
Mobility
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Identify Variables that influence body alignment and mobility.
- Differentiate isotonic, isometric, and isokinetic exercise.
- Describe the effects of exercise and immobility on major body systems.
- Assess body alignment, mobility, and activity tolerance, using appropriate interview and physical assessment skills.
- Develop nursing diagnoses that correctly identify mobility problems amenable to nursing interventions.
- Utilize principles of body mechanics when appropriate.
- Use safe patient handling and movement techniques and equipment when positioning, moving, lifting, and ambulating patients.
- Plan, implement, and evaluate nursing care related to select nursing diagnoses involving mobility problems.
Introduction
A strong, well-developed body of research evidence supports the role of exercise in improving the health status of individuals with cardiovascular disease, pulmonary dysfunction, disabilities of aging, and depression.
A growing body of research supports the preventive and therapeutic effects of exercise for individuals with hypertension, osteoporosis, coronary heart disease, mental health disorders, diabetes, cancer, arthritis, chronic fatigue syndrome.
An activity-exercise pattern refers to a person’s routine of exercise, activity, leisure, and recreation. It includes:
- activities of daily living (ADLs) that require energy expenditure such as hygiene, dressing, cooking, shopping, eating, working, and home maintenance.
- the type, quality, and quantity of exercise, including sports.
Mobility, the ability to move freely, easily, rhythmically, and purposefully in the environment, is an essential part of living. People must move to protect themselves from trauma and to meet their basic needs
Movement
3.1 NORMAL MOVEMENT
Normal movement and stability are the result of an intact musculoskeletal system, an intact nervous system, and intact inner ear structures responsible for equilibrium.
It involves four basic elements: body alignment (posture), joint mobility, balance, and coordinated movement.
- Alignment and Posture
Proper body alignment and posture bring body parts into position in a manner that promotes optimal balance and maximal body function whether the client is standing, sitting, or lying down.
A person maintains balance as long as the line of gravity (an imaginary vertical line drawn through the body’s center of gravity) passes through the center of gravity (the point at which all of the body’s mass is centered) and the base of support (the foundation on which the body rests).
Abdominal and skeletal muscles function almost continuously, making tiny adjustments that enable an erect or seated posture despite the endless downward pull of gravity. The extensor muscles, often referred to as the antigravity muscles, carry the major load as they keep the body upright.
- Joint mobility:
The bones of the skeleton articulate at the joints, and most of the skeletal muscles attach to the two bones at the joint.
These muscles are categorized according to the type of joint movement they produce on contraction. Muscles are therefore called flexors, extensors, internal rotators, and the like.
The flexor muscles are stronger than the extensor muscles. Thus, when a person is inactive, the joints are pulled into a flexed (bent) position. If this tendency is not counteracted with exercise and position changes, the muscles permanently shorten, and the joint becomes fixed in a flexed position (contracture).
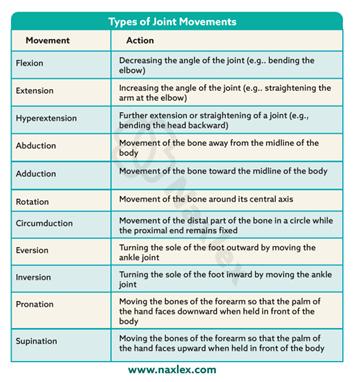
The range of motion (ROM) of a joint is the maximum movement that is possible for that joint. Joint range of motion varies from individual to individual and is determined by genetic makeup, developmental patterns, the presence or absence of disease, and the amount of physical activity in which the person normally engages.
- Balance:
The mechanisms involved in maintaining balance and posture are complex and involve informational inputs from the labyrinth (inner ear), from vision (vestibulo-ocular input), and from stretch receptors of muscles and tendons (vestibulospinal input).
Mechanisms of equilibrium (sense of balance) respond, frequently without our awareness, to various head movements.
Proprioception is the term used to describe awareness of posture, movement, and changes in equilibrium and the knowledge of position, weight, and resistance of objects in relation to the body.
- Coordinated movement:
Balanced, smooth, purposeful movement is the result of proper functioning of the cerebral cortex, cerebellum, and basal ganglia.
The cerebral cortex initiates voluntary motor activity, the cerebellum coordinates the motor activities of movement, and the basal ganglia maintain posture.
Factors Affecting Body Alignment and Activity
Body alignment, mobility, and daily activity are influenced by multiple factors: growth and development, nutrition, personal values/attitudes, external factors, and prescribed limitations.
1. Growth and Development
- Infants/Children: Movements initially reflexive - progress to controlled motor skills. Gross motor skills develop head-to-toe (head control - crawling - walking). Fine motor refinement (drawing, dressing, brushing teeth) occurs by preschool age. Immobility in children delays social/motor development.
- School-age (6–12 yrs): Motor skills refine further; PE and sports shape lifelong exercise patterns. Posture usually excellent.
- Adolescents: Growth spurts may cause postural issues (e.g., heavy bags, screen use). Habits may persist into adulthood.
- Adults (20–40 yrs): Few mobility issues except pregnancy, which alters balance. Moderate exercise is encouraged during pregnancy (with medical clearance). Benefits: prevents gestational diabetes, controls weight, reduces long-term obesity risk.
- Older Adults: Age-related changes: decreased muscle tone, bone density, flexibility, reaction time. Osteoporosis (common in women) - brittle bones, fractures, stooped posture, shuffling gait. Regular activity maintains strength, flexibility, bone health, reduces falls, obesity, diabetes, and improves mood.
2. Nutrition
Undernutrition: Weakness, fatigue, poor muscle development. Deficiencies: Vitamin D - bone deformities and Calcium & Vitamin D - osteoporosis risk.
Overnutrition (obesity): Alters posture, stresses joints, affects balance and movement.
3. Personal Values and Attitudes
Family influence shapes exercise habits. Sedentary lifestyle often passed on to children. Appearance, cultural roles, and location influence activity choices. Motivation can be enhanced through:
-
- Fun/social activities, music, goal-setting, progress tracking.
- Framing exercise as recreation, well-being, or self-care.
FIT model (Frequency, Intensity, Time) used for exercise prescription. Nurses should tailor exercise plans to client’s health, fitness, motivation, and safety.
4. External Factors
- Environment: Extreme heat/humidity - discourage activity. Safe, pleasant environments - encourage activity.
- Hydration: Short activity - 1–2 cups of water. Endurance events - hydration before, during, and after (water + sports drinks with sodium).
- Resources: Lack of money, facilities, or safe neighborhoods limits opportunities for activity.
- Technology: TV, computers, video games increase sedentary behavior (esp. in adolescents).
5. Prescribed Limitations
- Medical restrictions: Casts, splints, braces, traction limit movement to promote healing. Dyspnea - avoid exertion. Bed rest used for edema, pain relief, tissue repair, reducing oxygen needs.
