
Please set your exam date
Abruptio Placentae
Study Questions
Practice Exercise 1
A nurse is assessing a client with suspected abruptio placentae. Which of the following findings requires immediate intervention?
Explanation
Abruptio placentae involves the premature separation of a normally implanted placenta from the uterine wall before delivery. This detachment disrupts the maternal-fetal interface, leading to hemorrhage and impaired gas exchange. Significant placental abruption triggers maternal hypovolemic shock and fetal hypoxia, often manifesting as board-like abdominal rigidity and severe uterine tenderness.
Rationale for correct answer
The presence of maternal hypotension and tachycardia indicates compensated shock or impending circulatory collapse due to concealed or overt hemorrhage. These vital sign changes signal a critical loss of intravascular volume, necessitating rapid fluid resuscitation and potential emergency delivery.
Rationale for incorrect answers
Mild vaginal spotting is frequently associated with early placental separation or other cervical changes. While it requires monitoring, it does not always indicate life-threatening hemorrhage or immediate hemodynamic instability. This finding is less urgent than signs of active shock in the mother.
A fetal heart rate of 140 beats/min with moderate variability is a reassuring finding indicating adequate fetal oxygenation. Moderate variability reflects a healthy fetal nervous system responding to the environment. This does not require immediate intervention as it represents a Category 1 fetal heart rate tracing.
Intermittent uterine contractions are often observed in various stages of pregnancy and can occur with minor placental irritation. In abruptio placentae, the classic finding is uterine hypertonicity or high-frequency, low-amplitude contractions. Intermittent contractions alone do not signal acute distress requiring emergency surgical or medical intervention.
Test-taking strategy
- Identify the clinical urgency: The question asks for an immediate intervention, which directs the nurse to prioritize life-threatening complications.
- Apply ABC principles: Analyze the options for threats to Airway, Breathing, or Circulation.
- Evaluate maternal stability: Choice 3 (Hypotension and tachycardia) directly impacts maternal hemodynamics and indicates a circulatory crisis.
- Rule out stable findings:
- Choice 1 is a common symptom but not an acute emergency compared to shock.
- Choice 2 is a normal physiological response for a fetus.
- Choice 4 describes non-pathological contraction patterns.
- Select the option that indicates physiological instability and requires rapid resuscitation to prevent maternal or fetal mortality.
Take home points
- Abruptio placentae is characterized by painful vaginal bleeding and uterine tenderness.
- Maternal shock can occur even with minimal visible bleeding if the hemorrhage is concealed behind the placenta.
- Immediate intervention is required when vital signs indicate maternal hemodynamic compromise or fetal distress.
- Disseminated intravascular coagulation is a severe potential complication of placental abruption due to the release of thromboplastin.
A nurse assesses a client at 36 weeks gestation with sudden onset of severe abdominal pain and a rigid uterus. Which of the following conditions does the nurse suspect?
Explanation
Abruptio placentae involves the premature separation of a normally implanted placenta from the uterine wall before delivery. This detachment disrupts the maternal-fetal interface, leading to hemorrhage and impaired gas exchange. Significant placental abruption triggers maternal hypovolemic shock and fetal hypoxia, often manifesting as board-like abdominal rigidity and severe uterine tenderness.
Rationale for correct answer
2. The sudden onset of severe abdominal pain accompanied by a rigid uterus is the classic clinical presentation of placental abruption. The rigidity occurs due to extravasation of blood into the myometrium, causing significant uterine irritability and hypertonicity. These findings distinguish this obstetric emergency from other causes of late-pregnancy bleeding.
Rationale for incorrect answers
1. Placenta previa typically presents as painless bleeding in the third trimester of pregnancy. The placenta is implanted over or near the internal os, and it does not typically cause uterine rigidity or severe pain. Physical examination would reveal a soft, non-tender uterus rather than the firm, board-like abdomen seen here.
3. Preterm labor involves regular uterine contractions that result in cervical change before 37 weeks gestation. While contractions can be painful, they are usually intermittent rather than constant and severe. The uterus relaxes between contractions in preterm labor, unlike the sustained hypertonicity observed in a significant abruption.
4. Uterine atony is the failure of the uterus to contract effectively after delivery, leading to postpartum hemorrhage. It is characterized by a soft, boggy uterus upon palpation rather than a rigid one. Because the client in the scenario is still at 36 weeks gestation, atony is not a relevant diagnostic consideration.
Test-taking strategy
- Identify the cardinal signs: The question provides "sudden onset," "severe pain," and "rigid uterus" as the primary data points.
- Contrast painful vs. painless: In obstetric nursing, a major differentiator for third-trimester bleeding is the presence of pain. Abruptio is painful; Previa is painless.
- Assess uterine tone: A "rigid" or "board-like" uterus is a specific indicator of concealed or overt hemorrhage within the uterine wall, ruling out atony or normal labor.
- Apply gestational timing: The client is at 36 weeks, focusing the assessment on antepartum complications rather than postpartum issues like atony.
- Use a rule-out method:
- Rule out 1 because previa lacks severe pain and rigidity.
- Rule out 3 because labor contractions are intermittent and the uterus relaxes.
- Rule out 4 because atony occurs after birth and presents as "boggy," not rigid.
Take home points
- Abruptio placentae is a leading cause of maternal and fetal morbidity characterized by painful bleeding and uterine hypertonicity.
- A rigid, board-like abdomen is a hallmark sign indicating that blood has infiltrated the uterine muscle fibers.
- Management requires immediate assessment of maternal hemodynamic stability and fetal heart rate patterns.
- Distinguishing between placenta previa and abruption is critical, as vaginal exams are contraindicated in suspected previa but not necessarily in abruption.
A nurse is caring for a client with abruptio placentae. Which of the following are clinical manifestations associated with this condition? Select all that apply
Explanation
Abruptio placentae involves the premature separation of a normally implanted placenta from the uterine wall, leading to decidual hemorrhage and compromised fetal oxygenation. The accumulation of blood between the placenta and myometrium causes uterine hypertonicity and severe localized pain. This condition often results in consumptive coagulopathy, specifically disseminated intravascular coagulation, if thromboplastin is released into the maternal circulation from the damaged placental site.
Rationale for correct answers
1. The presence of painful uterine tenderness occurs as blood infiltrates the myometrium, causing significant tissue irritation and nerve stimulation. In abruptio placentae, the pain is often sudden, constant, and severe, distinguishing it from labor. This clinical hallmark results from the physical detachment and subsequent hematoma formation behind the placental plate.
2. A board-like uterine rigidity is a classic sign of a concealed hemorrhage where blood remains trapped within the uterine cavity. This internal pressure causes the uterus to become perpetually firm and unable to relax between contractions. This finding is a critical indicator of maternal hemodynamic risk and potential uterine rupture or ischemia.
4. Fetal heart rate abnormalities occur due to the direct disruption of the placental perfusion and gas exchange interface. As the surface area for nutrient transfer decreases, the fetus may exhibit late decelerations or sustained bradycardia. These abnormal tracings signal acute fetal hypoxia and necessitate immediate medical evaluation for emergency delivery.
Rationale for incorrect answers
3. Painless bright red vaginal bleeding is the defining characteristic of placenta previa, not abruptio placentae. In previa, the placenta is located over the cervical os, and bleeding occurs without the significant muscular irritation or hypertonicity seen in abruption. Identifying the absence of pain is a primary diagnostic step in differentiating between these two major causes of third-trimester bleeding.
5. A soft, non-tender uterus is the expected physical finding in a normal pregnancy or in a client with placenta previa. In contrast, abruptio placentae causes the uterus to become extremely irritable and firm to the touch. Finding a soft uterus effectively rules out the diagnosis of a significant placental separation where blood has accumulated within the myometrium.
Test-taking strategy
- Identify the Main Idea: The question focuses on the clinical manifestations of abruptio placentae, which is a "painful" obstetric emergency.
- Differentiate Pathophysiology: Contrast Abruption (premature separation, painful, rigid) with Previa (abnormal implantation, painless, soft).
- Categorize Symptoms:
- Uterine Tone: Look for terms like rigid, firm, or hypertonic (Choices 1 and 2).
- Pain Status: Select painful clinical findings over painless ones (Rule out Choice 3).
- Fetal Impact: Recognize that any placental separation compromises fetal oxygenation (Choice 4).
- Rule out the "Normals": A soft, non-tender uterus (Choice 5) is inconsistent with the internal bleeding and pressure associated with abruption.
- Selection: Choose all options that align with the inflammatory and hemorrhagic nature of placental detachment.
Take home points
- Abruptio placentae presents with the triad of abdominal pain, uterine rigidity, and vaginal bleeding.
- Uterine rigidity, often described as board-like, indicates a concealed hemorrhage with high internal pressure.
- Fetal distress is a common and early complication due to reduced uteroplacental blood flow.
Maternal vital signs must be monitored closely for signs of shock, even if external bleeding appears minimal.
A nurse explains abruptio placentae to a client. Which of the following best describes the primary cause of bleeding in this condition?
Explanation
Abruptio placentae involves the premature separation of a normally implanted placenta from the uterine wall before delivery. This detachment disrupts the maternal-fetal interface, leading to hemorrhage and impaired gas exchange. Significant placental abruption triggers maternal hypovolemic shock and fetal hypoxia, often manifesting as board-like abdominal rigidity and severe uterine tenderness.
Rationale for correct answer
2. The primary cause of bleeding is the mechanical detachment of the placenta from the decidua basalis. This separation causes rupture of the maternal spiral arteries, leading to hemorrhage into the retroplacental space. This specific disruption of the vascular attachment directly results in the clinical manifestations of abruption.
Rationale for incorrect answers
1. Placental implantation over the cervical os describes placenta previa, which is a distinct clinical entity from abruptio placentae. While both cause third-trimester bleeding, previa is characterized by painless hemorrhage due to the placenta's low-lying position. This anatomical malposition does not involve the premature detachment of a normally situated placenta.
3. Rupture of fetal blood vessels is the pathophysiology of vasa previa, where unprotected fetal vessels cross the internal os. In abruptio placentae, the bleeding is primarily maternal in origin from the decidua basalis vessels. Fetal vessel rupture causes rapid fetal exsanguination, which is a different mechanism than placental separation.
4. Degeneration of uterine fibroids, or leiomyomas, can cause localized pain and discomfort during pregnancy but is not a cause of placental hemorrhage. Fibroids are benign tumors of the myometrium that do not typically interfere with the structural integrity of the placental-uterine attachment. This condition does not result in the board-like rigidity seen in abruption.
Test-taking strategy
- Define the core pathology: The term "abruption" literally means to break off or tear away, which identifies separation as the key mechanism.
- Differentiate between placental emergencies: Distinguish between implantation errors (previa) and detachment errors (abruption) to eliminate Choice 1.
- Identify vascular source: Recognize that the hemorrhage in abruption stems from the maternal side (maternal spiral arteries) of the placenta-uterine interface rather than fetal vessels.
- Eliminate unrelated gynecological issues: Rule out Choice 4 as it describes a myometrial growth rather than a primary placental-vascular event.
- Focus on the anatomical disruption: Select the option that correctly describes the physical tearing of the placenta from its site of attachment.
Take home points
- Abruptio placentae is the premature separation of the placenta from the uterine wall after 20 weeks gestation.
- The primary pathology is the rupture of maternal spiral arteries in the decidua basalis.
- Clinical indicators include painful vaginal bleeding, uterine tenderness, and abdominal rigidity.
- Risk factors include maternal hypertension, abdominal trauma, cocaine use, and cigarette smoking.
A nurse is differentiating concealed from revealed abruptio placentae. Which findings are most consistent with concealed hemorrhage? Select all that apply
Explanation
Placental abruption with concealed hemorrhage involves blood trapped behind the placenta without egress through the cervix. This internal sequestration triggers retroplacental hematoma formation, leading to severe myometrial irritation and intravascular depletion despite absent external flow. Consumers of this condition often develop disseminated intravascular coagulation due to the massive release of tissue thromboplastin into the maternal venous circulation.
Rationale for correct answers
1. In a concealed abruption, the blood is trapped between the detached placenta and the uterine wall. Consequently, the nurse will observe minimal bleeding or even a total absence of vaginal discharge despite significant internal blood loss. This discrepancy often delays the diagnosis of life-threatening maternal hypovolemia.
2. Rapid maternal hypotension occurs because significant blood volume is lost into the retroplacental space rather than exiting the body. This occult blood loss leads to decreased cardiac output and systemic circulatory collapse. The nurse must monitor for tachycardia and narrow pulse pressures even when external bleeding is not visible.
4. Increasing fundal height is a definitive sign that the uterus is expanding to accommodate an accumulating internal hematoma. As blood fills the uterine cavity, the uterine fundus rises higher than expected for the current gestational age. This measurement provides an indirect quantification of the volume of concealed blood trapped within.
5. Board-like uterine rigidity results from blood infiltrating the uterine muscle fibers, a phenomenon known as Couvelaire uterus. The trapped blood causes intense muscular irritability and sustained hypertonicity. The uterus feels wood-like or exceptionally firm upon palpation and fails to relax, reflecting severe internal pressure.
Rationale for incorrect answers
3. A soft uterine tone is characteristic of a normal pregnancy or placenta previa, not abruptio placentae. In any significant abruption, the uterus becomes highly irritable and hypertonic due to the presence of retroplacental blood. Finding a soft uterus would effectively rule out the diagnosis of a concealed hemorrhage where internal pressure is high.
Test-taking strategy
- Analyze the Subtype: The question specifically asks for "concealed" abruption findings, which requires focusing on "hidden" blood loss versus "revealed" (visible) bleeding.
- Identify Internal Expansion Signs: Look for clinical indicators that the uterus is filling with fluid, such as increasing fundal height (Choice 4).
- Evaluate Uterine Response: Trapped blood acts as a severe irritant to the myometrium; therefore, the uterus must be rigid or board-like (Choice 5) rather than soft (Rule out Choice 3).
- Prioritize Systemic Stability: Recognize that the body reacts to intravascular volume loss regardless of whether the blood is visible. This justifies selecting hypotension (Choice 2) as a sign of hidden shock.
- Recognize the Paradox: Understand that in concealed cases, the severity of shock is often disproportionate to the amount of visible vaginal bleeding (Choice 1).
Take home points
- Concealed abruptio placentae is characterized by hidden retroplacental hemorrhage that does not escape through the vagina.
- The clinical triad for concealed abruption includes increasing fundal height, board-like uterine rigidity, and signs of shock.
- The absence of heavy vaginal bleeding does not exclude a diagnosis of severe placental abruption or maternal instability.
- Couvelaire uterus occurs when blood infiltrates the myometrium, leading to a purple discoloration and loss of contractile ability.
Practice Exercise 2
A nurse is assessing a client with a suspected placental abruption. Which of the following maternal conditions is most consistently associated with an increased risk for this complication?
Explanation
Abruptio placentae involves the premature separation of a normally implanted placenta from the uterine wall. Pathologically, it results from vascular degeneration of the decidua basalis maternal spiral arteries. This leads to decidual hemorrhage and hematoma formation, which mechanically detaches the placental plate. Risk factors include advanced maternal age, cocaine use, and abdominal trauma.
Rationale for correct answer
2. Chronic hypertension is the most significant and consistent risk factor for placental abruption. The chronic vasospastic process leads to degenerative changes in the spiral arteries, making them prone to rupture. This underlying vascular pathology compromises the integrity of the maternal-fetal interface, leading to detachment.
Rationale for incorrect answers
1. Hypothyroidism does not directly cause the vascular compromise required for placental detachment. While untreated thyroid disorders can lead to various obstetric complications like miscarriage or preterm birth, they lack the specific vasoconstrictive mechanism seen in abruption. It is not considered a primary risk factor for this acute emergency.
3. Gestational diabetes primarily affects fetal growth and metabolic stability rather than the structural attachment of the placenta. This condition is more closely linked to macrosomia and neonatal hypoglycemia than to premature separation. There is no direct pathophysiological link between maternal hyperglycemia and decidual artery rupture.
4. Iron deficiency anemia results in reduced hemoglobin levels but does not cause the vascular friability associated with abruption. While severe anemia may complicate the maternal response to hemorrhage, it is not an etiological factor for the abruption itself. It primarily influences oxygen-carrying capacity rather than uterine-placental adherence.
Test-taking strategy
- Identify the pathophysiological link: Recognize that abruptio placentae is essentially a vascular accident.
- Connect the dots: Look for the condition among the choices that is characterized by vasoconstriction and vessel damage.
- Rule out metabolic/nutritional issues: Eliminate gestational diabetes (Choice 3) and anemia (Choice 4) as they do not primarily cause arterial degeneration.
- Focus on hypertensive disorders: Recall that hypertension (chronic or gestational) is the single most common cause of non-traumatic abruption.
- Select the high-risk vascular condition: Choice 2 is the only option that directly impacts the health of the maternal spiral arteries.
Take home points
- Hypertension is the leading cause of placental abruption due to chronic vascular stress on the decidual arteries.
- Pathophysiological separation occurs because of retroplacental bleeding within the decidua basalis.
- Abruption can lead to significant maternal complications including DIC and hypovolemic shock.
- Assessment should focus on sudden onset of abdominal pain, uterine tenderness, and fetal distress.
A client at 36 weeks gestation presents with a sudden onset of severe, constant abdominal pain and a rigid, board-like abdomen. Dark red vaginal bleeding is noted. Which of the following conditions does the nurse suspect?
Explanation
Abruptio placentae involves the premature separation of a normally implanted placenta from the uterine wall before delivery. This detachment disrupts the maternal-fetal interface, leading to hemorrhage and impaired gas exchange. Significant placental abruption triggers maternal hypovolemic shock and fetal hypoxia, often manifesting as board-like abdominal rigidity and severe uterine tenderness.
Rationale for correct answer
2. The clinical triad of sudden severe pain, dark red bleeding, and uterine rigidity is pathognomonic for placental abruption. Separation causes blood to infiltrate the myometrium, resulting in a board-like abdomen and high resting tone. This condition requires immediate stabilization to prevent maternal disseminated intravascular coagulation or fetal demise.
Rationale for incorrect answers
1. Placenta previa is characterized by painless bleeding that is typically bright red rather than dark. The uterus remains soft and non-tender because the pathology involves abnormal implantation near the cervical os rather than premature detachment. Rigidity and severe constant pain are absent in classic cases of previa.
3. Preterm labor involves rhythmic, intermittent contractions that lead to cervical effacement and dilation before 37 weeks. While labor is painful, the uterus relaxes completely between contractions, unlike the sustained hypertonicity of an abruption. There is typically no board-like rigidity or significant dark red hemorrhage in uncomplicated labor.
4. Uterine atony refers to a lack of muscular tone in the uterus, but it occurs after delivery. It is the leading cause of postpartum hemorrhage and presents as a boggy uterus on palpation. Because this client is still pregnant at 36 weeks, atony is not a possible antepartum diagnosis.
Test-taking strategy
- Identify Cardinal Signs: Focus on the descriptors "severe, constant pain" and "rigid, board-like abdomen" which are specific to placental separation.
- Differentiate by Pain Status: Use the classic distinction that Abruptio is painful and Previa is painless to narrow the choices.
- Assess Uterine Tone: Eliminate options that involve a soft or boggy uterus, as "board-like" implies hypertonicity or internal hemorrhage.
- Timing of the Event: Recognize that Uterine Atony is a postpartum complication, making it irrelevant for a client at 36 weeks gestation.
- Use Pathophysiological Logic: Select the condition where blood acts as a muscle irritant, causing the sustained contraction and pain described in the stem.
Take home points
- Abruptio placentae is the premature detachment of the placenta and is a leading cause of third-trimester painful bleeding.
- A board-like, rigid abdomen indicates concealed or overt hemorrhage into the uterine musculature.
- Maternal hypertension and abdominal trauma are the most significant risk factors for this obstetric emergency.
- Management focuses on rapid fluid resuscitation, monitoring for coagulopathy, and assessing fetal well-being for emergency delivery.
A nurse is caring for a client who experienced blunt abdominal trauma following a motor vehicle accident. Which of the following assessment findings would suggest a concealed abruptio placentae? Select all that apply
Explanation
Concealed abruptio placentae involves the premature separation of the placenta where blood remains sequestered behind the placental plate. This internal hemorrhage creates a retroplacental hematoma, increasing intrauterine pressure and causing the myometrium to become engorged. The resulting uterine hypertonicity and distension lead to severe maternal pain and rapid fetal compromise due to impaired placental perfusion and maternal hypovolemia.
Rationale for correct answers
1. An increase in fundal height measurement occurs because the blood is trapped within the uterine cavity, causing the organ to expand internally. As the hematoma grows, the uterine volume increases, manifesting as a fundal height that is larger than expected for the current gestational age.
3. Persistent late decelerations reflect uteroplacental insufficiency caused by the detachment of the placental surface from the uterine wall. The reduction in functional surface area impairs oxygen transfer, leading to fetal hypoxia and the characteristic delayed deceleration pattern following uterine contractions.
4. A uterine resting tone of 25 mmHg indicates uterine hypertonicity, as a normal resting tone is typically ≤ 10 to 12 mmHg. The accumulation of blood within the myometrium prevents the muscle from relaxing completely, resulting in a sustained elevation of intrauterine pressure measured by an internal catheter.
5. Sudden, agonizing abdominal tenderness is the result of blood infiltrating the uterine muscle and the rapid distension of the uterine serosa. In concealed abruption, this exquisite tenderness is often constant and disproportionate to the amount of visible bleeding, signaling a severe internal injury.
Rationale for incorrect answers
2. Profuse, bright red vaginal discharge is a finding associated with revealed abruption or placenta previa, not concealed abruption. By definition, a concealed abruption involves trapped blood that does not escape through the cervix. The nurse would instead observe minimal to no vaginal bleeding despite clinical signs of maternal shock.
Test-taking strategy
- Define the Subtype: The question specifies "concealed" abruption, which means the nurse must look for signs of internal accumulation rather than external discharge.
- Analyze Uterine Changes: Trapped blood acts as a physical mass; therefore, the nurse should expect the uterus to grow (increased fundal height) and become unable to relax (elevated resting tone).
- Prioritize Fetal Response: Any placental separation, whether hidden or visible, compromises the oxygen supply, making fetal distress signs like late decelerations a priority.
- Differentiate Pain Profiles: Focus on the inflammatory nature of blood in the muscle; this leads to "agonizing" pain and rigidity rather than the painless nature of other obstetric conditions.
- Rule Out Visible Clues: In a "concealed" scenario, "profuse" bleeding (Choice 2) is the exact opposite of the pathophysiological mechanism being tested.
Take home points
- Concealed abruption is a hidden obstetric emergency where blood collects behind the placenta without external bleeding.
- The hallmark signs include increasing fundal height, uterine hypertonicity, and severe, constant abdominal pain.
- Fetal heart rate patterns, specifically late decelerations, are sensitive indicators of the severity of the placental separation.
- Blunt trauma is a high-risk trigger for abruption and necessitates at least 4 hours of continuous fetal monitoring.
A nurse is caring for a client with a suspected abruptio placentae. The client's blood pressure is 102/64 mm Hg and the pulse is 112 beats/minute. There is no visible vaginal bleeding. Which of the following actions is the priority for the nurse to perform?
