ≥0.3 mg/dL.
- Dipstick reading ≥1+ (if quantitative tests unavailable).
Renal Function Changes:
- Glomerular endotheliosis causes narrowing of capillary lumens and reduced filtration surface area.
- Serum Creatinine >1.1 mg/dL or doubling of baseline indicates renal insufficiency.
- Uric acid levels >5.5 mg/dL indicate decreased renal clearance.
- Oliguria (<500 mL/24h) is a sign of renal compromise.
|
Test |
Normal Pregnancy |
Preeclampsia |
|
Serum Creatinine |
0.4–0.8 mg/dL |
>1.1 mg/dL |
|
Uric Acid |
<5.5 mg/dL |
>6 mg/dL |
|
Proteinuria |
<150 mg/24h |
≥300 mg/24h |
Nursing Insights
- Monitor urine output hourly if magnesium sulfate is administered; decreased output increases toxicity risk.
- Collect 24-hour urine samples accurately—discard the first specimen, include all subsequent voids.
- Oliguria with dark urine suggests renal ischemia; report immediately.
1.4 Laboratory Tests (Liver, Platelet, Hemolysis Indices)
Key Laboratory Parameters:
- Platelet Count: <100,000/μL indicates thrombocytopenia.
- AST/ALT: Elevated >2× normal suggests hepatic injury.
- LDH (>600 IU/L): Indicates hemolysis.
- Peripheral Smear: Schistocytes confirm microangiopathic hemolysis.
- Haptoglobin: Decreased levels support diagnosis of hemolysis.
- Bilirubin: Mild elevation due to RBC breakdown.
- Serum Creatinine & Uric Acid: Elevated in renal involvement.
|
Test |
Normal Range |
Abnormal in HELLP |
Clinical Significance |
|
Platelets |
150,000–400,000 |
<100,000 |
Risk of bleeding |
|
AST/ALT |
<40 IU/L |
>70 IU/L |
Hepatic damage |
|
LDH |
<200 IU/L |
>600 IU/L |
Hemolysis |
|
Haptoglobin |
30–200 mg/dL |
Decreased |
Hemolysis marker |
Nursing Insights
- Always check trends, not single values—falling platelet count indicates disease progression.
- Avoid IM injections in thrombocytopenic patients to prevent hematoma.
- Right upper quadrant pain + elevated AST/ALT = impending hepatic rupture.
1.5 Fetal Assessment Findings
Fetal Complications:
- Intrauterine growth restriction (IUGR)
- Oligohydramnios
- Fetal distress
- Placental abruption
- Preterm delivery
- Intrauterine fetal demise (in severe cases)
Assessment Methods:
- Non-Stress Test (NST): Monitors fetal heart rate reactivity.
- Biophysical Profile (BPP): Evaluates fetal breathing, movement, tone, amniotic fluid volume, and heart rate.
- Doppler Velocimetry: Assesses umbilical artery blood flow resistance.
- Ultrasound: Monitors fetal growth and amniotic fluid index.
|
Test |
Normal Result |
Abnormal Finding |
Interpretation |
|
NST |
Reactive (≥2 accelerations/20 min) |
Non-reactive |
Fetal hypoxia |
|
BPP |
8–10 |
≤6 |
Compromised fetus |
|
Doppler S/D ratio |
<3.0 |
>3.0 |
Increased placental resistance |
Nursing Insights
- Daily fetal movement counts are vital for self-monitoring.
- If NST is non-reactive, prepare for BPP or CST (Contraction Stress Test).
Severe preeclampsia with non-reassuring fetal testing = indication for delivery.
Management Of Hypertensive Disorders In Pregnancy
Hypertensive disorders in pregnancy (HDP) encompass a spectrum of conditions including gestational hypertension, preeclampsia, eclampsia, chronic hypertension, and HELLP syndrome. The management focuses on maternal stabilization, prevention of complications (seizures, organ failure, stroke), and ensuring optimal fetal outcomes. Interventions are tailored based on disease severity, gestational age, and maternal-fetal condition.
1.1 Nursing Assessment and Monitoring
Accurate and continuous assessment is critical in managing hypertensive disorders in pregnancy to detect early deterioration and prevent maternal-fetal morbidity.
