
Comfort and sleep
Study Questions
Practice Exercise 1
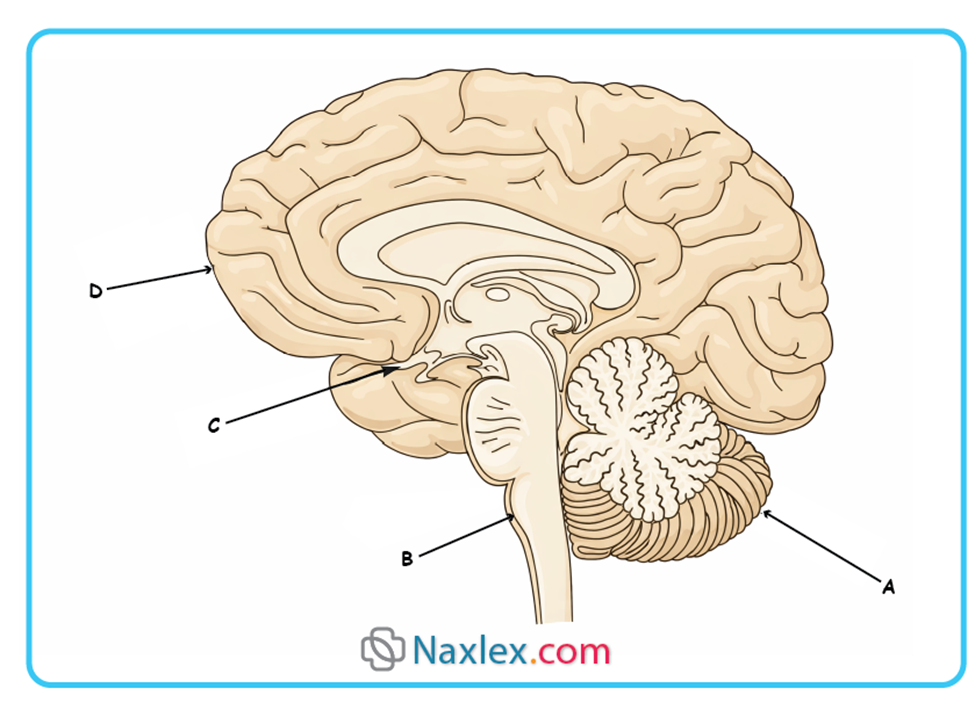
A client is admitted for a sleep disorder. The nurse knows that the reticular activating system (RAS) is involved in the sleep/ wake cycle. In the accompanying illustration, which letter indicates the location of the RAS?
Explanation
The reticular activating system is a complex network of neurons located within the brainstem that essentializes the transition between sleep and wakefulness. It functions as a filter for sensory input, selectively allowing stimuli to reach the cerebral cortex to maintain a state of cortical alertness. Dysregulation of this system can lead to profound circadian disturbances or prolonged states of unconsciousness such as a coma. The system's primary neurotransmitters, including norepinephrine and acetylcholine, are critical for the maintenance of high-frequency electroencephalogram activity associated with alertness.
Rationale for correct answer
2. The letter B points to the brainstem, specifically the region housing the midbrain, pons, and medulla where the reticular formation resides. This area acts as the physiological “on/off switch” for consciousness by relaying activating signals upward to the diencephalon and cortex. It is the primary site for the reticular activating system involved in the sleep-wake cycle.
Rationale for incorrect answers
1. The letter A indicates the cerebellum, which is primarily responsible for the coordination of voluntary motor movement, balance, and posture. While it has some connections to the brainstem, it does not serve as the central regulator for the sleep-wake cycle or cortical arousal. Damage here typically results in ataxia rather than primary sleep disorders.
3. Letter C identifies the hypothalamus, specifically near the optic chiasm and pituitary region, which contains the suprachiasmatic nucleus. While the hypothalamus regulates the circadian rhythm via light-dark signals, the actual Reticular Activating System (RAS) is structurally located lower in the brainstem core. The hypothalamus acts more as a master clock than the primary arousal system.
4. Letter D points to the frontal lobe of the cerebral cortex, the area responsible for executive function, decision making, and voluntary motor control. The cortex is the recipient of arousal signals from the RAS but does not contain the RAS itself. Disorders of the frontal lobe affect personality and cognition rather than the fundamental biological mechanism of wakefulness.
Test-taking strategy
- Anatomical Localization: Identify the core structure associated with the RAS, which is the brainstem. In the provided diagram, only B points directly to the brainstem column.
- Functional Mapping: Differentiate between the “Master Clock” (Hypothalamus - C) and the “Arousal System” (Brainstem - B). The RAS is always associated with the reticular formation of the brainstem.
- Elimination of Major Structures: Rule out the cerebellum (A) and the cerebrum (D) as they are the endpoints or accessory structures rather than the origin of the reticular activating system.
- Visual Cues: Look for the central “trunk” of the brain. The brainstem (B) is the vertical pathway through which all ascending arousal signals must pass to reach the higher centers.
- Neuroanatomy Basics: Remember that the “reticular” (net-like) formation is a characteristic histological feature of the brainstem's central core.
Take home points
- The Reticular Activating System (RAS) is located in the brainstem and is responsible for regulating wakefulness and sleep-to-wake transitions.
- The suprachiasmatic nucleus of the hypothalamus works in tandem with the RAS by utilizing melatonin to signal the timing of sleep.
A client tells the nurse that her 4-year-old daughter typically goes to bed at 10:30 pm and awakens each morning at 7 am. She does not take a nap in the afternoon. Which is the best response by the nurse?
Explanation
Preschoolers aged 3 to 5 years typically require 10 to 13 hours of sleep per 24-hour period to support neurodevelopmental growth and emotional regulation. While many children in this age group begin to relinquish their afternoon naps, their total nocturnal sleep duration must increase to compensate for the loss of daytime rest. Inadequate sleep in pediatrics often manifests as hyperactivity, irritability, and diminished cognitive performance during waking hours.
Rationale for correct answer
1. The child is currently only receiving 8.5 hours of sleep, which is significantly below the recommended duration for a 4-year-old. Moving the bedtime to 8 or 9 pm aligns the child's schedule with physiological needs, ensuring they achieve at least 10 to 11 hours of rest. This intervention addresses the sleep deficit while respecting the child's natural transition away from napping.
Rationale for incorrect answers
2. While quiet rest is beneficial, insisting on a nap for a child who has outgrown the need can create caregiver-child conflict and may not solve the underlying sleep debt. The primary issue is the insufficient nocturnal duration, not the lack of a daytime nap. Increasing nighttime sleep is a more effective strategy for this developmental stage.
3. Recommending the child sleep later in the morning is often impractical due to family schedules or future school requirements. Consistency in wake times is a pillar of sleep hygiene and helps regulate the circadian rhythm. Adjusting the bedtime is generally more sustainable and developmentally appropriate than altering the morning routine.
4. Reassuring the parent that 8.5 hours is normal is factually incorrect and constitutes clinical misinformation. While the child might have outgrown the nap, the current total sleep volume is inadequate for a preschooler's metabolic and neurological demands. The nurse must intervene to prevent the long-term effects of chronic pediatric sleep deprivation.
Test-taking strategy
- Knowledge of growth and development: Success in pediatric nursing questions requires knowing exact physiological ranges; 10 to 13 hours is the target for preschoolers.
- Mathematical assessment: Calculate the total hours of sleep provided in the stem (10:30 pm to 7:00 am = 8.5 hours) and compare it to the standard.
- Developmental transitions: Recognize that napping often ceases at age 4, but the total sleep requirement remains high, shifting the focus to earlier bedtimes.
- Clinical accuracy: Rule out options that validate insufficient care (Choice 4) or suggest impractical schedule changes (Choice 3).
- Prioritize sleep volume: The most effective way to close a sleep gap when napping has ceased is to move the bedtime earlier in the evening.
Take home points
- Chronic sleep deprivation in preschoolers is linked to behavioral issues that can be mistaken for attention-deficit/hyperactivity disorder (ADHD).
- A consistent bedtime routine (e.g., bath, reading) helps lower cortisol levels and prepares the child's brain for the transition to sleep.
- By age 5, only about 15% to 30% of children still require a daily afternoon nap, provided they get enough sleep at night.
A nurse assessing a client’s body temperature in the late afternoon notes it to be 37.2°C (99°F). The nurse assesses this as most likely due to what?
Explanation
Human body temperature is governed by the suprachiasmatic nucleus in the hypothalamus, which regulates a distinct diurnal variation over a 24-hour period. Temperature typically reaches its lowest point, or nadir, between 2 and 4 am, and climbs to its peak, or acme, in the late afternoon between 4 and 6 pm. This rhythmic fluctuation reflects changes in metabolic rate and peripheral vasomotor activity associated with the sleep-wake cycle. A reading of 37.2°C during this peak period often represents a physiological norm rather than a febrile state.
Rationale for correct answer
2. A temperature of 37.2°C in the late afternoon is a classic manifestation of the circadian rhythm where body temperature naturally peaks. The nurse must recognize that normal fluctuations can vary by as much as 0.5°C to 1.0°C throughout the day. This finding does not require clinical intervention as it aligns with the expected biological clock patterns.
Rationale for incorrect answers
1. While 37.2°C is slightly above the morning average, it lacks the specificity to be classified as a sign of infection without concurrent symptoms. Infection-related fevers typically present with higher elevations or lack the diurnal pattern seen in healthy individuals. Attributing this specific afternoon reading to pathology would be a clinical misinterpretation.
3. Hyperpyrexia is defined as an extreme elevation in body temperature, typically exceeding 41.0°C (105.8°F), which constitutes a medical emergency. 37.2°C is well within the sub-febrile range and is nowhere near the threshold for life-threatening heat illness. Using this term for a near-normal reading is a misuse of medical jargon.
4. Although a warm environment can influence surface temperature, the body’s homeostatic mechanisms usually maintain a stable core temperature in healthy adults. Circadian rhythm is a more predictable and likely cause for a routine afternoon elevation than environmental heat stress. This choice is less scientifically precise than the biological rhythm explanation.
Test-taking strategy
- Time of Day Recognition: In temperature questions, always note the specific time; “late afternoon” is the primary cue for the circadian peak.
- Identify Physiological Ranges: Differentiate between “normal variation” and “fever”; 37.2°C (99°F) is frequently the upper limit of the normal afternoon range.
- Terminology Hierarchy: Eliminate “Hyperpyrexia” immediately as it refers to extreme, dangerous temperatures (≥41°C).
- Pattern Analysis: Choose the answer that explains the “why” based on internal biological processes (circadian rhythm) over external factors (warm environment) when the value is marginally elevated.
- Clinical Prioritization: Focus on the most common and likely physiological cause before assuming a pathological process like infection.
Take home points
- Fever (pyrexia) is generally not clinically significant in an adult until it exceeds 38.0°C (100.4°F).
- Circadian rhythms affect not only temperature but also the secretion of cortisol, growth hormone, and catecholamines.
The nurse observes some involuntary muscle jerking in a sleeping client. The nurse determines that the client is most likely in which stage of sleep?
Explanation
Stage 1 NREM sleep represents the transitional phase between full wakefulness and light sleep, characterized by a decrease in physiological activity. During this stage, individuals often experience hypnagogic hallucinations or sudden, involuntary muscle contractions known as myoclonic jerks. These contractions result from the motor system's final discharges as the reticular activating system reduces its cortical stimulation. The individual remains easily arousable and may report they were not actually asleep if disturbed during this 5 to 10 minute period.
Rationale for correct answer
1. Involuntary muscle jerking, or hypnic jerks, are most prevalent during the transition into Stage 1 NREM. As the body relaxes, the brain may misinterpret the sensation of falling, triggering a startle response and muscle contraction. This stage is the lightest level of sleep, where the EEG shifts from alpha to theta waves.
Rationale for incorrect answers
2. Stage 2 NREM is characterized by the appearance of sleep spindles and K-complexes on the EEG, indicating a deeper state of rest. While some minor twitching may occur, the classic, forceful involuntary jerks associated with sleep onset have typically subsided by this point. The body is becoming more physiologically stable and less reactive to internal motor discharges.
3. Stage 4 NREM, also known as delta sleep, is the deepest stage of quiet sleep where muscle activity is significantly reduced. During this phase, the body focuses on tissue repair and growth hormone secretion rather than motor activity. Arousing a patient from this stage is difficult and usually does not involve acute jerking movements.
4. REM sleep is defined by muscle atonia, a state of near-total paralysis of the skeletal muscles to prevent dream enactment. Involuntary jerking is clinically inconsistent with the neural blockade of the spinal cord that occurs during this stage. Except for the extraocular muscles and the diaphragm, the body is functionally immobile during REM.
Test-taking strategy
- Identify the phenomenon: Recognize involuntary muscle jerking as the clinical description for a hypnic or myoclonic jerk.
- Stage association: Associate sleep-onset phenomena (hallucinations, jerks) exclusively with the lightest transition phase, which is Stage 1.
- Physiological trends: Remember that as NREM stages progress from 1 to 4, muscle activity and brain wave frequency consistently decrease.
- Rule out REM: Eliminate REM whenever muscle jerking is mentioned, as REM is defined by the absence of muscle tone (atonia).
- Keywords: Focus on the word “transitional”; Stage 1 is the only stage where the body is still close enough to wakefulness to exhibit these motor-sensory glitches.
Take home points
- Hypnic jerks are considered a normal physiological occurrence and are often exacerbated by caffeine, stress, or extreme fatigue.
- During Stage 1, the heart rate begins to slow and the muscles begin to relax, though the sleeper remains sensitive to environmental noise.
- If a patient frequently experiences violent movements during sleep, it may indicate a pathology like REM Sleep Behavior Disorder rather than normal Stage 1 jerks.
The nurse observes a slight increase in a client’s vital signs while they are sleeping during the night. According to the client’s stage of sleep, the nurse expects which of the following to be true?
Explanation
REM sleep is a period of intense brain activity that contrasts sharply with the physiological quiescence of NREM sleep. This stage is characterized by autonomic instability, leading to fluctuations in heart rate, blood pressure, and respiratory rate. Despite this internal arousal, the arousal threshold is at its highest, meaning the sleeper is most insulated from the external environment. This paradox of a highly active brain in a paralyzed, difficult-to-wake body is why it is often termed paradoxical sleep.
