
Bleeding
Lessons
- Objectives
- Introduction
- Implantation Bleeding
- Practice Exercise 1
- Spontaneous Abortion (Miscarriage)
- Practice Exercise 2
- Induced Abortion
- Practice Exercise 3
- Ectopic Pregnancy
- Practice Exercise 4
- Gestational Trophoblastic Disease (Hydatidiform Mole)
- Practice Exercise 5
- Nursing Management Of Pregnancy Bleeding
- Practice Exercise 6
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
After reviewing this study guide, the learner will be able to:
- Define implantation bleeding and differentiate it from abnormal pregnancy bleeding.
- Identify the types of abortion and their pathophysiological processes.
- Recognize clinical signs and symptoms associated with each type of abortion.
- Outline nursing assessment and interventions for pregnancy bleeding emergencies.
- Describe medical and surgical management options for induced and spontaneous abortion.
- Discuss ectopic pregnancy and gestational trophoblastic disease, including risks and complications.
- Provide patient education, psychosocial support, and counseling for women experiencing pregnancy loss.
- Apply critical thinking skills to practice and comprehensive questions related to pregnancy bleeding.
Introduction
Early pregnancy bleeding occurs particularly in the first trimester and represents a common clinical challenge in maternal-newborn nursing, necessitating a thorough understanding of its etiologies, assessment strategies, and management protocols. Vaginal bleeding occurs in approximately 15-25% of early pregnancies, with causes ranging from benign implantation bleeding to life-threatening conditions such as ectopic pregnancy or gestational trophoblastic disease. Implantation bleeding results from the embryo’s attachment to the uterine endometrium, typically presenting as light spotting. In contrast, spontaneous abortion—encompassing threatened, inevitable, incomplete, complete, missed, and recurrent types—accounts for a significant proportion of early pregnancy losses, often due to chromosomal abnormalities, maternal health conditions, or uterine anomalies. Other critical causes, including ectopic pregnancy and molar pregnancy, require urgent recognition due to their potential for severe maternal complications, such as hemorrhage or malignancy. Effective nursing care hinges on accurate assessment, including detailed history-taking, physical examination, and diagnostic testing, such as transvaginal ultrasound and quantitative human chorionic gonadotropin (hCG) levels. Interventions range from expectant management for threatened abortions to medical or surgical approaches for incomplete or ectopic pregnancies, alongside psychosocial support to address emotional distress. These comprehensive notes aim to equip nursing students with the scientific knowledge and practical skills necessary to manage pregnancy bleeding, emphasizing evidence-based practice and patient-centered care. The following sections will provide an in-depth exploration of implantation bleeding, abortion types, assessment techniques, interventions, and critical nursing insights to prepare students for clinical practice and academic success.
Implantation Bleeding
1.1 Definition and Pathophysiology
- Definition:
- Implantation bleeding refers to light vaginal spotting that occurs when a fertilized ovum (blastocyst) attaches to the endometrium of the uterine wall.
- Timing:
- Usually occurs 6–12 days after fertilization, often coinciding with the time a woman expects her menses.
- Pathophysiology:
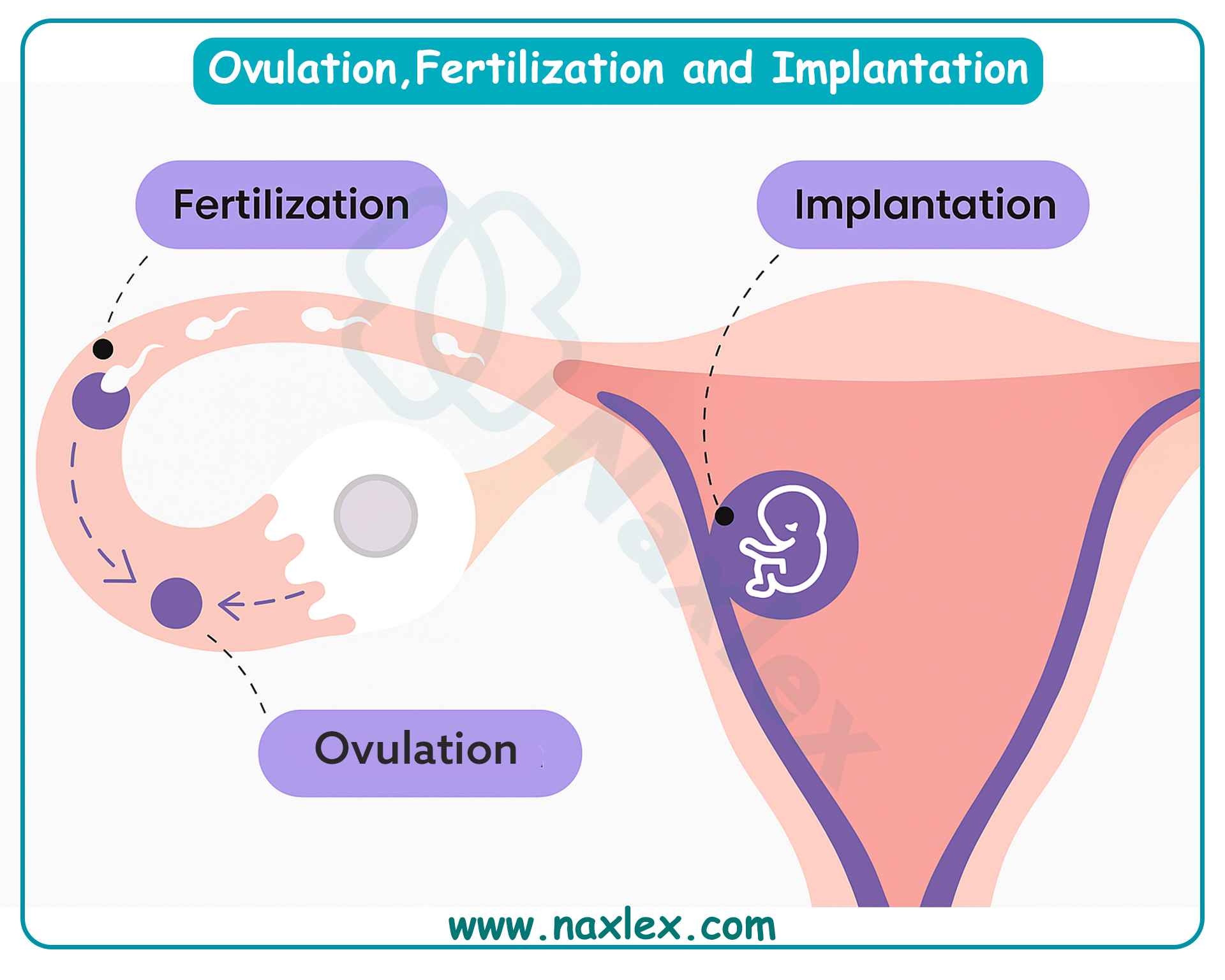
- Following fertilization, the blastocyst travels through the fallopian tube to the uterus.
- Enzymatic activity from trophoblastic cells invades the endometrial lining to establish vascular connections for nutrient exchange.
- During this invasion, small endometrial capillaries rupture, producing minimal bleeding.
- Unlike menstrual bleeding, which results from progesterone withdrawal and endometrial shedding, implantation bleeding is a localized vascular disruption.
Nursing Insights:
- Implantation bleeding is scant, self-limiting, and painless, unlike abnormal pregnancy bleeding.
- Many patients confuse it with early miscarriage or light menses. Nurses must carefully differentiate implantation spotting from pathological bleeding.
- Misinterpretation may lead to unnecessary anxiety or delayed prenatal care.
1.2 Clinical Presentation and Differentiation from Pathological Bleeding
- Typical clinical features:
- Light spotting, usually pink or brown in color.
- Duration: 1–2 days, rarely longer.
- Not associated with tissue passage or clots.
- Not accompanied by significant pain; mild uterine cramping may occur.
- Differentiation from pathological bleeding:
|
Feature |
Implantation Bleeding |
Threatened/Spontaneous Abortion |
Ectopic Pregnancy |
Molar Pregnancy |
|
Amount |
Light, scant |
Often heavier, may have clots/tissue |
Variable, often dark brown or bright red |
Can be profuse, abnormal |
|
Color |
Pink or brown |
Bright red |
Dark red/brown |
Grape-like vesicles possible |
|
Duration |
1–2 days |
Ongoing until resolved |
Persistent or sudden onset |
Prolonged |
|
Pain |
Minimal or none |
Moderate cramping |
Unilateral pelvic pain, shoulder pain if ruptured |
Uterine distension possible |
|
Cervical os |
Closed |
May be open |
May be closed or open |
Closed |
|
Associated findings |
No systemic signs |
Possible hypotension, tachycardia if severe |
Signs of shock if rupture |
High hCG, absence of fetus |
Nursing Insights:
- Always assess hemodynamic stability (BP, HR) when a pregnant patient presents with bleeding. Even if the patient suspects implantation spotting, the nurse should rule out life-threatening conditions like ectopic pregnancy.
- Nurses should instruct patients to report heavy bleeding, clots, severe pain, or dizziness immediately, as these are not features of implantation bleeding.
1.3 Diagnostic Considerations
- Implantation bleeding is a diagnosis of exclusion.
- Investigations may be minimal but are sometimes necessary to distinguish from pathological causes:
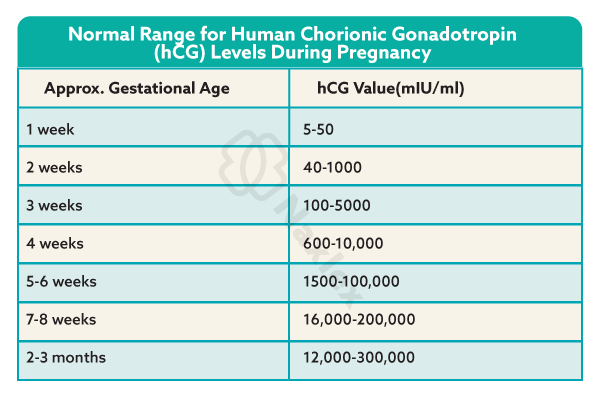
- Pregnancy test (urine or serum hCG): Confirms pregnancy. hCG levels will be rising but may still be low in very early implantation.
- Serial quantitative serum hCG:
- In viable pregnancy: doubles every 48–72 hours in early gestation.
- In abnormal pregnancy: plateauing or falling levels.
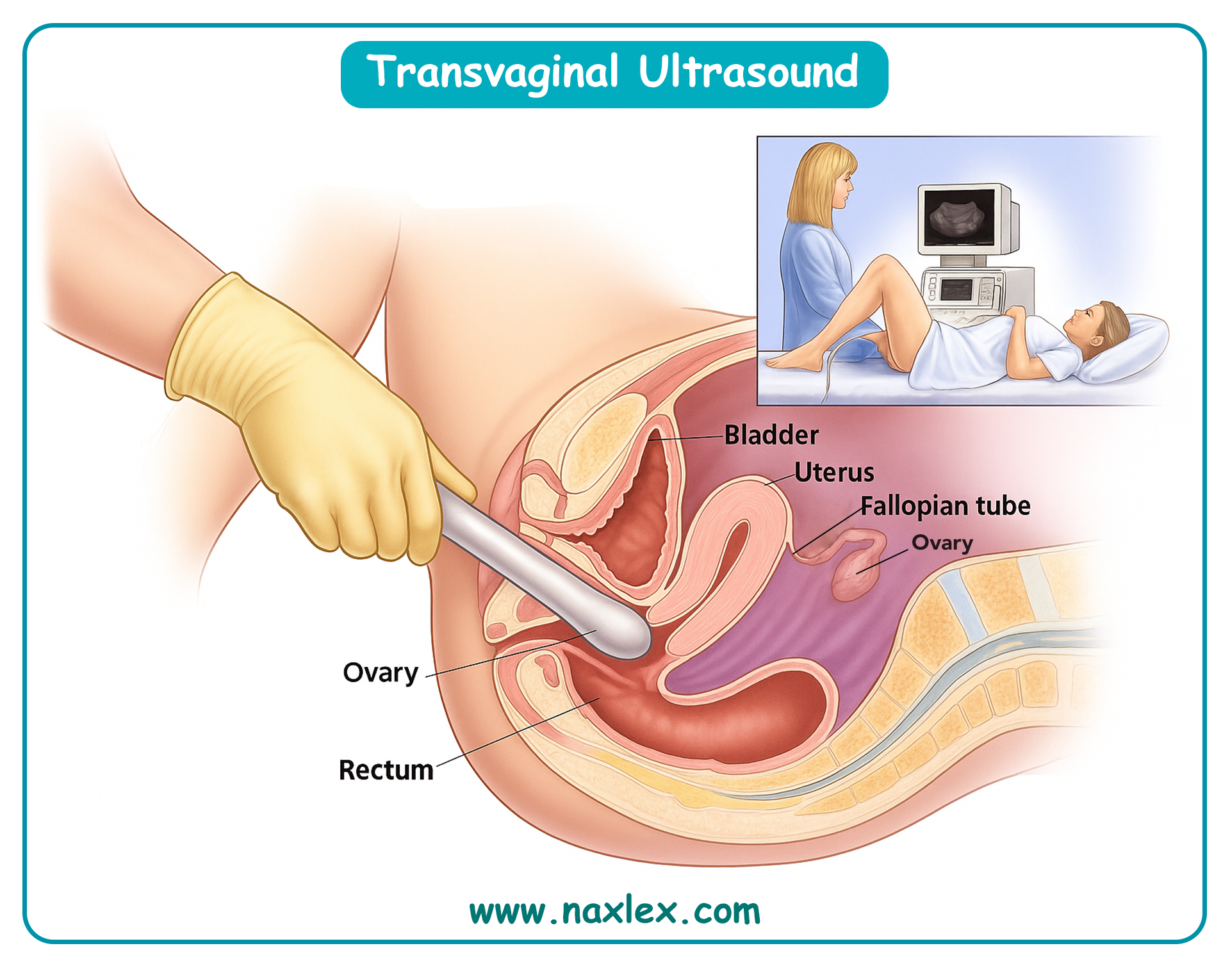
- Transvaginal ultrasound:
- May not yet show gestational sac if <5 weeks.
- Useful to exclude ectopic pregnancy or molar pregnancy in cases of abnormal presentation.
- Speculum exam:
- To rule out cervical pathology or trauma.
Nursing Insights:
- Nurses should avoid reassuring patients without evaluation. A small percentage of patients who believe they have implantation bleeding may actually be experiencing early pregnancy loss.
- Documentation of bleeding characteristics (onset, color, volume, associated symptoms) is essential for monitoring progression.
1.4 Nursing Interventions and Patient Education
- Assessment:
- Detailed history of bleeding (onset, duration, color, volume).
- Obstetric history (LMP, parity, prior miscarriages).
- Associated symptoms (pain, dizziness, passage of tissue).
- Vital signs for hemodynamic stability.
- Interventions:
- Reassure the patient if presentation is consistent with implantation bleeding.
- Provide anticipatory guidance: bleeding should not worsen, and systemic symptoms should not appear.
- Arrange follow-up for confirmation of viable pregnancy (serial hCG, ultrasound).
- Instruct on warning signs requiring urgent care:
- Heavy bleeding (soaking >1 pad/hour).
- Severe abdominal pain.
- Syncope or dizziness.
- Passage of tissue or clots.
- Patient Education:
- Explain that implantation bleeding is usually benign and self-limited.
- Emphasize that not all women experience implantation bleeding, and its absence does not indicate pregnancy failure.
- Encourage early initiation of prenatal care.
Nursing Insights:
- Nurses must always individualize care. While implantation bleeding is usually benign, nurses should never dismiss any first-trimester bleeding without evaluation.
- Emotional reassurance is critical. Patients may fear miscarriage, and clear, empathetic communication prevents unnecessary anxiety.
Spontaneous Abortion (Miscarriage)
Spontaneous abortion, commonly referred to as miscarriage, represents the unintended termination of a pregnancy before 20 weeks gestation or before the fetus reaches a weight of 500 grams, the threshold for viability. This clinical entity is a prevalent complication in early pregnancy, necessitating comprehensive nursing knowledge to assess, manage, and support affected patients. The following sections provide an in-depth exploration of the definition, epidemiology, etiology, pathophysiology, classification, assessment, interventions, complications, and psychosocial considerations of spontaneous abortion, equipping nursing students with the scientific foundation and practical skills required for effective maternal-newborn care.
1.1 Definition and Epidemiology
Spontaneous abortion is defined as the spontaneous loss of a pregnancy before 20 weeks gestation or a fetal weight less than 500 grams, resulting from natural causes without external intervention. It is a common obstetric complication, occurring in approximately 10-20% of recognized pregnancies, with higher rates in clinically unrecognized pregnancies.
- Epidemiological data:
- Approximately 80% of spontaneous abortions occur in the first trimester, with the incidence decreasing significantly after 12 weeks gestation.
- The true prevalence is likely higher, as many early losses occur before pregnancy confirmation, often mistaken for delayed menstruation.
- Advanced maternal age (>35 years) increases the risk, with miscarriage rates rising to 20-35% in women aged 35-40 and over 50% in women over 40.
- Recurrent spontaneous abortion, defined as three or more consecutive losses, affects approximately 1-2% of reproductive-age women.
- Impact on maternal health:
- Spontaneous abortion can lead to significant emotional and physical consequences, including grief, anxiety, and potential complications like hemorrhage or infection.
