
Hygiene
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Describe hygienic care that nurses provide to clients.
- Identify factors influencing personal hygiene.
- Identify normal and abnormal assessment findings while providing hygiene care.
- Apply the nursing process to common problems related to hygienic care.
- Demonstrate techniques for assisting patients with hygiene measures, including those used when administering various types of baths and those used in cleaning each part of the body.
- Describe agents commonly used on the skin and scalp, including any precautions necessary for their use.
- Plan, implement, and evaluate nursing care for common problems of the skin and mucous membranes.
Introduction
Personal hygiene is the self-care by which people attend to such functions as bathing, toileting, general body hygiene, and grooming.
Illness, hospitalization, and institutionalization generally require modifications in hygiene practices.
Nurses assisting patients with basic hygiene must respect individual patient preferences, providing only the care that patients cannot, or should not, provide for themselves.
Hygiene Practices
Hygienic practices include caring for the skin, hair, nails, mouth, teeth, and perineal area.
- Early morning care is provided to clients as they awaken in the morning. This care consists of providing a urinal or bedpan to the client confined to bed, washing the face and hands, and giving oral care.
- Morning care is often provided after clients have breakfast, although it may be provided before breakfast. It usually includes providing for elimination needs, a bath or shower, perineal care, back massages, and oral, nail, and hair care. Making the client’s bed is part of morning care.
- Hour of sleep or PM care is provided to clients before they retire for the night. It usually involves providing for elimination needs, washing face and hands, giving oral care, and giving a back.
- As-needed (prn) care is provided as required by the client
Functions of skin:
- Protects underlying tissues from injury
- Regulates the body temperature
- It secretes sebum- softens and lubricates the hair and skin, prevents the hair from becoming brittle, and decreases water loss. Bactericidal.
- Transmits sensations through nerve receptors.
- Produces and absorbs vitamin d
FACTORS AFFECTING PERSONAL HYGIENE
1. Culture
People from some cultures place a high value on personal cleanliness and feel unclean unless they shower or bathe at least once daily.
Culture may also influence whether bathing is a private or communal activity.
2. Socioeconomic class:
A person’s socioeconomic class and financial resources often define the hygiene options available to him or her eg. homeless people.
3. Spiritual practices
Spiritual practices, including religious beliefs, may dictate ceremonial washings and purifications, sometimes as a prelude to prayer or eating.
4. Developmental level
Family practices often dictate hygiene habits, such as morning or evening baths; the frequency of shampooing, tooth brushing, and clothing changes; feelings about nudity; and so on.
As adolescents become more concerned about their personal appearance, they may adopt new hygiene measures, such as taking showers more frequently and wearing deodorant.
5. Health state
Disease, surgery, or injury may reduce a person’s ability to perform hygiene measures or motivation to follow usual hygiene habits.
Weakness, dizziness, and fear of falling may prevent an individual from entering a tub or shower or from bending to wash the lower extremities.
6. Personal preferences:
People have different preferences with regard to hygiene practices such as taking a shower versus a tub bath, using bar soap versus liquid soap, and washing to wake oneself or to relax before sleep.
The Nursing Process For Skin Care And Personal Hygiene
5.1 ASSESSING
The comprehensive nursing assessment uses interview and physical assessment skills to elicit data about the patient’s hygiene status.
NURSING HISTORY
|
HYGIENE PRACTICES ASSESSMENTS |
|
|
Factors to assess |
Questions & approaches |
|
Daily and weekly bathing habits |
Tell me about your daily and weekly bathing habits. Are there special bathing or hygiene products you routinely use or can’t use? How can nurses best help you to meet your hygiene needs? |
|
Factors interfering with hygiene practices |
What recently or in the past has interfered with your hygiene practices? Does anything interfere with your ability to be as clean as you would like? |
|
Pain |
Do you have pain? Describe characteristics, onset, location, duration, associated symptoms, and intensity. Does the pain interfere with your ability to perform personal hygiene tasks? Does caring for yourself cause pain or discomfort? |
|
Exposure history |
Do you sunbathe? How much sun or tanning-booth exposure do you get? Do you use sunscreen? Does your job or daily activities/hobbies expose you to chemicals, such as bleach, petroleum, paint, insecticides, or cleaning products? |
|
History of skin or mucous membrane problems (nature, onset of problem and frequency, causes, severity, symptoms, interventions attempted, results) |
Describe any skin problems with rashes, lumps, itching, dryness, lesions, ecchymosis, or masses. What have you used to relieve these symptoms? |
|
Special hygiene practices • Mouth |
How do you clean your teeth and gums? How often do you have a dental examination? Do you have any dental appliances? Are there any tender areas or lesions in your mouth? |
|
• Eyes, ears, and nose |
Do you wear glasses or contact lenses to improve your vision? Do you wear a hearing aid? Have you experienced any discharge or bleeding from or swelling of your eyes, ears, or nose? |
|
• Hair |
Have you noticed any unusual dryness of the scalp or changes in hair texture and amount? |
|
• Feet and nails |
Is the appearance of the nails normal? How do you normally care for and clean your nails? Is the skin intact on the feet? Have you noticed any swelling of one or both feet? Do you wear any special shoes? |
|
• Perineum |
Have you noticed any unusual discharge, swelling, itching, or inflammation? Are you able to complete your own perineal care? Do you follow any special hygiene practices during menstruation? What type of feminine hygiene products (e.g., pads, tampons, douches) do you use? |
|
• Piercings |
Do you have any body piercings on your face, neck, arms, legs, torso, navel, or genitals? Have you experienced any problems related to the procedure? How do you care for your piercing(s)? |
Hygiene practices include bathing and care of the skin and specific body areas, including the oral cavity, eyes, ears, nose, hair, nails, feet, and perineal and vaginal areas.