Rationale for correct answer
3. In REM sleep, the brain is highly active, but the body’s responsiveness to the external environment is at its lowest point. The high arousal threshold means it would be most difficult to awaken the client compared to NREM stages. The increase in vital signs noted by the nurse is a classic autonomic hallmark of this specific sleep phase.
Rationale for incorrect answers
1. During the stage where vital signs increase (REM), the patient is least aware of their surroundings due to intense internal cognitive activity. Awareness is highest in Stage 1 NREM, where vital signs are typically decreasing or stable. This choice describes the opposite of the physiological state indicated by fluctuating vitals.
2. Delta sleep refers to Stage 3 and 4 NREM, which are characterized by the lowest heart and respiratory rates of the night. Vital signs in delta sleep are stable and slow, not increased or fluctuating. This stage represents physiological rest, which is the metabolic antithesis of the active REM stage.
4. Most NREM stages (especially 2, 3, and 4) are periods of physiologic calm where heart rate and blood pressure remain consistently low. An increase in vital signs is atypical for NREM and strongly suggests the transition into REM. Therefore, expecting this to be an NREM stage contradicts the clinical data provided in the question.
Test-taking strategy
- Vital Sign Trends: Associate increased or fluctuating vital signs with REM sleep and decreased/stable vital signs with NREM sleep.
- Defining paradox: Remember the Paradoxical Sleep rule: High internal activity (vitals/brain) equals high difficulty in waking the patient.
- Arousal threshold: Rank the stages of sleep by difficulty to wake: REM and Stage 4 are the hardest, but REM is uniquely paired with high vital signs.
- Autonomic clues: Use the autonomic nervous system's behavior as a diagnostic tool; sympathetic surges are a signature of REM.
- Elimination: If vitals are increasing, rule out NREM stages 2, 3, and 4, which are designated as the body's “rest and digest” or “cooling” periods.
Take home points
- REM sleep periods lengthen as the night progresses, with the longest durations occurring in the early morning hours.
- The “active brain” in REM consumes as much oxygen as the brain of an individual who is fully awake and performing a task.
- Most vivid and narrative dreaming occurs during REM sleep, facilitated by the high level of cortical electrical activity.
Practice Exercise 2
A 52-year-old male client mentions that his wife frequently complains about his snoring. During the physical exam, the nurse notes that his neck size is 18 inches, his soft palate and uvula are reddened and swollen, and he is overweight. What is the most appropriate nursing intervention for the nurse to recommend to this client?
Explanation
Obstructive sleep apnea is strongly associated with an increased neck circumference (≥17 inches in males) and a high body mass index. The reddened, swollen soft palate and uvula are clinical markers of vibratory trauma caused by chronic, heavy snoring. These physical findings, combined with obesity, significantly elevate the risk for nocturnal hypoxemia and secondary cardiovascular complications. Immediate diagnostic intervention is required to prevent long-term sequelae like systemic hypertension and stroke.
Rationale for correct answer
4. The presence of a large neck, obesity, and pharyngeal inflammation are classic indicators of obstructive sleep apnea. A referral for a polysomnography (sleep study) is the definitive nursing action to confirm the diagnosis and initiate treatment. This intervention addresses the potentially life-threatening nature of the airway obstruction rather than just the symptom of snoring.
Rationale for incorrect answers
1. Suggesting separate bedrooms is a palliative measure that addresses the wife's comfort but ignores the client's underlying medical risk. This approach delays the diagnosis of a serious respiratory disorder and does nothing to mitigate the patient's nocturnal hypoxia. It fails to meet the standard of care for a symptomatic patient.
2. While weight loss is a critical long-term management strategy for sleep apnea, it is not the immediate priority for a client with significant clinical markers. The nurse must first ensure a specialist evaluation to assess the severity of airway collapse and the need for CPAP therapy. Weight loss programs should be an adjunct to, not a replacement for, diagnostic testing.
3. Avoiding alcohol and sedatives is appropriate advice because these substances decrease pharyngeal muscle tone, worsening the obstruction. However, this advice alone is insufficient for a client already showing physical signs of severe apnea. It is a supportive measure that does not provide the necessary diagnostic confirmation or treatment.
Test-taking strategy
- Recognize red flags: A neck size >17 inches and an overweight status in a snoring patient are classic NCLEX indicators for sleep apnea.
- Prioritize diagnosis: When a client exhibits multiple symptoms of a serious condition, the most appropriate intervention is referral for definitive diagnostic testing.
- Address the root cause: Distinguish between interventions that treat the “nuisance” (snoring) and those that treat the pathology (airway obstruction).
- Safety first: Sleep apnea is a high-risk condition; always choose the path that leads to clinical evaluation and airway protection.
- Rule of thumb: For suspected sleep apnea, the gold standard is always a sleep study/specialist referral.
Take home points
- A neck circumference greater than 17 inches in men is one of the most predictive physical findings for obstructive sleep apnea.
- Redness of the uvula and soft palate is often caused by the mechanical stress of tissue vibration during snoring episodes.
A client falls asleep in the middle of a conversation. The nurse would suspect which disorder?
Explanation
Narcolepsy is a chronic neurological disorder caused by the brain's inability to regulate sleep-wake cycles normally. It often involves a deficiency in hypocretin, a neuropeptide in the hypothalamus that promotes wakefulness and stabilizes the transition between states. Individuals experience sleep attacks where they transition abruptly from wakefulness into REM sleep without the typical NREM progression. This condition is frequently associated with cataplexy, which is a sudden loss of muscle tone triggered by strong emotions.
Rationale for correct answer
2. The defining clinical characteristic of narcolepsy is the sudden, irresistible urge to sleep, even during active tasks like talking or eating. Falling asleep mid-conversation indicates a profound failure of the arousal system to maintain cortical alertness. This abrupt transition is a diagnostic hallmark that distinguishes narcolepsy from general fatigue or other sedative effects.
Rationale for incorrect answers
1. Hypersomnia involves excessive sleepiness where the individual may sleep for prolonged periods at night or nap frequently during the day. However, it does not typically manifest as the sudden sleep attacks seen in narcolepsy. Patients with hypersomnia usually have a more gradual onset of drowsiness rather than falling asleep instantly during social interaction.
3. Somnambulism, or sleepwalking, is a parasomnia that occurs during deep NREM sleep (Stages 3 and 4). It involves complex motor behaviors performed while the individual remains in a state of sleep. It is a disorder of arousal from sleep, not a disorder of sudden sleep onset during wakefulness as described in the scenario.
4. Sleep apnea is characterized by respiratory pauses during sleep due to upper airway obstruction or central nervous system signaling failures. While it causes significant daytime somnolence due to sleep fragmentation, it rarely results in falling asleep mid-sentence. The sleepiness in apnea is typically perceived as a heavy lethargy rather than an uncontrollable, instantaneous attack.
Test-taking strategy
- Identify key descriptors: Look for the phrase “in the middle of,” which implies an instantaneous and inappropriate transition from awake to asleep.
- Match pathology to symptom: Link “sudden sleep attacks” exclusively to narcolepsy in the hierarchy of sleep disorders.
- Rule of severity: Recognize that mid-conversation sleep is the most severe form of inappropriate sleep onset, pointing toward a primary neurological drive failure.
- Differentiate somnolence: Distinguish between feeling sleepy (apnea/hypersomnia) and suddenly sleeping (narcolepsy).
- Eliminate parasomnias: Rule out somnambulism (Choice 3) as it describes behavior during sleep, not the act of falling asleep.
Take home points
- Narcolepsy is a lifelong condition that typically manifests in adolescence or early adulthood.
- Safety is the priority nursing concern, as sleep attacks can occur while driving or operating heavy machinery.
A nurse is taking a sleep history from a client. The nurse recognizes that which statement made by the client needs further follow-up?
Explanation
Sleep latency is the period of time required to transition from full wakefulness to the initiation of Stage 1 NREM sleep. In a healthy adult with efficient sleep hygiene, this interval typically ranges from 10 to 30 minutes. A consistent delay in sleep onset exceeding 30 minutes indicates sleep-onset insomnia, which may be driven by hyperarousal, anxiety, or circadian rhythm misalignment. Assessing the etiology of prolonged latency is crucial for preventing the development of chronic sleep debt and associated cognitive impairment.
Rationale for correct answer
3. A sleep latency of 45 to 60 minutes is clinically significant and indicates difficulty initiating sleep, necessitating further assessment by the nurse. Prolonged latency can be a symptom of restless legs syndrome, psychological stress, or environmental disruptors. The nurse must investigate the client's evening habits and mental state to identify why the transition to unconsciousness is delayed.
Rationale for incorrect answers
1. Feeling refreshed upon awakening is a subjective indicator of restorative sleep and high sleep efficiency. This statement suggests that the client is successfully cycling through the deeper stages of NREM and REM sleep. It represents a normal, healthy finding that does not require clinical follow-up or intervention.
2. Utilizing soft music is a common relaxation technique that can help lower the heart rate and reduce cortisol levels before bed. For many individuals, this serves as a positive sensory cue for sleep and is an acceptable component of a bedtime routine. Unless the music is disruptive or too loud, it is considered a supportive habit.
4. Administering analgesics 30 minutes before bed is an appropriate intervention for pain-related insomnia. Managing physical discomfort allows the client to relax sufficiently for sleep onset and prevents nocturnal awakenings caused by pain surges. This timing aligns with the pharmacokinetic onset of most oral pain medications to ensure comfort at the time of retiring.
Test-taking strategy
- Identify the norm: Recognize that normal sleep latency is ≤30 minutes; any value above this (Choice 3) is a red flag in a sleep history.
- Assess restoration: Focus on the goal of sleep; feeling “refreshed” (Choice 1) is the primary positive outcome of a healthy sleep cycle.
- Routine evaluation: Distinguish between helpful routines (music) and harmful ones (caffeine/late exercise) to determine if follow-up is needed.
- Prioritize comfort: Validate the use of pain medication (Choice 4) as a necessary step for clients with chronic or acute physical distress.
- Identify data gaps: When a client reports a specific delay like “60 minutes,” the nurse's next step is always to explore the “why” through further questioning.
Take home points
- Sleep latency shorter than 5 minutes can indicate severe sleep deprivation or pathological sleepiness.
- Chronic difficulty falling asleep can lead to conditioned arousal, where the client feels more awake as bedtime approaches.
A nurse is working in a sleep disorder clinic. Which of the following is the most common complaint of clients visiting sleep disorder clinics?
Explanation
Insomnia is a prevalent sleep-wake disorder characterized by persistent dissatisfaction with sleep quantity or quality associated with difficulty initiating or maintaining sleep. It is often classified as chronic when symptoms occur at least 3 times per week for at least 3 months. This condition results in significant daytime impairment, including fatigue, decreased concentration, and mood disturbances. Because it is frequently comorbid with psychological stressors and medical conditions, it represents the primary reason individuals seek specialist evaluation in clinical settings.
Rationale for correct answer
3. Chronic insomnia is statistically the most frequent complaint encountered in sleep disorder clinics worldwide. It affects a vast portion of the population and serves as a gateway symptom for many other underlying health issues. Patients seek help because the persistent lack of restorative sleep severely impacts their occupational and social functioning.
Rationale for incorrect answers
1. Hypersomnia, or excessive daytime sleepiness, is a significant clinical finding but is less common as a primary presenting complaint than insomnia. While it occurs in conditions like Kleine-Levin syndrome, it is often a symptom of another disorder rather than the primary reason for a clinic visit. Most patients with hypersomnia are actually suffering from sleep deprivation or apnea.
2. Narcolepsy is a relatively rare neurological condition affecting approximately 1 in 2,000 individuals. While it is a serious disorder requiring specialist management, its low prevalence means it is not the “most common” complaint. Clinics see far more cases of behavioral and stress-induced insomnia than primary narcoleptic sleep attacks.
4. Enuresis, or bedwetting, is a parasomnia primarily seen in pediatric populations and is usually managed by pediatricians or urologists. While it can be a part of a sleep evaluation, it is a specialized complaint rather than a general one. It does not represent the majority of cases seen in an adult-focused or general sleep disorder clinic.
Test-taking strategy
- Frequency assessment: When asked for the most common complaint, choose the condition that has the highest prevalence in the general population (insomnia).
- Identify the core audience: Most sleep clinics deal with adult populations where stress and lifestyle-related sleep initiation issues predominate.
- Distinguish between symptom and disorder: Recognize that while many people are sleepy (hypersomnia), they usually complain of the inability to sleep well at night (insomnia).
- Prevalence knowledge: Use clinical data to rule out rare conditions like narcolepsy (Choice 2) when looking for the most frequent clinical encounter.
Take home points
- Insomnia can be primary or secondary to other conditions like chronic pain, depression, or respiratory disorders.
- Cognitive Behavioral Therapy for Insomnia (CBT-I) is the gold-standard treatment for chronic cases and is preferred over long-term medication.
A nurse is aware that a prolonged pattern of REM deprivation may result in which of the following?
Explanation
Rapid eye movement deprivation interferes with the brain's ability to process emotional regulation and consolidate memory, leading to profound cognitive disintegration. During this stage, the brain exhibits high metabolic activity and neuronal firing comparable to wakefulness, which is essential for psychological equilibrium. Prolonged deficit of this paradoxical sleep results in behavioral irritability, cognitive impairment, and severe perceptual distortions. Chronic disruption often manifests as hallucinatory experiences or disorientation, as the brain attempts to integrate dreaming activity into the waking state.
Rationale for correct answer
1. Significant and prolonged REM deprivation is clinically linked to the development of psychosis symptoms, including paranoia and hallucinations. Without the opportunity for REM-related neurochemical restoration, the cerebral cortex fails to maintain proper reality testing and executive function. This deficit creates a state of psychological instability that can mirror primary psychiatric disorders.
Rationale for incorrect answers
2. Deprivation of REM results in a total loss of dreaming opportunities during the period of restriction, rather than an increase. While a REM rebound occurs after sleep is restored, the deprivation period itself is characterized by the absence of these cycles. Therefore, it is impossible to have increased dreaming while the specific stage is being withheld.