- The condition is a leading cause of first-trimester hospitalization among pregnant women, necessitating prompt nursing assessment and intervention.
Nursing Insights
- Nurses must recognize that spontaneous abortion is a common occurrence, particularly in the first trimester, to provide accurate patient education and reduce unnecessary alarm.
- Understanding the higher incidence in older maternal age groups guides nurses in identifying at-risk patients during prenatal assessments.
- Accurate documentation of pregnancy history, including prior losses, is essential for identifying patients at risk for recurrent spontaneous abortion.
- Nurses should anticipate the emotional impact of miscarriage and prepare to offer empathetic support and resources during patient interactions.
1.2 Etiology and Risk Factors
Spontaneous abortion results from a complex interplay of genetic, maternal, environmental, and lifestyle factors. Identifying these etiologies and risk factors is critical for risk assessment and patient counseling.
- Genetic factors:
- Chromosomal abnormalities, primarily aneuploidy (e.g., trisomy 16, 21, or monosomy X), account for 50-60% of first-trimester spontaneous abortions.
- Parental balanced translocations or inversions increase the risk of embryonic chromosomal errors.
- Maternal medical conditions:
- Endocrine disorders, such as uncontrolled diabetes mellitus or hypothyroidism, impair embryonic development and implantation.
- Autoimmune conditions, like antiphospholipid syndrome (APS), cause recurrent thrombosis and placental insufficiency.
- Polycystic ovary syndrome (PCOS) is associated with hormonal imbalances that may disrupt early pregnancy maintenance.
- Uterine anomalies:
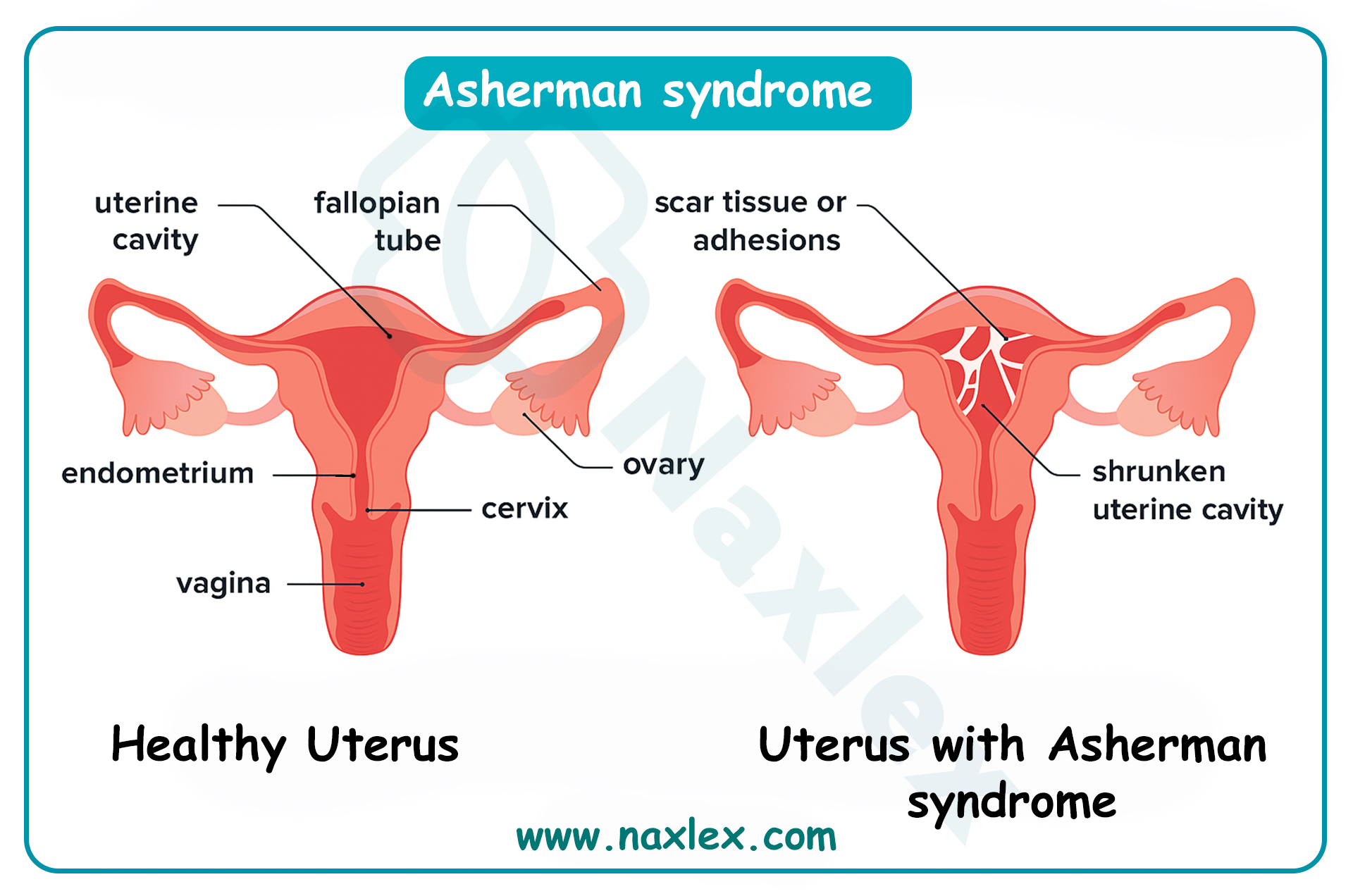
- Congenital anomalies, such as septate or bicornuate uterus, compromise endometrial blood supply and implantation.
- Acquired conditions, like Asherman syndrome (intrauterine adhesions), impair endometrial receptivity.
- Infections:
- Maternal infections, such as cytomegalovirus, toxoplasmosis, or bacterial vaginosis, may lead to embryonic demise or preterm labor.
- Lifestyle and environmental factors:
- Smoking, heavy alcohol consumption, and illicit drug use (e.g., cocaine) increase oxidative stress and impair fetal development.
- Exposure to environmental toxins, such as lead or radiation, is linked to higher miscarriage rates.
- Obesity (BMI >30) and extreme underweight (BMI <18.5) alter hormonal balance and increase risk.
- Other risk factors:
- Advanced paternal age (>40 years) may contribute to sperm DNA fragmentation, increasing miscarriage risk.
- Cervical insufficiency typically causes second-trimester losses due to premature cervical dilation.
- Trauma or severe stress may exacerbate underlying risk factors, though direct causation is less clear.
Nursing Insights
- Nurses must conduct a thorough history to identify risk factors, such as prior miscarriages, maternal age, or chronic conditions, to tailor patient education and referrals.
- Screening for lifestyle factors, including smoking or substance use, enables nurses to provide targeted counseling to mitigate modifiable risks.
- Recognizing the role of chromosomal abnormalities reassures patients that many miscarriages are not preventable, reducing feelings of guilt.
- Nurses should advocate for early screening for maternal infections or autoimmune disorders in patients with a history of pregnancy loss.
1.3 Pathophysiology of Pregnancy Loss
The pathophysiology of spontaneous abortion involves disruptions in the complex processes of embryonic development, implantation, and placental formation, leading to pregnancy failure.
- Embryonic factors:
- Chromosomal aneuploidy disrupts normal cell division and organogenesis, leading to nonviable embryos.
- Failure of trophoblast invasion impairs placental development, reducing nutrient and oxygen supply to the embryo.
- Maternal factors:
- Insufficient progesterone production by the corpus luteum or placenta fails to maintain endometrial integrity, triggering uterine contractions and expulsion.
- Thrombotic events in APS or other coagulopathies cause placental infarction and fetal demise.
- Endometrial and uterine factors:
- Inadequate decidualization due to hormonal imbalances or uterine anomalies compromises implantation stability.
- Intrauterine adhesions (Asherman syndrome) reduce endometrial surface area, hindering embryonic attachment.
- Immune and inflammatory responses:
- Dysregulated immune responses, such as excessive natural killer cell activity, may reject the embryo as foreign tissue.
- Systemic infections or localized endometritis trigger inflammatory cascades, leading to pregnancy loss.
- Vascular disruptions:
- Impaired spiral artery remodeling reduces uteroplacental blood flow, causing embryonic hypoxia and demise.
- Microhemorrhages or hematomas (e.g., subchorionic hematoma) may destabilize the implantation site.
Nursing Insights
- Understanding the role of progesterone in maintaining pregnancy guides nurses in monitoring for signs of hormonal insufficiency, such as early bleeding or cramping.
- Nurses must recognize that chromosomal abnormalities are the leading cause of first-trimester losses, informing empathetic patient education.
- Knowledge of uterine anomalies and their impact on implantation helps nurses advocate for imaging studies in patients with recurrent losses.
- Awareness of immune-mediated causes, such as APS, prompts nurses to assess for clotting disorders and coordinate multidisciplinary care.
1.4 Classification of Spontaneous Abortion
Spontaneous abortions are classified into distinct types based on clinical presentation, cervical status, and ultrasound findings. Each type has unique implications for management and nursing care.
1.4.1 Threatened Abortion
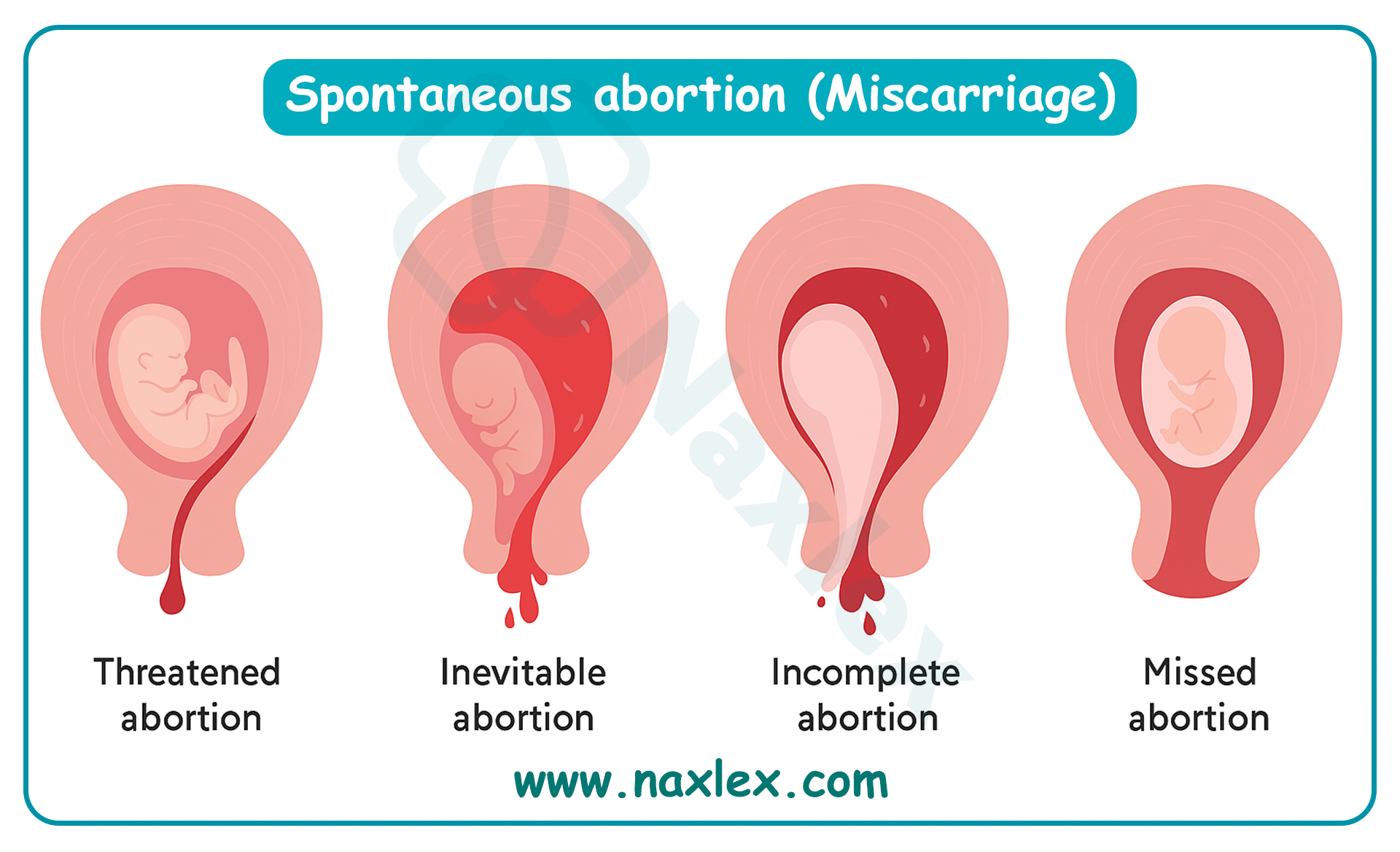
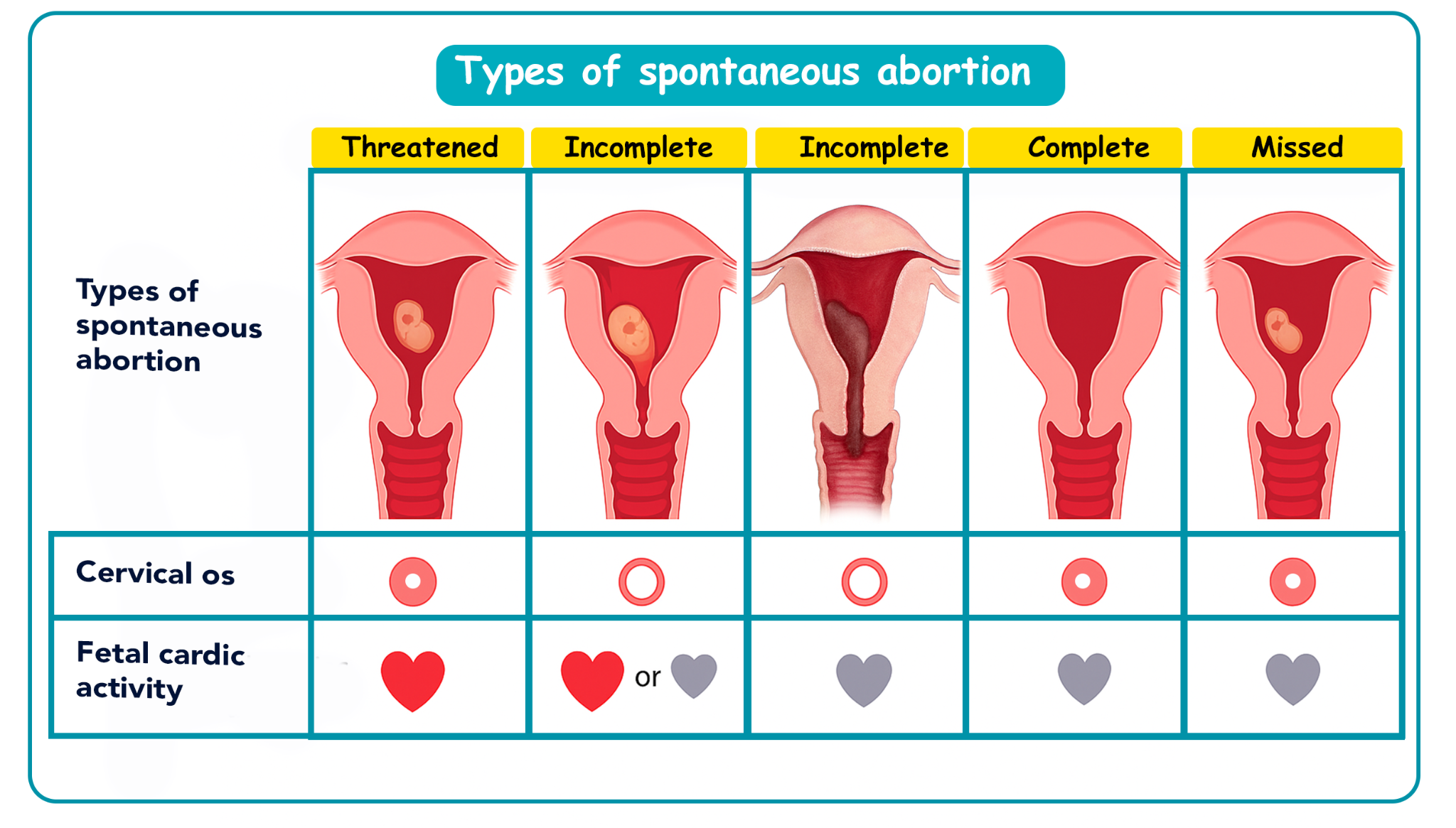
Threatened abortion is characterized by vaginal bleeding in the first 20 weeks of pregnancy with a closed cervical os and a viable intrauterine pregnancy confirmed by ultrasound.
- Clinical features:
- Light to moderate vaginal bleeding, typically bright red or brown, without passage of tissue.
- Mild cramping or pelvic discomfort may be present, but severe pain is absent.
- Fetal heart tones are detectable, and the cervix remains closed on examination.
- Prognosis:
- Approximately 50% of threatened abortions progress to normal pregnancies with appropriate management.
- Persistent bleeding or worsening symptoms may indicate progression to inevitable or incomplete abortion.
Nursing Insights
- Nurses must reassure patients that threatened abortion does not always lead to pregnancy loss, emphasizing the importance of pelvic rest and monitoring.
