
Nursing care during a pediatric emergency
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Understand the unique anatomical and physiological differences in children that impact emergency care.
- Understand the systematic approach to initial and secondary assessment of an ill or injured child.
- Understand how to perform age-appropriate Cardiopulmonary Resuscitation (CPR).
- Gain knowledge on the pathophysiology, diagnosis, and management of shock.
- Understand the pathophysiology, diagnosis, and management of trauma in pediatrics.
- Understand the pathophysiology, diagnosis, and management of acute poisonings
- Gain knowledge on the pathophysiology, diagnosis, and management of chronic heavy metal poisoning.
- Gain knowledge on the pathophysiology, diagnosis, and management of drowning.
- Identify key nursing diagnoses and interventions for various pediatric emergency situations.
Introduction
- Pediatric emergencies present a unique set of challenges due to the significant physiological and developmental differences between children and adults.
- Children are not simply "small adults"; their anatomy, metabolism, and psychological responses to illness and injury differ dramatically.
- The foundation of pediatric emergency care rests on a thorough understanding of the developmental stages and their impact on presentation and response to illness or injury. For example, an infant's large head size relative to their body makes them susceptible to head trauma, while their short, narrow, and more pliable airway can be easily compromised.
- Their higher metabolic rate and larger body surface area-to-weight ratio increase their risk for fluid and heat loss, and their underdeveloped immune systems make them more prone to severe infections.
- Furthermore, a child's psychological state and a parent's presence are critical factors in providing care; a calm, reassuring approach is essential for gaining a child's cooperation and alleviating parental anxiety.
- This document outlines the critical components of pediatric emergency care, starting with the fundamental principles of assessment and moving into specific clinical conditions.
- It is crucial that nurses are proficient in initial rapid assessment, which is the cornerstone of emergency care, to quickly identify life-threatening conditions.
Emergent Care
3.1. Initial Assessment
A systematic approach to assessing a critically ill or injured child is the cornerstone of effective emergent care. This process should be rapid and focused on identifying and correcting life-threatening conditions.
- Check for Safety: Before approaching the child, ensure the scene is safe for both you and the child. This includes checking for hazards like traffic, fire, or live electrical wires.
- Awaken the Child: Gently try to awaken the child by tapping their shoulder or the sole of their foot (for an infant) and asking if he or she is okay. Adding the child’s name, if it is known, may improve the possibility of the child responding. Use the AVPU scale (Alert, Verbal, Pain, Unresponsive) to assess their level of consciousness. When attempting to arouse the child, the nurse should be careful not to cause additional injury. In the case of a fall, for example, the neck should not be moved, if possible, to prevent injury to the spinal cord.
- Get Help: If the child fails to respond, the nurse should assume the worst and should shout “Help!” to attract the attention of others who can assist in the care of the child. If no one is available to assist, the nurse should care for the child for 2 full minutes, then leave the child and go to call for emergency personnel (e.g., call 911).
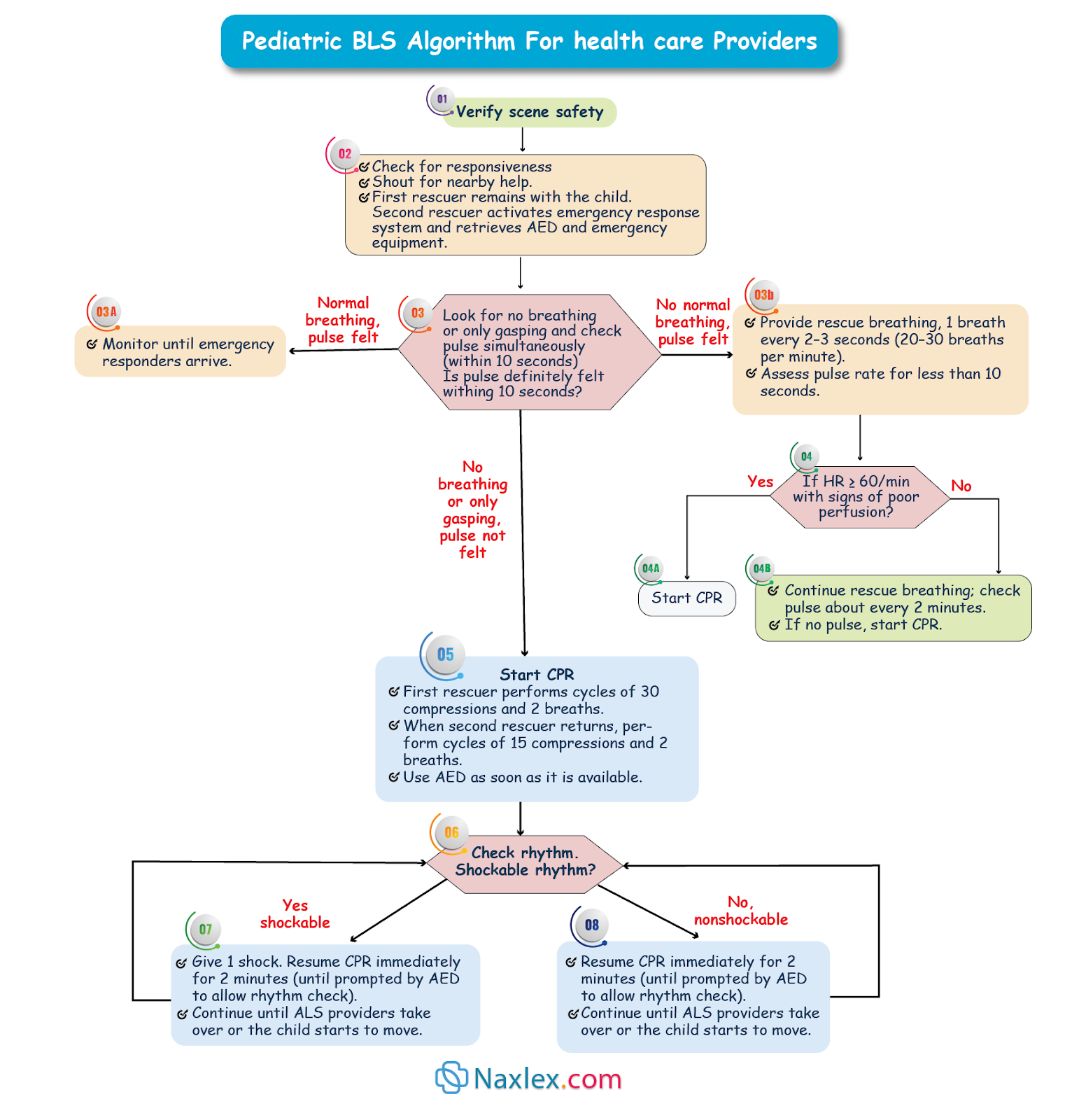
- Assess for Breathing: Look, listen, and feel for breathing. Look for chest rise and fall. Listen for breath sounds. Feel for air movement from the nose or mouth. Normal breathing should be effortless and quiet. Gasping is not considered effective breathing. If the child is not breathing at all or is only gasping for breath, the nurse should assume that the child is in need of resuscitation.
