A nurse is collecting data from a client who is 24 hr postpartum. Which of the following findings should the nurse expect?
Fundus soft, 2 fingerbreadths below the umbilicus
Fundus firm, 1 fingerbreadth below the umbilicus
Fundus firm, 4 fingerbreadths above the umbilicus
Fundus soft, to the right of the umbilicus
The Correct Answer is B
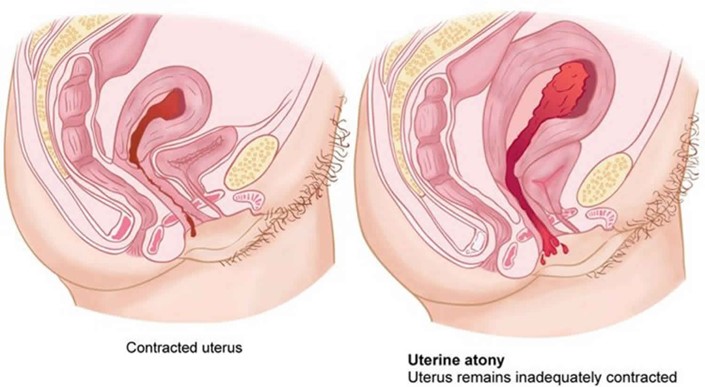
Choice A reason: Fundus soft, 2 fingerbreadths below the umbilicus is incorrect, as this finding indicates uterine atony and subinvolution. The fundus is the upper part of the uterus that can be palpated through the abdomen after birth. The fundus should be firm and midline to indicate adequate uterine contraction and involution. A soft or boggy fundus can increase the risk of hemorrhage and infection.
Choice B reason: Fundus firm, 1 fingerbreadth below the umbilicus is correct, as this finding indicates normal uterine contraction and involution. The fundus is normally at the level of the umbilicus immediately after birth and then descends about one fingerbreadth per day. A firm and midline fundus can prevent excessive bleeding and promote healing.
Choice C reason: Fundus firm, 4 fingerbreadths above the umbilicus is incorrect, as this finding indicates a higher than expected fundal height for a client who is 24 hr postpartum. The fundus is normally at the level of the umbilicus immediately after birth and then descends about one fingerbreadth per day. A high fundal height can indicate uterine atony, retained placental fragments, or bladder distension.
Choice D reason: Fundus soft, to the right of the umbilicus is incorrect, as this finding indicates uterine atony and bladder distension. The fundus should be firm and midline to indicate adequate uterine contraction and involution. A deviated fundus can indicate bladder distension, which can interfere with uterine contraction and involution and increase the risk of hemorrhage and infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice B reason:
Uterine atony is the failure of the uterus to contract and retract after delivery, which can lead to excessive bleeding and hemorrhage. The client is at risk for uterine atony due to delivering a large newborn, which can overstretch the uterine muscles and reduce their tone.
Choice A reason:
Puerperal infection is an infection of the reproductive tract that occurs within six weeks after delivery. The client is not at increased risk for puerperal infection due to delivering a large newborn, unless there are other factors such as prolonged labor, multiple vaginal exams, or episiotomy.
Choice C reason:
Thrombophlebitis is an inflammation of a vein with a blood clot formation. The client is not at increased risk for thrombophlebitis due to delivering a large newborn, unless there are other factors such as immobility, dehydration, or trauma.
Choice D reason:
Retained placental fragments are pieces of the placenta that remain in the uterus after delivery, which can cause bleeding and infection. The client is not at increased risk for retained placental fragments due to delivering a large newborn, unless there are other factors such as abnormal placental atachment, manual removal, or incomplete separation.
Correct Answer is B
Explanation
Choice A reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm above the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
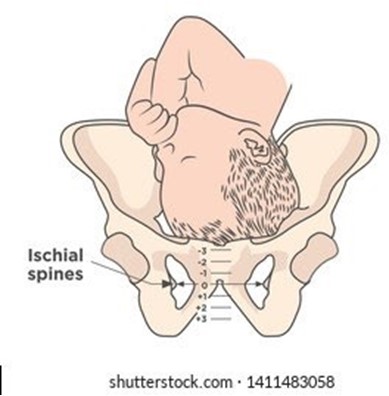
Choice B reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm above the ischial spines is correct, as this follows the correct order and measurement of cervical assessment. Cervical dilation, effacement, and station are recorded in that order to describe the progress of labor. Station refers to the relationship between the presenting part of the fetus and the maternal pelvis, measured by the level of the ischial spines. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
Choice C reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
Choice D reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not match the documentation of station. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today