
Capstone Exam 1
ATI Capstone Exam 1
Total Questions : 111
Showing 10 questions Sign up for moreA nurse is preparing to administer fluconazole 400 mg by intermittent IV bolus daily. Available is fluconazole 400 mg in 0.9% sodium chloride (NaCl) 200 mL to infuse over 2 hours. The nurse should set the IV pump to deliver how many mL/hr?
(Round the answer to the nearest tenth/whole number. Use a leading zero if it applies. Do not use a trailing zero.)
Explanation
The answer is 100.
Step 1: Determine the total volume to be infused. = 200 mL
Step 2: Determine the total time for infusion. = 2 hours
Step 3: Calculate the infusion rate in mL/hr. Calculation: 200 mL ÷ 2 hours = 100 mL/hr
The nurse should set the IV pump to deliver 100 mL/hr.
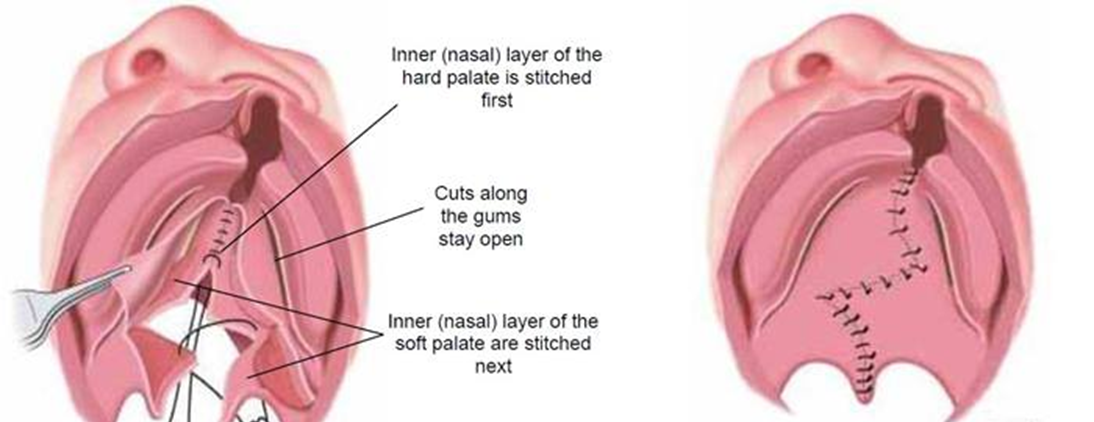
A nurse is caring for a toddler who is 24 hours postoperative following a cleft palate repair. Which of the following actions should the nurse take?
Explanation
Choice A reason: Apply Bilateral Wrist Restraints
Applying bilateral wrist restraints can be necessary in some cases to prevent the child from touching or interfering with the surgical site. However, restraints should be used as a last resort and only when absolutely necessary. They can cause distress and discomfort to the child and should be monitored closely to prevent any complications.
Choice B reason: Administer Opioids for Pain
Administering opioids for pain management is a common practice post-surgery to ensure the child is comfortable. However, opioids should be used cautiously due to the risk of side effects and potential for dependency. Non-opioid pain management strategies, such as acetaminophen or ibuprofen, are often preferred unless the pain is severe.
Choice C reason: Implement a Soft Diet
Implementing a soft diet is crucial for a child who is 24 hours postoperative following a cleft palate repair. The surgical site in the mouth is still healing, and a soft diet helps prevent any damage or irritation to the area. Soft foods are easier to swallow and less likely to cause pain or disrupt the healing process. Examples of soft foods include mashed potatoes, yogurt, and pureed fruits.
Choice D reason: Offer Fluids Through a Straw
Offering fluids through a straw is not recommended for a child who has undergone cleft palate repair. The suction created by using a straw can put pressure on the surgical site and potentially cause complications. Instead, fluids should be offered using a cup or a spoon to minimize any risk to the healing palate.