- Assess for a Pulse: This procedure should take no longer that 10 seconds.
- Infant (<1 year): Check the brachial pulse on the inside of the upper arm. This is because the carotid and femoral pulses are difficult to assess at this age.

-
- Child (1 year to puberty): Check the carotid or femoral pulse.

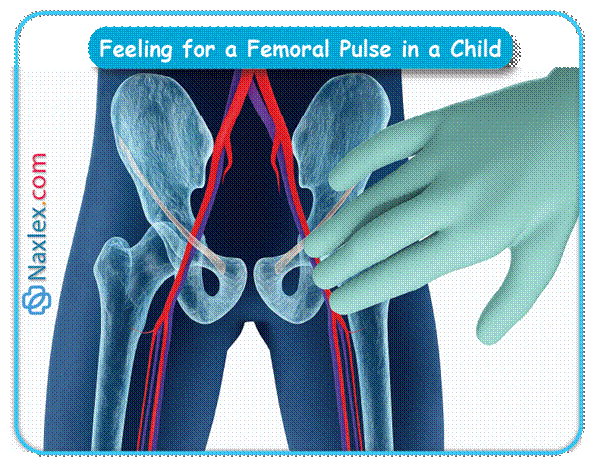
- Adolescent (puberty and older): Check the carotid pulse.
- If the pulse rate is greater than or equal to 60 bpm, rescue breaths should be administered at a rate of one every 3 to 5 sec (i.e., 12 to 20 per min).
- If the pulse rate is less than 60 bpm, and the child is exhibiting signs of poor oxygenation (e.g., pale, cyanotic), cardiopulmonary resuscitation (CPR) should be begun.
- Perform Age-Appropriate CPR (Acronym CAB): The standard CPR sequence has been updated to C-A-B (Compressions, Airway, Breathing) for most situations.
A. Infant CPR (under 1 year):
- Initial Step: If you are alone and a child suddenly collapses, call EMS first. If you find an unresponsive infant and do not witness the collapse, perform 2 minutes of CPR before calling for help. In addition, the nurse should obtain an automated external defibrillator (AED), if available.
- Circulation (Compressions):
- One-Rescuer Technique: Use two fingers placed on the sternum just below the nipple line.
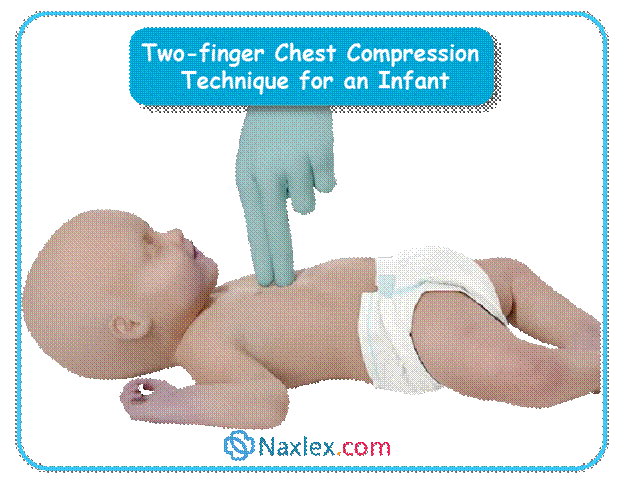
-
- Two-Rescuer Technique: At the time the infant is discovered, rescuer one should begin CPR using the two-thumb encircling hands technique. Wrap your hands around the infant's chest and use your thumbs to compress the sternum. This method is more effective and less tiring. Rescuer two should immediately call for emergency assistance and obtain an AED, if available. Once rescuer two returns, rescuer one should stop CPR, ending with the compression phase, and the AED procedure should be followed. Following each AED intervention, rescuers one and two should alternate positions between performing chest compressions and rescue breaths.

-
- Compression Rate: 100-120 compressions per minute.
- Compression Depth: Approximately 1.5 inches (4 cm) or one-third of the chest diameter.
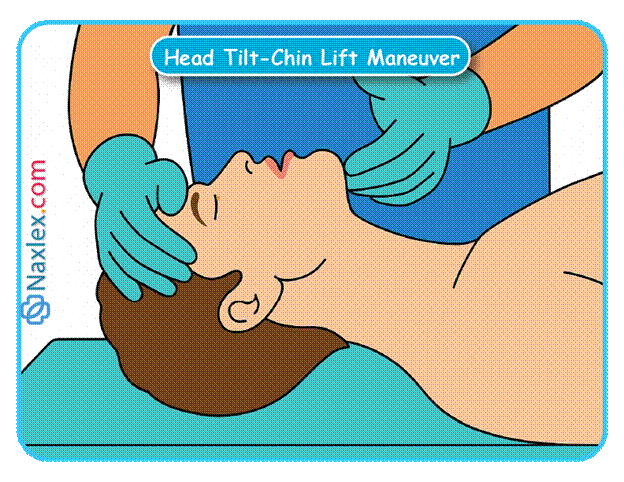
- Airway: Tilt the head back slightly and lift the chin to open the airway (sniffing position). Avoid overextending the neck.
- Breathing: Give two breaths over 1 second each, watching for visible chest rise. The ratio of compressions to breaths is 30:2 for one rescuer and 15:2 for two rescuers.
Nursing Insight: The AED should be used as soon as it is acquired. CPR should be stopped after the compression phase. The machine should be turned on. The AED pads should be applied to the infant’s chest, per machine instructions. (Adult pads may be used if the machine is not equipped with infant pads.). The AED prompts should be followed. After the AED sequence is complete, CPR should be resumed. An AED reanalysis and shock, if applicable, should be performed every 2 min or as prompted by the machine. The rescuer should continue CPR until emergency personnel arrive or until the child responds.

B. Child CPR (1 year to puberty):
- Initial Step: Call EMS immediately if you witness a child collapse. If the collapse is not witnessed, perform 2 minutes of CPR before calling.
- Circulation (Compressions):
- Technique: Use the heel of one or two hands on the lower half of the sternum.
- Compression Rate: 100-120 compressions per minute.
- Compression Depth: Approximately 2 inches (5 cm) or one-third of the chest diameter.
- Airway: Use the head-tilt/chin-lift maneuver.
- Breathing: Give two breaths, each over 1 second, watching for chest rise. The ratio is 30:2 for one rescuer and 15:2 for two rescuers.
C. Adolescent CPR (puberty and older):
- Adult CPR criteria should be employed when the victim is past the pubertal period. The adult CPR procedure should be performed as follows:
- Responsiveness assessed.
- Breathing assessed.
- Emergency personnel notified and an AED obtained as soon as the victim is found to be unresponsive and not breathing or gasping.
- Pulse assessed for a maximum of 10 sec. If a pulse is present, rescue breaths should be provided every 5 sec. If a pulse is absent, CPR procedure should be begun.
- Circulation (Compressions):
- Technique: Use two hands, interlocked fingers, on the lower half of the sternum.
