
HESI RN Fundamentals with NGN
HESI RN Fundamentals with NGN
Total Questions : 51
Showing 10 questions Sign up for moreA child has experienced several episodes of vomiting. After the nurse reviews the need to provide only clear liquids, the parent of the child reports making clear liquid popsicles out of flavored gelatin for the child. Which information should the nurse obtain about the popsicles?
Explanation
A. How many popsicles are available.
This information might be helpful for logistical purposes or to assess how much the child has consumed, but it's not directly relevant to ensuring the appropriateness of the popsicles for a clear liquid diet.
B. If the popsicles are completely frozen.
While it's important that popsicles are properly frozen to avoid potential choking hazards, this does not address whether the popsicles meet the dietary requirement of clear liquids.
C. The color and flavor of gelatin used.
While this might be of interest, the key concern is whether the popsicles contain any non-clear components like fruit or pulp.
D. Whether they contain pulp or fruit.
For a child who needs clear liquids, it is important to ensure that the popsicles do not contain any solids like fruit or pulp. Clear liquids are meant to be easily digestible and not irritate the stomach further. Popsicles with pulp or fruit can be too heavy and might not be appropriate in this situation.
The nurse is caring for a client with type 2 diabetes mellitus who had surgery for a large bowel resection with a colostomy placement. The client has now developed hyperglycemia which require self injections of insulin after discharge. When designing the postoperative plan of care, which outcome statement should the nurse use?
Explanation
A. The client will demonstrate ability to change the ostomy bag in two days.
This outcome statement focuses on the client's ability to perform a specific task related to ostomy care. While it's important for clients with a colostomy to learn how to change their ostomy bag, in the context of this scenario, where the client has developed hyperglycemia requiring insulin injections, the priority lies in managing their diabetes and adhering to the medication regimen. Therefore, while ostomy care is important, it may not be the most immediate concern.
B. The client will adhere to the medication regimen after discharge.
This outcome statement directly addresses the client's need to manage their hyperglycemia by adhering to the prescribed insulin regimen. Given that the client has developed hyperglycemia requiring insulin injections, ensuring medication adherence is crucial for controlling blood sugar levels and preventing complications associated with uncontrolled diabetes. This choice aligns with the client's health needs and goals following the surgical procedure and the development of hyperglycemia.
C. The client's breath sounds will be auscultated by the nurse every 4 hours.
This outcome statement focuses on monitoring the client's respiratory status by auscultating breath sounds at regular intervals. While respiratory assessment is important, especially postoperatively, it may not directly address the client's primary health concern in this scenario, which is managing hyperglycemia and insulin administration.
D. The client attempts to self-administer insulin but is unable to perform injection.
This outcome statement indicates the client's attempt to self-administer insulin but inability to perform the injection. While it's important for clients to be able to self-administer insulin, the emphasis in this scenario should be on ensuring that the client adheres to the medication regimen, rather than focusing solely on their ability to self-administer insulin immediately after discharge. Therefore, while self-administration of insulin is relevant, it may not be the most immediate priority in the postoperative plan of care.
A 16-year-old emancipated client is being seen in the emergency department following a minor automobile accident. The client's parents arrive and are asking questions about the client's laboratory results. Which response is best for the nurse to provide?
Explanation
A. "I'm sorry, but your child's medical Information is none of your business."
This response is confrontational and dismissive, and it doesn't effectively address the parents' concerns. It's important to maintain professionalism and respect even in challenging situations.
B. "I can only give medical Information to your child because they are legally an adult."This response respects the minor's emancipated status and acknowledges that, legally, the nurse can only disclose medical information to the emancipated minor themselves. It upholds the principles of patient confidentiality and autonomy while also providing clear and accurate information to the parents about their limitations regarding access to their child's medical information.
C."The healthcare provider will share this information with you," could potentially mislead the parents because it implies that the healthcare provider will provide them with the information directly. However, if the minor is legally emancipated, the healthcare provider would still be bound by confidentiality laws and would only be able to disclose information to the minor themselves unless there are extenuating circumstances or legal exceptions.
D. "I can give you those results as soon as I get them back from the laboratory."
While this response offers to provide information, it doesn't address the issue of confidentiality or the parents' role in receiving the information. It's also not accurate to promise the results directly without involving the healthcare provider, who is responsible for interpreting and discussing the results with the patient and family.
The nurse is caring for a client with a history of neuropathy who reports increasing numbness and tingling in the lower extremities. Which problem should the nurse determine is the priority for promoting foot care at this time?
