
Please set your exam date
Drugs Used to Treat Angina Pectoris
Study Questions
Practice Questions 1
A client comes to the emergency department complaining of chest pains, which started 1 hour ago while he was mowing the lawn. Nitroglycerin was given sublingually as prescribed. Which of the following adverse reactions would be most likely to occur?
Explanation
The nurse is caring for a client experiencing acute angina and administering sublingual nitroglycerin, a vasodilator used to reduce myocardial oxygen demand by dilating peripheral and coronary blood vessels. Patient education and monitoring for adverse effects are essential because nitroglycerin can cause predictable hemodynamic and neurological responses due to its mechanism of action, particularly in the acute setting.
Rationale for correct answer:
D. Headache. Nitroglycerin causes vasodilation of cerebral blood vessels, which increases intracranial blood flow and can trigger a throbbing headache. This is the most common and expected adverse effect of sublingual nitroglycerin, often appearing within minutes of administration. The headache is generally self-limiting and nurses should reassure the client that mild to moderate headaches are anticipated and not dangerous.
Rationales for incorrect answers:
A. Hypotension. Although nitroglycerin can cause systemic vasodilation and a drop in blood pressure, a significant hypotensive event is less common with a single sublingual dose in otherwise stable clients. Nurses should still monitor blood pressure, but hypotension is not the most likely adverse reaction.
B. Dizziness. Dizziness may occur secondary to hypotension or orthostatic changes, but it is generally less frequent and less pronounced than the headache. Monitoring and assisting the client to sit or lie down can prevent injury if dizziness develops.
C. GI distress. Gastrointestinal upset is not a typical adverse effect of nitroglycerin. The medication acts primarily on vascular smooth muscle rather than the gastrointestinal tract, so nausea or abdominal discomfort is uncommon.
Test-taking strategy:
• Focus on the pharmacologic effects of nitroglycerin, particularly vasodilation.
• Identify the most common, expected adverse effect rather than less likely or secondary effects.
• Consider the route of administration (sublingual) and its rapid onset when evaluating expected side effects.
Take-home points:
• Headache is the most common and expected adverse effect of sublingual nitroglycerin.
• Monitor blood pressure and assist with position changes to prevent dizziness or falls.
• Educate clients that headaches indicate the drug is working, and adverse effects are usually transient.
The nurse is teaching a client who is prescribed nitroglycerin (Nitro-Dur) transdermal patch for angina pectoris. Which of the following instructions should the nurse give the client?
Explanation
Clients prescribed transdermal nitroglycerin (Nitro-Dur) patches for angina pectoris require education on proper application, timing, and nitrate-free intervals to prevent tolerance. Nitroglycerin patches deliver continuous vasodilatory therapy to reduce myocardial oxygen demand. However, prolonged exposure without a nitrate-free period can diminish efficacy. Teaching must also include site rotation, safe removal, and timing to maximize therapeutic effect and minimize adverse reactions such as headache or hypotension.
Rationale for the correct answer:
A. “Remove the patch each evening and replace it with a new patch in the morning.” Transdermal nitroglycerin should be applied once daily to a hairless area and removed after 12–14 hours to allow a nitrate-free interval, which prevents tolerance. Continuous 24-hour application reduces the effectiveness of the drug, as vascular smooth muscle becomes desensitized to nitrate-induced vasodilation. Evening removal also reduces the risk of nocturnal hypotension or headache. Replacement in the morning ensures the client receives consistent antianginal coverage during periods of higher activity. Proper site rotation and skin assessment prevent local irritation.
Rationales for incorrect answers:
B. “Cut each patch in half if angina attacks are under control.” Nitroglycerin patches are not designed to be cut, except for specific formulations labeled for safe division. Cutting can lead to inaccurate dosing, loss of adhesive integrity, and uneven absorption, potentially causing either subtherapeutic effect or overdose.
C. “Take off the nitroglycerin patch temporarily for 30 min if a headache occurs.” Headaches from nitroglycerin may occur due to cerebral vasodilation, but removing the patch for brief intervals is not recommended because it disrupts the therapeutic effect. Headaches should be managed with analgesics and careful titration rather than temporary removal.
D. “Change the patch every 48 hr right after the first meal of the day.” Transdermal nitroglycerin is typically changed every 24 hours, not 48 hours, to maintain effective drug delivery. Changing it at inconsistent intervals risks breakthrough angina or subtherapeutic dosing. Timing with meals is unnecessary as food does not significantly affect transdermal absorption.
Test-taking strategy:
• Recall that nitrate tolerance develops with continuous exposure; always look for answers including a daily nitrate-free interval
• Eliminate options that suggest patch alteration, extended dosing, or temporary removal for minor side effects
• Focus on application technique, timing, and safety
Take-home points:
• Remove the nitroglycerin patch nightly to maintain a nitrate-free interval and prevent tolerance
• Do not cut patches unless specifically indicated by the manufacturer
• Manage nitroglycerin-induced headaches with analgesics, not temporary patch removal
The nurse is teaching a client who has angina how to use nitroglycerin transdermal ointment. Which of the following instructions by the nurse is appropriate?
Explanation
Nitroglycerin transdermal ointment is a topical nitrate therapy used to prevent anginal episodes by causing vasodilation, reducing myocardial oxygen demand, and improving coronary blood flow. Proper application is crucial for accurate dosing, predictable absorption, and avoidance of adverse effects such as hypotension or skin irritation. Patient education should emphasize measuring the dose, applying to appropriate areas, and using protective coverings, while avoiding practices that alter absorption or increase systemic effects.
Rationale for the correct answer:
A. “Spread the ointment onto a pre-marked paper using an applicator.” Nitroglycerin ointment should be applied using a specialized applicator or dosing paper to ensure the exact prescribed dose is delivered. Pre-marked paper or a measured applicator prevents over- or under-dosing, which could result in ineffective angina control or excessive hypotension. Applying the ointment as directed ensures consistent systemic absorption and maintains therapeutic efficacy.
Rationales for incorrect answers:
B. “Rub the ointment directly into your skin until it is no longer visible.” Rubbing nitroglycerin into the skin is contraindicated, as it can lead to rapid, unpredictable absorption, causing severe hypotension, dizziness, or reflex tachycardia. The ointment is designed to stay on the skin surface to provide controlled transdermal absorption over time.
C. “Cover the applied ointment with a clean gauze pad.” Covering nitroglycerin ointment with an occlusive dressing is not recommended, as it can increase systemic absorption and risk toxicity. The ointment should be lightly covered with a non-occlusive wrap only if necessary to prevent clothing contamination, not to enhance absorption.
D. “Apply the ointment to the same skin area each time.” Repeated application to the same site increases the risk of skin irritation, redness, and dermatitis. Sites should be rotated daily to prevent localized skin damage while maintaining effective nitrate therapy.
Test-taking strategy:
• Focus on medication administration guidelines for transdermal nitrates
• Identify options that maintain dose accuracy, controlled absorption, and skin safety
• Eliminate answers that suggest rubbing, occlusion, or repeated application to the same area, which increase risks of toxicity or irritation
Take-home points:
• Use pre-marked paper or an applicator to ensure accurate dosing of nitroglycerin ointment
• Do not rub the ointment into the skin or use occlusive dressings to prevent rapid absorption or toxicity
• Rotate application sites daily to protect the skin and maintain therapeutic effectiveness
A client takes an initial dose of a nitrate. Which symptom(s) will the nurse expect to occur?
Explanation
Nitrates are vasodilators used to relieve angina by relaxing vascular smooth muscle, which decreases myocardial oxygen demand and improves coronary blood flow. When a client takes an initial dose, the sudden vasodilation of cerebral vessels often triggers headaches, a common and expected side effect. Understanding these predictable responses helps the nurse provide anticipatory guidance and reinforce adherence, as these effects are typically transient and diminish with continued use.
Rationale for the correct answer:
B. Headaches. Nitrates cause dilation of intracranial blood vessels, leading to increased intracranial blood flow and subsequent throbbing headaches, particularly after the first dose or when the dose is increased. These headaches are usually temporary, may decrease in intensity with continued therapy, and can be managed with acetaminophen if necessary. This response is an expected pharmacologic effect, not a sign of toxicity. Educating clients that headaches are a common and non-threatening side effect can improve medication adherence.
Rationales for incorrect answers:
A. Nausea and vomiting. While gastrointestinal upset can occur, it is not a typical immediate response to nitrates. Persistent nausea may indicate other causes or a drug interaction, rather than a predictable pharmacologic effect of nitrate therapy.
C. Stomach cramps. Abdominal cramping is not commonly associated with nitrate use. It is not a reliable indicator of the drug’s pharmacologic action or an expected initial side effect.
D. Irregular pulse rate. Nitrates may slightly lower blood pressure and reflexively increase heart rate (reflex tachycardia), but an irregular pulse is not a standard expected effect. An irregular pulse may indicate a cardiac conduction abnormality or other pathology, requiring further assessment.
Test-taking strategy:
• Focus on the most common and expected side effect of vasodilation with initial nitrate therapy.
• Eliminate options that represent less common or unrelated adverse effects.
• Prioritize patient education and reassurance about predictable, non-threatening symptoms.
Take-home points:
• Headaches are the most common and expected side effect after the first nitrate dose.
• They result from cerebral vasodilation and typically diminish over time.
• Educating clients about this effect improves adherence and reduces anxiety about transient symptoms.
Practice Questions 2
The nurse is assessing a client who is receiving atenolol (Tenormin) for angina. Which of the following would be a cause for the nurse to hold the drug and inform the provider? Select all that apply
Explanation
Atenolol (Tenormin) is a cardioselective beta-1 adrenergic blocker used to manage angina pectoris, hypertension, and tachyarrhythmias. It works by decreasing heart rate, myocardial contractility, and cardiac output, which reduces myocardial oxygen demand and prevents anginal episodes. Because atenolol directly affects cardiac conduction and blood pressure, careful assessment of heart rate and blood pressure is essential prior to administration. Holding the drug for bradycardia or hypotension prevents adverse cardiovascular events such as syncope, severe hypotension, or heart block.
Rationale for the correct answers:
A. Heart rate of 50 beats/minute. Atenolol slows conduction through the sinoatrial and atrioventricular nodes. A heart rate below 60 bpm may indicate clinically significant bradycardia, which increases the risk of dizziness, hypotension, syncope, or worsening heart failure. Administration under these conditions can precipitate cardiovascular compromise.
C. Blood pressure 86/56 mmHg. Atenolol reduces myocardial contractility and systemic vascular resistance, lowering blood pressure. A systolic BP below 90 mmHg may indicate hypoperfusion of vital organs. Administering atenolol in this scenario could exacerbate hypotension, resulting in syncope, acute kidney injury, or myocardial ischemia.
Rationales for incorrect answers:
B. Heart rate of 124 beats/minute. Tachycardia may be a symptom of angina or another condition, but a heart rate above normal is not a contraindication to atenolol; the drug may actually be indicated to control elevated heart rate.
D. Blood pressure 156/88 mmHg. Hypertension is an indication for atenolol, and this reading does not require holding the drug. The medication is intended to safely lower elevated blood pressure over time.
E. Tinnitus and vertigo. These are not common side effects of atenolol. While these symptoms should be assessed further, they are not immediate contraindications for holding the medication unless they indicate another acute condition.