- Types of bed rest vary: Strict confinement vs. bathroom privileges.
3.2 EXERCISE
People participate in exercise programs to decrease risk factors for chronic diseases and to increase their health and well-being.
Functional strength is another goal of exercise, and is defined as the ability of the body to perform work.
Activity tolerance is the type and amount of exercise or ADLs an individual is able to perform without experiencing adverse effects.
Types of exercise:
Exercise involves the active contraction and relaxation of muscles. Exercises can be classified according to the type of muscle contraction (isotonic, isometric, or isokinetic) and according to the source of energy (aerobic or anaerobic).
According to the type of muscle contraction:
- Isotonic (dynamic) exercises are those in which the muscle shortens to produce muscle contraction and active movement. Most physical conditioning exercises—running, walking, swimming, cycling.
Isotonic exercises increase muscle tone, mass, and strength and maintain joint flexibility and circulation. During isotonic exercise, both heart rate and cardiac output quicken to increase blood flow to all parts of the body.
- Isometric (static or setting) exercises are those in which muscle contraction occurs without moving the joint (muscle length does not change).
These exercises involve exerting pressure against a solid object and are useful for strengthening abdominal, gluteal, and quadriceps muscles used in ambulation; for maintaining strength in immobilized muscles in casts or traction; and for endurance training.
- Isokinetic (resistive) exercises involve muscle contraction or tension against resistance. During isokinetic exercises, the person tenses (isometric) against resistance. These exercises are used in physical conditioning and are often done to build up certain muscle groups.
According to the source of energy
- Aerobic exercise is activity during which the amount of oxygen taken into the body is greater than that used to perform the activity. Aerobic exercises use large muscle groups that move repetitively. Aerobic exercises improve cardiovascular conditioning and physical fitness.
- Anaerobic exercise involves activity in which the muscles cannot draw out enough oxygen from the bloodstream, and anaerobic pathways are used to provide additional energy for a short time. This type of exercise is used in endurance training for athletes such as weight lifting and sprinting.
Intensity of exercise can be measured in three ways:
1. Target heart rate. The goal is to work up to and sustain a target heart rate during exercise, based on the person’s age. To determine target heart rate, first calculate the person’s maximum heart rate by subtracting his or her current age in years from 220. Then obtain the target heart rate by taking 60% to 85% of the maximum. Because heart rates vary among individuals, the tests that follow are replacing this measure.
2. Talk test. This test is easier to implement and keeps most people at 60% of maximum heart rate or more. When exercising, the person should experience labored breathing, yet still be able to carry on a conversation.
3. Borg scale of perceived exertion: This scale measures “how difficult” the exercise feels to the person in terms of heart and lung exertion. The scale progresses from 1 to 20 with the following markers: 7 = very, very light; 9 = very light; 11 = fairly light; 13 = somewhat hard; 15 = hard; 17 = very hard; and 19 = very, very hard.
Nursing insights: Guidelines and Minimal Requirements for Physical Activity
FREQUENCY AND DURATION
- Aerobic: Cumulative 30 minutes or more daily (can be divided throughout the day) of “moderate intensity” movement as measured by talk test and perceived exertion scale.
- Stretching: Should be added onto that minimum requirement so that all parts of the body are stretched each day.
- Strength training: Should be added onto these minimum requirements so that all muscle groups are addressed at least three times a week, with a day of rest after training.
TYPE OF EXERCISE
- Aerobic: Elliptical exercisers, walking, biking, gardening, dancing, and swimming are recommended for all individuals including beginners and older adults. Activities that are more strenuous include jogging, running, Spinning, power yoga, bouncing, boxing, and jumping rope.
- Stretching: Yoga, Pilates, qigong, and many other flexibility programs are effective.
- Strength training: Resistance can be provided with weights, bands, balls, apparatus, and body weight.
SAFETY
- Stress the importance of balance and prevention of falls, proper clothing to ensure thermal safety, checking equipment for proper function, wearing a helmet and other protective gear, using reflective devices at night, and carrying identification and emergency information.
Benefits of Exercise
Regular exercise is essential for mental and physical health, supporting multiple body systems.
1. Musculoskeletal System
- Maintains/increases muscle size, tone, strength (hypertrophy with strenuous exercise).
- Improves efficiency of muscle contraction.
- Joints: exercise provides nourishment, increased flexibility, stability, ROM.
- Bones: weight-bearing exercise strengthens bones; prevents osteoporosis.
- Reduces weakness, frailty, depression, falls in older adults.
2. Cardiovascular System
- AHA: 150 min/week moderate OR 75 min/week vigorous exercise.
- Benefits:
- increased HR and contraction strength.
- increased cardiac output and circulation.
- Stress reduction.
- Aerobic exercises (walking, cycling, yoga) improve BP, HR variability, circulation, and lower stress.
3. Respiratory System
- Improves ventilation, gas exchange, oxygenation.
- Enhances toxin elimination and brain oxygenation - better problem solving, stability.
- Prevents pooling of secretions, reduces infection risk.
- Helps in management of COPD (walking, cycling, strength training).
- Yoga breathing aids asthma control.
4. Gastrointestinal System
- Improves appetite, GI tone, and peristalsis.
- Relieves constipation (rowing, swimming, walking, sit-ups).
- Helps in IBS and digestive disorders.
5. Metabolic/Endocrine System
- Increases metabolic rate (up to 20x during strenuous exercise).
- Continued increased metabolism after activity.
- Uses triglycerides and fatty acids - decreases cholesterol, triglycerides, HbA1C.
- Promotes weight loss and insulin sensitivity.
6. Urinary System
- increased blood flow - better waste excretion.
- Prevents urinary stasis, reducing UTI risk.
7. Immune System
- Exercise aids lymphatic circulation - improved pathogen destruction.
- Moderate exercise enhances immunity.
- Excessive strenuous exercise may temporarily Decreased immunity - need rest for recovery.
8. Psychoneurologic System
- Depression/stress can reduce activity - slumped posture, fatigue.
- Regular exercise:
- improves mood, decreases anxiety and stress.
- increases neurotransmitters (serotonin, norepinephrine), increases endorphins.
- Improves sleep quality.
- Excessive exercise sometimes linked to eating disorders.
9. Cognitive Function
- Improves decision-making, problem solving, planning, attention.
- Strengthens neuronal connections.
- Cross-lateral movements (e.g., Brain Gym) aid ADD/ADHD, learning, mood disorders.
10. Spiritual Health
- Yoga and meditative movement - improve mind–body–spirit balance.
- Promote relaxation response (RR) - decrease HR, BP, RR, stress.
- Techniques:
- Progressive muscle relaxation.
- Labyrinth walking or finger-tracing mandalas - induce calm, reduce insomnia.