3. Sleep deficiency, particularly the loss of REM, is known to produce increased sensitivity to painful stimuli rather than a decrease. The lack of restorative sleep impairs the descending inhibitory pathways of the central nervous system, lowering the pain threshold. This results in an exacerbated perception of discomfort for the patient.
4. REM sleep is critical for maintaining cognitive vigilance and the processing of complex information. Deprivation leads to a marked decrease in mental alertness, resulting in slowed reaction times and impaired decision-making capabilities. This state of neurocognitive fatigue is a primary safety concern in clinical and occupational settings.
Test-taking strategy
- Psychological impact: Associate REM sleep with psychological and mental health; its loss will therefore cause mental and psychological breakdown.
- Identify physiological trends: Recognize that sleep deprivation generally makes everything worse (more pain, less alertness), which helps rule out Choices 3 and 4.
- Paradoxical definition: Remember that while REM is “paradoxical” sleep, its absence leads to the most “paradoxical” or extreme symptoms like psychosis.
- REBOND vs. Deprivation: Distinguish between the symptoms experienced during deprivation (psychosis) and the compensatory mechanism after (rebound dreaming).
- Clinical severity: Select the answer that reflects the most severe systemic consequence of failing to achieve the highest stage of cognitive rest.
Take home points
- The brain prioritize NREM sleep (physical repair) first; therefore, REM is usually the first stage lost during sleep restriction.
- REM sleep is essential for the unlearning of irrelevant synaptic connections, a process necessary for efficient cognitive function.
Practice Exercise 3
A client has a history of sleep apnea. Which is the most appropriate question for the nurse to ask?
Explanation
Obstructive sleep apnea involves recurrent episodes of upper airway collapse during sleep, leading to hypoxemia and hypercapnia. This fragmentation of sleep architecture results in significant excessive daytime somnolence, loud snoring, and witnessed apneic episodes. Chronic untreated cases often progress to pulmonary hypertension and right-sided heart failure due to persistent nocturnal oxygen desaturation.
Rationale for correct answer
4. The hallmark manifestation of sleep apnea is profound daytime lethargy resulting from repeated arousals. Asking about daytime sleepiness allows the nurse to quantify the severity of sleep fragmentation. It remains the most sensitive indicator for assessing functional impairment in these patients.
Rationale for incorrect answers
1. While chronic nocturnal hypoxia can eventually lead to atrial fibrillation or other dysrhythmias, this is a secondary complication. It does not assess the immediate, primary symptomatic impact of the breathing disorder itself. This question focuses on late-stage sequelae rather than diagnostic screening.
2. Although anatomic factors like a deviated septum can contribute to airway resistance, they are not the definitive cause of apnea. Many patients with nasal blockage do not experience pharyngeal collapse. This question ignores the complex neuromuscular and structural dynamics of the oropharynx.
3. Chest pain may indicate comorbid coronary artery disease or nocturnal angina related to hypoxemic stress on the myocardium. However, it is not a specific diagnostic feature of obstructive sleep apnea. It fails to address the respiratory cycles and sleep quality essential for management.
Test-taking strategy
- Assessment prioritization: When a question asks for the most appropriate question, focus on the assessment that identifies the primary symptom or chief complaint associated with the diagnosis.
- Defining characteristics: Identify the core clinical feature of the condition. For sleep apnea, the disruption of the sleep-wake cycle is the most direct consequence.
- Elimination of sequelae: Rule out options that address secondary complications (cardiac issues) until the primary symptomatic burden (sleepiness) is addressed.
- Patient Safety and Function: Daytime sleepiness is a critical safety concern, particularly for activities like driving, making it a priority in a nursing assessment.
- Symptom specificity: Differentiate between anatomical risk factors (nasal obstruction) and the resulting functional syndrome (sleep apnea). Always choose the functional impact over a possible contributing factor.
Take home points
- Obstructive sleep apnea is characterized by repetitive pauses in breathing due to soft tissue collapse in the pharynx despite ongoing respiratory effort.
- The Epworth Sleepiness Scale is a common clinical tool used to objectively measure the severity of daytime sleepiness in these clients.
A middle-aged client complains of difficulty sleeping because of significant concerns about financial problems. Which outcome would be the most appropriate for the nursing care plan? “By day 5, the client will:
Explanation
Insomnia secondary to psychosocial stressors involves prolonged sleep latency and fragmented sleep architecture due to hyperarousal. Financial anxiety triggers the hypothalamic-pituitary-adrenal axis, increasing cortisol and sympathetic activity which antagonizes the sleep-onset process. Effective nursing interventions focus on restoring sleep efficiency and stabilizing the circadian rhythm. Patients typically exhibit irritability, cognitive impairment, and reduced frustration tolerance when sleep deprivation persists.
Rationale for correct answer
2. A realistic nursing outcome must be measurable and specifically address the physiological deficit of insomnia. Reporting sleep onset within 30 minutes indicates improved sleep latency, a primary goal in behavioral sleep hygiene. This outcome directly evaluates the effectiveness of nursing interventions on the client's ability to initiate rest.
Rationale for incorrect answers
1. Expecting 8 to 10 hours of sleep is often unrealistic for middle-aged adults, as sleep requirements generally decrease with age. Most healthy adults function optimally on 7 to 8 hours. Setting an unattainable goal can increase client frustration and further exacerbate the anxiety-induced insomnia.
3. Solving financial crises is outside the professional scope of nursing practice and is an unrealistic clinical outcome. While a nurse may provide referrals to social services, the nursing diagnosis focuses on the human response to the stressor, which is the sleep disturbance itself.
4. Keeping busy until bedtime is a poor intervention that can actually increase physiological arousal and worsen sleep onset. Proper sleep hygiene dictates a “wind-down” period to allow for melatonin secretion. This choice fails to provide a measurable metric for evaluating the resolution of the sleep complaint.
Test-taking strategy
- Measurability and Specificity: Nursing outcomes must be SMART: Specific, Measurable, Attainable, Realistic, and Timely. Choice 2 provides a specific time frame (20 to 30 minutes) and a deadline (Day 5).
- Scope of Practice: Identify if the intervention or outcome falls within nursing jurisdiction. Resolving financial debt (Choice 3) is a social or financial counseling task, not a primary nursing outcome.
- Realistic Expectations: Evaluate the physiological norms for the age group. 10 hours of sleep (Choice 1) is generally excessive for a middle-aged adult and not a standard therapeutic target.
- Evidence-Based Sleep Hygiene: Rule out options that contradict known sleep science. High activity before bed (Choice 4) is contraindicated for insomnia, as it prevents the necessary drop in core body temperature and heart rate.
- Focus on the Nursing Diagnosis: The primary problem is “Insomnia.” The outcome must directly relate to the client's ability to sleep, rather than just the underlying stressor.
Take home points
- Insomnia is defined by difficulty with sleep initiation, maintenance, or quality despite adequate opportunity for sleep.
- Sleep latency is the amount of time it takes to transition from full wakefulness to sleep, with a normal range being 10 to 30 minutes.
A client reports to the nurse that she has been taking barbiturate sleeping pills every night for several months and now wishes to stop taking them. Which statement is the most appropriate advice for the nurse to provide the client?
Explanation
Barbiturates act as central nervous system depressants by enhancing the activity of gamma-aminobutyric acid (GABA) at the receptor complex. Chronic administration leads to pharmacological tolerance and physical dependence, characterized by significant alterations in sleep architecture, specifically REM suppression. Abrupt cessation after prolonged use triggers a potentially life-threatening withdrawal syndrome, including seizures, hyperthermia, and cardiovascular collapse.
Rationale for correct answer
4. Abrupt discontinuation of barbiturates after months of use is contraindicated due to the high risk of rebound insomnia and severe withdrawal symptoms. The nurse must advise the client to maintain the current regimen until a supervised taper is established by the provider. This ensures physiological stabilization while gradually down-regulating the central nervous system's dependence on the sedative-hypnotic agent.
Rationale for incorrect answers
1. Stopping the medication on a Friday night implies abrupt withdrawal, which is clinically unsafe regardless of the day of the week. Physical dependence on barbiturates requires a medical transition, not just weekend compensation for lost sleep. This advice ignores the risk of status epilepticus and autonomic instability associated with sudden drug removal.
2. Advising a client to continue a medication indefinitely because stopping is “impossible” is therapeutic nihilism and medically inaccurate. While long-term dependence makes cessation challenging, it is achievable through a controlled, slow reduction of the dosage. This statement fails to support the client's health promotion goal of becoming medication-free.
3. Recommending that the client simply discontinue the pills is dangerous nursing advice that could lead to fatal consequences. Barbiturate withdrawal is more physiologically taxing than opioid withdrawal and requires close monitoring and pharmacological support. This choice violates the fundamental nursing principle of maintaining patient safety during transitions of care.
Test-taking strategy
- Safety First: In pharmacology questions involving CNS depressants, benzodiazepines, or barbiturates, abrupt cessation is almost always the wrong answer due to seizure risks.
- Scope of Practice: The nurse identifies the danger but must direct the client to the primary care provider to manage the technical aspects of a medication taper.
- Identify the Risk: Recognize the “several months” timeframe as an indicator of physical dependence, which necessitates a different approach than short-term usage.
- Prioritize Physiological Integrity: Protecting the client from withdrawal-induced seizures (Risk Reduction) takes precedence over the client's immediate desire to stop the drug.
- Rule of Elimination: Eliminate any option that suggests stopping “cold turkey” or ignores the potential for life-threatening withdrawal symptoms.
Take home points
- Barbiturates significantly reduce REM sleep; sudden withdrawal causes REM rebound, leading to vivid nightmares and disrupted rest.
- Withdrawal symptoms usually manifest within 8 to 16 hours after the last dose and can peak with grand mal seizures.
- A gradual dose reduction, often involving switching to a long-acting agent like phenobarbital, is the standard protocol for detoxification.
A client who is in college was referred to the campus health service because of difficulty staying awake in class. What should be included in the nurse’ s assessment? Select all that apply.
Explanation
Excessive daytime somnolence in the collegiate population often stems from a misalignment of the circadian rhythm or poor sleep hygiene. Assessment must differentiate between primary sleep disorders, such as narcolepsy, and secondary causes like substance-induced sleep fragmentation or sleep debt. A thorough history identifies behavioral patterns and physiological stressors that impair cognitive vigilance and academic performance. Chronic sleep deprivation in young adults is strongly correlated with mood dysregulation and increased risk for motor vehicle accidents.
Rationale for correct answers
1. Quantifying sleep duration on weekdays versus weekends reveals sleep debt patterns and irregular sleep-wake cycles common in students. Significant discrepancy suggests a “catch-up” phenomenon, indicating that the baseline rest is insufficient for metabolic and neurological demands. This data is essential for diagnosing social jet lag and behavioral sleep restriction.
2. Alcohol is a potent REM suppressant that causes significant sleep fragmentation and mid-night awakenings as blood alcohol levels decline. Assessing consumption helps determine if the daytime lethargy is a result of poor quality rather than quantity of sleep. Chronic use alters the sleep architecture, leading to persistent daytime cognitive impairment.
3. Determining the symptom onset helps differentiate between acute, stress-related insomnia and chronic sleep disorders or underlying medical conditions. Knowing the duration and triggers provides a diagnostic timeline for evaluating the severity of the somnolence. This information guides the clinician in deciding if a specialist referral is necessary.
5. Many over-the-counter medications and herbal remedies possess sedative properties or interact with central nervous system stimulants like caffeine. Identifying all pharmacological substances is critical to rule out drug-induced drowsiness or paradoxical reactions that affect wakefulness. Some herbal supplements can interfere with sleep architecture or cause daytime grogginess.
Rationale for incorrect answers
4. Subjective boredom is not a clinical assessment for pathological daytime somnolence. If a client is physiologically rested, they should be able to maintain wakefulness even in less stimulating environments. Focusing on interest levels ignores the underlying physiological or behavioral causes of the inability to stay awake.
Test-taking strategy
- Comprehensive Assessment: In “Select all that apply” questions, prioritize options that collect objective and subjective data across physical, chemical, and behavioral domains.
- Clinical vs. Subjective: Distinguish between legitimate clinical factors (drugs, sleep hours, duration) and non-clinical environmental factors like “boring classes.”
- Identify Secondary Causes: Always assess for substance use (alcohol) and medications in any client presenting with altered levels of consciousness or alertness.
- Pattern Recognition: Look for options that allow for the comparison of habits (weekdays vs. weekends) to identify lifestyle-induced sleep deficits.
- Safety and Holistic View: Ensure the assessment covers the “what” (symptoms), the “when” (duration), and the “why” (drugs or alcohol).
Take home points
- Sleep debt is cumulative; the brain keeps an accurate accounting of lost sleep that must eventually be repaid.
- Alcohol might decrease sleep latency but severely disrupts the later stages of sleep, leading to non-restorative rest.
- Stimulant overuse (caffeine, nicotine) can cause a rebound effect of extreme tiredness once the substance is metabolized.
The nurse is discussing with an older client the factors that induce sleep. Which of the following does the nurse teach the client?
Explanation
Geriatric sleep is characterized by a significant decrease in sleep efficiency and alterations in the distribution of sleep stages. As the brain ages, there is a marked reduction in the duration of deep sleep (Stage 3 and 4 NREM) and a concurrent decline in total REM sleep. Older adults often experience nocturnal awakenings and a more superficial sleep depth, leading to a higher frequency of napping during the day. Understanding these age-related changes is vital for the nurse to distinguish between normal maturation and pathological insomnia in the elderly.
Rationale for correct answer
3. Research indicates that the total percentage of REM sleep tends to decrease as a person ages, particularly from late adulthood into senescence. This reduction in paradoxical sleep is often accompanied by the nearly complete loss of slow-wave sleep in the very elderly. Educating the client on these physiological shifts helps manage expectations regarding sleep quality and duration in later life.
Rationale for incorrect answers
1. Regular tea contains caffeine, a central nervous system stimulant that blocks adenosine receptors and increases sleep latency. Drinking caffeinated tea in the evening is more likely to prevent sleep than induce it, especially in older adults with slower metabolism. This advice contradicts standard sleep hygiene protocols for all age groups.