Assessment Components
- Blood Pressure (BP) Monitoring
- Measure BP using the same arm, in sitting or left lateral recumbent position.
- Use appropriately sized cuff; incorrect cuff size may falsely elevate readings.
- Diagnostic threshold:
- ≥140/90 mmHg after 20 weeks → Hypertensive disorder.
- ≥160/110 mmHg → Severe preeclampsia.
- Urinalysis
- Evaluate for proteinuria (≥300 mg/24 hr or +1 on dipstick).
- Protein/creatinine ratio ≥0.3 indicates significant proteinuria.
- Neurological Assessment
- Assess for headache, visual disturbances, hyperreflexia, clonus, confusion, or seizure activity.
- Respiratory Assessment
- Monitor for dyspnea, crackles, pulmonary edema.
- Renal Function
- Measure urine output (>30 mL/hr), serum creatinine, and BUN levels.
- Hepatic Function
- Monitor AST, ALT, and LDH for hepatic involvement or HELLP syndrome.
- Fetal Surveillance
- Conduct non-stress tests (NSTs), biophysical profiles (BPPs), and Doppler velocimetry.
- Assess for intrauterine growth restriction (IUGR).
Nursing Insights
- Frequent BP checks are vital; a sudden rise >30 mmHg systolic or >15 mmHg diastolic from baseline, even if <140/90 mmHg, can still signify pathology.
- Always assess deep tendon reflexes (DTRs)—hyperreflexia may indicate impending eclampsia.
- Monitor weight gain—>1 kg/week may indicate fluid retention.
- Document findings meticulously and report epigastric pain or visual changes immediately as these precede seizures.
1.2 Pharmacologic Management
Pharmacologic therapy aims to control hypertension, prevent seizures, and minimize maternal and fetal complications.
1.2.1 Antihypertensives
Commonly Used Medications
|
Medication |
Class |
Mechanism |
Key Nursing Considerations |
|
Labetalol |
β-blocker |
Reduces systemic vascular resistance without lowering cardiac output |
Monitor for bradycardia, avoid in asthma |
|
Hydralazine |
Vasodilator |
Direct arteriolar smooth muscle relaxation |
Monitor for reflex tachycardia, headache |
|
Nifedipine |
Calcium channel blocker |
Inhibits calcium ion influx in vascular smooth muscle |
Administer orally, avoid co-administration with MgSO₄ IV |
|
Methyldopa |
Centrally acting α2 agonist |
Reduces sympathetic tone |
Preferred for long-term control, monitor for sedation or liver dysfunction |
Therapeutic Goal
- Maintain systolic BP 130–150 mmHg and diastolic BP 80–100 mmHg.
- Avoid lowering BP too rapidly to prevent placental hypoperfusion.
Nursing Insights
- IV hydralazine or IV labetalol are used for acute severe hypertension.
- Avoid ACE inhibitors and ARBs—teratogenic and fetotoxic.
- Assess fetal heart rate (FHR) after maternal antihypertensive administration to ensure placental perfusion.
1.2.2 Magnesium Sulfate Therapy
Used for seizure prophylaxis and treatment in severe preeclampsia and eclampsia.
Mechanism of Action
- CNS depressant → reduces acetylcholine release at neuromuscular junction → prevents seizures.
- Also vasodilates cerebral vessels → reduces ischemia.
Dosage and Administration
- Loading dose: 4–6 g IV over 20–30 minutes.
- Maintenance: 2 g/hr continuous infusion.
- Continue for 24 hours postpartum or after last seizure.
Toxicity Monitoring
|
Parameter |
Normal |
Toxicity Indicator |
|
Deep tendon reflexes (DTRs) |
2+ |
Absent reflexes |
|
Respirations |
12-20/min |
<12/min |
|
Urine output |
≥30 mL/hr |
<30 mL/hr |
|
Serum Mg²⁺ |
4–7 mEq/L |
>8 mEq/L (toxic) |
Antidote
- Calcium gluconate 10%, 1 g (10 mL) IV over 3 minutes.
Nursing Insights
- Always use an infusion pump.
- Keep calcium gluconate readily available at bedside.
- Continuous fetal monitoring during therapy—maternal toxicity can cause fetal bradycardia.
- Report flushing, muscle weakness, or slurred speech promptly.