3.3 EFFECTS OF IMMOBILITY
Immobility negatively impacts multiple body systems. The severity depends on duration of inactivity, health status, and sensory awareness. Early ambulation is key to preventing complications.
1. Musculoskeletal System
- Disuse osteoporosis - bone demineralization (risk of fractures).
- Disuse atrophy - muscle wasting, Decreased strength and function.
- Contractures - permanent muscle shortening, deformities (foot drop, wrist drop, hip rotation).
- Joint stiffness/pain - immobility of collagen tissue and calcium deposits in joints.
2. Cardiovascular System
- Diminished cardiac reserve - tachycardia with minimal exertion.
- Valsalva maneuver (breath-holding during straining) - Decreased venous return, possible arrhythmias.
- Orthostatic hypotension - dizziness, fainting, Increased HR on standing due to poor vasoconstriction reflex.
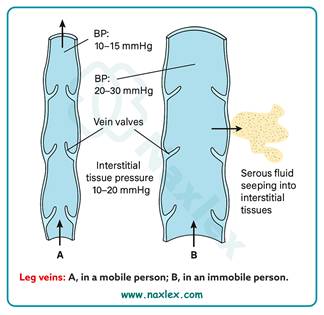
- Venous vasodilation/stasis - pooling of blood in legs, incompetent valves.
- Dependent edema - fluid accumulation in sacrum, heels, legs.
- Thrombus formation – DVT (deep venous thrombosis) risk, possible embolism (lungs, heart, brain).
3. Respiratory System
- Decreased lung expansion - shallow breathing, Decreased vital capacity.
- Pooling of secretions - risk of respiratory acidosis, infection.
- Atelectasis - collapse of alveoli from mucus blockages and Decreased surfactant.
- Hypostatic pneumonia - pooled secretions promote bacterial growth, serious infection risk.
4. Metabolic System
- Decreased Metabolic rate - reduced energy needs.
- Negative nitrogen balance - protein breakdown > synthesis, poor wound healing.
- Anorexia - decreased appetite, risk of malnutrition.
- Negative calcium balance - bone calcium loss due to lack of weight-bearing.
5. Urinary System
- Urinary stasis - incomplete emptying in supine position.
- Renal calculi - excess calcium in urine forms stones.
- Urinary retention - bladder distention, overflow incontinence.
- Urinary infections (UTIs) - stagnant urine supports bacterial growth, reflux may infect kidneys.
6. Gastrointestinal System
- Constipation/impaction - Decreased peristalsis, weak abdominal muscles, uncomfortable bedpan use.
- Straining (Valsalva) - Increased intra-abdominal pressure, risk to cardiovascular system.
7. Integumentary System
- Reduced skin turgor - skin atrophy, loss of elasticity.
- Skin breakdown/pressure ulcers - impaired circulation and nutrition supply to skin.
8. Psychoneurologic System
- Decreased Endorphins - poor mood regulation.
- Low self-esteem from dependency and loss of role.
- Emotional changes - apathy, withdrawal, regression, anger, aggression.
- Decreased Intellectual stimulation - poor concentration, problem-solving, decision-making.
- Time perception changes - altered awareness of intervals.
- Anxiety due to loss of control.
Nursing Management
4.1 ASSESSING
Assessment relative to a client’s activity and exercise should be routinely addressed and includes a nursing history and a physical examination of:
- body alignment
- gait
- appearance and movement of joints
- capabilities and limitations for movement
- muscle mass and strength
- activity tolerance
- problems related to immobility
- physical fitness.
NURSING HISTORY
An activity and exercise history is usually part of the comprehensive nursing history.
Daily activity level
• What activities do you carry out during a routine day?
• Are you able to carry out the following tasks independently?
- Eating
- Dressing and grooming
- Bathing d. Toileting
- Ambulating
- Using a wheelchair
- Transferring in and out of bed, bath, and car
- Cooking
- House cleaning
- Shopping
• Where problems exist in your ability to carry out such tasks:
- Would you rate yourself as partially or totally dependent?
- How is the task achieved (by family, friend, agency, or use of specialized equipment)?
Activity tolerance
• What types of activities make you tired?
• Do you ever experience dizziness, shortness of breath, marked increase in respiratory rate, or other problems following mild or moderate activity?
Exercise
• What type of exercise do you carry out to enhance your physical fitness?
• What is the frequency and length of this exercise session?
• Do you believe exercise is beneficial to your health? Explain.
Factors affecting mobility
• Environmental factors: Do stairs, lack of railings or other assistive devices, or an unsafe neighborhood impede your mobility or exercise regimen?
• Health problems: Do any of the following health problems affect your muscle strength or endurance: heart disease, lung disease, stroke, cancer, neuromuscular problems, musculoskeletal problems, visual or mental impairments, trauma, or pain?
• Financial factors: Are your finances adequate to obtain equipment or other aids that you require to enhance your mobility?
PHYSICAL EXAMINATION
Conduct the physical examination focusing on activity and exercise patterns
1. Body Alignment
Identify posture variations, learning needs, and factors causing poor posture.
Assessment:
- Inspect client standing from anterior, posterior, and lateral views.
- Normal findings:
- Shoulders and hips level
- Toes point forward
- Spine straight
- Abnormal findings:
- Slumped posture- neck flexed forward, abdomen protruding, pelvis thrust forward (lordosis), hyperextended knees - leads to fatigue and low back pain.
Contributing Factors: Fatigue, pain, compression fractures, muscle weakness, poor self-esteem.
2. Gait
Determine mobility and fall risk.
Normal Gait:
- Two phases: Stance (weight-bearing) and Swing (leg moves forward).
- Features:
- Chin level, gaze straight ahead
- Heel strikes ground before toe
- Feet dorsiflexed during swing phase
- Arms move opposite to legs
- Movement smooth, rhythmic, and coordinated
Normal pace:
- Adults: 70–100 steps/minute
- Older adults: ~40 steps/minute
Assess with/without assistive devices (e.g., cane, walker).
3. Appearance and Movement of Joints
Examine: Inspection, palpation, active/passive range of motion (ROM).
Assess for:
- Swelling, redness - inflammation/injury
- Deformities (bony enlargement, contractures)
- Symmetry of involvement and muscle development
- Tenderness or crepitation (crackling sound)
- Increased temperature (compare bilaterally)
- Degree of movement (use goniometer if indicated)
Precautions:
- Move joints smoothly, slowly, and rhythmically—never force.
