
HESI RN Med Surg
HESI RN Med Surg
Total Questions : 40
Showing 10 questions Sign up for moreThe nurse is assessing the lung sounds of a preschooler. Which action should the nurse implement to ensure the child's cooperation?
Explanation
Choice A reason: Having the child blow a cotton ball and have the parent catch it is not a good strategy to ensure the child's cooperation. This activity might distract the child from the assessment and make it difficult for the nurse to listen to the lung sounds.
Choice B reason: Allowing the child to use a stethoscope on a stuffed animal is a good strategy to ensure the child's cooperation. This activity helps the child to understand the purpose of the stethoscope and reduces the fear of the unfamiliar device. It also allows the nurse to observe the child's breathing pattern and chest movement.
Choice C reason: Offering the child bubbles before the stethoscope is placed is not a good strategy to ensure the child's cooperation. This activity might alter the child's breathing pattern and interfere with the accuracy of the assessment.
Choice D reason: Placing a toy in the child's hands while listening to the breath sounds is not a good strategy to ensure the child's cooperation. This activity might distract the child from the assessment and make it difficult for the nurse to listen to the lung sounds.

A child diagnosed with Kawasaki disease is brought to the clinic. The mother reports that her child is irritable, refuses to eat, and has skin peeling on both hands and feet. Which intervention should the nurse instruct the mother to implement first?
Explanation
Choice A reason: Encouraging the parents to rest when possible is not the first intervention that the nurse should instruct the mother to implement. While it is important for the parents to take care of themselves, the priority is to address the child's needs and comfort.
Choice B reason: Making a list of foods that the child likes is not the first intervention that the nurse should instruct the mother to implement. While it is important to maintain the child's nutrition and hydration, the child may not have an appetite due to the fever and inflammation caused by Kawasaki disease.
Choice C reason: Placing the child in a quiet environment is the first intervention that the nurse should instruct the mother to implement. This is because Kawasaki disease causes irritability and sensitivity to light and sound in the child. A quiet environment can help reduce the child's stress and discomfort.
Choice D reason: Applying lotion to hands and feet is not the first intervention that the nurse should instruct the mother to implement. While it is important to moisturize the skin and prevent cracking and infection, the lotion may not relieve the child's pain and inflammation.
During a follow-up clinic visit, a mother tells the nurse that her 5-month-old son who had surgical correction for tetralogy of Fallot (TOF) has rapid breathing, often takes a long time to eat, and requires frequent rest periods. The infant is not crying while being held and his growth is in the expected range. Which intervention should the nurse implement?
Explanation
Choice A reason: Obtaining a 12-lead electrocardiogram is not the first intervention that the nurse should implement. An electrocardiogram is a test that measures the electrical activity of the heart and can detect abnormalities in the heart rhythm or structure. However, it is not a priority for an infant who has already had surgical correction for TOF and is not showing signs of distress.
Choice B reason: Stimulating the infant to cry to produce cyanosis is not an intervention that the nurse should implement at all. Cyanosis is a bluish discoloration of the skin due to low oxygen levels in the blood. It is a common symptom of TOF and can be triggered by crying or other stressors. However, it is not a desirable outcome and can cause harm to the infant. The nurse should avoid provoking cyanosis and instead provide comfort and oxygen to the infant.
Choice C reason: Auscultating heart and lungs while the infant is held is the first intervention that the nurse should implement. This is a simple and noninvasive way to assess the infant's respiratory and cardiac status. The nurse can listen for any abnormal sounds, such as crackles, wheezes, or murmurs, that may indicate a problem. The nurse can also monitor the infant's heart rate and oxygen saturation. Holding the infant can provide comfort and security to the infant and the mother.
Choice D reason: Evaluating the infant for failure to thrive (FTT) is not the first intervention that the nurse should implement. FTT is a condition where an infant does not grow or gain weight as expected. It can be caused by various factors, such as inadequate nutrition, chronic illness, or psychosocial issues. However, the infant in this scenario is not showing signs of FTT, as his growth is in the expected range. The nurse should focus on the infant's current symptoms and needs.
The mother of a one-month-old infant calls the clinic to report that the back of her infant's head is flat. How should the nurse respond?