Test-taking strategy:
• Focus on vital signs directly affected by beta-blocker therapy (heart rate and blood pressure)
• Identify parameters indicating potential harm if the drug is administered
• Recognize that other symptoms or elevated vitals may require monitoring, not immediate withholding
Take-home points:
• Hold atenolol for bradycardia (HR < 60 bpm) or hypotension (SBP < 90 mmHg)
• Continuous monitoring of heart rate and blood pressure is essential to prevent adverse events
• Educate clients to report dizziness, syncope, or unusual fatigue that may indicate overmedication
A nurse is caring for a client with angina. The provider’s order reads, “Give metoprolol (Lopressor) 300 mg/day PO in 2 divided doses. The tablets are available in 50-mg strength. How many tablets will the client receive per dose?
Explanation
Step 1: Identify the total daily dose. The healthcare provider’s order specifies a total of 300 mg per day.
Step 2: Determine the number of doses per day. The order states the medication should be given in "2 divided doses."
Step 3: Calculate the dosage for a single administration. To find the amount for one dose, divide the total daily dose by the number of doses: 300 mg / 2 doses = 150 mg per dose.
Step 4: Identify the strength of the available medication. The tablets on hand are 50 mg each.
Step 5: Calculate the number of tablets required for the single dose. Divide the required dose by the strength of the tablet: 150 mg / 50 mg = 3 tablets.
Final Answer: The client will receive 3 tablets per dose (which equals 150 mg per dose).
Test-Taking Strategy:
- Determine if the answer should be calculated for the total daily amount or for a single dose.
- Highlight the phrase "divided doses" to ensure you include the division step before calculating the number of tablets.
- Verify your final answer by multiplying the tablets per dose by the number of doses to see if it matches the total daily order.
Take-Home Points:
- Metoprolol is a beta-blocker that requires the nurse to assess the patient's heart rate and blood pressure before every administration.
- The term "divided doses" implies the total daily amount must be split into equal parts to maintain a steady therapeutic level in the bloodstream.
- Always double-check the medication suffix, as immediate-release metoprolol tartrate and extended-release metoprolol succinate have different dosing schedules and instructions.
The nurse is caring for a client with angina who is to start beta blocker therapy. The nurse is aware that the presence of which condition may be a problem if these drugs are used? Select all that apply
Explanation
Beta blockers are cardiovascular medications that work by blocking beta-adrenergic receptors, resulting in reduced heart rate, myocardial contractility, and cardiac output, which decreases myocardial oxygen demand. They are used for management of hypertension, angina, certain arrhythmias, and post-myocardial infarction therapy. While effective, beta blockers can have significant interactions and contraindications, particularly in clients with conditions that may be exacerbated by beta-adrenergic blockade. Recognizing these high-risk conditions ensures safe initiation and prevents serious complications.
Rationale for the correct answer:
A. Diabetes mellitus. Beta blockers can mask classic signs of hypoglycemia, such as tachycardia and tremors, making it more difficult for clients with diabetes to recognize and respond to low blood glucose. Additionally, non-selective beta blockers can impair glycogenolysis, further increasing the risk of prolonged hypoglycemia. This requires careful monitoring and patient education before initiating therapy.
D. Asthma. Non-selective beta blockers block beta-2 adrenergic receptors in bronchial smooth muscle, which can cause bronchoconstriction and trigger asthma exacerbations. Even cardioselective beta blockers may pose some risk at higher doses. Clients with asthma require extreme caution, alternative therapy consideration, and close respiratory monitoring.
Rationales for incorrect answers:
B. Essential tremors. While beta blockers like propranolol are used to treat essential tremors, their presence is not a contraindication; in fact, it can be a therapeutic benefit.
C. Exertional angina. Beta blockers are indicated for exertional angina because they reduce myocardial oxygen demand during activity. This condition is a therapeutic indication, not a contraindication.
E. Hypertension. Beta blockers are commonly prescribed for hypertension and can effectively lower blood pressure. Their presence does not pose a safety problem but rather represents an appropriate therapeutic target.
Test-taking strategy:
• Identify comorbidities that could be negatively impacted by beta blockade.
• Focus on conditions associated with masked hypoglycemia, bronchospasm, or contraindicated pharmacologic effects.
• Eliminate options that represent therapeutic indications rather than risks.
Take-home points:
• Beta blockers may mask hypoglycemia symptoms in diabetes; monitor blood glucose closely.
• Asthma and other obstructive lung diseases are contraindications for non-selective beta blockers due to bronchospasm risk.
• Conditions like exertional angina and hypertension are indications, not contraindications, for beta blocker therapy.
A client is prescribed a beta blocker. The nurse acknowledges that beta blockers are as effective as antianginals because they do what?
Explanation
Beta blockers are cardiovascular medications commonly used to manage angina, hypertension, and arrhythmias. Their therapeutic effectiveness in angina is related to their ability to reduce myocardial oxygen demand by decreasing heart rate, myocardial contractility, and overall cardiac workload. This action helps prevent ischemia during exertion or stress, making beta blockers an essential component of chronic stable angina management.
Rationale for the correct answer:
C. Decrease heart rate and decrease myocardial contractility. Beta blockers, such as atenolol or metoprolol, act by blocking beta-1 adrenergic receptors in the heart, which reduces chronotropy (heart rate) and inotropy (contractile force). By lowering myocardial oxygen demand, they help prevent anginal episodes without directly increasing coronary blood flow. This mechanism makes them equally effective as other antianginal agents in managing chronic stable angina, particularly for effort-induced angina. They also help reduce mortality in patients with post-myocardial infarction heart disease.
Rationales for incorrect answers:
A. Increase oxygen to the systemic circulation. Beta blockers do not increase systemic oxygen delivery. Their primary effect is to reduce cardiac workload and oxygen demand, rather than enhancing oxygen availability.
B. Maintain heart rate and blood pressure. Beta blockers lower heart rate and blood pressure, rather than maintaining them. Maintenance of these parameters is not the therapeutic goal; reduction is essential for decreasing myocardial oxygen consumption.
D. Decrease heart rate and increase myocardial contractility. Beta blockers do not increase contractility; they reduce it. Increasing contractility would raise myocardial oxygen demand, counteracting their antianginal effect.
Test-taking strategy:
• Focus on the mechanism of action of beta blockers in angina management.
• Identify options that reduce cardiac workload and oxygen consumption, not those that increase oxygen supply or contractility.
• Remember that beta blockers are primarily negative chronotropes and inotropes.
Take-home points:
• Beta blockers reduce heart rate and myocardial contractility, decreasing oxygen demand.
• They prevent anginal episodes, especially exertional angina, rather than directly dilating coronary arteries.
• Understanding the mechanism helps anticipate effects, monitor safety, and educate clients effectively.
A nurse is caring for a client on a beta blocker. Which instruction will the nurse give the client regarding discontinuing the beta blocker?
Explanation
Beta blockers are cardiovascular medications used for angina, hypertension, and arrhythmias. They work by reducing heart rate, myocardial contractility, and cardiac workload, which decreases myocardial oxygen demand. When discontinuing beta blockers, abrupt cessation can cause serious adverse effects, including rebound angina, hypertension, and potentially life-threatening arrhythmias. Proper client education on gradual tapering ensures safety and prevents complications.
Rationale for the correct answer:
B. The beta blocker should not be abruptly stopped; the dose should be tapered down. Abrupt withdrawal of beta blockers can result in rebound sympathetic activity, which may cause tachycardia, angina exacerbation, myocardial infarction, or arrhythmias, particularly in clients with underlying ischemic heart disease. Tapering the dose gradually over 1–2 weeks allows the cardiovascular system to adjust, maintaining hemodynamic stability and reducing the risk of adverse cardiac events. This is a critical teaching point for clients preparing to discontinue therapy safely.
Rationales for incorrect answers:
A. The beta blocker should be abruptly stopped when another cardiac drug is prescribed. Abrupt discontinuation is dangerous, especially in clients with angina or heart disease. Switching to another cardiac drug does not prevent rebound effects, and abrupt withdrawal may trigger serious cardiac events.
C. The beta blocker dose should be maintained while taking another antianginal drug. While maintaining therapy may be appropriate in some cases, this statement does not address the safety concerns of discontinuation. The focus is on safe tapering, not simply continuing therapy alongside another drug.
D. Half the beta blocker dose should be taken for the next several weeks. Arbitrarily halving the dose without a structured tapering schedule may be ineffective or unsafe. Tapering should follow specific provider instructions based on the drug, duration of therapy, and client condition.
Test-taking strategy:
• Identify safety concerns related to abrupt discontinuation of beta blockers.
• Recognize rebound cardiovascular effects as a primary risk.
• Focus on answers that reflect gradual tapering and provider-guided dose adjustments.
Take-home points:
• Never abruptly stop beta blockers; always taper the dose gradually.
• Abrupt withdrawal can precipitate rebound angina, hypertension, or arrhythmias.
• Educate clients to follow provider-directed tapering schedules for safe discontinuation.
Practice Questions 3
A client with angina has been given a prescription for a calcium channel blocker. The nurse knows that this class of drugs is used to treat which type of angina?
Explanation
Calcium channel blockers (CCBs) are vascular smooth muscle relaxants that inhibit calcium influx into cardiac and arterial smooth muscle cells. This action promotes coronary artery dilation, reduces myocardial oxygen demand, and improves oxygen supply. CCBs are particularly effective in treating vasospastic (Prinzmetal’s) angina, which results from transient coronary artery spasms that restrict blood flow to the myocardium. Understanding the specific angina type targeted by CCBs is essential for safe and effective pharmacologic management.
Rationale for the correct answer:
D. Vasospastic angina is caused by sudden, reversible coronary artery vasospasm, often occurring at rest and sometimes associated with ST-segment elevation on ECG. Calcium channel blockers relax coronary smooth muscle, preventing or relieving these spasms, making them the treatment of choice. CCBs also improve myocardial oxygen delivery by reducing afterload and coronary resistance without significantly increasing heart rate.
Rationales for incorrect answers:
A.Effort (stable) angina occurs during physical activity or emotional stress due to fixed atherosclerotic plaque limiting coronary blood flow. First-line treatment includes beta blockers and nitrates to reduce myocardial oxygen demand; calcium channel blockers may be adjunct therapy if beta blockers are contraindicated.
B. Unstable angina is characterized by crescendo pain, unpredictability, and potential progression to myocardial infarction. Treatment focuses on antiplatelet therapy, anticoagulation, nitrates, and revascularization. CCBs are not primary therapy because they do not address the underlying thrombotic or plaque instability mechanisms.
C. Crescendo angina is essentially a form of unstable angina, with progressively severe, frequent, or prolonged episodes. Similar to unstable angina, management targets plaque stabilization and oxygen supply-demand balance, not coronary spasm, making CCBs secondary or adjunct therapy at best.
Test-taking strategy:
• Identify the mechanism of action of calcium channel blockers—relaxation of coronary smooth muscle and prevention of vasospasm.
• Associate CCBs with angina that occurs at rest rather than activity-induced angina.
• Eliminate options that are primarily managed with beta blockers, nitrates, or antiplatelet therapy.
Take-home points:
• Calcium channel blockers are first-line therapy for vasospastic (Prinzmetal’s) angina.
• They work by relaxing coronary arteries and reducing oxygen demand.
• CCBs are not the primary treatment for stable, unstable, or crescendo angina, but may be used adjunctively in specific scenarios.
The nurse is caring for a client on the calcium channel blocker diltiazem (Cardizem). Which statement by the client reflects the need for additional client education?