- Regular assessment of bleeding volume and vital signs is critical to detect progression to more severe types of abortion.
- Educating patients to avoid intercourse, tampons, and strenuous activity reduces the risk of exacerbating bleeding.
- Nurses should coordinate ultrasound follow-up to confirm fetal viability and monitor for complications like subchorionic hematoma.
1.4.2 Inevitable Abortion
Inevitable abortion is diagnosed when vaginal bleeding and uterine contractions occur with cervical dilation, indicating that pregnancy loss is unavoidable.
- Clinical features:
- Heavy vaginal bleeding, often with clots, accompanied by moderate to severe uterine cramping.
- Open cervical os on speculum examination, with or without passage of tissue.
- Fetal heart tones may be absent, though early in the process, viability may still be present.
- Progression:
- Inevitable abortion typically progresses to incomplete or complete abortion without intervention.
- Immediate management is required to prevent complications like hemorrhage.
Nursing Insights
- Nurses must prepare patients for the likelihood of pregnancy loss, providing emotional support while explaining the clinical findings.
- Monitoring for signs of hypovolemic shock (e.g., tachycardia, hypotension) is essential due to the risk of heavy bleeding.
- Nurses should ensure rapid access to medical or surgical interventions, such as misoprostol or dilation and curettage (D&C), to manage tissue expulsion.
- Accurate documentation of bleeding volume and cervical status guides the healthcare team in determining the urgency of intervention.
1.4.3 Incomplete Abortion
Incomplete abortion occurs when partial expulsion of the products of conception takes place, with retained tissue remaining in the uterus.
- Clinical features:
- Heavy vaginal bleeding with passage of clots or tissue fragments.
- Persistent uterine cramping due to incomplete expulsion.
- Open cervical os and ultrasound evidence of retained products of conception.
- Management considerations:
- Requires medical or surgical intervention to complete evacuation and prevent complications like infection or hemorrhage.
Nursing Insights
- Nurses must monitor for signs of infection, such as fever or foul-smelling discharge, in patients with incomplete abortion due to retained tissue.
- Assessing bleeding volume (e.g., soaking a pad in <1 hour) is critical to identify the need for urgent intervention.
- Nurses should prepare patients for potential procedures, such as D&C or misoprostol administration, explaining the process and expected outcomes.
- Providing pain management, such as ibuprofen or prescribed analgesics, improves patient comfort during the expulsion process.
1.4.4 Complete Abortion
Complete abortion is characterized by the full expulsion of all products of conception, with cessation of bleeding and a closed cervical os.
- Clinical features:
- Initial heavy bleeding and cramping, followed by cessation of symptoms.
- Ultrasound confirms an empty uterus with no retained tissue.
- Declining hCG levels post-expulsion, indicating complete resolution.
- Prognosis:
- Typically requires minimal intervention, with focus on monitoring for complications and providing emotional support.
Nursing Insights
- Nurses must confirm complete expulsion through ultrasound and declining hCG levels to ensure no retained tissue remains.
- Patient education on post-miscarriage care, including avoiding tampons and intercourse for 2-4 weeks, reduces infection risk.
- Monitoring for excessive bleeding or signs of infection post-expulsion is essential, even in complete abortion cases.
- Nurses should provide empathetic support, as patients may experience significant grief despite resolution of physical symptoms.
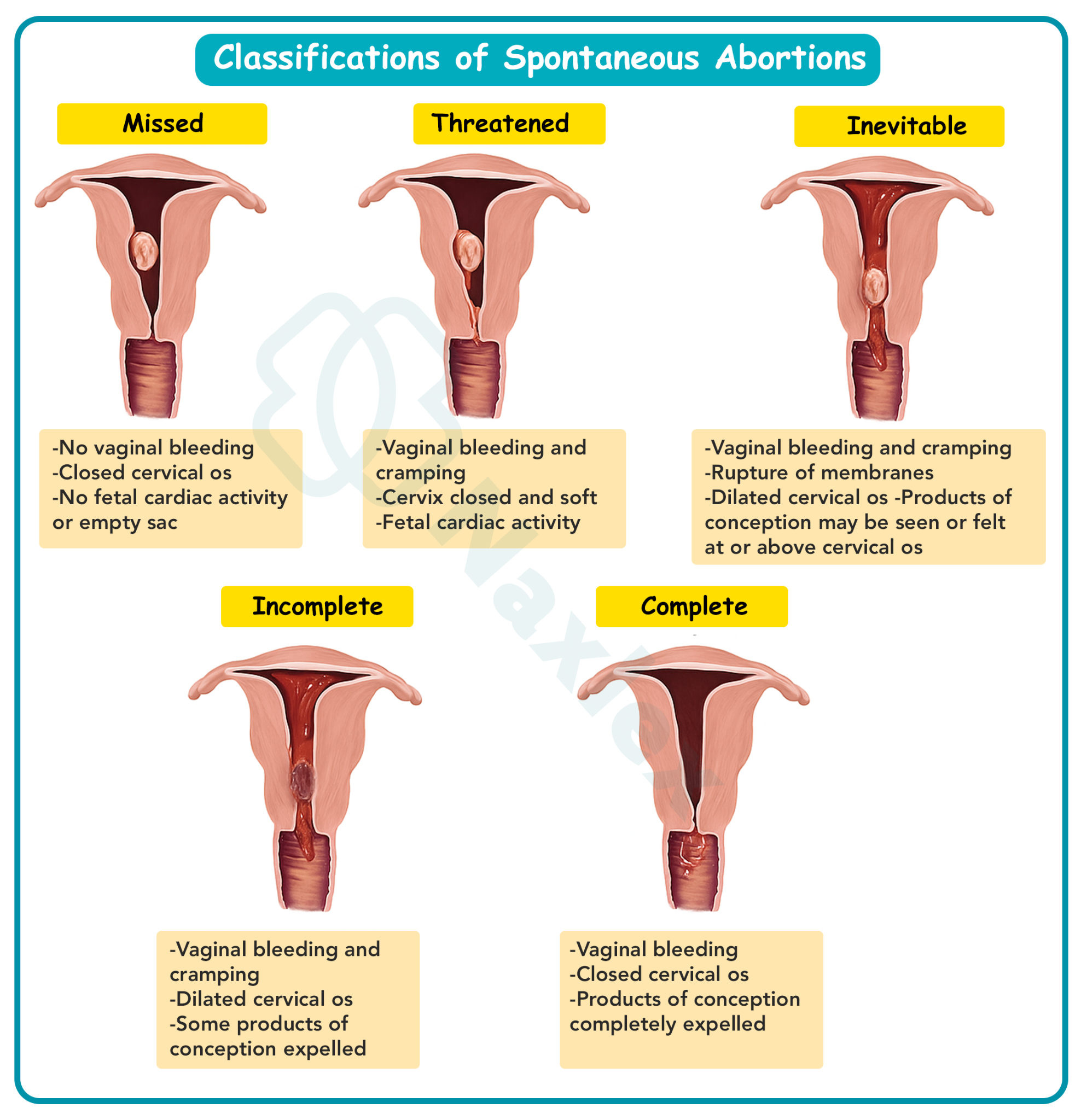
1.4.5 Missed Abortion
Missed abortion is defined as fetal demise without expulsion of the products of conception, often detected incidentally on ultrasound.
- Clinical features:
- Loss of pregnancy symptoms (e.g., nausea, breast tenderness) without vaginal bleeding.
- Ultrasound reveals an empty gestational sac or no fetal heartbeat.
- Closed cervical os, with no immediate signs of expulsion.
- Management considerations:
- May be managed expectantly, medically, or surgically, depending on patient preference and clinical stability.
Nursing Insights
- Nurses must recognize the absence of bleeding in missed abortion, prompting ultrasound evaluation in patients reporting loss of pregnancy symptoms.
- Providing emotional support is critical, as patients may be unaware of the loss until diagnostic confirmation, leading to sudden grief.
- Nurses should educate patients on management options (expectant, medical, or surgical), ensuring informed decision-making.
- Monitoring for complications, such as disseminated intravascular coagulation (DIC) with prolonged retention, is essential in missed abortion cases.
1.4.6 Recurrent (Habitual) Abortion
Recurrent abortion is defined as three or more consecutive spontaneous abortions before 20 weeks gestation, affecting 1-2% of women.
- Clinical features:
- Repeated pregnancy losses with similar clinical presentations (e.g., bleeding, cramping, or missed abortion).
- Often associated with underlying maternal or genetic factors requiring specialist evaluation.
- Etiology:
- Includes parental chromosomal abnormalities, uterine anomalies, APS, or endocrine disorders.
- Psychological stress and grief may compound physical risk factors.
Nursing Insights
- Nurses must advocate for referral to a reproductive endocrinologist for comprehensive evaluation in patients with recurrent abortion.
- Detailed history-taking to identify patterns of loss (e.g., timing, symptoms) guides diagnostic workup and management planning.
- Providing psychosocial support is critical, as recurrent losses lead to significant emotional distress and potential depression.
- Nurses should educate patients on modifiable risk factors, such as smoking cessation, to reduce the likelihood of future losses.
1.5 Assessment and Diagnostic Evaluation
Accurate assessment and diagnostic evaluation of spontaneous abortion are critical to determine the type, guide management, and identify complications.
- History taking:
- Document the onset, volume, and characteristics of vaginal bleeding (e.g., color, clots, tissue passage).
- Assess associated symptoms, such as cramping, loss of pregnancy symptoms, or systemic signs (e.g., fever, dizziness).
- Review obstetric history, including prior miscarriages, gestational age, and risk factors (e.g., smoking, chronic conditions).
- Physical examination:
- Speculum examination: Assess cervical os status (open vs. closed) and presence of tissue or clots at the os.
- Bimanual examination: Evaluate uterine size, consistency, and adnexal tenderness to rule out ectopic pregnancy or masses.
- Vital signs: Monitor for tachycardia, hypotension, or fever, indicating potential hemorrhage or infection.
- Diagnostic tests:
- Transvaginal ultrasound: Confirms intrauterine pregnancy, fetal viability, or retained products; key findings include empty gestational sac (missed abortion), open cervical os (inevitable/incomplete), or empty uterus (complete).
- Quantitative hCG levels: Doubling every 48-72 hours indicates viable pregnancy; plateauing or declining levels suggest nonviability.
- Serum progesterone: Levels <5 ng/mL indicate nonviable pregnancy; levels >25 ng/mL suggest viability.
- Complete blood count (CBC): Assesses hemoglobin/hematocrit for anemia due to blood loss.
- Blood type and Rh factor: Determines need for Rh immune globulin in Rh-negative patients.
- Coagulation studies: Rules out DIC in cases of prolonged retention (missed abortion).
- Differential diagnosis:
- Ectopic pregnancy: Adnexal mass or pain, abnormal hCG trends.
- Molar pregnancy: Grape-like vesicles, excessively elevated hCG, “snowstorm” ultrasound pattern.
- Cervical pathology: Friability or polyps causing bleeding without intrauterine pathology.
Nursing Insights
- Nurses must ensure accurate documentation of bleeding patterns and associated symptoms to guide diagnostic evaluation and management.
- Preparing patients for transvaginal ultrasound involves explaining the procedure and ensuring comfort to facilitate accurate imaging.
- Monitoring vital signs regularly detects early signs of hemodynamic instability, prompting timely intervention.
- Nurses should confirm Rh status and advocate for RhoGAM administration within 72 hours for Rh-negative patients to prevent isoimmunization.
1.6 Nursing and Medical Interventions for Each Type
Interventions for spontaneous abortion vary by type, ranging from expectant management to medical or surgical approaches, with nursing care focusing on monitoring, support, and complication prevention.
- Threatened abortion:
- Expectant management: Pelvic rest (avoiding intercourse, tampons, strenuous activity), serial hCG monitoring, and ultrasound follow-up to confirm viability.
- Nursing role: Educate on pelvic rest, monitor bleeding and vital signs, provide emotional support, and coordinate follow-up appointments.
- Inevitable abortion:
- Medical management: Misoprostol to facilitate uterine evacuation if incomplete expulsion occurs.
- Surgical management: Dilation and curettage (D&C) for excessive bleeding or patient preference.
- Nursing role: Administer pain relief, monitor for hemorrhage, prepare for surgical intervention, and provide empathetic communication.
- Incomplete abortion:
- Medical management: Misoprostol (800 mcg vaginally or orally) to promote expulsion of retained tissue.
- Surgical management: D&C to remove retained products and prevent complications.
- Nursing role: Monitor bleeding volume, administer medications as prescribed, assess for infection, and educate on post-procedure care.
- Complete abortion:
- Management: Confirm complete expulsion via ultrasound and declining hCG levels; no further intervention typically required.
- Nursing role: Monitor for complications (e.g., infection), provide discharge instructions, and offer grief counseling.
- Missed abortion:
- Expectant management: Await spontaneous expulsion if stable, with close monitoring.
- Medical management: Misoprostol or mifepristone to induce expulsion.
- Surgical management: D&C or vacuum aspiration for patient preference or prolonged retention.
- Nursing role: Educate on management options, monitor for DIC, provide emotional support, and coordinate follow-up.
- Recurrent abortion:
- Management: Referral to a reproductive endocrinologist for evaluation of underlying causes (e.g., APS, uterine anomalies).
- Nursing role: Coordinate specialist referrals, educate on modifiable risk factors, and provide ongoing psychosocial support.
Nursing Insights
- Nurses must educate patients on the rationale for pelvic rest in threatened abortion to enhance compliance and reduce bleeding risk.
- Administering misoprostol requires explaining side effects (e.g., cramping, diarrhea) and monitoring for excessive bleeding post-dose.
- Preparing patients for D&C involves preoperative education, ensuring informed consent, and monitoring for post-procedure complications.
- Nurses should advocate for RhoGAM administration in Rh-negative patients within 72 hours of miscarriage to prevent future complications.
1.7 Complications of Abortion
Spontaneous abortion may lead to several complications, necessitating vigilant nursing assessment and timely intervention.
- Hemorrhage:
- Excessive bleeding due to incomplete expulsion or uterine atony, leading to hypovolemic shock (tachycardia, hypotension, dizziness).
- Management includes fluid resuscitation, uterotonics (e.g., oxytocin), or surgical evacuation.
- Infection:
- Endometritis or sepsis from retained tissue or post-procedure contamination, presenting with fever, foul-smelling discharge, or pelvic pain.
- Treated with antibiotics and removal of retained products.
- Asherman syndrome:
- Intrauterine adhesions from repeated D&C procedures, leading to infertility or recurrent pregnancy loss.
- Diagnosed via hysteroscopy and managed with adhesiolysis.
- Disseminated intravascular coagulation (DIC):
- Rare in missed abortion with prolonged retention of nonviable tissue, causing coagulopathy and bleeding tendencies.
- Requires urgent hematological management and tissue evacuation.
- Rh isoimmunization:
- Occurs in Rh-negative mothers exposed to Rh-positive fetal blood, risking alloimmunization in future pregnancies.
- Prevented with RhoGAM administration within 72 hours.
- Psychological impact:
- Grief, depression, or anxiety following pregnancy loss, potentially requiring counseling or support group referral.
Nursing Insights
- Nurses must monitor for signs of hemorrhage, such as soaking a pad in <1 hour, and initiate fluid resuscitation promptly if instability is detected.
- Assessing for fever or foul-smelling discharge post-miscarriage is critical to identify and treat infection early.
- Educating patients on the risks of repeated D&C procedures, such as Asherman syndrome, supports informed decision-making for management options.
- Nurses should ensure RhoGAM is administered to Rh-negative patients to prevent isoimmunization, documenting the dose and timing.
1.8 Psychosocial and Emotional Considerations in Pregnancy Loss
Spontaneous abortion often results in significant emotional distress, requiring nurses to provide empathetic, patient-centered support to address grief and promote coping.
- Emotional responses:
- Patients may experience a range of emotions, including sadness, guilt, anger, or denial, which vary in intensity and duration.
- Partners and family members may also require support, as pregnancy loss affects the entire support system.
- Nursing interventions:
- Use active listening to validate patient feelings, avoiding dismissive phrases like “you can try again.”
- Offer information on support groups, counseling services, or chaplaincy for spiritual support.
- Provide a nonjudgmental environment, acknowledging the individual nature of grief.
- Cultural considerations:
- Cultural or religious beliefs may influence grieving processes, requiring tailored support and sensitivity.
- Nurses should inquire about cultural practices to ensure respectful care delivery.
- Follow-up care:
- Schedule follow-up appointments to assess emotional well-being and provide ongoing support.
- Refer patients with prolonged grief or depression to mental health professionals.
Nursing Insights
- Nurses must use empathetic communication, such as acknowledging the loss with phrases like “I’m so sorry for your loss,” to build trust and support patients.
- Offering resources, such as grief counseling or support group contacts, empowers patients to seek help during the grieving process.
- Recognizing cultural differences in grief expression ensures culturally competent care and enhances patient comfort.
- Nurses should monitor for signs of prolonged grief or depression, advocating for mental health referrals as needed.