2. While alcohol may initially act as a sedative to decrease sleep onset time, it severely disrupts sleep maintenance. Alcohol causes significant sleep fragmentation and suppresses REM architecture, leading to non-restorative rest and early morning awakenings. Large quantities of alcohol are especially dangerous for the elderly due to the risk of respiratory depression and falls.
4. Moderate physical activity is a well-documented promoter of sleep and generally increases the duration of both deep NREM and REM stages. Regular exercise helps stabilize the circadian rhythm and facilitates the drop in core body temperature necessary for sleep onset. It is only vigorous exercise performed immediately before bed that might negatively impact sleep initiation.
Test-taking strategy
- Developmental knowledge: Focus on the universal trend in aging: sleep becomes lighter, shorter, and REM/Deep stages consistently decrease.
- Pharmacological knowledge: Identify caffeine (Choice 1) and alcohol (Choice 2) as substances that impair sleep quality despite any perceived sedative effects of alcohol.
- Intervention impact: Recognize that healthy lifestyle choices like physical activity (Choice 4) are sleep promoters rather than inhibitors.
- Clinical reassurance: The nurse's role in geriatric care is often to explain that “lighter sleep” (Choice 3) is a natural part of aging, not necessarily a disease.
- Identifying REM trends: REM sleep occupies about 50% of an infant's sleep but drops to 20-25% in adults and continues to decline slightly in the elderly.
Take home points
- Older adults are more likely to experience circadian phase advance, leading them to feel sleepy earlier in the evening and wake earlier in the morning.
- The reduction in deep sleep makes the elderly more susceptible to being awakened by environmental noises or physical discomfort.
Comprehensive Questions
A new nursing graduate’s first job requires 12-hour night shifts. Which strategy will make it easier for the graduate to sleep during the day and remain awake at night?
Explanation
Shift work disorder results from a mismatch between the circadian rhythm and the required work-rest schedule. Exposure to morning sunlight triggers the suprachiasmatic nucleus to inhibit melatonin production, promoting wakefulness when sleep is needed. To facilitate daytime rest, the individual must minimize photic stimulation and maintain a cool, quiet environment to mimic nocturnal conditions. Chronic disruption of this cycle increases the risk for metabolic syndrome and cardiovascular disease.
Rationale for correct answer
1. Reducing light exposure during the morning commute prevents the suppression of endogenous melatonin by the retina. Utilizing dark sunglasses and blackout curtains creates a biological signal that promotes sleep onset during daylight hours. This strategy effectively anchors the circadian rhythm to the required daytime sleep period.
Rationale for incorrect answers
2. Physical exertion raises the core body temperature and stimulates the sympathetic nervous system, which antagonizes the transition to sleep. Post-shift exercise can lead to prolonged sleep latency, making it difficult to rest before the next shift. High-intensity activity should be completed at least 3 hours before an intended sleep period.
3. Consuming large quantities of caffeine at the start of a 12-hour shift may provide a temporary alertness boost but often leads to a “crash.” If caffeine is consumed too late in the shift, its long half-life will interfere with the ability to fall asleep upon returning home. Over-reliance on stimulants can further destabilize the underlying circadian architecture.
4. While bright light at night can improve alertness, this choice is less comprehensive than managing the light-dark cycle during the commute. Without protecting the eyes from morning sun, the benefit of night-shift lighting is negated by circadian resetting on the drive home. Choice 1 addresses the most critical barrier to daytime sleep consolidation.
Test-taking strategy
- Circadian Biology: Focus on interventions that manipulate light exposure, as light is the primary “zeitgeber” or time-giver for the human biological clock.
- Physiological antagonism: Rule out activities that stimulate the body, such as exercise (Choice 2) or heavy caffeine use (Choice 3), immediately prior to the desired sleep time.
- Comprehensive care: Look for the answer that addresses both the “awake at night” and “sleep during the day” aspects; Choice 1 directly facilitates the most difficult part: daytime rest.
- Environmental control: Prioritize strategies that modify the environment (darkness) to align with human physiology.
- Safety and adaptation: Shift work requires active management of the environment to prevent the negative health outcomes associated with chronic sleep deprivation.
Take home points
- Melatonin secretion is naturally inhibited by blue light; shift workers must block this light to successfully sleep during the day.
- Maintaining a consistent sleep-wake schedule, even on days off, helps stabilize the circadian rhythm for night-shift employees.
The nurse is answering questions after a presentation on sleep at a local senior citizens center. A woman in her late 70s asks for an opinion about the advisability of allowing her husband to nap for 15 to 20 minutes each afternoon. Which is the nurse’s best response?
Explanation
Sleep architecture changes significantly in late adulthood, characterized by increased sleep fragmentation and a reduction in deep, slow-wave sleep. Older adults often experience a circadian phase advance, leading to earlier bedtimes and early morning awakenings. Brief naps are often a compensatory mechanism for these changes and do not necessarily indicate pathological insomnia if nocturnal sleep remains satisfactory.
Rationale for correct answer
3. A brief “power nap” of ≤20 minutes can improve alertness and mood without causing sleep inertia or significantly reducing nocturnal sleep drive. If the husband has no difficulty with sleep initiation at night, the nap is considered a healthy adaptation to aging. This response supports the client's autonomy while providing safe, evidence-based parameters.
Rationale for incorrect answers
1. Restricting a nap and forcing stimulating activity can lead to over-exhaustion and increased irritability in the elderly. Unless the nap is excessively long, it generally does not cause nocturnal wakefulness. This advice is overly restrictive and ignores the normal physiological tendency for napping in the geriatric population.
2. This statement is dismissive and fails to account for the age-related changes in sleep efficiency that make napping common. Even with adequate nocturnal time in bed, the quality of sleep in the 70s is often lower, necessitating a brief afternoon rest. It ignores the reality of geriatric physiology.
4. Caffeine consumption in the afternoon can lead to nocturnal insomnia and increased frequency of nighttime urination (nocturia). Elderly patients are more sensitive to the diuretic effects and cardiac stimulation of caffeine. Recommending stimulants to bypass natural tiredness is inappropriate and potentially harmful for this age group.
Test-taking strategy
- Geriatric norms: Recognize that napping is a frequent and often normal part of the sleep-wake pattern in older adults.
- Conditional logic: Look for the answer that qualifies the advice; napping is “fine” unless it interferes with the primary goal (nocturnal sleep).
- Avoid harmful interventions: Rule out caffeine (Choice 4) for the elderly, as it carries risks for hypertension, tachycardia, and bladder irritation.
- Normal vs. Pathological: Distinguish between a short, refreshing nap and prolonged daytime somnolence, which might indicate depression or sleep apnea.
- Client-centered communication: The best response provides reassurance while defining the limits of healthy behavior.
Take home points
- Sleep efficiency naturally declines with age, meaning seniors spend more time in bed but less time in actual restorative sleep.
- Naps should be limited to 15 to 30 minutes; longer naps can lead to sleep inertia and difficulty falling asleep at night.
The client tells the nurse that her sleep tends to be very light and that it is difficult for her to get back to sleep if she’s awakened at night. Which interventions should the nurse implement? Select all that apply
Explanation
Hospital-induced sleep fragmentation occurs when environmental stimuli and clinical interruptions disrupt the circadian rhythm and sleep architecture. Light sleepers often spend more time in stage N1 and N2 sleep, making them highly susceptible to arousal from sudden auditory peaks. Maintaining sleep continuity is essential for immune function, wound healing, and psychological stability during acute illness. Chronic sleep deprivation in the clinical setting can lead to intensive care delirium and impaired pain modulation.
Rationale for correct answers
1. Noise reduction is a primary nursing responsibility to prevent the disruption of non-REM sleep. Maintaining low conversation volumes in hallways and nursing stations eliminates startle responses that trigger sympathetic activation. This intervention directly modifies the environment to accommodate the client's sensitivity to auditory disturbances.
3. Clustering nursing care at 90-minute or 3-hour intervals aligns with the natural ultradian cycles of human sleep. A full sleep cycle typically lasts 90 to 110 minutes; therefore, timing interventions at these specific increments allows the client to complete full cycles of restorative rest. This strategy minimizes the physiological impact of necessary clinical interruptions.
4. Consistent auditory stimuli, such as a fan, provide white noise that masks erratic environmental sounds. By raising the auditory threshold for arousal, the nurse helps the client remain in deeper stages of sleep despite hospital activity. This is a non-pharmacological method to stabilize the sensory environment for light sleepers.
Rationale for incorrect answers
2. Soft music is not always beneficial because it contains variable frequencies and rhythms that can be stimulating rather than sedating. Unlike white noise, music may capture cognitive attention, preventing the brain from transitioning into a truly restful state. For a light sleeper, any distinct sound can become a focal point of wakefulness.
5. Elevated ambient temperatures interfere with the natural nocturnal thermoregulation required for deep sleep. The human body must experience a slight drop in core temperature to initiate and maintain the sleep state. Increasing room temperature typically leads to restlessness, diaphoresis, and increased sleep fragmentation.
Test-taking strategy
- Physiological alignment: Select interventions that respect the 90-minute architecture of the human sleep cycle, as seen in Choice 3.
- Environmental modification: Prioritize actions that reduce peak noises or provide masking sounds (Choices 1 and 4) to protect the client's sensory threshold.
- Thermoregulation principles: Recall that a cool environment (generally 60 to 67 degrees Fahrenheit) is clinically superior to a warm one for promoting sleep.
- Cluster care: Use the principle of clustering to minimize the frequency of awakenings while still meeting the client's medical needs.
- Assess Music vs. White Noise: Distinguish between white noise (consistent/masking) and music (variable/potentially stimulating) when the goal is to prevent arousal in light sleepers.
Take home points
- Sleep cycles repeat approximately every 90 minutes, progressing through N1, N2, N3, and finally REM sleep.
- The peak noise levels in hospitals often exceed 80 to 90 decibels, which is sufficient to trigger a stress response even if the patient remains asleep.
- Melatonin production is most efficient in environments that are dark, quiet, and slightly cool.
A nurse is aware that which of the following records muscle tone?
Explanation
Polysomnography utilizes a battery of electrophysiological sensors to categorize the stages of sleep and monitor neuromuscular activity. During sleep studies, the assessment of skeletal muscle activity is essential to differentiate between NREM and REM sleep states. In REM sleep, the brain sends inhibitory signals to the spinal cord, resulting in a state of active paralysis or atonia. Measuring these electrical potentials allows clinicians to diagnose disorders such as REM sleep behavior disorder or periodic limb movement disorder.
Rationale for correct answer
4. The electromyograph (EMG) is the specific instrument used to record the electrical activity and muscle tone of skeletal muscles. During sleep studies, EMG electrodes are typically placed on the mentalis muscle (chin) or the anterior tibialis (legs). Changes in the EMG amplitude are the definitive markers for the loss of muscle tone characteristic of REM sleep.
Rationale for incorrect answers
1. The electroencephalograph (EEG) measures the electrical activity of the cerebral cortex, specifically recording brain waves. It is used to identify sleep stages such as delta waves in deep sleep or sleep spindles in stage N2. It does not provide direct data regarding the tension or contraction of peripheral muscles.
2. The electrocardiograph (ECG) records the electrical impulses of the heart's conduction system to monitor cardiac rhythm. While it is part of a sleep study to detect arrhythmias associated with nocturnal apnea, it has no role in assessing the tone of skeletal muscle. It is strictly for myocardial assessment.
3. The electrooculograph (EOG) is designed to measure the resting potential of the retina and the movement of the eyes. It is critical for identifying the rapid eye movements that define the REM stage of sleep. It cannot measure the electrical activity or tone of skeletal muscle groups.
Test-taking strategy
- Etymology clues: Use the Greek roots: “myo” means muscle, “electro” means electricity, and “graph” means record. Therefore, EMG is the recording of muscle electricity.
- Functional matching: Match the organ to the test: EEG = Brain; ECG = Heart; EOG = Eyes; EMG = Muscle.
- Polysomnography components: Remember that a full sleep study requires all four “graphs” to create a complete picture of the patient's sleep architecture.
- Identify the goal: The question asks specifically for “muscle tone,” which is a motor function, directing you away from cortical (EEG) or sensory (EOG) measures.
- Differentiate EMG use: Recognize that while EMG is used in neurology for nerve conduction, in sleep medicine, its primary role is detecting the atonia of REM sleep.
Take home points
- Atonia (complete loss of muscle tone) is a protective mechanism during REM sleep to prevent the individual from physically acting out dreams.
- Increased EMG activity during sleep can indicate bruxism (teeth grinding) or restless legs syndrome.
- The EEG is the gold standard for determining if a patient is actually asleep, while the EMG and EOG help classify the specific sleep stage.
A nurse is preparing a staff education program on sleep. How many cycles of sleep does a person typically go through each night?
Explanation
Sleep architecture is organized into repetitive ultradian cycles that consist of distinct NREM and REM stages. Each complete cycle typically lasts approximately 90 to 120 minutes, allowing for the necessary physiological transitions from light to slow-wave sleep and eventually into paradoxical sleep. For an average adult obtaining 7 to 8 hours of rest, these cycles repeat in a predictable sequence throughout the night. Disruption of these consolidated cycles often leads to cognitive deficits, impaired immune function, and a significant increase in metabolic stress markers.
Rationale for correct answer
2. A person typically completes 4 or 5 sleep cycles during a standard nocturnal period of 7 to 8 hours. Each cycle represents a full progression through the sleep stages, ensuring a balance between physical restoration in NREM and cognitive processing in REM. This number of cycles is the biological standard required for the brain to maintain homeostatic equilibrium and neuroplasticity.
Rationale for incorrect answers
1. Completing only 2 or 3 cycles would provide roughly 3 to 4.5 hours of sleep, which is insufficient for most adults. This level of sleep restriction prevents the longer REM periods that occur in the latter half of the night. Chronic deprivation at this level results in severe daytime impairment and accumulated sleep debt.
3. Experiencing 10 to 12 cycles would require a total sleep duration of 15 to 18 hours, which is pathological for an adult. Such hypersomnolence is atypical and may indicate underlying neurological disorders or severe clinical depression. It far exceeds the physiological norm for healthy human sleep-wake regulation.
