
Diabetes Mellitus
Lessons
- Objectives
- Introduction
- Pathophysiology Of Diabetes In Pregnancy
- Practice Exercise 1
- Types Of Diabetes In Pregnancy
- Risk Factors For Gestational Diabetes Mellitus
- Practice Exercise 2
- Screening And Diagnosis Of Gestational Diabetes Mellitus
- Practice Exercise 3
- Maternal And Fetal Complications Of Diabetes In Pregnancy
- Practice Exercise 4
- Management Of Diabetes In Pregnancy
- Practice Exercise 5
- Fetal Surveillance And Monitoring In Gdm
- Practice Exercise 6
- Patient Education And Health Promotion
- Practice Exercise 7
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
At the end of this topic, the learner should be able to:
- Explain the pathophysiology of diabetes in pregnancy, emphasizing alterations in glucose metabolism, hormonal influences, maternal adaptations, and fetal glucose regulation.
- Differentiate between preexisting diabetes mellitus (Type 1 and Type 2) and gestational diabetes mellitus (GDM) based on etiology, timing of onset, and pathophysiological mechanisms.
- Identify maternal and fetal risk factors that predispose to the development of gestational diabetes mellitus, distinguishing modifiable from non-modifiable elements.
- Discuss the screening and diagnostic procedures for gestational diabetes mellitus, including one-step and two-step testing, glucose challenge test (GCT), and oral glucose tolerance test (OGTT), and interpret diagnostic thresholds.
- Describe the maternal complications of diabetes in pregnancy such as diabetic ketoacidosis (DKA), preeclampsia, polyhydramnios, and infections, including their pathogenesis and clinical implications.
- Analyze the fetal complications associated with maternal diabetes, including congenital anomalies, macrosomia, intrauterine growth restriction (IUGR), respiratory distress syndrome, and neonatal hypoglycemia.
- Outline evidence-based management strategies for diabetes in pregnancy, including preconception counseling, medical nutrition therapy (MNT), physical activity, pharmacological interventions (insulin and oral hypoglycemics), and glucose monitoring.
- Explain nursing management during labor and delivery, focusing on glycemic control, fetal monitoring, and prevention of maternal and neonatal complications.
- Discuss postpartum management, emphasizing glucose regulation, maternal recovery, and strategies to prevent long-term metabolic disease.
- Evaluate fetal surveillance techniques such as nonstress test (NST), biophysical profile (BPP), amniotic fluid index (AFI), and ultrasound for growth monitoring, and interpret findings in the context of maternal diabetes.
- Implement comprehensive patient education on self-monitoring of blood glucose, recognition and management of hypoglycemia and hyperglycemia, and the importance of adherence to prescribed therapy.
- Promote breastfeeding and long-term lifestyle modifications that reduce the risk of progression from gestational diabetes to Type 2 diabetes mellitus.
- Apply critical thinking in answering NCLEX-style practice questions on the diagnosis, management, and nursing care of patients with diabetes in pregnancy.
Introduction
Diabetes mellitus in pregnancy represents a spectrum of metabolic disturbances that significantly influence both maternal and fetal outcomes. It is characterized by varying degrees of carbohydrate intolerance resulting in hyperglycemia, which may be preexisting (Type 1 or Type 2 diabetes mellitus) or first recognized during pregnancy (gestational diabetes mellitus).
Pregnancy induces profound hormonal, metabolic, and vascular changes designed to meet fetal nutritional demands. These adaptations include increased insulin resistance, enhanced lipolysis, and altered glucose utilization. While these changes are physiological, excessive insulin resistance or inadequate pancreatic β-cell compensation leads to maternal hyperglycemia.
Hyperglycemia during pregnancy poses risks for maternal complications such as preeclampsia, polyhydramnios, and diabetic ketoacidosis, and for fetal complications including congenital malformations, macrosomia, and neonatal hypoglycemia. Furthermore, gestational diabetes increases the mother’s lifetime risk of developing Type 2 diabetes and predisposes the child to obesity and metabolic syndrome later in life.
Early identification, tight glycemic control, and multidisciplinary management are critical to optimizing outcomes. The nurse plays a pivotal role in patient education, glucose monitoring, nutritional guidance, and emotional support—ensuring safe pregnancy progression and delivery for both mother and infant.
Pathophysiology Of Diabetes In Pregnancy
1.1 Overview Of Glucose Metabolism In Pregnancy
- Pregnancy induces dynamic changes in maternal carbohydrate metabolism that occur in a predictable pattern across trimesters, designed to optimize substrate supply to the fetus while maintaining maternal homeostasis.
- In early pregnancy (first trimester) maternal metabolism is relatively anabolic: increased maternal insulin sensitivity and enhanced glycogen and fat storage occur to build maternal energy reserves. These changes facilitate implantation and organogenesis and provide substrates for later fetal growth.
- In late pregnancy (second and third trimesters) maternal metabolism shifts to a catabolic state characterized by progressive insulin resistance, increased lipolysis, and mobilization of maternal fat stores to provide continuous glucose, free fatty acids, and ketone bodies for the fetus.
- Glucose crosses the placenta by facilitated diffusion via GLUT transporters (primarily GLUT1). Fetal glucose concentration is normally 70–80% of maternal glucose; therefore, maternal hyperglycemia leads directly to fetal hyperglycemia.
- Fetal insulin does not cross the placenta; fetal pancreatic β-cells respond to increased fetal glucose by hypertrophy and hyperplasia and by secreting increased insulin, which acts as a fetal growth factor and promotes adiposity.
- The balance between maternal insulin secretion and insulin resistance determines maternal glycemia. If β-cell compensation is adequate, normoglycemia is maintained; if compensation is inadequate, maternal hyperglycemia develops, resulting in gestational diabetes or exacerbation of preexisting diabetes.
Nursing Insights
- Nurses must understand that pregnancy physiology intentionally reduces maternal insulin sensitivity in late gestation to prioritize fetal nutrient supply; therefore, deterioration of glycemic control commonly occurs in the second and third trimesters. Practical implication: anticipate increased insulin requirements during late pregnancy and adjust therapy based on frequent glucose monitoring.
- Recognize GLUT1-mediated placental glucose transfer implies that any maternal hyperglycemia is transmitted to the fetus quickly; therefore, transient maternal hyperglycemia (postprandial peaks) can have immediate fetal metabolic consequences.
- When caring for pregnant patients, chart trends rather than single values because physiologic gestational changes alter expected glucose patterns across trimesters.
1.2 Hormonal Influences On Insulin Resistance
- Multiple placental and maternal hormones produce progressive insulin antagonism during pregnancy. The net effect is decreased maternal insulin sensitivity and increased hepatic glucose production. Key mediators include:
- Human placental lactogen (hPL) (also called human chorionic somatomammotropin): produced by syncytiotrophoblasts; it increases maternal lipolysis and decreases maternal insulin sensitivity, thereby increasing maternal free fatty acids and glucose availability for the fetus.
- Placental growth hormone (PGH): gradually replaces pituitary growth hormone in late pregnancy and increases maternal insulin resistance and hepatic gluconeogenesis.
- Progesterone and estrogen: exert complex modulatory effects that contribute to insulin resistance through alterations in insulin receptor signaling and adipose tissue metabolism.
- Cortisol: maternal adrenal cortisol rises in pregnancy; cortisol exerts anti-insulin effects by promoting gluconeogenesis and decreasing peripheral glucose uptake.
- Prolactin: influences β-cell mass and insulin secretion; has adaptive roles but can contribute to altered glucose homeostasis.
- Catecholamines: elevated in stress and can transiently raise glucose through glycogenolysis and gluconeogenesis.
- Mechanisms of insulin resistance:
- Post-receptor signaling defects: decreased insulin-stimulated glucose transporter translocation (reduced GLUT4 activity in maternal skeletal muscle and adipose tissue).
- Increased adipokines and inflammatory mediators from adipose tissue that impair insulin receptor signaling (e.g., TNF-α, IL-6).
- Increased hepatic glucose output due to hormonal stimulation of gluconeogenic enzymes (PEPCK, G6Pase).
Table — Hormones and Their Major Metabolic Effects in Pregnancy
|
Hormone |
Source |
Principal Metabolic Effects |
|
Human placental lactogen (hPL) |
Placenta |
↑ Lipolysis; ↑ Insulin resistance; fetal nutrient supply |
|
Placental growth hormone (PGH) |
Placenta |
↑ Hepatic gluconeogenesis; ↑ Insulin resistance |
|
Progesterone |
Ovary + Placenta |
Modulates glucose uptake; contributes to insulin resistance |
|
Estrogen |
Ovary + Placenta |
Alters insulin receptor signaling; affects adiposity |
|
Cortisol |
Maternal adrenal |
↑ Gluconeogenesis; ↓ peripheral glucose uptake |
|
Prolactin |
Pituitary |
↑ β-cell mass/function (adaptive) |
Nursing Insights
- Human placental lactogen is a dominant mediator of pregnancy-associated insulin resistance; when asked in exams, identify hPL as the hormone most directly correlated with maternal insulin resistance and increased free fatty acids. Clinically, anticipate insulin requirements to increase as hPL levels rise (mid-to-late pregnancy).
- Understand that multiple hormones cumulatively produce insulin resistance; therefore, single-hormone-focused interventions are insufficient — management must be multifactorial (nutrition, exercise, pharmacotherapy).
- For patients with intercurrent illness or corticosteroid therapy, expect acute worsening of hyperglycemia due to additive cortisol effects — increase monitoring and adjust therapy promptly.
1.3 Differences Between Preexisting Diabetes Mellitus And Gestational Diabetes Mellitus
- Timing and diagnosis:
- Preexisting diabetes mellitus is present before conception and includes Type 1 (autoimmune β-cell destruction with absolute insulin deficiency) and Type 2 (insulin resistance with relative insulin deficiency) diabetes. These patients carry risks from the earliest stages of embryogenesis, including congenital anomalies if glycemic control is poor during organogenesis (first trimester).
- Gestational diabetes mellitus (GDM) is glucose intolerance first recognized in pregnancy, usually diagnosed in the second or third trimester. GDM generally does not cause congenital anomalies attributable to hyperglycemia in the first trimester unless undiagnosed preexisting diabetes existed.
- Pathophysiologic substrate:
- Type 1: autoimmune-mediated β-cell loss → absolute insulin deficiency.
- Type 2: chronic insulin resistance often with β-cell dysfunction; obesity common.
- GDM: relative β-cell insufficiency that cannot compensate for pregnancy-induced insulin resistance.
- Maternal risks:
- Preexisting diabetes: higher rates of congenital malformations, miscarriage, exacerbation of microvascular disease (retinopathy, nephropathy), and chronic diabetes complications that can progress during pregnancy.
- GDM: higher risk of hypertensive disorders, cesarean delivery, and progression to Type 2 diabetes postpartum.
- Fetal/neonatal risks:
- Both conditions increase risks of macrosomia, birth trauma, neonatal hypoglycemia, and respiratory morbidity; preexisting diabetes carries a greater risk of structural congenital anomalies (cardiac, neural tube) due to hyperglycemia during organogenesis.

- Management differences:
- Preexisting diabetes requires preconception optimization of glycemic control (A1c target individualized, often <7% or lower if safe), adjustment of medications preconception (e.g., insulin preferred, teratogenic drugs stopped), and early pregnancy high-intensity surveillance.
- GDM management typically begins with medical nutrition therapy and glucose monitoring; pharmacologic therapy is initiated if glycemic targets are not met. Screening at 24–28 weeks is standard for average-risk women; high-risk women are screened earlier.
Nursing Insights
- For examinations and clinical practice, remember: congenital anomalies are primarily a risk of preexisting diabetes due to hyperglycemia during organogenesis; in contrast, GDM typically manifests after organogenesis and therefore is less associated with structural malformations.
- Clinically, a woman presenting with hyperglycemia at first prenatal visit should be evaluated for overt diabetes (preexisting) rather than assumed to have GDM; management and counseling differ substantively.
- Nurses should screen prior diagnosis and medication lists at the initial visit: if the patient uses oral hypoglycemics or has an A1c consistent with diabetes, manage as preexisting diabetes and initiate multidisciplinary care immediately.
1.4 Maternal Metabolic Adaptations To Pregnancy
- Pregnancy features both anabolic and catabolic phases with biochemical adaptations:
- Anabolic phase (first half of pregnancy): increased insulin sensitivity, increased maternal adipose deposition, increased hepatic glycogen stores, and increased appetite. These changes conserve energy and build maternal nutrient stores.
- Catabolic phase (second half of pregnancy): progressive insulin resistance, increased mobilization of lipids (elevated maternal free fatty acids and glycerol), enhanced hepatic gluconeogenesis, and increased basal metabolic rate. These changes ensure continuous nutrient flow to the fetus.
- Alterations in maternal lipid metabolism: pregnancy induces hyperlipidemia (↑ triglycerides, ↑ LDL cholesterol), which supplies substrates for placental steroidogenesis and fetal fat accretion. Elevated maternal lipids can also worsen insulin resistance.
- Protein metabolism: maternal protein turnover increases to supply fetal growth demands; maternal nitrogen balance is maintained by increased dietary intake and enhanced renal conservation.
- Energy balance and insulin requirements: insulin requirements typically decline slightly in early pregnancy, then rise progressively after 20 weeks and may double or triple by late third trimester in women with diabetes. Immediately postpartum, insulin sensitivity rapidly increases and insulin requirements drop precipitously; failure to anticipate this can cause maternal hypoglycemia.
