A nurse is assessing a client who is 8 hr postpartum and multiparous. Which of the following findings should alert the nurse to the client's need to urinate?
Moderate swelling of the labia
Fundus three fingerbreadths above the umbilicus
Moderate lochia rubra
Blood pressure 130/84 mm Hg
The Correct Answer is B
Choice B reason:
A fundus that is elevated and displaced from the midline indicates a full bladder, which can interfere with uterine contraction and increase the risk of hemorrhage. The nurse should assist the client to void or catheterize her if necessary.
Choice A reason:
Moderate swelling of the labia is a normal finding after vaginal delivery, and does not indicate a need to urinate. The nurse should apply ice packs and perineal pads to reduce edema and discomfort.
Choice C reason:
Moderate lochia rubra is a normal finding during the first 24 hr postpartum, and does not indicate a need to urinate. The nurse should monitor the amount and color of lochia, and change the perineal pads as needed.
Choice D reason:
A blood pressure of 130/84 mm Hg is within the normal range for a postpartum client, and does not indicate a need to urinate. The nurse should monitor the blood pressure for signs of hypertension or hypotension, which can indicate complications such as preeclampsia or hemorrhage.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
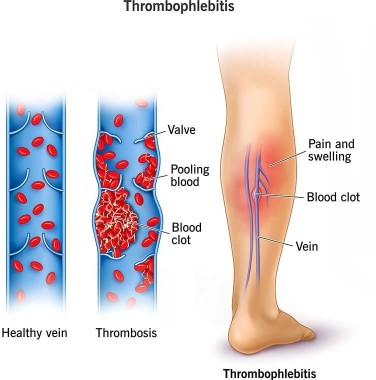
Choice A reason: Apply warm, moist soaks to the client's lower legs is incorrect, as this action is not effective for preventing thrombophlebitis. Warm, moist soaks can provide comfort and reduce inflammation, but they do not improve blood circulation or prevent clot formation.
Choice B reason: Have the client ambulate frequently in the hallway is correct, as this action can prevent thrombophlebitis by improving venous return and preventing stasis. The nurse should encourage and assist the client to ambulate early and frequently after a cesarean birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide support as needed.
Choice C reason: Keep the client on bed rest is incorrect, as this action can increase the risk of thrombophlebitis by reducing blood flow and promoting stasis. Bed rest can also delay wound healing and increase the risk of infection and deconditioning. The nurse should avoid keeping the client on bed rest unless absolutely necessary.
Choice D reason: Place pillows under the client's knees while she is resting in bed is incorrect, as this action can impair blood circulation and increase the risk of thrombophlebitis. Placing pillows under the knees can cause pressure on the popliteal veins and reduce venous return. The nurse should advise the client to avoid crossing their legs or placing pillows under their knees while resting in bed.
Correct Answer is D
Explanation
Choice A reason:
Maternal opioid administration is incorrect, as this factor can cause late decelerations in the fetal heart rate. Late decelerations are symmetrical decreases in the FHR that begin after the peak of the contraction and return to baseline after the contraction ends, which indicate uteroplacental insufficiency. Maternal opioid administration can reduce maternal blood pressure and placental perfusion, leading to fetal hypoxia.
Choice B reason:
Fetal head compression is incorrect, as this factor can cause early decelerations in the fetal heart rate. Early decelerations are symmetrical decreases in the FHR that mirror the contractions, which indicate fetal head compression and vagal stimulation. Fetal head compression occurs as the fetus descends into the birth canal and does not pose a threat to the fetal well-being.
Choice C reason:
Uteroplacental insufficiency is incorrect, as this factor can cause late decelerations in the fetal heart rate. Uteroplacental insufficiency refers to a reduced blood flow and oxygen delivery to the fetus through the placenta, which can result from maternal hypotension, uterine hyperstimulation, placental abruption, or other conditions. Uteroplacental insufficiency can cause fetal hypoxia and acidosis.
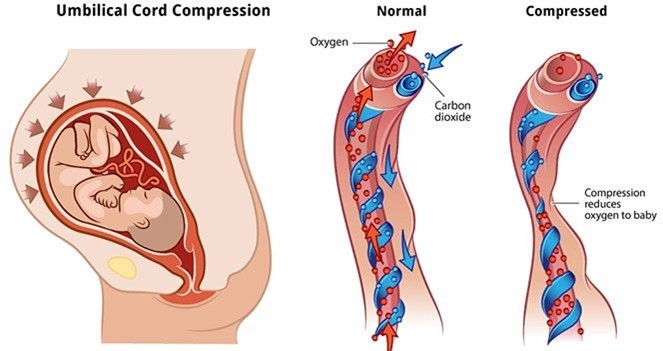
Choice D reason:
Umbilical cord compression is correct, as this factor can cause variable decelerations in the fetal heart rate. Variable decelerations are abrupt decreases in the FHR that vary in onset, duration, and depth, which indicate umbilical cord compression and reduced blood flow to the fetus. Umbilical cord compression can occur due to cord prolapse, nuchal cord, short cord, or other causes. The nurse should reposition the client, administer oxygen, and prepare for delivery if indicated.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today