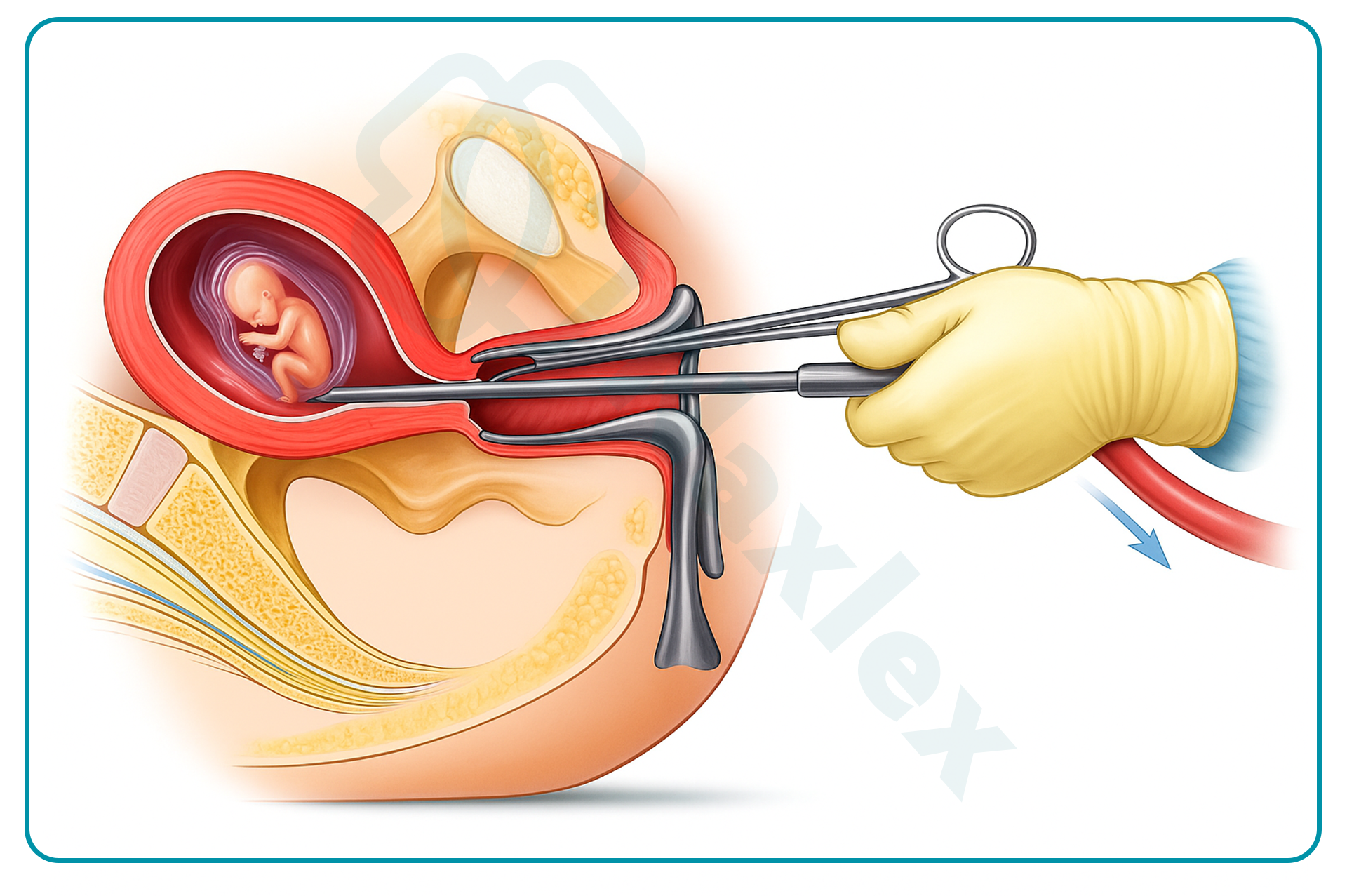
Induced Abortion
Induced abortion constitutes the deliberate termination of a pregnancy through medical or surgical means, performed under controlled clinical conditions to ensure patient safety and efficacy. This procedure, encompassing both therapeutic and elective indications, requires comprehensive nursing knowledge of legal frameworks, indications, methodologies, and supportive care to address the physical, emotional, and ethical dimensions of patient care. The following sections delineate the definition, legal considerations, indications, methods, nursing responsibilities, complications, and post-procedure counseling for induced abortion, providing nursing students with a scientifically rigorous foundation for evidence-based practice in maternal-newborn nursing.
1.1 Definition and Legal Considerations
Induced abortion is defined as the intentional interruption of pregnancy before fetal viability, utilizing pharmacological agents or mechanical procedures to expel the products of conception. It is distinguished from spontaneous abortion by its elective or therapeutic intent, with procedures typically performed before 20 weeks gestation to minimize maternal risks.
- Therapeutic versus elective abortion:
- Therapeutic abortion is performed to preserve maternal life or health, or due to fetal anomalies incompatible with life.
- Elective abortion occurs at the patient's request without medical necessity, often for socioeconomic, personal, or psychological reasons.
- Legal considerations:
- In the United States, following the 2022 Dobbs v. Jackson Women's Health Organization Supreme Court decision, abortion legality is regulated at the state level, with variations ranging from permissive access up to viability to near-total bans with exceptions for maternal life endangerment.
- Federal laws, such as the Partial-Birth Abortion Ban Act of 2003, prohibit certain late-term procedures, while the Hyde Amendment restricts federal funding for abortions except in cases of rape, incest, or life endangerment.
- Internationally, the World Health Organization advocates for safe abortion access as a reproductive right, with legal frameworks varying by country (e.g., liberal in Canada and Europe, restrictive in many Latin American and African nations).
- Informed consent is mandatory, requiring patients to receive comprehensive information on risks, benefits, alternatives, and gestational age limitations.
- Ethical implications for nursing:
- Nurses must adhere to institutional policies, personal ethics, and professional codes (e.g., American Nurses Association Code of Ethics), which support patient autonomy while allowing conscientious objection with appropriate referral.
- Documentation of consent, gestational age verification via ultrasound, and compliance with state-mandated waiting periods or counseling requirements are essential.
Nursing Insights
- Nurses must verify state-specific legal requirements, such as mandatory ultrasound or waiting periods, to ensure procedural compliance and protect patient rights.
- Obtaining comprehensive informed consent involves explaining procedure details, risks, and alternatives in a nonjudgmental manner to empower patient decision-making.
- In cases of conscientious objection, nurses should facilitate seamless referral to another provider without delaying care, maintaining professional integrity.
- Accurate documentation of gestational age and fetal viability assessment prevents legal challenges related to late-term procedures.
1.2 Indications for Induced Abortion
Indications for induced abortion encompass a broad spectrum of maternal, fetal, and psychosocial factors, guiding clinical decision-making to optimize patient outcomes.
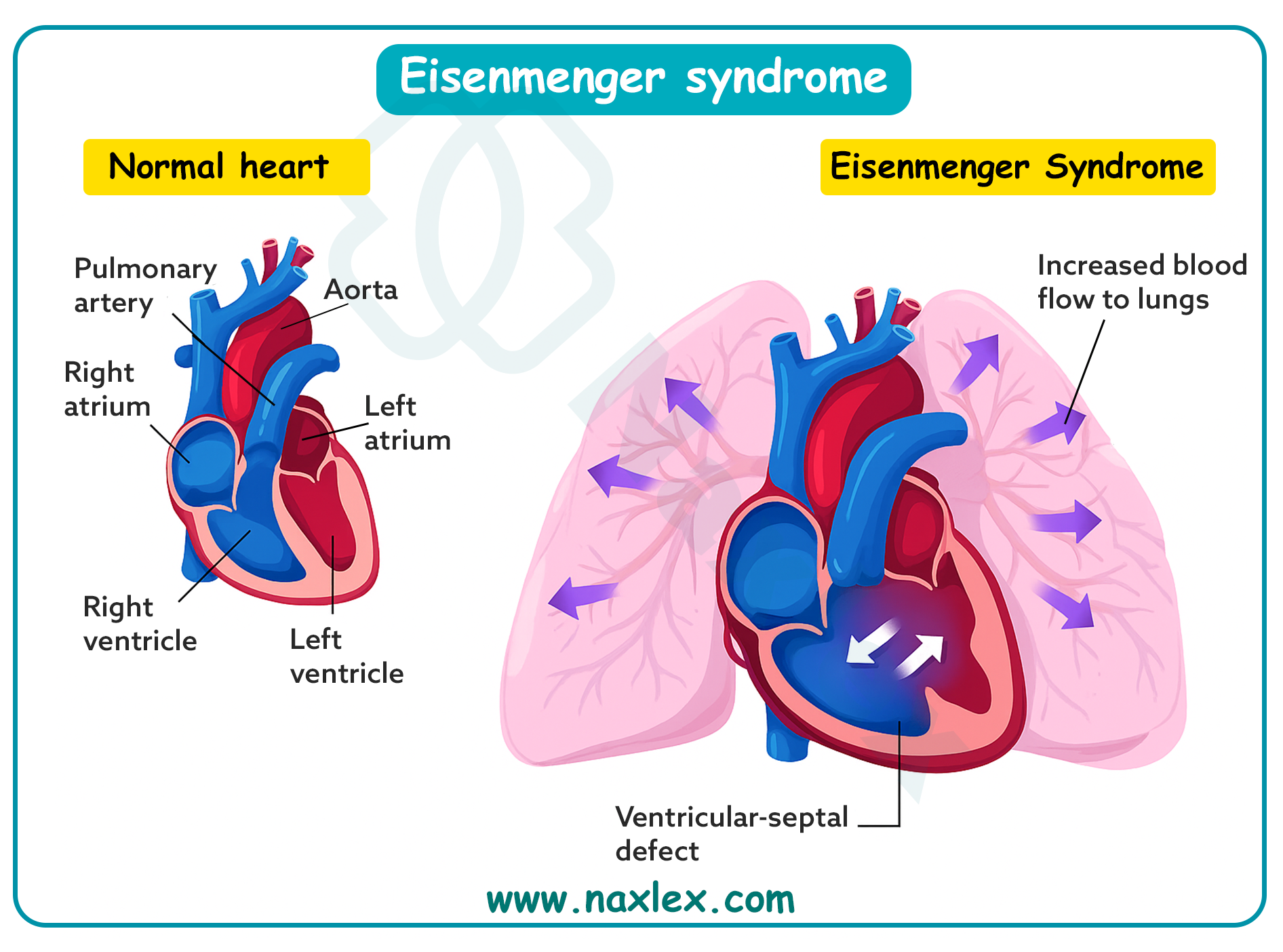
- Maternal health indications:
- Life-threatening conditions, such as severe preeclampsia, eclampsia, or cardiac disease (e.g., Eisenmenger syndrome), where continuation poses imminent risk.
- Oncological diagnoses requiring immediate chemotherapy or radiation incompatible with pregnancy.
- Severe psychiatric disorders, including suicidal ideation, where pregnancy exacerbates mental health crises.
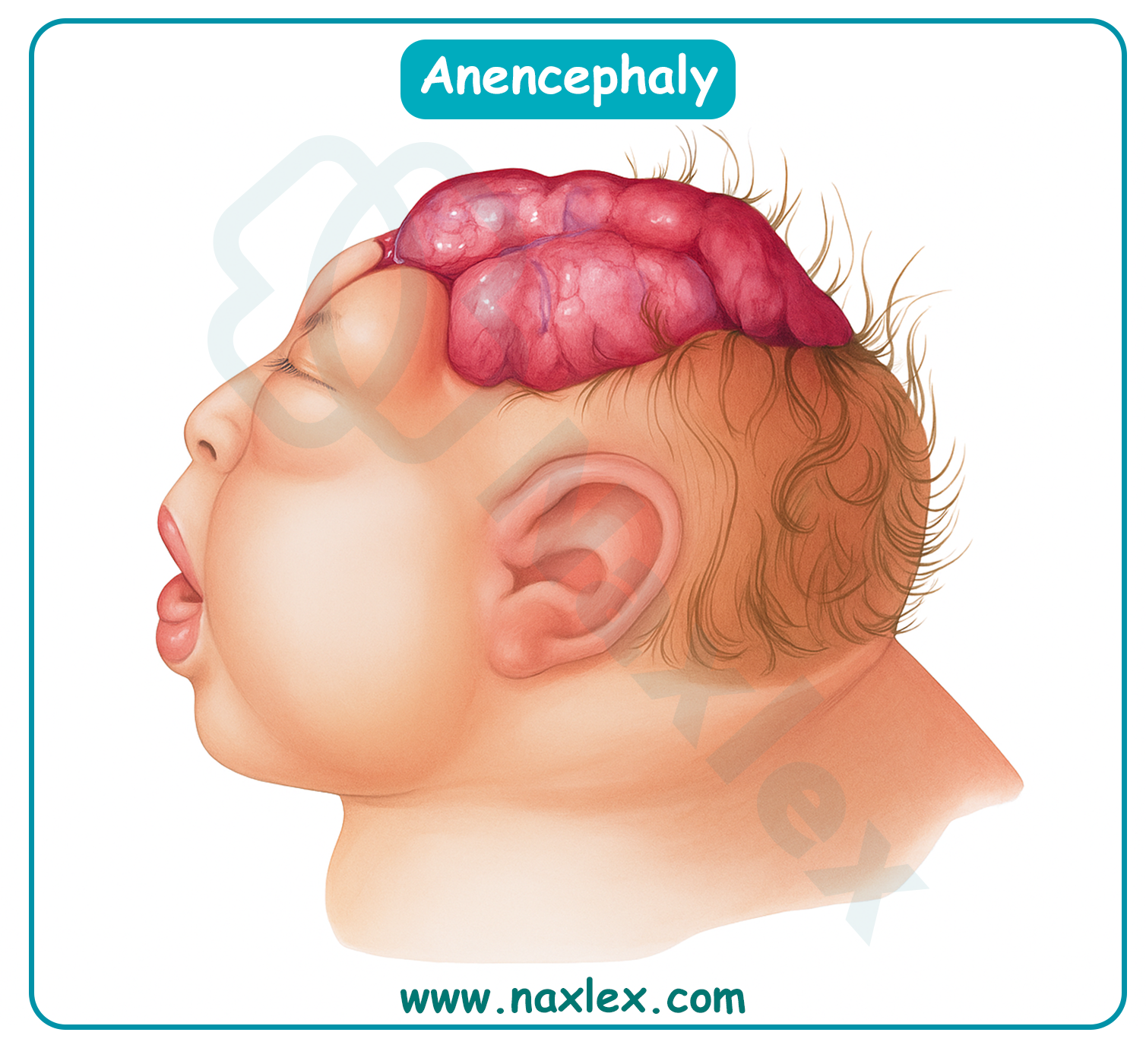
- Fetal indications:
- Congenital anomalies incompatible with extrauterine life, such as anencephaly or bilateral renal agenesis, confirmed via amniocentesis or chromosomal analysis.
-
- Genetic disorders, including trisomy 13 or 18, detected through noninvasive prenatal testing (NIPT) or invasive diagnostics.
- Elective indications:
- Socioeconomic constraints, including financial instability, lack of support, or career considerations.
- Personal circumstances, such as relationship issues, age, or parity preferences.
- Contraceptive failure or unintended pregnancy, particularly in adolescents or women with multiple prior pregnancies.
- Combined indications:
- Rape, incest, or sexual assault, often compounded by psychological trauma.
- Substance use disorders, where fetal exposure risks developmental abnormalities.
Nursing Insights
- Nurses must conduct sensitive history-taking to identify indications, ensuring confidentiality and nonjudgmental support for patients disclosing sensitive information like assault.
- Verifying fetal anomalies through ultrasound or genetic testing requires empathetic communication of results to facilitate informed decision-making.
- Assessing psychosocial factors, such as support systems, guides referral to social services or counseling to address barriers to care.
- Nurses should advocate for timely access to abortion services in maternal health emergencies to prevent complications like maternal mortality.
1.3 Methods of Induced Abortion
Induced abortion methods are selected based on gestational age, patient preference, medical history, and facility resources, with efficacy rates exceeding 95% for most procedures.
1.3.1 Medical (Mifepristone, Misoprostol, Methotrexate)
Medical abortion involves pharmacological induction of pregnancy termination, suitable for gestations up to 10-11 weeks, offering a non-invasive alternative.
- Mifepristone and misoprostol regimen:
- Mifepristone (200 mg orally) antagonizes progesterone receptors, inhibiting uterine decidualization, reducing hCG production, and sensitizing the myometrium to prostaglandins.
- Misoprostol (800 mcg buccally, vaginally, or sublingually) 24-48 hours later induces cervical softening, uterine contractions, and expulsion of products, mimicking spontaneous abortion.
- Efficacy: 95-98% complete abortion rate; follow-up ultrasound or hCG assessment confirms success.
- Methotrexate:
- Administered intramuscularly (50 mg/m²) for early gestations (<7 weeks) or ectopic pregnancies, it inhibits dihydrofolate reductase, disrupting trophoblastic cell proliferation and DNA synthesis.
- Followed by misoprostol 3-7 days later to facilitate expulsion.
- Monitoring includes serial hCG levels (decline >15% by day 4 indicates success) and liver function tests due to hepatotoxicity risk.
- Pharmacokinetics and side effects:
- Common side effects include nausea, vomiting, diarrhea, and heavy bleeding/cramping; rare complications involve incomplete abortion (5%) or sepsis.
- Contraindications: Ectopic pregnancy, adrenal insufficiency, chronic corticosteroid use, or IUD in situ.
Nursing Insights
- Nurses must educate patients on the expected timeline of expulsion (4-6 hours post-misoprostol) and provide pain management strategies, such as ibuprofen, for cramping.
- Monitoring for excessive bleeding (soaking >2 pads/hour) post-medication requires telephone triage protocols to ensure timely intervention.