Table — Summary of Maternal Metabolic Changes Across Pregnancy
|
Metabolic Domain |
Early Pregnancy (Anabolic) |
Late Pregnancy (Catabolic) |
|
Insulin sensitivity |
↑ |
↓ (progressive insulin resistance) |
|
Hepatic gluconeogenesis |
Baseline |
↑ |
|
Lipolysis |
Baseline |
↑ (↑ free fatty acids) |
|
Insulin requirements (diabetic patients) |
↓/stable |
↑ (may double/triple) |
|
Fetal glucose transfer |
Increasing |
Maximal (via GLUT1) |
Nursing Insights
- Anticipate increasing insulin requirements in the second and third trimesters for patients on insulin; schedule more frequent glucose checks and adjust sliding scales accordingly. Practical tip: document trends to guide dose titration rather than react to single abnormal readings.
- After delivery, anticipate rapid decrease in insulin needs; implement protocols for postpartum insulin dose reduction and vigilant hypoglycemia monitoring in the immediate postpartum period.
- Understand the metabolic rationale for counseling about diet composition: distributing carbohydrate intake and providing adequate protein and complex carbohydrates maintains maternal-fetal glucose homeostasis while reducing postprandial peaks.
1.5 Fetal Glucose Metabolism And Insulin Response
- The fetus relies predominantly on maternal glucose delivered via placental transfer; fetal endogenous gluconeogenesis is minimal until late gestation. Fetal glucose concentration is proportional to maternal glucose concentration, typically ~70–80% of maternal levels.
- Fetal pancreatic β-cells respond to increased glucose with increased insulin secretion. Fetal hyperinsulinemia is a key mediator of many diabetic pregnancy complications:
- Fetal macrosomia results from insulin-stimulated adipogenesis and somatic growth; fetal insulin acts as an anabolic growth factor.

- Polyhydramnios can occur due to fetal hyperglycemia-induced osmotic diuresis increasing fetal urine output.
- Delayed pulmonary maturation: fetal hyperinsulinemia antagonizes cortisol-induced surfactant synthesis, increasing the risk of respiratory distress syndrome (RDS) even at term or near-term.
- After birth, the abrupt interruption of maternal glucose supply combined with persistent neonatal hyperinsulinemia predisposes the neonate to hypoglycemia within the first hours after delivery. Risk is highest in neonates of mothers with poorly controlled diabetes or those with marked maternal hyperglycemia.
- Other fetal metabolic consequences: intermittent fetal hyperglycemia can increase fetal oxygen consumption and result in relative fetal hypoxemia, promoting polycythemia and hyperbilirubinemia after birth due to increased erythropoiesis and subsequent hemolysis.
Nursing Insights
- Recognize that fetal hyperinsulinemia is central to the pathogenesis of macrosomia, polyhydramnios, RDS, neonatal hypoglycemia, and polycythemia; thus, maternal glycemic control during pregnancy is the primary preventive strategy.
- Intrapartum nursing care should anticipate that neonates of diabetic mothers require early feeding and glucose monitoring within the first 1–2 hours after birth; arrange neonatal glucose checks per protocol (e.g., at 30–60 minutes, and serially thereafter) to detect hypoglycemia early.
- Understand the physiologic basis for increased risk of RDS in infants of diabetic mothers: counsel that even term infants may need respiratory support and monitoring, and coordinate neonatal respiratory preparedness during delivery.
Types Of Diabetes In Pregnancy
1.1 Preexisting Diabetes Mellitus (Type 1 And Type 2)
- Definition and general considerations
- Preexisting diabetes mellitus refers to hyperglycemic disorders that are present prior to conception and therefore expose the embryo and fetus to abnormal metabolic milieu from conception onward.
- Two principal types are Type 1 diabetes mellitus (T1DM) and Type 2 diabetes mellitus (T2DM); each has distinct pathophysiology, clinical course, and obstetric implications that influence prenatal counseling, antenatal surveillance, intrapartum management, and postpartum follow-up.
- Type 1 Diabetes Mellitus (T1DM)
- Pathophysiology: autoimmune-mediated destruction of pancreatic β-cells leading to absolute insulin deficiency and requirement for exogenous insulin replacement.
- Clinical phenotype: often presents in childhood/adolescence but can present at any age; typically lean body habitus but not universally.
- Pregnancy implications:
- High risk for congenital anomalies if glycemic control is poor during organogenesis (first trimester).
- Increased risk of diabetic microvascular complications (retinopathy, nephropathy) progression during pregnancy; pregnancy may transiently worsen retinopathy.
- Greater variability in glycemic control with risk of hypoglycemia (especially in early pregnancy) due to increased insulin sensitivity in the first trimester and changing insulin requirements.
- Preconception optimization of glycemic control (A1c target individualized; frequently ≤7% if achievable without significant hypoglycemia) is crucial to reduce malformation risk.
- Type 2 Diabetes Mellitus (T2DM)
- Pathophysiology: chronic peripheral insulin resistance combined with relative β-cell dysfunction; frequently associated with obesity, dyslipidemia, hypertension, and metabolic syndrome.
- Clinical phenotype: commonly diagnosed in adulthood; often associated with overweight/obesity and features of insulin resistance.
- Pregnancy implications:
- Many women with T2DM are diagnosed before pregnancy but some have undiagnosed diabetes discovered at first prenatal visit.
- Risk for congenital anomalies exists if hyperglycemia is present during organogenesis; the degree of risk correlates with the level and duration of hyperglycemia.
- These women frequently have comorbidities (e.g., hypertension, dyslipidemia) that increase obstetric risk (preeclampsia, cesarean delivery).
- Management often requires transition from oral hypoglycemics to insulin preconception or in early pregnancy because many oral agents are not recommended in pregnancy (exceptions and evolving evidence exist for metformin in selected settings).
- Shared features and practical concerns for preexisting diabetes
- Both types require individualized preconception counseling, medication review, and glycemic optimization before conception.
- Women with preexisting diabetes need early fetal anatomic ultrasound, targeted screening for microvascular complications, and more intensive fetal surveillance in pregnancy.
- Insulin regimens almost always need adjustment during pregnancy; physiologic insulin needs fall in early pregnancy and then rise markedly in the second and third trimesters.
Nursing Insights
- Assess medication lists at the first prenatal visit: if the patient is on oral hypoglycemics, treat as potential T2DM and coordinate prompt evaluation of A1c and fasting glucose; do not assume GDM.
- Teach patients about the importance of preconception glycemic control; specifically document their last A1c and counsel on target values and risks of poor control in early pregnancy.
- Monitor for and document baseline microvascular disease (retinopathy, nephropathy): arrange ophthalmology review and renal function assessment early in pregnancy.
- Practical tip: instruct patients on how to adjust insulin with symptomatic hypoglycemia in early pregnancy and caution about nocturnal hypoglycemia; promote frequent SMBG (self-monitoring blood glucose) during periods of regimen change.
1.2 Gestational Diabetes Mellitus (GDM)
- Definition
- Gestational diabetes mellitus is glucose intolerance with onset or first recognition during pregnancy. It typically manifests in the second or third trimester when the physiological insulin resistance of pregnancy peaks. GDM usually resolves after delivery but indicates future risk for Type 2 diabetes.
- Pathophysiology (concise recap relevant here)
- Pregnancy-associated hormonal changes (hPL, placental growth hormone, cortisol, progesterone, estrogen) increase insulin resistance. GDM occurs when pancreatic β-cell insulin secretion is insufficient to overcome this resistance. The result is maternal hyperglycemia with maternal–fetal metabolic consequences.
- Clinical features and course
- GDM often is asymptomatic and detected by screening at 24–28 weeks in average-risk women or earlier in those at high risk.
- Glycemic abnormalities are most frequently postprandial hyperglycemia; fasting hyperglycemia is less commonly predominant but can occur.
- GDM is associated with excess fetal growth (macrosomia), polyhydramnios, birth trauma, neonatal hypoglycemia, and increased cesarean rates.
- Management overview (brief here; detailed management is in Section 12)
- Initial management focuses on medical nutrition therapy (MNT), physical activity, and SMBG. If glycemic targets are not achieved, pharmacologic therapy (insulin preferred; oral agents like metformin or glyburide used selectively) is initiated.
- Postpartum follow-up with a 75-g OGTT at 6–12 weeks postpartum is recommended to identify persistent diabetes.
Nursing Insights
- Do not delay screening in high-risk women—they may have overt preexisting diabetes rather than GDM; early screening at the first prenatal visit is important.
- Educate patients that GDM is a marker of future cardiometabolic risk; emphasize lifestyle modification postpartum to reduce risk of Type 2 diabetes.
- Practical patient education point: explain that successful initial management is often diet and exercise; clarify SMBG targets and frequency to empower self-management.
1.3 Classification Of Diabetes In Pregnancy
- Simplified classification schema (useful for clinical communication and documentation):
- Overt diabetes in pregnancy (preexisting diabetes)
- Type 1 diabetes mellitus
- Type 2 diabetes mellitus
- Previously undiagnosed diabetes identified in early pregnancy (A1c ≥6.5% or fasting glucose ≥126 mg/dL) — treat as overt diabetes.
- Gestational diabetes mellitus (GDM)
- GDM diagnosed in pregnancy (usually per 75-g one-step or 2-step approach).
- Subcategories for clinical nuance
- Diet-controlled GDM (managed with MNT alone)
- Pharmacologically treated GDM (requires insulin and/or oral agents)
- GDM with complications (e.g., polyhydramnios, macrosomia)
- Overt diabetes in pregnancy (preexisting diabetes)
- Clinical documentation and coding implications
- Distinguish in notes between pregestational (preexisting) and gestational diabetes for appropriate antenatal surveillance and for postpartum follow-up planning.
- Use objective criteria (A1c, fasting glucose, OGTT results) to classify and to guide management pathways.
Table — Key Clinical Differences at a Glance
|
Feature |
Preexisting Diabetes (T1/T2) |
GDM |
|
Onset |
Before conception or identified at first visit |
Typically diagnosed after 24 weeks |
|
Risk of congenital anomalies |
High if poor control during organogenesis |
Low unless undiagnosed preexisting diabetes |
|
Primary pathophysiology |
T1: absolute insulin deficiency; T2: chronic insulin resistance |
Relative β-cell insufficiency vs pregnancy insulin resistance |
|
Surveillance intensity |
High (early fetal ultrasound, microvascular monitoring) |
Moderate to high (growth scans, glycemic monitoring) |
|
Postpartum diabetes risk |
Often persists (T1/T2) |
Increased lifetime risk of T2DM; often resolves postpartum |
Nursing Insights
- When triaging pregnant patients, always determine whether diabetes is preexisting or gestational because immediate management, preconception counseling history, and surveillance differ markedly.
- Document key objective values (A1c, fasting glucose, OGTT results) in the chart so that any clinician can rapidly determine classification and next steps.
Practical bedside reminder: if A1c ≥6.5% or fasting glucose ≥126 mg/dL early in pregnancy, treat as overt diabetes and escalate referrals.
Risk Factors For Gestational Diabetes Mellitus
1.1 Modifiable Risk Factors
- Obesity and elevated pre-pregnancy BMI
- Pre-pregnancy BMI ≥30 kg/m² is a strong predictor of GDM due to preexisting insulin resistance mediated by adiposity and associated inflammatory adipokines (e.g., TNF-α, IL-6).
- Weight reduction prior to conception reduces GDM risk and improves pregnancy outcomes.
- Excessive gestational weight gain
- Weight gain above Institute of Medicine (IOM) recommendations increases insulin resistance and GDM risk; counseling on appropriate gestational weight gain tailored to pre-pregnancy BMI is essential.
- Poor diet quality
- Diets high in refined carbohydrates and saturated fats and low in fiber increase insulin resistance and glucose excursions. Dietary modification emphasizing complex carbohydrates, fiber, and balanced macronutrient distribution mitigates risk.
- Physical inactivity / Sedentary lifestyle
- Lack of regular moderate-intensity exercise reduces insulin-stimulated glucose uptake by skeletal muscle and increases GDM risk.
- Smoking
- Cigarette smoking has been associated with insulin resistance and adverse metabolic effects, contributing to higher GDM risk.
- Polycystic ovary syndrome (PCOS) (modifiable to an extent)
- PCOS is associated with insulin resistance; weight management and preconception optimization can reduce GDM risk.
- Previous GDM (modifiable risk via postpartum lifestyle)
- Women with prior GDM have a high recurrence risk; postpartum lifestyle interventions (diet, exercise, weight control) reduce recurrence.
Nursing Insights
- Implement targeted preconception counseling focusing on weight optimization and smoking cessation for women planning pregnancy; document BMI and provide specific, evidence-based weight goals.
- Provide concrete dietary guidance: recommend distribution of carbohydrates across meals and 2–3 snacks, prioritize complex carbohydrates and vegetable fiber, and avoid sugar-sweetened beverages.
- Encourage and prescribe (documented) moderate-intensity exercise (e.g., 30 minutes brisk walking most days) unless contraindicated; explain mechanisms (improved insulin sensitivity) to enhance adherence.
1.2 Non-Modifiable Risk Factors
- Advanced maternal age
- Maternal age ≥35 years is associated with increased risk of GDM, likely due to age-related decline in β-cell function and increased insulin resistance.
- Ethnicity/race
- Certain ethnic groups have higher GDM prevalence (e.g., Hispanic, South Asian, Native American, African descent). Ethnic predisposition likely reflects genetic predisposition and sociocultural determinants of metabolic risk.
- Family history of Type 2 diabetes (first-degree relative)
- A positive family history indicates genetic susceptibility to insulin resistance and β-cell dysfunction.
- History of macrosomic infant or prior obstetric history
- Previous delivery of a macrosomic infant (e.g., birth weight >4,000 g or large-for-gestational-age) or prior GDM increases recurrence risk.
