
Caring for the special needs child
Study Questions
Practice Exercise 1
Which of the following is an example of a normalization strategy for a child with a chronic illness?
Explanation
Normalization is the process of supporting children with chronic illness to live as normal a life as possible. Disability normalization involves encouraging inclusive environments where children with disabilities are treated as full participants in school and community life.
Rationale for correct answer:
B. Allowing the child to attend school and participate in age-appropriate activities promotes independence and self-esteem, encourages peer interaction and social development, helps maintain a sense of routine and normalcy despite medical challenges.
Rationale for incorrect answers:
A. Restricting the child's social interactions to prevent infection is overly restrictive and isolates the child. It may cause social and emotional harm, unless specifically required during immune suppression.
C. Encouraging the child to focus solely on their illness and treatment reinforces the “sick role” and limits opportunities for growth, play, and socialization.
D. Keeping the child isolated at home to reduce stress increases loneliness and delays normal developmental experiences. Stress is better managed through coping strategies and supportive environments, not isolation.
Take home points:
- Normalization is integration of illness into daily life, not making the illness the focus of life.
- Encourage participation in school, play, and family activities whenever possible.
- Provide anticipatory guidance to parents: reasonable limits and expectations foster independence.
A nurse is working with a family struggling to cope with their child's chronic illness. What is the most effective initial nursing intervention?
Explanation
Coping refers to the thoughts, behaviors, and emotional strategies people use to manage stress, adversity, or challenging situations. It’s how we adapt, whether consciously or unconsciously, to internal pressures (like anxiety or grief) or external demands like illness, conflict, or change.
Rationale for correct answer:
C. Families of children with chronic illness often experience stress, grief, guilt, and helplessness. The most effective initial nursing intervention is to provide emotional support through therapeutic communication. Actively listening and validating feelings builds trust between the nurse and family, helps the family feel heard and understood, and opens the door for further teaching, coping strategies, and resource referral.
Rationale for incorrect answers:
A. Telling them to be strong for their child minimizes the family’s emotions. It is not therapeutic and may make them feel guilty for expressing distress.
B. Referring them to a psychologist without discussion is premature. The family may feel dismissed or abandoned. Referral can be helpful later, but not as an initial step.
D. Providing them with a list of all available resources without explanation may overwhelm the family. Resources should be explained after establishing rapport and understanding needs.
Take home points
- Therapeutic communication comes first in family-centered nursing care.
- Listening and validation build a foundation for later education, resources, and referrals.
- Families coping with chronic illness benefit most when nurses provide emotional support + practical guidance.
When caring for a 4-year-old with a disability, the nurse notes that while encouraging the child to take part in his care, the mother constantly gives into the child, allowing him to have his own way. What anticipatory guidance can the nurse give to promote normalization in this relationship?
Explanation
Normalization is a key principle in pediatric nursing care for children with disabilities. It encourages families to treat their child as normally as possible while providing the necessary support.
Rationale for correct answer:
B. Explaining to parents that establishing reasonable limits fosters independence and age-appropriate responsibility is the best anticipatory guidance. This approach allows the child to grow within their abilities, preventing over-dependence while encouraging self-esteem and confidence.
Rationale for incorrect answers:
A. Telling parents that “giving in” is not a detriment is inaccurate. Constantly giving in may foster dependency, behavioral problems, and hinder independence.
C. Advising parents to wait until just before procedures to explain them is not developmentally appropriate. Children should be prepared according to their level of understanding, which reduces anxiety and builds trust.
D. Suggesting that siblings should not have similar rules undermines family consistency. While accommodations may be necessary, children with disabilities should still be part of the family unit with expectations tailored but not completely exempt.
Take home points
- Normalization means integrating children with disabilities into everyday routines with appropriate expectations.
- Setting consistent and reasonable limits helps children develop independence and self-confidence.
- Parents should prepare children for procedures at their developmental level, not delay explanations until the last minute.
- Consistency in family rules and expectations promotes fairness and stability for all siblings.
Children with disabilities or chronic illness and their families may have different methods of coping than those of healthy children. Often they have a resilience that is to be admired. Which of these statements reflect ways that they foster this resilience? Select all that apply
Explanation
Families of children with chronic illness or disabilities often develop resilience through positive coping strategies that foster hope, independence, and acceptance. These methods help both the child and family adapt to ongoing challenges while maintaining a sense of normalcy.
Rationale for correct answers:
B. Developing relationships with other families in similar circumstances provides social support, reduces isolation, and fosters shared understanding.
C. Parents who set long-term goals instill a sense of hope and direction, helping the child and family look beyond daily struggles.
D. Focusing on the child’s strengths and encouraging independence promotes self-esteem and helps the child achieve developmental milestones within their abilities.
E. Accepting that chronic illness is part of living allows families to move forward, adapt routines, and maintain quality of life instead of remaining stuck in denial or grief.
Rationale for incorrect answer:
A. Protecting the child from learning about their illness is not adaptive. Age-appropriate education about the illness fosters coping, trust, and empowerment. Shielding the child may increase anxiety and hinder self-management skills.
Take home points
- Resilience in families of children with chronic illness is built on support networks, hope, independence, and acceptance.
- Open communication and age-appropriate education about illness empower children rather than protect them.
- Families thrive when they balance realistic limitations with a focus on strengths and possibilities.
Which of the following factors should a nurse consider when managing the pain of a terminally ill child? Select all that apply
Explanation
Effective pain management in terminally ill children focuses on comfort, dignity, and quality of life. The nurse’s role is to ensure that the child’s pain is adequately controlled using both pharmacologic and non-pharmacologic methods, while addressing misconceptions parents or providers may have about opioid use.
Rationale for correct answers:
A. Breakthrough pain is common in terminal illness, and timely administration of additional doses is essential for relief.
B. Opioid drugs such as morphine are the mainstay for severe pain in terminal illness. Doses are titrated upward as needed to maintain optimal comfort, without a ceiling limit in palliative care.
D. Nurses may fear that high opioid doses hasten death, but according to the principle of double effect, the intent is comfort, not hastening death. When administered appropriately, opioids relieve suffering without intentionally causing death.
E. Non-pharmacologic interventions (music therapy, distraction, guided imagery, relaxation techniques) complement medications and give the child and family a sense of control, improving quality of life.
Rationale for incorrect answers:
C. Addiction is not a concern in terminal pediatric pain management. The focus is on comfort, not long-term dependence. Educating parents about this distinction is essential to reduce fear and ensure the child receives appropriate relief.
Take home points
- Scheduled opioid dosing with breakthrough coverage ensures consistent comfort in terminally ill children.
- Addiction is not a concern at end-of-life care, comfort and dignity are the priority.
- The principle of double effect supports opioid use even at higher doses if the intent is pain relief, not hastening death.
- Combining pharmacologic and non-pharmacologic strategies provides holistic care for both child and family.
It is important to consider the child’s developmental understanding of death when working with that child. Which option is the preschool child’s developmental stage?
Explanation
Preschool children (ages 3–5) are in the preoperational stage of cognitive development. They use magical thinking and egocentrism, often believing their thoughts or behaviors are powerful enough to cause events, including death. This belief can lead them to feel responsible or guilty when someone dies.
Rationale for correct answer:
A. Preschoolers believe their thoughts are sufficient to cause death due to magical thinking and egocentrism. They may think, “If I was mad at Mommy and she got sick, I made it happen.” This belief is developmentally normal but can cause distress and guilt if not addressed with reassurance.
Rationale for incorrect answers:
B. While preschoolers do have magical thinking, the key distinction is their specific belief that their own thoughts or actions can directly cause death, making option 1 the more precise answer.
C. A concrete understanding of death develops later, in school-age children, who begin to grasp death’s permanence and universality.
D. Viewing events only in their own frame of reference (living) describes toddlers, who do not comprehend death but react to separation and changes in routine.
Take home points
- Preschoolers (3–5 years): Believe their thoughts or actions can cause death (magical thinking, guilt).
- School-age children (6–12 years): Understand death as final, universal, and irreversible.
- Toddlers: Have no real concept of death, only separation anxiety.
- Adolescents: Grasp the finality of death but may feel invulnerable themselves, leading to risk-taking behaviors.
Practice Exercise 2
A child has been diagnosed with fragile X syndrome. Which of the following health-care referrals should the nurse encourage the parents to make? The nurse should encourage the parents to consult with a(n):
Explanation
Fragile X Syndrome (FXS) is caused by a mutation in the FMR1 gene on the X chromosome, which normally produces a protein (FMRP) essential for brain development. In FXS, this gene is either silenced or doesn’t produce enough of the protein, leading to developmental challenges.
Rationale for correct answer:
B. Families benefit from counseling to learn about the genetic basis of fragile X syndrome, recurrence risks, and implications for siblings and extended family. Genetic counseling also provides emotional support and guidance in navigating available interventions and support services.
Rationale for incorrect answers:
A. Fragile X syndrome does not typically require orthopedic intervention as a priority. While children may have joint laxity or hypotonia, these issues are usually managed through physical/occupational therapy, not surgery.
C. Unless feeding issues or obesity develop, dietary management is not a primary concern in fragile X syndrome. This referral may be useful in some cases but is not a priority.
D. While recurrent ear infections may occur, otolaryngologist referral is not universally required for all children with fragile X. It may be appropriate based on symptoms but not the first or most important referral.
Take home points
- Fragile X syndrome is a hereditary condition, and genetic counseling is crucial for families to understand risks, recurrence, and support options.
- Early interventions (speech therapy, occupational therapy, behavioral therapy) are key to improving outcomes.
- Nurses should ensure families receive appropriate referrals to support services and education tailored to developmental needs.
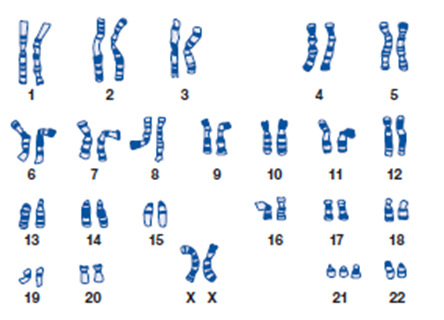
The nurse notes the following genomic nomenclature and karyotype in the amniocentesis report. Which of the following interpretations of the report is appropriate for the nurse to make?
Nomenclature: 47, XX, +21
Explanation
Down syndrome is a genetic condition caused by the presence of an extra copy of chromosome 2A. This additional genetic material affects how the body and brain develop, leading to a range of physical, cognitive, and developmental differences.
Rationale for correct answer:
A. The karyotype 47, XX, +21 indicates that the fetus is female (XX) and has an extra chromosome 21, consistent with trisomy 21 (Down syndrome).
Rationale for incorrect answers:
B. Fragile X is due to a trinucleotide (CGG) repeat expansion on the X chromosome, not an extra chromosome. It would not appear as “+21” in karyotype nomenclature.
C. A fetus born with shortened palpebral fissures and hypoplastic upper lip are features associated with fetal alcohol syndrome, not trisomy 2A.