1. Skin:
Any past or current problems:
- How long have you had this problem?
- Does it bother you?
- How does it bother you? Does it itch?
- Have you found anything that helps relieve these symptoms?
2. Oral cavity:
Obtain a nursing history related to the oral cavity, including structures such as the teeth, tongue, and salivary glands.
Identify any variables known to cause oral problems, such as:
- deficient self-care abilities
- poor nutrition
- excessive intake of refined sugars
- family history of periodontal disease
- ingestion of chemotherapeutic agents that produce oral lesions
Patients at increased risk for oral problems include:
- Those who are seriously ill, comatose, dehydrated, confused, depressed, or paralyzed
- Patients who are mouth breathers
- Those who can have no oral intake of nutrition or fluids
- Those with nasogastric tubes or oral airways in place
- Those who have had oral surgery are also at increased risk.
3. Eyes, ears and nose:
- Ask the patient to identify any special eye, ear, or nose care that he or she performs.
- Also, address any specific care measures related to the use and care of visual aids or prosthetics (glasses, contact lenses, artificial eye) and hearing aids.
- Inquire about any history of eye, ear, and nose problems, and related treatments.
4. Hair:
Identify the patient’s usual hair and scalp care practices, including styling preferences. Note any history of hair or scalp problems; possible causes of changes in the distribution, texture, or amount of hair; and related treatments.
Be alert for any factors that are known to cause hair or scalp problems or that require special care such as deficient self-care abilities, immobility, malnutrition, and treatments known to result in hair loss (e.g., certain chemotherapeutic agents).
5. Nails and feet:
- Gather information about the patient’s normal nail and foot care practices.
- Include the type of footwear worn and any history of nail or foot problems and their treatments.
- Foot problems, particularly common in people with diabetes mellitus and peripheral vascular disease, often require hospitalization.
- Identify any variables known to cause nail and foot problems, such as deficient self-care abilities, vascular disease, arthritis, diabetes mellitus, history of biting nails or trimming them improperly, frequent or prolonged exposure to chemicals or water, trauma, ill-fitting shoes, or obesity.
6. Perineal and vaginal areas:
Note any history of perineal or vaginal problems and related treatments.
Identify any variables known to cause perineal or vaginal problems or to create a need for special care, such as urinary or fecal incontinence, an indwelling Foley catheter, childbirth, douching, rectal or genital surgery, and diseases such as urinary tract infection, diabetes mellitus, and certain sexually transmitted infections (STIs) (e.g., herpes).
PHYSICAL ASSESSMENT
Assessment of body systems provides data about hygiene status and ability to maintain personal hygiene. Nurses can detect problems early and initiate appropriate interventions.
1. Musculoskeletal System
- Purpose: Determines ability to perform hygiene tasks independently.
- Common issues: Muscle weakness, decreased range of motion, impaired balance, fatigue, lack of coordination.
- Impact: May limit bathing, grooming, or oral care.
2. Skin Assessment
- Method: Inspect and palpate systematically (head-to-toe, good lighting, compare bilaterally).
- Assess: Cleanliness, color, texture, temperature, turgor, moisture, sensation, vascularity, lesions.
- Risk factors for skin problems: Immobility, poor self-care, malnutrition, dehydration, decreased sensation, sun exposure, vascular disorders, irritants (secretions, devices).
- Documentation: Use precise terms-location, size, distribution, appearance, consistency.
