A nurse is preparing to administer dinoprostone gel to a client who is pregnant. The client asks the nurse about the purpose of the medication. Which of the following responses should the nurse make?
Dinoprostone stimulates uterine contractions.
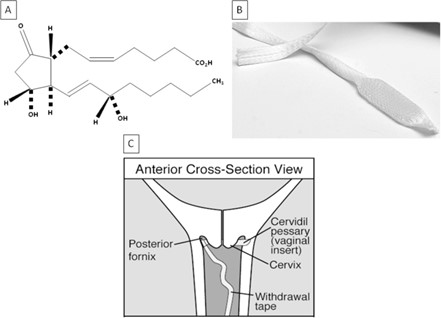
Dinoprostone promotes softening of the cervix.
Dinoprostone relaxes uterine contractions.
Dinoprostone assists with ending the pregnancy.
The Correct Answer is B
Choice A reason:
Dinoprostone stimulates uterine contractions is incorrect, as this is not the primary purpose of the medication. Dinoprostone is a prostaglandin that can induce labor by ripening the cervix and enhancing uterine contractility, but it is not used solely for stimulating contractions.
Choice B reason:
Dinoprostone promotes softening of the cervix is correct, as this is the main purpose of the medication. Dinoprostone is used to prepare the cervix for labor by increasing its softness, dilation, and effacement. This can facilitate the descent of the fetus and shorten the duration of labor.
Choice C reason:
Dinoprostone relaxes uterine contractions is incorrect, as this is the opposite effect of the medication. Dinoprostone can increase uterine tone and frequency, which can help initiate or augment labor. The nurse should monitor the client for signs of uterine hyperstimulation or fetal distress.
Choice D reason:
Dinoprostone assists with ending the pregnancy is incorrect, as this is not the intended use of the medication. Dinoprostone can be used to terminate a pregnancy in some cases, such as fetal demise or missed abortion, but it is not routinely used for this purpose. The nurse should explain to the client that dinoprostone is used to induce labor and not to end a pregnancy.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: In 3 to 5 days after delivery is correct, as this is the average time for breast milk production to begin after birth. Breast milk production is stimulated by the drop in progesterone levels that occurs after the placenta is delivered, as well as by the suckling of the baby. The nurse should encourage the client to breastfeed frequently and effectively to promote milk production and prevent engorgement.
Choice B reason: In 6 to 8 days after delivery is incorrect, as this is a longer than average time for breast milk production to begin after birth. Breast milk production usually begins within the first week after birth, although it may vary depending on individual factors. The nurse should assess the client for any factors that may delay or inhibit milk production, such as stress, fatigue, pain, or medication.
Choice C reason: Within 2 days after delivery is incorrect, as this is a shorter than average time for breast milk production to begin after birth. Breast milk production usually begins within the first week after birth, although it may vary depending on individual factors. The nurse should educate the client that before breast milk comes in, the breasts produce colostrum, which is a thick, yellowish fluid that contains antibodies and nutrients for the baby.
Choice D reason: In about 10 days after delivery is incorrect, as this is a longer than average time for breast milk production to begin after birth. Breast milk production usually begins within the first week after birth, although it may vary depending on individual factors. The nurse should assess the client for any factors that may delay or inhibit milk production, such as stress, fatigue, pain, or medication.
Correct Answer is B
Explanation
Choice A reason: Perform fundal massage is incorrect, as this action is not indicated for a client who has a firm and midline fundus. Fundal massage is used to stimulate uterine contraction and prevent hemorrhage in clients who have a boggy or deviated fundus.
Choice B reason: Assist the client to ambulate is correct, as this action can promote lochia drainage and prevent pooling of blood in the vagina. The nurse should encourage the client to ambulate early and frequently after birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide assistance as needed.
Choice C reason: Check for blood under the client's butock is incorrect, as this action is not necessary for a client who has a small amount of lochia rubra on the perineal pad. Lochia rubra is normal and expected in the first few days after birth, and it indicates that the placental site is healing. The nurse should check for blood under the butock only if there is suspicion of excessive bleeding or concealed hemorrhage.
Choice D reason: Increase the rate of the IV fluids is incorrect, as this action is not indicated for a client who has a small amount of lochia rubra on the perineal pad. Increasing the rate of IV fluids can cause fluid overload and electrolyte imbalance in the client. The nurse should maintain the IV fluids at the prescribed rate and monitor the client's intake and output.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today