1.2.3 Corticosteroid Therapy
Administered for fetal lung maturation and maternal stabilization in HELLP syndrome.
Common Drugs
- Betamethasone 12 mg IM every 24 hours × 2 doses.
- Dexamethasone 6 mg IM every 12 hours × 4 doses.
Indications
- Gestational age <34 weeks with preeclampsia/eclampsia.
- HELLP syndrome to improve platelet count and hepatic function.
Nursing Insights
- Monitor maternal glucose—corticosteroids can cause transient hyperglycemia.
- Observe for signs of infection—steroids can suppress immune response.
1.3 Fluid Management
Fluid therapy in hypertensive disorders requires caution due to the risk of pulmonary edema and renal compromise.
Guidelines
- Restrict total fluid intake to ~80 mL/hr or <100 mL/hr.
- Maintain urine output ≥30 mL/hr.
- Avoid fluid boluses unless in hypovolemic shock.
- Use crystalloids; avoid colloids unless severe hypoproteinemia.
Monitoring
- Strict intake and output (I&O) charting.
- Daily weights and lung auscultation to detect early fluid overload.
- Evaluate central venous pressure (CVP) if indicated.
Nursing Insights
- Overhydration can precipitate pulmonary edema especially with MgSO₄ therapy.
- In HELLP syndrome, volume expansion may improve perfusion but must be closely monitored.
1.4 Nutritional and Lifestyle Modifications
- Dietary Management
- Balanced diet rich in protein, calcium, vitamin C, and fiber.
- Avoid excess sodium intake.
- Encourage adequate hydration, unless contraindicated.
- Activity
- Encourage bed rest in left lateral position to improve uteroplacental blood flow.
- Reduce stress and provide psychological support.
- Weight Monitoring
- Weekly weight monitoring to detect fluid retention.
Nursing Insights
- Educate patient on home BP monitoring and symptom tracking (headache, vision changes, epigastric pain).
- Encourage follow-up visits and postpartum surveillance for at least 6 weeks.
1.5 Timing and Mode of Delivery
Decision Factors
- Gestational age
- Severity of maternal disease
- Fetal condition and viability
|
Condition |
Recommended Timing |
Mode of Delivery |
|
Gestational hypertension |
≥37 weeks |
Vaginal preferred |
|
Preeclampsia without severe features |
37 weeks |
Vaginal induction |
|
Severe preeclampsia |
≥34 weeks or earlier if maternal/fetal distress |
Cesarean section may be indicated |
|
Eclampsia |
After stabilization and seizure control |
Expedite delivery—vaginal if feasible |
Nursing Insights
- Never induce labor in unstable eclamptic patients until airway and seizures are managed.
- Magnesium sulfate should be continued throughout labor and for 24 hours postpartum.
1.6 Postpartum Management
Postpartum care focuses on preventing complications, monitoring resolution, and educating for future risk reduction.
Key Interventions
- Continue BP monitoring for ≥72 hours after delivery.
- Maintain MgSO₄ infusion for 24 hours post-delivery or last seizure.
- Observe for:
- Seizures
- Pulmonary edema
- Renal failure
- Postpartum hemorrhage due to uterine atony from MgSO₄.
- Long-term counseling
- Risk of recurrence in future pregnancies.
- Increased lifetime risk of cardiovascular disease.
Nursing Insights
- Teach the mother about warning signs (severe headache, visual changes, swelling, chest pain).
- Advise follow-up for renal function and BP checks at 6 weeks postpartum.
- Encourage contraceptive counseling—avoid estrogen-containing contraceptives in persistent hypertension.
Hellp Syndrome (Hemolysis, Elevated Liver Enzymes, Low Platelet Count)
1.1 Definition and Diagnostic Criteria
- HELLP syndrome is a severe variant of preeclampsia characterized by:
- H: Hemolysis – destruction of red blood cells.
- EL: Elevated liver enzymes – indicating liver dysfunction.
- LP: Low platelet count – thrombocytopenia <100,000/μL.
- Diagnostic criteria typically include:
- Hemolysis: Presence of schistocytes on peripheral blood smear, elevated lactate dehydrogenase (LDH >600 IU/L), decreased haptoglobin.
- Elevated Liver Enzymes: AST or ALT >70 IU/L.
- Low Platelets: <100,000/μL.