- Prior impaired glucose tolerance or impaired fasting glucose
- Documented prediabetes prior to pregnancy predicts higher GDM risk.
- Genetic predisposition
- Polymorphisms related to insulin secretion and action increase risk; while not modifiable, they inform individualized risk assessment.
Table — Major Modifiable vs Non-Modifiable Risk Factors
|
Modifiable Risk Factors |
Non-Modifiable Risk Factors |
|
Obesity (pre-pregnancy BMI ≥30 kg/m²) |
Advanced maternal age (↑ risk with age) |
|
Excessive gestational weight gain |
Ethnic background (e.g., Hispanic, South Asian) |
|
Sedentary lifestyle |
Family history of T2DM |
|
Poor diet (high refined carbs, low fiber) |
Prior GDM or macrosomic infant |
|
Smoking |
Prior impaired glucose tolerance/prediabetes |
|
PCOS (partially modifiable via weight loss) |
Genetic predisposition |
Nursing Insights
- At booking/first prenatal visit, perform targeted risk stratification: record pre-pregnancy BMI, family history, ethnicity, obstetric history (previous macrosomia/GDM), and PCOS/other endocrine disorders. Use this stratification to determine timing of screening (early vs routine 24–28 weeks).
- Provide culturally sensitive education: tailor dietary and exercise recommendations to the patient's cultural food practices, socioeconomic context, and access to resources.
- Create a documented individualized care plan that lists modifiable risks with explicit, measurable interventions (e.g., "Patient will perform 30 minutes brisk walking 5 days/week" and "Patient will reduce sugar-sweetened beverage intake to 0/week").
Screening And Diagnosis Of Gestational Diabetes Mellitus
Screening and diagnosis of gestational diabetes mellitus (GDM) require clear understanding of the available approaches, standardized test procedures, diagnostic thresholds, and postpartum surveillance. The clinician must balance sensitivity and specificity of screening strategies with local practice patterns and patient risk profile. Below are comprehensive, detailed, and clinically practical notes that synthesize current, commonly used diagnostic approaches and the nursing implications for each step.
1.1 Screening Guidelines (One-Step And Two-Step Approaches)
- General principles:
- Screening for GDM identifies women with glucose intolerance that developed or was first recognized during pregnancy and allows timely interventions to reduce maternal and fetal complications.
- There are two widely used screening strategies: the one-step approach (IADPSG / WHO style using 75-g OGTT) and the two-step approach (ACOG/older U.S. practice using a non-fasting 50-g glucose challenge test followed by a diagnostic 100-g OGTT if the screen is positive). Choice of approach depends on institutional policy, population characteristics, and resource availability.
- One-Step Approach (75-g OGTT — IADPSG / WHO style):
- Single fasting 75-g oral glucose tolerance test performed at 24–28 weeks for average-risk women (earlier if high risk).
- Advantages: single diagnostic test; harmonizes screening/diagnosis; based on pregnancy outcomes (HAPO study) to identify women at increased risk of adverse outcomes.
- Disadvantages: increases the number of women diagnosed with GDM compared with two-step; requires fasting and more laboratory resources.
- Two-Step Approach (50-g GCT screening followed by 100-g OGTT diagnostic test):
- Step 1: Non-fasting 50-g glucose challenge test (GCT) at 24–28 weeks. If result ≥ threshold (commonly 130–140 mg/dL depending on institutional cutpoint), proceed to Step 2.
- Step 2: Fasting 100-g 3-hour OGTT with measurement of fasting, 1-hour, 2-hour, and 3-hour values; diagnostic thresholds (Carpenter-Coustan or NDDG) are applied to determine GDM.
- Advantages: fewer women undergo the full OGTT; more widely used historically in the U.S.; convenient initial non-fasting screen.
- Disadvantages: requires two clinical visits if positive screen; possible false negatives/positives depending on screening threshold.
Table — One-Step vs Two-Step Approach (Key Operational Differences)
|
Feature |
One-Step (75-g OGTT) |
Two-Step (50-g GCT → 100-g OGTT) |
|
Test timing |
24–28 weeks (earlier if high risk) |
24–28 weeks (earlier if high risk) |
|
Fasting required |
Yes |
No for GCT; Yes for OGTT |
|
Number of blood draws |
Fasting, 1h, 2h |
Non-fasting 1h (GCT); if positive → fasting, 1h, 2h, 3h (OGTT) |
|
Diagnostic thresholds |
IADPSG/WHO criteria |
Carpenter-Coustan or NDDG thresholds |
|
Pros |
Single diagnostic test; outcome-based |
Fewer full OGTTs; long historical use |
|
Cons |
More diagnoses; requires fasting |
Two steps; potential for extra visits |
Nursing Insights
- Know your institution’s protocol: before ordering or scheduling, verify whether the clinic/hospital uses one-step or two-step screening because patient preparation and scheduling differ.
- Educate patients clearly about fasting requirements and dietary preparation to avoid invalid results; failure to follow preparation increases false negatives/positives.
- For high-risk women (e.g., prior GDM, obesity, strong family history), the nurse should ensure early screening at the first prenatal visit in addition to the routine 24–28 weeks screen.
1.2 Glucose Challenge Test (GCT)
- Purpose and rationale:
- The 50-g oral glucose challenge test is a screening test designed to identify women who need definitive diagnostic testing (OGTT). It screens primarily for postprandial glucose dysregulation and is convenient because it does not require fasting.
- Test procedure (standardized steps):
- Patient does not need to fast for the 50-g GCT; however, standard diet in preceding days is advisable (see Nursing Insights).
- Administer 50 g of oral glucose solution; start timer at ingestion completion.
- Draw a venous blood sample exactly at 1 hour post ingestion to measure plasma glucose. Do not use fingerstick unless validated by laboratory protocol.
- Interpret using institution threshold (common thresholds: ≥130 mg/dL, ≥135 mg/dL, or ≥140 mg/dL). Lower thresholds increase sensitivity but increase false positives; many institutions use 140 mg/dL as a balance.

- Advantages and limitations:
- Advantage: patient convenience (non-fasting), low resource burden.
- Limitation: not diagnostic—requires follow-up OGTT if positive; sensitivity and specificity vary by threshold and population.
Nursing Insights
- Be precise about timing: the 1-hour draw must be accurate; documenting the exact ingestion and blood draw times prevents misinterpretation.
- Warn patients about possible nausea when drinking concentrated glucose solution and provide strategies (sip slowly if tolerated).
- If the patient is vomiting shortly after ingestion, the test must be repeated; document occurrence and reason for repeat.
- Instruct patients to avoid smoking or vigorous activity during the hour between ingestion and blood draw because both can alter glucose measurements.
1.3 Oral Glucose Tolerance Test (OGTT)
- Indications:
- Per the two-step approach, indicated when the 50-g GCT is above the institutional cutpoint.
- Per the one-step approach, the 75-g OGTT is the primary diagnostic test at 24–28 weeks (or earlier if high risk / abnormal fasting glucose).
- Also indicated postpartum (75-g OGTT) to detect persistent diabetes.
- Preparation for OGTT:
- Fasting: patient should fast for 8–14 hours prior to the test; only water is permitted.
- Diet: recent evidence and many guidelines recommend consuming a usual diet containing adequate carbohydrates for at least 3 days prior to the test to avoid false positives due to carbohydrate restriction.
- Medications: review medications that may affect glucose (e.g., corticosteroids, beta-blockers) and coordinate testing around such exposures when possible.
- Activity and smoking: advise avoidance of vigorous activity and smoking before and during the test.

- Test types and procedures:
- 75-g 2-hour OGTT (One-step): fasting venous glucose drawn, administer 75 g glucose, then draw at 1 hour and 2 hours. Used for both diagnosis and postpartum evaluation (75 g postpartum).
- 100-g 3-hour OGTT (Two-step diagnostic test): fasting venous glucose drawn, administer 100 g glucose, then draw at 1 hour, 2 hours, and 3 hours. Diagnostic thresholds differ by Carpenter-Coustan vs older NDDG criteria.
- Common diagnostic threshold sets (widely used):
- IADPSG / WHO (One-step 75-g OGTT) — diagnostic if any one of the following is met or exceeded:
- Fasting ≥ 92 mg/dL
- 1-hour ≥ 180 mg/dL
- 2-hour ≥ 153 mg/dL
- Carpenter-Coustan (100-g OGTT, Two-step) — GDM diagnosed if ≥2 values meet or exceed:
- Fasting ≥ 95 mg/dL
- 1-hour ≥ 180 mg/dL
- 2-hour ≥ 155 mg/dL
- 3-hour ≥ 140 mg/dL
- NDDG (older) thresholds use slightly higher cutpoints (e.g., fasting 105 mg/dL); many centers still reference Carpenter-Coustan.
- IADPSG / WHO (One-step 75-g OGTT) — diagnostic if any one of the following is met or exceeded:
Table — OGTT Types and Common Diagnostic Cutpoints
|
Test |
Timing |
Common Diagnostic Cutpoints |
|
75-g OGTT (IADPSG/WHO) |
Fasting, 1h, 2h |
Fasting ≥92 mg/dL; 1h ≥180 mg/dL; 2h ≥153 mg/dL; any one abnormal = GDM |
|
100-g OGTT (Carpenter-Coustan) |
Fasting, 1h, 2h, 3h |
Fasting ≥95 mg/dL; 1h ≥180 mg/dL; 2h ≥155 mg/dL; 3h ≥140 mg/dL; ≥2 abnormal = GDM |
Nursing Insights
- Preparation is critical: ensure patient has fasted 8–14 hours and had normal carbohydrate intake in prior days. If the patient fasted but had inadequate carbohydrate intake in prior days, consider rescheduling or document potential for false results.
- Strict timing of blood draws and accurate sample handling are essential; label tubes clearly and communicate timing to lab staff.
- Be aware that different diagnostic criteria exist; when communicating results to the patient and providers, clearly state which criteria were used (e.g., “75-g OGTT, IADPSG criteria applied”).
- For the 100-g OGTT, instruct patients to plan for a clinical visit of at least 3 hours and provide a comfortable setting; consider antiemetic measures if prior nausea with concentrated glucose.
1.4 Diagnostic Criteria
- Interpretation depends on the chosen approach: the nurse must know which criteria apply locally and document them clearly in the chart. Below are operational rules for interpretation.
- 75-g OGTT (IADPSG/WHO; One-step): diagnosis of GDM is made if any one value meets or exceeds the threshold (fasting ≥92 mg/dL; 1-hour ≥180 mg/dL; 2-hour ≥153 mg/dL). This approach increases sensitivity and identifies women with milder abnormalities associated with adverse outcomes.
- 100-g OGTT (Carpenter-Coustan; Two-step diagnostic): diagnosis is made if two or more values meet or exceed thresholds (fasting ≥95 mg/dL; 1-hour ≥180 mg/dL; 2-hour ≥155 mg/dL; 3-hour ≥140 mg/dL). Use of Carpenter-Coustan criteria is common in centers using the two-step approach.
- Overt Diabetes vs GDM:
- If early pregnancy testing (first prenatal visit) shows A1c ≥6.5% or fasting glucose ≥126 mg/dL or random glucose ≥200 mg/dL with symptoms, the patient is considered to have overt diabetes (preexisting) and should be managed accordingly; do not label as GDM.
- Borderline or discordant results:
- If one test is borderline or if clinical suspicion is high despite negative screening, consider repeat testing, early postpartum testing, or referral to endocrinology as appropriate. Clinical judgment is required for cases with discordant results and multiple comorbidities.
Nursing Insights
- When communicating results, always specify the test type, numeric values, and which diagnostic criteria were applied; e.g., “75-g OGTT: fasting 94 mg/dL, 1h 178 mg/dL, 2h 160 mg/dL — IADPSG criteria: 2-hour abnormal → GDM.” Clear documentation prevents misclassification.
- Educate patients on the distinction between overt diabetes and GDM to reduce anxiety and ensure appropriate follow-up; explain that overt diabetes requires more intensive management.
- For borderline abnormal results, create a follow-up plan: increased SMBG, repeat OGTT, or referral within days to weeks depending on clinical risk.
1.5 Postpartum Screening For Persistent Glucose Intolerance
- Rationale: GDM frequently resolves after delivery, but women with GDM are at substantially higher lifetime risk of Type 2 diabetes; postpartum testing identifies persistent diabetes or prediabetes and permits early preventive measures.
- Recommended timing and tests:
- 6–12 weeks postpartum: perform a 75-g 2-hour OGTT (preferred) to detect persistent diabetes or impaired glucose tolerance. This timing allows for return toward baseline insulin sensitivity and a reliable assessment of glucose metabolism.
- Alternative or adjunct tests: fasting plasma glucose and hemoglobin A1c can be used but are less sensitive for detecting impaired glucose tolerance in the early postpartum period; if using A1c, interpret cautiously in women with recent blood loss or transfusion.
- Subsequent screening: if postpartum OGTT is normal, repeat screening for diabetes at least every 1–3 years (frequency individualized by other risk factors). Annual screening may be appropriate for women with multiple risk factors (obesity, strong family history).
- Long-term follow-up and prevention:
- Counsel and support lifestyle interventions: weight reduction if overweight, regular physical activity, and dietary modifications to prevent progression to Type 2 diabetes. Breastfeeding is encouraged and associated with improved maternal glucose metabolism.
- Consider referral to primary care or endocrinology for ongoing surveillance and risk management; discuss use of metformin for diabetes prevention in selected high-risk women per clinical guidelines.