4. Capabilities and Limitations for Movement
Assess for:
- Effects of illness or devices (IV lines, casts)
- Mental alertness, ability to follow directions
- Medication effects (narcotics, sedatives, antihistamines)
- Balance and coordination
- Orthostatic hypotension: Dizziness, BP drop, tachycardia on standing
- Pain (may need analgesic before movement)
- Vision (adequacy for safe ambulation)
Evaluate assistance needs for:
- Turning in bed
- Moving from supine - sitting or standing
- Rising from chair
- Maintaining balance and posture while walking or standing
5. Muscle Mass and Strength
Determine readiness for movement or ambulation and prevent injury.
Assess:
- Upper and lower extremity strength (important for using crutches/walkers)
- Compare muscle size and tone bilaterally
Nursing Consideration: Provide assistance as needed to prevent strain or falls.
6. Activity Tolerance
Determine client’s strength and endurance for daily activities.
Assess in clients who are:
- Cardiopulmonary compromised
- Immobilized long-term
- Experiencing muscle wasting, pain, fatigue, or depression
Monitor:
- Heart rate, respiratory rate, rhythm, blood pressure
- At four intervals:
- Before activity (baseline)
- During activity
- Immediately after
- 3 minutes post-activity (recovery)
Stop activity if:
- Facial pallor, dizziness, weakness
- Change in consciousness
- Marked increase in HR or RR
- Irregular rhythm
- Dyspnea or chest pain
- Diastolic BP change ≥ 10 mmHg
Normal recovery: HR returns to baseline within 5 minutes.
7. Problems Related to Immobility
Assessment Methods: Inspection, palpation, auscultation, lab results, body weight, fluid intake/output.
Importance:
- Establish baseline data early for comparison.
- Identify at-risk clients early to prevent complications.
At-Risk Clients:
- Poorly nourished
- Decreased pain/pressure sensation
- Cardiovascular, pulmonary, or neuromuscular issues
- Altered level of consciousness
Common Complications: Pressure injuries, contractures, DVT, pneumonia, constipation, urinary stasis.
4.2 DIAGNOSING
NANDA International includes the following nursing diagnostic labels for activity and exercise problems:
• Activity Intolerance: insufficient physiological or psychological energy to endure or complete required or desired daily activities. Wilkinson suggests specifying the level of endurance. Levels include:
Level I: Walks regular pace on level ground but becomes more short of breath than normal when climbing one or more flights of stairs.
Level II: Walks one city block or 500 feet on level ground or climbs one flight of stairs slowly without stopping.
Level III: Walks no more than 50 feet on level ground without stopping and is unable to climb one flight of stairs without stopping.
Level IV: Dyspnea and fatigue at rest.
• Risk for Activity Intolerance: vulnerable to experiencing insufficient physiological or psychological energy to endure or complete required or desired daily activities, which may compromise health.
• Impaired Physical Mobility: limitation in independent, purposeful physical movement of the body or of one or more extremities. More specific versions of this diagnosis are
- Impaired Bed Mobility
- Impaired Transfer Ability
- Impaired Walking Impaired
- Wheelchair Mobility
- Impaired Sitting
• Sedentary Lifestyle: reports a habit of life that is characterized by a low physical activity level.
• Risk for Disuse Syndrome: vulnerable to deterioration of body systems as the result of prescribed or unavoidable musculoskeletal inactivity, which may compromise health
Depending on the data obtained, problems with mobility often affect other areas of human functioning and indicate other diagnoses. In these instances, the mobility problem becomes the etiology. The etiology needs to be described more explicitly in terms such as reduced ROM, neuromuscular impairment or musculoskeletal impairment of upper and lower extremities, or joint pain. Examples in which Impaired Physical Mobility is the etiology follow:
- Fear (of falling)
- Ineffective Coping
- Situational Low Self-Esteem
- Powerlessness
- Risk for Falls.
When problems associated with prolonged immobility arise, many other diagnoses may be necessary. Examples include, but are not limited to, the following:
• Ineffective Airway Clearance if there is stasis of pulmonary secretions
• Risk for Infection if there is stasis of urinary or pulmonary secretions
• Risk for Injury if orthostatic hypotension is present
• Disturbed Sleep Pattern if there is a lack of daytime physical activity
• Risk for Situational Low Self-Esteem if there is functional impairment and/or role disturbance.
4.3 PLANNING
To promote safe mobility, maintain independence, and prevent complications of immobility through individualized nursing goals and interventions.
Nursing Outcomes Classification (NOC)
Helpful NOC labels for planning care include:
- Activity tolerance
- Ambulation
- Balance
- Body positioning
- Coordinated movement
- Endurance
- Fall prevention behavior
- Fatigue level
- Immobility consequences (physiological & psycho-cognitive)
- Joint movement
- Mobility
- Physical fitness
- Play participation
- Self-care
Nursing Responsibilities
- Positioning, transferring, and ambulating clients are usually independent nursing functions.
- Primary care practitioner prescribes activity restrictions or specific positions after surgery, anesthesia, or musculoskeletal/neurologic trauma.
- Every client must have a written activity order upon admission.
Nursing Considerations in Planning
- Identify clients needing assistance with body alignment or movement.
- Determine the degree of assistance required.
- Encourage maximum independence while ensuring safety.
- Provide guidance and education on proper body mechanics and safe movement.
Overall Client Goals
The client will:
- Demonstrate increased tolerance for physical activity.
- Have restored or improved ambulation and ability to perform ADLs.
- Remain free from injury related to falls or improper body mechanics.
- Show enhanced physical fitness.
- Remain free from complications associated with immobility.
Planning for Home Care
For clients discharged with mobility or activity problems:
Nurse should:
- Assess actual and potential health problems, strengths, and available resources.
- Conduct a Home Care Assessment to identify environmental and physical barriers.
- Develop a discharge plan addressing:
- Mobility limitations
- Required assistive devices
- Support systems
- Instructional needs for client and family (safe ambulation, transfers, exercises).
Teaching focus: Safe movement, prevention of falls, maintaining mobility, and proper body mechanics.
4.4 IMPLEMENTING
Nurses can initiate and apply a wide variety of exercise and activity interventions as needed to address a multitude of client concerns.
Nursing strategies to maintain or promote body alignment and mobility involve:
- positioning clients appropriately
- moving and turning clients in bed
- transferring clients
- providing ROM exercises
- ambulating clients with or without mechanical aids
- strategies to prevent the complications of immobility
Whenever positioning, moving, and ambulating clients, nurses must use proper body mechanics and assistive lifting/moving equipment to avoid musculoskeletal strain and injury.
Using Body Mechanics
Body mechanics is the term used to describe the efficient, coordinated, and safe use of the body to move objects and carry out the ADLs.
When a person moves, the center of gravity shifts continuously in the direction of the moving body parts. Balance depends on the interrelationship of the center of gravity, the line of gravity, and the base of support.
The closer the line of gravity is to the center of the base of support, the greater the person’s stability.
Conversely, the closer the line of gravity is to the edge of the base of support, the more precarious the balance. If the line of gravity falls outside the base of support, the person falls.