Explanation
Abruptio placentae involves the premature separation of the decidua basalis from the uterine wall. This obstetric emergency triggers concealed hemorrhage, leading to retroplacental hematoma formation and potential consumptive coagulopathy or disseminated intravascular coagulation.
Rationale for correct answers
3. In cases of concealed abruption, an increasing fundal height indicates internal bleeding within the uterine cavity. The nurse must monitor for uterine retroplacental hematoma expansion, which manifests as a rising fundus and board-like abdominal rigidity.
Rationale for incorrect answers
1. Performing a sterile digital vaginal exam is strictly contraindicated until placenta previa is ruled out via ultrasonography. Manual manipulation of the cervix can exacerbate maternal hemorrhage or trigger massive bleeding if the placental location is low-lying.
2. While a wedge prevents supine hypotension, it does not address the priority assessment of occult maternal hemorrhage. The client exhibits tachycardia and borderline hypotension, indicating hypovolemic shock from blood loss that is not visible externally.
4. Amniocentesis is not indicated for the management of suspected placental abruption and may delay emergency intervention. This procedure carries risks of further placental trauma and is irrelevant for assessing acute hemorrhage or fetal distress.
Test-taking strategy
- Identify the Core Issue: The client presents with signs of hypovolemic shock (tachycardia 112 beats/minute, low blood pressure 102/64 mm Hg) despite having no visible vaginal bleeding. This indicates concealed abruption.
- Prioritization Framework: Use the nursing process (Assessment before Implementation). Options 1, 2, and 4 are interventions, while 3 is an assessment.
- Evaluate Assessments: Determining fundal height is the specific assessment used to detect occult bleeding in the uterus when external bleeding is absent.
- Eliminate Contraindications: Rule out Option 1 immediately, as vaginal exams are dangerous in late-pregnancy bleeding of unknown origin.
- Assess Clinical Relevance: Rule out Option 4 as it is a diagnostic tool for genetic or lung maturity, not acute trauma. Rule out Option 2 as a supportive measure that does not provide diagnostic data on the bleeding.
Take home points
- Concealed abruptio placentae is characterized by a firm, board-like abdomen and rising fundal height due to internal hematoma.
- Clinical signs of hypovolemic shock like tachycardia and hypotension may precede visible blood loss in placental abruption.
- Vaginal examinations are avoided in any pregnant client with third-trimester bleeding until the placental location is confirmed by ultrasound.
- Definitive management of severe abruption often requires rapid hemodynamic stabilization followed by emergency cesarean delivery.
A nurse is teaching a client about risk factors for abruptio placentae. Which of the following statements by the client indicates a correct understanding of the teaching?
Explanation
Abruptio placentae involves the premature separation of the placental attachment from the uterine decidua prior to delivery. This pathological detachment results from vascular disruption and hemorrhage into the decidua basalis, often secondary to chronic hypertension, vasoconstrictive substances, or sudden intrauterine pressure changes.
Rationale for correct answers
2. Tobacco use causes localized arteriolar vasoconstriction and placental hypoxemia, which compromises the integrity of the decidual vessels. Chronic exposure to nicotine and carbon monoxide leads to placental vascular insufficiency, significantly elevating the statistical risk for spontaneous detachment.
Rationale for incorrect answers
1. Fetal macrosomia, or having a large baby, is typically associated with gestational diabetes rather than placental abruption. While uterine overdistension from polyhydramnios or multifetal gestation is a risk, a simple history of macrosomic infants is not a primary etiology.
3. A previous cesarean delivery is a significant risk factor for both placenta previa and abruptio placentae. Uterine scarring alters subsequent placental implantation and endometrial vascularization, making the placenta more susceptible to separation during the current pregnancy or subsequent labors.
4. Moderate exercise is generally encouraged during pregnancy and does not trigger placental detachment through an elevated heart rate. The actual physical risk factors involve direct abdominal trauma or sudden uterine decompression, rather than the physiological cardiovascular changes associated with routine aerobic activity.
Test-taking strategy
- Analyze the Question: The goal is to identify a correct risk factor for abruptio placentae from the client's perspective.
- Identify Modifiable Risks: Tobacco use is a well-documented behavioral risk factor. The vasoconstrictive properties of nicotine directly impact placental perfusion and uterine health.
- Evaluate Clinical History: Acknowledge that while uterine scarring (from cesareans) affects placental health, the client's statement in choice 3 incorrectly limits the risk to only placenta previa.
- Eliminate Misconceptions: Rule out exercise (choice 4) as the cause of abruption, as normal maternal tachycardia does not disrupt placental adherence.
- Differentiate Pathologies: Distinguish between risk factors for metabolic issues like macrosomia (choice 1) and vascular emergencies like abruption.
Take home points
- Hypertension, including chronic and gestational types, remains the most prevalent risk factor for placental abruption.
- Substance use involving tobacco or cocaine causes significant vascular damage and ischemia within the decidua basalis.
- Sudden uterine decompression, such as after the rupture of membranes in polyhydramnios, can mechanically trigger placental separation.
- Prior history of abruptio placentae increases the recurrence risk in subsequent pregnancies by approximately 10 to 15 percent.
Practice Exercise 3
A nurse is caring for a client with suspected abruptio placentae. Which of the following laboratory tests is the most essential for the nurse to monitor to detect the onset of Disseminated Intravascular Coagulation (DIC)?
Explanation
Abruptio placentae triggers systemic pathological coagulation through the release of tissue thromboplastin from the traumatized decidua into maternal circulation. This initiates a cascade of consumptive coagulopathy where massive microvascular thrombi deplete platelets and clotting factors, leading to widespread hemorrhagic diathesis and organ dysfunction.
Rationale for correct answers
2. Monitoring the coagulation profile, specifically prothrombin time, activated partial thromboplastin time, and fibrinogen levels, is critical for diagnosing secondary DIC. A decrease in fibrinogen < 150 mg/dL and elevated fibrin degradation products indicate the exhaustion of the maternal clotting reservoir during placental separation.
Rationale for incorrect answers
1. Serum glucose levels are unrelated to the acute hematological disruption seen in placental abruption or the subsequent clotting cascade failure. While hyperglycemia may occur under general physiological stress, it provides no diagnostic value for detecting intravascular coagulation or maternal-fetal hemorrhage risk.
3. Liver function tests assess hepatic enzyme levels like aspartate aminotransferase and alanine aminotransferase, which are more relevant to preeclampsia syndromes like HELLP. While the liver synthesizes clotting factors, these tests do not track the acute consumption of fibrinogen or platelets during abruption.
4. Thyroid stimulating hormone panels evaluate endocrine function and the metabolic status of the thyroid gland rather than hematological stability. This laboratory assessment has no clinical utility in the emergency management of abruptio placentae or the detection of acute consumptive coagulopathy.
Test-taking strategy
- Identify the Complication: The question asks how to monitor for Disseminated Intravascular Coagulation (DIC) in the context of abruptio placentae.
- Understand DIC Pathophysiology: Recognize that DIC is a hematological emergency characterized by the rapid consumption of clotting factors and platelets.
- Select Specific Markers: Focus on laboratory values that directly measure clotting ability. Fibrinogen and platelets are the most sensitive markers in obstetric DIC.
- Rule out Irrelevant Systems: Eliminate metabolic (glucose), endocrine (TSH), and chronic hepatic (LFTs) tests as they do not address the acute vascular crisis.
- Prioritize Life-Threatening Data: In an abruption, the risk of maternal exsanguination is high; therefore, coagulation profiles are the most essential data points for immediate clinical decision-making.
Take home points
- Abruptio placentae is a leading cause of DIC in pregnancy due to the release of tissue factor into the maternal bloodstream.
- Laboratory findings in DIC include prolonged bleeding times, decreased fibrinogen, decreased platelets, and elevated D-dimer.
- Clinical manifestations of DIC include bleeding from venipuncture sites, petechiae, hematuria, and oozing from mucous membranes.
- Immediate management requires addressing the underlying cause (delivery of the fetus) and replacing depleted blood components and clotting factors.
A client with suspected abruptio placentae develops signs of systemic bleeding. Which of the following laboratory findings would the nurse expect to be consistent with Disseminated Intravascular Coagulation (DIC)?
Explanation
Abruptio placentae initiates a massive release of tissue thromboplastin into the maternal venous system, catalyzing the conversion of prothrombin to thrombin. This triggers an uncontrolled systemic proteolysis where the exhaustion of clotting factors and platelets occurs simultaneously with excessive fibrinolysis, resulting in microvascular thrombosis and subsequent multi-organ ischemia.
Rationale for correct answers
3. In DIC, fibrinogen levels drop significantly below the normal pregnancy range (300 to 600 mg/dL) as it is rapidly converted to fibrin to form widespread microclots. A fibrinogen level < 150 mg/dL is a hallmark of consumptive coagulopathy, directly increasing the risk of spontaneous maternal exsanguination.
Rationale for incorrect answers
1. A nurse would expect a thrombocytopenia, or decreased platelet count, rather than an increase. Platelets are consumed in the formation of thousands of microscopic thrombi throughout the vasculature, leaving the systemic circulation depleted and unable to maintain primary hemostasis at injury sites.
2. The prothrombin time (PT) and activated partial thromboplastin time (aPTT) would be prolonged, not decreased. A decrease would imply a hypercoagulable state, whereas DIC causes a prolonged duration for clot formation due to the depletion of essential circulating coagulation factors and plasma proteins.
4. Hemoglobin and hematocrit typically decrease in the presence of systemic bleeding and retroplacental hemorrhage. An increase in these values would suggest hemoconcentration, but in acute abruptio placentae with DIC, hemodilution or frank blood loss leads to a rapid decline in red cell indices.
Test-taking strategy
- Identify the Pathological State: The question asks for laboratory findings specific to Disseminated Intravascular Coagulation (DIC).
- Apply Concept of Consumption: Recognize that DIC is a "consumption" disease. Therefore, most "building blocks" of a clot (platelets, fibrinogen, factors) will be decreased in laboratory results.
- Analyze Timing Indicators: Realize that tests measuring the time it takes to clot (PT, aPTT) will be increased because the necessary factors are missing.
- Rule out Normal Responses: Hemoglobin/hematocrit (choice 4) will drop during any major bleed, but they are not specific biomarkers for the coagulation cascade failure of DIC itself.
- Eliminate Opposite Trends: Rule out choice 1 and 2 because they describe a hypercoagulable or normal state, which contradicts the "bleeding" presentation mentioned in the stem.
Take home points
- DIC is a secondary complication where the body's clotting mechanisms become overactive and then exhausted.
- Key laboratory indicators of DIC include decreased fibrinogen, decreased platelets, and elevated fibrin split products (D-dimer).
- Prothrombin time (PT) and partial thromboplastin time (PTT) are prolonged due to the depletion of clotting factors.
- Clinical monitoring must include assessing for "oozing" at IV sites, gums, and the surgical site, as these are early signs of coagulopathy.
A nurse is reviewing the plan of care for a client admitted with a potential concealed placental abruption. Which of the following diagnostic actions should the nurse anticipate? Select all that apply
Explanation
Abruptio placentae is the pathological detachment of the placenta from the uterine wall prior to the second stage of labor. This separation triggers thromboplastin release into the maternal circulation, leading to concealed or overt hemorrhage and potential consumptive coagulopathy.
Rationale for correct answers
1. A transvaginal ultrasound is the primary diagnostic tool used to perform a differential diagnosis between abruption and placenta previa. Although ultrasound has low sensitivity for detecting the abruption itself, ruling out a low-lying placenta is mandatory before any manual cervical manipulation.
2. A STAT fibrinogen level is essential to screen for consumptive coagulopathy and impending disseminated intravascular coagulation. In severe abruption, fibrinogen is rapidly depleted to form retroplacental clots, and levels below 150 mg/dL indicate a critical risk for systemic maternal hemorrhage.
4. Serial complete blood counts (CBC) allow the medical team to track hemodynamic stability and the extent of concealed blood loss. A declining hematocrit reflects active hemorrhage, even when external vaginal bleeding is absent, guiding the necessity for blood product transfusion and emergency delivery.
Rationale for incorrect answers
3. While MRI can visualize a retroplacental hematoma, it is not a standard or practical diagnostic action in an acute obstetric emergency. The time required for imaging is prohibitive, as immediate delivery is often necessitated by maternal instability or a non-reassuring fetal heart rate.
5. Umbilical artery Doppler velocimetry is a diagnostic tool primarily used to assess placental insufficiency in chronic conditions like fetal growth restriction. It is not indicated for the acute management of abruptio placentae, where continuous electronic fetal monitoring is the gold standard for assessment.
Test-taking strategy
- Analyze the Question Type: This is a Select all that apply (SATA) question regarding the diagnostic workup for an acute obstetric emergency.
- Identify the Priority: The priority is to assess for maternal hemorrhage (occult or overt) and rule out other causes of third-trimester bleeding.
- Evaluate Laboratory Needs: Because abruption is a common trigger for DIC, laboratory tests that evaluate clotting (like fibrinogen) are always anticipated.
- Assess Imaging Utility: Contrast the speed and utility of ultrasound (fast, rules out previa) against MRI (slow, impractical for emergencies).
- Differentiate Chronic vs. Acute: Recognize that Doppler studies are for chronic growth monitoring, whereas abruption requires immediate assessment of blood volume and clotting status.
Take home points
- Ultrasound is utilized in third-trimester bleeding primarily to rule out placenta previa rather than to confirm an abruption.
- Fibrinogen levels are a more sensitive indicator of the severity of placental abruption than traditional coagulation times (PT/aPTT).
- Concealed abruption must be suspected when maternal vital signs indicate shock despite the absence of visible vaginal bleeding.
- The Kleihauer-Betke test may also be anticipated to detect the presence of fetal erythrocytes in maternal circulation.
A nurse is assessing a client at 32 weeks gestation with severe abdominal pain. The primary health care provider states that the ultrasound did not show any evidence of a retroplacental clot. Which of the following responses by the nurse is most appropriate?
Explanation
Abruptio placentae is the premature separation of the placenta from the uterine decidua. This condition often results in concealed hemorrhage, where blood is trapped between the placenta and the uterine wall, making it undetectable via traditional imaging modalities. Clinical diagnosis relies on uterine tenderness and hypertonicity.
Rationale for correct answers
2. Ultrasonography has a low sensitivity (approximately 25% to 50%) for detecting acute placental abruption. The nurse must prioritize clinical findings such as abdominal pain and uterine rigidity over negative imaging results to ensure maternal and fetal safety.
Rationale for incorrect answers
1. Discharging the client based solely on a negative ultrasound is dangerous and represents medical negligence. In the presence of severe abdominal pain at 32 weeks, the risk of fetal distress or maternal hemorrhage necessitates inpatient observation and continuous monitoring.
3. Repeating ultrasounds every 30 minutes is clinically inefficient and delays definitive management. Diagnostic focus should shift from imaging to hemodynamic assessment and electronic fetal monitoring, as retroplacental clots may never become clearly visible on a standard ultrasound.
4. Attributing severe abdominal pain to Braxton-Hicks contractions is a significant diagnostic error. Braxton-Hicks are typically painless and irregular, whereas the pain from abruption is constant, severe, and associated with uterine hypertonicity, regardless of what the imaging suggests.
Test-taking strategy
- Evaluate Imaging Reliability: Recognize that in obstetrics, ultrasound is excellent for ruling out placenta previa but unreliable for ruling out abruptio placentae.
- Prioritize Clinical Presentation: When a client presents with "severe abdominal pain" (a classic symptom of abruption), the nurse must trust the clinical signs over a negative diagnostic test.
- Eliminate Unsafe Actions: Rule out discharge (choice 1) and misattribution of pain (choice 4) as they ignore potential emergencies.
- Identify Appropriate Nursing Judgment: Choice 2 demonstrates the correct understanding of the limitations of medical technology and the necessity of ongoing clinical vigilance.
- Assess Resource Utility: Rule out choice 3 as frequent repetition of an insensitive test does not change the clinical priority of stabilizing the patient.
Take home points
- A negative ultrasound does not exclude the diagnosis of abruptio placentae because clots can be isoechoic with the placenta.
- Clinical diagnosis of abruption is based on the triad of abdominal pain, uterine tenderness, and vaginal bleeding (if overt).
- Continuous electronic fetal monitoring is essential to detect early signs of fetal hypoxia resulting from decreased placental perfusion.
- Abruptio placentae is a leading cause of maternal and fetal morbidity and requires immediate stabilization and possible emergency delivery.
A nurse is caring for a client with a fibrinogen level of 90 mg/dL following a premature placental separation. Which of the following clinical findings should the nurse monitor for most closely?
Explanation
Disseminated intravascular coagulation involves systemic microvascular thrombosis and subsequent factor exhaustion. This results in pathological consumption of fibrinogen, causing the maternal plasma concentration to drop below the critical threshold of 150 mg/dL. Consequently, the client develops hemorrhagic diathesis, manifesting as uncontrolled bleeding from minor trauma sites or mucosal surfaces.
Rationale for correct answers
2. A fibrinogen level of 90 mg/dL is significantly below the normal range (200 to 400 mg/dL) and indicates consumptive coagulopathy. The nurse must monitor for venipuncture oozing because the body lacks sufficient clotting factors to maintain primary and secondary hemostasis at invasive access points.
Rationale for incorrect answers
1. Increased urine output is not expected in the setting of acute blood loss and pathological clotting. The nurse should instead anticipate oliguria (output < 30 mL/hour) as a result of decreased renal perfusion from hypovolemic shock or microthrombi obstructing the glomerular capillaries.
3. Maternal blood pressure typically decreases, not increases, as a result of hemorrhagic shock. Rapidly increasing blood pressure is a hallmark of preeclampsia, whereas placental abruption complicated by DIC leads to circulatory collapse and hypotension once compensatory mechanisms like peripheral vasoconstriction fail.
4. Sudden, bright red, and painless vaginal bleeding is the classic presentation of placenta previa, not abruptio placentae. Abruption usually causes painful bleeding or concealed hemorrhage with uterine rigidity, and the development of DIC suggests a more severe, systemic disruption of the coagulation profile.
Test-taking strategy
- Analyze the Laboratory Value: Recognize that a fibrinogen level of 90 mg/dL is critically low (normal is 200 to 400 mg/dL).
- Connect Data to Complication: Associate low fibrinogen and premature placental separation with Disseminated Intravascular Coagulation (DIC).
- Identify Clinical Manifestations: In DIC, look for signs of spontaneous bleeding. The "oozing" from IV sites is a classic, early clinical indicator of factor depletion.
- Rule out Distractors: Eliminate choice 4 because "painless" bleeding contradicts the pain associated with abruption. Eliminate choice 3 as hypotension is the expected trend in hemorrhage.
- Prioritize Assessment: Choose the finding that directly reflects the coagulation failure indicated by the laboratory result provided in the stem.
Take home points
- Fibrinogen levels below 100 to 150 mg/dL in a pregnant client are highly suggestive of severe placental abruption and DIC.
- DIC causes bleeding from multiple sites including the gums, nose, gastrointestinal tract, and any existing surgical or IV sites.
- Treatment involves the administration of cryoprecipitate or fresh frozen plasma to replace fibrinogen and other clotting factors.
- Accurate intake and output monitoring is essential to detect renal failure caused by microvascular thrombi in the kidneys.
Practice Exercise 4
A nurse is monitoring a client with abruptio placentae who has developed Disseminated Intravascular Coagulation (DIC). Which of the following clinical signs should the nurse prioritize for monitoring?
Explanation
Disseminated intravascular coagulation is a pathological consumption of clotting factors secondary to the systemic release of tissue thromboplastin. This leads to intravascular microthrombi formation and subsequent widespread fibrinolysis, causing multi-organ dysfunction and profound hemorrhagic diathesis. Maternal plasma fibrinogen typically drops below 150 mg/dL during this acute coagulopathy cascade.
Rationale for correct answers
2. The nurse must prioritize monitoring for spontaneous bleeding from invasive sites such as venipuncture or catheterization points. In DIC, the depletion of platelets and clotting factors prevents secondary hemostasis, resulting in persistent oozing. This clinical sign indicates that the maternal coagulation system is failing to maintain vascular integrity despite therapeutic interventions.
Rationale for incorrect answers
1. Blood glucose levels are typically not the primary focus during the management of acute DIC. While metabolic stress may cause transient hyperglycemia, it does not provide information regarding the coagulation status or the severity of the placental abruption. Monitoring glucose is secondary to assessing for systemic hemorrhage and organ perfusion.
3. Increased fetal heart rate variability is generally a sign of a well-oxygenated fetus with an intact autonomic nervous system. In abruptio placentae, the nurse would instead expect decreased variability or late decelerations due to placental insufficiency. DIC further compromises uteroplacental perfusion, likely leading to a non-reassuring fetal heart rate tracing.
4. Decreased uterine tenderness would suggest an improvement in the condition, whereas DIC usually accompanies worsening abruption. In this pathology, the uterus remains firm, hypertonic, and excessively tender due to concealed hemorrhage and myometrial irritation. A reduction in tenderness without delivery does not align with the clinical progression of consumptive coagulopathy.
Test-taking strategy
- Identify the Physiological Crisis: The question focuses on the priority clinical sign in a client already diagnosed with DIC secondary to abruption.
- Recall DIC Pathophysiology: DIC is characterized by the paradox of widespread clotting followed by the inability to clot at all due to factor depletion.
- Prioritize Life-Threatening Signs: Apply the Risk Reduction principle. Bleeding from venipuncture sites (choice 2) is a direct manifestation of the coagulopathy and signals a high risk for exsanguination.
- Differentiate Normal vs. Abnormal: Rule out choice 3 because "increased variability" is a positive sign, not a complication.
- Analyze Disease Progression: Rule out choice 4 as it describes an improvement in symptoms, while the question asks for signs to monitor for monitoring the crisis.
- Eliminate Irrelevant Data: Rule out choice 1 as glucose monitoring does not address the hematological emergency at hand.
Take home points
- Disseminated intravascular coagulation is a common and severe complication of placental abruption due to the release of thromboplastin.
- Spontaneous oozing from intravenous sites, gums, or incisions is an early and critical indicator of maternal factor depletion.
- Management of DIC requires the rapid identification of the underlying cause and replacement of fibrinogen via cryoprecipitate or fresh frozen plasma.
- Fetal monitoring is crucial as maternal coagulopathy often leads to acute placental insufficiency and subsequent fetal hypoxia.
A client with abruptio placentae has a Couvelaire uterus. The nurse understands that this condition can lead to which of the following complications?
Explanation
A Couvelaire uterus occurs when retroplacental hemorrhage forces blood to extravasate into the uterine myometrium and beneath the serosa. This widespread interstitial bleeding disrupts the normal architectural arrangement of myometrial fibers and interferes with efficient mechanical contractions. This loss of muscular integrity prevents the physiologic ligation of spiral arteries following delivery of the placenta, often requiring aggressive surgical or pharmacological management to control subsequent maternal blood loss.
Rationale for correct answers
2. The infiltration of blood into the myometrium causes uterine atony by physically separating the muscle fibers, which prevents the uterus from contracting. Without effective contraction, the client is at extreme risk for postpartum hemorrhage because the uterine sinuses remain open. This specific pathological state often results in a boggy, bluish, or purple-appearing uterus that fails to respond to standard oxytocic medications.