Explanation
Diltiazem (Cardizem) is a calcium channel blocker used primarily for the management of hypertension, chronic stable angina, and certain arrhythmias. It works by inhibiting calcium influx into cardiac and vascular smooth muscle, resulting in vasodilation, decreased myocardial oxygen demand, and slowed conduction through the AV node. Client education focuses on long-term use, proper administration, adverse effects, and safety precautions, particularly regarding hypotension and drug interactions.
Rationale for the correct answer:
A. “I can take this drug to stop an attack of angina.” Diltiazem is a maintenance medication that prevents angina by reducing cardiac workload and myocardial oxygen demand over time. It is not a rapid-acting antianginal agent, so it cannot relieve acute chest pain. Clients should be instructed to use sublingual nitroglycerin or other prescribed fast-acting medications for acute attacks. Misunderstanding this distinction could result in delayed treatment of acute ischemia. This increases the risk of myocardial infarction or serious complications.
Rationales for incorrect answers:
B. “I understand that food and antacids alter the absorption of this oral drug.” Oral diltiazem’s absorption can be affected by food and antacids, which may alter its bioavailability. Recognizing this supports safe and effective administration and demonstrates correct understanding.
C. “When the long-acting forms are taken, the drug cannot be crushed.” Extended-release diltiazem formulations are designed to release the drug slowly; crushing or splitting them can cause dose dumping, toxicity, or subtherapeutic effects, so this statement is accurate and requires no correction.
D. “This drug may cause my blood pressure to drop, so I need to be careful when getting up.” Hypotension and orthostatic changes are common with diltiazem due to its vasodilatory effect. This demonstrates awareness of a significant adverse effect and the need for safety precautions, making it correct patient education.
Test-taking strategy:
• Identify statements that indicate misconceptions about acute vs. maintenance therapy.
• Focus on the primary pharmacologic action and onset of effect.
• Eliminate options that reflect accurate safety and administration knowledge.
Take-home points:
• Diltiazem is for prevention, not acute relief, of angina.
• Extended-release forms should never be crushed or split.
• Educate clients about orthostatic hypotension and factors that alter absorption, such as food or antacids.
Practice Questions 4
The nurse is teaching a client who has angina pectoris and is learning how to treat acute anginal attacks. The clients asks, “What is my next step if I take one tablet, wait 5 minutes, but still have anginal pain?”
Which of the following replies by the nurse is appropriate?
Explanation
Clients with angina pectoris are commonly prescribed sublingual nitroglycerin for the rapid relief of acute myocardial ischemia caused by coronary artery vasoconstriction. Effective teaching must emphasize timing, emergency response, and safe medication sequencing. Delayed intervention during persistent chest pain can result in myocardial infarction or sudden cardiac death. Understanding when to escalate care is critical for client safety.
Rationale for the correct answer:
B. “Call 911 and take a second sublingual tablet.” This reflects the correct, evidence-based protocol for managing acute anginal pain. If chest pain is not relieved after one sublingual nitroglycerin tablet after 5 minutes, the client should activate emergency medical services immediately. Ongoing pain may indicate evolving myocardial infarction rather than stable angina. While waiting for emergency responders, the client may take a second sublingual nitroglycerin tablet, provided blood pressure is stable and no contraindications exist. This prioritizes life-saving care over medication-only management.
Rationales for the other options:
A. “Take two tablets at the same time and then call 911.” Taking multiple tablets simultaneously is unsafe and not recommended. Nitroglycerin can cause severe hypotension, syncope, and reflex tachycardia if overdosed. Tablets must be taken one at a time, spaced 5 minutes apart, to allow assessment of response and hemodynamic stability.
C. “Take a sustained-release nitroglycerin capsule rather than a sublingual tablet and wait 5 more minutes before calling 911.” Sustained-release nitroglycerin is not appropriate for acute anginal attacks due to delayed onset of action. Using this formulation during active chest pain can dangerously delay treatment and emergency evaluation.
D. “Wait another 5 minutes before taking a second sublingual tablet.” Delaying emergency services places the client at significant risk. Persistent chest pain after the first dose is a medical emergency, and waiting without calling 911 may result in irreversible myocardial damage.
Test-taking strategy:
- Identify symptoms suggesting possible myocardial infarction, not just stable angina
- Prioritize emergency activation over continued self-management
- Recognize that sublingual nitroglycerin is taken one tablet at a time, not simultaneously
- Eliminate options that delay definitive care or misuse drug formulations
Take-home points:
- Persistent chest pain after one nitroglycerin tablet requires immediate EMS activation
- Sublingual nitroglycerin is used for acute relief, not sustained-release formulations
- Early emergency response saves myocardium and reduces mortality
A client who has angina is prescribed nitroglycerin. Which are appropriate nursing interventions for nitroglycerin? Select all that apply
Explanation
Nitroglycerin is a nitrate vasodilator commonly prescribed for acute or chronic angina. Its primary mechanism is smooth muscle relaxation, resulting in venous and arterial dilation, which decreases myocardial oxygen demand. Nursing care focuses on safe administration, prevention of hypotension, patient education, and adherence to emergency protocols. Understanding appropriate interventions ensures the client receives maximum therapeutic benefit while minimizing adverse effects and complications.
Rationales for correct answers:
A. Have the client sit or lie down when taking a sublingual nitroglycerin tablet. Sublingual nitroglycerin causes rapid vasodilation, which can result in orthostatic hypotension, dizziness, or syncope. Having the client sit or lie down reduces the risk of falls and injuries during hypotensive episodes, ensuring safe administration during acute anginal attacks.
B. Teach the client who has taken a tablet to call 911 in 5 minutes if chest pain persists. Standard angina protocol instructs clients to take one sublingual tablet at the onset of chest pain. If pain persists after 5 minutes, a second tablet may be taken and emergency services contacted. This ensures timely treatment of potential myocardial infarction and prevents delay in accessing life-saving care.
E. Warn the client against ingesting alcohol while taking nitroglycerin. Alcohol potentiates vasodilation caused by nitroglycerin, increasing the risk of severe hypotension, syncope, or dizziness. Education about alcohol avoidance is critical for safety during both acute and chronic therapy.
Rationales for incorrect answers:
C. Apply Transderm-Nitro patch to a hairy area to protect skin from burning. Patches should be applied to hairless, clean, dry skin to ensure proper absorption. Hair can interfere with adhesion and drug delivery, while using a hairy area does not protect from adverse effects.
D. Call the health care provider after taking five tablets if chest pain persists. Taking more than three sublingual tablets within 15 minutes is unsafe and indicates a possible myocardial infarction. The priority is immediate emergency care rather than contacting the provider.
Test-taking strategy:
- Focus on safety interventions and prevention of hypotension or falls.
- Identify instructions that align with acute angina protocol (one tablet, repeat in 5 minutes, max three tablets, call 911).
- Eliminate options that violate administration guidelines or delay emergency care.
Take-home points:
- Sit or lie down when taking sublingual nitroglycerin to prevent falls from hypotension.
- Follow the 5-minute rule: one tablet, repeat if pain persists, do not exceed three tablets, and call 911.
- Avoid alcohol during therapy to reduce the risk of severe hypotension and syncope.
The nurse is caring for a client who is prescribed isosorbide mononitrate (Imdur) for chronic stable angina
and develops reflex tachycardia. Which of the following medications should the nurse expect to administer?
Explanation
Isosorbide mononitrate (Imdur) is a long-acting nitrate used to prevent episodes of chronic stable angina by promoting venous and coronary vasodilation, reducing myocardial oxygen demand. A known side effect of nitrates is reflex tachycardia, which occurs as a compensatory sympathetic response to vasodilation and decreased blood pressure. Reflex tachycardia can increase myocardial oxygen demand, potentially worsening angina, and requires management with medications that control heart rate.
Rationale for the correct answer:
D. Metoprolol is a cardioselective beta-1 adrenergic blocker that decreases heart rate, myocardial contractility, and oxygen demand. Administering metoprolol in response to nitrate-induced reflex tachycardia helps attenuate the compensatory sympathetic response, reducing the risk of angina exacerbation. Beta blockers are often used in combination with nitrates to optimize antianginal therapy while minimizing adverse cardiovascular effects.
Rationales for incorrect answers:
A. Furosemide is a loop diuretic primarily used to treat fluid overload, heart failure, and hypertension. It does not affect heart rate directly and would not address reflex tachycardia caused by vasodilation. Its use in this scenario would be inappropriate and would not prevent increased myocardial oxygen demand.
B. Captopril is an ACE inhibitor used to lower blood pressure and improve outcomes in heart failure. While it reduces afterload and preload, it does not directly control reflex tachycardia. Administering captopril in this context would not counteract the tachycardic response to isosorbide mononitrate.
C. Ranolazine is an antianginal agent that works by inhibiting the late sodium current in cardiac myocytes. It improves myocardial efficiency but does not acutely reduce heart rate. Therefore, it is ineffective for treating nitrate-induced reflex tachycardia.
Test-taking strategy:
• Recognize that reflex tachycardia from nitrates is a compensatory increase in heart rate
• Choose medications that directly reduce heart rate (beta-blockers)
• Eliminate options that act on blood pressure or myocardial oxygen utilization indirectly but do not control heart rate
Take-home points:
• Reflex tachycardia is a common adverse effect of long-acting nitrates like isosorbide mononitrate
• Beta-1 selective blockers, such as metoprolol, are the preferred treatment to control heart rate and prevent angina exacerbation
• Other cardiovascular drugs, including diuretics, ACE inhibitors, or ranolazine, do not manage reflex tachycardia and are not appropriate for this indication
The nurse has ordered nitroglycerin patches for a client with a history of angina. What teaching will the nurse give to this client?
Explanation
Nitroglycerin patches are a form of transdermal nitrate therapy. Nitroglycerin works by dilating coronary and systemic blood vessels, which reduces myocardial oxygen demand and helps prevent anginal episodes. Proper patch application and rotation are essential to maintain therapeutic efficacy, minimize tolerance, and prevent skin irritation. Client education focuses on correct administration, adherence, and safety measures to ensure optimal angina management.
Rationale for correct answer:
C. Remove the old patch before applying a new one. Transdermal nitroglycerin patches should be applied to clean, dry, hairless skin, and the previous patch must be removed before a new one is applied. Leaving multiple patches on at the same time can lead to excessive vasodilation, hypotension, and severe headache. Rotating application sites helps prevent skin irritation and ensures consistent drug absorption. Proper application and removal are critical for both safety and therapeutic effect.
Rationales for incorrect answers:
A. Keep the patches in the refrigerator. Nitroglycerin patches should be stored at room temperature, away from heat and moisture. Refrigeration is unnecessary and may affect the adhesive properties, potentially reducing drug delivery.
B. Use the patches only if the chest pain is severe. Transdermal nitroglycerin is intended for prevention of angina, not for acute attacks. Clients should have short-acting forms, such as sublingual tablets, for acute chest pain. Using the patch only during pain undermines its prophylactic purpose.
D. Apply the patch only to the upper arm or thigh areas. While patches can be applied to various hairless skin areas, they are not limited to the upper arm or thigh. The key is clean, dry, hairless skin with rotation of sites. Limiting to only these areas is unnecessarily restrictive and may reduce flexibility in patch application.
Test-taking strategy:
• Focus on proper administration, adherence, and safety for transdermal nitrate therapy.
• Distinguish prophylactic use from acute treatment of angina.
