
Maternity Exam
ATI Maternity Exam
Total Questions : 44
Showing 10 questions Sign up for moreA nurse is collecting data from a client who is postpartum. Which of the following findings should alert the nurse to the possibility of a postpartum complication?
Explanation
Choice A reason:
A urinary output of 2,000 mL/12 hr is normal for a postpartum client, as the body eliminates excess fluid accumulated during pregnancy.
Choice B reason:
A temperature of 100.4 F for two days indicates a possible infection, such as endometritis or mastitis, and requires further evaluation and treatment.
Choice C reason:
Chills shortly following delivery are common and benign and are caused by hormonal changes and fluid shifts.
Choice D reason:
A fundus at the umbilicus level is expected for a postpartum client and indicates that the uterus is involuting properly.

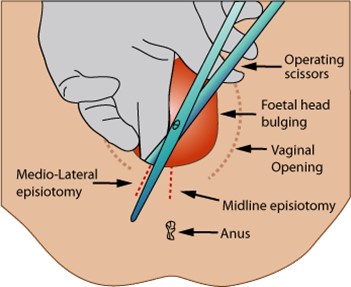
A nurse is caring for a client who has unrelieved episiotomy pain 8 hr following delivery. Which of the following actions should the nurse take?
Explanation
Choice A reason:
A warm sitz bath can promote healing and comfort, but it is not recommended until 24 hr after delivery, as it can increase swelling and bleeding.
Choice B reason:
An ice pack can reduce inflammation and pain by causing vasoconstriction and numbing the area. It should be applied for 20 minutes at a time, with a cloth barrier between the skin and the ice.
Choice C reason:
A soft pillow under the client's butocks can increase pressure on the perineum and worsen the pain. The client should be encouraged to lie on her side or sit in a semi-Fowler's position.
Choice D reason:
A heating lamp can dry out the wound and delay healing. It can also cause burns and discomfort. It should be avoided for episiotomy care.
A nurse is assisting with the care of a client who is multigravid and in active labor with 7 cm of cervical dilation and 100% effacement. The fetus is at +1 station, and the client's amniotic membranes are intact. The client suddenly states that she needs to push. Which of the following is the appropriate nursing response?
Explanation
Choice A reason:
Panting can help prevent premature pushing and reduce the risk of cervical edema or laceration. The client should be instructed to take short, shallow breaths through her mouth during contractions until she reaches 10 cm of dilation.
Choice B reason:
Assessing the perineum for signs of crowning is not a priority at this stage, as the fetus is not yet at a low enough station to be visible. Crowning usually occurs when the fetus is at +4 or +5 station.
Choice C reason:
Assisting the client into a comfortable position is important, but it does not address the urge to push. The client should be encouraged to change positions frequently to promote fetal descent and comfort.
Choice D reason:
Helping the client to the bathroom to empty her bladder is not advisable, as it can increase the risk of cord prolapse or rupture of membranes. The client should have an indwelling catheter inserted if she is unable to void spontaneously.
A nurse is caring for a client 2 hr following a spontaneous vaginal delivery and notes that the client has saturated two perineal pads with blood in a 30-min period. Which of the following actions should the nurse take first?
Explanation
Choice A reason:
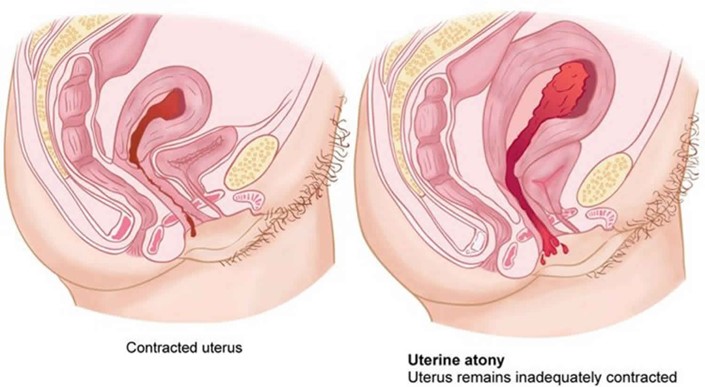
Checking the consistency of the client's uterine fundus is the first action the nurse should take, as it can indicate the cause of excessive bleeding. A boggy or soft fundus indicates uterine atony, which is the most common cause of postpartum hemorrhage. The nurse should massage the fundus until it becomes firm and contracted.
