
Upper Respiratory Tract Infections
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Understand the common upper respiratory tract infections (URTIs) in children, including their etiology, pathophysiology, and clinical manifestations.
- Differentiate between various URTIs, such as acute viral nasopharyngitis, streptococcal pharyngitis, tonsillitis, infectious mononucleosis, and influenza, based on their unique signs and symptoms.
- Understand the diagnostic evaluation and therapeutic management for each specific URTI, including the appropriate use of antibiotics for bacterial infections and supportive care for viral illnesses.
- Understand the indications for tonsillectomy and adenoidectomy, and the comprehensive pre-operative, intra-operative, and post-operative care required.
- Identify and implement key nursing care management strategies for children with URTIs.
- Understand the critical complications associated with specific URTIs, such as rheumatic fever, post-streptococcal glomerulonephritis, and splenic rupture in infectious mononucleosis.
- Educate caregivers on home care measures, prevention strategies, and when to seek immediate medical attention for worsening symptoms or complications.
- Identify key nursing diagnoses and interventions for children with URTIs.
Introduction
- Upper Respiratory Tract Infections (URTIs) are a group of the most prevalent acute illnesses affecting the pediatric population, accounting for a significant number of doctor visits, hospitalizations, and school absences.
- These infections target the anatomical structures of the upper airway, including the nose, paranasal sinuses, pharynx, larynx, and tonsils.
- While URTIs are generally self-limiting, they can lead to serious complications and distress for both the child and their caregivers.
- Understanding these illnesses is paramount for any healthcare professional, especially nurses, who are often the first point of contact and play a crucial role in assessment, management, and family education.
- While most URTIs are viral and self-limiting, some can be bacterial and require specific treatment to prevent serious complications.
- Children, especially those in daycare or school, are highly susceptible to URTIs due to their developing immune systems and close contact with peers. Hand hygiene is paramount in the prevention of spread of URTIs.
- While URTIs share some overlapping symptoms, their etiologies, potential complications, and management strategies differ significantly.
Acute Viral Nasopharyngitis
- Acute viral nasopharyngitis, commonly known as the common cold, is the most frequent infectious disease in humans.
Incidence
- Very High: Children experience an average of 6-10 colds per year, with infants and toddlers having even more. This frequency decreases with age as immunity develops.
- Seasonal Peaks: More common during colder months (e.g., in Kenya, during long rainy seasons like March-May and short rainy seasons like Oct-Dec), but can occur year-round.
Pathophysiology
- The virus enters the respiratory tract, primarily through the nasal passages or conjunctiva, and replicates in the epithelial cells of the nasopharynx. This leads to an inflammatory response, causing local tissue edema, increased mucus production, and vasodilation.
Etiology
- Viruses: Over 200 different viruses can cause the common cold.
- Rhinoviruses: Most common (30-80%).
- Coronaviruses: (10-15%).
- Adenoviruses, Respiratory Syncytial Virus (RSV), Parainfluenza viruses, Enteroviruses, Metapneumovirus: Also significant contributors.
Clinical Manifestations
Symptoms typically appear 1-3 days after exposure and last for about 7-10 days, though some can linger for weeks.
- Initial:
- Sore throat or "scratchy" throat.
- Rhinorrhea (runny nose): Clear, watery discharge initially, becoming thicker and sometimes yellowish/greenish.
- Sneezing.
- Irritability (in infants/young children).
- Progressive:
- Nasal congestion: Leading to mouth breathing, especially in infants.
- Cough: Often develops later, can be mild to severe.
- Low-grade fever: More common in infants and young children.
- Decreased appetite.
- Headache, muscle aches (malaise): More common in older children and adults.
Diagnostic Evaluation
- Clinical Diagnosis: Primarily based on characteristic signs and symptoms. No specific laboratory tests are routinely needed.
- Exclusion: Rule out other conditions with similar symptoms such as allergies, influenza, bacterial infections.
Therapeutic Management
- Supportive Care: No cure for the common cold; treatment focuses on symptom relief.
- Hydration: Encourage oral fluids (water, juice, electrolyte solutions) to prevent dehydration and thin secretions.
- Rest: Promote adequate rest.
- Humidification: Cool-mist humidifier in the child's room can soothe irritated airways and loosen secretions.
- Nasal Saline Drops/Spray: To loosen mucus, followed by suctioning for infants/young children.
- Antipyretics/Analgesics: Acetaminophen or ibuprofen for fever, aches, and pain. Aspirin is contraindicated in children due to the risk of Reye's syndrome.
- Avoid: Over-the-counter (OTC) cough and cold medications (decongestants, antitussives) are generally not recommended for children under 6 years old due to potential serious side effects and lack of proven efficacy.