• Remember patch rotation and removal of the old patch to avoid overdose or skin irritation.
Take-home points:
• Always remove the old nitroglycerin patch before applying a new one.
• Transdermal patches are for prevention, not acute relief; sublingual nitrates should be available for breakthrough pain.
• Store patches at room temperature and rotate application sites to prevent skin irritation and maintain efficacy.
Comprehensive Questions
A client is being discharged with nitroglycerin (Nitrostat) for sublingual use. While planning client education, what instruction will the nurse include?
Explanation
Nitroglycerin (Nitrostat) sublingual tablets are a rapid-acting nitrate used to relieve acute anginal episodes by dilating coronary arteries, reducing myocardial oxygen demand, and improving blood flow to ischemic tissue. Proper client education is essential for safe and effective self-administration, preventing complications such as hypotension, syncope, or delayed emergency care. Clients must understand dosing intervals, maximum doses, and when to seek immediate medical attention to manage angina safely.
Rationale for the correct answer:
B. “Put one tablet under your tongue for chest pain. If pain does not subside, you may repeat in 5 minutes, taking no more than three tablets.” This aligns with standard guidelines for sublingual nitroglycerin use. One tablet is placed sublingually, allowing rapid absorption through the oral mucosa. If pain persists, the dose may be repeated in 5 minutes, not exceeding three doses within 15 minutes. After the doses without relief, the client should call 911 immediately. This ensures timely pain relief while preventing excessive hypotension or delayed care in the event of a myocardial infarction.
Rationales for incorrect answers:
A. “Swallow three tablets immediately for pain and call 911.” Swallowing sublingual nitroglycerin is ineffective, as first-pass metabolism inactivates the drug, and taking three tablets at once risks severe hypotension and syncope. This is unsafe and contradicts established administration protocols.
C. “Call your health care provider when you have chest pain.” He will tell you how many tablets to take.” Delaying action until contact with a healthcare provider puts the client at risk for prolonged myocardial ischemia. Angina requires immediate self-management with a known dosing regimen to prevent complications.
D. “Place three tablets under your tongue and call 911.” Administering three tablets simultaneously is dangerous, potentially causing profound hypotension and reflex tachycardia. Only one tablet should be given at a time, with repeat doses based on symptom persistence.
Test-taking strategy:
• Focus on acute angina management protocols
• Identify instructions that emphasize single dosing, timing intervals, and emergency actions
• Eliminate options that suggest simultaneous multiple dosing, delayed care, or incorrect administration routes
Take-home points:
• Sublingual nitroglycerin should be administered one tablet at a time, repeated every 5 minutes as needed
• Do not exceed three doses within 15 minutes; call 911 if pain persists
• Proper education ensures rapid symptom relief and prevention of complications such as hypotension or myocardial infarction
The nurse is caring for a client with chronic stable angina who is receiving isosorbide dinitrate (Isordil). Which of the following are common adverse effects of isosorbide?
Explanation
Isosorbide dinitrate (Isordil) is a nitrate vasodilator commonly prescribed for chronic stable angina. It works by relaxing vascular smooth muscle, resulting in venous and arterial dilation, which decreases myocardial oxygen demand by reducing preload and afterload. Because nitrates cause systemic vasodilation, clients are at risk for hypotension and reduced cerebral perfusion, which can manifest as light-headedness and dizziness. Proper patient education and monitoring help prevent falls and other complications related to hypotension.
Rationale for the correct answer:
D. Light-headedness and dizziness. Nitrates induce peripheral vasodilation, leading to decreased systemic vascular resistance. The resultant drop in blood pressure can reduce cerebral perfusion, causing dizziness, light-headedness, or syncope, particularly upon standing (orthostatic hypotension). These adverse effects are common, expected, and usually transient, but clients must be instructed to rise slowly from sitting or lying positions to reduce fall risk.
Rationales for incorrect answers:
A. Flushing and headache. While these are common adverse effects of nitrates, the onset is usually transient and less clinically significant than hypotensive effects. Flushing and headache are not the most concerning or frequent in chronic stable angina management with isosorbide dinitrate.
B. Tremors and anxiety. These symptoms are not typically associated with nitrates. They are more characteristic of sympathomimetic or stimulant medications, making this option inaccurate.
C. Sleepiness and lethargy. Sedation is not a common effect of nitrates. Dizziness from hypotension may cause a secondary sensation of fatigue, but direct CNS depression is uncommon.
Test-taking strategy:
• Focus on physiologic effects of nitrates (vasodilation → hypotension → cerebral hypoperfusion)
• Recognize adverse effects that are directly related to the drug’s mechanism of action
• Eliminate options that describe effects unrelated to vascular smooth muscle relaxation
Take-home points:
• Isosorbide dinitrate commonly causes light-headedness and dizziness due to hypotension.
• Clients should rise slowly from lying or sitting positions to prevent falls.
• Monitor blood pressure and educate clients about position changes and fall precautions during therapy.
A nurse is caring for a client who is experiencing chest pain. Place the following nursing interventions in order:
Explanation
When a client experiences chest pain, rapid assessment and safe intervention are critical to prevent myocardial injury and ensure client safety. Nursing management focuses on assessing pain characteristics, evaluating hemodynamic stability, administering rapid-acting antianginal therapy, reassessing the heart rate and blood pressure for effectiveness, and documenting care to maintain continuity and legal standards.
Rationale for the correct answer:
C. Assess the location, quality, and intensity of pain. The first step is a thorough pain assessment to differentiate angina from other causes of chest pain. Evaluating onset, duration, radiation, associated symptoms, and intensity establishes a baseline and informs treatment priorities.
B. Assess heart rate and blood pressure. Before giving nitroglycerin, it is essential to evaluate hemodynamic status. Nitroglycerin can cause vasodilation, leading to hypotension and reflex tachycardia. Baseline vital signs ensure safe administration and allow early detection of adverse effects.
A. Administer nitroglycerin sublingually. Sublingual nitroglycerin provides rapid relief by dilating coronary arteries and reducing myocardial oxygen demand. It should be given after confirming stable vital signs to prevent complications such as hypotension or syncope.
E. Evaluate the location, quality, and intensity of pain. Reassessing pain determines whether the intervention is effective or if further treatment is needed. Persistent or worsening pain may indicate myocardial infarction, requiring urgent escalation of care.
D. Document interventions and outcomes. Accurate documentation of assessments, medications, dosages, vital signs, and client responses is essential for continuity of care, quality monitoring, and legal compliance.
Test-taking strategy:
• Prioritize steps that ensure safety and effectiveness: assess → intervene → evaluate → document.
• Consider the mechanism of action of nitroglycerin and its hemodynamic effects.
• Always reassess both pain and vital signs before repeating or escalating therapy.
Take-home points:
• Assess pain characteristics and vital signs before giving nitroglycerin.
• Reassess pain and hemodynamic status after administration to evaluate effectiveness.
• Document all interventions, assessments, and client responses for safety and continuity of care.
The nurse is educating a client about erectile dysfunction drugs such as sildenafil (Viagra) that are contraindicated in clients taking nitrates for angina. What is the primary concern with concurrent administration of these drugs?
Explanation
When educating a client about erectile dysfunction drugs such as sildenafil (Viagra), it is essential to emphasize drug interactions, cardiovascular effects, and client safety. Sildenafil is a phosphodiesterase type 5 (PDE5) inhibitor that promotes smooth muscle relaxation and vasodilation to facilitate penile erection. Nitrates, used for angina management, also cause vascular smooth muscle relaxation, leading to systemic vasodilation. Understanding the additive hypotensive effects of these medications is critical, as concurrent use can result in life-threatening hypotension.
Rationale for the correct answer:
B. They decrease blood pressure and may result in prolonged and severe hypotension when combined with nitrates. Sildenafil and other PDE5 inhibitors potentiate the vasodilatory effects of nitrates. This can produce a rapid, profound, and potentially fatal drop in blood pressure, leading to syncope, myocardial ischemia, or shock. The interaction is pharmacodynamically significant, and the timing of administration matters, as PDE5 inhibitors can remain active for several hours, increasing the risk of hypotension if nitrates are taken concurrently. Therefore, concurrent administration is strictly contraindicated, and alternative angina treatments or erectile dysfunction therapies should be considered.
Rationales for incorrect answers:
A. They contain nitrates, resulting in an overdose. PDE5 inhibitors do not contain nitrates. The risk is not due to drug content but to additive pharmacologic effects on vascular smooth muscle, so this statement is inaccurate.
C. They will adequately treat the client’s angina as well as erectile dysfunction. PDE5 inhibitors do not provide antianginal effects. Using them for angina would be ineffective and potentially dangerous due to exacerbation of hypotension.
D. They will increase the possibility of nitrate tolerance developing and should be avoided unless other drugs can be used. Nitrate tolerance develops with continuous nitrate exposure, not with PDE5 inhibitors. Avoiding concurrent use is due to severe hypotension, not tolerance mechanisms.
Test-taking strategy:
• Focus on mechanisms of action and pharmacodynamic interactions.
• Recognize which drug combinations produce additive vasodilation and hypotension.
• Prioritize options that highlight safety risks and contraindications.
Take-home points:
• Sildenafil and nitrates are strictly contraindicated due to risk of severe hypotension.
• PDE5 inhibitors do not treat angina; using them with nitrates is unsafe.
• Educate clients about timing and potential drug interactions with all vasodilators.
A client has a new prescription for transdermal nitroglycerin patches. The nurse teaches the client that these patches are most appropriately used for which reason?
Explanation
Transdermal nitroglycerin patches are long-acting nitrate preparations used primarily for the prevention of angina pectoris in clients with chronic stable angina. These patches deliver continuous vasodilation by releasing nitroglycerin through the skin, which reduces myocardial oxygen demand and improves coronary blood flow. Client education emphasizes the prophylactic purpose, correct application, rotation of skin sites, and adherence to daily nitrate-free intervals to prevent tolerance.
Rationale for the correct answer:
C. To prevent the occurrence of angina. Transdermal nitroglycerin is designed for long-term prophylaxis of angina rather than acute symptom relief. Continuous absorption maintains a steady plasma concentration, reducing the frequency and severity of anginal episodes. Proper use includes removing the patch nightly to allow a nitrate-free period and prevent tolerance, then applying a new patch in the morning.
Rationales for incorrect answers:
A. To relieve exertional angina. Patches are not fast-acting and do not provide immediate relief of acute exertional chest pain. Sublingual nitroglycerin or rapid-acting sprays are indicated for acute anginal attacks.
B. To prevent palpitations. Nitroglycerin’s primary action is vasodilation, which decreases myocardial oxygen demand. It does not directly affect cardiac rhythm, so it is not used to prevent palpitations.
D. To stop an episode of angina. The onset of action for transdermal patches is too slow to abort an acute anginal episode. Using patches for acute attacks can delay appropriate therapy, increasing the risk of myocardial ischemia.
Test-taking strategy:
• Distinguish between prophylactic and acute therapy in angina management.
• Identify which nitrate formulations act rapidly versus long-acting.
• Focus on therapeutic purpose and onset of action to determine the correct answer.
Take-home points:
• Transdermal nitroglycerin is for prevention, not treatment, of angina.
• Acute angina requires sublingual or spray nitroglycerin for rapid relief.
• Educate clients on application, rotation of sites, and nitrate-free intervals to maintain efficacy and reduce tolerance.
The nurse with adequate knowledge about the administration of intravenous nitroglycerin will recognize that which of the following statements is correct?