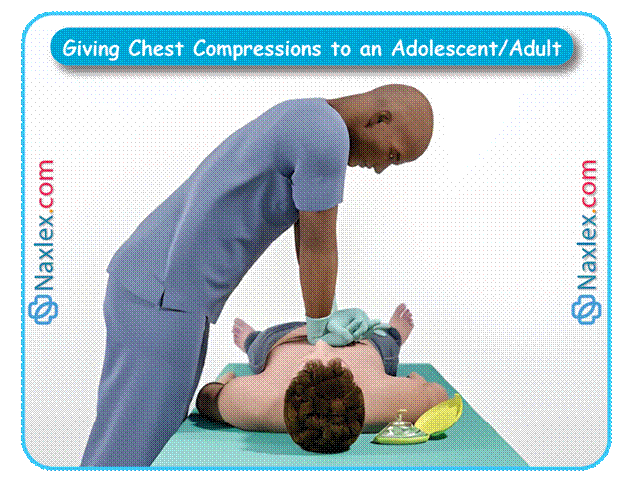
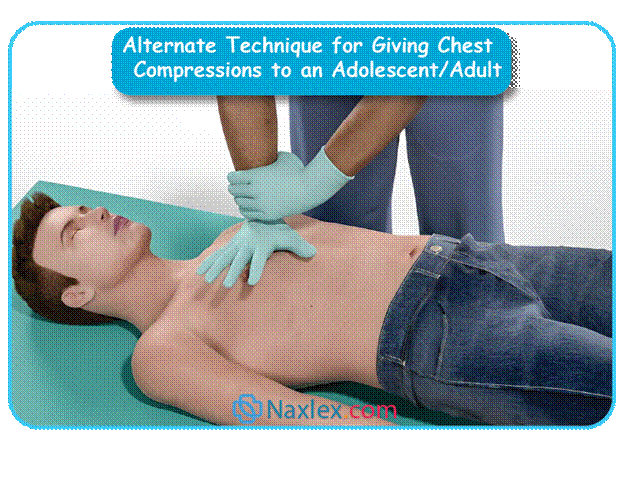
-
- Compression Rate: 100-120 compressions per minute.
- Compression Depth: At least 2 inches (5 cm).
- Airway: Use the head-tilt/chin-lift maneuver.
- Breathing: Give two breaths, each over 1 second. The ratio is 30:2 regardless of the number of rescuers.
Nursing Insight: The most likely cause of cardiopulmonary arrest in a child is different from that of an adult. In infants, the most common causes of cardiopulmonary arrest are congenital heart disease, sudden infant death syndrome, and prematurity. For children over 1 year of age, the most common causes of cardiopulmonary arrest are accidental injury and respiratory failure resulting from an acute or chronic upper respiratory illness. Except during the infancy period, cardiopulmonary arrest rarely is caused by a cardiac event as it is in adults.
3.2. Secondary Assessment
Once the immediate life threats have been managed, perform a more detailed secondary assessment. This is a head-to-toe examination to identify less critical injuries or conditions.
- SAMPLE History:
- S: Signs/Symptoms
- A: Allergies
- M: Medications
- P: Past medical history
- L: Last meal/oral intake
- E: Events leading to the injury/illness
- Head-to-toe Physical Examination:
- Head/Neck: Look for signs of trauma (bruising, swelling, deformities), pupillary response, and airway patency.
- Chest: Assess for equal chest rise, breath sounds, and any signs of injury.
- Abdomen: Palpate for tenderness, rigidity, or distension.
- Extremities: Assess for fractures, dislocations, and neurovascular status (pulses, capillary refill, sensation).
- Back: Log-roll the child to inspect the spine for signs of injury, especially if a spinal injury is suspected.
Obstructed Airway
- Incidence: Obstructed airway is a leading cause of death and disability in children, particularly those under 3 years of age.
- Etiology: Common causes include foreign body aspiration (e.g., small toys, buttons, coins, food like hot dogs, carrots, candies, or grapes), infections (e.g., croup, epiglottitis), and trauma.
- Pathophysiology: An obstructed airway prevents adequate oxygen exchange. This leads to hypoxemia (low oxygen in the blood) and hypercapnia (high carbon dioxide). If not corrected, this rapidly progresses to respiratory arrest, cardiac arrest, and anoxic brain injury.
- Diagnosis: Diagnosis is based on a rapid assessment of the child's symptoms.
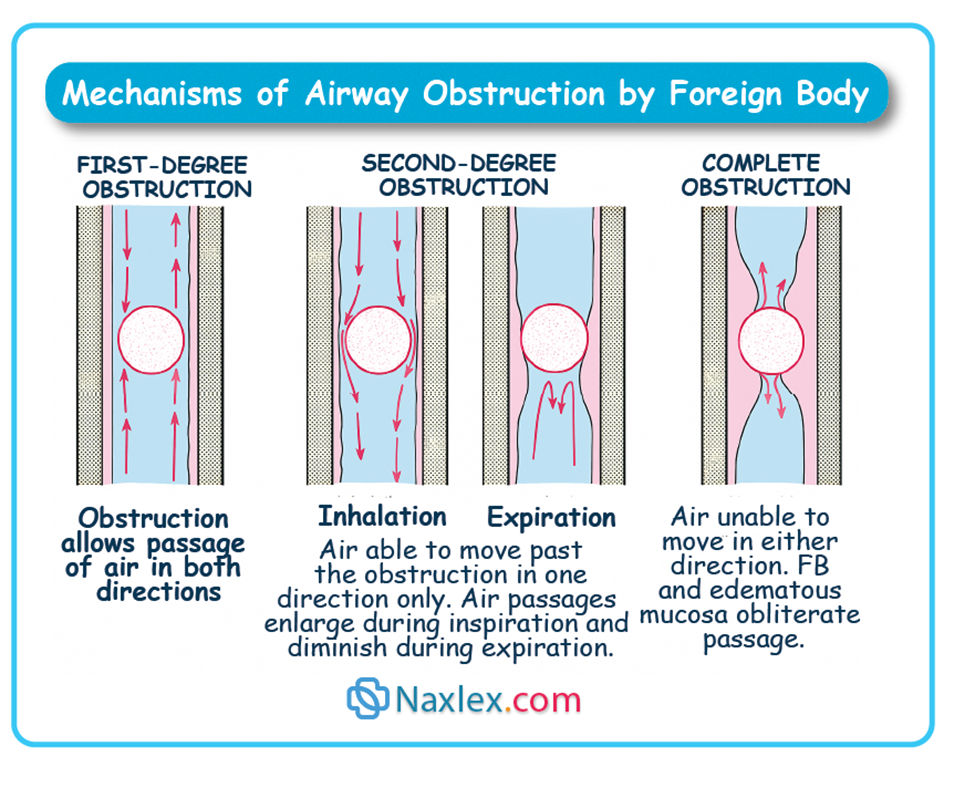
- Mild/first-degree Obstruction: Child is conscious, able to cough, and may have wheezing between coughs. Do not interfere with their cough, as this is the most effective way to clear the obstruction.