- Honey: Can be used for cough relief in children over 1 year of age. Honey should be avoided in infants due to the risk of infantile botulism.
Prevention
- Hand Hygiene: Frequent and thorough handwashing with soap and water is the most effective prevention.
- Avoid Touching Face: Discourage touching eyes, nose, and mouth.
- Avoid Sick Individuals: Limit exposure to people with colds.
- Good Nutrition & Rest: Support a healthy immune system.
- Vaccinations: Keep up-to-date with routine childhood immunizations.
Nursing Care Management
- Assessment:
- Monitor respiratory status (rate, effort, presence of retractions, nasal flaring).
- Assess hydration status (mucous membranes, urine output, fontanelles in infants).
- Temperature monitoring.
- Assess for complications (e.g., ear pain, worsening cough, difficulty breathing).
- Interventions:
- Airway Management: Nasal saline and suctioning for infants; elevate head of bed for older children.
- Hydration: Offer fluids frequently.
- Comfort: Administer antipyretics as ordered. Provide a cool-mist humidifier.
- Education:
- Teach caregivers about symptom management at home.
- Emphasize hand hygiene.
- Advise on when to seek medical attention (e.g., difficulty breathing, high fever, signs of ear infection, lethargy).
- Dispelling myths about antibiotics for viral infections.
- Nursing Insight: Educate parents that green or yellow nasal discharge does not automatically mean a bacterial infection; it's a normal progression of a viral cold.
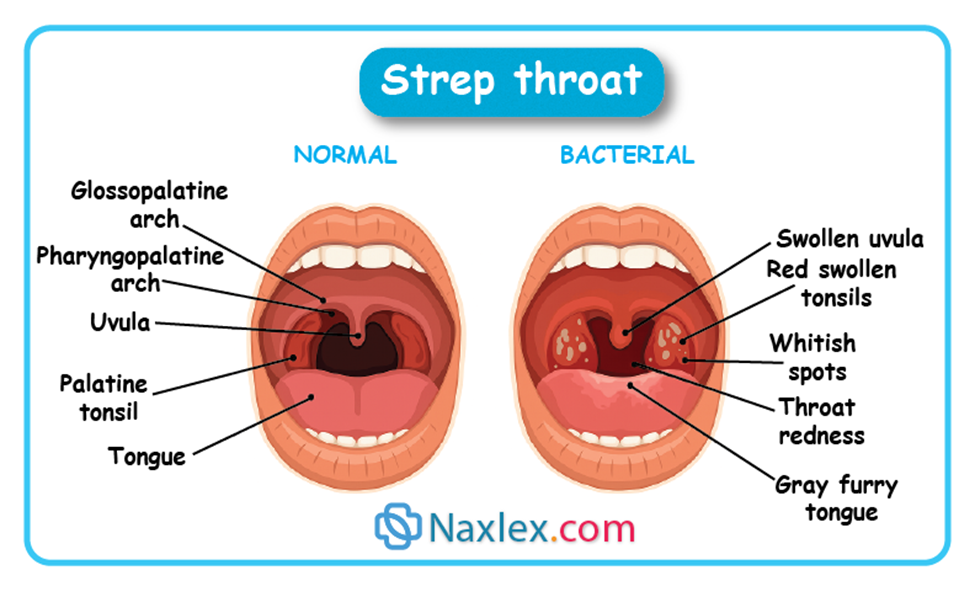
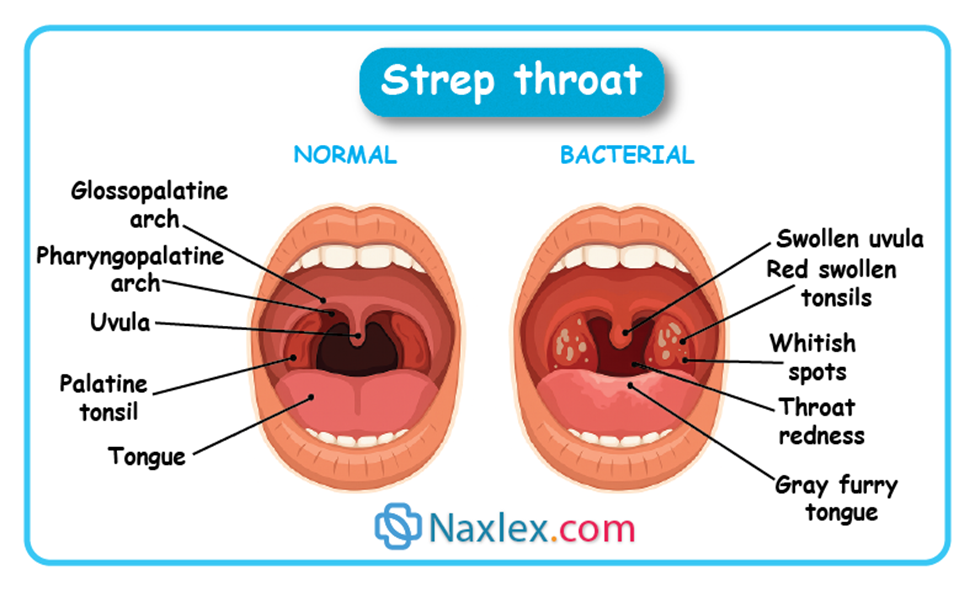
Acute Streptococcus Pharyngitis
- Acute streptococcal pharyngitis is a bacterial infection of the pharynx caused by Group A Streptococcus (Streptococcus pyogenes). It's important to treat to prevent complications like rheumatic fever and post-streptococcal glomerulonephritis.