D. A fetus born with hypertonic reflexes and spastic posturing suggest cerebral palsy, a neuromotor disorder that develops postnatally, not a chromosomal abnormality identified on karyotype.
Take home points
- 47, XX, +21 = Female with trisomy 21 (Down syndrome).
- Down syndrome features include intellectual disability, characteristic facial features, and increased risk for cardiac and other health issues.
- Other syndromes (fragile X, fetal alcohol syndrome, cerebral palsy) have different etiologies and would not appear as +21 on karyotype.
A couple is being discharged from the hospital with their 2-day-old Down syndrome baby. The nurse is
Explanation
Down syndrome is a genetic condition caused by the presence of an extra copy of chromosome 21, which is why it's also called trisomy 2A. This additional genetic material affects how the body and brain develop, leading to a range of physical, cognitive, and developmental differences.
Rationale for correct answer:
B. Hypotonia is a hallmark of Down syndrome. It can contribute to poor feeding (difficulty sucking/swallowing), delayed motor milestones (sitting, crawling, walking), and increased joint laxity. Nurses should prepare parents for supportive interventions such as physical therapy and feeding support.
Rationale for incorrect answers:
A. Small cerebral ventricles is not a typical feature of Down syndrome. Cerebral changes are more related to intellectual disability and increased risk of early-onset Alzheimer’s disease, not ventricular size.
C. Children with Down syndrome do feel pain; in fact, they may have increased risk of infection or injury due to hypotonia and joint laxity. This is incorrect.
D. Down syndrome is not associated with impaired renal function as a primary characteristic. Renal issues may occur but are not a defining physiological feature.
Take home points
- Hypotonia is a key physiologic characteristic of Down syndrome and has implications for feeding, motor skills, and development.
- Parents should be educated on the importance of early interventions such as physical therapy, occupational therapy, and feeding support.
- Discharge teaching should always emphasize supporting development and recognizing health concerns such as feeding problems, infection, and congenital heart disease risk.
A mother of a child born with Down syndrome is overwhelmed with the future and asks many questions. Which of the following facts should the nurse be aware of? Select all that apply
Explanation
When counseling families of children with Down syndrome, it is essential that nurses provide accurate, supportive, and evidence-based information. This helps parents cope, plan for the future, and provide the best care for their child.
Rationale for correct answers:
A. Eighty percent of infants with Down syndrome are born to women under 35 because younger women have higher fertility rates, even though the risk increases with maternal age.
B. Feeding difficulties are common due to hypotonia and a protruding tongue. Using a small, straight-handled spoon placed to the side and back of the mouth helps with effective feeding.
C. Many parents of children with Down syndrome report that the experience, although challenging, has made them stronger, more compassionate, and accepting of others.
E. A child’s lack of clinging or molding is due to hypotonia and not emotional detachment or parental rejection. This distinction reassures parents.
Rationale for incorrect answers:
D. Placement in regular classrooms with support has been found to be beneficial, not detrimental. Inclusion promotes socialization and learning opportunities, although individual support may be needed.
F. Development in Down syndrome is delayed compared to mental age, not accelerated. Milestones are achieved later, often several years behind peers, especially in motor and language areas.
Take home points
- Most children with Down syndrome are born to younger mothers, despite increased risk in older women.
- Feeding support and special techniques are often needed in infancy due to hypotonia and tongue protrusion.
- Many parents find resilience and strength in raising a child with Down syndrome.
- Inclusion in regular classrooms can support development when tailored assistance is provided.
A 4-year-old with Down syndrome is being seen in the pediatric clinic. The nurse reminds the parents
Explanation
Down syndrome is a genetic condition caused by the presence of an extra copy of chromosome 2A. This additional genetic material affects how the body and brain develop, leading to a range of physical, cognitive, and developmental differences.
Rationale for correct answer:
A. Children with Down syndrome are at high risk for respiratory tract infections due to hypotonia including weak muscle tone and leading to poor cough and difficulty clearing secretions, anatomical airway differences including smaller trachea, enlarged tonsils/adenoids, and macroglossia, and immune system compromise, making them more susceptible to infections. Any upper respiratory illness in these children can rapidly progress to pneumonia or airway obstruction, requiring immediate medical care.
Rationale for incorrect answers:
B. Pendulous abdomen is common in Down syndrome due to hypotonia; not an urgent concern.
C. Elevated temperature alone is not specific or emergent unless linked to respiratory symptoms.
D. Protruding brow is a facial characteristic of Down syndrome, but not an urgent clinical finding.
Take-Home Points:
- Children with Down syndrome require close monitoring for respiratory complications.
- Parents should seek medical care promptly if their child has:
- Cough, congestion, or difficulty breathing.
- Signs of infection such as lethargy, decreased feeding, or fever with respiratory symptoms.
- Preventive measures: routine vaccinations, RSV prophylaxis in infancy, and regular ENT evaluations.
Practice Exercise 3
Early detection of hearing impairment in infants is crucial for:
Explanation
Hearing impairment, also known as hearing loss is a condition where a person experiences partial or complete inability to hear sounds. It can affect one or both ears and vary in severity from mild to profound.
Rationale for correct answer:
C. Hearing impairment in infants can delay the development of speech, language, and social interaction skills. Early detection through newborn hearing screening and timely interventions (hearing aids, cochlear implants, or speech therapy) help the child achieve normal communication and social milestones.
Rationale for incorrect answers:
A. Early detection doesn’t eliminate the need for surgical correction if structural issues exist.
B. Hearing impairment itself doesn’t cause other disabilities; it mainly affects language and psychosocial development.
D. Early detection does not prevent hearing aids. It actually ensures they are provided as early as needed.
Take home points
- Universal newborn hearing screening should be done within the first month of life.
- Intervention should start before 6 months to optimize outcomes.
- The goal is to promote language, communication, cognitive, and social development.
A nurse is caring for a child with Autism Spectrum Disorder. The nurse notices the child is becoming increasingly agitated. What is the most appropriate action?
Explanation
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition that affects how a person communicates, interacts socially, and processes sensory information. The term “spectrum” reflects the wide range of symptoms, abilities, and challenges that individuals with autism may experience.
Rationale for correct answer:
C. Children with Autism Spectrum Disorder (ASD) often become agitated due to sensory overload such as too much noise, light, or activity. The best intervention is to remove the child from the overstimulating environment and place them in a calm, quiet space to help them self-regulate. This approach prevents escalation and respects the child’s need for a structured, low-stimulation setting.
Rationale for incorrect answers:
A. Physically restraining the child should only be a last resort when there is risk of harm. It may increase distress and agitation in ASD.
B. Introducing new toys to distract them may actually increase agitation due to unfamiliarity or overstimulation. Children with ASD prefer routine and familiar objects.
D. Telling them to stop their behavior is a verbal commands and are often ineffective, as the child may not process them in moments of agitation and may feel more frustrated.
Take home points
- First-line nursing action: reduce environmental stimuli.
- Maintain structured routines and provide predictable, calm settings.
- Use familiar comfort objects or coping strategies if needed.
- Restraints and verbal scolding should be avoided unless safety is compromised.
When a child with a visual impairment is hospitalized, the nurse should ensure that which of the following interventions are carried out to decrease stress for the child during the hospitalization? Select all that apply
Explanation
Hospitalization can be especially stressful for children with visual impairment. Nurses can reduce anxiety and foster trust by ensuring consistency, orientation, reassurance, and clear communication.
Rationale for correct answers:
A. Reassurance throughout treatment is essential since the child cannot rely on visual cues. Explaining each step helps reduce fear and uncertainty.
B. Ensuring parents are comfortable with room organization provides safety and consistency for the child. Parents can help the child learn where objects are placed, preventing accidents.
C. Assigning the same nurse whenever possible offers consistency, familiarity, and trust, which are especially important for visually impaired children.
E. Health care providers should always identify themselves upon entering the room so the child feels secure and included in interactions.
Rationale for incorrect answer:
D. Taking over most of the child’s care is not appropriate. Children with visual impairments benefit from independence and normalization of daily routines. Encouraging self-care and parent involvement fosters autonomy, not dependence.
Take home points
- Provide clear explanations and reassurance since visual cues are absent.
- Maintain consistency in caregivers and environment for security.
- Always announce your presence and actions to avoid startling or confusing the child.
- Encourage independence and participation, rather than overprotecting, to support normal development.
Understanding autism spectrum disorders (ASDs) is very important for those who care for children. Goals of treatment for these children include:
Explanation
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition that affects how a person communicates, interacts socially, and processes sensory information. The term “spectrum” reflects the wide range of symptoms, abilities, and challenges that individuals with autism may experience.
Rationale for correct answer:
C. Providing a structured routine is a cornerstone of ASD management. Predictability helps reduce anxiety, improves cooperation, and allows children to function more effectively.
Rationale for incorrect answers:
A. Placement in a long-term care setting is not the goal. Most children with ASD remain at home with their families and benefit from community-based support and interventions.
B. Sharing a hospital room with another child may actually increase stress and overstimulation. Children with ASD often do better in quieter, less stimulating environments.
D. Comforting children with ASD does not always involve holding or cuddling. Many children with ASD dislike physical touch or find it overstimulating. Comfort should be based on the child’s individual needs and preferences.
Take home points
- Structured routines are essential for children with ASD.
- Family and community support are prioritized over long-term institutional placement.
- Minimize overstimulation in hospital and home environments.
- Comfort measures
- should be individualized, as many children with ASD may not tolerate physical affection.
Comprehensive Questions
The parents of a 5-year-old with special health care needs talk to the parents of a 10-year-old with a similar condition for quite a while each day. What is the nurse’s interpretation of this behavior?
Explanation
Support from other parents of children with special health care needs is a powerful coping mechanism. Shared experiences foster understanding, reduce isolation, and help families adapt to challenges more effectively than professional advice alone at times.
Rationale for correct answer:
C. Support between parents of special children is extremely valuable. Parents often find strength, comfort, and practical advice from those who have experienced similar challenges. These peer connections promote resilience, normalize feelings, and provide ongoing emotional support.
Rationale for incorrect answers:
A. Assuming the nurse has not provided enough support is inaccurate. While professional support is important, peer support adds a unique dimension that nurses cannot replace.
B. Viewing the relationship as potentially unhealthy is incorrect. Unless it becomes exclusive or fosters dependency, peer support is beneficial, not harmful.
D. Confidentiality is not a concern here as long as families willingly share their own experiences. The nurse must only safeguard protected health information.
Take home points
- Parent-to-parent support is highly effective in managing stress and promoting coping for families of children with special needs.
- Nurses should encourage peer connections through support groups or networking opportunities.
- Professional support and peer support complement each other, ensuring holistic family care.
- Confidentiality concerns arise only if health professionals disclose private information, not when parents voluntarily share.
The nurse is caring for a child who has received all possible medical care for cancer, yet continues to experience relapse and metastasis. It is time to make the transition from curative care attempts to palliative care. What is the most important nursing consideration at this time?