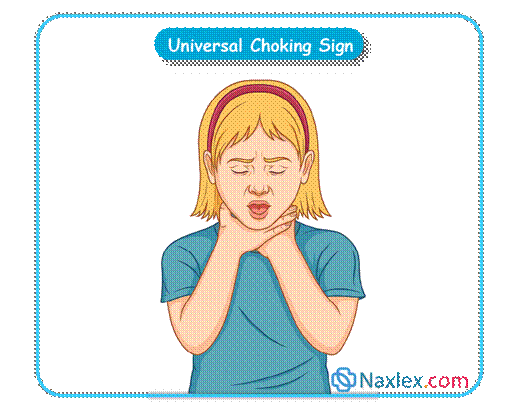
- Moderate/second-degree Obstruction: Th e conscious child will appear frightened and panicky with inspiratory stridor and ineffective cough, little to no air exchange. They may also wrap his or her hands around his or her own throat to indicate the presence of an obstruction.
-
- Severe/complete Obstruction: Child is unable to speak or cough, has silent coughs, or is making high-pitched sounds (stridor). They may be cyanotic (blue) and become unresponsive.
- Treatment:
A. Mild Obstruction: Unless the obstruction should worsen, emotional support should be provided while the child coughs up the obstruction.
B. Moderate to severe obstructions:
-
- Conscious Infant (under 1 year) with Moderate to Severe Obstruction: Perform a combination of 5 back blows and 5 chest thrusts until the obstruction is cleared or the infant becomes unresponsive.

-
- Conscious Child (over 1 year)/Adolescent with Moderate to Severe Obstruction: Perform the Heimlich maneuver (abdominal thrusts).

-
- Unconscious Child/Adolescent: Begin CPR. After each set of compressions, check the mouth for a foreign object and remove it if visible. Do not perform blind finger sweeps.
- The child may require bronchoscopy or laryngoscopy for removal of the object.
- Nursing Considerations/Diagnoses:
- Nursing Diagnoses:
- Ineffective Airway Clearance related to foreign body aspiration.
- Impaired Gas Exchange.
- Risk for injury/Deficient knowledge: Parents must be educated regarding safety precautions to take in order to prevent airway obstructions. Parents should be strongly encouraged to become certified in CPR and other first aid skills.
- Grieving/Risk for Complicated Grieving: If the child dies.
- Interventions:
- Rapidly assess the level of obstruction.
- Perform age-appropriate maneuvers to dislodge the foreign body.
- Provide supplemental oxygen.
- Prepare for intubation if other measures fail.
- Provide psychological support to the child and family.
- Nursing Diagnoses:
Shock
- Incidence: Shock is a common and often underestimated cause of death in children. It can progress rapidly and is often a result of an underlying condition.
- Etiology:
- Hypovolemic Shock: Most common type in children, often caused by dehydration from vomiting, diarrhea, or burns. It is also caused by extensive loss of blood.
- Distributive Shock: Caused by widespread vasodilation, often seen in sepsis from micro-organisms such as Escherichia coli, Streptococcus pyogenes (group A strep), and Neisseria meningitides. It may also be caused anaphylaxis or drug overdose.
- Cardiogenic Shock: Caused by severe injury to the heart muscle, for instance, due to heart failure.
- Obstructive Shock: Caused by a physical obstruction of blood flow (e.g., tension pneumothorax, cardiac tamponade).
- Pathophysiology: Shock is a state of inadequate tissue perfusion and oxygen delivery to meet metabolic demands. Children have a remarkable ability to compensate for early shock by increasing heart rate and systemic vascular resistance. This compensatory phase can be deceptive, as it may mask the severity of the condition. As shock progresses, compensatory mechanisms fail, leading to hypotension (a late and ominous sign), organ dysfunction, and multi-organ failure.
- Signs and symptoms:
- Initial Signs (Compensated Shock): Tachycardia (most common and earliest sign), tachypnea, weak peripheral pulses, cool extremities, prolonged capillary refill time (>2 seconds), and decreased urine output.
- Late Signs (Decompensated Shock): Hypotension, altered mental status, apnea, and weak or absent central pulses.
- Diagnosis: Early diagnosis is critical. Clinical picture in conjunction with X-rays and a variety of laboratory data, including blood cultures, complete blood counts (CBC), lumbar puncture, blood gases, and serum electrolytes.
- Treatment:
- Initial Management: Administer 100% oxygen and establish IV or intraosseous (IO) access.
- Fluid Resuscitation: Administer a rapid bolus of 20 mL/kg of an isotonic crystalloid (e.g., normal saline or lactated Ringer's) over 5-10 minutes. This may be repeated up to three times.
- Vasopressors: If hypotension persists after fluid resuscitation, vasopressors (e.g., dopamine, norepinephrine) may be initiated.
- Treat the Underlying Cause: Treat the cause of the shock, whether it's infection (antibiotics), hemorrhage (blood products), or an allergic reaction (epinephrine).
- Extracorporeal membrane oxygenation (ECMO): This is a is a life-support system that acts as an artificial heart and/or lungs. It's used for patients with severe heart or lung failure that can't be treated with conventional methods, such as a mechanical ventilator. It is a treatment similar to cardiopulmonary bypass, usually only used as treatment for infants and young children. Its primary purpose is to give the patient's heart and lungs time to rest and heal. It doesn't cure the underlying disease.
- Nursing Considerations/Diagnoses:
- Nursing Diagnoses:
- Risk for Ineffective Tissue Perfusion related to decreased circulating volume.
- Risk for Ineffective Airway Clearance.
- Risk for Decreased Cardiac Output.
- Risk for Deficient Fluid Volume: Administer prescribed IV fluids.
- Risk for Altered Coping/Anxiety: Calmly provide the child and parents with information regarding care, employing simple and concise language; provide opportunities for the child and parents to express fears and concerns; refer the family to social services as needed; assist the family to identify support systems and coping strategies.
- If the child dies, Grieving/Risk for Complicated Grieving: Provide the parents and others, if appropriate, with the opportunity to express their feelings; allow the parents, if appropriate, time to be with and to say good-bye to their child; educate the parents regarding the 5 stages of grief.
- Interventions:
- Continuous monitoring of vital signs, including heart rate, blood pressure, respiratory rate, and oxygen saturation.
- Assess capillary refill time and skin temperature frequently.
- Monitor urine output (a key indicator of renal perfusion).
- Administer prescribed fluids and medications.
- Maintain a calm environment to reduce stress and metabolic demands.
- Nursing Diagnoses:
Trauma
- Incidence: Trauma is the leading cause of death in children and adolescents. Motor vehicle accidents (when the child is a passenger in the car or when the child is a pedestrian), falls, gun trauma, and child abuse are common etiologies.
- Etiology:
- Blunt Trauma: Most common in children.
- Penetrating Trauma: Less common but often more severe.
- Pathophysiology:
- Children's unique anatomy makes them more vulnerable to severe trauma. Their larger head-to-body ratio increases the risk of head injuries. Their abdominal organs are less protected by muscle and fat, making them susceptible to blunt force injury. Their more pliable bones are more prone to "greenstick" fractures.
