A nurse is assisting in the care of a client who is in active labor. The nurse notes variable decelerations of the FHR. The nurse should identify which of the following as a cause of variable decelerations?
Fetal head compression
Polyhydramnios
Maternal fever
Umbilical cord compression
The Correct Answer is D
Choice A reason:
Fetal head compression is incorrect, as this factor can cause early decelerations in the fetal heart rate. Early decelerations are symmetrical decreases in the FHR that mirror the contractions, which indicate fetal head compression and vagal stimulation. Fetal head compression occurs as the fetus descends into the birth canal and does not pose a threat to the fetal well-being.
Choice B reason:
Polyhydramnios is incorrect, as this factor can cause variable or late decelerations in the fetal heart rate, depending on the underlying cause. Polyhydramnios refers to an excessive amount of amniotic fluid, which can result from fetal anomalies, maternal diabetes, multiple gestation, or other conditions. Polyhydramnios can cause umbilical cord prolapse, uterine overdistension, or placental abruption, leading to reduced blood flow and oxygen delivery to the fetus.
Choice C reason:
Maternal fever is incorrect, as this factor can cause late decelerations in the fetal heart rate. Late decelerations are symmetrical decreases in the FHR that begin after the peak of the contraction and return to baseline after the contraction ends, which indicate uteroplacental insufficiency. Maternal fever can increase maternal and fetal metabolism and oxygen demand, leading to fetal hypoxia and acidosis.
Choice D reason:
Umbilical cord compression is correct, as this factor can cause variable decelerations in the fetal heart rate. Variable decelerations are abrupt decreases in the FHR that vary in onset, duration, and depth, which indicate umbilical cord compression and reduced blood flow to the fetus. Umbilical cord compression can occur due to cord prolapse, nuchal cord, short cord, or other causes. The nurse should reposition the client, administer oxygen, and prepare for delivery if indicated.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
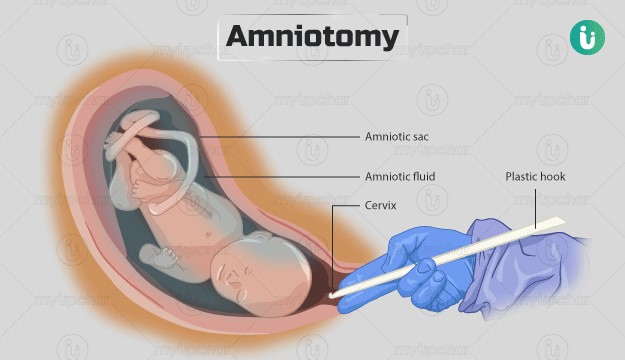
Choice A reason: Check the client's temperature every 4 hr is incorrect, as this action is not frequent enough for a client who had an amniotomy. The nurse should check the client's temperature every 2 hr after an amniotomy, as there is an increased risk of infection due to the rupture of membranes. The nurse should also monitor for signs of chorioamnionitis, such as foul-smelling amniotic fluid, maternal tachycardia, or fetal tachycardia.
Choice B reason: Remind the client to bear down with each contraction is incorrect, as this action is not appropriate for a client who is in the active phase of the first stage of labor. The nurse should instruct the client to avoid bearing down or pushing until they are in the second stage of labor, when the cervix is fully dilated and effaced. Bearing down too early can cause cervical edema, lacerations, or exhaustion.
Choice C reason: Maintain the client in the lithotomy position is incorrect, as this action is not optimal for a client who is in the active phase of the first stage of labor. The lithotomy position is a supine position with the legs elevated and abducted, which can reduce blood flow to the uterus and placenta, increase perineal edema, and limit pelvic outlet diameter. The nurse should encourage the client to change positions frequently and use upright or lateral positions that can enhance uterine contractility, fetal descent, and maternal comfort.
Choice D reason: Encourage the client to empty the bladder every 2 hr is correct, as this action can promote labor progress and prevent bladder distension and infection. The nurse should assist the client to void every 2 hr after an amniotomy, as there may be decreased sensation of bladder fullness due to pressure from the fetal head. A full bladder can interfere with uterine contractions, fetal descent, and cervical dilation.
Correct Answer is D
Explanation
Choice A reason: Amniotic fluid in the vaginal vault indicates that the membranes have ruptured, but this does not necessarily mean that the client is in labor. Some women may have a slow leak of amniotic fluid for hours or days before labor begins. Rupture of membranes also increases the risk of infection, so the nurse should monitor the client's temperature and fetal heart rate.
Choice B reason: Contractions every 3 to 4 minutes are a sign of labor, but they are not enough to confirm it. The nurse should also assess the duration and intensity of the contractions, as well as the client's response to them. Some women may have false labor contractions, also known as Braxton Hicks contractions, which are irregular, mild, and do not cause cervical changes.
Choice C reason: Pain just above the navel is not a typical sign of labor. It may indicate other problems, such as placental abruption, uterine rupture, or fetal distress. The nurse should report this finding to the nurse midwife and check for other signs of bleeding, shock, or fetal compromise.
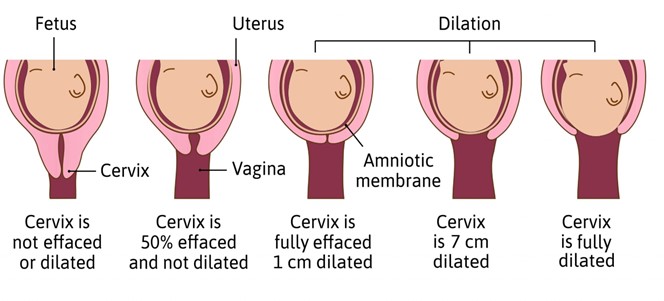
Choice D reason: Cervical dilation is the most reliable indicator of labor. It means that the cervix is opening and thinning out to allow the passage of the fetus. The nurse should measure the cervical dilation in centimeters and document it along with the station and effacement of the cervix.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today