- Administering methotrexate involves assessing baseline liver and renal function, with follow-up labs to detect rare toxicities like leukopenia.
- Providing antiemetics prophylactically enhances patient comfort during the medical abortion process.
1.3.2 Surgical (Vacuum Aspiration, D&C, D&E)
Surgical methods provide definitive termination through mechanical evacuation, preferred for gestations beyond medical limits or patient preference for immediacy.
- Manual vacuum aspiration (MVA):
- Performed under local anesthesia up to 12 weeks, involving cervical dilation followed by aspiration using a 50-60 mL syringe to remove products.
- Efficacy: >99%; minimal blood loss (<50 mL) and rapid recovery.
- Electric vacuum aspiration (EVA):
- Utilizes suction cannula connected to electric pump for gestations 6-14 weeks, often with paracervical block or sedation.
- Sharp curettage may be combined for complete evacuation.
- Dilation and curettage (D&C):
- Involves mechanical dilation of cervix with laminaria or misoprostol, followed by sharp curette scraping of endometrium; used for incomplete spontaneous abortions or early induced terminations.
- Risks include uterine perforation (0.5%) or Asherman syndrome with repeated use.
- Dilation and evacuation (D&E):
- For second-trimester (13-24 weeks), combines vacuum aspiration with forceps extraction of fetal parts after osmotic dilators (laminaria) soften cervix over 24-48 hours.
- Requires general anesthesia; efficacy >99%, but higher risks of hemorrhage or infection.
- Procedural considerations:
- Preoperative ultrasound confirms gestational age and location; RhoGAM for Rh-negative patients.
- Postoperative verification via ultrasound or pathology ensures complete evacuation.
Nursing Insights
- Nurses must prepare patients for vacuum aspiration by explaining the procedure's brevity (5-10 minutes) and providing sedation options for anxiety reduction.
- Intra-procedure monitoring includes vital signs and pain assessment during D&E to detect complications like perforation.
- Post-D&C, nurses assess for retained products by monitoring bleeding and scheduling follow-up ultrasound if hCG persists.
- Using osmotic dilators requires patient education on expected cramping and discharge during overnight placement.
1.4 Nursing Responsibilities Pre, Intra, and Post Procedure
Nursing responsibilities in induced abortion span preoperative preparation, intraoperative support, and postoperative monitoring to ensure safety and holistic care.
- Pre-procedure responsibilities:
- Conduct comprehensive assessment, including vital signs, laboratory tests (CBC, Rh type, coagulation profile), and psychosocial evaluation.
- Verify informed consent, administer preoperative medications (e.g., misoprostol for cervical ripening, antibiotics prophylaxis).
- Provide education on procedure expectations, pain management, and recovery timeline; confirm gestational age via ultrasound.
- Intra-procedure responsibilities:
- Assist with positioning, monitor vital signs, and administer sedation or analgesia as ordered.
- Ensure sterile technique, prepare instruments, and provide emotional support during the procedure.
- Observe for immediate complications, such as vasovagal response or excessive bleeding.
- Post-procedure responsibilities:
- Monitor recovery in PACU for vital signs, bleeding, and pain; assess for perforation or infection signs.
- Provide discharge instructions on bleeding (expect light for 1-2 weeks), activity restrictions (no heavy lifting for 1 week), and warning signs (fever >100.4°F, foul discharge).
- Administer RhoGAM if indicated and schedule follow-up for hCG or ultrasound confirmation.
Nursing Insights
- Preoperative anxiety assessment allows nurses to offer calming techniques or referrals to counseling, enhancing patient cooperation.
- Intra-procedure, maintaining a supportive presence reduces patient distress during painful aspects like speculum insertion.
- Post-procedure vital sign monitoring every 15 minutes initially detects hypovolemia from undetected hemorrhage.
- Discharge teaching includes contraception options to prevent unintended pregnancies, tailored to patient preferences.
1.5 Complications and Risk Reduction
Complications of induced abortion are rare (<2%) but require vigilant monitoring and preventive strategies to mitigate risks.
- Immediate complications:
- Hemorrhage (0.4-1%), due to uterine atony or laceration, managed with uterotonics or re-aspiration.
- Infection (0.5%), endometritis or pelvic inflammatory disease, prevented with doxycycline prophylaxis.
- Uterine perforation (0.1-0.3%), detected intraoperatively via resistance or ultrasound, potentially requiring laparoscopy.
- Delayed complications:
- Retained products (1-2%), causing persistent bleeding; confirmed by ultrasound and treated with repeat evacuation.
- Asherman syndrome from aggressive curettage, leading to amenorrhea; risk reduced with ultrasound guidance.
- Cervical incompetence from trauma, increasing future preterm labor risk.
- Risk reduction strategies:
- Preoperative antibiotics (doxycycline 100 mg BID x 2 doses) reduce infection by 50%.
- Ultrasound guidance minimizes perforation and incomplete evacuation.
- Patient selection excludes contraindications like coagulopathy.
Nursing Insights
- Nurses monitor post-procedure bleeding pad counts hourly to quantify loss and intervene early for hemorrhage.
- Administering prophylactic antibiotics pre-procedure prevents ascending infections in high-risk patients.
- Educating on signs of perforation, such as severe pain or shoulder tip pain, prompts immediate return to care.
- Follow-up calls 24-48 hours post-discharge assess for delayed complications like retained tissue.
1.6 Post-Abortion Counseling and Contraception
Post-abortion counseling addresses emotional recovery and reproductive planning, integrating contraception to support future autonomy.
- Counseling components:
- Validate emotional responses, including relief, guilt, or grief; refer to counseling for complex reactions.
- Discuss physical recovery, resuming menses (2-4 weeks), and fertility return (immediately post-procedure).
- Address myths, such as infertility risk (no increased long-term risk with safe procedures).
- Contraception options:
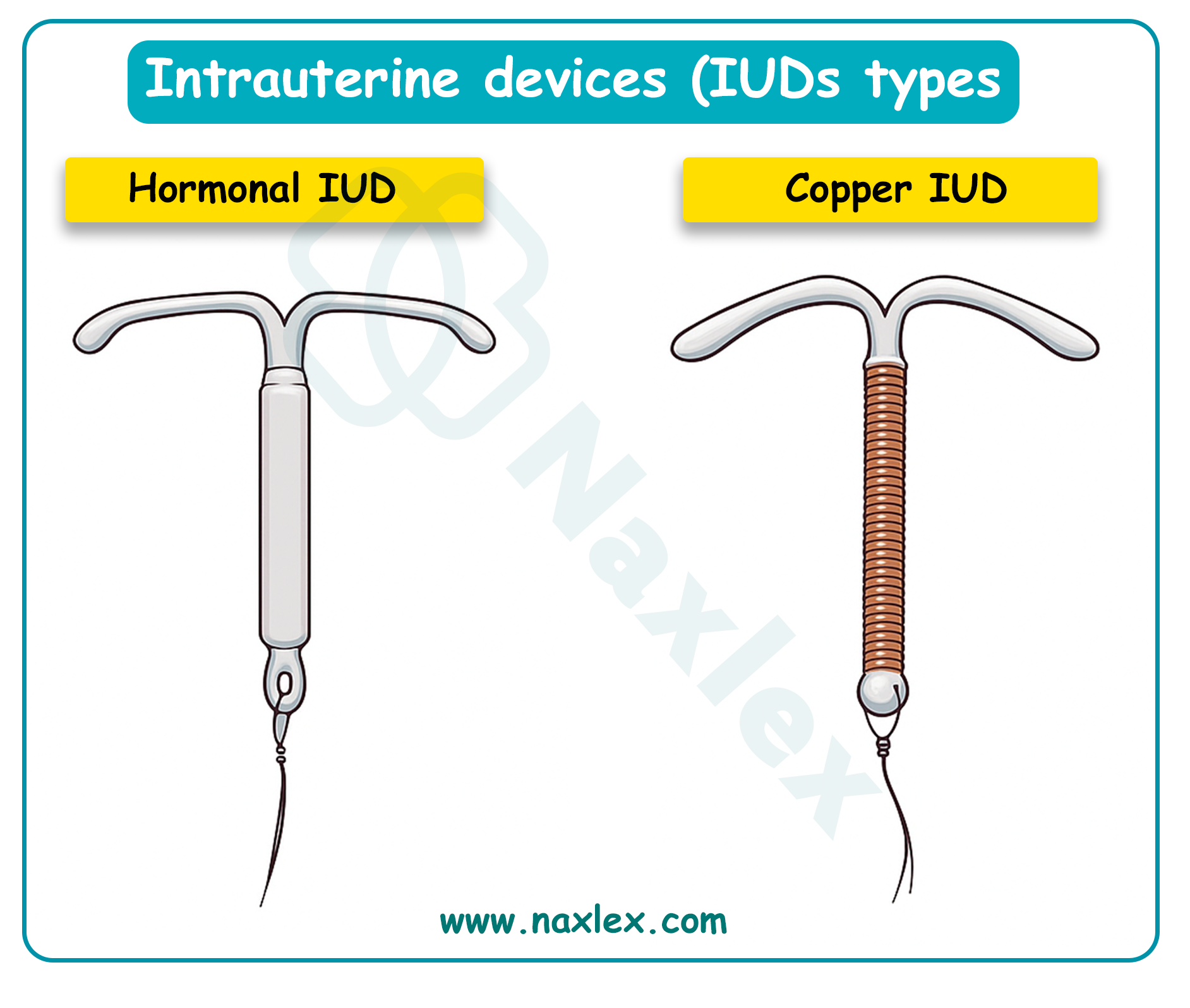
- Immediate initiation: Progestin-only pills, patch, or ring effective from day 1; IUD insertion post-procedure.
- Long-acting reversible contraception (LARC): Intrauterine devices (copper or levonorgestrel) with >99% efficacy, inserted immediately to reduce repeat unintended pregnancies.
- Barrier methods: Condoms for STI prevention; combined hormonal methods after 1 week.
- Follow-up care:
- Clinic visit 1-2 weeks post-procedure for complication assessment and contraception initiation.
- hCG monitoring if medical abortion to confirm decline (>90% drop indicates success).
Nursing Insights
- Nurses facilitate open discussions on emotions, using active listening to identify needs for grief support or psychiatric referral.
- Offering immediate contraception, like etonogestrel implant, empowers patients and reduces unintended pregnancy rates by 80%.
- Tailoring contraception to patient lifestyle (e.g., depot medroxyprogesterone for irregular access) enhances adherence.
- Scheduling follow-up ensures resolution of complications and reinforces education on warning signs.
Ectopic Pregnancy
Ectopic pregnancy constitutes a critical obstetric emergency wherein the fertilized ovum implants outside the endometrial cavity, predominantly within the fallopian tube, posing substantial risks to maternal health and fertility. This pathological implantation disrupts normal embryonic development and may culminate in life-threatening complications, necessitating prompt recognition and intervention in maternal-newborn nursing practice. The ensuing sections expound upon the definition, pathophysiology, risk factors, clinical manifestations, diagnostic modalities, therapeutic interventions, and associated complications of ectopic pregnancy, furnishing nursing students with an exhaustive, scientifically grounded compendium to facilitate proficient clinical acumen and patient-centered care.
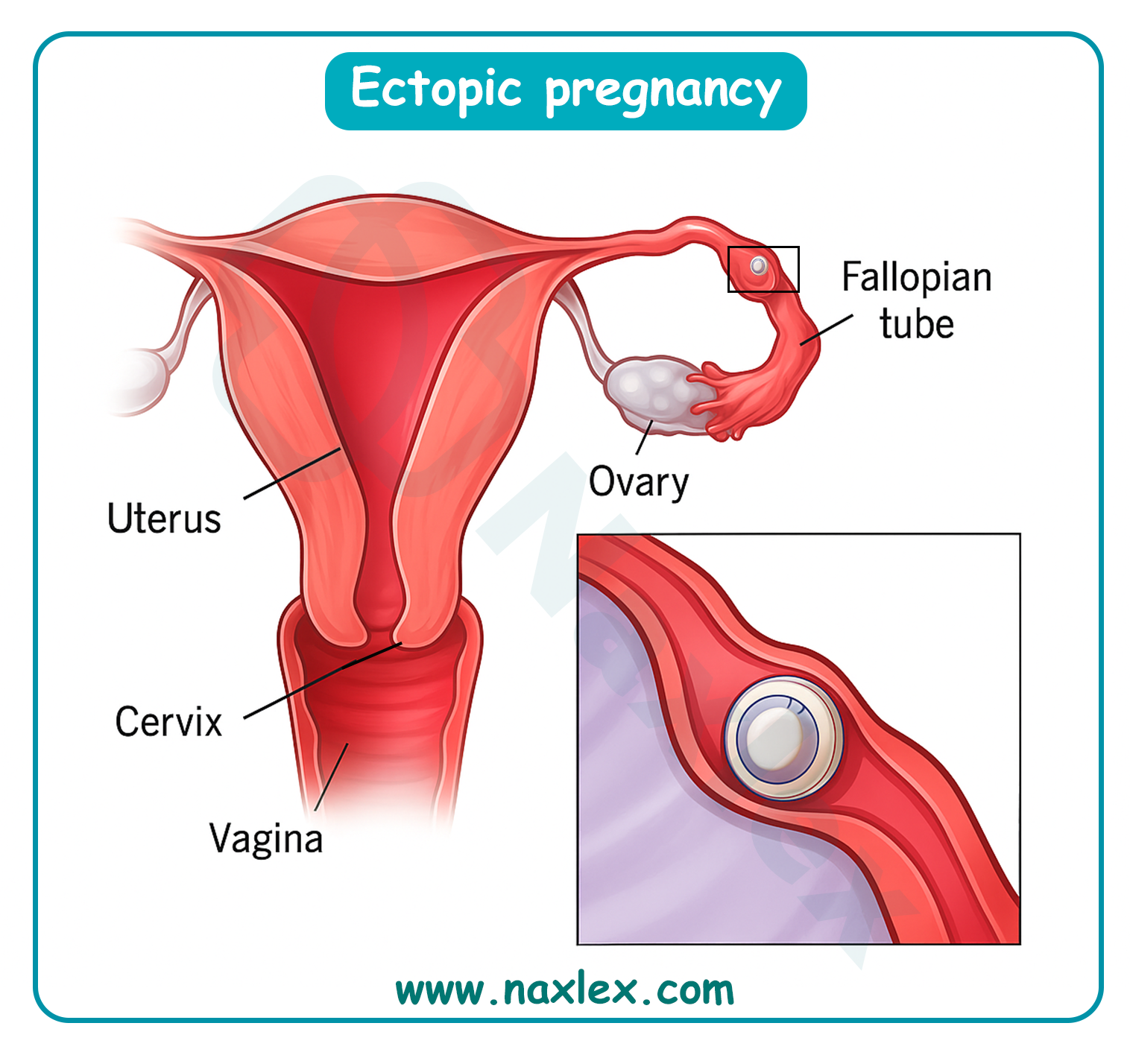
1.1 Definition and Pathophysiology
Ectopic pregnancy is delineated as the aberrant implantation of a fertilized ovum exterior to the uterine endometrial cavity, with approximately 97% of instances occurring within the fallopian tube, encompassing ampullary (70%), isthmic (12%), fimbrial (11%), and interstitial (2-3%) segments. Extratubal sites, comprising ovarian, abdominal, cervical, and cesarean scar implantations, account for the residual 3%, each engendering distinctive pathophysiological sequelae and management imperatives.
- Pathophysiological mechanisms:
- The primordial etiology resides in impeded zygotic transit through the fallopian tube, attributable to ciliary dysfunction, muscular dysmotility, or anatomical obstructions, precipitating premature trophoblastic invasion and implantation within the tubal mucosa.
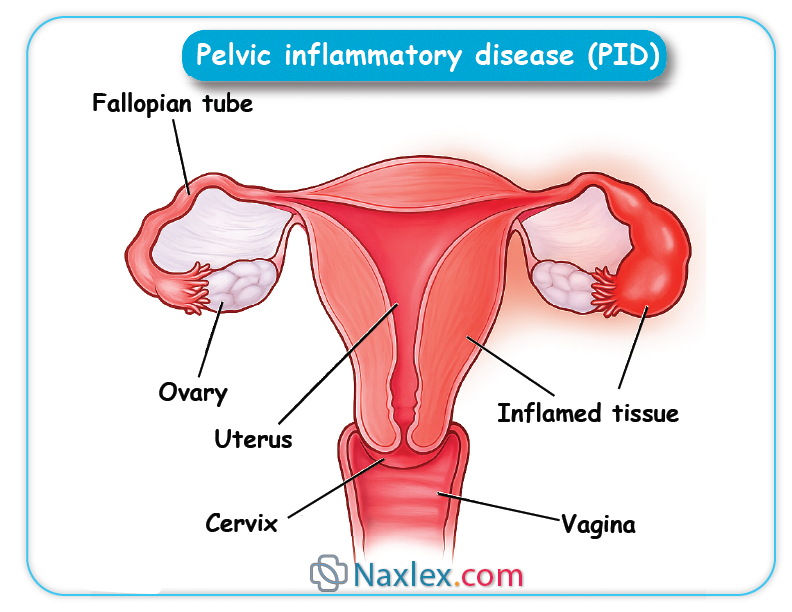
- Inflammatory perturbations, such as those induced by Chlamydia trachomatis or Neisseria gonorrhoeae, engender salpingitis, culminating in ciliary epithelial damage, intraluminal adhesions, and hydrosalpinx formation, thereby retarding embryonic progression and fostering ectopic nidation.