Nursing Insights
- Arrange postpartum OGTT prior to hospital discharge planning: schedule testing for 6–12 weeks and provide reminder systems (calls/texts) because many women do not return for postpartum care.
- Educate patients about the high risk of progression to Type 2 diabetes and the importance of postpartum screening and lifestyle changes; provide written, culturally relevant materials and local resources (nutritionists, community exercise programs).
- Coordinate care transitions: ensure a documented handoff to primary care with results and a plan for long-term screening; consider electronic reminders in the chart.
Maternal And Fetal Complications Of Diabetes In Pregnancy
Diabetes in pregnancy predisposes both the mother and fetus to a spectrum of pathophysiologic derangements that arise from maternal hyperglycemia, fetal hyperinsulinemia, altered placental function, and associated comorbidities. The following sections examine maternal complications and fetal/neonatal complications in depth, with mechanistic explanations, clinical manifestations, diagnostic considerations, and nursing implications.
1.1 Maternal Complications
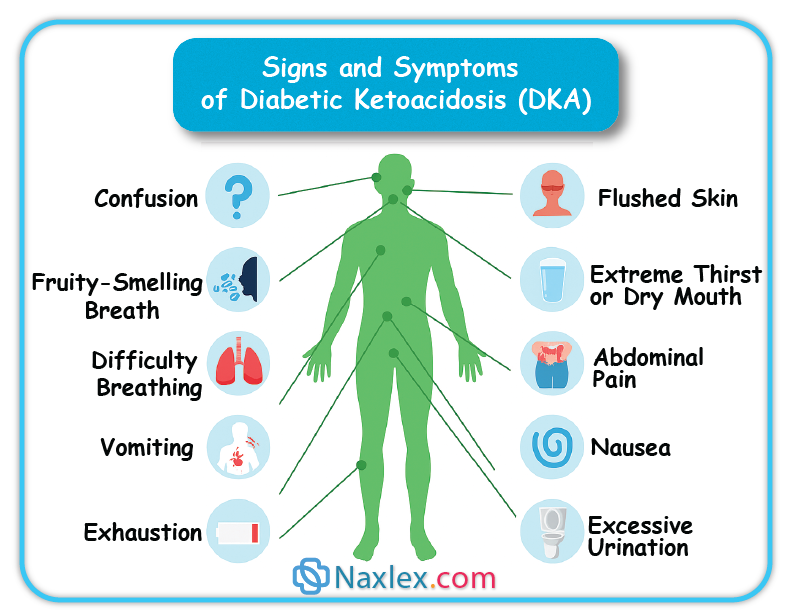
1.1.1 Diabetic Ketoacidosis (DKA)
- Pathophysiology and precipitating factors
- Diabetic ketoacidosis is an acute, life-threatening decompensation characterized by absolute or relative insulin deficiency, marked hyperglycemia, increased lipolysis, ketogenesis with accumulation of ketone bodies (β-hydroxybutyrate, acetoacetate), metabolic acidosis (anion gap), and osmotic diuresis.
- Pregnancy increases susceptibility to DKA at lower glucose thresholds due to placental hormones (hPL, cortisol) that enhance insulin resistance and due to increased maternal respiratory alkalosis (which shifts the bicarbonate buffer). Common precipitants include infection, vomiting, missed insulin doses, corticosteroid administration, and intercurrent illness.
- Clinical features in pregnancy
- Maternal: polyuria, polydipsia, dehydration, nausea, vomiting, abdominal pain, Kussmaul respirations, altered mental status, hypotension, tachycardia.
- Fetal: uterine hypoperfusion and fetal distress can occur rapidly because maternal acidosis and hypovolemia reduce uteroplacental perfusion; intrauterine fetal demise is a known complication of severe DKA.
- Diagnosis
- Laboratory: plasma glucose often >200 mg/dL but may be lower in pregnancy; serum β-hydroxybutyrate elevated; arterial or venous blood gas showing high anion gap metabolic acidosis; serum electrolytes with variable potassium (initially normal/high then total body potassium depletion), elevated BUN/creatinine if volume depleted. Urinalysis positive for ketones (but serum measurement preferred).
- Note: in pregnancy, DKA can occur with modest hyperglycemia (e.g., 200–300 mg/dL) compared with nonpregnant thresholds; maintain high suspicion.
- Management principles
- Immediate resuscitation: secure airway, oxygen as needed, aggressive IV fluid resuscitation with isotonic crystalloid (e.g., 0.9% NaCl) to restore intravascular volume and perfusion.
- Insulin therapy: continuous IV regular insulin infusion after initial fluid resuscitation (bolus and infusion per protocol) to suppress ketogenesis and reduce glucose gradually; avoid rapid osmolar shifts.
- Electrolyte repletion: anticipate hypokalemia with insulin therapy; monitor serum potassium and replace promptly to maintain safe ranges (typically K+ target 4–5 mEq/L).
- Correct acidosis and underlying precipitants (e.g., treat infection, antiemetics for vomiting).
- Fetal monitoring: continuous fetal heart rate monitoring for viable fetuses after maternal stabilization; do not proceed to emergent cesarean for abnormal FHR until maternal resuscitation has been attempted unless nonreassuring FHR persists despite stabilization.
- Prognosis and prevention
- With prompt recognition and aggressive management, maternal and fetal outcomes improve; however, delays increase risk of fetal demise. Prevention includes strict adherence to insulin regimens, sick-day rules (adjust insulin, maintain hydration, contact provider early), and prompt treatment of infections.
Nursing Insights
- Recognize atypical presentation: in pregnancy, DKA may present with lower glucose values; therefore, do not rely solely on an absolute glucose threshold to exclude DKA. Act on clinical symptoms (nausea/vomiting, abdominal pain, tachypnea) with prompt bedside glucose and ketone assessment.
- Implement sick-day protocols: educate patients to check ketones when ill or hyperglycemic (>250 mg/dL), to not stop insulin, to hydrate with carbohydrate-containing fluids as advised, and to seek immediate care for persistent vomiting or positive ketones.
- In acute management, the nurse must vigilantly monitor fluid input/output, hourly glucose, insulin infusion parameters, cardiac telemetry, and frequent electrolyte checks, with particular attention to potassium replacement timing relative to insulin infusion.
- Coordinate maternal-fetal monitoring: after maternal stabilization begins, ensure continuous FHR monitoring for viable fetus and notify obstetric team of any persistent nonreassuring tracings; document maternal interventions and fetal responses precisely.
1.1.2 Preeclampsia
- Pathophysiologic link to diabetes
- Diabetes (especially preexisting T2DM with chronic vascular disease) increases risk of gestational hypertension and preeclampsia due to endothelial dysfunction, chronic inflammation, preexisting hypertension, and microvascular disease. Hyperglycemia promotes oxidative stress and impaired nitric oxide–mediated vasodilation, augmenting preeclampsia risk.
- Clinical implications
- Pregnant women with diabetes have higher incidence of severe preeclampsia, earlier onset disease, and increased maternal complications (eclampsia, HELLP syndrome). Concomitant nephropathy increases risk for superimposed preeclampsia and worsened renal outcomes.
- Diagnosis and surveillance
- Standard diagnostic criteria for preeclampsia apply (new-onset hypertension ≥140/90 mm Hg with proteinuria or end-organ dysfunction after 20 weeks). In women with preexisting proteinuria or chronic hypertension, diagnosis of superimposed preeclampsia requires new or worsening hypertension, sudden increase in proteinuria, or new end-organ dysfunction.
- Surveillance: tighter blood pressure monitoring, renal function tests, urine protein quantification, and ophthalmologic assessment if retinopathy suspected.
Nursing Insights
- For women with diabetes, document baseline blood pressure and renal function early; institute frequent antenatal BP checks and educate patients to monitor for preeclampsia symptoms (headache, visual changes, epigastric pain, rapid edema) and to report them immediately.
- Recognize that preeclampsia in a woman with diabetic nephropathy may be difficult to differentiate; serial trends in BP, urine protein, and laboratory markers (platelets, LFTs) help clarify superimposed disease.
- Prepare for early delivery if severe preeclampsia develops; ensure neonatal team notification due to increased likelihood of prematurity and neonatal complications.
1.1.3 Polyhydramnios
- Mechanism
- Polyhydramnios (excess amniotic fluid) occurs in diabetic pregnancies predominantly due to fetal hyperglycemia → fetal osmotic diuresis → increased fetal urine output → excess amniotic fluid volume. Additional contribution may come from fetal gastrointestinal anomalies or impaired swallowing in other contexts, but in diabetes osmotic diuresis is common.
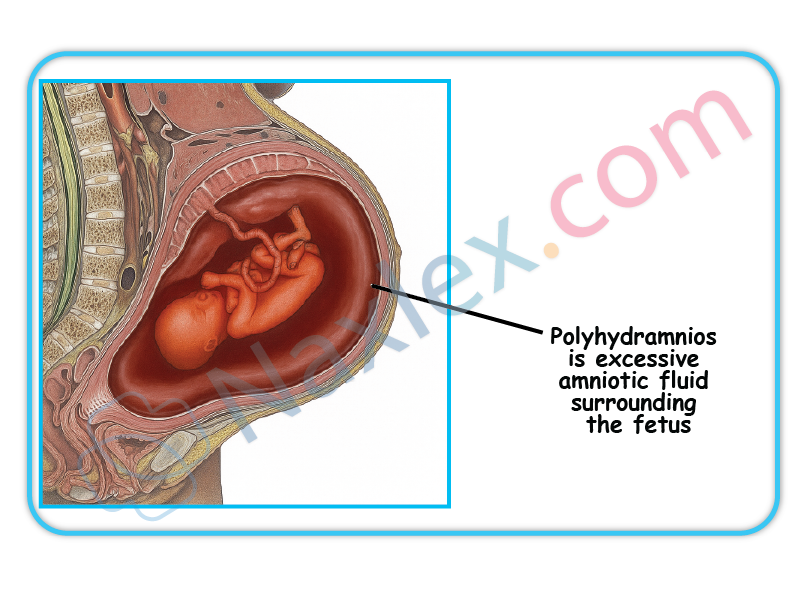
- Clinical consequences
- Increased risk of preterm labor, malpresentation, uterine overdistension, placental abruption, and postpartum hemorrhage due to uterine atony. Polyhydramnios can complicate intrapartum management and increase cesarean risk.
- Diagnosis and monitoring
- Ultrasound measurement using amniotic fluid index (AFI) or single deepest pocket (SDP) methods; AFI >25 cm or SDP >8 cm commonly used thresholds for polyhydramnios (guidelines vary). Serial ultrasounds to monitor progression.
Nursing Insights
- When polyhydramnios is identified, counsel patient about signs of preterm labor and decreased fetal movement; increase antenatal surveillance and plan for potential preterm delivery.
- Expect more intensive intrapartum management: anticipate need for tocolysis if preterm labor occurs (balance against maternal glycemic control and other contraindications) and prepare for possible postpartum hemorrhage—ensure uterotonics are available and blood loss monitoring is meticulous.
1.1.4 Infections
- Increased susceptibility and mechanisms
- Hyperglycemia impairs leukocyte function (chemotaxis, phagocytosis), impairs complement activity, and augments glucose in body fluids, providing pro-growth conditions for pathogens. Diabetic pregnancy predisposes to urinary tract infections (including asymptomatic bacteriuria progressing to pyelonephritis), vulvovaginal candidiasis, and surgical site infections postpartum or after cesarean.
- Clinical impact
- Infections can precipitate metabolic decompensation (DKA), cause preterm labor, and increase maternal morbidity. Pyelonephritis in pregnancy is associated with sepsis and preterm birth.
Nursing Insights
- Screen for and promptly treat asymptomatic bacteriuria in pregnant women with diabetes as per guidelines because of higher progression risk to pyelonephritis.
- Provide patient education on genital hygiene, recognizing signs of infection (fever, dysuria, foul-smelling discharge), and early reporting. Emphasize blood glucose optimization to reduce infection risk.
- In perioperative settings (e.g., cesarean delivery), implement strict sterile technique and glycemic control to reduce surgical site infections; coordinate appropriate antibiotic prophylaxis.
1.2 Fetal Complications
Fetal and neonatal complications arise predominantly from maternal hyperglycemia causing fetal hyperinsulinemia, abnormal growth patterns, altered organ maturation, and metabolic instability postdelivery.
1.2.1 Congenital Anomalies
- Epidemiology and risk factors
- Preexisting maternal diabetes (especially poor glycemic control during organogenesis, i.e., first trimester) increases the risk of structural congenital anomalies—most commonly congenital cardiac defects (septal defects, conotruncal anomalies), neural tube defects (spina bifida), and caudal regression spectrum. GDM diagnosed after the first trimester is less commonly associated with congenital anomalies unless preexisting diabetes was unrecognized.
- Pathophysiology
- Hyperglycemia during embryogenesis induces oxidative stress, alters gene expression, and interferes with morphogenetic signaling pathways, increasing malformation risk. Elevated A1c in early pregnancy strongly correlates with increased malformation rates.
- Screening and prevention
- Preconception glycemic optimization (A1c target individualized, commonly <7% if safely achievable) reduces anomaly risk. Early anatomic ultrasound (dating and targeted anatomy scan) and first-trimester nuchal translucency and cell-free DNA screening are used per obstetric guidelines.
Nursing Insights
- Counsel women with preexisting diabetes about the critical importance of preconception A1c optimization and early first-trimester glycemic control to reduce congenital anomaly risk.
- Facilitate early referral for high-resolution fetal anatomic ultrasound and maternal–fetal medicine consultation when pregestational diabetes or early hyperglycemia is present.