Incidence
- Common in School-aged Children: Most prevalent in children 5-15 years old. Less common under 3 years.
- Seasonal: Peaks in late fall, winter, and early spring.
Pathophysiology
The bacteria adhere to the pharyngeal epithelium, releasing toxins and enzymes that cause inflammation and tissue damage. This leads to the characteristic symptoms of strep throat.
Etiology
- Bacteria: Group A β-hemolytic Streptococcus (Streptococcus pyogenes).
- Transmission: Droplet transmission from respiratory secretions of infected individuals (coughing, sneezing).
Clinical Manifestations
Symptoms usually have an abrupt onset.
- Abrupt onset of sore throat.
- Pain on swallowing.
- Fever (often high).
- Headache.
- Abdominal pain, nausea, vomiting: Common in younger children.
- Beefy red pharynx.
- Palatal petechiae: Small red spots on the soft palate.
- White or yellow exudate (pus) on tonsils and pharynx.
- Swollen, tender anterior cervical lymph nodes.
- Absent cold symptoms: (e.g., runny nose, cough, hoarseness) – this helps differentiate from viral infections.
- Scarlatiniform rash (Scarlet Fever): Fine, sandpaper-like rash, especially on the trunk and extremities, with flushed cheeks and circumoral pallor (pale area around the mouth). This is a complication of strep throat.
Diagnostic Evaluation
- Rapid Strep Test (Rapid Antigen Detection Test - RADT):
- Detects GAS antigens from a throat swab.
- Results within minutes.
- High specificity, but variable sensitivity.
- Positive RADT: Confirms strep throat, treatment initiated.
- Negative RADT in children: Should be confirmed with a throat culture due to potential for false negatives and the importance of treating GAS infections. Adults with a negative RADT generally do not require a confirmatory culture.
- Throat Culture:
- Gold standard for diagnosis.
- Takes 24-48 hours for results.
Nursing Insight: Ensure proper technique for throat swab collection to get an adequate sample. Touch both tonsils and posterior pharynx.
Therapeutic Management
- Antibiotics: Crucial to prevent complications.
- Penicillin V: Drug of choice (10 days orally).
- Amoxicillin: Often preferred for taste and once-daily dosing.
- Penicillin G Benzathine (Bicillin L.A.): Single intramuscular injection for non-compliant patients or if oral adherence is a concern. Very painful injection, often mixed with lidocaine.
Drug Alert: Never administer penicillin G procaine or penicillin G benzathine suspensions intravenously; they may cause embolism or toxic reaction with ensuing death in minutes. Instead, administer these medications deep into the muscle tissue to decrease localized reactions and pain.
-
- Erythromycin or Azithromycin: For penicillin-allergic patients.
- Symptomatic Relief:
- Analgesics/Antipyretics: Acetaminophen or ibuprofen for pain and fever.
- Warm salt water gargles: For older children.
- Cool or warm drinks, soft foods.
Nursing Care Management
- Assessment:
- Monitor for signs of dehydration.
- Assess pain level.
- Observe for rash (Scarlet Fever).
- Monitor for complications (e.g., worsening symptoms, joint pain, dark urine - signs of rheumatic fever or glomerulonephritis).
- Interventions:
- Administer antibiotics as prescribed: Emphasize completing the full 10-day course, even if symptoms improve, to prevent complications.
- Pain Management: Offer analgesics, provide soothing liquids/foods.
- Hydration: Encourage fluids.
- Infection Control: Educate on hand hygiene, avoiding sharing utensils/drinks.
- Education:
- Explain the importance of antibiotic adherence.
