
HESI Pediatric N158 Proctored Exam
HESI Pediatric N158 Proctored Exam
Total Questions : 54
Showing 10 questions Sign up for moreDuring her sports physical examination, 15-year-old female requests oral contraceptives. She explains that she is sexually active and does not want her parents to know. Which action should the nurse take?
Explanation
Answer: (B) Counsel the client about the risks and benefits of using oral contraceptives.
Rationale:
(A) Encourage the client to discuss her need for contraceptives with her parents: Encouraging open communication with parents is important, but this action might not be the most appropriate in this context. The client has expressed a desire for confidentiality, and respecting her autonomy is essential, particularly when it comes to sensitive topics like sexual health.
(B) Counsel the client about the risks and benefits of using oral contraceptives: Providing counseling about the risks and benefits of oral contraceptives is the most appropriate action. It ensures the client is informed and able to make a decision that is right for her health and circumstances. The nurse can also discuss other contraceptive options and provide education on safe sex practices. This approach respects the client's autonomy and privacy while ensuring she receives the necessary information to make an informed choice.
(C) Explain that she needs parental approval to receive contraceptives: In many areas, adolescents have the right to obtain contraceptives without parental consent. Requiring parental approval might not only be legally incorrect but could also discourage the client from seeking necessary healthcare, potentially putting her at risk.
(D) Tell the client how to receive a variety of free oral contraceptives from the clinic: While providing information about accessing contraceptives is helpful, this option alone does not address the need for thorough counseling about the risks and benefits. It's important to ensure that the client understands the implications of using oral contraceptives and has the opportunity to ask questions and receive guidance tailored to her individual needs.
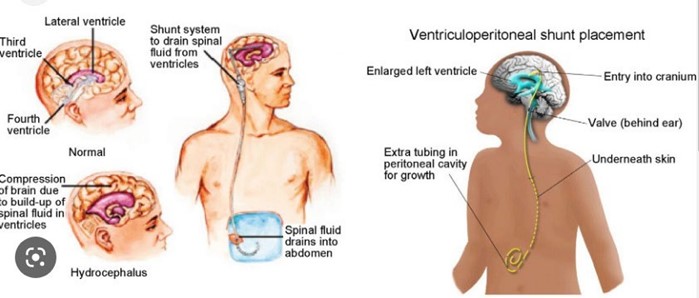
The nurse is monitoring a child with hydrocephalus who received a repeat ventriculoperitoneal (VP) shunt yesterday. Which assessment finding indicates to the nurse that the shunt is functioning normally?
Explanation
The absence of continuous headaches in the child indicates that the VP shunt is functioning normally. A VP shunt is used to treat hydrocephalus by draining excess cerebrospinal fluid from the brain to the abdomen. If the shunt is functioning properly, it should relieve pressure on the brain and reduce symptoms such as headaches. The other options (A, B, and C) do not directly indicate whether the shunt is functioning normally or not.
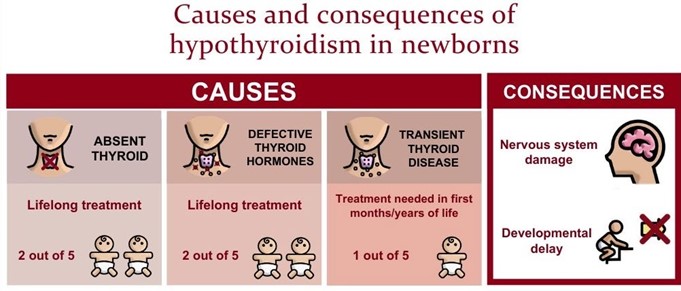
A breastfeeding infant, screened for congenital hypothyroidism, is found to have low levels of thyroxine (T4) and high levels of thyroid stimulating hormone (TSH). Which is the best explanation for this finding?
Explanation
In a normal infant, T4 levels increase after birth due to stimulation by TSH from the pituitary gland. In this case, the T4 level is low and the TSH level is high, indicating that the thyroid gland is not producing enough T4 in response to TSH stimulation. This suggests that the infant may have congenital hypothyroidism, which requires prompt treatment to prevent developmental delays and other complications.
The low T4 level is not a direct cause of the high TSH level; rather, the high TSH level is a compensatory mechanism to increase T4 production. It is not normal for a breastfeeding infant to have high thyroxine levels. While the thyroid gland may take a few weeks to reach normal function after birth, the persistent low T4 and high TSH levels in this infant suggest a more serious issue.