Common Skin Problems
- Dry Skin
- Symptoms: Scaling, flaking, itching, cracks.
- Care: Short lukewarm baths, mild soap, gentle drying, daily moisturizers, hydration, humidifier.
- Acne
- Symptoms: Plugged pores, pustules.
- Care: Gentle cleansing, oil-free products, avoid squeezing, keep hair clean/off face, sunscreen (avoid sun sensitivity).
- Skin Rashes
- Causes: Allergens, sun, systemic meds.
- Care: Mild cleansing, moisturizing (dry rash), drying agent (wet rash), tepid baths, antiseptic sprays, avoid irritant, see MD if worsening.

3. Oral Cavity
- Assess:
- Lips: Color, moisture, ulcers, edema.
- Mucosa/Gums: Color, lesions, bleeding, edema, exudate.
- Teeth: Caries, dentures, devices.
- Tongue: Color, symmetry, texture, lesions.
- Palates/Oropharynx: Intactness, lesions, tonsils, uvula movement.
- Other: Odors, mastication, swallowing ability.
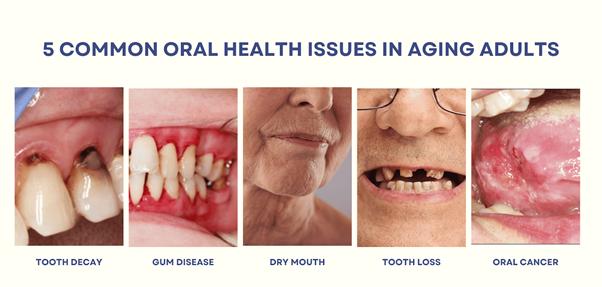
Common Oral Problems
- Dental Caries: From plaque buildup- cavities. Prevention: limit sweets, fluoride toothpaste, flossing, regular dental visits.
- Periodontal Disease: Gingivitis/periodontitis- bleeding gums, pockets, tooth loss, halitosis. Requires dental care.
- Stomatitis: Oral mucosa inflammation; causes: infection, trauma, deficiencies.
- Glossitis: Inflamed tongue; causes: Vit B12, folate, iron deficiency.
- Cheilosis: Lip fissures; cause: Vit B complex deficiency.
- Dry mucosa: From dehydration, mouth breathing, meds.
- Oral Malignancies: Persistent sores, patches, swelling-early detection critical.
4. Eyes, Ears, Nose
- Eyes: Position, alignment, appearance, lashes, conjunctivae, blink reflex, visual acuity.
- Ears: Position, wax buildup, discharge, hearing acuity. (Older adults-dry cerumen may impair hearing).
- Nose: Appearance, patency, tenderness, discharge, bleeding, edema.
5. Hair & Scalp
- Assess: Texture, cleanliness, oiliness, scaling, lesions, dandruff, infestations, hair loss.
- Common Problems:
- Dandruff: Flaking/itching - treat with medicated shampoo.
- Alopecia: Hair loss (localized/systemic causes). Can be due to infection, hormones, deficiencies, medications, aging. Treatments: Minoxidil, hairpieces, transplantation.
- Pediculosis (Lice): Head, body, pubic lice. Signs: Nits, itching, scratch marks. Treatment: Pediculicides, environmental cleaning, repeat treatment.
- Ticks: Disease carriers. Remove with tweezers (close to skin), cleanse area.
6. Nails & Feet
- Assess nails: Cleanliness, intactness, contour, cap refill, nail base (redness, swelling, discharge, tenderness).
- Skin of feet: Cleanliness, swelling, lesions, inflammation, orthopedic problems, condition between toes.
7. Perineal & Vaginal Areas
- Male: Lesions, swelling, tenderness, discharge.
- Female: Color, size, lesions, masses, discharge.
- Anal area: Cracks, nodules, veins, polyps.
- Note odors (may indicate infection/poor hygiene).
5.2 DIAGNOSING
A careful assessment of the adequacy of a patient’s hygiene practices and the assessment of the skin, mucous membranes, and other body areas may lead to the identification of numerous patient problems that can be classified as nursing diagnoses.
The etiology of the problem directs nursing interventions
Each nursing diagnosis statement identifies a patient problem and suggests expected patient outcomes.