Body balance, therefore, can be greatly enhanced by
-
- widening the base of support
- lowering the center of gravity, bringing it closer to the base of support.
The base of support is easily widened by spreading the feet farther apart. The center of gravity is readily lowered by flexing the hips and knees until a squatting position is achieved.
Manually moving and lifting clients often cause musculoskeletal disorders (MSDs).
This limit should be further reduced if the health care worker is lifting in a restricted space, sitting or kneeling, twisting, one-handed, or with arms extended; if working longer than 8 hours; or if the client is combative, cannot follow direction, or has physical or medical conditions that impact his or her being lifted or moved.
If the weight to be lifted exceeds 35 pounds or the other conditions exist, assistive devices should be used.
Lifting: It is important to remember that nurses should not lift more than 35 pounds without assistance from proper equipment and/or other individuals.
Types of assistive equipment include mobile-powered or mechanical lifts, ceiling-mounted lifts, sit-to-stand powered lifts, friction-reducing devices, and transfer chairs.
Pulling and Pushing: When pulling or pushing an object, a person maintains balance with least effort when the base of support is increased in the direction in which the movement is to be produced or opposed.
When pulling an object, a person can enlarge the base of support by
(a) moving the rear leg back if the person is facing the object
(b) moving the front foot forward if the person is facing away from the object
Preventing Back Injury
Nurses provide clients with the opportunity to change positions, expand their lungs, or change their environments as appropriate.
Two movements to avoid because of their potential for causing back injury are twisting (rotation) of the thoracolumbar spine and acute flexion of the back with hips and knees straight (stooping).
- Understand that the use of body mechanics will not necessarily prevent injury if manually handling a load greater than 35 pounds without the use of assistive devices.
- Avoid lifting anything greater than 35 pounds. Use assistive equipment, get help from coworkers, and participate in the purchasing/ordering process of appropriate assistive equipment for your work setting.
- Become consciously aware of your posture and body mechanics.
- When standing for a period of time, periodically move legs and hips, and flex one hip and knee and rest your foot on an object if possible.
- When sitting, keep your knees slightly higher than your hips.
- Use a firm mattress and soft pillow that provide good body support at natural body curvatures.
- Exercise regularly to maintain overall physical condition and regulate weight; include exercises that strengthen the pelvic, abdominal, and spinal muscles.
- Avoid movements that cause pain or require spinal flexion with straight legs (e.g., toe-touching and sit-ups) or spinal rotation (twisting).
- When moving an object, spread your feet apart to provide a wide base of support.
- Wear comfortable low-heeled shoes that provide good foot support and reduce the risk of slipping, stumbling, or turning your ankle.
Positioning clients
Purpose of Positioning
- To maintain good body alignment, comfort, and safety.
- To prevent complications such as:
- Pressure ulcers
- Contractures
- Nerve and vessel damage
- Muscle discomfort
- To promote circulation, muscle tone, and postural reflexes.
Frequency of Position Changes
- Clients should be repositioned at least every 2 hours, day and night.
- More frequent repositioning is required if there is a risk of skin breakdown.
Clients Requiring Assistance
- Independent clients: Reposition themselves; need minimal guidance.
- Dependent clients: Weak, frail, paralyzed, in pain, or unconscious — rely entirely on nurses for repositioning.
- Best practice: Use two or more nurses and assistive devices to prevent injury and maintain client dignity.
Key Nursing Responsibilities
Before and After Positioning
Assess skin for redness, breakdown, or irritation. Provide skin care and ensure dryness. Check for comfort and adjust support as needed.
During Positioning
Maintain proper alignment and joint support. Ensure mattress is firm and supportive: Avoid sagging or overly soft surfaces and use bed boards for clients with back issues. Keep bed linens clean, dry, and wrinkle-free. Ensure freedom of movement (loosen top bedclothes). Use support devices (pillows, wedges, trochanter rolls) only as needed to: Maintain alignment, Relieve pressure and Prevent strain or deformity.
Avoid:
-
- Placing bony prominences directly over each other
- Pressure on areas like the popliteal space
- Friction (rubbing between skin and sheets)
- Shearing forces (skin stationary while deep tissues slide, especially when semi-sitting)
Preventing Friction and Shearing
- Friction: Caused by rubbing of sheets or rough surfaces - skin abrasion.
- Shearing: Combination of friction and pressure; occurs when the client slides downward in bed - damages deep tissues, especially over the sacrum.
- Prevention:
- Lift, don’t drag, during repositioning.
- Use draw sheets or sliding boards.
- Keep head of bed at lowest elevation possible to prevent sliding.
Client-Centered Positioning
Always ask the client which position feels most comfortable. Combine visual alignment with client feedback to ensure both comfort and correct positioning. Document preferred positions and effectiveness of alignment techniques.
|
Position |
Description |
Angle of Elevation / Body Alignment |
Uses / Indications |
Precautions / Disadvantages |
|
Fowler’s Position
|
Semisitting position with head and trunk raised. |
Head and trunk raised 45°–60°; knees may or may not be flexed. |
- Facilitates breathing and chest expansion. - Beneficial for clients with respiratory or cardiac problems. |
- Avoid excessive pillows behind the head (risk of neck flexion contractures). - Encourage occasional rest without pillow to maintain neck extension. |
|
Semi-Fowler’s (Low Fowler’s) |
Mild elevation of head and trunk. |
15°–45°, typically 30°. |
- Common resting position. - Used in tube feeding and for postoperative comfort. |
- May still allow some risk of aspiration if head not elevated adequately. |
|
High-Fowler’s |
Nearly upright sitting position. |
60°–90° (often 90°). |
- Promotes maximum lung expansion. - Used for severe respiratory distress, swallowing, and eating. |
- May cause pressure on sacrum and buttocks; use pillows or cushions. |
|
Orthopneic Position
|
Client sits upright, leaning forward on an overbed table. |
Sitting upright with overbed table supporting arms. |
- Facilitates maximum chest expansion. - Used for clients with difficulty exhaling (e.g., COPD, asthma). |
- May not be tolerated for long; requires good trunk strength to maintain. |
|
Dorsal Recumbent (Back-Lying)
|
Head and shoulders slightly elevated. |
Supine with small pillow under head and shoulders. |
- Provides comfort and relaxation. - Used post-surgery (esp. spinal or after anesthesia). |
- Risk of pressure on sacrum and heels if maintained long.- Not same as flat supine position. |
|
Prone Position
|
Client lies on abdomen, head to one side. |
Flat, hips not flexed. |
- Promotes hip and knee extension. - Prevents flexion contractures. - Promotes oral drainage (e.g., post mouth/throat surgery). |
- Not suitable for spinal, cardiac, or respiratory problems. - May cause lordosis, neck strain, and plantar flexion. - Use for short periods only. |
|
Lateral (Side-Lying) Position
|
Client lies on one side with top leg flexed and in front. |
One side of body; top hip and knee flexed. |
- Relieves pressure on sacrum and heels. - Promotes good spinal alignment.- Comfortable for sleeping and resting. |
- Requires frequent turning to prevent pressure injuries. - Support pillows may be needed for alignment. |
|
Sims’ (Semiprone) Position
|
Halfway between lateral and prone. |
Lower arm behind body; upper arm flexed; both legs flexed (upper leg more). |
- Facilitates oral drainage and prevents aspiration. - Used for unconscious or paralyzed clients, enemas, rectal exams, and pregnancy comfort. |
- May cause pressure on humerus and clavicle on dependent side. - Must ensure proper limb support. |




4.4 IMPLEMENTING (CONTINUED)
Moving and Turning Clients in Bed
Ill or immobile clients often need assistance to move in bed. Nurses must balance client independence with safety, maintain correct body alignment, and use proper techniques and assistive devices to prevent injury to both client and caregiver.