The nurse observes a mother giving her 11-month-old ferrous sulfate (iron drops), followed by 2 ounces (60 mL) of orange juice. What should the nurse do next?
Explanation
The nurse should give the mother positive feedback about the way she administered the medication. Giving the infant orange juice after administering the iron drops is a good practice because vitamin C in the orange juice can enhance the absorption of iron. The other options (A, C, and D) are not appropriate actions for the nurse to take in this situation.

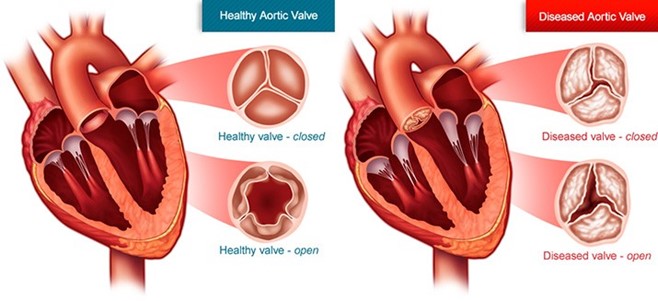
The nurse is assessing an infant with aortic stenosis and identifies bilateral fine crackles in both lung fields. Which additional finding should the nurse expect to obtain?
Explanation
Aortic stenosis is a narrowing of the aortic valve, which can cause decreased blood flow from the left ventricle to the systemic circulation. In infants with aortic stenosis, the left ventricle must work harder to pump blood through the narrowed valve, which can lead to left ventricular hypertrophy, heart failure, and pulmonary edema. Bilateral fine crackles in both lung fields may indicate fluid overload in the lungs, which is a common complication of heart failure. Hypotension and tachycardia may also be present due to decreased cardiac output.
Option A is not a typical finding associated with aortic stenosis.
Option B is not directly related to the infant's cardiac condition.
Option C is not a typical finding associated with heart failure.
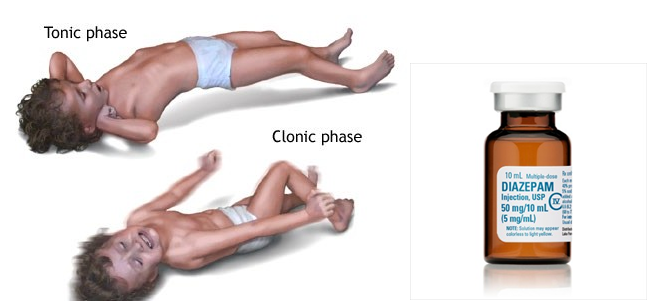
A child who weighs 30 kg is experiencing a grand mal seizure. The healthcare provider prescribes diazepam 0.3 mg/kg/dose intravenous (IV) STAT. The medication is available in 5 mg/mL vials.
How many mL should the nurse administer?
(Enter a numeric value only. If rounding is required, round to the tenth).
Explanation
The nurse should administer 1.8 mL of diazepam.
To calculate the volume of diazepam to be administered, you would first calculate the total dose of diazepam for this child by multiplying the child's weight (30 kg) by the prescribed dose (0.3 mg/kg). This calculation gives a total dose of 9 mg (30 kg x 0.3 mg/kg = 9 mg). Next, you would divide the total dose (9 mg) by the concentration of the medication (5 mg/mL) to determine the volume to be administered. This calculation gives a volume of 1.8 mL (9 mg / 5 mg/mL = 1.8 mL).
The nurse is assessing a preschool-aged child who presents with flank pain, dysuria, and low-grade fever. To determine a possible urinary tract infection, which additional information should the nurse gather from the parent?
Explanation
To determine a possible urinary tract infection in a preschool-aged child who presents with flank pain, dysuria, and low-grade fever, the nurse should gather additional information from the parent about new onset bedwetting. New onset bedwetting can be a sign of a urinary tract infection in children. The other options (A, B, and D) are not directly related to determining a possible urinary tract infection in this situation.
A newborn with a repaired gastroschisis is transferred to the paediatric unit after several days in the paediatric intensive care unit. The infant is receiving parenteral nutrition and continuous enteral feedings.
To maintain normal growth and development of the infant, which action should the nurse include in the plan of care?