The following are examples of appropriate nursing diagnoses:
- Bathing Self-Care Deficit related to postoperative weakness
- Pain related to alteration in skin integrity
- Ineffective Coping related to chronic skin disease
- Ineffective Health Maintenance: dental caries related to deficient oral hygiene practices
- Impaired Oral Mucous Membrane related to malnutrition and dehydration
- Impaired Social Interaction related to negative body image: acne
- Imbalanced Nutrition: Less Than Body Requirements related to stomatitis
Outcome Identification And Planning
The plan of nursing care identifies nursing measures to assist the patient to develop or maintain hygiene practices that contribute to a sense of well-being. Appropriate expected outcomes include the following: The patient will:
- Verbalize feeling comfortable and clean
- Participate fully in necessary hygiene measures according to cognitive, sensory, mobility, and endurance abilities
- Maintain intact skin and mucous membranes
- Demonstrate correct skin care measures (when indicated) such as oral care, care of eyes, ears, and nose, nail and foot care, and perineal and vaginal care
- Demonstrate signs of healing in existing lesions (oral, scalp, or perineal)
- Exhibit lips, oral mucosa, gums, and tongue that are intact, moist, and free of inflammation and lesions
- Verbalize importance of good teeth-brushing habits, fluoride use, and regular dental examinations
- Demonstrate healthy functioning of eyes, ears, and nose
- Exhibit eyes, ears, and nose that appear clean
- Demonstrate proper use and care of visual or auditory aids
- Exhibit clean hair
- Verbalize satisfaction with appearance
- Participate in hair and scalp care as able
- Exhibit intact, clean, and manicured nails
- Demonstrate intact, clean, and lesion-free foot skin
- Report reduced or absent nail and foot problems (specify: calluses, corns, plantar warts, ingrown nails, athlete’s foot)
Implementation
General Principles
- Respect patient preferences and cultural norms.
- Encourage self-care as much as possible to maintain independence.
- Maintain privacy and dignity.
- Promote physiologic and psychological wellness.
- Hygiene care is an opportunity for:
- Assessing skin and overall health
- Teaching self-care
- Strengthening nurse-patient rapport
Scheduled Hygiene Care
1. Early Morning Care
- Soon after waking.
- Focus: Toileting, face and hand washing, oral care, comfort measures.
- Prepares patient for breakfast or tests.
2. Morning Care (A.M.)
- After breakfast.
- Includes: Toileting, oral care, bathing, back massage, hair care (shaving if indicated), dressing, skin care (e.g., pressure ulcer prevention), cosmetics, positioning.
- Enhances morale and hygiene.
3. Afternoon Care (P.M.)
- After lunch, before visitors/rest.
- Focus: Comfort, handwashing, oral care, toileting, bed linen straightening, repositioning for mobility-impaired patients.
4. Hour of Sleep Care (H.S.)
- Before bedtime.
- Include: Toileting, face and hand washing, oral care, back massage, linen change, positioning, and accessibility of call light and personal items.
5. As-Needed Care (P.R.N.)
- Provided in addition to scheduled care.
- Examples: Oral care every 1-2 hours for high-risk patients, changing linens/clothing for diaphoretic patients.
- Sometimes care may be withheld for uninterrupted rest if clinically appropriate.
Bathing and Skin Care
Purposes of Bathing
- Cleansing and conditioning skin
- Relaxation and comfort
- Promoting circulation and joint mobility
- Stimulating respiration
- Improving self-image and sensory input
- Strengthening nurse-patient relationship
Types of Bathing
- Shower
- Preferred for ambulatory patients.
- Safety: Mats, non-slip strips, proper temperature (110-115°F / 43-46°C).
- Provide a chair or stool if needed.
- Assist with entering/exiting tub; maintain privacy.
- Reduce stimuli for confused patients.
- Tub Bath
- Used based on patient tolerance and facility policy.
- Assist with safe entry/exit and provide support.
- Bed Bath
- For patients confined to bed or with limited mobility.
- Provide basin of warm water, bath blanket, privacy, and accessible call light.
- Patients may assist with areas they can reach; nurse completes rest.
- Bag Bath / Disposable Bath
- Pre-moistened or reusable washcloths in a bag.
- No rinsing required; skin allowed to air-dry.
- Time-saving, effective for patients with mild to moderate skin impairments.
Promoting Skin Health
- Use soap substitutes or nonsoap emollient cleansers to prevent drying.
- Apply topical emollients (lotions, creams, gels, ointments) post-bath to hydrate and restore skin barrier.
- Use skin barrier products (creams, films, ointments) to protect vulnerable skin (e.g., around stomas, wounds, exposure to urine/feces).
- Application frequency: Ideally twice daily or as indicated by skin condition.
Massaging the Back
- Follow bath with backrub to:
- Relieve muscle tension, promote relaxation
- Improve circulation
- Reduce pain, anxiety, and distress
- Improve sleep quality
- Assess skin for breakdown
- Duration: 4-6 minutes; warm lotion recommended.
- Contraindications: Recent back surgery, fractures, or other specific medical conditions.