- When the child can return to school (usually 24 hours after starting antibiotics and fever-free).
- Signs and symptoms of potential complications (e.g., rheumatic fever - joint pain, cardiac issues; glomerulonephritis - dark urine, swelling).
Prevention
- Hand Hygiene: Frequent handwashing.
- Avoid Sharing: Do not share eating utensils, cups, or food.
- Stay Home When Sick: Prevent spread, especially during the first 24 hours of antibiotic treatment.
- Prompt Treatment: Early diagnosis and treatment prevent complications and reduce transmission.
Tonsillitis
- Tonsillitis is an inflammation or infection of the palatine tonsils. It can be viral or bacterial.
Incidence
- Common in Children: Especially school-aged children. Declines with age.
- Viral: More common.
- Bacterial: Often Group A Streptococcus.
Pathophysiology
Infection of the tonsils leads to inflammation, edema, and sometimes exudate. The tonsils are lymphoid tissues that play a role in immunity, trapping pathogens entering the respiratory tract. When overwhelmed, they become infected.
Etiology
- Viruses: Adenoviruses, Epstein-Barr virus (EBV), enteroviruses, influenza, parainfluenza.
- Bacteria: Most commonly Streptococcus pyogenes (Group A Strep), but also Staphylococcus aureus, Haemophilus influenzae, Mycoplasma pneumoniae.
Clinical Manifestations
Symptoms vary depending on the cause (viral vs. bacterial) and the child's age.
- Sore throat: Often severe, making swallowing difficult.
- Difficulty swallowing (dysphagia).
- Fever: Can be high.
- Headache.
- Mouth breathing: Due to enlarged tonsils obstructing the airway.
- Snoring/Obstructive sleep apnea: In severe cases with significant tonsillar hypertrophy.
- Muffled voice.
- Halitosis (bad breath).
- Abdominal pain, nausea, vomiting: Especially in younger children with strep tonsillitis.
- Enlarged, red tonsils: May have white or yellow exudate (pus).
- Tender, enlarged cervical lymph nodes.
Diagnostic Evaluation
- Clinical Examination: Visual inspection of the throat.
- Rapid Strep Test/Throat Culture: To rule out or confirm Group A Strep infection.
- Monospot Test: If infectious mononucleosis is suspected (e.g., older child with lymphadenopathy, fatigue, splenomegaly).
Therapeutic Management
A. Medical Treatment
- Viral Tonsillitis:
- Supportive Care: Similar to the common cold.
- Pain relief: Acetaminophen or ibuprofen.
- Hydration: Encourage fluids.
- Rest.
- Warm salt water gargles: For older children.
- Bacterial Tonsillitis (Strep):
- Antibiotics: Penicillin V or amoxicillin for 10 days. Erythromycin for penicillin-allergic individuals.
- Symptomatic relief: As above.
B. Surgical Treatment: Tonsillectomy and Adenoidectomy (T&A)
Removal of the palatine tonsils (tonsillectomy) and pharyngeal tonsils (adenoids) (adenoidectomy).
Indications for T&A:
- Recurrent Tonsillitis:
- 7 or more episodes in the preceding year.
- 5 or more episodes per year in the preceding 2 years.
- 3 or more episodes per year in the preceding 3 years.
- Definition of episode: Sore throat and one of the following: fever >38.3°C, cervical lymphadenopathy (>2cm), tonsillar exudate, or positive Group A Strep test.
- Obstructive Sleep Apnea (OSA): Due to tonsillar and/or adenoidal hypertrophy causing upper airway obstruction. This is the most common indication for T&A in children today.
- Peritonsillar Abscess: Not responding to antibiotics or recurrent.
- Malocclusion/Oronasal facial growth abnormalities: Due to chronic mouth breathing from enlarged adenoids.
- Chronic Otitis Media with Effusion (OME): Adenoidectomy alone or with T&A can improve Eustachian tube function.
- Chronic Tonsillitis: Persistent sore throat, halitosis, and cryptic tonsils that are not responsive to medical management.
Pre-operative Care:
- Assessment:
- Complete history and physical examination.
- Allergies, current medications.
- Bleeding disorders (e.g., hemophilia, von Willebrand disease), family history of bleeding.
- Ask specifically about NSAID use (ibuprofen, aspirin) in the past 1-2 weeks due to increased bleeding risk.
- Loose teeth (risk of aspiration during intubation).
- Baseline vital signs.
- Diagnostic Tests:
- Complete Blood Count (CBC) with differential.
- Coagulation studies (PT, PTT, INR) if a bleeding disorder is suspected or patient on anticoagulants.
- Type and screen (rarely needed unless high bleeding risk).