- Assess the client’s ability to move and assist before performing any repositioning.
- Maintain proper body alignment to prevent strain on the musculoskeletal system.
- Use assistive devices and adequate staff to ensure safety.
- Promote client comfort, privacy, and dignity during all movements.
- Follow agency policy on the use of mechanical lifts and assistance requirements.
Assistive Equipment
- Hydraulic lifts: Used for transfers between bed, wheelchair, stretcher, or bathtub.
- Friction-reducing devices: Minimize skin shear during repositioning.
- Overhead trapeze: Allows partially mobile clients to assist in movement.
- Pillows and rolls: Maintain alignment and prevent pressure injuries.
Assessment Before Moving
Evaluate:
- Physical ability (muscle strength, paralysis)
- Cognitive ability and understanding of instructions
- Willingness to participate
- Degree of discomfort or pain (administer analgesia if needed)
- Weight and body size
- Effects of medications (e.g., those causing drowsiness or hypotension)
- Presence of lines, catheters, or drains
- Risk of orthostatic hypotension
Planning
- Review previous records for mobility limitations.
- Gather assistive devices and required personnel.
- Explain the procedure clearly to the client and family.
- Provide privacy and perform hand hygiene.
- Adjust bed height and lock wheels before starting.
Body Mechanics for Nurses
- Face the direction of movement to avoid twisting.
- Use a wide stance for stability.
- Flex hips, knees, and ankles to lower center of gravity.
- Engage core muscles before movement.
- Rock body weight (front to back or back to front) to move smoothly.
SKILL: Moving a Client Up in Bed
Purpose: Reposition clients who have slid down in bed or to promote comfort and alignment.
Implementation:
- Flatten the bed as tolerated and remove pillows.
- Protect the head with a pillow against the bed frame.
- Use appropriate devices and assistance based on client’s weight:
- <200 lb: Friction-reducing sheet + 2 assistants.
- 201–300 lb: Slide sheet + 4 assistants or air transfer + 2 assistants.
- 300 lb: Air transfer system or total lift.
- Encourage client to flex knees, push with feet, and assist as able.
- Move client smoothly on count of three using proper body mechanics.
- Reposition and support client comfortably, raise head of bed if indicated.
Documentation:
- Time and new position
- Pressure areas noted
- Devices used
- Client’s ability to assist
- Client response (comfort, dizziness, anxiety)
SKILL: Turning a Client (Lateral or Prone Position)
Purpose: For repositioning, pressure relief, linen changes, or procedures (e.g., placing a bedpan).
Preparation:
- Check for IV lines, catheters, and mobility aids.
- Use assistive devices or mechanical lifts if needed.
- Ensure two or more caregivers for safety.
Performance Steps:
- Explain procedure, perform hand hygiene, and ensure privacy.
- Flatten bed, lock wheels, and raise bed to working height.
- Move client toward opposite edge of bed to prevent falling off after turning.
- Cross client’s near leg over the far leg and position near arm across the chest.
- Slightly abduct far shoulder to prevent it from being trapped.
- With one hand on shoulder and the other on hip, roll client toward you.
- Support head and limbs with pillows.
- For prone position, keep the far arm alongside the body before turning.
- Avoid pulling client once prone to prevent injury to breasts or genitals.
Documentation:
- Positions changed from/to
- Skin condition and pressure areas
- Client’s ability to assist
- Response to repositioning
- Use of support devices
Delegation
- Moving and turning clients can be delegated to Unlicensed Assistive Personnel (UAP) if the nurse:
- Assesses the client first.
- Ensures necessary equipment and assistance are available.
- Instructs UAP to report changes in condition (e.g., pain, dizziness, weakness).
Evaluation
After moving:
- Assess comfort, pain, dizziness, anxiety
- Check body alignment and vital signs (if needed)
- Verify safety measures (side rails up, call light within reach)
Safety Tips
- Never lift more than 35 lb of a client’s weight—use assistive devices.
- Always lock wheels on the bed and equipment.
- Maintain client privacy and dignity.
- Avoid twisting the spine or overreaching.
- Ensure communication and coordination among assisting personnel.
NURSING INSIGHTS: Positioning, Moving, and Turning Clients
INFANTS
• Position infants on their back for sleep, even after feeding. There is little risk of regurgitation and choking, and the rate of sudden infant death syndrome (SIDS) is significantly lower in infants who sleep on their backs.
• The skin of newborns can be fragile and may be abraded or torn (sheared) if the infant is pulled across a bed.
CHILDREN
• Carefully inspect the dependent skin surfaces of all infants and children confined to bed at least three times in each 24-hour period.
OLDER ADULTS
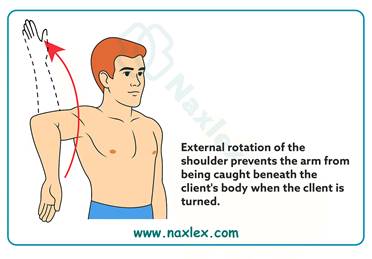
• In clients who have had cerebrovascular accidents (strokes), there is a risk of shoulder displacement on the paralyzed side from improper moving or repositioning techniques. Use care when moving, positioning in bed, and transferring. Pillows or foam devices are helpful to support the affected arm and shoulder and prevent injury.
• Decreased subcutaneous fat and thinning of the skin place older adults at risk for skin breakdown. Repositioning approximately every 2 hours (more or less, depending on the unique needs of the individual client) helps reduce pressure on bony prominences and avoid tissue trauma.
Using Mechanical Aids for Walking
Mechanical aids for ambulation include canes, walkers, and crutches. These devices help clients with impaired mobility maintain balance, stability, and independence.
1. Canes
Types
- Standard cane: Single straight leg.
- Tripod cane: Three feet for increased support.