- Position: Prone or side-lying if prone not possible.
SKILL: Giving a Bed Bath
Purpose: To maintain patient hygiene, prevent infection, promote comfort, preserve skin integrity, and respect patient dignity and privacy.
Preparation
- Review Patient Chart: Assess limitations in mobility or activity to prevent discomfort or injury.
- Gather Supplies: Basin, warm water (110-115°F), soap/skin cleanser, towels, washcloths, bath blanket, clean gown, gloves, PPE if indicated. Bring all equipment to bedside to save time and avoid unnecessary strain.
- Hand Hygiene & PPE: Perform hand hygiene. Use gloves or other PPE based on transmission precautions.
- Patient Identification & Communication: Identify patient. Explain procedure. Assess ability to assist and personal hygiene preferences.
- Privacy & Environment: Close curtains and doors if possible. Adjust room temperature. Ensure comfort and prevent heat loss.
- Pre-Bath Preparations: Remove sequential compression devices and antiembolism stockings per protocol. Offer bedpan or urinal to reduce interruptions. Adjust bed to caregiver elbow height for proper ergonomics.
Positioning & Linen Management
- Position Patient: Assist patient to side of bed nearest to you. Patient lies on back.
- Linen Handling: Loosen top covers; place bath blanket over patient. Remove top sheet while maintaining privacy. Fold soiled linen carefully; place in laundry bag to prevent contamination.
- Gown Removal: Remove gown while keeping bath blanket in place. Handle IV lines carefully, maintaining flow rates.
- Safety Measures: Raise side rails for safety. Ensure gloves are worn if contact with body fluids is anticipated.
Bathing Procedure
Face, Neck, and Ears: Use a clean, damp washcloth; no soap unless indicated. Apply emollient for skin integrity.
Arms: Expose far arm first; place towel underneath. Wash hand, arm, axilla with firm strokes. Rinse and dry; apply emollient.
Chest and Abdomen: Cover chest with towel; lower bath blanket. Wash, rinse, dry chest and abdominal folds. Inspect umbilical area and skin creases.
Legs and Feet: Expose far leg; place towel underneath. Wash from ankle to groin, rinse, dry; apply emollient. Wash and dry feet thoroughly, including between toes. Repeat for near leg and foot.
Back and Buttocks: Assist patient to prone or side-lying position. Expose back/buttocks with bath blanket and towel for privacy. Wash, rinse, dry; focus on skin folds and bony prominences. Inspect for redness or skin breakdown.
Backrub: Optional, if not contraindicated. Improves circulation, relaxation, and tissue integrity. Apply emollient or skin barrier as needed.
Perineal Care: Refill basin with clean water; use fresh washcloth and towel. Assist patient or perform care if unable. Apply skin barrier if indicated to protect skin from moisture and irritants. Maintain privacy and warmth.


Finishing Up
- Gown & Grooming: Help patient into a clean gown. Assist with personal toiletries (deodorant, cosmetics). Protect pillow with towel and groom hair.
- Safety & Comfort: Ensure patient is comfortable. Raise side rails. Return bed to lowest position.
- Bed Linen: Change soiled linens per policy. Dispose of contaminated linens properly.
- Hand Hygiene & PPE: Remove gloves and PPE. Perform hand hygiene.
Key Principles of giving a bed bath:
|
Step |
Rationale |
|
Hand hygiene & PPE |
Prevents spread of microorganisms. |
|
Privacy & warmth |
Maintains dignity and prevents heat loss. |
|
Patient participation |
Encourages independence and individualized care. |
|
Proper bed height & positioning |
Prevents caregiver musculoskeletal strain. |
|
Emollients |
Maintain and restore skin integrity. |
|
Firm, long strokes |
Stimulate circulation, remove debris, relax patient. |
|
Skin fold inspection |
Prevent odor, skin breakdown, infections, and decubitus ulcers. |
|
Perineal care |
Reduces risk of infection and discomfort. |
|
Gloves change for perineal care |
Prevents contamination and transmission of pathogens. |
|
Backrub |
Enhances circulation, relaxation, and tissue health. |
Documentation
- Note patient’s tolerance, assistance needed, areas of skin breakdown, and any abnormal findings.
- Record skin care products applied, patient response, and completion of procedure.
Oral Hygiene
Importance
- Prevents deterioration of oral cavity.
- Reduces colonization of pathogens- lowers risk of aspiration pneumonia and systemic infection.
- Supports comfort and well-being.
Techniques
- Tooth Brushing
- Soft-bristled, small brush to reach all teeth; clean tongue.
- Brush after meals; clean brushes between uses.
