A nurse is assisting with the care of a client who had an epidural anesthesia block during the early stages of labor. The client's blood pressure is 80/40 mm Hg and the fetal heart recording is 140/min. Which of the following actions should the nurse take first?
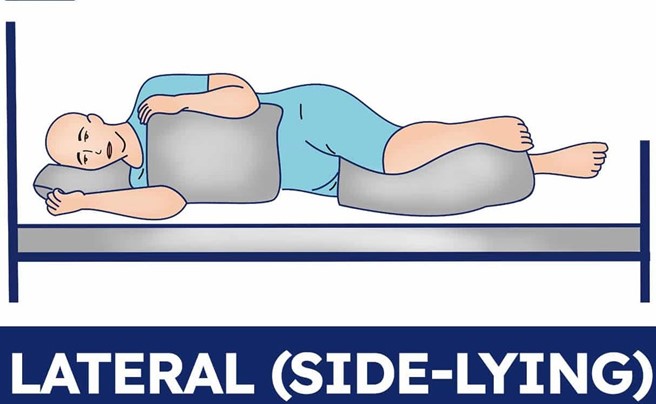
Place the client in a lateral position.
Notify the provider.
Increase IV fluid rate.
Elevate the legs.
The Correct Answer is A
Choice A reason:
Placing the client in a lateral position is the first action the nurse should take, as it can improve maternal and fetal circulation by relieving pressure on the inferior vena cava. The client's blood pressure is low, which can indicate hypotension due to epidural anesthesia or supine hypotension syndrome.
Choice B reason:
Notifying the provider is an important action, as it can facilitate further interventions and monitoring for the client and the fetus. However, this is not the first action the nurse should take, as it does not address the immediate problem of hypotension.
Choice C reason:
Increasing IV fluid rate is an important action, as it can expand blood volume and increase blood pressure. However, this is not the first action the nurse should take, as it may not be effective if the client is in a supine position.
Choice D reason:
Elevating the legs is an important action, as it can enhance venous return and increase blood pressure. However, this is not the first action the nurse should take, as it may worsen supine hypotension syndrome by increasing pressure on the inferior vena cava.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason:
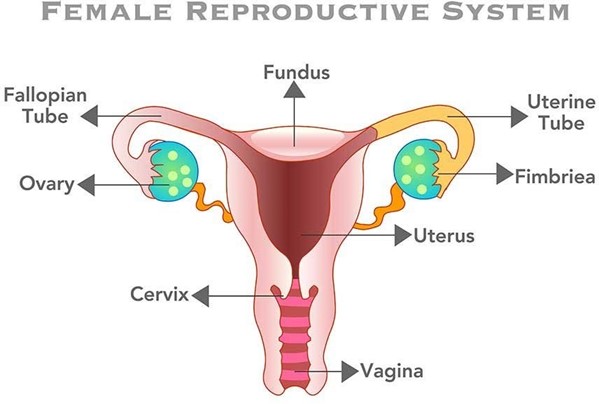
Checking the consistency of the client's uterine fundus is the first action the nurse should take, as it can indicate the cause of excessive bleeding. A boggy or soft fundus indicates uterine atony, which is the most common cause of postpartum hemorrhage. The nurse should massage the fundus until it becomes firm and contracted.
Choice B reason:
Having the client use the bedpan to urinate is an important action, as a full bladder can displace the uterus and prevent it from contracting properly. However, this is not the first action the nurse should take, as it does not address the immediate source of bleeding.
Choice C reason:
Increasing the client's fluid intake is an important action, as it can help replace fluid loss and prevent hypovolemia and shock. However, this is not the first action the nurse should take, as it does not stop the bleeding.
Choice D reason:
Preparing to administer oxytocic medication is an important action, as it can stimulate uterine contractions and reduce bleeding. However, this is not the first action the nurse should take, as it requires a provider's prescription and may not be necessary if fundal massage is effective.
Correct Answer is ["C","D","E"]
Explanation
Choice A reason: While ice packs can help reduce swelling and discomfort, they are not essential for preventing infection.
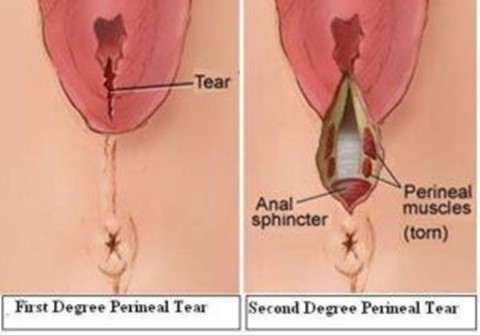
Choice B reason: Sit on an inflatable donut to protect the perineum is incorrect, as this can increase pressure and blood flow to the perineum and delay healing. The nurse should advise the client to avoid sitting on hard or uneven surfaces and to use a pillow or a cushion for comfort.
Choice C reason: Perform hand hygiene before and after voiding is correct, as this can prevent contamination and infection of the perineal area. The nurse should instruct the client to wash their hands with soap and water or use an alcohol-based hand sanitizer before and after using the toilet.
Choice D reason: Blot the perineal area dry after voiding is correct, as this can keep the perineal area clean and dry and prevent irritation and infection. The nurse should instruct the client to use a clean, soft cloth or tissue and gently pat or blot the perineal area from front to back after voiding.
Choice E reason: Clean the perineal area from front to back is correct, as this can prevent bacteria from entering the vagina or urethra and causing infection. The nurse should instruct the client to use a peri-botle filled with warm water and squirt it over the perineal area from front to back after each voiding or bowel movement. The client should also change their perineal pad frequently and dispose of it properly.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today