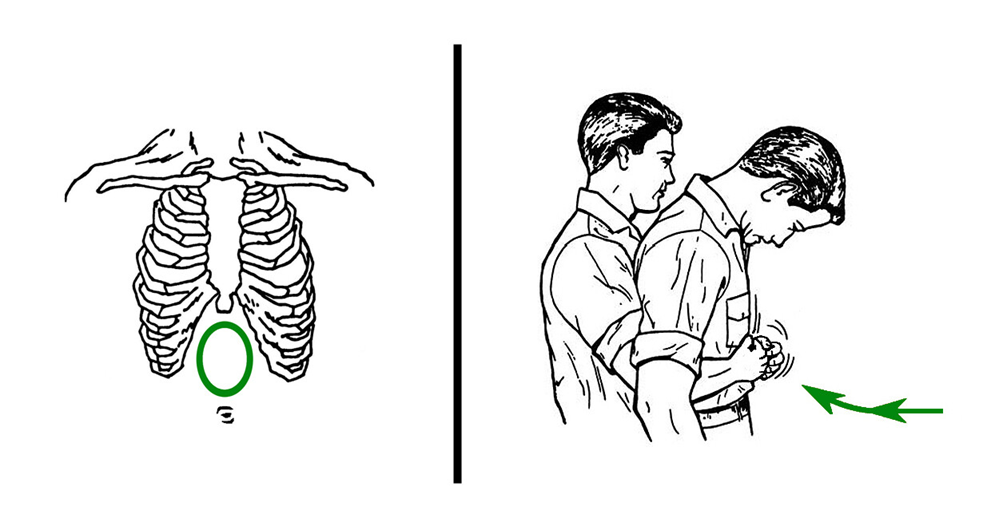
A nurse is caring for a client who develops an airway obstruction from a foreign body but remains conscious. Which of the following actions should the nurse take first?
Explanation
Choice A reason: Perform a Blind Finger Sweep
Performing a blind finger sweep is not recommended because it can push the foreign object further into the airway, making the obstruction worse. This method is only advised if the object is clearly visible and can be safely removed without causing further harm.
Choice B reason: Turn the Client to the Side
Turning the client to the side can be helpful in certain situations, such as when the client is unconscious or at risk of vomiting. However, in the case of a conscious client with a foreign body airway obstruction, this action does not directly address the obstruction and is not the first priority.
Choice C reason: Insert an Oral Airway
Inserting an oral airway is typically used to maintain an open airway in an unconscious patient who cannot maintain their own airway. For a conscious client with a foreign body obstruction, this action is not appropriate and could cause further complications.
Choice D reason: Administer the Abdominal Thrust Maneuver
Administering the abdominal thrust maneuver (also known as the Heimlich maneuver) is the recommended first action for a conscious client with a foreign body airway obstruction. This technique involves standing behind the client, placing a fist just above their navel, and delivering quick, upward thrusts to expel the foreign object. This method is effective in creating an artificial cough that can dislodge the obstruction.
A nurse is reviewing the laboratory test results from a client who has prerenal acute kidney injury (AKI). Which of the following electrolyte imbalances should the nurse expect?
Explanation
Choice A reason: Hypophosphatemia
Hypophosphatemia, or low phosphate levels, is not typically associated with prerenal acute kidney injury (AKI). Prerenal AKI is primarily related to decreased blood flow to the kidneys, which does not directly affect phosphate levels. Hypophosphatemia is more commonly seen in conditions such as refeeding syndrome, chronic alcoholism, and certain endocrine disorders.
Choice B reason: Hyperkalemia
Hyperkalemia, or elevated potassium levels, is a common electrolyte imbalance in prerenal acute kidney injury (AKI). When kidney function is impaired, the kidneys are less able to excrete potassium, leading to its accumulation in the blood. This can result in dangerous cardiac arrhythmias and requires prompt management. Hyperkalemia is often seen in various types of AKI, including prerenal, intrinsic, and postrenal causes.
