A nurse is collecting data from a client who is 14 hr postpartum. The nurse notes breasts soft, fundus firm, slightly deviated to the right; moderate lochia rubra; temperature 37.7° C (100° F), pulse rate 88/min, respiratory rate 18/min. Which of the following actions should the nurse perform?
Encourage the client to nurse more frequently so her milk will come in.
Increase IV fluids.
Ask the client to empty her bladder.
Report the client's temperature elevation.
The Correct Answer is C
Choice A reason: Encourage the client to nurse more frequently so her milk will come in is incorrect, as this action is not related to the data collected by the nurse. The nurse notes that the client's breasts are soft, which indicates that the milk has not come in yet. This is normal and expected for a client who is 14 hr postpartum, as milk production usually begins around 72 to 96 hr after birth. The nurse should encourage the client to nurse frequently and effectively to stimulate milk production and prevent engorgement.
Choice B reason: Increase IV fluids is incorrect, as this action is not indicated by the data collected by the nurse. The nurse notes that the client's vital signs are within normal limits, except for a slight temperature elevation. Increasing IV fluids can cause fluid overload and electrolyte imbalance in the client. The nurse should maintain the IV fluids at the prescribed rate and monitor the client's intake and output.
Choice C reason: Ask the client to empty her bladder is correct, as this action is indicated by the data collected by the nurse. The nurse notes that the client's fundus is firm but slightly deviated to the right, which suggests bladder distension. A full bladder can interfere with uterine contraction and involution and increase the risk of hemorrhage and infection. The nurse should assist the client to empty their bladder and reassess the fundal position.
Choice D reason: Report the client's temperature elevation is incorrect, as this action is not necessary for a slight temperature elevation in a postpartum client. The nurse notes that the client's temperature is 37.7° C (100° F), which is slightly above normal but within the range of expected findings for a postpartum client. A mild temperature elevation in the first 24 hr after birth can be due to dehydration, exertion, or hormonal changes and does not indicate infection. The nurse should encourage oral fluid intake and monitor the temperature every 4 hr.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason:
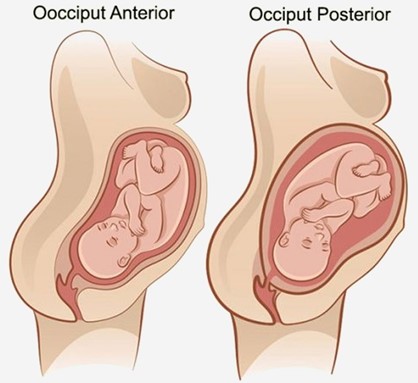
Fetal position is persistent occiput posterior is correct, as this position can cause difficult, prolonged labor and severe backache. The occiput posterior position means that the back of the fetal head is facing the maternal sacrum, which can result in poor alignment and descent, increased pressure on the maternal sacrum and nerves, and increased risk of perineal trauma. The nurse should encourage the client to change positions frequently, use pelvic rocking exercises, apply counterpressure to the sacrum, and administer analgesics as needed.
Choice B reason:
Fetal attitude is in general flexion is incorrect, as this attitude can facilitate normal labor and delivery. The fetal attitude refers to the degree of flexion or extension of the fetal head and limbs in relation to the fetal trunk. General flexion means that the fetal head is flexed on the chest, the arms are crossed over the chest, and the legs are flexed at the knees. This attitude allows the smallest diameter of the fetal head to pass through the birth canal.
Choice C reason:
Fetal lie is longitudinal is incorrect, as this lie can facilitate normal labor and delivery. The fetal lie refers to the relationship between the long axis of the fetus and the long axis of the mother. Longitudinal lie means that both axes are parallel, which allows for either a vertex (head-first) or a breech (butocks-first) presentation.
Choice D reason:
Maternal pelvis is gynecoid is incorrect, as this pelvis can facilitate normal labor and delivery. The maternal pelvis refers to the shape and size of the bony pelvis that affects the passage of the fetus. Gynecoid pelvis is the most common and favorable type for vaginal birth, as it has a rounded inlet, a wide pubic arch, and adequate outlet dimensions.
Correct Answer is A
Explanation
Choice A reason: The client is Rh negative and the newborn is Rh positive is correct, as this finding indicates a risk of Rh incompatibility and sensitization. Rh incompatibility occurs when the mother has Rh-negative blood and the baby has Rh-positive blood, which can cause maternal antibodies to atack the fetal red blood cells. Sensitization occurs when the maternal antibodies cross the placenta and enter the fetal circulation, which can cause hemolytic disease of the newborn. The nurse should administer Rho(D) immune globulin to prevent sensitization and protect future pregnancies.
Choice B reason: The client is Rh negative and the newborn is Rh negative is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If both the mother and the baby have Rh-negative blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Choice C reason: The client is Rh positive and the newborn is Rh positive is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If both the mother and the baby have Rh-positive blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Choice D reason: The client is Rh positive and the newborn is Rh negative is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If the mother has Rh-positive blood and the baby has Rh- negative blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today