Explanation
A. Risk for infection:
Neuropathy can compromise the ability to detect injuries or wounds on the feet. Consequently, there's a risk of wounds going unnoticed, becoming infected, and leading to serious complications. While preventing infection is important, the primary concern in this scenario is preventing the occurrence of wounds or skin breakdown in the first place.
B. Impaired physical mobility:
Impaired physical mobility may be a concern for clients with neuropathy, especially if it affects their ability to walk or perform activities of daily living. However, in this scenario, the client is reporting increasing numbness and tingling in the lower extremities, indicating a sensory issue rather than a motor one. Therefore, while physical mobility is important, it may not be the immediate priority for promoting foot care in this case.
C. Risk for impaired skin integrity:
This option addresses the potential risk of skin breakdown or damage due to decreased sensation in the lower extremities, which is characteristic of neuropathy. With increasing numbness and tingling, there's a higher risk that the client may not be able to perceive injuries or pressure points, leading to skin damage or ulceration. Preventing skin integrity issues is crucial to avoid complications such as infections or wounds.
D. Self-care deficit:
Neuropathy can indeed impact a person's ability to perform self-care activities, including foot care. However, the priority in this scenario is to prevent complications related to neuropathy, such as skin integrity issues, rather than addressing deficits in self-care abilities. While self-care education and support may be necessary in the long term, immediate intervention to prevent skin breakdown takes precedence.
The nurse enters a client's room to perform a physical assessment and finds the client crying. Which response is best for the nurse to provide?
Explanation
A. "I am sorry to disturb you at a difficult time. This can wait until later."
This response acknowledges the client's distress but does not actively engage with the client's emotions or offer support. It also suggests postponing the assessment, which may not be necessary if the client is willing to discuss their feelings.
B. “While touching the client's forearm, asks, 'Would you like to talk about it?'"
This response demonstrates empathy and offers the client an opportunity to express their feelings if they wish to do so. By gently touching the client's forearm and asking if they would like to talk, the nurse conveys support and openness to the client's emotional needs.
C. "This is a bad time. I can see you are upset. I can come back later."
While this response acknowledges the client's emotions and offers to return later, it may not be the most helpful approach. It assumes that the client does not want to engage in conversation at that moment without giving them the opportunity to express their preferences.
D. “Gives the client a hug and says, 'It is okay to cry when you are sad.'"
While offering physical comfort like a hug can be appropriate in some situations, it's important to respect the client's personal boundaries and preferences, especially if they are in distress. Additionally, some clients may not feel comfortable with physical touch from healthcare providers. This response also assumes the client's emotions without directly addressing their needs or offering them an opportunity to express themselves verbally.
The nurse is interviewing a client with lower abdominal pain and dysuria, and needs to question the client about sexual activity. Which approach is best for the nurse to use?
Explanation
In this situation, the best approach for the nurse to use when questioning the client about sexual activity is:
A. Ask questions in a vague, nonspecific format.
This approach may lead to confusion or misunderstanding on the part of the client and may not elicit the necessary information about sexual activity. It's important for the questions to be clear and specific to ensure accurate assessment and appropriate care.
B. Get the most difficult questions over with first.
Starting with the most difficult or sensitive questions may put the client on the defensive or make them feel uncomfortable. It's generally more effective to build rapport and trust with the client before broaching sensitive topics.
C. Begin with questions that are less sensitive in nature.
This approach allows the nurse to establish rapport and build trust with the client before addressing more sensitive topics such as sexual activity. Starting with less sensitive questions can help the client feel more comfortable and open up about their concerns.
D. Share personal values to put the client at ease.
Sharing personal values may not be appropriate or helpful in this context, as it could potentially influence the client's responses and compromise the objectivity of the assessment. The focus should be on creating a safe and supportive environment for the client to discuss their health concerns without feeling judged.
The nurse is using guided imagery with a client who is experiencing chronic pain. The nurse should direct the client's attention on which focus?
Explanation
A. Positive external places:
Guided imagery typically involves directing the client to visualize calming and peaceful external environments, such as a beach, forest, or other positive, serene places. This technique helps divert the client's attention away from pain and promotes relaxation.
B. Emotional reflection:
Emotional reflection may be part of the guided imagery process, especially if it helps the client process and cope with their emotions related to chronic pain. However, the primary focus of guided imagery is typically on visualization techniques rather than emotional reflection alone.
C. Motivational phrases:
Motivational phrases can be helpful in some relaxation techniques, but in guided imagery for chronic pain management, the emphasis is usually on visualizing soothing images or scenarios rather than repeating motivational phrases.
D. Tranquil sounds:
Tranquil sounds may be part of a relaxation strategy, but guided imagery specifically involves visualizing calming scenes, not just focusing on sounds.