- Hormonal disequilibria, including elevated progesterone levels from progestin-only contraceptives or luteal phase defects, attenuate tubal peristalsis and ciliary beat frequency, augmenting the propensity for tubal implantation.
- Trophoblastic proliferation within the confined tubal lumen elicits distension, vascular erosion, and potential rupture, instigating hemoperitoneum and hypovolemic shock.
- In extratubal ectopics, such as ovarian pregnancies, implantation ensues upon fertilization within the ovarian cortex or peritoneal surface, adhering to Spiegelberg's criteria: intact ipsilateral tube, fetal sac occupying ovarian position, tubo-ovarian ligament connection, and histologically confirmed ovarian tissue.
- Cesarean scar ectopics arise from implantation within myometrial dehiscence at prior hysterotomy sites, potentially evolving into placenta accreta spectrum disorders if undiagnosed.
Nursing Insights
- Nurses must apprehend that ectopic pregnancy predominantly manifests in the fallopian tube's ampullary segment, where the luminal diameter permits initial embryonic growth prior to symptomatic presentation.
- Recognition of inflammatory etiologies, such as pelvic inflammatory disease, mandates nurses to elicit comprehensive sexual histories to identify at-risk patients during initial assessments.
- Comprehension of hormonal influences on tubal motility equips nurses to counsel patients on the augmented ectopic risk associated with progestin-based contraceptives.
- Awareness of extratubal variants, like cesarean scar ectopics, prompts nurses to scrutinize obstetric histories for prior cesarean deliveries in symptomatic patients.
1.2 Risk Factors
Risk factors for ectopic pregnancy encompass a multifarious array of anatomical, infectious, hormonal, and iatrogenic elements that compromise fallopian tube integrity and functionality, escalating the incidence from the baseline 1-2% in the general populace to substantially higher strata in predisposed cohorts.
- Tubal pathology and surgical history:
- Prior pelvic inflammatory disease (PID), engendered by ascending chlamydial or gonococcal infections, inflicts irreversible tubal scarring, amplifying risk sixfold.
-
- Previous ectopic pregnancy confers a 10-15% recurrence risk, escalating to 25% following two incidents, attributable to persistent tubal aberrations.
- Tubal reconstructive surgery, including salpingostomy or salpingectomy, predisposes to ectopic implantation due to altered tubal architecture and ciliary impairment.
- Infectious and inflammatory contributors:
- Endometriosis induces peritubal adhesions and inflammatory milieux, hindering zygotic transit.
- History of sexually transmitted infections (STIs) correlates with tubal damage, necessitating serological screening in at-risk demographics.
- Hormonal and contraceptive influences:
- Progestin-only contraceptives, including intrauterine devices (IUDs), attenuate tubal motility, with 50% of IUD-associated pregnancies being ectopic.
- Assisted reproductive technologies (ART), such as in vitro fertilization (IVF), heighten risk threefold owing to multiple embryo transfers and underlying infertility etiologies.
- Demographic and lifestyle factors:
- Advanced maternal age (>35 years) correlates with diminished tubal function and cumulative exposure to risk elements.
- Cigarette smoking impairs ciliary activity via nicotine-induced vasoconstriction and oxidative stress, conferring a twofold risk elevation.
- Prior abdominal surgeries, including appendectomy or cesarean sections, may engender adhesions impeding tubal patency.
- Genetic and anatomical predispositions:
- Congenital tubal anomalies, such as diverticula or elongated tubes, inherently obstruct zygotic passage.
- Diethylstilbestrol (DES) exposure in utero historically augmented tubal malformations, though contemporary incidence wanes.
Nursing Insights
- Nurses must prioritize elicitation of PID history during antepartal assessments, as it constitutes the paramount modifiable risk factor amenable to prophylactic antibiotic therapy.
- Counseling on smoking cessation is imperative, given its dose-dependent augmentation of ectopic risk, with nurses facilitating nicotine replacement referrals for gravid patients.
- In patients utilizing IUDs, nurses should advocate for prompt pregnancy testing upon missed menses to expedite ectopic detection.
- Recognition of ART-associated risks mandates nurses to coordinate multidisciplinary care with reproductive endocrinologists for high-risk surveillance.
1.3 Clinical Manifestations
Clinical manifestations of ectopic pregnancy are insidious and protean, often masquerading as normal early gestation or other gynecologic pathologies, necessitating astute nursing vigilance for timely intervention.
- Primary symptoms:
- Unilateral lower abdominal pain, emanating from tubal distension or rupture, frequently colicky or sharp, intensifying with movement or palpation.
- Vaginal bleeding or spotting, typically scant and dark, arising from endometrial decidual shedding secondary to suboptimal hCG support.
- Shoulder-tip pain (Kehr's sign), indicative of diaphragmatic irritation from hemoperitoneum, heralding tubal rupture.
- Associated systemic symptoms:
- Dizziness, syncope, or orthostatic hypotension, reflective of hypovolemic compromise from intra-abdominal hemorrhage.
- Gastrointestinal perturbations, including nausea, vomiting, or diarrhea, attributable to peritoneal irritation or hormonal fluxes.
- Urinary frequency or dysuria, ensuing from bladder compression by adnexal masses.
- Advanced presentations:
- Hemodynamic instability, encompassing tachycardia, hypotension, and pallor, signifying massive hemoperitoneum post-rupture.
- Abdominal rigidity, rebound tenderness, or guarding, denoting peritonitis from blood extravasation.
- Atypical manifestations:
- In cervical ectopics, profuse painless bleeding predominates due to vascular erosion.
- Abdominal ectopics may present with fetal movements or acute abdomen from organ compression.
Nursing Insights
- Nurses must discern unilateral abdominal pain as a cardinal ectopic harbinger, prompting immediate β-hCG quantification and ultrasonographic evaluation.
- Elicitation of shoulder-tip pain during physical assessments signifies hemoperitoneum, necessitating emergent surgical consultation.
- Monitoring for syncope in ambulatory patients underscores the need for orthostatic vital signs to unmask occult hypovolemia.
- Recognition of gastrointestinal symptoms mandates differential consideration of appendicitis or ovarian torsion in diagnostic algorithms.
1.4 Diagnostic Evaluation
Diagnostic evaluation of ectopic pregnancy integrates biochemical assays, imaging modalities, and clinical correlation to affirm extrauterine implantation and appraise stability, circumventing misdiagnosis that could precipitate morbidity.
- Biochemical markers:
- Quantitative serum β-hCG assay, wherein subnormal doubling (less than 53% increment over 48 hours) or plateauing levels intimate ectopic gestation.
- Discriminatory zone threshold (1500-2000 mIU/mL) whereby absence of intrauterine sac on transvaginal ultrasound strongly suggests ectopy.
- Serum progesterone levels below 5 ng/mL corroborate nonviability, albeit nonspecific for localization.
- Imaging techniques:
- Transvaginal ultrasonography (TVUS), the diagnostic cornerstone, visualizing adnexal masses, extrauterine gestational sacs, or yolk sacs with 84-97% sensitivity.
- Color Doppler enhancement delineates trophoblastic vascularity (ring-of-fire sign) in tubal ectopics.
- Transabdominal ultrasound supplements for advanced gestations or abdominal ectopics, though less resolute.
- Magnetic resonance imaging (MRI) elucidates atypical implantations, such as interstitial or cesarean scar ectopics, via T2-weighted sequences.
- Invasive diagnostics:
- Culdocentesis, aspirating nonclotting blood from the cul-de-sac, confirms hemoperitoneum in ruptured cases, albeit infrequently employed.
- Diagnostic laparoscopy affords definitive visualization and therapeutic potential in equivocal scenarios.
- Differential diagnostic considerations:
- Exclusion of intrauterine pregnancy via TVUS, with pregnancy of unknown location (PUL) warranting serial β-hCG surveillance.
Nursing Insights
- Nurses must ensure patient preparation for TVUS, including bladder emptying and consent procurement, to optimize imaging quality.
- Interpretation of β-hCG trends necessitates nurses to schedule serial draws precisely 48 hours apart for accurate viability assessment.
- Advocacy for MRI in complex cases equips nurses to coordinate with radiologists for expeditious atypical ectopic delineation.
- In PUL scenarios, nurses implement vigilant monitoring protocols, educating patients on rupture warning signs to avert delays.
1.5 Nursing and Medical Interventions
Nursing and medical interventions for ectopic pregnancy prioritize hemodynamic stabilization, pregnancy termination, and fertility preservation, tailored to patient stability and gestational locale.
- Medical management:
- Methotrexate administration (50 mg/m² intramuscularly) for unruptured ectopics with β-hCG <5000 mIU/mL, adnexal mass <3.5 cm, and absent fetal cardiac activity, inhibiting folate-dependent trophoblastic proliferation.
- Single-dose protocol entails β-hCG monitoring on days 4 and 7, with >15% decline signifying success; two-dose regimen augments efficacy for higher-risk cases.
- Contraindications encompass hemodynamic instability, renal impairment (creatinine >1.3 mg/dL), or hepatic dysfunction (AST/ALT >2x upper limit).
- Surgical interventions:
- Laparoscopic salpingostomy evacuates the ectopic while conserving the tube, ideal for fertility-desirous patients with contralateral tube compromise.
- Salpingectomy excises the affected tube, preferred in recurrent ectopics or rupture scenarios.
- Laparotomy reserved for massive hemorrhage or surgical instability.
- Nursing interventions:
- Preoperative preparation includes NPO status, intravenous access for fluid resuscitation, and RhoGAM administration (300 mcg) for Rh-negative patients within 72 hours.
- Intraoperative monitoring encompasses vital signs, blood loss quantification, and analgesia provision.
- Postoperative care involves pain management, bleeding surveillance, and infection prophylaxis with cefazolin.
- Expectant management:
- Reserved for asymptomatic patients with β-hCG <200 mIU/mL and declining trends, entailing weekly β-hCG assays until resolution.
Nursing Insights
- Nurses administer methotrexate post-counseling on side effects (stomatitis, gastrointestinal distress), ensuring follow-up β-hCG compliance to detect treatment failure.
- Preparation for salpingostomy involves educating patients on fertility implications, with nurses facilitating reproductive counseling referrals.
- Intravenous fluid bolus (crystalloids 20 mL/kg) in unstable patients stabilizes hemodynamics prior to surgical transfer.
- RhoGAM prophylaxis mandates nurses to confirm Rh status expeditiously to avert isoimmunization in subsequent pregnancies.
1.6 Complications (Rupture, Hemorrhagic Shock, Future Fertility)
Complications of ectopic pregnancy principally encompass tubal rupture, hemorrhagic shock, and impaired future fertility, mandating proactive nursing surveillance and mitigative strategies.
- Tubal rupture:
- Occurs in 15-20% of ectopics, precipitating hemoperitoneum from trophoblastic erosion of tubal vasculature, manifesting as acute abdominal agony and peritonitis.
- Risk escalates with β-hCG >5000 mIU/mL or adnexal mass >3 cm.
- Hemorrhagic shock:
- Ensues from voluminous intraperitoneal bleeding (up to 2 liters), evoking class III/IV shock with tachycardia (>120 bpm), hypotension (<90 mmHg systolic), oliguria, and altered mentation.
- Management entails massive transfusion protocol activation, with packed red blood cells, fresh frozen plasma, and platelets in 1:1:1 ratio.
- Impact on future fertility:
- Post-ectopic infertility afflicts 30-50% of patients, attributable to tubal scarring, adhesions, or contralateral tube involvement.
- Salpingectomy halves fertility rates compared to salpingostomy, though recurrence risk diminishes.
- Chronic pelvic pain or dyspareunia may ensue from pelvic adhesions.
- Other sequelae:
- Sepsis from infected hemoperitoneum or post-surgical infection, necessitating broad-spectrum antibiotics.
- Psychological ramifications, including anxiety or post-traumatic stress, warranting mental health referrals.
Nursing Insights
- Nurses monitor for rupture via serial abdominal exams, alerting for rebound tenderness indicative of peritonitis.
- In hemorrhagic shock, nurses initiate large-bore IV access and crystalloid infusion while preparing for blood product administration.
- Fertility counseling post-salpingectomy involves discussing IVF options, with nurses coordinating endocrinologist consultations.
- Surveillance for sepsis includes temperature monitoring and prompt antibiotic initiation for fever >38.3°C.
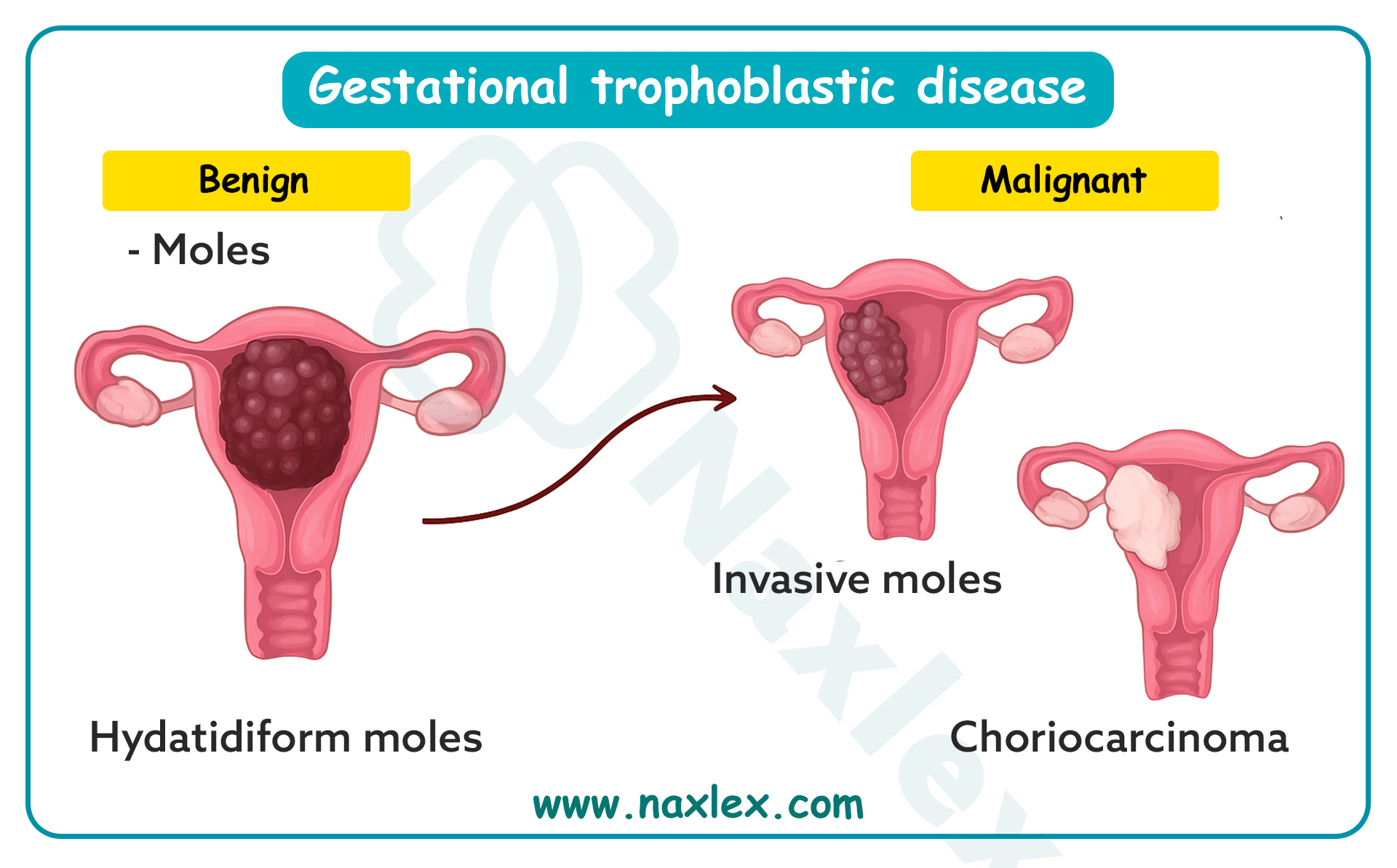
Gestational Trophoblastic Disease (Hydatidiform Mole)
Gestational trophoblastic disease (GTD) encompasses a spectrum of proliferative disorders originating from placental trophoblastic tissue, with hydatidiform mole representing the benign antecedent characterized by aberrant villous edema and trophoblastic hyperplasia. This pathological entity poses significant risks for malignant transformation and maternal complications, necessitating vigilant nursing surveillance and multidisciplinary management in maternal-newborn care. The subsequent sections delineate the definition, pathophysiology, clinical presentation, diagnostic workup, management strategies, long-term surveillance, and patient education facets of hydatidiform mole, equipping nursing students with a comprehensive, scientifically rigorous framework for clinical proficiency and patient advocacy.