Explanation
Safe and compassionate care during the transition from curative to palliative treatment in pediatric oncology emphasizes supporting both the child and family. Nurses play a key role in ensuring that families remain central to decision-making, honoring their values, preferences, and cultural beliefs.
Rationale for correct answer:
C. Families are the primary caregivers and advocates for the child. Including them ensures respect for their values, promotes understanding of the goals of care, and helps them adjust emotionally to the transition. This approach enhances shared decision-making, maintains dignity, and strengthens coping mechanisms.
Rationale for incorrect answers:
A. The health care professionals should make the decision about the child’s care excludes the family, undermines trust, and disregards their role as the child’s advocate. Ethical pediatric care requires family participation in all major decisions.
B. Continuing aggressive treatment without benefit may increase suffering, prolong distress, and is not consistent with palliative principles. Hope can be reframed toward comfort, quality of life, and meaningful moments.
C. Palliative care is available across settings, including hospitals, hospices, and home. The choice depends on family preference, resources, and the child’s needs.
Take home points
- In pediatric palliative care, family-centered decision-making is essential.
- Nurses should support the family by providing honest information, emotional support, and guidance.
- Hope is not lost, rather, it is redirected toward comfort, dignity, and quality of life.
- Palliative care can occur in hospitals, hospices, or at home depending on the child and family’s wishes.
The nurse is caring for a 3-year-old with a gastrostomy tube and tracheostomy who is on supplemental oxygen and multiple medications. The mother is rooming in during this hospitalization. What is the priority nursing action?
Explanation
Safe and effective pediatric nursing care requires collaboration with caregivers, especially when caring for children with complex medical needs like a gastrostomy tube, tracheostomy, and multiple medications.
Rationale for correct answer:
B. Parents of medically complex children develop extensive expertise in daily care. The nurse should acknowledge this knowledge, involve the mother as a partner in care, and integrate her input into the plan. This approach promotes safety, minimizes errors, and supports family-centered care.
Rationale for incorrect answers:
A. Incorporating the mother’s assistance in care when convenient minimizes her role and implies she is only helpful occasionally. Her involvement should be central, not optional.
C. While caregiver rest is important, dismissing her may cause anxiety and reduce continuity of care. Instead, the nurse should support her presence and encourage breaks as appropriate.
D. While providing family-centered care since the mother is there is correct in principle, it is too general. True family-centered care requires specifically acknowledging the mother’s expertise and integrating her knowledge, making option 2 the best choice.
Take home points
- Parents of chronically ill children are vital partners in care and should be recognized as experts.
- Family-centered care means active, equal collaboration, not just presence or occasional involvement.
- Nurses should validate and respect parental input while ensuring safety and professional oversight.
- Empowering parents improves trust, adherence, and outcomes in children with complex health needs.
The nurse is caring for a child with a developmental disability who is starting kindergarten this year. The mother is tearful and doesn’t want the child to go to school. What is the best response by the nurse?
Explanation
Supporting families of children with developmental disabilities requires empathy, validation, and encouragement. Starting school can be an emotional milestone for any parent, and even more so when additional needs are involved. The nurse’s best response is one that normalizes the mother’s feelings, showing understanding and compassion without judgment.
Rationale for correct answer:
D. “It is normal to feel stressed or sad at this time.” This statement validates the mother’s emotions, reassures her that her reaction is expected, and opens the door for further supportive discussion. It reflects therapeutic communication, which acknowledges feelings without dismissing or minimizing them.
Rationale for incorrect answers:
A. “Do you need some time alone to collect yourself?” This may come across as dismissive and does not directly validate her emotions. It could shut down communication instead of fostering support.
B. “You’ve known for a while this time would come.” This response is non-therapeutic, potentially judgmental, and invalidates her feelings by suggesting she should be prepared.
C. “Can I call your husband or a friend for you?” While offering support is helpful, this bypasses the opportunity for the nurse to provide direct emotional support and validation. It shifts responsibility away instead of first acknowledging her feelings.
Take home points
- Therapeutic communication involves validating emotions, showing empathy, and encouraging expression.
- Parents of children with disabilities often experience added stress during developmental milestones, nurses should provide reassurance and support.
- Avoid dismissive, judgmental, or minimizing statements; instead, acknowledge feelings as normal and offer continued guidance.
- Validation builds trust and strengthens the nurse-family relationship.
The parents of a child with a developmental disability ask the nurse for advice about disciplining their child. What is the best response by the nurse?
Explanation
Discipline in children with developmental disabilities should be consistent, developmentally appropriate, and aligned with family values. Nurses should guide parents toward strategies that foster independence, promote acceptable behavior, and respect the child’s unique needs.
Rationale for correct answer:
A. “You should choose methods that are most congruent with your values about discipline.” This response emphasizes the importance of aligning discipline strategies with the family’s beliefs, which promotes consistency and follow-through. It avoids a one-size-fits-all approach and instead empowers parents to apply discipline in a way that supports both the child’s development and the family’s framework.
Rationale for incorrect answers:
B. “Children like this really can’t follow directions, so they may be very hard to discipline.” This is discouraging, non-therapeutic, and untrue. Children with developmental disabilities can follow directions with structure, patience, and consistency.
C. “Punish your child only for socially unacceptable or offending behaviors.” Discipline should focus on teaching, guiding, and reinforcing positive behavior, not solely punishment. Limiting discipline to punishment misses the opportunity for positive reinforcement and skill development.
D. “Spanking works well for this type of child, as they really don’t like pain.” Corporal punishment is inappropriate and harmful. It does not teach desired behaviors, may cause fear or aggression, and is not recommended in pediatric nursing practice.
Take home points
- Discipline for children with developmental disabilities should be consistent, individualized, and value-based.
- Positive reinforcement, clear expectations, and patience are more effective than punishment.
- Nurses should empower and support parents with strategies that respect both the child’s abilities and the family’s beliefs.
- Corporal punishment is never an appropriate recommendation in pediatric nursing.
A nurse, who is caring for a chronically ill 6-year-old child in a long-term care facility, has identified
Explanation
A chronically ill child demonstrating detachment behaviors may appear indifferent to the parents, show minimal distress upon separation, or redirect attachment to caregivers such as nurses. This behavior reflects ineffective coping, often seen when the child has experienced prolonged hospitalizations or repeated separations from parents.
Rationale for correct answer:
C. Hugging the nurse and ignoring the parents indicates detachment. Instead of showing distress or seeking comfort from parents, the child transfers attachment to the nurse and minimizes interaction with the parents. This is a maladaptive coping response to prolonged separation and hospitalization.
Rationale for incorrect answers:
A. Crying and begging the parents to stay represents separation anxiety, not detachment. It reflects active emotional attachment and protest.
B. Waving good bye and asking the parents when they would return is a healthy coping behavior, showing trust and security in the parents’ return. It is not detachment.
D. Grabbing the legs of the parents and refusing to let them go reflects protest behavior, not detachment. The child is still strongly attached and resists separation.
Take home points
- Detachment behaviors occur when a child adapts to repeated separation by withdrawing emotional connection from parents and attaching to others.
- This indicates ineffective coping and requires interventions to support parent-child bonding.
- Nurses should encourage frequent parental involvement and provide opportunities for positive interactions.
- Distinguishing between protest, despair, and detachment phases of separation anxiety is key in pediatric nursing.
A mother comments to a nurse working on the pediatric unit, “My second child just does not seem to be acting like or responding the same way as my first child.” Nursing interventions to respond to this inquiry should include which of the following? Select all that apply
Explanation
When a parent expresses concern that their child is not acting like or responding the same as a sibling, the nurse should perform a thorough developmental assessment while also supporting the parent emotionally. The focus is on assessing possible developmental issues while reassuring the parent appropriately.
Rationale for correct answers:
A. Assessment for dysmorphic syndromes is important if developmental differences are noted. Conditions such as congenital anomalies or microcephaly may underlie developmental delays.
B. Inquiring about temperament such as irritability and lethargy helps identify possible neurological, metabolic, or developmental issues influencing the child’s behavior.
C. Explaining that all children are different is key for parental reassurance. Comparison with siblings can create unnecessary anxiety or pressure; each child develops uniquely.
D. Noting language development appropriate for the child’s age is a standard part of developmental assessment and can reveal early indicators of delays or disorders.
Rationale for incorrect answer:
E. Meeting siblings to assess similarities is not necessary for evaluating developmental differences. Assessment should be focused on the individual child’s growth and milestones, not comparisons to family traits.
Take home points
- Parental concerns about differences between siblings should always be taken seriously.
- A thorough developmental assessment such as growth, language, behavior, and neurological signs is essential.
- Normalize differences while carefully evaluating for potential disorders.
- Avoid direct sibling comparisons, each child has unique developmental patterns.
When interacting with a parent at her child’s well visit, which statement by the mother would be an indication for a speech referral? Select all that apply
Explanation
Speech and language milestones are critical indicators of a child’s development. Certain delays or persistent speech difficulties are red flags that warrant referral for a speech and language evaluation.
Rationale for correct answers:
A. Failure to speak any meaningful words at 2 years old is a developmental red flag. By this age, children should be using several single words spontaneously. Lack of expressive language warrants referral.
C. Failure to use sentences of three or more words by 3 years old indicates a possible expressive language delay. Most 3-year-olds should be able to form short, understandable sentences.
D. Stuttering or dysfluency can be normal in preschoolers (ages 2–5), especially during language bursts. However, persistent or significant dysfluency (such as repeating sounds, words, or phrases) can indicate a need for evaluation.
E. Frequent omission of final consonants in a 3-year-old is concerning. While some articulation errors are normal, consistent omission of final consonants after age 3 is not developmentally appropriate.
Rationale for incorrect answers:
B. Using different words or nicknames for people is typical of normal language development and shows creativity in communication.
E. Omission of word endings such as plurals or verb tenses may still be developmentally normal at 3 years old. Many children master these grammatical rules closer to age D.
Take home points
- By age 2: Child should use at least 50 words and begin combining words.
- By age 3: Child should form 3–4 word sentences and be mostly understandable to familiar listeners.
- Speech referral red flags: no meaningful words at 2, no short sentences at 3, and persistent articulation errors (e.g., omitting final consonants).
- Some errors (stuttering, word endings) are developmentally normal at 3 years.
A baby with trisomy 21 is admitted to the newborn nursery. The baby should be assessed for which of
Explanation
Down syndrome is a genetic condition caused by the presence of an extra copy of chromosome 21, which is why it's also called trisomy 2A. This additional genetic material affects how the body and brain develop, leading to a range of physical, cognitive, and developmental differences.
Rationale for correct answer:
A. A single transverse palmar crease is a common finding in infants with Down syndrome. While it can also appear in healthy infants, its presence along with other physical characteristics supports the diagnosis of trisomy 2A.
Rationale for incorrect answers:
B. The presence of extra digits is associated more with trisomy 13 (Patau syndrome), not trisomy 2A.
C. A transient skin color change (half red, half pale) due to immature blood vessel regulation in newborns. It is a benign and temporary finding, not specific to Down syndrome.
D. Benign bluish pigmentation commonly found on the sacral area of infants with darker skin tones. These are unrelated to chromosomal abnormalities.