- HELLP syndrome may present with or without hypertension or proteinuria.
Nursing Insights:
- Early recognition is critical; HELLP can progress rapidly and lead to life-threatening maternal and fetal complications.
- Blood pressure may not always be severely elevated; nurses must rely on laboratory values and symptoms.
- Educate staff to monitor patients with preeclampsia for sudden right upper quadrant pain, nausea, or malaise, which may indicate HELLP.
1.2 Pathophysiology
- Endothelial dysfunction leads to microvascular damage.
- Hemolysis occurs due to microangiopathic destruction of RBCs as they pass through narrowed vessels.
- Liver dysfunction is caused by periportal hemorrhage, fibrin deposition, and hepatocellular necrosis.
- Platelet consumption occurs in the formation of microthrombi, causing thrombocytopenia.
- Associated with abnormal placentation, vasospasm, and systemic inflammatory response.
Nursing Insights:
- Nurses must understand that HELLP is part of the preeclampsia spectrum, not a separate disease.
- Continuous monitoring of labs and maternal/fetal status is essential due to rapid deterioration risk.
1.3 Clinical Manifestations
- Common Symptoms:
- Right upper quadrant or epigastric pain.
- Nausea and vomiting.
- Malaise or fatigue.
- Headache and visual disturbances.
- Hypertension may be present but not always.
- Physical Findings:
- Jaundice (from hemolysis).
- Edema.
- Signs of bleeding (petechiae, ecchymosis).
Nursing Insights:
- Monitor for subtle signs of liver dysfunction, such as persistent epigastric pain unrelieved by antacids.
- Assess for bleeding tendencies due to low platelets.
- Educate patient to report sudden headaches, visual changes, or right upper quadrant pain immediately.
1.4 Laboratory Findings
|
Parameter |
Expected Finding in HELLP Syndrome |
Nursing Implications |
|
Hemolysis |
Schistocytes on smear, LDH >600 IU/L, low haptoglobin |
Monitor for anemia, tachycardia, pallor |
|
Liver Enzymes |
AST/ALT >70 IU/L |
Assess for hepatic tenderness, jaundice |
|
Platelets |
<100,000/μL |
Monitor for bleeding, avoid invasive procedures |
|
Bilirubin |
Mildly elevated |
Monitor for jaundice and hemolysis |
|
Urinalysis |
Variable proteinuria |
Assess renal function and risk of preeclampsia |
Nursing Insights:
- Laboratory trends are more important than a single value.
- Frequent monitoring is essential; rapid deterioration can occur within hours.
1.5 Management and Nursing Interventions
- Definitive Treatment: Delivery of the fetus; timing depends on gestational age and maternal/fetal stability.
- Medical Management Prior to Delivery:
- Blood pressure control (Labetalol, Hydralazine, Nifedipine).
- Seizure prophylaxis: Magnesium sulfate.
- Corticosteroids to enhance fetal lung maturity if preterm.
- Platelet transfusion if count <50,000/μL prior to cesarean or invasive procedures.
- Supportive Care:
- Bed rest in left lateral position.
- Monitor input/output, daily weights.
- Oxygen therapy if hypoxia.
- Monitor for complications: DIC, hepatic rupture, renal failure.
Nursing Insights:
- Continuous maternal and fetal monitoring is mandatory.
- Prepare for emergency delivery if signs of deterioration arise.
- Educate patient and family about the seriousness of HELLP syndrome and expected interventions.
- Monitor for magnesium sulfate toxicity: absent deep tendon reflexes, respiratory depression, decreased urine output.
1.6 Maternal and Fetal Complications
- Maternal:
- Disseminated intravascular coagulation (DIC).
- Hepatic rupture or subcapsular hematoma.
- Acute renal failure.
- Pulmonary edema.
- Placental abruption.
- Fetal:
- Preterm birth.
- Intrauterine growth restriction (IUGR).
- Fetal hypoxia.
- Stillbirth.
Nursing Insights:
- Anticipate NICU admission for preterm infants.
- Assess for signs of maternal shock or bleeding.
- Educate parents on potential neonatal complications and need for monitoring.
Eclampsia: Seizure Management And Nursing Care
1.1 Pathophysiology of Seizures
- Eclampsia is defined as the occurrence of tonic-clonic seizures in a woman with preeclampsia, not attributable to other neurological conditions.
