A nurse is assisting with the care of a client who is in labor. The client's labor is difficult and prolonged and she reports a severe backache. Which of the following factors is a contributing cause of difficult, prolonged labor?
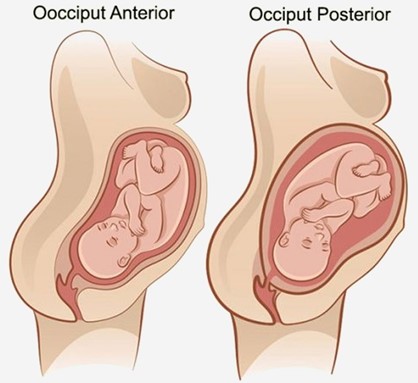
Fetal position is persistent occiput posterior.
Fetal attitude is in general flexion.
Fetal lie is longitudinal.
Maternal pelvis is gynecoid.
The Correct Answer is A
Choice A reason:
Fetal position is persistent occiput posterior is correct, as this position can cause difficult, prolonged labor and severe backache. The occiput posterior position means that the back of the fetal head is facing the maternal sacrum, which can result in poor alignment and descent, increased pressure on the maternal sacrum and nerves, and increased risk of perineal trauma. The nurse should encourage the client to change positions frequently, use pelvic rocking exercises, apply counterpressure to the sacrum, and administer analgesics as needed.
Choice B reason:
Fetal attitude is in general flexion is incorrect, as this attitude can facilitate normal labor and delivery. The fetal attitude refers to the degree of flexion or extension of the fetal head and limbs in relation to the fetal trunk. General flexion means that the fetal head is flexed on the chest, the arms are crossed over the chest, and the legs are flexed at the knees. This attitude allows the smallest diameter of the fetal head to pass through the birth canal.
Choice C reason:
Fetal lie is longitudinal is incorrect, as this lie can facilitate normal labor and delivery. The fetal lie refers to the relationship between the long axis of the fetus and the long axis of the mother. Longitudinal lie means that both axes are parallel, which allows for either a vertex (head-first) or a breech (butocks-first) presentation.
Choice D reason:
Maternal pelvis is gynecoid is incorrect, as this pelvis can facilitate normal labor and delivery. The maternal pelvis refers to the shape and size of the bony pelvis that affects the passage of the fetus. Gynecoid pelvis is the most common and favorable type for vaginal birth, as it has a rounded inlet, a wide pubic arch, and adequate outlet dimensions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Inform the client that she can go to the bathroom whenever needed is incorrect, as this action can put the client at risk of injury or complications. The client may experience orthostatic hypotension, dizziness, weakness, or bleeding after a vaginal birth, which can impair their ability to ambulate safely and independently. The nurse should assist the client to the bathroom and monitor their vital signs and lochia.
Choice B reason: This is the correct action. The nurse should assess the client for any residual effects of analgesia, such as dizziness or unsteadiness, which could increase the risk of falls if the client tries to get up.
Choice C reason: Advise the client to remain in bed for the next few hours is incorrect, as this action can increase the risk of bladder distension, infection, or thrombosis. The nurse should encourage and assist the client to ambulate early and frequently after a vaginal birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide support as needed.
Choice D reason: While assisting the client is a good approach, it is important to first evaluate her condition to ensure it is safe for her to get out of bed. If she has been assessed and is deemed safe to ambulate, assisting her to the bathroom with support might be appropriate. However, the initial step is to assess her condition.
Correct Answer is B
Explanation
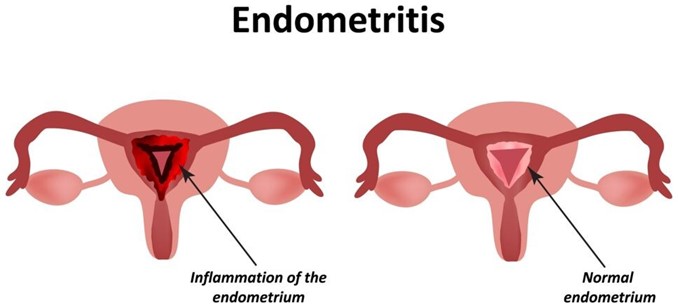
Choice A reason: Hematuria is blood in the urine. It is not a symptom of endometritis, which is an inflammation or infection of the uterine lining. Hematuria can have many other causes, such as urinary tract infections, kidney stones, bladder cancer, or trauma.
Choice B reason: Pelvic pain is one of the most common symptoms of endometritis. It can be caused by the inflammation or infection of the uterine lining, which can also spread to other pelvic organs. Pelvic pain can be dull, sharp, cramping, or constant, and it may worsen with movement or intercourse¹³.
Choice C reason: Pink lochia is normal vaginal discharge after childbirth. It consists of blood, mucus, and tissue from the uterus. It usually lasts for a few weeks and gradually changes color from red to pink to brown to white. Pink lochia is not a sign of endometritis, unless it is foul-smelling, heavy, or persists beyond six weeks.
Choice D reason: Bradycardia is a slow heart rate, usually below 60 beats per minute. It is not a symptom of endometritis, which can cause fever and tachycardia (fast heart rate). Bradycardia can have many other causes, such as heart disease, medication side effects, hypothyroidism, or electrolyte imbalance.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today