- Preparation:
- NPO (Nothing by Mouth): For specified time before surgery (usually 6-8 hours for solids, 2-4 hours for clear liquids) to prevent aspiration.
- Education: Explain the procedure simply to the child (if age-appropriate) and parents. Discuss expectations for recovery, pain, and diet.
- Consent: Ensure informed consent is signed.
Intra-operative Care:
- Positioning: Supine with head extended (Rose position) to provide clear surgical field.
- Anesthesia: General anesthesia.
- Procedure: Tonsils and/or adenoids are removed using various techniques (e.g., electrocautery, laser, microdebrider). Meticulous hemostasis is crucial.
Post-operative Care (Immediate):
- Positioning:
- Initially prone or side-lying: To facilitate drainage of secretions and prevent aspiration.
- Once fully awake and stable: Head of the bed elevated.
- Vital Signs: Monitor frequently (every 15-30 minutes initially) for stability, signs of hemorrhage such as increased pulse, decreased BP, and pallor, or respiratory distress.
- Airway Management:
- Observe for signs of respiratory obstruction such as stridor, retractions, and nasal flaring.
- Keep suction available but avoid deep suctioning unless necessary to prevent trauma to the surgical site.
- Hemorrhage:
- Most critical complication.
- Signs: Frequent swallowing, even while sleeping, is the earliest sign of bleeding. Also, bright red vomiting, pallor, restlessness, increased heart rate, decreased blood pressure (late sign).
- Intervention: Report immediately to surgeon. Position on side. Prepare for potential return to OR.
- Pain Management:
- Administer prescribed analgesics (e.g., acetaminophen with codeine, ibuprofen after initial bleeding risk passes, hydrocodone).
- Avoid aspirin or NSAIDs initially due to increased bleeding risk.
- Ice collar to the neck.
- Hydration/Diet:
- Start with clear, cool liquids (water, clear juice, ice chips) once fully awake and gag reflex returns. This should be provided within the first 24 hours. Avoid red-colored liquids as they can mimic blood.
- Advance to soft, bland foods such as pudding, gelatin, mashed potatoes, well-cooked pasta, 1-2 days postoperative.
- Avoid: Hot foods, spicy foods, acidic juices, crunchy foods (chips, toast, pretzels) that can irritate the surgical site or dislodge clots. Avoid milk products such as milk, ice cream, and pudding initially because they coat the throat causing the child to cough to clear the throat.
- Nausea/Vomiting: Common. Administer antiemetics as ordered.
Pre-operative Nursing Diagnoses:
- Anxiety (child and parents) related to surgical procedure and unfamiliar environment.
- Deficient Knowledge related to surgical procedure and post-operative care.
Intra-operative Nursing Diagnoses:
- Risk for Aspiration related to NPO status and general anesthesia.
- Risk for Injury related to surgical procedure and positioning.
Post-operative Nursing Diagnoses:
- Acute Pain related to surgical incision.
- Risk for Hemorrhage related to surgical site.
- Risk for Deficient Fluid Volume related to decreased oral intake and potential bleeding.
- Impaired Oral Mucous Membrane related to surgical trauma.
- Risk for Ineffective Airway Clearance related to edema or bleeding.
- Deficient Knowledge (caregiver) related to home care and signs of complications.
Caregiver Education (Home Care):
- Pain Management: Administer prescribed pain medication regularly, even if the child seems okay, to stay ahead of the pain. Use a timer for doses.
- Hydration: Emphasize fluid intake to prevent dehydration.
- Diet:
- Day 1-2: Clear, cool liquids, ice pops, popsicles, diluted juice, bland pureed foods.
- Day 3-7: Soft, bland foods, like mashed potatoes, scrambled eggs, well-cooked pasta, soft cereals, pudding, cooked vegetables.
- Avoid for 2 weeks: Crunchy, hard, spicy, acidic, or hot foods. Examples to avoid: chips, pretzels, toast, crackers, highly acidic juices (orange, grapefruit), carbonated drinks.
- Activity:
- Rest for the first few days.
- Avoid strenuous activity, heavy lifting, or vigorous play for 1-2 weeks.
- Avoid blowing nose vigorously or clearing throat frequently.
- Bleeding:
- Most critical warning sign: Frequent swallowing. Teach parents to check the back of the throat with a flashlight if concerned.
- When to call: Any signs of bleeding (bright red blood, frequent swallowing, vomiting bright red blood), fever, increased pain not controlled by medication, refusal to drink.
- Do not give the child any straws, forks, or sharp objects that can be put into the mouth.
- Bad breath/Ear pain: Common for about a week. Ear pain is referred pain from the throat.