- Waddell’s triad, refers to the traumatic injuries sustained by pedestrian children who are hit by a car. The children are injured in three distinctly serious ways:
i. Abdominal injuries that occur during the initial strike.
ii. Injuries to the extremities that occur when the child lands on the ground after being thrown through the air.
iii. Head injuries that occur when the child lands on his or her head after being thrown through the air. Because children’s heads are often the heaviest parts of their bodies, their heads frequently sustain serious injury.
- Diagnosis:
- Clinical picture in conjunction with X-rays and a variety of laboratory data including blood cultures, CBCs, lumbar puncture, blood gases, and serum electrolytes.
- Primary Survey (ABCDEs):
- Airway with cervical spine protection
- Breathing and ventilation
- Circulation with hemorrhage control
- Disability (neurologic status)
- Exposure (completely undress the child to examine for injuries)
- Secondary Survey: A more detailed head-to-toe examination.
- Treatment:
- Stabilization: Maintain a patent airway and provide oxygen. Control any external bleeding.
- Immobilization: Immobilize the cervical spine until cleared.
- Fluid Resuscitation: Administer isotonic fluids for hypovolemic shock.
- Surgical Intervention: For internal bleeding or organ damage.
- Prevention:
- The parents and child must be educated regarding car and pedestrian safety practices
- Infants and young children should be supervised whenever on elevated surfaces.
- All firearms and ammunition should be kept in separate, locked safes.
- Nursing Considerations/Diagnoses:
- Nursing Diagnosis:
- Risk for Ineffective Tissue Perfusion related to hemorrhage.
- Deficient knowledge: Parents must be educated regarding safety precautions to take to prevent traumatic injury. Parents should be encouraged to become certified in CPR and other first aid skills.
- Risk for Impaired Gas Exchange: Assist with intubation, as needed, administer oxygen, as needed, carefully monitor vital signs
- Risk for Deficient Fluid Volume: Administer IV therapy, as ordered, maintain strict intake and output.
- Risk for Infection: Employing the five rights of medication administration, administer safe dosages of antibiotics/antivirals/antifungals, as prescribed.
- Risk for Altered Coping/Anxiety: calmly provide the child and parents with information regarding trauma care, employing simple and concise language. Provide opportunities for the child and parents to express fears, concerns, and guilt. Refer the family as needed to social services.
- Risk for Altered Parenting: Depending on the source of the injury/emergency, and if applicable, the nurse should notify child protective services of child abuse or child neglect.
- If the child dies, Grieving/Risk for Complicated Grieving.
- Interventions:
- Maintain cervical spine immobilization.
- Monitor for signs of hemorrhage (tachycardia, hypotension).
- Maintain body temperature to prevent hypothermia.
- Administer pain management.
- Be vigilant for signs of child abuse, especially in cases where the history does not match the injury.
- Nursing Diagnosis:
Acute Poisonings
- Incidence: Poisonings are a major cause of pediatric emergencies. Most are unintentional and occur in toddlers and preschoolers. Intentional poisoning (i.e., from the ingestion of alcohol and/or prescription medications) most commonly is seen in the adolescent population.
- Etiology:
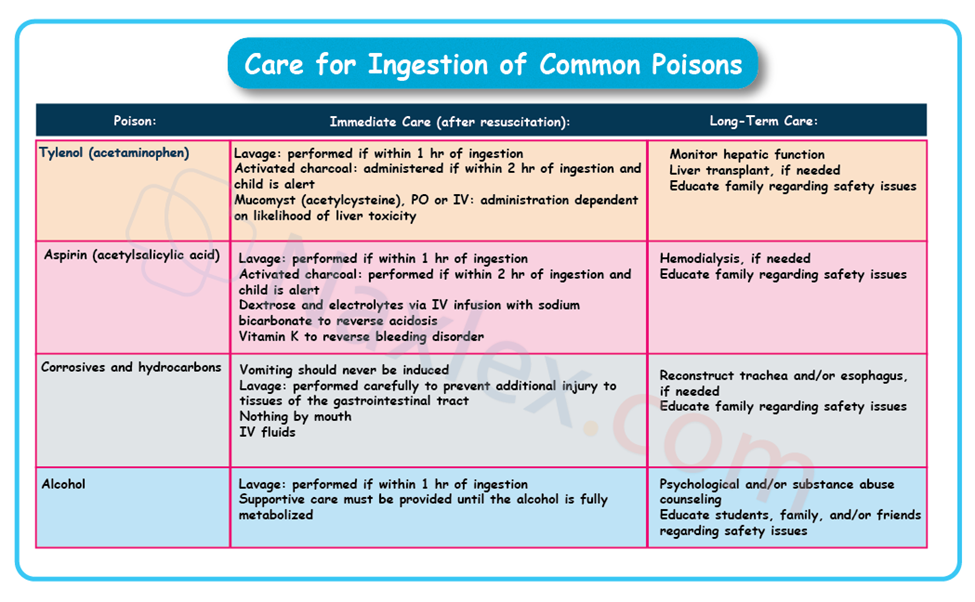
- Medication ingestion: Tylenol (acetaminophen), aspirin (acetylsalicylic acid), and vitamins are the most common poisons in toddlers and preschoolers. Prescription medications (e.g., analgesics, narcotics, antidepressants, antianxiety medications, as well as illicit drugs) often are purposefully ingested by older school-age and adolescent children.
- Other poisons that may be ingested: Cleaning products, gasoline, and kerosene most commonly are ingested by toddlers and preschoolers. Alcohol most commonly is ingested by older school-age and adolescent children. Poisons may also be “ingested” via the respiratory system in the form of a gas or aerated particles or via the skin in the form of a topical substance.
- Pathophysiology:
The effects of poisoning depend on the substance ingested, the dose, and the child's body weight. Children have a higher metabolic rate and a smaller body mass, making them more susceptible to the toxic effects of substances.
-
- Acetaminophen: Ingestion of greater than 150 mg/kg is considered toxic. Therapeutic dose is 10 to 15 mg/kg every 6 to 8 hr. Hepatotoxicity can develop from the physiological metabolism of the medication.
- Signs and symptoms depend on the quantity ingested. Initially, nausea and vomiting and flu-like symptoms. After 24 hours, elevated liver enzymes, elevated bilirubin, and right upper quadrant pain. In 3 to 7 days, the child may develop liver failure. After 1 week, either the child will recover or the child’s health will deteriorate further.
- Acetaminophen: Ingestion of greater than 150 mg/kg is considered toxic. Therapeutic dose is 10 to 15 mg/kg every 6 to 8 hr. Hepatotoxicity can develop from the physiological metabolism of the medication.

-
- Aspirin: Ingestion of greater than 150 mg/kg is considered toxic. Therapeutic dose is 10 to 15 mg/kg every 4 to 6 hr. Many organ systems may be adversely affected. Initially, the child will exhibit respiratory alkalosis in an attempt to compensate for the ingestion. The alkalosis quickly shifts to metabolic acidosis with hypokalemia and dehydration when the salicylic acidemia overwhelms the compensatory response.