Take home points
- Simian crease is a key physical finding in Down syndrome, though not diagnostic on its own.
- Other common Down syndrome features: hypotonia, upslanting palpebral fissures, epicanthal folds, flat nasal bridge, and small ears.
- Distinguish Down syndrome features from findings related to other syndromes (e.g., polydactyly in trisomy 13).
- Early recognition allows prompt evaluation for associated conditions (e.g., congenital heart disease, GI anomalies).
A nurse suspects that a newly delivered baby has Down syndrome. The nurse noted that the baby
exhibited which of the following physiological characteristics? Select all that apply
Explanation
Down syndrome is a genetic condition caused by the presence of an extra copy of chromosome 21, which is why it's also called trisomy 2A. This additional genetic material affects how the body and brain develop, leading to a range of physical, cognitive, and developmental differences.
Rationale for correct answers:
B. Protruding tongue is common in infants with Down syndrome, often due to hypotonia and a relatively small oral cavity.
D. Wide, flat nasal bridge is a typical facial characteristic of Down syndrome, helping distinguish craniofacial appearance in affected infants.
Rationale for incorrect answers:
A. Elongated face is not characteristic of Down syndrome. It is more commonly seen in conditions like Marfan syndrome.
C. Infants with Down syndrome typically have small, low-set ears, not large or high-set.
E. Asymmetric Moro reflex usually suggests birth injury such as brachial plexus injury or clavicle fracture rather than Down syndrome.
Take home points
- Classic Down syndrome features in newborns include: hypotonia, protruding tongue, wide flat nasal bridge, small ears, simian crease, and upslanting palpebral fissures.
- Differentiating features are important because other syndromes (e.g., trisomy 13 or 18, Marfan syndrome) have distinct facial/physical characteristics.
- Early recognition allows timely screening for associated conditions such as congenital heart disease, GI anomalies, and thyroid dysfunction.
A nurse working in a preschool has just been advised that a toddler with fragile X syndrome has been admitted to the school. The nurse should advise the teacher that the child may exhibit which of the following characteristics?
Explanation
Fragile X Syndrome (FXS) is caused by a mutation in the FMR1 gene on the X chromosome, which normally produces a protein (FMRP) essential for brain development. In FXS, this gene is either silenced or doesn’t produce enough of the protein, leading to developmental challenges.
Rationale for correct answer:
B. Aggressive behavior is common in fragile X syndrome. Children may exhibit aggression toward themselves or others, often triggered by stress, overstimulation, or difficulty with communication. This is a key behavioral manifestation educators and nurses should anticipate.
Rationale for incorrect answers:
A. Lordotic posturing is not a typical finding. Lordosis is more associated with musculoskeletal or spinal conditions.
C. Two different eye colors is called heterochromia, which is unrelated to fragile X syndrome.
D. Asynchronous breathing is not associated with fragile X. Breathing irregularities are not part of the syndrome’s typical manifestations.
Take home points
- Fragile X syndrome is the most common inherited cause of intellectual disability.
- Key features include: intellectual disability, speech and developmental delays, social anxiety, hyperactivity, and behavioral issues including aggression.
- Physical features may include a long face, large ears, and macroorchidism (after puberty).
- Nurses and teachers should be prepared to implement behavioral support strategies and foster structured, low-stress environments.
A child has been diagnosed with fragile X syndrome. The nurse would predict that the child may exhibit which of the following signs/symptoms?
Explanation
Fragile X Syndrome (FXS) is caused by a mutation in the FMR1 gene on the X chromosome, which normally produces a protein (FMRP) essential for brain development. In FXS, this gene is either silenced or doesn’t produce enough of the protein, leading to developmental challenges.
Rationale for correct answer:
B. Arm flapping is a common behavioral feature of fragile X syndrome, often triggered by excitement, stress, or overstimulation. It reflects the syndrome’s link to autistic-like behaviors and sensory processing challenges.
Rationale for incorrect answers:
A. Strabismus may occur in many children but is not a defining or common feature of fragile X syndrome.
C. Vision deficit is not a hallmark feature of fragile X. Visual problems can occur in any child but are not specifically linked to this condition.
D. Nevus flammeus, also known as a “port-wine stain,” this is a vascular birthmark unrelated to fragile X syndrome.
Take home points
- Fragile X syndrome features include: intellectual disability, speech/language delay, autistic-like behaviors (hand flapping, poor eye contact), hyperactivity, anxiety, and sometimes aggression.
- Physical features may include long face, large protruding ears, and (post-puberty) macroorchidism.
- Behavioral manifestations (such as arm flapping) are often the most noticeable signs in childhood and affect learning and social integration.
- Early intervention with speech therapy, occupational therapy, and behavioral support is critical.
A school nurse suspects that a 5-year-old child has autism spectrum disorder. The nurse’s suspicion is based on which of the following observations? The nurse noted that the child: Select all that apply
Explanation
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition that affects how a person communicates, interacts socially, and processes sensory information. The term “spectrum” reflects the wide range of symptoms, abilities, and challenges that individuals with autism may experience.
Rationale for correct answers:
A. Has yet to learn his colors or the names of animals: Language and developmental delays are common in children with autism spectrum disorder (ASD). Difficulty with basic learning tasks is often an early sign.
B. Becomes upset each time the teacher asks the child to stop what he is doing: Children with ASD often show resistance to change or transitions, and may have difficulty stopping repetitive or preferred activities.
E. Covers his ears whenever the school principal makes an announcement on the loud speaker: Many children with ASD have sensory sensitivities such as hypersensitivity to sounds, lights, or textures.
Rationale for incorrect answers:
C. Is the first in line when it is time to go out to play in the playground: This behavior is normal enthusiasm for play, not an indicator of autism.
D. Runs to the teacher to get a kiss whenever he gets hurt while playing: Children with ASD often have difficulty with social reciprocity and seeking comfort from others. Running for a kiss when hurt indicates appropriate social/emotional response, not autism.
Take home points
- Key features of autism spectrum disorder include:
- Communication difficulties (speech delay, trouble naming objects, poor eye contact).
- Repetitive or restrictive behaviors (rigid routines, upset with change).
- Sensory sensitivities (covering ears, avoiding textures).
- Impairment in social reciprocity (not usually seeking comfort, trouble forming peer relationships).
A 9-year-old child with autism spectrum disorder has been admitted to the hospital. Which of the
following interventions is important for the nurse to perform during the child’s stay?
Explanation
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition that affects how a person communicates, interacts socially, and processes sensory information. The term “spectrum” reflects the wide range of symptoms, abilities, and challenges that individuals with autism may experience.
Rationale for correct answer:
A. Children with autism spectrum disorder (ASD) thrive on structure, predictability, and routine. A strict, consistent schedule for treatments, meals, and daily care reduces anxiety and behavioral outbursts. Sudden changes can be very distressing for children with ASD.
Rationale for Incorrect Answers:
B. Children with ASD may have difficulty with social interactions and overstimulation in busy playrooms. Play therapy can be helpful, but it should be individualized and not forced.
C. Keeping all of the room lights on throughout the night is not appropriate; it may worsen sleep disturbances is already common in autism and cause sensory overload.
D. Providing the child with sugar-free juice at snack time is not specific to autism management. Unless the child has diabetes or dental concerns, this intervention is not related to autism care.
Take home points
- Nursing care for children with autism should prioritize:
- Consistency and routine in care.
- Minimizing sensory overload (noise, light, crowds).
- Respecting communication styles (use of pictures, simple words, or devices).
- Creating a safe, structured environment to reduce anxiety.
As the nurse caring for a culturally diverse population, it is important to understand cultural health beliefs of families. This can best be accomplished by:
Explanation
When caring for culturally diverse families, the nurse’s priority is to understand the parents’ perception of the illness or disability. This approach acknowledges their beliefs, values, and concerns, allowing the nurse to provide culturally sensitive care while building trust.
Rationale for correct answer:
C. By exploring the parents’ perceptions, concerns, and worries, the nurse gains insight into how the family views the illness, its seriousness, and how they believe it should be managed. This facilitates individualized, culturally competent care and promotes collaboration.
Rationale for incorrect answers:
A. Asking about the extended family’s views may provide some information, but it does not directly address the parents’ own beliefs and perceptions, which are essential for guiding care.
B. Exploring alternative therapies is important but comes after understanding the family’s overall view of the illness. It is one aspect of cultural care, not the starting point.
D. Acknowledging language barriers is necessary, but it does not justify health care professionals making decisions without family input. Professional interpreters should be used to ensure communication and respect for family values.
Take home points
- The first step is to understand the family’s own perception of the illness/disability.
- Cultural competence means listening, respecting, and integrating beliefs into care when safe and possible.
- Extended family input and alternative therapies can be explored after building understanding.
- Use interpreters, not assumptions, to overcome language barriers and support shared decision-making.
Lessons
- Objectives
- Introduction
- Impact of chronic illness, disability, or end-of-life care for the child and family
- Practice Exercise 1
- Cognitive impairement in children
- Practice Exercise 2
- Sensory impairment in children
- Communication impairment in children
- Practice Exercise 3
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Analyze the impact of chronic illness and disability on the family’s developmental trajectory and coping mechanisms.
- Define the principles of palliative care and the nurse’s role in managing terminal illness in childhood.
- Discuss the ethical and legal considerations surrounding end-of-life decisions, including advance directives and organ donation.
- Develop a nursing care plan that addresses the specific physical and social needs of children with Down syndrome and fragile X syndrome.
- Identify assessment techniques and interventions for children with varying degrees of hearing and visual impairments.
- Compare the behavioral and communication strategies used to support children with autism spectrum disorder (ASD).
- Synthesize the components of bereavement care for families experiencing the loss of a child.
- Apply the principles of family-centered care to a multidisciplinary approach for children with complex healthcare requirements.
Introduction
- Family-centered care is an innovative and foundational philosophy that serves as the cornerstone of pediatric nursing.
- It's not just a set of guidelines, but a deep-seated belief system that recognizes the family as the constant in a child’s life, while the healthcare providers and medical conditions are in flux.
- This model moves beyond the traditional disease-focused approach, where care is delivered primarily by medical professionals, to a collaborative partnership among the healthcare team, the child, and the family.
- In the context of a child with a special need, whether it's a chronic illness, a disability, or a life-limiting condition, this philosophy becomes even more critical.
- These are situations where the child and family will be navigating the healthcare system for years, if not a lifetime. Therefore, care must be tailored not only to the child's medical needs but also to the family’s unique values, strengths, and daily realities.
- The goal of family-centered care is to empower families to be active, informed decision-makers, ensuring that care is not just medically sound but also respectful of their beliefs and cultural background.
- This partnership enhances the child’s health and overall well-being by fostering a sense of control and resilience within the family unit.
- The essence of family-centered care is to create a seamless, supportive, and compassionate environment where the child can thrive and the family can cope, knowing they are a vital and respected part of the care team.
- It's about seeing the child not just as a patient but as a unique individual within the loving context of their family.