Rationale for incorrect answers
1. Preeclampsia is a multisystem disorder characterized by new-onset hypertension and proteinuria, rather than a direct complication of myometrial bleeding. While preeclampsia is a significant risk factor for causing abruptio placentae, a Couvelaire uterus itself does not pathologically trigger the vasospastic processes or endothelial dysfunction associated with preeclampsia.
3. Placenta accreta involves the abnormal adherence of the placenta directly to or through the myometrium due to a defective decidua basalis. While both conditions involve the myometrium, Couvelaire uterus is an acute consequence of internal hemorrhage, not a pre-existing structural implantation defect where chorionic villi invade the uterine wall.
4. Fetal growth restriction is a chronic manifestation of long-term placental insufficiency and inadequate nutrient exchange over weeks or months. Couvelaire uterus is an acute surgical finding associated with sudden, severe placental abruption and massive bleeding, which occurs far too rapidly to influence the trajectory of fetal weight gain or symmetric growth.
Test-taking strategy
- Identify the Pathological Mechanism: Focus on what a Couvelaire uterus actually is: blood infiltrating the uterine muscle.
- Evaluate Muscle Function: Understand that any muscle saturated with blood will fail to contract effectively.
- Connect to Clinical Outcomes: In the context of the third and fourth stages of labor, a failure of the uterus to contract (atony) leads directly to massive hemorrhage.
- Rule out Chronicity: Eliminate choice 4 as "growth restriction" is a chronic process, whereas abruption/Couvelaire is an acute event.
- Distinguish Etiology vs. Complication: Recognize that choice 1 is a cause of abruption, not a result of the Couvelaire uterus complication itself.
- Clarify Structural Defects: Differentiate between blood infiltration (Couvelaire) and tissue invasion (accreta) to rule out choice 3.
Take home points
- Couvelaire uterus is a severe form of placental abruption where blood penetrates the uterine myometrium, giving it a characteristic bluish discoloration.
- The primary clinical concern with this condition is uterine atony, as the infiltrated blood prevents the muscle fibers from constricting blood vessels.
- Healthcare providers must be prepared for emergency hysterectomy if the hemorrhage cannot be controlled by conservative measures or uterotonic drugs.
- Accurate assessment of fundal tone and blood loss is mandatory in the immediate postpartum period for any client with a history of severe abruption.
A nurse is caring for a client who is experiencing placental abruption. Which of the following complications should the nurse anticipate and monitor for? Select all that apply
Explanation
Severe abruptio placentae involves the total detachment of the placenta, causing a sudden interruption in fetal oxygenation and massive maternal hemorrhage. This obstetric emergency triggers circulatory collapse and systemic inflammatory responses, leading to multisystem organ failure, specifically affecting the renal and endocrine systems due to profound hypovolemic shock and microvascular thrombosis.
Rationale for correct answers
1. Significant blood loss leads to renal ischemia and decreased glomerular filtration rates. The nurse must monitor for acute kidney injury, characterized by oliguria < 30 mL/hour and rising creatinine, as the body shunts blood away from the kidneys to maintain cerebral and cardiac perfusion during hemorrhage.
2. The nurse should anticipate maternal hypotension and a narrow pulse pressure as compensatory mechanisms fail. This occurs when intravascular volume decreases sharply, leading to reduced stroke volume and a subsequent drop in systolic blood pressure, which is a late sign of significant internal or external bleeding.
3. Hypoxia initially triggers a sympathetic response resulting in fetal tachycardia > 160 beats per minute. As placental separation progresses, persistent bradycardia < 110 beats per minute occurs because the fetus can no longer compensate for the total lack of gas exchange, signaling imminent fetal demise.
5. Sheehan syndrome is a rare but serious complication involving ischemic necrosis of the anterior pituitary gland following severe postpartum hemorrhage. The nurse must monitor for this pituitary insufficiency because the gland, enlarged during pregnancy, is highly vulnerable to infarction during periods of profound systemic hypotension.
Rationale for incorrect answers
4. Gestational diabetes mellitus is a metabolic disorder characterized by insulin resistance and glucose intolerance beginning during pregnancy. It is caused by placental hormones like human placental lactogen and is not an acute complication resulting from the trauma or vascular disruption of a placental abruption.
Test-taking strategy
- Analyze the Question Type: This is a Select all that apply (SATA) question focusing on systemic complications of a severe maternal-fetal emergency.
- Prioritize Pathophysiology: Connect the primary event (massive bleeding) to the secondary effects of hypovolemic shock.
- Evaluate Organ Systems: Identify which organs are most sensitive to a drop in blood pressure. The kidneys (choice 1) and the pituitary gland (choice 5) are highly susceptible to ischemic damage.
- Assess Fetal Response: Remember the sequence of fetal distress. Initial stress causes tachycardia, while terminal hypoxia results in bradycardia.
- Determine Cardiovascular Trends: In shock, blood pressure falls and the difference between systolic and diastolic pressure (pulse pressure) narrows as peripheral resistance increases.
- Eliminate Unrelated Conditions: Rule out choice 4 as it is a chronic metabolic condition, not an acute result of hemorrhage or vascular separation.
Take home points
- Acute kidney injury is a frequent complication of severe abruption due to prolonged hypotension and potential microvascular damage from DIC.
- Sheehan syndrome involves permanent pituitary damage and must be suspected if a mother fails to lactate or has severe lethargy post-hemorrhage.
- Fetal monitoring typically reveals late decelerations and a loss of variability before progressing to terminal bradycardia in a complete abruption.
- Immediate management of severe abruption includes rapid volume expansion, blood product replacement, and emergency cesarean section to prevent maternal-fetal mortality.
A nurse is caring for a client 2 hours postpartum following a delivery complicated by a concealed placental abruption. The client’s uterus is boggy and displaced to the right, and there is heavy lochia rubra. Which of the following is the most likely cause of this finding?
Explanation
Postpartum hemorrhage often results from failure of the myometrium to achieve effective contraction, a state termed uterine atony. In the context of abruption, retroplacental hemorrhage forces blood into the uterine musculature, causing a Couvelaire uterus, which disrupts myofibril integrity and prevents the physiological occlusion of the spiral arteries, leading to significant maternal blood loss.
Rationale for correct answers
2. A Couvelaire uterus occurs when intramyometrial hemorrhage prevents the uterus from contracting efficiently after delivery. This uterine atony is a direct consequence of the previous concealed abruption, where blood infiltration inhibits the muscle's ability to maintain a firm tone, resulting in the boggy assessment finding noted.
Rationale for incorrect answers
1. Sheehan syndrome involves necrosis of the pituitary gland due to severe hypovolemic shock and does not directly cause an acutely boggy or displaced uterus. While it is a complication of the massive hemorrhage that atony might cause, it manifests later with failure to lactate or adrenal insufficiency rather than immediate uterine flaccidity.
3. Retained placental fragments can cause uterine atony and heavy bleeding, but the displacement of the uterus to the right specifically suggests bladder distension. Although fragments interfere with uterine involution, they do not typically cause the lateral displacement described, which is more characteristic of a full bladder interfering with the fundal position.
4. Neonatal respiratory distress syndrome is a complication affecting the newborn infant due to surfactant deficiency and pulmonary immaturity. It has no physiological impact on maternal uterine tone or the lochia flow volume during the postpartum period, making it irrelevant to the assessment findings of the mother's fundus and bleeding.
Test-taking strategy
- Identify the Primary Assessment: Focus on the descriptors boggy uterus and heavy lochia rubra, which are classic signs of uterine atony.
- Connect to Clinical History: Link the "concealed placental abruption" mentioned in the stem to the specific pathology of a Couvelaire uterus, where blood infiltrates the myometrium.
- Analyze Fundal Displacement: Recognize that while a boggy uterus indicates atony, displacement to the right usually indicates a full bladder, though the question asks for the "most likely cause" of the overall clinical finding in this high-risk context.
- Prioritize Pathophysiology: Choose the option that explains the muscular failure (atony) resulting from the specific obstetric complication (abruption/Couvelaire) described in the scenario.
- Eliminate Irrelevant Options: Rule out neonatal issues (choice 4) and late-onset endocrine complications (choice 1) that do not explain acute postpartum fundal tone.
Take home points
- Couvelaire uterus is a surgical and clinical finding where the myometrium is saturated with blood, leading to severe uterine atony.
- Uterine atony is the most common cause of postpartum hemorrhage and requires immediate intervention with fundal massage and uterotonics.
- A uterus displaced to the right in the postpartum period indicates a distended bladder, which prevents the uterus from contracting and increases bleeding risk.
- Management of atony following a severe abruption may include oxytocin, methylergonovine, or carboprost, and in refractory cases, surgical intervention.
A nurse is assessing a client with a suspected placental abruption. The client’s fibrinogen level is 85 mg/dL. Which of the following actions should the nurse perform first?
Explanation
Disseminated intravascular coagulation involves systemic microvascular thrombosis and subsequent factor exhaustion. This results in pathological consumption of fibrinogen, causing the maternal plasma concentration to drop below the critical threshold of 150 mg/dL. Consequently, the client develops hemorrhagic diathesis, manifesting as uncontrolled bleeding from minor trauma sites or mucosal surfaces. The etiology involves massive tissue factor release from the traumatized decidua, which bypasses normal regulatory pathways.
Rationale for correct answers
3. A fibrinogen level of 85 mg/dL indicates severe consumptive coagulopathy. The nurse must immediately notify the provider to initiate blood product replacement, such as cryoprecipitate or fresh frozen plasma. This intervention is necessary to restore hemostatic stability and prevent maternal exsanguination during the acute abruption event.
Rationale for incorrect answers
1. Administering prenatal vitamins is a chronic nutritional intervention with no clinical relevance in an acute emergency. During a placental abruption with signs of DIC, the nurse must prioritize hemodynamic stabilization over routine medication. Vitamins do not address the immediate life-threatening depletion of fibrinogen or clotting factors.
2. Encouraging ambulation is strictly contraindicated in suspected placental abruption due to the risk of exacerbating hemorrhage. Activity increases intra-abdominal pressure and could worsen the placental separation. The client must remain on strict bed rest to minimize further vascular disruption and maternal-fetal metabolic demand.
4. A digital vaginal exam is contraindicated in any third-trimester bleeding until placenta previa is ruled out. Even in known abruption, manual cervical manipulation can increase maternal bleeding or trigger further placental detachment. Nursing care focuses on non-invasive assessments like external monitoring and evaluating laboratory profiles.
Test-taking strategy
- Identify the Critical Value: Recognize that 85 mg/dL is a critically low fibrinogen level (normal pregnancy range 300 to 600 mg/dL).
- Connect to Pathology: Link low fibrinogen in the context of abruption to Disseminated Intravascular Coagulation (DIC).
- Prioritize Life-Threatening Issues: Apply the ABC and Patient Stability principles. A client with DIC is highly unstable and at risk for massive hemorrhage.
- Select Immediate Intervention: Choice 3 is the only action that addresses the clotting factor deficiency.
- Eliminate Contraindicated Actions: Rule out Choice 4 and Choice 2 as they are physically dangerous for a patient with placental separation.
- Rule out Irrelevant Tasks: Choice 1 is a low-priority routine task that ignores the acute physiological crisis.
Take home points
- Fibrinogen levels below 100 mg/dL in the third trimester are diagnostic for severe consumptive coagulopathy.
- Immediate notification of the surgical and anesthesia teams is required when laboratory results indicate an impending hematological collapse.
- Cryoprecipitate is the preferred blood product for rapidly replacing fibrinogen in obstetric emergencies.
- Bed rest and continuous fetal heart rate monitoring are mandatory nursing interventions for suspected placental abruption.
Practice Exercise 5
A nurse is caring for a client with suspected abruptio placentae who is experiencing fetal distress. Which of the following is the most appropriate medical management for this client?
Explanation
Abruptio placentae involves the premature separation of the placental attachment from the uterine wall, which acutely compromises fetoplacental circulation. This disruption leads to maternal-fetal gas exchange failure and severe fetal hypoxia, necessitating immediate surgical intervention to prevent intrauterine fetal demise.
Rationale for correct answers
3. When fetal distress is present in the context of placental abruption, an immediate cesarean section is the definitive medical management. Rapid delivery is mandatory to rescue the fetus from an hypoxic environment and to allow the uterus to contract, thereby controlling maternal hemorrhage from the denuded placental site.
Rationale for incorrect answers
1. Expectant management is only appropriate for stable clients with a partial abruption and a reassuring fetal heart rate. In the presence of fetal distress, delaying delivery through observation increases the risk of fetal death and maternal complications like disseminated intravascular coagulation or hemorrhagic shock.
2. The administration of tocolytics is generally contraindicated in cases of suspected placental abruption with hemodynamic instability. Using medications to stop contractions can mask the signs of uterine hypertonicity and delay the necessary delivery, potentially worsening both maternal hemorrhage and fetal gas exchange.
4. Amnioinfusion is used to resolve variable decelerations caused by umbilical cord compression, not to treat placental separation. This procedure does not address the underlying pathology of decreased perfusion at the maternal-fetal interface and would cause a dangerous delay in performing the required emergency surgery.
Test-taking strategy
- Analyze the Clinical Conflict: The stem identifies a high-risk diagnosis (abruptio placentae) coupled with an acute complication (fetal distress).
- Identify the Priority Goal: The immediate priority is the safety of the fetus and mother, which requires resolving the source of the distress.
- Determine Definitive Care: In obstetric emergencies where the "pump" (placenta) has failed, the only way to save the fetus is delivery.
- Eliminate Delaying Tactics: Rule out choice 1 and 4 as they do not provide a definitive solution to the lack of oxygenation.
- Assess Contraindications: Rule out choice 2 because tocolysis is dangerous in an active abruption where uterine monitoring and delivery are paramount.
Take home points
- Fetal distress in the presence of placental abruption is a surgical emergency requiring delivery regardless of gestational age.
- Signs of fetal distress include persistent late decelerations, terminal bradycardia, or a sinusoidal heart rate pattern.
- Nursing priorities during the transition to the operating room include oxygen administration, lateral positioning, and rapid fluid resuscitation.
- Emergency cesarean section serves the dual purpose of fetal rescue and providing access to the uterus to manage maternal bleeding.
A nurse is preparing a client with a marginal placental abruption at 32 weeks’ gestation for expectant management. Which of the following instructions is the most appropriate for the nurse to include?
Explanation
Marginal abruptio placentae involves partial separation of the placental periphery from the decidua. This condition requires intensive hemodynamic monitoring to detect expansion of retroplacental hematomas. Management protocols focus on prolonging gestation while preventing maternal hemorrhage or fetal asphyxiation through strict activity restriction and avoidance of cervical trauma.
Rationale for correct answer
1. Maintaining strict bed rest is essential to minimize intrauterine pressure and mechanical disruption of the placental site. Avoiding sexual activity prevents vaginal and cervical stimulation, which could trigger uterine contractions or exacerbate marginal bleeding, potentially leading to a complete and life-threatening detachment.
Rationale for incorrect answers
2. Inducing labor immediately is not indicated for a stable marginal abruption at 32 weeks’ gestation. Expectant management aims to achieve fetal maturity by delaying delivery if the maternal vital signs remain stable and the fetal heart rate tracing is reassuring and reactive.
3. Increasing physical activity is dangerous and contraindicated, as it can worsen placental separation through increased abdominal pressure. Physical exertion does not facilitate placental reattachment, as the physiological damage to the decidua basalis is irreversible and requires stabilization rather than movement to prevent exsanguination.
4. Daily vaginal examinations are contraindicated because manual manipulation of the cervix can trigger massive bleeding. Clinical monitoring for progress in expectant management relies on non-invasive methods like external fetal monitoring and ultrasonography to ensure the placental position and maternal stability are maintained.
Test-taking strategy
- Analyze the Clinical Scenario: The client has a "marginal" abruption and is being prepared for "expectant management" at 32 weeks (preterm).
- Identify the Goal of Expectant Management: The objective is to prolong pregnancy safely to allow for fetal lung maturation (often using betamethasone) while avoiding further detachment.
- Evaluate Safety and Risk: Rule out any interventions that increase mechanical stress or cervical stimulation. Choice 1 reduces these risks, while choices 3 and 4 increase them.
- Determine Timing of Delivery: Rule out immediate induction (choice 2) because the definition of expectant management implies waiting and monitoring rather than active, immediate delivery, provided both mother and fetus are stable.
- Apply Knowledge of Placental Physiology: Recognize that a detached placenta cannot reattach (ruling out choice 3), so the focus must remain on preventing further separation.
Take home points
- Expectant management for marginal abruption is only appropriate if maternal hemodynamics are stable and fetal heart rate patterns remain reassuring.
- Bed rest and pelvic rest are mandatory components of care to prevent further mechanical disruption of the decidua-placental interface.
- Corticosteroids like betamethasone should be administered to accelerate fetal lung maturity in cases of preterm placental abruption.
- Any increase in vaginal bleeding, sudden abdominal pain, or uterine rigidity necessitates immediate re-evaluation and possible emergency cesarean section.
A nurse is caring for a client admitted with abruptio placentae who is actively bleeding and showing signs of hypovolemic shock. Which of the following interventions is the priority for the nurse to perform?
Explanation
Hypovolemic shock in obstetrics results from acute blood loss, causing decreased mean arterial pressure and compromised tissue perfusion. This state triggers compensatory vasoconstriction and tachycardia, potentially leading to multi-organ failure if the circulating volume is not restored immediately to maintain uteroplacental blood flow and maternal hemodynamic stability.
Rationale for correct answer
3. In the setting of active hemorrhage and shock, the nurse must prioritize volume expansion through rapid infusion of crystalloids and blood products. Restoring circulatory volume is critical to prevent cardiac arrest and ensures that vital organs, including the uterus, receive adequate oxygenated blood to maintain cellular function.
Rationale for incorrect answers
1. Oral iron supplements are used for the long-term management of iron-deficiency anemia and are inappropriate in an acute crisis. During active bleeding, the gastrointestinal tract has decreased perfusion, and iron cannot correct the immediate deficit in blood volume or oxygen-carrying capacity required to sustain life.
2. While intravenous access is necessary, a 22-gauge catheter is too small for the rapid resuscitation required in hypovolemic shock. Standard emergency protocols dictate the use of large-bore needles, typically 18-gauge or larger, to facilitate the high-flow administration of warmed fluids and packed red blood cells.
4. High-Fowler's position is contraindicated in hypovolemia as it promotes venous pooling in the lower extremities and reduces venous return to the heart. The nurse should instead maintain a lateral tilt or supine position to maximize cardiac output and improve cerebral and placental perfusion during a hemorrhagic event.
Test-taking strategy
- Identify the Physiological Threat: The client is in hypovolemic shock, which is a life-threatening emergency requiring immediate circulation support.
- Apply the ABCs: Under the Circulation principle, restoring volume is the priority. Choice 3 directly addresses the immediate need for intravascular volume.
- Evaluate Equipment Adequacy: Recognize that in a "STAT" or "rapid" resuscitation scenario, small-bore IVs (choice 2) are insufficient for mass transfusion protocols.
- Assess Positioning Logic: Understand that high-Fowler's (choice 4) is for respiratory distress, whereas shock requires positions that favor venous return.
- Distinguish Acute vs. Chronic: Eliminate choice 1 because iron therapy is a nutritional intervention for stable patients, not an emergency treatment for exsanguination.
Take home points
- The priority in hemorrhagic shock is the restoration of intravascular volume to maintain organ perfusion and maternal-fetal stability.
- Large-bore intravenous access (14 to 18 gauge) is mandatory for the rapid administration of fluids and blood components in obstetric emergencies.
- Positioning a pregnant client with a lateral tilt prevents aortocaval compression, which is vital during resuscitation to maximize cardiac output.
- Crystalloid solutions like Lactated Ringer's are typically the initial fluid of choice followed by blood products in a 1:1:1 ratio if a massive transfusion is needed.
A nurse is caring for a client at 33 weeks gestation who is being managed conservatively for a Grade 1 placental abruption. Which of the following orders should the nurse anticipate? Select all that apply
Explanation
Placental abruption involving partial separation of the decidua basalis requires intensive maternal-fetal surveillance to detect worsening concealed hemorrhage. Conservative management aims to achieve fetal maturity while monitoring for coagulopathy and fetal heart rate abnormalities, provided the maternal hemodynamic status remains stable.
Rationale for correct answers
1. The nurse anticipates administering betamethasone to stimulate fetal surfactant production. This corticosteroid is vital at 33 weeks to reduce the risk of neonatal respiratory distress syndrome if the abruption progresses and necessitates an early delivery.
2. Continuous fetal monitoring is essential to detect early signs of hypoxia or placental insufficiency. Because an abruption can expand suddenly, the nurse must observe for late decelerations or a loss of variability that indicates compromised fetal oxygenation.
4. Monitoring the coagulation profile and fibrinogen is necessary to detect early consumptive coagulopathy. Serial laboratory assessments ensure that the nurse identifies fibrinogen depletion before the client develops clinical signs of disseminated intravascular coagulation or systemic hemorrhage.
Rationale for incorrect answers
3. Immediate induction with oxytocin is inappropriate for a Grade 1 abruption undergoing conservative management. The goal is to avoid unnecessary uterine activity that could exacerbate placental separation, provided the mother is stable and fetal well-being is confirmed.
5. A sterile vaginal exam is strictly contraindicated because it can cause mechanical trauma to the cervix and lower uterine segment. Manual manipulation may trigger massive bleeding or worsening of the abruption, making non-invasive clinical assessments the priority for monitoring.
Test-taking strategy
- Analyze the Question Type: This is a Select all that apply (SATA) question regarding the conservative (non-emergency) management of a preterm abruption.
- Identify the Goal of Care: At 33 weeks, the priority is to prolong pregnancy if possible, but prepare for preterm delivery.
- Evaluate Pharmacological Interventions: Corticosteroids like betamethasone (choice 1) are standard for any preterm condition where delivery is possible within 7 days.
- Assess Monitoring Priorities: Constant vigilance for fetal status (choice 2) and hematological stability (choice 4) is required to detect the transition from Grade 1 to a more severe grade.
- Rule out Contraindications: Eliminate invasive procedures (choice 5) and aggressive labor stimulants (choice 3) that increase the risk of total detachment.
- Utilize Prioritization Principles: Favor assessment and prevention of complications in a stable, conservative management case over active labor interventions.
Take home points
- Conservative management of Grade 1 abruption requires strict bed rest and continuous monitoring of maternal and fetal status.
- Betamethasone is administered intramuscularly in two doses, 24 hours apart, to enhance fetal lung maturity in preterm gestations.
- Fibrinogen levels should be maintained > 150 to 200 mg/dL to ensure adequate maternal clotting ability during observation.
- Any evidence of worsening abdominal pain, uterine rigidity, or non-reassuring fetal heart tones necessitates a shift to active delivery management.
A nurse is caring for a client with abruptio placentae who has a fibrinogen level of 95 mg/dL and is scheduled for an emergency cesarean section. Which of the following blood products should the nurse expect the primary health care provider to order first to address the fibrinogen level?
Explanation
Disseminated intravascular coagulation involves systemic microvascular thrombosis and subsequent factor exhaustion. This results in pathological consumption of fibrinogen, causing the maternal plasma concentration to drop below the critical threshold of 150 mg/dL. Consequently, the client develops hemorrhagic diathesis, manifesting as uncontrolled bleeding from minor trauma sites or mucosal surfaces. The etiology involves massive tissue factor release from the traumatized decidua, which bypasses normal regulatory pathways.