Explanation
Intravenous (IV) nitroglycerin is a potent vasodilator used for acute angina, uncontrolled hypertension, and perioperative cardiac management. The IV form provides rapid, titratable vasodilation for emergent situations and requires strict handling, monitoring, and administration protocols to ensure efficacy and patient safety. Understanding pharmacokinetics, light sensitivity, and infusion requirements is essential for nurses administering this medication.
Rationale for the correct answer:
C. Intravenous nitroglycerin must be protected from exposure to light through use of special tubing. Nitroglycerin in IV form is highly photosensitive, and exposure to light can cause degradation of the drug, reducing potency and therapeutic effect. To maintain stability, it should be administered using opaque or aluminum-coated tubing and covered IV bags. Nurses must also titrate the infusion carefully while continuously monitoring blood pressure and heart rate to prevent hypotension or reflex tachycardia, common adverse effects of rapid vasodilation.
Rationales for incorrect answers:
A. The intravenous form is given by IV push injection. IV nitroglycerin is not given as a bolus due to the risk of sudden, profound hypotension and reflex tachycardia. Continuous IV infusion is required to achieve controlled therapeutic effects safely.
B. Because the intravenous forms are short-lived, the dosing must be every 2 hours. IV nitroglycerin has a very short half-life (1–4 minutes), but it is administered via continuous infusion, not intermittent dosing, allowing precise titration to achieve the desired effect. Intermittent dosing would be unsafe and ineffective.
D. Intravenous nitroglycerin can be given via gravity drip infusions. Gravity drip administration is unreliable for titratable dosing and can lead to erratic blood levels and hypotension. IV nitroglycerin must be administered with an electronic infusion pump to allow accurate and safe titration.
Test-taking strategy:
• Focus on the pharmacologic properties of IV nitroglycerin, including light sensitivity and rapid onset.
• Eliminate options that describe unsafe or imprecise administration methods.
• Remember that IV forms of vasodilators are continuous infusions requiring specialized tubing and close monitoring.
Take-home points:
• IV nitroglycerin must be protected from light to preserve potency.
• It should be administered continuously via electronic pump, not as a bolus or gravity drip.
• Close monitoring of blood pressure, heart rate, and infusion rate is essential to prevent hypotension and ensure therapeutic efficacy.
A 68-year-old male client has been taking the nitrate isosorbide dinitrate (Isordil) for 2 years for angina. He recently has been experiencing erectile dysfunction and wants a prescription for sildenafil (Viagra). Which response would the nurse most likely hear from the prescriber?
Explanation
Nitrates, such as isosorbide dinitrate, are commonly prescribed for angina pectoris to dilate coronary arteries, reduce myocardial oxygen demand, and relieve chest pain. Sildenafil (Viagra) and other phosphodiesterase type 5 (PDE5) inhibitors are used to treat erectile dysfunction by enhancing nitric oxide–mediated vasodilation in penile tissue. Concurrent use of nitrates and PDE5 inhibitors is contraindicated because their combined vasodilatory effects can lead to profound and potentially life-threatening hypotension, syncope, and cardiovascular collapse. Understanding this interaction is critical for safe prescribing and patient education.
Rationale for the correct answer:
B. “Taking sildenafil with the nitrate may result in severe hypotension, so a contraindication exists.” This statement accurately reflects the absolute contraindication of combining nitrates and PDE5 inhibitors. Both drugs increase levels of cyclic guanosine monophosphate (cGMP), leading to systemic vasodilation and decreased blood pressure. In elderly clients or those with pre-existing cardiovascular disease, this can precipitate shock, myocardial ischemia, or sudden death, which is why prescribers must not co-administer these medications.
Rationales for incorrect answers:
A. “He will have to be switched to isosorbide mononitrate if he wants to take sildenafil.” Switching from one nitrate to another does not eliminate the risk, as all nitrates have similar vasodilatory effects; the contraindication remains.
C. “I'll write a prescription, but if he uses it, he needs to stop taking the isosorbide for one dose.” Temporarily holding the nitrate does not reliably prevent severe hypotension, because nitrates have variable half-lives and active metabolites. The interaction can still occur, making this approach unsafe.
D. “These drugs are compatible with each other, and so I'll write a prescription.” This is factually incorrect; combining PDE5 inhibitors and nitrates is contraindicated and can result in life-threatening hypotension.
Test-taking strategy:
• Focus on drug interactions and contraindications rather than therapeutic intent.
• Identify medications with additive vasodilatory effects.
• Prioritize patient safety and recognize absolute contraindications in cardiovascular care.
Take-home points:
• PDE5 inhibitors (e.g., sildenafil) are contraindicated with nitrates due to severe hypotension risk.
• All forms of nitrates, including isosorbide dinitrate and mononitrate, pose the same interaction risk.
• Patient education must emphasize avoiding concurrent use and reporting any chest pain management concerns to a healthcare provider.
The nurse is reviewing drug interactions with a male client who has a prescription for isosorbide dinitrate (Isordil) as treatment for angina symptoms. Which substances listed below could potentially result in a drug interaction? Select all that apply
Explanation
Isosorbide dinitrate is a nitrate vasodilator used to treat angina pectoris by reducing myocardial oxygen demand through venous and arterial dilation. Nitrates interact with substances that also affect vascular tone or blood pressure, potentially causing additive hypotension, syncope, or cardiovascular collapse. Recognizing these interactions is essential for patient safety, adherence, and the prevention of life-threatening complications.
Rationale for the correct answers:
A. A glass of wine. Alcohol is a vasodilator that can potentiate the hypotensive effects of nitrates. Even moderate alcohol intake can lead to dizziness, syncope, and falls, especially in older adults or those with pre-existing cardiovascular disease. Patients should be cautioned about concurrent alcohol use when taking nitrates.
C. Tadalafil (Cialis), an erectile dysfunction drug. PDE5 inhibitors like tadalafil enhance nitric oxide–mediated vasodilation, which can synergistically lower blood pressure when combined with nitrates. This interaction can precipitate severe hypotension, myocardial ischemia, or shock, making concurrent use contraindicated.
E. Carvedilol (Coreg), a beta blocker. Carvedilol reduces heart rate and cardiac output. When combined with nitrates, the additive effect on blood pressure reduction can lead to symptomatic hypotension, dizziness, or syncope, particularly at therapy initiation or dose escalation. Close monitoring of hemodynamic parameters is necessary.
Rationales for the incorrect answers:
B. Thyroid replacement hormone. Thyroid hormone does not directly interact with nitrates or significantly affect blood pressure in a way that creates an acute risk. Standard dosing for hypothyroidism is generally safe.
D. Metformin (Glucophage), an antidiabetic drug. Metformin does not have pharmacodynamic or pharmacokinetic interactions with nitrates. Blood pressure and vascular effects are not significantly altered, making co-administration generally safe.
Test-taking strategy:
• Identify drugs or substances with additive vasodilatory effects when considering nitrates.
• Focus on interactions that increase risk for hypotension, dizziness, or syncope.
• Remember that PDE5 inhibitors and alcohol are high-risk combinations with nitrates.
Take-home points:
• Avoid alcohol while taking nitrates due to risk of additive hypotension.
• PDE5 inhibitors (e.g., tadalafil, sildenafil) are contraindicated with nitrates.
• Monitor blood pressure closely when combining nitrates with beta blockers or other antihypertensives.
The nurse is taking a medication history from a client who has angina and is to begin taking ranolazine (Ranexa). The nurse should report which of the following medications in the client’s history that may interact with ranolazine? Select all that apply
Explanation
Ranolazine (Ranexa) is an antianginal medication that works by inhibiting the late sodium current in cardiac myocytes, which reduces intracellular calcium accumulation, decreases ventricular tension, and improves myocardial oxygen efficiency. It is prescribed for chronic angina when other therapies are insufficient. Ranolazine has multiple drug interactions, primarily through CYP3A metabolism and P-glycoprotein pathways, making it essential to review the client’s medication history carefully to prevent toxicity, arrhythmias, or adverse effects.
Rationale for the correct answers:
A. Digoxin (Lanoxin). Ranolazine can increase serum digoxin levels via P-glycoprotein inhibition, raising the risk of digoxin toxicity, which may present as arrhythmias, nausea, or visual disturbances. Monitoring and possible dose adjustment are required when these drugs are co-administered.
B. Simvastatin (Zocor). Ranolazine inhibits CYP3A4, which can significantly increase simvastatin plasma levels, elevating the risk of rhabdomyolysis and myopathy. Dose adjustments or alternative statins may be necessary to reduce complications.
C. Verapamil (Calan). Both verapamil and ranolazine are CYP3A inhibitors, and co-administration can elevate ranolazine levels, increasing the risk of QT prolongation and ventricular arrhythmias. Careful monitoring or avoidance is indicated.
Rationales for incorrect answers:
D. Amlodipine (Norvasc). Amlodipine is a CYP3A4 substrate, but it has a minimal effect on ranolazine metabolism at typical doses. While caution is advised, it is not considered a major interacting drug requiring reporting in this context.
E. Nitroglycerin transdermal patch (Nitro-Dur). Nitroglycerin can be safely co-administered with ranolazine. Their mechanisms are complementary (nitrate-induced vasodilation vs. sodium channel inhibition) without significant pharmacokinetic or pharmacodynamic interaction.
Test-taking strategy:
• Identify medications metabolized via CYP3A or P-glycoprotein pathways that can interact with ranolazine
• Focus on drugs with narrow therapeutic indices like digoxin or medications prone to QT prolongation
• Eliminate options that do not affect ranolazine metabolism or increase its toxicity risk
Take-home points:
• Ranolazine interacts with CYP3A4 inhibitors and P-glycoprotein substrates, including digoxin, verapamil, and simvastatin
• Co-administration with these drugs may lead to toxicity or serious arrhythmias
• Nitrates and calcium channel blockers like amlodipine can be used concurrently with minimal risk, but monitoring is recommended
Case Scenario
A client seen in the emergency department came in complaining of pain in the chest radiating down the left arm. It started while the client was mowing the lawn.
The client was diagnosed with angina and the nurse was evaluating the anginal attack.
Which assessment data are needed for evaluation? Indicate with an X which data are essential and which are unrelated to evaluating an anginal attack.
Explanation
The nurse is evaluating a client presenting with anginal chest pain, which is typically caused by myocardial ischemia due to reduced coronary blood flow. Proper assessment requires distinguishing clinical signs directly associated with angina from unrelated information, ensuring accurate diagnosis, treatment planning, and timely interventions. Understanding the pattern, associated symptoms, and risk factors is essential for safe and effective management.
Rationale for correct answer:
ESSENTIAL ASSESSMENT DATA
- Pain occurring with exercise. Angina is often exertional, triggered by increased myocardial oxygen demand. Documenting the relationship between activity and pain helps determine the pattern of ischemia.
- Shortness of breath with chest pain. Dyspnea is a common associated symptom of myocardial ischemia and may indicate more severe or extensive cardiac involvement.
- Indigestion or nausea present. Gastrointestinal symptoms, particularly nausea or epigastric discomfort, can occur with angina, especially in older adults or women, and should be noted.
- Family history for heart disease. A positive family history is a significant risk factor for coronary artery disease, providing context for the client’s presentation.
- Feeling faint or lightheaded. Presyncope or dizziness can result from decreased cardiac output during an anginal episode and signals hemodynamic compromise.