- Fever: Low-grade fever is common for 1-2 days. Report persistent high fever.
- Follow-up: Schedule follow-up appointment with the surgeon.
Nursing Insight: Using a straw creates negative pressure in the mouth and throat. This suction can dislodge clots that are forming at the surgical site (tonsillar beds). If the clot is disturbed, it can lead to hemorrhage, one of the most serious postoperative complications of a tonsillectomy. Furthermore, the sucking motion can irritate the healing tissues in the oropharynx. This delays healing and increases discomfort.
Complications of Surgery:
- Hemorrhage:
- Primary (within 24 hours): Most common. Typically due to dislodgement of clot or inadequate hemostasis.
- Secondary (5-10 days post-op): Occurs when the scab separates. Can be severe.
- Management: Return to OR for cauterization or ligation.
- Dehydration: Due to pain making swallowing difficult.
- Infection: Local wound infection.
- Airway Obstruction: Due to edema or bleeding.
- Voice Change: Temporary, usually resolves. Rarely permanent.
- Pharyngeal Stenosis: Rare, due to excessive tissue removal.
Nursing Insight: For a child post-tonsillectomy, "frequent swallowing" is a red flag, even if they're sleeping. Wake them gently and observe the back of their throat if you suspect bleeding.
Drug Alert: Codeine is contraindicated in pediatric patients post tonsillectomy and adenoidectomy. In 2012 the US Food and Drug Administration issued a Drug Safety Communication that codeine use in certain children after tonsillectomy and/or adenoidectomy may lead to rare but life-threatening adverse events or death. In 2013 a boxed warning (the Food and Drug Administration’s strongest) was added to codeine drug labels to warn about the risks associated with it and to contraindicate its use in this population.
Infectious Mononucleosis
- Infectious mononucleosis is an acute infectious disease caused by the Epstein-Barr Virus (EBV), primarily affecting adolescents and young adults.
Incidence
- Common in Adolescents/Young Adults: Peaks between 15-24 years of age.
- Rare in Young Children: If infected, often asymptomatic or mild.
Pathophysiology
- EBV is a herpesvirus that primarily infects B lymphocytes and epithelial cells of the oropharynx. The virus remains latent in B cells throughout life. During primary infection, there is a proliferation of infected B cells and a robust cytotoxic T-cell response, leading to characteristic symptoms.
Etiology
- Epstein-Barr Virus (EBV): A type of herpesvirus.
- Transmission: Primarily through saliva ("kissing disease"), but also through sharing drinks, utensils. Less contagious than the common cold.
- Incubation Period: Long, 30-50 days.
Clinical Manifestations
Highly variable. The classic triad of symptoms includes:
- Fever: Often prolonged (weeks).
- Pharyngitis: Severe sore throat, often with exudative tonsillitis.
- Lymphadenopathy: Generalized, especially posterior cervical, axillary, and inguinal nodes. Nodes are often tender.
- Fatigue/Malaise: Profound and can be debilitating, lasting for weeks to months.
- Splenomegaly: Enlarged spleen (in 50-60% of cases).
- Hepatomegaly: Enlarged liver (in 10-15% of cases).
- Rash: Maculopapular rash, especially if treated with ampicillin or amoxicillin.
- Palatal petechiae: Small red spots on the soft palate.
- Periorbital edema: Swelling around the eyes.
Diagnostic Evaluation
- Monospot Test (Heterophile Antibody Test):
- Detects heterophile antibodies, which appear during the first 2-3 weeks of illness.
- Positive: Confirms mono in older children/adults.
- Negative in young children: May need further testing as young children don't always produce heterophile antibodies.
- EBV-Specific Antibody Tests:
- Detect specific antibodies (e.g., VCA-IgM, VCA-IgG, EBNA) to confirm EBV infection, especially in uncertain cases or young children.
- Complete Blood Count (CBC):
- Lymphocytosis: Increased white blood cells, predominantly lymphocytes.
- Atypical Lymphocytes: Characteristic abnormal lymphocytes seen on blood smear.
- Liver Function Tests (LFTs): May be elevated due to liver involvement.
Therapeutic Management
- Supportive Care: No specific antiviral treatment.
- Rest: Crucial for recovery, especially during the acute phase. Activity should be gradually increased.
- Hydration: Encourage fluids.
- Pain Relief: Acetaminophen or ibuprofen for fever, sore throat, and body aches.
- Corticosteroids: May be used in severe cases (e.g., significant airway obstruction from tonsillar hypertrophy, severe thrombocytopenia, hemolytic anemia, CNS involvement) to reduce inflammation.