Choice B reason:
Having the client use the bedpan to urinate is an important action, as a full bladder can displace the uterus and prevent it from contracting properly. However, this is not the first action the nurse should take, as it does not address the immediate source of bleeding.
Choice C reason:
Increasing the client's fluid intake is an important action, as it can help replace fluid loss and prevent hypovolemia and shock. However, this is not the first action the nurse should take, as it does not stop the bleeding.
Choice D reason:
Preparing to administer oxytocic medication is an important action, as it can stimulate uterine contractions and reduce bleeding. However, this is not the first action the nurse should take, as it requires a provider's prescription and may not be necessary if fundal massage is effective.
A nurse is caring for a client who is 12 hr postpartum. The nurse recognizes the client is in the dependent, taking-in phase of maternal postpartum adjustment. Which of the following is an expected finding during this period?
Explanation
Expressions of excitement are typical during the dependent, taking-in phase, which lasts for the first 24 to 48 hr after delivery. The client may relive and review her labor and delivery experience, and may need reassurance and validation from others.
Choice B reason:
Lack of appetite is not an expected finding during the dependent, taking-in phase, as the client may have increased hunger and thirst after delivery. The nurse should encourage adequate nutrition and hydration to promote healing and lactation.
Choice C reason:
Eagerness to learn newborn care skills is more characteristic of the dependent-independent, taking-hold phase, which begins around the third day postpartum. During this phase, the client becomes more confident and interested in caring for herself and her newborn.
ChoiceD reason:
Focus on the family unit and its members is more characteristic of the interdependent, letting-go phase, which occurs after the first week postpartum. During this phase, the client redefines her role within the family and society, and integrates the newborn into her life.
A nurse is caring for a client following a cesarean birth. The client tells the nurse that she is hungry. Which of the following actions should the nurse take first?
Explanation
Choice B reason:
Auscultating the client's abdomen is the first action the nurse should take, as it can assess the return of bowel function after surgery. The nurse should listen for bowel sounds in all four quadrants, and note their frequency and quality.
Offering clear liquids is an important action, as it can provide hydration and nutrition for the client. However, this is not the first action the nurse should take, as it may cause nausea and vomiting if the client's bowel function has not returned.
Choice C reason:
Checking the client's chart for a diet prescription is an important action, as it can ensure that the client follows the provider's orders and does not consume anything contraindicated. However, this is not the first action the nurse should take, as it does not address the client's hunger or bowel function.
Choice D reason:
Giving the client soda crackers is an important action, as it can provide a bland and easily digestible food for the client. However, this is not the first action the nurse should take, as it may be too solid for the client's stomach if her bowel function has not returned.
A nurse is assessing a client who is 8 hr postpartum and multiparous. Which of the following findings should alert the nurse to the client's need to urinate?
Explanation
Choice B reason:
A fundus that is elevated and displaced from the midline indicates a full bladder, which can interfere with uterine contraction and increase the risk of hemorrhage. The nurse should assist the client to void or catheterize her if necessary.
Choice A reason:
Moderate swelling of the labia is a normal finding after vaginal delivery, and does not indicate a need to urinate. The nurse should apply ice packs and perineal pads to reduce edema and discomfort.
Choice C reason:
Moderate lochia rubra is a normal finding during the first 24 hr postpartum, and does not indicate a need to urinate. The nurse should monitor the amount and color of lochia, and change the perineal pads as needed.
Choice D reason:
A blood pressure of 130/84 mm Hg is within the normal range for a postpartum client, and does not indicate a need to urinate. The nurse should monitor the blood pressure for signs of hypertension or hypotension, which can indicate complications such as preeclampsia or hemorrhage.
A nurse is caring for a postpartum client following a vaginal birth of a newborn weighing 4252 g (9 lb 6 oz). The nurse should identify that this client is at risk for which of the following postpartum complications?
Explanation
Choice B reason:
Uterine atony is the failure of the uterus to contract and retract after delivery, which can lead to excessive bleeding and hemorrhage. The client is at risk for uterine atony due to delivering a large newborn, which can overstretch the uterine muscles and reduce their tone.