- Reporting palpitations. Arrhythmias may accompany angina or precipitate myocardial ischemia, making this symptom clinically relevant.
- Smoking history. Tobacco use increases atherosclerotic risk and directly contributes to coronary artery disease, making it essential in risk assessment.
UNRELATED ASSESSMENT DATA
- Periods of insomnia. While overall health is important, sleep patterns do not directly evaluate an anginal attack.
- Unable to remember recent events. Cognitive deficits are unrelated to the acute assessment of angina.
- Reporting muscle cramps in lower legs. Peripheral muscle cramps are not linked to myocardial ischemia and are unrelated in the context of anginal assessment.
Test-taking strategy:
• Focus on symptoms and risk factors directly associated with myocardial ischemia.
• Eliminate assessment data unrelated to acute angina presentation, such as general health concerns or non-cardiac symptoms.
• Prioritize information that helps determine the pattern, severity, and triggers of anginal attacks.
Take-home points:
• Essential assessment data include pain characteristics, associated symptoms, and cardiac risk factors.
• Distinguish unrelated health information to avoid misprioritization during evaluation.
• Comprehensive assessment allows timely and accurate management of anginal episodes.
Choose the most likely option for the information missing from the following sentence by selecting from the list of options provided.
The nurse discussed with the client in the scenario that there are different types of angina and stated that
Explanation
Correct answer: The nurse discussed with the client in the scenario that there are different types of angina and stated that chronic stable angina occurs with a fixed obstruction; compared with unstable angina, which occurs with new thrombus formation.
The nurse is educating the client about different types of angina, emphasizing the pathophysiology and triggers of each type. Understanding these distinctions helps the client recognize warning signs, respond appropriately to symptoms, and adhere to prescribed interventions. Chronic stable angina and unstable angina differ in their underlying mechanisms, onset, and clinical significance, which directly impacts risk assessment and management strategies.
Rationale for correct answer:
Chronic stable angina occurs with a fixed obstruction; compared with unstable angina, which occurs with new thrombus formation. Chronic stable angina is typically caused by atherosclerotic plaque narrowing the coronary arteries, resulting in predictable episodes of myocardial ischemia, usually triggered by exertion or stress. The obstruction is relatively fixed, so symptoms are consistent in frequency, duration, and intensity, and subside with rest or nitroglycerin.
Unstable angina, in contrast, arises from acute changes in a coronary artery, such as plaque rupture or thrombus formation, leading to sudden partial occlusion. Symptoms are more severe, unpredictable, and can occur at rest, signaling a higher risk for myocardial infarction. Recognizing these distinctions allows clients and healthcare providers to identify urgent cardiac events requiring prompt intervention.
Rationales for incorrect options:
Palpitations are a symptom rather than a type of angina.
Vasodilation does not accurately explain the mechanism of stable versus unstable angina.
Dysrhythmias are a possible complication but not the defining mechanism of chronic stable angina.
A fixed obstruction defines stable angina, not unstable angina; unstable angina involves dynamic obstruction such as thrombus formation.
Test-taking strategy:
• Focus on the pathophysiology and triggers of angina types.
• Recall that chronic stable angina = fixed atherosclerotic obstruction, predictable, whereas unstable angina = dynamic obstruction, unpredictable, new thrombus formation.
• Eliminate options that confuse symptoms, complications, or unrelated mechanisms with the type of angina.
Take-home points:
• Chronic stable angina occurs due to a fixed obstruction, causing predictable, exertion-related symptoms.
• Unstable angina involves new thrombus formation, resulting in unpredictable and potentially life-threatening episodes.
• Accurate knowledge of angina types supports patient education, early symptom recognition, and timely emergency interventions.
After the administration of sublingual nitroglycerin to the client in the scenario with angina, the nurse explained to the client which of the following adverse effects may be experienced? Select all that apply
Explanation
The nurse is caring for a client with angina pectoris, a condition caused by myocardial ischemia due to reduced coronary blood flow. The client has been prescribed sublingual nitroglycerin, a nitrate that dilates coronary and systemic blood vessels, improving oxygen delivery to the heart and relieving chest pain. While nitroglycerin is highly effective for acute anginal attacks, it is associated with specific cardiovascular and systemic adverse effects that clients should understand to ensure safe use and proper monitoring. Client education emphasizes recognizing common side effects, preventing falls, and knowing when to seek medical attention.
Rationale for correct answers:
B. Nausea. Nitroglycerin can cause nausea due to vasodilation and mild hypotension, which may reduce gastrointestinal perfusion or trigger vagal responses. Clients may experience mild gastrointestinal upset, which typically resolves with symptom management.
C. Lightheadedness. As a potent vasodilator, nitroglycerin lowers systemic blood pressure, which can lead to dizziness or lightheadedness, particularly when changing positions (orthostatic hypotension). This effect is important for fall prevention, and clients should be advised to sit or lie down when taking sublingual tablets.
E. Headache. Headache is a common and expected adverse effect of nitroglycerin due to cerebral vasodilation. Although uncomfortable, it generally indicates the medication is pharmacologically active. Analgesics may be used if headaches are severe, but clients should report persistent or unusual headaches.
G. Syncope. Severe hypotension or rapid vasodilation can occasionally lead to syncope. Clients must be cautioned about standing quickly after taking nitroglycerin and to notify healthcare providers if fainting occurs.
Rationales for incorrect answers:
A. Drowsiness. Nitroglycerin does not directly affect the central nervous system to induce drowsiness, so this is not a typical adverse effect.
D. Vasoconstriction. Nitroglycerin causes vasodilation, not vasoconstriction.
F. Pain control. Pain relief is the therapeutic effect, not an adverse effect of nitroglycerin.
8. Shortness of breath. While hypotension-related dizziness may occur, nitroglycerin does not typically cause shortness of breath; respiratory symptoms would indicate another underlying condition.
Test-taking strategy:
• Identify common cardiovascular-related adverse effects of nitrates.
• Distinguish between therapeutic outcomes and side effects.
• Consider the mechanism of action (vasodilation leading to hypotension) when evaluating adverse effects.
Take-home points:
• Common adverse effects of sublingual nitroglycerin include nausea, lightheadedness, headache, and syncope.
• Advise clients to sit or lie down during administration to reduce risk of falls.
• Educate clients that headaches indicate drug activity and are generally harmless but should be reported if severe or persistent.
Choose the most likely option for the information missing from the following sentence by selecting from the list of options provided.
The client in the scenario diagnosed with angina will have their symptoms controlled with medications such as
Explanation
Correct answer: The client in the scenario diagnosed with angina will have their symptoms controlled with medications such as metoprolol and isosorbide dinitrate, which are classified as beta-adrenergic blocker and nitrate, respectively.
The nurse is educating the client about medications used to manage angina, emphasizing their mechanisms of action and therapeutic effects. Proper understanding helps the client adhere to therapy, recognize expected effects, and monitor for adverse reactions. Beta-adrenergic blockers and nitrates are commonly prescribed to prevent anginal episodes, reduce myocardial oxygen demand, and improve exercise tolerance.
Rationale for correct answer:
Metoprolol and isosorbide dinitrate, which are classified as beta-adrenergic blocker and nitrate, respectively. Metoprolol, a beta-adrenergic blocker, works by blocking beta1 receptors in the heart, leading to decreased heart rate, myocardial contractility, and cardiac output, which collectively reduce myocardial oxygen demand. This makes the heart less susceptible to ischemia during exertion.
Isosorbide dinitrate, a nitrate, acts primarily through vasodilation, particularly of the venous system, which reduces preload and myocardial oxygen consumption. Nitrates also dilate coronary arteries to improve oxygen supply to ischemic myocardial tissue. When used together, these drugs complement each other by reducing oxygen demand (beta blocker) and improving oxygen supply (nitrate), effectively preventing anginal attacks.
Rationales for incorrect options:
HMG-CoA inhibitors (statins) lower cholesterol but do not directly control anginal symptoms.
ACE inhibitors and ARBs manage hypertension and heart failure but are not first-line for symptom control in stable angina.
Statins address lipid management, not angina symptom relief, though beta blockers are correct in mechanism.
ARBs like losartan reduce blood pressure and cardiovascular risk but do not directly alleviate anginal symptoms.
Test-taking strategy:
• Identify the medications that directly relieve or prevent angina symptoms.
• Recall mechanisms of action. beta blockers reduce myocardial oxygen demand, nitrates reduce preload and improve coronary perfusion.
• Eliminate options involving drugs that target risk factors rather than acute or exertional anginal symptoms.
Take-home points:
• Beta-adrenergic blockers decrease heart rate and myocardial oxygen demand to prevent angina.
• Nitrates dilate blood vessels, improving oxygen supply and reducing cardiac workload.
• Combining these medications provides complementary mechanisms to optimize angina symptom control.
The nurse administering the calcium channel blocker amlodipine (Norvasc) explained to the client what effect the drug has on the heart. Which statement is appropriate for the nurse to make? Select all that apply
Explanation
The nurse is educating a client about amlodipine (Norvasc), a calcium channel blocker, which is commonly prescribed for angina and hypertension. Calcium channel blockers work by inhibiting the influx of calcium ions into cardiac and vascular smooth muscle, leading to vasodilation, decreased myocardial contractility, and reduced oxygen demand on the heart. Understanding the mechanism of action and therapeutic effects helps the client use the medication safely, adhere to treatment, and recognize the benefits and limitations of therapy.
Rationale for correct answers:
A. “This drug will prevent angina by dilating the coronary vessels.” Amlodipine relaxes coronary artery smooth muscle, improving blood flow to the myocardium. This vasodilation reduces ischemia during exertion or stress, preventing anginal episodes. Improved coronary perfusion is a primary mechanism for symptom relief in angina.
C. “This drug will prevent angina by blocking the movement of calcium ions, which in turn decreases oxygen demand on the heart.” By blocking L-type calcium channels, amlodipine reduces calcium entry into myocardial cells, decreasing myocardial contractility and vascular tone. This lowers systemic vascular resistance and myocardial oxygen consumption, making it easier for the heart to meet oxygen demands and preventing ischemic pain.
Rationales for incorrect answers:
B. “This drug will prevent angina by blocking the receptors in the heart that increase the heart rate.” This describes beta-adrenergic blockers, not calcium channel blockers. Amlodipine does not selectively block beta receptors, so heart rate modulation is not its primary effect.
D. “This drug will prevent angina by blocking the conversion of angiotensin I to angiotensin II, which is a potent vasoconstrictor.” This describes ACE inhibitors, not calcium channel blockers. Amlodipine does not interfere with the renin-angiotensin-aldosterone system.
E. “This drug will prevent angina by blocking the sodium channels in the myocardial cells.” Sodium channel blockade is the mechanism of class I antidysrhythmic drugs (e.g., lidocaine or flecainide), not calcium channel blockers.
Test-taking strategy:
• Focus on the mechanism of action of calcium channel blockers.
• Eliminate options describing other cardiovascular drug classes (beta blockers, ACE inhibitors, sodium channel blockers).
• Connect the pharmacologic effect to angina prevention via decreased myocardial oxygen demand.
Take-home points:
• Amlodipine prevents angina primarily by dilating coronary vessels and reducing calcium influx into myocardial cells.
• It decreases myocardial oxygen demand, alleviating ischemic pain.
• Clients should understand the specific mechanism of action to recognize how the medication works and differentiate it from other cardiac drugs.