Explanation
Choice A reason: Positioning the infant on the stomach occasionally when awake and active is the best response that the nurse can give to the mother. This is because it can help prevent and correct the flat head syndrome, also known as plagiocephaly, by taking pressure off the back of the head and allowing the skull to reshape naturally. It can also promote the infant's motor development and strengthen the neck and shoulder muscles. However, the nurse should also remind the mother to always place the infant on the back when sleeping, as this is the safest position to reduce the risk of sudden infant death syndrome (SIDS) .
Choice B reason: Turning the infant on the left side braced against the crib when sleeping is not a good response that the nurse can give to the mother. This is because it can increase the risk of SIDS, as the infant may roll over to the stomach or suffocate from the bedding or the crib. It can also worsen the flat head syndrome by creating another flat spot on the left side of the head.
Choice C reason: Placing a small pillow under the infant's head while lying on the back is not a good response that the nurse can give to the mother. This is because it can increase the risk of SIDS, as the pillow may cover the infant's face or cause the infant to overheat. It can also interfere with the natural reshaping of the skull and cause neck strain.
Choice D reason: Propping the infant in a sitting position with a cushion when not sleeping is not a good response that the nurse can give to the mother. This is because it can put too much pressure on the spine and the pelvis, which are still developing in the infant. It can also limit the infant's movement and exploration, which are important for learning and development.
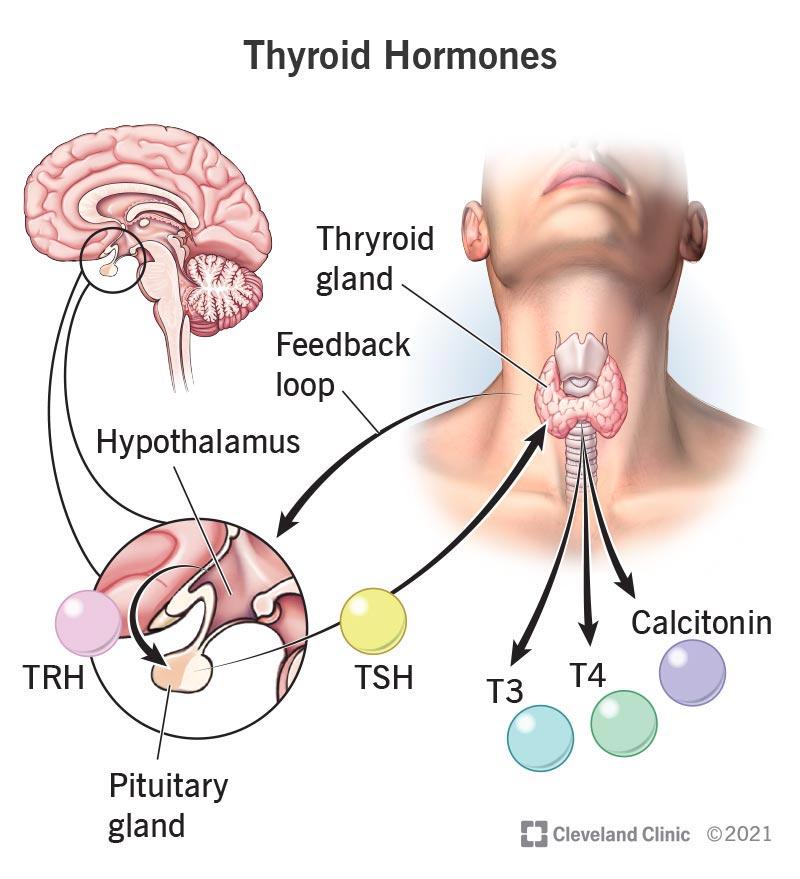
The nurse is caring for a one-month-old infant admitted for suspected congenital hypothyroidism. Which diagnostic test results should the nurse report to the healthcare provider?
Explanation
Choice A reason: Luteinizing hormone (LH) levels are not relevant for the diagnosis of congenital hypothyroidism. LH is a hormone that regulates the reproductive system and is not affected by thyroid function.
Choice B reason: Thyroxine (T4) is the main hormone produced by the thyroid gland and is essential for growth and development. Low levels of T4 indicate hypothyroidism and require treatment with thyroid hormone replacement. High levels of T4 indicate hyperthyroidism and require treatment with anti-thyroid drugs.
Choice C reason: Growth hormone (GH) levels are not relevant for the diagnosis of congenital hypothyroidism. GH is a hormone that stimulates growth and metabolism and is not affected by thyroid function.