Rationale for correct answer
3. In the setting of severe hypofibrinogenemia < 100 mg/dL, cryoprecipitate is the priority blood product. It contains a high concentration of fibrinogen, von Willebrand factor, and factor 8, which are essential for achieving rapid hemostasis. This concentrated volume allows for the fast replacement of specific clotting factors without the risk of significant circulatory overload during an emergency surgical procedure.
Rationale for incorrect answers
1. Packed Red Blood Cells (PRBCs) are primarily indicated to improve oxygen-carrying capacity and restore hemoglobin levels in cases of acute blood loss. While PRBCs are necessary for hemodynamic stability during a massive hemorrhage, they do not contain significant amounts of fibrinogen. Administering only PRBCs fails to correct the underlying coagulopathy present in this client.
2. Whole blood is rarely used in modern obstetric practice because it contains dilute amounts of clotting factors compared to component therapy. Using whole blood is less efficient than targeted administration of specific components like cryoprecipitate or fresh frozen plasma. It also increases the risk of transfusion-associated circulatory overload without rapidly correcting the critical fibrinogen deficit.
4. Normal Saline 0.9% is an isotonic crystalloid used for initial volume resuscitation and maintaining mean arterial pressure. While essential for treating hypovolemic shock, saline contains no coagulation proteins and will further dilute existing clotting factors. Excessive crystalloid use can exacerbate dilutional coagulopathy, worsening the client’s inability to form stable clots during the cesarean section.
Test-taking strategy
- Identify the Specific Laboratory Deficit: The question provides a fibrinogen level of 95 mg/dL, which is critically low (normal > 200 mg/dL).
- Recall Component Therapy: Determine which blood product is the most concentrated source of the missing factor (fibrinogen).
- Apply Prioritization Principles: Although all listed items (except oral iron) might be used in a hemorrhage, the question asks which is used "first to address the fibrinogen level."
- Rule out General Volume Expanders: Eliminate Normal Saline and PRBCs as they do not provide coagulation proteins.
- Differentiate Clotting Products: Choose cryoprecipitate over Fresh Frozen Plasma or Whole Blood because cryoprecipitate has the highest concentration of fibrinogen per unit volume.
- Assess Procedural Needs: Recognize that correcting a coagulopathy is a pre-surgical priority before an emergency cesarean section to prevent intraoperative exsanguination.
Take home points
- Cryoprecipitate is the primary treatment for replacing fibrinogen in obstetric patients with values < 150 mg/dL.
- Each unit of cryoprecipitate typically raises the maternal fibrinogen level by approximately 7 to 10 mg/dL.
- Targeted component therapy is superior to whole blood for the rapid correction of specific hematological deficiencies in DIC.
- Correction of a coagulopathy must occur concurrently with surgical preparation to ensure maternal survival during emergency delivery.
Practice Exercise 6
A nurse is assessing a client with suspected abruptio placentae. Which of the following clinical findings should the nurse understand requires immediate intervention?
Explanation
Abruptio placentae involves the premature separation of the placental attachment from the uterine decidua prior to delivery. This pathological detachment results from vascular disruption and hemorrhage into the decidua basalis, often secondary to chronic hypertension or trauma. Circulatory collapse occurs when hypovolemic shock ensues from massive retroplacental or overt hemorrhage, necessitating immediate fluid resuscitation and stabilization.
Rationale for correct answer
3. Maternal hypotension and tachycardia are indicative of circulatory collapse and signify stage 2 or higher hemorrhagic shock. These vital sign alterations require immediate intervention because they reflect a critical loss of intravascular volume that compromises both maternal organ perfusion and essential uteroplacental gas exchange.
Rationale for incorrect answers
1. Mild vaginal spotting is a frequent clinical sign of a grade 1 abruption or even normal cervical effacement. While it requires ongoing monitoring, it does not represent the same level of acute instability as systemic hemodynamic changes. Spotting alone does not signal the immediate necessity for emergency resuscitation or surgical delivery.
2. A fetal heart rate of 140 bpm with moderate variability is a reassuring finding indicating an oxygenated fetus with an intact autonomic nervous system. This category 1 tracing suggests that the placenta is still providing adequate perfusion. Therefore, it does not demand the immediate, life-saving interventions required for maternal or fetal distress.
4. Intermittent uterine contractions are common during late pregnancy or the early stages of a partial abruption event. While they contribute to the clinical picture, they are not life-threatening on their own. The nurse prioritizes signs of maternal shock or fetal compromise over the presence of regular or irregular uterine activity.
Test-taking strategy
- Identify the Priority Finding: Look for signs of hemodynamic instability or fetal compromise that require rapid action to prevent mortality.
- Apply Prioritization Frameworks: Use the ABC (Airway, Breathing, Circulation) principle to identify that hypotension and tachycardia (Choice 3) relate to a circulation crisis.
- Evaluate Clinical Stability: Compare stable findings (reassuring fetal heart rate) against unstable findings (hypovolemic shock).
- Rule out Non-Urgent Signs: Eliminate mild spotting or intermittent contractions as they do not indicate an immediate threat to life compared to cardiovascular collapse.
- Focus on Shock Indicators: Recognize that narrowing pulse pressure, tachycardia, and hypotension are late signs of severe internal bleeding that mandate a "STAT" response.
Take home points
- Maternal tachycardia and hypotension are late indicators of significant blood loss due to the high compensatory capacity of the pregnant cardiovascular system.
- Hemodynamic stabilization through rapid crystalloid infusion and blood product administration is the priority for a client in shock.
- Reassuring fetal heart rate patterns (110 to 160 bpm with moderate variability) allow for more conservative management if the mother is stable.
- Abruptio placentae must be managed as a surgical emergency if there is evidence of maternal exsanguination or non-reassuring fetal status.
A nurse is caring for a client with abruptio placentae. Which of the following is a key nursing responsibility during an abruptio placentae emergency?
Explanation
Abruptio placentae involves the premature separation of the placental attachment from the uterine decidua prior to delivery. This pathological detachment results from vascular disruption and hemorrhage into the decidua basalis, leading to acute maternal-fetal compromise. Because the condition can progress rapidly to maternal exsanguination or fetal demise, the healthcare team must function with high efficiency to stabilize the patient and facilitate delivery.
Rationale for correct answer
2. The nurse must coordinate rapid interdisciplinary intervention among the obstetric, anesthesia, neonatal, and surgical teams to ensure maternal and fetal survival. Abruptio placentae is an obstetric emergency requiring synchronized actions like blood product preparation, surgical suite readiness, and continuous monitoring to manage potential complications such as shock or disseminated intravascular coagulation.
Rationale for incorrect answers
1. Encouraging patient ambulation is strictly contraindicated as it can increase intra-abdominal pressure and exacerbate the placental separation. In the presence of an abruption, the client must remain on strict bed rest in a lateral tilt position to maximize placental perfusion and prevent further mechanical detachment of the placenta.
3. Oral hydration is insufficient and unsafe for managing the acute hypovolemia associated with a placental abruption. The nurse must instead initiate large-bore intravenous access (18-gauge or larger) for the rapid administration of isotonic crystalloids and blood products to restore circulating volume and maintain organ perfusion during a hemorrhage.
4. Frequent vaginal examinations are contraindicated in third-trimester bleeding until placenta previa has been definitively ruled out by ultrasound. Furthermore, manual cervical manipulation can trigger heavier bleeding or worsen the abruption; therefore, assessments should be limited to non-invasive external fetal and uterine monitoring.
Test-taking strategy
- Identify the Acuity: The stem describes an "emergency" situation involving placental separation, which indicates a high risk for maternal-fetal mortality.
- Prioritize Interdisciplinary Care: In any high-stakes clinical crisis, communication and coordination among the healthcare team are the highest nursing priorities to ensure timely definitive care.
- Apply Safety Constraints: Rule out interventions that could cause harm, such as ambulation (choice 1) or invasive examinations (choice 4), which may worsen bleeding.
- Evaluate Fluid Management: Differentiate between routine hydration and emergency resuscitation; oral fluids (choice 3) are never the priority in an active hemorrhage or shock state.
- Focus on Timing: Choose the answer that addresses the need for rapid action and surgical readiness, which are the hallmarks of managing an acute placental detachment.
Take home points
- Rapid communication with the anesthesia and neonatal teams is vital for the successful management of a severe placental abruption.
- Monitoring for signs of disseminated intravascular coagulation, such as oozing from IV sites, is a critical nursing assessment during the emergency.
- Large-bore intravenous access must be established immediately to facilitate the massive transfusion protocols required for maternal stabilization.
- Continuous electronic fetal monitoring is necessary to detect early signs of fetal hypoxia that mandate an immediate emergency cesarean section.
A nurse is monitoring the hourly urine output of a client with a severe placental abruption. The nurse should understand that which of the following output levels most accurately reflects adequate renal perfusion?
Explanation
Severe abruptio placentae induces hypovolemic shock through massive hemorrhage, leading to significant reductions in mean arterial pressure and cardiac output. This triggers a compensatory sympathetic response that shunts blood away from the kidneys, potentially causing acute tubular necrosis if glomerular filtration is not maintained by restoring an adequate circulating volume. Monitoring urine output serves as a non-invasive surrogate for assessing visceral perfusion and the success of fluid resuscitation efforts.
Rationale for correct answer
4. A urine output of 35 mL/hour exceeds the minimum clinical threshold of 30 mL/hour required to demonstrate adequate perfusion of the renal parenchyma. In a hemorrhagic emergency like placental abruption, maintaining this level ensures that glomerular filtration is sufficient to prevent metabolic waste accumulation and permanent renal injury. This value confirms that the compensatory mechanisms or medical fluid resuscitations are successfully sustaining vital organ blood flow.
Rationale for incorrect answers
1. An output of 10 mL/hour indicates severe renal ischemia and is a diagnostic sign of oliguria. This critically low volume suggests that the client is in a state of decompensated shock, where the kidneys are not receiving enough blood to maintain basic filtration. The nurse must recognize this as a failure of hemostatic stability requiring immediate aggressive intervention to prevent multi-organ failure.
2. Producing only 15 mL/hour reflects significant hypoperfusion and remains well below the standard physiological requirement for an adult patient. This level of output suggests that the extracellular fluid volume is severely depleted due to the abruption. Persistent output at this rate will lead to electrolyte imbalances and the rapid progression of acute kidney injury secondary to the hemorrhage.
3. Although 25 mL/hour is closer to the target, it still falls below the hemodynamic threshold of 30 mL/hour used to define adequate renal function. While it may show a slight improvement over lower values, it indicates that the circulating volume is still insufficient to fully perfuse the renal cortex. The nurse must continue to monitor and potentially increase intravenous fluids to reach safer perfusion parameters.
Test-taking strategy
- Identify the Physiological Marker: Urine output is the gold standard for assessing end-organ perfusion in the context of shock and hemorrhage.
- Recall Standard Parameters: Use the medical standard of 30 mL/hour as the minimum acceptable output for an average-sized adult to indicate adequate renal health.
- Apply Comparative Analysis: Look at the options and identify which value is the only one that exceeds the 30 mL/hour requirement.
- Evaluate Clinical Priority: In a client with severe abruption, any value below 30 mL/hour signals circulatory insufficiency and the need for more volume.
- Select the Positive Outcome: Choice 4 (35 mL/hour) is the only finding that allows the nurse to conclude that the resuscitation efforts are currently meeting the body's metabolic demands.
Take home points
- Hourly urine output is a critical indicator of maternal hemodynamic status and the severity of blood loss in placental abruption.
- A minimum threshold of 30 mL/hour is required to confirm that the kidneys and other vital organs are being adequately perfused.
- Oliguria (less than 30 mL/hour) in an obstetric emergency often precedes the development of disseminated intravascular coagulation and acute kidney injury.
- Successful fluid resuscitation is evidenced by stabilizing vital signs and the restoration of urine output to within normal limits.
A nurse is caring for a client with a confirmed placental abruption. Which of the following actions should the nurse include in the plan of care to maximize fetal oxygenation? Select all that apply
Explanation
Abruptio placentae results in the pathological premature separation of the placenta, causing a significant reduction in the surface area available for maternal-fetal gas exchange. This leads to fetal hypoxia and acidosis due to impaired uteroplacental perfusion and retroplacental hematoma expansion. Management must focus on optimizing maternal hemodynamic status and oxygen saturation to maintain an adequate partial pressure of oxygen within the intervillous space of the remaining attached placenta.
Rationale for correct answers
1. Positioning the client with a lateral tilt or a wedge under the right hip prevents aortocaval compression by the gravid uterus. This action optimizes venous return and cardiac output, which directly enhances the volume of oxygenated blood delivered to the uteroplacental unit during an abruption.
2. Administering supplemental oxygen at 8 to 10 L/minute via a non-rebreather mask maximizes maternal arterial oxygen tension. This creates a favorable oxygen gradient between maternal and fetal circulations, ensuring that the fetus receives the highest possible concentration of oxygen through the remaining functional placental tissue.
4. The nurse must discontinue oxytocin to stop uterine contractions that further compromise placental blood flow. Hypertonic contractions or tachysystole associated with abruption increase intramyometrial pressure, which occludes the spiral arteries and exacerbates the existing fetal hypoxia and maternal-fetal gas exchange deficit.
Rationale for incorrect answers
3. While fluid resuscitation is necessary, a 22-gauge catheter is a small-bore device that is inappropriate for the rapid volume expansion required in a hemorrhage. Standard obstetric emergency protocols necessitate an 18-gauge or larger catheter to allow for the high-flow administration of crystalloids and blood products.
5. Performing a digital vaginal exam is contraindicated as it may increase maternal bleeding or aggravate the placental detachment site. Unless a cord prolapse is visualized or strongly suspected through monitoring, manual manipulation of the cervix should be avoided in the setting of active third-trimester hemorrhage.
Test-taking strategy
- Analyze the Nursing Goal: The question specifically asks for actions that maximize fetal oxygenation, requiring a focus on perfusion and oxygen delivery.
- Evaluate Maternal Positioning: Recognize that the supine position is detrimental due to vena cava compression. A right-hip wedge (choice 1) effectively provides a left lateral tilt to improve cardiac output.
- Assess Oxygen Delivery Systems: Identify the non-rebreather mask (choice 2) as the standard tool for intrauterine resuscitation to provide high-flow, high-concentration oxygen.
- Determine Uterine Influence: Understand that oxytocin (choice 4) increases uterine tone; stopping it reduces the mechanical resistance to placental blood flow, thereby aiding the fetus.
- Critique Equipment Choices: Rule out choice 3 because a 22-gauge needle is unsuitable for emergency resuscitation where large-bore access is the gold standard for circulation support.
Take home points
- Intrauterine resuscitation for placental abruption includes lateral positioning, high-flow oxygen, and intravenous fluid boluses.
- Discontinuing uterotonics like oxytocin is a priority to decrease uterine resting tone and improve maternal-fetal gas exchange.
- Aortocaval compression must be avoided in all late-gestation emergencies to ensure maximal maternal stroke volume and placental perfusion.
- Sterile vaginal examinations should be avoided in the presence of unexplained vaginal bleeding or suspected placental separation.
A nurse is assessing a client with a concealed placental abruption. Which of the following findings would be the most significant indicator that the internal bleeding is increasing?
Explanation
Concealed abruptio placentae involves hemorrhage sequestered behind the placenta, causing myometrial distension and increased intrauterine pressure. This retroplacental hematoma expansion leads to uterine hypertonicity and board-like rigidity without overt vaginal bleeding. Hemodynamic stability may temporarily mask the severity of internal sequestration, but progressive fundal displacement signifies worsening hematoma volume and potential myometrial infiltration.
Rationale for correct answer
3. An increase in fundal height indicates that the retroplacental hematoma is expanding and displacing the uterus upward. Because the hemorrhage is concealed, manual measurement of the uterine size is the most sensitive bedside indicator of internal bleeding volume. This finding suggests a significant accumulation of sequestered blood within the decidual interface, necessitating immediate surgical or medical re-evaluation to prevent uterine rupture or coagulopathy.
Rationale for incorrect answers
1. A decrease in the intensity of abdominal pain is not expected in a worsening placental abruption. Typically, the pain remains constant or increases as blood infiltrates the myometrium, causing significant tissue irritation. A reduction in pain might suggest a resolution of the event or a different diagnosis, rather than the progression of concealed hemorrhage.
2. While an increase in maternal heart rate to 115 bpm indicates compensatory tachycardia, it is a non-specific sign of physiological stress. Tachycardia can result from pain, anxiety, or maternal dehydration rather than just acute blood loss. In the pregnant population, heart rate changes often occur late in the process of hemorrhagic shock, making it less specific than direct uterine measurements.
4. An increase in blood pressure to 150/95 mmHg is more characteristic of gestational hypertension or preeclampsia. In the setting of severe internal bleeding, the nurse would anticipate maternal hypotension as the intravascular volume is depleted. Hypertension does not serve as a clinical indicator that concealed bleeding is increasing; it is instead a primary risk factor for the abruption itself.
Test-taking strategy
- Identify the Condition: The question specifies a concealed abruption, meaning blood is trapped behind the placenta and not exiting the vagina.
- Determine the Best Assessment Tool: Since the blood cannot be seen, the nurse must monitor for signs of internal expansion.
- Evaluate Clinical Indicators: Compare systemic signs (tachycardia) with localized signs (fundal height). In concealed hemorrhage, the physical displacement of the uterus is a more direct and significant indicator of the volume of trapped blood.
- Rule out Distractors: Eliminate choice 4 because blood pressure typically falls in hemorrhage. Eliminate choice 1 because pain typically increases with uterine distension.
- Focus on Objectivity: An hourly 2 cm increase in fundal height (choice 3) provides an objective measurement of worsening pathology that is specific to the concealed nature of the bleed.
Take home points
- Increasing fundal height is the classic clinical hallmark of worsening concealed placental abruption.
- Concealed abruption often manifests with extreme uterine tenderness and a board-like abdomen due to retroplacental pressure.
- Maternal vital signs can remain within normal limits until 25% to 30% of the total blood volume is lost.
- Monitoring for decreasing fibrinogen and platelet counts is essential to detect the onset of secondary consumptive coagulopathy.
Comprehensive Questions
A nurse is educating a client with a history of abruptio placentae about future pregnancies. Which of the following instructions should the nurse include?
Explanation
Placental abruption recurrence is a significant clinical concern, as individuals with a prior history have a risk ranging from 5 to 15 percent in subsequent gestations. This pathological predisposition is often linked to underlying maternal vascular dysfunction, chronic hypertension, or inflammatory processes within the decidua. Effective management in future pregnancies requires intensive surveillance and the optimization of maternal health to mitigate the risk of repeat placental separation.
Rationale for correct answer
2. The nurse must encourage early prenatal care to establish a baseline and monitor for risk factors like preeclampsia. Close monitoring of maternal blood pressure and serial ultrasounds to assess fetal growth and placental integrity are essential. These proactive assessments allow for the early detection of placental insufficiency or worsening hypertensive trends that could trigger another abruption event.
Rationale for incorrect answers
1. Advising that the recurrence risk is minimal is medically inaccurate and provides a false sense of security. A history of abruption is one of the strongest predictors for future occurrences, and routine visits may not be frequent enough to detect the subtle hemodynamic or fetal changes associated with a recurring detachment.
3. Recommending the avoidance of all physical activity is an unnecessary restriction that is not supported by current obstetric evidence. While heavy lifting or trauma should be avoided, moderate activity is generally encouraged to maintain cardiovascular health unless specific contraindications, such as cervical insufficiency or active bleeding, are present in the current pregnancy.
4. Suggesting a home birth is highly inappropriate for a client with a history of high-risk obstetric complications. Placental abruption is an unpredictable emergency that requires hospital resources, including immediate surgical access and blood product availability. A home birth setting would lack the life-saving equipment necessary to manage the rapid hemorrhage or fetal distress associated with an abruption.
Test-taking strategy
- Evaluate Risk Levels: Recognize that a history of placental abruption significantly increases the risk for future pregnancies.
- Identify Evidence-Based Care: Choose the option that emphasizes vigilant monitoring (Choice 2) rather than dismissing the risk (Choice 1).
- Assess Setting Appropriateness: Rule out home birth (Choice 4) for any patient with a history of major hemorrhage or surgical emergencies.
- Determine Rational Restrictions: Differentiate between "safety precautions" and "excessive restrictions"; avoiding all activity (Choice 3) is an over-generalization that lacks scientific basis.
- Focus on Modifiable Factors: Highlight blood pressure monitoring as a key intervention because hypertension is a primary, manageable risk factor for placental separation.
Take home points
- The risk of recurrent placental abruption increases significantly after one episode and rises further after two previous occurrences.
- Management of subsequent pregnancies involves frequent ultrasound assessments to monitor for intrauterine growth restriction and placental abnormalities.
- Controlling maternal hypertension and encouraging smoking cessation are the most effective strategies to reduce the risk of a repeat abruption.
- Delivery is often considered between 37 and 39 weeks gestation in high-risk cases to avoid the increased incidence of late-term placental separation.
A client at 30 weeks gestation asks how to prevent abruptio placentae. Which of the following risk reduction strategies should the nurse prioritize?
Explanation
Placental abruption is primarily driven by vascular endothelial dysfunction and acute vasospasm within the decidual spiral arteries. These pathological changes are significantly exacerbated by exogenous vasoconstrictors, which trigger decidual hemorrhage and mechanical separation of the placenta. Risk reduction focuses on eliminating modifiable triggers that compromise the integrity of the maternal-fetal interface and maintain stable systemic perfusion.
Rationale for correct answer
2. Avoiding smoking and illicit drugs, particularly cocaine, is the most effective strategy for risk reduction. Tobacco contains nicotine, which causes vasoconstriction, while cocaine induces profound arterial spasm and acute hypertension, both of which directly lead to premature separation of the placenta. Eliminating these chemical stressors preserves the vascular health of the decidua basalis and prevents the sudden disruptions in blood flow that cause abruption.
Rationale for incorrect answers
1. Limiting fluid intake to prevent edema is not an effective or safe strategy for preventing placental abruption. Restricting fluids can lead to maternal dehydration and reduced intravascular volume, which may actually decrease placental perfusion. Edema in pregnancy is often physiological or related to preeclampsia, but fluid restriction is not the indicated management for preventing vascular detachment.
3. Daily vigorous exercise is not a recognized strategy for preventing abruption and may actually increase the risk if it leads to abdominal trauma or maternal exhaustion. While moderate physical activity is generally healthy, vigorous exertion in the third trimester can increase intra-abdominal pressure. Abruptio placentae prevention relies more on hemodynamic stability than on increasing physical intensity during the late stages of gestation.
4. Reducing protein intake to decrease placental size is scientifically incorrect and medically dangerous. Proper nutrition, including adequate protein, is essential for healthy placental development and fetal growth. A smaller placenta does not reduce the risk of abruption; rather, nutritional deficiencies can weaken maternal vascular walls and increase the risk of gestational complications and poor fetal outcomes.
Test-taking strategy
- Identify Modifiable Risk Factors: Focus on the environmental and behavioral choices that have a documented causal link to placental separation.