Choice C reason: Hypercalcemia
Hypercalcemia, or high calcium levels, is not typically associated with prerenal AKI. In fact, AKI can sometimes lead to hypocalcemia (low calcium levels) due to impaired kidney function affecting calcium and phosphate metabolism. Hypercalcemia is more commonly associated with conditions such as hyperparathyroidism, malignancies, and certain medications.
Choice D reason: Hypernatremia
Hypernatremia, or high sodium levels, is also not a typical finding in prerenal AKI. Prerenal AKI is usually characterized by volume depletion, which can lead to hyponatremia (low sodium levels) due to the body’s attempt to retain water and maintain blood pressure. Hypernatremia is more commonly seen in conditions involving excessive water loss or inadequate water intake.

Explanation
Choice A reason: Exophthalmos
Exophthalmos, or bulging eyes, is not a typical symptom of hypothyroidism. Instead, it is commonly associated with hyperthyroidism, particularly Graves’ disease. In hypothyroidism, the thyroid gland is underactive, leading to a different set of symptoms.
Choice B reason: Photophobia
Photophobia, or sensitivity to light, is not a common symptom of hypothyroidism. While hypothyroidism can cause a variety of symptoms, photophobia is more often associated with conditions affecting the eyes or the nervous system.
Choice C reason: Lethargy
Lethargy, or extreme fatigue, is a common symptom of hypothyroidism. When the thyroid gland does not produce enough thyroid hormones, the body’s metabolism slows down, leading to feelings of tiredness and lack of energy. This is one of the hallmark symptoms of hypothyroidism and can significantly impact a person’s daily life.
Choice D reason: Weight Loss
Weight loss is not typically associated with hypothyroidism. In fact, weight gain is more common due to the slowed metabolism caused by an underactive thyroid. Individuals with hypothyroidism often experience difficulty losing weight and may gain weight even with a normal diet and exercise routine.
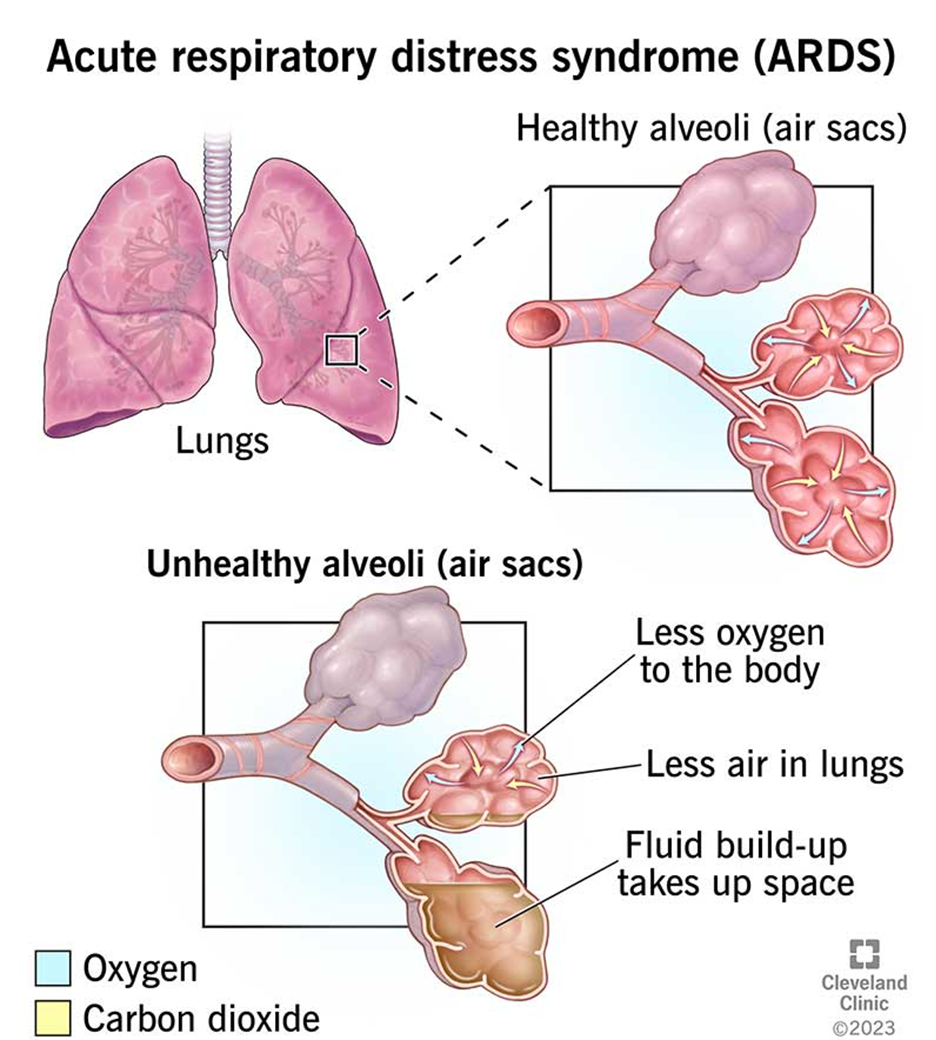
A nurse is caring for a client who has acute respiratory distress syndrome (ARDS) and requires mechanical ventilation. The client receives a prescription for pancuronium. The nurse recognizes that this medication is for which of the following purposes?
Explanation
Choice A reason: Induce Sedation
Pancuronium is not used to induce sedation. It is a neuromuscular blocking agent (NMBA) that causes paralysis of skeletal muscles. Sedation is typically achieved using medications such as benzodiazepines or propofol, which act on the central nervous system to produce a calming effect.