1.2.2 Macrosomia
- Definition and mechanism
- Fetal macrosomia is often defined as birth weight >4,000 g or >4,500 g depending on context; large-for-gestational-age (LGA) refers to birth weight >90th percentile for gestational age. Maternal hyperglycemia → increased transplacental glucose → fetal hyperglycemia → fetal pancreatic β-cell hypertrophy and hyperinsulinemia → insulin-mediated somatic growth and adipose deposition → macrosomia.

- Complications
- Increased risk of shoulder dystocia, brachial plexus injury, clavicle fracture, birth trauma, perineal lacerations, postpartum hemorrhage, and cesarean delivery. Long-term risks include childhood obesity and metabolic syndrome.
- Prediction and management
- Ultrasound estimation of fetal weight in the third trimester can suggest macrosomia but has limited accuracy. Clinical decisions regarding mode of delivery consider estimated fetal weight, maternal pelvis, prior obstetric history, and comorbidities. Tight maternal glycemic control, particularly limiting postprandial hyperglycemia, reduces macrosomia risk.
Nursing Insights
- Anticipate shoulder dystocia in labor for macrosomic infants: prepare necessary equipment (e.g., neonatal resuscitation, shoulder dystocia pack), ensure team readiness, and document maneuvers if dystocia occurs.
- Educate diabetic pregnant patients on the role of postprandial glucose control in preventing excess fetal growth; reinforce SMBG and MNT adherence.
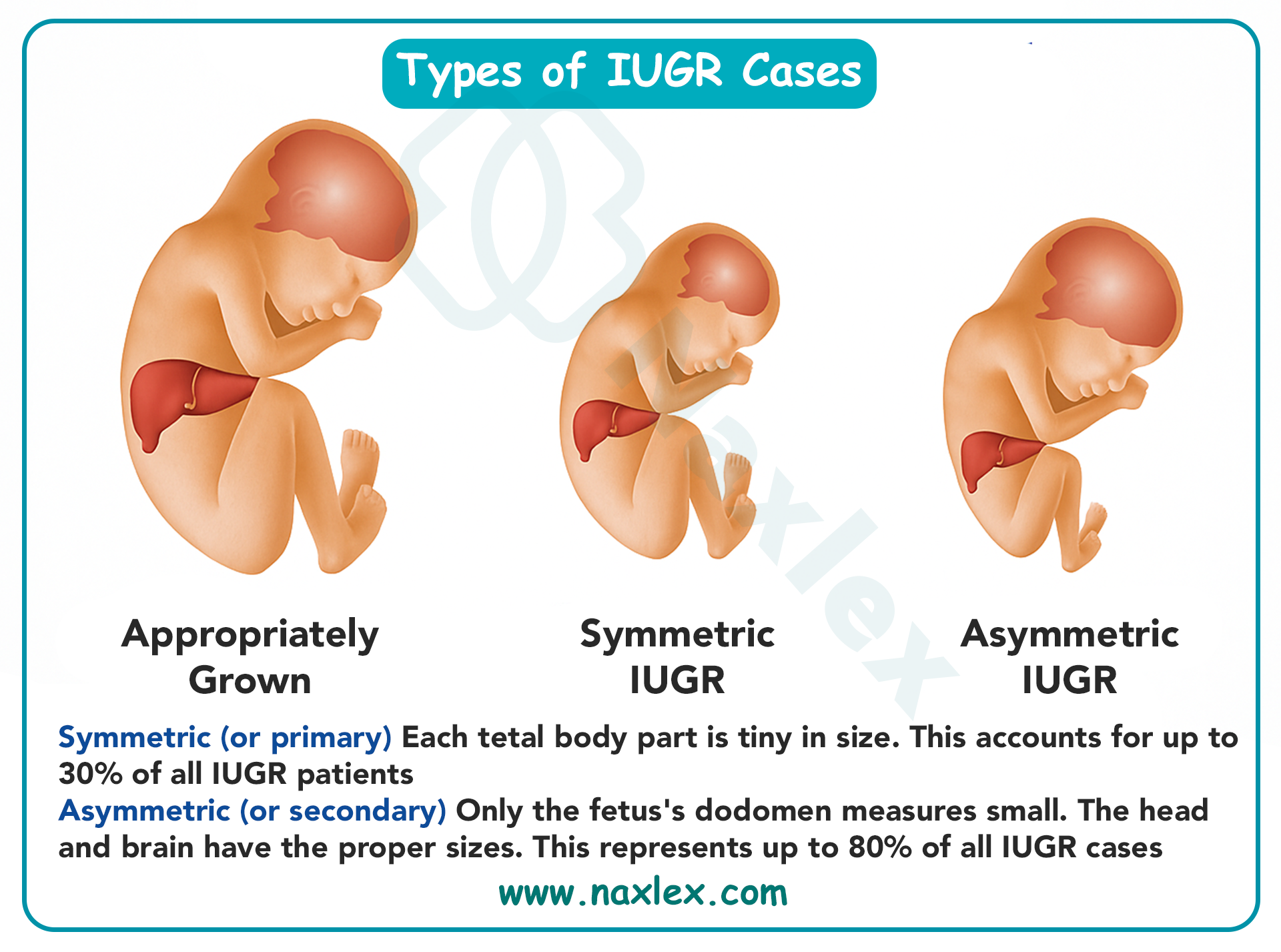
1.2.3 Intrauterine Growth Restriction (IUGR)
- Etiology in diabetic pregnancies
- IUGR may occur particularly in women with long-standing pregestational diabetes complicated by vascular disease (placental insufficiency due to diabetic vasculopathy), maternal hypertension, or nephropathy. IUGR in diabetes is thus usually associated with maternal vascular disease, unlike macrosomia which is associated with maternal hyperglycemia without significant vascular compromise.
- Clinical significance
- IUGR increases risks of oligohydramnios, stillbirth, perinatal morbidity, and long-term neurodevelopmental sequelae. Management focuses on close fetal surveillance and timely delivery when intrauterine environment is unsafe.
Nursing Insights
- Identify patients with microvascular disease (retinopathy, nephropathy) as higher risk for IUGR; schedule serial growth ultrasounds and Doppler studies as indicated.
- Educate such patients that optimal blood pressure and glycemic control reduce placental insufficiency progression and that antenatal surveillance is essential.
1.2.4 Respiratory Distress Syndrome (RDS)
- Mechanism
- Fetal hyperinsulinemia antagonizes cortisol-stimulated surfactant production and type II pneumocyte maturation, delaying lung maturity even when the fetus is at or near term. This biochemical interference increases the risk of RDS in infants of diabetic mothers (IDMs).
- Clinical presentation and risk factors
- Tachypnea, nasal flaring, retractions, grunting, hypoxemia soon after birth. Risk is greater with poor maternal glycemic control, prematurity, and fetal hyperinsulinemia.
- Prevention and management
- Optimize maternal glycemic control antenatally. For preterm deliveries or high RDS risk, antenatal corticosteroids may be administered according to obstetric guidelines (weigh benefits vs potential hyperglycemic effects). Neonatal management includes CPAP, supplemental oxygen, surfactant administration as indicated, and NICU support.
Nursing Insights
- Anticipate possible respiratory support for neonates of diabetic mothers even if delivery occurs at term; ensure neonatal team present at delivery and prepare equipment for immediate respiratory stabilization.
- Monitor neonate closely in the immediate postnatal period for respiratory distress signs and coordinate early blood glucose checks due to concurrent risk of hypoglycemia.
1.2.5 Neonatal Hypoglycemia
- Pathophysiology
- After delivery, the neonate’s continuous maternal glucose supply ceases abruptly while neonatal hyperinsulinemia (from in utero exposure to maternal hyperglycemia) persists, causing rapid decline in neonatal blood glucose and hypoglycemia. Risk is higher when maternal hyperglycemia is poorly controlled in late pregnancy or when infants are macrosomic.
- Clinical features
- Jitteriness, lethargy, poor feeding, apnea, temperature instability, seizures in severe cases. Neonatal hypoglycemia can lead to neuronal injury if severe and prolonged.
- Screening and management
- Early feeding (breast or formula) within 30–60 minutes of birth is recommended for infants at risk; frequent glucose monitoring per protocol (e.g., within 30–60 minutes of birth, then at 2–4 hours and before feeds as needed). Thresholds for intervention vary by institution (common action thresholds: <40–45 mg/dL in first 24 hours), and management includes enteral feeding, oral glucose gel, and intravenous dextrose (e.g., D10W bolus followed by infusion) for refractory or severe hypoglycemia.
Nursing Insights
- Implement early and proactive glucose monitoring for infants of diabetic mothers: ensure first glucose check within 30–60 minutes after birth and before next feed. Document timing of feeds and glucose values precisely.
- Educate parents prenatally about risk of neonatal hypoglycemia, the importance of early feeding, and possible need for NICU observation if hypoglycemia occurs.
- For symptomatic neonates or persistent low glucose, prepare to initiate IV glucose therapy and coordinate with neonatal team for further stabilization and neuroprotective measures.
Table — Maternal vs Fetal/Neonatal Complications (Concise Comparison)
|
Maternal Complications |
Mechanism / Clinical Notes |
Fetal/Neonatal Complications |
Mechanism / Clinical Notes |
|
Diabetic ketoacidosis (DKA) |
Insulin deficiency → ketogenesis; precipitated by infection, vomiting |
Congenital anomalies |
Early hyperglycemia → teratogenesis (cardiac, neural tube) |
|
Preeclampsia |
Endothelial dysfunction, microvascular disease |
Macrosomia/LGA |
Fetal hyperinsulinemia → adipogenesis |
|
Polyhydramnios |
Fetal osmotic diuresis from hyperglycemia |
IUGR |
Maternal vascular disease → placental insufficiency |
|
Infection (UTI, candidiasis) |
Hyperglycemia impairs immunity |
Respiratory distress syndrome (RDS) |
Fetal hyperinsulinemia delays surfactant synthesis |
|
— |
— |
Neonatal hypoglycemia |
Abrupt loss of maternal glucose + persistent fetal insulin |
Management Of Diabetes In Pregnancy
Comprehensive management of diabetes in pregnancy integrates preconception optimization, individualized medical nutrition therapy, exercise, vigilant glucose monitoring, safe pharmacotherapy when required, and multidisciplinary peripartum and postpartum planning. The goal is to maintain maternal euglycemia within pregnancy-specific targets to minimize maternal and fetal complications while preserving maternal safety.
1.1 Preconception Counseling And Glycemic Control
- Purpose and rationale:
- Preconception counseling reduces the risk of congenital anomalies, spontaneous abortion, and other adverse outcomes by achieving stable glycemic control during organogenesis (first 8–10 weeks).
- Counseling addresses medication safety, optimization of chronic comorbidities (hypertension, renal disease, retinopathy), immunizations, weight optimization, and psychosocial readiness.
- Key elements of preconception management:
- Document and review recent A1c (goal individualized; many programs target ≤7% if achievable without significant hypoglycemia; tighter targets such as <6.5% may be considered in selected patients with close monitoring).
- Review and adjust medications: discontinue teratogenic agents (e.g., statins, certain ACE inhibitors) and arrange transition to pregnancy-safe alternatives; plan insulin initiation or adjustment as needed.
- Optimize blood pressure with pregnancy-safe antihypertensives if indicated (coordinate with obstetric/primary care).
- Screen for and document baseline microvascular complications (ophthalmology for retinopathy, urine albumin/creatinine and serum creatinine for nephropathy).
- Provide individualized family-planning counseling and folic acid supplementation (higher-dose folic acid for women with pregestational diabetes or prior neural tube defect).
Nursing Insights
- Obtain and record the last A1c value in the chart and counsel the woman on target ranges and risks of elevated A1c during early pregnancy; schedule follow-up visits to titrate therapy preconception.
- Review all current medications and provide a clear written plan for which drugs to stop and which to continue; confirm understanding and document patient acknowledgement.
- Facilitate referrals (endocrinology, MFM, ophthalmology) before conception; proactively schedule these so the patient completes evaluations prior to pregnancy.
1.2 Medical Nutrition Therapy (MNT)
- Principles and goals:
- MNT aims to achieve euglycemia, appropriate gestational weight gain, and adequate fetal nutrition. It individualizes caloric needs based on pre-pregnancy BMI while focusing on macronutrient distribution that prevents large postprandial glycemic excursions.
- Caloric needs and distribution:
- Energy requirements should be individualized:
- Underweight (BMI <18.5): modest caloric increase above baseline.
- Normal weight (BMI 18.5–24.9): additional ~300 kcal/day during 2nd and 3rd trimesters is often recommended.
- Overweight/obese (BMI ≥25): restrict excessive caloric excess; individualized calorie prescription aiming for appropriate gain per IOM guidelines.
- Macronutrient distribution (example evidence-based framework):
- Carbohydrates: ~40–50% of total daily calories with emphasis on complex carbohydrates and fiber.
- Protein: 20–25% of calories (sufficient to support fetal growth).
- Fat: 25–35% of calories emphasizing unsaturated fats and limiting saturated/trans fats.
- Meal pattern: 3 balanced meals + 2–3 snacks (including bedtime snack if needed) to avoid fasting hypoglycemia and reduce postprandial peaks.
- Energy requirements should be individualized:
- Glycemic carbohydrate management:
- Emphasize low glycemic index carbohydrates, high fiber, and even distribution of carbohydrate across meals rather than large boluses.
- Avoid sugar-sweetened beverages and high-simple-sugar intake. Encourage portion control and carbohydrate counting for patients on insulin.
- Micronutrients and other considerations:
- Ensure adequate folate, iron, calcium, vitamin D, and other prenatal micronutrients per standard prenatal guidelines.