- Seizures are caused primarily by cerebral vasospasm, endothelial dysfunction, and increased blood-brain barrier permeability, leading to cerebral edema.
- Cerebral vasospasm results in decreased cerebral perfusion, ischemia, and hypoxia, precipitating neuronal hyperexcitability and seizure activity.
- Endothelial injury triggers microvascular leakage, protein extravasation, and contributes to increased intracranial pressure.
- Magnesium sulfate is used as prophylaxis and treatment because it stabilizes neuronal membranes, acts as a CNS depressant, and reduces neuromuscular excitability.
Nursing Insights
- Nurses must understand that seizures in eclampsia are a medical emergency; rapid recognition and intervention are critical to prevent maternal and fetal morbidity.
- The pathophysiological cascade of vasospasm → edema → ischemia → seizure explains the need for blood pressure control and magnesium therapy.
- Seizure prophylaxis in preeclampsia with severe features reduces the risk of progression to eclampsia by 50–70%.
1.2 Clinical Manifestations
- Prodromal signs: Severe headache, visual disturbances (scotomata, blurred vision), hyperreflexia, epigastric or right upper quadrant pain.
- Seizure characteristics: Tonic-clonic movements, loss of consciousness, possible tongue biting, incontinence.
- Vital signs: Marked hypertension (systolic ≥160 mmHg, diastolic ≥110 mmHg), tachycardia, variable respiratory pattern.
- Laboratory abnormalities: May include hemolysis, elevated liver enzymes, low platelets (HELLP syndrome), and proteinuria.
Nursing Insights
- Early identification of prodromal signs allows for preemptive magnesium sulfate administration to prevent seizure occurrence.
- Monitoring for neurological changes is critical; nurses should document reflexes, level of consciousness, and visual disturbances.
- Maternal and fetal monitoring must be continuous, especially during seizure episodes, to detect hypoxia or fetal distress.
1.3 Nursing Interventions During a Seizure
- Immediate safety measures:
- Position patient on her side (left lateral preferred) to maintain airway and reduce aspiration risk.
- Remove sharp objects from the environment to prevent injury.
- Do not restrain the patient forcefully; allow movements while preventing harm.
- Airway management:
- Maintain patent airway; provide supplemental oxygen if needed.
- Prepare for suctioning if secretions compromise airway.
- Medication administration:
- Administer IV magnesium sulfate as ordered for seizure control.
- Antihypertensives (e.g., labetalol, hydralazine) to control severe hypertension.
- Monitoring:
- Continuous maternal vital signs and fetal heart rate monitoring.
- Assess for trauma, incontinence, and postictal confusion after seizure ends.
Nursing Insights
- Nurses should anticipate and prepare emergency equipment: oxygen, suction, IV access, magnesium sulfate, and antihypertensives.
- Protecting the patient from injury during seizure outweighs all other interventions initially.
- Understanding magnesium sulfate pharmacology (therapeutic range 4–7 mEq/L) allows early recognition of toxicity (loss of reflexes, respiratory depression).
1.4 Post-Seizure Care
- Assess airway, breathing, circulation immediately after seizure termination.
- Reposition patient to left lateral position to optimize placental perfusion.
- Monitor vital signs every 5–15 minutes until stable.
- Evaluate neurological status: level of consciousness, pupil reaction, reflexes.
- Check urine output to monitor renal perfusion and magnesium excretion.
- Assess fetal status: non-stress test, continuous electronic fetal monitoring.
- Document seizure duration, type, medications administered, and maternal/fetal response.
Nursing Insights
- Postictal monitoring is critical for secondary complications, including hypoxia, aspiration, and recurrence of seizure.
- Nurses should anticipate possible progression to HELLP syndrome or multi-organ dysfunction post-seizure.
- Early initiation of IV fluids with caution prevents pulmonary edema in hypertensive patients.
1.5 Prevention and Long-Term Management
- Seizure prophylaxis: IV magnesium sulfate for preeclampsia with severe features.
- Blood pressure control: Labetalol, hydralazine, nifedipine as indicated.
- Patient education: Recognize warning signs (headache, visual changes, epigastric pain), adhere to antihypertensive therapy, and report symptoms immediately.