- Signs and symptoms: Initially, nausea and vomiting with hyperpnea, followed by central nervous system changes (i.e., confusion, seizures, coma), renal failure, bleeding, hyponatremia, hypokalemia, hypoglycemia, dehydration, tinnitus or deafness.
- Aspirin: Ingestion of greater than 150 mg/kg is considered toxic. Therapeutic dose is 10 to 15 mg/kg every 4 to 6 hr. Many organ systems may be adversely affected. Initially, the child will exhibit respiratory alkalosis in an attempt to compensate for the ingestion. The alkalosis quickly shifts to metabolic acidosis with hypokalemia and dehydration when the salicylic acidemia overwhelms the compensatory response.
-
- Cleaning supplies, gasoline, and other such substances: Severe damage to the mouth, esophagus, and stomach, respiratory compromise, and blood chemistry disruptions.
- Alcohol: a physiological depressant.
- Signs and symptoms: Confusion, vomiting, stupor, and respiratory compromise.
- Diagnosis:
- History: The most important tool is a detailed history, including the substance, amount, and time of ingestion.
- Physical Examination: Look for signs and symptoms consistent with the suspected poison (e.g., pinpoint pupils with opioids, dry/red skin with anticholinergics).
- Toxicology Screen: Blood and urine tests can identify the substance.
- Treatment:
- Immediate care at the scene.
- Assess the child: The child must be assessed for responsiveness and for the need of emergency intervention. The child’s immediate, physiological needs must be met.
- Terminate the exposure: depending on the situation, for the safety of the child and/or the nurse, this action may take precedence over the assessment of the child. If possible, exposure to the poison should be terminated.
- Medications or alcohol: if safe to perform, remove all of the residual substance from the child’s mouth.
- Gas or topical: if safe to perform, the child must immediately be removed from the area where the gas or topical is being emitted, the source of the gas or topical must be shut off, and/or contaminated clothing must be removed.
- Identify the poison: The exact identity of the poison must be determined. The victim and/or witnesses should be queried. Any empty containers should be located, inspected, and saved.
- Call the poison control center (PCC): PCC should be called and notified of the identity of the substance. Any actions recommended by the PCC should be implemented (flushing the eyes and/or skin with water).
- Seek emergency medical assistance: Following immediate intervention and if recommended by PCC, the child should be seen and evaluated in an emergency department.
- Follow-up treatment: All evidence of the exposure should be taken to the emergency department for analysis, such as: Vomitus, urine, empty bottles, and containers. Specific treatment is dependent on the exact poison.
- Immediate care at the scene.
Use of Activated Charcoal (AC) in Poisoning
- Activated charcoal (AC) is a gastric decontamination agent used in the emergency management of patients who have acutely ingested certain toxins or medications. The primary mechanisms of action are adsorption and enhanced elimination.
- Adsorption (Primary):
- AC is a highly porous substance with a very large surface area.
- It physically adsorbs (binds to the surface of) many drugs and toxins in the gastrointestinal (GI) tract.
- This binding prevents the toxins from being absorbed into the bloodstream, thereby reducing or preventing systemic toxicity.
- Enhanced Elimination (Multiple-Dose Activated Charcoal - MDAC):
- In cases where a drug undergoes enterohepatic or enteroenteric recirculation (re-entering the gut from the blood/liver), repeated doses of AC can bind to the drug as it re-enters the gut.
- This interrupts the recirculation and creates a concentration gradient (a "sink" effect) that draws more drug from the blood into the gut for binding and elimination, thus accelerating its clearance from the body.
- Examples of drugs that benefit from MDAC: Carbamazepine, Dapsone, Phenobarbital, Quinine, Theophylline.
Indications and Timing of AC
AC is generally reserved for significant, potentially life-threatening ingestions of an adsorbable toxin. It is not recommended for routine use.
|
Type of Treatment |
Timing and Purpose |
Examples of Ingestions |
|
Single Dose AC (SDAC) |
Most effective when administered as soon as possible, ideally within 1 hour of ingestion, to block absorption of the toxin. |
Most drugs and toxins that are well-adsorbed. |
|
Multi-Dose AC (MDAC) |
Used to enhance elimination and disrupt recirculation. Can be beneficial hours after ingestion, especially for: |
Drugs with enterohepatic circulation (e.g., Digoxin) or those that slow gut motility (e.g., anticholinergics, opioids, and salicylates/aspirin). |
Key Contraindications of AC
|
Contraindication Category |
Examples of Substances |
Rationale |
|
Unprotected Airway |
Any obtunded, drowsy, or seizing patient with a risk of vomiting/aspiration (unless the airway is protected by intubation). |
High risk of aspiration pneumonitis, which can be fatal. |
|
Corrosive/Caustic Agents |
Strong Acids (e.g., toilet cleaner) and Alkalis (e.g., lye) |
May make an endoscopic evaluation more difficult; the risk of vomiting/aspiration is high. |
|
Ineffective Binding |
Alcohols (Ethanol, Methanol, Glycols), Metals (Iron, Lithium, Lead), Cyanide, and Hydrocarbons (e.g., gasoline, paint thinner). |
These substances are either poorly adsorbed or are small, polar molecules. |
|
Gastrointestinal Issues |
Bowel obstruction, ileus, or GI perforation/hemorrhage risk. |
Can worsen obstruction; multiple doses require active bowel sounds. |
Adverse Effects of AC
|
Common Adverse Effects |
Serious/Rare Adverse Effects |
|
Black stools (expected and harmless) |
Aspiration Pneumonitis or Respiratory Failure (most serious risk) |
|
Constipation |
Bowel Obstruction (often from a charcoal-bezoar, especially with MDAC or reduced gut motility) |
|
Nausea and Vomiting |
Dehydration and Electrolyte Imbalance (particularly when co-administered with a cathartic like Sorbitol) |
|
Stomach pain/Gastric Distention |
Drug-drug interactions (reduces absorption of oral antidotes, e.g., N-acetylcysteine) |
- Nursing Considerations/Diagnoses:
- Nursing Diagnosis:
- Risk for Injury related to ingestion of a poisonous substance.
- Deficient Knowledge/Anxiety/Risk for Altered Coping
- Interventions:
- Immediately contact the Poison Control Center for guidance.
- Identify the substance ingested and the amount.
- Administer prescribed treatments (activated charcoal, antidotes).
- Monitor for signs of deterioration.
- Educate the family on poison prevention.
- Nursing Diagnosis:
Chronic Heavy Metal Poisoning
- Incidence: Chronic heavy metal poisoning, such as lead poisoning, is a significant public health issue, especially in children from low-income or older housing areas. Iron is another commonly ingested heavy metal.
- Etiology:
- Lead is internalized via two routes: oral ingestion and respiratory inhalation.
- Many indoor paints contained lead until 1978. Paint chipping from furniture, walls, antique toys, and other objects can be ingested. Paint sanded during renovations can be aerosolized and breathed in.
- The plumbing in many old homes is comprised of lead pipes and/or lead soldering. Lead leaches into the water and is consumed.
