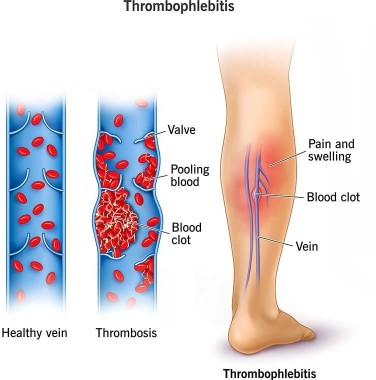
A nurse is caring for a client who is 1 day postpartum following a cesarean birth. To prevent thrombophlebitis, the nurse should contribute which of the following interventions to the client's plan of care?
Apply warm, moist soaks to the client's lower legs.
Have the client ambulate frequently in the hallway.
Keep the client on bed rest.
Place pillows under the client's knees while she is resting in bed.
The Correct Answer is B
Choice A reason: Apply warm, moist soaks to the client's lower legs is incorrect, as this action is not effective for preventing thrombophlebitis. Warm, moist soaks can provide comfort and reduce inflammation, but they do not improve blood circulation or prevent clot formation.
Choice B reason: Have the client ambulate frequently in the hallway is correct, as this action can prevent thrombophlebitis by improving venous return and preventing stasis. The nurse should encourage and assist the client to ambulate early and frequently after a cesarean birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide support as needed.
Choice C reason: Keep the client on bed rest is incorrect, as this action can increase the risk of thrombophlebitis by reducing blood flow and promoting stasis. Bed rest can also delay wound healing and increase the risk of infection and deconditioning. The nurse should avoid keeping the client on bed rest unless absolutely necessary.
Choice D reason: Place pillows under the client's knees while she is resting in bed is incorrect, as this action can impair blood circulation and increase the risk of thrombophlebitis. Placing pillows under the knees can cause pressure on the popliteal veins and reduce venous return. The nurse should advise the client to avoid crossing their legs or placing pillows under their knees while resting in bed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: The client is Rh negative and the newborn is Rh positive is correct, as this finding indicates a risk of Rh incompatibility and sensitization. Rh incompatibility occurs when the mother has Rh-negative blood and the baby has Rh-positive blood, which can cause maternal antibodies to atack the fetal red blood cells. Sensitization occurs when the maternal antibodies cross the placenta and enter the fetal circulation, which can cause hemolytic disease of the newborn. The nurse should administer Rho(D) immune globulin to prevent sensitization and protect future pregnancies.
Choice B reason: The client is Rh negative and the newborn is Rh negative is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If both the mother and the baby have Rh-negative blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Choice C reason: The client is Rh positive and the newborn is Rh positive is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If both the mother and the baby have Rh-positive blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Choice D reason: The client is Rh positive and the newborn is Rh negative is incorrect, as this finding does not indicate a risk of Rh incompatibility or sensitization. If the mother has Rh-positive blood and the baby has Rh- negative blood, there is no antigen-antibody reaction and no need for Rho(D) immune globulin.
Correct Answer is B
Explanation
Choice A reason: Request the RN perform a cervical examination is incorrect, as this action is not indicated for a client who has a history of genital herpes. A cervical examination can introduce infection and trauma to the cervix and increase the risk of viral shedding and transmission to the fetus. The nurse should avoid performing or requesting a cervical examination unless absolutely necessary.
Choice B reason: Initiate fetal monitoring for baseline and changes is correct, as this action is appropriate for any client who is in labor. Fetal monitoring can provide information about the fetal heart rate, variability, accelerations, decelerations, and contractions. The nurse should monitor the fetal status continuously and report any abnormal findings to the provider.
Choice C reason: Prepare for a vaginal birth is incorrect, as this action may not be possible for a client who has a history of genital herpes. A vaginal birth can expose the fetus to the herpes virus and cause neonatal infection, which can be life-threatening. The nurse should assess the client for signs of active lesions or prodromal symptoms and prepare for a cesarean birth if indicated.
Choice D reason: Administer antibiotics is incorrect, as this action is not effective for a client who has a history of genital herpes. Genital herpes is caused by a virus, not a bacteria, and antibiotics have no effect on viral infections. The nurse should administer antiviral medications as prescribed to reduce viral shedding and transmission to the fetus.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today