
LPN Fundamentals Exam 1
ATI LPN Fundamentals Exam 1
Total Questions : 59
Showing 10 questions Sign up for moreA nurse is reinforcing teaching about values to a newly licensed nurse. Which of the following statements by the newly licensed nurse indicates an understanding?
Explanation
Choice A reason: This statement is incorrect because a nurse’s personal values can and do influence ethical decisions. The nurse should be aware of their own values and how they affect their judgment and actions. The nurse should also respect the values of others and avoid imposing their own values on the clients or colleagues.
Choice B reason: This statement is incorrect because value clarification is not related to maintaining clinical competency. Value clarification is a process of identifying, examining, and prioritizing one’s values. It can help the nurse to understand their own values and beliefs, as well as those of the clients and the profession.
Choice C reason: This statement is correct because it is important that the nurse is aware of the client’s values. The nurse should assess the client’s values and preferences, and incorporate them into the plan of care. The nurse should also respect the client’s right to self-determination and autonomy, and support the client in making informed decisions.
Choice D reason: This statement is incorrect because a nurse's behaviors and actions are not called values. Values are the beliefs and principles that guide one’s decisions and actions. A nurse's behaviors and actions are the expressions of their values, as well as their knowledge, skills, and attitudes.
A charge nurse is reinforcing teaching with a newly licensed nurse about the advantages of electronic documentation. Which of the following information should the nurse include in the teaching?
Explanation
Choice A: This is the correct answer. A portal is a secure online platform that enables clients to access their health information, communicate with their providers, request appointments, refill prescriptions, and more. This enhances client satisfaction, engagement, and empowerment.
Choice B: This is incorrect. Same day access to client health record is not an advantage of electronic documentation, but a requirement for any documentation system. Clients have the right to access their health information within a reasonable time frame, regardless of whether it is paper-based or electronic.
Choice C: This is incorrect. The increase of duplicate tests performed on client is not an advantage of electronic documentation, but a disadvantage. Duplicate tests can result from poor communication, lack of interoperability, or human error. Electronic documentation can help reduce duplicate tests by facilitating data sharing, standardizing formats, and alerting providers of previous tests.
Choice D: This is incorrect. Decrease in coordination of client care is not an advantage of electronic documentation, but a disadvantage. Coordination of client care is essential for ensuring quality, safety, and continuity of care. Electronic documentation can improve coordination of client care by allowing multiple providers to access and update the same information, enabling real-time collaboration, and providing decision support tools.
A charge nurse is reinforcing teaching with a newly licensed nurse about accessing a client's medical records. Which of the following should the nurse include in the teaching?
Explanation
Choice A reason: This statement is incorrect because a nurse cannot access the records of any client in the healthcare facility, unless they have a legitimate need to do so. Accessing the records of clients who are not under their care is a violation of the client's privacy and confidentiality, and may result in legal or disciplinary actions.
Choice B reason: This statement is correct because a nurse can only access the records of clients they are actively caring for, as part of their professional duty and responsibility. Accessing the records of clients they are caring for is necessary to provide safe and effective care, and to communicate with other members of the healthcare team.
Choice C reason: This statement is incorrect because a nurse cannot share information from the client’s medical record with immediate family members, unless the client has given consent, or the disclosure is authorized by law. Sharing information from the client's medical record with family members without the client's permission is a breach of the client's privacy and confidentiality, and may cause harm or distress to the client or the family.
Choice D reason: This statement is incorrect because a nurse cannot share information about a client with clients who have a similar diagnosis, unless the client has given consent or the disclosure is authorized by law. Sharing information about a client with other clients without the client's permission is a breach of the client's privacy and confidentiality, and may compromise the client's dignity or safety.
A nurse is obtaining a health history from a client. Which of the following findings should the nurse identify as a nonmodifiable risk factor for disease?
Explanation
Choice A reason: Genetics is a nonmodifiable risk factor for disease because it is determined by the inherited traits from the parents. Genetics can influence the susceptibility, severity, and progression of certain diseases, such as cancer, diabetes, or cardiovascular disease. The nurse cannot change the client's genetic makeup, but can help the client to manage their condition and prevent complications.
Choice B reason: Sunbathing is a modifiable risk factor for disease because it is influenced by the client's behavior and lifestyle. Sunbathing can increase the exposure to ultraviolet (UV) radiation, which can damage the skin cells and cause skin cancer, premature aging, or sunburn. The nurse can educate the client on the importance of sun protection, such as using sunscreen, wearing protective clothing, and avoiding peak hours of sun exposure.
Choice C reason: Smoking is a modifiable risk factor for disease because it is influenced by the client's behavior and lifestyle. Smoking can harm the lungs, heart, blood vessels, and other organs, and increase the risk of various diseases, such as chronic obstructive pulmonary disease (COPD), lung cancer, or coronary artery disease. The nurse can assist the client in quitting smoking, such as providing counseling, nicotine replacement therapy, or pharmacological interventions.