Impact of chronic illness, disability, or end-of-life care for the child and family
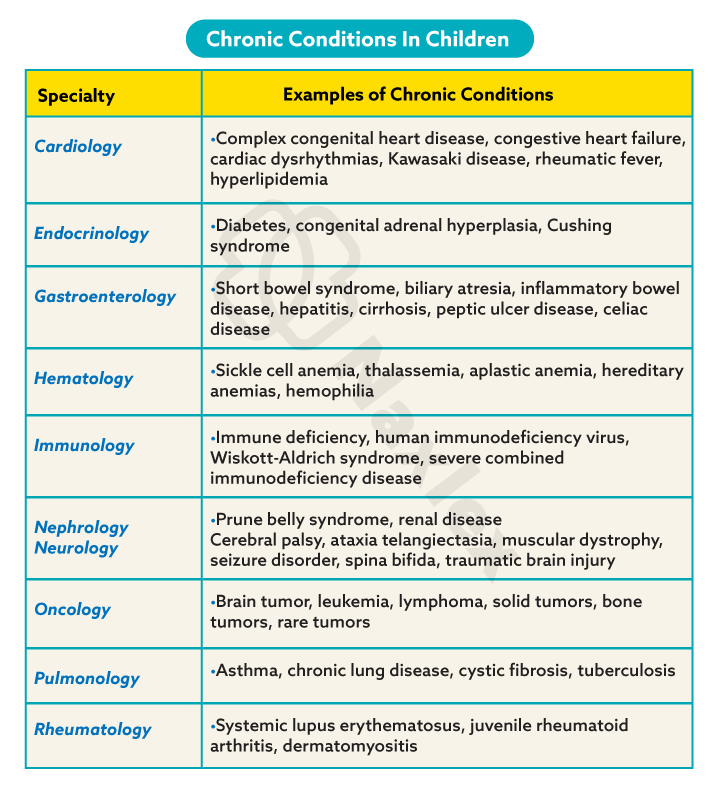
Chronic or complex conditions are those that last at least 12 months and may require ongoing medical care. These conditions have a profound and lasting impact on the child and their family, requiring a shift in lifestyle, emotional management, and long-term planning.
3.1. Perspectives on the Care of Children and Families Living With or Dying From Chronic or Complex Diseases
- The experience is highly individualized but often includes a rollercoaster of emotions. Families may feel overwhelmed, isolated, or misunderstood. The healthcare perspective has evolved from a disease-centric model to a holistic, family-centered approach.
- This shift acknowledges that the family’s well-being is integral to the child’s outcome. Care is focused on optimizing the child’s quality of life, promoting normalcy, and supporting the family's ability to cope.
3.2. The Family of the Child With a Chronic or Complex Condition
Impact of the Child's Chronic Illness
- A chronic illness can create significant financial strain, as families face costs for medical equipment, therapies, and lost wages. Social isolation can occur due to frequent hospitalizations or the child's inability to participate in typical social activities. The family's dynamics often change, with parents becoming primary caregivers, and siblings sometimes feeling neglected or resentful.
Coping with Ongoing Stress and Periodic Crises
- Families must develop long-term coping strategies. They face ongoing stress from daily care routines, medication schedules, and managing symptoms. Periodic crises (e.g., flare-ups, new diagnoses) can be particularly stressful, requiring immediate adaptation and decision-making. Effective coping includes seeking information, building support networks, and maintaining a sense of hope.
Assisting Family Members in Managing Their Feelings
- Nurses play a crucial role in helping families manage feelings of grief, anger, guilt, and anxiety. This involves active listening, validating their emotions, and providing a safe space to express their fears. Nurses should encourage parents to seek counseling or support groups and remind them that their feelings are valid.
Establishing a Support System
A strong support system is vital. This can include:
- Formal Support: Healthcare professionals, social workers, therapists, and support groups.
- Informal Support: Friends, family, and community groups. Nurses should facilitate connections to these resources, helping families build a network that can provide emotional, practical, and financial support.
3.3. The Child With a Chronic or Complex Condition
Developmental Aspects
Chronic illness can disrupt a child’s normal development.
- Infants: May struggle to form secure attachments due to frequent hospitalizations.
- Toddlers: May experience delays in autonomy as parents are forced to be overly protective.
- Preschoolers: May feel guilt or shame, believing they are responsible for their illness.
- School-Age Children: May feel different from peers, leading to social isolation and poor self-esteem.
- Adolescents: May struggle with identity formation, independence, and body image issues.
Coping Mechanisms
Children use various coping strategies:
- Regression: Reverting to earlier behaviors such as thumb-sucking.
- Fantasy/Play: Using imagination to process their feelings.
- Denial: Ignoring or minimizing the illness's impact.
- Information-Seeking: Learning about their condition to feel a sense of control.
- Support-Seeking: Turning to family, friends, or other children with similar conditions.
3.4. Nursing Care of the Family and Child With a Chronic or Complex Condition
Assessment
- Comprehensive Assessment: Go beyond the physical symptoms to include psychosocial, developmental, and family assessments.
- Family Strengths and Needs: Identify the family's current coping strategies, resources, and areas where they need support.
- Child's Understanding: Assess the child's developmental level and their perception of the illness.
Provide Support at the Time of Diagnosis
- Honest Communication: Deliver information clearly and compassionately.
- Emotional Support: Allow time for the family to process the news and express their feelings.
- Connect to Resources: Immediately provide information on support groups, social services, and relevant organizations.
Support the Family's Coping Methods
- Validate Feelings: Acknowledge the family's grief and stress.
- Empowerment: Encourage the family to be active participants in the child's care and decision-making.
- Problem-Solving: Help families identify and implement effective coping strategies.
Educate About the Disorder and General Health Care
- Disease-Specific Education: Teach families about the condition, treatment plans, and potential complications.
- Medication Management: Ensure they understand medication schedules, dosages, and side effects.
- Emergency Preparedness: Train them on how to handle crises and when to seek emergency care.
Promote Normal Development
- Normalization: Encourage routines and activities that mimic those of healthy peers (e.g., attending school, playing sports, having sleepovers).
- Advocate for the Child: Ensure school and community environments are inclusive and accommodating.
- Developmental Milestones: Focus on achievable milestones and celebrate small victories.
Establish Realistic Future Goals
- Collaborative Goal-Setting: Work with the family and child to set attainable short-term and long-term goals.
- Focus on Quality of Life: The primary goal should be to enhance the child's quality of life and promote happiness and well-being.
3.5. Palliative Care in Childhood Terminal Illness
Palliative care is a specialized form of medical care for individuals with serious illnesses. It focuses on providing relief from the symptoms, pain, and stress of the illness, with the goal of improving the quality of life for both the patient and the family.
Scope of the Problem
Many children live with life-limiting illnesses, such as certain genetic disorders, congenital anomalies, or advanced cancers. Palliative care is not just for the final days but can be introduced at the time of diagnosis and provided alongside curative treatments.
Principles of Palliative Care
- Holistic Approach: Addresses physical, psychological, social, and spiritual needs.
- Affirmation of Life: Views dying as a normal process.
- Neither Hastens Nor Postpones Death: Aims to provide comfort, not to shorten or prolong life unnecessarily.
- Family-Centered: The family is a unit of care and is supported throughout the process and after the child's death.
Goals of Care
- Pain and Symptom Management: Aggressively manage pain, nausea, and other distressing symptoms.
- Comfort: Keep the child as comfortable as possible.
- Emotional and Spiritual Support: Provide counseling, emotional support, and spiritual guidance.
- Quality of Life: Enhance the child’s quality of life, allowing them to participate in meaningful activities for as long as possible.
Awareness of Dying in Children with Life-Threatening Illness
Children, even very young ones, often have an innate understanding of their condition. Their awareness is often expressed through symbolic play, questions, or nonverbal cues. It's crucial for nurses to be attuned to these cues and to communicate honestly and at a developmentally appropriate level.
Children's Understanding of and Reactions to Dying
- Infants/Toddlers: No concept of death. React to separation and changes in routine.
- Preschoolers: See death as temporary or reversible. May believe they are responsible for the death.
- School-Age Children: Begin to understand that death is permanent and universal. May personify death as a "boogeyman."
- Adolescents: Have a mature understanding of death but may feel invincible or angry. They are concerned with loss of control and independence.
Delivery of Palliative Care Services
Palliative care can be provided in various settings:
- Hospital: Inpatient units or palliative care teams.
- Home: Hospice care services that bring care to the home.
- Hospice Facilities: Specialized centers for end-of-life care.
3.6. Nursing Care of the Child and Family at the End of Life
Management of Pain and Suffering
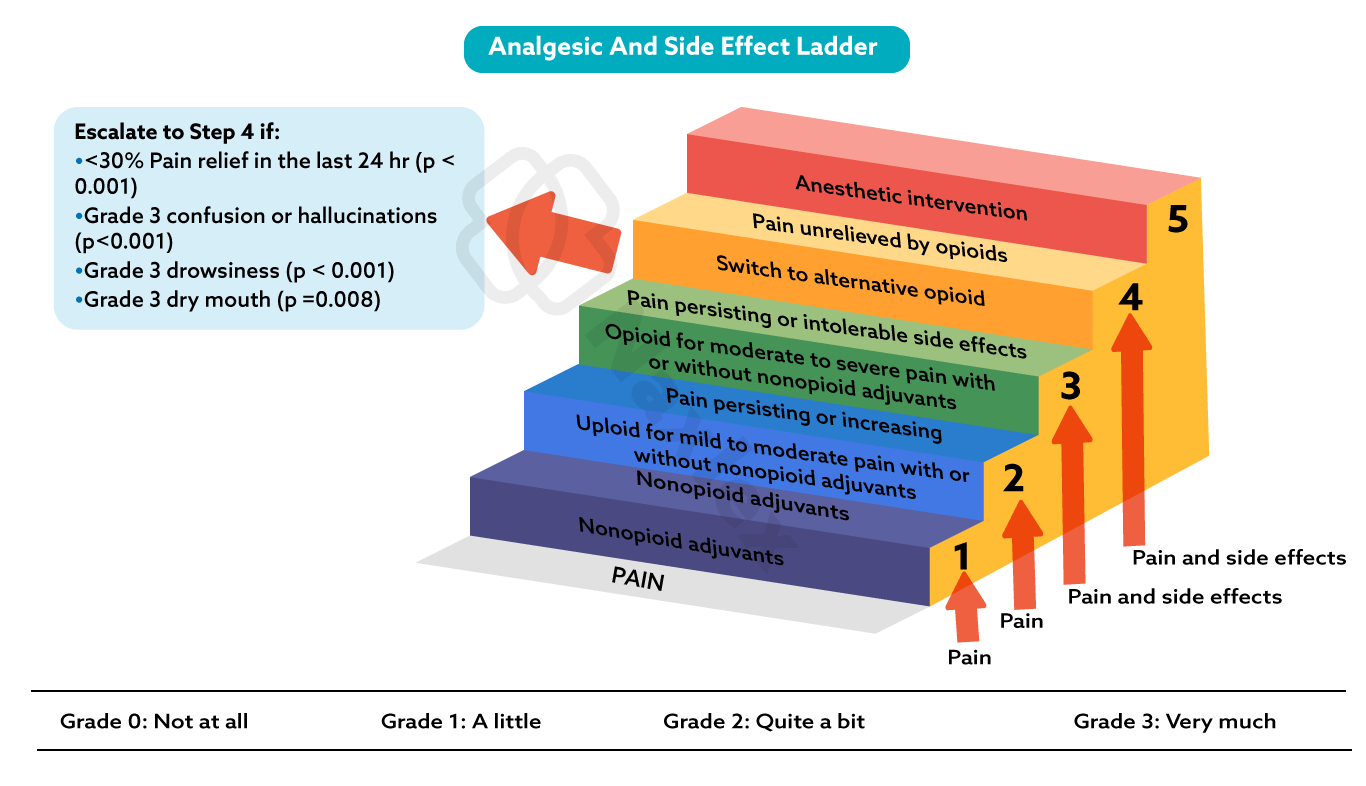
- Pharmacological: Give pain control for children in the terminal stages of illness or injury the highest priority. Despite ongoing efforts to educate physicians and nurses on pain management strategies in children, studies have reported that children continue to be undermedicated for their pain. Nearly all children experience some amount of pain in the terminal phase of their illness.