- Tailor MNT to cultural food preferences and socioeconomic realities.
Table — Example Daily Meal Distribution (Illustrative)
|
Meal |
Carbohydrate Strategy |
Notes |
|
Breakfast |
Moderate carbohydrate bolus with protein/fat to slow absorption |
Avoid high-sugar cereals; choose whole grains |
|
Midmorning snack |
Small carbohydrate + protein |
Prevents early hypoglycemia |
|
Lunch |
Balanced carbohydrate + protein + vegetables |
Emphasize complex carbs |
|
Afternoon snack |
Similar to midmorning |
Useful for glycemic stabilization |
|
Dinner |
Balanced with attention to evening postprandial levels |
Monitor bedtime glucose |
|
Bedtime snack (if needed) |
Protein + small carbohydrate |
Prevents nocturnal hypoglycemia |
Nursing Insights
- Provide concrete meal examples and portion visuals rather than abstract percentages; e.g., "1 slice whole-grain bread or 1/2 cup cooked rice = ~15 g carbohydrate."
- Teach carbohydrate counting basics and how to adjust insulin (if on insulin) relative to carbohydrate intake.
- Reinforce that MNT is medical treatment: document nutrition goals in the plan of care and coordinate referral to a registered dietitian specializing in diabetes and pregnancy.
1.3 Physical Activity And Exercise Recommendations
- Rationale:
- Exercise increases insulin-mediated glucose uptake in skeletal muscle, improves insulin sensitivity, supports weight management, and reduces GDM risk/severity.
- Recommended activity:
- For uncomplicated pregnancies, advise moderate-intensity aerobic activity such as brisk walking, swimming, or stationary cycling for ≥150 minutes/week (e.g., 30 minutes on most days), unless contraindicated.
- Strength training and pelvic floor exercises may be included with appropriate supervision. Avoid high-impact contact sports or activities with high fall risk.
- Precautions:
- Contraindications include maternal cardiac/pulmonary disease, premature labor risk, uncontrolled preeclampsia, or other obstetric restrictions. Screen for contraindications before recommending exercise.
- Monitor for symptoms of hypoglycemia during/after exercise in women on insulin; advise a small carbohydrate snack if glucose trending low.
Nursing Insights
- Provide prescribed, written exercise plans individualized to fitness level and cultural context; document exercise counseling and patient acceptance.
- Teach SMBG actions around exercise: check glucose before, during (if prolonged), and after exercise; adjust carbohydrate intake or insulin per individualized plan.
1.4 Pharmacological Management
Pharmacologic therapy is indicated when MNT and exercise do not achieve glycemic targets. Insulin remains the preferred pharmacotherapy for pregnancy due to its efficacy and lack of placental transfer; certain oral agents are used selectively with informed counseling.
1.4.1 Insulin Therapy
- Rationale and advantages:
- Insulin does not cross the placenta, allows precise titration (basal and bolus), and is effective at achieving euglycemia; therefore it is the gold standard in pregnancy when pharmacologic therapy is required.
- Types of insulin and typical roles:
- Rapid-acting analogs: insulin lispro and aspart — used for premeal/bolus control due to rapid onset and shorter duration.
- Short-acting regular insulin: alternative for prandial coverage, but slower onset and longer peak than rapid analogs.
- Intermediate-acting: NPH — traditionally used as basal coverage in split-mix regimens.
- Long-acting analogs: detemir and glargine — used as basal insulin in some patients; evidence supports safety and efficacy but practice varies by institution.
- Insulin pumps (CSII): appropriate for motivated, experienced patients with Type 1 diabetes; requires specialized support.
- Regimen strategies:
- Basal-bolus (preferred): long-acting basal insulin + rapid-acting bolus insulin with meals to mimic physiologic insulin.
- Split-mixed: premixed insulin preparations 2–3 times daily may be used in some settings but allow less flexibility.
- Titration principles: adjust based on SMBG results, focusing on fasting and postprandial targets; increase basal insulin for elevated fasting glucose, increase bolus insulin for postprandial hyperglycemia.
- Glycemic targets commonly used in pregnancy: (document which institutional targets are used)
- Fasting (preprandial) ≤95 mg/dL.
- 1-hour postprandial ≤140 mg/dL or 2-hour postprandial ≤120 mg/dL (use one convention consistently per institution).
- Individualize targets for patients at risk of hypoglycemia.
- Practical dosing considerations:
- Insulin requirements typically decrease in early pregnancy, then rise in the 2nd and 3rd trimesters (may double/triple by late pregnancy in some patients).
- Monitor for and manage hypoglycemia, especially nocturnal episodes; provide sick-day insulin adjustment education.
- During labor, IV insulin infusion protocols are commonly used to maintain intrapartum euglycemia (see Section 12.6).
Nursing Insights
- Teach patients injection technique, site rotation, storage, and hypoglycemia recognition/treatment; assess competency with return demonstration.
- Maintain clear orders for insulin adjustment rules: e.g., if fasting glucose >95 on 2 consecutive days, increase basal insulin by X% or Y units (institution-specific). Document and follow protocols rather than ad hoc changes.
- For patients on insulin pumps, coordinate with endocrinology for pump management during labor and anesthesia; ensure backup subcutaneous or IV insulin orders are available.
1.4.2 Oral Hypoglycemics (Metformin, Glyburide)
- Metformin:
- Mechanism: decreases hepatic gluconeogenesis and improves peripheral insulin sensitivity.
- Placental transfer: metformin crosses the placenta; long-term effects remain under investigation though many studies support its relative safety and efficacy in GDM and in women with T2DM or PCOS.
- Clinical use: used as monotherapy or adjunct in selected women, particularly where insulin access is limited, or to reduce maternal weight gain; used with counseling about placental transfer and potential need for supplemental insulin if glycemic targets are not met.
- Glyburide (glibenclamide):
- Mechanism: sulfonylurea that stimulates insulin secretion.
- Placental transfer: older data suggested minimal placental transfer, but more recent studies show measurable transfer; Glyburide may increase fetal insulin and risk of neonatal hypoglycemia in some settings.
- Clinical use: used in some centers for GDM when patients decline insulin, with awareness of variable efficacy and neonatal considerations.
- Clinical considerations and caveats:
- Insulin remains the preferred first-line pharmacotherapy for most pregnant patients requiring medication due to its established safety profile.
- If oral agents are used, counsel the patient thoroughly about risks/benefits, monitor closely, and be prepared to escalate to insulin if glycemic targets are not achieved.
Nursing Insights
- When oral agents are used, ensure informed consent documentation and provide clear instructions regarding SMBG frequency and indications for switching to insulin.
- Monitor neonates for hypoglycemia more vigilantly when maternal oral hypoglycemics were used in late pregnancy; notify neonatal team of maternal medications.
1.5 Monitoring Blood Glucose Levels
- Self-monitoring of blood glucose (SMBG):
- Frequency: typical SMBG schedules include fasting and 1- or 2-hour postprandial checks after each meal (total 4 checks/day) for many women with GDM; women with preexisting diabetes or on insulin may perform more frequent checks (preprandial, 1-2 hour postprandial, bedtime, and occasionally overnight).
- Targets: fasting ≤95 mg/dL, 1-hour postprandial ≤140 mg/dL or 2-hour postprandial ≤120 mg/dL (adopt institutional standard).
- Documentation: patients should record values, meal content, insulin doses, and symptoms for provider review.
- Glycated hemoglobin (A1c):
- Use for preconception and early pregnancy assessment; A1c is less useful for tight day-to-day titration in pregnancy but provides long-term glycemic indicator. Interpret A1c with knowledge of physiologic changes in pregnancy and potential confounders (anemia, hemoglobinopathy).
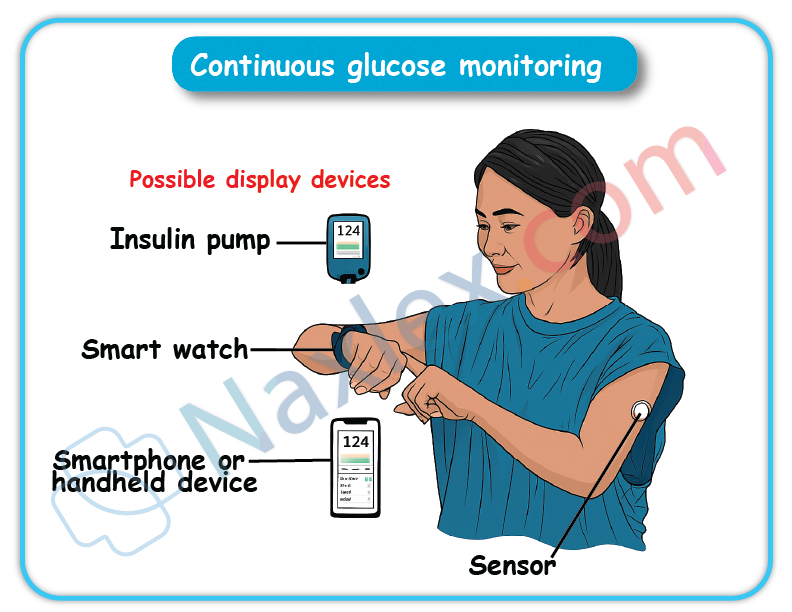
- Continuous glucose monitoring (CGM):
- CGM may be used increasingly in pregnant women with Type 1 diabetes and selected high-risk patients to improve time-in-range and reduce hypoglycemia; CGM can guide insulin titration and detect nocturnal hypoglycemia. Institutional policies on CGM use vary.
- Point-of-care meter considerations:
- Ensure meter accuracy and appropriate calibration; provide education on proper technique (handwashing, correct sample volume, strip storage). Confirm that meters used at bedside and by patients are validated and that staff/documentation matches device readings.
Nursing Insights
- Teach patients how to respond to out-of-range SMBG values with explicit action plans (when to adjust insulin per sliding rules, when to call provider, when to seek emergency care).
- Emphasize trend interpretation: advise patients and clinicians to make insulin adjustments based on consistent patterns rather than single isolated readings.
- For hospitalized patients, implement clear glucose monitoring schedules and ensure hourly or more frequent checks if on IV insulin infusions, per protocol.
1.6 Nursing Management During Labor And Delivery
- Goals during labor:
- Maintain maternal blood glucose in a euglycemic range to minimize neonatal hypoglycemia risk while avoiding maternal hypoglycemia. Prevent large maternal-to-fetal glucose fluctuations. Facilitate safe anesthesia and surgical planning if cesarean delivery is required.
- Common intrapartum protocol elements:
- Frequent glucose monitoring (e.g., hourly) during active labor.
- For women on insulin: transition to an IV insulin infusion (regular insulin) with concomitant dextrose-containing fluids as needed to maintain target glucose, or continue subcutaneous regimens for short labors per institutional protocol.
- Typical intrapartum glucose target frequently used: 70–110 mg/dL (institution-dependent). Avoid glucose >110–140 mg/dL to reduce fetal hyperglycemia and subsequent neonatal hypoglycemia.
- For women not on insulin with well-controlled GDM, some centers monitor and treat only if glucose exceeds threshold; protocols vary.
- Perioperative considerations for cesarean delivery:
- Coordinate timing of last subcutaneous insulin dose relative to anesthesia/surgery; often switch to IV insulin infusion perioperatively to maintain tighter control and permit rapid adjustments.
- Monitor fluid balance and electrolytes; be aware of corticosteroid use (for fetal lung maturity) that will acutely raise maternal glucose.
- Neonatal preparation and communication:
- Notify neonatal/pediatric team before delivery of infants of diabetic mothers; ensure plan for early feeding, glucose monitoring, and possible NICU support if needed.
Nursing Insights
- Ensure clear orders for intrapartum insulin protocols and dextrose administration; document hourly glucose values and insulin rates meticulously.
- Prepare for potential neonatal hypoglycemia: have glucose gel, formula, or IV dextrose available and ensure neonatal team presence for high-risk deliveries.
- Educate laboring patients about the rationale for IV lines, frequent fingersticks, and possible temporary changes to their usual insulin regimen.
1.7 Postpartum Management And Follow-Up
- Immediate postpartum physiologic changes:
- After placental delivery, insulin resistance declines rapidly; insulin requirements drop precipitously in insulin-treated women. Risk for hypoglycemia increases if pre-pregnancy insulin dosing is continued unchanged.
- Immediate postpartum tasks:
- For mothers on insulin, reduce insulin dosage significantly (commonly ~20–50% reduction depending on pre-delivery requirements and breastfeeding intentions) and monitor glucose closely for the first 24–72 hours. Use inpatient glucose checks to guide dosing.
- For women who had GDM but were not previously on medications, frequent glucose monitoring in immediate postpartum is recommended to confirm euglycemia prior to discharge. Many will not require pharmacotherapy but need postpartum screening.
- Breastfeeding considerations:
- Breastfeeding improves maternal glucose metabolism and reduces postpartum weight; encourage and support lactation. Adjust insulin dosing as breastfeeding can increase insulin sensitivity and lower glucose; monitor to avoid hypoglycemia.
- Postpartum diabetes screening:
- Perform a 75-g 2-hour OGTT at 6–12 weeks postpartum to detect persistent diabetes or impaired glucose tolerance (see Section 8.5). If OGTT abnormal, arrange appropriate long-term care and discuss prevention strategies.
- If postpartum screening is normal, counsel on lifestyle modification and schedule periodic glucose screening (at least every 1–3 years, individualized).
- Long-term follow-up and prevention:
- Provide education on lifestyle interventions, weight reduction, and, when appropriate, consider referral to diabetes prevention programs. Discuss contraception and planning for subsequent pregnancies with glycemic optimization.