- Automotive gasoline contained lead until the 1970s. The exhaust from automobiles contaminated the soil throughout the United States. The contaminated dirt and dust surrounding homes can be ingested on hands that are washed infrequently.
- Iron is usually ingested through accidental ingestion most frequently by toddlers and preschoolers.
- Lead is internalized via two routes: oral ingestion and respiratory inhalation.
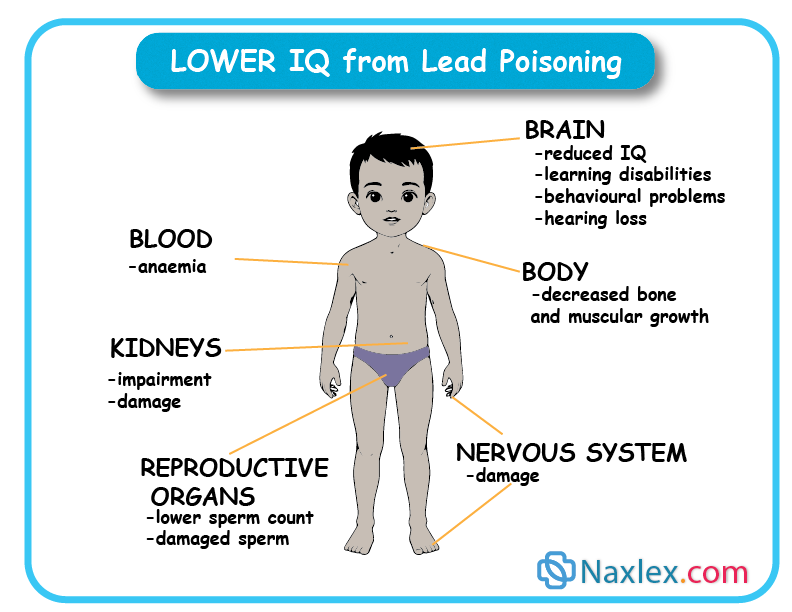
- Pathophysiology:
Multiple systems are affected adversely by lead.
-
- Hematological system: adverse effects are reversible. Anemia develops because lead interferes with the biosynthesis of the heme portion of the hemoglobin molecule.
- Gastrointestinal system: adverse effects are reversible and include nausea and vomiting, constipation, and anorexia. Lead in the GI tract can be seen on an x-ray.
- Renal system: adverse effects are reversible unless there has been continued ingestion over a long period of time. Lead damages the tubules of the kidney, leading to abnormal excretion of glucose and proteins.
- Skeletal system: If ingested over long periods of time, lead deposits in the bone marrow of the long bones. Lead lines can be seen on x-rays.
- Central nervous system: adverse effects may be irreversible. Lead ingestion results in fluid shift s in the brain and increased intracranial pressure resulting in cortical atrophy and lead encephalopathy.
Signs and symptoms.
-
-
- Lower levels: hyperactivity, learning disabilities, and lowered IQ.
- Higher levels: convulsions, paralysis, blindness, mental retardation, coma, and death.
-
- Diagnosis:
- In many states, it is the law to assess blood lead levels (BLLs) during early childhood. All children receiving Medicaid are mandated to receive a blood lead assessment at 12 months and 24 months of age.
- CBCs, urinalyses, and x-rays.
- Blood lead levels (BLLs).
- BLL of 5 mcg/dL or higher is considered abnormal.
- BLL greater than or equal to 45 mcg/dL is dangerously elevated and requires medical intervention.
- Lead mobilization tests.
- Treatment:
Prevention
-
- Healthy diet: Lead has a strong affinity for combining with the heme portion of the red blood cell. Children who consume diets that are low in iron and vitamin C are, therefore at higher risk of developing lead toxicity than are children with diets high in iron and vitamin C. A diet high in calcium helps to protect the long bones from lead deposition.
- Water: Water in every home, especially those with well water, should be assessed for lead contamination. If lead is found in the water, only cold water should be used for drinking and cooking because lead leaches more rapidly into hot than cold water. Before using the cold water, it should be allowed to run into the sink for 1 full minute because lead leaches more rapidly into standing water than into flowing water. If lead levels are still high after the above interventions, only bottled water should be consumed.
- Other exposures: Dissuade pica (i.e., the ingestion of nonfood substances, such as dirt). Frequently cleanse such things as hands, floors, windowsills, and toys to remove lead dust. Remove children and pregnant and lactating women from environs undergoing renovations.
Treatment guidelines, as recommended by the Centers for Disease Control and Prevention (CDC)
- BLL 5 to 9 mcg/dL: The health-care provider should investigate the possible sources of exposure to lead. The parents and others should be educated on ways to reduce lead exposure. BLL should be reassessed in 3 to 6 months.
- BLL 10 to 14 mcg/dL: All of the above, except that the BLL should be reassessed in 1 to 3 months
- BLL 15 to 44 mcg/dL: A representative from the department of health may visit the home to assess the home for possible sources of lead exposure, educate the parents about lead exposure, and encourage the parents to provide the child with foods high in iron, vitamin C, and calcium.
- BLL greater than or equal to 45 mcg/dL: All of the above plus chelation therapy.
Chelation therapy.
-
- Chelation therapy is performed to remove heavy metals from the body. Because the therapy itself may result in adverse effects, it should be conducted only under medical supervision.
Nursing Insight: Children who are receiving chelating agents should have their BLLs monitored carefully. In some instances, BLLs actually rise while on chelating agents because lead enters the bloodstream from the bones or gastrointestinal system for excretion through the kidneys. Nephrotoxicity and neurotoxicity may result.
-
- Chelation medications commonly administered are:
- Chemet (succimer): may be administered on an outpatient basis.
- Adverse effects: Serious: neutropenia and arrhythmias. Common: nausea and vomiting, rash, pruritus, and elevated liver enzymes.
- Cuprimine (d-penicillamine) may be administered on an outpatient basis.
- Adverse effects: Many serious side effects, including thrombocytopenia, leukopenia, aplastic anemia, hypersensitivity reaction, and pancreatitis. Common side effects include anorexia, epigastric pain, nausea and vomiting, diarrhea, proteinuria, and pruritic rash.
- BAL in oil (dimercaprol): administered while the child is in the hospital. BLLs should be assessed after 48 hr to determine whether therapy is still needed.
- Adverse effects: Severe side effect: neutropenia. Many common side effects, including pain at the injection site, nausea and vomiting, hypertension, tachycardia, conjunctivitis, and paresthesias.
- Calcium disodium versenate (edetate disodium calcium or CaNa2EDTA).
- Adverse effects: Severe side effects include dangerously low hypoglycemia, hypocalcemia, kidney failure, and seizures. Common side effect: malabsorption of vitamins, including vitamin C and the B vitamins.
- Chemet (succimer): may be administered on an outpatient basis.
- Chelation medications commonly administered are:
Nursing Insight: BAL and CaNa2EDTA rarely are administered for a BLL less than 70 mcg/dL unless the child is exhibiting signs of encephalopathy.
- Nursing Considerations/Diagnoses:
- Nursing Diagnosis:
- Impaired Neurological Function related to lead exposure.