- Avoid:
- Antibiotics: Ineffective against viruses. Avoid ampicillin/amoxicillin as they cause a widespread rash in mononucleosis patients.
Prognosis
- Self-limiting: Most individuals recover within 2-4 weeks.
- Fatigue: Can persist for several months.
- Full recovery: Common, but the virus remains latent.
Complications
- Splenic Rupture: Most serious complication, though rare. Occurs due to splenomegaly, making the spleen fragile. Can be spontaneous or result from trauma.
- Symptoms: Sudden severe abdominal pain (especially left upper quadrant), left shoulder pain (Kehr's sign), signs of hypovolemic shock.
- Management: Medical emergency.
- Resumption of Contact Sports: Crucial education point. Avoid contact sports and strenuous activities for at least 3-4 weeks from the onset of symptoms, or until splenomegaly has resolved (confirmed by physical exam or ultrasound). Some recommend longer (up to 6-8 weeks).
- Airway Obstruction: Due to massive tonsillar and adenoidal hypertrophy.
- Neurological Complications: Meningitis, encephalitis, Guillain-Barré syndrome (rare).
- Hematologic Complications: Hemolytic anemia, thrombocytopenia (rare).
- Hepatitis: Mild liver inflammation is common.
- Peritonsillar Abscess.
Nursing Care Management
- Assessment:
- Monitor for signs of respiratory distress (if tonsils are enlarged).
- Assess for splenomegaly/hepatomegaly (gentle palpation).
- Monitor for abdominal pain (signs of splenic rupture).
- Assess fatigue level and activity tolerance.
- Interventions:
- Rest: Emphasize the importance of adequate rest.
- Pain Relief: Administer analgesics.
- Hydration: Encourage fluids.
- Education:
- Explain the viral nature of the illness and the importance of supportive care.
- Educate on avoidance of contact sports and strenuous activity (3-4 weeks or until spleen size normalizes) to prevent splenic rupture.
- Advise on symptom progression and when to seek medical attention (e.g., severe abdominal pain, worsening breathing, yellow skin/eyes).
- Explain the contagiousness and importance of not sharing drinks/utensils.
- Discuss the prolonged fatigue.
- Nursing Insight: Always ask about contact sports when educating a teen with mono. This seemingly benign instruction can prevent a life-threatening emergency!
Influenza
- Influenza is a highly contagious acute viral infection of the respiratory tract caused by influenza viruses.
Incidence
- Seasonal Epidemics: Occur annually, typically in colder months. In Kenya, this can align with rainy seasons.
- Pandemics: Can occur periodically when new, highly virulent strains emerge.
- Impact: Causes significant morbidity and mortality, especially in young children, elderly, and those with chronic health conditions.
Pathophysiology
- Influenza viruses primarily target and replicate in the respiratory epithelial cells, causing cellular destruction and inflammation. This leads to the characteristic symptoms and can predispose individuals to secondary bacterial infections.
Etiology
- Influenza Viruses:
- Type A: Most common and causes severe epidemics/pandemics.
- Type B: Causes less severe, more localized epidemics.
- Type C: Causes mild illness, not associated with epidemics.
- Transmission: Droplet transmission (coughing, sneezing) and direct contact with contaminated surfaces. Highly contagious.
- Incubation Period: 1-4 days.
Clinical Manifestations
Symptoms are typically more severe and abrupt in onset than the common cold.
- Abrupt onset of:
- Fever: Often high (39-40°C), chills.
- Headache.
- Myalgia (muscle aches): Often severe.
- Malaise/Fatigue: Profound.
- Sore throat.
- Dry, hacking cough: Can be severe and persistent.
- Nasal congestion/Rhinorrhea: Less prominent than common cold.
- Nausea, vomiting, diarrhea: More common in children.
Diagnostic Evaluation
- Rapid Influenza Diagnostic Tests (RIDTs):
- Detect influenza viral antigens from nasal swab, throat swab, or nasal aspirate.
- Results within 15-30 minutes.
- Limitations: Variable sensitivity (can have false negatives), better specificity. A negative RIDT doesn't rule out flu, especially during peak season.
- Reverse Transcription Polymerase Chain Reaction (RT-PCR):
- More sensitive and specific than RIDTs.
- Used for definitive diagnosis, especially in hospitalized patients or for public health surveillance.
- Results take longer.
- Clinical Diagnosis: Often based on characteristic symptoms during flu season, especially if other community members are infected.
Therapeutic Management
- Antiviral Medications:
- Neuraminidase Inhibitors: Oseltamivir (Tamiflu), Zanamivir (Relenza), Peramivir (Rapivab).