The nurse is caring for a client one week postsurgery. Which finding should the nurse expect to see if the surgical incision is healing properly?
Explanation
A. A well approximated incision site:
A properly healing surgical incision typically appears well approximated, meaning the wound edges are closely aligned and held together with sutures or staples. This indicates that the wound is healing as expected and that the risk of infection and complications is minimized.
B. Erythema and serosanguineous exudate:
Erythema (redness) and serosanguineous exudate (pinkish fluid composed of serum and blood) can be normal findings in the early stages of wound healing, but they may also indicate inflammation or infection if they persist or worsen over time.
C. Eschar and slough in the wound:
Eschar (dead tissue) and slough (yellow or white necrotic tissue) are signs of tissue necrosis or delayed wound healing. They indicate that the wound is not healing properly and may require intervention such as debridement to remove dead tissue and promote healing.
D. Beefy red granulation tissue:
Beefy red granulation tissue is a sign of the proliferative phase of wound healing and indicates that the wound is healing from the bottom up. While granulation tissue is a positive sign of healing, it typically appears later in the healing process rather than one week post-surgery.
After completing daily charting at 1400, the nurse realizes that a 0900 occurrence was not entered. Which is the best way for the nurse to enter computer documentation of the 0900 occurrence?
Explanation
A. Enter the occurrence after the 1400 notes and identify as "late entry":
While entering the occurrence after the 1400 notes is an option, labeling it as a "late entry" may not provide sufficient clarity regarding the timing of the documentation. Using a "late entry" label could potentially lead to confusion or misinterpretation.
B. Request removal initiated by the Health Information Manager:
Requesting removal of the 1400 notes by the Health Information Manager is not necessary in this scenario. The focus should be on accurately documenting the missed occurrence rather than removing previously entered documentation.
C. Create an electronic correction after 1400 notes are officially unlocked:
Making an electronic correction implies that there was an error in the original documentation. Since the issue here is not correcting an error but rather adding missed documentation, creating a correction may not be appropriate.
D. Make an electronic addendum following the 1400 documentation:
An electronic addendum allows the nurse to add additional information to the chart without altering the original entry. This approach maintains the integrity of the original documentation while clearly indicating that the 0900 occurrence was added after the fact. It's important to ensure that the addendum clearly identifies the timing of the documentation to maintain accuracy and transparency in the medical record.
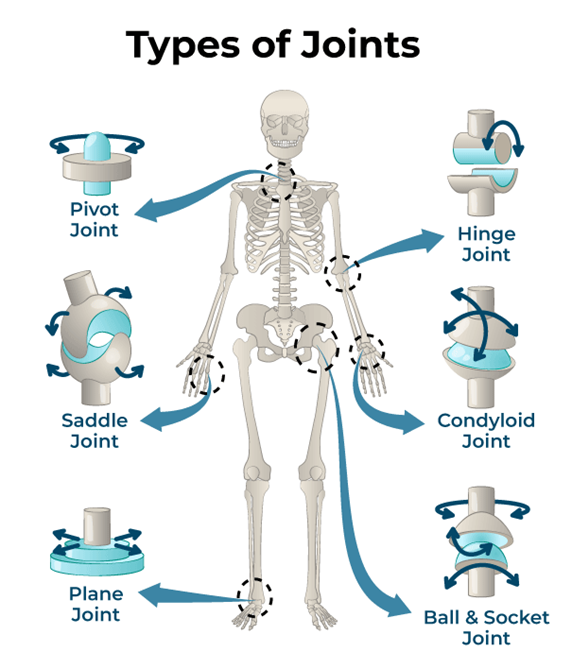
The nurse is teaching a client how to do active range of motion (ROM) exercises. To exercise the hinge joints, which action should the nurse instruct the client to perform?
Explanation
A. Turn the head to the right and left:
Turning the head involves rotation of the cervical spine, which primarily consists of pivot joints rather than hinge joints. This action is more relevant to the movement of pivot joints.
B. Extend the arm at the side and rotate in circles:
Extending the arm and rotating it in circles primarily involves the movement of ball-and-socket joints, such as the shoulder joint, rather than hinge joints.
C. Bend the arm by flexing the ulna to the humerus:
This action involves bending the arm at the elbow joint by flexing the ulna (forearm bone) towards the humerus (upper arm bone). The elbow joint is a hinge joint, allowing primarily flexion and extension movements.
D. Tilt the pelvis forwards and backwards:
Tilting the pelvis forwards and backwards primarily involves the movement of ball-and-socket joints in the hip area, rather than hinge joints.
You just viewed 10 questions out of the 51 questions on the HESI RN Fundamentals with NGN Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