- Postpartum monitoring: Blood pressure and neurological status for at least 72 hours postpartum; complications can occur after delivery.
- Long-term management: Counsel on future cardiovascular risks, including chronic hypertension and stroke risk.
Nursing Insights
- Nurses must emphasize early recognition and intervention for recurrent preeclampsia in future pregnancies.
- Continuous patient education is necessary for adherence to lifestyle modifications: low-sodium diet, regular prenatal visits, and blood pressure monitoring.
- Follow-up includes renal function and liver enzymes in patients with HELLP syndrome history.
Maternal And Fetal Complications Of Hypertensive Disorders
1.1 Maternal Complications
- Definition: Hypertensive disorders of pregnancy (HDP) encompass a spectrum of conditions including gestational hypertension, preeclampsia, eclampsia, and HELLP syndrome, all of which can significantly affect maternal physiology.
- Acute Maternal Complications:
- Cerebral Complications:
- Cerebral edema, vasospasm, and hemorrhage leading to seizures or stroke.
- Visual disturbances: scotomata, blurred vision, and retinal detachment in severe preeclampsia.
- Nursing Insights: Monitor neurological status continuously, assess deep tendon reflexes, and report sudden changes such as severe headache or visual blurring.
- Cardiovascular Complications:
- Pulmonary edema due to increased vascular permeability and left ventricular dysfunction.
- Severe hypertension (>160/110 mmHg) can precipitate myocardial ischemia.
- Nursing Insights: Assess lung sounds, oxygen saturation, and maintain strict fluid balance. Administer antihypertensives as ordered.
- Renal Complications:
- Acute kidney injury due to glomerular endotheliosis.
- Proteinuria ≥300 mg/24h, elevated serum creatinine.
- Nursing Insights: Monitor urine output hourly, daily weights, and renal laboratory parameters.
- Hepatic Complications:
- HELLP syndrome: hemolysis, elevated liver enzymes (AST, ALT), low platelets (<100,000/mm³).
- Risk of hepatic rupture or subcapsular hematoma.
- Nursing Insights: Monitor right upper quadrant pain, liver function tests, and prepare for emergent interventions.
- Hematologic Complications:
- Thrombocytopenia increases risk of hemorrhage during labor or postpartum.
- Disseminated intravascular coagulation (DIC) can develop.
- Nursing Insights: Monitor CBC, coagulation profiles, and implement bleeding precautions.
- Cerebral Complications:
- Long-Term Maternal Complications:
- Increased risk of chronic hypertension, cardiovascular disease, and renal disease later in life.
- Nursing Insights: Educate patients about lifestyle modification, follow-up blood pressure monitoring, and cardiovascular risk reduction.
1.2 Fetal and Neonatal Complications
- Placental Insufficiency:
- Inadequate uteroplacental perfusion leads to intrauterine growth restriction (IUGR).
- Nursing Insights: Monitor fetal growth via serial ultrasounds and Doppler studies.
- Prematurity:
- Early delivery may be required for maternal/fetal indications, increasing risk for neonatal morbidity.
- Nursing Insights: Administer corticosteroids (e.g., Betamethasone) to enhance fetal lung maturity when preterm birth is anticipated.
- Hypoxia and Acidosis:
- Chronic uteroplacental insufficiency may lead to fetal hypoxemia and acidemia.
- Nursing Insights: Continuous fetal monitoring, non-stress tests, and biophysical profiles are critical.
- Perinatal Mortality:
- Severe preeclampsia/eclampsia increases the risk of stillbirth and neonatal death.
- Nursing Insights: Ensure timely delivery and neonatal resuscitation preparedness.
- Long-Term Neonatal Sequelae:
- Increased risk for neurodevelopmental delays and cardiovascular issues in offspring.
1.3 Long-Term Sequelae for Mother and Child
- Maternal:
- Persisting hypertension, increased risk of ischemic heart disease, stroke, and chronic kidney disease.
- Nursing Insights: Encourage cardiovascular risk assessment, lifestyle modification, and regular follow-up.
- Child:
- Offspring may have low birth weight, developmental delays, and increased susceptibility to hypertension and metabolic syndrome later in life.
- Nursing Insights: Monitor growth and developmental milestones, coordinate pediatric follow-up care.