- Electric/automatic brushes are effective.
- Flossing
- Removes debris and bacteria between teeth once daily.
- Mouthwash
- Reduces plaque, gingivitis, halitosis; fluoride rinses prevent cavities.
- Not effective for systemic halitosis (e.g., onion/garlic).
- Dentures
- Remove and clean daily; use cool/lukewarm water, soft brush.
- Store in cold water when not in use; avoid wrapping in tissue.
- Encourage patient to brush gums and tongue before reinsertion.
- Handle carefully to prevent damage.
Nursing insights: Special Considerations
- Patients with physical/cognitive limitations may require frequent assistance (every 1-2 hours).
- Moisturize lips and oral mucosa regularly if patient cannot drink.
- Older adults or patients with dexterity issues are at higher risk for inadequate oral hygiene.
SKILL: Assisting patient with oral care
Purpose: To maintain oral hygiene, prevent infection, promote comfort, and preserve healthy teeth and gums.
Preparation
- Hand Hygiene & PPE: Perform hand hygiene. Put on gloves if assisting; use additional PPE as indicated. Prevents spread of microorganisms.
- Patient Identification & Communication: Identify the patient. Explain the procedure to promote cooperation and reduce anxiety.
- Equipment & Environment
- Assemble equipment (toothbrush, toothpaste, dental floss, mouthwash, towel, emesis basin) on overbed table within reach.
- Close room door or curtains for privacy.
- Adjust bed to comfortable working height (elbow height of caregiver). Organization facilitates task performance; privacy maintains dignity; proper bed height reduces caregiver strain.
- Patient Positioning: Assist patient to sitting position if allowed, or side-lying if necessary- prevents aspiration of fluids. Place towel across patient’s chest; towel protects patient’s clothing.
Oral Care Procedure
Brushing Teeth
- Moisten toothbrush and apply toothpaste.
- Hold brush at 45-degree angle to gum line.
- Brush from gum line to crown:
- Outer and inner surfaces.
- Biting surfaces.
- Back-and-forth motion.
- Brush tongue gently.
- Have patient rinse vigorously with water; use suction if patient cannot expectorate.
Proper brushing removes plaque, tartar, and debris. Tongue brushing removes coating and bacteria. Suction prevents aspiration if patient cannot spit.
Flossing (if indicated)
- Remove ~6 inches of floss or use floss holder.
- Wrap floss around index fingers, keeping 1-1.5 inches taut.
- Insert gently between teeth, moving down to gums; then up and down along both sides of each tooth.
- Repeat between all teeth.
- Have patient rinse thoroughly.
Flossing removes plaque and promotes healthy gums. Taut floss ensures proper cleaning. Gentle technique prevents gum trauma.
Optional Care
- Offer mouthwash for freshening- Mouthwash improves oral freshness.
- Apply lip balm or petroleum jelly to prevent dryness.

Finishing Up
- Remove equipment; discard gloves.
- Raise side rail and lower bed.
- Assist patient to comfortable position.
- Remove any PPE used.
- Perform hand hygiene.
Note:
- Proper removal of gloves and PPE prevents infection transmission.
- Hand hygiene protects both patient and caregiver.
- Positioning ensures comfort and safety.
Key Principles of oral care
|
Step |
Key Point |
Rationale |
|
Hand hygiene & PPE |
Before procedure |
Prevents spread of microorganisms |
|
Patient ID & explanation |
Communication before care |
Promotes cooperation, reduces anxiety |
|
Proper positioning |
Sitting or side-lying |
Prevents aspiration; enhances comfort |
|
Brushing technique |
45° angle, thorough coverage |
Removes plaque, tartar, and debris; protects gums |
|
Tongue brushing |
Gentle |
Reduces coating, bacteria, and odor |
|
Flossing |
Taut floss, gentle |
Cleans interdental surfaces; prevents gum trauma |
|
Mouthwash/lip care |
Optional |
Promotes freshness and comfort |
|
Disposal & hygiene |
Remove gloves/PPE, hand hygiene |
Prevents infection transmission |
|
Comfort & safety |
Bed rails, patient positioning |
Ensures safety and dignity |
Eye Care
Normal Eye Care:
- Eyes are naturally cleaned by lacrimal secretions.
- During illness, eyes may produce excess secretions; appear glasslike.
Techniques for Cleaning Eyes:
- Wear gloves.
- Use water or normal saline; never use soap.
- Position patient on the same side as the eye being cleaned.
- Wipe from inner canthus to the outer canthus.
- Use a clean section of cloth or a new cotton ball for each wipe.
- For stubborn secretions: apply a warm, wet compress for 3-5 minutes.