4. Transitioning through 20 to 25 cycles is physically impossible within a single night as it would imply cycles lasting only 20 minutes. Such extreme sleep fragmentation would mean the individual never enters deep NREM or REM stages. This pattern would reflect a complete collapse of sleep architecture rather than a typical night of rest.
Test-taking strategy
- Mathematical calculation: Use the 90-minute rule for a standard cycle and multiply by a healthy 7.5-hour sleep duration (450 minutes / 90 minutes = 5 cycles).
- Identify normative data: Differentiate between infant and adult patterns; while infants have shorter cycles, the question refers to a general person, implying the adult standard.
- Architecture knowledge: Recall that the proportion of REM sleep increases in later cycles, making the completion of 4 to 5 cycles essential for mental health.
- Rule of extremes: Eliminate options that represent extreme sleep deprivation (Choice 1) or extreme oversleeping/fragmentation (Choices 3 and 4).
- Clinical significance: Focus on the range that supports optimal “restorative sleep,” which is the primary objective of nursing education programs.
Take home points
- The first sleep cycle of the night is usually the shortest, with subsequent cycles featuring longer REM periods and shorter deep sleep stages.
- Interruption of a sleep cycle can lead to sleep inertia, characterized by grogginess and impaired motor dexterity upon awakening.
- Most adults need to complete at least 4 cycles to feel refreshed and maintain high-level executive functioning the following day.
A nurse is educating a client about a sleep diary. Which of the following descriptions is true of the diagnostic tool?
Explanation
A sleep diary is a prospective self-reporting tool used to identify patterns, triggers, and the severity of sleep disturbances over time. It serves as a bridge between the patient’s subjective experience and objective diagnostic testing like polysomnography. By tracking external variables, clinicians can identify circadian rhythm misalignments or poor hygiene habits that contribute to insomnia. Accurate documentation of lifestyle factors is essential for developing a personalized behavioral intervention plan, such as Stimulus Control Therapy.
Rationale for correct answer
2. A comprehensive sleep diary must include a record of daily physical activity because exercise significantly influences sleep latency and quality. Physical exertion helps regulate the circadian clock and promotes deep NREM sleep, provided it is not performed too close to bedtime. Tracking activity levels allows the nurse to correlate sedentary behavior or over-exertion with specific sleep outcomes.
Rationale for incorrect answers
1. To be diagnostically significant and account for variable patterns, a sleep diary is generally kept for at least 14 days (2 weeks). A 1-week log is often insufficient to capture the differences between weekday and weekend sleep-wake cycles. Longer tracking periods are necessary to establish a reliable baseline of the patient's sleep architecture.
3. Recording body temperature each evening is not a standard component of a clinical sleep diary. While core temperature fluctuations are part of the circadian rhythm, they are typically measured in research settings using specialized equipment. For routine diagnostic purposes, tracking substances and activities is far more clinically relevant than self-monitoring temperature.
4. A sleep diary reports objective data points (such as the number of awakenings, time of lights out, and caffeine intake) rather than just primarily subjective feelings. While it is self-reported, the goal is to provide a factual timeline of events. Stating it is primarily subjective diminishes the quantitative value of the specific metrics recorded by the patient.
Test-taking strategy
- Component identification: Look for the answer that includes a known zeitgeber or influencer of sleep; physical activity is a primary driver of sleep drive.
- Standard duration: Remember the two-week rule for behavioral logs in sleep medicine to ensure data reliability.
- Objective vs. Subjective: Differentiate between “how I felt” (subjective) and “what I did/what time it was” (objective). A diary focuses on the latter.
- Feasibility check: Evaluate if the task is a standard clinical recommendation; patients are rarely asked to take their temperature for sleep logs (Choice 3).
- Clinical utility: Choose the option that provides the most actionable data for a nursing care plan involving sleep hygiene.
Take home points
- Sleep diaries should include the timing of caffeine, alcohol, and nicotine consumption, as these substances directly impair sleep quality.
- Patients should be instructed to complete the diary twice daily: once in the morning (about the night) and once in the evening (about the day).
- The log helps differentiate between sleep maintenance insomnia (waking up) and sleep onset insomnia (trouble falling asleep).
A nurse should suggest that a client should do which of the following to help them get to sleep?
Explanation
Sleep initiation is significantly influenced by psychological conditioning and the stabilization of the circadian rhythm. Maintaining a consistent bedtime routine facilitates the transition from wakefulness to sleep by lowering cortical arousal and signaling the brain to increase melatonin secretion. Disruptions to these established patterns, common in the hospital environment, can lead to increased sleep latency and fragmented rest. Behavioral interventions that mimic the home environment are considered first-line nursing strategies for promoting optimal sleep hygiene.
Rationale for correct answer
1. Following a usual routine utilizes the principle of association to prepare the body and mind for rest. Predictable activities, such as reading or performing hygiene rituals, help decrease environmental stress and promote relaxation. This approach is the most effective non-pharmacological intervention for maintaining the client's normal sleep-wake cycle during times of illness or hospitalization.
Rationale for incorrect answers
2. Consuming several glasses of water immediately before bed is contraindicated as it leads to nocturia, the frequent need to urinate during the night. This disrupts sleep maintenance and prevents the client from completing full, restorative sleep cycles. Fluid intake should be restricted in the hours leading up to bedtime to ensure nocturnal continuity.
3. A large snack or heavy meal before bed can cause gastrointestinal discomfort and acid reflux, which interfere with the ability to fall and stay asleep. While a light, carbohydrate-based snack may promote sleep, excessive calories increase metabolic activity and core body temperature. This physiological activation is the antithesis of the cooling process required for deep sleep.
4. Relying on a sedative-hypnotic every night is inappropriate due to the high risk of pharmacological tolerance and physical dependence. These medications often alter sleep architecture by suppressing REM and deep NREM stages. Long-term use can lead to rebound insomnia upon discontinuation and should be reserved for short-term, acute situations under strict supervision.
Test-taking strategy
- Prioritize natural interventions: In nursing care plans, always select non-invasive, behavioral modifications like routines before considering pharmacological or physiological disruptors.
- Identify disruptors: Rule out choices that introduce new problems, such as nocturia (Choice 2) or indigestion (Choice 3), which are known barriers to sleep.
- Assess sustainability: Evaluate if the intervention is safe for long-term use; nightly sedation (Choice 4) is generally unsafe and is not a primary nursing recommendation.
- Focus on habituation: Recognize that the brain thrives on cues; the usual routine is a powerful cue for the nervous system to down-regulate.
- Clinical safety: Select the option that supports the highest quality of sleep architecture without the side effects of medications or metabolic interruptions.
Take home points
- Bedtime routines should ideally begin 30 to 60 minutes before the intended sleep time to allow for physiological winding down.
- Nocturia is a leading cause of sleep fragmentation in older adults and can be mitigated by shifting fluid intake to earlier in the day.
- Sleep hygiene education is a core nursing competency that empowers patients to manage insomnia without initial pharmaceutical intervention.
A nurse is caring for a client who reports vivid dreams during sleep. Active dreaming occurs during what stage of sleep?
Explanation
REM sleep is characterized by high-frequency, low-voltage brain waves similar to those seen in an active wakefulness state. This stage is associated with intense cortical activation and the processing of emotional experiences through narrative-driven mental activity. While some fragmented thoughts occur in NREM, the dreams in REM are typically vivid and elaborate, involving complex visual imagery and emotional depth. The body maintains a state of functional paralysis during this time to protect the individual from physically responding to the dream content.
Rationale for correct answer
4. Most active dreaming occurs during the REM (Rapid Eye Movement) stage, where the brain's metabolic rate increases significantly. Dreams during this period are more likely to be narrative and vivid, and patients are more likely to remember them if awakened. This stage represents the peak of cognitive processing and emotional integration during the sleep cycle.
Rationale for incorrect answers
1. Stage 2 NREM is a period of light sleep where cognitive activity is minimal and focused on basic memory stabilization. While sleep thoughts may occur, they lack the narrative structure and intensity of true REM dreams. It is primarily a transitional stage where the brain prepares for deeper levels of unconsciousness.
2. Stage 3 NREM represents the beginning of deep sleep, characterized by slow delta waves and reduced cerebral blood flow. Mental activity during this stage is usually non-vivid and disconnected, consisting of isolated images rather than complex dreams. The focus here is on physical restoration rather than active, narrative dreaming.
3. Stage 4 NREM is the deepest phase of sleep, where the arousal threshold is highest and brain activity is at its lowest. Dreams in this stage are rare and, if they occur, are typically vague and conceptual rather than vivid or active. Awakening a patient from this stage usually results in significant disorientation rather than dream recall.
Test-taking strategy
- Categorization of dreams: Distinguish between sleep thoughts (NREM) and vivid dreams (REM).
- Physiological correlation: Match active dreaming with “active” brain waves (REM/Paradoxical sleep).
- Atonia context: Recognize that vivid dreaming requires the muscle paralysis (atonia) found only in REM to prevent injury.
- Stage progression: Recall that REM periods lengthen throughout the night, which explains why most people remember vivid dreams just before waking in the morning.
- Elimination: Rule out NREM stages 1 through 4 when the question specifies “vivid” or “active” dreaming, as these are primarily quiet sleep phases.
Take home points
- The first REM period of the night usually lasts about 10 minutes, but the final period can last up to an hour.
- REM dreams are often characterized by bizarre content and a lack of logical progression due to the inactivity of the prefrontal cortex.
- During REM, the sympathetic nervous system is active, leading to increased heart rate and irregular breathing.
A nurse is describing illness as a stressor that can influence sleep during various stages. Which example would be most appropriate for the nurse to use?
Explanation
Metabolic and endocrine disorders significantly alter the homeostatic regulation of sleep architecture by interfering with neurochemical signaling. Thyroid hormones modulate the sensitivity of the reticular activating system and influence the duration of various sleep phases. Hypothyroidism specifically causes a reduction in metabolic rate, leading to decreased slow-wave sleep and increased daytime somnolence. Chronic hormonal imbalances disrupt the ultradian rhythm, resulting in non-restorative rest and impaired physical recovery.
Rationale for correct answer
1. Hypothyroidism is a well-documented endocrine stressor that disrupts the normal progression of sleep, specifically decreasing the amount of deep NREM sleep (Stages 3). This metabolic slowing impairs the body’s ability to achieve the most physiologically restorative phases of rest. Consequently, patients often experience persistent fatigue despite spending excessive hours in bed.
Rationale for incorrect answers
2. Patients with coronary artery disease are actually more prone to experiencing nocturnal angina during REM sleep rather than NREM. The autonomic instability and sympathetic surges characteristic of REM sleep increase myocardial oxygen demand. This makes the paradoxical stage a higher risk period for cardiac ischemia than the stable NREM phases.
3. Seizure activity in patients with epilepsy is frequently suppressed during REM sleep due to cortical desynchronization and muscle atonia. Conversely, seizures are much more likely to occur during NREM sleep, particularly during the transitions between stages 1 and 2. The synchronized brainwaves of NREM provide a more fertile environment for the propagation of electrical discharges.
4. Gastric acid secretion in individuals with peptic ulcer disease typically increases during REM sleep due to parasympathetic dominance. This surge in hydrochloric acid often causes nocturnal awakening characterized by epigastric pain. The relatively quiet metabolic state of NREM sleep is not the primary period for these symptomatic gastric secretions.
Test-taking strategy
- Endocrine associations: Link thyroid function directly to the volume and depth of NREM sleep stages.
- REM pathophysiology: Remember that REM is a period of autonomic storms; thus, cardiac and gastric symptoms are more likely during REM.
- Epilepsy patterns: Differentiate between NREM (synchronized/pro-seizure) and REM (desynchronized/anti-seizure) to rule out Choice 3.
- Metabolic rate: Recognize that low metabolic states (hypothyroidism) correlate with a reduction in the active deep NREM repair stages.
- Elimination of common errors: Avoid the misconception that all illnesses worsen during NREM; the physiological intensity of REM is a major trigger for specific symptoms.
Take home points
- Hypothyroidism is associated with excessive sleep duration but poor sleep quality due to the loss of delta-wave activity.
- Hyperthyroidism has the opposite effect, often causing fragmented sleep and shortened sleep latency due to hyperarousal.
A nurse is educating a client on caffeine use. Which of the following statements should the nurse include?
Caffeine should be:
Explanation
Caffeine is a methylxanthine derivative that acts as a potent adenosine receptor antagonist within the central nervous system. By blocking adenosine, which is a byproduct of energy metabolism that promotes sleep pressure, caffeine maintains a state of artificial alertness. It has a significant pharmacokinetic half-life, typically ranging from 3 to 7 hours in healthy adults. This prolonged duration of action means that consumption in the late afternoon or evening significantly increases sleep latency and reduces the depth of slow-wave sleep.
Rationale for correct answer
3. To minimize the disruption of sleep architecture, caffeine should be avoided at least 4 to 5 hours before the intended bedtime. This timeframe allows the plasma concentration of the stimulant to decline sufficiently so it does not interfere with adenosine binding. Adhering to this restriction is a fundamental component of sleep hygiene education to reduce nocturnal wakefulness.
Rationale for incorrect answers
1. Avoiding caffeine for only 30 minutes before bedtime is clinically ineffective because the drug will still be at peak or near-peak levels during sleep onset. The metabolic clearance of caffeine takes much longer than half an hour. Such late consumption will inevitably result in sleep fragmentation and difficulty initiating rest.
2. Combining caffeine with milk does not neutralize or counteract its stimulatory effects on the central nervous system. While milk provides tryptophan, the pharmacological potency of the caffeine remains unchanged and will still block the sleep-promoting receptors. This statement provides the client with false reassurance regarding their sleep hygiene habits.
4. Encouraging caffeine use to combat the effects of sleeplessness creates a maladaptive cycle of stimulant dependence and worsening insomnia. This “caffeine-rest” loop prevents the body from resolving the underlying sleep debt and can mask symptoms of serious disorders like apnea. The nurse should promote sleep consolidation rather than pharmacological compensation for fatigue.