Choice D reason: Follicle stimulating hormone (FSH) levels are not relevant for the diagnosis of congenital hypothyroidism. FSH is a hormone that regulates the reproductive system and is not affected by thyroid function.
An adolescent with a congenital heart defect is admitted for diagnostic testing with surgery scheduled in 3 days. Which intervention should the nurse implement to best support the client's psychosocial needs?
Explanation
Choice A reason: Enabling limited time for cell phone use is not the best intervention that the nurse can implement to support the client's psychosocial needs. While cell phone use can help the client stay connected with their peers and social media, it can also be a source of distraction and stress. The nurse should encourage the client to balance their cell phone use with other activities that promote their well-being.
Choice B reason: Providing an activity room to spend time with other adolescents is the best intervention that the nurse can implement to support the client's psychosocial needs. This intervention can help the client cope with the anxiety and isolation that may result from their condition and hospitalization. It can also provide an opportunity for the client to interact with other adolescents who have similar experiences and challenges, and to engage in fun and meaningful activities that enhance their self-esteem and mood.
Choice C reason: Delivering 3 meals and snacks each day upon request is not the best intervention that the nurse can implement to support the client's psychosocial needs. While it is important to maintain the client's nutrition and hydration, it is not enough to address their emotional and social needs. The nurse should also encourage the client to eat with other adolescents or family members when possible, and to express their preferences and concerns about their food.
Choice D reason: Allowing family and friends to be present during assessments is not the best intervention that the nurse can implement to support the client's psychosocial needs. While it is important to involve the client's family and friends in their care, it is not necessary to have them present during every assessment. The nurse should respect the client's privacy and autonomy, and ask for their consent before allowing others to observe or participate in their assessments. The nurse should also provide the client with opportunities to talk to their family and friends in a comfortable and confidential setting.
An infant who is developmentally delayed has a ventricular peritoneal (VP) shunt for hydrocephalus. The nurse makes a postoperative home visit to assess the child's progress. During the visit, the mother tells the nurse, "When the shunt is removed, the pressure in my baby's head will be gone." Which response should the nurse provide?
Explanation
Choice A reason: "Many infants outgrow the need for a shunt after the neonatal period." is not a correct response that the nurse should provide. This statement is false, as most infants with hydrocephalus will need a shunt for life. Only a small percentage of infants with post-hemorrhagic hydrocephalus may outgrow the need for a shunt .
Choice B reason: "The shunt will be replaced as your child grows to reduce pressure in the brain." is the correct response that the nurse should provide. This statement is true, as the shunt will need to be adjusted or replaced as the child grows to accommodate the changes in the size and shape of the head and the amount of fluid drainage. The nurse should educate the mother about the signs and symptoms of shunt malfunction and the need for regular follow-up visits.
Choice C reason: "Other pathways in the brain will drain fluid after the shunt is removed." is not a correct response that the nurse should provide. This statement is false, as the shunt is not removed unless there is a serious complication or the child no longer needs it. The shunt is a permanent device that bypasses the blocked or impaired pathways in the brain and allows the fluid to drain into the abdomen. Without the shunt, the fluid will accumulate in the brain and cause increased pressure and damage.
Choice D reason: "The shunt will have to be reinserted only if an infection or blockage develops." is not a correct response that the nurse should provide. This statement is false, as the shunt is not removed and reinserted unless there is a serious complication or the child no longer needs it. The shunt is a permanent device that stays in place unless it malfunctions or becomes infected. The nurse should educate the mother about the signs and symptoms of shunt infection and the need for prompt treatment.
An infant who has a Wilms' tumor is admitted for surgery. Which intervention should the nurse implement during the preoperative period?
Explanation
Choice A reason: Careful bathing and handling that avoids abdominal manipulation is the best intervention that the nurse can implement during the preoperative period. This is because Wilms' tumor is a rare kidney cancer that mainly affects children and can rupture or spread if touched or pressed. The nurse should avoid any unnecessary pressure on the abdomen and use gentle movements when bathing and handling the infant.
Choice B reason: Administering pain medication based on the FACES pain scale is not the best intervention that the nurse can implement during the preoperative period. This is because the FACES pain scale is a tool that helps children aged 3 and older to communicate their pain level by pointing to a face that matches their pain. However, the infant in this scenario is too young to use this scale and may not be able to express their pain verbally. The nurse should use other methods to assess the infant's pain, such as observing their behavior, vital signs and facial expressions.