- Recall Pathophysiology: Connect the role of vasoconstriction to the etiology of abruption. Choice 2 addresses the two most common chemical causes of placental vascular spasm.
- Evaluate Safety and Health: Rule out Choice 1 and Choice 4 as they describe nutritional restrictions that are harmful to both the mother and the developing fetus.
- Analyze Activity Levels: Recognize that "vigorous" exercise (Choice 3) is rarely the priority in high-risk obstetric teaching compared to lifestyle modifications.
- Prioritize Prevention: Apply the principle of health promotion, selecting the intervention that eliminates the most significant and preventable chemical triggers for the condition.
Take home points
- Smoking increases the risk of placental abruption by approximately 40% for every pack of cigarettes smoked per day.
- Cocaine use is a leading cause of severe, acute placental abruption due to sudden, intense vasospasm and hypertensive crisis.
- Chronic hypertension and preeclampsia are the most common underlying medical conditions associated with an increased risk of placental separation.
- Maternal education should focus on signs to report immediately, such as sudden abdominal pain, uterine tenderness, or vaginal bleeding.
A nurse is providing discharge teaching to a client with a recent mild abruptio placentae episode. Which of the following should the nurse include? Select all that apply
Explanation
Mild abruptio placentae involves focal separation of the placenta where maternal and fetal hemodynamics remain transiently stable. Discharged clients require vigilant surveillance for recurrent hemorrhage and chronic placental insufficiency, as the initial detachment site can act as a nidus for further decidual hematoma expansion or intrauterine growth restriction.
Rationale for correct answers
1. Daily assessment of fetal kick counts is mandatory to evaluate the integrity of the remaining fetoplacental unit. A reduction in movement signals fetal hypoxia secondary to chronic placental insufficiency, necessitating immediate clinical evaluation to prevent intrauterine fetal demise following the initial separation event.
2. The client must report vaginal bleeding or sudden abdominal tenderness, as these indicate a progression of the abruption grade. Recurrent hemorrhage can lead to systemic shock or disseminated intravascular coagulation, making prompt recognition of these hallmark symptoms the highest priority for maternal safety.
4. Consistent high-risk monitoring via frequent prenatal visits ensures serial ultrasound and laboratory assessments of placental health. These appointments allow for the detection of fetal growth restriction or worsening maternal hypertension, which are common sequelae in patients with a history of placental detachment.
Rationale for incorrect answers
3. Resuming sexual intercourse is contraindicated due to the risk of mechanical cervical stimulation and uterine activity. Pelvic rest is essential to prevent decidual trauma, which could trigger further placental separation and life-threatening hemorrhage in a client who has recently experienced a mild abruption.
5. Self-administering home anticoagulants is strictly contraindicated because it significantly increases the risk of uncontrolled maternal hemorrhage. Since the primary pathology of abruption involves vascular disruption, thinners would interfere with the body's ability to achieve hemostasis at the retroplacental site, potentially causing fatal exsanguination.
Test-taking strategy
- Identify the Condition Status: The client is being discharged after a "mild" episode, implying they are currently stable but remain at high risk for recurrence.
- Focus on Surveillance: Prioritize actions that involve monitoring for complications. Daily fetal movement (choice 1) and symptom reporting (choice 2) are standard non-invasive monitoring tools.
- Apply Safety Constraints: Rule out activities that cause mechanical or chemical disruption. Pelvic rest (ruling out choice 3) and avoiding anticoagulation (ruling out choice 5) are critical to prevent worsening the hemorrhage.
- Support Continuity of Care: Recognize that a history of abruption necessitates a high-risk classification (choice 4) for all subsequent prenatal care to ensure timely medical intervention if the condition deteriorates.
- Differentiate Grade 1 Management: In mild cases, the goal is extension of gestation, making patient education on warning signs the most vital discharge component.
Take home points
- Fetal kick counts serve as a critical daily indicator of fetal well-being and placental reserve in high-risk pregnancies.
- Pelvic rest, including the avoidance of intercourse and douching, is mandatory to minimize the risk of recurrent placental separation.
- Anticoagulant therapy is generally avoided in active or recent abruption due to the high risk of exacerbating retroplacental bleeding.
- Prompt reporting of uterine rigidity, pain, or bleeding is the most effective way to prevent maternal-fetal mortality at home.
A nurse is teaching a client with chronic hypertension about preventing placental complications. Which statement indicates understanding?
Explanation
Chronic hypertension is a primary etiological factor for placental abruption, as persistent elevated pressure causes degenerative changes in the decidual spiral arteries. These vascular lesions lead to arterial rupture and the formation of a retroplacental hematoma, which mechanically shears the placenta from the uterine wall. Effective management requires consistent pharmacological control of systemic pressure to maintain endothelial integrity and prevent the sudden onset of life-threatening placental separation.
Rationale for correct answer
1. Continuing antihypertensive medication as prescribed is essential to prevent the acute spikes in blood pressure that trigger vascular disruption. Stable control of maternal hemodynamics reduces the shear stress on the delicate decidual vessels, thereby decreasing the statistical probability of premature placental detachment and ensuring consistent uteroplacental perfusion throughout the remainder of the gestation.
Rationale for incorrect answers
2. Skipping medication when blood pressure is normal at home is dangerous because it leads to rebound hypertension and unstable vascular resistance. Chronic hypertension in pregnancy requires a steady-state concentration of medication to prevent pathological fluctuations that could rupture the spiral arteries. Normal home readings are a result of the medication's efficacy, not an indication that the underlying vascular pathology has resolved.
3. Avoiding prenatal visits is unsafe because placental complications, such as growth restriction or early detachment, often begin without overt maternal symptoms. Frequent surveillance is necessary to monitor fetal well-being via ultrasound and to assess for the development of superimposed preeclampsia, which significantly increases the risk of a catastrophic abruption event compared to controlled chronic hypertension alone.
4. Smoking even occasionally is unacceptable because nicotine induces acute vasospasm and further damages the vascular endothelium. When combined with chronic hypertension, the chemical toxins in cigarettes act synergistically to increase placental friability and hypoxia. Controlling blood pressure does not negate the direct ischaemic damage caused by tobacco use, which remains a leading modifiable risk factor for placental separation.
Test-taking strategy
- Identify the Core Risk Factor: Recognize that chronic hypertension is the most significant medical risk factor for placental abruption.
- Focus on Compliance: In chronic disease management, medication adherence (Choice 1) is almost always the priority teaching point to ensure long-term stability.
- Evaluate Safety Logic: Rule out Choice 2 and Choice 3 because they involve self-management that bypasses medical supervision and physiological consistency.
- Assess Behavioral Risks: Eliminate Choice 4 because smoking is a multiplicative risk factor that is never "safe" in a high-risk pregnancy, regardless of blood pressure status.
- Prioritize Prevention: Select the statement that demonstrates an understanding of hemodynamic stability as the primary defense against decidual vascular rupture.
Take home points
- Strict blood pressure control (typically aiming for < 140/90 mmHg) is the most effective way to reduce the risk of hypertension-related abruption.
- Chronic hypertension increases the risk of superimposed preeclampsia, which is a major trigger for severe placental separation.
- Patients must be educated that antihypertensive therapy is a preventative measure, not a reactive treatment for temporary symptoms.
- Smoking cessation and avoiding vasoconstrictive substances are mandatory to preserve the microvascular health of the placenta.
A nurse is counseling a client with prior abruptio placentae. Which instructions are appropriate for risk reduction in future pregnancies? Select all that apply
Explanation
Placental abruption recurrence is a significant clinical concern, as individuals with a prior history have a risk ranging from 5 to 15 percent in subsequent gestations. This pathological predisposition is often linked to underlying maternal vascular dysfunction, chronic hypertension, or inflammatory processes within the decidua. Effective management in future pregnancies requires intensive surveillance and the optimization of maternal health to mitigate the risk of repeat placental separation.
Rationale for correct answers
1. Performing an early ultrasound is essential to establish a baseline for placental location and to rule out concurrent pathologies like placenta previa. While abruption is a clinical diagnosis, serial ultrasonographic imaging allows the clinician to monitor for the development of retroplacental hematomas or signs of placental insufficiency that may precede a full detachment.
2. Consistent blood pressure control is the most critical intervention for reducing the risk of recurrence. Chronic hypertension causes arteriolar degeneration within the decidua, and maintaining systolic and diastolic levels within target ranges (typically < 140/90) reduces the mechanical stress that triggers vascular rupture and subsequent placental separation.
3. Avoiding tobacco and recreational drugs is a mandatory lifestyle modification to prevent acute vasoconstrictive events. Substances like cocaine and nicotine induce arterial spasms and placental hypoxia, which are potent triggers for decidual hemorrhage, making their elimination a priority in a high-risk obstetric plan.
5. Optimal maternal nutrition and hydration support the overall health of the vascular system and promote adequate plasma volume. Maintaining an appropriate extracellular volume ensures consistent uteroplacental perfusion, which helps preserve the integrity of the maternal-fetal interface and supports healthy placental development throughout the pregnancy.
Rationale for incorrect answers
4. Delaying the report of any symptoms is dangerous, as placental abruption can progress from mild to life-threatening within minutes. Even mild pain or spotting must be reported immediately to allow for STAT evaluation of fetal well-being and maternal stability, as prompt intervention is the only way to prevent catastrophic outcomes.
Test-taking strategy
- Identify the High-Risk Status: A client with a prior abruption is at significantly higher risk for recurrence and requires more than routine care.
- Prioritize Modifiable Factors: Focus on interventions that directly affect vascular health, such as blood pressure control (choice 2) and substance avoidance (choice 3).
- Assess Monitoring Protocols: Recognize that serial assessments (choice 1) are a standard of care for high-risk pregnancies to detect early signs of placental failure.
- Eliminate Delaying Behaviors: Rule out choice 4 based on the principle of safety; in a high-risk scenario, any new symptom requires an emergent rather than elective evaluation.
- Promote General Wellness: Include choice 5 as a foundational element of prenatal health that supports a stable maternal environment.
Take home points
- Recurrence risk of placental abruption increases significantly with each subsequent pregnancy, necessitating a high-risk obstetric classification.
- Chronic hypertension and preeclampsia are the strongest predictors of repeat abruption and require aggressive pharmacological management.
- Smoking cessation reduces the risk of placental separation by improving decidual vascular integrity and oxygenation.
- Immediate reporting of uterine tenderness, rigidity, or bleeding is vital to ensure maternal and fetal survival through rapid delivery.
A nurse is caring for a client with placenta previa. Which of the following is a hallmark symptom of this condition?
Explanation
Placenta previa occurs when the placenta implants in the lower uterine segment, partially or totally covering the internal cervical os. As the lower segment thins and the cervix begins to efface, the inelastic placental attachment is disrupted, leading to the rupture of maternal intervillous vessels. This results in maternal hemorrhage without associated myometrial irritation, typically occurring during the third trimester when the lower uterine segment undergoes physiological elongation.
Rationale for correct answer
2. The presence of bright red, painless vaginal bleeding is the classic clinical manifestation of placenta previa. Because the bleeding originates from the detachment of the placenta from the lower uterine segment rather than a traumatic separation of the decidua, there is no myometrial tension or associated pain. This hallmark symptom typically occurs suddenly and may be episodic as the pregnancy progresses toward term.
Rationale for incorrect answers
1. Painful uterine contractions and a board-like rigidity of the abdomen are characteristic of abruptio placentae. These findings indicate that blood is infiltrating the myometrium or sequestering behind the placenta, causing significant tissue irritation. In placenta previa, the uterus remains soft and non-tender because the blood escapes through the cervix rather than being trapped within the muscular wall.
3. Increased fetal movement is not a diagnostic finding for placenta previa, and fetal tachycardia is often a non-specific response to maternal stress. While severe hemorrhage can eventually lead to fetal hypoxia and a non-reassuring heart rate, it is not a primary hallmark used to differentiate previa from other causes of late-gestational bleeding. Fetal status usually remains stable until maternal hypovolemia becomes significant.
4. Severe localized abdominal tenderness is a hallmark of placental abruption or uterine rupture, where the visceral peritoneum is irritated by internal bleeding. Placenta previa is characterized specifically by its lack of pain, as the placental separation occurs at the internal os where blood exits freely. Tenderness would suggest a different pathological process involving the upper uterine segment or an inflammatory abdominal condition.
Test-taking strategy
- Identify the Core Condition: Focus on the specific pathology of placenta previa versus its primary differential, abruptio placentae.
- Differentiate Pain Levels: Use the classic diagnostic rule that previa is painless while abruption is painful.
- Observe Bleeding Characteristics: Recognize that the color of blood in previa is typically bright red because it is fresh and exits the cervix immediately.
- Apply Anatomical Knowledge: Understand that because the placenta is over the cervical os, any bleeding is usually external and non-irritating to the uterine muscle.
- Rule out Rigidity: Eliminate any options describing uterine hardness or tenderness, as these are incompatible with the soft uterus seen in a previa assessment.
Take home points
- Painless, bright red vaginal bleeding in the second or third trimester is placenta previa until proven otherwise by ultrasound.
- A soft, relaxed, and non-tender uterus is the expected physical finding when assessing a client with a suspected placenta previa.
- Digital vaginal examinations are strictly contraindicated in these clients because they can trigger catastrophic and uncontrollable maternal hemorrhage.
- Management of stable placenta previa focuses on bed rest, pelvic rest, and scheduled cesarean delivery to avoid labor-related detachment.
A nurse is educating a pregnant client about preventing placental complications. Which of the following advice is most relevant to reducing the risk of abruptio placentae?
Explanation
Placental abruption is primarily driven by vascular endothelial dysfunction and acute vasospasm within the decidual spiral arteries. These pathological changes are significantly exacerbated by exogenous vasoconstrictors, which trigger decidual hemorrhage and mechanical separation of the placenta. Risk reduction focuses on eliminating modifiable triggers that compromise the integrity of the maternal-fetal interface and maintain stable systemic perfusion.
Rationale for correct answer
2. Avoiding tobacco and illicit drugs, specifically cocaine, is the most effective lifestyle modification for risk reduction. These substances induce profound arterial spasm and acute hypertension, leading to a rupture of the decidual vessels. Eliminating these chemical stressors preserves the vascular health of the maternal-fetal unit and prevents the sudden disruptions in blood flow that cause premature separation.
Rationale for incorrect answers
1. Increasing caffeine intake is not a recommended strategy and may actually be detrimental during pregnancy. High levels of caffeine can lead to maternal tachycardia and may contribute to vasoconstriction, which does not help in preventing abruption. Blood pressure should be managed through balanced nutrition and, if necessary, pharmacological interventions prescribed by a provider rather than stimulant dietary habits.
3. Restricting fluid intake to manage edema is an unsafe practice that leads to maternal dehydration. Adequate intravascular volume is required to maintain renal perfusion and ensure that the placenta receives sufficient blood flow. Edema is often a physiological result of increased plasma volume or venous stasis, and limiting water does not prevent the vascular rupture associated with abruption.
4. Resting in a supine position is contraindicated in late pregnancy because it causes aortocaval compression. The weight of the gravid uterus obstructs the inferior vena cava, decreasing venous return and cardiac output. This position reduces placental perfusion and can worsen fetal hypoxia, whereas a lateral tilt is the preferred position to maximize oxygen delivery.
Test-taking strategy
- Identify Modifiable Risks: Focus on the environmental and behavioral choices that have a documented causal link to placental separation.
- Recall Pathophysiology: Connect the role of vasoconstriction to the etiology of abruption. Choice 2 addresses the two most common chemical causes of placental vascular spasm.
- Evaluate Safety Logic: Rule out Choice 1 and Choice 3 because they describe nutritional restrictions or habits that are harmful to both the mother and the developing fetus.
- Assess Positioning Logic: Understand that the supine position (Choice 4) is physiologically detrimental in the third trimester due to pressure on major vessels.
- Prioritize Prevention: Apply the principle of health promotion, selecting the intervention that eliminates the most significant and preventable chemical triggers for the condition.
Take home points
- Smoking cessation is a primary intervention because nicotine increases the risk of decidual necrosis and subsequent placental separation.
- Cocaine use is a leading cause of catastrophic abruption due to the induction of severe, acute hypertensive crises and vasospasm.
- Maternal position should be optimized to the left lateral side to ensure maximum cardiac output and placental oxygenation.
- Chronic hypertension must be controlled throughout pregnancy to prevent the degenerative vascular changes that predispose the client to abruption.
A nurse is monitoring a client with abruptio placentae. Which of the following fetal heart rate patterns should the nurse understand is the most concerning for terminal hypoxia?
Explanation
Abruptio placentae initiates a cascade of uteroplacental insufficiency as the detachment area increases, reducing the maternal-fetal gas exchange surface. This leads to progressive fetal acidemia and anaerobic metabolism, eventually exhausting the fetal compensatory mechanisms. When the myocardium can no longer maintain cardiac output under hypoxic conditions, a failure of the conduction system occurs, manifesting as a terminal decline in the baseline heart rate.
Rationale for correct answer
3. Persistent bradycardia, defined as a baseline heart rate < 110 bpm for 10 minutes or more, is the most ominous sign of terminal hypoxia. In the context of an abruption, this pattern signifies that the fetus has reached the limit of its physiological compensation and is experiencing myocardial depression. This necessitates immediate, emergent delivery to prevent intrauterine fetal demise, as it often precedes fetal asystole.
Rationale for incorrect answers
1. Early decelerations are generally considered benign findings caused by fetal head compression during contractions. They are characterized by a symmetrical decrease and return to baseline that mirrors the uterine contraction, representing a vagal response. Because they do not indicate a lack of oxygen or placental separation, they are not concerning for hypoxia in a client with an abruption.
2. Moderate variability (6 to 25 bpm) is a hallmark of a well-oxygenated fetus with an intact and functioning autonomic nervous system. It indicates that the fetal brain is receiving adequate perfusion and is able to regulate the heart rate in response to hemodynamic changes. This is a reassuring finding that would suggest the abruption has not yet caused significant systemic compromise to the fetus.
4. Short-term accelerations are abrupt increases in the fetal heart rate that indicate fetal movement and a reactive, healthy neurological state. Accelerations are the primary component of a reactive non-stress test, confirming that the fetus is not currently acidotic or hypoxic. Their presence is a positive prognostic indicator and is the opposite of the patterns seen during terminal respiratory or circulatory failure.
Test-taking strategy
- Identify the Goal: The question asks for the most concerning pattern related to "terminal hypoxia," which implies an immediate threat to life.
- Rank Fetal Heart Patterns: Classify the choices into reassuring (moderate variability, accelerations) and non-reassuring (bradycardia) categories.
- Link Pathophysiology to Patterns: Recognize that bradycardia (choice 3) in an emergency abruption scenario represents the final stage of fetal exhaustion.
- Rule out Physiological Responses: Eliminate early decelerations (choice 1) as they are a mechanical response to head compression, not a marker of placental failure.
- Differentiate Between Decelerations: Recall that while late decelerations are worrisome, persistent bradycardia is more indicative of an imminent terminal event.
Take home points
- Persistent fetal bradycardia in the presence of maternal hemorrhage indicates severe fetal acidosis and requires immediate surgical intervention.
- Moderate variability is the most important indicator of fetal central nervous system integrity and adequate oxygenation.
- Late decelerations often precede bradycardia as the placenta continues to detach, signaling a transition from compensation to decompensation.
- Sinusoidal patterns may also be observed in severe abruption, indicating profound fetal anemia due to feto-maternal hemorrhage.
A nurse is caring for a client with abruptio placentae who is experiencing fetal distress. What is the most appropriate medical management for the primary health care provider to perform?
Explanation
Abruptio placentae with fetal distress represents a critical failure of uteroplacental perfusion due to premature decidual separation. This pathological state induces rapid fetal acidemia and hypoxia as the respiratory surface area of the placenta diminishes. Immediate surgical intervention is required to prevent irreversible neurological injury or intrauterine fetal demise when compensatory mechanisms like tachycardia or peripheral vasoconstriction fail to maintain fetal cerebral oxygenation.
Rationale for correct answer
3. Immediate cesarean section is the definitive treatment for fetal distress in the presence of placental abruption. Removing the fetus from a hypoxic environment stops the progression of acidemia caused by the loss of placental gas exchange. This rapid intervention is necessary to ensure neonatal survival and to allow for direct hemostatic control of maternal retroplacental hemorrhage.
Rationale for incorrect answers
1. Expectant management is only appropriate for preterm gestations where both the mother and fetus are hemodynamically stable. Weekly ultrasounds are insufficient when active distress is present, as the condition can progress to total detachment within minutes. Delaying delivery in a distressed fetus significantly increases the risk of stillbirth and maternal coagulopathy.
2. Tocolytics are generally contraindicated in the management of moderate to severe placental abruption. Attempting to delay delivery when the fetus is already showing signs of distress allows the hematoma to expand further. This pharmacological intervention masks the uterine hypertonicity that often accompanies abruption and delays the life-saving extraction of the compromised neonate.
4. Induction of labor with oxytocin is inappropriate when fetal distress is already established. Uterine contractions further compress the already compromised spiral arteries, exacerbating intervillous hypoxia and worsening the fetal condition. A high-dose drip increases the risk of uterine rupture and rapid maternal exsanguination during a severe placental separation event.
Test-taking strategy
- Identify the Physiological Crisis: The question identifies both abruptio placentae and fetal distress, signaling a Category 3 emergency.
- Prioritize Rapid Delivery: In obstetric emergencies where the fetus is unstable, the fastest and safest delivery method (cesarean section) is the priority.
- Apply Stability Principles: Rule out expectant management (choice 1) and tocolytics (choice 2) because they are only for stable patients without distress.
- Evaluate Uterine Stress: Eliminate oxytocin induction (choice 4) as it increases uterine pressure, which is dangerous for a fetus already lacking sufficient oxygen.
- Determine Definitive Care: Recognize that once the placental-fetal unit has failed, the only way to save the fetus is to bypass the placenta through surgery.
Take home points
- Fetal distress in the context of placental abruption mandates an immediate emergency cesarean section regardless of gestational age.
- Tocolytic therapy should be avoided in placental abruption as it can mask clinical symptoms and delay necessary surgical intervention.
- Conservative management is reserved only for Grade 1 abruptions where maternal and fetal vital signs remain within normal limits.
- Prompt delivery is also a maternal life-saving measure as it allows the uterus to contract down and achieve hemostasis at the detachment site.
A nurse is educating a client who had a placental abruption in a previous pregnancy. Which of the following information regarding the risk of recurrence should the nurse provide?
Explanation
Placental abruption recurrence stems from underlying vascular endothelial dysfunction and chronic decidual arteriopathy. This pathological predisposition leads to defective placentation and increased friability of the spiral arteries in subsequent gestations. Chronic hypertension, preeclampsia, and thrombophilias further exacerbate the risk, with recurrence rates ranging between 5% and 15% after 1 episode and increasing to 25% after 2 previous episodes.
Rationale for correct answer
2. The nurse correctly identifies a significantly increased risk of recurrence for the client. Epidemiological data confirms that a history of premature separation is one of the strongest predictors for future abruption events. Close maternal-fetal surveillance is required in subsequent pregnancies to monitor for signs of placental insufficiency or early decidual hemorrhage.