- Deficient Knowledge: educate parents and child regarding the importance of handwashing and the avoidance of pica.
- Risk for Altered Growth and Development: monitor the child’s growth and development using growth charts and development assessments.
- Risk for Injury related to chelation therapy.
- Risk for Impaired Coping/Anxiety/Guilt: allow parents and the child to express their concerns.
- Interventions:
- Educate parents on lead prevention strategies, such as frequent hand washing, removing shoes before entering the home, and cleaning surfaces.
- Refer the family to local health departments for lead abatement programs.
- Provide nutritional counseling, as a diet high in calcium and iron can help reduce lead absorption.
- Nursing Diagnosis:
Drowning
- Incidence: Drowning is a leading cause of accidental death in children, especially in the 1-4 year age group.
- Etiology: Drowning can occur in as little as an inch of water. Common scenarios include unsupervised access to pools, bathtubs, and open bodies of water.
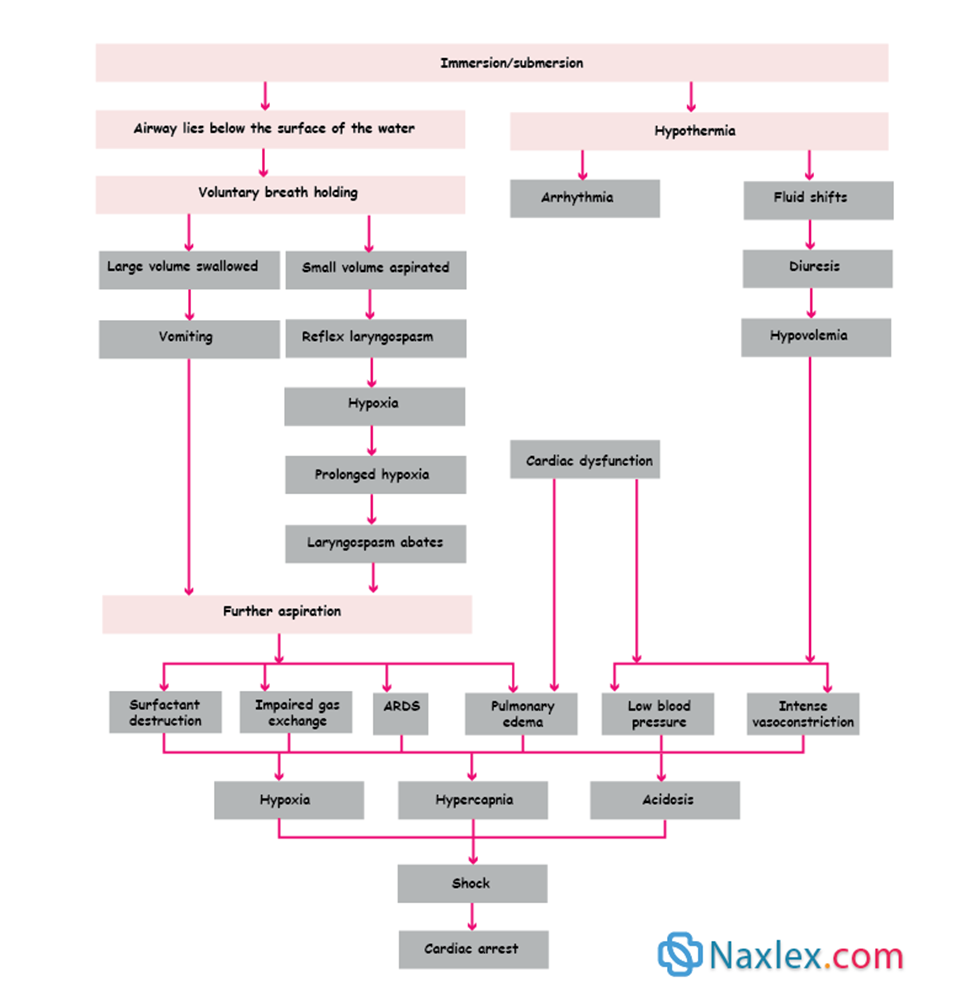
- Pathophysiology:
- Submersion: The child becomes submerged in a liquid.
- Laryngospasm: The initial response is often a spasm of the vocal cords to prevent water from entering the lungs.
- Hypoxemia: The laryngospasm leads to hypoxemia.
- Aspiration: If the child relaxes, a large amount of water may be aspirated into the lungs, leading to pulmonary edema, respiratory distress, and death.
- Hypothermia: Cold water can lead to rapid hypothermia, which may be protective in some cases by slowing metabolic rate but can also complicate resuscitation.
- Diagnosis:
- Clinical Presentation: The child may be unresponsive, cyanotic, and not breathing.
- Initial Assessment: Focus on the ABCs. The duration of submersion and the temperature of the water are critical pieces of information.
- Treatment:
- Immediate Resuscitation: Begin CPR as soon as the child is out of the water. Breaths are the priority in drowning victims, so the A-B-C (Airway, Breathing, Compressions) protocol may be used in some guidelines.
- Supportive Care: Once in the hospital, supportive care includes intubation, mechanical ventilation, and treatment of hypothermia and electrolyte imbalances.
- Nursing Considerations/Diagnoses:
- Nursing Diagnosis:
- Ineffective Breathing Pattern related to aspiration.
- Risk for Hypothermia: monitor core temperature, wet clothing should be removed, administer warmed IV fluids.
- Risk for Complicated Grieving if the child dies.
- Interventions:
- Provide immediate and aggressive respiratory support.
- Monitor for complications like acute respiratory distress syndrome (ARDS) and pneumonia.
- Provide emotional support and grief counseling for the family.
- Educate the family on water safety and prevention strategies.
- Nursing Diagnosis:
Summary
- Pediatric emergencies demand a unique and specialized approach that recognizes the distinct anatomical, physiological, and psychological characteristics of children.
- The foundation of effective care is a rapid, systematic assessment using a structured framework (e.g., the Pediatric Assessment Triangle or the ABCDE approach) to quickly identify and intervene in life-threatening conditions. The initial assessment is followed by a more detailed secondary survey to uncover the full extent of the child's illness or injury.
- This document has explored the key aspects of managing critical pediatric conditions, from the foundational principles of CPR to the nuanced care required for specific emergencies.
- We have highlighted the differences in providing CPR for infants, children, and adolescents, underscoring the importance of age-appropriate techniques.
- We have also detailed the pathophysiology, diagnosis, and treatment for common emergencies such as obstructed airway, shock, trauma, and poisoning, emphasizing the need for prompt recognition and targeted interventions.
- The nurse serves as a source of calm, clear communication, and compassionate support. Furthermore, a significant component of pediatric emergency care is prevention. By educating families on topics such as water safety, poison control, and car seat usage, nurses can play a vital role in reducing the incidence of these tragic events.
- Pediatric emergency nursing is a dynamic and challenging field that requires continuous learning and skill refinement. By mastering the core principles of assessment, intervention, and compassionate care, nurses can make a tangible difference in the lives of children and their families, ensuring the best possible outcomes in the most challenging of circumstances.