Choice B reason: Suppress Respiratory Effort
Pancuronium is used to suppress respiratory effort in patients with ARDS who require mechanical ventilation. By causing muscle paralysis, pancuronium helps to synchronize the patient’s breathing with the ventilator, reducing the risk of ventilator-induced lung injury and improving oxygenation. This is particularly important in severe cases of ARDS where patient-ventilator dyssynchrony can be detrimental.
Choice C reason: Decrease Chest Wall Compliance
Decreasing chest wall compliance is not a purpose of pancuronium. In fact, pancuronium does not directly affect chest wall compliance. Instead, it works by blocking the transmission of nerve impulses to the muscles, leading to muscle relaxation and paralysis.
Choice D reason: Decrease Respiratory Secretions
Pancuronium does not decrease respiratory secretions. Medications such as anticholinergics (e.g., atropine) are used to reduce secretions. Pancuronium’s primary role is to facilitate mechanical ventilation by ensuring complete muscle relaxation.
Explanation
Choice A reason: Decrease the Infusion Rate on the IV
Decreasing the infusion rate on the IV is the appropriate action to take when a client experiences flushing of the neck and tachycardia while receiving vancomycin. These symptoms are indicative of vancomycin flushing syndrome (VFS), also known as “red man syndrome,” which is a reaction caused by the rapid infusion of vancomycin. Slowing the infusion rate allows the body more time to metabolize the drug and can help alleviate the symptoms.
Choice B reason: Document that the Client Experienced an Anaphylactic Reaction to the Medication
Documenting that the client experienced an anaphylactic reaction is not accurate in this scenario. Vancomycin flushing syndrome is an anaphylactoid reaction, not an anaphylactic one. Anaphylactoid reactions are not mediated by IgE antibodies and do not require prior sensitization to the drug. Therefore, it is important to distinguish between the two and document the reaction correctly.
Choice C reason: Change the IV Infusion Site
Changing the IV infusion site is not necessary in this case. The symptoms of flushing and tachycardia are related to the rate of vancomycin infusion, not the site of infusion. Therefore, changing the site would not address the underlying issue.
Choice D reason: Apply Cold Compresses to the Neck Area
Applying cold compresses to the neck area may provide some symptomatic relief, but it does not address the root cause of the reaction. The primary intervention should be to slow the infusion rate to prevent further release of histamine and alleviate the symptoms.