Nursing Insights
- Before discharge, provide explicit written and verbal instructions for glucose monitoring at home, signs of hypoglycemia, insulin adjustments (if applicable), and timing of postpartum OGTT. Schedule the 6–12 week OGTT appointment and remind the patient to attend.
- Coordinate handoff to primary care: send discharge summary documenting antepartum glycemic control, medications used in pregnancy, and recommendations for postpartum screening and follow-up.
- Emphasize breastfeeding benefits and provide practical lactation resources; educate on how breastfeeding may change medication needs and blood glucose patterns.
Summary Table — Management Components and Nursing Actions
|
Management Component |
Core Actions |
Nursing Responsibilities |
|
Preconception care |
A1c optimization, med review, referrals |
Document A1c, med changes, arrange referrals |
|
MNT |
Individualized calories, carb distribution |
Provide meal plans, RD referral, education |
|
Exercise |
Moderate activity 150 min/week |
Prescribe safe exercise, counsel on SMBG with exercise |
|
Insulin therapy |
Basal-bolus preferred, titration |
Teach injection technique, monitor SMBG, adjust doses per protocol |
|
Oral agents |
Metformin/glyburide selective use |
Counsel on risks/benefits, monitor closely |
|
Monitoring |
SMBG, A1c, CGM as indicated |
Teach SMBG, ensure documentation, trend-based adjustments |
|
Labor |
IV insulin protocols, hourly glucose |
Implement protocol, document, coordinate neonatal team |
|
Postpartum |
Reduce insulin needs, OGTT 6–12 wks |
Adjust dosing, schedule OGTT, provide discharge education |
Fetal Surveillance And Monitoring In Gdm
Effective fetal surveillance in pregnancies complicated by gestational diabetes mellitus (GDM) aims to identify fetal compromise early, guide timing of delivery, and reduce perinatal morbidity and mortality. Surveillance strategies integrate physiologic fetal testing (cardiotocography), biophysical assessment, ultrasound-based amniotic fluid assessment, and growth monitoring with Doppler evaluation when indicated. Frequency and modality are individualized based on glycemic control, pharmacologic therapy (insulin use), presence of comorbidities (preeclampsia, fetal growth abnormalities), and gestational age.
1.1 Nonstress Test (NST)
- Definition and purpose
- The nonstress test (NST) is a noninvasive antepartum fetal surveillance tool that records fetal heart rate (FHR) patterns in response to spontaneous fetal activity. The NST assesses fetal autonomic function and oxygenation indirectly by observing accelerations in FHR and baseline variability.
- Physiologic basis
- Fetal heart rate accelerations are mediated by intact fetal autonomic nervous system response to movement and reflect adequate fetal oxygenation and metabolic reserve. Loss of accelerations or reduced variability may indicate fetal hypoxia, acidemia, or neurologic depression.
- Indications in GDM
- NST is used for antepartum surveillance in women with poorly controlled GDM, women requiring insulin, and those with additional risk factors (hypertension, decreased fetal movement, oligohydramnios, preterm labor). Many institutions initiate NSTs at 32–34 weeks for insulin-treated GDM; timing varies by local protocol and risk assessment.
- Test procedure
- Apply a tocodynamometer to monitor uterine activity and a Doppler transducer to record fetal heart rate. The patient is usually seated or semi-recumbent. Continuous monitoring for 20–40 minutes is standard; if fetal sleep suspected, extend monitoring or use vibroacoustic stimulation (VAS).
- Document fetal movements, maternal position, medications given, and duration of the test.
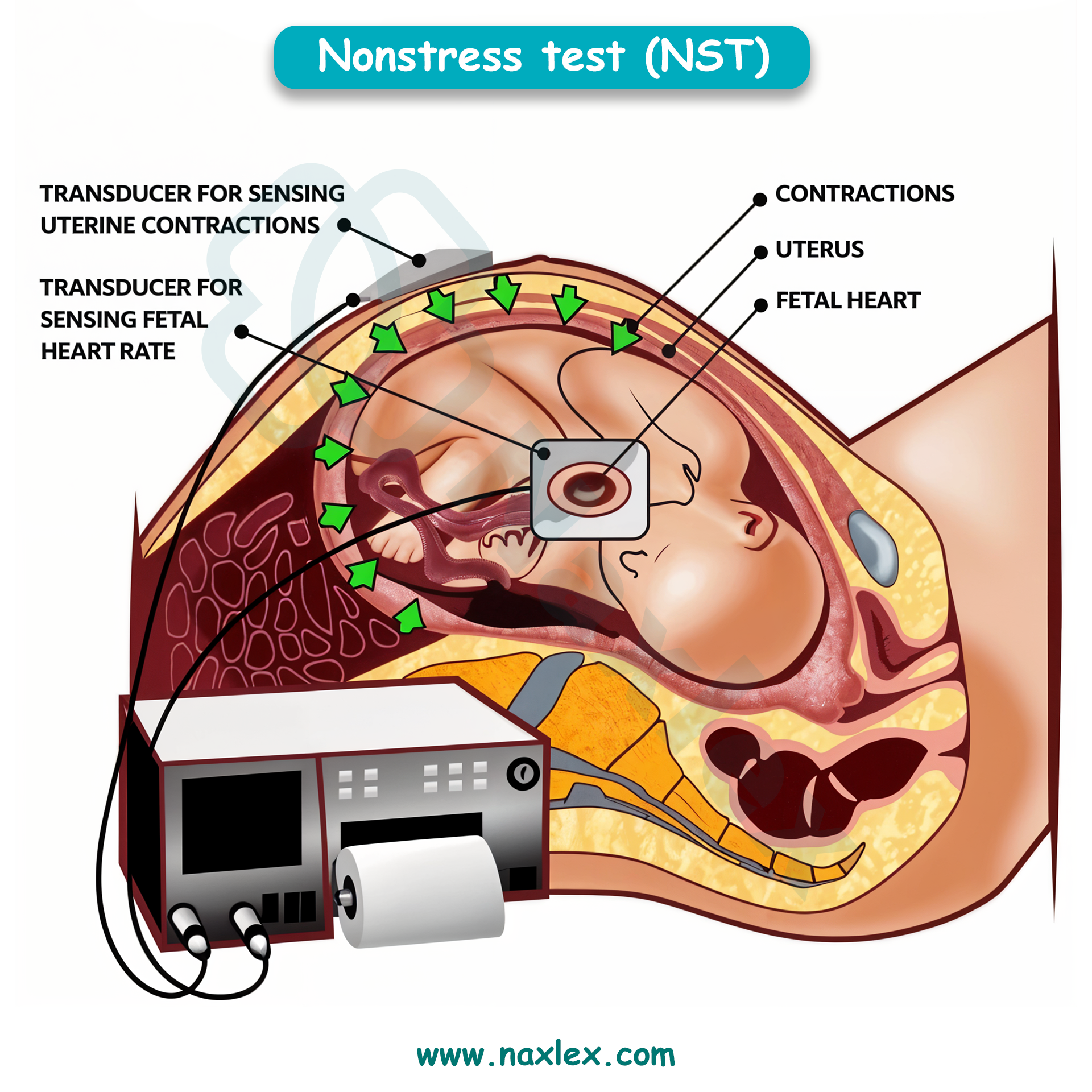
- Interpretation (standard criteria for a reactive NST)
- Reactive NST: ≥2 accelerations over baseline within 20 minutes.
- For fetuses ≥32 weeks: acceleration defined as ≥15 bpm above baseline lasting ≥15 seconds.
- For fetuses <32 weeks: acceleration defined as ≥10 bpm for ≥10 seconds.
- Nonreactive NST: fewer than required accelerations in a 40-minute period; requires further evaluation via vibroacoustic stimulation and/or biophysical profile (BPP).
- Reactive NST: ≥2 accelerations over baseline within 20 minutes.
- Vibroacoustic Stimulation (VAS)
- Used to arouse a sleeping fetus and provoke accelerations. Apply VAS for brief durations per protocol; if reactive, conclude test. If nonreactive despite VAS, proceed to BPP or extended monitoring.
- Limitations
- False positives (nonreactive despite a well fetus) due to fetal sleep cycles, maternal medications (e.g., opioids), or technician error. NST assesses only short-term fetal status and must be correlated with other testing and clinical context.
Nursing Insights
- Prepare the patient: advise her to eat a light snack prior to NST if allowed to reduce false nonreactive results due to low fetal activity; document timing of last meal.
- Accurately document test start and end times and maternal position; fetal movement events recorded by the patient should be correlated with tracings.
- If NST is nonreactive, promptly perform VAS per protocol and escalate to BPP or specialist consultation if still nonreactive—do not dismiss a nonreactive NST in a high-risk GDM pregnancy.
1.2 Biophysical Profile (BPP)
- Definition and components
- The biophysical profile integrates ultrasound assessment of fetal well-being with cardiotocography (NST) to produce a composite score reflecting fetal oxygenation and neurologic function. The standard BPP comprises 5 components, each scored 0 or 2:
- NST (reactive = 2)
- Fetal breathing movements (≥1 episode of rhythmic breathing ≥30 seconds within 30 minutes = 2)
- Gross fetal body movements (≥3 discrete body/limb movements in 30 minutes = 2)
- Fetal tone (≥1 episode of extension with return = 2)
- Amniotic fluid volume (single deepest pocket ≥2 cm or AFI >5 cm = 2)
- The biophysical profile integrates ultrasound assessment of fetal well-being with cardiotocography (NST) to produce a composite score reflecting fetal oxygenation and neurologic function. The standard BPP comprises 5 components, each scored 0 or 2:
- Scoring and interpretation
- Total score ranges 0–10.
- 8–10: reassuring (if AFI normal).
- 6: equivocal—may prompt extended monitoring, repeat testing within 24 hours, or delivery depending on gestational age and clinical context.
- ≤4: nonreassuring—often indicates potential fetal compromise; consider delivery if gestational age appropriate or intensive monitoring and further assessment.
- Total score ranges 0–10.
- Indications in GDM
- BPP is commonly used when NST is nonreactive, when fetal growth restriction or oligohydramnios is identified, or when there are additional risk factors (e.g., poor glycemic control, preeclampsia). In insulin-requiring GDM, BPP may be part of twice-weekly surveillance starting in the third trimester (institution-dependent).
- Practical procedure considerations
- Perform BPP in a calm environment; ensure maternal bladder is empty for accurate ultrasound. The full assessment may take 30–60 minutes. Document each component explicitly.
Nursing Insights
- Understand that BPP integrates multiple indicators of fetal well-being; a low BPP score in a GDM pregnancy should prompt immediate multidisciplinary discussion (obstetrician, MFM, neonatology).
- For equivocal scores (6), coordinate repeat testing and ensure maternal glucose is optimized prior to repeat testing because maternal hyperglycemia may transiently affect fetal activity patterns.
- Teach patients what BPP evaluates and the possible clinical pathways (repeat testing, induction, or cesarean) depending on results.
1.3 Amniotic Fluid Index (AFI)
- Definition and measurement
- AFI quantifies amniotic fluid using ultrasound by dividing the uterus into four quadrants and summing the deepest vertical pocket in each quadrant. An alternate method is the single deepest pocket (SDP) measurement. AFI and SDP are used to identify oligohydramnios and polyhydramnios.
- Thresholds and clinical interpretation
- AFI ≤5 cm: oligohydramnios (some centers use ≤5 cm).
- AFI 5.1–25 cm: generally normal (ranges vary).
- AFI >25 cm: polyhydramnios.
- Single deepest pocket: SDP <2 cm suggests oligohydramnios; SDP ≥8 cm suggests polyhydramnios. Institutional cutoffs may vary; clinicians should apply local guidelines.
- Relevance to GDM
- Polyhydramnios is more common in poorly controlled GDM due to fetal osmotic diuresis from hyperglycemia. Polyhydramnios increases risks for preterm labor, malpresentation, and postpartum hemorrhage. Oligohydramnios may occur with fetal growth restriction or ruptured membranes and requires different management.
- Surveillance and management
- Serial AFI monitoring is performed when abnormal volumes are detected or when maternal glycemic control is poor. Management depends on severity: mild polyhydramnios may be observed with tighter glycemic control; severe polyhydramnios may require therapeutic amnioreduction or preterm delivery if complications occur. Oligohydramnios often triggers closer surveillance and assessment of fetal status.
Nursing Insights
- When AFI abnormality is documented, ensure documentation includes method used (AFI vs SDP), numeric value, and scanner/operator. This precision guides clinical decisions.
- Counsel patients with polyhydramnios on signs of preterm labor and increased fetal movement surveillance; increase frequency of antenatal contact as indicated.
- Coordinate multidisciplinary care for severe polyhydramnios (MFM, neonatology) and prepare for potential interventions (amnioreduction, preterm delivery).
1.4 Ultrasound Evaluation Of Fetal Growth
- Biometric parameters and estimated fetal weight (EFW)
- Standard fetal biometric measures include:
- Biparietal diameter (BPD) — transverse skull diameter.
- Head circumference (HC) — skull circumference.
- Abdominal circumference (AC) — key parameter reflecting fetal adiposity and energy stores.
- Femur length (FL) — long bone measurement.
- Standard fetal biometric measures include:

- Algorithms (Hadlock formulas) combine these measures to calculate estimated fetal weight (EFW) and percentile for gestational age.
- Timing and frequency in GDM
- For pregnancies with GDM, growth ultrasound timing is individualized: many clinicians obtain an ultrasound in the third trimester (28–32 weeks) for baseline and then serial ultrasounds every 3–4 weeks if glycemic control is suboptimal, if fetal macrosomia is suspected, or if insulin therapy is required. Frequency increases for suspected macrosomia, polyhydramnios, or maternal vascular disease (to assess for IUGR).
