A nurse is collecting data from a client who is 3 days postpartum and is breastfeeding. Her fundus is three fingerbreadths below the umbilicus, and her lochia rubra is moderate. Her breasts feel hard and warm. Which of the following recommendations should the nurse give the client?
Wear a nipple shield.
Express milk from both breasts.
Obtain a prescription for an antibiotic.
Apply a heating pad to her breasts.
The Correct Answer is B
Choice A reason: Wear a nipple shield is incorrect, as this recommendation is not indicated for a client who has engorged breasts. A nipple shield is a thin, flexible device that covers the nipple and areola and can help with latch problems, flat or inverted nipples, or sore nipples. However, a nipple shield can also reduce milk transfer, stimulate less milk production, and cause nipple confusion or preference.
Choice B reason: Express milk from both breasts is correct, as this recommendation can help relieve engorgement and maintain milk production. Engorgement is a normal and expected phenomenon that occurs when the milk comes in, usually around 72 to 96 hr after birth. Engorgement can cause breast fullness, tenderness, warmth, and hardness. The nurse should advise the client to express milk from both breasts by breastfeeding frequently and effectively or by using a breast pump or hand expression.
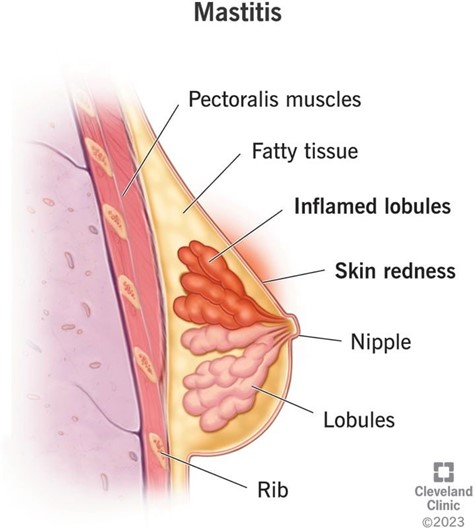
Choice C reason: Obtain a prescription for an antibiotic is incorrect, as this recommendation is not indicated for a client who has engorged breasts. An antibiotic is used to treat mastitis, which is an infection and inflammation of the breast tissue that can cause redness, pain, swelling, warmth, and fever in the affected breast. The nurse should assess the client for signs of mastitis and report any abnormal findings to the provider.
Choice D reason: Apply a heating pad to her breasts is incorrect, as this recommendation can worsen engorgement and cause discomfort. A heating pad can increase blood flow and swelling in the breasts, which can impair milk flow and increase pain. The nurse should advise the client to apply cold compresses or cabbage leaves to her breasts to reduce inflammation and discomfort.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice B reason:
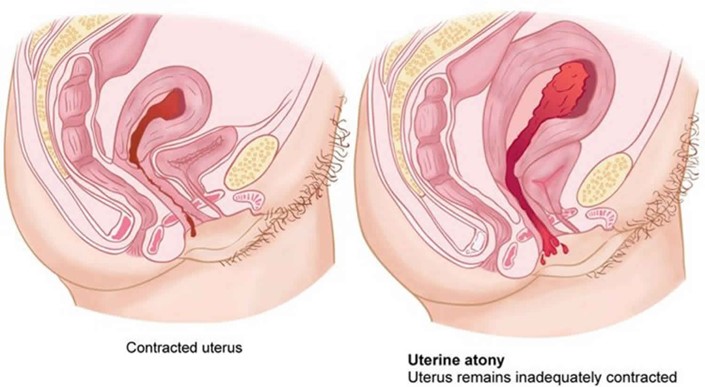
Uterine atony is the failure of the uterus to contract and retract after delivery, which can lead to excessive bleeding and hemorrhage. The client is at risk for uterine atony due to delivering a large newborn, which can overstretch the uterine muscles and reduce their tone.
Choice A reason:
Puerperal infection is an infection of the reproductive tract that occurs within six weeks after delivery. The client is not at increased risk for puerperal infection due to delivering a large newborn, unless there are other factors such as prolonged labor, multiple vaginal exams, or episiotomy.
Choice C reason:
Thrombophlebitis is an inflammation of a vein with a blood clot formation. The client is not at increased risk for thrombophlebitis due to delivering a large newborn, unless there are other factors such as immobility, dehydration, or trauma.
Choice D reason:
Retained placental fragments are pieces of the placenta that remain in the uterus after delivery, which can cause bleeding and infection. The client is not at increased risk for retained placental fragments due to delivering a large newborn, unless there are other factors such as abnormal placental atachment, manual removal, or incomplete separation.
Correct Answer is D
Explanation
Choice A reason: Amniotic fluid in the vaginal vault indicates that the membranes have ruptured, but this does not necessarily mean that the client is in labor. Some women may have a slow leak of amniotic fluid for hours or days before labor begins. Rupture of membranes also increases the risk of infection, so the nurse should monitor the client's temperature and fetal heart rate.
Choice B reason: Contractions every 3 to 4 minutes are a sign of labor, but they are not enough to confirm it. The nurse should also assess the duration and intensity of the contractions, as well as the client's response to them. Some women may have false labor contractions, also known as Braxton Hicks contractions, which are irregular, mild, and do not cause cervical changes.
Choice C reason: Pain just above the navel is not a typical sign of labor. It may indicate other problems, such as placental abruption, uterine rupture, or fetal distress. The nurse should report this finding to the nurse midwife and check for other signs of bleeding, shock, or fetal compromise.
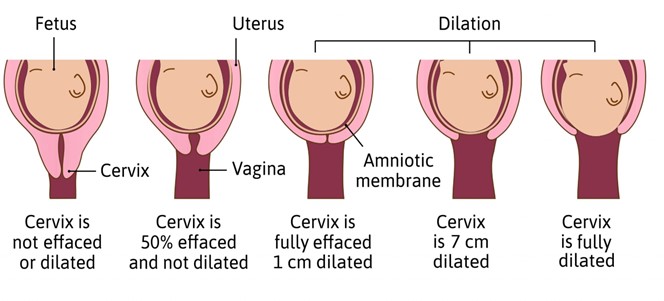
Choice D reason: Cervical dilation is the most reliable indicator of labor. It means that the cervix is opening and thinning out to allow the passage of the fetus. The nurse should measure the cervical dilation in centimeters and document it along with the station and effacement of the cervix.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today