- Quad cane: Four feet; provides the greatest stability.
Features:
Rubber tips prevent slipping. Standard cane length ≈ 91 cm (36 in); adjustable aluminum canes: 56–97 cm (22–38 in). Elbow should be slightly flexed when the cane is in use.
How to Use a Cane
- Hold the cane on the stronger side of the body.
- Place the cane tip 15 cm (6 in) to the side and in front of the near foot.
When maximum support is required:
- Move cane forward about 30 cm (1 ft).
- Move weaker leg forward to the cane (weight on cane + strong leg).
- Move stronger leg forward past cane and weak leg.
- Repeat sequence.
When less support is needed:
- Move cane and weak leg together.
- Move strong leg forward (weight on cane and weak leg).
2. Walkers
Types
- Standard walker: Four rubber-tipped legs; must be lifted to move. The standard walker needs to be picked up to be used. The client therefore requires partial strength in both hands and wrists, strong elbow extensors, and strong shoulder depressors. The client also needs the ability to bear at least partial weight on both legs.
- Two-wheeled walker: Two legs with wheels and two without; offers more stability than four-wheeled models.
- Four-wheeled (roller) walker: Easier to move; includes hand brakes and often a seat; less stable.
Height Adjustment:
- Hand bar should be just below the waist, elbows slightly flexed (~30°).
- Too low leads to stooping; too high leads to shoulder strain.
How to Use a Walker
For maximum support:
- Move walker ahead ~15 cm (6 in).
- Move right foot up to walker (weight on left leg + arms).
- Move left foot up to meet right foot.
If one leg is weak:
- Move walker and weak leg together about 15 cm (6 in).
- Move stronger leg ahead (weight on arms + weak leg).
Note: When educating clients about the use of walkers, inform them that when transferring from chair or commode, they should back the walker to the chair or toilet seat and use arms of chair or commode to assist in sitting and standing. Teach clients to always use both hands when using a walker to transfer from standing to sitting
3. Crutches
Types
- Axillary (underarm) crutch: Most common; used for temporary needs.
- Lofstrand (forearm) crutch: Has a cuff around the forearm for wrist stability.
- Platform crutch: Allows forearm weight bearing for clients unable to bear weight on hands.
All crutches need rubber suction tips for traction.
Measuring for Crutches
- Supine method: Measure from anterior axillary fold to heel; add 2.5 cm (1 in).
- Standing method: Shoulder rest should be 2.5–5 cm (1–2 in) below axilla (≈ three finger widths).
- Handgrip height: When standing, elbows should flex about 30°.
- Body weight should be borne by hands, not the axillae, to prevent radial nerve injury (crutch palsy).
Crutch Gaits
|
Gait |
Description |
Requirements |
|
Four-point |
Right crutch → left foot → left crutch → right foot. Always 3 points of contact. |
Weight-bearing on both legs; safe and stable. |
|
Three-point |
Both crutches + weak leg → strong leg. |
Full weight-bearing on one leg only. |
|
Two-point |
Right crutch + left foot → left crutch + right foot. |
Partial weight-bearing on each foot; faster gait. |
|
Swing-to |
Move both crutches forward → swing body to crutches. |
Used by clients with leg paralysis. |
|
Swing-through |
Move both crutches forward → swing body past crutches. |
Requires strength and coordination. |
Tripod (Crutch) Stance
Crutches placed 15 cm (6 in.) in front and to the sides of feet. Feet slightly apart; head and back erect; weight on hands, not axillae. Provides wide base of support. Use a gait belt for safety during training.
Sitting and Standing with Crutches
Getting into a chair:
- Stand with back of unaffected leg centered against chair.
- Transfer both crutches to affected side and hold by hand bars.
- Hold chair arm with unaffected hand, lean forward, and sit down slowly.

Getting out of a chair:
- Move to edge; place unaffected leg under chair edge.
- Hold crutches in affected hand, chair arm with unaffected hand.
- Push up using both arms and unaffected leg, then assume tripod stance.
Using Crutches on Stairs
Going up stairs:
- Assume tripod position.
- Move strong leg up first.
- Move crutches and weak leg up to the same step.
- Repeat.
(Strong leg goes up first.)
Going down stairs:
- Assume tripod position.
- Move crutches and weak leg down first.
- Move strong leg down to the same step.
- Repeat.
(Weak leg goes down first.)
Transferring clients
Transferring clients means safely moving them between surfaces — such as from bed to chair, wheelchair, commode, or stretcher. The nurse must assess the client’s physical and mental ability, plan the transfer carefully, and ensure safety throughout the procedure.
Assistive devices include:
- Gait/transfer belts
- Sliding or transfer boards
- Friction-reducing devices (slide sheets, air transfer systems)
- Mechanical lifts
Key Assessment Before Transfer
Assess the client’s:
- Body size and weight
- Muscle strength and joint mobility
- Ability to bear weight and pivot
- Balance and activity tolerance
- Ability to follow instructions and cooperate
- Presence of pain, paralysis, or orthostatic hypotension
- Environment – available space, obstacles, and equipment condition
Planning
Review previous notes for client’s transfer ability. Administer pain medication before transfer if needed. Determine:
-
- The number of assistants required.
- Equipment needed (belt, slide sheet, lift, wheelchair, etc.).
- Client’s participation level.
Remove obstacles and ensure enough space. Assign one person to give commands during the transfer. Explain the procedure to both client and staff.
Gait/Transfer Belts
Used to control client movement during transfers or ambulation. Best for: Clients who can bear some weight and need minimal assistance.
Avoid using on:
-
- Clients requiring full lifting.
- Bariatric clients.
- Clients at high fall risk.
Do not use to lift clients from the floor.
- Belt should be snug around waist; use handles if available.
Sliding/Transfer Boards
Made of low-friction material; used between bed and chair. Suitable for clients who can sit upright and have upper-body strength. Client may self-transfer or be gently pushed/pulled using a slide sheet. Promotes independence and energy conservation for nurses.
General Transfer Guidelines
- Support the client, not the equipment.
- Provide privacy and use proper body mechanics (bend knees, straight back).
- Use step-by-step instructions to guide client movements.
- Lock wheels on beds, wheelchairs, and stretchers.
- Never leave clients unattended on stretchers or wheelchairs without brakes, straps, or side rails engaged.
- Always push a stretcher from the head end for safety.
SKILL: Transferring Between Bed and Chair/Wheelchair
Purpose
To assist clients in safely moving between bed, wheelchair, commode, or toilet.
Steps
- Preparation: Lock bed and wheelchair wheels. Place wheelchair parallel to the bed, on the client’s stronger side. Raise footplates and remove armrests if necessary.
- Assist Client: Help client sit on edge of bed; check for orthostatic hypotension. Ensure feet flat on floor and nonskid shoes/slippers worn. Place gait belt securely.