- The current standard for treating children’s pain is according to the World Health Organization’s analgesic and side-effect stepladder that takes into account the intolerable side effects of opioids. This approach promotes individualizing the pain intervention to children’s level of reported pain. Children’s pain is assessed frequently, and medications are adjusted as necessary. Pain medications are given on a regular schedule, and extra doses for breakthrough pain are available to maintain comfort. Opioid drugs such as morphine are given for severe pain, and the dosage is increased as necessary to maintain optimum pain relief.
- Occasionally children require very high doses of opioids to control pain. This may occur for several reasons. The child on long-term opioid pain management can become tolerant of the drug, so more drug must be given to maintain the same level of pain relief. This is not to be confused with addiction, which is a psychologic dependence on the side effects of opioids. Addiction is not a factor in managing terminal pain in a child, and the nurse plays an important role in educating parents that their child will not become addicted.
- Other reasons for increasing dosages of opioids include progression of disease and other physiologic causes of pain. It is important to understand that there is no maximum dosage that can be given to control pain. However, nurses often express concern that administering dosages of opioids that exceed those with which they are familiar will hasten the child’s death. The principle of double effect addresses such concerns. It provides an ethical standard that supports the use of interventions that have the intention of relieving pain and suffering even though there is a foreseeable possibility that death may be hastened. In cases in which the child is terminally ill and in severe pain, using large doses of opioids and sedatives to manage pain is justified when no other treatment options are available that would relieve the pain but make the possibility of death less likely.
- Non-Pharmacological: Use comfort measures like massage, music therapy, aromatherapy, and therapeutic touch.
Parents' and Siblings' Need for Education and Support Through the Caregiving Process
- Empower Parents: Teach parents how to administer medications and provide comfort measures.
- Sibling Support: Acknowledge and address the siblings' feelings. Involve them in age-appropriate ways and provide resources like grief counseling for children.
Care at the Time of Death
- Creating a Sacred Space: Ensure the room is quiet and private. Allow the family to be present and to hold the child.
- Comforting the Family: Provide a gentle presence, offer a quiet cup of tea, and ask what they need.
Postmortem Care
- Respectful Care: Provide meticulous, respectful care for the body. Clean the body, dress the child in their own clothes, and remove medical equipment.
- Privacy: Ensure the family has private time with the child.
Care of the Family Experiencing Unexpected Childhood Death
Unexpected death such as sudden infant death syndrome (SIDS) and accidents is particularly traumatic. Nurses must be a calm, supportive presence, providing clear information and connecting the family with grief resources and support systems immediately.
3.7. Special Decisions at the Time of Dying and Death
Right to Die and Do-Not-Attempt Resuscitation (DNAR) Orders
- Ethical Considerations: These are complex decisions that require open communication between the family, child (if appropriate), and healthcare team.
- Legal Framework: DNAR orders must be legally documented and respect the child's and family's wishes.
Viewing of the Body
- Psychological Benefits: Viewing the body can help families achieve a sense of closure and begin the grieving process.
- Preparation: Prepare the family for what they will see. Ensure the child's appearance is as peaceful as possible.
Organ or Tissue Donation and Autopsy
- Discuss these options with extreme sensitivity and respect. Written consent from the family is required before donation can proceed. When requests for organ donation are made, health care practitioners must address common misunderstandings families have about brain death and organ donation. Provide clear, factual information about the process and purpose.
Siblings' Attendance at Funeral Services
- One of the most frequent concerns of parents is whether young or school-age children should attend funeral or burial services. Sharing moments of deep significance with parents helps children understand the experience and deal with their own feelings, and depriving them of this opportunity may leave children with lifelong regrets. However, a child should never be forced to attend a postdeath service.
- Children need preparation for postdeath services. They should be told what to expect, particularly how the deceased person will look if the coffin is open. Ideally a parent explains the details to the child. If the parent’s grief prevents this communication, a significant family member or friend should substitute.
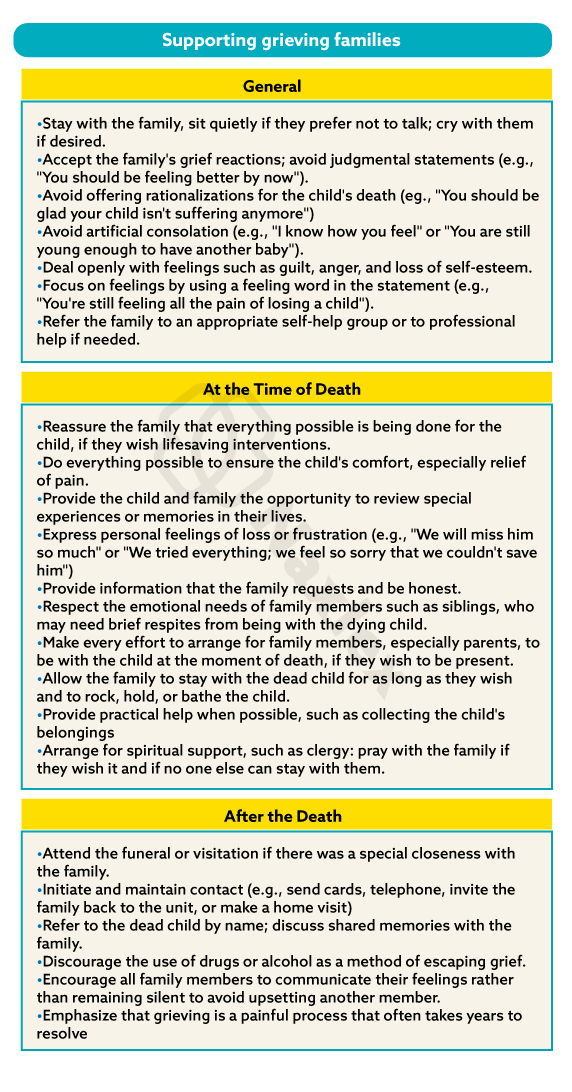
3.8. Care of the Grieving Family
Grief, Mourning, and Bereavement Programs
- Grief: The internal emotional response to loss.
- Mourning: The external, social expression of grief.
- Bereavement: The state of having suffered a loss.
- Bereavement Programs: Hospitals often have programs that offer follow-up support, support groups, and counseling for months or even years after the death.
3.9. The Nurse and the Child With Life-Threatening Illness
Nurses' Reaction to Caring for Children With Life-Threatening Illnesses
Caring for a dying child is emotionally and physically draining. Nurses may experience compassion fatigue, burnout, and secondary traumatic stress. It is a profound loss for the nurse as well.
Coping with Stress
- Self-Care: Nurses must prioritize their own mental and emotional health.
- Debriefing: Participate in formal debriefing sessions with colleagues to process feelings.
- Peer Support: Rely on colleagues who understand the unique challenges of pediatric palliative care.
Cognitive impairement in children
Cognitive impairment (CI), also known as intellectual disability, refers to a significant limitation in intellectual functioning and adaptive behavior. It can range from mild to profound and can be caused by various factors, including genetics, brain injury, or environmental factors. The impact on the child includes delays in communication, learning, and self-care. The family often faces challenges in education, daily care, and social integration.
5.1. Nursing Care of Children With Impaired Cognitive Function
5.1.1. Down Syndrome
- Caused by an extra copy of chromosome 21 (trisomy 21).

- Although children with trisomy 21 are born to parents of all ages, there is a statistically greater risk in older women, particularly those older than 35 years of age. For example, in women 35 years old, the chance of conceiving a child with Down syndrome is about 1 in 350 live births; but in women 40 years old, it is about 1 in 100. However, the majority (approximately 80%) of infants with Down syndrome are born to women younger than 35 years old because younger women have higher fertility rates.
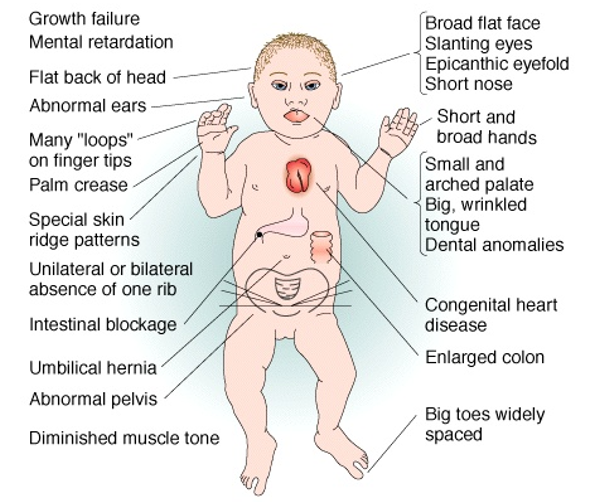
Physical Features
- Facial features: A flattened facial profile, a small nose, and upward-slanted eyes.
- Ears and mouth: Small ears and a small mouth, which can make the tongue appear larger.
- Neck and hands: A short neck and small hands with a single crease across the palm, known as a simian crease.
- Muscle tone: Low muscle tone (hypotonia), which can affect physical development.
- Height: Shorter stature compared to peers.
Developmental and Health Concerns
- Cognitive development: Individuals with Down syndrome have some degree of cognitive impairment, ranging from mild to moderate. This can affect learning, problem-solving, and speech development.
- Congenital heart defects: About half of all babies with Down syndrome are born with a heart defect, some of which require surgery early in life.
- Hearing and vision problems: People with Down syndrome are at a higher risk for hearing loss and vision problems like cataracts.
- Gastrointestinal issues: Conditions such as celiac disease and other digestive problems are more common.
- Increased risk of other conditions: Individuals with Down syndrome have a higher risk of developing conditions such as leukemia, thyroid disease, and obstructive sleep apnea.
Diagnosis and Management
Diagnosis
Down syndrome can be diagnosed during pregnancy through prenatal screening and diagnostic tests or after birth through a karyotype test.