1.1 Definition and Pathophysiology
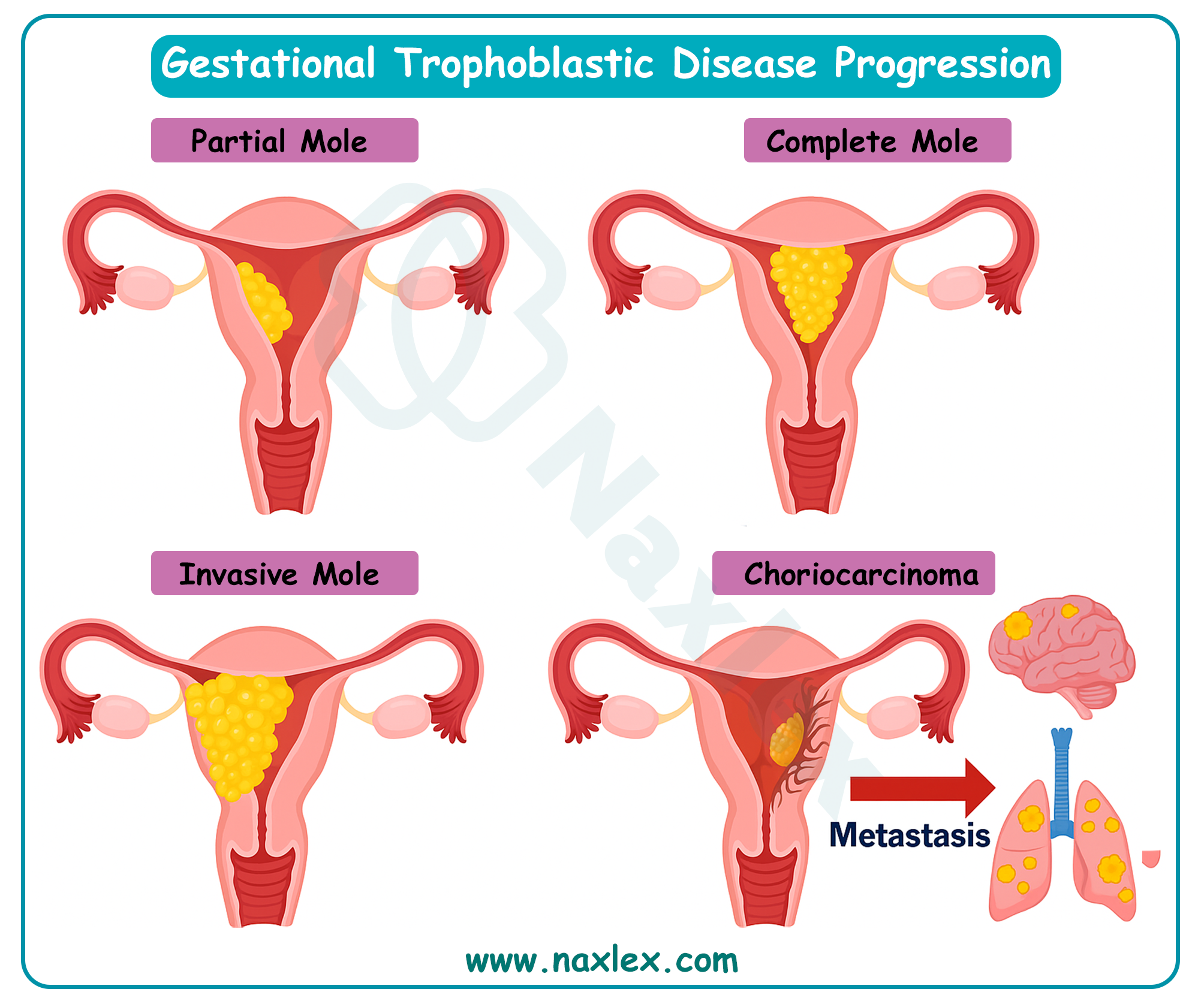
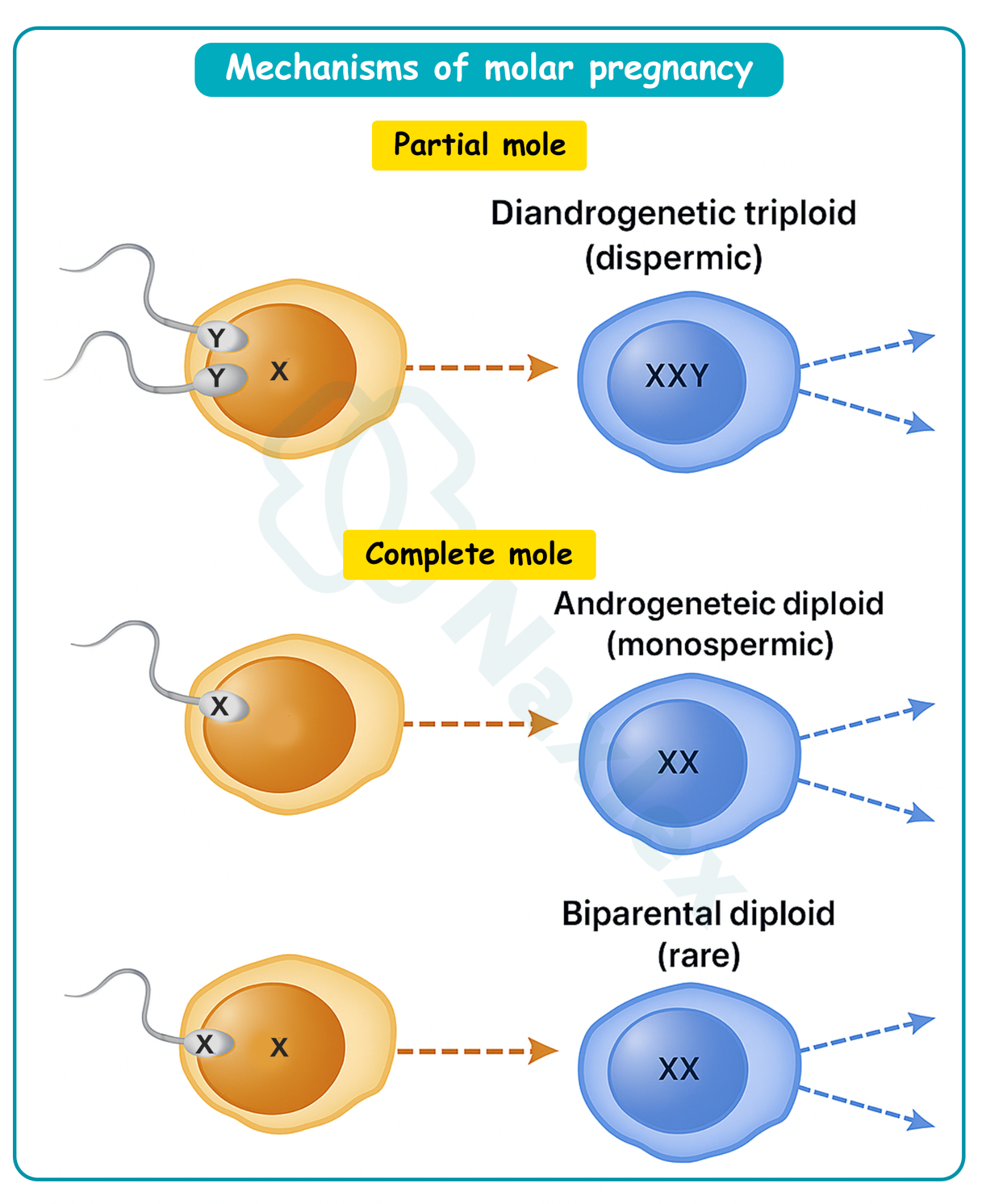
Gestational trophoblastic disease is defined as a heterogeneous group of neoplastic disorders arising from anomalous trophoblastic proliferation, with hydatidiform mole constituting a premalignant variant manifesting as cystic degeneration of chorionic villi and exuberant syncytiotrophoblastic and cytotrophoblastic hyperplasia. Complete moles exhibit diploid androgenetic karyotypes devoid of fetal tissue, whereas partial moles display triploid karyotypes with rudimentary fetal elements, both culminating in placental malformation and potential metastatic sequelae.
- Genetic underpinnings:
- Complete hydatidiform moles predominantly harbor a 46,XX karyotype derived from paternal duplication of a haploid sperm fertilizing an anucleate ovum, or rarely 46,XY from dispermic fertilization, resulting in absent maternal genomic contribution and universal trophoblastic hyperplasia.
- Partial hydatidiform moles arise from dispermic fertilization of a haploid ovum, yielding a 69,XXY or 69,XXX triploid karyotype, incorporating both maternal and paternal genomes, and manifesting focal villous edema with identifiable fetal structures.
-
- Molecular aberrations, including paternal uniparental disomy or imprinting defects in genes like NLRP7 and KHDC3L, predispose to recurrent moles, particularly in familial biparental complete moles.
- Pathophysiological progression:
- Trophoblastic hyperplasia engenders excessive human chorionic gonadotropin (hCG) secretion, precipitating theca lutein cysts, hyperthyroidism, and early-onset preeclampsia via angiogenic dysregulation.
- Villous stromal edema and cistern formation disrupt placental architecture, impeding embryonic development and fostering grape-like vesicular clusters.
- Invasive potential manifests as myometrial penetration in invasive moles, or distant metastases in choriocarcinoma, driven by unchecked cytotrophoblastic invasion and vascular remodeling.
- Epidemiological correlates:
- Incidence approximates 1 in 1000 pregnancies in Western nations, escalating to 1 in 400 in Asian populations, attributable to dietary folate deficiencies or genetic predispositions.
Nursing Insights
- Nurses must distinguish complete from partial moles genetically, as complete variants harbor higher malignant transformation risks, guiding intensified surveillance protocols.
- Recognition of hCG-driven hyperthyroidism mandates thyroid function assessment in symptomatic patients to avert thyrotoxicosis complications.
- Awareness of familial recurrent moles prompts genetic counseling referrals for affected patients, facilitating preconception risk mitigation.
- Comprehension of villous edema mechanisms equips nurses to anticipate vesicular passage, preparing patients for potential expulsion events.
1.2 Clinical Presentation
Clinical presentation of hydatidiform mole typically emerges in the first trimester, characterized by exaggerated gestational symptoms secondary to supraphysiologic hCG levels and uterine distension, often mimicking normal pregnancy or miscarriage but distinguished by hallmark vesicular expulsion and multisystemic manifestations.
- Primary obstetric symptoms:
- Vaginal bleeding, ranging from spotting to profuse hemorrhage, arises from trophoblastic erosion of endometrial vessels, often accompanied by passage of grape-like hydropic villi.
- Uterine size-date discrepancy, with fundal height exceeding gestational age by 4-6 cm, attributable to molar tissue proliferation and theca lutein cyst formation.
- Absence of fetal heart tones or movements, reflecting embryonic demise or absence in complete moles.
- Endocrine and systemic manifestations:
- Severe hyperemesis gravidarum, induced by elevated hCG stimulating chemoreceptor trigger zones and gastric dysmotility.
- Hyperthyroidism, presenting with tachycardia, tremors, and heat intolerance, secondary to hCG's thyrotropin-like activity on thyroid-stimulating hormone receptors.
- Early preeclampsia before 20 weeks, manifesting as hypertension (>140/90 mmHg), proteinuria, and edema, driven by angiogenic imbalance with elevated soluble fms-like tyrosine kinase-1 (sFlt-1).
- Rare presentations:
- Respiratory distress from trophoblastic embolization or hyperthyroidism-induced high-output cardiac failure.
- Ovarian torsion secondary to enlarged theca lutein cysts (>6 cm), eliciting acute abdominal pain.
- Asymptomatic detection:
- Incidental ultrasonographic identification during routine antenatal screening, revealing characteristic snowstorm patterns.
Nursing Insights
- Nurses must quantify vaginal bleeding via pad counts to gauge hemorrhagic risk, intervening promptly for hemodynamic instability.
- Palpation for uterine size discrepancies during examinations alerts nurses to molar suspicion, prompting expeditious ultrasonographic referral.
- Assessment for hyperemesis involves electrolyte monitoring to prevent dehydration and metabolic derangements in affected patients.
- Vigilance for preeclamptic signs pre-20 weeks distinguishes moles from normal gestations, facilitating antihypertensive initiation.
1.3 Diagnostic Workup
Diagnostic workup for hydatidiform mole integrates biochemical assays, imaging modalities, and histopathological confirmation to differentiate from viable pregnancies or other gestational pathologies, ensuring accurate classification and risk stratification.
- Biochemical evaluations:
- Quantitative serum hCG exceeding 100,000 mIU/mL, disproportionately elevated for gestational age, reflecting trophoblastic hyperactivity.
- Thyroid function tests revealing suppressed thyroid-stimulating hormone and elevated free thyroxine, corroborating hCG-induced thyrotoxicosis.
- Complete blood count and coagulation profile to assess anemia or disseminated intravascular coagulation from hemorrhagic complications.
- Imaging modalities:
- Transvaginal ultrasonography, the diagnostic mainstay, depicting a heterogeneous intrauterine mass with cystic spaces (snowstorm appearance) sans fetal structures in complete moles, or focal cystic changes with fetal remnants in partial moles.
- Doppler ultrasonography identifies absent fetal heartbeat and augmented vascularity surrounding the molar tissue.
- Chest radiography screens for pulmonary metastases in suspected invasive disease, manifesting as cannonball lesions.
- Histopathological confirmation:
- Post-evacuation tissue examination reveals edematous villi with central cisterns, trophoblastic proliferation, and karyotypic analysis (diploid vs. triploid).
- Immunohistochemical staining for p57 (absent in complete moles due to paternal imprinting) differentiates complete from partial variants.
- Differential diagnostics:
- Exclusion of multiple gestation or anembryonic pregnancy via ultrasound, with serial hCG trends distinguishing nonviable intrauterine pregnancies.
Nursing Insights
- Nurses facilitate hCG sampling, educating patients on the necessity of serial measurements to monitor disease regression post-evacuation.
- Preparation for ultrasonography involves bladder management and consent, optimizing visualization of molar characteristics.
- Coordination of histopathological submissions ensures timely karyotyping, informing malignancy risk assessments.
- Interpretation of chest radiographs in high-risk patients prompts nurses to advocate for oncologic consultations upon metastatic detection.
1.4 Management and Interventions
Management of hydatidiform mole prioritizes uterine evacuation, complication mitigation, and prevention of malignant progression, employing surgical, pharmacological, and supportive interventions tailored to molar subtype and patient stability.
- Surgical interventions:
- Suction dilation and curettage (D&C) under ultrasonographic guidance constitutes the primary evacuative modality, minimizing perforation risks and ensuring comprehensive molar tissue removal.
- Hysterectomy reserved for patients with completed childbearing or invasive disease, obviating surveillance needs but preserving ovaries.
- Pharmacological management:
- Prophylactic uterotonics (oxytocin or methylergonovine) post-evacuation to avert atony-induced hemorrhage.
- RhoGAM administration (300 mcg) for Rh-negative patients to preclude isoimmunization from fetal-maternal hemorrhage.
- Chemoprophylaxis with methotrexate in high-risk complete moles (e.g., hCG >100,000 mIU/mL) to mitigate persistent disease, though controversial due to toxicity.
- Supportive care:
- Fluid resuscitation and blood transfusion for hemorrhagic shock, guided by hemoglobin levels and vital signs.
- Antihypertensives (labetalol or hydralazine) for preeclamptic management, with magnesium sulfate for seizure prophylaxis.
- Risk-stratified approaches:
- Partial moles managed conservatively with D&C, given lower malignant potential (5%) versus complete moles (15-20%).
Nursing Insights
- Nurses administer uterotonics post-D&C, monitoring for contractile efficacy to prevent postpartum hemorrhage.
- RhoGAM dosing requires Rh status confirmation, with nurses documenting administration to safeguard future pregnancies.
- Fluid balance assessment in preeclamptic patients prevents pulmonary edema from overhydration.
- Advocacy for chemoprophylaxis in select cases involves toxicity education, ensuring informed consent.
1.5 Long-Term Follow-Up and Surveillance
Long-term follow-up and surveillance post-molar evacuation are imperative to detect persistent gestational trophoblastic neoplasia (GTN) or choriocarcinoma, employing serial hCG monitoring and contraceptive counseling to preclude confounding pregnancies.
- hCG surveillance protocols:
- Weekly quantitative hCG assays until three consecutive normal levels (<5 mIU/mL), followed by monthly assessments for 6-12 months, with plateauing or rising titers indicating GTN.
- Urinary hCG testing supplements serum assays for patient convenience in resource-limited settings.
- Imaging and laboratory follow-up:
- Baseline chest X-ray post-evacuation, with computed tomography or magnetic resonance imaging for suspected metastases (e.g., pulmonary, hepatic).
- Thyroid function normalization monitoring in hyperthyroid cases, with levothyroxine if persistent.
- Contraceptive mandates:
- Hormonal contraception (excluding IUDs initially) for 6-12 months to avert pregnancy interference with hCG surveillance.
- Malignancy risk stratification:
- High-risk features (age >40, hCG >100,000 mIU/mL, uterine size >20 weeks) warrant intensified monitoring and potential prophylactic chemotherapy.
Nursing Insights
- Nurses schedule hCG follow-ups, educating patients on compliance to detect GTN early, preventing metastatic dissemination.
- Contraceptive counseling emphasizes barrier methods initially, transitioning to hormonal agents post-normalization.
- Monitoring for metastatic symptoms (e.g., hemoptysis) prompts urgent imaging referrals.
- Documentation of surveillance adherence ensures continuity in multidisciplinary care.
1.6 Patient Education and Emotional Support
Patient education and emotional support in hydatidiform mole encompass malignancy risk elucidation, surveillance adherence, and psychosocial interventions to ameliorate grief and anxiety associated with pregnancy loss and oncologic potential.
