A nurse is caring for a client who is postpartum and is breastfeeding her infant. Which of the following findings indicates mastitis?
Swelling in both breasts
Cracked and bleeding nipples
Increase in breast milk
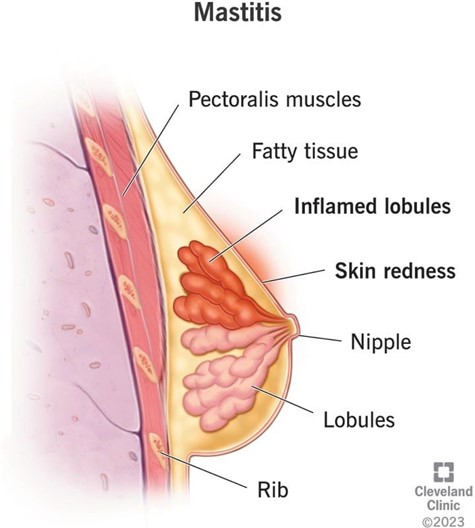
Red and painful area in one breast
The Correct Answer is D
Choice A reason: Swelling in both breasts is incorrect, as this finding does not indicate mastitis. Swelling in both breasts can occur due to engorgement, which is a normal and expected phenomenon in the first few days after birth or when milk production increases. Engorgement can cause breast fullness, tenderness, and warmth, but it does not cause infection or inflammation.
Choice B reason: Cracked and bleeding nipples is incorrect, as this finding does not indicate mastitis. Cracked and bleeding nipples can occur due to poor latch, improper positioning, or excessive suction of the baby. Cracked and bleeding nipples can cause pain, discomfort, and risk of infection, but they do not cause mastitis by themselves.
Choice C reason: Increase in breast milk is incorrect, as this finding does not indicate mastitis. Increase in breast milk can occur due to hormonal changes, frequent breastfeeding, or stimulation of the breasts. Increase in breast milk can cause engorgement, but it does not cause infection or inflammation.
Choice D reason: Red and painful area in one breast is correct, as this finding indicates mastitis. Mastitis is an infection and inflammation of the breast tissue that usually affects one breast at a time. Mastitis can cause redness, pain, swelling, warmth, and fever in the affected breast. Mastitis can occur due to blocked milk ducts, bacterial invasion, or poor hygiene. The nurse should advise the client to continue breastfeeding or pumping, apply warm compresses, massage the breast gently, and take antibiotics as prescribed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
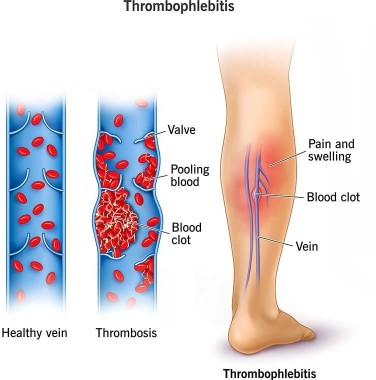
Choice A reason: Apply warm, moist soaks to the client's lower legs is incorrect, as this action is not effective for preventing thrombophlebitis. Warm, moist soaks can provide comfort and reduce inflammation, but they do not improve blood circulation or prevent clot formation.
Choice B reason: Have the client ambulate frequently in the hallway is correct, as this action can prevent thrombophlebitis by improving venous return and preventing stasis. The nurse should encourage and assist the client to ambulate early and frequently after a cesarean birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide support as needed.
Choice C reason: Keep the client on bed rest is incorrect, as this action can increase the risk of thrombophlebitis by reducing blood flow and promoting stasis. Bed rest can also delay wound healing and increase the risk of infection and deconditioning. The nurse should avoid keeping the client on bed rest unless absolutely necessary.
Choice D reason: Place pillows under the client's knees while she is resting in bed is incorrect, as this action can impair blood circulation and increase the risk of thrombophlebitis. Placing pillows under the knees can cause pressure on the popliteal veins and reduce venous return. The nurse should advise the client to avoid crossing their legs or placing pillows under their knees while resting in bed.
Correct Answer is A
Explanation
Choice A reason: A precipitous birth is a delivery that occurs in less than 3 hours from the onset of labor. This can cause uterine atony, which is the failure of the uterus to contract and compress the blood vessels after the placenta is delivered. Uterine atony is the most common cause of postpartum hemorrhage²³.
Choice B reason: A small for gestational age newborn is not a risk factor for postpartum hemorrhage. It may be associated with other conditions, such as placental insufficiency or intrauterine growth restriction, but these do not directly increase the risk of bleeding after delivery.
Choice C reason: A two-vessel umbilical cord is a cord that has one artery and one vein instead of the normal two arteries and one vein. This can be a marker for congenital anomalies or placental abnormalities, but it does not increase the risk of postpartum hemorrhage by itself.
Choice D reason: Gestational hypertension is a condition where the blood pressure rises above 140/90 mm Hg after 20 weeks of pregnancy. It can lead to complications such as preeclampsia, eclampsia, or HELLP syndrome, which can affect the clotting system and cause bleeding disorders. However, gestational hypertension alone does not increase the risk of postpartum hemorrhage unless it is associated with these severe conditions¹⁴.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today