- Prenatal Screening: These tests, such as blood tests and ultrasounds, estimate the probability of a baby having Down syndrome.
- Prenatal Diagnostic Tests: These include chorionic villus sampling (CVS) and amniocentesis, which analyze a sample of the placenta or amniotic fluid, respectively, to confirm the presence of an extra chromosome 21.
- Postnatal Karyotype Test: A blood sample from the newborn is analyzed to count the number of chromosomes and confirm the diagnosis.
Management
There is no cure for Down syndrome, but early intervention and ongoing medical care can significantly improve the quality of life for individuals with the condition.
- Early Intervention: Programs that include physical therapy, speech therapy, and occupational therapy can help children with Down syndrome develop motor skills, communication abilities, and self-care skills.
- Medical Care: Regular check-ups are essential to monitor for and manage associated health issues like heart defects, hearing loss, and thyroid problems.
- Education: Children with Down syndrome often benefit from specialized educational support and inclusive classroom settings.
- Community Support: Support groups and advocacy organizations play a crucial role in providing resources and promoting the inclusion of people with Down syndrome in society.
Assisting the Family in Preventing Physical Problems
- Many of the physical characteristics of infants with Down syndrome present challenges and nursing problems. The hypotonicity of muscles and hyperextensibility of joints complicate positioning. The limp, flaccid extremities resemble the posture of a rag doll; as a result, holding the infant is difficult and cumbersome. Sometimes parents perceive this lack of the infant’s molding to their bodies as evidence of inadequate parenting.
- The extended body position promotes heat loss because more surface area is exposed to the environment. Encourage the parents to swaddle or wrap the infant snugly in a blanket before picking up the child to provide security and warmth. The nurse should discuss with parents their feelings concerning attachment to the child, emphasizing that the child’s lack of clinging or molding is a physical characteristic and not a sign of detachment or rejection.
- Decreased muscle tone compromises respiratory expansion. In addition, the underdeveloped nasal bone causes a chronic problem of inadequate drainage of mucus. The constant stuffy nose forces the child to breathe by mouth, which dries the oropharyngeal membranes, increasing the susceptibility to upper respiratory tract infections. Measures to lessen these problems include clearing the nose with a bulb-type syringe, rinsing the mouth with water after feedings, increasing fluid intake, and using a cool-mist vaporizer to keep the mucous membranes moist and the secretions liquefied.
- Other helpful measures include changing the child’s position frequently, practicing good hand washing, and properly disposing of soiled articles, such as tissues. If antibiotics are ordered, the nurse stresses the importance of completing the full course of therapy for successful eradication of the infection and prevention of growth of resistant organisms.
- Inadequate drainage resulting in pooling of mucus in the nose also interferes with feeding. Because the child breathes by mouth, sucking for any length of time is difficult. When eating solids, the child may gag on the food because of mucus in the oropharynx. Parents are advised to clear the nose before each feeding; give small, frequent feedings; and allow opportunities for rest during mealtime.
- The protruding tongue also interferes with feeding, especially of solid foods. Parents need to know that the tongue thrust is not an indication of refusal to feed but a physiologic response. Parents are advised to use a small but long, straight-handled spoon to push the food toward the back and side of the mouth. If food is thrust out, it should be refed.
- Dietary intake needs supervision. Decreased muscle tone affects gastric motility, predisposing the child to constipation. Dietary measures, such as increased fiber and fluid evacuation. The child’s eating habits may need careful scrutiny to prevent obesity. Height and weight measurements should be obtained on a serial basis.
5.1.2. Fragile X Syndrome
- Cause: A genetic condition caused by a mutation on the X chromosome. It is the most common inherited cause of cognitive impairment. It is caused by a mutation in the FMR1 gene on the X chromosome, which normally produces the Fragile X Mental Retardation Protein (FMRP) essential for brain development. In FXS, this gene is either silenced or doesn’t produce enough of the protein, leading to developmental challenges. Males are often more severely affected than females.
Physical Features
- A long, narrow face.
- Large, prominent ears.
- A prominent jaw and forehead.
- Flexible joints.
- Flat feet.
- Enlarged testicles (macroorchidism) in post-pubertal males.
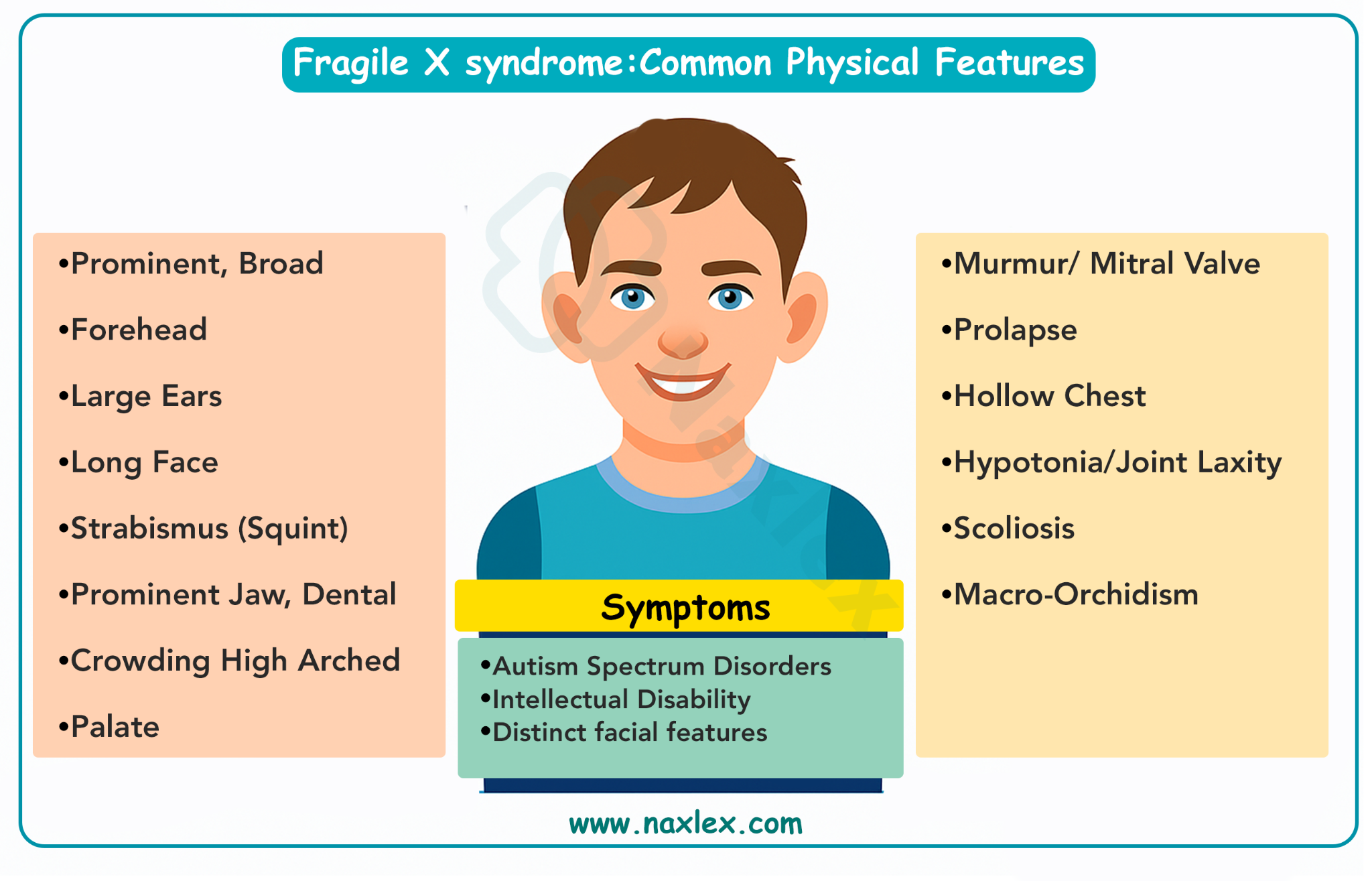
Developmental and Behavioral Characteristics
- Intellectual disability: The severity ranges from mild to moderate or severe.
- Developmental delays: Delays in reaching milestones like crawling, walking, and speaking are common.
- Behavioral challenges: Individuals may exhibit hyperactivity, anxiety, social avoidance, and poor eye contact.
- Autistic-like behaviors: Many with FXS show repetitive behaviors like hand-flapping and have sensory sensitivities to things like loud noises or bright lights.
- Speech and language difficulties: Problems with clear speech, stuttering, and repetitive speech are frequently observed.
Diagnosis and Treatment
There is no cure for Fragile X syndrome, but early and comprehensive intervention can make a significant difference in a person's life.
Diagnosis
A diagnosis is made through a genetic test, usually a blood test, which counts the number of CGG repeats in the FMR1 gene. This can be done prenatally or at any point after birth. Early diagnosis is key to starting supportive therapies as soon as possible.
Treatment
Management of FXS focuses on addressing the specific symptoms and providing support.
- Early Intervention: Therapies such as physical, speech, and occupational therapy help with developmental delays.
- Education: Tailored educational plans and support help individuals with learning difficulties.
- Behavioral Therapy: This can help manage behavioral issues like anxiety, hyperactivity, and social challenges.
- Medication: Medications may be used to treat co-occurring conditions, such as ADHD, anxiety, or seizures.
Sensory impairment in children
7.1. Hearing Impairment
Hearing impairment in children refers to a reduced ability to hear sounds, ranging from mild to profound. Early detection and intervention are crucial because a child's hearing ability is directly linked to their development of speech, language, and social skills.
Types and Causes
Hearing impairment in children is categorized into three main types based on where the problem occurs in the ear.
Types
- Conductive Hearing Loss: This type occurs when sound is blocked from reaching the inner ear. It often results from issues in the outer or middle ear. This can be temporary and is the most common type in children.
- Sensorineural Hearing Loss: This is a permanent form of hearing loss caused by damage to the inner ear (cochlea) or the auditory nerve. It can range from mild to profound.
- Mixed Hearing Loss: A combination of both conductive and sensorineural hearing loss.
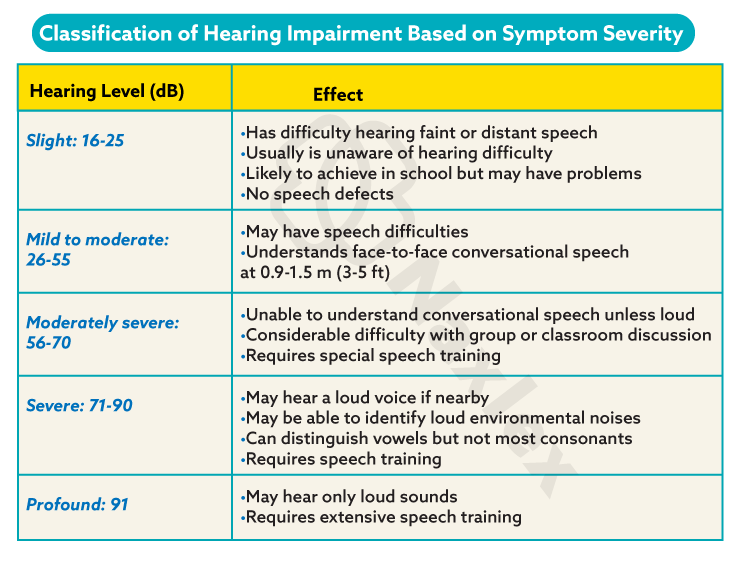
Causes
Causes can be categorized as congenital (present at birth) or acquired (developing after birth).