Test-taking strategy
- Half-Life awareness: Always choose the longest reasonable timeframe for avoiding stimulants (4 to 5 hours) to account for drug metabolism.
- Identify pharmacological facts: Rule out myths like “milk counteracts caffeine,” as nutritional additives do not change the drug's mechanism of action.
- Health promotion: Avoid recommending the treatment of one problem (sleeplessness) with a substance that causes another (caffeine dependence).
- Physiological impact: Focus on how the drug affects the brain (adenosine receptors) rather than just the timing of the dose.
Take home points
- Caffeine reduces the total amount of Stage 3 and 4 NREM sleep, leading to a feeling of being unrefreshed even if sleep duration is adequate.
- Individual sensitivity to caffeine varies; some people may need to stop consumption as early as noon to avoid nocturnal insomnia.
- Hidden sources of caffeine, such as certain analgesics, chocolate, and decaffeinated coffee, can also contribute to sleep disturbances.
A nurse is creating a staff education program on sedative-hypnotics. The nurse should be aware of which of the following considerations?
Explanation
Sedative-hypnotics are pharmacological agents that depress central nervous system activity to reduce sleep latency and improve sleep maintenance. These medications primarily modulate the gamma-aminobutyric acid (GABA) receptor complex to induce sedation. However, the brain rapidly develops pharmacological tolerance, where the neural receptors become less responsive to the drug over a short period. This leads to a significant loss of therapeutic efficacy and increases the risk of dose escalation and subsequent physical dependence or rebound insomnia.
Rationale for correct answer
2. Most sedative-hypnotic medications lose their effectiveness after several weeks of consecutive nightly use. The body’s homeostatic mechanisms adapt to the presence of the drug, leading to receptor down-regulation. Consequently, the medication no longer provides the same sedative benefit, and the patient may experience refractory insomnia if they do not rotate or discontinue the pharmacological therapy.
Rationale for incorrect answers
1. Taking sedative-hypnotics with alcohol is strictly contraindicated due to the risk of synergistic depression of the central nervous system. This combination can lead to fatal respiratory depression, profound hypotension, and coma. The nurse must educate the staff and patients that alcohol significantly increases the toxicity and lethality risk of these medications.
3. These medications should not be given at intervals during the night because their prolonged half-life would result in significant morning grogginess and impaired motor function. Administering a dose late in the night increases the risk of daytime sedation, falls, and cognitive clouding. They are intended for a single dose at the initial bedtime only.
4. Combining sedatives with daytime amphetamines creates a dangerous cycle of chemical stimulants and depressants that destabilizes the autonomic nervous system. This “upper-downer” cycle prevents the establishment of a natural sleep architecture and can lead to severe cardiovascular stress. The goal of nursing care is to promote sleep hygiene rather than managing side effects with more drugs.
Test-taking strategy
- Identify tolerance: Recognize that the primary clinical limitation of hypnotics is the rapid development of tolerance, usually within 2 to 4 weeks.
- Safety red flags: Immediately rule out any option that suggests mixing CNS depressants with alcohol (Choice 1), as this is a fundamental safety violation.
- Assess pharmacokinetics: Understand that the duration of action for sleep meds requires a full night's rest; interval dosing (Choice 3) causes daytime impairment.
- Avoid polypharmacy: Reject interventions that use one high-risk drug (amphetamines) to treat the side effects of another (sedatives) unless clinically indicated for specific disorders like narcolepsy.
- Clinical sustainability: Choose the option that reflects the long-term reality of drug therapy: decreased effectiveness over time.
Take home points
- Non-benzodiazepine “Z-drugs” (like zolpidem) were designed to have fewer side effects but still carry significant risks for sleep-walking and dependence.
- Rebound insomnia occurs when these medications are stopped abruptly, often resulting in sleep that is worse than before the treatment started.
- Sedative-hypnotics should be limited to the lowest effective dose for the shortest possible duration, typically not exceeding 7 to 14 days.
A nurse is developing a plan for a client who was diagnosed with narcolepsy. Which interventions should the nurse include in the plan? Select all that apply
Explanation
Narcolepsy is a neurological syndrome characterized by a deficiency in hypocretin-producing neurons, leading to impaired regulation of sleep-wake boundaries. Patients suffer from cataplexy, sleep paralysis, and hypnagogic hallucinations as REM sleep components intrude into wakefulness. Management requires a multi-modal approach combining behavioral conditioning with pharmacological support to improve daytime alertness and stabilize nocturnal rest. Promoting safety is the primary nursing objective, as sleep attacks can occur without warning during high-risk activities.
Rationale for correct answers
1. Scheduled brief naps of 15 to 20 minutes can significantly reduce daytime sleepiness and the frequency of unintended sleep attacks. These naps provide a temporary refractory period against the irresistible urge to sleep, allowing the college student or worker to maintain better focus. Limiting the duration prevents sleep inertia and interference with nocturnal sleep consolidation.
4. A regular exercise program helps stabilize the circadian rhythm and promotes a more consolidated nocturnal sleep period. Physical activity increases metabolic alertness during the day and can help mitigate the weight gain often associated with narcolepsy. It serves as a non-pharmacological adjunct to improve the overall circadian health of the patient.
5. Modafinil is a first-line wake-promoting agent used to treat the excessive daytime sleepiness of narcolepsy. The nurse must educate the client about side effects like headache, nausea, and the rare but serious Stevens-Johnson syndrome. Understanding the medication's profile ensures patient compliance and the early detection of adverse pharmacological reactions.
Rationale for incorrect answers
2. Alcohol is a REM suppressant and a central nervous system depressant that can worsen the symptoms of narcolepsy. It increases the likelihood of sleep fragmentation and can trigger or exacerbate the daytime drowsiness the patient is trying to avoid. Alcohol use should be minimized or eliminated to maintain a stable neurochemical environment.
3. Large meals, particularly those high in carbohydrates, can induce postprandial somnolence and trigger sleep attacks in narcoleptic patients. It is more appropriate to recommend small, frequent meals throughout the day to keep blood sugar levels stable and minimize lethargy. A heavy lunch would significantly impair the client's ability to remain awake and alert in the afternoon.
Test-taking strategy
- Identify selective targets: In SATAs focus on interventions that promote alertness (naps, exercise, meds) and avoid those that induce drowsiness (alcohol, large meals).
- Nap duration: Remember that for narcolepsy, naps must be short (Choice 1) to be therapeutic; long naps disrupt the already fragile sleep-wake cycle.
- Pharmacology focus: Always include patient education on newly prescribed medications (Choice 5) like modafinil or armodafinil.
- Circadian stabilization: Recognize that exercise (Choice 4) is a universal tool for stabilizing biological rhythms across most sleep disorders.
- Rule out depressants: Exclude any substance that depresses the CNS, such as wine (Choice 2), when the goal is to increase wakefulness.
Take home points
- Patients with narcolepsy should avoid jobs that require long-distance driving or the operation of heavy, dangerous machinery.
- The tetrad of narcolepsy includes excessive daytime sleepiness, cataplexy, sleep paralysis, and hypnagogic hallucinations.
The nurse recognizes that which statements made by a client indicate an understanding of behaviors that will promote sleep? Select all that apply
Explanation
Sleep hygiene encompasses a suite of behavioral and environmental modifications designed to strengthen the circadian drive and reduce nocturnal arousal. The brain utilizes environmental cues to regulate the secretion of endogenous melatonin and synchronize the internal biological clock. Maintaining a clear distinction between the sleep environment and stimulating activities prevents the development of conditioned insomnia, where the bed becomes associated with wakefulness. Consistent implementation of these habits improves sleep efficiency and facilitates more rapid transitions into the deeper, restorative stages of NREM sleep.
Rationale for correct answers
1. Utilizing the bed only for sleep and intimacy is a core principle of stimulus control therapy. Avoiding television in bed prevents blue light exposure, which suppresses melatonin, and eliminates cognitive stimulation that keeps the brain in an alert state. This behavior helps re-establish the bed as a monotropic cue for sleep.
2. Caffeine is a methylxanthine that blocks adenosine receptors, effectively masking the physiological drive to sleep for several hours. Avoiding caffeine in the afternoon and evening ensures that the drug's pharmacokinetic half-life does not interfere with sleep onset. This action allows the natural accumulation of sleep pressure throughout the day.
5. Engaging in regular exercise during daylight hours is clinically proven to improve sleep quality by increasing the duration of deep NREM sleep. Physical activity helps regulate the body temperature cycle, with the subsequent post-exercise cooling facilitating easier sleep initiation. It also serves as a healthy outlet for psychological stress that might otherwise cause nocturnal rumination.
Rationale for incorrect answers
3. Napping late in the evening significantly reduces the homeostatic sleep drive, making it much more difficult to fall asleep at the scheduled bedtime. This “sleep snacking” fragments the nocturnal period and can lead to sleep-onset insomnia. Naps should be restricted to the early afternoon and limited to 20 minutes to avoid interfering with night rest.
4. Consuming a large meal close to bedtime increases metabolic activity and can cause gastrointestinal distress or acid reflux. The digestive process raises the core body temperature, which is the physiological opposite of the cooling required for sleep. Eating dinner at least 3 hours before retiring is the recommended standard for optimal sleep hygiene.
Test-taking strategy
- Stimulus control: Identify “watching TV in bed” as a primary disruptor of the mental association between the bed and sleep.
- Chemical interference: Recognize that caffeine (Choice 2) is a long-acting stimulant that must be restricted well before the desired sleep time.
- Physiological needs: Associate exercise (Choice 5) with improved sleep quality, provided it is not performed in the immediate pre-sleep period.
- Rule of thermodynamics: Eliminate Choice 4 because digestion generates heat, and sleep requires a drop in body temperature.
- Homeostatic drive: Understand that late naps (Choice 3) “drain the battery” of sleepiness needed for a consolidated night of rest.
Take home points
- The bedroom should be kept cool, dark, and quiet to provide an optimal environment for the maintenance of sleep continuity.
- A consistent wake-up time, even on weekends, is more important for circadian stability than a consistent bedtime.
A 72-year-old client asks the nurse about using an over-the-counter antihistamine as a sleeping pill to help her get to sleep. What is the nurse’s best response?
Explanation
The geriatric population is highly susceptible to the anticholinergic effects of first-generation antihistamines, such as diphenhydramine. These medications cross the blood-brain barrier and exert significant central nervous system depression, which is prolonged in the elderly due to reduced renal and hepatic clearance. In addition to sedation, these agents cause blurred vision, urinary retention, and orthostatic hypotension. The Beers Criteria specifically identifies these drugs as potentially inappropriate medications for older adults due to the disproportionate risk of adverse events compared to their therapeutic benefit.
Rationale for correct answer
2. Antihistamines are contraindicated for sleep in the elderly because they frequently cause cognitive impairment and delirium. The sedative effect combined with potential dizziness significantly increases the incidence of falls and related fractures in the 70s age group. The nurse must prioritize patient safety by discouraging the use of these agents in favor of non-pharmacological interventions.
Rationale for incorrect answers
1. Stating that antihistamines are “better than prescription medications” is factually incorrect and potentially dangerous. While some prescriptions have risks, first-generation antihistamines often have a more hazardous side-effect profile in the elderly than modern, low-dose sleep aids. This response fails to address the specific physiological risks associated with over-the-counter sedative use.
3. Claiming that antihistamines do not have many side effects is a significant clinical error and provides the client with false information. In the elderly, these drugs are notorious for causing dry mouth, constipation, and hangover effects the following morning. The nurse has a professional obligation to disclose the multisystemic risks these drugs pose to geriatric patients.
4. While sleep hygiene is always a good plan, combining it with antihistamines in an older adult is inappropriate advice. The risk of paradoxical excitation or severe confusion outweighs the benefit of using an over-the-counter sleep aid. The nurse should recommend behavioral strategies alone or a formal evaluation by a primary care provider before any drug use.
Test-taking strategy
- Geriatric safety: In older adults, always prioritize the risk of falls and confusion over the need for pharmacological sleep induction.
- Beers criteria knowledge: Recall that diphenhydramine and other anticholinergics are listed as high-risk medications for the elderly.
- Identify side effects: Look for the answer that accurately describes the systemic impact: “confusion” and “risk of falls” are classic antihistamine sequelae in seniors.
- Rule out misinformation: Eliminate options that downplay drug risks (Choice 3) or make broad, unscientific comparisons (Choice 1).
- Scope of nursing: The nurse's role is to educate on the dangers of self-medication with high-risk over-the-counter substances.
Take home points
- First-generation antihistamines have a long half-life in older adults, often leading to daytime somnolence and increased accident risk.
- Anticholinergic toxicity in the elderly can manifest as acute confusion, often mistaken for early-onset dementia or worsening cognitive decline.
A registered nurse is caring for a client with insomnia. Which sleep-hygiene actions at bedtime can the nurse delegate to assistive personnel? Select all that apply
Explanation
Delegation in the clinical setting requires the registered nurse to assign tasks based on the scope of practice and the stability of the client. Assistive personnel can perform non-invasive, routine comfort measures that support the nursing care plan but do not require clinical judgment or complex assessment. Providing a therapeutic environment through sensory modification is a key component of environmental sleep hygiene that can be safely managed by unlicensed staff. Effective delegation allows the nurse to focus on pharmacological management and the evaluation of complex patient responses.
Rationale for correct answers
1. Providing a back rub is a basic comfort measure that promotes physical relaxation and reduces muscle tension. This task does not require clinical reasoning and is well within the training of assistive personnel to assist with sleep induction. It serves as a non-pharmacological intervention to decrease the client's sympathetic nervous system activity before rest.
2. Facilitating a quiet environment by turning on music (as specified in the care plan) is a technical task that can be delegated. Assistive personnel can ensure the volume and type of music align with the client's preferences and the nurse's instructions. This helps establish a consistent routine without necessitating the direct presence of the registered nurse.
3. Dimming the lights is a fundamental environmental modification that supports the natural production of endogenous melatonin. This simple action helps synchronize the client's circadian rhythm with the desired sleep time. It is a predictable task that assistive personnel can perform as part of the standard evening “wind-down” procedures.