- Interpretation and limitations
- AC is the most sensitive parameter for fetal overgrowth in diabetic pregnancies because fetal adipose tissue accumulation is prominent.
- Ultrasound EFW has ±10–15% error margin; accuracy decreases at extremes of fetal weight (macrosomia or severe growth restriction). Maternal obesity and operator variability further reduce precision.
- Large AC percentile or rapid abdominal growth trajectory is a predictor of macrosomia; management decisions (mode/timing of delivery) integrate ultrasound estimates with clinical context.
- Doppler studies
- Indicated when placental insufficiency or IUGR is suspected. Common assessments include:
- Umbilical artery Doppler: elevated resistance/reversed end-diastolic flow indicates severe placental insufficiency.
- Middle cerebral artery (MCA): increased diastolic flow (brain-sparing) suggests fetal hypoxia.
- Ductus venosus: abnormal flow patterns indicate severe compromise.
- In GDM with vascular disease, Doppler surveillance complements growth scans to detect placental insufficiency and guide timing of delivery.
- Indicated when placental insufficiency or IUGR is suspected. Common assessments include:
- Clinical application: delivery planning
- When ultrasound suggests macrosomia (EFW >4,000–4,500 g depending on clinical context), discuss delivery options with the patient, balancing cesarean risk vs vaginal delivery with shoulder dystocia risk. Consider maternal pelvis, prior obstetric history, and estimated accuracy limitations.
- For IUGR with abnormal Dopplers, expedited delivery may be indicated despite prematurity risk, after weighing fetal maturity and neonatal support availability.
Nursing Insights
- Document EFW and percentile trend rather than single value; successive growth percentiles and abdominal circumference velocity guide clinical decisions more effectively than a one-time estimate.
- Educate mothers on the inherent measurement error of ultrasound EFW and set realistic expectations—avoid overreliance on precise weight predictions; instead, focus on risk mitigation strategies (glycemic control, intrapartum planning).
- Ensure coordination of care when abnormal growth or Dopplers are found: schedule MFM consultation, fetal surveillance (NST/BPP), and neonatal team notification for complex delivery planning.
Patient Education And Health Promotion
- Patient education and health promotion in gestational diabetes mellitus encompass multifaceted strategies to empower pregnant individuals with knowledge and skills for self-management, emphasizing blood glucose monitoring techniques to detect deviations from targets like fasting <95 mg/dL and 1-hour postprandial <140 mg/dL, recognition and prompt management of hypoglycemia and hyperglycemia to prevent neuroglycopenic symptoms or ketoacidosis, the physiological benefits of breastfeeding in enhancing maternal insulin sensitivity through prolactin-mediated glucose utilization in mammary glands, and long-term lifestyle modifications including dietary adherence and physical activity to mitigate the 50-70% lifetime risk of progression to type 2 diabetes mellitus via improved beta-cell function and reduced visceral adiposity.
- Educational approaches utilize adult learning principles, incorporating motivational interviewing to address barriers like cultural beliefs or socioeconomic constraints, with reinforcement through written materials, digital apps for glucose tracking, and group sessions to foster peer support, ultimately reducing complication rates such as macrosomia by 40% and improving postpartum glucose tolerance.
- Health promotion extends to family involvement for sustained behavioral change, with emphasis on annual screening post-GDM to detect prediabetes early, defined as impaired fasting glucose 100-125 mg/dL, allowing interventions like metformin to delay diabetes onset by 30-40%.
Nursing Insights
- Nurses deliver patient education by assessing literacy levels at initial diagnosis, using teach-back methods to confirm understanding of glucose targets, ensuring patients verbalize fasting <95 mg/dL in real clinic interactions to enhance retention and compliance.
- In group education sessions, nurses facilitate discussions on cultural meal adaptations, demonstrating low-glycemic index food choices to maintain euglycemia without restricting traditions.
1.1 Patient Teaching On Blood Glucose Monitoring
- Patient teaching on blood glucose monitoring involves comprehensive instruction on self-monitoring of blood glucose using capillary sampling with glucometers to quantify plasma glucose levels, targeting fasting values <95 mg/dL, 1-hour postprandial <140 mg/dL, and 2-hour postprandial <120 mg/dL to avert fetal hyperinsulinemia and maternal ketoacidosis in gestational diabetes mellitus.
- Techniques include hand hygiene to prevent contamination, lancet device usage for fingerstick with alternating sites to minimize neuropathy, strip insertion into calibrated meters for accurate enzymatic readings, and logging results with meal correlations to identify patterns like dawn phenomenon from overnight hepatic gluconeogenesis.
- Continuous glucose monitoring systems provide interstitial glucose trends every 5 minutes via subcutaneous sensors, alerting for hypoglycemia <70 mg/dL or hyperglycemia >180 mg/dL, with calibration twice daily against capillary values for precision within 10-15%.
- Education covers meter maintenance, error troubleshooting like insufficient sample yielding "LO" readings, and integration with apps for data sharing with providers, reducing A1c by 0.5-1% through timely adjustments.
- Step-by-step procedure: Wash hands with soap, dry thoroughly to avoid dilution errors, prick fingertip laterally to reduce pain, apply drop to strip without smearing for capillary action, read result in 5-10 seconds.
- Common errors: Expired strips causing overestimation by 20-30 mg/dL, cold hands vasoconstricting flow necessitating warm compresses.
- Frequency: 4-7 times daily including fasting, pre/post-meals, bedtime, and 3 AM if nocturnal risks.
- Advanced features: Bluetooth syncing for trend graphs showing time in range >70% between 70-140 mg/dL, predictive alarms for impending lows.
Nursing Insights
- Nurses teach blood glucose monitoring by demonstrating lancet loading and strip handling, having patients return-demonstrate to ensure proficiency, correcting errors like over-milking finger that hemolyzes samples in real teaching sessions.
- For non-English speakers, nurses use pictorial guides and interpreters, verifying understanding through simulated logs to promote accurate self-management.
Nursing Insights
- In low-resource settings, nurses prioritize affordable meters, teaching strip conservation techniques like single-use per test to sustain monitoring adherence.
1.2 Recognition And Management Of Hypoglycemia And Hyperglycemia
- Recognition of hypoglycemia in gestational diabetes mellitus involves identifying neuroadrenergic symptoms like tremors, sweating, tachycardia from counterregulatory epinephrine release when glucose <70 mg/dL, progressing to neuroglycopenic manifestations such as confusion, seizures if <50 mg/dL due to cerebral glucose deprivation.
- Management adheres to the 15-15 rule: Ingestion of 15 g fast-acting carbohydrates like glucose tablets, rechecking in 15 minutes, repeating if persistent, followed by protein-carbohydrate snack to sustain levels via delayed absorption.
- Hyperglycemia recognition includes polydipsia, polyuria from osmotic diuresis when glucose >180 mg/dL, with ketonuria indicating starvation amid insulin deficiency, risking ketoacidosis if >240 mg/dL with pH <7.3.
- Management entails correction boluses of rapid insulin 1 unit/50 mg/dL above target, hydration to dilute glucose, and activity to enhance uptake, with urine ketone checks if >200 mg/dL to guide therapy.
- Hypoglycemia triggers: Overdosing insulin, skipped meals delaying gastric emptying in pregnancy, exercise depleting glycogen without adjustment.
- Severe cases: Intramuscular glucagon 1 mg for unconsciousness, activating hepatic glycogenolysis within 10 minutes.
- Prevention: Bedtime snacks with 15-30 g carbohydrates, avoiding alcohol inhibiting gluconeogenesis.
- Hyperglycemia causes: Infection elevating cytokines like interleukin-6 impairing insulin signaling, stress hormones cortisol promoting gluconeogenesis.
- Chronic effects: Accelerated fetal adipogenesis if sustained >140 mg/dL postprandially.
- Emergency: Hospitalization for DKA with fluids, insulin drip at 0.1 units/kg/hour.
|
Condition |
Glucose Level |
Symptoms |
Immediate Management |
|
Hypoglycemia |
<70 mg/dL |
Shakiness, hunger, irritability |
15 g carbs, recheck 15 min |
|
Severe Hypoglycemia |
<50 mg/dL |
Confusion, seizure |
Glucagon IM, medical help |
|
Hyperglycemia |
>180 mg/dL |
Thirst, frequent urination |
Insulin correction, hydrate |
|
DKA |
>240 mg/dL with ketones |
Nausea, abdominal pain |
IV fluids, insulin infusion |
Nursing Insights
- Nurses teach hypoglycemia recognition by listing symptoms in handouts, role-playing scenarios where patients identify shakiness post-exercise, instructing to treat immediately with juice in daily life.
- For hyperglycemia, nurses demonstrate ketone strip usage, advising ER visit if positive and glucose >250 mg/dL to prevent fetal distress.
Nursing Insights
- In elderly GDM patients, nurses adjust teaching for visual impairments, using large-print logs and voice-activated meters to ensure accurate monitoring.
1.3 Importance Of Breastfeeding
- Breastfeeding in postpartum GDM women confers metabolic benefits by improving insulin sensitivity through prolactin-stimulated glucose uptake in lactocytes for lactose synthesis, reducing blood glucose by 5-10 mg/dL and decreasing type 2 diabetes risk by 15-20% per year of lactation via enhanced beta-cell regeneration.
- Physiological mechanisms include oxytocin release contracting myoepithelial cells for milk ejection, suppressing hypothalamic-pituitary-adrenal axis to lower cortisol, and mobilizing visceral fat stores for energy, aiding weight loss of 0.5-1 kg/month postpartum.
- Neonatal advantages encompass reduced obesity risk in offspring by 25% from bioactive factors like leptin regulating appetite, and lower infection rates from immunoglobulins, crucial in hypoglycemic neonates of diabetic mothers.
- Recommendations: Exclusive breastfeeding for 6 months, with 10-12 feeds daily to establish supply, overcoming barriers like delayed lactogenesis in GDM from insulin resistance via frequent pumping.
- Maternal benefits: Decreased ovarian and breast cancer risks by 4-10% per year lactated, improved bone mineralization postpartum.
- Challenges: Nipple pain from improper latch, mastitis risk elevated 20% in diabetics from glycosylated milk fostering bacteria.
- Support: Lactation consultants for positioning, monitoring infant weight gain >20 g/day.
- Long-term: Cumulative lactation >12 months halves diabetes progression, via epigenetic modifications enhancing insulin gene expression.
Nursing Insights
- Nurses promote breastfeeding by assessing latch in hospital, teaching hand expression for colostrum to stabilize neonatal glucose in hypoglycemic infants.
- For working mothers, nurses advise pumping schedules every 3 hours, storing milk at 4°C for 4 days to maintain supply.
1.4 Long-Term Lifestyle Modifications To Prevent Type 2 Diabetes
- Long-term lifestyle modifications post-GDM focus on sustained weight management targeting BMI <25 kg/m² through caloric deficit of 500 kcal/day via portion control and increased fiber >25 g/day to enhance satiety via delayed gastric emptying, reducing type 2 diabetes incidence by 50-60% over 10 years.
- Physical activity ≥150 min/week moderate aerobic like cycling activates peroxisome proliferator-activated receptor gamma improving adiponectin levels for insulin sensitization, combined with resistance training building muscle mass for glucose disposal.
- Dietary patterns emphasize Mediterranean style with monounsaturated fats >30% calories from olive oil, limiting refined sugars <25 g/day to prevent beta-cell exhaustion from glucotoxicity.
- Annual screening with 75 g OGTT detects prediabetes early, allowing metformin if lifestyle insufficient, with smoking cessation and alcohol <14 units/week further mitigating cardiovascular risks elevated 2-fold post-GDM.
- Weight loss mechanisms: 7-10% reduction improves hepatic insulin sensitivity, decreasing gluconeogenesis via reduced intrahepatic triglycerides.
- Exercise benefits: High-intensity interval training alternates bursts elevating catecholamines for lipolysis.
- Dietary specifics: Glycemic load <80/day from whole grains, vegetables to minimize postprandial spikes.
- Behavioral strategies: Self-efficacy building via goal-setting, tracking apps for accountability, family involvement for sustainability.
Nursing Insights
- Nurses tailor modifications by setting SMART goals like 30 min walks 5 days/week, following up quarterly to adjust for barriers like fatigue.
- In ethnic groups, nurses incorporate cultural foods low in glycemic index, teaching label reading to avoid hidden sugars.
Summary
- Diabetes in pregnancy, including preexisting type 1/2 diabetes mellitus and gestational diabetes mellitus (GDM), involves altered glucose metabolism from hormonal insulin resistance, requiring vigilant management to prevent maternal complications like preeclampsia/DKA and fetal issues such as macrosomia/anomalies.
- Key concepts: Pathophysiology highlights placental hormones like hPL inducing resistance; types differentiate chronic preexisting from transient GDM; risk factors include obesity/ethnicity; screening uses OGTT at 24-28 weeks; complications encompass maternal hypertension/polyhydramnios and fetal IUGR/RDS/hypoglycemia.
- Management strategies: Preconception A1c <6.5%, MNT with 40-50% carbs, exercise 150 min/week, insulin/oral agents, SMBG 4-7x/day, intrapartum glucose control, postpartum OGTT.
- Fetal surveillance: NST reactive with accelerations, BPP score ≥8/10, AFI 5-25 cm, ultrasound for growth >90th/<10th percentile.
- Patient education: SMBG techniques, hypo/hyperglycemia management (15-15 rule/insulin correction), breastfeeding for sensitivity, long-term lifestyle to prevent type 2 DM via weight/activity.