Rationale for incorrect answers
1. Stating there is zero risk is a significant medical error that ignores the hereditary and vascular nature of placental detachment. Clinicians must acknowledge that the recurrence risk is approximately 10 to 15 times higher than the general population rate. Providing false reassurance prevents the client from seeking the necessary high-risk prenatal care required for safety.
3. The claim that abruption only occurs in primigravidas is scientifically inaccurate, as multiparity is actually a known risk factor. Chronic vascular damage and uterine scarring from previous deliveries can predispose multigravid patients to decidual bleeding. The condition can occur in any pregnancy where the maternal-fetal vascular interface is compromised by hypertension or trauma.
4. Fetal sex does not have a clinically significant correlation with the pathophysiological mechanisms of decidual vessel rupture. The risk of abruption is dictated by maternal factors such as blood pressure, smoking status, and uterine health rather than fetal genetics. Educating a client that the risk is gender-dependent is a baseline misconception that lacks empirical evidence.
Test-taking strategy
- Analyze the Risk Profile: Recognize that a history of placental abruption automatically classifies a future pregnancy as high-risk.
- Evaluate Accuracy: Rule out absolute terms like "zero risk" (choice 1) or "only occurs in" (choice 3), as medical conditions rarely follow absolute rules.
- Identify Evidence-Based Trends: Choose the option that aligns with the known recurrence statistics of 5% to 15% (choice 2).
- Rule out Biological Myths: Eliminate choice 4 as it introduces an irrelevant variable (fetal sex) into a vascular pathology discussion.
- Prioritize Education: The goal of counseling a high-risk client is to ensure they understand the need for enhanced monitoring in the future.
Take home points
- A history of placental abruption necessitates a high-risk obstetric referral for all subsequent pregnancies.
- Recurrence risk increases significantly if the previous abruption was associated with severe maternal hypertension or preeclampsia.
- Serial ultrasound monitoring for fetal growth and placental integrity is recommended starting in the second trimester of the next pregnancy.
- Modifiable risk factors such as smoking and illicit drug use must be eliminated to improve future placental outcomes.
A nurse is teaching a group of student nurses about the clinical differences between placenta previa and abruptio placentae. Which of the following findings are characteristic of abruptio placentae? Select all that apply
Explanation
Abruptio placentae involves the premature separation of the decidua basalis, leading to retroplacental hemorrhage and myometrial irritation. This pathological process causes uterine hypertonicity as blood infiltrates the muscular fibers, a condition known as Couvelaire uterus, which results in significant maternal distress. Unlike previa, the bleeding is often associated with metabolic acidosis and rapid fetal decompensation due to the sudden loss of functional gas exchange surface area.
Rationale for correct answers
2. The client reports sudden pain that is typically described as intense, constant, and localized to the uterus. This occurs because the expanding hematoma increases intrauterine pressure and chemically irritates the myometrium. The presence of significant pain is a primary diagnostic hallmark that differentiates this condition from the painless bleeding seen in placenta previa.
4. The fetal heart rate often exhibits late decelerations or a significant loss of variability. These patterns reflect fetal hypoxia resulting from the reduced surface area for placental gas exchange and maternal hypovolemia. Because the detachment occurs abruptly, the fetus has limited time to compensate, leading to rapid signs of intrauterine distress on the monitor.
5. The uterine tone is increased and typically presents as a board-like rigidity on palpation. This tonicity is a direct result of blood infiltration into the uterine muscle, which prevents the uterus from relaxing between contractions or even when at rest. This physical finding is essential for the clinical diagnosis of severe concealed or overt placental detachment.
Rationale for incorrect answers
1. A uterus that is soft and non-tender is a classic finding in placenta previa, not abruptio placentae. In abruption, the accumulation of blood within the uterine wall creates extreme sensitivity and firmness. Finding a relaxed uterus during a bleeding episode helps the clinician rule out a detachment and points toward an abnormal placental implantation site instead.
3. Bright red, painless bleeding is the signature clinical manifestation of placenta previa. In contrast, the blood in an abruption may be dark red due to sequestration or may even be completely concealed behind the placental plate. The absence of pain and uterine tenderness is the key feature that excludes an abruption in the differential diagnosis.
Test-taking strategy
- Differentiate the Pathologies: Focus on the uterine tone and the presence or absence of pain to distinguish between the two conditions.
- Identify Hallmark Signs: Recall the "3 Ts" of abruption: Tension (board-like), Tenderness (painful), and Tone (hypertonicity).
- Assess Fetal Impact: Recognize that abruption is much more likely to cause acute distress (Choice 4) than an initial previa episode.
- Apply Comparative Rules: Rule out choice 1 and choice 3 because they describe the painlessoft nature of placenta previa.
- Prioritize Physical Assessment: Value the objective finding of a board-like abdomen (Choice 5) as it is a specific indicator of significant retroplacental hemorrhage.
Take home points
- Abruptio placentae presents with a rigid, tender uterus and constant pain, while placenta previa is characterized by a soft uterus and painless bleeding.
- Fetal distress is a common and early complication of placental abruption due to the rapid compromise of the maternal-fetal gas exchange unit.
- Abruption can be concealed (no visible blood) or overt (visible bleeding), making uterine rigidity a more reliable indicator than the amount of external blood.
- Immediate intervention is required for abruption to prevent maternal complications like disseminated intravascular coagulation and fetal death.
A nurse is preparing the discharge plan for a client who was managed conservatively for a small, stable placental abruption. Which of the following instructions should the nurse include? Select all that apply
Explanation
Expectant management of a stable placental abruption requires the maintenance of a hemostatic balance at the site of the existing decidual hematoma. This clinical approach aims to prolong gestation to improve fetal maturity while minimizing the risk of recurrent hemorrhage or chronic placental insufficiency. Clients must be strictly educated on identifying markers of secondary detachment and fetal compromise, as the initial site of separation remains a permanent area of vascular vulnerability throughout the remainder of the pregnancy.
Rationale for correct answers
1. Daily assessment of fetal movements provides a non-invasive method for monitoring fetal well-being in a client with compromised placental reserve. A count of fewer than 10 movements within a 2-hour period indicates potential fetal hypoxia and requires immediate medical evaluation. This practice empowers the client to detect subtle changes in intrauterine status that could signal a worsening of the abruption or chronic insufficiency.
3. The client must report any vaginal bleeding immediately because even a small amount can indicate an expansion of the retroplacental hematoma. Recurrence is a significant risk, and fresh bleeding signals a disruption of the decidual interface that could rapidly progress to a life-threatening emergency. Prompt notification allows for STAT assessment of maternal hemodynamic stability and fetal heart rate patterns.
4. Maintaining pelvic rest is mandatory to prevent mechanical irritation of the cervix and lower uterine segment, which could trigger uterine activity. Avoiding heavy lifting reduces intra-abdominal pressure, thereby decreasing the physical stress on the fragile placental attachment site. These restrictions are vital to prevent the progression of a stable, marginal abruption into a more extensive and dangerous separation.
Rationale for incorrect answers
2. Resuming sexual intercourse is strictly contraindicated for any client with a history of placental abruption. The mechanical stimulation of the cervix and the prostaglandins in semen can trigger uterine contractions, which increase the risk of recurrent hemorrhage and further placental detachment. Pelvic rest must be maintained regardless of the absence of active bleeding to preserve the integrity of the pregnancy.
5. Increasing physical activity to include aerobic exercise is dangerous for a client managed conservatively for placental separation. Vigorous movement can increase the shear forces between the placenta and the uterine wall, potentially causing a catastrophic re-bleed. The focus for these clients is on restricted activity to minimize maternal heart rate spikes and maintain stable uteroplacental perfusion at the existing site.
Test-taking strategy
- Identify the Management Goal: Conservative management (expectant management) focuses on safety and surveillance to reach a safer gestational age.
- Evaluate Activity Risks: Rule out any choice that increases physical or mechanical stress, such as exercise (choice 5) or intercourse (choice 2), as these threaten decidual stability.
- Prioritize Monitoring: Select options that provide objective criteria for the client to assess stability, such as fetal kick counts (choice 1).
- Apply the Pelvic Rest Rule: In cases of third-trimester bleeding or placental issues, pelvic rest (choice 4) is a standard safety precaution to prevent trauma to the placental site.
- Identify Red Flags: Any instruction to immediately report a hallmark symptom (choice 3) is a priority in discharge teaching for a high-risk obstetric patient.
Take home points
- Daily fetal movement monitoring is a critical surrogate for assessing placental gas exchange in the home setting.
- Pelvic rest, including the total avoidance of douching and intercourse, is required to prevent mechanical disruption of the placenta.
- Any recurrence of vaginal bleeding or new-onset abdominal pain must be treated as a potential obstetric emergency.
- Conservative management is only maintained as long as maternal vital signs and fetal heart rate patterns remain reassuring.
A nurse is assessing a client for Disseminated Intravascular Coagulation (DIC) following a severe placental abruption. Which of the following assessment findings would support this diagnosis? Select all that apply
Explanation
Disseminated intravascular coagulation is a secondary consumptive coagulopathy triggered by the release of tissue thromboplastin from the damaged placenta into maternal circulation. This massive activation of the clotting cascade leads to widespread microvascular thrombi, which paradoxically exhaust the available supply of platelets and coagulation factors. Consequently, the client experiences systemic hemorrhage as the body loses its ability to form stable clots, while simultaneous fibrinolysis generates fibrin degradation products that further inhibit primary hemostasis.
Rationale for correct answers
1. Oozing of blood from a venipuncture site is a classic clinical indicator of a profound coagulation deficit. In the context of an abruption, this finding suggests that the circulating levels of clotting factors have been depleted to the point where the body cannot maintain hemostasis at previous trauma sites. This "weeping" from minor puncture wounds is a hallmark sign that the client has transitioned into the hemorrhagic phase of the disorder.
2. The development of petechiae on the chest and arms reflects microvascular bleeding due to a critical lack of platelets. These small, non-blanchable red or purple spots indicate that capillary integrity is failing because there are insufficient thrombocytes to plug minute endothelial gaps. Petechiae serve as an early cutaneous warning of widespread consumption of the cellular components necessary for blood transition from a liquid to a solid state.
4. Spontaneous bleeding from the mucous membranes, such as the gums, indicates that the depletion of coagulation factors has reached a systemic level. This occurs because the fibrinogen stores are being rapidly utilized to form unnecessary microclots elsewhere in the body. Spontaneous gingival hemorrhage is a high-priority assessment finding that confirms the client is at extreme risk for internal exsanguination following the initial placental event.
Rationale for incorrect answers
3. A fibrinogen level significantly elevated above 450 mg/dL is an incorrect finding for this diagnosis, as fibrinogen is consumed, not increased. In an active case of consumption, the nurse would expect to see levels drop well below the normal pregnancy range (usually < 150 mg/dL). An elevated level would suggest a normal physiological response to pregnancy or an acute phase reactant, rather than the pathological depletion seen in this syndrome.
5. A platelet count of 450,000/mm3 is within the normal or slightly high range and contradicts a diagnosis of this nature. The consumption of thrombocytes during the widespread formation of microthrombi results in thrombocytopenia, typically with counts falling significantly below 100,000/mm3. A high or normal count indicates that the hemostatic system is still intact and the client is not currently suffering from this specific consumptive complication.
Test-taking strategy
- Identify the Core Pathology: Recognize that this condition is a consumption disorder, meaning that laboratory values for clotting components will be decreased.
- Recognize Clinical Bleeding: Look for signs of bleeding in unexpected areas, such as old IV sites (choice 1) or mucous membranes (choice 4).
- Evaluate Lab Values: Rule out choice 3 and choice 5 because they describe elevated or normal values; the correct laboratory signs include decreased fibrinogen and decreased platelets.
- Observe Skin Changes: Understand that petechiae and purpura (choice 2) are the primary dermatological manifestations of the low platelet counts associated with this emergency.
- Link to the Cause: Connect the placental abruption to the release of thromboplastin, which acts as the "match" that starts the systemic fire of microclotting and subsequent bleeding.
Take home points
- Disseminated intravascular coagulation is a life-threatening emergency characterized by both excessive clotting and paradoxical systemic bleeding.
- Laboratory markers include decreased platelets, decreased fibrinogen, prolonged prothrombin time, and elevated D-dimer levels.
- Nursing management must focus on volume replacement and the administration of blood products like fresh frozen plasma and cryoprecipitate.
- Frequent assessment for occult bleeding, such as hematuria or melena, is vital to detect internal progression of the coagulopathy.
A nurse is caring for a client at 32 weeks gestation with a suspected concealed abruptio placentae. Which of the following nursing actions are priorities? Select all that apply
Explanation
Concealed abruptio placentae is a high-acuity obstetric emergency characterized by the sequestration of blood between the decidua basalis and the uterine wall. This internal hemorrhage creates a retroplacental hematoma that increases intrauterine pressure, leading to myometrial tetany and maternal-fetal hemodynamic collapse. Because the bleeding is not visible externally, clinical assessment must focus on detecting occult expansion of the hematoma and maintaining systemic oxygenation to preserve fetal viability during the acute event.
Rationale for correct answers
1. Establishing a large-bore peripheral venous access device (18-gauge or larger) is a critical priority to facilitate rapid volume expansion. In a severe abruption, the client can lose a significant portion of their circulating volume into the retroplacental space, requiring immediate administration of crystalloids or blood products. Maintaining vascular patency ensures that the clinical team can respond to sudden hypovolemic shock without delay.
2. Monitoring the fundal height every hour provides an objective measurement of the volume of concealed blood accumulating within the uterus. As the retroplacental hematoma expands, it physically displaces the uterus upward, causing the uterine fundus to rise in the abdomen. This assessment is the most sensitive bedside indicator of progressive hemorrhage when external vaginal bleeding is absent or minimal.
4. Administering supplemental oxygen at 10 L/minute via a non-rebreather mask maximizes maternal arterial oxygen saturation. This intervention enhances the oxygen gradient across the functional portion of the placenta that remains attached. By increasing the partial pressure of oxygen in the intervillous space, the nurse helps mitigate the fetal hypoxia caused by the reduction in placental surface area.
Rationale for incorrect answers
3. Placing the client in a supine position is contraindicated because it causes the gravid uterus to compress the inferior vena cava and descending aorta. This aortocaval compression reduces venous return to the heart, leading to decreased maternal cardiac output and worsened placental perfusion. The nurse should instead use a lateral tilt or side-lying position to optimize maternal hemodynamics and fetal oxygenation.
5. Performing a digital vaginal exam is strictly contraindicated in the presence of third-trimester vaginal bleeding or suspected placental detachment until placenta previa is ruled out. Manual manipulation of the cervix can exacerbate placental separation or trigger massive hemorrhage from the lower uterine segment. Assessing for cervical ripening is not a priority during an acute abruption, as the immediate focus is on maternal-fetal stabilization and potential emergency delivery.
Test-taking strategy
- Identify the Emergency: Recognize that concealed abruption involves hidden internal bleeding that requires indirect monitoring and aggressive stabilization.
- Prioritize Circulation (C): Choice 1 addresses the need for intravenous access to manage potential or actual hypovolemic shock.
- Prioritize Oxygenation (A/B): Choice 4 addresses the immediate need to improve fetal gas exchange through maternal oxygen therapy.
- Select Condition-Specific Assessment: In a concealed bleed, the most specific physical assessment is measuring the rising fundus (choice 2).
- Eliminate Harmful Actions: Rule out the supine position (choice 3) and vaginal exams (choice 5) because they compromise perfusion or increase the risk of further bleeding.
Take home points
- Increasing fundal height and board-like abdominal rigidity are the primary clinical indicators of a concealed placental abruption.
- Large-bore intravenous access (18-gauge) is mandatory for all clients with suspected abruption to allow for rapid fluid and blood resuscitation.
- Oxygen therapy via non-rebreather mask is a standard component of intrauterine resuscitation to support fetal oxygenation during placental failure.
- Aortocaval compression must be avoided by maintaining the client in a lateral position to ensure maximal maternal-fetal blood flow.
A nurse is teaching a client about risk reduction for placental abruption in a future pregnancy. Which of the following statements by the client indicates an understanding of the teaching? Select all that apply
Explanation
Placental abruption risk reduction in subsequent gestations focuses on mitigating vascular stressors and preventing mechanical trauma to the uterine wall. Recurrence is often driven by chronic hypertension or inflammatory changes that weaken the decidual vessels, making them prone to rupture. By addressing modifiable behavioral factors and ensuring strict hemodynamic control, the structural integrity of the maternal-fetal interface can be better preserved, reducing the statistical probability of a repeat decidual hemorrhage.
Rationale for correct answers
1. Correct seatbelt placement is a vital safety measure to prevent blunt abdominal trauma, which is a leading external cause of abruption. Placing the lap belt low, under the belly and across the hips, ensures that the force of a sudden stop is distributed to the pelvic bones rather than the gravid uterus. This prevents the shearing force between the placenta and the uterine wall that occurs during rapid deceleration or direct impact.
2. Consistent attendance at prenatal appointments allows for the early detection and management of gestational hypertension or preeclampsia. Stable control of maternal blood pressure reduces the hydrostatic pressure within the spiral arteries of the decidua. This proactive monitoring is essential for identifying vascular trends that could lead to a recurrence of placental detachment if left untreated.
3. Cessation of tobacco use before conception eliminates a major chemical trigger for placental vascular damage. Nicotine and other toxins in cigarettes cause vasoconstriction and contribute to decidual necrosis, which significantly increases the risk of abruption. Stopping smoking restores better placental oxygenation and improves the overall health of the maternal vascular endothelium, creating a safer environment for the next pregnancy.
5. Consulting with a maternal-fetal specialist before conception allows for the development of a tailored high-risk management plan. This approach ensures that any underlying thrombophilias or chronic conditions are addressed before the physiological demands of pregnancy begin. Establishing a plan for serial ultrasounds and frequent surveillance provides a structured framework for the early detection of placental insufficiency.
Rationale for incorrect answers
4. Believing that extra monitoring is only necessary if bleeding occurs is a dangerous misconception that ignores the risk of concealed abruption. Many placental complications, including growth restriction and retroplacental hematoma formation, occur without overt vaginal bleeding. Waiting for symptoms to appear before seeking enhanced surveillance would delay the detection of fetal compromise or worsening maternal hypertensive states.
Test-taking strategy
- Identify the Preventative Focus: The goal is to find actions that actively reduce risk or enhance the detection of early complications.
- Assess Mechanical Safety: Recognize that trauma prevention (choice 1) is a key component of obstetric education for preventing sudden placental separation.
- Prioritize Clinical Surveillance: Value consistent monitoring (choice 2 and choice 5) over reactive care (choice 4) for high-risk obstetric histories.
- Eliminate Behavioral Triggers: Connect smoking cessation (choice 3) directly to the preservation of placental vascular health and decidual integrity.
- Rule out Reactive Management: Eliminate choice 4 because it suggests a wait-and-see approach, which is inappropriate for a condition that can be fatal before symptoms are visible.
Take home points
- Proper seatbelt use involves placing the lap belt under the abdomen to protect the placenta from shearing forces during trauma.
- Smoking and illicit drug use are the most significant modifiable risk factors for the recurrence of placental abruption.
- Preconception counseling with a high-risk specialist is recommended to optimize maternal health and establish a surveillance protocol.
- Chronic hypertension must be aggressively managed as it is the most common underlying cause of non-traumatic placental separation.
Exams on Abruptio Placentae
Custom Exams
Login to Create a Quiz
Click here to loginLessons
- Objectives
- Introduction
- Overview Of Abruptio Placentae
- Practice Exercise 1
- Etiology And Risk Factors
- Clinical Manifestations And Assessment Findings
- Practice Exercise 2
- Diagnostic Evaluation
- Practice Exercise 3
- Complications Of Abruptio Placentae
- Practice Exercise 4
- Medical And Obstetric Management
- Practice Exercise 5
- Nursing Management Of Abruptio Placentae
- Practice Exercise 6
- Patient Education And Prevention Strategies
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
Upon completion of this section, the nursing student will be able to:
- Define abruptio placentae using correct obstetric terminology and medical language.
- Distinguish abruptio placentae from other causes of antepartum hemorrhage.
- Describe the epidemiology and incidence of abruptio placentae across maternal populations.
- Identify population-level trends and high-risk groups.
- Explain the pathophysiology of placental separation at the maternal–fetal interface.
- Correlate placental separation with maternal hemorrhage and fetal hypoxia.
- Differentiate the types of abruptio placentae based on bleeding patterns and clinical presentation.
- Compare revealed, concealed, and mixed hemorrhage.
- Apply foundational knowledge of abruptio placentae to early clinical recognition and nursing assessment.
Introduction
Abruptio placentae is a serious obstetric complication characterized by premature separation of a normally implanted placenta from the uterine wall after 20 weeks of gestation and before delivery of the fetus.
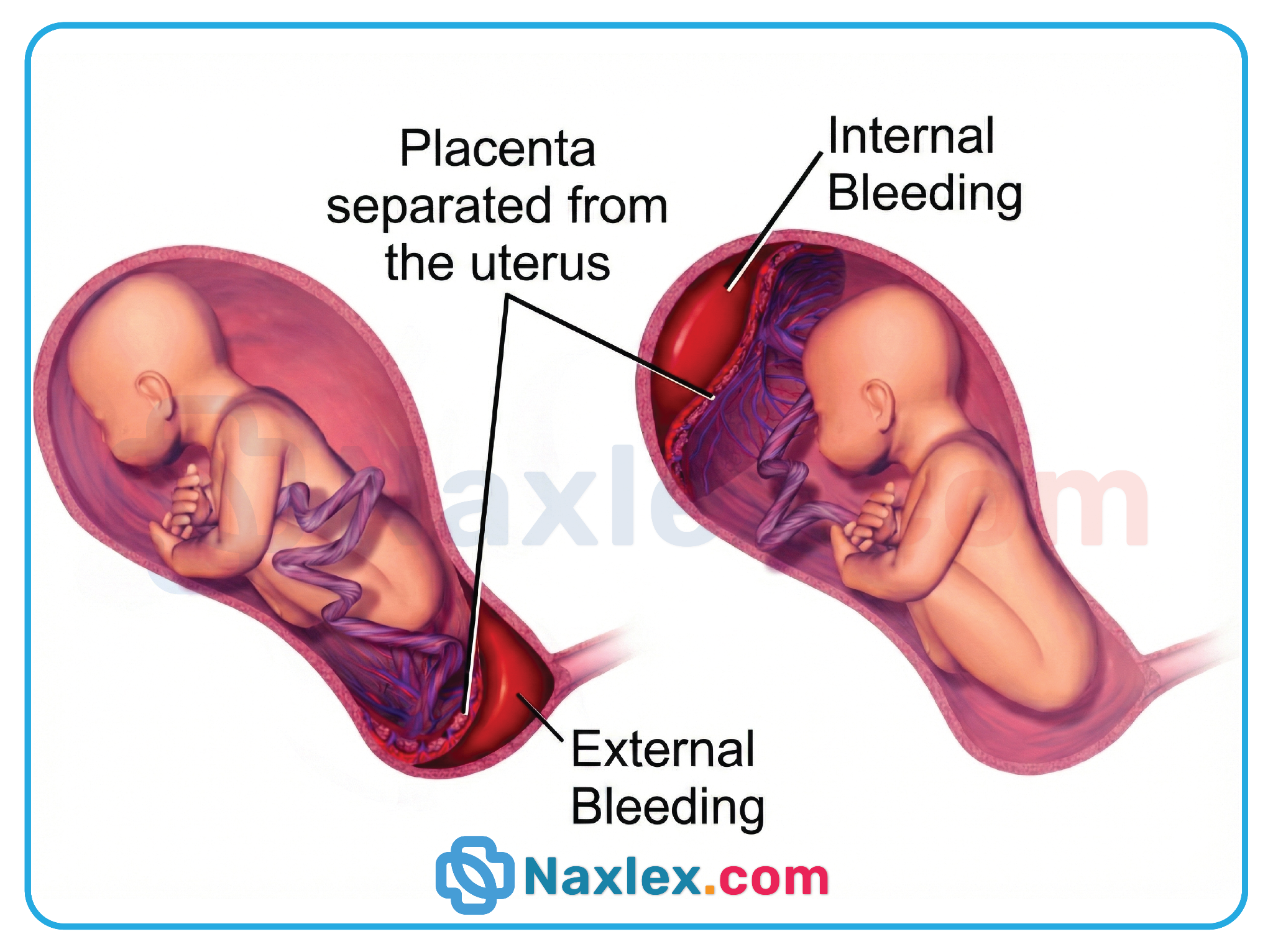
- Abruptio placentae represents a true obstetric emergency due to the risk of:
- Severe maternal hemorrhage
- Fetal hypoxemia and acidosis
- Disseminated intravascular coagulation (DIC)
- Maternal and fetal mortality
- The condition disrupts uteroplacental perfusion, impairing oxygen and nutrient delivery to the fetus.