The nurse was discussing risk factor management with the client who was admitted with chest pain and realized that the client needed further education after he made which statement?
Explanation
The nurse is providing education on risk factor management for coronary artery disease (CAD) and angina, emphasizing lifestyle modification, adherence to treatment, and preventive measures. Effective client teaching focuses on reducing modifiable risk factors such as smoking, sedentary lifestyle, poor diet, and lack of engagement in self-care, in addition to taking prescribed medications. Misconceptions about relying solely on medications indicate the need for further education to ensure comprehensive management and prevention of future cardiac events.
Rationale for correct answer:
D. “I figure I don’t need to do anything different; I can just take my pills for this.” This demonstrates a misunderstanding of CAD management. While medications are important for controlling symptoms and preventing complications, lifestyle modifications are critical in reducing risk factors such as hyperlipidemia, hypertension, obesity, and smoking-related vascular damage. Without addressing modifiable behaviors, the client remains at high risk for recurrent angina, myocardial infarction, or other cardiovascular events. The nurse should provide targeted education on diet, exercise, smoking cessation, and stress management in addition to pharmacologic therapy.
Rationales for incorrect answers:
A. “I know that I should quit smoking. I have been meaning to for a while, but this really hits home that I need to.” This statement shows awareness and motivation to reduce a major modifiable risk factor, demonstrating appropriate understanding of preventive measures.
B. “I think maybe I should learn to cook because my wife always insists on meat and potatoes and gravy; we have such heavy meals.” This indicates recognition of dietary modification as part of CAD risk management, which is consistent with proper client education.
C. “I walk every day with my dog for at least 20 minutes and longer in nice weather.” This shows engagement in regular physical activity, an important nonpharmacologic strategy to improve cardiovascular health and manage angina risk.
Test-taking strategy:
• Identify statements that reflect misconceptions or unsafe assumptions about CAD management.
• Focus on modifiable lifestyle factors versus sole reliance on medications.
• Prioritize teaching opportunities that enhance long-term cardiovascular outcomes.
Take-home points:
• Medications alone are insufficient for CAD management; lifestyle modification is essential.
• Encourage clients to address smoking, diet, and physical activity alongside prescribed therapy.
• Assess client understanding regularly and provide reinforcement to ensure adherence to comprehensive preventive strategies.
Exams on Drugs Used to Treat Angina Pectoris
Custom Exams
Login to Create a Quiz
Click here to loginLessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Define angina pectoris and explain its pathophysiology.
- Identify the types of angina (stable, unstable, and variant/Prinzmetal) and describe their clinical manifestations.
- Explain the primary goals of pharmacologic therapy for angina.
- Classify the main pharmacologic agents used to treat angina and describe their therapeutic categories.
- Describe the mechanism of action of organic nitrates, beta-blockers, calcium channel blockers, antiplatelet agents, ACE inhibitors, and statins.
- Identify routes of administration and dosage forms for each drug class.
- Recognize expected pharmacologic effects and clinical outcomes of the medications.
- Identify common and serious adverse effects, contraindications, and precautions for each class of antianginal medications.
- Outline key nursing interventions to ensure safe administration and detect complications.
- Educate patients effectively on proper medication use and lifestyle modifications.
Introduction
Angina pectoris
- Angina pectoris is a clinical syndrome characterized by transient chest discomfort or pain resulting from myocardial ischemia.
- This is typically due to an imbalance between myocardial oxygen supply and demand.
- It is most commonly associated with coronary artery disease (CAD), where atherosclerotic plaque reduces coronary perfusion.
Angina pectoris may present in several clinically distinct forms; stable, unstable, and variant (Prinzmetal) angina.
Each of them is defined by unique pathophysiologic mechanisms, precipitating factors, and implications for pharmacologic management and nursing care.
- Stable angina
Stable angina is the most common form and is typically caused by fixed atherosclerotic narrowing of the coronary arteries, resulting in predictable episodes of myocardial ischemia.
Symptoms are usually precipitated by increased myocardial oxygen demand, such as during physical exertion, emotional stress, or exposure to cold, and are relieved by rest or short-acting nitrates.
Because coronary obstruction is relatively constant, stable angina reflects a chronic imbalance between oxygen supply and demand.
- Unstable angina
Unstable angina represents a more acute and dangerous condition and is often classified as part of the acute coronary syndrome (ACS) spectrum.
It is commonly caused by plaque rupture, platelet aggregation, and partial thrombus formation. This leads to a sudden reduction in coronary blood flow.
Anginal episodes may occur at rest, with minimal exertion, or with increasing frequency and severity, and are often poorly relieved by rest or nitrates.
Unstable angina signals a high risk for myocardial infarction and sudden cardiac death, requiring urgent medical intervention.
- Variant angina (Prinzmetal angina
Variant angina (Prinzmetal angina) is caused by transient coronary artery vasospasm, rather than fixed atherosclerotic obstruction.
It typically occurs at rest, often during the early morning hours, and may be accompanied by transient ST-segment elevation on ECG during episodes of chest pain.
Myocardial ischemia in variant angina results from temporary reduction in coronary blood flow due to smooth muscle constriction.
This form of angina responds well to vasodilator therapy, particularly calcium channel blockers and nitrates. Beta-blockers may worsen symptoms in some patients.
PHARMACOLOGICAL MANAGEMENT FOR ANGINA
Pharmacologic therapy targets two primary objectives:
- Reduction of myocardial oxygen demand
- Enhancement of oxygen supply to ischemic myocardial tissue.
The medications are carefully selected based on the type of angina, comorbid conditions, and patient-specific risk factors.
Nursing considerations, patient education, and continuous monitoring are crucial for optimizing therapy and preventing complications.
The pharmacologic classes include:
- Organic Nitrates: Nitrates primarily dilate venous and coronary vessels, reducing myocardial workload and oxygen demand while relieving coronary spasms. They are the mainstay for both acute and prophylactic angina therapy.
- Beta-Adrenergic Blockers: By selectively blocking beta-1 adrenergic receptors in the heart, these medications reduce heart rate, myocardial contractility, and blood pressure, thereby lowering oxygen consumption and preventing angina episodes.
- Calcium Channel Blockers: These relax vascular smooth muscle, producing arterial vasodilation and decreased afterload. Non-dihydropyridine agents additionally decrease heart rate and myocardial contractility, effectively reducing oxygen demand.
- Antiplatelet Agents: By inhibiting platelet aggregation, these agents decrease the risk of thrombus formation within coronary arteries, providing cardioprotective benefits, especially in patients with chronic stable angina or post-myocardial infarction.
- ACE Inhibitors: These medications block the conversion of angiotensin I to angiotensin II, causing vasodilation, reduced afterload, and cardioprotective effects, particularly important for patients with coexisting hypertension or post-MI remodeling risk.
- Cholesterol-Lowering Medications (Statins): Statins inhibit HMG-CoA reductase, reducing endogenous cholesterol synthesis, lowering low-density lipoprotein (LDL) levels, and decreasing atherosclerotic plaque progression, which is essential for long-term angina and cardiovascular risk management.
Organic Nitrates
Drug Name
- Generic: Nitroglycerin
- Brand Names: Nitrostat (sublingual), Nitro-Dur (transdermal patch), Nitro-Bid (ointment), Nitro-Time (oral capsule), Nitrolingual (spray), Nitro-Bid IV
Classification
- Pharmacologic class: Organic nitrate
- Therapeutic class: Antianginal
Mechanism of Action (MOA)
- Dilates veins - decreases venous return (preload) - reduces myocardial oxygen demand.
- Relaxes coronary artery spasms in variant angina - increases oxygen supply.
- NCLEX focus: Relieves chest pain by balancing oxygen supply and demand.
Indications
- Acute angina attacks
- Chronic stable angina prophylaxis
- Variant (Prinzmetal’s) angina
- Heart failure post-MI
- Perioperative blood pressure control
Routes of Administration
- Sublingual tablet
- Translingual spray
- Oral extended-release capsule
- Transdermal patch
- Topical ointment
- Intravenous infusion
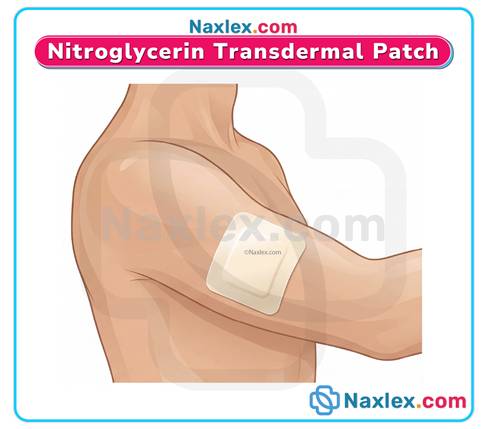
Pharmacologic Effects
- Relief of angina
- Prevention of anginal episodes
- Reduction in myocardial oxygen demand
Common Adverse Effects
- Headache
- Dizziness
- Orthostatic hypotension
- Reflex tachycardia
- Flushing
Serious Adverse Reactions
- Severe hypotension - syncope
- Tolerance with long-term use
- Rare: increased intracranial pressure
Contraindications & Precautions
- Hypersensitivity to nitrates
- Severe anemia
- Head trauma or intracranial pressure
- Pregnancy Risk Category C
- Caution: renal/liver dysfunction, concurrent antihypertensives
Nursing Interventions
- Monitor BP and HR before and during administration
- Sit or lie patient down if dizziness occurs
- Rotate patch/ointment sites to avoid skin irritation
- Educate on nitrate-free periods to reduce tolerance (10–12 hr/day)
- Continuous cardiac monitoring for IV use
Monitoring
- BP, HR
- ECG for IV infusion
- Monitor frequency, duration, and intensity of angina
Patient Education
- Use sublingual tablet or spray at first sign of chest pain; do not exceed 3 tablets in 15 min
- Store sublingual tablets properly (cool, dark place)
- Avoid alcohol and PDE5 inhibitors (Viagra, Cialis, Levitra)
- Record angina episodes
Antidote / Reversal Agents
- Supportive care for hypotension: Trendelenburg position, IV fluids, vasopressors if needed
Drug Interactions
- PDE5 inhibitors - life-threatening hypotension
- Alcohol, beta-blockers, calcium channel blockers - additive hypotensive effects
Sublingual Tablets & Translingual Spray
- Rapid onset, short duration – used to treat acute angina
- Place tablet under tongue; spray onto oral mucosa, do not inhale
- Store in original container, cool and dark
Oral Extended-Release Capsules
- Slow onset, long duration – used to prevent angina
- Take on empty stomach with ≥8 oz water
- Do not crush or chew
Transdermal Patch
- Slow onset, long duration - used to prevent angina
- Apply to hairless area
- Rotate the application sites
- Remove at night to prevent tolerance
- Do not cut the transdermal patch
Topical Ointment
- Apply the specific dose to a clean, hairless area, cover with plastic wrap
- Wash hands after application
- Rotate the application sites
- Remove the previous dose before the new application
Intravenous
- Continuous infusion for uncontrolled angina, or acute heart failure post-MI
- Use manufacturer IV tubing or glass bottle
- Titrate slowly.