Summary
Definition and Classification of Hypertensive Disorders in Pregnancy
- Gestational Hypertension
- Blood pressure ≥140/90 mmHg after 20 weeks of gestation without proteinuria.
- No previous history of hypertension prior to pregnancy.
- Usually resolves by 12 weeks postpartum.
- Nursing Insights: Monitor for progression to preeclampsia, teach self-monitoring of blood pressure at home, and encourage rest and lifestyle modifications.
- Preeclampsia
- Blood pressure ≥140/90 mmHg after 20 weeks gestation with proteinuria (≥300 mg/24 hours) or signs of end-organ dysfunction.
- Classified into:
- Without severe features: BP 140–159/90–109 mmHg, mild proteinuria, absence of end-organ damage.
- With severe features: BP ≥160/110 mmHg, severe proteinuria, neurological symptoms (headache, visual changes), epigastric or right upper quadrant pain, pulmonary edema, renal or hepatic dysfunction.
- Nursing Insights: Frequent maternal and fetal monitoring is essential, educate patient about warning signs (headache, visual disturbances, epigastric pain), prepare for potential early delivery.
- Eclampsia
- Onset of seizures in a woman with preeclampsia not attributable to other causes.
- Seizures may occur antepartum, intrapartum, or postpartum.
- Nursing Insights: Priority interventions include airway protection, seizure management with magnesium sulfate, continuous fetal monitoring, and rapid response to maternal complications.
- Chronic Hypertension
- Hypertension present before pregnancy or diagnosed before 20 weeks gestation.
- May coexist with superimposed preeclampsia.
- Nursing Insights: Monitor for maternal complications (stroke, renal failure) and fetal complications (IUGR, preterm birth).
- HELLP Syndrome (Hemolysis, Elevated Liver enzymes, Low Platelets)
- A severe variant of preeclampsia.
- Lab findings:
- Hemolysis: schistocytes, elevated LDH
- Elevated liver enzymes: AST, ALT
- Low platelets: <100,000/μL
- Clinical manifestations: epigastric or right upper quadrant pain, nausea, malaise, possible jaundice.
- Nursing Insights: Monitor for signs of bleeding, prepare for transfusion or early delivery, frequent lab monitoring, assess for liver rupture or DIC.
Pathophysiology
- Abnormal trophoblastic invasion leads to inadequate remodeling of spiral arteries, resulting in poor uteroplacental perfusion.
- Endothelial dysfunction: causes vasoconstriction, platelet aggregation, increased vascular permeability, and end-organ ischemia.
- Anti-angiogenic factors like sFlt-1 inhibit VEGF and placental growth factor, contributing to hypertension and proteinuria.
Clinical Manifestations
|
Feature |
Preeclampsia Without Severe Features |
Preeclampsia With Severe Features |
HELLP Syndrome |
|
BP |
140–159/90–109 mmHg |
≥160/110 mmHg |
Often ≥160/110 mmHg |
|
Proteinuria |
≥300 mg/24 hr |
Severe |
Variable |
|
Edema |
Mild |
Generalized |
Often present |
|
Neurological Symptoms |
Rare |
Headache, visual disturbances |
May occur |
|
GI Symptoms |
Nausea mild |
Epigastric pain |
Severe epigastric/RUQ pain, N/V |
|
Lab Abnormalities |
Mild |
Elevated creatinine, LFTs |
Hemolysis, elevated AST/ALT, thrombocytopenia |
Complications
- Maternal: cerebral hemorrhage, pulmonary edema, renal failure, abruptio placentae, DIC.
- Fetal: IUGR, preterm birth, hypoxia, stillbirth.
Management Principles
- Delivery is the definitive treatment for preeclampsia and HELLP syndrome.
- Seizure prophylaxis: Magnesium sulfate infusion.
- Monitor for toxicity: respiratory rate <12, loss of deep tendon reflexes, decreased urine output.
- Antidote: calcium gluconate.
- Blood pressure control: Labetalol, hydralazine, nifedipine.
- Corticosteroids: Betamethasone for fetal lung maturity if preterm delivery anticipated.
Postpartum Considerations
- Hypertensive disorders may persist or present up to 12 weeks postpartum.
- Monitor BP, urine output, neurological status.
- Patient education on warning signs: headaches, visual changes, epigastric pain, and swelling.