Explanation
Choice A reason: Veracity
Veracity refers to the ethical principle of truthfulness and honesty. In the context of nursing, it involves providing accurate and complete information to patients. While veracity is crucial in maintaining trust between the nurse and the patient, it is not directly related to the decision to discontinue a medication due to adverse effects.
Choice B reason: Fidelity
Fidelity involves being faithful to commitments and promises made to patients. It includes maintaining confidentiality and being loyal to the patient’s best interests. Although fidelity is important in the nurse-patient relationship, it does not specifically address the ethical considerations involved in discontinuing a harmful medication.
Choice C reason: Nonmaleficence
Nonmaleficence is the ethical principle of doing no harm. In this scenario, discontinuing the experimental chemotherapy medication due to evidence of rapidly advancing kidney failure aligns with the principle of nonmaleficence. The nurse and healthcare team are acting to prevent further harm to the patient by stopping a treatment that is causing significant adverse effects.
Choice D reason: Autonomy
Autonomy refers to respecting the patient’s right to make their own decisions about their healthcare. This includes providing the patient with all necessary information to make informed choices. While autonomy is a fundamental ethical principle, the decision to discontinue the medication in this case is primarily based on preventing harm, which aligns more closely with nonmaleficence.
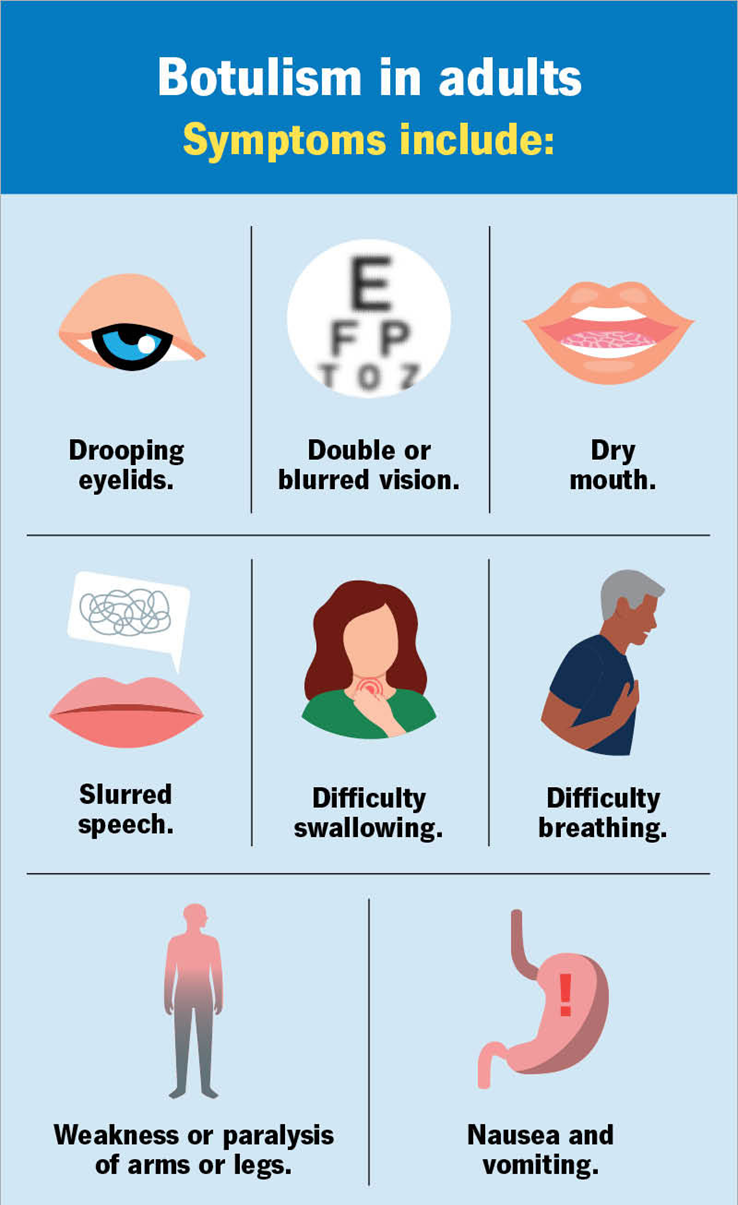
A nurse is preparing a response protocol for botulism as a bioterrorism agent. The nurse should prepare the protocol based on which of the following information? (Select all that apply.)