Choice D reason: Unhealthy diet is a modifiable risk factor for disease because it is influenced by the client's behavior and lifestyle. Unhealthy diet can lead to obesity, malnutrition, or metabolic disorders, and increase the risk of various diseases, such as diabetes, hypertension, or stroke. The nurse can advise the client on the benefits of a balanced diet, such as eating more fruits, vegetables, whole grains, lean proteins, and healthy fats, and limiting the intake of salt, sugar, and saturated fats.
A nurse on an inpatient mental health unit is assisting with the admission of a client who reports feeling depressed, sad, moody, and overly anxious. Which of the following assessments should the nurse make first?
Explanation
Choice A reason: This statement is incorrect because psychiatric history is not the most urgent assessment to make for a client who reports feeling depressed and anxious. Psychiatric history can provide valuable information about the client's diagnosis, treatment, and response, but it is not a priority over the client's safety and wellbeing.
Choice B reason: This statement is correct because suicide risk is the most urgent assessment to make for a client who reports feeling depressed and anxious. Suicide risk can indicate the client's level of hopelessness, despair, and intent to harm themselves. The nurse should assess the client's suicidal thoughts, plans, means, and access, and implement appropriate interventions to prevent self harm or suicide.
Choice C reason: This statement is incorrect because support systems are not the most urgent assessment to make for a client who reports feeling depressed and anxious. Support systems can provide emotional, social, and practical assistance to the client, but they are not a priority over the client's safety and wellbeing.
Choice D reason: This statement is incorrect because coping abilities are not the most urgent assessment to make for a client who reports feeling depressed and anxious. Coping abilities can reflect the client's strategies and skills to manage their stress and emotions, but they are not a priority over the client's safety and wellbeing.
A nurse is assisting with teaching a class about medically futile treatment. The nurse should include which of the following as an example of medically futile treatment?
Explanation
Choice A reason: This statement is incorrect because administering an antiemetic to a client who has post chemotherapy nausea is not medically futile. It is a supportive measure that can help the client to manage the side effects of chemotherapy and improve their comfort and quality of life.
Choice B reason: This statement is incorrect because administering a narcotic analgesic to a client who has end stage cancer is not medically futile. It is a palliative measure that can help the client to relieve their pain and suffering and improve their comfort and quality of life.
Choice C reason: This statement is incorrect because administering oral care for a client who has post chemotherapy mucositis is not medically futile. It is a preventive measure that can help the client to avoid infections and complications and improve their oral health and hygiene.
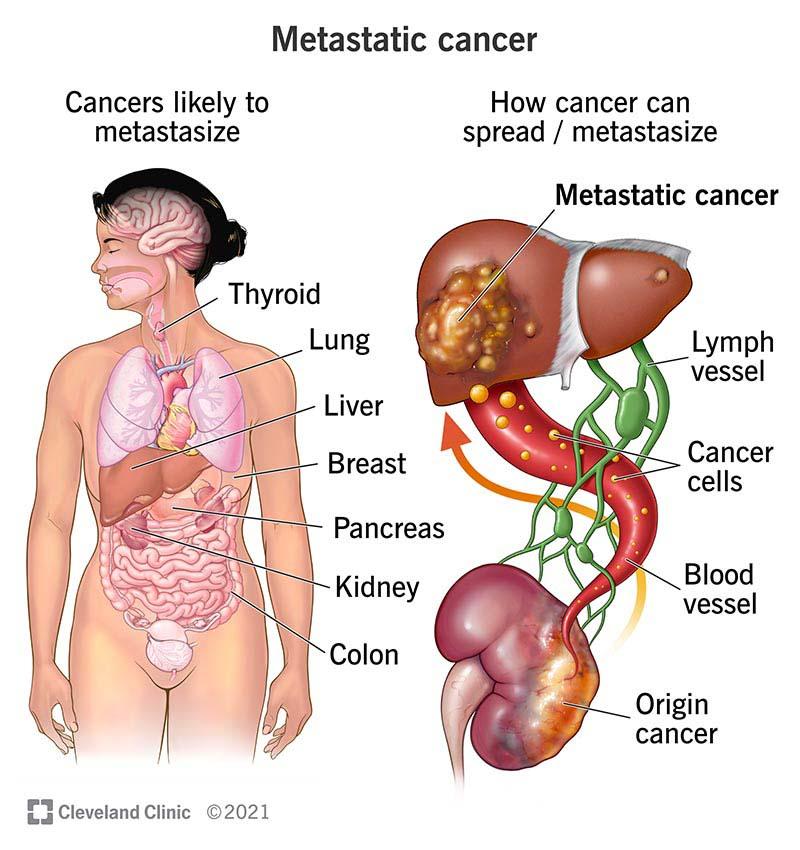
Choice D reason: This statement is correct because administering chemotherapy to a client who has metastatic cancer is medically futile. It is a curative measure that has no reasonable chance of achieving its intended goal of eradicating the cancer or prolonging the client's survival. It may also cause harm or distress to the client by exposing them to unnecessary risks and side effects.
A nurse is assisting with teaching a class about client advocacy. The nurse should include which of the following as an example of client advocacy?
Explanation
Choice A reason: This statement is incorrect because protecting a client’s personal health information is not an example of client advocacy, but a legal and ethical obligation of the nurse. The nurse should follow the principles of confidentiality and privacy, and only share the client’s information with authorized persons or entities, or with the client’s consent.