- Clinical severity varies widely, ranging from mild separation with minimal symptoms to catastrophic placental detachment.
Nursing Insights
- Vaginal bleeding may be absent or minimal despite massive internal blood loss.
- Pain is a key differentiating feature between abruptio placentae and placenta previa.
- A firm or board-like uterus is a red flag finding that requires immediate escalation of care.
Overview Of Abruptio Placentae
3.1 Definition and Terminology
Abruptio placentae is defined as the partial or complete premature separation of the placenta from the decidua basalis of the uterus prior to fetal delivery.
- Occurs after 20 weeks gestation
- Results in hemorrhage between the placenta and uterine wall
- Leads to compromised maternal–fetal exchange
Key Terminology
- Placental abruption: Synonymous with abruptio placentae
- Antepartum hemorrhage: Vaginal bleeding occurring after 20 weeks gestation
- Couvelaire uterus: Blood infiltration into the myometrium causing uterine atony
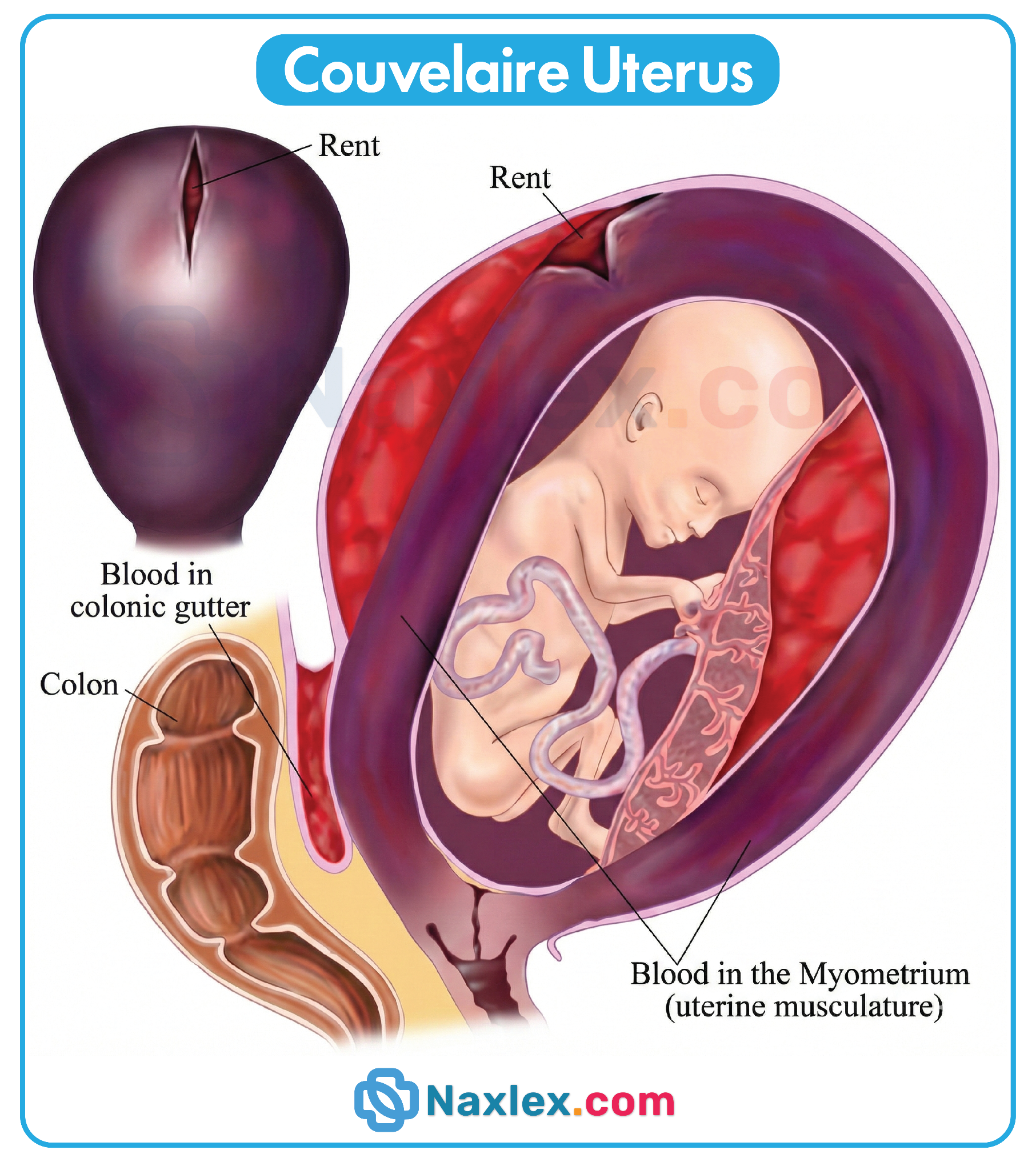
Nursing Insights
- The degree of placental separation does not always correlate with visible bleeding.
- Fetal compromise can occur rapidly even with small placental detachments.
3.2 Epidemiology and Incidence
- Incidence ranges from 0.5–1.5% of all pregnancies.
- Abruptio placentae accounts for a significant proportion of antepartum fetal deaths.
- Higher incidence is observed in:
- Clients with chronic hypertension
- Clients with a history of prior placental abruption
- Clients exposed to trauma or substance use
Nursing Insights
- A prior history of abruptio placentae increases recurrence risk by 10–15%.
- Disparities exist due to access to prenatal care and chronic disease burden.
3.3 Pathophysiology of Placental Separation
Abruptio placentae begins with rupture of maternal vessels in the decidua basalis.
- Blood accumulates between the placenta and uterine wall forming a retroplacental hematoma.
- Progressive separation reduces surface area available for gas exchange.
- Uterine irritability and hypertonicity develop due to blood infiltration.
Physiological Consequences
- Maternal hypovolemia due to acute blood loss
- Fetal hypoxemia and metabolic acidosis
- Activation of coagulation cascade leading to DIC
Nursing Insights
- Fetal distress reflects placental insufficiency, not primary fetal pathology.
- Continuous uterine rigidity suggests ongoing concealed hemorrhage.
3.4 Types of Abruptio Placentae
Revealed (External) Hemorrhage
- Blood escapes through the cervix resulting in visible vaginal bleeding.
- Uterus may be tender but less rigid.
- Bleeding severity is more accurately estimated.
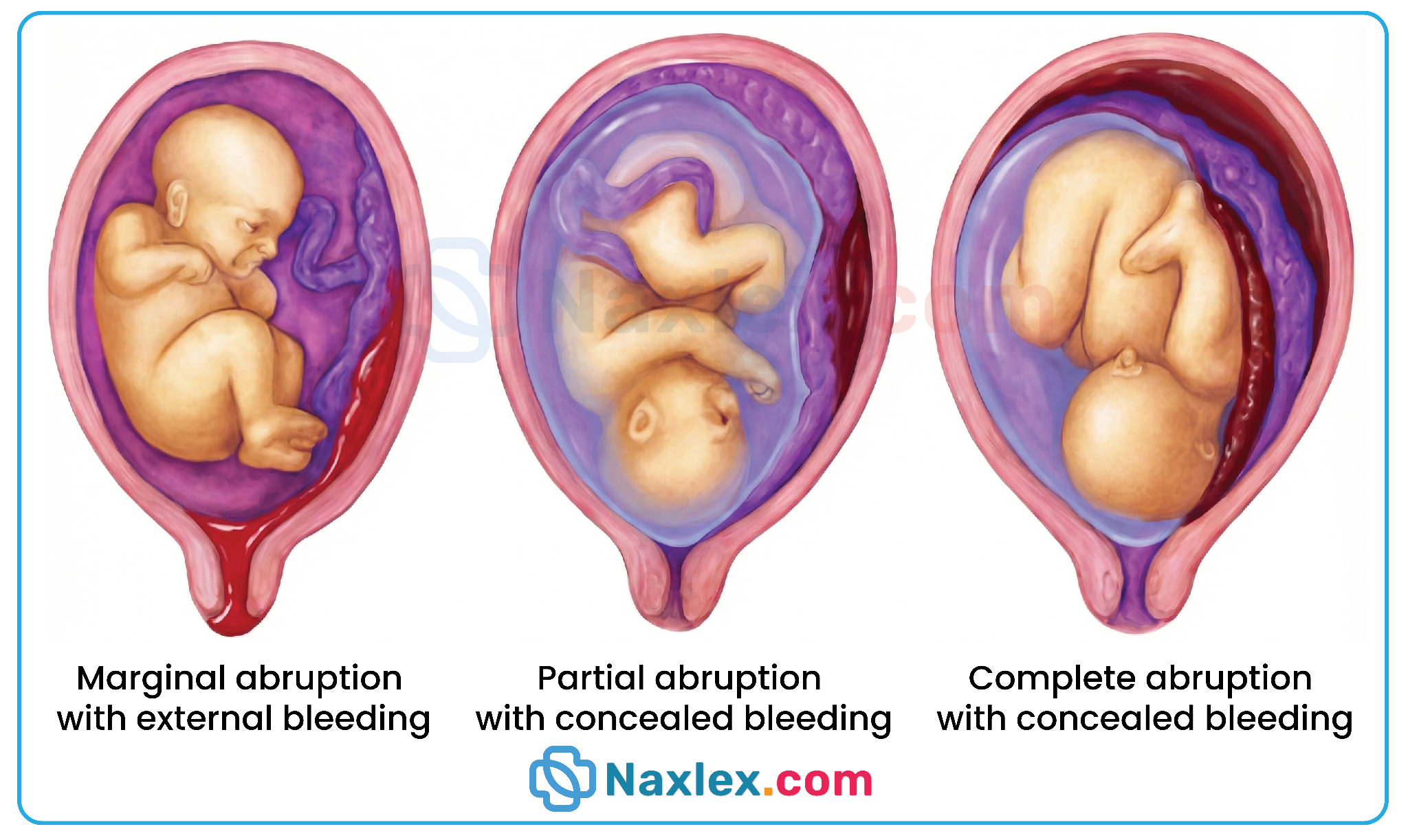
Concealed (Internal) Hemorrhage
- Blood remains trapped behind the placenta.
- Minimal or absent vaginal bleeding.
- Uterus becomes firm, tense, and board-like.
- High risk for maternal shock and DIC.
Mixed Hemorrhage
- Features of both concealed and revealed bleeding.
- Partial external bleeding with ongoing internal accumulation.
Nursing Insights
- Concealed hemorrhage is more dangerous due to delayed recognition.
- Maternal vital signs may deteriorate before bleeding is visually apparent.
Etiology And Risk Factors
The precise primary etiology of abruptio placentae is often multifactorial, involving a combination of chronic vascular degeneration and acute mechanical or chemical triggers.
- Vascular Pathologies and Hypertension
- Chronic Hypertension: This is the most consistent maternal predisposing factor, leading to degenerative changes in the spiral arterioles.
- Preeclampsia and Gestational Hypertension: Acute vasospasm and endothelial damage increase the friability of the placental-uterine interface.
- Lifestyle and Substance Use
- Cocaine Use: This is a high-yield risk factor due to the profound localized vasoconstriction and acute maternal hypertension it induces, which can cause immediate placental shearing.

-
- Tobacco Smoking: Nicotine and carbon monoxide cause placental hypoxemia and vasoconstriction, leading to vascular necrosis of the decidua.
- Mechanical and Physical Factors
- Abdominal Trauma: Blunt force trauma from motor vehicle accidents, falls, or domestic violence can cause a "shearing" effect where the inelastic placenta detaches from the elastic uterine wall.
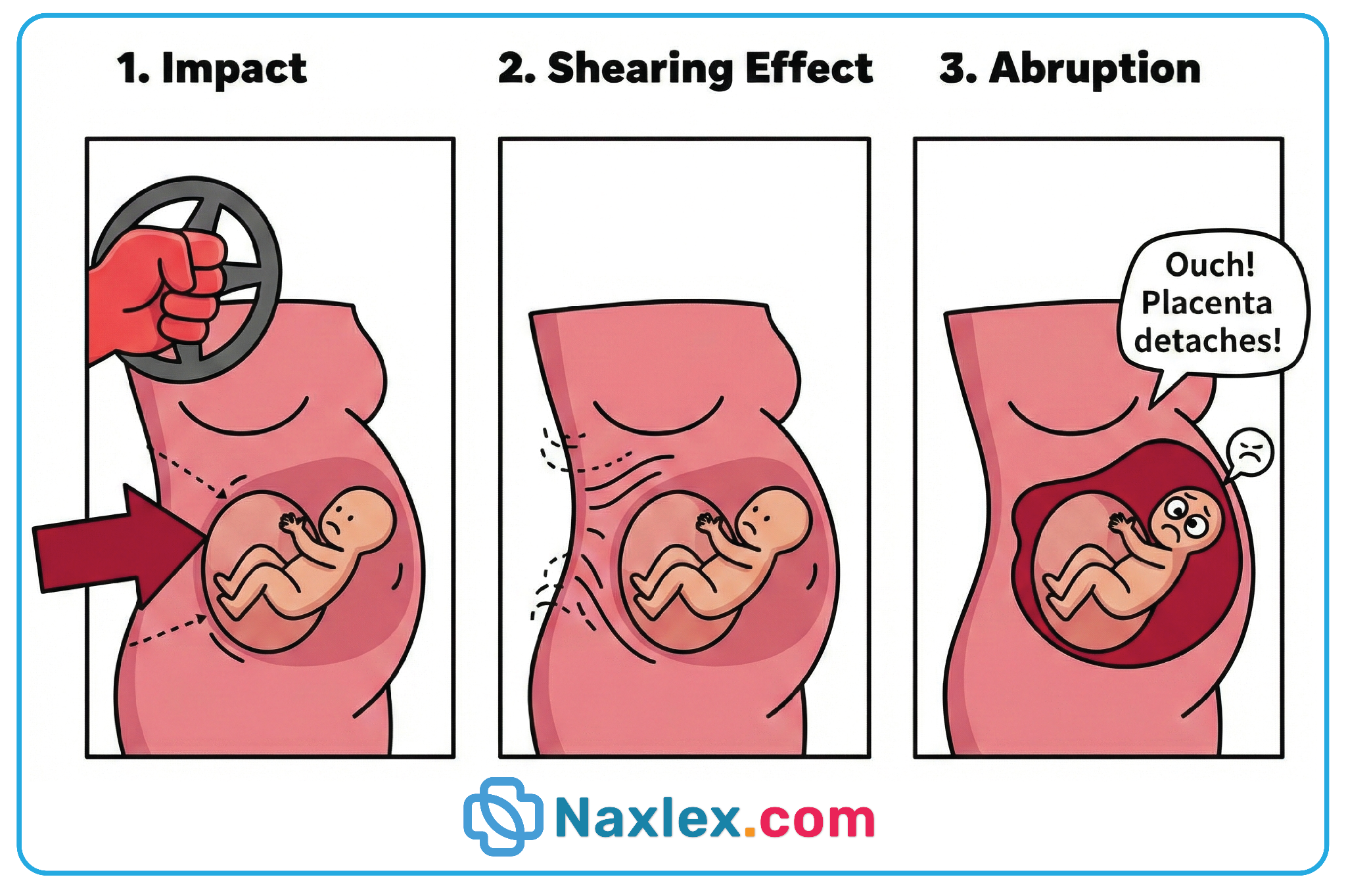
-
- Sudden Uterine Decompression: Rapid loss of amniotic fluid, such as during spontaneous rupture of membranes in polyhydramnios or the delivery of the first twin, can cause the uterus to shrink rapidly, pulling away from the placenta.
- Obstetric History and Demographics
- Prior Abruption: A client with one previous abruption has a 5% to 17% recurrence risk; after 2 previous abruptions, the risk exceeds 25%.
- Advanced Maternal Age: Increased risk in clients > 35 years of age due to associated vascular comorbidities.
- Multiparity: High parity is statistically correlated with a higher incidence of placental attachment anomalies.
Nursing Insights
A nurse must prioritize screening every pregnant client for domestic violence and substance use at every prenatal visit and upon admission to the labor unit. Because cocaine-induced abruption can occur with minimal external bleeding but extreme uterine tetany, a toxicology screen is a critical component of the assessment for any client presenting with sudden, unexplained abdominal pain.
Clinical Manifestations And Assessment Findings
6.1 Maternal Clinical Manifestations
- Abdominal Pain: Typically described as sudden, intense, and unremitting (localized or generalized).
- Uterine Tenderness and Rigidity: The uterus may feel "board-like" on palpation due to high resting tone (hypertonicity).
- Vaginal Bleeding: May be absent (concealed), dark red (old blood), or bright red (active bleeding).
- Hemodynamic Instability: Signs of hypovolemic shock (hypotension, tachycardia) that may be disproportionate to visible blood loss.
6.2 Fetal Clinical Manifestations
- Abnormal Fetal Heart Rate (FHR) Patterns: Early signs include fetal tachycardia; late signs include recurrent late decelerations, decreased variability, or a sinusoidal pattern.
- Fetal Bradycardia: Indicates terminal hypoxia and requires immediate delivery.
- Decreased Fetal Movement: A subjective report by the client indicating fetal distress.
6.3 Differences Between Concealed and Revealed Abruptio Placentae
|
Feature |
Revealed (External) |
Concealed (Internal) |
|
Visible Bleeding |
Evident vaginal bleeding (often dark red) |
No visible vaginal bleeding |
|
Pain Level |
Severe, but may be intermittent |
Agonizing, constant, and unremitting |
|
Uterine Tone |
Increased/Hypertonic |
Rigid, "board-like," and extremely hard |
|
Fundal Height |
Remains consistent with gestational age |
Increases as internal hematoma expands |
|
Shock |
Correlates with visible blood loss |
Out of proportion to visible blood loss |
6.4 Physical Examination Findings
- Uterine Palpation: The nurse will note a lack of uterine relaxation between contractions (tachysystole).
- Vital Signs: Narrowing pulse pressure, tachycardia, and eventual tachypnea (Respiratory Rate > 20 breaths/min).
- Fundal Height: Measuring the fundus is essential; a rise of 1 cm or more in an hour can indicate a significant concealed hemorrhage.
6.5 Differential Diagnoses of Abruptio Placentae
- Placenta Previa: Characterized by painless, bright red bleeding and a soft, non-tender uterus.
- Uterine Rupture: Often occurs during labor in a client with a previous cesarean scar; characterized by a sudden loss of fetal station and "recession" of the presenting part.
- Preterm Labor: Characterized by rhythmic contractions and cervical change, usually without the board-like rigidity seen in abruption.
Nursing Insights
When a client is admitted with suspected abruption, the nurse must never perform a digital vaginal examination until placenta previa has been ruled out by ultrasound. However, once abruption is confirmed, the nurse must be prepared for "precipitous labor" as the blood within the myometrium acts as a powerful uterine irritant, often causing the cervix to dilate very rapidly.
Diagnostic Evaluation
8.1 Clinical Diagnosis and Limitations
- Primary Diagnostic Method: Abruptio placentae is primarily a clinical diagnosis based on the triad of sudden abdominal pain, uterine hypertonicity/tenderness, and vaginal bleeding.
- Diagnostic Challenges:
- In concealed abruptions, external bleeding is absent, making the diagnosis entirely dependent on physical assessment and fetal heart rate patterns.
- Initial symptoms may mimic other conditions, such as preterm labor or appendicitis, potentially delaying life-saving intervention.
- Limitations of Clinical Assessment:
- Subjective assessment of pain may vary between clients.
- External bleeding is an unreliable indicator of total blood loss, as several liters can be sequestered in the retroplacental space.
8.2 Laboratory Investigations
- Complete Blood Count (CBC):
- Hemoglobin and Hematocrit: Serial monitoring is required; however, values may initially appear normal due to hemoconcentration until compensatory fluid shifts occur.
- White Blood Cell Count: May be elevated as a physiological response to stress and tissue necrosis.
- Coagulation Profile:
- Prothrombin Time (PT) and Activated Partial Thromboplastin Time (aPTT): These values become prolonged as clotting factors are consumed in the formation of the retroplacental hematoma.
- Platelet Count: Thrombocytopenia (Platelets < 150,000/mm³) occurs rapidly in severe cases as platelets are trapped within the site of separation.
- Fibrinogen Levels:
- Critical Marker: Fibrinogen is the most sensitive indicator of the severity of abruption.
- Normal Pregnancy Levels: Typically elevated (300 to 600 mg/dL).
- Critical Levels: A level < 200 mg/dL is highly suggestive of a major abruption; levels < 100 mg/dL indicate a severe risk for Disseminated Intravascular Coagulation (DIC).
8.3 Imaging Studies
- Ultrasound (US) Findings:
- Sensitivity: Ultrasound is relatively insensitive for detecting abruption, identifying only 25% to 50% of cases.
- Purpose: The primary role of ultrasound is to rule out placenta previa, not to definitively rule out abruption.
- Visual Evidence: Findings may include retroplacental clots (hyperechoic or isoechoic to the placenta) and increased placental thickness.