Explanation
Choice A reason: Botulism is Acquired Through Direct Contact with an Infected Person
Botulism is not acquired through direct contact with an infected person. It is caused by a toxin produced by the bacterium Clostridium botulinum. The most common forms of botulism are foodborne, wound, and infant botulism. Foodborne botulism occurs when a person ingests food containing the toxin, while wound botulism occurs when the bacteria infect a wound and produce the toxin. Infant botulism occurs when infants ingest spores of the bacteria, which then grow and produce the toxin in their intestines.
Choice B reason: Notify the Centers for Disease Control and Prevention (CDC) When More Than Three Cases Are Confirmed
While notifying the CDC is crucial in the event of a botulism outbreak, the specific threshold for notification can vary. Generally, any suspected case of botulism should be reported to public health authorities immediately due to the severity of the disease and the potential for outbreaks. The CDC provides guidelines for reporting and managing botulism cases.
Choice C reason: Botulism Can Produce Paralysis Within 12 to 72 Hours Following Exposure
Botulism can indeed produce paralysis within 12 to 72 hours following exposure. The toxin affects the nervous system, leading to muscle paralysis. Early symptoms include weakness, dizziness, and dry mouth, followed by more severe symptoms such as blurred vision, difficulty swallowing, and muscle weakness. If left untreated, botulism can lead to respiratory failure and death.
Choice D reason: Vomiting and Diarrhea Are Expected Findings Following Exposure
Vomiting and diarrhea are not typical symptoms of botulism. The primary symptoms are related to muscle paralysis and neurological impairment. Gastrointestinal symptoms may occur in some cases of foodborne botulism, but they are not the hallmark signs of the disease.
Choice E reason: Botulism is a Toxin Found in Castor Beans
Botulism is not a toxin found in castor beans. The toxin found in castor beans is ricin, which is a different type of bioterrorism agent. Botulism is caused by the botulinum toxin produced by Clostridium botulinum bacteria.
A nurse in a provider’s office is assessing a client who has rheumatoid arthritis (R
Explanation
Choice A reason: Low-Grade Fever
Low-grade fever is a common early symptom of rheumatoid arthritis (RA). It is often associated with the body’s inflammatory response to the autoimmune activity occurring in the joints. While it can persist throughout the disease, it is not considered a late manifestation.
Choice B reason: Weight Loss
Weight loss can occur in RA due to chronic inflammation and its effects on metabolism and appetite. However, it is more commonly seen in the early to middle stages of the disease rather than as a late manifestation. Persistent inflammation can lead to muscle wasting and weight loss, but these are not specific to the advanced stages of RA.
Choice C reason: Anorexia
Anorexia, or loss of appetite, is another symptom that can be present in RA. It is often related to the chronic inflammation and pain associated with the disease, which can reduce a person’s desire to eat. Like weight loss, anorexia can occur at various stages of RA and is not specifically a late manifestation.
Choice D reason: Knuckle Deformity
Knuckle deformity is a late manifestation of rheumatoid arthritis. As RA progresses, the chronic inflammation can lead to joint damage and deformities, particularly in the hands and fingers. This includes changes such as ulnar deviation, swan neck deformities, and boutonnière deformities. These deformities result from the destruction of joint tissues and the formation of scar tissue, which can significantly impair hand function.

You just viewed 10 questions out of the 111 questions on the ATI Capstone Exam 1 Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