Rationale for incorrect answers
4. Providing a cup of coffee at bedtime is contraindicated because caffeine is a central nervous system stimulant that prevents sleep. Even if the client requests it, the nurse must ensure that detrimental substances are not provided. This is a matter of clinical safety and professional judgment that should not be delegated or encouraged.
5. Monitoring for the therapeutic effect or adverse reactions of a medication is a core component of the nursing process. This requires advanced assessment skills and the ability to interpret physiological data, which cannot be delegated to assistive personnel. The registered nurse remains legally responsible for evaluating the client's response to any pharmacological intervention.
Test-taking strategy
- Delegation principles: Use the five rights of delegation; tasks that are routine, non-invasive, and require no assessment are delegable.
- Scope of practice: Remember that Unlicensed Assistive Personnel (UAP) cannot “E-A-T”: Evaluate, Assess, or Teach.
- Identify contraindications: Rule out Choice 4 immediately as it violates basic sleep hygiene and safety principles for a client with insomnia.
- Focus on comfort: Prioritize physical and environmental tasks (Choices 1, 2, and 3) as the most appropriate for delegation.
- Critical thinking: Recognize that monitoring medication effect (Choice 5) is a high-level evaluative task reserved for licensed nursing staff.
Take home points
- Delegation must be based on the specific job description of the assistive personnel and the facility's policy.
- The nurse must always follow up with the assistive personnel to ensure the delegated tasks were completed and the client is comfortable.
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Explain the physiology and the functions of sleep.
- Identify the characteristics of the NREM and REM sleep states.
- Describe variations in sleep patterns throughout the life span.
- Identify factors that affect sleep.
- Describe common sleep disorders.
- Identify the components of a sleep pattern assessment.
- Develop nursing diagnoses, outcomes, and nursing interventions related to sleep problems.
- Describe interventions that promote sleep.
Introduction
Sleep is a basic human need; it is a universal biologic process common to all people. Humans spend about one third of their lives asleep. We require sleep for many reasons: to cope with daily stresses, to prevent fatigue, to conserve energy, to restore the mind and body, and to enjoy life more fully. Sleep enhances daytime functioning, and is vital for cognitive, physiological, and psychosocial function.
Furthermore, many members of the general public and health professionals are unaware of the consequences of chronic sleep loss (e.g., increased risk of hypertension, diabetes, obesity, depression, heart attack, and stroke).
Physiology Of Sleep
Historically viewed as a state of unconsciousness, sleep is now defined as an altered state of consciousness characterized by:
- Decreased perception of and reaction to the environment.
- Minimal physical activity and variable levels of consciousness.
- Selective responsiveness to meaningful external stimuli (e.g., a mother reacting to her infant's cry while ignoring other sounds).
- Integration of sensory information by the reticular formation (RF) located in the brainstem.
Neurochemical and hormonal regulation
The Sleep/Wake cycle is regulated by the Reticular Activating System (RAS) and specific neurotransmitters.
Wakefulness-Promoting Factors
- Reticular Activating System (RAS): A network of ascending nerve fibers in the brainstem that maintains cerebral cortical arousal.
- Acetylcholine: Released in the reticular formation; levels peak during REM sleep and wakefulness.
- Dopamine: Released in the midbrain to support cortical activation.
- Noradrenaline: Released in the pons to influence arousal.
- Cortisol: Reaches highest levels at daylight to promote alertness.
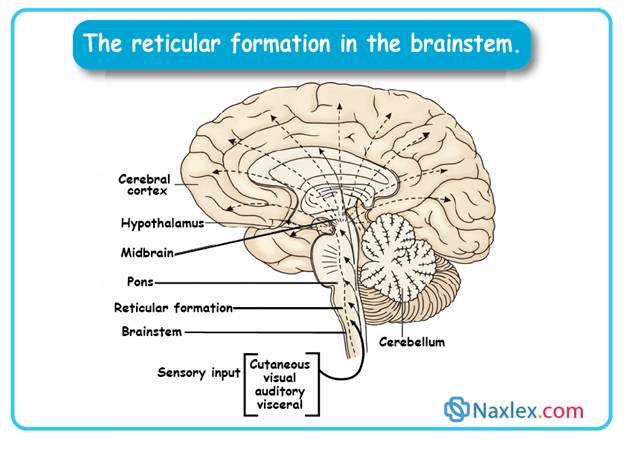
Sleep-Promoting Factors
- Serotonin: Lessens the response to sensory stimulation.
- Gamma-aminobutyric acid (GABA): Inhibits neurons within the RAS to “shut off” activity.
- Melatonin: Secreted by the pineal gland in response to darkness; induces drowsiness.
- Growth Hormone: Secreted during deep sleep stages for tissue repair and protein synthesis.
Circadian Rhythms
- Definition: A 24-hour internal biologic clock (Latin: circa dies, “about a day”).
- Synchronization: Controlled endogenously but synchronized by exogenous “zeitgebers” like light and darkness.
- Physiological Indicators: Core body temperature and blood pressure follow circadian patterns.
- Development: Regularity begins at 6 weeks of age; established by 3 to 6 months in infants.
- Circadian Synchronization: Occurs when the sleep/wake cycle aligns with the body temperature rhythm (awake when temp is highest, asleep when temp is lowest).
NREM (Non-Rapid Eye Movement) Sleep
NREM accounts for 75% to 80% of total sleep time. It is divided into 3 distinct stages:
- Stage 1: Very light sleep lasting several minutes. Characterized by drowsiness, side-to-side eye rolling, and slight decreases in heart and respiratory rates. Low-voltage brain waves are present.
- Stage 2: Deeper than stage 1; requires more intense stimuli (touching/shaking) to awaken. Body temperature falls, and eyes remain still.
- Stage 3: Deep sleep or “Delta sleep.” Heart and respiratory rates drop 20% to 30% below waking baseline. Skeletal muscles are highly relaxed, reflexes are diminished, and snoring is common. This stage is essential for energy restoration and growth hormone release.
REM (Rapid Eye Movement) Sleep
Also known as “Paradoxical Sleep” because the EEG resembles a wakeful state.
- Occurrence: Recurs approximately every 90 minutes; lasts 5 to 30 minutes.
- Physiology: Brain metabolism increases by up to 20%. High levels of acetylcholine and dopamine.
- Characteristics: Distinctive rapid eye movements, dramatic decrease in voluntary muscle tone (muscle atonia), and absent deep tendon reflexes.
- Function: Associated with dreaming and the stimulation of brain regions used for learning, thinking, and organizing information.
Sleep cycles and architecture
Adults typically experience 4 to 6 cycles during 7 to 8 hours of sleep.
- Cycle Duration: 90 to 110 minutes.
- Progression: Stage 1 NREM > Stage 2 NREM > Stage 3 NREM > Stage 2 NREM > Stage 1 NREM > REM.
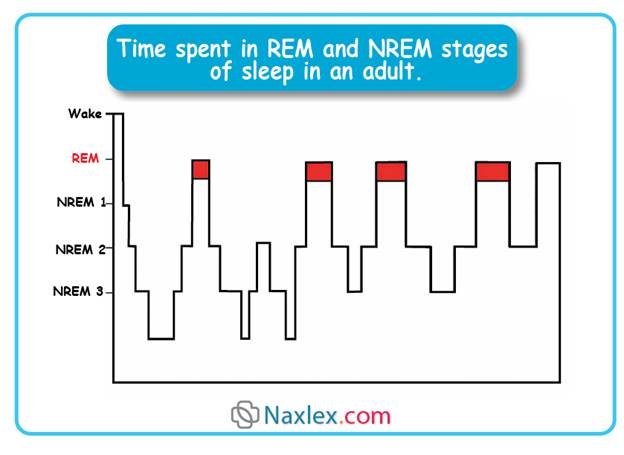
- Temporal Shifts: Stage 3 (deep sleep) periods are longer in the first half of the night. REM periods lengthen as the night progresses.
- Interruption: If awakened, the sleeper must restart at Stage 1 NREM.
Clinical Significance of sleep
- Energy Restoration: Necessary for protein synthesis and cellular repair.
- Psychological Health: Sleep loss leads to emotional irritability, poor concentration, and impaired decision-making.
- Clinical Alert: Sleep deprivation in clinical settings contributes to:
- Immunosuppression and inflammation.
- Alterations in sympathetic/parasympathetic equilibrium.
- Increased insulin resistance.
- Heightened anxiety and fear.
3.1 NORMAL SLEEP PATTERNS AND REQUIREMENTS
1. Developmental Requirements and Patterns
Newborns (0 to 2 Months)
- Duration: 12 to 18 hours per day on an irregular schedule.
- Sleep Architecture: 50% NREM (Quiet Sleep) and 50% REM (Active Sleep).
- Characteristics: Enter REM sleep immediately. Sleep cycles are approximately 50 minutes.
- Clinical Note: Exposure to light and play during the day helps establish circadian rhythms.
Infants (3 Months to 1 Year)
- Duration: 9 to 12 hours per 24-hour period by 1 year.
- Pattern: Wake every 3 to 4 hours to eat; by 6 months, most sleep through the night (12 am to 5 am).
- Sleep Architecture: 50% is light sleep with significant vocalization and movement.
- Self-Soothing: Putting infants to bed while drowsy (not asleep) prevents them from becoming “signalers” who require parental intervention to return to sleep.
Toddlers (1 to 3 Years)
- Duration: 12 to 14 hours recommended.
- Pattern: Transition from two naps to one afternoon nap.
- Characteristics: Common resistance to bedtime and nighttime fears/nightmares.
- Intervention: Consistent routines and security objects (blankets/toys) provide comfort.
Preschoolers (3 to 5 Years)
- Duration: 11 to 13 hours.
- Characteristics: Sleep needs fluctuate with growth spurts. Bedtime resistance remains common.
- Night Terrors: Preschoolers may experience night terrors or nightmares. Limiting television exposure is recommended to reduce these occurrences.
School-Age Children (5 to 12 Years)
- Duration: 10 to 11 hours.
- Challenges: Increased homework, sports, and screen time (computers/TV) reduce total sleep.
- Clinical Alert: Presence of a TV or computer in the bedroom is directly correlated with decreased sleep duration.
Adolescents (12 to 18 Years)
- Duration: 9 to 10 hours required; rarely achieved.
- Biological Shift: Circadian rhythms shift naturally toward later sleep and wake times (Delayed Sleep Phase).
- Environmental Triggers: Blue-spectrum light from electronics (phones/Internet) inhibits sleep onset.
- Clinical Manifestations: Sleep deprivation correlates with lower grades, negative moods, and 16.5% higher motor vehicle crash rates.
- Development: Males may experience nocturnal emissions (normal physiological event).
Adults
- Duration: 7 to 8 hours is standard, though range is 6 to 10 hours.
- Vulnerable Groups: Students, shift workers, travelers, and those with chronic pain or stress.
- Gender Factors: Pregnancy, menses, and perimenopause significantly alter sleep architecture.
- Indicators of Deprivation: Drowsiness during non-fatiguing tasks, irritability, and impaired short-term memory.
Older Adults (65+ Years)
- Duration: Sleep need does not decrease, but the ability to maintain sleep diminishes.
- Advanced Sleep Phase Syndrome: Tendency to retire 1 hour earlier and wake 1.3 hours earlier than younger adults.
- Sleep Architecture: Diminished REM sleep and more frequent nocturnal awakenings (average 6 times per night).
- Clinical Conditions:
- Flattened circadian rhythm.
- Sundown Syndrome: Agitation, anxiety, and aggression in the late afternoon/night, often associated with dementia.
2. General Principles of Sleep Management
- Clinical Importance: Sleep deprivation causes significant cognitive impairment and systemic health problems.
- Hospitalization: Reestablishing sleep/wake rhythms post-surgery is critical; daytime napping should be encouraged in hospitalized clients to offset nocturnal disruptions.
- Hygiene: Regular, consistent bedtime routines are the primary intervention across all age groups to promote sleep efficacy.
3.2 FACTORS AFFECTING SLEEP
1. Physiological and medical factors
Both the quality (subjective energy level upon awakening) and quantity (total sleep time) are influenced by health status.
Impact of Illness
- Respiratory conditions: Dyspnea (shortness of breath), nasal congestion, and sinus drainage impede sleep onset.
- Gastrointestinal disorders: Gastric and duodenal ulcers cause pain during REM sleep due to increased gastric acid secretions.
- Endocrine disturbances:
- Hyperthyroidism: Increases sleep latency (time taken to fall asleep).
- Hypothyroidism: Decreases Stage 3 (deep) sleep.
- Estrogen deficiency: Low levels lead to excessive fatigue and sleep fragmentation via vasomotor symptoms (hot flashes/night sweats).
- Thermoregulation: Pyrexia (elevated body temperature) reduces delta sleep and REM sleep.
- Nocturia: The need to urinate during the night disrupts sleep cycles.
REM rebound
- Individuals deprived of REM sleep (due to alcohol, medications, or illness) will subsequently spend a disproportionately high amount of time in the REM stage to compensate.
2. Lifespan considerations and clinical pathologies
Pediatric sleep disturbances
- Trained Night Feeder: Infants >4 months of age do not physiologically require nocturnal feedings. Expectations for mid-night feedings are learned behaviors.
- Sleep Refusal: Common in toddlers; triggered by separation anxiety, stress, or inconsistent routines.
- Night Terrors (Pavor Nocturnus): Partial awakenings from NREM Stage 3 sleep (usually ages 3 to 6). Characterized by screaming and thrashing. Unlike nightmares, there is no memory of the event, and it occurs in deep sleep rather than REM.
Adult and geriatric challenges
- Middle-aged adults: Sleep often disrupted by caregiver strain (caring for elderly parents or ill partners).
- Older Adults: Diminished sleep quality due to:
- Side effects of polypharmacy.
- Gastroesophageal Reflux Disease (GERD).
- Pain from osteoarthritis and impaired mobility.
- Delirium and Dementia (e.g., Sundown Syndrome).
3. Psychosocial and lifestyle factors
Emotional Stress
- Greatest cause of insomnia. Stress activates the Hypothalamic-Pituitary-Adrenal (HPA) axis.
- Anxiety increases circulating norepinephrine via sympathetic nervous system stimulation, leading to frequent awakenings and reduced REM/deep sleep.