Choice B reason: This statement is incorrect because keeping a promise to return to a client’s room is not an example of client advocacy, but a professional and courteous behavior of the nurse. The nurse should be honest, reliable, and respectful to the client, and follow through with their commitments and expectations.
Choice C reason: This statement is incorrect because accepting responsibility for their own actions is not an example of client advocacy, but a personal and professional accountability of the nurse. The nurse should be aware of their scope of practice, standards of care, and code of ethics, and act accordingly. The nurse should also admit their mistakes, report errors, and seek help when needed.
Choice D reason: This statement is correct because communicating a client’s wishes to their provider is an example of client advocacy. The nurse should act as a liaison between the client and the provider, and ensure that the client’s needs, preferences, and values are respected and considered in the decision-making process. The nurse should also support the client’s right to self-determination and informed consent.
A nurse is preparing to delegate tasks to an assistive personnel (AP). The nurse should identify which of the following as one of the five rights of delegation?
Explanation
Choice A reason: This statement is incorrect because right documentation is not one of the five rights of delegation. Right documentation is a responsibility of the nurse and the AP, but it is not a criterion for deciding what tasks to delegate and to whom. The five rights of delegation are right task, right circumstance, right person, right direction, and right supervision.
Choice B reason: This statement is correct because right communication is one of the five rights of delegation. Right communication means that the nurse provides clear, concise, and specific instructions to the AP, and that the AP acknowledges and understands the instructions. Right communication also involves feedback, reporting, and documentation between the nurse and the AP.
Choice C reason: This statement is incorrect because right time is not one of the five rights of delegation. Right time is a factor that affects the delegation process, but it is not a criterion for deciding what tasks to delegate and to whom. The five rights of delegation are right task, right circumstance, right person, right direction, and right supervision.
Choice D reason: This statement is incorrect because right room is not one of the five rights of delegation. Right room is a factor that affects the delegation process, but it is not a criterion for deciding what tasks to delegate and to whom. The five rights of delegation are right task, right circumstance, right person, right direction, and right supervision.
A charge nurse is assisting in providing an in-service to a group of nurses about the benefits of an interprofessional team. Which of the following information should the nurse include in the teaching?
Explanation
Choice A reason: This statement is incorrect because an interprofessional team does not necessarily decrease the number of visits to client by staff. In fact, an interprofessional team may increase the frequency and quality of communication and interaction between the client and the staff, as each member of the team contributes their expertise and perspective to the client's care. This can enhance the client's satisfaction, engagement, and education.
Choice B reason: This statement is correct because an interprofessional team can improve the efficiency in client care services. An interprofessional team can coordinate and integrate the care delivery across different disciplines, settings, and levels of care, reducing the duplication, fragmentation, or gaps in the services. This can also lower the costs and risks of care, and improve the outcomes and quality of care.
Choice C reason: This statement is incorrect because an interprofessional team does not increase the length of stay for client. On the contrary, an interprofessional team can reduce the length of stay for client by providing timely, appropriate, and effective care that meets the client's needs and goals. This can also prevent the readmission or complication of the client, and facilitate the transition and discharge of the client.
Choice D reason: This statement is incorrect because an interprofessional team does not decrease the number of referrals needed for client. Rather, an interprofessional team can enhance the referral process by ensuring that the client receives the right service from the right provider at the right time. An interprofessional team can also collaborate and communicate with the referral sources, and follow up on the client's progress and response to the service.
A nurse is preparing to complete an occurrence report for a client who fell at the facility. Which of the following actions should the nurse take?
Explanation
Choice A reason: This statement is correct because the nurse should use objective terminology when documenting the occurrence. Objective terminology means using factual, unbiased, and verifiable information, such as the date, time, location, witnesses, and events of the occurrence. The nurse should avoid using subjective, opinionated, or judgmental language, such as blaming, criticizing, or speculating about the occurrence.
Choice B reason: This statement is incorrect because the nurse should not wait at least 12 hours to report the occurrence. The nurse should report the occurrence as soon as possible, preferably within an hour of the incident. The nurse should also notify the appropriate personnel, such as the charge nurse, the provider, and the risk manager. Delaying the report may compromise the client's safety and wellbeing, and the accuracy and completeness of the documentation.
Choice C reason: This statement is incorrect because the nurse should not omit the name of the individuals involved in the occurrence. The nurse should include the name of the client, the staff, and any other relevant parties, such as family members or visitors. The nurse should also document the role and actions of each individual, and their response to the occurrence. Omitting the name of the individuals may affect the accountability and follow-up of the occurrence.
Choice D reason: This statement is incorrect because the nurse should not document completion of the report in the client’s medical record. The nurse should document the occurrence report separately from the client’s medical record, and follow the facility's policy and procedure for filing and storing the report. The nurse should also document the occurrence in the client’s medical record, but only the facts and the nursing actions, not the details or the existence of the report. Documenting completion of the report in the client’s medical record may expose the facility to legal liability or litigation.
You just viewed 10 questions out of the 59 questions on the ATI LPN Fundamentals Exam 1 Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