Explanation
To maintain normal growth and development of an infant with a repaired gastroschisis who is receiving parenteral nutrition and continuous enteral feedings, the nurse should include offering a pacifier for non- nutritive sucking in the plan of care. Non-nutritive sucking can help promote the development of the infant's oral motor skills and support normal feeding behaviors. The other options (B, C, and D) are not directly related to maintaining normal growth and development in this situation.

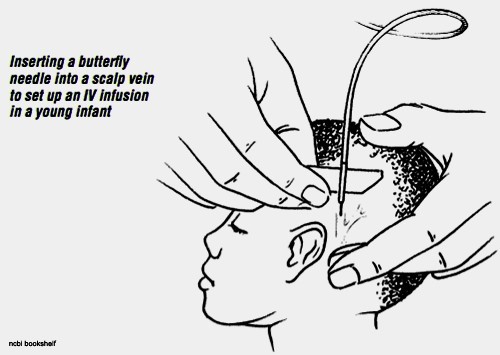
When starting a peripheral intravenous (IV) infusion on an infant, which intervention should the nurse implement?
Explanation
Peripheral intravenous (IV) infusion is a common procedure performed on infants in a hospital setting. The selection of the IV site is critical to ensure proper placement and to prevent complications.
When starting a peripheral IV infusion on an infant, the nurse should select a site that is least restrictive to the infant. This involves selecting a site that will not restrict the infant's movement and cause discomfort. The site should be accessible, visible, and easily palpable, such as the hand, wrist, or antecubital fossa.
Assessing the dorsal surface of the feet for an IV site is not recommended as it is an area of high risk for infiltration and may restrict the infant's movement.
Instructing parents to sing or croon to the infant may provide comfort and distraction, but it is not a critical intervention when starting a peripheral IV infusion.
Applying soft restraints to all four extremities is not recommended as it may cause physical and emotional distress to the infant. It should only be used as a last resort if the infant is at high risk of self-injury or if the procedure cannot be safely performed without restraints.
Therefore, the nurse should implement the intervention of selecting a site that is least restrictive to the infant when starting a peripheral IV infusion.
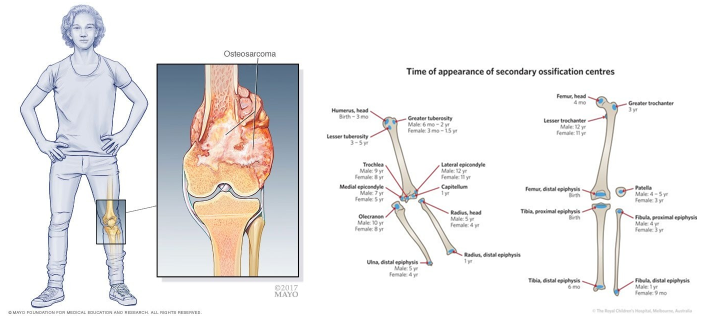
An adolescent client reports to the nurse of walking with a limp due to pain localized in the right knee which worsens at night but denies any recent injury or trauma. The nurse observes swelling and tenderness in the right lower thigh, and imaging results reveal radial ossification in the soft tissues.
Which condition should the nurse consider as the probable cause of the findings?
Explanation
The adolescent client's symptoms of localized pain, swelling, and tenderness, particularly at night, are suggestive of a malignancy such as osteosarcoma, which is the most common primary bone tumor in children and adolescents.
Radial ossification in the soft tissues is a characteristic finding in osteosarcoma and is indicative of bone production by malignant cells. Other imaging modalities, such as X-rays, computed tomography (CT), and magnetic resonance imaging (MRI), may also reveal osteolytic or osteoblastic lesions in the bone.
Growing pains are a common, benign condition that occur in children and do not typically present with the
symptoms described in the case scenario.
Rhabdomyolysis is a medical emergency that involves the breakdown of skeletal muscle tissue and release of muscle fiber contents into the bloodstream. It can present with muscle pain, swelling, and tenderness, but typically occurs as a result of injury, infection, or drug toxicity.
Hemosiderosis is a rare condition characterized by the accumulation of iron in various tissues, including the liver, spleen, and bone marrow. It may present with symptoms such as fatigue, joint pain, and abdominal pain, but is not typically associated with the symptoms and imaging findings described in the case scenario.
Therefore, the nurse should consider osteosarcoma as the probable cause of the adolescent client's symptoms and imaging findings, and should collaborate with the healthcare team to develop a plan of care for diagnosis and treatment.
You just viewed 10 questions out of the 54 questions on the HESI Pediatric N158 Proctored Exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