- Always clean the other eye afterward.
Unconscious Patients:
- Blink reflex may be diminished/absent; eyelids may remain open.
- Provide eye care every 4 hours to prevent corneal ulceration.
- Use saline or artificial tears and a protective eye shield.
Eyeglass Care
- Place glasses lenses up when not in use.
- Clean over a terry towel with warm water and soap or special cleaner.
- Rinse thoroughly and dry with soft cotton cloth.
- Avoid hot water, paper tissues, or silicone tissues to prevent scratching.
Contact Lens Care
- Types: Hard (rigid gas-permeable) and soft (daily, extended, or disposable).
- Perform strict hand hygiene; wear gloves before handling.
- Avoid exposure to cosmetics, soaps, smoke, or noxious vapors.
- Hard lenses: wear 12-16 hours max; remove before sleeping.
- Extended-wear soft lenses: 1-30 days, cleaned at least weekly.
- Disposable lenses: vary from daily to 14 days depending on type.
- Remove immediately if excessive tearing, redness, or pain occurs.
- Nurses are responsible for removing lenses in unconscious patients.
- Use gentle pressure or suction device for hard lenses; do not remove if eye injury present.
Artificial Eye Care
- Encourage patient self-care if possible.
- Equipment: basin, soap, water, saline.
- Flush socket with saline before replacing the prosthesis.
- Keep patient lying down to prevent dropping the prosthesis.
Ear Care and Nose care
Ear care
- Clean outer ears only; dry carefully with a soft towel.
- Avoid cotton swabs, pins, paper clips, or fingernails.
- Hearing aid care:
- Check batteries regularly.
- Clean earpieces daily with mild soap and water.
- Whistling sound- battery functioning.
- For mild hearing loss without hearing aid:
- Avoid noisy areas, ensure good lighting, face speaker, ask for repetition, consider amplitude devices.
Nose Care
- Clean by gently blowing both nostrils open.
- Apply warm, moist compress to soften crusts.
- Use disposable tissues.
- Avoid irrigations and inserting cotton swabs deeply.
Hair Care
- Daily brushing: distributes oils, prevents matting, stimulates circulation.
- Long hair: consider braiding; avoid tight braids.
- Special considerations for curly or chemically straightened hair.
- Shampooing:
- Can be done in shower by patient or bedside if on bedrest.
- Bedside hair care: use warm water, shampoo, conditioner; protect with towel or hair tray.
- Rinseless shampoos or shampoo caps available.
- Cultural sensitivity: style hair according to patient preference.
Shaving
- Requires patient consent.
- Electric razors recommended for patients on anticoagulants or bleeding disorders.
- Shave after warm bath/shower to soften hair.
Procedure:
- Perform hand hygiene and put on disposable gloves (contact with blood is possible if any skin nicks occur).
- Cover patient’s chest with a towel or waterproof pad. Fill bath basin with warm (43° to 46°C [110° to 115 °F]) water. Press a warm washcloth on the patient’s facial skin to soften the hair.
- Dispense shaving cream into palm of hand. Rub hands together, then apply to area to be shaved in a layer approximately 0.5” thick.
- With one hand, pull the skin taut at the area to be shaved. Using a smooth stroke, begin shaving. If shaving the face, shave with the direction of hair growth in downward, short strokes. If shaving a leg, shave against the hair in upward, short strokes.
- Wash off residual shaving cream.
- If patient requests, apply aftershave or lotion to area shaved.
- Remove and discard gloves and perform hand hygiene.
Fingernail Care
- File nails in oval shape; avoid cutting too deep.
- Remove hangnails carefully.
- Push back cuticles gently after soaking.
- Apply emollient to prevent hangnails.
- Avoid contact with harsh soaps and acetone-based polish removers.
Foot Care
- Especially important for elderly, diabetics, or patients with circulatory problems.
- Techniques:
- Wash with mild soap and tepid water; clean interdigital spaces.
- Dry thoroughly; apply moisturizer to dry areas.
- Diabetics: sprinkle talcum/cornstarch between toes; file nails, avoid cutting.
- Avoid cutting corns/calluses; consult podiatrist if present.
- Wear appropriate footwear and socks; avoid going barefoot.
- Elevate feet if swollen; avoid heating pads.
- Report any foot problems promptly.
Perineal and Genital Care:
1. Perineal Care
- Perform in a matter-of-fact, dignified manner to reduce embarrassment.
- Supplies: mild unscented soap, water, washcloths, disposable gloves.
- Steps:
- Provide privacy, explain procedure, perform hand hygiene, wear gloves.