Choice A reason:
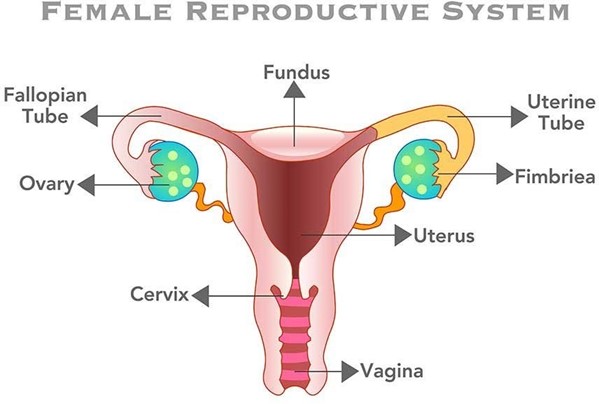
Puerperal infection is an infection of the reproductive tract that occurs within six weeks after delivery. The client is not at increased risk for puerperal infection due to delivering a large newborn, unless there are other factors such as prolonged labor, multiple vaginal exams, or episiotomy.
Choice C reason:
Thrombophlebitis is an inflammation of a vein with a blood clot formation. The client is not at increased risk for thrombophlebitis due to delivering a large newborn, unless there are other factors such as immobility, dehydration, or trauma.
Choice D reason:
Retained placental fragments are pieces of the placenta that remain in the uterus after delivery, which can cause bleeding and infection. The client is not at increased risk for retained placental fragments due to delivering a large newborn, unless there are other factors such as abnormal placental atachment, manual removal, or incomplete separation.
A nurse is assisting with the care of a client who had an epidural anesthesia block during the early stages of labor. The client's blood pressure is 80/40 mm Hg and the fetal heart recording is 140/min. Which of the following actions should the nurse take first?
Explanation
Choice A reason:
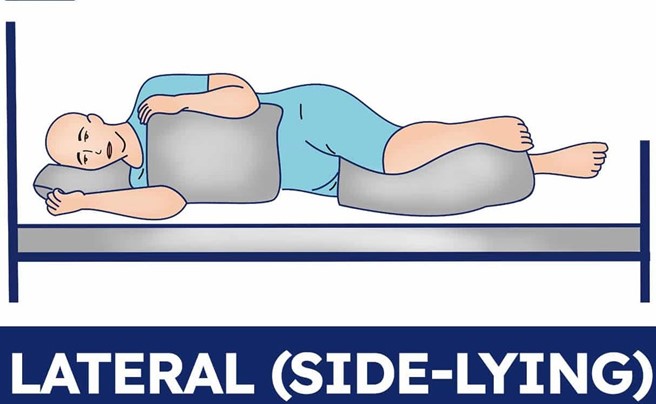
Placing the client in a lateral position is the first action the nurse should take, as it can improve maternal and fetal circulation by relieving pressure on the inferior vena cava. The client's blood pressure is low, which can indicate hypotension due to epidural anesthesia or supine hypotension syndrome.
Choice B reason:
Notifying the provider is an important action, as it can facilitate further interventions and monitoring for the client and the fetus. However, this is not the first action the nurse should take, as it does not address the immediate problem of hypotension.
Choice C reason:
Increasing IV fluid rate is an important action, as it can expand blood volume and increase blood pressure. However, this is not the first action the nurse should take, as it may not be effective if the client is in a supine position.
Choice D reason:
Elevating the legs is an important action, as it can enhance venous return and increase blood pressure. However, this is not the first action the nurse should take, as it may worsen supine hypotension syndrome by increasing pressure on the inferior vena cava.
A nurse is assisting with the care of a client who is in the first stage of labor. The nurse observes the umbilical cord protruding from the vagina. Which of the following actions should the nurse take first?
Explanation
Choice D reason:
Placing the client in a knee-chest or Trendelenburg position is the first action the nurse should take, as it can relieve pressure on the cord and prevent compression and fetal hypoxia. The nurse should also use a sterile gloved hand to hold the presenting part off the cord.
Choice A reason:
Preparing the client for an emergency cesarean birth is an important action, as it can facilitate prompt delivery and prevent fetal compromise. However, this is not the first action the nurse should take, as it does not address the immediate problem of cord prolapse.
Choice B reason:
Covering the cord with a sterile, moist saline dressing is an important action, as it can prevent drying and infection of the cord. However, this is not the first action the nurse should take, as it does not address the immediate problem of cord compression.
Choice C reason:
Explaining to the client what is happening is an important action, as it can provide emotional support and education for the client. However, this is not the first action the nurse should take, as it does not address the immediate problem of cord prolapse.
You just viewed 10 questions out of the 44 questions on the ATI Maternity Exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