- Mechanism: Inhibit viral replication.
- Effectiveness: Most effective when started within 48 hours of symptom onset. Can shorten duration of illness, reduce severity, and prevent complications.
- Indications: High-risk individuals (young children, elderly, chronic medical conditions), severe illness, hospitalized patients.
- Supportive Care:
- Rest: Ample rest.
- Hydration: Encourage fluids to prevent dehydration.
- Antipyretics/Analgesics: Acetaminophen or ibuprofen for fever, headache, muscle aches.
- Humidifier: To soothe cough.
Prevention
- Influenza Vaccine:
- Annual vaccination: Recommended for everyone 6 months of age and older.
- Types: Inactivated influenza vaccine (IIV) via injection, or Live Attenuated Influenza Vaccine (LAIV) via nasal spray (for healthy individuals 2-49 years old, not pregnant).
- Timing: Best administered before the flu season begins (e.g., by October/November in the Northern Hemisphere).
- Even if the vaccine doesn't completely prevent flu, it significantly reduces the severity of illness and risk of complications.
- Hand Hygiene: Frequent handwashing with soap and water or alcohol-based hand sanitizer.
- Avoid Touching Face: Reduce self-inoculation.
- Avoid Sick Individuals: Limit close contact.
- Cover Coughs and Sneezes: Use a tissue or inner elbow.
- Stay Home When Sick: To prevent spreading the virus.
Nursing Care Management
- Assessment:
- Monitor respiratory status (rate, effort, oxygen saturation).
- Assess for dehydration.
- Monitor temperature and pain.
- Observe for signs of complications (e.g., secondary bacterial pneumonia, otitis media, worsening respiratory distress).
- Interventions:
- Administer antiviral medications: If prescribed, emphasize starting within 48 hours.
- Symptom Management: Provide antipyretics, analgesics, cool mist humidifier.
- Hydration: Offer fluids frequently.
- Rest: Encourage rest.
- Infection Control: Isolation precautions if hospitalized, educate on hand hygiene, cough etiquette, staying home when sick.
- Education:
- Importance of annual flu vaccination.
- Symptom management at home.
- When to seek medical attention (e.g., difficulty breathing, chest pain, sudden dizziness, severe vomiting, signs of dehydration).
- Differentiation between cold and flu symptoms.
- Nursing Insight: When a child presents with sudden high fever, severe body aches, and fatigue during flu season, consider influenza even if initial rapid tests are negative.
Summary
- Upper Respiratory Tract Infections (URTIs) are a broad category of illnesses affecting the nose, pharynx, larynx, and tonsils, representing some of the most common reasons for healthcare visits, especially in children.
- The Common Cold (Acute Viral Nasopharyngitis) is the most frequent URTI, caused by over 200 viruses, predominantly rhinoviruses. Its incidence is highest in young children (6-10 colds/year), decreasing with age. Antibiotics are ineffective, and OTC cough/cold medications are discouraged in young children due to safety concerns. Prevention hinges on rigorous hand hygiene and avoiding touching the face.
- Acute Streptococcal Pharyngitis (Strep Throat) is a bacterial infection caused by Group A Streptococcus (Streptococcus pyogenes), primarily affecting school-aged children. It's significant due to its potential for serious non-suppurative complications like rheumatic fever and post-streptococcal glomerulonephritis. Antibiotic therapy, typically penicillin or amoxicillin for 10 days, is essential to eradicate the bacteria, prevent complications, and reduce contagiousness.
- Tonsillitis, the inflammation of the palatine tonsils, can be viral or bacterial. It presents with a severe sore throat, difficulty swallowing, fever, and sometimes mouth breathing due to enlarged tonsils. Medical management is supportive for viral cases and antibiotics for bacterial. Surgical management (Tonsillectomy and Adenoidectomy - T&A) is considered for specific indications.
- Infectious Mononucleosis ("Mono"), caused by the Epstein-Barr Virus (EBV), primarily affects adolescents and young adults. It's known for its classic triad of fever, severe pharyngitis (often with exudative tonsillitis), and generalized lymphadenopathy. Splenomegaly is common and is the basis for the most serious complication: splenic rupture.
- Influenza (Flu) is a highly contagious viral infection that causes annual epidemics. Symptoms are abrupt and more severe than the common cold, including high fever, chills, headache, severe myalgia, profound fatigue, and a dry, hacking cough. Antiviral medications (e.g., oseltamivir) are effective if started within 48 hours of symptom onset, especially in high-risk individuals, to reduce severity and complications. Supportive care (rest, hydration, analgesics) is also essential. The most effective preventive measure is annual influenza vaccination for all individuals 6 months and older.