- Wash and rinse groin area:
- Female: spread labia, wash from pubic area to the anal area.
- Male: wash tip of penis first (circular motion), then shaft downward.
- Uncircumcised males: retract foreskin while washing, return it afterward.
- Wash and rinse scrotum gently.
- Dry thoroughly, apply emollient as indicated; avoid powder.
- Turn patient to side, cleanse anal area from least to the most contaminated.
- Remove gloves, perform hand hygiene.
Nursing insights: Special Considerations
-
- Patients with indwelling catheters: catheter care usually follows perineal care.
- Incontinent patients:
- Risk for skin damage due to moisture, pH changes, bacterial overgrowth, friction.
- Use perineal skin cleansers, moisturizers, barriers.
- Clean immediately after soiling; avoid harsh soap and forceful scrubbing.
2. Vaginal Care
- Vaginal secretions are normally odor-free; mild soap and water sufficient.
- Routine douching is unnecessary and discouraged (removes normal flora, may cause irritation or infection).
- Deodorants:
- Not necessary; no proven therapeutic benefit.
- External use only; avoid broken skin and sanitary products.
- Educate patients on safe use if insisted upon.
3. Care for Body Piercings
- Piercings may be present on face, ears, neck, torso, genitals.
- Care includes assessment and wound aftercare.
- Techniques aim to prevent infection and promote healing.
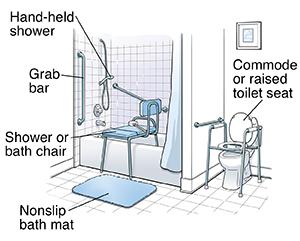
Environmental Care
- Clean, clutter-free, safe, and pleasant environment improves well-being.
- Essentials: bed, overbed table, bedside stand, chairs, call light, oxygen, suction, bath/emesis basins, linens.
- Always ask permission before handling patient’s personal items.
- Maintain ventilation and odor control (empty waste, use deodorizers as needed).
- Room temperature: 20-23°C (68-74°F); respect patient preference.
- Minimize noise and harsh lighting; protect patient privacy.
Bed Safety and Comfort
- Bed responsibilities: safe, comfortable, and functional.
- Motorized beds: adjust height, head, and foot positions; teach patient/family safe use.
- Side rails: use as indicated and per policy.
- Locks: wheels/casters locked when stationary.
- Before leaving bedside:
- Bed lowest position.
- Safe bed position.
- Functioning bed controls and call light.
- Side rails raised if indicated.
- Mattress firm, clean, water-repellent; therapeutic mattresses as needed.
- Bed linens: clean, free of crumbs/wrinkles, patient comfortably warm.
- Change after bath or when soiled; coordinate with assistive personnel.
Making a Bed
- Occupied bed: use appropriate technique to maintain comfort.
- Minor variations are acceptable depending on patient condition or equipment.
- Protect pressure areas from rough edges or wrinkles.
Skin Care and Hygiene Education
1. Soaps and Detergents
- Soaps: vegetable/animal fats; detergents: petroleum derivatives.
- Non-soap cleansers may benefit dry or sensitive skin.
- Expensive products are not more effective than standard options.
2. Deodorants and Antiperspirants
- Perspiration odor caused by bacterial action on sweat.
- Keep body and clothing clean.
- Use deodorants/antiperspirants after cleansing.
- Use with care to prevent irritation; contraindicated in some situations (e.g., pre-mammography, post-mastectomy).
3. Cosmetics
- Enhance appearance; may improve self-esteem.
- Cultural/religious considerations may limit use.
- Avoid contaminated cosmetics; do not share.
- Discard after 2-4 months, especially near eyes.
- Keep applicators clean.
Summary
- Various health beliefs, personal, sociocultural, economic, and developmental factors influence patients’ hygiene preferences and practices.
- Sound clinical judgment requires you to consider a patient’s condition, anticipate any risks or problems, gather thorough assessment data, and then analyze data to form nursing diagnoses.
- Hygiene needs, preferences, and the ability to participate in care change as people age.
- Assess a patient’s skin, feet and nails, oral mucosa, hair, and eyes and ears to obtain a complete assessment of the patient’s hygiene needs.
- Assess a patient’s physical and cognitive ability to perform basic hygiene measures.
- Vascular insufficiency and reduced mobility, cognition, and sensation increase a patient’s risk for impaired skin integrity.
- Diabetes mellitus and peripheral vascular diseases increase the patient’s risk for foot and nail problems.
- Clinical judgment and critical thinking about a patient’s hygiene preferences, needs, and ability to participate in care results in patient-centered hygiene care matching the patient’s needs and preferences.