- Congenital:
- Genetic Factors: Responsible for more than half of congenital cases, often hereditary.
- Maternal Infections: Infections during pregnancy, such as rubella, cytomegalovirus (CMV), or herpes.
- Complications at Birth: Prematurity, low birth weight, or a lack of oxygen during delivery.
- Acquired:
- Chronic Ear Infections: Repeated middle ear infections, often leading to fluid buildup known as glue ear, are the number one cause of temporary hearing loss in children.
- Infections: Diseases like meningitis, measles, or mumps can cause permanent hearing loss.
- Head Trauma or exposure to loud noises.
Signs and Symptoms
Signs of hearing impairment can vary by age. The following are general indicators to watch for.
In Infants (Birth to 1 year)
- Doesn't startle or cry at loud noises.
- Doesn't turn their head toward a sound source by six months of age.
- Doesn't babble or try to imitate sounds.
In Toddlers and Children
- Delayed or unclear speech.
- Often says "huh?" or asks for things to be repeated.
- Doesn't follow directions.
- Turns up the volume of the TV or radio too high.
- Seems inattentive or doesn't respond when called from another room.
- Has difficulty locating where a sound is coming from.
- School performance declines.
Diagnosis and Management
Diagnosis
Early diagnosis is critical. Many newborns receive a hearing screening before leaving the hospital. If a child shows signs later, a full audiological evaluation is necessary.
- Newborn Screening: Tests like Otoacoustic Emissions (OAEs) or Auditory Brainstem Response (ABR) can be used on newborns while they're sleeping.
- Behavioral Audiometry: For older children, audiologists use age-appropriate methods like Visual Reinforcement Audiometry (rewarding head turns to sound) and Play Audiometry (having the child perform a task when they hear a sound).
Management
Treatment and intervention are tailored to the type and severity of hearing loss.
- Hearing Aids: These amplify sounds and are the most common solution for many types of permanent hearing loss.
- Cochlear Implants: A surgically implanted electronic device that provides a sense of sound for individuals with severe to profound sensorineural hearing loss.
- Medical Treatment: For conductive hearing loss, treatments like antibiotics for infections or ear tubes to drain fluid may be used.
- Therapies: Speech and language therapy is essential for all children with hearing impairment to support communication development. Additionally, a family may choose communication methods like sign language.
Nursing Insight:
-
- Early Detection: Advocate for newborn hearing screenings.
- Communication: Use sign language, lip-reading, and written communication.
- Technology: Educate families on the use of hearing aids, cochlear implants, and other assistive devices.
7.2. Visual Impairment
Visual impairment in children, which can include both low vision and blindness, is a significant health concern because a child's sight is critical for learning and development. Early detection and proper management can help them reach their full potential.
Types and Causes
Visual impairment can be caused by a variety of conditions that affect either the eye itself or the visual pathways in the brain.
Refractive Errors
These are the most common cause of vision problems in children and are often correctable with glasses. They occur when the eye doesn't properly focus light onto the retina.
- Myopia (Nearsightedness): Blurry distant vision.
- Hyperopia (Farsightedness): Blurry near vision.
- Astigmatism: Blurry vision at all distances due to an irregularly shaped cornea.
Other Eye Conditions
- Amblyopia (Lazy Eye): The most common cause of vision loss in children. It occurs when the brain and eye don't work together properly, leading to reduced vision in one eye. It can be caused by a misalignment of the eyes or an uncorrected refractive error.
- Strabismus (Crossed Eyes): A misalignment of the eyes that can lead to amblyopia if left untreated.
- Cataracts: Clouding of the eye's lens. While more common in adults, children can be born with them or develop them later.
- Retinopathy of Prematurity (ROP): An eye disorder that affects premature babies, causing abnormal growth of blood vessels in the retina.
Conditions Affecting the Brain
- Cortical Visual Impairment (CVI): This is a leading cause of permanent visual impairment in children in developed countries. It results from damage to the brain's visual pathways and is not an issue with the eyes themselves.
- Genetic Factors: Many inherited conditions, such as retinitis pigmentosa, can cause vision loss.
- Infections: Certain infections during pregnancy, like rubella or toxoplasmosis, can lead to vision problems.
Signs and Symptoms
Signs of a visual impairment can be subtle and may vary depending on the child's age. It's important for parents and caregivers to be vigilant.
- In Infants (Birth to 1 year):
- Not making eye contact or not following a moving object by 3-4 months.
- Constant eye rubbing or eye tearing.
- An eye that constantly turns inward or outward.
- A white or cloudy spot in the pupil.
- Extreme light sensitivity.
- In Older Children:
- Frequent squinting or tilting the head to see.
- Complaining of headaches or eye strain.
- Sitting too close to the TV or holding books very close to their face.
- Losing their place while reading or using a finger to track words.
- Seeming clumsy or bumping into objects.
Diagnosis and Management
Early diagnosis is crucial for the best outcomes.
Diagnosis
A child's vision is often screened by a pediatrician, but a comprehensive eye exam by a pediatric ophthalmologist or optometrist is the standard for diagnosis.
- Infants: An eye doctor can perform an exam by observing how the child's eyes fixate on and follow objects. They can also use specialized tests to check the retina and optic nerve.
- Older Children: Visual acuity is tested using charts with letters or symbols. The eye doctor will also check for eye alignment, focusing ability, and overall eye health.
Management
Treatment depends on the underlying cause.
- Corrective Lenses: Glasses or contact lenses are used to correct refractive errors.
- Patching or Atropine Drops: For amblyopia, a patch is placed over the stronger eye or drops are used to blur it, forcing the weaker eye to work harder.
- Surgery: May be required to correct conditions like cataracts or strabismus.
- Low Vision Aids: For children with permanent vision loss, specialists can provide tools like magnifiers, large-print books, or assistive technology to help them learn and function independently.
- Nursing Care:
- Safe Environment: Ensure the child’s environment is free of hazards.
- Sensory Stimulation: Encourage the use of other senses, such as touch and sound.
- Developmental Milestones: Explain how visual impairment may alter typical milestones (e.g., reaching for objects, crawling).
Communication impairment in children
Autism Spectrum Disorders (ASD)
- Autism Spectrum Disorder (ASD) is a complex neurodevelopmental disorder that affects how a person processes information and interacts with the world. The term "spectrum" reflects the wide range of symptoms, skills, and levels of impairment that can occur in people with ASD. No two people with autism are alike.
Core Characteristics
A diagnosis of ASD is based on two core sets of behaviors, as outlined in the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders):
- Deficits in Social Communication and Interaction: This includes difficulty with back-and-forth conversation, poor or inconsistent eye contact, and challenges understanding non-verbal cues like facial expressions and body language. They may also have trouble developing and maintaining relationships.
- Restricted, Repetitive Behaviors or Interests: These behaviors can include repetitive motor movements (like hand-flapping or rocking), a strong adherence to routines, and highly focused, sometimes obsessive, interests in specific topics or objects. Many people with ASD also have sensory sensitivities, being either over-responsive or under-responsive to stimuli like sounds, light, or textures.
Levels of Support
The DSM-5 classifies the severity of ASD into three levels based on the amount of support an individual needs. It's important to note that these levels can change over time with intervention.
- Level 1: Requiring Support. Individuals at this level may have noticeable impairments in social communication without support. They may have difficulty initiating social interactions and might seem to have a reduced interest in social activities. They can function independently in many areas of life, but their behaviors might cause significant interference.
- Level 2: Requiring Substantial Support. These individuals have marked deficits in both verbal and non-verbal communication, even with support. Their social impairments are obvious to others. They often have repetitive behaviors and a strong resistance to change that significantly interferes with their daily functioning.
- Level 3: Requiring Very Substantial Support. This is the most severe level, with profound deficits in communication skills. Individuals may have very limited or no intelligible speech. They often have extreme difficulty coping with change, and their restricted or repetitive behaviors markedly interfere with all aspects of their lives.
Causes and Risk Factors
The exact cause of ASD isn't known, but research suggests it's a combination of genetic and environmental factors.
- Genetic Factors: ASD often runs in families, and research has identified several genes associated with the disorder. Some genetic conditions, such as Fragile X syndrome and Down syndrome, have a higher co-occurrence with ASD.
- Environmental Factors: While no specific environmental cause has been definitively proven, research suggests certain factors may increase risk, including advanced parental age at the time of conception and certain maternal infections during pregnancy. It's important to note that extensive research has shown no link between vaccines and autism.
Diagnosis and Interventions
There is no single medical test for ASD. Diagnosis is based on a comprehensive evaluation of a person's behavior and developmental history.
- Diagnosis: The process usually involves behavioral screenings by a doctor, developmental questionnaires for parents, and a full evaluation by specialists like a developmental pediatrician or psychologist. The earlier a diagnosis is made, the sooner intervention can begin, which can lead to better outcomes.
- Interventions: While there's no "cure" for autism, a variety of therapies can help individuals develop skills and manage challenges. Common interventions include:
- Applied Behavior Analysis (ABA): A structured, evidence-based approach to teaching new skills and reducing challenging behaviors.
- Speech-Language Therapy: Focuses on improving verbal, non-verbal, and social communication skills.
- Occupational Therapy: Helps with daily living skills and sensory integration issues.
- Social Skills Training: Teaches social cues and skills for interacting with others.
Summary
- Caring for a child with special needs is a profound journey that requires a comprehensive, family-centered approach.
- Nursing care in this context is multifaceted and extends far beyond the clinical setting. It encompasses a holistic assessment that considers not only the child’s physical condition but also their developmental, psychosocial, and emotional needs.
- For children with chronic illnesses or life-limiting conditions, nursing care is focused on providing unwavering support at the time of diagnosis, educating families about their child's disorder, and helping them promote normal development despite the challenges.
- At the end of life, nurses provide meticulous care to the child while offering compassionate emotional and physical support to the family, addressing their grief and helping them navigate difficult decisions such as DNAR orders and postmortem care. This also extends to supporting siblings and the family after the death, acknowledging the profound and lasting impact of their loss.
- For children with cognitive or sensory impairments, the focus of nursing care shifts to advocacy and education.
- Nurses play a crucial role in helping families understand specific conditions like Down syndrome or Fragile X syndrome, and in implementing strategies to foster the child's development. This includes teaching families how to use simplified language and visual aids for communication, and connecting them to early intervention programs.
- The nurse's role is to act as an advocate, educator, and compassionate presence, empowering families to navigate these challenges and providing the best possible care for the child.