- Ensure continuous cardiac monitoring
Beta-adrenergic Blockers
Drug Name
- Generic: Metoprolol
- Brand Names: Lopressor, Toprol XL
Classification
- Pharmacologic class: Beta-1 selective adrenergic blocker
- Therapeutic class: Antianginal, antihypertensive
Mechanism of Action (MOA)
- Blocks beta-1 receptors: decreases HR, contractility, and BP;reduces myocardial oxygen demand
- NCLEX focus: Prevents angina by reducing workload of heart
Therapeutic Uses / Indications
- Chronic stable angina
- Hypertension
- Post-MI to prevent recurrent events
- Heart failure (selective agents)
Routes of Administration
- Oral (immediate or extended-release)
- IV (for acute situations)
Pharmacologic Effects
- Lowered HR, BP, and myocardial oxygen consumption
- Prevention of angina attacks
Common Adverse Effects
- Fatigue
- Dizziness
- Bradycardia
- Hypotension
Serious Adverse Reactions
- Heart block
- Severe bradycardia
- Pulmonary edema in heart failure patients
Contraindications & Precautions
- Severe bradycardia or heart block
- Cardiogenic shock
- Pregnancy Risk Category C
- Use cautiously in asthma (non-selective beta-blockers)
Nursing Interventions
- Monitor HR and BP before each dose
- Hold if HR <50 bpm or systolic BP <90 mmHg
- Educate patient to rise slowly to prevent dizziness
Monitoring
- HR, BP
- ECG if IV
- Blood glucose in diabetics (may mask hypoglycemia)
Patient Education
- Take at same time daily
- Do not abruptly stop (risk of rebound angina/MI)
- Monitor for dizziness, fatigue, or slow HR
Antidote / Reversal Agents
- Atropine for bradycardia
- IV fluids, vasopressors for hypotension
Drug Interactions
- Calcium channel blockers; additive bradycardia
- Insulin; hypoglycemia may be masked
- Digoxin; bradycardia risk
Calcium Channel Blockers
Drug Name
- Generic: Amlodipine, Diltiazem
- Brand Names: Norvasc (Amlodipine), Cardizem, Tiazac (Diltiazem)
Classification
- Pharmacologic class: Calcium channel blocker (dihydropyridine: amlodipine; nondihydropyridine: diltiazem)
- Therapeutic class: Antianginal, antihypertensive
Mechanism of Action (MOA)
- Relax vascular smooth muscle; vasodilation; decreased afterload and coronary resistance
- Nondihydropyridines (diltiazem) also decrease HR - reduce myocardial oxygen demand
Indications
- Chronic stable angina
- Variant angina
- Hypertension
- Arrhythmias (diltiazem)
Routes of Administration
- Oral (PO)
- Extended-release formulations
- IV (diltiazem for acute arrhythmias)
Pharmacologic Effects
- Reduced angina frequency
- Decreased BP and afterload
- Improved coronary perfusion
Common Adverse Effects
- Peripheral edema (amlodipine)
- Headache, dizziness
- Flushing
- Bradycardia (diltiazem)
Serious Adverse Reactions
- Severe hypotension
- Heart block (diltiazem)
- Worsening heart failure
Contraindications & Precautions
- Severe hypotension
- Heart block (for nondihydropyridines)
- Heart failure with reduced ejection fraction
- Pregnancy: use cautiously
Nursing Interventions
- Monitor BP, HR, and edema
- Assess for chest pain frequency
- Educate patient on slow position changes
Monitoring
- ECG for heart rate and rhythm
- BP monitoring
Patient Education
- Avoid grapefruit juice (increases drug levels)
- Report dizziness, slow HR, swelling
- Take extended-release tablets whole
Antidote / Reversal Agents
- IV calcium or vasopressors for severe hypotension
Drug Interactions
- Beta-blockers; additive bradycardia
- Grapefruit juice; increased drug levels
- Digoxin; increased levels (diltiazem)
Antiplatelet Agents
Drug Name
- Generic: Aspirin, Clopidogrel
- Brand Names: Bayer (Aspirin), Plavix (Clopidogrel)
Classification
- Pharmacologic class: Antiplatelet
- Therapeutic class: Cardioprotective
Mechanism of Action (MOA)
- Inhibits platelet aggregation - prevents thrombus formation
- NCLEX focus: Reduces risk of MI in angina patients
Indications
- Chronic stable angina
- Acute coronary syndrome
- Post-MI prophylaxis
Routes of Administration
- Oral
Pharmacologic Effects
- Reduced clot formation
- Prevention of MI and stroke
Common Adverse Effects
- GI upset
- Heartburn
- Bleeding tendencies

Serious Adverse Reactions
- GI bleeding
- Hemorrhagic stroke
- Thrombocytopenia
Contraindications & Precautions
- Active bleeding
- Peptic ulcer disease
- Pregnancy Category C (aspirin: D in 3rd trimester)
Nursing Interventions
- Assess for signs of bleeding
- Monitor platelet counts if prolonged therapy
- Teach patient to report unusual bruising or bleeding
Monitoring
- CBC, Hgb, Hct
- Stool for occult blood
Patient Education
- Take with food to prevent GI upset
- Avoid OTC NSAIDs unless approved
- Use soft toothbrush and electric razor
Antidote / Reversal Agents
- Platelet transfusion for severe bleeding
Drug Interactions
- Anticoagulants - increased bleeding risk
- NSAIDs - increased GI bleeding
Ace Inhibitors
Drug Name
- Generic: Lisinopril
- Brand Names: Prinivil, Zestril
Classification
- Pharmacologic class: ACE inhibitor
- Therapeutic class: Antihypertensive, cardioprotective
Mechanism of Action (MOA)
- Blocks conversion of angiotensin I - II - vasodilation and decreased afterload
- Reduces cardiac workload and risk of remodeling post-MI
Indications
- Chronic stable angina (cardioprotective)
- Hypertension
- Heart failure
- Post-MI prevention
Routes of Administration
- Oral
Pharmacologic Effects
- Lowered BP
- Reduced angina frequency
- Cardioprotective effects
Common Adverse Effects
- Dry cough
- Dizziness
- Hyperkalemia
Serious Adverse Reactions
- Angioedema
- Severe hypotension
- Renal impairment
Contraindications & Precautions
- Pregnancy Category D
- Bilateral renal artery stenosis
- Hyperkalemia
Nursing Interventions
- Monitor BP, HR
- Assess for cough, angioedema
- Monitor renal function and electrolytes
Monitoring
- Serum creatinine, BUN
- Potassium levels
Patient Education
- Rise slowly to avoid dizziness
- Report swelling of face, lips, tongue
- Avoid potassium supplements or salt substitutes
Antidote / Reversal Agents
- Supportive care; IV fluids, vasopressors if severe hypotension
Drug Interactions
- Potassium-sparing diuretics - hyperkalemia
- NSAIDs - reduced antihypertensive effect
- Other antihypertensives - additive hypotension
Cholesterol-lowering Medications (statins)
Drug Name
- Generic: Atorvastatin
- Brand Names: Lipitor
Classification
- Pharmacologic class: HMG-CoA reductase inhibitor
- Therapeutic class: Lipid-lowering, cardioprotective
Mechanism of Action (MOA)
- Inhibits HMG-CoA reductase - decreases cholesterol synthesis - reduces plaque formation
- NCLEX focus: Lowers LDL, reduces atherosclerotic risk
Indications
- Hypercholesterolemia
- Cardiovascular disease prevention
- Post-MI secondary prevention
Routes of Administration
- Oral
Pharmacologic Effects
- Lower LDL cholesterol
- Reduce risk of MI and stroke
Common Adverse Effects
- Mild GI upset
- Muscle pain or weakness (myalgia)
- Headache
Serious Adverse Reactions
- Rhabdomyolysis (muscle breakdown)
- Hepatotoxicity
Contraindications & Precautions
- Active liver disease
- Pregnancy Category X
- Caution in older adults
Nursing Interventions
- Baseline liver function tests
- Monitor for muscle pain, weakness
- Educate patient to report dark urine, muscle tenderness
Monitoring
- ALT, AST (liver function)
- CK if muscle pain occurs
Patient Education
- Take at bedtime
- Avoid grapefruit juice
- Maintain diet and exercise
Antidote / Reversal Agents
- No specific antidote; discontinue drug if severe toxicity occurs
Drug Interactions
- CYP3A4 inhibitors - increase risk of rhabdomyolysis
- Other hepatotoxic drugs - additive liver damage
Summary
- Angina pectoris: Chest pain from myocardial ischemia due to imbalance of oxygen supply and demand.
- Types: Stable, unstable, and variant (Prinzmetal) angina.
- Treatment goals:
- Reduce myocardial oxygen demand
- Increase oxygen supply to ischemic myocardium
- Nursing priorities: Monitor vital signs, patient education, and continuous assessment to prevent complications.
Pharmacologic Classes:
- Organic Nitrates (e.g., Nitroglycerin)
- Action: Venous and coronary vasodilation; reduce preload; relieve coronary spasms.
- Use: Acute angina, prophylaxis, variant angina, heart failure post-MI.
- Routes: Sublingual, spray, oral ER, transdermal patch, topical ointment, IV.
- Key monitoring: BP, HR, angina frequency; rotate patch/ointment sites.
- Patient teaching: Nitrate-free periods, avoid PDE5 inhibitors, proper storage.
- Beta-Adrenergic Blockers (e.g., Metoprolol)
- Action: Beta-1 blockade; reduce HR, contractility, BP; lower oxygen demand.
- Use: Chronic stable angina, hypertension, post-MI, heart failure (selective).
- Monitoring: HR, BP, ECG (IV), blood glucose in diabetics.
- Patient teaching: Do not abruptly stop; report dizziness, fatigue, bradycardia.
- Calcium Channel Blockers (e.g., Amlodipine, Diltiazem)
- Action: Arterial vasodilation; non-dihydropyridines decrease HR and contractility.
- Use: Stable angina, variant angina, hypertension, arrhythmias (diltiazem).
- Monitoring: BP, HR, ECG, edema.
- Patient teaching: Avoid grapefruit juice, report slow HR or swelling.
- Antiplatelet Agents (e.g., Aspirin, Clopidogrel)
- Action: Inhibit platelet aggregation; prevent coronary thrombosis.
- Use: Chronic stable angina, ACS, post-MI prophylaxis.
- Monitoring: Signs of bleeding, platelet count, CBC, stool occult blood.
- Patient teaching: Take with food, avoid OTC NSAIDs, use soft toothbrush.
- ACE Inhibitors (e.g., Lisinopril)
- Action: Block angiotensin I → II conversion; vasodilation; reduced afterload; cardioprotective.
- Use: Chronic stable angina (cardioprotection), hypertension, heart failure, post-MI.
- Monitoring: BP, renal function, potassium, signs of angioedema.
- Patient teaching: Rise slowly, avoid potassium supplements, report facial swelling.
- Cholesterol-Lowering Medications (Statins, e.g., Atorvastatin)
- Action: Inhibit HMG-CoA reductase; lower LDL; reduce atherosclerotic plaque progression.
- Use: Hypercholesterolemia, cardiovascular prevention, post-MI.
- Monitoring: Liver function tests, CK for muscle symptoms.
- Patient teaching: Take at bedtime, avoid grapefruit juice, maintain diet and exercise.
Key Nursing Points Across Classes:
- Assess angina frequency, intensity, and triggers.
- Monitor vital signs and cardiac rhythm as indicated.
- Educate patients on drug-specific precautions, side effects, and lifestyle modifications.
- Recognize serious adverse effects (e.g., severe hypotension, heart block, bleeding, rhabdomyolysis).
- Ensure patient adherence and safe administration, including route-specific considerations.
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Drugs Used to Treat Angina Pectoris
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