- Client Instructions: Lean forward slightly from hips. Strong leg under bed edge, weaker leg forward. Place hands on bed, not on nurse’s neck, for pushing.
- Nurse Positioning: Stand in front and slightly to weak side. Hold gait belt and support client’s shoulder. Flex knees and hips; keep a broad stance. Brace client’s knees/feet to prevent slipping.
- Standing and Pivoting: On cue (“1–2–3, stand”), client pushes down while nurse transfers weight and assists to standing. Allow time for stability, then pivot or take steps toward chair.
- Sitting: Have client feel chair with legs, then reach for armrests. Slowly lower client by bending knees and hips. Ensure client sits well back for stability. Replace footplates and remove belt.
Variations
- Two-nurse transfer: One on each side holding belt and elbows.
- Injured leg: Transfer toward strong side.
- Slide board: Use for clients unable to stand but able to use upper body.
Documentation
- Client’s ability to bear weight/pivot.
- Number of staff and devices used.
- Duration and tolerance of sitting up.
- Response to transfer and safety measures.
SKILL: Transferring Between Bed and Stretcher
Purpose
For moving supine clients between surfaces (e.g., bed to stretcher).
Assistive Devices
- Slide sheet, lateral transfer board, or air transfer system.
- Weight-based staffing recommendations:
- < 200 lb: 2 caregivers + friction-reducing device.
- 201–300 lb: 4 caregivers or air transfer system.
- 300 lb: 2 caregivers + ceiling lift or air system.
Steps
- Preparation: Lower bed head and adjust height slightly higher than stretcher. Place friction-reducing device under client. Position stretcher parallel to bed and lock wheels. Fill gap with blankets if needed.
- Transfer: If independent, let client lift or roll over. If dependent: Caregiver at bed pushes; others pull client using sheet or board. Client’s arms crossed and neck flexed to prevent injury. Use planned verbal cue to coordinate motion.
- After Transfer: Raise side rails and/or fasten safety straps. Unlock wheels and move stretcher away safely.
- Variation- Transfer Board: Smooth board (45–55 cm × 182 cm) with handholds. Roll client laterally, insert board, then slide across. Apply safety belts over chest, abdomen, and legs.
Documentation
- Equipment used.
- Number of staff.
- Safety measures (locked wheels, belts, side rails).
- Destination and reason for transfer.
Providing range of motion (ROM) exercises
Purpose: To maintain joint mobility, prevent contractures and stiffness, and promote circulation in clients with restricted activity or immobility. Helps preserve muscle tone and joint flexibility when clients cannot move independently.
Types of ROM Exercises
|
Type |
Description |
Who Performs It |
Purpose/Benefit |
|
Active ROM (AROM) |
Client independently moves each joint through full range |
Client |
Maintains muscle strength, endurance, and joint flexibility; promotes circulation and cardiorespiratory function |
|
Passive ROM (PROM) |
Another person moves the client’s joints through full range |
Nurse or caregiver |
Maintains joint flexibility and prevents contractures (does not build muscle strength) |
|
Active-Assistive ROM (AAROM) |
Client uses stronger limb to move weaker limb; nurse assists to complete motion |
Client + nurse |
Improves mobility and flexibility, especially useful for stroke or hemiplegic clients |
General Guidelines
- Perform ROM to the point of slight resistance, never pain.
- Movements should be smooth, slow, and rhythmic, avoiding jerky or forceful motion.
- Use the same sequence for every session to ensure consistency.
- Perform 3–5 repetitions for each movement, twice daily (e.g., during bathing).
- Support the joint above and below during movement to prevent strain or injury.
- Encourage client participation whenever possible.
For Active ROM
- Teach client the purpose and correct technique.
- Perform movements systematically in the same order each session.
- Each exercise should be done 3 times, twice daily.
- Stop if pain or discomfort occurs.
Older adults: Focus on maintaining ROM sufficient for Activities of Daily Living (ADLs) (e.g., dressing, bathing, walking). Full ROM in all joints is not necessary.
For Passive ROM
- Explain purpose and obtain cooperation.
- Ensure rings are removed to prevent swelling or injury.
- Client should wear a loose gown, covered with a bath blanket for warmth and privacy.
- Use correct body mechanics to avoid self-injury.
- Expose only the limb being exercised.
- Support joints with hands or forearms; never pull on a limb.
- If spasticity occurs: pause, apply gentle pressure until muscle relaxes, then continue.
- If rigidity occurs: apply slow, steady pressure and continue gently.
- Avoid hyperextension, especially in arthritic joints.
- Assess skin condition during exercises.
For Active-Assistive ROM
- Client uses stronger limb to assist weaker limb.
- Nurse completes movement to full range if client fatigues.
- Especially useful for clients recovering from stroke or hemiplegia.
- Enhances coordination, independence, and self-care ability.
Safety & Evaluation
- Monitor client’s tolerance, pain level, and muscle tone.
- Document:
- Type of ROM performed
- Client’s participation and tolerance
- Joints exercised
- Any discomfort or complications observed
4.5 EVALUATING
The goals established during the planning phase are evaluated according to specific desired outcomes, also established in that phase.
If outcomes are not achieved, the nurse, client, and support person if appropriate need to explore the reasons before modifying the care plan.
For example, the following questions may be considered if an immobilized client fails to maintain muscle mass and tone and joint mobility:
- Has the client’s physical or mental condition changed motivation to perform required exercise?
- Were appropriate range-of-motion exercises implemented?
- Was the client encouraged to participate in self-care activities as much as possible?
- Was the client encouraged to make as many decisions as possible when developing a daily activity plan and to express concerns?
- Did the nurse provide appropriate supervision and monitoring?
- Was the client’s diet adequate to provide appropriate nourishment for energy requirements?
Summary
- Exercise and activity are essential components for maintaining and regaining health and wellness.
- Purposeful coordinated movement of the body relies on the integrated functioning of the musculoskeletal system, the nervous system, and the vestibular apparatus of the inner ear.
- People maintain alignment and balance when the line of gravity passes through the center of gravity and the base of support.
- Exercise is classified as either isotonic, isometric, or isokinetic and as either aerobic or anaerobic.
- Immobility affects almost every body organ and system adversely.
- An activity and exercise history includes daily activity level, activity tolerance, type and frequency of exercise, and factors affecting mobility.
- Positioning a client in good body alignment and changing the position regularly and systematically are essential aspects of nursing practice.
- Before moving, turning, or transferring a client, the nurse must consider the client’s health status and degree of exertion permitted, physical ability to assist, ability to comprehend instruction, degree of discomfort, client’s weight, and whether to use assistive devices or another caregiver to assist.
- Clients need specific instructions about appropriate use of canes, walkers, and crutches.