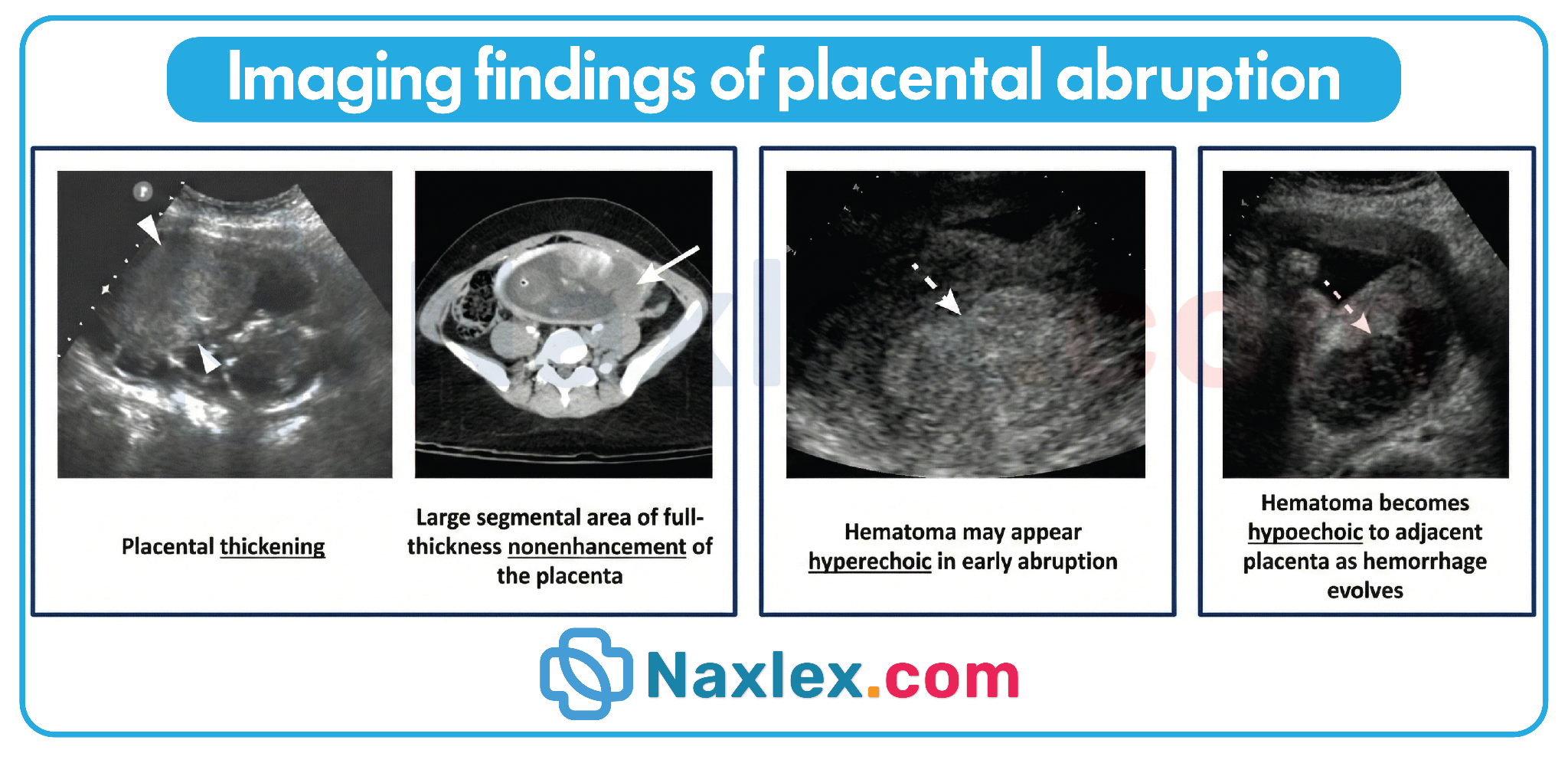
- Doppler Velocimetry:
- Utility: Used to evaluate umbilical artery blood flow.
- Findings: In placental insufficiency secondary to abruption, there may be absent or reversed end-diastolic flow, indicating high resistance and severe fetal compromise.
Nursing Insights A nurse must prioritize laboratory results over ultrasound findings when abruption is suspected. If the ultrasound is negative but the client has a rigid abdomen and the fibrinogen level is dropping, the nurse must advocate for immediate intervention. A "negative" ultrasound does NOT rule out a life-threatening abruption!
Complications Of Abruptio Placentae
Abruptio placentae, also known as placental abruption, is the premature separation of a normally implanted placenta after 20 weeks gestation and before the birth of the fetus. This obstetric emergency can lead to significant maternal and fetal morbidity and mortality. Complications arise due to maternal hemorrhage, fetal hypoxia, and associated coagulopathy.
Maternal Complications
- Hemorrhagic Shock
- Rapid blood loss can exceed 1,000 mL depending on severity of abruption.
- Manifestations include hypotension (BP <90/60 mmHg), tachycardia (>100 bpm), pallor, diaphoresis, and anxiety.
- Nursing Insights: Immediate recognition of hypovolemic shock is critical; prioritize large-bore IV access (14–16G) and fluid resuscitation with isotonic crystalloids.
- Disseminated Intravascular Coagulation (DIC)
- Caused by release of thromboplastin from retroplacental clot.
- Clinical signs: oozing from IV sites, ecchymoses, prolonged bleeding, decreased fibrinogen.
- Labs: prolonged PT/PTT, thrombocytopenia, low fibrinogen, elevated D-dimer.
- Nursing Insights: Monitor for unexplained bleeding and prepare blood products (FFP, platelets, cryoprecipitate).
- Couvelaire Uterus
- Extravasation of blood into the myometrium and peritoneal tissues.
- Uterus appears blue or purplish, rigid, and poorly contractile.
- Increases risk of uterine atony and postpartum hemorrhage (PPH).
- Nursing Insights: Anticipate potential hysterectomy in severe cases; monitor uterine tone postpartum.
- Acute Kidney Injury (AKI)
- Secondary to hypovolemia and shock.
- Monitor urine output (<30 mL/hr may indicate renal compromise) and renal function tests (BUN, creatinine).
- Nursing Insights: Maintain adequate IV fluids and monitor hemodynamics to prevent renal ischemia.
- Anemia
- Blood loss leads to decreased hemoglobin and hematocrit.
- Nursing Insights: Monitor CBC, assess for fatigue, tachycardia, pallor; prepare for transfusions if indicated.
- Infection
- Risk increases with prolonged hemorrhage or invasive procedures.
- Nursing Insights: Monitor temperature, WBC count, and signs of endometritis postpartum.
Fetal Complications
- Fetal Hypoxia
- Impaired uteroplacental perfusion leads to decreased oxygen and nutrient delivery.
- Fetal heart rate (FHR) abnormalities: late decelerations, decreased variability, bradycardia.
- Nursing Insights: Continuous electronic fetal monitoring (EFM) is essential; prepare for emergent cesarean if nonreassuring FHR is detected.
- Intrauterine Growth Restriction (IUGR)
- Chronic or recurrent abruption reduces placental function, impairing fetal growth.
- Nursing Insights: Serial ultrasounds and Doppler studies to monitor growth trajectory.
- Preterm Birth
- Often occurs due to maternal instability or fetal compromise.
- Nursing Insights: Administer corticosteroids (betamethasone 12 mg IM q24h ×2) to enhance fetal lung maturity if preterm delivery anticipated.
- Fetal Demise
- Severe abruptio can lead to fetal death due to acute hypoxia.
- Nursing Insights: Prepare family for counseling; initiate appropriate bereavement support if fetal demise occurs.
Other Complications
- Uterine Rupture
- Rare, but may occur in severe, concealed hemorrhage with prior uterine scarring.
- Nursing Insights: Assess for sudden abdominal pain, loss of fetal station, and maternal shock.
- Postpartum Hemorrhage
- Secondary to uterine atony, retained clot, or Couvelaire uterus.
- Nursing Insights: Monitor fundal tone, vital signs, and vaginal bleeding; be prepared for uterotonic therapy (oxytocin, misoprostol) or surgical intervention.
Table: Key Maternal vs. Fetal Complications
|
Complication |
Maternal Clinical Manifestations |
Fetal Clinical Manifestations |
Nursing Interventions |
|
Hemorrhagic Shock |
Hypotension, tachycardia, pallor |
Possible fetal tachycardia initially |
Rapid IV fluids, monitor vitals, prep for transfusion |
|
Disseminated Intravascular Coagulation (DIC) |
Oozing, ecchymosis, prolonged PT/PTT |
Fetal distress secondary to maternal instability |
Monitor labs, administer blood products |
|
Couvelaire Uterus |
Uterine rigidity, poor contraction |
Risk of fetal hypoxia due to reduced perfusion |
Monitor uterine tone, prepare for hysterectomy |
|
Fetal Hypoxia |
- |
Late decelerations, bradycardia |
Continuous EFM, prepare for emergent delivery |
|
Preterm Birth |
- |
Immature lungs, risk for RDS |
Administer corticosteroids, neonatal ICU prep |
|
Fetal Demise |
- |
Absence of FHR |
Emotional support, bereavement counseling |
Nursing Insights
- Rapid Recognition and Prioritization
- Maternal vital sign changes may precede fetal compromise; always stabilize mother first.
- Continuous Fetal Monitoring
- Essential to detect early signs of fetal hypoxia; tachycardia may initially indicate stress, whereas bradycardia indicates severe compromise.
- Preparation for Emergent Delivery
- Cesarean section is often indicated for maternal or fetal instability.
- Fluid and Blood Management
- Establish at least 2 large-bore IV lines, monitor urine output, prepare for massive transfusion if necessary.
- Patient and Family Support
- Emotional support, clear communication, and counseling are critical, especially in cases of fetal loss.
Medical And Obstetric Management
12.1 Management Based on Severity
- Mild Abruption (Grade 1):
- Clinical Presentation: Minimal vaginal bleeding (< 500 mL), mild uterine tenderness, and no signs of maternal shock or fetal distress.
- Management Strategy: Conservative or expectant management is employed if the client is stable and the fetus is preterm.
- Monitoring: Continuous external fetal monitoring (EFM) and serial assessment of maternal vital signs and hematological parameters (Complete Blood Count and Coagulation Profile).
- Moderate to Severe Abruption (Grade 2 and 3):
- Clinical Presentation: Significant hemorrhage (revealed or concealed), persistent uterine tetany/rigidity, and evidence of maternal compromise (tachycardia, hypotension) or fetal distress (late decelerations, bradycardia).
- Management Strategy: Active management focusing on rapid stabilization and delivery.
- Emergency Interventions: Immediate stabilization of maternal hemodynamics using large-bore (16 or 18-gauge) peripheral venous access devices (VAD) and aggressive fluid resuscitation.
12.2 Management Based on Gestational Age
- Preterm (< 34 Weeks Gestation):
- Stable Client/Fetus: Expectant management is utilized to allow for fetal lung maturity.
- Antenatal Corticosteroids: Administration of Betamethasone (12 mg Intramuscularly every 24 hours for 2 doses) to enhance fetal surfactant production.
- Tocolysis: Controversial and generally avoided; however, may be used cautiously in very mild cases to facilitate corticosteroid administration.
- Term or Near-Term (≥ 36 Weeks Gestation):
- Preferred Action: Delivery is indicated to prevent further placental separation and sudden intrauterine fetal demise (IUFD).
- Route: Method of delivery is determined by maternal stability and fetal heart rate patterns.
12.3 Vaginal Delivery Versus Cesarean Delivery
- Vaginal Delivery:
- Indications: Recommended if the mother is hemodynamically stable, the fetal heart rate is reassuring, or in the event of intrauterine fetal demise (IUFD) where a cesarean provides no fetal benefit but increases maternal surgical risk.
- Augmentation: Amniotomy (artificial rupture of membranes) is performed early to decrease intrauterine pressure and potentially decrease the entry of thromboplastin into maternal circulation. Oxytocin may be used with extreme caution.
- Cesarean Delivery:
- Indications: Emergent cesarean is the gold standard for severe abruption with evidence of acute fetal distress, maternal hemodynamic instability, or failed trial of labor.
- Risk Factors: High risk for Disseminated Intravascular Coagulation (DIC) and Couvelaire uterus, which may complicate the surgical procedure.
12.4 Blood Product Replacement Therapy
- Crystalloid Resuscitation: Initial fluid replacement with Lactated Ringer's or Normal Saline 0.9% to maintain a urine output of > 30 mL/hour and a Hematocrit of > 30%.
- Packed Red Blood Cells (PRBCs): Indicated for active hemorrhage or symptomatic anemia to maintain oxygen-carrying capacity.
- Fresh Frozen Plasma (FFP): Utilized to replace clotting factors if the Prothrombin Time (PT) or Activated Partial Thromboplastin Time (aPTT) are prolonged.
- Cryoprecipitate: The primary treatment for low fibrinogen levels (< 150 mg/dL) to provide concentrated fibrinogen and Factor VIII.
- Platelets: Transfused if the platelet count drops below 50,000/mm³ in the presence of active bleeding.
Nursing Insights A nurse must ensure that a "Type and Crossmatch" for at least 2 to 4 units of Packed Red Blood Cells is maintained at all times for a client with a suspected abruption. In an emergency, the nurse should anticipate the administration of O-negative blood if crossmatched blood is not yet available. The nurse must also monitor for Transfusion-Associated Circulatory Overload (TACO) and Hemolytic reactions during rapid replacement therapy.
Nursing Management Of Abruptio Placentae
The nursing management of abruptio placentae is centered on the rapid identification of clinical deterioration, maintenance of maternal hemodynamic stability, and vigilant surveillance of fetal oxygenation status. Because placental abruption is a life-threatening emergency, nursing actions must be prioritized based on the ABC (Airway, Breathing, Circulation) framework of emergency care.
14.1 Priority Nursing Assessments
- Cardiovascular Assessment:
- Monitor maternal vital signs every 5 to 15 minutes during the acute phase.
- Assess for clinical markers of hypovolemic shock, including tachycardia, tachypnea, narrow pulse pressure, and hypotension.
- Evaluate peripheral perfusion by assessing capillary refill time, skin temperature, and the presence of diaphoresis.
- Uterine and Obstetric Assessment:
- Perform frequent palpation of the uterus to detect increasing tonus or "board-like" rigidity.
- Measure fundal height serially; an upward trend in fundal height is a primary indicator of concealed retroplacental hemorrhage.
- Quantify vaginal bleeding by weighing peripads (1 g = 1 mL) and assessing for the presence of dark red blood or clots.
- Hematological Surveillance:
- Assess for systemic signs of Disseminated Intravascular Coagulation (DIC), such as petechiae, ecchymosis, or spontaneous bleeding from the gums and IV venipuncture sites.
- Monitor laboratory values closely, specifically Hemoglobin (Hgb), Hematocrit (Hct), Platelets, Fibrinogen, and Fibrin Split Products (FSP).
Nursing Insights A nurse must never perform a digital vaginal examination on a client presenting with unexplained third-trimester bleeding until placenta previa has been definitively ruled out via ultrasound. Performing a vaginal exam in the presence of previa can trigger catastrophic hemorrhage. The nurse should also be aware that maternal blood pressure may remain within "normal" limits initially due to the physiological hypervolemia of pregnancy, making tachycardia a more sensitive early sign of blood loss.
14.2 Emergency Nursing Interventions
- Positioning: Place the client in a lateral recumbent position (left side preferred) to displace the uterus from the inferior vena cava, thereby maximizing venous return and placental perfusion.
- Oxygen Therapy: Administer supplemental oxygen via a non-rebreather face mask at 8 to 10 L/minute to optimize maternal arterial oxygen saturation and fetal oxygen delivery.
- Interdisciplinary Coordination: Activate the rapid response team or obstetric emergency team and notify the neonatal intensive care unit (NICU) of a high-risk delivery.
- Preoperative Preparation: If fetal distress or maternal instability is noted, immediately prepare the client for an emergent cesarean section by ensuring informed consent is obtained and the client is NPO (nothing by mouth).
14.3 Fluid and Hemodynamic Management
- Vascular Access: Establish and maintain at least two large-bore (16- or 18-gauge) peripheral intravenous (IV) catheters for rapid volume expansion.
- Volume Resuscitation: Initiate rapid infusion of isotonic crystalloids (e.g., Lactated Ringer’s) as ordered to stabilize blood pressure.
- Blood Component Therapy: Administer Packed Red Blood Cells (PRBCs) and fresh frozen plasma (FFP) as indicated by the "massive transfusion protocol" to correct anemia and coagulopathy.
- Renal Perfusion Monitoring: Insert an indwelling Foley catheter with a urometer to monitor hourly urine output.
Nursing Insights The nurse must strictly maintain urine output at ≥ 30 mL/hour. A drop below this threshold is a direct indicator of inadequate organ perfusion and impending acute tubular necrosis. During rapid fluid resuscitation, the nurse must also auscultate lung sounds frequently to detect crackles, which could indicate pulmonary edema or fluid volume overload.
14.4 Fetal Monitoring Responsibilities
- Continuous Surveillance: Utilize continuous external electronic fetal monitoring (EFM) to assess fetal heart rate (FHR) patterns.
- Detection of Hypoxia: Monitor for signs of fetal compromise, including:
- Loss of Variability: Indicates fetal central nervous system depression.
- Late Decelerations: Signals uteroplacental insufficiency.
- Sinusoidal Pattern: Highly suggestive of severe fetal anemia or terminal hypoxia.
- Baseline Shifts: Note any sustained fetal tachycardia (> 160 bpm) or bradycardia (< 110 bpm) and report immediately to the primary health care provider.
Nursing Insights If the nurse observes a non-reassuring fetal heart rate pattern, the "POIS" acronym should be followed: Position (Lateral), Oxygen (10 L non-rebreather), IV fluids (Increase rate), and Stop Oxytocin (if infusing). This provides the best chance for intrauterine resuscitation before surgical intervention.
14.5 Pain Management and Comfort Measures
- Assessment of Pain: Use a standardized pain scale to differentiate between the rhythmic pain of contractions and the constant, agonizing pain associated with placental separation.
- Pharmacological Intervention: Administer IV analgesics as ordered, keeping in mind that maternal hypotension may contraindicate certain regional anesthetics (like epidurals) during an active abruption.
- Psychological Support: Provide clear, concise explanations of procedures to the client and partner to reduce anxiety and the physiological stress response, which can further compromise uterine blood flow.
Patient Education And Prevention Strategies
16.1 Antenatal Education
- Definition and Purpose
- Antenatal education involves instructing the client and family about recognizing complications, optimizing maternal-fetal outcomes, and ensuring early intervention for placental disorders.
- Education focuses on risk recognition, warning signs, and lifestyle modifications to prevent abruptio placentae.
- Key Teaching Points
- Educate clients about signs of placental complications:
- Sudden abdominal or back pain.
- Vaginal bleeding, dark red or brown.
- Uterine tenderness or rigidity.
- Decreased or absent fetal movement.
- Lifestyle modifications:
- Avoid smoking, cocaine, and illicit drug use, as these increase placental abruption risk by causing vasoconstriction and vascular injury.
- Manage chronic hypertension with antihypertensive therapy as prescribed.
- Limit exposure to trauma and advise on safe physical activity.
- Explain fetal monitoring and follow-up visits:
- Non-stress tests (NST) and ultrasonography may be used to monitor fetal well-being.
- Emphasize reporting decreased fetal movement immediately.
- Discuss emergency preparedness:
- Identify when to seek immediate care for sudden bleeding or pain.
- Review hospital admission process for potential antepartum hemorrhage.
- Educate clients about signs of placental complications:
Nursing Insights
- Nurses should assess the client’s understanding of warning signs at each prenatal visit.
- Reinforce the importance of adherence to antihypertensive medication to prevent abruptio placentae.
- Educate families about emergency transport and hospital protocols in case of sudden hemorrhage.
- Explain that placental abruption can recur, especially in clients with prior history.
16.2 Risk Reduction Strategies
- Primary Risk Reduction
- Smoking cessation significantly reduces abruptio placentae incidence.
- Avoidance of illicit drugs, particularly cocaine and methamphetamines.
- Management of maternal hypertension via medication adherence and frequent blood pressure monitoring.
- Reduce mechanical trauma risk (seatbelt safety, avoiding high-impact sports).
- Secondary Prevention
- Early identification of placental location via ultrasound (placenta previa or low-lying placenta).
- Monitoring fetal growth and movement regularly.
- Close supervision of clients with prior abruptio placentae or multiple gestations.
- Tertiary Prevention
- Rapid recognition and intervention for placental separation.
- Immediate hospitalization for symptomatic clients.
- Early cesarean delivery in severe cases to prevent fetal and maternal compromise.
Nursing Insights
- Document baseline maternal vital signs and fetal heart rate in high-risk clients.
- Educate clients that even minor trauma or sudden abdominal impact can precipitate placental abruption.
- Reinforce hydration, rest, and blood pressure monitoring to optimize placental perfusion.
- Counsel on family planning and future pregnancy risk reduction, particularly after prior abruptio placentae.
16.3 Discharge Teaching
- Client Instructions
- Report any vaginal bleeding immediately, regardless of amount.
- Monitor and record fetal movements daily.
- Maintain scheduled prenatal appointments for high-risk monitoring.
- Adhere to antihypertensive therapy and other prescribed medications.
- Avoid heavy lifting, sexual intercourse, and strenuous activity until cleared by the primary health care provider.
- Home Safety Measures
- Ensure emergency transport plans are available.
- Educate family members on recognizing signs of maternal shock (pale skin, tachycardia, hypotension).
- Maintain hydration and balanced diet to optimize maternal-fetal health.
Nursing Insights
- Reinforce red-flag recognition: sudden pain, bleeding, or reduced fetal movement.
- Teach peripartum self-monitoring techniques, including kick counts and blood pressure tracking.
- Encourage psychological support, as abruptio placentae can cause anxiety and fear about future pregnancies.
16.4 Education for Future Pregnancies
- Preconception Counseling
- Evaluate for underlying hypertension, coagulopathies, or vascular conditions.
- Discuss risk factors for recurrence, especially in clients with prior abruptio placentae.
- Prenatal Surveillance
- Early ultrasound assessment of placental location in subsequent pregnancies.
- Frequent maternal and fetal monitoring for high-risk clients.
- Reinforce lifestyle modifications, including abstinence from tobacco and drugs.
- Interdisciplinary Approach
- Collaboration with obstetric specialists for delivery planning.
- Formulate emergency plans for rapid cesarean delivery if abruption occurs.
- Optimize nutritional and cardiovascular health prior to conception.
Nursing Insights
- Clients should be counseled that recurrence risk is increased (10–15% after previous abruption).
- Emphasize importance of early detection through regular prenatal visits.
- Educate regarding timely reporting of warning signs to prevent maternal-fetal compromise.
Summary
- Abruptio placentae is premature separation of a normally implanted placenta, leading to maternal and fetal complications.
- Risk factors: chronic hypertension, prior abruption, trauma, smoking, illicit drug use, multiparity, advanced maternal age.
- Clinical manifestations: sudden onset abdominal/back pain, uterine rigidity, dark red bleeding, fetal distress.
- Maternal complications: hemorrhagic shock, disseminated intravascular coagulation (DIC), renal failure.
- Fetal complications: hypoxemia, acidosis, preterm birth, intrauterine growth restriction (IUGR), fetal demise.
- Nursing priorities: rapid assessment, stabilization, fetal monitoring, preparation for possible cesarean delivery, client education.
- Prevention: risk factor modification, strict prenatal care, lifestyle changes, early detection, education on warning signs.
- Nurses must understand the pathophysiology of placental separation to anticipate maternal-fetal complications.
- Early recognition of maternal shock and fetal distress is critical.
- Education about lifestyle modification and recurrence prevention is as important as acute management.
- Effective communication with primary health care providers ensures timely interventions and improves outcomes.
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Abruptio Placentae
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