Environmental Influences
- Habituation: Absence of usual stimuli or presence of unfamiliar noise (especially in hospitals) inhibits relaxation.
- Temperature and Ventilation: Extreme heat or cold and poor air quality reduce sleep efficacy.
Lifestyle and Motivation
- Shift Work: Night workers face conflicts with rising body temperatures in the morning. Using dark wrap-around sunglasses and light-blocking shades can mitigate the alerting effects of daylight.
- Exercise: Moderate exercise early in the day promotes sleep, but late-day vigorous activity delays sleep onset.
- Diet: Weight gain is associated with sleep fragmentation. L-tryptophan (found in milk and cheese) serves as a precursor for sleep-inducing neurotransmitters.
4. Chemical stimulants and substance use
- Caffeine: CNS stimulant that interferes with sleep when consumed in the afternoon or evening.
- Alcohol: While it may hasten sleep onset, it severely disrupts REM sleep and leads to REM rebound (nightmares) as it is metabolized.
- Nicotine: A stimulant; smokers are typically “light sleepers” and experience more difficulty falling asleep than nonsmokers.
5. Pharmacological impact on sleep architecture
- Hypnotics: Interfere with deep sleep stages and suppress REM sleep.
- Beta-Blockers: Known to cause insomnia and vivid nightmares.
- Narcotics (e.g., Morphine): Suppress REM sleep; cause drowsiness but frequent awakenings.
- Antidepressants: Suppress REM sleep (therapeutic for mood but results in REM rebound upon discontinuation).
- Tranquilizers: Directly interfere with REM sleep.
Common Sleep Disorders
A comprehensive understanding of sleep pathology allows nursing professionals to evaluate clinical complaints and facilitate referrals to sleep medicine specialists. While research typically categorizes these conditions as dyssomnias, parasomnias, and secondary sleep disorders, clinical practice prioritizes symptomatic presentation, including insomnia, hypersomnolence, and parasomnias.
5.1 INSOMNIA
Insomnia is the pathological inability to initiate or maintain sleep, resulting in non-restorative rest. It represents the most prevalent sleep-related complaint in the United States.
- Acute insomnia: Transient episodes lasting 1 to several nights, frequently precipitated by psychological stressors.
- Chronic insomnia: Symptoms persisting for > 1 month.
- Chronic-intermittent insomnia: A cyclical pattern of sleep disturbance followed by brief periods of adequate sleep.
Clinical manifestations
- Insomnia
- Difficulty falling asleep
- Waking up frequently during the night
- Difficulty returning to sleep
- Waking up too early in the morning
- Unrefreshing sleep
- Daytime sleepiness
- Difficulty concentrating
- Irritability
Risk Factors and Pathophysiology
Primary risk factors include advanced age and female gender. In women, sleep architecture is often disrupted by hormonal fluctuations associated with menstruation, gestation, and menopause. In geriatric populations, increased incidence is frequently secondary to comorbid medical conditions.
Therapeutic Interventions
Management emphasizes behavioral modification:
- Stimulus Control: Optimizing the sleep environment to strengthen the association between the bed and sleep.
- Cognitive Therapy: Restructuring maladaptive beliefs regarding sleep.
- Sleep Restriction: Limiting nocturnal time in bed to increase sleep efficiency.
Pharmacological Considerations
The efficacy of long-term sedative-hypnotics is clinically debated due to potential for physiological dependence and failure to address etiology. Antihistamines, such as diphenhydramine, present significant risks—particularly in geriatric clients—due to anticholinergic (atropine-like) effects, vertigo, and orthostatic hypotension. These agents are contraindicated in patients with asthma, glaucoma (increased intraocular pressure), hyperthyroidism, or cardiovascular hypertension.
5.2 EXCESSIVE DAYTIME SLEEPINESS (EDS)
EDS arises from hypersomnia, narcolepsy, sleep apnea, or chronic sleep deprivation.
Hypersomnia
Characterized by achieving sufficient nocturnal sleep durations yet failing to maintain daytime wakefulness. Etiologies include Central Nervous System (CNS) trauma, metabolic acidosis, uremia, or hepatic dysfunction.
Narcolepsy
A neurological disorder stemming from a deficiency in hypocretin (orexin) within the CNS.
- Clinical Markers: Excessive daytime somnolence and sleep-onset REM periods (SOREMPs) occurring within 15 minutes of sleep onset.
- Tetrad of Symptoms: Cataplexy (sudden bilateral loss of muscle tone triggered by emotion), sleep paralysis, hypnagogic hallucinations, and fragmented nocturnal sleep.
- Treatment: Management includes CNS stimulants (methylphenidate, amphetamines) and cerebral cortex stimulants (xanthines/caffeine). Cataplexy is managed with MAOIs, SSRIs, or Sodium Oxybate. Modafinil is utilized for its mood-altering and wake-promoting effects with lower abuse potential.
Sleep Apnea
Characterized by repetitive cessation of respiration during sleep. Clinical abnormality is defined as > 5 apneic episodes per hour, with each pause lasting > 10 seconds.
- Obstructive sleep apnea (OSA): Physical occlusion of the pharynx or oropharynx. Predisposing factors include obesity, tonsillar hypertrophy, and deviated nasal septum.
- Central sleep apnea: A neurological deficit in the respiratory drive center; common in brainstem injury or muscular dystrophy.
- Mixed apnea: A combination of obstructive and central components.
- Complications: Untreated apnea may lead to pulmonary hypertension, cardiac arrhythmias, and right-sided or left-sided heart failure. Management includes CPAP therapy or surgical intervention (e.g., UPPP).
INSUFFICIENT SLEEP
Voluntary or unintentional sleep deprivation leads to significant cognitive and physiological impairments.
- Physiological impact: Wakefulness for 19 consecutive hours produces cognitive deficits equivalent to a Blood Alcohol Concentration (BAC) of 0.05. Wakefulness for 24 hours equates to a BAC of 0.10.
- Clinical manifestations: Reduced vigilance, distractibility, diplopia, and increased risk of medical errors among healthcare providers.
5.3 PARASOMNIAS
Parasomnias are abnormal behavioral, experiential, or physiological events occurring in association with sleep or sleep-stage transitions.
- NREM Parasomnias: Includes somnambulism (sleepwalking) and sleep terrors.
- REM Parasomnias: Includes nightmare disorder and REM sleep behavior disorder.
- Miscellaneous Parasomnias: Includes nocturnal enuresis and sleep-related hallucinations, often secondary to substance use or medical comorbidities.
Bruxism: Usually occurring during stage 2 NREM sleep, this clenching and grinding of the teeth can eventually erode dental crowns, cause teeth to come loose, and lead to deterioration of the temporomandibular (TMJ) joint, called TMJ syndrome.
Enuresis: Bed-wetting during sleep can occur in children over 3 years old. More males than females are affected. It often occurs 1 to 2 hours after falling asleep, when rousing from NREM stage 3.
Periodic limb movement disorder (PLMD): In this condition, the legs jerk twice or three times per minute during sleep. It is most common among older adults. This kicking motion can wake the client and result in poor sleep. PLMD differs from restless leg syndrome (RLS), which occurs whenever the person is at rest, not just at night when sleeping. RLS may occur during pregnancy or be due to other medical problems that can be treated. Many clients with PLMD or RLS respond well to medications such as levodopa, pramipexole, ropinirole, and gabapentin.
Sleeptalking: Talking during sleep occurs during NREM sleep before REM sleep. It rarely presents a problem to the person unless it becomes troublesome to others.
Sleepwalking: Sleepwalking (somnambulism) occurs during stage 3 of NREM sleep. It is episodic and usually occurs 1 to 2 hours after falling asleep. Sleepwalkers tend not to notice dangers (e.g., stairs) and often need to be protected
Nursing Management Of Sleep Disorders
7.1. NURSING ASSESSMENT
A comprehensive evaluation involves subjective data collection and objective clinical findings.
1. Sleep History
Obtain for all non-critically ill admissions. Key assessment parameters include:
- Usual sleep-wake cycle and diurnal nap patterns.
- Nocturnal symptoms: Loud snoring (suggestive of Obstructive Sleep Apnea), excessive motor activity (thrashing), or nocturnal enuresis.
- Daytime impact: Excessive daytime sleepiness (EDS) during sedentary or critical tasks (e.g., driving).
- Pharmacological history: Use of prescription hypnotics, CNS stimulants, OTC antihistamines, or herbal supplements (e.g., guarana).
2. Physical examination Focus on indicators of sleep-disordered breathing:
- Obesity (Body Mass Index assessment).
- Pharyngeal findings: Enlarged/reddened uvula and soft palate, hypertrophic tonsils or adenoids.
- Anatomical markers: Male neck circumference > 17.5 inches; deviated nasal septum.
3. Diagnostic tools
- Sleep diary: Conducted for 1 to 2 weeks to track caffeine/alcohol intake, bedtime rituals, and exact sleep-wake timings.
- Polysomnography (Sleep Study): Simultaneous recording of EEG (brain waves), EOG (eye movements), and EMG (muscle tension). Monitors respiratory effort, ECG, leg movements, and SpO2 via pulse oximetry.
7.2. NANDA NURSING DIAGNOSES
- Insomnia: Related to sensory overstimulation or circadian rhythm disruption.
- Risk for Injury: Related to somnambulism (sleepwalking).
- Impaired Gas Exchange: Related to alveolar hypoventilation in sleep apnea.
- Fatigue: Related to non-restorative sleep or insufficient sleep duration.
7.3. NURSING INTERVENTIONS & IMPLEMENTATION
1. Sleep hygiene education
- Maintain a consistent sleep-wake schedule 7 days a week.
- Restrict daytime naps to 15 to 30 minutes (geriatric clients only; avoid in younger insomniacs).
- Exercise daily but avoid vigorous exertion < 3 hours before sleep.
- Stimulus Control: Utilize the bed strictly for sleep and sexual activity.
2. Environmental & Dietary management
- Environment: Maintain a cool, dark, and quiet room. Use “white noise” rather than music.
- Diet: Avoid heavy/spicy meals 2 to 3 hours before bedtime. Restrict alcohol and caffeine ≥ 4 hours before sleep.
- Nocturnal Habits: If unable to sleep, leave the bedroom and engage in a low-stimulus activity until drowsy.
3. Clinical/Hospital environment modification
- Minimize light: Close curtains, use night-lights, and employ flashlights for drainage checks.
- Noise Reduction: Conduct shift reports away from patient rooms; wear rubber-soled shoes; oil equipment wheels; decrease paging system volume after 2100 hours.
- Cluster Care: Schedule nursing interventions to allow for uninterrupted 90-minute sleep cycles.
4. Pharmacological management of sleep
I. Classification and mechanisms
Pharmacological interventions for sleep disorders primarily utilize two classes of drugs, often prescribed on a pro re nata (PRN) basis:
- Sedative-Hypnotics: Induce sleep by producing generalized Central Nervous System (CNS) depression.
- Antianxiety Agents (Anxiolytics): Reduce cortical arousal by facilitating inhibitory neurotransmitters that suppress responsiveness to external stimuli.
Ii. Clinical considerations and pharmacokinetics
- Sleep architecture: Most sedative-hypnotics alter the NREM/REM cycle, potentially reducing REM sleep. Newer agents, such as zolpidem, are noted for maintaining REM integrity.
- Half-Life and Metabolism: The half-life (t1/2) determines the duration of action and risk of residual effects.
- Short t1/2 (e.g., Zaleplon, t1/2 = 1): Ideal for sleep initiation; lower risk of morning somnolence.
- Long t1/2 (e.g., Flurazepam, t1/2 = 47 to 100): Effective for sleep maintenance but increases “hangover” effects and psychomotor impairment.
- Dosage Protocols: Initiate therapy with the lowest effective dose. Geriatric clients require vigilant monitoring due to age-related metabolic changes that increase susceptibility to ataxia and cognitive impairment.
Iii. Contraindications and risk factors
- Respiratory Disorders: Contraindicated in clients with suspected sleep-disordered breathing (e.g., Sleep Apnea).
- Organ Dysfunction: Use caution or avoid in clients with hepatic or renal insufficiency.
- Maternal Health: Antianxiety medications are contraindicated in pregnancy (teratogenic risk) and lactation (excretion in breast milk).
- Dependency and Tolerance: Physiological tolerance can develop within 4 to 6 weeks. Abrupt cessation of barbiturates may precipitate severe withdrawal, including tremors, tachycardia, and seizures.
Iv. Nursing interventions and client teaching
- Safety Precautions: Caution clients regarding impaired driving or machinery operation, even if they no longer perceive drowsiness.
- REM Rebound: Inform clients that discontinuing long-term use may cause 1 to 2 nights of intense dreaming.
- Administration: Ensure patients take the medication immediately before bedtime to minimize the risk of injury during the onset of sedation.
Select sedative-hypnotics by half-life
|
Medication |
Half-Life (Hours) |
|
Zaleplon (Sonata) |
1 |
|
Melatonin |
1 |
|
Zolpidem (Ambien) |
2.5 |
|
Triazolam (Halcion) |
2 to 3 |
|
Eszopiclone (Lunesta) |
5 to 6 |
|
Chloral hydrate |
8 to 11 |
|
Temazepam (Restoril) |
8 to 24 |
|
Lorazepam (Ativan) |
10 to 20 |
|
Flurazepam (Dalmane) |
47 to 100 |
7.4. EVALUATION
Assess the efficacy of interventions based on:
- Patient-reported quality of sleep and feeling of restoration upon awakening.
- Objective observations of sleep duration and daytime alertness.
- Compliance with behavioral modifications (e.g., caffeine cessation, regular sleep schedule).
Summary
- Sleep is a naturally occurring altered state of consciousness in which a person’s perception and reaction to the environment are decreased.
- The sleep cycle is controlled by specialized areas in the brainstem and is affected by the individual’s circadian rhythm.
- NREM sleep consists of three stages, progressing from stage 1, very light sleep, to stage 3 deep sleep. NREM sleep dominates during naps and nocturnal sleep periods. NREM sleep is essential for physiological well-being.
- REM sleep recurs about every 90 minutes and is often associated with dreaming. REM sleep is essential for psychosocial and mental equilibrium.