Choice C reason: Including the prone position in the every 2 hour turning schedule is not the best intervention that the nurse can implement during the preoperative period. This is because the prone position, which is lying on the stomach, can increase the risk of rupture or spread of the tumor. The nurse should avoid placing the infant in this position and instead use other positions that are comfortable and safe for the infant.
Choice D reason: Giving antiemetic medications to prevent nausea and vomiting is not the best intervention that the nurse can implement during the preoperative period. This is because antiemetic medications are drugs that prevent or treat nausea and vomiting caused by chemotherapy, radiation therapy or surgery. However, the infant in this scenario has not yet undergone any of these treatments and may not have any symptoms of nausea and vomiting. The nurse should only give antiemetic medications if the infant shows signs of nausea and vomiting or if prescribed by the doctor.
An infant born 2 days ago has not passed a meconium stool and begins to vomit bilious secretions. Which action should the nurse take first?
Explanation
Choice A reason: Measuring abdominal circumference is not the first action that the nurse should take. This is because abdominal circumference is not a reliable indicator of bowel obstruction or perforation, which are possible complications of meconium ileus. Measuring abdominal circumference may also delay more urgent interventions, such as fluid resuscitation and decompression.
Choice B reason: Gathering supplies for an intravenous (IV) infusion is the first action that the nurse should take. This is because the infant is at risk of dehydration, electrolyte imbalance, and shock due to vomiting and bowel obstruction. The nurse should prepare to administer IV fluids, antibiotics, and blood products as ordered by the healthcare provider.
Choice C reason: Monitoring strict urinary output is not the first action that the nurse should take. This is because urinary output is not the most sensitive indicator of fluid status in infants, especially those with renal insufficiency or oliguria. Monitoring urinary output may also delay more urgent interventions, such as fluid resuscitation and decompression.
Choice D reason: Preparing for anorectal manometry is not the first action that the nurse should take. This is because anorectal manometry is a diagnostic test that measures the pressure and function of the anal and rectal muscles. It is not indicated for infants with suspected meconium ileus, which is a mechanical obstruction of the bowel by thick and sticky meconium. Preparing for anorectal manometry may also delay more urgent interventions, such as fluid resuscitation and decompression.
The nurse is conducting an admission assessment of an infant with heart failure who is scheduled for repair of restenosis of coarctation of the aorta that was repaired 4 days after birth. Findings include blood pressure higher in the arms than the lower extremities, pounding brachial pulses, and slightly palpable femoral pulses. Which pathophysiologic mechanism supports these findings?
Explanation
Choice A reason: The lumen of the aorta reduces the volume of blood flow to the lower extremities is the correct pathophysiologic mechanism that supports the findings. This is because coarctation of the aorta is a congenital condition that causes a narrowing of the aorta, usually near the ductus arteriosus. This results in increased resistance to blood flow from the heart to the lower body, leading to higher blood pressure and stronger pulses in the upper extremities and lower blood pressure and weaker pulses in the lower extremities.
Choice B reason: The aortic semilunar valve obstructs blood flow into the systemic circulation is not the correct pathophysiologic mechanism that supports the findings. This is because the aortic semilunar valve is located at the base of the aorta and prevents blood from flowing back into the left ventricle. If the valve is obstructed, it would cause aortic stenosis, which is a different condition from coarctation of the aorta. Aortic stenosis would cause symptoms such as chest pain, shortness of breath, and fainting.
Choice C reason: The pulmonic valve prevents adequate blood volume into the pulmonary circulation is not the correct pathophysiologic mechanism that supports the findings. This is because the pulmonic valve is located at the base of the pulmonary artery and prevents blood from flowing back into the right ventricle. If the valve is obstructed, it would cause pulmonic stenosis, which is a different condition from coarctation of the aorta. Pulmonic stenosis would cause symptoms such as cyanosis, fatigue, and heart murmur.
Choice D reason: An opening in the atrial septum causes a murmur due to a turbulent left to right shunt is not the correct pathophysiologic mechanism that supports the findings. This is because an opening in the atrial septum is a defect in the wall that separates the two upper chambers of the heart. It would cause a condition called atrial septal defect, which is different from coarctation of the aorta. Atrial septal defect would cause symptoms such as difficulty breathing, frequent respiratory infections, and heart palpitations.
You just viewed 10 questions out of the 40 questions on the HESI RN Med Surg Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