- Educational components:
- Instruction on recognizing GTN signs (persistent bleeding, abdominal pain) and the imperative of contraceptive compliance to facilitate hCG monitoring.
- Counseling on future pregnancy deferral for 6-12 months post-normal hCG, with preconception folate supplementation to mitigate recurrence.
- Emotional support strategies:
- Validation of grief through active listening, acknowledging the dual loss of pregnancy and malignancy threat.
- Referral to support groups or psychologists for coping with anxiety, particularly in recurrent cases.
- Cultural and holistic considerations:
- Tailoring education to cultural beliefs, incorporating family involvement where appropriate.
- Provision of written resources and follow-up calls to reinforce teaching and assess emotional well-being.
Nursing Insights
- Nurses educate on GTN warning signs, empowering patients for self-monitoring and prompt reporting.
- Grief validation involves empathetic phrasing, such as "Your feelings are valid," fostering therapeutic alliances.
- Contraceptive education includes efficacy discussions, ensuring patient autonomy in method selection.
- Follow-up calls assess adherence and emotional status, facilitating timely interventions.
Nursing Management Of Pregnancy Bleeding
Nursing management of pregnancy bleeding encompasses a systematic approach to assessment, stabilization, pharmacological administration, fluid resuscitation, and psychosocial support to mitigate maternal morbidity and mortality associated with conditions such as spontaneous abortion, ectopic pregnancy, and gestational trophoblastic disease. Nurses play a pivotal role in orchestrating timely interventions, coordinating multidisciplinary care, and advocating for patient-centered outcomes in the context of early pregnancy complications. The following sections elucidate the comprehensive nursing strategies for initial assessment, emergency interventions, pharmacological management, fluid replacement, and patient education, providing a scientifically robust foundation for nursing students to excel in maternal-newborn care.
1.1 Initial Nursing Assessment of a Patient with Bleeding
Initial nursing assessment of a patient presenting with vaginal bleeding in early pregnancy is a critical step to determine the etiology, severity, and urgency of intervention, integrating subjective history, objective physical findings, and diagnostic adjuncts to formulate a differential diagnosis and guide care.
- Subjective assessment:
- Elicit a detailed obstetric history, including gestational age, last menstrual period, gravidity, parity, and prior pregnancy losses or ectopic pregnancies.
- Quantify bleeding characteristics, including onset, duration, volume (number of pads soaked per hour), color, and presence of clots or tissue passage.
- Ascertain associated symptoms, such as abdominal pain (location, quality, intensity), shoulder pain, syncope, nausea, or loss of pregnancy symptoms.
- Review risk factors, including smoking, pelvic inflammatory disease, assisted reproductive technology use, or history of uterine anomalies.
- Objective physical examination:
- Measure vital signs (pulse, blood pressure, respiratory rate, temperature) to detect tachycardia (>100 bpm), hypotension (<90/60 mmHg), or fever (>100.4°F).
- Perform abdominal palpation to assess for tenderness, guarding, rebound, or uterine size-date discrepancies suggestive of molar pregnancy.
- Conduct a speculum examination to evaluate cervical os status (open vs. closed), bleeding source (cervical vs. uterine), and presence of vesicular tissue.
- Execute a bimanual examination to assess uterine size, adnexal masses, or tenderness indicative of ectopic pregnancy.
- Diagnostic support:
- Order quantitative serum β-human chorionic gonadotropin (β-hCG) levels to evaluate pregnancy viability, with subnormal doubling (<53% over 48 hours) suggesting ectopic or nonviable gestation.
- Arrange transvaginal ultrasonography to confirm intrauterine pregnancy, identify ectopic masses, or visualize molar snowstorm patterns.
- Obtain complete blood count (CBC) to assess hemoglobin and hematocrit for anemia, and blood type with Rh factor for isoimmunization risk.
- Collect coagulation profiles (PT/INR, aPTT) to rule out disseminated intravascular coagulation in prolonged missed abortions or molar pregnancies.
Nursing Insights
- Quantification of bleeding via pad counts (e.g., soaking >2 pads/hour indicates heavy bleeding) guides urgency of escalation to obstetric providers.
- Assessment of shoulder pain during history-taking prompts immediate suspicion of hemoperitoneum from ectopic rupture, necessitating urgent ultrasound.
- Accurate documentation of cervical os status during speculum exam differentiates threatened from inevitable miscarriage, informing management.
- Obtaining obstetric history, including prior ectopic pregnancies, heightens vigilance for recurrence, prompting expedited β-hCG and imaging.
1.2 Emergency Nursing Interventions for Hemodynamic Instability
Emergency nursing interventions for hemodynamic instability in pregnancy bleeding focus on rapid stabilization, hemorrhage control, and preparation for definitive treatment to avert hypovolemic shock and maternal mortality, particularly in ectopic rupture or severe miscarriage-related hemorrhage.
- Immediate stabilization measures:
- Position the patient supine with legs elevated to enhance venous return, unless contraindicated by respiratory distress.
- Administer high-flow oxygen (10-15 L/min via non-rebreather mask) to optimize tissue perfusion in hypovolemic states.
- Establish large-bore intravenous access (16-18 gauge, two lines) for rapid fluid administration and potential blood transfusion.
- Hemorrhage control:
- Monitor bleeding via pad counts and visual estimation, reporting saturation of >2 pads/hour or passage of large clots (>5 cm).
- Administer uterotonics (e.g., oxytocin 20 units in 1 L normal saline at 125 mL/hour) as ordered to promote uterine contraction in miscarriage-related bleeding.
- Prepare for emergent surgical intervention (e.g., dilation and curettage, laparoscopy) in cases of persistent hemorrhage or ectopic rupture.
- Hemodynamic monitoring:
- Continuously monitor vital signs every 5-15 minutes, noting tachycardia (>120 bpm), hypotension (<90 mmHg systolic), or oliguria (<30 mL/hour).
- Assess for signs of shock, including pallor, cool clammy skin, altered mentation, or delayed capillary refill (>2 seconds).
- Initiate continuous pulse oximetry and electrocardiography to detect hypoxia or arrhythmias secondary to hypovolemia.
- Coordination of care:
- Alert obstetric and surgical teams for immediate consultation in cases of suspected rupture or massive hemorrhage.
- Prepare for transfer to operating room or intensive care unit if class III/IV shock (blood loss >1500 mL) is evident.
Nursing Insights
- Rapid establishment of IV access with two large-bore catheters ensures adequate fluid delivery, critical for stabilizing hypovolemic patients.
- Continuous vital sign monitoring every 5 minutes in unstable patients detects deteriorating trends, prompting immediate escalation.
- Administration of oxygen enhances oxygen delivery to tissues, mitigating hypoxic injury during hemorrhagic shock.
- Accurate communication of bleeding volume to surgical teams facilitates timely operative intervention, reducing maternal morbidity.
1.3 Pharmacological Management (e.g., Rh Immune Globulin, Misoprostol, Methotrexate)
Pharmacological management in pregnancy bleeding employs targeted medications to prevent isoimmunization, facilitate uterine evacuation, or treat ectopic pregnancies, with nursing responsibilities encompassing administration, monitoring, and patient education.
- Rh immune globulin (RhoGAM):
- Administered intramuscularly (300 mcg) within 72 hours to Rh-negative patients with bleeding to prevent alloimmunization from fetal-maternal hemorrhage.
-
- Indications include miscarriage, ectopic pregnancy, molar pregnancy, or invasive procedures (e.g., D&C).
- Dosage adjustments (e.g., microdose 50 mcg for <12 weeks gestation) depend on gestational age and bleeding volume.
- Misoprostol:
- Utilized (800 mcg vaginally, buccally, or sublingually) to induce uterine contractions in incomplete or inevitable miscarriages, promoting expulsion of retained products.
- Side effects include severe cramping, nausea, diarrhea, and fever, necessitating pre-administration antiemetics (e.g., ondansetron) and analgesics (e.g., ibuprofen 800 mg).
- Contraindications include pelvic infection or known hypersensitivity.
- Methotrexate:
- Administered intramuscularly (50 mg/m²) for unruptured ectopic pregnancies with β-hCG <5000 mIU/mL, adnexal mass <3.5 cm, and no fetal cardiac activity.
- Inhibits folate-dependent trophoblastic proliferation, requiring serial β-hCG monitoring (days 4 and 7) for >15% decline to confirm efficacy.
- Side effects include stomatitis, gastrointestinal distress, and rare hepatotoxicity, necessitating baseline liver function tests.
- Supportive medications:
- Antibiotics (e.g., doxycycline 100 mg BID for 7 days) for infection prophylaxis post-D&C or in septic abortions.
- Uterotonics (e.g., methylergonovine 0.2 mg IM every 2-4 hours) to control post-evacuation hemorrhage from uterine atony.
Nursing Insights
- Verification of Rh status prior to RhoGAM administration prevents unnecessary dosing and ensures timely prophylaxis for isoimmunization prevention.
- Patient education on misoprostol includes expected cramping and bleeding within 4-6 hours, with instructions to report excessive bleeding (>2 pads/hour).
- Monitoring methotrexate patients involves assessing for abdominal pain post-dose, indicating potential ectopic rupture, and ensuring follow-up β-hCG compliance.
- Administration of prophylactic antibiotics pre-D&C reduces endometritis risk, with nurses confirming patient allergies to avoid adverse reactions.
1.4 Fluid and Blood Replacement Therapy
Fluid and blood replacement therapy is a cornerstone of managing pregnancy bleeding with significant blood loss, aiming to restore intravascular volume, maintain tissue perfusion, and correct anemia or coagulopathy in conditions like ectopic rupture or molar hemorrhage.
- Fluid resuscitation:
- Initiate crystalloid infusion (normal saline or lactated Ringer’s) at 20 mL/kg bolus for hypotension or tachycardia, titrating to stabilize blood pressure (>90 mmHg systolic).
- Monitor fluid balance to prevent overload, assessing for pulmonary edema (crackles, dyspnea) or renal compromise (urine output <30 mL/hour).
- Use warmed fluids to prevent hypothermia in massive hemorrhage scenarios.
- Blood transfusion:
- Transfuse packed red blood cells (PRBCs) for hemoglobin <7 g/dL or symptomatic anemia (e.g., syncope, dyspnea), targeting hemoglobin >8 g/dL.
- Administer fresh frozen plasma (FFP) and platelets in a 1:1:1 ratio with PRBCs for massive transfusion protocols in class III/IV shock (>1500 mL loss).
- Crossmatch blood products, confirming compatibility and monitoring for transfusion reactions (fever, urticaria, hemolysis).
- Coagulopathy management:
- Assess for disseminated intravascular coagulation (DIC) in prolonged missed abortions or molar pregnancies, monitoring fibrinogen (<200 mg/dL), D-dimer, and platelet counts.
- Administer cryoprecipitate or fibrinogen concentrates for hypofibrinogenemia, guided by coagulation studies.
- Monitoring and evaluation:
- Perform serial CBCs to track hemoglobin trends post-transfusion, ensuring resolution of anemia.
- Evaluate hemodynamic response via vital signs and urine output, adjusting infusion rates accordingly.
Nursing Insights
- Nurses initiate crystalloid boluses promptly in hypotensive patients, monitoring urine output to confirm adequate renal perfusion.
- Crossmatching for blood products requires accurate patient identification to prevent transfusion errors, with nurses verifying labels at bedside.
- Assessment for transfusion reactions involves monitoring vital signs every 15 minutes during initial PRBC infusion, stopping transfusion for fever or chills.
- Documentation of fluid input/output and transfusion volumes ensures precise tracking, guiding multidisciplinary fluid management decisions.
1.5 Patient Education, Counseling, and Supportive Care
Patient education, counseling, and supportive care in pregnancy bleeding address physical recovery, emotional processing, and future reproductive planning, fostering informed decision-making and psychosocial resilience in patients experiencing miscarriage, ectopic pregnancy, or molar pregnancy.
- Physical recovery education:
- Instruct on expected bleeding patterns (light spotting for 1-2 weeks post-miscarriage or D&C) and warning signs (soaking >2 pads/hour, fever >100.4°F, foul discharge).
- Advise pelvic rest (no intercourse, tampons, or douching) for 2-4 weeks to prevent infection or cervical trauma.
- Recommend activity restrictions, avoiding heavy lifting (>10 lbs) for 1 week post-procedure to minimize bleeding risk.
- Emotional and psychosocial support:
- Employ active listening and validate emotions (e.g., grief, guilt, anger), acknowledging the individual nature of pregnancy loss experiences.
- Refer to grief counseling or support groups for patients exhibiting prolonged distress or signs of depression.
- Involve partners or family members, with patient consent, to enhance support networks and reduce isolation.
- Reproductive planning:
- Counsel on contraception options (e.g., hormonal pills, IUDs) to prevent unintended pregnancies, particularly in molar pregnancies requiring 6-12 months hCG surveillance.
- Discuss fertility prospects, reassuring patients that one miscarriage does not significantly increase future risk, but recurrent losses warrant specialist referral.
- Educate on preconception folate supplementation (400-800 mcg daily) to reduce recurrence in molar or spontaneous abortions.
- Follow-up care:
- Schedule follow-up visits 1-2 weeks post-event for hCG monitoring, ultrasound, or complication assessment.
- Provide written discharge instructions and 24/7 contact numbers for reporting complications like persistent bleeding or fever.
Nursing Insights
- Education on warning signs empowers patients to seek timely care for complications like infection or hemorrhage, reducing morbidity.
- Active listening during counseling builds trust, encouraging patients to express fears about future pregnancies or malignancy risks.
- Contraceptive counseling post-molar pregnancy emphasizes barrier methods initially to avoid confounding hCG results, transitioning to long-acting options.
- Scheduling follow-up hCG tests ensures compliance, with nurses reinforcing the importance of detecting persistent trophoblastic disease.
Summary
Pregnancy bleeding, encompassing implantation bleeding, spontaneous abortion, induced abortion, ectopic pregnancy, gestational trophoblastic disease (GTD), and comprehensive nursing management, represents a critical domain in maternal-newborn nursing, requiring precise assessment, timely interventions, and empathetic psychosocial support to mitigate maternal morbidity and emotional distress. Implantation bleeding, a benign process occurring 6-12 days post-conception due to blastocyst embedding, presents as light, self-limiting spotting, distinguished from pathological bleeding (e.g., miscarriage, ectopic) through clinical history, transvaginal ultrasound, and β-hCG monitoring; nurses reassure patients and educate on warning signs like heavy bleeding or pain.
Spontaneous abortion, affecting 10-20% of pregnancies before 20 weeks, arises from chromosomal abnormalities, maternal conditions (e.g., diabetes), or lifestyle factors (e.g., smoking), with classifications including threatened (light bleeding, closed cervix), inevitable (open cervix, nonviable), incomplete (partial tissue expulsion), complete (full expulsion, empty uterus), missed (fetal demise without expulsion), and recurrent (≥3 losses). Nurses assess bleeding volume, cervical status, and perform diagnostics (ultrasound, β-hCG, CBC), administering misoprostol or preparing for D&C while providing RhoGAM for Rh-negative patients and counseling for grief; complications include hemorrhage, infection, and Asherman syndrome. Induced abortion, either therapeutic (e.g., maternal health risks) or elective, employs medical methods (mifepristone/misoprostol, methotrexate) or surgical techniques (vacuum aspiration, D&C, D&E), with nurses ensuring informed consent, monitoring for complications (e.g., uterine perforation), and offering contraception counseling post-procedure.
Ectopic pregnancy, primarily tubal (97%), results from impaired zygotic transit due to pelvic inflammatory disease, prior ectopics, or smoking, manifesting as unilateral pain, scant bleeding, or shoulder pain (hemoperitoneum); diagnostics involve β-hCG (subnormal doubling), ultrasound, and laparoscopy, with methotrexate for unruptured cases and salpingostomy/salpingectomy for rupture, while nurses monitor for hemorrhagic shock and reduced fertility (30-50%). Gestational trophoblastic disease, specifically hydatidiform mole, features villous edema and trophoblastic hyperplasia (complete: diploid, no fetus; partial: triploid, fetal remnants), presenting with bleeding, vesicle passage, hyperemesis, and early preeclampsia; suction D&C is primary, with hCG surveillance for 6-12 months to detect persistent neoplasia, and nurses educate on contraception and GTN signs. Nursing management of pregnancy bleeding integrates initial assessment (history, vitals, speculum exam), emergency interventions (oxygen, IV access, uterotonics), pharmacological administration (RhoGAM within 72 hours, misoprostol, methotrexate), and fluid/blood replacement for hypovolemia, with crystalloids and transfusions guided by hemoglobin and vital signs.
Nurses educate on bleeding expectations, pelvic rest, and complication signs (fever, foul discharge), employing active listening to validate grief and referring for counseling, while ensuring follow-up for hCG monitoring and contraception planning. Practice questions across sections emphasize symptom recognition (e.g., shoulder pain for ectopic rupture), interventions (e.g., D&C for molar pregnancy), and risk factors (e.g., PID, smoking), reinforcing clinical acumen. Comprehensive questions cover miscarriage causes (chromosomal abnormalities), uterine anomalies (septate uterus, Asherman syndrome), and post-procedure care, ensuring no overlap with prior questions. This holistic framework equips nursing students to navigate the complexities of pregnancy bleeding, balancing scientific precision with compassionate care to optimize maternal outcomes and emotional resilience.
